Form No. 3-189 (09-17) 2018 Dental Choice & Dental Choice Plus Coverage for individuals & families One Mission: You Meridian 3000 E. Pine Ave. Meridian, ID 83642 Lewiston 866-841-2583 208-746-0531 Pocatello 275 S. 5th Ave. Pocatello, ID 83201 208-232-6206 Twin Falls 1503 Blue Lakes Blvd. N. Twin Falls, ID 83301 208-733-7258 Idaho Falls 1910 Channing Way Idaho Falls, ID 83404 208-522-8813 Coeur d’Alene 1450 NW Blvd., Suite 106 Coeur d’Alene, ID 83814 208-666-1495 Blue Cross of Idaho Sales 888-462-7677 Customer Service 800-365-2345 bcidaho.com One Mission: You © 2017 by Blue Cross of Idaho, an independent licensee of the Blue Cross and Blue Shield Association Parent or Guardian Consent to Application By completing this section and signing this application, I represent that the person listed as the applicant on this application is under 18 years of age and is making application for health coverage with my full knowledge and consent. I hereby accept full responsibility for the payment of premiums and the answers and information provided in this application. Print Name _______________________________________________________________________________________Date (mm/dd/yyyy)__________________ Address (if different than dependent) _________________________________________________________________ Statement of Understanding By signing this application, I represent that all my answers are complete and accurate to the best of my knowledge and belief and that I understand and agree to the following conditions: • No independent producer, agent or employee of the insurance carrier can change any part of this application or waive the requirement that I answer all questions completely and accurately. • The insurance carrier may terminate or rescind an insured’s coverage for any intentional misrepresentation, omission of fact by, concerning or on behalf of any insured that was or would have been material to the insurance carrier’s acceptance of a risk, extension of coverage, provision of benefits, or payment of any claim. • If this application is approved, coverage for me and any eligible persons named on this application will begin on the effective date assigned by the insurance carrier. • I understand that this application will become part of the contract between the insurance carrier and me. • I affirm that I have reviewed all answers given on this application and, regardless of whether an independent producer or other person has filled out the answers for me, I verify that the answers are true and complete. I acknowledge and understand my health plan may request or disclose health information about me or my dependents (persons who are eligible for benefits coverage and are listed on the application) for the purpose of facilitating healthcare treatment, payment or for the purpose of business operations necessary to administer healthcare benefits; or as required by law. Health information requested or disclosed may be related to treatment or services performed by: • A physician, dentist, pharmacist or other physical or behavioral healthcare practitioner; • A clinic, hospital, long-term care or other medical facility; • Any other institution providing care, treatment, consultation, pharmaceuticals or supplies or; • An insurance carrier or group health plan. Health information requested or disclosed may include, but is not limited to: claims records, correspondence, medical records, billing statements, diagnostic imaging reports, laboratory reports, dental records, or hospital records (including nursing records and progress notes). I affirm the answers in this “Dental Choice/Dental Choice Plus Individual Enrollment Application” are complete and correct. I am providing these answers as part of the application procedure required by this insurance carrier to enroll in its insurance coverage. I understand that the insurance carrier will rely on each answer in making its determination to extend coverage and to determine the type of coverage offered. I understand if I have made any misstatement or omission in this application, the insurance carrier may take any action available by law, including but not limited to, retroactive adjustment of premiums or claims. Further, I understand that any fraud or intentional misrepresentation of material fact in my completion of this application is cause for retroactive termination of coverage by the insurance carrier and/or other action available at law. I will promptly inform the insurance carrier in writing if anything happens before my coverage takes effect that makes an answer on this application incomplete or incorrect. Following receipt of a fully-executed application, coverage will be in force as of the effective date determined by the insurance carrier under applicable law. _____________________________________________ ________________ Applicant/Responsible Party Signature Date _____________________________________________ ________________ Spouse’s Signature (if applying for coverage) Date Independent Producer (Agent) Information Agent’s Name Blue Cross of Idaho No. Signature of Agent Date (mm/dd/yy) For Office Use Only Electronic System ID Form No. 3-189A (09-16) 18-080-01/18 18-081-01/18 Policy Form Numbers: 18-079-01/18

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Form No. 3-189 (09-17)
2018 Dental Choice &
Dental Choice Plus Coverage for
individuals & families
One Mission: You
Meridian3000 E. Pine Ave.
