1 2014 Medical School Annual Return (MSAR) The Quality Lead is the nominated person within each medical school who will be our point of contact for this MSAR with us. If necessary, please include additional details of anyone who should receive feedback and other communications regarding the MSAR. Senior Managers signing off on behalf of the Medical School are responsible for assuring the quality and accuracy of the return. We work with the Medical Schools Council (MSC) in a number of policy areas and so will share information such as student profile and progression from your responses with them to support our work. We take our responsibilities under the Data Protection Act very seriously; any data you provide will be stored securely and confidentially. Please note that we are subject to the Freedom of Information Act 2000. If we receive a request, we may be required to disclose any information you provide to us unless a relevant exemption applies. We do not intend to publish the full MSAR returns from schools; however, we may publish selected information. There have been a number of revisions made to the 2014 MSAR in order to make it as easy as possible to complete. These alterations are described below: The total number of questions has reduced from 26 to 20. Whilst some have been removed or combined, there are also some new questions. We have highlighted the question numbers, theme and domains below. Question 5 – Domain 2 – Independent reviews of student complaints Question 10 - Domain 3 - Exit arrangements for students Questions 12 & 13 - Domain 5 - Prescribing Safety Assessment (PSA) and Medical Schools Council Assessment Alliance Question 20 – Additional question - Feedback on the Undergraduate Progression Reports which are due to be published at the end of September 2014. We have added three new fields to the MSAR Excel template ‘Section C 3 – SFtP’. These changes focus on professionalism and Student Fitness to Practice concerns. We appreciate that this data may not be accessible to all schools for this year’s return, and so are optional in 2014, but will be mandatory from 2015: For any professionalism or SFtP concern, please provide the Entry Method of that student. For any professionalism or SFtP concern, please provide the Location of Qualification Attainment of that student.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
2014 Medical School Annual Return (MSAR)
The Quality Lead is the nominated person within each medical school who will be our point of contact for this MSAR with us. If necessary, please include additional details of anyone who should receive feedback and other communications regarding the MSAR. Senior Managers signing off on behalf of the Medical School are responsible for assuring the quality and accuracy of the return. We work with the Medical Schools Council (MSC) in a number of policy areas and so will share information such as student profile and progression from your responses with them to support our work.
We take our responsibilities under the Data Protection Act very seriously; any data you provide will be stored securely and confidentially. Please note that we are subject to the Freedom of Information Act 2000. If we receive a request, we may be required to disclose any information you provide to us unless a relevant exemption applies. We do not intend to publish the full MSAR returns from schools; however, we may publish selected information.
There have been a number of revisions made to the 2014 MSAR in order to make it as easy as possible to complete. These alterations are described below:
The total number of questions has reduced from 26 to 20. Whilst some have been removed or combined, there are also some new questions. We have highlighted the question numbers, theme and domains below.
Question 5 – Domain 2 – Independent reviews of student complaints
Question 10 - Domain 3 - Exit arrangements for students Questions 12 & 13 - Domain 5 - Prescribing Safety Assessment (PSA) and Medical
Schools Council Assessment Alliance
Question 20 – Additional question - Feedback on the Undergraduate Progression
Reports which are due to be published at the end of September 2014.
We have added three new fields to the MSAR Excel template ‘Section C 3 – SFtP’. These changes focus on professionalism and Student Fitness to Practice concerns. We appreciate that this data may not be accessible to all schools for this year’s return, and so are optional in 2014, but will be mandatory from 2015:
For any professionalism or SFtP concern, please provide the Entry Method of that student.
For any professionalism or SFtP concern, please provide the Location of Qualification Attainment of that student.

2
If there is a professionalism or SFtP concern relating specifically to ‘Health’, please advise whether the concern relates to either ‘Adverse Physical Health’ or ‘Adverse mental Health’.
As in previous years, we request that you provide details of all low level professionalism concerns that have reached stages A – B of the process; and also all cases student fitness to practise cases reaching stages C – D of the process.
The deadline for this MSAR is 31st December 2014.
We want to make completing the MSAR as easy as possible, so if you need any help with completing this return, feel free to contact Nathan Brown or another member of the quality team on [email protected] or 020 7189 5221.
3
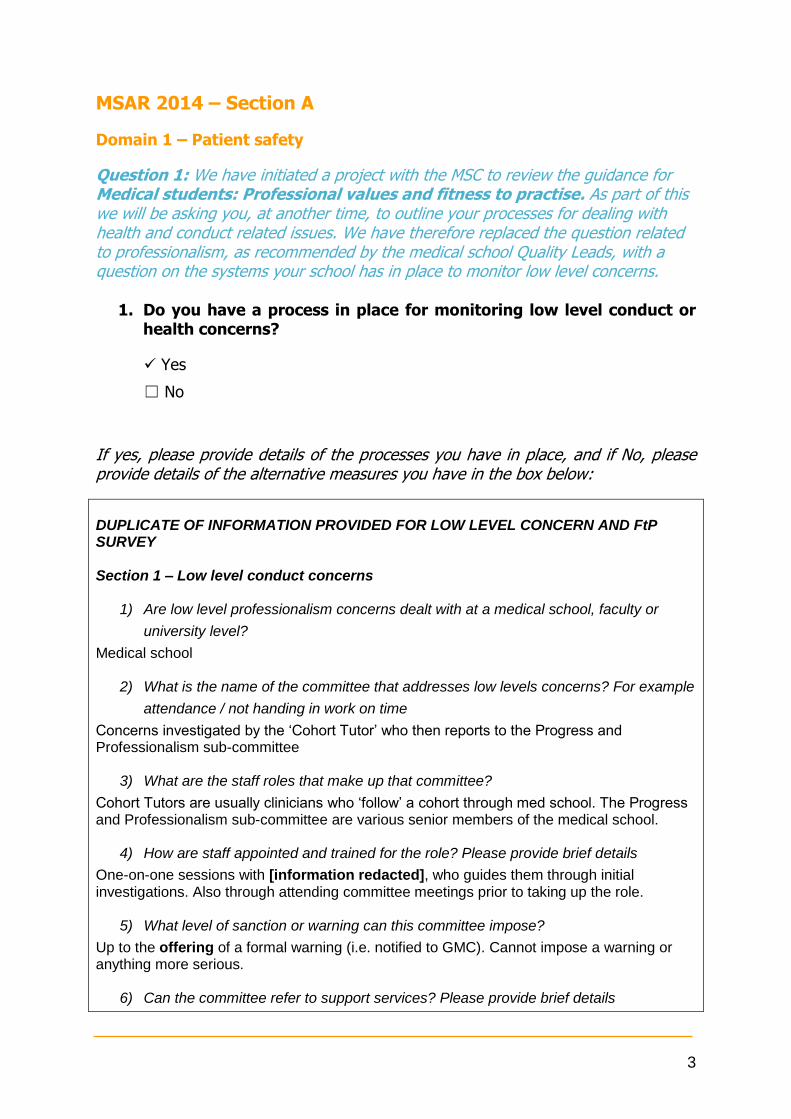
MSAR 2014 – Section A
Domain 1 – Patient safety
Question 1: We have initiated a project with the MSC to review the guidance for Medical students: Professional values and fitness to practise. As part of this we will be asking you, at another time, to outline your processes for dealing with health and conduct related issues. We have therefore replaced the question related to professionalism, as recommended by the medical school Quality Leads, with a question on the systems your school has in place to monitor low level concerns.
