Prepared for the Foundation of the American College of Healthcare Executives Session 25AB Bringing Revenue Cycle Into The 21 st Century Presented by: Michael G. Brokloff, FACHE Caludia E. Crist, RN, FACHE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Prepared for the Foundation of the American College of Healthcare Executives
Session 25AB Bringing Revenue Cycle Into The 21st
Century
Presented by: Michael G. Brokloff, FACHE Caludia E. Crist, RN, FACHE


1
Bringing Revenue Cycle into the 21st Century
Course 25A,B
Mike Brokloff, FACHEClaudia Crist, RN, FACHE
Learning Objectives• Describe the business, cultural and patient cases
supporting the transformation to a shared services organization.
• Discuss the steps necessary to transform your organization to a shared services model: • Service level agreements• Service catalogs• Operating metrics
2

2
Presenter Bios
3
Michael Brokloff, MBA, FACHE joined Sutter Health in February of 2013 as part of the startup of its Shared Services Center in Roseville CA. As the Service and Performance Management Leader he directs the internal operations of the center including: metrics analysis and reporting, process improvement (Lean), business deployment and project management.
After serving in the US Navy, Mike joined GE as a Field Engineer and held positions in operations, sales and marketing leadership until leaving in 2001 for a startup opportunity.In 2004 Mike joined Philips Medical Systems / Dunlee as the Director of Glassware Solutions where he developed and launched a program that quickly grew for account for 1/3 of Dunlee’scommercial revenue. He later Joined DMS Health Group as their VP of Service, then returned to GE as a Director of Service in Northern California. He joined Sutter Shared Services in February of 2013.
Mike has an AS from the University of the State of New York, a BS from Brigham Young University, and an MBA from California State Polytechnic University. He is a Fellow in the American College of Healthcare Executives and on the board of the California Association of Healthcare Leaders.
Presenter Bios
4
Claudia Crist, RN, MHA, FACHE worked for Sutter Health from 2000 until her appointment in January 2015, to Deputy Director of Health Care Delivery Systems with the California Department of Health Care Services. At Sutter Health, she most recently served as Revenue Cycle Process Leader for Sutter Shared Services in Roseville, Sacramento.
Prior to her role in Revenue Cycle, Ms. Crist served as Assistant Administrator at Sutter Medical Center, Sacramento, a 600+ bed acute care hospital (2008-2013). Additional work experience and background include Leadership Training and Development, Internal Audit, Nursing (critical care, emergency, corrections), as well as Physician Assistant (Germany). Ms. Crist also served as lecturer for "U.S. Healthcare Delivery Systems" at the California State University Chico (2013-2014).
Ms. Crist earned her MHA from the University of Southern California, her BS in Health Care Administration from Bellevue University, and her BSN Degree from College of the Canyons. She is an alumna of the Sutter Health Leadership Academy and a Fellow of the American College of Healthcare Executives.

3
Agenda• Shared Services Model
• Change Levers
• Transformation Journey - Business Case
• Governance / Accountability
• Cultural Transformation
• Leadership Lesson Learned
• Q&A
5
A Bit About Sutter Health
6
• 5,000 physicians (physician medical foundation model; plus 4 IPAs); aligned under the Sutter Medical Network
• 24 acute care hospitals
• Approximately 48,000 employees
• $9.6 billion in revenues (2013)
• Home health and hospice services throughout Northern Calif.
• Outpatient surgery and specialty care centers
• Medical research and medical education/training
• 24 fundraising organizations
Serving more than 100 communities with:
6