Meridian, ID 83642
Lewiston866-841-2583208-746-0531
Pocatello275 S. 5th Ave.
Pocatello, ID 83201208-232-6206
Twin Falls1503 Blue Lakes Blvd. N.
Twin Falls, ID 83301208-733-7258
Idaho Falls1910 Channing Way
Idaho Falls, ID 83404208-522-8813
Coeur d’Alene1450 NW Blvd., Suite 106Coeur d’Alene, ID 83814
208-666-1495
Blue Cross of IdahoSales 888-462-7677
Customer Service 800-365-2345
bcidaho.com
One Mission: You
© 2017 by Blue Cross of Idaho, an independent licensee of the Blue Cross and Blue Shield Association
Parent o
r Gu
ardian
Co
nsen
t to A
pp
lication
By co
mp
leting
this sectio
n an
d sig
nin
g th
is app
lication
, I represen
t that th
e perso
n listed
as the ap
plican
t on
this ap
plicatio
n is u
nd
er 18 years of ag
e an
d is m
aking
app
lication
for h
ealth coverag
e with
my fu
ll kno
wled
ge an
d co
nsen
t. I hereb
y accept fu
ll respo
nsib
ility for th
e paym
ent o
f prem
ium
s an
d th
e answ
ers and
info
rmatio
n p
rovided
in th
is app
lication
.
Print N
ame _______________________________________________________________________________________D
ate (mm
/dd/yyyy) __________________A
dd
ress (if different than dependent) _________________________________________________________________
Statem
ent o
f Un
derstan
din
gB
y sign
ing
this ap
plicatio
n, I rep
resent th
at all my an
swers are co
mp
lete an
d accu
rate to th
e best o
f my kn
ow
ledg
e and
belief an
d th
at I u
nd
erstand
and
agree to
the fo
llow
ing
con
ditio
ns:
• N
o independent producer, agent or employee of the insurance carrier can change
any part of this application or waive the requirem
ent that I answer all questions
completely and accurately.
• The insurance carrier m
ay terminate or rescind an insured’s coverage for any
intentional misrepresentation, om
ission of fact by, concerning or on behalf of any insured that w
as or would have been m
aterial to the insurance carrier’s acceptance of a risk, extension of coverage, provision of benefits, or paym
ent of any claim.
• If this application is approved, coverage for m
e and any eligible persons named on this
application will begin on the effective date assigned by the insurance carrier.
• I understand that this application w
ill become part of the contract betw
een the insurance carrier and m
e.•
I affirm that I have review
ed all answers given on this application and, regardless of
whether an independent producer or other person has filled out the answ
ers for me, I
verify that the answers are true and com
plete.I ackn
ow
ledg
e and
un
derstan
d m
y health
plan
may req
uest o
r disclo
se h
ealth in
form
ation
abo
ut m
e or m
y dep
end
ents (p
erson
s wh
o are elig
ible
for b
enefits coverag
e and
are listed o
n th
e app
lication
) for th
e pu
rpo
se of
facilitating
health
care treatmen
t, paym
ent o
r for th
e pu
rpo
se of b
usin
ess o
peratio
ns n
ecessary to ad
min
ister health
care ben
efits; or as req
uired
by
law.
Health
info
rmatio
n req
uested
or d
isclosed
may b
e related to
treatmen
t or
services perfo
rmed
by:
• A
physician, dentist, pharmacist or other physical or behavioral healthcare practitioner;
• A
clinic, hospital, long-term care or other m
edical facility;•
Any other institution providing care, treatm
ent, consultation, pharmaceuticals or
supplies or;•
An insurance carrier or group health plan.
Health
info
rmatio
n req
uested
or d
isclosed
may in
clud
e, bu
t is no
t limited
to
: claims reco
rds, co
rrespo
nd
ence, m
edical reco
rds, b
illing
statemen
ts, d
iagn
ostic im
agin
g rep
orts, lab
orato
ry repo
rts, den
tal record
s, or h
osp
ital reco
rds (in
clud
ing
nu
rsing
record
s and
pro
gress n
otes).