1. Do you have a process in place for monitoring low level conduct or health concerns?
Yes
☐ No
If yes, please provide details of the processes you have in place, and if No, please provide details of the alternative measures you have in the box below:
DUPLICATE OF INFORMATION PROVIDED FOR LOW LEVEL CONCERN AND FtP SURVEY Section 1 – Low level conduct concerns
1) Are low level professionalism concerns dealt with at a medical school, faculty or
university level?
Medical school
2) What is the name of the committee that addresses low levels concerns? For example
attendance / not handing in work on time
Concerns investigated by the ‘Cohort Tutor’ who then reports to the Progress and Professionalism sub-committee
3) What are the staff roles that make up that committee?
Cohort Tutors are usually clinicians who ‘follow’ a cohort through med school. The Progress and Professionalism sub-committee are various senior members of the medical school.
4) How are staff appointed and trained for the role? Please provide brief details
One-on-one sessions with [information redacted], who guides them through initial investigations. Also through attending committee meetings prior to taking up the role.
5) What level of sanction or warning can this committee impose?
Up to the offering of a formal warning (i.e. notified to GMC). Cannot impose a warning or anything more serious.
6) Can the committee refer to support services? Please provide brief details
4
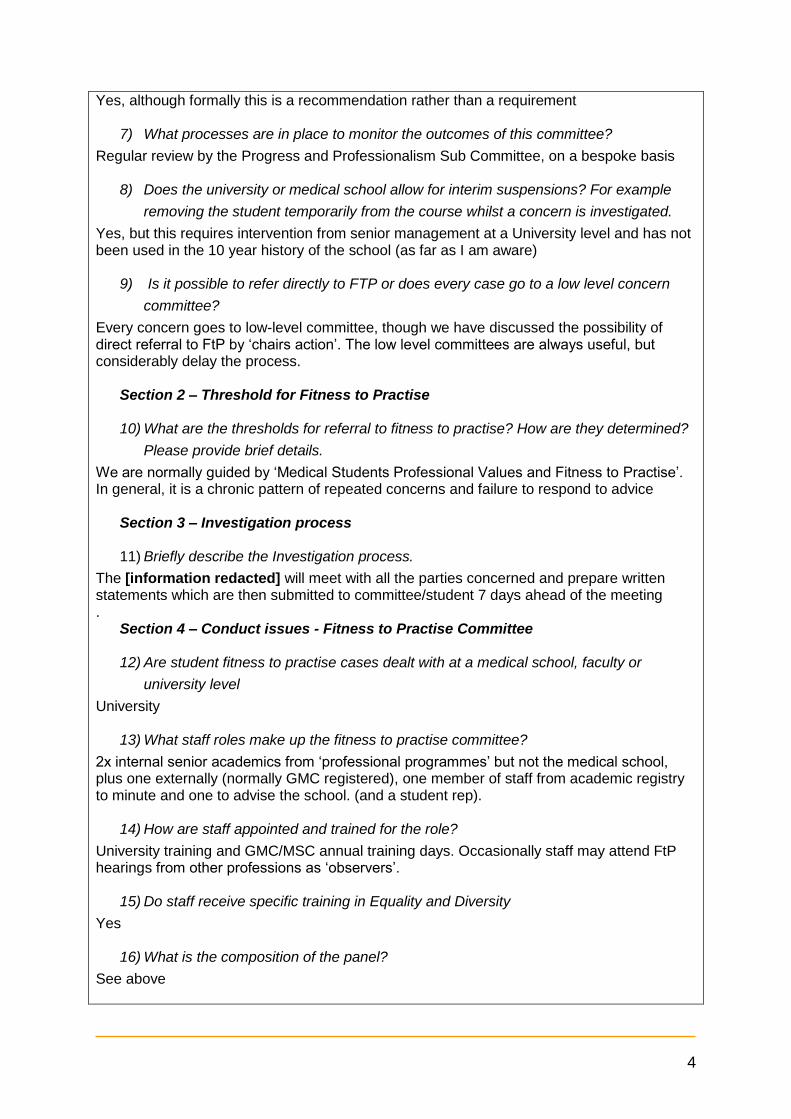
Yes, although formally this is a recommendation rather than a requirement
7) What processes are in place to monitor the outcomes of this committee?
Regular review by the Progress and Professionalism Sub Committee, on a bespoke basis
8) Does the university or medical school allow for interim suspensions? For example
removing the student temporarily from the course whilst a concern is investigated.
Yes, but this requires intervention from senior management at a University level and has not been used in the 10 year history of the school (as far as I am aware)
9) Is it possible to refer directly to FTP or does every case go to a low level concern
committee?
Every concern goes to low-level committee, though we have discussed the possibility of direct referral to FtP by ‘chairs action’. The low level committees are always useful, but considerably delay the process.
Section 2 – Threshold for Fitness to Practise 10) What are the thresholds for referral to fitness to practise? How are they determined?
Please provide brief details.
We are normally guided by ‘Medical Students Professional Values and Fitness to Practise’. In general, it is a chronic pattern of repeated concerns and failure to respond to advice
Section 3 – Investigation process 11) Briefly describe the Investigation process.
The [information redacted] will meet with all the parties concerned and prepare written statements which are then submitted to committee/student 7 days ahead of the meeting .
Section 4 – Conduct issues - Fitness to Practise Committee
12) Are student fitness to practise cases dealt with at a medical school, faculty or
university level
University
13) What staff roles make up the fitness to practise committee?
2x internal senior academics from ‘professional programmes’ but not the medical school, plus one externally (normally GMC registered), one member of staff from academic registry to minute and one to advise the school. (and a student rep).
14) How are staff appointed and trained for the role?
University training and GMC/MSC annual training days. Occasionally staff may attend FtP hearings from other professions as ‘observers’.
15) Do staff receive specific training in Equality and Diversity
Yes
16) What is the composition of the panel?
See above

5
17) Is written guidance provided to students?
Yes
18) Is the student permitted legal representation?
Yes 19) What level of sanction or warning can this committee impose?
Up to expulsion
20) How are conditions monitored?
Reviewed by [information redacted] who, if necessary, can reconvene the committee (without student) or full committee (with student)
21) Is a formal outcome letter issued?
Yes
Health Issues
Section 5 – low level health issues
22) Are low level health concerns dealt with at a medical school, faculty or university
level
Med School and Occ Health
23) Referral to committee: would this be the standard low level concerns committee or a
specific health committee?
Standard Progress and Professionalism Sub Committee is relates to FtP. There is a ‘Student Support and Guidance Committee’ whose role is to proactively tackle health issues before they become a concern. This is very successful.
24) Is it possible to refer health cases directly to FTP or does every case go to a low level
concern committee?
As for conduct
25) Staff roles that make up committee if different from that outlined previously
As for conduct, though [information redacted] may be specifically included.