4
What exactly is a Shared Services Organization?
• Not Centralization
• Not Outsourcing
• Business model that leverages resources across the organization to lower costs and drive standardization while meeting agreed upon Service Level Agreements.
• Integrated service model with:
– Client Governance
– Service Level Agreements
– Charge for services performed
7
Why a Shared Services Organization?
• In Recent Poll of Peeriosity Members, 61% of respondents indicated that cost savings, or productivity improvement was their primary reason for determining if a service should be a shared service
• Their #2 reason was to standardize their processes across their enterprise
8
5
Benefits of Shared Services
• Lower costs through standardization, productivity enhancements and economies of scale
• Standardizing on best practices across the organization
• Common patient / employee / vendor / clinician experience
• Service Level Agreements that clearly define service delivery standards
• Allows leadership to focus on patients and operating priorities because shared services are performed consistently
• Standardized systems and processes allow for meaningful metrics
9
Why Sutter Went With Shared Services
10
“It is our obligation to ensure all costs are the lowest they can be to prevent reduction or
elimination of essential services and programs in our communities.”
Sutter Health Senior Leadership
10

6
Video #1
11
Payment Restraint ACO’s implementationValue Based Purchasing Readmission penalties
Insurance Market Changes More High Deductible Health Plans
Access to Care ACA Health Insurance Exchanges Medicaid expansion
Employer Mandate Defined Employer Contributions
Payment Reform Bundled payments
Shifting Risks – Cost Mandates
2010
2020 +
12

7
Keys to Success
• Understanding that the current model is un-sustainable
• Executive Leadership and Sponsorship
• Well defined stakeholder governance (roles & responsibilities)
• Key Performance Metrics: agreed upon definitions and baseline
• A service mindset: from the back-room to the front-room
• Openness to change: “Not invented here”, embracing best practices
• A commitment to continuous improvement
13
Sutter Shared Services (S3)
14
Revenue Cycle
Human Resources
Supply Chain Finance
Credentials Verification eQuip
Performance Management

8
15
Project TimelineSutter Board approves project
Sutter Announces S3 – RosevilleS3 opens it’s doors
East Bay RCValley Biomed
Alta Bates RC
Sac FinanceValley RC
East Bay / PeninsulaBiomed
Peninsula RC Sutter CVSystem Supply Chain
Various PayrollVarious FinanceVarious HR
Sac RC 1
Sac RC 2
SurgeryCenter Acquisitions
Scheduling 35 New centers
Original Plan Complete
Video 3 r1

9
Video #4
18

10
Change Levers
19
BUSINESS PROCESS RE-ENGINEERING
Reduce, Simplify, Eliminate
SPEND MANAGEMNT
Strategic Sourcing, Facilities Spend
Optimization
ECONOMIES OF SKILL AND SCALE
Centers Of Expertise, Shared Services,
Outsourcing
TECHNOLOGY ENABLEMENT
Automation, IS Infrastructure/Systems Optimization
PERFORMANCE CULTURE
Accountability, Transparency and Measurability
Video 2 r1

11
21
1. Increased effectiveness/efficiency, reduced workforce
2. Different work force structure, elimination of duplicate efforts, favorable labor arbitrage, revised union contracts
3. Increase in “managed spend”, consolidated vendor contracts, reduced category options
4. Consolidated IT infrastructure, rationalized application portfolio, retired systems
5. Clear accountability, performance based rewards, control over services vs. workforce, no opt out solutions
Results from Using Performance Levers
21
Revenue CycleScheduling
Verification/Authorization
Financial Counseling/
POS Collection
Revenue Capture
Case Management
Coding
Health Information
Management
Billing/Follow Up
DenialsPre-
Admission
Customer Service
22

12
Revenue Cycle Business Case
23
Opportunity Types
Cost reduction
Net revenue improvement
One-time cash improvement
Business Case - Patient Access Services
24
Project
Annual Net Benefit
($M) Description of Business CaseAvoidable Write-off Improvement
$ 48 Reduce preventable insurance write-offs to improve net revenue capture.
Patient Liability Collection
$ 42 Increased patient liability collections / reduced bad debt