I affirm th
e answ
ers in th
is “Den
tal Ch
oice/D
ental C
ho
ice Plu
s Ind
ividu
al E
nro
llmen
t Ap
plicatio
n” are com
plete an
d co
rrect. I am p
rovidin
g
these an
swers as p
art of th
e app
lication
pro
cedu
re requ
ired by th
is in
suran
ce carrier to en
roll in
its insu
rance coverage. I u
nd
erstand
th
at the in
suran
ce carrier will rely o
n each
answ
er in m
aking
its d
etermin
ation
to exten
d coverage an
d to
determ
ine th
e type o
f coverage o
ffered. I u
nd
erstand
if I have m
ade any m
isstatemen
t or
om
ission
in th
is app
lication
, the in
suran
ce carrier may take any actio
n
available by law
, inclu
din
g b
ut n
ot lim
ited to, retro
active adju
stmen
t of
prem
ium
s or claim
s. Furth
er, I un
derstan
d th
at any fraud
or in
tentio
nal
misrep
resentatio
n o
f material fact in
my co
mp
letion
of th
is app
lication
is cau
se for retro
active termin
ation
of coverage by th
e insu
rance carrier
and
/or o
ther actio
n availab
le at law. I w
ill pro
mp
tly info
rm th
e insu
rance
carrier in w
riting
if anythin
g h
app
ens b
efore m
y coverage takes effect th
at makes an
answ
er on
this ap
plicatio
n in
com
plete o
r inco
rrect. Fo
llowin
g receip
t of a fu
lly-executed
app
lication
, coverage will b
e in
force as o
f the effective d
ate determ
ined
by the in
suran
ce carrier un
der
app
licable law
.
_____________________________________________ ________________
Ap
plican
t/Resp
on
sible Party S
ign
ature
Date
_____________________________________________ ________________
Sp
ou
se’s Sig
natu
re (if applying for coverage) D
ate
Ind
epen
den
t Pro
du
cer (Agen
t) Info
rmatio
nA
gent’s N
ame
Blu
e Cro
ss of Id
aho
No.
Sig
natu
re of A
gent
Date (m
m/d
d/yy)
For O
ffi ce Use O
nly
Electro
nic S
ystem ID
Form N
o. 3-189A (09-16)
18-080-01/1818-081-01/18
Policy Form Numbers:18-079-01/18

Healthy teeth, healthy bodyDid you know that your overall health is affected by your oral health?
Our Dental Choicesm and Dental Choice Plussm plans offer low deductibles and out-of-pocket maximums, with no waiting periods for Basic and Major Dental Services for kids.
Whatever plan you’re looking for, we’ve got you covered.
STOP PROBLEMS BEFORE THEY START
Preventive care is a top priority under both the Dental Choice and Dental Choice Plus plans. In fact, after you pay a low copayment, we pick up 100 percent of the dentist's charge for your preventive dental care when you see an in-network dentist.
Preventive services include regular exams, cleanings, X-rays and fluoride treatment.
It’s important to know that pediatric dental insurance is considered one of the 10 essential health benefits according to the Affordable Care Act.
Our Dental Choice and Dental Choice Plus plans for children meet all of the ACA requirements.
ACA ALL THE WAY
Den
tal C
ho
ice/
Den
tal C
ho
ice
Plu
sIn
div
idu
al E
nro
llmen
t A
pp
licat
ion
Ap
plic
ant
Info
rmat
ion
You
are
: o
New
Ap
plic
ant
o
Res
po
nsi
ble
Par
ty (
Ap
ply
ing
on
ly f
or
dep
end
ent
cove
rag
e)
You
r N
ame
(firs
t, in
itia
l, la
st)
So
cial
Sec
uri
ty N
um
ber
D
ate
of
Bir
th (
mm
/dd
/yyy
y)
Ag
eo
Mal
e o
Fem
ale
Phy
sica
l Ad
dre
ssC
ity,
Sta
te, Z
ip C
od
eC
ou
nty
Mai
ling
Ad
dre
ss (
stre
et o
r ro
ute
)C
ity,
Sta
te, Z
ip C
od
eC
ou
nty
Bill
ing
Ad
dre
ss (
if d
iffer
ent
fro
m m
ailin
g a
dd
ress
)C
ity,
Sta
te, Z
ip C
od
eC
ou
nty
Idah
o R
esid
ent
o Y
es
o N
oPr
efer
red
Ph
on
e
Alt
ern
ate
Ph
on
eo
I d
on’
t h
ave
a p
ho
ne
Em
ail A
dd
ress
Mar
ital
Sta
tus
o
Sin
gle
o
Mar
ried
Do
yo
u h
ave
a cu
rren
t Id
aho’
s d
rive
r’s
licen
se o
r Id
aho
iden
tifi
cati
on
car
d?
