2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors Barbara S. Apgar MD, MS Professor Emerita of Family Medicine Michigan Medicine University of Michigan Ann Arbor, Michigan

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2019ASCCPRisk-BasedManagementConsensusGuidelinesforAbnormalCervicalCancerScreeningTestsand
CancerPrecursors
BarbaraS.ApgarMD,MS
ProfessorEmeritaofFamilyMedicineMichiganMedicine
UniversityofMichiganAnnArbor,Michigan
Disclosures
• ASCCPCasesoftheMonthCommitteeChair(current)• ASCCPBoardofDirectors,GuidelinesCommittees,DirectorofComprehensiveColposcopyCourses(former)
• NofinancialcompensationfromASCCPapp
• Images:ApgarB,BrotzmanG,SpitzerM.IntegratedTextandAtlas,2004,2008.ElsevierPublishing.
• Slides:CompilationofASCCPslides/algorithmsandpersonalcollection• AllslidedataarefromPetersRetalunlessotherwisespecified
Objec&ves
• Understandthedifferencesbetweenthe2012and2019ASCCPguidelines
• Reviewthescien=ficevidenceusedtoconstructthe2019guidelines.
• Summarizetheprinciplesofthe2019guidelines.• UnderstandhowtointerprettheresultsontheASCCPapp.
Equalmanagementforequalrisk
Managementisbasedonrisk,notresults
Na=onalCancerIns=tuteandASCCPcollaboratedonaformalconsensusguidelineprocessin2001,2006,2012andnowin2019.TheroleofNCIepidemiologistsandsta=s=cianswhospecializeincervicalscreeningistoprovideepidemiologicevidenceregardingtestperformancebasedonNCIandotherresearch.TheroleofASCCPistoconveneandconductconsensusconferencesbringingtogetherorganiza=onsand“stakeholders”tocreatetheguidelines.Goalwastoproduceconsensusrecommenda=onsbasedonrisk,toachievealongshelf-lifeforthe2019versionbeforeanotherconsensusconferenceisneededdespitenewcompe=ngtestsandstrategies.18–monthcollabora=veeffortfor2019guidelines.
NCI sta&s&cians had input from many sources
• Therisk-basedapproachprovedadequateformostclinicalscenariosexceptforwomeninspecialpopula=onsandtopicsbesthandledbyconven=onalmanagementalgorithms,guidedbyexpertopinion.
• Risk-basedapproachwastranslatedinto“management”throughuseofclinicalac'onthresholdsthatweredeterminedbytheconsensusgrouprepresen=ngthe19organiza=ons.
• Determinedtrade-offsinbenefitsandharms.
The new risk-based management
consensus guidelines use RISK and CLINICAL ACTION THRESHOLDS to determine the appropriate
course of management of cervical cancer screening abnormali&es.
NCIHPVepidemiologistsandsta=s=cianses=matedtherisksofCIN3+byHPVtests,cytology,pastscreeningtestsand
colposcopicbiopsyresults.
Tables of risk es&mates were generated from a prospec&ve longitudinal cohort of > 1.5 million pa&ents followed for over a
decade at Kaiser Permanente Northern California (KPNC)
Allowedobserva=onofdetaileddataandfollow-upofCIN2andCIN3,AISandcancer.
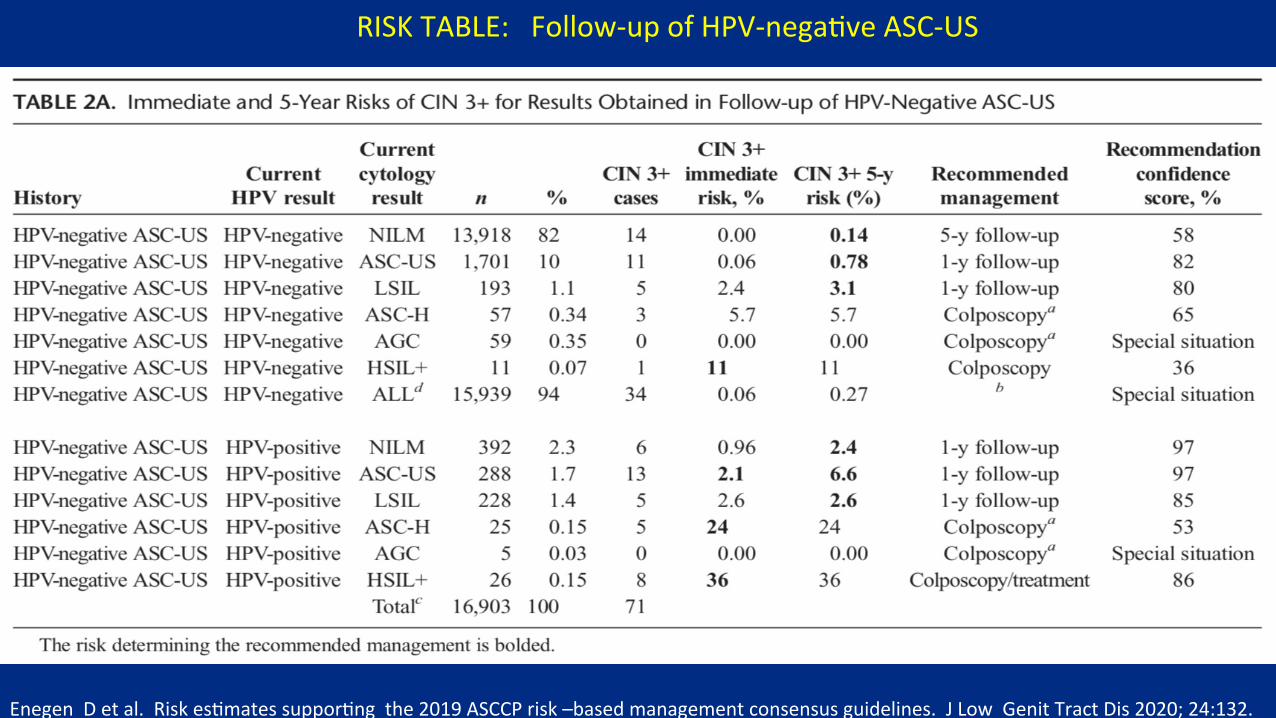
RISKTABLE:Follow-upofHPV-nega=veASC-US
EnegenDetal.Riskes=matessuppor=ngthe2019ASCCPrisk–basedmanagementconsensusguidelines.JLowGenitTractDis2020;24:132.
Adherence to cervical cancer guidelines
• Significantdifferencebetweenclinician’sdecisionsandactualguidelinestheybelievedtheywerefollowing.
• Confusionandoverloadmaycontributetononadherencebyclinicians.• Skepticismofutilityofguidelines.
• Mayreverttooverscreeningto“playitsafe”.• Maybelievethatguidelinesareriskyandinappropriate.• Needtoexplainguidelinestoskepticalpatientsevenifbelieveguidelinesareauthoritative
• Maybelievebenefitsandharmsarenotbalanced.
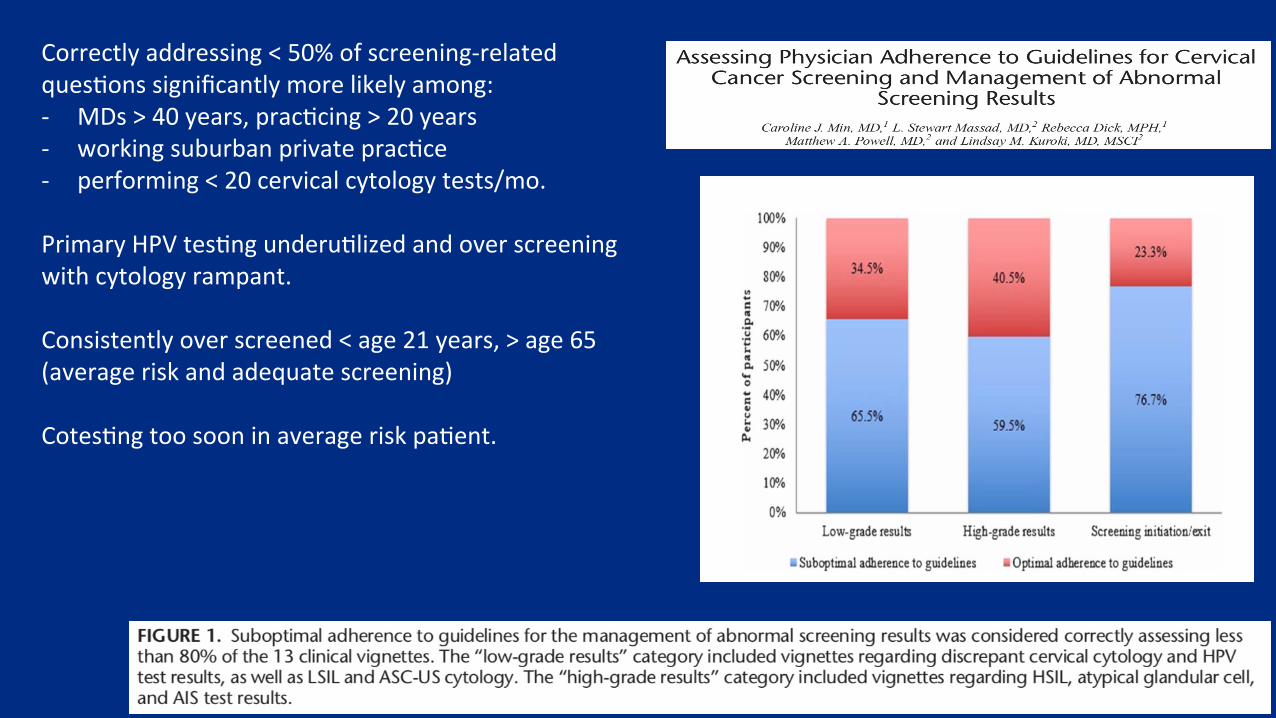
Correctlyaddressing<50%ofscreening-relatedques=onssignificantlymorelikelyamong:- MDs>40years,prac=cing>20years- workingsuburbanprivateprac=ce- performing<20cervicalcytologytests/mo.PrimaryHPVtes=ngunderu=lizedandoverscreeningwithcytologyrampant.Consistentlyoverscreened<age21years,>age65(averageriskandadequatescreening)Cotes=ngtoosooninaverageriskpa=ent.
Adherencetocervicalcancerguidelines
• Translatingevidence-basedinterventionsintoclinicalpracticeisincrediblycomplexandchallenging(84%ofcliniciansthoughtguidelinesunclear).
• Howtoimprove:
• Capitalizeuseoftechtoolstoincreaseadherence.• Decreasealgorithmuse(risk,notresults).
Whywererevisionstothe2012guidelinesneeded?
• Revisionmotivatedbythecomplexityofthe2012guidelinesasnewtestsbecameavailable.
• Toomany“acceptable”choicestocontinueasbefore.• MANYmorealgorithmswouldberequiredfornewtestslikeextendedgenotypingandinfluenceofpast-historyoncurrentresults.
Whywererevisionstothe2012guidelinesneeded?
• SufficientdatabecameavailableintheUSshowingthatincorporationoftherisk-basedapproachcouldprovidemoreappropriateandpersonalizedmanagementforthepatient.
• Basedoncurrentresultsandpasthistory.
• Newrecommendationsforcervicalcancerscreeningintroducedsince2012.
• PrimaryHPVtestingasascreeningoptionforpatients25yearsandolder.
Whywererevisionstothe2012guidelinesneeded?
• 2012guidelinespresentedaconceptualbreakthroughinrisk-basedmanagement.
• Retainedacontinuedrelianceoncomplicatedalgorithmswithoutincorporatingpastscreeninghistory.
• 2019guidelinesreflectamorenuancedunderstandingofhowpriorresultsaffectrisk.
• MorevariablesavailableincludingthenaturalprogressionofHPV.
Comparison of 2012 and 2019 guidelines
• Changefromtestresults-basedalgorithms(2012)• “ColposcopyisrecommendedforpatientswithHPV-positiveASC-US,LSIL”.
• Changetorisk-basedguidelines(2019)
• “Colposcopyisrecommendedforanycombinationofhistoryandcurrenttestresultsyieldinga4.0%orgreaterprobabilityoffindingCIN3+.”
2019guidelinesemphasizereductionofinvasiveprocedureswhilemaintaininghighstandardsofcancerprevention
• Colposcopicbiopsyconfirminglow-gradeornormalhistologyreducestheestimatedriskofhavingprecancer/cancerinthenext3years.
• AllowspatientswithHPV+ASC-USorLSILattheir1-yearfollow-upvisitaftercolposcopicbiopsyshowingnormalorlow-gradehistologytoreturnforrepeatHPV-basedtestingin1moreyear,ratherthanimmediatelyreturntocolposcopy.

TREATwomenwithhighrisk
ofdevelopinginvasivedisease
OBSERVEwomenwhoarenotathighriskofdevelopinginvasive
diseaseand
protectthemfromover-treatment
2012PrinciplesCarriedForward
• Timelydetectionandtreatmentofthehighestgradeofprecancers(CIN3/AIS)arethebenchmarkusedforallguidelines.
• Guidelinesapplytoallindividualswithacervix.
• Includestransgendermenwithacervix,includingthosewhohaveundergonesupracervicalhysterectomy.
2012PrinciplesCarriedForward
Guidelinesapplytoasymptomaticpatientswhorequiremanagementofabnormalcervicalscreeningtestresults.
• Abnormaluterineorvaginalbleedingoravisiblyabnormal-appearingcervixrequireappropriatediagnostictestingtoR/Ocancer.
• Balancingbenefitsandrisks.• Guidelinesmaximizecervicalcancerpreventionandminimizeharmsfromovertreatmentandovertesting.
Changesfrom2012GuidelinesPatientswithminorabnormalities
• Colposcopycanbedeferredforcertainpatients.
• PatientswithLSILorASC-UScytologycandefercolposcopyifresultswereprecededby:
• negativescreeningwithHPV-basedtestingwithinthepast5years
• colposcopywhereprecancerwasnotfoundinthepastyear.• Pasthistoryisimportant!
• Newdataindicatethatfollow-upinoneyearissafe.
Changes from 2012 Guidelines Treatment
• ExcisionaltreatmentispreferredtoablativetreatmentforhistologicHSIL(CIN2or3)intheUS.• Excisionisalsorecommendedforadenocarcinomainsitu(AIS)
• ObservationispreferredforLSIL(CIN1)
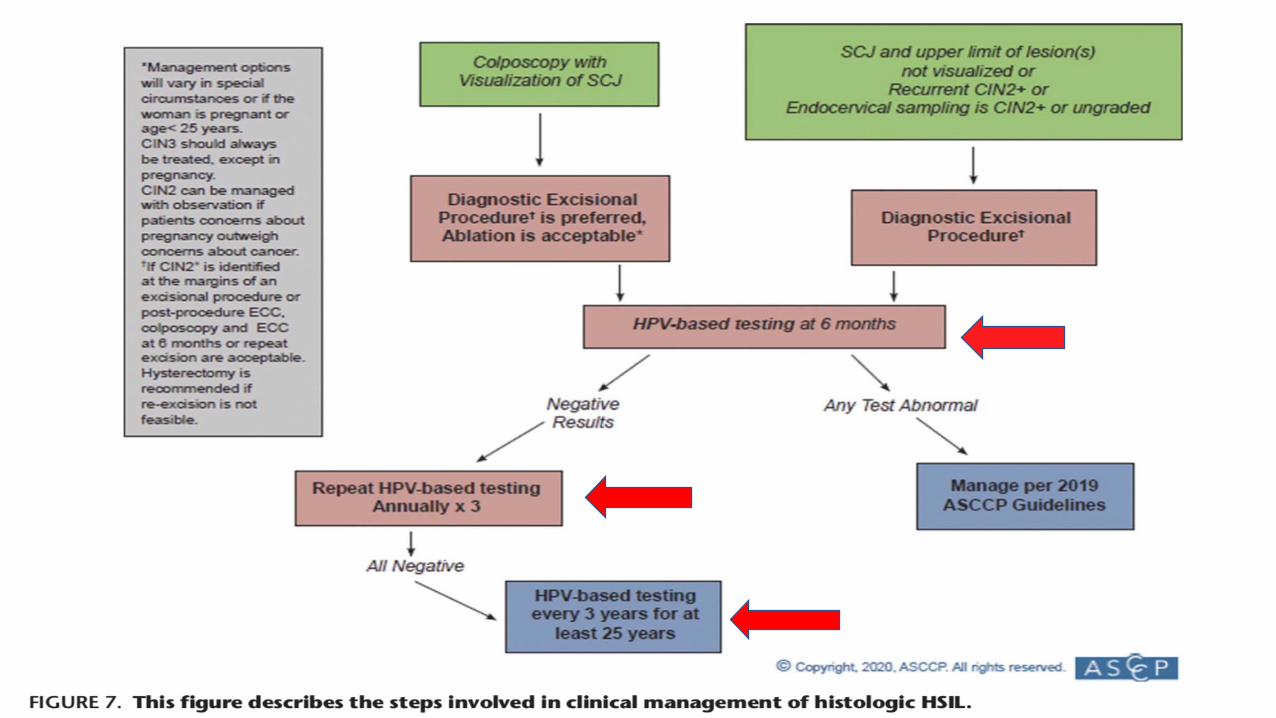
ManagementofwomenwithBiopsy-confirmedHistologicHSIL(CIN2and3)
2012EitherExcisionorAblationofT-zone
Isacceptable
2019DiagnosticExcisionalProcedureisPreferredAblationisacceptable
Changes from 2012 Guidelines Treatment guidelines divided into pa&ents
younger than age 25 years or 25 years or older
• 2012guidelinesconsideredpatientsages21-24tobeaspecialpopulation.Term“youngwomen”isnolongerused(2019).
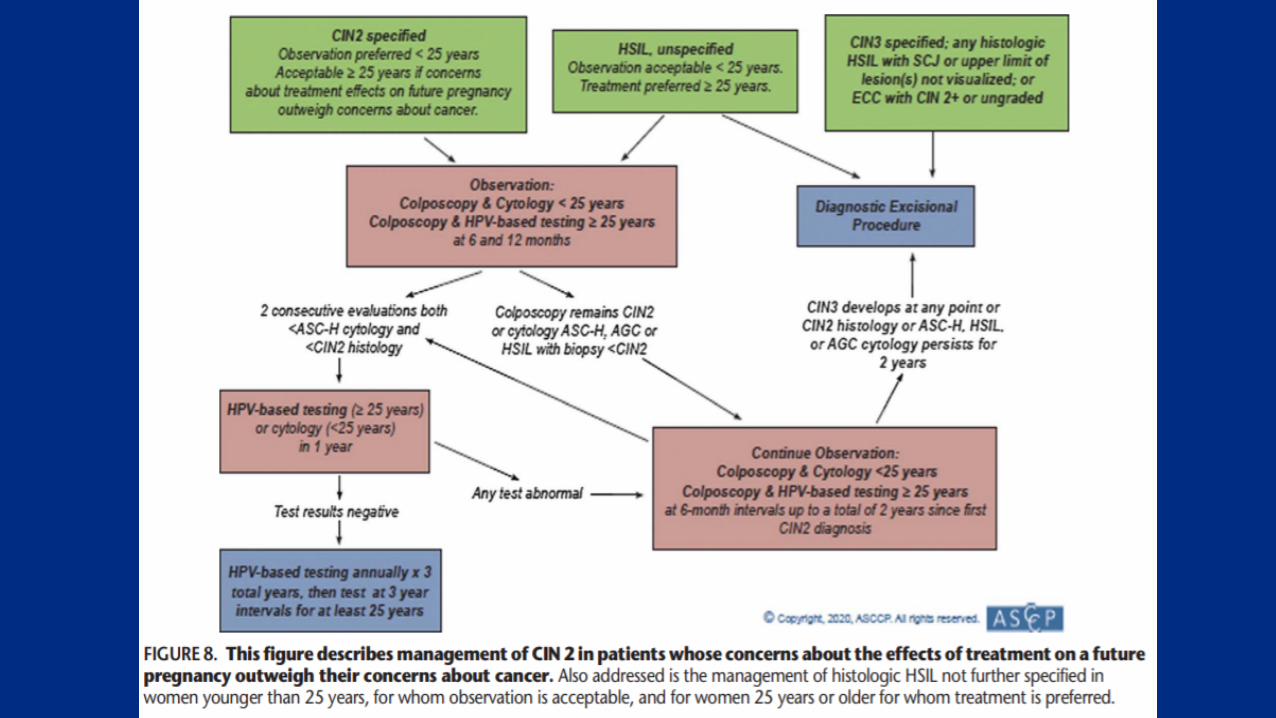
• 2019guidelinesrecognizethatpatientsofvariousagesareconcernedaboutthepotentialimpactoftreatmentonfuturepregnancyoutcomes.
• Appwillaskyouifpatientisconcernedaboutfuturepregnancy.
• Shareddecision-makingiscriticalwhenpatientsconsidertreatmentofhistologicHSIL(CIN2)andabnormalitieswithalowlikelihoodofunderlyingCIN3+suchashistologicLSIL(CIN1).
