2012 CPT UPDATES AAHAM January 20, 2012 Presented by Lynn Pascoe, CHCA, CHCC, CPC, CPC-I, CEMC, PCS, CCP Innovative Medical Practices, LLC

2012 CPT UPDATES AAHAM January 20, 2012 Presented by Lynn Pascoe, CHCA, CHCC, CPC, CPC-I, CEMC, PCS, CCP Innovative Medical Practices, LLC.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2012 CPT UPDATESAAHAM
January 20, 2012
Presented by Lynn Pascoe, CHCA, CHCC, CPC, CPC-I, CEMC, PCS,
CCPInnovative Medical Practices, LLC
Innovative Medical Practices, All Rights Reserved 2011 2
Disclaimer
• Every reasonable effort has been taken to ensure that the educational information provided in today’s presentation is accurate and useful. Pursuant to the protection of proprietary documentation under established copyright laws, the attendee may not distribute and/or sell all or any portion of this material.
• This handout material is designed to provide information in regard to the subject matter presented and is based on presenters experiences, opinion and interpretation. Failure to abide fully with all the terms and conditions contained in this material may result in possible civil and criminal penalties including liquidating damages.
• Current Procedural Terminology (CPT®) is copyright 2012 American Medical Association. All Rights Reserved. CPT is a registered trademark of the American Medical Association.
• We appreciate your understanding and compliance with this notice and hope you find the information presented of benefit.
Innovative Medical Practices, All Rights Reserved 2011 3
Agenda
1.CMS MFS, ABNs, ACA updates and modifiers
2. 2012 CPT Code Changes
3.Question and Answer
Innovative Medical Practices, All Rights Reserved 2011 4
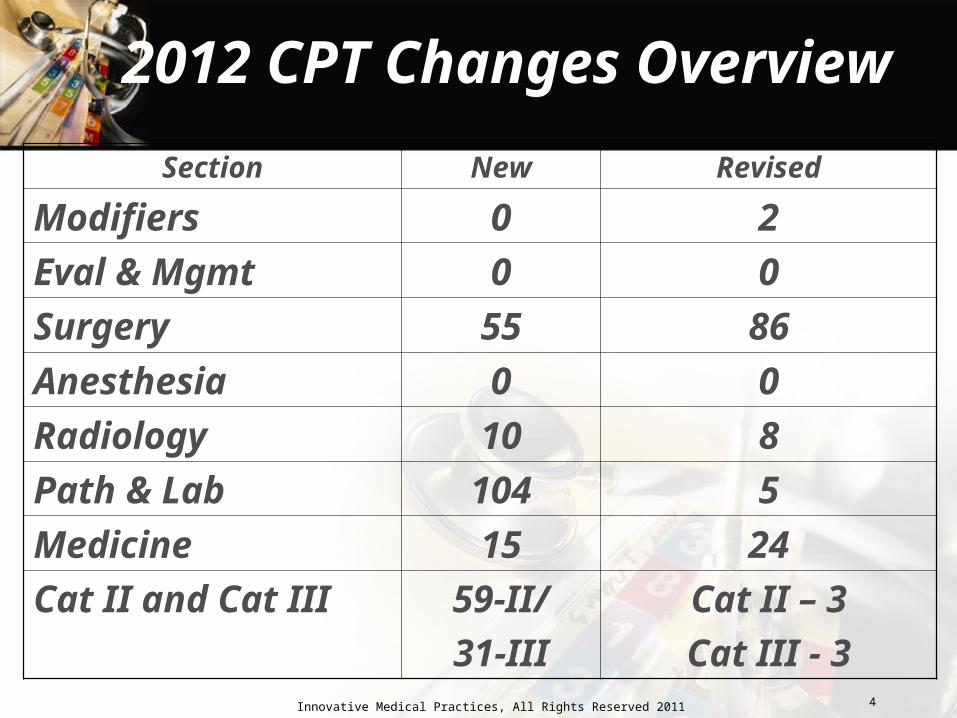
2012 CPT Changes Overview
Section New Revised
Modifiers 0 2
Eval & Mgmt 0 0
Surgery 55 86
Anesthesia 0 0
Radiology 10 8
Path & Lab 104 5
Medicine 15 24
Cat II and Cat III 59-II/
31-III
Cat II – 3
Cat III - 3
Innovative Medical Practices, All Rights Reserved 2011 5
Revised ABN
• Form CMS-R-131 (03/11) Form Approved OMB No. 0938-0566
• Must be in place by 1/1/2012 – Older versions invalid
• The mandatory use date has been changed from September of 2011 to January of 2012 to accommodate those providers and suppliers with pre-printed stockpiles of ABNs - additional time to exhaust their supplies of the outgoing ABN.
