-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
1/39
MINISTRY of FOREIGN AFFAIRS/DENMARKGROSS NATIONAL HAPPINESS COMMISSION/BHUTAN
Joint Evaluation of Danish-BhutaneseCountry Programme 2000-09
Thematic Paper onLocal Service Delivery
Lham DorjiCentre for Bhutan Studies
August 2010
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
2/39
Table of content
1.Introduction 12.Overview of decentralisation reforms and impacts on local service delivery system 1
2.1 Underlying framework 12.2Introduction of DYT and GYT Acts and amendments over time 22.3 Participatory approaches to planning 32.4 Resource allocation 32.5 Service delivery trends 3
3.Policies and programmes aimed at improved local service delivery 54.Service delivery outcome 7
4.1 Education services and outcomes 74.2 Health services and outcomes 94.3 Agriculture and environmental services 164.4 Governance 194.5 Communication 20
5.Challenges on improved public service delivery 205.1 Mandates and responsibilities 215.2Capacity of local government 225.3 Participatory planning 245.4 Service delivery 25
6.Recommendations and conclusion 276.1 Access to services 276.2 Decentralisation 286.3 Civil society 306.4 Accountability 30
Annex 1: Prevalence of deprivation across five dimensions, by regionAnnex 2: Various livestock service centres (1998-2008)Annex 3: Number of ICT facilities (2000-08)
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
3/39
Abbreviations and acronyms
AHB Annual Health BulletinBHU Basic Health UnitCBO Community-Based Organization
CBR Crude Birth RateCBS Centre for Bhutan StudiesCSO Civil Society OrganizationDSP Decentralisation Support ProgrammeECCD Early Childhood Care and DevelopmentEPI Expanded Programme on ImmunizationFYP Five-Year PlanGAO Gewog Administrative OfficerGDP Gross Domestic ProductGNH Gross National HappinessGNHC Gross National Happiness CommissionHDI Human Development IndexHR Human ResourceHRD Human Resource DevelopmentHRO Human Resource OfficerHTF Health Trust FundIMR Infant Mortality RateLGDP Local Governmnet Development ProgrammeMDG Millennium Development GoalsMoE Ministry of EducationMoF Ministry of FinanceMoH Ministry of HealthNEC National Environmental CommissionNFE Non-Formal EducationODA Official Development AssistanceORC Out-Reach ClinicPHCB National Population and Housing Census (2005)
RCSC Royal Civil Service CommissionRGoB Royal Government of BhutanRIARD Rapid Impacts Assessment of Rural DevelopmentRIM Royal Institute of ManagementRNR Renewable Natural ResourcesUSD US Dollars
VHW Village Health Worker
Bhutanese termsChimi Representative of village at National Assembly (up until 2008)Dzongdag District administratorDzongkhag District (there are 20 in Bhutan)Dzongkhag Yargye Tshogdu (DYT) orDzongkhag Tshogdu (DT)
District Development Committee
Gewog Administrative block (there are 205 in Bhutan)Gewog Yargye Tshogdu (GYT) or GewogTshogde (GT)
Gewog Development Committee
Gup Elected representative at gewog levelMaangmi Deputy to gupTshogpa Representative of a village
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
4/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 1
1. Introduction
This thematic paper is prepared as a part of the Joint Evaluation of Danish-BhutaneseCountry Programme which is guided by the following overall objectives:
1. To assess and document the relevance and effectiveness of Danish support to povertyreduction and democratisation in Bhutan 2000-09, and
2. To consolidate and enhance the sustainability of the outcomes achieved throughlearning and adjustments to the cooperation during the last programme period 2009-13 and beyond.
The Danish bilateral assistance to Bhutan in its present form will gradually be phased outfrom 2013. It is anticipated that the collaboration will gradually be replaced by other forms ofcollaboration such as business-to-business joint activities and various kinds of cultural andnon-governmental programmes. This paper summarises the current state of local servicedelivery in Bhutan and the challenges this face. It further elaborates the assessment made in
the synthesis report and should be seen as a supplement to the thematic paper ondecentralisation and local empowerment. Hence, while the latter focuses on achievementsand challenges faced by the decentralisation process, the present paper is primarilyconcerned with the populations access to basic services.
This paper draws on the relevant official documents, donor reports and field interviews toevaluate the policies, practical challenges and development of decentralised local serviceprovisions in Bhutan. It focuses primarily on the service delivery in education, health,governance and renewable natural resource sectors, key priorities of the Bhutan-DenmarkCountry Programme.
First, the general analysis of how decentralisation reforms have contributed to improving
local service delivery is made within the context of the countrys overall development policyframework. Second, it examines the policies, programmes and financing mechanisms ofservice delivery. Third, the progress and outcomes of decentralised service delivery isassessed. Fourth, it identifies the general issues and challenges of improving decentralisedlocal service delivery system. Finally, the paper concludes with recommendations for raisingthe local service delivery performance.
2. Overview of decentralisation reforms and impacts on local servicedelivery system
2.1 Underlying frameworkThe underlying framework of Bhutans development approach is the Gross NationalHappiness (GNH): Bhutan 2020: A vision for Peace, Prosperity and Happiness. The overarchinggoals of Vision 2020 are: the country should be able to sustain the rising cost of social sectorinvestments, meet the growing physical infrastructure needs and raise living standard andthe quality of life bypromoting equitable access to improved quality of social services.1 BhutansVision 2020 has set the following goals between 2000 and 2020 (for the selected sectors):
1. The country to deliver healthcare services similar to other developing countries withdrastic reduction in maternal and child mortality rate and improved integration ofindigenous health service system.
1 10th Five-Year Plan Documents, Volume I, pp, 19.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
5/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 2
2. The education system to evolve and be able to develop culturally conscious children,being curious to learn and acquire skills and ready for employment. The other goals are tofully attain enrolment level at class X by 2012 and realize full adult literacy by 20172.
3. To develop the governance system with required institutions for democratisation anddecentralisation processes; to strengthen the local governments that are capable ofplanning, carrying our management functions and delivering local services; and to fulfilboth national and local priorities and aspirations through efficient, transparent andaccountable governance mechanisms3.
4. The environment sector to maintain the forest coverage of not less than 60% withprotected national parks and richer biodiversity, and sustainable use of natural resourcesfor socio-economic development.4
2.2 Introduction of DYT and GYT Acts and amendments over time
Decentralisation reforms have changed the state-people relationship from the providers-
recipients to the partnership one. Since the introduction of Dzongkhag Yargay Tshogchung(DYT), district development committee in 1981, ordinary people increasingly took part indrawing of five-year plans (FYPs). They were not only engaged in identifying their needsand priorities, but also in implementing the programmes. The institution of Gewog YargayTshogchung (GYT), gewog development committees, in 1991 further shifted the serviceprovision points from the central to local governments.
The GYT Act (2002) established three categories of functions for the GYTs: regulatory,administrative andfinancial. In terms of regulatory functions, the GYTs were given power tomonitor sanitation standards, environmental management, livestock disease control, housingmanagement and development of local enterprises and promotion of co-operatives.