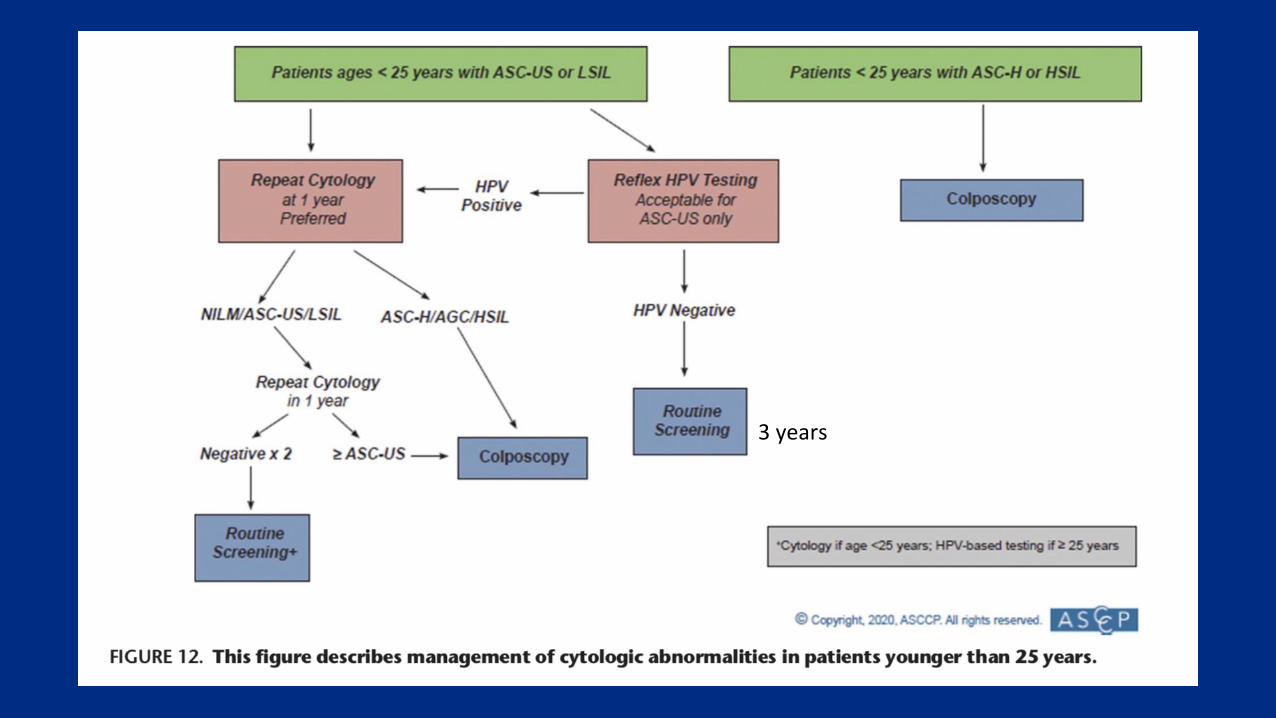
3years
2019Guidelines:Patientsolderthan65years
• Approximately20%ofcervicalcancersoccurinpatients>65yrs.
• Samemanagementaspatientsaged25to65yearsifscreeningisperformedandabnormalitiesfound.
• Dataonprognosticvalueofspecificscreeningresultsislimitedinolderpatients.
Ifpatientisundergoingsurveillanceforabnormalresultsortreatmentforprecancer,stoppingsurveillanceisunacceptableifpatientishealthybut
acceptableiflimitedlifeexpectancy.
2019Specialpopulations:Immunocompromised• HIV***
• Cervicalcancerscreeningguidelinessupportedbypublications.• Literatureislimitedforconditionsthatsuppresscell-mediatedimmunitybutwhichhavebeenassociatedwithvirallyinducedcancers,includingcervicalcancer.
• Solidorganorstemcelltransplant***• Systemiclupuserythematous• Inflammatoryboweldisease• Rheumatologicdiseaserequiringimmunosuppressivetx
• Lackofdata(KPNC)precludesriskestimationforimmunosuppressed.
RiskofCIN3+amongHIV+women
• HIV+womenhavehigherriskofCIN3+withlow-gradecytologicabnormalities.
• SexuallyactiveHIV+patientswithHPVhaveahighrateofprogressiontoprecancer.
• HighprevalenceofHPVbeforeage30years.• HigherratesofacquiringHPVandlowerratesofclearingit,thanHIV-negativewomen.
• HIV+womenare2.5timesmorelikelytohaveanHPVinfectionprogresstoHSILthanHIV-negativepatients.
LiuG,etal.HIV-posi=vewomenhavehigherriskofhumanpapillomavirusinfec=on,precancerouslesions,andcervicalcancer.AIDS.2018;32(6)HilaryKetal.CancerEpidemiolBiomarkersPreven=on2017;26(6):886.
ImmunocompromisedwomenwithoutHIV
• UsethesamecervicalcancerscreeningandabnormalresultmanagementguidelinesdevelopedforwomenwithHIV.
• Screeningshouldbeginwithin1yearoffirstinsertionalsexualactivityandcontinuethroughoutpatient’slifetime.
• Annuallyfor3years.• Every3years(cytologyonly)untilageof30years• Continuingwithcytologyaloneorcotestingevery3yearsatage30.
2019guidelinesforimmunocompromisedpatientsofanyage
• ColposcopyreferralrecommendedforallwomenwithcytologyresultsofHPV+ASC-US.
• ForallcytologyresultsofLSILorworse,refertocolposcopyregardlessofHPVtestsifdone.
2012 and 2019 Guidelines: Pregnancy
• Pregnancywasconsideredaspecialpopulationwheremanagementoptionsweighedrisktomotherandfetusversusriskofmissingcancer(2012guidelines).
• Rateorriskofprogressiontocervicalcancerisnotdifferentinpregnancy.
• 2019guidelinesdonotlistpregnancyasaspecialpopulation.• Datainpregnancyarelimited.
• Norandomized-controlledtrials.
2019 Guidelines: Pregnancy
• ManagementofabnormalscreeningresultsusesameClinicalActionThresholdsforsurveillanceandcolposcopy/treatmentestablishedfornon-pregnantwomen.
• EMB,ECCandtreatmentwithoutbiopsyareunacceptable.Ectocervicalbiopsiesappeartobesafe.
• Colposcopyperformedbyanexperiencedclinicianpreferred.• Colposcopyexperienceisknowntoaffecttheabilitytodistinguishcancersfrompregnancy-relatedchanges.
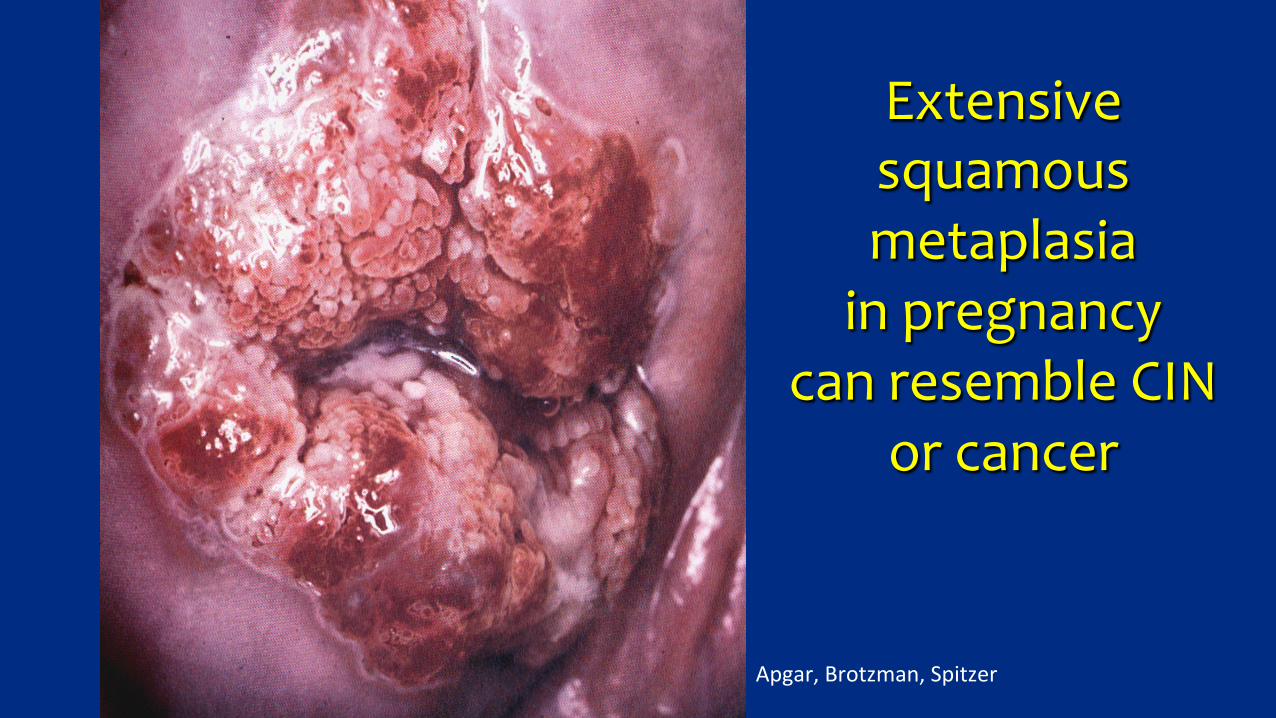
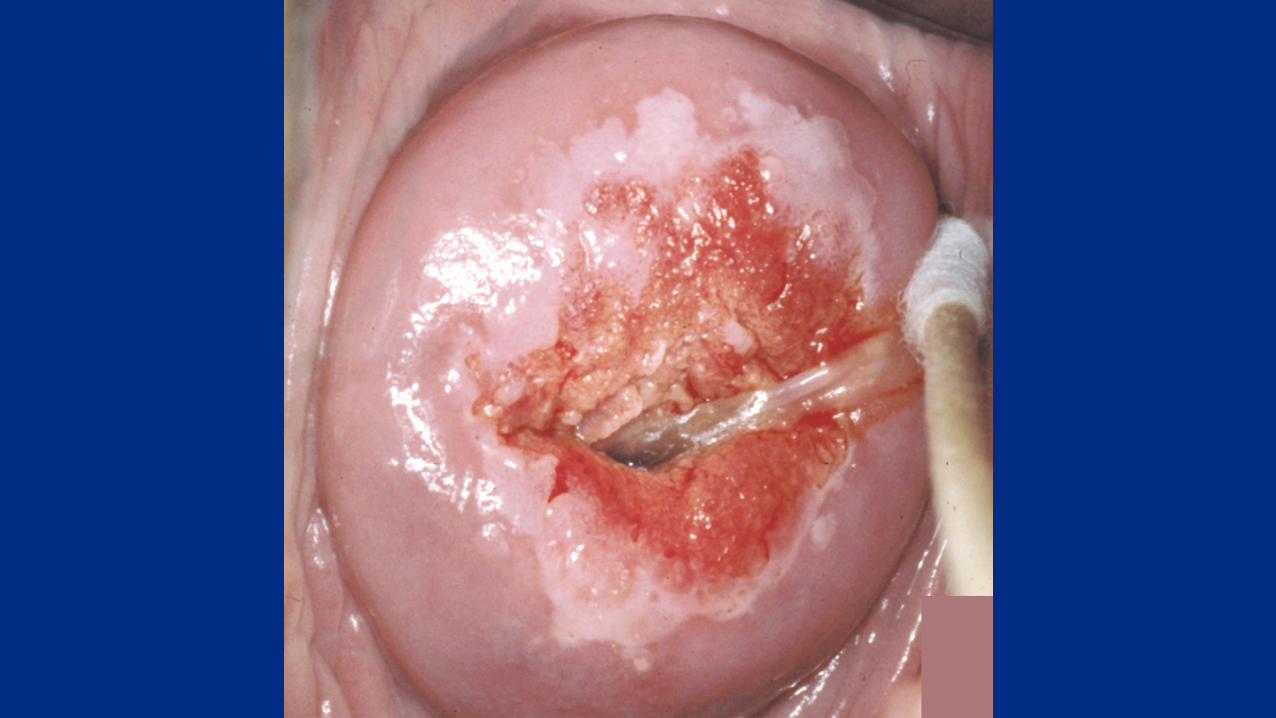
Extensivesquamousmetaplasiainpregnancy
canresembleCINorcancer
Apgar,Brotzman,Spitzer
2019 Guidelines: Pregnancy • 2019guidelinesallowdeferralofcolposcopyforminorabnormalitiesinwomenwithpriornegativeHPVtestingorcolposcopy.
• IfHSIL(CIN2or3)isdiagnosedatthefirstcolposcopy,surveillance(colposcopyandcytology/HPVdependingonage)ispreferredevery12-24weeks.
• Repeatbiopsyisrecommendedifinvasionissuspectedortheappearanceofthelesionworsens.
• Deferringcolposcopytothepostpartumperiodisacceptable.• Notearlierthan4weeksafterdelivery.
DiagnosticexcisionfordiagnosisortreatmentofHSIL(CIN2,3)shouldbedeferreduntilafterdeliveryunlessinvasivediseaseisdetectedorissuspected.
Excludeinvasionbycolposcopyandbiopsy.
Strongsuspicionofinvasionrequiresadiagnostic
excisiontoexcludeinvasionanddeterminedepthofinvasion.
2019GuidingPrinciple#1
• ThelongeranHPVinfectionhasbeenpresent,the
highertheriskofpre-cancerandcancer.
• Timematters.• Typematters(HPV16mostdangerous).
RiskisgreatlyreducedifpriorscreeningroundwasHPV-negative.
WhatisHPV-basedtesting?PrimaryHPVtestingorcotesting
• MostHPVDNAassaysapprovedforadjuncttestingwithcytology.
• subsetofassaysapprovedforHPVtestingalone,withoutcytology.
• UseofprimaryHPVscreeningwilllikelyincreaseinthefuture.
• Notalllabsequippedforitnow.• HPV16/18+testshavehighestriskofCIN3andoccultcancers.
• Additionaldiagnosticproceduresrecommendedforall+tests.
PrimaryHPVscreening
FDA-approvedforpatients25yearsandolder
Primary HPV tes&ng and reflex tes&ng
• ReflexcytologyrecommendedforallHPV+primaryscreeningresults,regardlessofHPVgenotype.
• Ifreflextes=ngnotfeasible,pa=entsshouldgodirectlytocolpo.• Collectcytologyatcolposcopytoprovidefurtherinfoforrisk-basedmanagement.
• Combiningahighspecificitytest(HSILcytology)withahighsensi=vitytest(HPVtest)allowsmoreprecise,risk-basedmanagement.
• Expeditedtreatmentonlypossibleifcytologyisperformed.
2019 guidelines prefer HPV tes&ng for follow- up
• SurveillancewithcytologyaloneisacceptableonlyifHPV-basedtes=ngisnotavailable.
• Cytologyislesssensi=vethanHPVtes=ngfordetec=onofprecancerandhastobeperformedmoreolen.
• Cytologyisrecommendedat6-monthintervalswhenHPV-basedtes=ngisrecommendedannually.
• Cytologyisrecommendedannuallywhen3-yearintervalsarerecommendedforHPV-basedtes=ng.
SurveillancewithHPV-basedtestingafterTreatmentCIN2or3
• Con=nueHPV-basedtes=ngat3-yearintervalsforatleast25years.• Con=nuedsurveillanceat3-yearintervalsbeyond25yearsisacceptableifpa=ent’slifeexpectancyandabilitytobescreenedarenotcompromised.
• 2012guidelinesrecommendedreturnto5-yearintervalsanddidnotspecifywhenscreeningshouldstop.
• Newevidenceindicatesthatriskremainselevatedforatleast25years
• Noevidencethattreatedpa=entseverreturntorisklevelscompa=blewith5-yearintervals.
2019guidelinesalignmanagementrecommendationswithcurrentunderstandingofHPVnaturalhistory
• CurrentHPVtestresults(themostimportantpredictionfactorofCIN3+)arenecessaryformanagement.
◆ IfoncogenicHPVispersistent,theriskofcervicalcancerisincreasedsubstantially.◆ Longerpersistence=greaterrisk.
FindingcarcinogenicHPVtypesdoesnot
provideadiagnosisofCIN3orcancer
ItidentifiesagroupofwomeninwhomCIN3+ismorelikely
WomentestingnegativeforoncogenicHPVhaveextremelylowriskofdevelopingcervicalcancer
over5years(KPNC)
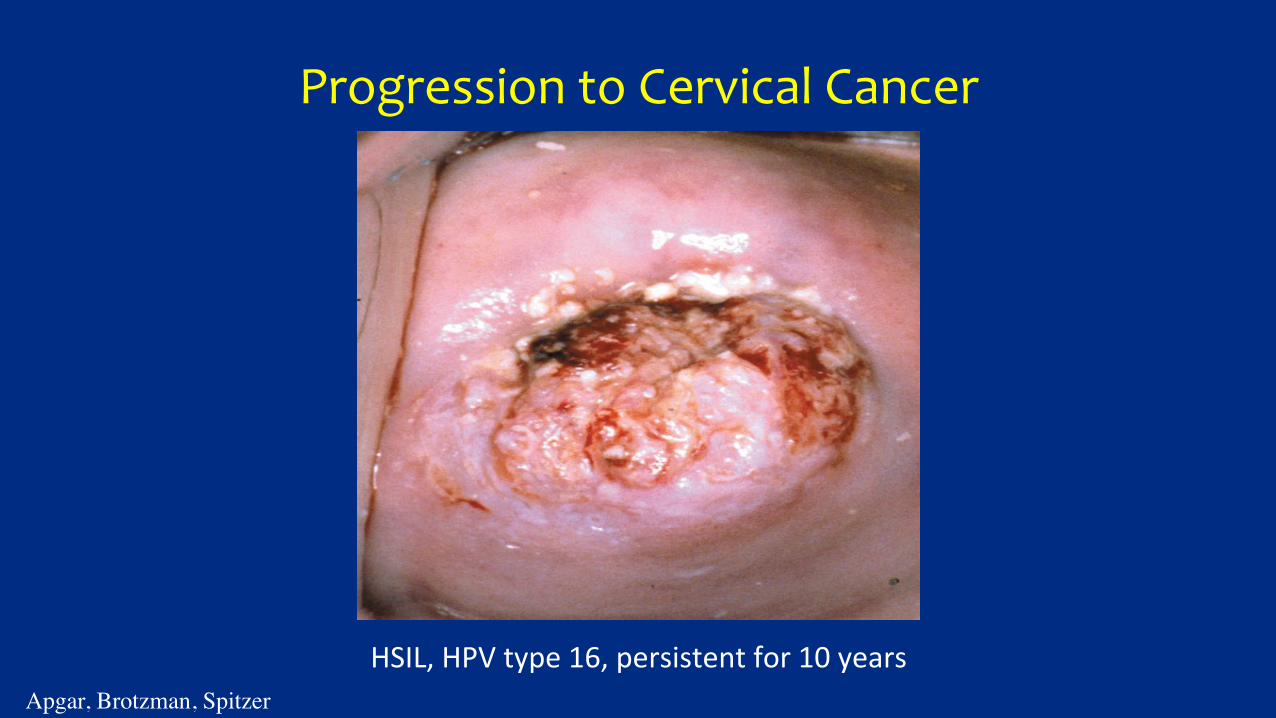
ProgressiontoCervicalCancer
HSIL,HPVtype16,persistentfor10years
Apgar, Brotzman, Spitzer
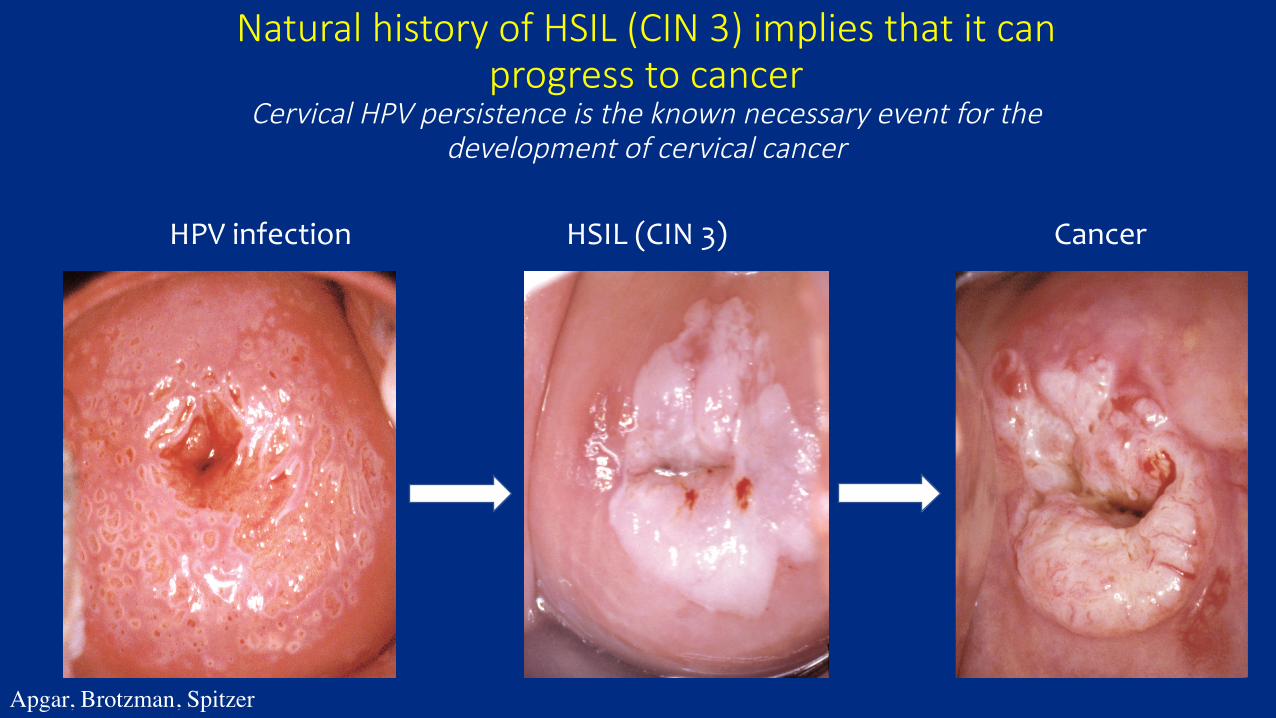
◆ Natural history of HSIL (CIN 3) implies that it can
progress to cancerCervical HPV persistence is the known necessary event for the
development of cervical cancer HPVinfectionHSIL(CIN3) Cancer
Apgar, Brotzman, Spitzer
ΗΠς ανδ περσιστενχε: µετα-αναλψσισ• AssociationsbetweenHPVpersistenceandCIN2+werestrongerwhenpersistence>12months.