Innovative Medical Practices, All Rights Reserved 2011 6
Revised ABN
• CMS - no substantial changes to the form other than the new release date
• New form shows that it was reviewed and approved by the Executive Office of Management and Budget.
• Formatting changes intended to comply with accessibility standards in Section 508 of the Rehabilitation Act of 1973.
• There are also no changes other than formatting to the instructions for use of the ABN.
Innovative Medical Practices, All Rights Reserved 2011 7
2012 Medicare Physician Fee Schedule
• Significant in Fed Reg were comments re: forecast of CMS’ plan to carry out government mandates for a value-based payment modifier, which will actually modify payments under the Medicare Physician Fee Schedule based on Medicare's record of the quality of care you provide to patients compared with the cost of that care.
• Sound familiar? PQRS or P4P
Innovative Medical Practices, All Rights Reserved 2011 8
2012 Medicare Physician Fee Schedule
• What is clear from the rule is that the process is underway to put the value-based modifier in place by 2015 for some physicians (based on claims and quality reporting in 2013) and
• By 2017 for all physicians (probably based on claims and quality reporting in 2015).
Innovative Medical Practices, All Rights Reserved 2011 9
2012 Medicare Physician Fee Schedule
CMS has this to say in the final rule: "We strongly encourage physicians to participate in the
Physician Quality Reporting System program and the EHR Incentive Program sooner rather than later and to choose to report quality of care measures that best reflect their practice and patient population.
Although we have not yet proposed the value modifier methodology, our primary interest at this point is to increase the quality of care for Medicare beneficiaries.
We note that we also plan to propose a value modifier in rule making during 2012, prior to the initial performance period. Thus, we believe it is reasonable to encourage physicians to report appropriate quality measures well in advance and irrespective of the exact value modifier methodology at this time."
Innovative Medical Practices, All Rights Reserved 2011 10
Bundling and Misvalued Services
• CMS RUC committee continues to evaluate CPT services that are performed together 75% or more
• Results in bundling codes and payment reductions – continue each year
• CMS include review of codes with low RVUs but high utilization, codes that have the largest growth in utilization in the Medicare database, site of service anomalies, etc.
• Practices should be prepared to negotiate adequate payments from commercial payer contracts
Innovative Medical Practices, All Rights Reserved 2011 11
Preventive Medicine and Screening Services
Modifier Updates
Innovative Medical Practices, All Rights Reserved 2011 12
Affordable Care Act (ACA)
• Commercial plans – Eff 9/23/2010 – renewal of all commercial plans
• No cost sharing
• Modifier -33 comes into play
• US Preventive Services Task Force – “we are determining what is a ‘no cost’ service versus costing sharing”
• Cost sharing may be allowed if service is not completely preventive
Innovative Medical Practices, All Rights Reserved 2011 13
Affordable Care Act (ACA)
• Example #1
– Pt is seen for follow up of DM
– MD orders a screening blood glucose because one had not been done recently
– MD reports 99213 – has cost sharing (off copay)
• Lab test has no cost sharing USPSTF A/B
Innovative Medical Practices, All Rights Reserved 2011 14
Affordable Care Act (ACA)
• Example #2:
– MD sees a 45 y.o. patient for preventive medical exam (99396) and orders a screening PSA
– 99396 has NO cost sharing
• Lab test has cost sharing PSA is not a USPSTF A/B test
Innovative Medical Practices, All Rights Reserved 2011 15
Affordable Care Act (ACA)
• Example #3– At an annual well woman exam the MD performs a
Gail model risk assessment and asks about personal and family hx of thromboembolic disease.