The administrative functions of GYTs were to identify, prioritise, formulate and monitorgewog plans with the administrative and technical support from the dzongkhag sector staff.The GYTs were to manage a wide-range of development activities like temple management,water supply schemes, irrigation channels, footpaths, mule tracks, farm roads, suspensionbridges, Out-Reach Clinics (ORCs), micro-hydels, community schools, award of contractworks and emergency relief measures.
Thefinancial powers of the GYTs were to approve the annual budget, outsource developmentworks (costing above Nu. 50,000), re-appropriate budgets, collect rural taxes, raise funds,and review expenditures. The financial power has been limited to the rules and regulationsof the Ministry of Finance (MoF).
However, the GYTs enjoyed limited scope to fund the public services through taxes andother revenues. They relied on the Governments annual grants. These grants used to bechannelled through dzongkhag administrations. The grants were given as per the approvedlocal programmes. The MoF used to issue the GYTs the budgeting guidelines and ceiling foreach activity or sector during the planning process itself. The GYTs used to submit the plansand budgetary requisitions to the DYTs, which after reviewing them would forward them tothe central government. The MoF would hold annual negotiations with the DYT members inthe presence of the representatives of the sector ministries involved mainly to review andcomment on the feasibility and implementation modalities of each programme.
2 Ibid. p. 20.3
Ibid. p. 20.4 Ibid. p. 20.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
6/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 3
The three year rolling budget was introduced in 2002-03. The GYTs were given spendingdiscretions as measures to strengthen fiscal decentralisation. However such fiscal discretionwas considered unsatisfactory. The expenditures were subjected to auditing by the RoyalAudit Authority.
2.3 Participatory approaches to planning
The 8th FYP (1997-2002) was the first plan which saw real involvement of the local people,especially at dzongkhag level in the bottom-up planning and implementation withtechnical backup from the civil servants. Local consultations in development planning andlocal service delivery preceded the introduction of legal provisions of the GYTs and DYTs in2002. The GYT and DYT Acts of 2002 and the elections of local heads (gups) in 2002 (on thebasis of adult franchise) further led to administrative decentralisation, and raised thefoundation for fiscal decentralisation. These altered the local administration system andmechanism for budget and resource allocations and for service provisions as the GYTs weregiven some discretion to take up activities of importance for local development and servicedelivery.
The drafting of the 9th FYP (2002-07) was widely gewog-based. The GYTs assessed localneeds, selected schemes for inclusion under sector programmes and carried out priorityfunding. The gewog plans were disaggregated at the dzongkhag and central levels, and thesystem of direct transfer of funds to the local governments was introduced by establishingLetter of Credit Accounts. A Decentralisation Support Programme (DSP) supported blockgrants allowing the gewogs full discretion on activities of the local priorities and needs.
The central government managed some sector programmes to substantiate the localgovernments efforts to improve service delivery and development. Some of the specificdonor-funded programmes were managed as separate projects. They served as programmesupplements for the local development and service delivery. In short, the system of localservice provision and development was, more or less, based on the three-pronged intertwinedapproach.
2.4 Resource allocation
The modality of resource allocation was drastically changed in the 10th FYP (2008-13). Thedzongkhags and gewogs now receive formula-based annual grants from the centralgovernment. This formula considersgeographic area,poverty incidence andpopulation size ofeach gewog. The central sectoral agencies provide earmarked grants to the localgovernments. The multi-year planning and budgeting system is prepared based on annualwork plans with additional two years projection on programmes and budgetary targets.
Among several objectives of Bhutans decentralisation policy like creating space for democraticparticipation, power devolution, local development, and enriching quality of life, one of itskey goals was to provide equitable social infrastructure and quality services. Improving socialconditions of the people through improved social service delivery was the main objective ofthe 9th FYP as well.
2.5 Service delivery trends
The Human Development Index (HDI) trend for the country improved from 0.550 in 1998 to0.613 in 2006 taking Bhutan from being a low human development country to becoming amedium one. The positive trend in HDI can be largely attributed to sustained higher
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
7/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 4
investments in social sectors, the raise in local service delivery performance and the realincome growth.5
The education and health sectors represent the realisation of decentralised service delivery.The management, monitoring and supporting of community schools and non-formal
education programmes were decentralised to the community. The district education sectorprovided teachers and other educational resources, and was responsible for theimplementation of all education activities from primary to higher secondary levels. Theinnovation grants for the local level schools further contributed towards decentralisedschool planning and financial management system.
In 2002, the management of health clinics and ORCs was decentralised to the GYTs with thesupport from the dzongkhag health sector. The district health sector managed hospitals andBasic Health Units (BHUs) while the construction of hospitals and BHUs were done by thecentral sector agency.
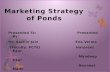
The survey conducted by the Gross National Happiness Commission (GNHC) in 20076proved that education was the most accessible service sector (98%) and health the secondhighest. The least accessible service sector was income generating supports, which calls forcaution. Figure 1 shows the peoples perception re. the accessibility of various services.
Providing access to services is one thing, but how satisfied the people are with the services isanother critical dimension. The GNH Survey (2008) conducted by the Centre for BhutanStudies (CBS) revealed the level of peoples satisfaction with various service deliveryprogrammes. The nature of services were categorised into two: the education, health andenvironment sectors (in Category 1) and electricity, roads and employment sectors in(Category 2). The overall satisfaction with the first category was high; the satisfaction on thesecond category, particularly in rural areas was considerably lower than the satisfaction with
social and environmental services. The urban people reported dissatisfaction with theprovision of employment services.
Table 1 provides the details of the survey. The people rated their highest satisfaction with theeducational services, then provision of health services and environmental conservationservices. These were the main sectors under Danidas sector support programme in the 9th FYP.The area receiving the lowest level of satisfaction was the Governments effort to reducedisparity or the gap between the rich and poor, to ensure employment opportunities and toreduce corruption.
The decentralisation reforms has brought about significant changes in local developmentand improved local service delivery. However, the higher cost of service delivery to
inaccessible communities as well as the context of poor management capacity and fiscalconstraints was and is still a big challenge. This challenge can be put within the context ofrelatively diverse local contexts, availability of socio-economic infrastructure, coordination,and varying capacities of the GYTs.
Figure 1: Accessibility to different service sector (survey, 2007)
5 Ibid. pp. 13-14.6
These survey findings have now been published with the title Rapid Impacts Assessment of RuralDevelopment, 2007.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
8/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 5
Source: Rapid Impact Assessment of Rural Development, 2007, Planning Commission, GNHC.