26) How are staff appointed and trained for the role? Please provide brief details
As for conduct
27) What are the outcomes available to this committee?
As for conduct
28) Please provide details of the support services that this committee can recommend.
Student Support, Occ health, Welfare, Disability office
29) What processes are in place for monitoring the outcomes of this committee?
As for conduct
30) When can students be referred to Occupational Health?
6
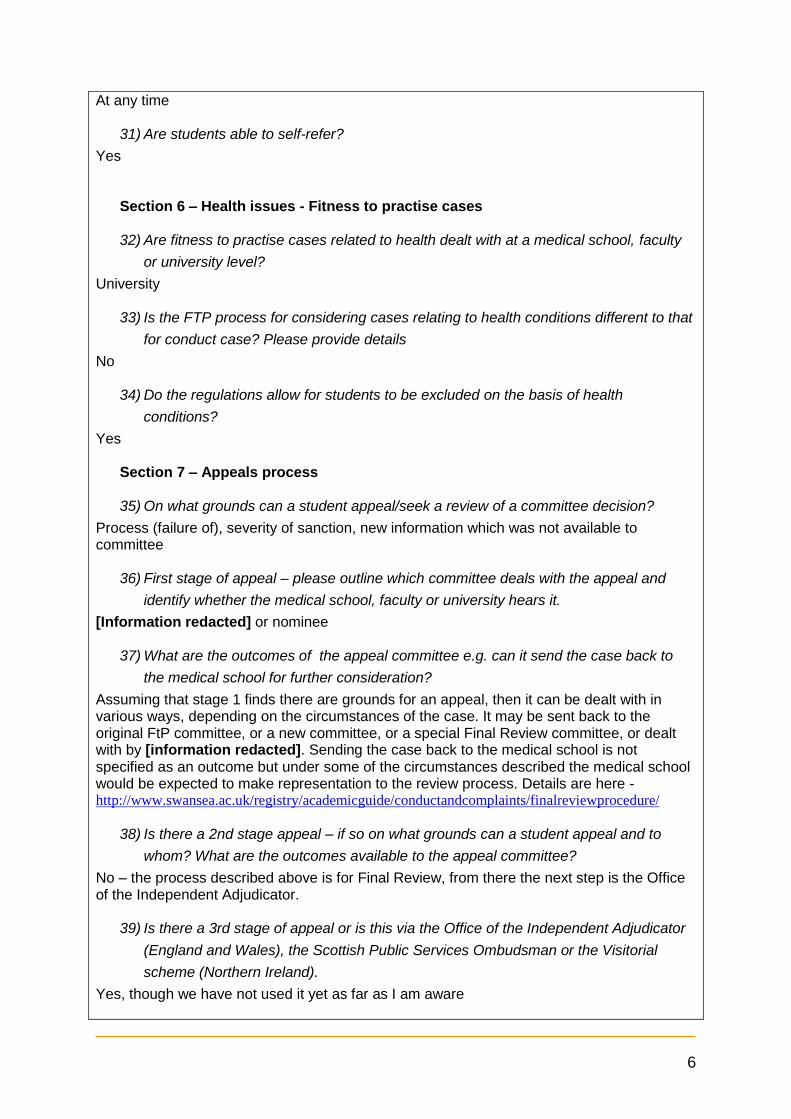
At any time
31) Are students able to self-refer?
Yes
Section 6 – Health issues - Fitness to practise cases
32) Are fitness to practise cases related to health dealt with at a medical school, faculty
or university level?
University
33) Is the FTP process for considering cases relating to health conditions different to that
for conduct case? Please provide details
No
34) Do the regulations allow for students to be excluded on the basis of health
conditions?
Yes
Section 7 – Appeals process
35) On what grounds can a student appeal/seek a review of a committee decision?
Process (failure of), severity of sanction, new information which was not available to committee
36) First stage of appeal – please outline which committee deals with the appeal and
identify whether the medical school, faculty or university hears it.
[Information redacted] or nominee
37) What are the outcomes of the appeal committee e.g. can it send the case back to
the medical school for further consideration?
Assuming that stage 1 finds there are grounds for an appeal, then it can be dealt with in various ways, depending on the circumstances of the case. It may be sent back to the original FtP committee, or a new committee, or a special Final Review committee, or dealt with by [information redacted]. Sending the case back to the medical school is not specified as an outcome but under some of the circumstances described the medical school would be expected to make representation to the review process. Details are here - http://www.swansea.ac.uk/registry/academicguide/conductandcomplaints/finalreviewprocedure/
38) Is there a 2nd stage appeal – if so on what grounds can a student appeal and to
whom? What are the outcomes available to the appeal committee?
No – the process described above is for Final Review, from there the next step is the Office of the Independent Adjudicator.
39) Is there a 3rd stage of appeal or is this via the Office of the Independent Adjudicator
(England and Wales), the Scottish Public Services Ombudsman or the Visitorial
scheme (Northern Ireland).
Yes, though we have not used it yet as far as I am aware

7
Question 2: Paragraph 35 of Tomorrow’s Doctors 2009 (TD09) stresses the significance of student clinical supervision with regard to patient safety. We would like to know about the nature of these issues, how you address them, subsequent evaluation or monitoring in place and current status. This information will enable us to cross-reference with information we hold about postgraduate training delivered in the same LEPs and highlight areas of potential concern.
2. Have you identified, in the last academic year, any issues with clinical supervision (supervision by clinicians during clinical placements) within your Local Education Providers (LEPs) and if so what steps are you taking to resolve them?
Please use the D1- Q2 sheet in the annex (Excel).

8
Domain 2 - Quality assurance, review and evaluation
When responding to questions relating to good practice, please refer to the definition which can be found in the Quality Improvement Framework (QIF) on Page 27: ‘Good practice includes areas of strength, good ideas and innovation in medical education and training. Good practice should include exceptional examples which have potential for wider dissemination and development, or a new approach to dealing with a problem from which other partners might learn. The sharing of good practice has a vital role in driving improvement, particularly in challenging circumstances.’
Question 3: Paragraph 41 of TD09 states that medical schools will have systems to monitor the quality of teaching and facilities on placements. We use your responses to this question to build links between evidence gathered from undergraduate education with postgraduate training and education.
3. We would like to know:
a. The list of quality management visits you have undertaken in the 2013/14 academic year
b. Details of any concerns or areas of good practice identified during these visits. Please also provide us with the actions which you have taken to address concerns or promote good practice
Please use the D2- Q3 sheet in the annex (Excel format).
Question 4: We particularly want to hear of any instances of good practice. Please detail the relevant TD09 domain when giving examples. If you would like to be considered as a case study which is shared with others, please check the box at the end of the question.