– Based on this a f/u visit occurs to discuss chemoprophylaxis of breast cancer. Mole is also checked
– MD reports 99214 for 2nd visit– Cost sharing does not apply to the 99214 (mod 33) as
the primary purpose was preventive USPSTF A/B
Innovative Medical Practices, All Rights Reserved 2011 16
Affordable Care Act (ACA)
• The Patient Protection and Affordable Care Act (PPACA) requires all health care insurance plans to begin covering preventive services and immunizations without any cost-sharing, i.e., they must provide first-dollar-coverage for specified preventive services.
• The timing is dependent on when health insurance plans renew or change.
Innovative Medical Practices, All Rights Reserved 2011 17
Affordable Care Act (ACA)
• The regulations specify that plans cannot impose cost-sharing requirements, such as co-pays, coinsurance or deductibles with respect to specified preventive services, when preventive services are billed separately.
• When these services are part of an office visit, the visit may not require cost-sharing if the primary reason for the visit is to receive preventive services.
Innovative Medical Practices, All Rights Reserved 2011 18
Modifier 33 – Preventive Services
• Modifier -33: Been in effect since 1/1/2011
• Not found in the inside front cover of CPT
• Created to aid compliance with new health care member cost sharing for defined preventive services for non-grandfathered policies.
• The appropriate use will reduce claim adjustments related to preventive services
• Reduce corresponding refunds to policy members.
Innovative Medical Practices, All Rights Reserved 2011 19
Rationale Modifier 33
• All health care plans to begin covering immunizations and preventive services without any cost sharing, modifier 33 has been added to identify a service as a preventive service.
• The new mandate may also affect payer coverage or payment policies for services listed in the Counseling Risk Factor Reduction and Behavior Change Intervention section of CPT (99401–99429)
• AMA has publication with table on uses of Mod -33
Innovative Medical Practices, All Rights Reserved 2011 20
CMS Annual Wellness Visit (AWV)
• Sect 4013 of ACA-allows coverage and payment for an annual wellness visit after 1/1/2011 for an individual who is more than 12 months out from the effective date of his/her 1st MCR B coverage period, and hasn’t received either an IPPE or an annual wellness visit within the past 12 months
• G0438 – Annual wellness visit, personalized prevention plan, first visit (2.43 work RVUs)
• G0439 – AWV, PPP, subsequent visit, 1.50 work RVUs
Innovative Medical Practices, All Rights Reserved 2011 21
Modifier 33 – Preventive Services
• Examples: – Welcome to Medicare P/E – IPPE (MCR
initial preventive P/E-G0402)– Annual Wellness Visit (G0438 and G0439)
• CMS Quick Reference Guide for Preventive Services – Preventive Services Manual – Table for Mod-33 scenarios
• http://www.healthcare.gov/law/resources/regulations/ prevention/recommendations.html
Innovative Medical Practices, All Rights Reserved 2011 22
Differences between G codes and 99381-99397
• Requirements for G0438-G0439 (1/1/11) for AWV (Annual wellness visit; includes a personalized prevention plan of service (pps), initial visit and subsequent visits) different from PMS
• AWV does NOT include a complete P/E
• AWV focuses on:
– Identification of risk factors
– Personalized health advice and referral for..
Innovative Medical Practices, All Rights Reserved 2011 23
Modifier PT (HCPCS II)
• If MD converts screening test to a diagnostic test i.e., CPT 45385 – diagnostic colonoscopy, append modifier –PT
• In this case the patient’s deductible should be waived but coinsurance may apply.