13
Shared Services Patient Access Center (Pre-Service)
Point of Service(at or near service)
Financial Clearance
Financial Counseling
Scheduled Services
Current State Future StateKey Gaps
One-stop registration for patients
Streamlined registration and validation processes
service / time of Varying pre-service / time of service patient experiences across entities
Limited self-service options for scheduling, pre-service processing, and check-in
Duplicate requests for patient data within and across entities
Workflow not always automated
Limited up front patient liability estimation, communication and collection
Multiple entry / exit points with some intake areas not reporting directly to Patient Access
Sac Sierra
Regional Contact Center
Patient Access Initiative
Multiple Access Points
PCR CVR
East Bay West Bay
Regional Contact Center
Entity-based Financial Clearance
Entity-based Financial Clearance
Multiple Access Points
Multiple Access Points
Entity-based Financial Clearance
Multiple Access Points
Multiple Access Points
25
Operating Model Patient Access Center
26
Sutter Health – Patient Access Center
Financial ClearancePrimarily outbound callsAccount level management
Functions Include:
Financial ClearancePrimarily outbound callsAccount level management
Functions Include:
Pre-registration Completion Insurance Verification ABN / Medical Necessity Pre-certification / Authorization (initial)
Referral Management Patient Liability Estimation /
Notification / Collection Initiate Assessment of Financial
Counseling
Worklist and referral-driven work
Patient Access Center
Functions Included: Evaluation of assistance eligibility Assistance Applications /
Insurance Enrollment Self Pay Collections Payment Plan Options Low Interest Loans
On-site Financial
Counselors
Affiliate-based
services
Rea
l Tim
e R
efer
ral
Financial Counseling
Revenue Management Data Warehouse and Decision Support
Customer Excellence
Financial Clearance Worklist•Scheduled Accounts
• Unscheduled Admissions
Standardized P&P Standardized Technology Enablers Standardized QA and Training Standardized Metrics
Patient Access Clinical Resource
Assist with Medical Necessity, Authorizations and Level of Care Pre-Service, Liaison with Physician Office
Worklist-driven; exception-based work
26

14
Business Case - Charge Capture / Charge Description Master
27
Project Benefit Type
Annual Net Benefit
($M) Charge Capture Net Revenue
Improvement$ 17
Description of Business CaseAccuracy of charges captured and/or reimbursement associated with charges through enterprise-wide approach to coordinate, deploy and audit charge capture & reconciliation activities and CDM management.
Charge Capture and Charge Description Master Management
Current State
Enterprise level CDM with inconsistent regional charge master management
Future StateKey Gaps
• Multiple CDM items with same CPT Code
• Inconsistent data and charging
• Lack of standardization in charge master management across regions and affiliates
• Significant percentage of manual charge entry
• Potential for errors or missed charges
• High volume of paper orders from external providers
• Lack of specialized skills / knowledge Enterprise level CDM with standardized
charge master management
Charge capture accountability widely distributed and managed
inconsistently, driving compliance riskShared services support of charge
capture with joint accountability between department / practice and enterprise
Dedicated resources with appropriate skill level to support departments with
consistent and compliant CDM and charge capture activities
Charge Capture/CDM Initiative - Operating Model Migration
28

15
Operating Model - Charge Capture/CDMSutter Health Enterprise Standards
Charge Capture / CDM Shared Services
Level 2 –Shared responsibility to confirm accurate and complete charge capture for each encounter
Level 3 – High level monitoring of daily revenue to identify and manage anomalies
Provider Documentation
Charges
Codes
Charge Capture Audit Charge Capture Recovery (in
coordination with Disputed Claims/PFS)
Regulatory and Compliance Readiness
Local / Department / Practice
CDM Standardization
Charge Master Management
Item Master and CDM linkage
Regulatory and Compliance Readiness
Bil
lin
g S
yste
m
CDM Management
Ch
arg
e R
eco
nci
liati
on
an
d
Mo
nit
ori
ng
CDM Change Request
Level 1 – reconciling encounters to schedule
Local / Department / Practice
Exc
epti
on
-Bas
ed P
roce
ssin
gCharge Capture Audit
and Compliance
Provider Documentation/ Electronic Charge Capture
Real-time charge capture edits
Charge EditsHIM / Coding
feedback loop (documentation / charge discrepancies)
Reimbursement
Corporate Compliance
29
Business Case - Health Information Management
30
ProjectBenefit Type
AnnualNet
Benefit ($M) Description of Business Case
Hospital ProjectsCoding Performance Support
Cost Reduction
$ 1 Reduction in coding operating costs
HIM Operations Cost Reduction
$ 3 Reductions driven by leading practice productivity standards enabled by the consolidated enterprise model.