• HPVpersistencestronglyandpositivelyassociatedwithallgradesofCIN.
• AssociationsstrongerforCIN2/3+thanCIN1.• Emphasizedimportanceofpersistenceasaclinicalmarker.
• Long-termHPVpositivityclearlyassociatedwithneoplastictransformation.
KoshiolJetal.AmJEpidemiol2008;168:123-137.
2019GuidingPrinciple#2Personalizedrisk-basedmanagementispossible
• Recommendationsof1,3,5yearsurveillance,colposcopyortreatmentcorrespondtoarangeofriskforCIN3+calleda“ariskstratum”.• determinedbycurrentresultsandpasthistory.
• Thelowerthresholdofeachriskstratum,calledtheClinicalActionThreshold,definesthelevelatwhichthemanagementchangestoanotherlevel.
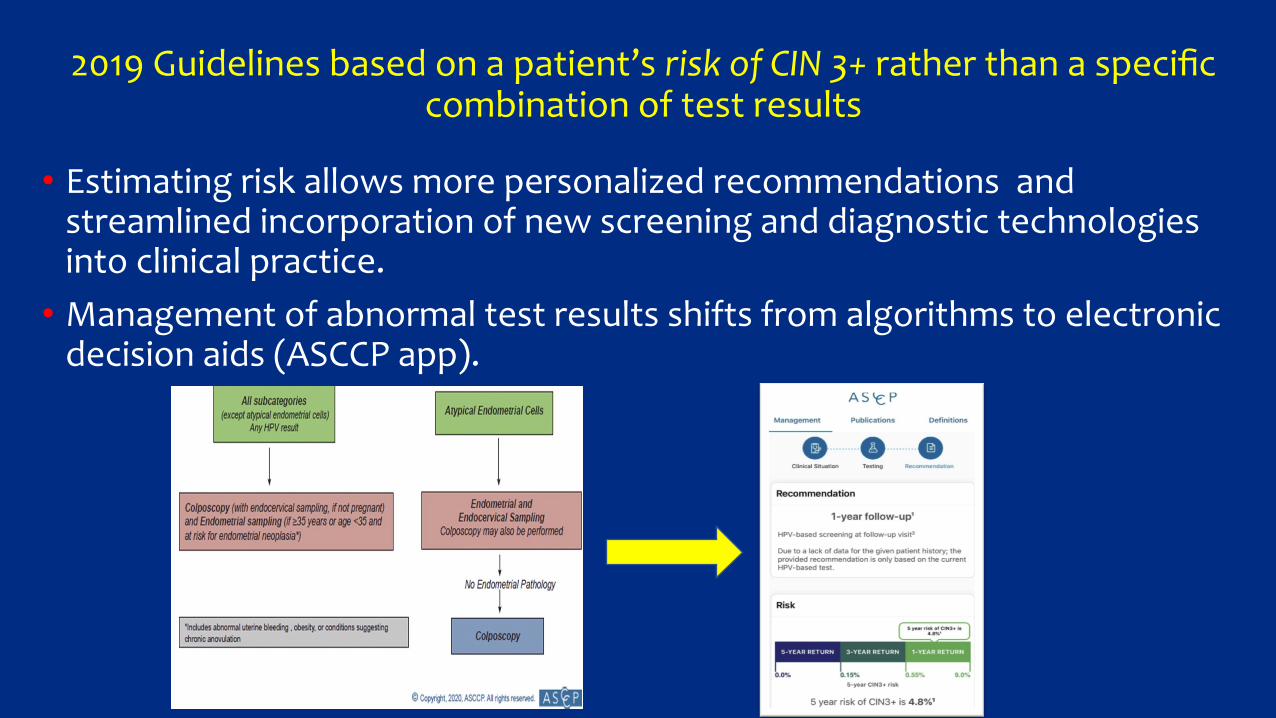
2019Guidelinesbasedonapatient’sriskofCIN3+ratherthanaspecificcombinationoftestresults
• Estimatingriskallowsmorepersonalizedrecommendationsandstreamlinedincorporationofnewscreeninganddiagnostictechnologiesintoclinicalpractice.
• Managementofabnormaltestresultsshiftsfromalgorithmstoelectronicdecisionaids(ASCCPapp).
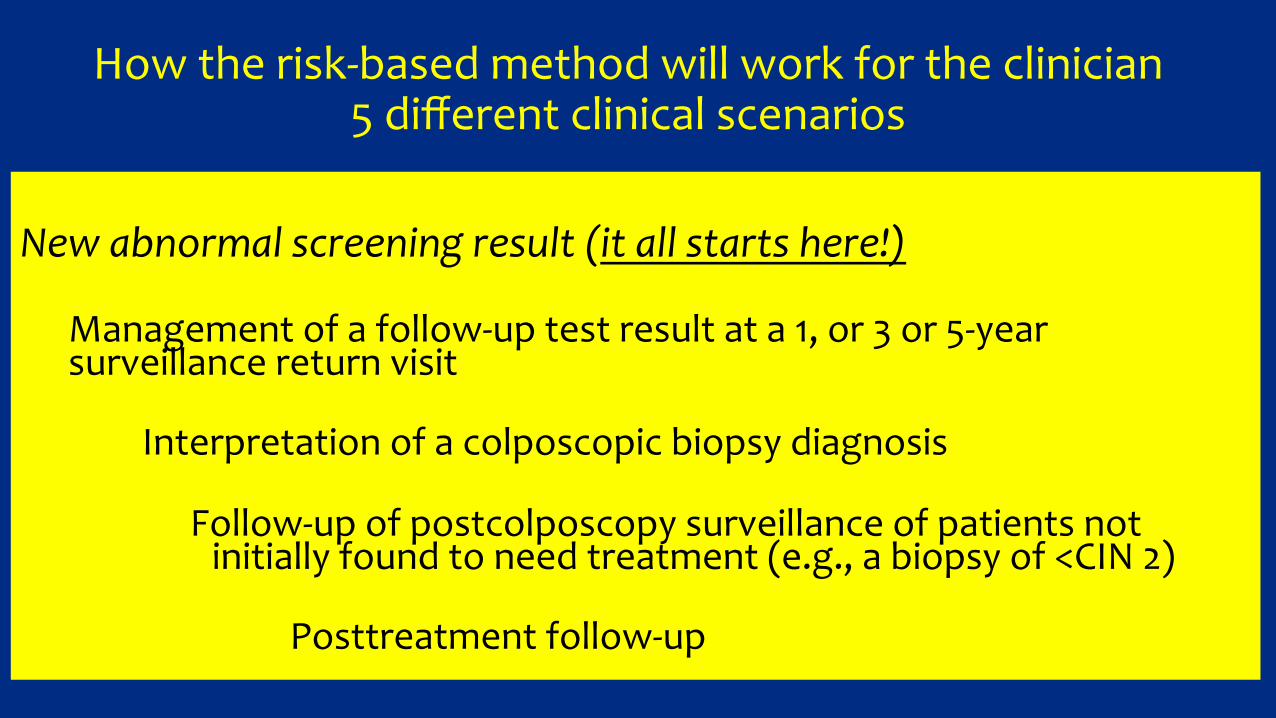
Howtherisk-basedmethodwillworkfortheclinician5differentclinicalscenarios
Newabnormalscreeningresult(itallstartshere!)
Managementofafollow-uptestresultata1,or3or5-yearsurveillancereturnvisit
Interpretationofacolposcopicbiopsydiagnosis
Follow-upofpostcolposcopysurveillanceofpatientsnotinitiallyfoundtoneedtreatment(e.g.,abiopsyof<CIN2)
Posttreatmentfollow-up
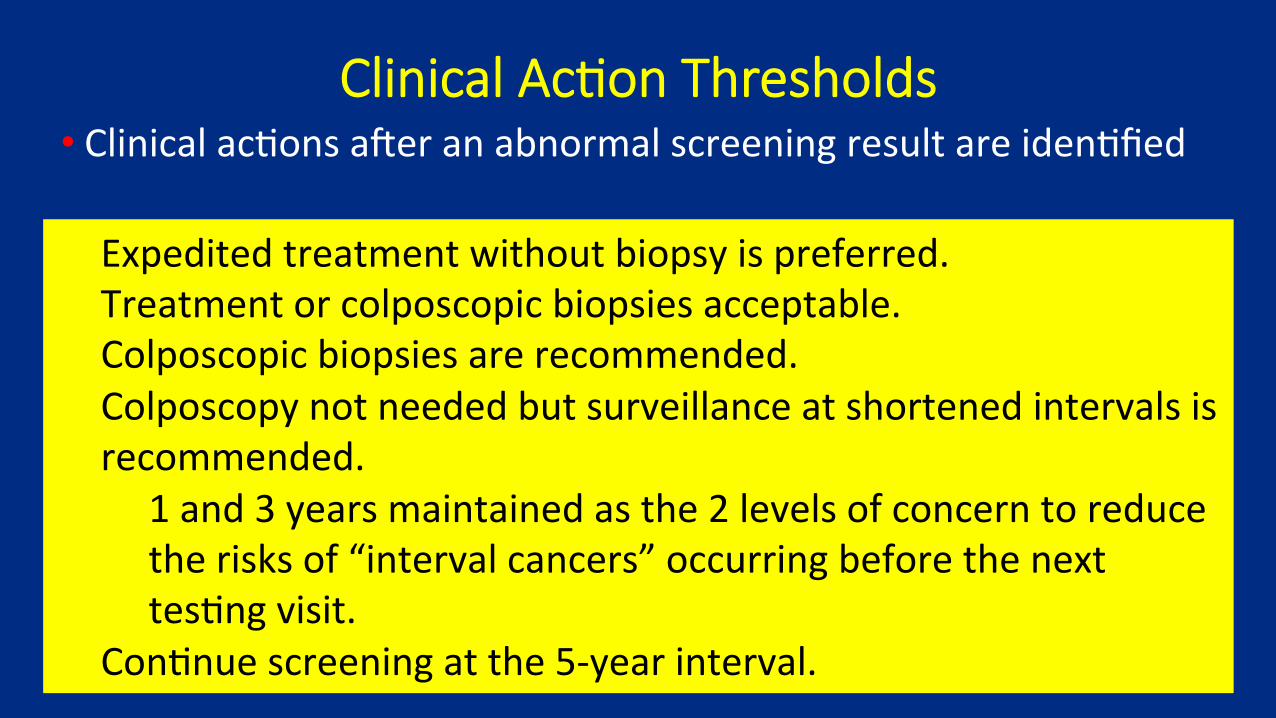
Clinical Ac&on Thresholds • Clinicalac=onsaleranabnormalscreeningresultareiden=fied
Expeditedtreatmentwithoutbiopsyispreferred.Treatmentorcolposcopicbiopsiesacceptable.Colposcopicbiopsiesarerecommended.Colposcopynotneededbutsurveillanceatshortenedintervalsisrecommended.
1and3yearsmaintainedasthe2levelsofconcerntoreducetherisksof“intervalcancers”occurringbeforethenexttes=ngvisit.
Con=nuescreeningatthe5-yearinterval.
Pa&ent will likely aYend >1 management visit aZer ini&al abnormal screening results
• Mostvisitswillinvolvecommon,benignandminorcytologicabnormali5es.
1.Thecommonini=alvisitsthataremainlyminorabnormali=esarehandledbyuseofrisktablesandclinicalac=onthresholds.
• Postcolposcopymanagementdecisionsareabout½asfrequentasini=almanagementvisits.
2.Treatmentandposoreatmentvisitsareuncommon(1/10thasfrequentasini=almanagementvisits)butareimportantforpreven=ngcancer.
Managementafteranabnormalscreeningresult
• Recommendationsforcolposcopy,treatmentorsurveillancewillbebasedonthepatient’sriskofCIN3+asdeterminedby:
• Currentresults• Pasthistory(includingunknownhistory)
• CurrentHPVtestresults(themostimportantpredictionfactorforCIN3+)arenecessaryformanagement.
• Thesamecurrenttestresultsmayyielddifferentmanagementrecommendationsdependingonthepasttestresults.
2019Guidelines:CurrentResultsandHistory
• 2centralquestionsunderlieriskestimates.
• Whatarethecurrentresults?• Resultsforwhichtheclinicianisseekingguidance:anHPVtestorcotestresultoracolposcopy/biopsyresult.
• Whatpastresults(notedunderhistory)affecttheriskestimateforthecurrentresults?
• DocumentednegativecytologyprovidesrelativelylessreductioninriskcomparedwithanegativeHPVorcotestashistory.
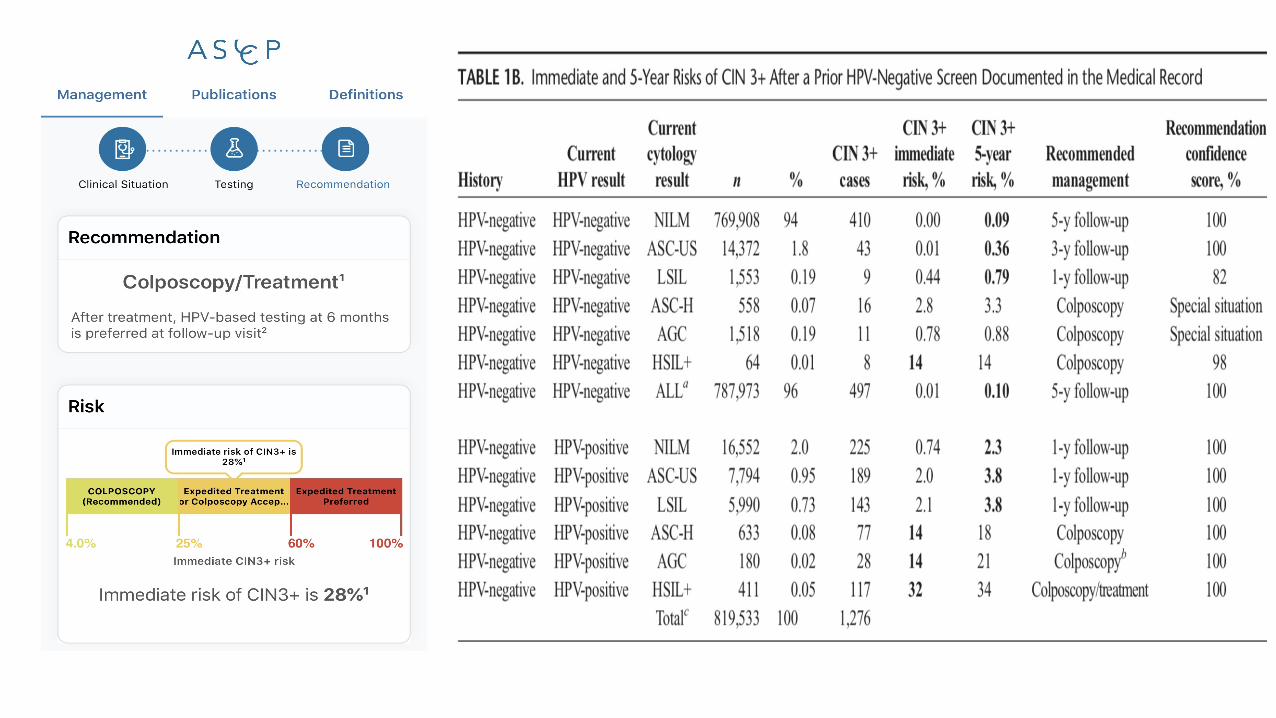
Iden&fy risk of CIN 3+ for each pa&ent Egermenetal.Riskestimatessupportingthe2019ASCCPrisk-basedmanagementconsensus
guidelines.JLowGenitTractDis2020;24:132-143.
• Mostpa=entscanbemanagedbyiden=fyingtheirrisklevelandlinkingittoarecommendedclinicalac1on.
• Returntorou=nescreening.• Surveillancewithrepeattes=ngat1,3or5yearintervals.• Colposcopy.• Treatment.
• Thisinforma=onisaccessibleviasmartphoneapp(purchase)orwebthroughhop://www.asccp.org(nocost)
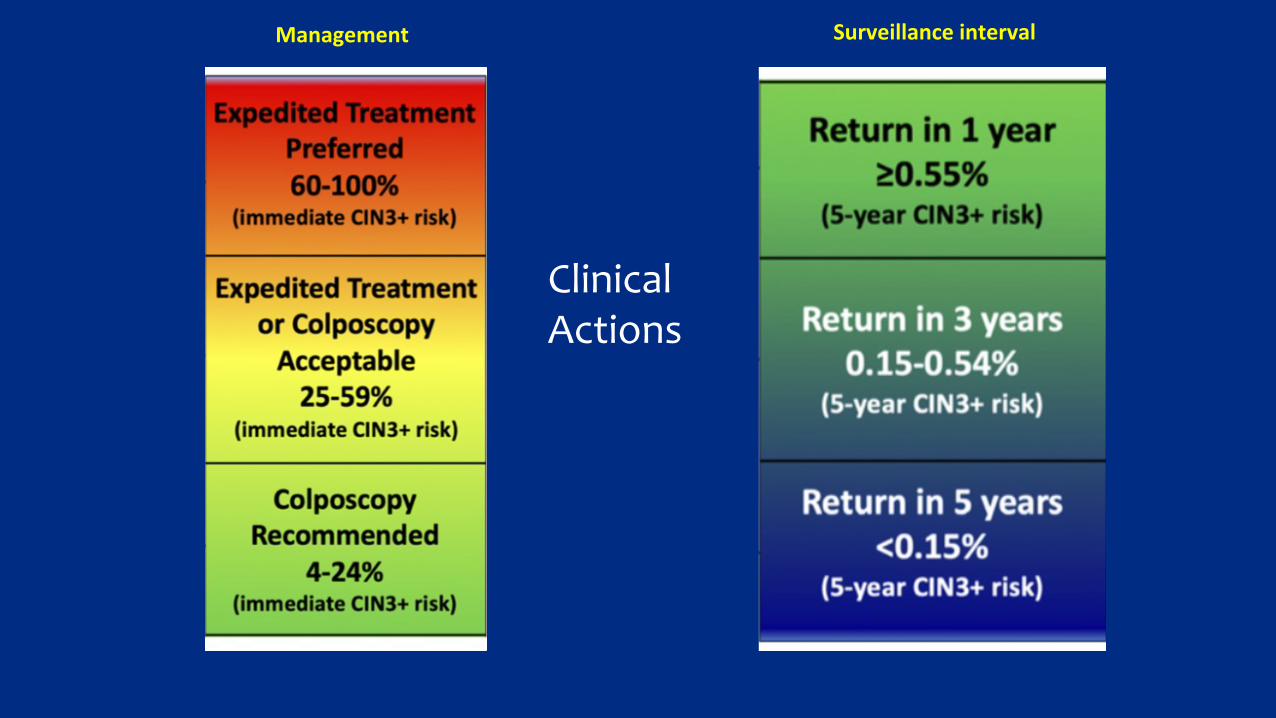
Management Surveillanceinterval
ClinicalActions
How is the pa&ent’s risk determined?
• Managementbasedonapatient’sriskofCIN3+.• 2019guidelinesmakerecommendationsbasedon:
• ImmediateCIN3+riskistheprobabilityofpatientcurrentlyhavingCIN3+.
• 5-yearCIN3+riskistheprobabilityofdevelopingCIN3+overthenext5years.
• Extensivedataanalysisproducedriskestimatesforallcombinationsoftestsandrecentscreeninghistory.
CIN3+chosenasthebestsurrogateforcancerrisk
• CIN3+includesCIN3,AISandrarecasesofinvasivecancerfoundatscreening.
• CIN3+chosenasendpointinsteadofcancer.• CancerisuncommoninUS.• Riskissignificantlydecreasedbyprecursortreatment.
• CIN3+choseninsteadofCIN2.• Isamorepathologicallyreproduciblediagnosis.• HPVtypesinCIN3+lesionsapproximateclosertoinvasivecancerthanthelargerrangeoftypesinCIN2.
• CIN2hasappreciableregressionratesinabsenceoftreatment.
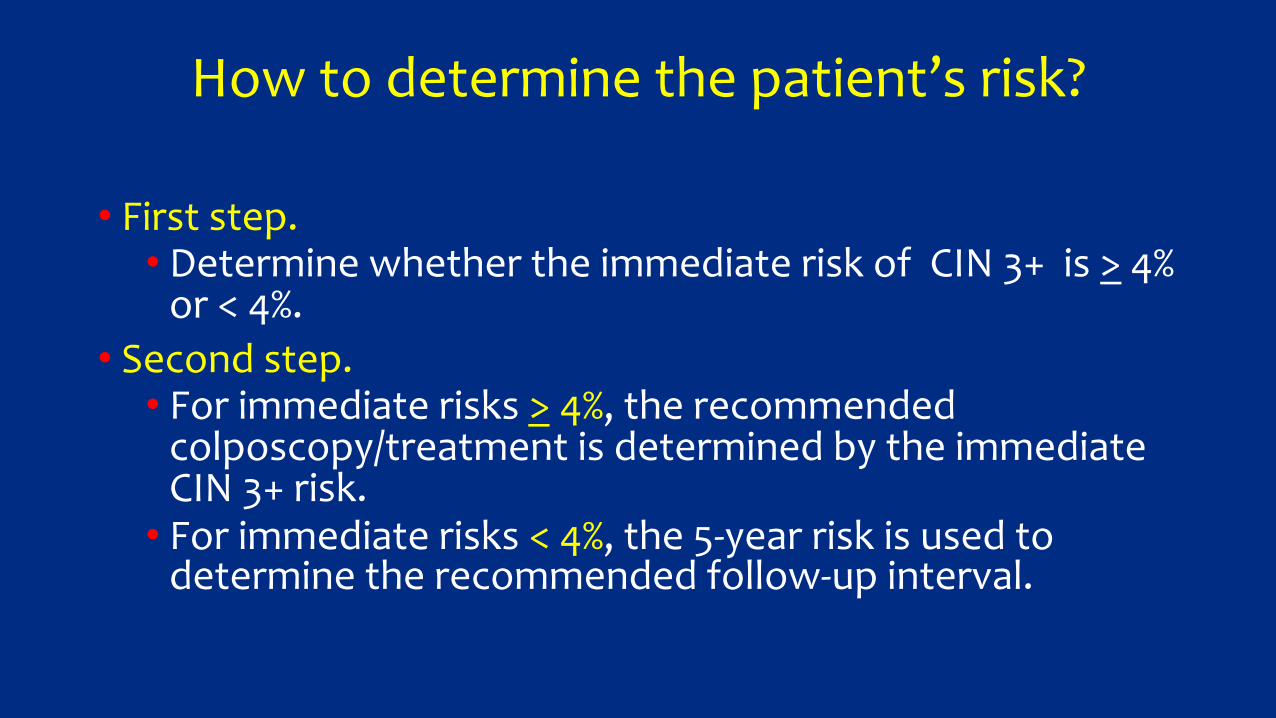
Howtodeterminethepatient’srisk?