• Can use with appropriate CPT code for colonoscopy, flexible sigmoidoscopy or barium enema when the service is initiated as a colorectal cancer screening service but becomes a diagnostic service
• Part B deductible does not apply• This modifier is valid for CPT codes 10000 through
69999
Innovative Medical Practices, All Rights Reserved 2011 24
Examples HCPCS Modifier PT
• 68 y.o. presents for pre-scheduled screening colonoscopy (HCPCS II code G0121)
• Polyp discovered and service turns into CPT 45385 polypectomy
• add-on PT to 45385• Copay and deductible waived for this service• Diagnosis does not affect benefit• Anesthesia – moderate sedation included in CRC
screen, but if anesthesia services used, cost sharing applied
• Lab/Path – cost sharing applies
Innovative Medical Practices, All Rights Reserved 2011 25
Modifier -92 Revised
• Modifier -92: Alternative laboratory platform testing when:
– A lab test is performed using a kit or transportable instrument that wholly or in part consists of a single use, disposable chamber
– That test doesn't require permanent dedicated space
– The test is designed to be carried or transported to the vicinity of the patient for immediate testing at the site
Innovative Medical Practices, All Rights Reserved 2011 26
Modifier -92 Revised
• CMS – modifier 92 indicates POS HIV testing
• CMS Transmittal 2277 states modifier -92 effective 10/1/11 for this purpose
• www.cms.gov/transmittals/downloads/R2277CP.pdf
Innovative Medical Practices, All Rights Reserved 2011 27
Evaluation and Management Services
Innovative Medical Practices, All Rights Reserved 2011 28
Evaluation & Management Services
• CPT Added back Decision Tree – New versus Established Patients page 5 of CPT Professional 2012
• Revised guidelines New and Established Patients
• Observation care (typical times added)
• Prolonged Services (editorial changes)
• Inpatient Neonatal Intensive Care Services – guideline revisions
Innovative Medical Practices, All Rights Reserved 2011 29
New vs Established Patient
Solely for the purposes of distinguishing between new and established patients, professional services are those face-to-face services rendered by a physician and reported by a specific CPT code(s). A new patient is one who h as not received any professional services from the physician or another physician of the exact same specialty and subspecialty who belongs to the same group practice, within the past three years
Innovative Medical Practices, All Rights Reserved 2011 30
New vs Established Patient
An established patient is one who has received professional services from the physician or another physician of the exact same specialty and subspecialty who belongs to the same group practice, within the past three years
See Decision TreeBottom line: did the MD have personal
knowledge/relationship with the patient(s)
Innovative Medical Practices, All Rights Reserved 2011 31
Question 1: New or Established
• Drs. Smith and Jones are in the same nephrology group practice. Dr. Smith is a general nephrologist. Dr. Jones does interventional nephrology exclusively. Dr. Jones has separate boards in I/N and payers classify him in that specialty.
• Dr. Smith refers a patient to Dr. Jones for consideration of a clotted fistula. Is this a new patient to Dr. Jones?
Innovative Medical Practices, All Rights Reserved 2011 32
Question 1: New or Established
• Answer:
– The patient is “new” to Dr. Jones
– Specialty is not exactly the same
– Payer recognizes specialty and physician has designation through separate boards
Innovative Medical Practices, All Rights Reserved 2011 33
Question 2: New or Established?
• Dr. Brown, a cardiologist, is treating a patient with CAD. He is not responding well to treatment and he elects to send the patient to Dr. White who is a cardiologist CAD specialist in his practice for further recommendations.
• Is this a new patient to Dr. White or established?
Innovative Medical Practices, All Rights Reserved 2011 34
Question 2: New or Established?
• Answer:
– The patient is “established” to Dr. White
– Specialists/subspecialists are the same in the same group practice
– Many subspecialty areas do not have board certifications
Innovative Medical Practices, All Rights Reserved 2011 35
Initial Observation Codes (99218-99220)
• RUC established median timesestablished median times and recommended RVUs
• CPT may adopt these times as typical for a service
• Times are most relevant in relation to Prolonged Services
• Times are consistent with Initial Hospital Care at the same level (99221-99223)
Innovative Medical Practices, All Rights Reserved 2011 36
Prolonged Services
• Codes 99354-99355 (Office or outpatient) and 99356-99357 (inpt or OBS) gain instructions that state: these codes may be used by “other qualified healthcare professionals”
• Face to Face reference removed and “Direct patient contact” defined
• Rationale relates to face-to-face and units of time as both being direct
• Inpatient side – floor/unit time is considered face-to-face
Innovative Medical Practices, All Rights Reserved 2011 37
Prolonged Services – CMS Manual
• Claims Manual 100-4 CH 12:
*30.6.15.1 Prolonged Services with Direct Face-to-Face Patient Contact Service (codes 99354-99357)
Definition: Prolonged MD services 99356 in the inpt setting, with direct face-to-face patient contact which require one hr beyond the usual services are payable when they are billed on the same day by the same MD or qualified NPP as the companion E/M codes. Each add’l 30 min of direct f to f contact following the first hour or prolonged services may be reported by 99357.