16
HIM (Coding and HIM Operations / Support)
Current State Future StateKey Gaps
training Inconsistent HIM training and QA processes
Wide variation in coding and documentation practices across entities
Multiple workarounds due to hybrid systems
Lack of standardization of processes leading to incomplete documentation
Lack of workload balancing
Regional and/or site-specific HIM coding and operations – managed
separately on hybrid systems
Enterprise HIM operations and coding – centrally managed with standardized processes, procedures and systems
Enterprise Shared Services HIM
HIM/Coding Initiative - Operating Model Migration
Record Completion Coding & Abstracting EMPI Support Release of Information Documentation / EHR
Support Health Information Access
& Monitoring
Sac Sierra
RegionalHIM
PCR CVR
East Bay West Bay
RegionalHIM
RegionalHIM
Regional HIM
Entity-based HIM
Site-based Functions• Medical Staff & Customer Support (ROI)• Administrative Support
Site-based Functions• Medical Staff & Customer Support (ROI)• Administrative Support
31
HIM Shared service workload management approach – single pool of resources cross-
trained to work across sites / regions Enable virtual / remote deployment of staff with centralized management Implementation of Computer Assisted Coding and Direct-to-Bill
Clinical Key clinical documentation required for coding and other functions available real-
time or within a standard defined service level agreement Clinical Documentation Improvement – integration between documentation and
coding
Department / Practices Structure and processes to continuously improve record completion processes
and timeliness; includes coordination and feedback loop among Coding, HIM Operations, medical staff leadership, Clinical Documentation Improvement (CDI), Quality, Risk and Case Management
HIM/Coding Initiative - Operating Model Migration
32
17
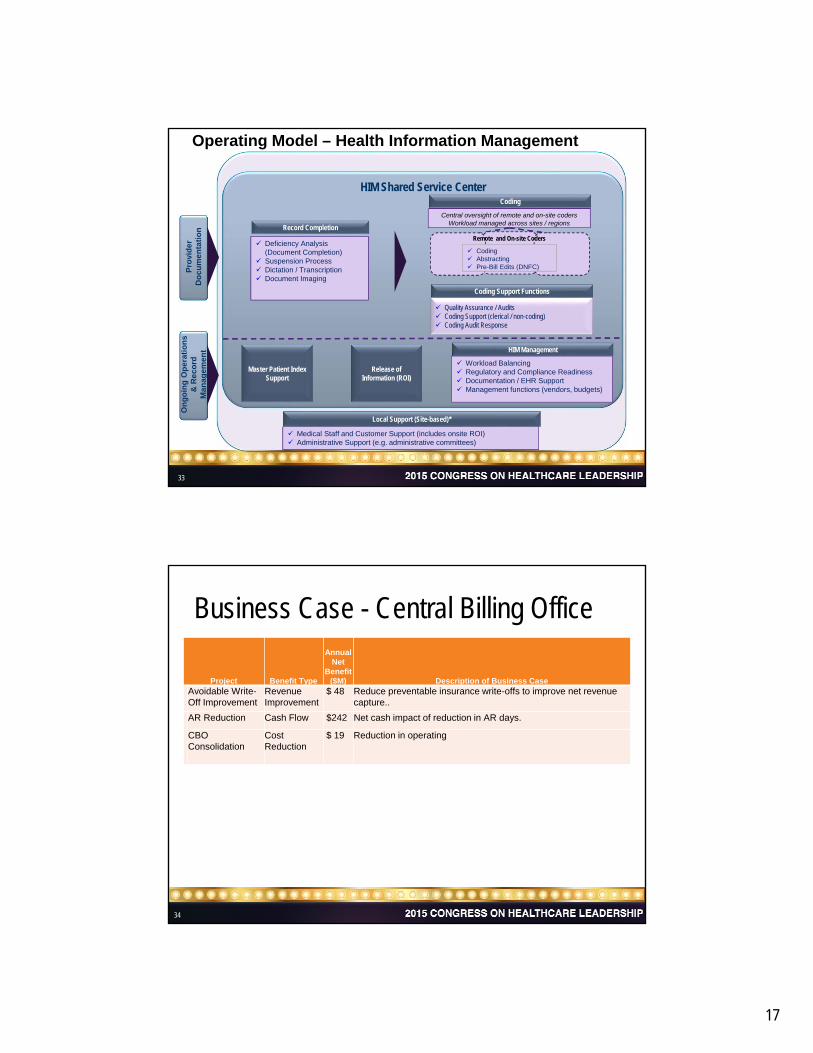
HIM Shared Service Center
Operating Model – Health Information Management
Central oversight of remote and on-site codersWorkload managed across sites / regions
Coding Support Functions
Quality Assurance / Audits Coding Support (clerical / non-coding) Coding Audit Response
Pro
vid
er
Do
cu
me
nta
tio
n
Deficiency Analysis (Document Completion)
Suspension Process Dictation / Transcription Document Imaging
Master Patient IndexSupport
Release of Information (ROI)
Workload Balancing Regulatory and Compliance Readiness Documentation / EHR Support Management functions (vendors, budgets)
Medical Staff and Customer Support (includes onsite ROI) Administrative Support (e.g. administrative committees) Medical Staff and Customer Support (includes onsite ROI) Administrative Support (e.g. administrative committees)
Local Support (Site-based)*
On
go
ing
Op
erat
ion
s &
Re
co
rd
Man
agem
ent
Remote and On-site Coders
Coding Abstracting Pre-Bill Edits (DNFC)
Coding
HIM Management
Record Completion
33
Business Case - Central Billing Office
34
Project Benefit Type
AnnualNet
Benefit($M) Description of Business Case
Avoidable Write-Off Improvement
Revenue Improvement
$ 48 Reduce preventable insurance write-offs to improve net revenue capture..
AR Reduction Cash Flow $242 Net cash impact of reduction in AR days.
CBO Consolidation
Cost Reduction
$ 19 Reduction in operating