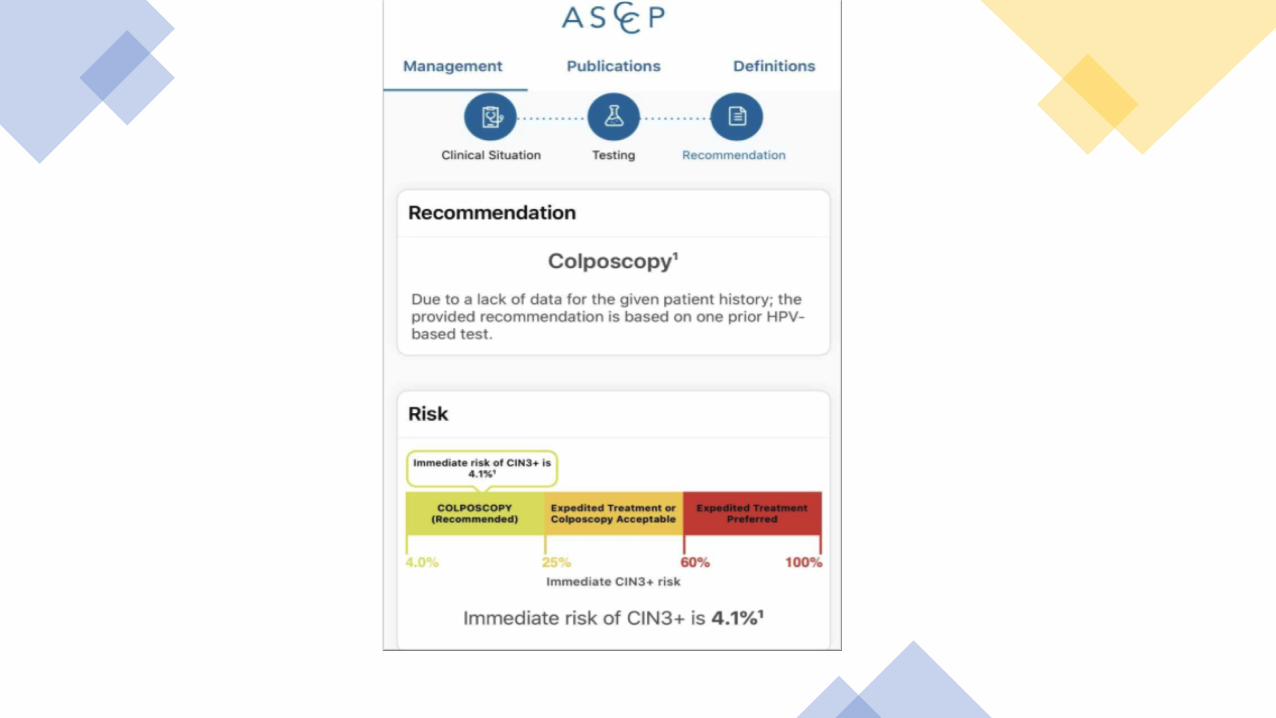
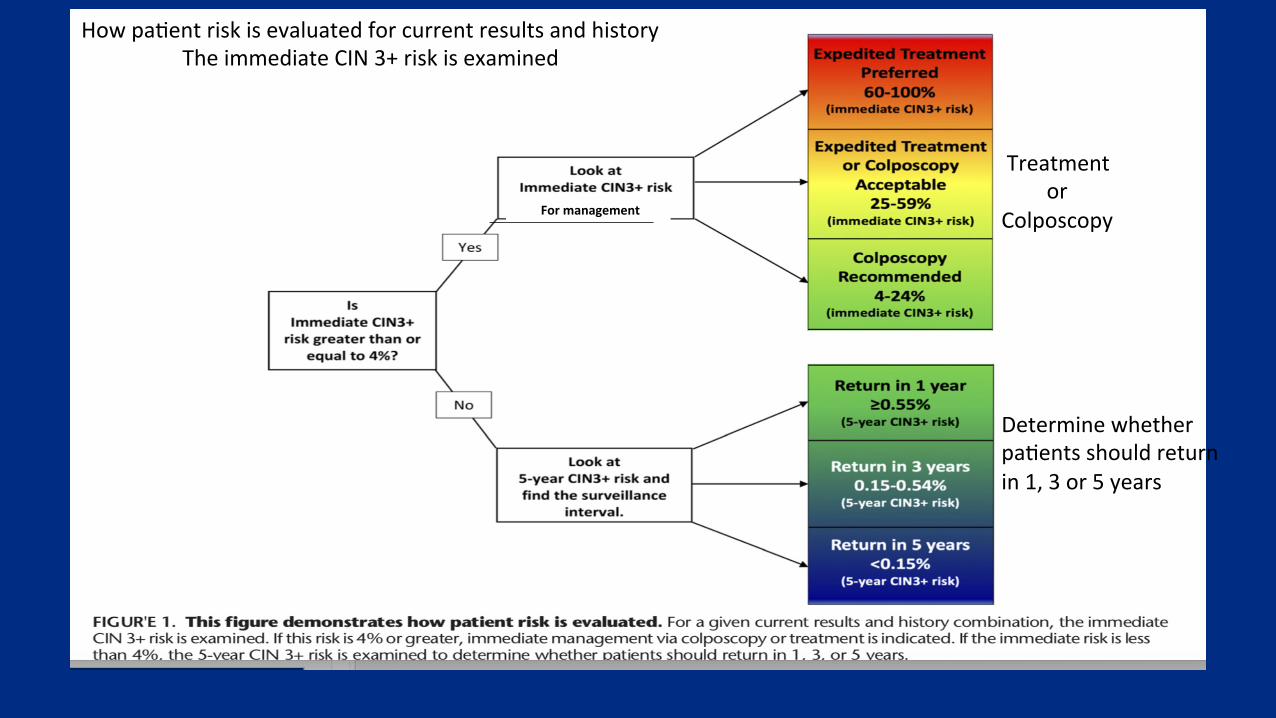
• Firststep.• DeterminewhethertheimmediateriskofCIN3+is>4%or<4%.
• Secondstep.• Forimmediaterisks>4%,therecommendedcolposcopy/treatmentisdeterminedbytheimmediateCIN3+risk.
• Forimmediaterisks<4%,the5-yearriskisusedtodeterminetherecommendedfollow-upinterval.
Whythe4%estimatedriskofCIN3+?
• TheClinicalActionThresholdofa4%immediateriskofCIN3+wasconsideredareasonablebalanceofbenefitsandharms.
• ValidationoftheThresholdincludedseveralstudypopulations:KPNC,NMHPVPapRegistry,CDCbreastandcervicalcancerearlydetectionprogram,BDOnclaritytrials.
• 4%thresholdfunctionedsimilarly.• Examinedclustersofpatientsindifferentresultgroups.
• High-graderesults• Low-graderesults• Combinationsforwhichcolpohasnotbeenperformed.
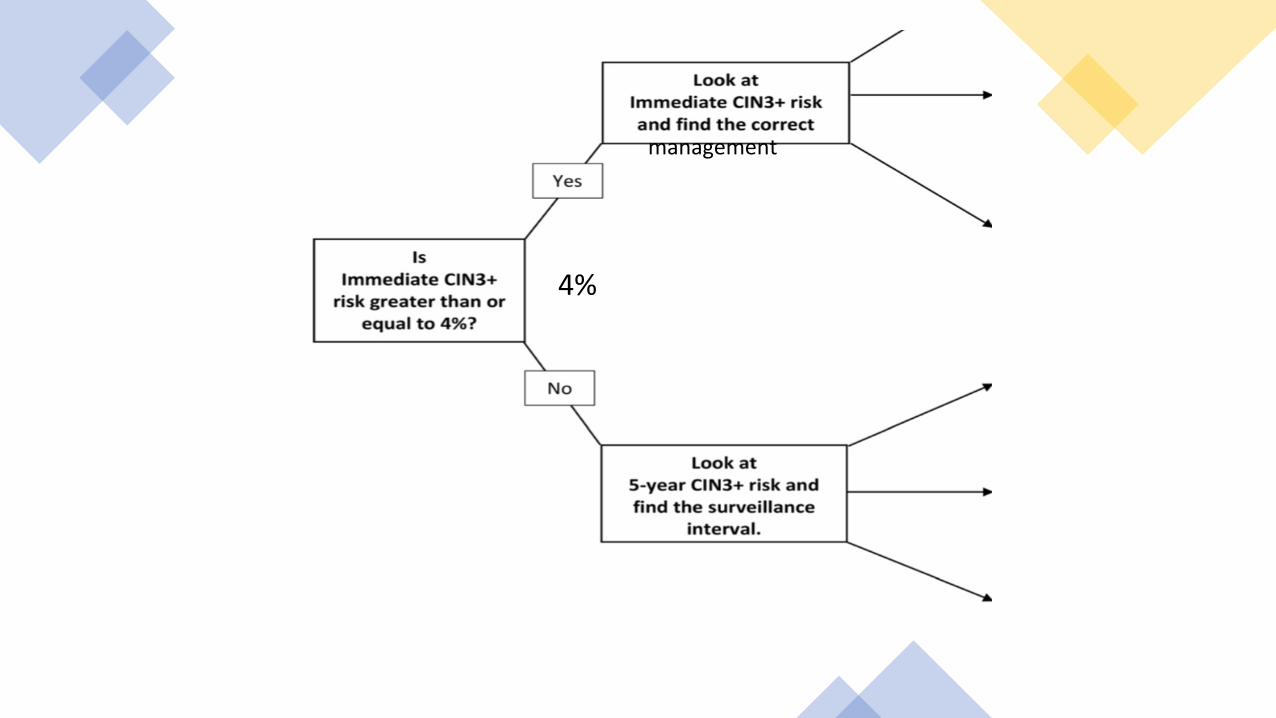
management
4%
Formanagement
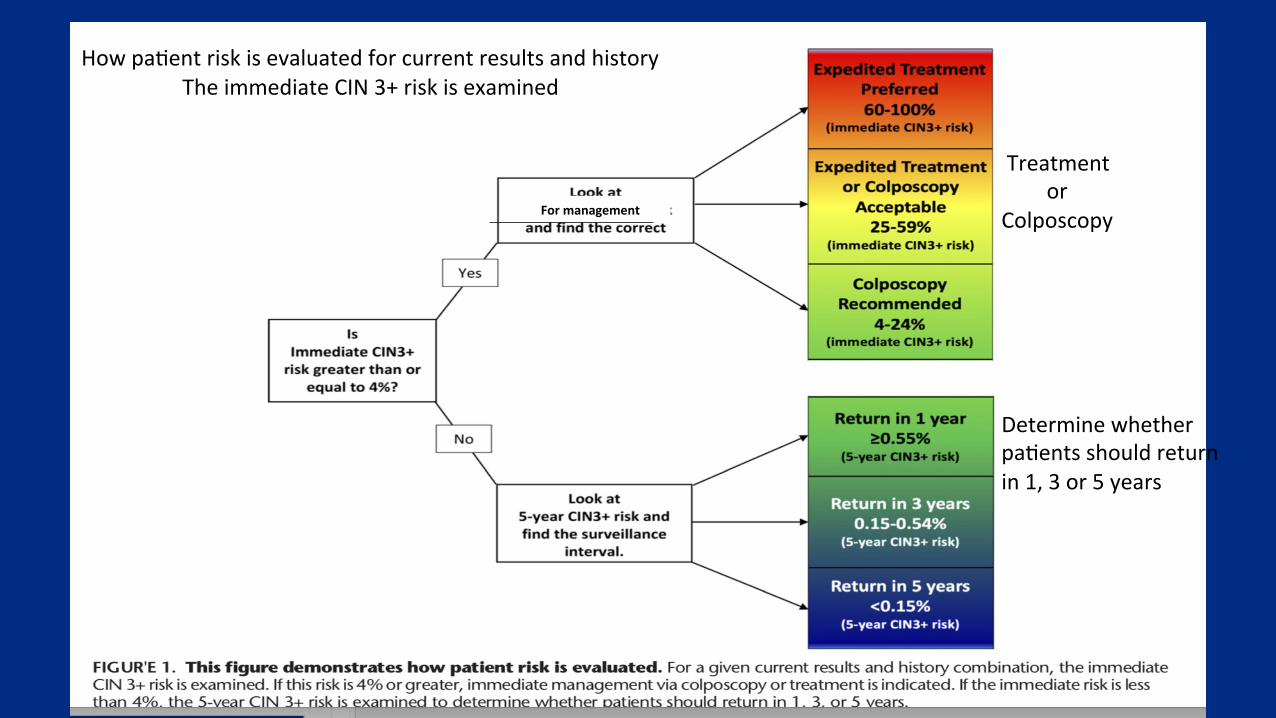
Howpa=entriskisevaluatedforcurrentresultsandhistory
TheimmediateCIN3+riskisexamined
Treatmentor
Colposcopy
Determinewhetherpa=entsshouldreturnin1,3or5years
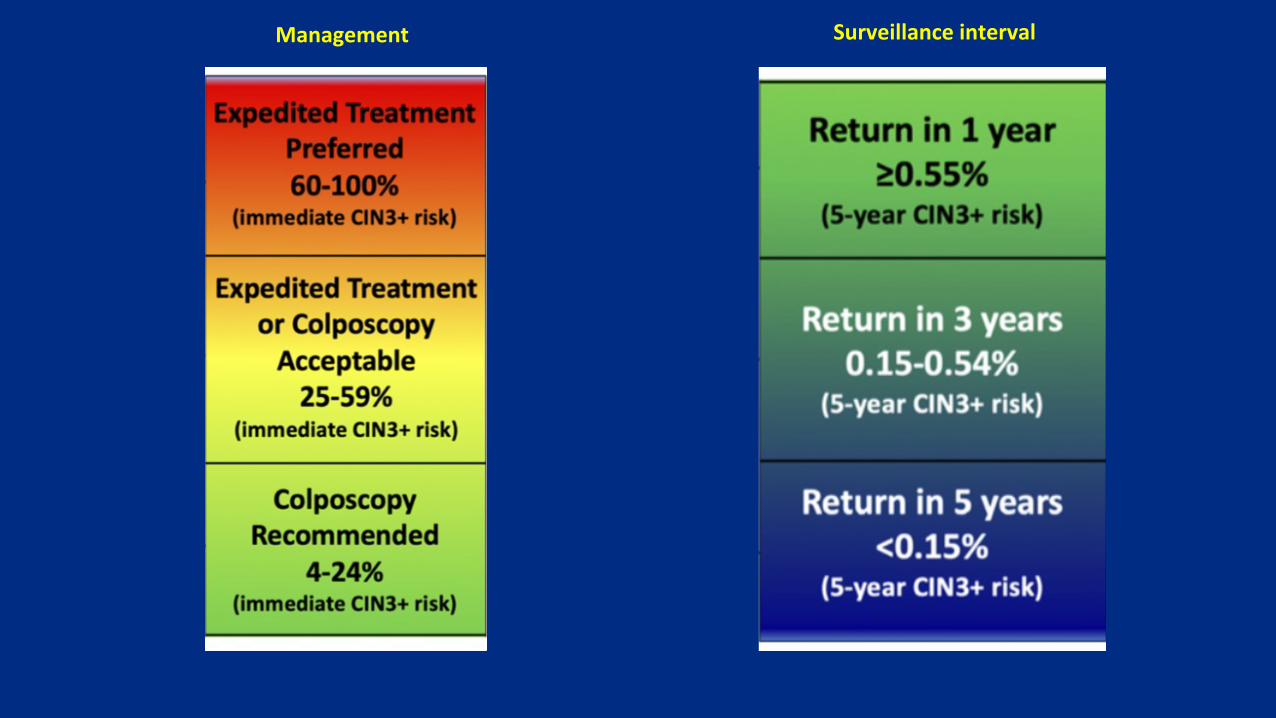
Management Surveillanceinterval
That important clinical ac&on threshold Consensus:Theclinicalac1onthresholdforreferraltocolposcopy
ortreatmentisa>4.0%immediateriskofCIN3+.
• Op=onsbasedonimmediateriskofCIN3+>4.0%:• Expeditedtreatmentwithoutbiopsyispreferred.
• Treatmentorcolposcopicbiopsiesacceptable. • Colposcopicbiopsiesarerecommended.