Innovative Medical Practices, All Rights Reserved 2011 38
Prolonged Services – CMS Manual
• Requirement for Physician Presence
– In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.
Innovative Medical Practices, All Rights Reserved 2011 39
Inpatient Neonatal IC Services and Pediatric CC Services
• Added guidelines:– Define more precisely the services included
and how the codes are applied• New codes: Car Seat Evaluation (94780-94781)
for nursing observation, vital signs, and bundled with the global neonatal and pediatric initial and subsequent critical care initial and continuing intensive care codes
• Set up to determine airway integrity before releasing infant to car seat
Innovative Medical Practices, All Rights Reserved 2011 40
Integumentary System
• Complete overhaul of skin replacement/skin substitute codes
• CPT cleaned up wound debridement guidance and code descriptions – (11042-11047)
• Revised guidelines directs coders to use modifier -59 with either codes 11042 or 11044 as appropriate
• Many codes in 15300-15431 range deleted
Innovative Medical Practices, All Rights Reserved 2011 41
Integumentary System
• Replaced by fewer and much more simplified codes ex: 15271
– Application of skin substitute graft to trunk, arms, legs, total wound surface areas up to 100 sq cm; first 25 sq cm or less wound surface area
– 15272….each add’l 25 sq cm wound surface area or part thereof
Innovative Medical Practices, All Rights Reserved 2011 42
Musculoskeletal
Not many changes to this system

Innovative Medical Practices, All Rights Reserved 2011 43
Musculoskeletal
• Mostly descriptor revisions– Clarify the intent of the service – Describe bundled services
Ex: Percutaneous vertebroplasty (22520-22522) specifically identify bone bx as an bundled service if performed
• Several injection procedures such as 27096 – injection for Sacroiliac joint, now clearly includes imaging guidance
Innovative Medical Practices, All Rights Reserved 2011 44
Musculoskeletal
• 2 new codes for treatment of Dupuytren’s contracture (pronounced "DOO puh trenz)- Patient’s can’t straighten their fingers
20527 – injection enzyme palmar fascial cord
Caveat -paired with hundreds of codes from the surgical section; especially those related to trigger point injections, fracture and dislocation services.
Innovative Medical Practices, All Rights Reserved 2011 45
Musculoskeletal
• Application of Casts/Strapping – Lower Extremity
29582 thigh and leg, including ankle and foot, when performed
• Like 20527 – bundled with many surgery specialty codes – be sure to check new CCI edits
• Also – remember the rules governing casts and strapping – who can use and when is appropriate
Innovative Medical Practices, All Rights Reserved 2011 46
Musculoskeletal
• 2 new codes: 22633 and 22634 describe arthrodesis via combined posterior and posterolateral techniques with posterior interbody technique
Innovative Medical Practices, All Rights Reserved 2011 47
Changes in Respiratory Surgical SystemChanges in Respiratory Surgical System
Innovative Medical Practices, All Rights Reserved 2011 48
Respiratory
• Significant changes with a full page of new instructions and added parenthetical notes that reflect current practice.
