Satrajit Roychoudhury East User Group Meeting 2014 Oct 22 nd 2014 A Bayesian Industry Approach to Phase I Combination Trials in Oncology

2014-10-22 EUGM | ROYCHAUDHURI | Phase I Combination Trials
Aug 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Satrajit Roychoudhury
East User Group Meeting 2014
Oct 22nd 2014
A Bayesian Industry Approach to Phase I Combination Trials in Oncology
Beat Neuenschwander
Alessandro Matano
Zhongwen Tang
Simon Wandel
Stuart Bailey
Statistical Methods in Drug Combination Studies, Boca Raton, FL: Chapman & Hall/CRC Press (2015)
Book Chapter and Authors
Acknowledgements
2 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

Table of Content
1. Introduction
2. Phase I Design Framework
3. Methodology
4. Applications
5. Implementation Issues
6. Conclusion
3 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

1. Introduction
In Oncology, challenges in Phase I trials are many: while keeping patient safety within acceptable limits, the trials should be small, adaptive, and enable a quick declaration of the maximum tolerable dose (MTD) and/or recommended phase II dose (RP2D).
The objective of this chapter is to provide a comprehensive overview, which includes;
• a rationale based on general clinical and statistical considerations,
• a summary of the methodological components, and
• applications
4 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

1. Introduction Challenges and Design Requirements
Phase I Trial Challenges Design Requirements
Untested drug or combination in treatment-resistant patients
Escalating dose cohorts with small number of patients (e.g. 3-6)
Primary objective: determine Maximum Tolerated Dose (MTD)
Accurately estimate MTD
High toxicity potential: safety first Robustly avoid toxic doses (“overdosing”)
Most responses occur 80%-120% of MTD
Avoid sub therapeutic doses while controlling overdosing
Find best dose for dose expansion (which generally becomes the recommended phase II dose)
Enroll more patients at acceptable, active doses (flexible cohort sizes)
Complete trial in timely fashion Use available information efficiently
5 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

2. Phase I design framework Traditional 3+3 design
Trial Data
0/3,0/3,1/3,...
Dose escalation
decision from
predefined
algorithm
Very simple BUT
• Poor targeting of true MTD
• Highly variable estimates
High attrition rates in phase II and III
• How many failures are due to the wrong dose coming
from phase I?
6 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

2. Phase I design framework Why Bayesian modeling?
Bayesian approach offers a way to quantify our knowledge and assess risk.
• Given what I have seen, what can I say about the true risk of dose limiting toxicity (DLT)?
Models allow us to share information between doses – efficient use of data.
Flexibility to include additional patients, unplanned doses, change schedules.
Higher chance to find the correct MTD (Rogatko et al. (2007)).
7 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