18
Current State Future StateKey Gaps
CBO (Patient Financial Services) - Operating Model Migration
35
PFS Shared Services Center Hospital
Single CBO
Patient Financial Service Functions
CBOPFS
East Bay Region
Cornel FPO
~100% cash Posting
Central Valley Region
Peninsula Coastal Region
CBO PFS
West Bay Region
Sacramento Sierra Region Billing
CBOPFS
CBOPFS
CBOPFS
CBOPFS
Not leveraging economies of skill, scale and technology
Denial rates of 1-4% leaves significant uncollected $$
Too many manual processes and unnecessary rework
Inconsistent and confusing patient experience (billing & customer service)
Lack of consistent, standard policies and procedures across Regions to achieve best practice
Data / performance metrics and reporting not standardized across Region or enterprise
Use of different vendors across all entities with limited SLAs in place
Not leveraging economies of skill, scale and technology
Denial rates of 1-4% leaves significant uncollected $$
Too many manual processes and unnecessary rework
Inconsistent and confusing patient experience (billing & customer service)
Lack of consistent, standard policies and procedures across Regions to achieve best practice
Data / performance metrics and reporting not standardized across Region or enterprise
Use of different vendors across all entities with limited SLAs in place
Follow-up
Cash Posting
Denial Mgmt.
Core Support
Consolidate and standardize around an integrated best practice. Accelerate cash flow, reduce cost and write-offs
Clearly defined metrics and service level agreements to support expected outcomes
CustomerService
3535
Sutter Health – Patient Financial Shared Services
36
Standardized P&P Standardized Technology Enablers Standardized QA and Training Standardized Metrics
Revenue Management Data Warehouse and Decision Support
Customer Excellence
Claim Submission Resolution of pre-bill and payer claim edits Claim submission to re-engineered payer
relationship
Disputed Claims Resolution Direct denials to appropriate area for resolution Monitor resolution and accountability Track denial management and prevention efforts
Cash & Remittance Processing Electronic posting of third party payments Review of exception reports for manual posting Refund processing
Vendor Management Ensure accounts are transferred timely to vendors
for follow-up Generate and review KPI and dashboard reports
Follow-up Claims queued by payer, patient type Follow-up of unpaid claims that are not denied Analysis for over / under payment
Customer Service Respond to inbound customer inquiries Make outbound patient calls where necessary Review and process refund request
Sutter Health CBO Single CBO
CBO Consolidation Operating Model
36