4. Please tell us about any innovations you are piloting or potential areas of good practice in the box below.
Domain Example of Good Practice
Domain 5 The diversity of external health care and non- clinical teachers we bring in for MHS is an example of good practice- third sector organisations (Hafal, CASIP), homelessness nurses, industry, informatics experts, bioinformatics experts, F1 doctors for debrief sessions, writers, transplant nurses, brief interventions for alcohol and smoking, healthcare managers, economists etc
Domain 5 High fidelity simulation is well established as a means of developing both clinical and non-technical skills to increase participants' competency and confidence, and reduce the incidence of adverse clinical events. Tomorrow's Doctors, 2009 (TD09) requires medical simulation and non-technical skills

9
Domain Example of Good Practice training to be provided as part of the undergraduate medical school curriculum. We have been running high fidelity simulation training for Swansea University College of Medicine Graduate Entry Medicine (GEM) students since 2009. The sessions are delivered in three half-day periods during years three and four of the GEM course. The session themes are based around Surgery, Medicine, and Paediatrics to complement the corresponding clinical placements in the curriculum. Small groups (five students) are used in order to maximise opportunities for interactivity and deep learning, and generate a safe non-threatening learning environment. During a session, each student assumes the roles of "Leader", "Assistant", and "Observer" in five simulated clinical emergencies. The sessions are not subject to assessment, and emphasis is on experiential learning. Each scenario typically lasts for 15 minutes, and is followed by a 20-40 minute period of reflection and learner-centred debriefing during which learning occurs. This is peer-led, but facilitated by the faculty and an appropriate Specialist Clinician (Consultant Surgeon, Physician, or Paediatrician). Learning objectives are clearly stated, explicit links are made with other learning activities in the GEM curriculum, and students are directed to resources to consolidate and reinforce their experience from the session. We collect anonymised feedback from all students after every session, and use this to identify areas for change and development. The same scenarios are used for every group of students to ensure consistency of approach and equal opportunities for learning. The session content, scenarios, and learning objectives were developed following a lengthy Learning Needs Assessment exercise involving senior educators and Specialist Clinicians. Content selection emphasises: a) common clinical scenarios which the students are likely to encounter as junior doctors (e.g. acute asthma, myocardial infarction); and b) scenarios reproducing medical conditions which are rare (and therefore may not be encountered by students during their clinical placements) but should never be missed (e.g. anaphylactic shock, meningococcal septicaemia). Content was then optimised through an iterative process to maximise the learning benefit of each session. In 2013, we undertook an extensive blueprinting exercise in which every scenario was mapped to both the content of related learning weeks within the four year Graduate Entry Medicine (GEM) degree curriculum; and also to the appropriate 32 core practical skills from TD09. In collaboration with the Specialist Clinicians, we undertake an annual review of all of the scenarios in order to identify any areas which require change or greater emphasis, and ensure ongoing alignment with the GEM curriculum.
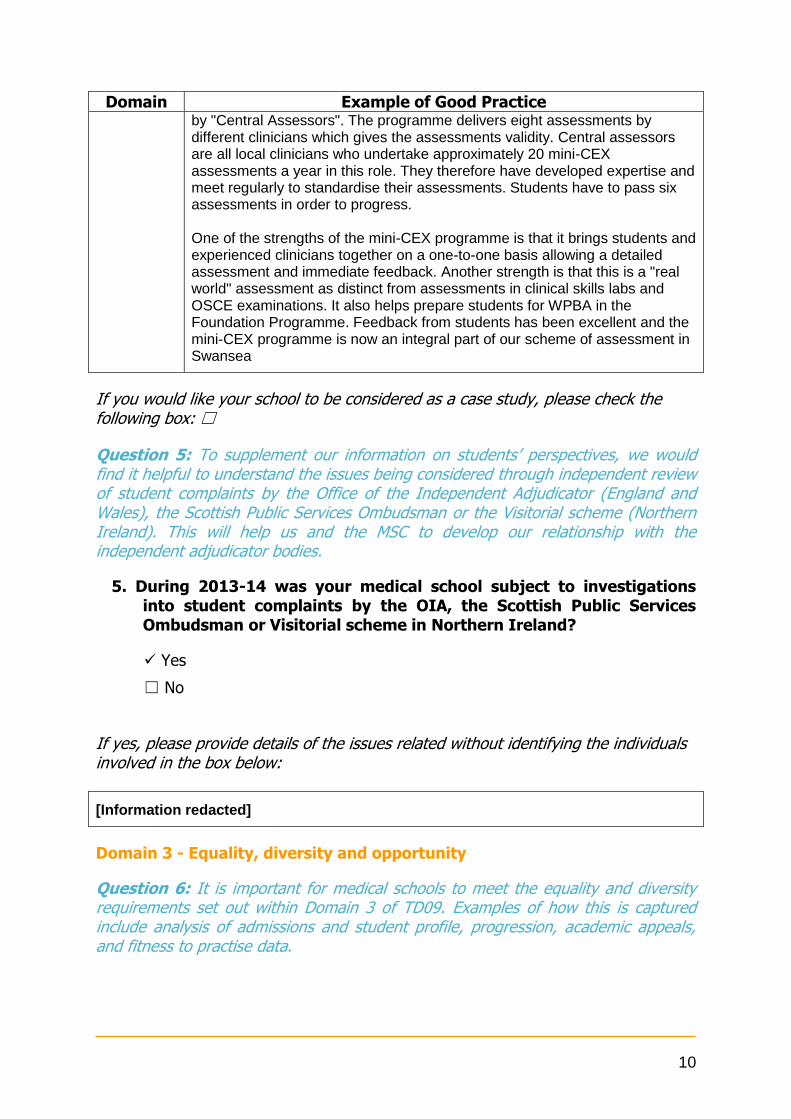
Domain 5 Final year students in the Swansea College of Medicine undertake eight summative mini-CEX assessments over the course of the year. Four of these are performed by their clinical supervisor at the time and four are performed
10
Domain Example of Good Practice by "Central Assessors". The programme delivers eight assessments by different clinicians which gives the assessments validity. Central assessors are all local clinicians who undertake approximately 20 mini-CEX assessments a year in this role. They therefore have developed expertise and meet regularly to standardise their assessments. Students have to pass six assessments in order to progress. One of the strengths of the mini-CEX programme is that it brings students and experienced clinicians together on a one-to-one basis allowing a detailed assessment and immediate feedback. Another strength is that this is a "real world" assessment as distinct from assessments in clinical skills labs and OSCE examinations. It also helps prepare students for WPBA in the Foundation Programme. Feedback from students has been excellent and the mini-CEX programme is now an integral part of our scheme of assessment in Swansea
If you would like your school to be considered as a case study, please check the following box: ☐
Question 5: To supplement our information on students’ perspectives, we would find it helpful to understand the issues being considered through independent review of student complaints by the Office of the Independent Adjudicator (England and Wales), the Scottish Public Services Ombudsman or the Visitorial scheme (Northern Ireland). This will help us and the MSC to develop our relationship with the independent adjudicator bodies.
5. During 2013-14 was your medical school subject to investigations into student complaints by the OIA, the Scottish Public Services Ombudsman or Visitorial scheme in Northern Ireland?
Yes
☐ No
If yes, please provide details of the issues related without identifying the individuals involved in the box below:
[Information redacted]
Domain 3 - Equality, diversity and opportunity
Question 6: It is important for medical schools to meet the equality and diversity requirements set out within Domain 3 of TD09. Examples of how this is captured include analysis of admissions and student profile, progression, academic appeals, and fitness to practise data.