o Y
es
o N
oId
aho
dri
ver’
s lic
ense
or
iden
tifi
cati
on
car
d n
um
ber
___
____
____
____
____
____
____
____
____
____
_ E
xpir
atio
n d
ate
____
____
____
__ If
yo
u a
re u
nab
le t
o p
rovi
de
an Id
aho
dri
ver’
s lic
ense
or
iden
tifi
cati
on
car
d n
um
ber
, to
est
ablis
h r
esid
ency
yo
u m
ust
pro
vid
e co
pie
s o
f tw
o o
ther
fo
rms
of
do
cum
enta
tio
n t
hat
co
nta
in y
ou
r n
ame
and
res
iden
tial
ad
dre
ss w
ith
th
is c
om
ple
ted
ap
plic
atio
n.
Exa
mp
les
incl
ud
e h
om
e m
ort
gag
e st
atem
ent;
leas
e o
r lo
an a
gre
emen
t; h
om
eow
ner
’s, r
ente
r’s,
or
car
insu
ran
ce p
olic
y; o
r cu
rren
t b
ank
stat
emen
ts
(wit
hin
th
e la
st 6
0 d
ays)
. Th
ese
do
cum
ents
mu
st c
on
tain
th
e ap
plic
ant’s
nam
e an
d r
esid
enti
al a
dd
ress
.
Dep
end
ent
Info
rmat
ion
– L
ist a
ll el
igib
le d
epen
dent
s yo
u w
ish
to e
nrol
l, in
clud
ing
any
child
who
is u
nder
the
age
of 2
6 or
who
is m
edic
ally
cer
tifie
d as
dis
able
d an
d de
pend
ent u
pon
you
for s
uppo
rt (c
opy
of c
ertif
icat
ion
requ
ired)
. If y
ou h
ave
mor
e de
pend
ents
to in
clud
e, m
ake
a co
py o
f thi
s pa
ge a
nd a
ttac
h.
List
all
elig
ible
dep
end
ents
yo
u w
ish
to
en
roll,
incl
ud
ing
any
ch
ild w
ho
is u
nd
er t
he
age
of
26; o
r w
ho
is m
edic
ally
cer
tifi
ed a
s d
isab
led
an
d
dep
end
ent
on
par
ent
for
sup
po
rt
(co
py
of
cert
ific
atio
n r
equ
ired
).
Dep
end
ent
1: L
egal
Nam
e (fi
rst,
mid
dle
init
ial,
last
)R
elat
ion
ship
:
o L
egal
sp
ou
se
o C
hild
o
Ste
p-c
hild
o
Oth
erG
end
er:
o M
ale
o F
emal
e
So
cial
Sec
uri
ty N
um
ber
(re
qu
ired
)
D
ate
of
Bir
th (m
m/d
d/yy
)D
oes
dep
end
ent
1 liv
e at
th
e sa
me
add
ress
as
you
? o
Yes
o N
o
Dep
end
ent
2: L
egal
Nam
e (fi
rst,
mid
dle
init
ial,
last
)R
elat
ion
ship
:
o L
egal
sp
ou
se
o C
hild
o
Ste
p-c
hild
o
Oth
erG
end
er:
o M
ale
o F
emal
e
So
cial
Sec
uri
ty N
um
ber
(re
qu
ired
)
D
ate
of
Bir
th (m
m/d
d/yy
)D
oes
dep
end
ent
2 liv
e at
th
e sa
me
add
ress
as
you
? o
Yes
o N
o
Dep
end
ent
3: L
egal
Nam
e (fi
rst,
mid
dle
init
ial,
last
)R
elat
ion
ship
:
o L
egal
sp
ou
se
o C
hild
o
Ste
p-c
hild
o
Oth
erG
end
er:
o M
ale
o F
emal
e
So
cial
Sec
uri
ty N
um
ber
(re
qu
ired
)
D
ate
of
Bir
th (m
m/d
d/yy
)D
oes
dep
end
ent
3 liv
e at
th
e sa
me
add
ress
as
you
? o
Yes
o N
o
Dep
end
ent
4: L
egal
Nam
e (fi
rst,
mid
dle
init
ial,
last
)R
elat
ion
ship
:
o L
egal
sp
ou
se
o C
hild
o
Ste
p-c
hild
o
Oth
erG
end
er:
o M
ale
o F
emal
e
So
cial
Sec
uri
ty N
um
ber
(re
qu
ired
)
D
ate
of
Bir
th (m
m/d
d/yy
)D
oes
dep
end
ent
4 liv
e at
th
e sa
me
add
ress
as
you
? o
Yes
o N
o
Pre
miu
m C
alcu
lati
on
– 1
st m
onth
’s p
rem
ium
requ
ired
with
app
licat
ion.