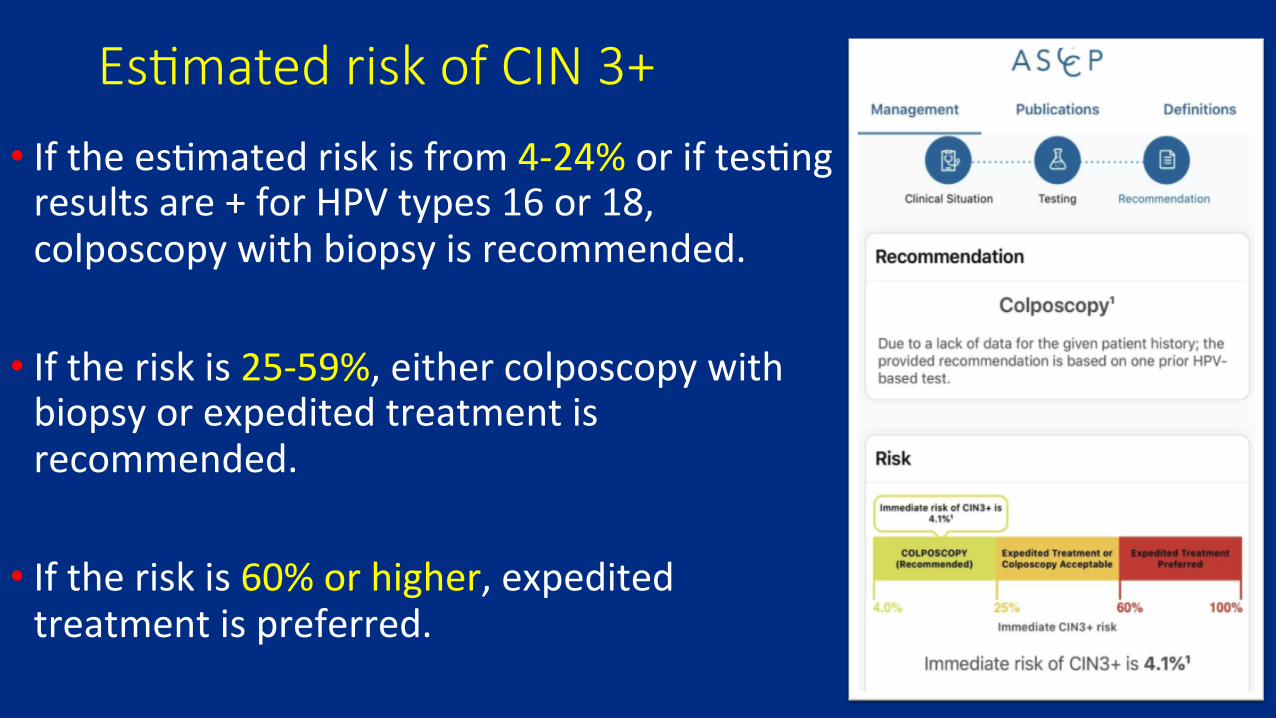
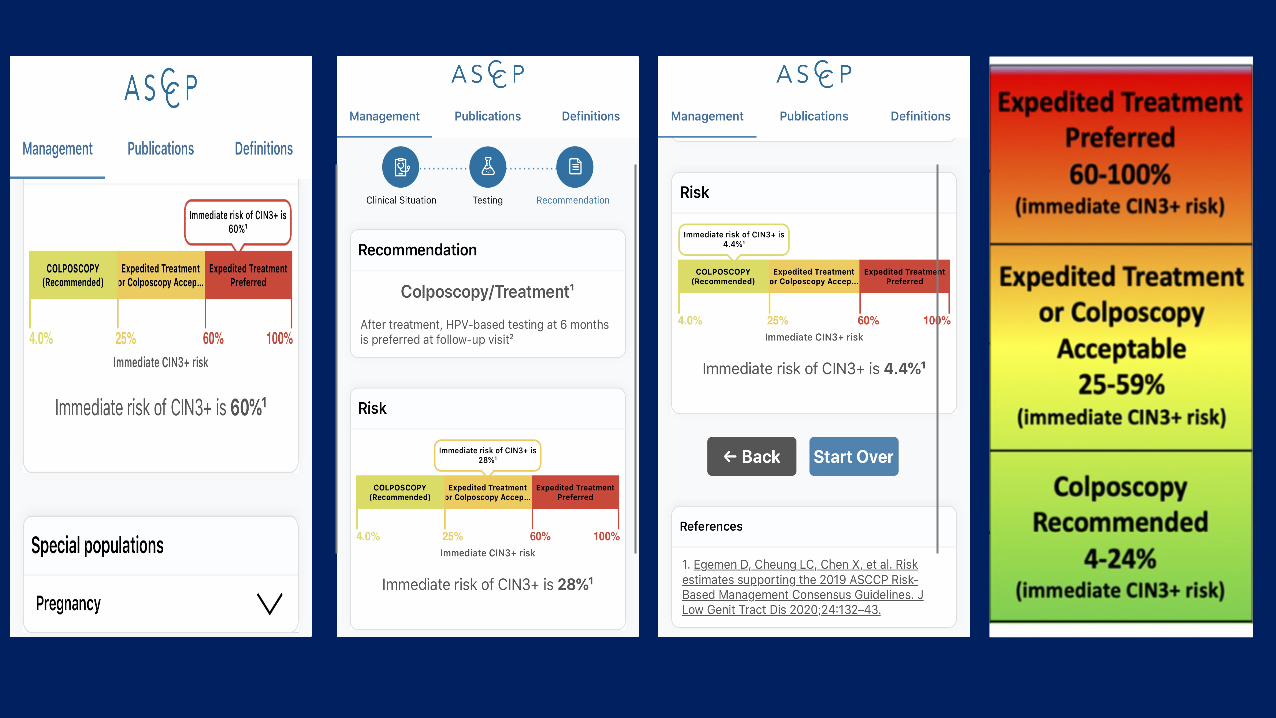
Es&mated risk of CIN 3+
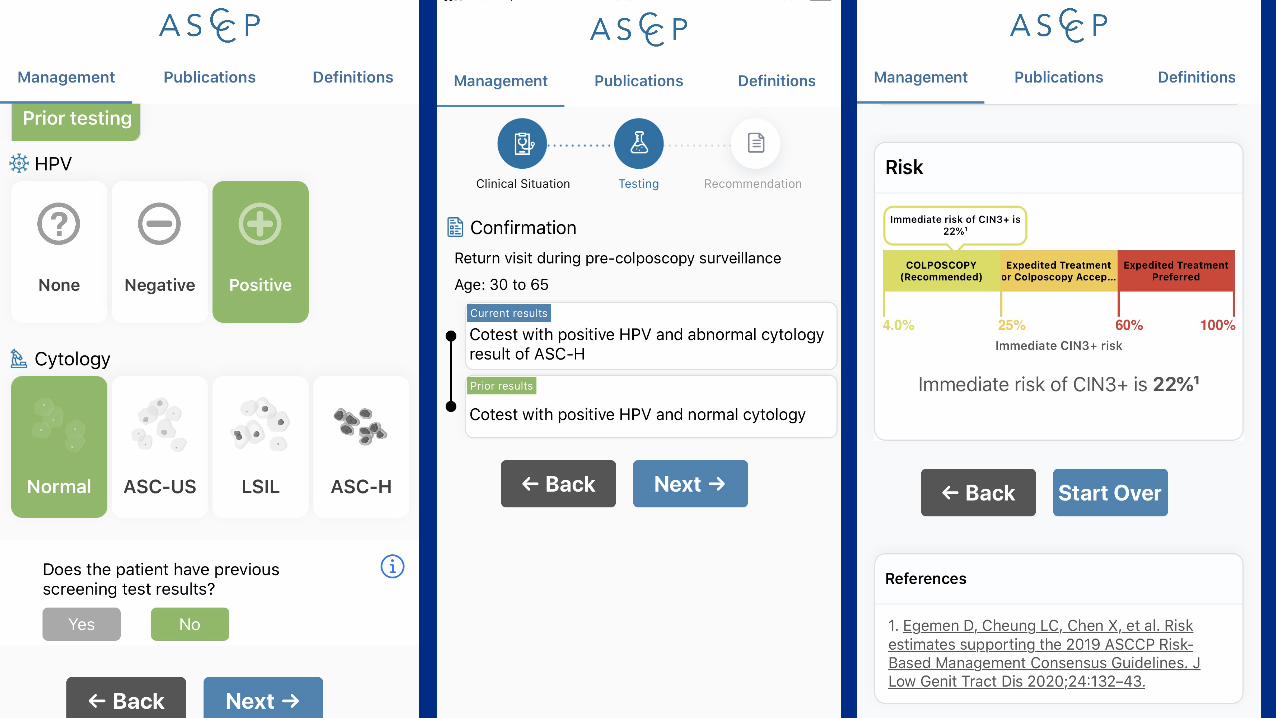
• Ifthees=matedriskisfrom4-24%oriftes=ngresultsare+forHPVtypes16or18,colposcopywithbiopsyisrecommended.
• Iftheriskis25-59%,eithercolposcopywithbiopsyorexpeditedtreatmentisrecommended.
• Iftheriskis60%orhigher,expeditedtreatmentispreferred.
Expedited Treatment (ET) is defined as treatment without preceding colposcopic biopsy
• Fornon-pregnantpa=ents>25years,ETispreferredwhentheimmediateriskofCIN3+is>60%.
• Acceptableforthosewithrisksbetween25%and60%.
• ETispreferredfornon-pregnantpa=ents>25yearswithHPVtype16+HSILandneverorrarelyscreenedpa=entswithHPV+HSILcytologyregardlessofgenotype.
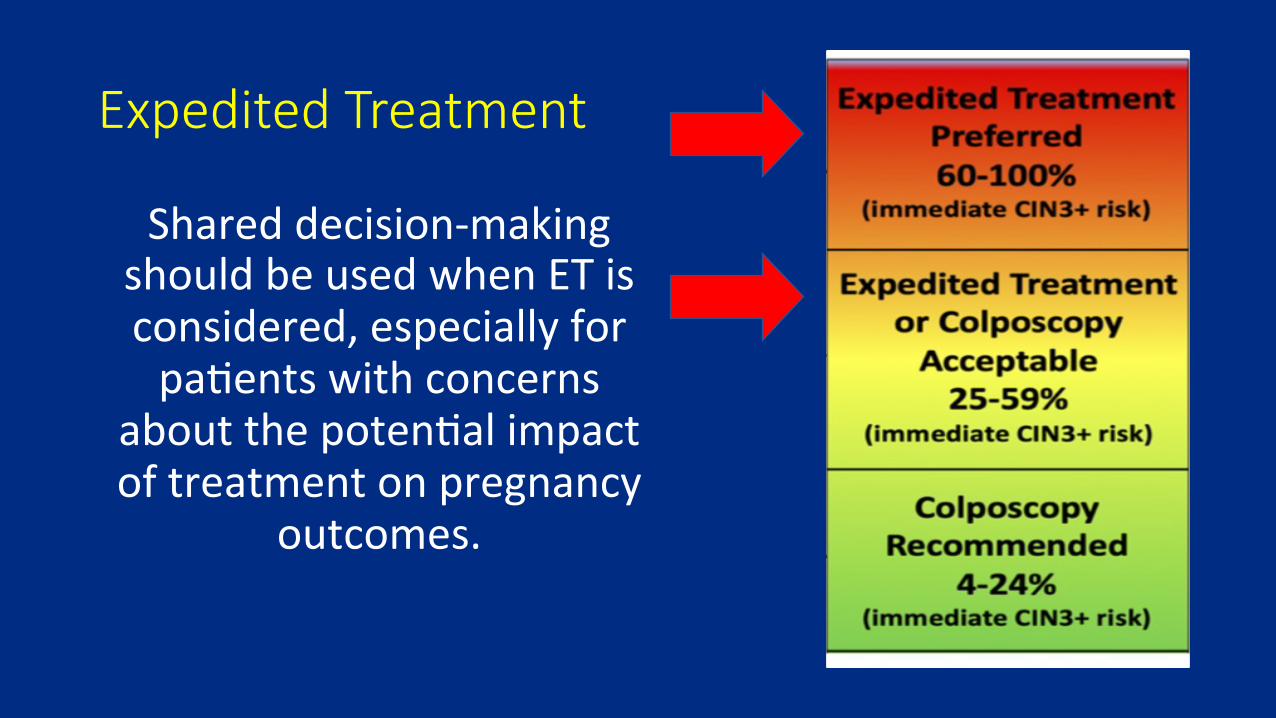
Expedited Treatment
Shareddecision-makingshouldbeusedwhenETisconsidered,especiallyforpa=entswithconcerns
aboutthepoten=alimpactoftreatmentonpregnancy
outcomes.
ThatimportantclinicalactionthresholdConsensus:Theclinicalactionthresholdforreferraltosurveillance
isa<4.0%immediateriskofCIN3+
• OptionsbasedonanimmediateriskofCIN3+<4%.• Lookatthe5-yearCIN3+risk
• FindthesurveillanceintervallevelandrepeatHPV-basedtestingin1,3or5years
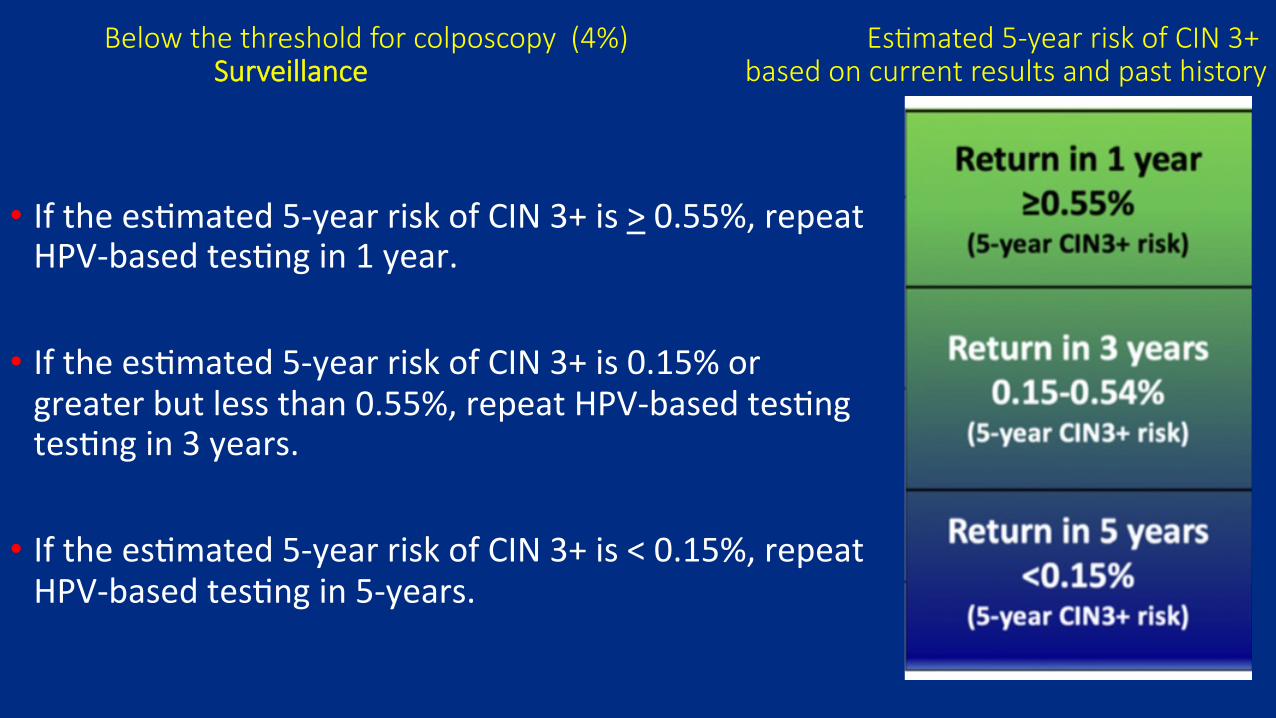
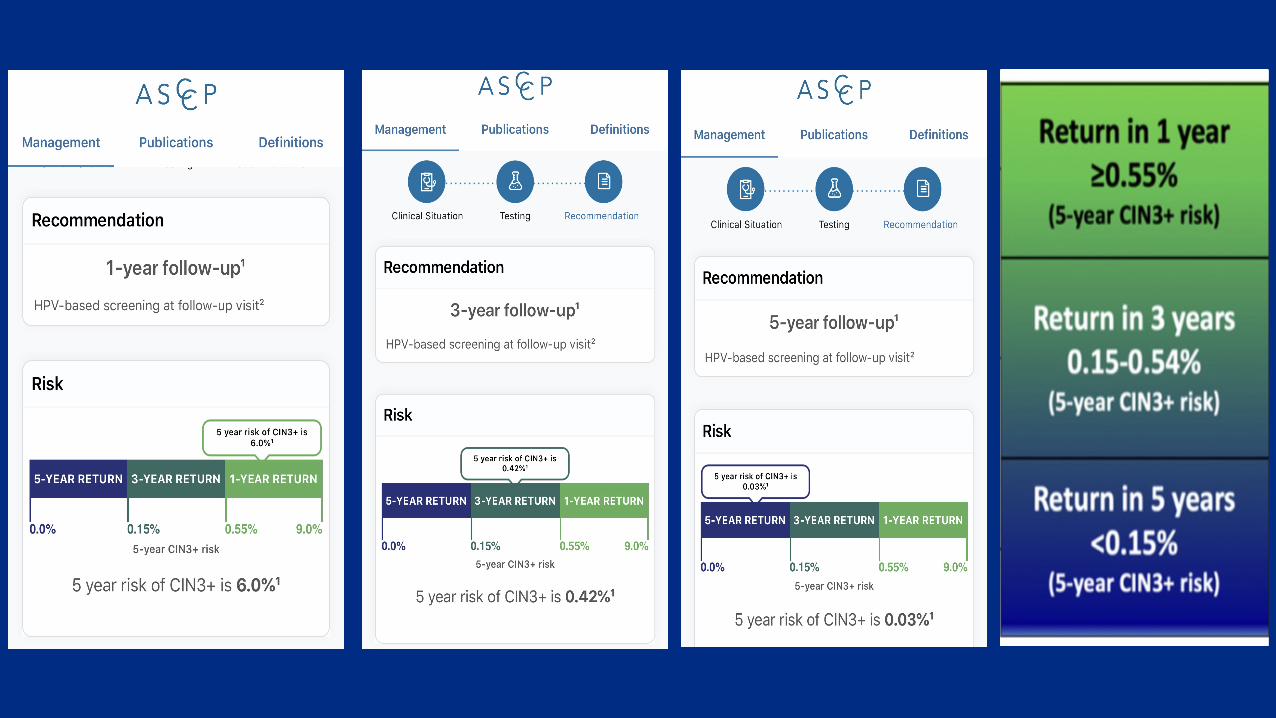
Below the threshold for colposcopy (4%) Es&mated 5-year risk of CIN 3+ Surveillance based on current results and past history
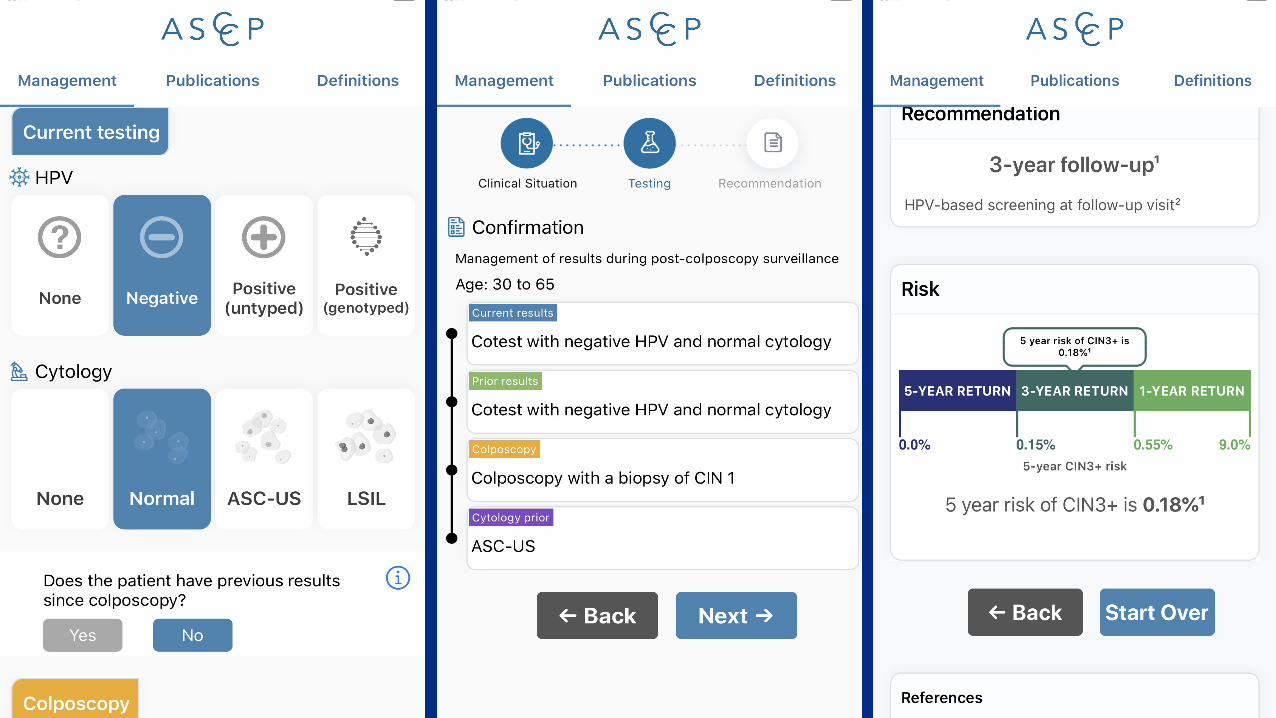
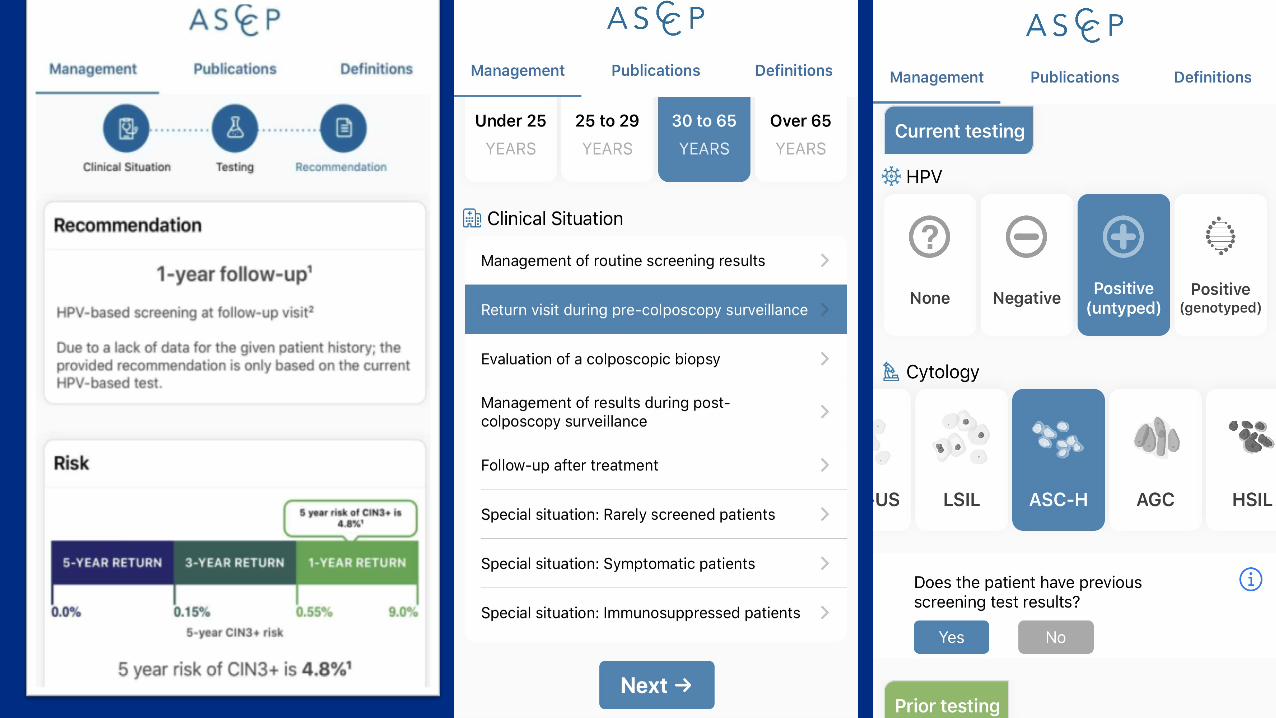
• Ifthees=mated5-yearriskofCIN3+is>0.55%,repeatHPV-basedtes=ngin1year.
• Ifthees=mated5-yearriskofCIN3+is0.15%orgreaterbutlessthan0.55%,repeatHPV-basedtes=ngtes=ngin3years.