11
6a. Please briefly tell us how in the academic year 2013/14 you used evidence to monitor how you are meeting the equality and diversity requirements set out in Domain 3 of TD09.
The Equality and Diversity (E and D) requirements have been addressed through the work of the College of Medicine Graduate Entry Medicine (GEM) Course E and D Sub-committee, the College of Medicine E and D Committee (newly inaugurated, to cover staff, research and teaching) and the Swansea University Equal Opportunities (EO) Committee (this includes representation from the College of Medicine). The GEM sub-committee has agreed terms of reference to specifically meet the requirements for TD09 (Domain3). The key areas for the E and D domain remain the development of policy (in line with University policy), monitoring of all aspects of course delivery, data analysis on E and D issues and staff training and development in this area. Data collection for E and D continues at College and University levels for students who have been through the admissions and enrolment processes. At college level this involves an anonymised student survey. This is voluntary for the new intake students each year, and gives a snapshot of the demographic in terms of the protected characteristics of the new intake compared to previous years (i.e. trends). The admissions sub-committee monitors applications to the course and the subsequent admissions data is held by the University admissions. The university data is published by college in the annual Equal Opportunities Report. Detailed analysis of the university data may allow future cross referencing with student academic performance or progression. In terms of fitness to practice data and appeals, the numbers for our small cohort have been too small to make meaningful judgements at this stage.
6b. Please tell us the biggest challenges you face in promoting fairness and equality in medical education and training.
Brief details of challenges Data collected by the Swansea University E O committee and published in the annual report highlight significant inequalities with respect to some of the better studied protected characteristics to date, e.g. gender and ethnicity, whilst the picture is still emerging for some of the protected characteristics for which data collection has just begun in earnest since the last Equality Act (2010). The challenges have been met head on. Key developments in this area include the granting of the Athena SWAN Charter bronze award initially to the university and then also to the College of Medicine. This charter recognises good practice for women working in the STEM subjects and Medicine. The change in culture and range of activities and policies in this area have supported gender equality in professional life for teaching and research staff at the College of Medicine.
A further key development has been the initiation of steps towards the University applying for The Race Charter Mark (also assessed by the Equality Challenge Unit, as for Athena SWAN). We hope that Swansea University will be in the first group of

12
universities applying for this recognition in the area of ethnicity by 2016. Initial staff discussions, including College of Medicine staff, have already occurred to establish the framework for this submission.
Question 7: This Guidance on Supporting medical students with mental health conditions was published in July 2013. We would like to measure its impact and you gave us feedback that case studies would be the most effective way of sharing the learning and experiences of different medical schools. We will build these into an anonymised set of case studies for your reference.
7. Please provide a brief case study outlining the management and support of a student with a mental health condition. Please highlight any changes in the management of students as a consequence of implementation of the GMC guidance: managing students with mental health conditions. If you do not have a suitable case study, please tick the box below:
[Information redacted]
☐ No case study available
Question 8: Three areas were highlighted by our review of health and disability in medical education and training, and we want to build a picture of current arrangements for each and identify practice to share among all schools. We are particularly interested to hear about instances where there is an identifiable individual who students can contact for advice.
8. You only need to complete this question if you have made changes since the 2013 MSAR.
If so, please let us know how your students can access the following and give brief details of what they consist of. Please include links to relevant information if helpful.
If no changes have been made, please leave blank.
a. Careers advice in relation to those with disabilities
No changes

13
b. Occupational health services
No changes
c. Advice on reasonable adjustments and support in making sure they are implemented once agreed, including when on placements.
No changes
Question 9: Following our work on health and disability in medical education and training during 2012-14, we are continuing to monitor practice on reasonable adjustments to share good practice and identify any areas of difficulty across medical schools.
9. Please tell us about adjustments relating to the 2013/14 academic year only:
a. Any new reasonable adjustments you made which you had not made before.
b. Any requests for reasonable adjustments that you turned down and why.
c. Any cases where a student was withdrawn from the course on the grounds that they would be unable to meet the outcomes required for graduation due to disability.
Criteria Brief details of new reasonable adjustment
a. New Reasonable Adjustments
[Information redacted]
b. Refusal of reasonable adjustments
None
c. Withdrawn from course due to disability
None
Question 10: We are aware that a small number of students are unable to continue their studies due to health, academic or conduct reasons. We wish to better understand and share practice on the exit arrangements and awards that are in place for such students.
10. Please briefly describe the exit arrangements and awards you have in place for students who are unable to continue to study medicine.
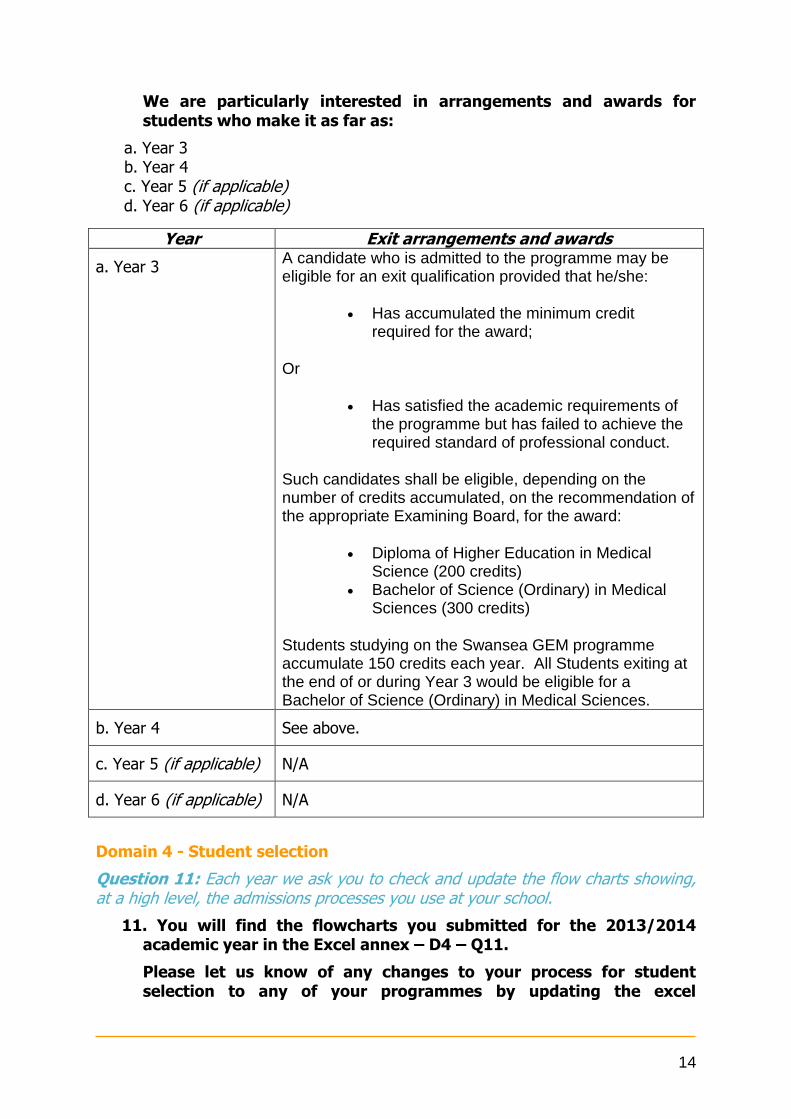
14
We are particularly interested in arrangements and awards for students who make it as far as:
a. Year 3 b. Year 4 c. Year 5 (if applicable) d. Year 6 (if applicable)
Year Exit arrangements and awards
a. Year 3 A candidate who is admitted to the programme may be eligible for an exit qualification provided that he/she:
Has accumulated the minimum credit required for the award;
Or
Has satisfied the academic requirements of the programme but has failed to achieve the required standard of professional conduct.