Table 1: Perception Survey on satisfaction with different service sectors
Service Types Excellent Good Poor
Education services 73 24 2
Healthcare services 72 25 1
Environment conservation and services 67 30 1
Electricity 57 28 14
Roads networks and services 49 36 14
Reduction of corruption 38 39 10
Employment opportunities 38 48 11
Reducing inequity 37 47 11
Source: GNH Survey, CBS, 2008
There was also a salient need to promote greater transparency, accountability and efficiencyin local service delivery; and the need to represent the local interests and concerns at thenational decision-making level in bringing equitable access to service and infrastructure.Decentralisation reforms were the important aspects of the Governments effort to promotegood governance. Many constitutional bodies were established to regulate and coordinatedemocratic processes.
3. Policies and programmes aimed at improved local service delivery
The core principle of the countrys development planning has essentially focused on thefundamental objectives of achieving broad-based and sustainable growth, and on improvingthe overall quality of life through better service delivery mechanisms.7 The Constitution nowmandates provision of free education to all school-going age up to class X; and to maketechnical and vocational education and higher education accessible to all on merit system.
The Government adopted four-pillar approach to create enabling conditions for GrossNational Happiness. The four pillars of GNH were cultural preservation, conservation of
7 10th Five-Year Plan Documents, Volume I, page, 20.
Household Interview (responding 'Yes to access to
service types)
98 94 93 90 90 90 88 82 77 7155
16
0
20
40
60
80
100120
Education
Sanitation
Livestock
Forestry
RuralCredit
Agriculture
Health
Water
Telephone
Roads
Electricity
Income
Generation
Service Types
Percentage
Percentage
Percentage
Percentage
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
9/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 6
environment, promotion of good governance and advancement of balanced socio-economicdevelopment. These pillars were fully attuned to the Millennium Development Goals(MDGs).
The development principle adopted then was that the best way to deliver basic public
services to the people is through decentralised policy mechanisms and democratic localparticipation. To fulfil this policy objective, the efforts were made to devolve and enhancethe power, responsibilities, budgets and human resource capacity of the local electedgovernment system. The Government long recognised that it could deliver efficient andcheaper local services only through its close association and partnership with the localpeople and other service providers. It emphasised community participation in decision-making, implementation and monitoring of the programmes.
Firstly, the Government made tremendous effort to develop the democratic institutions ofgovernance and effective legal system so that it could better respond to the needs andpriorities of the people. The three main principles adopted to promote good governance
were efficiency, accountability and transparency all crucial to enhance the Governmentsresponsiveness to the needs of the people.
Secondly, the Government focused on addressing structural problems and in prioritisingsocial sector expenditures (health and education), promoting decentralisation anddemocratisation through strengthening of administrative and legal institutions (goodgovernance), and private sector development and sustainable use of natural resources(environmental issues). Danidas sector support programmes conformed to these policiesand programmes.
Thirdly, despite a low tax base8, the social sector received more than a quarter of the 9thFYPs total budget. The country fulfilled its commitment to the Global 20:20 Compact that
entailed every country to invest more than 20% in the social sectors. The health, educationand other basic services were provided almost free.
Fourthly, as a donor-dependent country, and to ensure sustainability of foreign aid, theGovernment prudently spent the donors money on poverty reduction through improvedsocial service provision. The total Official Development Assistance (ODA) in the 9th FYPrecorded the increase by more than 45%9, though ODA as a total percentage of GDP hasgone down at less than 20% at present.
Lastly, the Government initiated a Poverty Reduction Strategy Paper process as a part of thebroader ongoing efforts to combat poverty. Its main objective was to strengthen the strategicframework for poverty reduction, improve donor coordination, and build support for new
initiatives in public expenditure management.10 Recognising the difficulty of reaching theun-reached, the overall objectives of the 9th FYP werepoverty reduction and effectivemainstreaming of rural communities into the development process through the provision ofimproved and equitable services.11
8 While the Revenue and Tax Authority is the principal collector of taxes, dzonkhags generate a small revenue fromlocal licenses and fees.9 10th Five-Year Plan Documents, Volume I.10 Department of Planning (2004). Poverty Reduction Strategy Paper, Cover Note the Ninth Main Document, p. 6. 11 Planning Commission (2006). Draft Tenth Plan (2008-13). RGoB: Thimphu.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
10/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 7
4. Service delivery outcome
4.1 Education services and outcomes
Both education and health sectors represented progressive implementation of successfulservice provisions through a mix of decentralised and centralised approaches. The provisionof free education was recognised as an effective tool of poverty reduction. The per capitarecurrent costs of education continued to be relatively high due to the low teacher-pupil ratioand the high proportion of schools which have to cater to highly scattered settlements. Thecost of transporting education materials to remote schools also remained exorbitantly high.
The 9th FYP adopted the education sector as one of the main countrys strategic areas,allocating it the largest share of its resources. The increase in the resources (15% of total planoutlay) was possible due to a large portion of Danidas support to this sector. The capitalgrant supported Ministry of Educations effort to maintain a balance between the increasedenrolment and infrastructure need, and to improve the learning environment and services ofhigher educational needs. Danida supported the construction of schools using Light Gauge
Steel Framing on a pilot basis to minimise the use of timber, sand and stones, and to decreasetime taken to construct schools. This project conformed to one of the six strategic objectivesof the education sectors strategy of realising Vision 2020 to take advantage of neweducational innovations and technologies to increase access to and improve the quality ofeducation.
There has been a 72% increase in the number of schools between 2001 and 2008 and about58% increase in the number of higher learning institutes. In the 9th FYP alone, 111 communityand primary schools were established increasing the total primary enrolment from 93, 974 in2003 to 106,100 in 2008.12 The same plan period saw the increase in Gross Primary EnrolmentRate from 81% to 112% and Nett Primary Enrolment Rate from 62% to 82%. There are now
355 community and primary schools.Figure 2: No. of primary and secondary schools and education institutes 2001 and 2007
Source: Ministry of Education, 2009.
Figure 2 above depicts the increase in the number of schools and education institutesbetween 2001 and 2008. In the Rapid Impact Assessment of Rural Development, education
12 10th FYP Document, page 85.
375 397426 447
458489 502
523
11 11 14 14 18 18 19 190
100
200
300
400
500
600
2001 2002 2003 2004 2005 2006 2007 2008
ear
Number
No. of Schools No. of Institutes
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
11/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 8
was perceived as the most accessible service (national average was 98%). The sameassessment concluded that 71% of respondents perceived schools as accessible within adistance of one hour.
Rapid expansion in the number of schools from 375 in 2001 to 523 in 2008 indicated markedimprovement in the accessibility to educational services. The number of students enrolled inthe primary schools increased dramatically such as increase of the number of class Xstudents entering class XI from 8,464 in 2002 to 16,155 in 2008. This double-fold increase wasprompted by two main factors: Increase in the number of students at the primary and lowersecondary schools and increase in the number of higher secondary schools. Many highschools have improved their infrastructure facilities with proper library rooms, computerfacilities and laboratories. Table 2 shows the number of students in schools between 2002and 2008.