Tota
l pre
miu
m is
cal
cula
ted
on a
per
-per
son
basi
s. P
rem
ium
s fo
r dep
ende
nts
unde
r age
19
are
capp
ed a
t a 3
-chi
ld ra
te w
ith A
pplic
ant c
over
age.
See
Pre
miu
m C
hart
for a
pplic
able
rate
s.
Req
ues
ted
Eff
ecti
ve d
ate:
___
____
___
/___
____
___
/___
____
___
(Ear
liest
effe
ctiv
e da
te w
ill b
e th
e 1s
t of
the
mon
th f
ollo
win
g re
ceip
t of
app
licat
ion
and
prem
ium
pay
men
t)
Pla
n S
elec
ted
: o
Den
tal C
ho
ice
o
Den
tal C
ho
ice
Plu
sN
OT
E: F
or
enro
llees
ove
r ag
e 19
, bo
th p
lan
s h
ave
a si
x-m
on
th w
aiti
ng
per
iod
fo
r B
asic
Den
tal S
ervi
ces
and
12-
mo
nth
wai
tin
g p
erio
d f
or
Maj
or
Den
tal S
ervi
ces.
Ap
plic
ant
Prem
ium
– b
ased
on
ag
e; s
ee P
rem
ium
Ch
art
(writ
e in
N/A
if y
ou a
re r
espo
nsib
le p
arty
onl
y)$
Dep
end
ent
1 Pr
emiu
m –
bas
ed o
n a
ge;
see
Pre
miu
m C
har
t$
Dep
end
ent
2 Pr
emiu
m –
bas
ed o
n a
ge;
see
Pre
miu
m C
har
t$
Dep
end
ent
3 Pr
emiu
m –
bas
ed o
n a
ge;
see
Pre
miu
m C
har
t$
Dep
end
ent
4 Pr
emiu
m –
bas
ed o
n a
ge;
see
Pre
miu
m C
har
t$
Tota
l mo
nth
ly p
rem
ium
$
© 2
016
by B
lue
Cro
ss o
f Id
aho,
an
inde
pend
ent
licen
see
of t
he B
lue
Cro
ss a
nd B
lue
Shi
eld
Ass
ocia
tion
3000
E. P
ine
Ave
. • M
erid
ian
, Id
aho
836
42 •
208
-345
-455
0M
ailin
g A
dd
ress
: P.O
. Box
740
8 •
Bo
ise,
ID 8
3707
-140
8
Form
No.
3-1
89A
(09-
16)

We are whereyou areNo matter if you're at home or on the road, your Blue Cross of Idaho dental plan gives you access to quality dental care. Our network includes more than 4 out of 5 Idaho dentists and over 240,000 dental providers across the United States. Locating a network provider is easy: just visit bcidaho.com/findaprovider to find a dentist near you.