19
Participants Responsibilities
Single Cross-Functional Committee:• Key Regional & Business
Executives• Key Corporate Function
Executives (HR, FI, etc)• SSS Executives/SVP
Strategic:• Formulate Shared Services strategic direction• Review Shared Services performance• Determine scope expansion (i.e. new functions)• Promote environment of joint commitment• Resolve strategic issues• Shared Services priorities
Multiple Single-FunctionCommittees:• Business Operational
Leads• SSS Executives
Tactical:• Respond to items from Super Users • Review performance and manage costs • Manage service expectations and SLAs• Monitor scope/ change requests • Resolve escalated issues (e.g. performance,
process design)
Multiple Single Sub-Functional Groups:• Business Process Users
(Super-Users)• Process Owners• Functional Managers
Operational:• Super User Committees provide functionally
specific feedback and serve as process champions
• Day to day queries regarding service delivery• Service performance issues• Resolve operational issues• First level of issue escalation
37
SSS
Steering
Committee
SSS Client Advisory Committees
SSS Functional
Super Users
Strategic Direction Setting
Issue Escalation
Performance
Governance / Accountability
37
Governance Impact
38
Enabling benefits beyond centralization
CENTRALIZATION SHARED SERVICES
ConsolidationRe-organization and de-layering
Resource Strategy
Re-engineeringSimplified, standardized system/process
SLAsClear 2-way services
agreed by clients
Performance Mgmt.Metrics, Targets,
Scorecards
Service/Cost Transparency
Global End-to-End Process
Visibility, Governance
Lack of Clarity Services, Costs
Corp. CultureTenure, wages, back-
office mentality
Exceptions Increase
Shadow Cost Increase
Benefits of centralization shrink due to lack of shared accountability for performance and increase in shadow cost over time
RA
NG
E O
F B
EN
EF
ITS
Transition from Centralization to Full Value of Shared Services
Many organizations stop here leaving value behind and decreasing the likelihood of sustainability and scalability
38

20
Approved by Support Function Transformation Steering Committee November 27th, 2012
Service: 3.5 Record Completion
Service Description:
This service addresses all inquiries for assembling and analyzing and completion of patient records.
Key Activities/Responsibilities:
ActivityResponsibility
S3 Client Other
Identification of chart / encounterdeficiency
X X
Processing of deficiency X
Completion of records X
Deficiency notification and suspension X
Service Measures:
Service Level Agreements:• 98% of deficiency analysis
validation completed within 24 hours
Operating Level Agreements:• < 5% delinquent (as defined by
state requirements -14 days) records for the system on a daily basis
How You Can Help:
Clients:Resolve identified deficiencies.
Clients:
Client & Customer: Operations
Chargeback Details:
Enter description of the chargeback model for this services.
Key Cost Drivers:
Enter key cost driver variables.
Sample Service Catalog Page
3939
Service Level Agreements
1. Output: Deficiency Analysis Completed2. Metric: Within 24 Hours3. Target: 98%
Clearly Defined Up FrontCost vs BenefitBest PracticeApproved by Client Advisory
Group and Steering Committee
40