Table 2: Number of students enrolled in the educational institutions from 2002-08 (9th FYP)
Schools 2002 2003 2004 2005 2006 2007 2008
Community Primary School 20,978 22,502 24,533 26,965 29,132 28,953 29,702Primary Schools 28,849 26,168 26,508 25,879 25,745 23,585 22,813
Lower Secondary 41,985 46,856 48,089 48,995 50,576 48,716 48,706
Middle Secondary 19,194 17,735 20,775 20,641 21,236 29,829 32,292
Higher Secondary 8,464 11,268 10,865 13,145 14,414 14,963 16,155
Private Schools 3,813 4,631 5,218 5,763 5,421 6,148 7,444
Total 123,283 129,160 135,988 141,388 146,524 152,194 157,112
Source: Statistical Yearbook of Bhutan, 2006 & 2009, National Statistical Bureau.
The basic education completion rates have improved significantly to 54% and gender parityindex of 1.02 for primary education. These successes had come about despite several
challenges such as inaccessibility, dispersed population, low literacy, significant ruralpoverty and shortage of teachers and other educational facilities.
However, the analysis of census data, 2005, revealed the education deprivation as the mostcommon deprivation in the country. According to this analysis, 23% of school-going childrenin 2005 had not been enrolled in schools (Table 3).13 This was the situation in 2005, anddefinitely, the rate of education deprivation might have gone down in 2009, as many schoolswere opened in the south between 2005 and 2009.
Table 3: Child poverty as multiple deprivations (2005)
Incidence(prevalence) of
deprivation
Number of childrenin relevant age
cohort
Of which experiencingsevere deprivation,% (Bristol Standard)
Of which experiencingless severe
deprivation, % (MDGstandard)
Education 145,411 23 27
Information 232,915 21 22
Shelter 232,915 20 35
Water 232,915 15 15
Sanitation 232,915 9 9
Food No data No data No data
Health No data No data No data
Total 232,915
Source: Population and Housing Census of Bhutan 2005, Office of Census Commissioner, 2006.
13
The authors analysis of Child Poverty and Disparity in Bhutan, 2008. This study was a part of global childstudy funded by Unicef.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
12/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 9
There was also a significant rural urban disparity in education deprivation. About 28.4% ofchildren in rural areas had not been enrolled in schools compared to 9.6% in the urbancentres. The common reasons stated for non-enrolment were the non-affordability ofnominal cost of uniforms and school fees, age factor and lack of income generating activities
(poverty).The percentage prevalence of various dimensions of poverty by districts is given in Annex 1.Deprivation of education and access to information were two important dimensions ofpoverty affecting the Bhutanese children in 2005.
The Governments commitment to raise the enrolment rate has put immense pressure onalready constrained teaching resources and other educational infrastructure at the secondaryschools. The teacher shortage continues to be a major problem. There is also a significantneed to maintain staff morale and improve teachers performance, especially in rural schools.
Serious mismatch between school leavers and availability of secure employmentopportunities has now become a critical concern for the Government. The Governmentseffort to encourage them to take up vocational training has been seriously constrained byshortage of vocational training institutes. This leads to rising social problems such as youthproblems manifested in the form of drug abuse and petty crimes in urban centres.
In the 9th FYP, Early Childhood Care and Development (ECCD) had been given a priority,but except for a few centres in urban areas, extending ECCD to rural areas remained as ahurdle. The Government plans to promote the home-based ECCD programme. It has beentrying to benefit from the progress made in non-formal adult education programme likedeveloping post-literacy materials highlighting the theme of ECCD.
The national adult literacy rate in 2005 was 53%, which by international standard was not soencouraging. The Government has been expanding access to non-formal education asmeasures to reduce adultfunctional illiteracy. Non-Formal Education (NFE) programme wasconsidered successful; NFE Centres increased from 365 centres in 2003 to 747 centres in 2008.The number of NFE learners increased from 12,838 to 13,839 within the same period.
4.2 Health services and outcomes
The government emphasised the health sector as fundamental to fulfilling the broaddevelopment philosophy of Gross National Happiness. The Constitution of the Kingdom ofBhutan, Article 9 Sections 16 and 21 states that access to free basic education and free healthcareare inalienable rights of all the Bhutanese. The Constitution provides for the provision of free,universal and pro-poor health policy.
The Governments health policy constitute the provision of free healthcare services to allcitizens by promoting primary healthcare with an integrated and holistic mix of preventive,promotive and curative care services. One of the core visions of the health sector as reflectedin the Vision 2020 is to ensure primary health care services, extending them to thepopulation in the remotest part of the country through establishment of Out-Reach Clinicsand drawing extensively from the community participation.
The most important goals of the health sector and indicators in the 9th FYP are shown in theTable 4 below:
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
13/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 10
Table 4: Specific Activities Goals and Indicators for the 9th Plan
Indicators 9th FYP Targets
Reduce Total Fertility Rate from 4.7 4
Reduce population Growth Rate from 2.5%
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
14/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 11
the central ministry coordinated with other ministries and municipal governments throughmulti-sectoral task forces. The main partners in the health sector were India, Danida, Unicef,United Nations Population Fund (UNFPA), World Health Organization, Japan, and theWorld Bank.
Figure 3: Trend in healthcare service coverage (1985-2008)
Health coverage (%)
-
10
20
30
40
50
60
70
80
90
100
1985
1988
1989
1990
1991
1992
1997
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Year
Percentage
Source: Ministry of Health and National Statistical Bureau.
Remarkable achievements have been made in expanding healthcare service coverage withphysical access to primary healthcare maintained constantly at 90% (since 1997). Figure 3shows the trend maintained in terms of primary healthcare services from 1985 to 2008.
With about 756 health facilities including training institutes and 519 ORCs, 30 hospitals and178 BHUs across the country by 2008, access to primary, secondary and tertiary healthcare
services has improved substantially. Table 5 provides the details of health facilities by year(from 1998 to 2008).
Table 5: The number of health facilities (2000-08)
Indicators/Year 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Hospitals 28 29 29 29 29 29 29 29 29 30
Indigenous hospital 1 1 1 1 1 1 1 1 1 1
Indigenous dispensaries 11 13 17 19 19 21 21 21 21 26
Training institutes 3 3 3 3 3 3 3 3 3 3
Basic Health Units (BHU) 145 168 168 166 172 176 176 176 178 178
Out-Reach Clinics (ORC) 454 454 461 455 440 476 485 514 519 519
Total health institutions 642 668 679 673 664 706 715 744 751 757
Source: Ministry of Health and National Statistical Bureau.
About 13% (2,214) of the total civil servants (17,178) are now employed in the MoH. Between2002 and 2008, the staff intake into health has almost doubled. Table 6 shows the growth inhealth personnel from 2004 to 2008.
The number of doctors has increased to 171 in 2008 from 135 in 2004. 90 doctors are servingin dzongkhags. The annual increase in the number of doctors and nurses between 1997 and2008 has led to a decrease in the number of population per doctor or nurse (as depicted inthe Figure 4).