Dental Choice (Under Age 19)
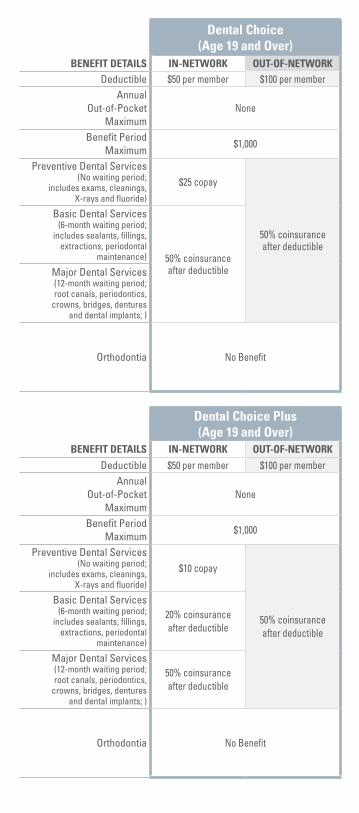
Dental Choice (Age 19 and Over)
BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORK BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORKDeductible $0 per member $100 per member Deductible $50 per member $100 per member
Annual Out-of-Pocket
Maximum
$350 Individual/ $700 Two or more $10,000
Annual Out-of-Pocket
Maximum None
Benefit Period Maximum
NoneBenefit Period
Maximum$1,000
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$25 copay
50% coinsurance after deductible
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$25 copay
50% coinsurance after deductible
Basic Dental Services (No waiting period;
includes sealants, fillings, extractions, periodontal
maintenance)
50% coinsurance after deductible
Basic Dental Services (6-month waiting period;
includes sealants, fillings, extractions, periodontal
maintenance) 50% coinsurance after deductibleMajor Dental Services
(No waiting period; root canals, periodontics,
crowns, bridges, dentures and dental implants)
Major Dental Services (12-month waiting period; root canals, periodontics,
crowns, bridges, dentures and dental implants; )
Orthodontia (For medically-necessary,
non-cosmetic treatment in accordance with Blue Cross
of Idaho medical policies; prior authorization required)
80% coinsurance after deductible Orthodontia No Benefit
Dental Choice Plus (Under Age 19)
Dental Choice Plus (Age 19 and Over)
BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORK BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORKDeductible $0 per member $100 per member Deductible $50 per member $100 per member
Annual Out-of-Pocket
Maximum
$350 Individual/ $700 Two or more $10,000
Annual Out-of-Pocket
Maximum None
Benefit Period Maximum
NoneBenefit Period
Maximum$1,000
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$15 copay
50% coinsurance after deductible
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$10 copay
50% coinsurance after deductible
Basic Dental Services (No waiting period;
includes sealants, fillings, extractions, periodontal
maintenance)
20% coinsurance after deductible
Basic Dental Services (6-month waiting period;
includes sealants, fillings, extractions, periodontal
maintenance)
20% coinsurance after deductible
Major Dental Services (No waiting period;
root canals, periodontics, crowns, bridges, dentures
and dental implants) 50% coinsurance after deductible
Major Dental Services (12-month waiting period; root canals, periodontics,
crowns, bridges, dentures and dental implants; )
50% coinsurance after deductible
Orthodontia (For medically-necessary,
non-cosmetic treatment in accordance with Blue Cross
of Idaho medical policies; prior authorization required)
80% coinsurance after deductible Orthodontia No Benefit
Dental Choice (Under Age 19)
Dental Choice (Age 19 and Over)
BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORK BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORKDeductible $0 per member $100 per member Deductible $50 per member $100 per member
Annual Out-of-Pocket
Maximum
$350 Individual/ $700 Two or more $10,000
Annual Out-of-Pocket
Maximum None
Benefit Period Maximum
NoneBenefit Period
Maximum$1,000
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$25 copay
50% coinsurance after deductible
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$25 copay
50% coinsurance after deductible
Basic Dental Services (No waiting period;
includes sealants, fillings, extractions, periodontal
maintenance)
50% coinsurance after deductible
Basic Dental Services (6-month waiting period;
includes sealants, fillings, extractions, periodontal
maintenance) 50% coinsurance after deductibleMajor Dental Services
(No waiting period; root canals, periodontics,
crowns, bridges, dentures and dental implants)
Major Dental Services (12-month waiting period; root canals, periodontics,
crowns, bridges, dentures and dental implants; )
Orthodontia (For medically-necessary,
non-cosmetic treatment in accordance with Blue Cross
of Idaho medical policies; prior authorization required)
80% coinsurance after deductible Orthodontia No Benefit
Dental Choice Plus (Under Age 19)
Dental Choice Plus (Age 19 and Over)
BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORK BENEFIT DETAILS IN-NETWORK OUT-OF-NETWORKDeductible $0 per member $100 per member Deductible $50 per member $100 per member
Annual Out-of-Pocket
Maximum
$350 Individual/ $700 Two or more $10,000
Annual Out-of-Pocket
Maximum None
Benefit Period Maximum
NoneBenefit Period
Maximum$1,000
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$15 copay
50% coinsurance after deductible
Preventive Dental Services (No waiting period;
includes exams, cleanings, X-rays and fluoride)
$10 copay
50% coinsurance after deductible
Basic Dental Services (No waiting period;
includes sealants, fillings, extractions, periodontal
maintenance)
20% coinsurance after deductible
Basic Dental Services (6-month waiting period;
includes sealants, fillings, extractions, periodontal