21
Operating Level Agreements
1. Clearly define customer dependencies needed to meet SLA commitments
2. Measured and reported with SLAs
41
SLA Scorecard - How are we performing?
42

22
Cultural TransformationEveryone is Important• Everyone Contributes
• Performance trumps position
We Believe we Can Achieve • Change because we want to
• Proud to say “Not Invented Here”
43
Customer #1 Team #2 Me #3• Share everything
• Colaborate for greater success
Do What You Say You Will Do• Own it
• Don’t pass the buck
Paperless – Technology EnabledOpen – Shared & Collaborative Performance / Metrics Driven
Cultural Transformation
44

23
Cultural Transformation
45
• Develop your shared values and cultural statements before your start the first employee.
• Provide a fair and defendable process to transition impacted staff.
• Use limited term resources for all transitional work and strictly enforce PCD discipline.
• Invest in a strong New Employee Orientation. Everyone participates in the process - No exceptions.
• Set expectations: startup, still evolving, ask for help, do teambuilding
• Invest in communication: over-communicate, be clear and consistent, share the good the bad and the ugly.
Cultural Transformation
46
• Don’t hold out for a “best practice”. Start with strong, agreed upon work flows and process improve as you learn and grow.
• Design in LEAN or another process improvement methodology
• Must be perceived as fair to affected employees. Consider using a “salary place holder” for year 1st for negatively impacted salaries.
• Do all you can reasonably do to avoid lay-offs but ensure positions are eliminated from legacy organizations per business case.
• Listen to your employees so you understand their issues and perspectives BUT leadership decides priorities.
• Train, Train, Train: new processes, new technologies, new structure, new culture

24
Video #5
To Wrap Up
• Shared Services is an organizational transformation• Shared Services drive cost reduction through
Standardization, Best Practices, Automation, Consistent Patient Experience
• Consultants can help: Experience, Proven Change Models, Speed of Change but leadership must Own and Sponsor the transformation
• Change because you want to or be changed because you have to
48

25
Video #6
Q&A
50
26
Presenter Contact Information• Michael Brokloff, Service and Performance Leader
Sutter Shared Services
• (916) 297-9735
• Claudia Crist
• Revenue Cycle Operations Leader
• (916) 297 8000
51
BibliographyPeeriosity for Shared Services
Industry peer group for Shared Services Operations
www.peeriosity.com
Johns Hopkins University & Medicine Shared Services
Multi-Functional Shared Services Portal
http://ssc.jhmi.edu/
Barbara Quinn, Robert S. Cooke, Andrew Kris
Shared Services: Mining for Corporate Gold
Financial Times Prentice Hall, 2000
Donniel S. Schulman, Martin J. Harmer, John R. Dunleavy,
James S. Lusk
Shared Services: Adding Value to the Business Units
John Wiley & Sons 1999
Daniel C. Melchior Jr.
Shared Services: A Manager's Journey
John Wiley & Sons 2008
Kyle A. Schumacher, Ed.D.
Viewing The Impact of Shared Services Through The
Four Frames of Bolman and Deal
Department of Leadership, Educational Psychology and Foundations
Northern Illinois University, 2011
Mark Wnorowski
Simulation- Based Patient-Centered Shared Service Resource
Planning and Staffing
Binghamton University 2011
52