2. Phase I design framework Clinically driven, statistically supported decisions
DLT rates
p1, p2,...,pMTD,...
(uncertainty!)
Historical
Data
(prior info)
Model based
dose-DLT
relationship
Trial Data
0/3,0/3,1/3,...
Clinical
Expertise
Dose
recommen-
dations
Decisions Dose Escalation
Decision
Model Inference Decision/Policy
Responsible: Statistician Responsible: Investigators/Clinician
Informing: Clinician (Prior, DLT) Informing: Statistician (risk)
8 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Single Agent Model (Neuenschwander et. al. 2008)
Data: (#DLT/#Patients): 𝑟𝑑~ Binomial(π𝑑, 𝑛𝑑)
Parameter Model: logit 𝜋𝑑 = log(α) + β log(d/d*)
Prior: (log(α), log(β)) ~ N2(m1, m2, s1, s2, corr)
Model parameter α and β can be interpreted as;
α is the odds, of a DLT at d*, an arbitrary scaling dose.
β > 0 is the increase in the log-odds of a DLT by a unit increase in log-dose.
Can be extended by adding additional covariates/relevant predictors representing different patient-strata.
9 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Developing drug combinations: Paradigm change from single agent
There is no longer one MTD but a many
- e.g. given drug A = X mg, MTD of drug B is Y mg.
- Critical to determine the MTD boundary and the set of acceptable doses.
Still in “learning phase”
- Flexibility (e.g., variable cohort sizes, split cohorts).
- Bayesian model summarizes knowledge on all dose pairs, sets upper bound on dosing.
- Actual decisions use additional information (e.g. efficacy, PK, biomarkers, later cycle AE) to select “best” dose pair(s) for next cohort.
10 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Interaction: Antagonism, independence or synergy
There are a number of factors that may lead to increased or decreased risk of toxicity;
• Drug-Drug Interaction seen in the PK profiles, e.g.
- AUC or Cmax for one or both compounds is significantly increased/decreased compared to being given alone.
- May be competitively using/inhibiting CYP enzyme causing lower clearance.
• Overlapping toxicities, e.g.
- If drug 1 and drug 2 have similar toxicity profiles, giving them together may cause a significant increase in the observed rate.
- Equally, the combination may cause the same toxicity in the same subset of patients but at a higher grade, whilst other patients are unaffected.
- Two toxicities that, when they occur together increase the risk of DLT in a patient.
• Pathway interactions, feedback loops that either trigger additional toxicities or provide protective effects.
11 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Dual and Triple Combination Model
Proposed model has two parts: (multiplicative odds model)
• Marginal effects: 2 parameters per agent representing single agent toxicities. • Interaction: 1 parameter for Dual interaction (Dual combo model). : 4 parameters for Dual and triple(extra) interaction (Triple combo model).
Extension of Thall et. al. Biometrics (2003).
Properties for proposed combination models
• Parsimonious since the number of tested dose combinations in phase I trials is usually fairly small.
• Have easily interpretable parameters similar to Base model.
• Allow for interaction.
• Have the ability to incorporate single-agent information.
12 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Metrics for Dosing Recommendations
Posterior Distribution: The result of the Bayesian analysis is the posterior distribution of which, in turn , leads to the posterior of for each dose group. Our approach relies formally on this metric (using principle of escalation with overdose control (EWOC)) for suggesting feasible dose for next cohort.
Predictive Distribution: The predictive distribution of the number of DLT “r*” in the next cohort with size “n”. This metric is used informally in discussions with clinical teams.
A Formal Decision Analysis: We do not use formal decision analysis to identify the dose range for further dosing or the MTD/RP2D.
13 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Choice of Prior: Using Contextual Information or Co-data
Key question: Can we use available information as prior?
Naive views
• The information is of no value because we simply don‘t know what‘s going to happen in our trial
• Or, transform these data into a prior that is worth N patients
• Eg. N=200, with observed rate = 0.10. Use a Beta(20,180) prior.
Between-trial heterogeneity discounting historical data
• After discounting, prior may be Beta(2,18)
• Don‘t use 10% as a rule of thumb for discounting!
Methodology: meta-analytic-predictive (MAP) • Random-effects meta-analysis of historical data/parameters 1,... H
• with a prediction for the parameter * in the new trial
• basic assumption: exchangeable parameters
14 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Meta-analytic-predictive (MAP) Prior
Similarity Scenario
H Historical Trials with Effects 1,..., H
Data from Historical Trials Yh h=1,...,H
Similarity of Parameters 1, ..., H, * ~ N(µ,2)
Meta-Analytic-Predictive (MAP) Prior * | Y1,..., YH
Challenge: how large is ? (cannot be inferred if for small H)
15 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology MAP Prior for Oncology Phase I
Different types of a-priori information in Phase I
• Animal data (2 species, e.g. dog and rat) Requires discounting of information due to between-species
extrapolation.
• Historical data for same compound in another indication (with similar toxicity profile), one or more trials. Requires moderate to substantial discounting of information due to between-trial/indication extrapolation.
Typically these priors have relatively little weight, 3 to 9 pts.
• Compared to phase I sample sizes of 15 to 30 patients, this is still relevant information.
16 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology MAP Priors for Phase I Combination Studies
Prior for single-agent parameters
• Bivariate normal prior: from co-data (historical/external data), with appropriate discounting due to between-trial variability using MAP.
Prior for interaction parameter (odds-multipliers) ’s
• Normal (no restriction) or log-normal (synergistic toxicity)
• Pre-clinical/Clinical information can be incorporated in the prior of interaction parameter. But often no information is available. Therefore weakly-informative priors are used.
17 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