maintenance)
20% coinsurance after deductible
Major Dental Services (No waiting period;
root canals, periodontics, crowns, bridges, dentures
and dental implants) 50% coinsurance after deductible
Major Dental Services (12-month waiting period; root canals, periodontics,
crowns, bridges, dentures and dental implants; )
50% coinsurance after deductible
Orthodontia (For medically-necessary,
non-cosmetic treatment in accordance with Blue Cross
of Idaho medical policies; prior authorization required)
80% coinsurance after deductible Orthodontia No Benefit

Monthly Premium Rates for 2018
AGEDENTAL CHOICE
DENTAL CHOICE PLUS
0-20 $28.07 $34.05
21-24 $30.11 $34.97
25-29 $31.32 $36.37
30-34 $31.35 $36.41
35-39 $32.10 $37.29
40-44 $33.75 $39.20
45-49 $35.89 $41.68
50-54 $37.92 $44.04
55-59 $38.75 $45.00
60-64 $39.68 $46.09

Monthly Premium Rates for 2018
AGEDENTAL CHOICE
DENTAL CHOICE PLUS
0-20 $28.07 $34.05
21-24 $30.11 $34.97
25-29 $31.32 $36.37
30-34 $31.35 $36.41
35-39 $32.10 $37.29
40-44 $33.75 $39.20
45-49 $35.89 $41.68
50-54 $37.92 $44.04
55-59 $38.75 $45.00
60-64 $39.68 $46.09

GENERAL EXCLUSIONS AND LIMITATIONSThere are no benefits for services, supplies, drugs or other charges that are: Procedures that are not included in the Closed List of Dental Covered Services; or that are not Medically Necessary for the care of an Insured's covered dental condition; or that do not have uniform professional endorsement.Charges for services that were started prior to the Insured’s Effective Date. The following guidelines will be used to determine the date when a service is deemed to have been started: • For full dentures or partial dentures: on the date the final
impression is taken. • For fixed bridges, crowns, inlays or onlays: on the date the
teeth are first prepared.• For root canal therapy: on the later of the date the pulp
chamber is opened or the date canals are explored to the apex.
• For periodontal Surgery: on the date the Surgery is actually performed.
• For all other services: on the date the service is performed.
• For orthodontic services, if benefits are available under this Policy: on the date any bands or other appliances are first inserted.
Cast restorations (crowns, inlays or onlays) for teeth that are restorable by other means (i.e., by amalgam or composite fillings).Replacement of an existing crown, inlay or onlay that was installed within the preceding five (5) years or replacement of an existing crown, inlay or onlay that can be repaired. Appliances, restorations or other services provided or performed solely to change, maintain or restore vertical dimension or occlusion. A service for cosmetic purposes, unless necessitated as a result of Accidental Injuries received while the Insured was covered by Blue Cross of Idaho. In excess of the Maximum Allowance.A partial or full removable denture for fixed bridgework, or the addition of teeth thereto, if involving a replacement or modification of a denture or bridgework that was installed during the preceding five (5) years.Orthodontic services and supplies unless otherwise specifically listed in the Closed List of Dental Covered Services.Replacement of lost or stolen appliances.Ridge augmentation procedures.Any procedure, service or supply other than vestibuloplasty, alveoloplasty or alveolectomy required to prepare the alveolus, maxilla or mandible for a prosthetic appliance. Excluded services include, but are not limited to stomatoplasty and synthetic bone grafts to the alveolars, maxilla or mandible.Any procedure, service or supply required directly or indirectly to treat a muscular, neural, orthopedic or skeletal disorder, dysfunction or Disease of the temporomandibular joint (jaw hinge) and its associated structures including, but not limited to, myofascial pain dysfunction syndrome. Orthognathic Surgery, including, but not limited to, osteotomy, ostectomy and other services or supplies to augment or reduce the upper or lower jaw.Temporary dental services. Charges for temporary services are considered an integral part of the final dental services and are not separately payable. Any service, procedure or supply for which the prognosis for

success is not reasonably favorable. Myofunctional therapy and biofeedback procedures.For hospital Inpatient or Outpatient care for extraction of teeth or other dental procedures.Occlusal adjustments.Not prescribed by or upon the direction of a Provider.Investigational in nature.Provided for any condition, Disease, Illness or Accidental Injury to the extent that the Insured is entitled to benefits under occupational coverage, obtained or provided by or through the employer under state or federal Workers’ Compensation Acts or under Employer Liability Acts or other laws providing compensation for work-related injuries or conditions. This exclusion applies whether or not the Insured claims such benefits or compensation or recovers losses from a third party;Provided or paid for by any federal governmental entity or unit except when payment