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
15/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 12
Table 6: Growth in health personnel from 2004 to 2008
Health personnel 2004 2005 2006 2007 2008
Doctors 144 145 150 154 171
DHOs/ ADHOs 23 22 22 37 38
Health Workers 201 171 229 232 425
Basic Health Workers 171 210 173 173 na
Sister and Nurses / B.Sc Nurses 522 538 587 559 567
General Nurse Midwife/Staff Nurses 183 202 200 255 Na
Auxiliary Nurse Midwife 140 134 134 123 na
Assistant Nurses 175 174 174 176 99
Other Technicians 368 438 420 510 552
Indigenous Physicians 31 30 30 38 na
Indigenous Compounders/Menpas 26 36 42 43 54
Malaria Workers 47 48 48 48 48
Village Health Workers (VHW) 1,201 1,200 1,087 1,200 1,200
Source: Annual Health Bulletin 2009, MOH.
However, MoH still faces acute shortage of manpower in all staff categories, and acutely so,the shortage of doctors, nurses and technicians. The Government plans to open up a medicalcollege. This is expected to resolve the shortage of doctors in the country.
Figure 4: Population per doctor and nurse 1997-2008
0
1000
2000
3000
4000
5000
6000
7000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Population per doctor Population per nurse Note: Base on the PHCB 2005 and assuming a 1.3 % annual population growth throughout the period. A largerpopulation growth in the past would tend to make the curves steeper.
Source: Health Sector Review 2007, Annual Health Bulletin 2007-09.
The child and maternal mortality rates are the important indicators of the populationsaccess to healthcare services, and can show if a country has a sufficient and equitabledistribution of basic goods and services. As shown in Table 7, mothers from the poorestgroup have lesser tendency of seeking prenatal care. This suggests theprenatal care coverageshould be targeted specifically to the mothers in the lower income groups.
The causes of maternal mortality are home deliveries, economic problems, lack of funds withthe MoH, inadequate antenatal clinics, low literacy and knowledge, cultural and religiousbeliefs and poor anaemia control. The underlying causes of maternal mortality are maternalanaemia, limited access to Emergency Maternal Obstetric Centres and inadequate capacityand unattractive facilities for the institutional deliveries. The immediate causes are childbirthcomplications and non-institutional home deliveries.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
16/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 13
Table 7: Wealth quintile and prenatal care
Wealth quintile Prenatal care No prenatal care
Q1 (Poorest) 81.49 18.51Q2 87.15 12.85
Q3 85.84 14.16
Q4 92.52 7.48
Q5 (Richest) 93.58 6.42
87.57 12.43
Source: Bhutan Living Standards Survey, 2007.
Pregnancy complications topped the list for hospital admission between 2006 and 2007.However, the chances of safe delivery and child survival have improved drasticallycomparing to the situation in 2000. The single-most key contributing factor for such an
outcome was an inadequate provision of antenatal care services. The antenatal care coverage(2000-07) for at least once a year was 88%, delivery care coverage by skilled attendants atbirth was 56% and delivery care coverage at the institutions was 55%. The MaternalMortality Rate in 2007 was reported to be 255.14 Table 8 shows the progressive increase in allaspects of maternal and childcare aspects between 2004 and 2008.
Table 8: Maternal and childcare indicators (2004-08)
Type of care 2004 2005 2006 2007 2008
Maternal health care attendance(a) 58,804 54,142 48,859 49,004 53,352
Antenatal 58,804 54,142 48,859 49,004 53,352
Deliveries attended 7,284 6,957 7,675 7,422 8,621Home 2,125 1,629 1,317 1,064 927
Hospital/Basic Health Units 5,159 5,328 6,358 6,358 7,694
Child health care attendance 150,416 161,004 171,135 172,955 187,342
First visit 15,231 15,090 14,589 13,285 14,575
Re-visit 135,185 145,914 156,546 159,670 172,767
Malnourished children (b) 14,312 15,095 16,788 55,529 17,342
All malnourished 13,915 15,095 16,788 55,050 17,342
Third degree 397 n.a 428 479 n.a
Source: Annual Health Bulletin, 2009, MoH.
Antenatal Care Service programmes were used as a platform for programmes to tackle otherproblems like nutrition, reproductive health, HIV/AIDS, STD and Acute RespiratoryInfection. Reproductive healthcare was an important component of primary healthcare in thecountry. The family planning policy emphasised providing every individual or couple withaccess to family planning information, services and counselling. Over the past five years, theuse of various contraceptive methods has increased by an overall 50% as shown in the Table9.
The Crude Birth Rate (CBR) dropped from 38 in 1990 to 19 in 2007 with small variationsbetween urban and rural CBR. The General Fertility Rate was higher in urban areas (84 per
14 http://www.unicef.org/infobycountry/bhutan_statistics.html.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
17/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 14
1,000) than in rural areas (72 per 1,000). Total Fertility Rate (TFR) was 2.5. The rural TFR was2.7 and urban TFR was 2.1, indicating the women in rural areas gave more births comparedto women in urban areas. Higher TFR in rural areas was partly attributed to lack ofknowledge on the significance of family planning in rural areas and higher women illiteracy
rates. Crude Death Rate was seven deaths per 1,000 population with eight per 1,000 in ruralareas and five per 1,000 people in urban centres. CBR was high among infants with infantmortality rate of 41 per 1,000 children.
Table 9: Types and usage of contraceptive methods (2004-08)
Type of Services 2004 2005 2006 2007 2008
Tubectomy 1,364 1,364 1,844 2,808 2,733
Vasectomy 4,919 4,919 7,202 8,927 9,433
Intra uterine device (IUD) Pills (OCP) 2,111 1,305 1,598 2,610 1,970
Condoms 18,807 20,210 32,074 34,688 40,274
Injection DMPA 1,000,679 1,163,234 1,517,705 1,607,790 1,462,467
Other methods 40,745 41,005 57,985 67,965 71,738Total 1,068,625 1,232,037 1,618,408 1,724,788 1,588,615
Source: Annual Health Bulletin, 2009, MoH.
There is no consistent data on child mortality rate in the country. According to the 2006sNational Health Bulletin, 2006, both under-5 mortality (U5MR) and Infant Mortality Rate(IMR) have improved between 1984 and 2006. U5MR dropped to 61.5 deaths per 1,000 livebirths in 2007 from 96.9 in 1994. The Infant Mortality Rate (IMR) has dropped from70.7/1,000 (almost 71 deaths per 1,000 live births) in 1994 to 60.5/1,000 in 2000 and further to40.1/1,000 in 2009 (the same figure is reported for 2009 in the 2010 Annual Health Bulletin).15
In 1990, about 40% of the population had access to clean drinking water; this increased to
78% in 2005. Likewise, in 2005, about 86% of the population had access to basic sanitationlike pits, latrines etc.16 The challenges of providing safe drinking water and sanitation so farwere: (1) acute shortage of specialised manpower to maintain water facilities, lack ofcoordination among stakeholders and technical and financial sustainability. About one-thirdof the existing water supply schemes are in need of urgent repairs. Table 10 shows theconstant increase in the rural water supply schemes. By 2008, EPI coverage has risen to 90%and access to latrines to 90%.