Such candidates shall be eligible, depending on the number of credits accumulated, on the recommendation of the appropriate Examining Board, for the award:
Diploma of Higher Education in Medical Science (200 credits)
Bachelor of Science (Ordinary) in Medical Sciences (300 credits)
Students studying on the Swansea GEM programme accumulate 150 credits each year. All Students exiting at the end of or during Year 3 would be eligible for a Bachelor of Science (Ordinary) in Medical Sciences.
b. Year 4 See above.
c. Year 5 (if applicable) N/A
d. Year 6 (if applicable) N/A
Domain 4 - Student selection
Question 11: Each year we ask you to check and update the flow charts showing, at a high level, the admissions processes you use at your school.
11. You will find the flowcharts you submitted for the 2013/2014 academic year in the Excel annex – D4 – Q11.
Please let us know of any changes to your process for student selection to any of your programmes by updating the excel
15
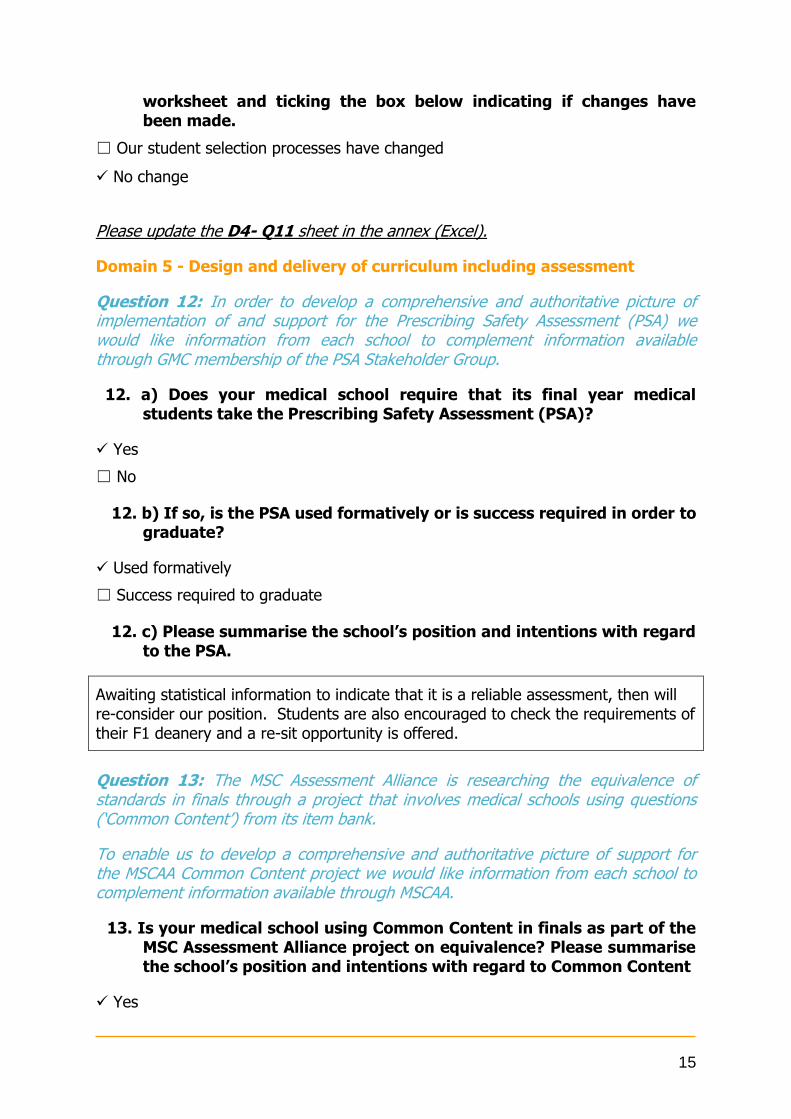
worksheet and ticking the box below indicating if changes have been made.
☐ Our student selection processes have changed
No change
Please update the D4- Q11 sheet in the annex (Excel).
Domain 5 - Design and delivery of curriculum including assessment
Question 12: In order to develop a comprehensive and authoritative picture of implementation of and support for the Prescribing Safety Assessment (PSA) we would like information from each school to complement information available through GMC membership of the PSA Stakeholder Group.
12. a) Does your medical school require that its final year medical students take the Prescribing Safety Assessment (PSA)?
Yes
☐ No
12. b) If so, is the PSA used formatively or is success required in order to graduate?
Used formatively
☐ Success required to graduate
12. c) Please summarise the school’s position and intentions with regard to the PSA.
Awaiting statistical information to indicate that it is a reliable assessment, then will re-consider our position. Students are also encouraged to check the requirements of their F1 deanery and a re-sit opportunity is offered.
Question 13: The MSC Assessment Alliance is researching the equivalence of standards in finals through a project that involves medical schools using questions (‘Common Content’) from its item bank.
To enable us to develop a comprehensive and authoritative picture of support for the MSCAA Common Content project we would like information from each school to complement information available through MSCAA.