3. Methodology Robust Mixture Prior
The use of historical data requires an extrapolation from the past to the future. Predictions are always difficult.
What if there is a possibility that the chosen prior will be in conflict with the actually observed data?
Possible robustification: MAP Mixture Priors
• Adding a weakly informative component to MAP may address the issue.
• Mixture weights represent the degree of similarity between codata and new trial.
• Mixture priors are more robust against prior-data conflict, and should be used more often (rarely seen in practice).
18 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial
4. Applications Practical consideration for Implementation
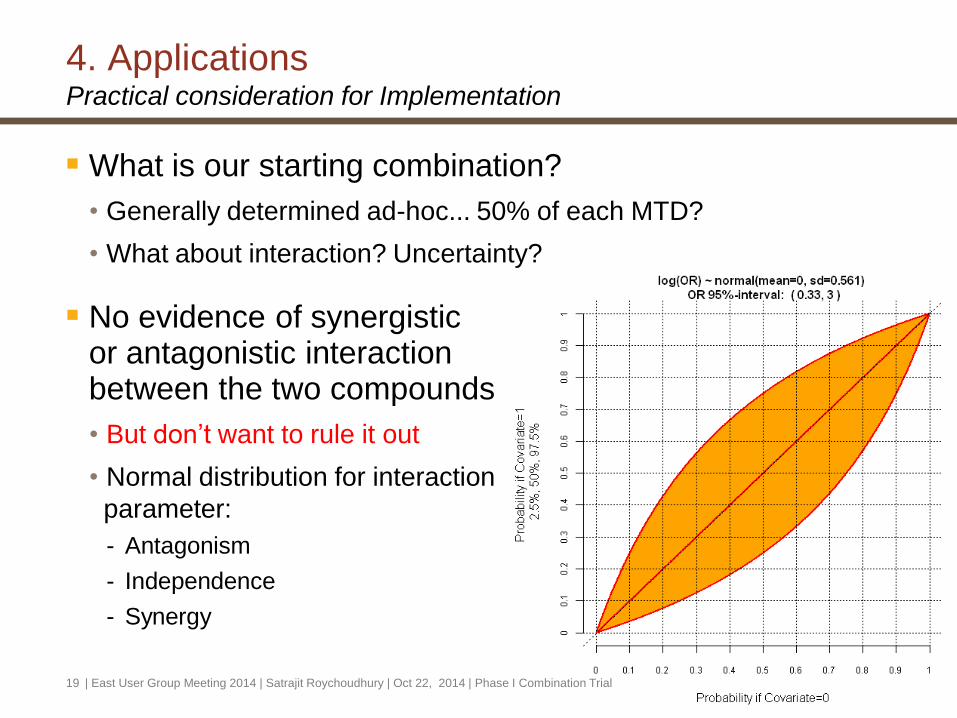
What is our starting combination?
• Generally determined ad-hoc... 50% of each MTD?
• What about interaction? Uncertainty?
No evidence of synergistic or antagonistic interaction between the two compounds
• But don’t want to rule it out
• Normal distribution for interaction
parameter:
- Antagonism
- Independence
- Synergy
19 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Dual-Combination Trial: Background
Combination of two new compounds
• Compound 1: d1 = 3, 4.5, 6, 8; d1* = 3 (all mg)
• Compound 2: d2 = 33.3, 50, 100, 200, 400, 800, 1120; d2* = 960 (all mg)
• Dose-limiting data (DLT): days 1 - 28
• Toxicity intervals for 𝜋𝑑: [0-0.16), [0.16-0.35), [0.35-1.00]
• EWOC: P(𝜋𝑑 >= 0.35) < 0.25
Actual dosing decisions
• must respect EWOC criterion.
• should also acknowledge other relevant information (PK, efficacy, ...).
Additional design constraints
• Cohort size 3 to 6
• Only one compound's dose can be increased; max. increment of 100%.
20 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Rules to determine MTD
Dose escalations continue until declaration of the MTD.
A dose is potential candidate for MTD when;
1. At least 6 patients have been treated at this dose
2. This dose satisfies one of the following conditions:
- The probability of targeted toxicity exceeds 50%:
- or, a minimum of number of 15 patients have already been treated in the trial.
21 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Dual-Combination Trial: Prior derivation
Relevant (single-agent) data was identified
MAP approach to derive priors based on this data: discussion with clinical team about similarity
No a-priori evidence for interaction between the two compounds, but considerable uncertainty
22 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Dual-Combination Trial: Full history (1/2)
23 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Dual-Combination Trial: Full history (2/2)
Cohort 1
3 mg / 400mg
0 DLT / 3 Patients
Cohort 2a
3 mg / 800mg
1 DLT / 3 Patients
Cohort 2b
6 mg / 400mg
1 DLT / 3 Patients
Cohort 3a
3 mg / 800mg
1 DLT / 3 Patients
... Cohort 3b
6 mg / 400mg
0 DLT / 3 Patients
24 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial
5. Applications MTD Declaration
3-800: grade 2 adverse events, moderate increase in magnitude and duration of QT.
4.5-600: experienced grade 1 and/or grade 2 adverse events, No QT prolongation. BUT none of the patients had a relevant tumor lesion decrease.
6-400: experienced grade 2 adverse events, but easily managed with appropriate dose reductions, No QT prolongation. Moreover, encouraging efficacy signals were observed.
Based on clinical and statistical findings : 6-400 mg was declared as the MTD and RP2D.
| East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial 25