Table 10: Rural water supply and immunization schemes (trend, 2003-08)
Indicators/Year 1985 2001 2002 2003 2004 2005 2006 2007 2008
Rural water supply scheme (nos.) 150 1,944 3,383 3,383 3,852 3,852 3,852 3,852 4,112
Rural population access to piped water (%) 14 65 78 78 78 84 78 78 90
Rural population access to latrine (%) 65 80 88 88 80 89 89 89 90
Universal child immunization coverage (%) - 90 90 90 84 87 90 90 90
Source: Ministry of Health, 2009.
15National Population and Housing Census of Bhutan, 2005. Figures published by Unicef tend to be higher (lesspositive). For instance, Unicef sets the IMR to 54/1,000 (2008) and the U5MR to 81/1,000 (2008)(www.unicef.org/infobycountry/bhutan-statistics.html).
16Planning Commission, now Gross National Happiness Commission, July 2007, Bhutan MDG needs Assessmentand the costing, 2006-15, pp.50.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
18/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 15
Bhutan has achieved almost close to 100% immunisation coverage for children. It hasdeclared universal childhood immunisation in 1991. However, there was some variationamong dzongkhags. The Government had initiated multi-year plan of action for EPI,including the improvement of vaccine quality and health workers capacity. However, the
Government still faces resource constraints to sustain 100% EPI coverage.The outcomes of primary healthcare service coverage are distinctly manifested in the overallincrease in the quality of life. Despite this, the health sector is still confronted with manychallenges. In terms of physical access, Bhutan Living Standard Survey (BLSS) 2007 showedan estimate of 88% of the population living within two hours distance from the healthservice delivery point. Only 40% of the population lived within a distance of half an hourwalk in comparison to 92% of the urban residents (see Table 11).
Table 11: Geographical accessibility in terms of time taken to reach health facility
Time needed to reach nearest health facility
Date source< hr
< 1hr
< 2hrs
< 3hrs
< 6hrs
Noaccess Av time (minutes)
Walking distance
NHS 2000 All 57% 67% 78% 89% 96% 4% n.a.
RIARD 2007 All n.a. 63% 78% 88% n.a. 12% n.a.
Distance using usual means of transportation
BLSS 2003 All 63% 91%
BLSS 2007 All 56% 73% 88% n.a. n.a. n.a. Poor: 109;Non-poor: 56
Urban 92% 99 % 100% n.a 0% All: 19
Rural 40% 61% 82% n.a. n.a. n.a. All: 84;Poor: 111; Non-poor: 76
Sources: Bhutan Living Standards Survey 2003 & 2007; National Health Survey 2000; RIARD 2007.
Long distance to healthcare centres served as deterrents for the people to access healthcare
services. According to the 2005s NHPC, 12.4 % of the population reported that they do notattend health centres because they are located too far from those centres. Lack of time andtransport facilities were two important factors that determined the communitys usage ofhealthcare services. In urban areas, waiting time is one of the reasons for dissatisfaction withthe healthcare service. The physical accessibility aside, there was a significant difference[between regions] in terms of using the healthcare services. Residents in rural areas soughthealthcare service less often when ill than urban residents (rural 88% and urban 97%, BLSS2007). Therefore, the need to reach healthcare services to the un-reached population stillremains a task, and has got to put efforts to attain universal basic healthcare services.
As per BLSS, 2007, the institutional deliveries remained low, possibly due to low level ofacceptability of services. The low number of female workers in the local health facilities and
unfriendly delivery rooms are some of the reasons for less institutional deliveries. Therewere just seven Emergency Obstetric Cares Units in 2007.
The peoples perception (household-based) on the provision of healthcare services like onthe competence of staff, availability of medicines and quality of facilities is given in the Table12.
88% of the people (RIARD, 2007) have reported they had access to healthcare services and60% of them reported the accessibility of health centres within a distance of one-hour walk.The majority of the people surveyed have rate good in areas such as competency of staff,availability and affordability of medicines, and quality of medicines. However, only 41% ofthem rated good for time taken to wait to access health care services.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
19/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 16
Table 12. Distribution of Household by the assessment of quality of BHU/hospital services
Good Satisfactory Bad Doesn't know Total
Competence of medical staff
Urban 76% 21% 2% 2% 100%Rural 84% 13% 1% 2% 100%
Total 82% 15% 1% 2% 100%
Availability of medicines
Urban 74% 23% 2% 1% 100%
Rural 80% 18% 1% 1% 100%
Total 78% 19% 1% 1% 100%
Affordability of medicines
Urban 64% 27% 3% 6% 100%
Rural 60% 25% 4% 10% 100%
Total 61% 26% 4% 9% 100%
Quality of facilitiesUrban 73% 26% 0% 1% 100%
Rural 81% 16% 1% 2% 100%
Total 79% 19% 1% 2% 100%
Waiting times
Urban 31% 44% 24% 2% 100%
Rural 57% 34% 6% 3% 100%
Total 49% 37% 11% 2% 100%
Source: National Statistical Bureau based on Bhutan Living Standard Survey 2007 data.
The prevalence of under-5 ARI, diarrhoea, dysentery, worm infestations, skin diseases andeyes-ears disorder are still high. There is still a need to enhance integrated management ofchildhood morbidities. The morbidities are common among the children and can be preventedthrough an integrated approach to nutrition, proper hygiene practices, immunisation,improvement in sanitation and access to clean water, etc. The increased resources must beallocated to nutrition, immunisation, water and sanitation and health awareness andeducation programmes.
4.3 Agriculture and environmental services
More than 69% of the countrys population still depends on subsistence agriculture. There isa huge shortage of food. This is caused by poor soil fertility, pests and diseases, threat fromwildlife and lack of proper post-harvest management practices, as well as the impacts ofclimate change. More than half of the rural households were reported to experience seasonal
food shortage.The provision of agricultural development services has been recognised as crucial toimprove the national food security. The Government made effort to improve a minimum of70% food grain self-sufficiency through delivery of improved seeds, technology and otherextension services.
The Renewable Natural Resource (RNR) sector is important. It contributes to GDP (one-fifth)and is the major source of employment activity. The RNR sector has critical role to play inenvironmental management and conservation. The rural economy depends on the utilisationof different natural resources through a mixed land-use pattern for subsistence production.The main objectives for the RNR sector are: to attain national food security; to conserve and
manage natural resources; to enhance rural income; and to generate employment
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
20/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 17
opportunities. One of the RNR strategies constituted delivery of extension services. The topdemand from the rural people had always been related to RNR services.
Table 13 gives the details of various agriculture service centres provided by the Governmentbetween 1997 and 2008. The major thrust had been on improving the peoples access to RNR
services. The number of RNR Centres has, therefore, increased from 35 in 1997 to 114 in 2008.They are mostly located in the gewog centres for easy access. However, according to RIARD(2007), 35% of the respondents reported RNR services as accessible within one hour distance,which means that many farmers still have to walk minimum of two hours to access RNRextension services.