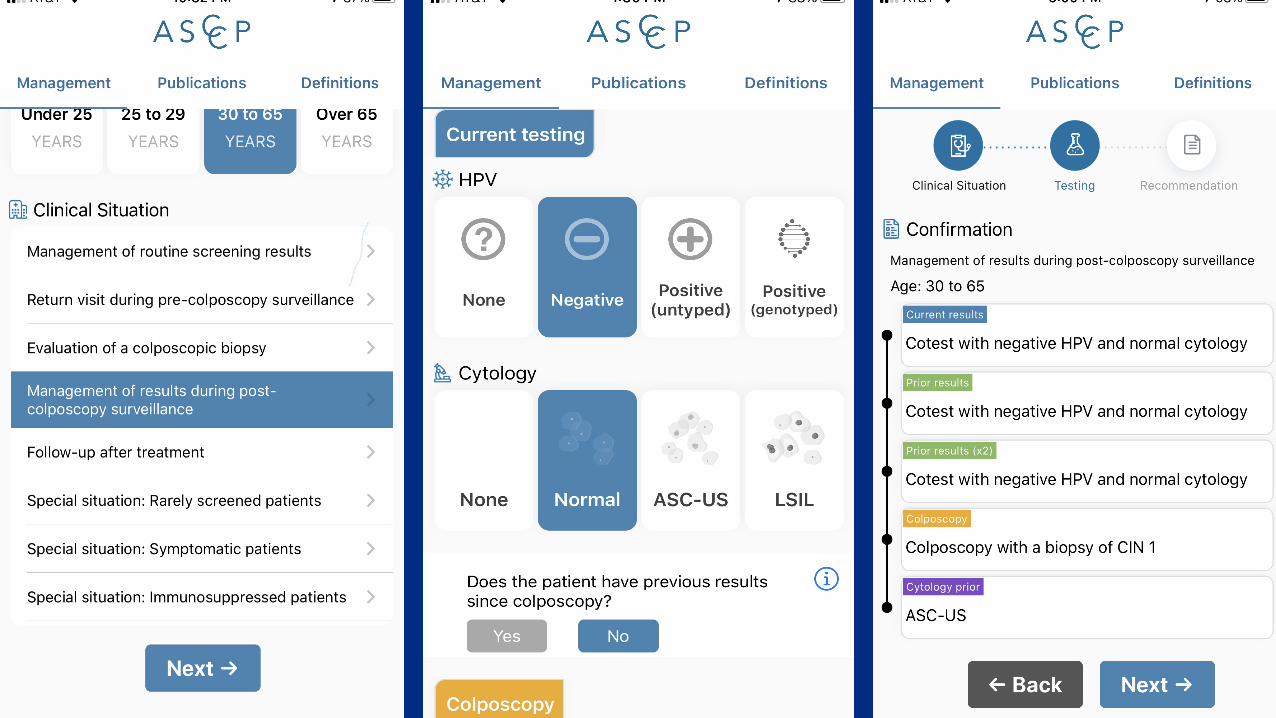
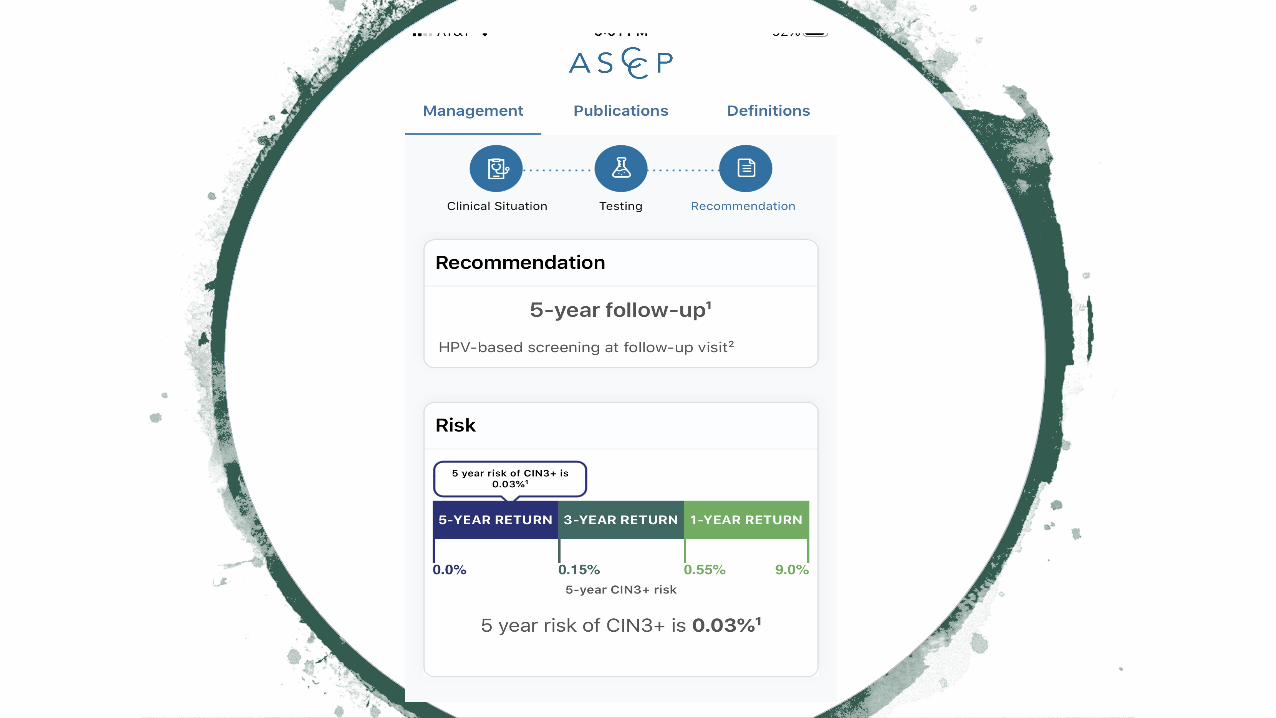
• Ifthees=mated5-yearriskofCIN3+is<0.15%,repeatHPV-basedtes=ngin5-years.
11/5/20, 11(56 AMMobile App - ASCCP
Page 1 of 2https://www.asccp.org/mobile-app
(0) View Cart [email protected] 0 My ASCCP
Search
Mobile App
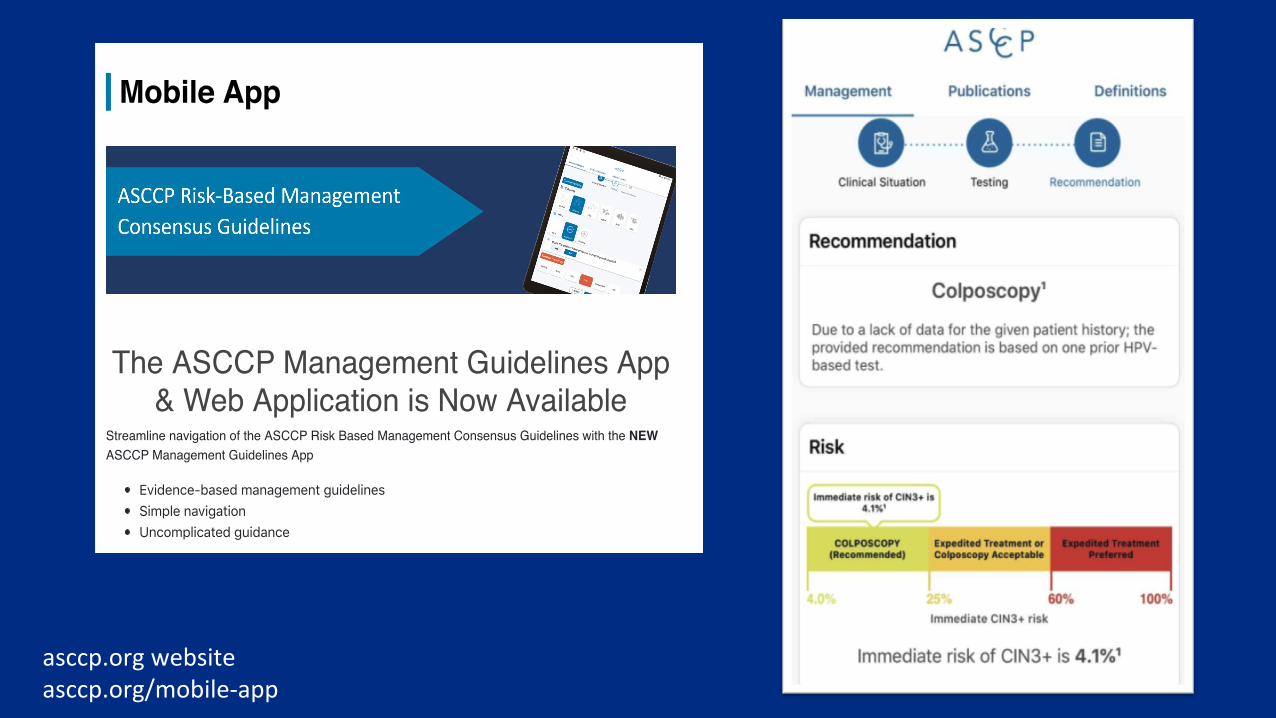
The ASCCP Management Guidelines App& Web Application is Now Available
Streamline navigation of the ASCCP Risk Based Management Consensus Guidelines with the NEWASCCP Management Guidelines App
Evidence-based management guidelinesSimple navigationUncomplicated guidance
Need Help?
Quick Start Guide
Walk through the Appwith Cases
User Guide
asccp.orgwebsiteasccp.org/mobile-app
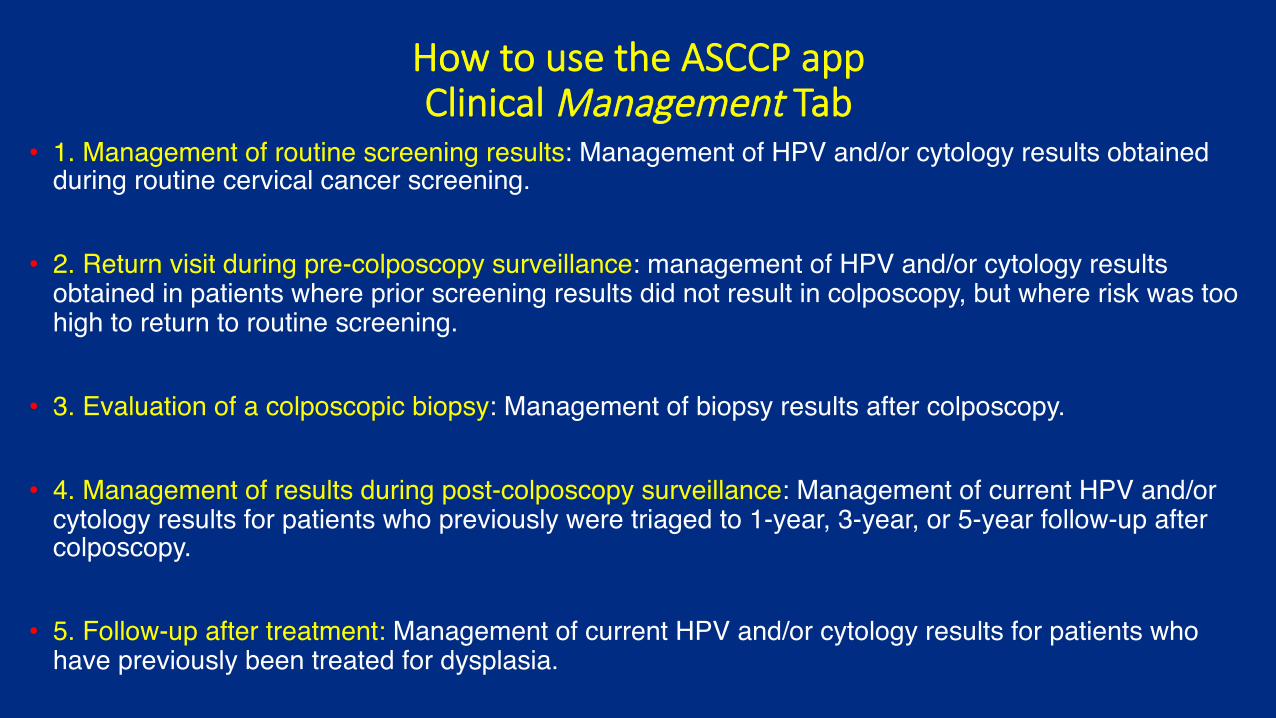
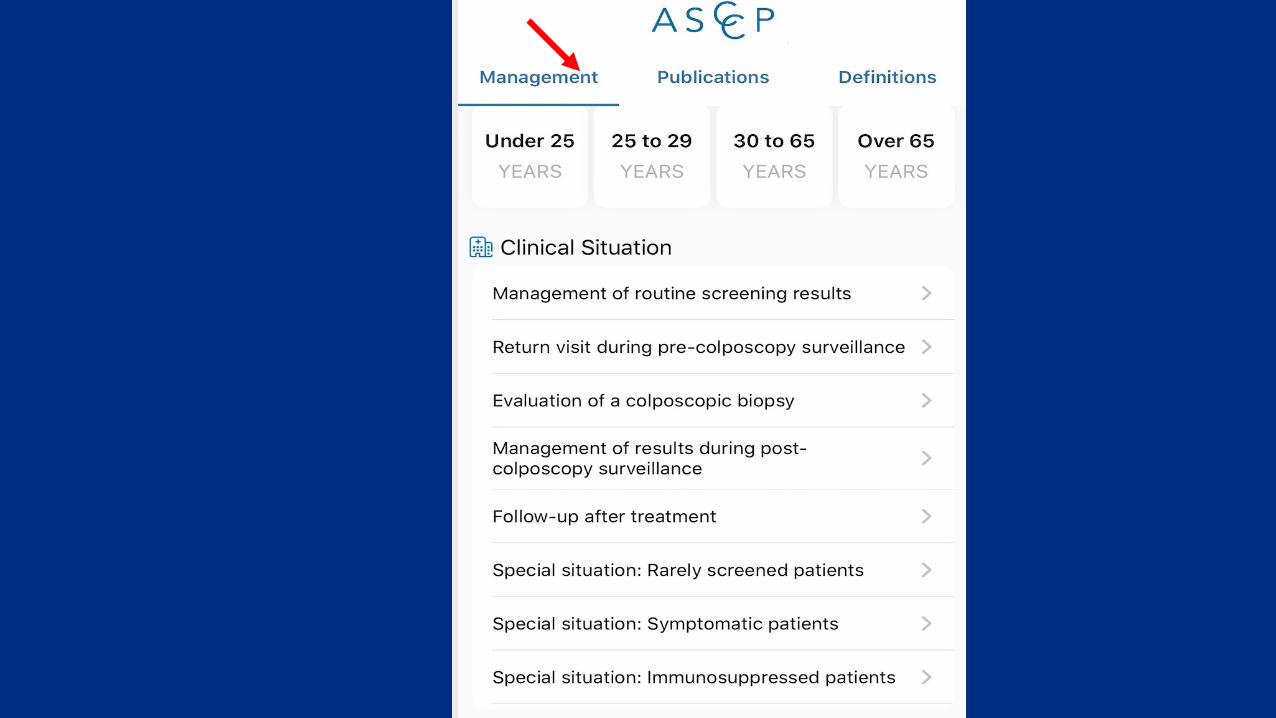
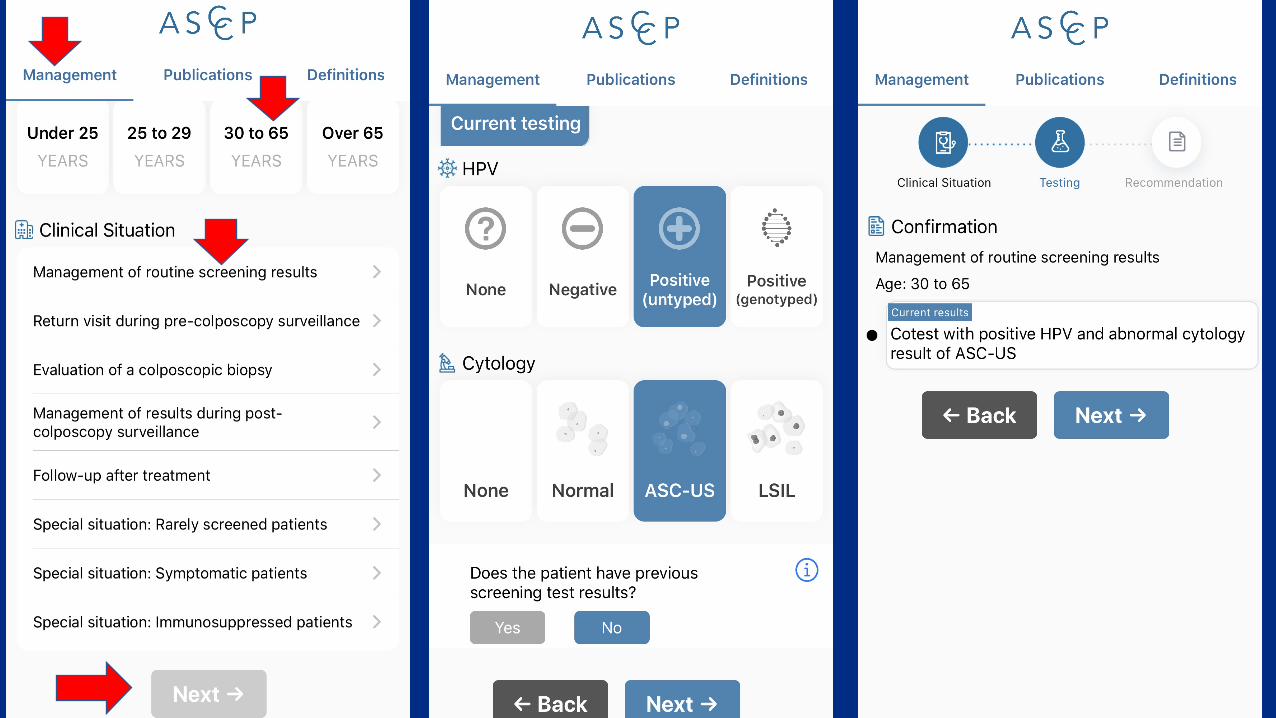
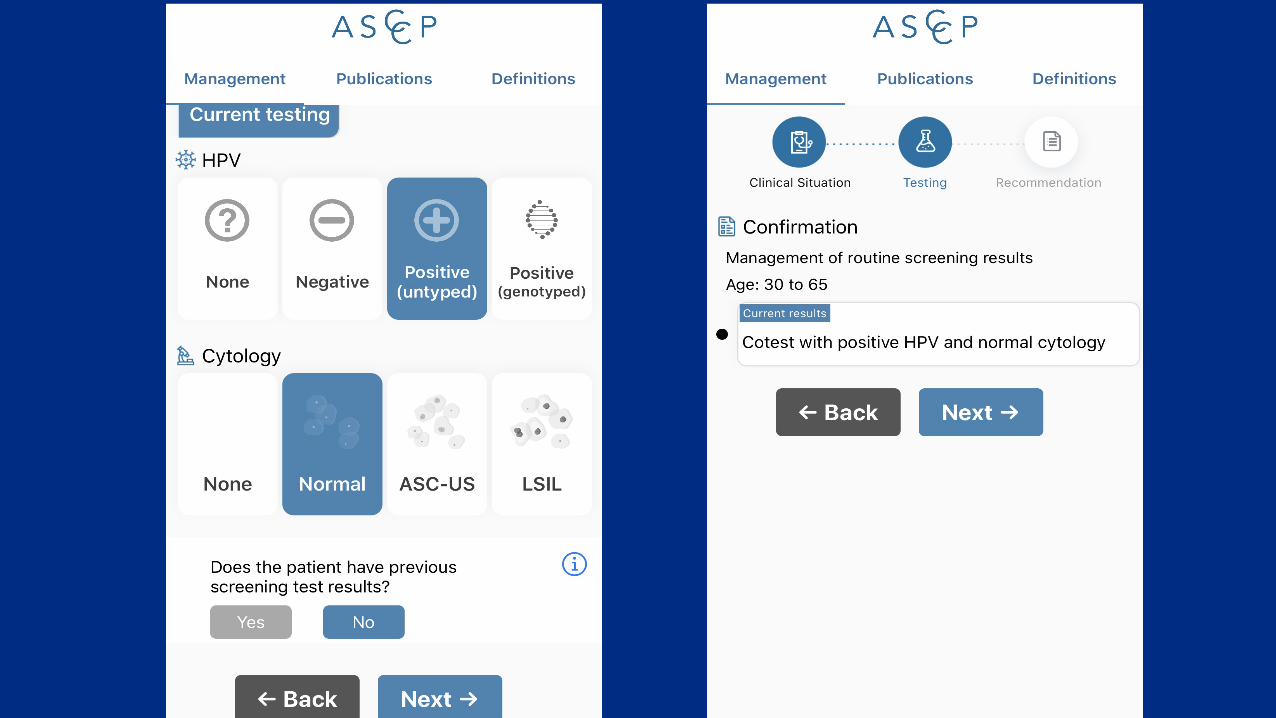
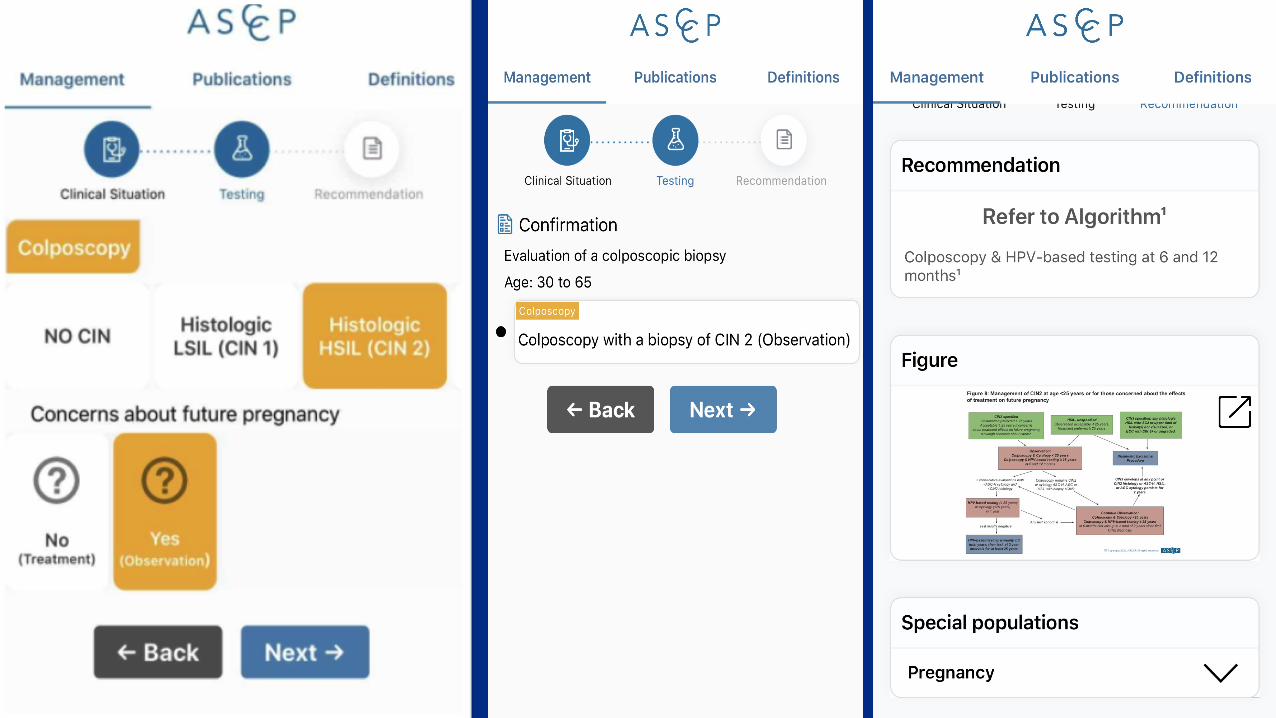
How to use the ASCCP app Clinical Management Tab
• 1. Management of routine screening results: Management of HPV and/or cytology results obtained during routine cervical cancer screening.