4. Applications Triple-Combination Trial: Background
Triple combination
• One «backbone», two experimental
• Agent 1: 100, 200, 300, 400 mg
• Agent 2: 10, 20, 30, 40 mg
• Agent 3: 250 mg (fixed)
Stage-wise approach considered reasonable
• Find MTD for agent 2 + 3
• Escalation of agents 1 and 2 (agent 3 fixed)
Prior derivation similar to dual combination case.
26 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Triple-Combination Trial: Model assessment (1/3)
Stage I: Data scenarios for Dual Combination
27 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Triple-Combination Trial: Model assessment (2/3)
Stage II: Data scenarios for Triple Combination
28 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

4. Applications Triple-Combination Trial: Model assessment (3/3)
Operating characteristics: Assumed true toxicity rates
Metrics
29 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

5. Implementation issues Practical guide
Some of the points that need to be considered when implementing the proposed Bayesian adaptive design in clinical practice.
Discussion with clinical colleagues
Expertise in Bayesian Statistics
Computations
Study Protocols
Review Boards
30 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

5. Implementation issues Discussion with clinical colleagues
Discussing important features with clinical colleagues: key responsibilities of a statistician when designing and implementing clinical trials.
Recommended to explain the main features of the approach using visual illustrations, non-statistical language, and common sense.
A good preparation includes a mimicked dose-escalation meeting using data scenarios to highlight various possible outcomes.
31 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

5. Implementation issues Expertise in Bayesian Statistics and Computation
Expertise in Bayesian Statistics: Implementing the proposed approach requires:
• Technical skills related to the concrete implementation
• the ability to explain in simple language
• Training/workshop/case studies for clinician and statistician
• project-related regular interactions between statisticians and clinicians
Computation: Require a tool that allows to extract the relevant metrics for inference and decision making:
• WinBUGS/R
• JAGS
• Stan
32 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

5. Implementation issues Study Protocols
Requires more attention when Bayesian methods are used.
A clear description of the model and prior needs to be provided in protocol.
If an informative prior based on external information is used, the derivation of the prior should be clear in protocol.
The actual process for dose-escalations needs to be described as well.
Further technical details including data scenarios and operating characteristic may be covered in a statistical appendix.
33 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

5. Implementation Issues Review Boards
Experience shows that discussions with HA and IRB/IEC around these issues lead to a better understanding and appreciation of the rationale and intent of the proposed approach.
“Typical” questions include;
• A 25% risk of overdose is too high.
• The design allows too many patients to be exposed at once to a new dose level.
• The design must be set up in a way that observation of 2 DLT at a dose level means that this dose cannot be used again.
• The design makes a recommendation, but the clinician decides the dose. This implies that a decision may overrule the original recommendation, and patients may be dosed at unsafe dose levels.
34 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

6. Conclusion
Detailed explanation of phase I (combination) approach
• Concepts
• Mathematical background
• Examples
• Practical implementation
Covers about 10 years of practical expertise
• Methodological work
• Operational experience (> 100 trials)
• Technical implementation
Standard at Novartis Oncology (others just taking up)
35 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

References (1/2)
[1] Neuenschwander, Matano, Tang, Roychoudhury, Wandeland Bailey. A Bayesian Industry Approach to Phase I Combination Trials in Oncology. Statistical Methods in Drug Combination Studies, Boca Raton, FL: Chapman & Hall/CRC Press 2015.
[2] Neuenschwander, Branson, Gsponer. Critical aspects of the Bayesian approach to phase I cancer trials. StatMed 2008.
[3] Rogatko, Schoeneck, Jonas et al. Translation of innovative designs into phase I trials. JCO 2007.
36 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial

References (2/2)
[4] Babb, Rogatko, Zacks. Cancer phase I clinical trials: efficient dose escalation with overdose control. Statistics in Medicine 1998.
[5] Thall, Lee. Practical model-based dose-finding in phase I clinical trials: methods based on toxicity. Int J Gynecol Cancer 2003.
[6] Thall, Millikan, Mueller, Lee. Dose-finding with two agents in phase I oncology trials. Biometrics 2003.
[7] O’Quigley, Pepe, Fisher. Continual reassessment method: a practical design for phase I clinical trials in cancer. Biometrics 1990.
37 | East User Group Meeting 2014 | Satrajit Roychoudhury | Oct 22, 2014 | Phase I Combination Trial
Related Documents