Irrigation development has been an important area of the agriculture sector programme.Despite loss of paddy land to urbanisation, rice production has increased over the years. In2005, more than 67,000 MT of rice was produced. The agriculture sector focused on buildingnew irrigation channels and on rehabilitating and renovating the existing ones with thesupport from the communities. In the 9th FYP, more than 133 km of irrigation channels were
built and about 133 km of the old ones repaired.
Table 13: Various Agriculture Services from 1997 to 2008Agriculture and Environment 2000 2001 2002 2003 2004 2005 2006 2007 2008
Agriculture Extension Centres 159 159 79 79 69 51 51 49 50
Agriculture Seed Protection Farms 11 11 11 11 11 11 11 11 11
Plant Protection Centres 3 3 3 3 3 1 1 1 1
Farm Mechanization Centres 3 3 3 3 3 3 3 3 3
Farm Mechanization Trainings Centres 1 1 1 1 1 1 1 1 1
National Mushroom Centres 1 1 1 1 1 1 1 1 1
National Post Harvest Centre 1 1 1 1
RNR centres 35 35 74 74 85 90 95 110 114
RNR Research Centres 4 4 4 4 4 4 4 4 4
RNR Research sub-Centres 6 6 6 6 6 6 6 6 6
Soil & Plant Analytical Laboratory 1 1 1 1 1 1 1 1 1
National Resources Training Institutes 1 1 1 1 1
Source: National Statistical Bureau, 2009.
With 98% of Bhutans poor people living in the rural sphere, Bhutan DevelopmentCorporation Limited is an important credit provider. Micro-financing or rural credit schemesare in a nascent stage. The other essential rural agriculture services consist of provision of
inputs like seeds, fertilizers and tools; access to micro-credit; and access to markets.The production and distribution of improved variety of seeds was a critical determinant ofthe agricultural production so far. Druk Seed Corporation has been distributing the seeds,though; it was not able to fully meet the demands for seeds by small farm holders due tohigh transportation costs to rural areas. The production and distribution of seeds to farmershas remained more or less centralised with no involvement of local producer groups orassociations in this venture.
Improving rural access was recognised as crucial to delivering agriculture input services andaccess to and from markets. Farm roads and power tillers tracks topped the list in localdevelopment priorities, but building roads had been always difficult given the rugged
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
21/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 18
terrain and scattered settlements. However, in the 9th FYP, approximately 800 km of farmroads and 173 km of power tiller tracks have been built.
The other sector of importance for the rural population is livestock farming. The list ofvarious livestock facilities and services (1998-2008) is given as Annex 2.
A rich biodiversity and forest cover and their conservation constituted an overridingnational priority. Maintaining healthy ecology was considered crucial because without it,Bhutan could have become vulnerable to soil erosion, landslides, forest fires, soil depletionwhich would have strong negative impacts on the overall development. The goal of ensuringenvironmental sustainability was pertinent to poverty eradication activities and goals. Thecountry still retains about 72% of its total land under forest cover, 29% under protected areaand 9% as biological corridors.
Danida supported the National Environment Commission (NEC) in strengtheninglegislation, institutionalising environmental assessment process and informationdissemination, and to create enabling policy and legal framework for participatory andsustained management and use of natural resources. The social forestry and communityforest management programmes placed the people at the centre of development andconservation. The GYT Act 2002 empowered the GYTs to manage the community forest,identify parks and frame rules and programmes to prevent local environmental issues.
A new forest development and management schemes helped forests regenerate quickly,bringing direct benefit to the people in terms of availability of fodder, firewood, leaf litter,timber, mushroom and cordyceps. The enforcement of stringent forest rules and regulations,however, also has affected the peoples access to forest resources. The wildlife threat to thecrops has negative impacts on the farm livelihood.
At present, 31% of the population live in urban areas. With rampant urbanisation, majortowns have started facing some environmental issues like waste disposal, deterioration of airquality through pollution and proliferation of squatter settlements. The current urbandevelopment constitutes programmes to improve the standard of living in urban areas witha strong emphasis on the creation of infrastructure, a healthy environment and effectiveservice delivery mechanisms (urban utilities such as water, drainage system, waste disposal,sewerage). The need to improve the livability of the urban environment has long beenrecognised. Danida has been the important partner with the Government in developingurban sector like construction of sewerage facilities in Thimphu and Phuentsholing.However, the quality of urban infrastructure and services are poor in several new townships,in terms of access to water, improper waste disposal, sanitation facilities and provision ofother utilities.
Bhutan Development Finance Corporation is the only financial institution providing credit tothe rural people with its 23 branches across the country. Its field staff travel on motorcyclesto disburse credits, collect payment and savings, but the cost of operation has been extremelyhigh. BDFCL schemes has been plagued by other factors like high costs of administration,low recovery rates, poor market linkages and entrepreneurship, low literacy, and lowrecycling of funds. Rural credit service, though widely available has not been so successfulbecause of the nature of operations specific to conditions imposed that are not alwaysconducive to the poor villagers and small farm holders. The majority of farmers lackcollateral or lack a reliable and diverse source of income to repay. The fear of inability torepay loans deters them from availing the credit facilities.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
22/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 19
4.4 Governance
The access to a proper justice system was considered as an inalienable rights of every citizen,and thus, since 1980s, the Judiciary has been establishing itself as an independent branch ofthe Government, enhancing equal and easy access to justice by improving infrastructure and
institutional capacity. Many of the district courts share buildings with the dzongkhagadministrations, and face the problem of overcrowding and lack of privacy for litigants.Most of the court buildings are in dilapidated conditions and require repairs.
Since 1992, Denmark has supported the Judiciary in improving physical and technicalinfrastructure, organizational development, training and education of judges and benchclerks and legal awareness campaigns. By 2008, five new district court buildings have beenbuilt with the support of Danida. The other donors supporting Judiciary were SDC, UNDPand UNICEF.
The Governments focus on capacity, institutional and operational strengthening of theJudiciary and the donors support programmes resulted in many dzongkhag courts having
separate court buildings. Judicial and legal services to the general public have improved. ICTis now used to enhance efficiency in delivering judicial services. LAN is used in almost allthe district courts. Despite progress in the judicial sector, the infrastructure problems stillexist in many district and dungkhag courts. Many of these courts are not appropriatelyhoused and do not have adequate facilities for effective judicial processes.
The effectiveness of judicial service provision was assed using data from GNH surveyconducted by the CBS in 2008. The court services, according to this perception survey weredivided into two categories: Whether the courts were providing quick justice; and whetherjustice provided was fair or impartial. The survey of 950 respondents revealed that only31.2% of the respondents rated provision of quick justice by courts as excellent, 41.3% rated itas good and 12.3% rated it poor. In terms of fair judgment, 34.7% rated it excellent, 42% ratedit good and 6% rated it poor.