• 2. Return visit during pre-colposcopy surveillance: management of HPV and/or cytology results obtained in patients where prior screening results did not result in colposcopy, but where risk was too high to return to routine screening.
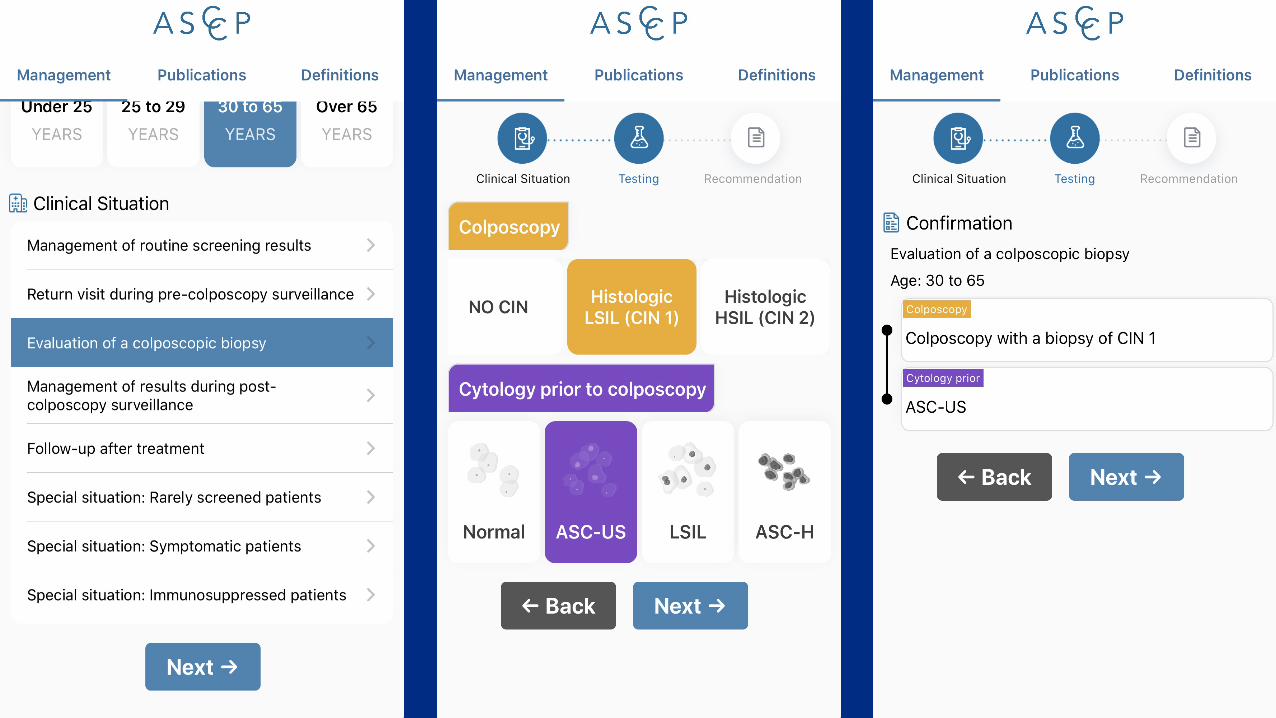
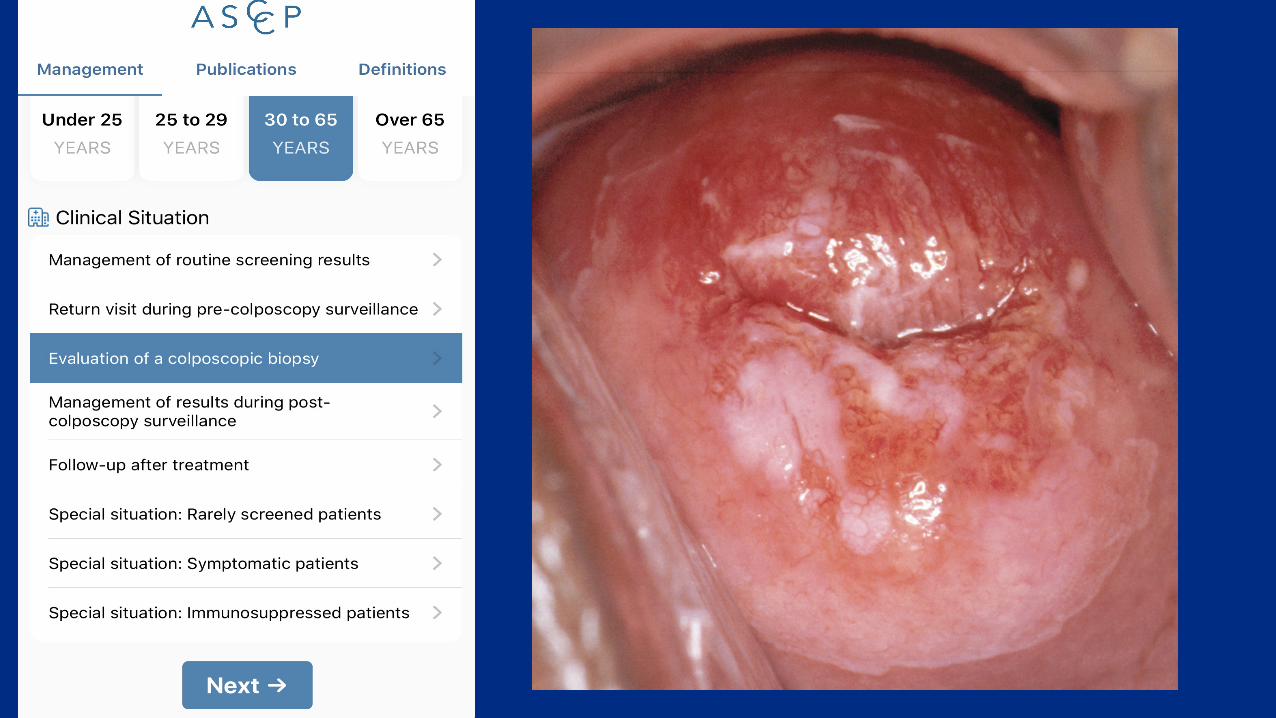
• 3. Evaluation of a colposcopic biopsy: Management of biopsy results after colposcopy.
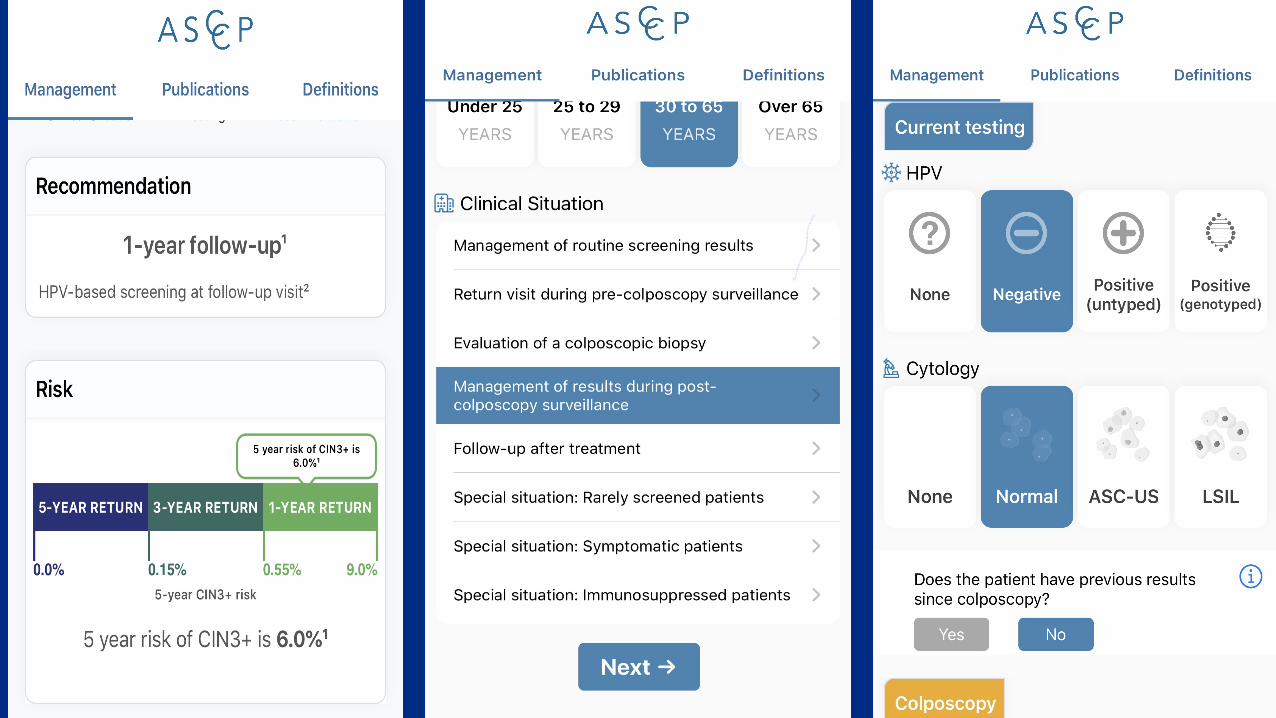
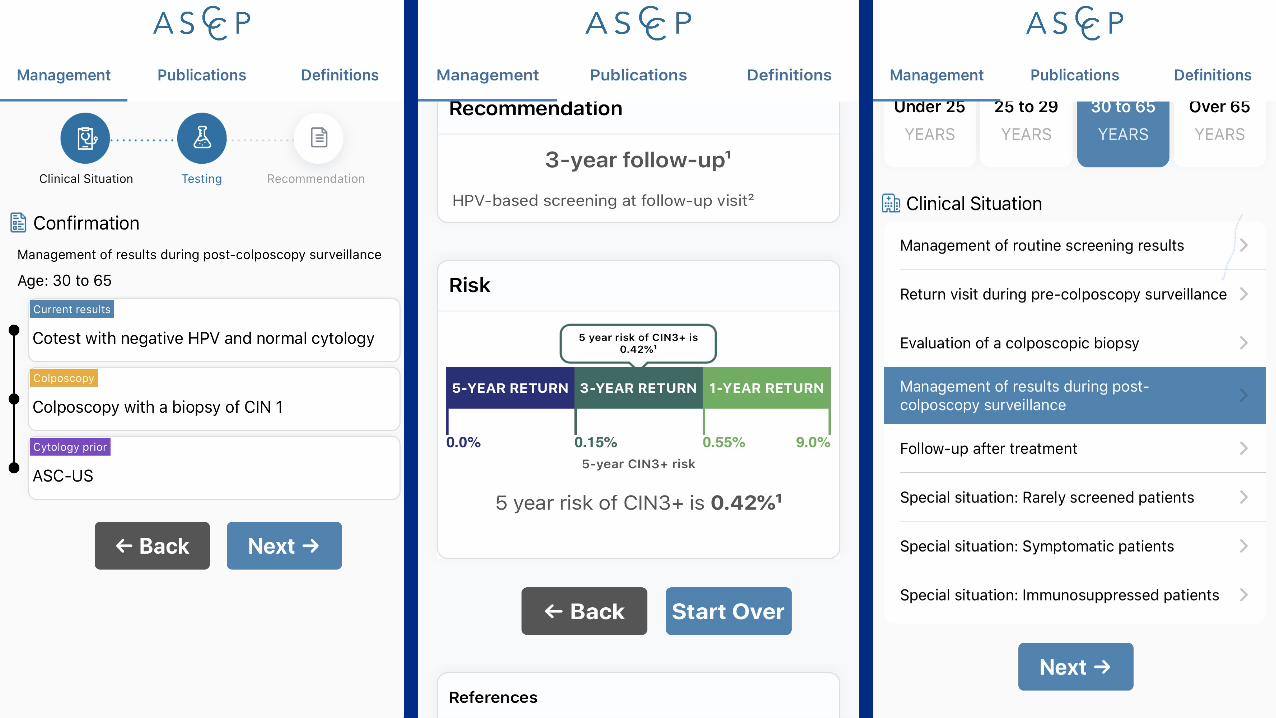
• 4. Management of results during post-colposcopy surveillance: Management of current HPV and/or cytology results for patients who previously were triaged to 1-year, 3-year, or 5-year follow-up after colposcopy.
• 5. Follow-up after treatment: Management of current HPV and/or cytology results for patients who have previously been treated for dysplasia.
How to use the ASCCP app Publica&ons and Defini&ons tab
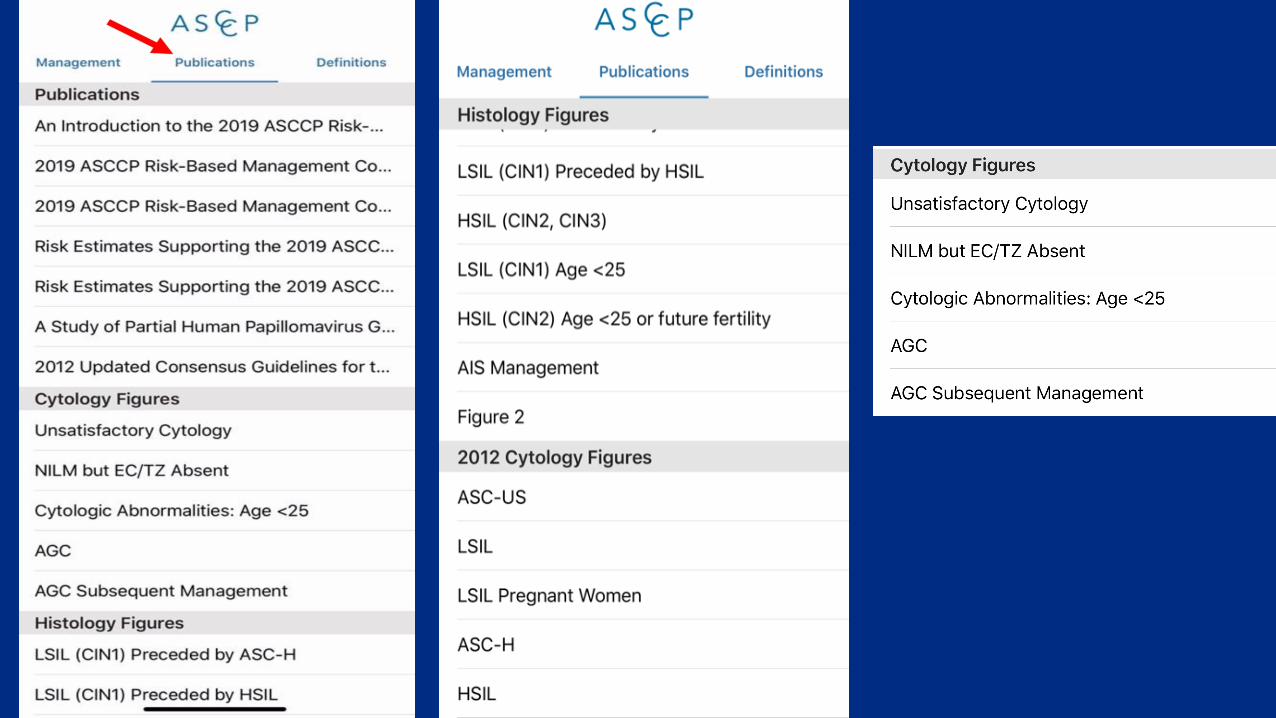
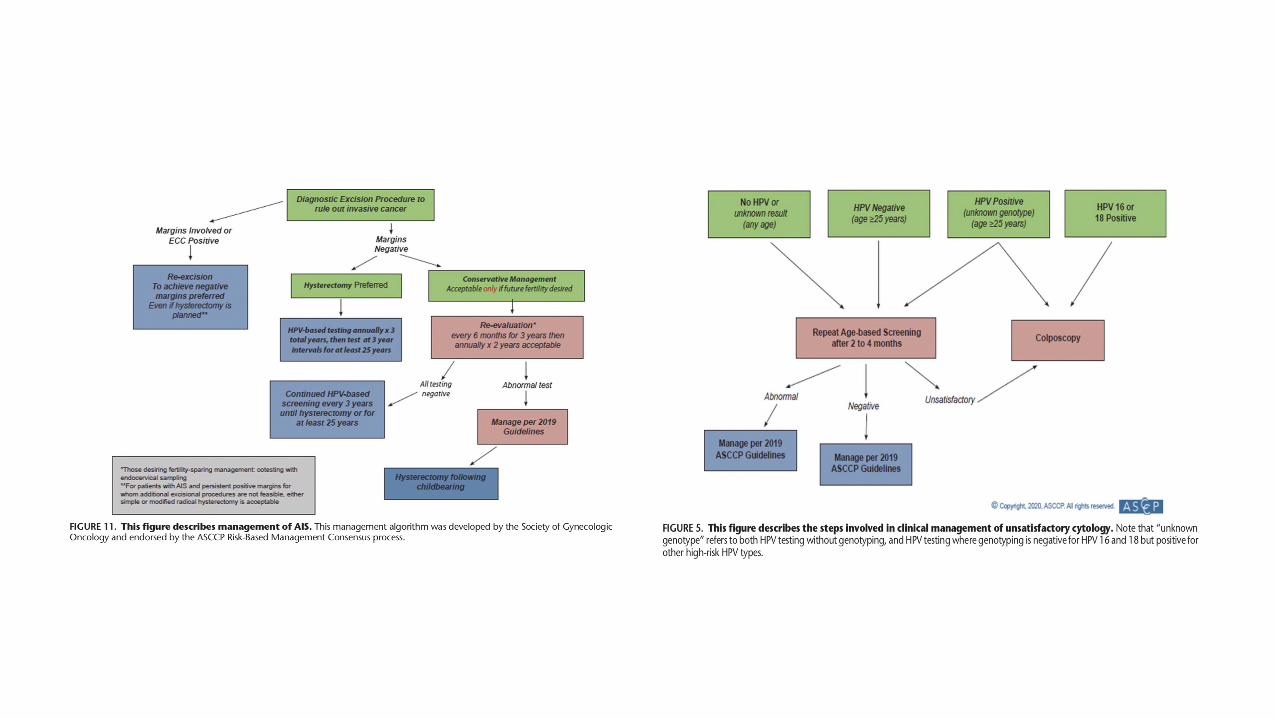
• Publica=onstab-Thishasallthemainpapersthatwereusedinconjunc=onwiththedevelopmentoftheguidelines.Therearealsocytologyfigures,histologyfigures,datatables,andtheoldercytologyalgorithmsforreference.
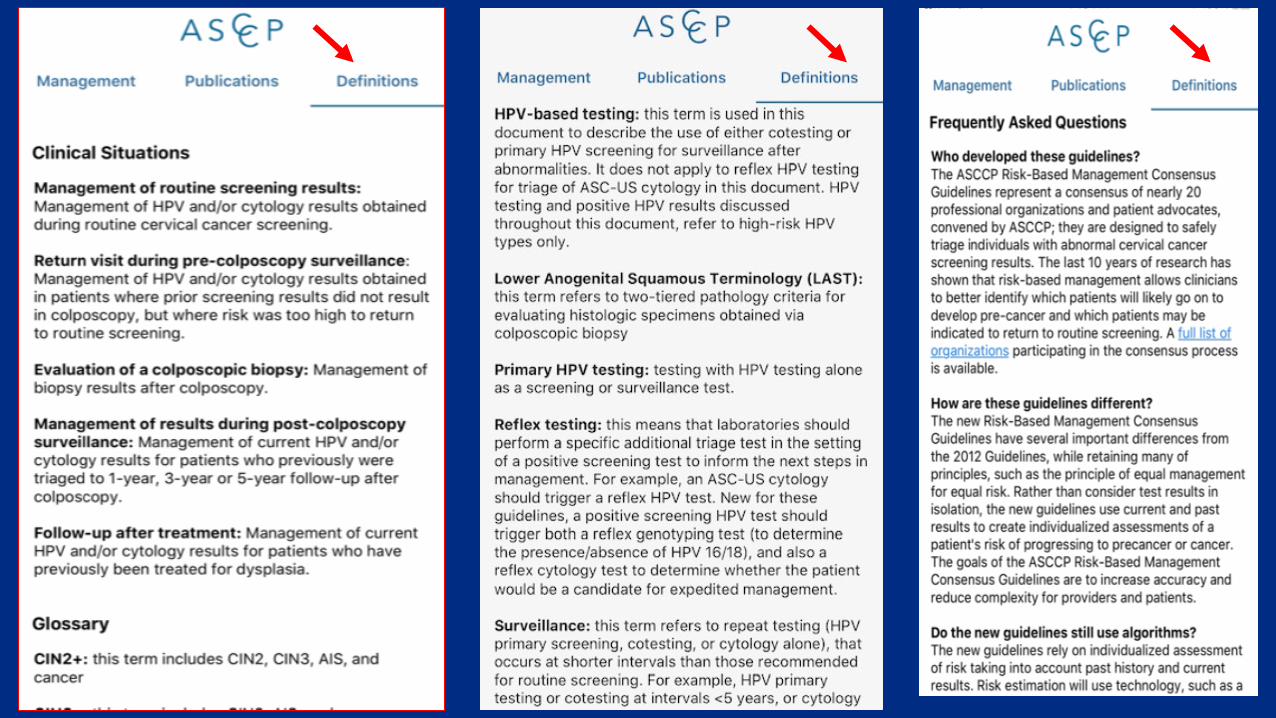
• Defini=onstab-Defini=onsoftermsintheapp,asummaryofthechangesinthecurrentguidelinesfrompriorguidelines,andfrequentlyaskedques=ons.