• Every “removal of lung” code (32440-32491) has been revised
• 6 new codes – thoracotomy (32096-32098) with bx– 32505-+32507 with wedge resection– Entirely new category (32601-32674) for VATS
thoracic surgery with a dozen new codes
Innovative Medical Practices, All Rights Reserved 2011 49
Cardiovascular
Innovative Medical Practices, All Rights Reserved 2011 50
Cardiovascular
• Cardiology: Again – CPT recognized several codes often reported together– Revised guidelines including new definitions
• Radiological S&I is now included in these codes
– Numerous revised codes– Numerous new codes (9)– New Table (pg 171 for Pacemakers) to assist
with coding
Innovative Medical Practices, All Rights Reserved 2011 51
Cardiovascular
• Combination codes were added to report renal catheterization and angiography (36251-36254)
• New codes include the S&I portion again
• Additional instructions given to clarify replacement of ventricular assist device pumps (33981-33983) including removal of the new pump in addition to connection, de-airing, and initiation of new pump
Innovative Medical Practices, All Rights Reserved 2011 52
Digestive
Innovative Medical Practices, All Rights Reserved 2011 53
Digestive
• Few changes in this surgical section• Several parenthetical notes added• Ex: Stomach: Laparoscopy codes (43644-
43659) instructs, “for laparoscopic implantation, revision or removal of gastric neurostimulator electrodes, lesser curvature (morbid obesity) use 43659”.
• 3 new codes (49082-49084 describe abdominal paracentesis replace deleted codes 49080 and 49081
Innovative Medical Practices, All Rights Reserved 2011 54
Digestive
Incision ▲ 47000 Biopsy of liver, needle;
percutaneous
– Rationale:
• Code 47000 revised, adding the conscious sedation symbol to note that moderate sedation is inherently included as part of this procedure
Innovative Medical Practices, All Rights Reserved 2011 55
Male/Female Genital Systems
• No changes in Male GU system portion
• Female GU system:
– Several parenthetical notes added throughout the section
– Example: Instruction to report 11981 for insertion of a non-biodegradable contraception implant, and 11976-11981 for removal with subsequent insertion

Innovative Medical Practices, All Rights Reserved 2011 56
Nervous and Pain Medicine
Innovative Medical Practices, All Rights Reserved 2011 57
Nervous and Pain Medicine
• New guidelines – such as use of fluoroscopy– Placement and use of a catheter– Threading a catheter– Intermittent bolus– Reporting of codes 62310-62319– Percutaneous spinal procedures (clarification)– Endoscopic assistance during an open procedure
• Revised codes• New codes• Deleted codes
Innovative Medical Practices, All Rights Reserved 2011 58
Nervous and Pain Medicine
• Majority of guidelines changes for refinement and clarification
• Codes 64622-64627 deleted; replaced by 64633-64636 for destruction of paravertebral facet joints by neurolytic agent
• New codes specify location (cervical, lumbar, etc.) and the number of joint injected
– Single and then each additional
Innovative Medical Practices, All Rights Reserved 2011 59
Eye/Ocular Adnexa and Auditory
• Minor revisions with new parenthetical instructions
– E.g., “For fitting contact lens for treatment of disease, see 92071, 92072
– Must have evidence of disease
• Deletion 69802 – Labyrinthotomy with perfusion with mastoidectomy
Innovative Medical Practices, All Rights Reserved 2011 60
Radiology
Innovative Medical Practices, All Rights Reserved 2011 61
Radiology
• MANY changes for developing codes for new services and deleting codes for obsolete services
• Spine Radiology
– Part of the on-going “clean-up” of radiology codes
• Elimination of potential ambiguity
• Clarification of “complete” study
• Focus on number of views, rather than specific types of views
Innovative Medical Practices, All Rights Reserved 2011 62
Radiology
• Improvement in technical notes
• Last yr concurrent CT of abdomen/pelvis are reported with single bundled code
• Same principle now applies to CT Angiography - bundled
– CTA: Technical note
• Always includes IV contrast
• Do not report CT separately for same session
• Bottom line – don’t unbundle
Innovative Medical Practices, All Rights Reserved 2011 63
Radiology
• New codes for intra-operative radiation treatment delivery (77424, 77425)
– Intraoperative radiation treatment management (77469)
• New instructions specify radiation tx management is reported in units of five fractions or treatment sessions, regardless of the actual time period in which services performed
Innovative Medical Practices, All Rights Reserved 2011 64
Radiology
• Atherectomy code deleted and replaced with other codes
• Summary:
– Bundle, bundle, bundle
– Most changes are modification and clarifications and deletions
Innovative Medical Practices, All Rights Reserved 2011 65
Path and Lab
• Summary of changes:
– 2 new codes: 86386, 87389
– 5 revised codes: 86703, 88312-14, 88319
– 2 deleted codes: 88107, 88318
– 2 Category III codes: 0279T, 0280T
– Revision of Modifier -92
– AND………………..