under this Policy is expressly required by federal law, or provided or paid for by any state or local governmental entity or unit where its charges therefor would vary, or are or would be affected by the existence of coverage under this Policy; orFor which payment has been made under Medicare Part A and/or Part B.Provided for any condition, Accidental Injury, Disease or Illness suffered as a result of any act of war or any war, declared or undeclared.Furnished by a Provider who is related to the Insured by blood or marriage and who ordinarily dwells in the Insured’s household.Received from a dental, vision or medical department maintained by or on behalf of an employer, a mutual benefit association, labor union, trust or similar person or group.For personal hygiene, comfort, beautification or convenience items even if prescribed by a Dentist, including but not limited to, air conditioners, air purifiers, humidifiers, physical fitness equipment or programs.For telephone consultations; for failure to keep a scheduled visit or appointment; for completion of a claim form; for interpretation services; or for personal mileage, transportation, food or lodging expenses, or for mileage, transportation, food or lodging expenses billed by a Dentist or other Provider.For Congenital Anomalies, or for developmental malformations, unless the patient is an Eligible Dependent child. For the treatment of injuries sustained while committing a felony, voluntarily taking part in a riot, or while engaging in an illegal act or occupation, unless such injuries are a result of a medical condition or domestic violence.For treatment or other health care of any Insured in connection with an Illness, Disease, Accidental Injury or other condition which would otherwise entitle the Insured to Covered Services under this Policy, if and to the extent those benefits are payable to or due the Insured under any medical payments provision, no fault provision, uninsured motorist provision, underinsured motorist provision, or other first party or no fault provision of any automobile, homeowner's or other similar policy of insurance, contract or underwriting plan. In the event Blue Cross of Idaho for any reason makes payment for or otherwise provides benefits excluded by this provision, it shall succeed to the rights of payment or reimbursement of the compensated Provider, the Insured, and the Insured's heirs and personal representative against all insurers, underwriters, self-insurers or other such obligors contractually liable or obliged to the Insured or his or her estate for such services, supplies, drugs or other charges so provided by Blue Cross of Idaho in connection with such Illness, Disease, Accidental Injury or

other condition.Any services or supplies for which an Insured would have no legal obligation to pay in the absence of coverage under this Policy or any similar coverage; or for which no charge or a different charge is usually made in the absence of insurance coverage or for which reimbursement or payment is contemplated under an agreement entered into with a third party.Provided to persons who were enrolled as Eligible Dependents after they cease to qualify as Eligible Dependents due to a change in eligibility status which occurs during the Policy term.Provided outside the United States, which if had been provided in the United States, would not be Covered Services under this Policy.Not directly related to the care and treatment of an actual condition, Illness, Disease or Accidental Injury.For acupuncture or hypnosis.Repair, removal, cleansing or reinsertion of Implants.Precision or semi-precision attachments (including Implants placed to support a fixed or removable denture).Denture duplication. Oral hygiene instruction.Treatment of jaw fractures.Charges for acid etching.Charges for oral cancer screening which are included in a regular oral examination.No benefits are available for replacement and/or repair of orthodontic appliances. This includes removable and/or fixed retainers.RIGHT TO REVIEW DENTAL WORK Before providing benefits for Covered Services, Blue Cross of Idaho has the right to refer the Insured to a Dentist of its choice and at its expense to verify the need, quantity and quality of dental work claimed as a benefit under this section. CARE RENDERED BY MORE THAN ONE (1) DENTIST If an Insured transfers from the care of one (1) Dentist to another Dentist during a Dental Treatment Plan, or if more than one (1) Dentist renders services for one (1) dental procedure, Blue Cross of Idaho will pay no more than the amount that it would have paid had but one (1) Dentist rendered the service. ALTERNATE TREATMENT PLAN If a Dentist and an Insured select a Dental Treatment Plan other than that which is customarily provided by the dental profession, payments of benefits available under this section shall be limited to the Dental Treatment Plan that is the standard and most economical, according to generally accepted dental practices.
Related Documents