Sent from my iPhone
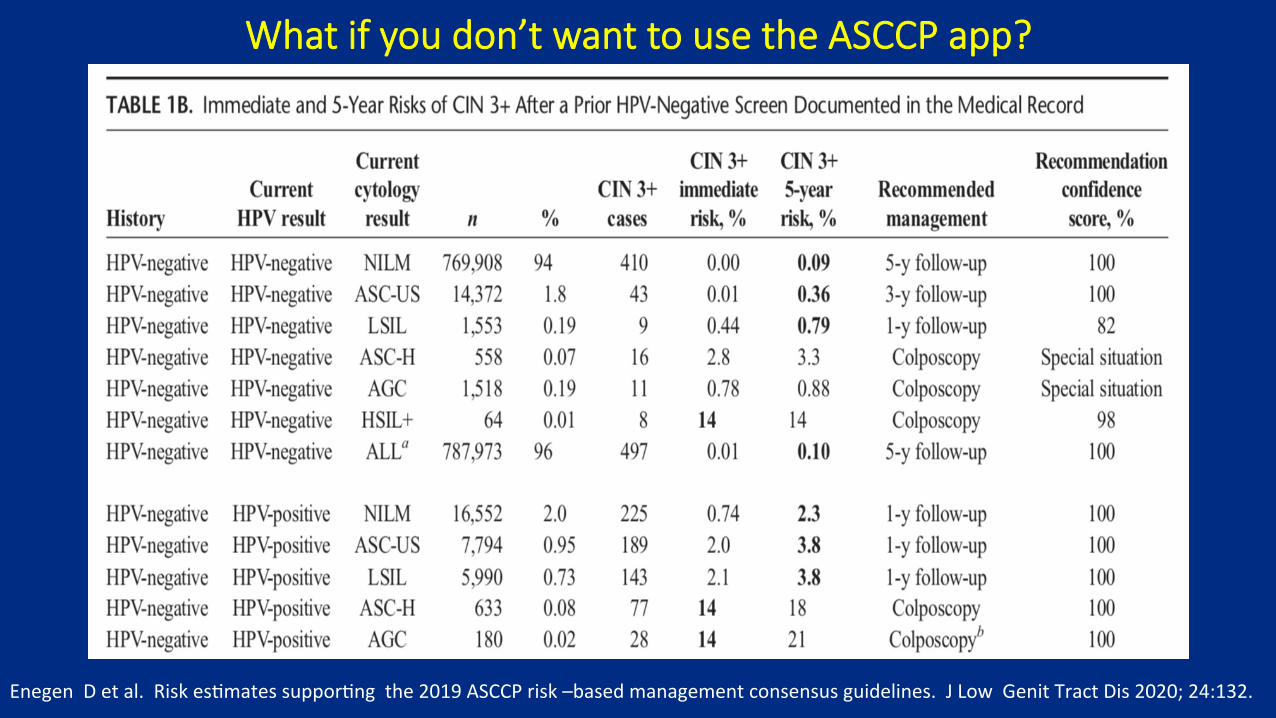
What if you don’t want to use the ASCCP app?
EnegenDetal.Riskes=matessuppor=ngthe2019ASCCPrisk–basedmanagementconsensusguidelines.JLowGenitTractDis2020;24:132.
Cases
• 32-year-oldpa=entpresentsforcervicalcancerscreening.Shedeniesanyabnormali=es.Shedeniescolposcopyorcervicaltreatmentinthepast.Hermedicalrecordsarenotavailablesoherprecisehistoryisunknown.ScreeningshowsHPV+ASC-US.Nogenotypingwasavailable.
• WhatisherimmediateriskofCIN3+?
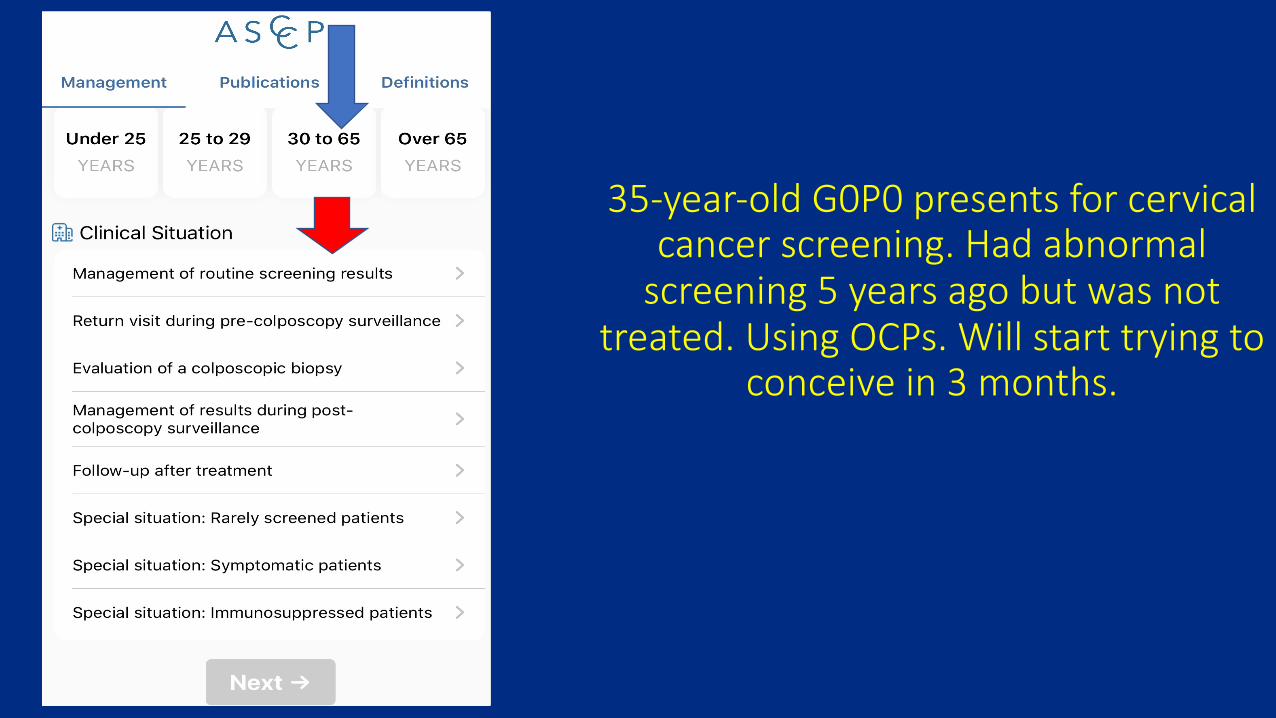
35-year-old G0P0 presents for cervical cancer screening. Had abnormal
screening 5 years ago but was not treated. Using OCPs. Will start trying to
conceive in 3 months.
2019 Guiding Principle #3 Guidelines will allow updates
• Incorporatenewtestmethodsastheyarevalidated.
• AdjustfordecreasingCIN3+risksasmorepatientswhoreceivedHPVvaccinationreachscreeningage.
• The2019guidelinesbuildaframeworkthatallowsincorporationofnewtechnologiesandmodifiedstrategieswithoutrequiringfullconsensusconferences.
• Revisionsmayrapidlyincorporatenewfindingsandbequicklydisseminatedtooptimizepatientcare.
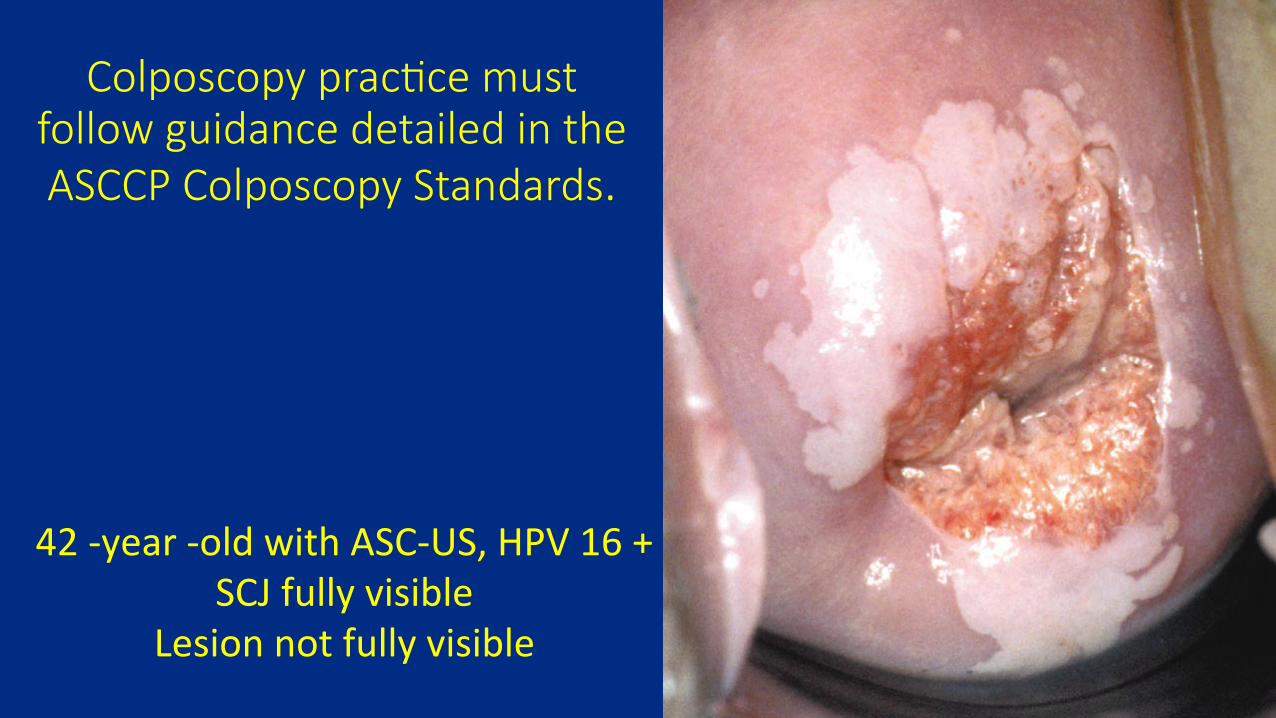
2019GuidingPrinciple#4
ColposcopypracticemustfollowguidancedetailedintheASCCPColposcopyStandards.
• Colposcopywithtargetedbiopsyremainstheprimarymethodofdetectingprecancersrequiringtreatment.
• Biopsiesshouldbetakenofalldiscreteacetowhiteareas,usually2-4biopsies/colposcopy.
• ASCCPStandardsemphasizetheneedforbiopsiesevenwhenthecolpoimpressionisnormalbutanydegreeofacetowhiteness,metaplasiaorotherabnormalityispresent.
KhanMJ,WernerCL,DarraghTM,etal.ASCCPColposcopyStandards:RoleofColposcopy.JLowerGenitTractDis2017;21:223-229.
2019 Guiding Principle #4
Colposcopy prac&ce must follow guidance detailed in the ASCCP Colposcopy Standards.
42-year-oldwithASC-US,HPV16+SCJfullyvisible
Lesionnotfullyvisible
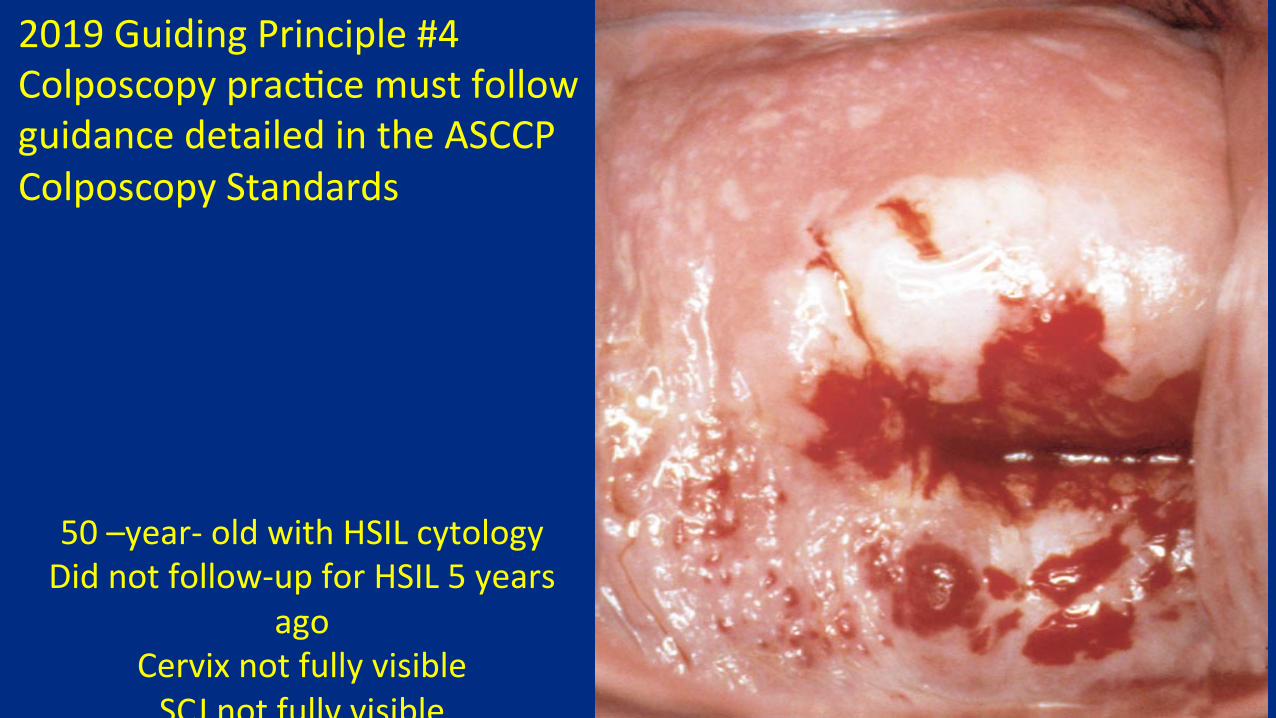
2019GuidingPrinciple#4Colposcopyprac=cemustfollowguidancedetailedintheASCCPColposcopyStandards
50–year-oldwithHSILcytologyDidnotfollow-upforHSIL5years
agoCervixnotfullyvisibleSCJnotfullyvisible
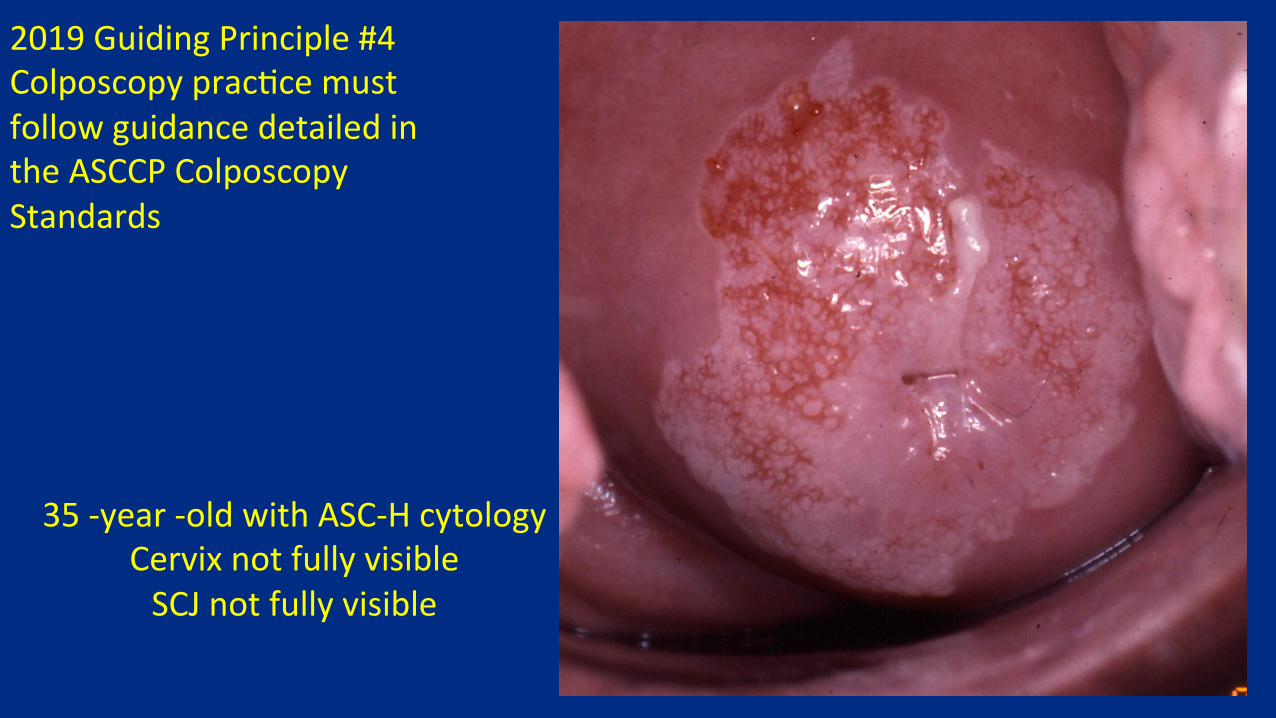
2019GuidingPrinciple#4Colposcopyprac=cemustfollowguidancedetailedintheASCCPColposcopyStandards
35-year-oldwithASC-HcytologyCervixnotfullyvisibleSCJnotfullyvisible
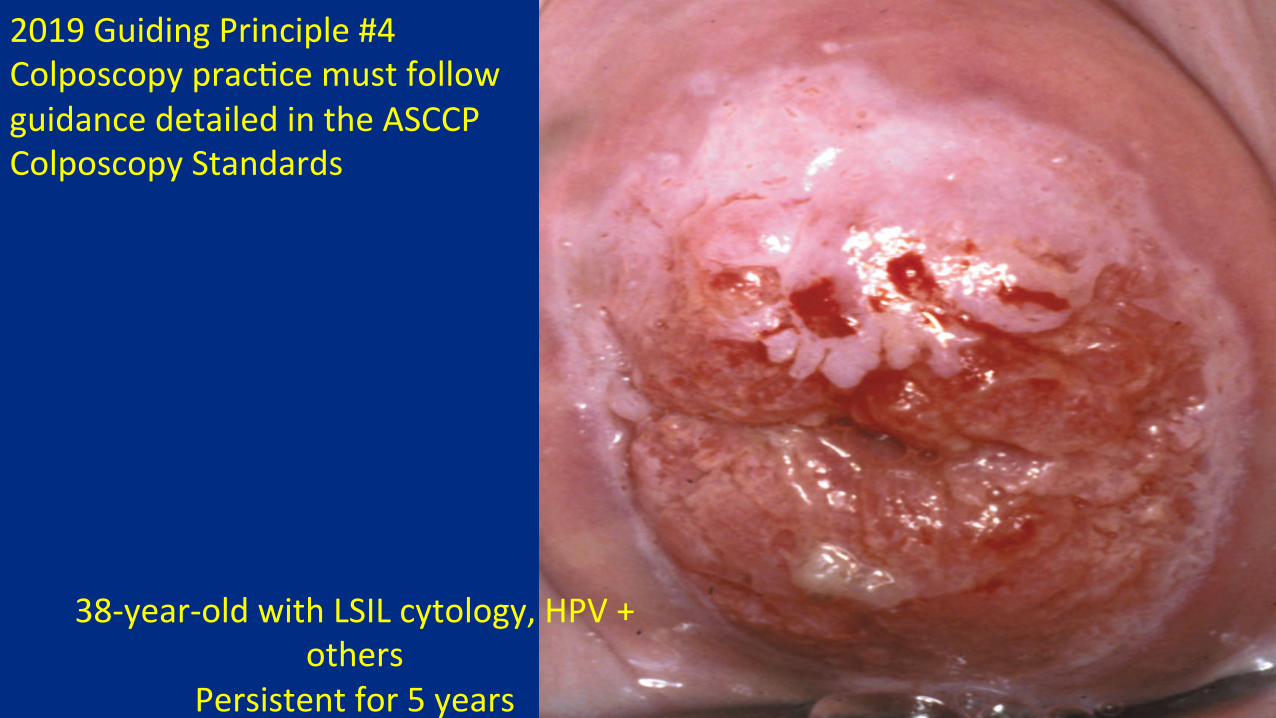
38-year-oldwithLSILcytology,HPV+others
Persistentfor5yearsSCJfullyvisible
2019GuidingPrinciple#4Colposcopyprac=cemustfollowguidancedetailedintheASCCPColposcopyStandards
Formanagement
Howpa=entriskisevaluatedforcurrentresultsandhistoryTheimmediateCIN3+riskisexamined
Treatmentor
Colposcopy
Determinewhetherpa=entsshouldreturnin1,3or5years

Thanks!
Related Documents