American College of Healthcare Executives
Disclosure of Relevant Financial Relationships
By Faculty and Planners of Continuing Education Activities
It is the policy of the American College of Healthcare Executives (ACHE) to ensure balance, independence, objectivity
and scientific rigor in all of its directly sponsored or jointly sponsored Continuing Education (CE) activities. The
intention of this policy is to identify potential conflicts of interest, facilitate resolution according to protocols, and ensure
that disclosure is provided to participants prior to the beginning of the activity so that learners may formulate their own
judgments as to the objectivity of the activity. Failure to disclose is grounds for dismissal as a faculty member or planner.
All individuals in a position to influence and/or control the content of ACHE directly and jointly sponsored CE activities
must disclose to ACHE and subsequently to learners that the individual has either no relevant financial relationships or
the nature of the financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of
commercial services discussed in the CE activities.
Conflict of Interest: Circumstances create a conflict of interest when an individual has received financial benefits in any
amount from a commercial interest within the past 12 months and that individual is in a position to affect the content of
CE regarding products or services of commercial interest.
Commercial Interest: A commercial interest is considered any entity producing, marketing, re-selling, or distributing
goods or services.
Financial Relationships: A financial interest is established by payments for various activities to the individual, the
individual’s spouse or partner by proprietary companies related to the content of a CE program. Examples of payments
that constitute financial interests include grants or research support, employment, consultation, speaking or teaching
activities, or royalties for companies. Financial interest also includes owning stock or options in any amount in these
types of companies.
Michael G. Brokloff, FACHEName:
Event Title: 2015 Congress on Healthcare Leadership
Program Title: Bringing Revenue Cycle Into The 21st Century (25A and 25B)
Relationship: Faculty
Do you or any immediate family member have a financial relationship or interest (currently or within the past 12 months)
with a proprietary entity? No
If Yes, please indicate the individual, organization and he nature of the financial relationship below.
Do you intend to discuss an unapproved/investigative use of a commercial product/device? If yes, please
disclosure such references to the learner in the educational activity. No
I will adhere to the ACHE policy on Conflict of Interest Disclosure. I will uphold the ACHE standard to insure
that balance, independence, objectivity and scientific rigor are maintained in the planning and presentation of
this CE activity.
Michael Brokloff October 03, 2014
DateSignature

American College of Healthcare Executives
Disclosure of Relevant Financial Relationships
By Faculty and Planners of Continuing Education Activities
It is the policy of the American College of Healthcare Executives (ACHE) to ensure balance, independence, objectivity
and scientific rigor in all of its directly sponsored or jointly sponsored Continuing Education (CE) activities. The
intention of this policy is to identify potential conflicts of interest, facilitate resolution according to protocols, and ensure
that disclosure is provided to participants prior to the beginning of the activity so that learners may formulate their own
judgments as to the objectivity of the activity. Failure to disclose is grounds for dismissal as a faculty member or planner.
All individuals in a position to influence and/or control the content of ACHE directly and jointly sponsored CE activities
must disclose to ACHE and subsequently to learners that the individual has either no relevant financial relationships or
the nature of the financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of
commercial services discussed in the CE activities.
Conflict of Interest: Circumstances create a conflict of interest when an individual has received financial benefits in any
amount from a commercial interest within the past 12 months and that individual is in a position to affect the content of
CE regarding products or services of commercial interest.
Commercial Interest: A commercial interest is considered any entity producing, marketing, re-selling, or distributing
goods or services.
Financial Relationships: A financial interest is established by payments for various activities to the individual, the
individual’s spouse or partner by proprietary companies related to the content of a CE program. Examples of payments
that constitute financial interests include grants or research support, employment, consultation, speaking or teaching
activities, or royalties for companies. Financial interest also includes owning stock or options in any amount in these
types of companies.
Claudia E. Crist, RN, FACHEName:
Event Title: 2015 Congress on Healthcare Leadership
Program Title: Bringing Revenue Cycle Into The 21st Century (25A and 25B)
Relationship: Faculty
Do you or any immediate family member have a financial relationship or interest (currently or within the past 12 months)
with a proprietary entity? No
If Yes, please indicate the individual, organization and he nature of the financial relationship below.
Do you intend to discuss an unapproved/investigative use of a commercial product/device? If yes, please
disclosure such references to the learner in the educational activity. No
I will adhere to the ACHE policy on Conflict of Interest Disclosure. I will uphold the ACHE standard to insure
that balance, independence, objectivity and scientific rigor are maintained in the planning and presentation of
this CE activity.
Claudia Crist September 30, 2014
DateSignature
Related Documents