Innovative Medical Practices, All Rights Reserved 2011 66
Path and Lab
• New Molecular Pathology Section in CPT!– Guidelines and Introductory Notes (2 full pages)– Definitions
• Tier 1 – 92 new codes• Human Leukocyte Antigen (HLA) typing
– Tier 2 – • 9 new codes/levels
• Current CPT coding was more non-uniform than uniform for a given analysis
• Concern that we don’t stifle innovation and technology and want to provide beneficial results for our patients
Innovative Medical Practices, All Rights Reserved 2011 67
Medicine
Innovative Medical Practices, All Rights Reserved 2011 68
Immunization Administration for Vaccines/Toxoids
Revised guidelines: ”A component refers to all antigens in a vaccine
that prevents disease(s) caused by one organism (90460-61). Multi-valent antigens or multiple serotypes of antigens against a single organism are considered a single component vaccine
– Combination vaccines are those that contain multiple vaccine components.
– Conjugates or adjuvants contained in vaccines are not considered to be component parts of the vaccine as defined above”.
Innovative Medical Practices, All Rights Reserved 2011 69
Immunization Administration for Vaccines/Toxoids
• What does this mean?
– Descriptor revisions clarify immunization coding (90460, +90461) by vaccine component, rather than per injection
– Clarifies original intent
– Pneumococcal vaccine has up to 23 antigens, but is a single disease vaccine (not a combo in any way)
Innovative Medical Practices, All Rights Reserved 2011 70
Immunization Administration for Vaccines/Toxoids
• What does this mean (con’t)?
– Influenza has multiple sub-types, but is fundamentally a single disease vaccine
– Confusion in code 90644: tetanus toxoid as a conjugate vs tetanus vaccine
–90644 descriptor revised
• 90470 H1N1 immunization administration IM, Intranasal is deleted
Innovative Medical Practices, All Rights Reserved 2011 71
Immunization Administration for Vaccines/Toxoids
Influenza coding
• One major change - inclusion of 90654 (Influenza virus vaccine, split virus, preservative-free, for intradermal use),
• Adds another choice to flu vaccine coding
• Addition expands on the code family 90655-90668 that already addressed influenza vaccines
Innovative Medical Practices, All Rights Reserved 2011 72
Immunization Administration for Vaccines/Toxoids
• Code 90654 is not age specific unlike codes 90655-90658 which specify the patient’s age (either 6 to 35 months of age, or age 3 years and older).
• Code 90654 represents an intradermal injection (administered to the dermal layer of skin), whereas other codes (e.g. 90655-90658 and 90662) describe intramuscular injections (administered to muscle tissue) and intranasal administration (e.g. 90660).
Innovative Medical Practices, All Rights Reserved 2011 73
Immunization Administration for Vaccines/Toxoids
• Code 90654 represents the vaccine product only.
• You must include the appropriate administration code (90460-90474) on your claim.
• If your physician provides a significant, separately identifiable E/M service during the encounter for the vaccine, you must also report the appropriate E/M code (99201-99205 for a new patient or 99211-99215 for an established patient).
Innovative Medical Practices, All Rights Reserved 2011 74
Medicine
• Esophageal motility study – use revised codes 91010 (for motility study) and +91013 for stimulation or perfusion
• 92070 deleted; replaced with 2 new codes (92071and 92072) for contact lens fitting to treat specific ocular surface disease
• Full page instructions added for sleep medicine testing
• New codes for EMGs per extremity
• Hydration codes 96360 and +93631 significant additional instructions – clarifies meaning of initial infusion and concurrent infusion

Innovative Medical Practices, All Rights Reserved 2011 75
Questions
Innovative Medical Practices, All Rights Reserved 2011 76
Thank You!!!!!!!
Lynn L. Pascoe, CHCA, CHCC, CPC, CPC-I, CEMC, PCS, CCP
Innovative Medical Practices, LLC
(410) 859-5757 (410) 850-0360
Mobile: (443) 822-0519
Email: [email protected]
Related Documents