13. Is your medical school using Common Content in finals as part of the MSC Assessment Alliance project on equivalence? Please summarise the school’s position and intentions with regard to Common Content
Yes
16
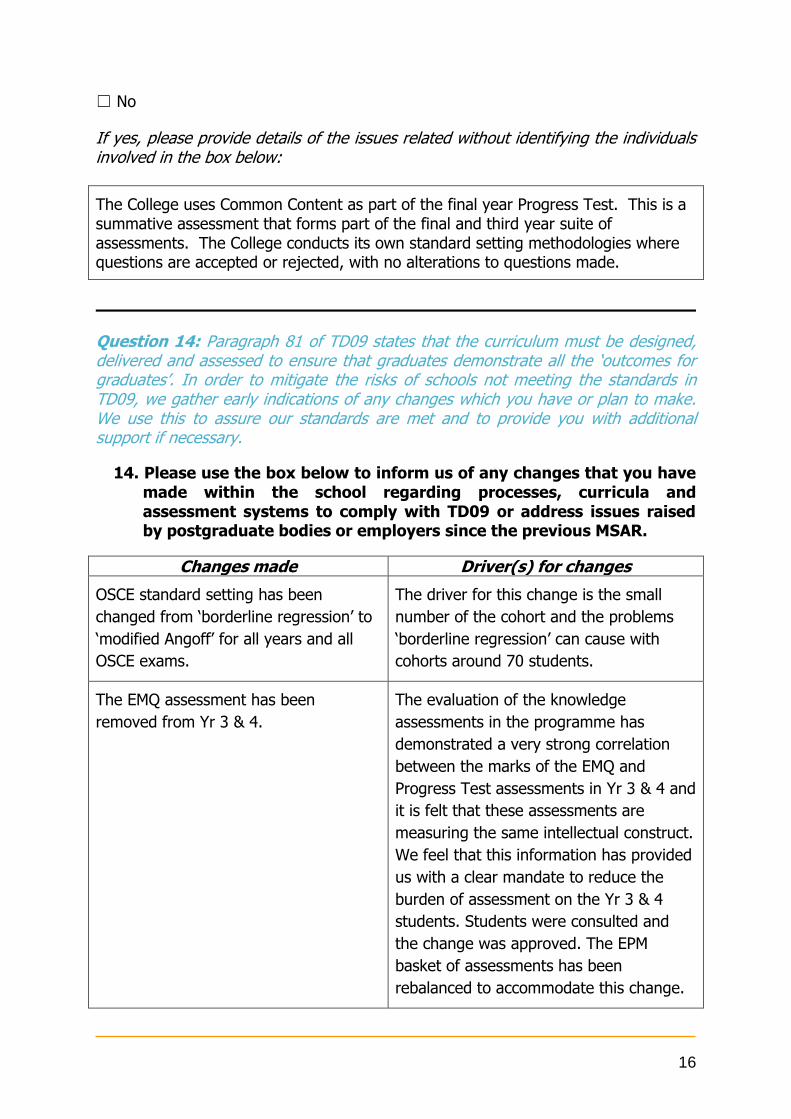
☐ No
If yes, please provide details of the issues related without identifying the individuals involved in the box below:
The College uses Common Content as part of the final year Progress Test. This is a summative assessment that forms part of the final and third year suite of assessments. The College conducts its own standard setting methodologies where questions are accepted or rejected, with no alterations to questions made.
Question 14: Paragraph 81 of TD09 states that the curriculum must be designed, delivered and assessed to ensure that graduates demonstrate all the ‘outcomes for graduates’. In order to mitigate the risks of schools not meeting the standards in TD09, we gather early indications of any changes which you have or plan to make. We use this to assure our standards are met and to provide you with additional support if necessary.
14. Please use the box below to inform us of any changes that you have made within the school regarding processes, curricula and assessment systems to comply with TD09 or address issues raised by postgraduate bodies or employers since the previous MSAR.
Changes made Driver(s) for changes
OSCE standard setting has been
changed from ‘borderline regression’ to
‘modified Angoff’ for all years and all
OSCE exams.
The driver for this change is the small
number of the cohort and the problems
‘borderline regression’ can cause with
cohorts around 70 students.
The EMQ assessment has been
removed from Yr 3 & 4.
The evaluation of the knowledge
assessments in the programme has
demonstrated a very strong correlation
between the marks of the EMQ and
Progress Test assessments in Yr 3 & 4 and
it is felt that these assessments are
measuring the same intellectual construct.
We feel that this information has provided
us with a clear mandate to reduce the
burden of assessment on the Yr 3 & 4
students. Students were consulted and
the change was approved. The EPM
basket of assessments has been
rebalanced to accommodate this change.
17
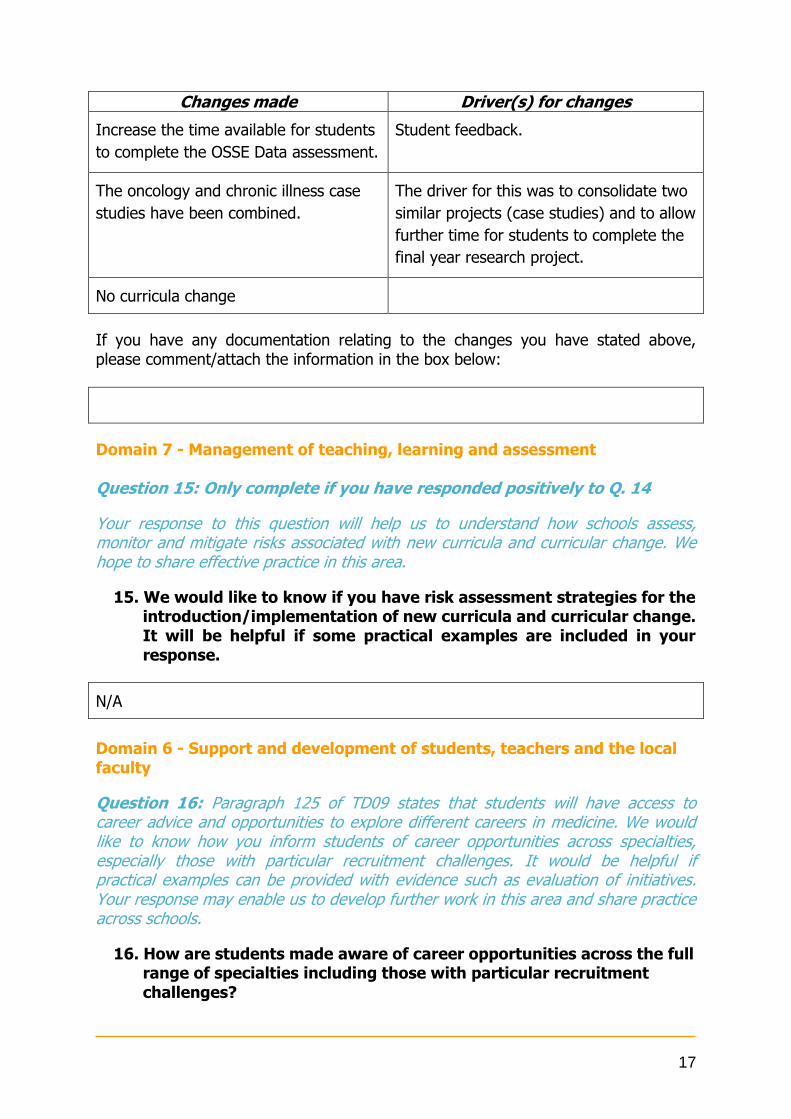
Changes made Driver(s) for changes
Increase the time available for students
to complete the OSSE Data assessment.
Student feedback.
The oncology and chronic illness case
studies have been combined.
The driver for this was to consolidate two
similar projects (case studies) and to allow
further time for students to complete the
final year research project.
No curricula change
If you have any documentation relating to the changes you have stated above, please comment/attach the information in the box below:
Domain 7 - Management of teaching, learning and assessment Question 15: Only complete if you have responded positively to Q. 14
Your response to this question will help us to understand how schools assess, monitor and mitigate risks associated with new curricula and curricular change. We hope to share effective practice in this area.
15. We would like to know if you have risk assessment strategies for the introduction/implementation of new curricula and curricular change. It will be helpful if some practical examples are included in your response.
N/A
Domain 6 - Support and development of students, teachers and the local faculty
Question 16: Paragraph 125 of TD09 states that students will have access to career advice and opportunities to explore different careers in medicine. We would like to know how you inform students of career opportunities across specialties, especially those with particular recruitment challenges. It would be helpful if practical examples can be provided with evidence such as evaluation of initiatives. Your response may enable us to develop further work in this area and share practice across schools.
16. How are students made aware of career opportunities across the full range of specialties including those with particular recruitment challenges?
18
Domain 9 – Outcomes
Question 17: Please raise any issues you would like us to consider around the outcomes and practical procedures currently in TD09. Your input is essential to ensure that medical school perspectives and knowledge are reflected and to demonstrate an open and inclusive approach to the review.
17. Does the medical school have any concerns about, or suggestions for amendments to, the GMC’s outcomes for graduates (TD09, paragraphs 7-23) or practical procedures (TD09, Appendix 1)?
Please set out these concerns and suggestions and explain the background to them, giving any evidence available.
The College of Medicine in Swansea has been working with the outcomes outlined in the document TD09 and feel they broadly reflect what needs to be covered in an undergraduate curriculum However, the practical procedures have become slightly outdated
1. Pregnancy testing – this has become an electronic test in most Health boards and not something that medical staff do in their normal routine
2. Dosage and administration of insulin and use of sliding scales – the use of sliding
scales is not used in clinical practice in local Health Boards The addition of blood gas taking would be useful though I have concerns that we would be attempting to get all our graduates competent before F1 in something which is difficult to do on real patients – I think the achievement of competence on patients could remain in F1 but that undertaking the procedure on a manikin and understanding the underpinning knowledge required to a desired level would be achievable and realistic in an undergraduate programme
Careers support is provided in a variety of manners to GEM students throughout their 4 year course. There are regular careers evenings, which aim to highlight the different specialty options available to the students, with interactive talks from both consultants and junior doctors1. Personal tutors are an initial point of contact for all students and there is also list of Careers Advisors available by specialty that students can access for specific careers advice2. In addition there is support from the College of Medicine’s Careers and Employability staff eg CV workshops and situational judgement tests. Regular contact is also made with GEM students to alert them of local and national meetings of interest eg BMJ Careers Fairs and events held at the Royal Colleges. Careers information available on line is also signposted eg the Welsh Deanery website. Clinicians also support student led events such as those run by the Swansea Surgical Society3. Documents available for review on request: 1 Example of a Careers Evening 2 Sample List of Careers Advisors 3 Example of Surgical Society Event

19
Question 18: In the outcomes for graduates in TD09 we require that they are able to provide appropriate healthcare and understand health inequalities (paragraphs 10d, 11b, 13a, 14a and 20d). Information from medical schools about current arrangements will help us to review the outcomes for graduates in TD09.
18. How does the curriculum address providing appropriate healthcare and understanding health inequalities, particularly relating to people from lower socioeconomic backgrounds, lesbian gay bisexual or transgender people, and people with learning disabilities?
Socioeconomic background
LGBT Learning disabilities
What does the curriculum say?
A fundamental (introductory) session focuses on health inequalities and diversity in all its guises (including LGBT and Learning Disabilities). The relevance of these concepts to clinical practice is reinforced repeatedly throughout the Medicine, Health and Society curriculum. Examples include Public
Understanding and awareness of impact in fundamental session and then subsequent integrated sessions e.g. epidemiology etc
A fundamental (introductory) session focuses on health inequalities and diversity in all its guises (including LGBT and Learning Disabilities). The relevance of these concepts to clinical practice is reinforced repeatedly throughout the Medicine, Health and Society curriculum. Examples include Public Health and epidemiology sessions, Professional Practice sessions as well as in sessions addressing medical ethics, medical law, and behavioural and social science. In addition, one teaching week in
20
Health and epidemiology sessions, Professional Practice sessions as well as in sessions addressing medical ethics, medical law, and behavioural and social science.
Y2 is dedicated to cerebral palsy and ASD. Learning disability is covered in some detail throughout the week.
How is this assessed? Some knowledge is assessed by single best answer questions. However, the issues are mainly assessed in Student Selected Clinical Projects and written reflections, where appreciation of diversity can be explored and discussed theoretically and practically in relation to clinical experience.
Some knowledge is assessed by single best answer questions. However, the issues are mainly assessed in Student Selected Clinical Projects and written reflections, where appreciation of diversity can be explored and
Some knowledge is assessed by single best answer questions. However, the issues are mainly assessed in Student Selected Clinical Projects and written reflections, where appreciation of diversity can be explored and discussed theoretically and practically in relation to clinical experience.
21
discussed theoretically and practically in relation to clinical experience.
Please give examples of any challenges
Please give examples of any initiatives
Question 19: Paragraph 14J of TD09, which covers the doctor as a practitioner and includes outcome requirements on the diagnosis and management of clinical presentations, requires that students must:
Contribute to the care of patients and their families at the end of life, including management of symptoms, practical issues of law and certification, and effective communication and team working.
The care of dying people is an important issue, and it is key that students are prepared effectively. We would like to know how you have reflected on and made changes as a result of the Leadership alliance on the Care of Dying People report.
19. How does your school teach students how to best handle the issue of the care of dying people?
As part of the Medicine, Health & Society curriculum, Y2 students have a two-hour teaching session from a Consultant in Palliative Care called “Death and Dying”. The explicit learning outcome is: to apply understanding of the impact of terminal diagnoses, the context and processes of dying, and the meaning of loss to clinical practice examples. Y3 students have a one-hour session on “Assisted Dying” with the following learning outcome: to understand the clinical, ethical, legal and social considerations surrounding requests for assisted suicide or euthanasia and their implications for medical practice. As part of trauma week, and following a session on organ donation, Y4 students are engaged in a structured debate about “Organ donation and transplant services / Organ donation, including autonomy, consent and self-ownership”. The learning outcome is: to gain an understanding of the role of the transplant team and the

22
screening process for potential transplant donors and recipients and to understand the ethical arguments for and against the opt-in/opt-out systems and to evaluate them in the light of international comparators.
As part of Integrated Clinical Method teaching, Y2 students complete an ICM Communication Skills Station on ‘breaking bad news’. Y3 students have a half day teaching session on end of life decision making and pathways, decisions relating to resuscitation (DNA CPR), as well as further ‘breaking bad news’ stations.

23
Additional question
Question 20: In autumn 2014 we will be publishing reports around Medical School Progression Data and we have asked you to update us through the MSAR on how you have used this new information to improve your understanding of and make improvements to the quality of training. We would like to work with schools on case studies to be published in spring 2015.
20. Please provide information on how you have used the new reports to understand or improve the quality of training or highlight any other points of interest in relation to the data.
Not applicable to Swansea University, College of Medicine as we had our first graduates in July 2014.
If you would like your school to be considered as a case study for our 2015
publication, please check the following box: ☐
Thank you for completing the questions for the 2014/15 MSAR. The deadline for this return is the 31st December 2014; please ensure you have completed each of the following:
☐ Section A (Word) – MSAR qualitative questions.
☐ Annex to Section A (Excel) – Templates for D1-Q2, D2-Q3 and D4-Q11.
☐ Section B (Excel) – Quality Visits/QIF visits requirements (if applicable).
☐ Section C (Excel) – Worksheets.
We want to make completing the MSAR as easy as possible, so if you need any help with completing this return, feel free to contact Nathan Brown or another member of the quality team on [email protected] or 020 7189 5221.
Related Documents