The timeliness of court adjudications has improved on average between 2000 and 2006(shown in Figure 5). However, substantial numbers of court cases have taken more than 108days. The reason was a shortage of judges, which calls for the need to train more judges(Human Resource). The increase in number of appeal cases increased in 2006 to 173 from 123in 2004, showing peoples dissatisfaction with the services of local courts17. The generalperception on courts performance in dzongkhags like Thimphu, Dagana,Wangduephodrang, Trashigang and Samdrupjongkhar was poor according to the samesurvey.
The general perception on the leadership qualities of local leaders: Gups, mangmis andtshogpas were higher than that on leadership qualities of dzongdags. This may have to dowith the local people having to deal more with the GYT leaders than the dzongkhag officials.The people consider leaders as good based on past performance experience, maintainingharmonious relations with the people and those who understand communitys problems.Ability to read and write is not so important a criterion, and this presents an interestingpolicy issue.
17 P. Rabten, GNH Survey Findings.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
23/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 20
Figure 5: Duration of number of courts cases (2000-06)
Duration and number of courts cases between 2000-2006
1896
3162
3550
5721
4388
2695
37083753
6064
48274975
5471
6158
5641
0
1000
2000
3000
4000
5000
6000
7000
2000 2001 2002 2003 2004 2005 2006
Year
No.ofcourtcasesadjucated
More than 108 days
Less than 108 days
Source: www.judiciary.gov.bt, html/case/statistics.php
4.5 Communication
Another important service area where considerable improvements have been achievedincludes telecommunications and postal service sectors. The Information andCommunication (ICT) sector is beginning to play a key role in socio-economic growth,transfer of knowledge, improvement of efficiency and transparency, improvement of localservice delivery and empowerment of the poor. At present, all the 20 dzongkhags and 199gewogs (out of 205) are connected with telecommunication networks including mobilenetworks. The Wide Area Network (WAN) intranet and Local Area Networks (LAN) are
established in all the 20 dzongkhags. E-service is expected to improve the speed of servicedelivery to the people. This has been already happening as the dzongkhags and other serviceagencies have their own websites from which the public can download forms, or makeseveral online applications.
There has been drastic improvement in the provision of service by the telecommunicationsector as is evident from the increase in the number of telephone exchanges, number oftelephone connections and number of internet connections. Annex 3 shows that the numberof telephone exchange has increased from 26 in 2000 to 82 in 2008; and internet connectionsfrom 446 in 2000 to 5,422 in 2008. The table showing the number of ICT facilities (2000-08) isattached as Annex 3. Over the years, the postal service facilities and wireless stations have
decreased, and this signifies the positive impact of ICT on the communication sector.
5. Challenges on improved public service delivery
The provision of quality and equitable services is challenged by the geo-physical nature ofthe country and scattered settlements. The inaccessibility of certain communities to the maincentres of development hampers delivery of basic goods and services, escalates their costsand creates disparities. Frequent landslides and road blockages, and the need to maintain theroads and other communication infrastructure take away substantial amount of funds,thereby resulting in fewer resources for local service delivery.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
24/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 21
5.1 Mandates and responsibilities
There seems to be a further need to improve an accountability mechanism and efficienttransparency system in service delivery. The community involvement - especially the poorerones - in the assessment of quality and efficiency of public service delivery has not improved
as purported. The local communities do not have adequate mechanisms to monitor and toconduct social auditing or to participate in expenditure tracking, though social auditing iscrucial in assessing the social or community benefits of the public services. The poor peopletend to remain satisfied with what is provided to them. The roles of community-basedorganizations, now recognised as civil society organizations, in analysing and engaging in policydialogue are limited.
Policy makers are compelled to remain poorly responsive to the pledges of the communitymembers due to a long channel of reporting. Policy makers at the central level could hardlyreach the unreached and poor because of the higher cost involved. It was for this reason thatGood Governance Plus, 2005: In Pursuit of Gross National Happiness notes that the route ofaccountability is often too long and policy makers can rarely be reached by clients, especially
poor clients with information, complaints and feedback.
The report further notes that the policy makers cannot necessarily lead to improved publicservice delivery even if the clients reach them because of the long route of accountabilitybetween the policy makers and service providers. Even if the services were to be provided,timeliness of delivery is an issue. The Government has identified ICT as an effective tool tocurb this long route of accountability and a useful tool to improve access to information andservices to remote regions, but most of the gewogs still lack IT capacity, both in terms ofresources and technical skills. The gewog ICT centres are still in a nascent stage.
One of the objectives of decentralisation is to enhance the policy dialogue between thecentral level and DYTs and GYTs, but the link between various ministries, sector agencies,
and local governments is ambiguous. For example, the Ministry of Home and CulturalAffairs is still seen as the main agent for receiving the development related complaints orfeedbacks (from the local people) and as the lead agency to coordinate decentralised servicedelivery. The minutes of the DYTs and GYTs meetings are therefore usually submitted tothis ministry, which are hardly analysed leading to ill-response or inaction as this ministry isnot fully responsible for entire sets of public services18. It is mainly responsible for culturepromotion, security, census and immigration and disaster management. Dasho Karma Urapoints out the need to enhance inter-agency coordination, and for relevant phases ofdeliberations at the DYTs and GYTs to be passed through the concerned ministries to thecentral government for effective decisions.
DYT and GYT minutes contain deliberations on issues covering all aspects of servicedelivery and have implications for relevant agencies and ministries. The GYT minutes arenormally written in Dzongkha, whereas English is popular in many of the central ministries.This creates certain communication gaps or impedes exchange of information between thecentral and local governments. Ura further notes: At the moment, there is noinstitutionalisation of feedback and no unit to process information gathering from the localgovernment levels. The information flow, according to Ura, is one-way and like emptying itinto a vacuum, which affects the service delivery. The communication linkages in most casesare weak and lack dissemination of information on the plans, schemes, outcomes, costs andbenefits.
18 Dasho Karma Ura, Archers and Deities.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
25/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 22
The GYT Act 2002 empowers local governments to hold gewog field staff accountable for theservice they provide, but there is no clear way of doing it. These officials are moreaccountable to the district administrator (dzongdag) and the root sectors rather than beingaccountable to thegups or other GYT members. There are no proper sanctions or rewards.
There is no system of reporting the monitoring aspects to improve the outcomes of varioussector service provisions.
Gups who are mainly responsible for decision making and implementing service deliveryactivities may have some conflict of interests. The local leaders are not highly educated andtrained to make effective decisions and implement the programmes. Moreover, the GYTs areconstrained by shortage of staff, including technical personnel. The DYTs comprise of gups,mangmis as indirectly elected members and dzongkhag sector staff as the observers. TheDYT members are mostly men, thus limiting the role of women in decision-making ondevelopment and service delivery. Either dzongdag or other sector heads advises the DYTson all matters of policy, rules and procedures. There is an active dialogue between the sectorstaff and the DYT members on issues such as progress reports, planning schedules andpolicy queries, but there is not so much information flow back to the GYTs.
5.2 Capacity of local government
The important dimension of local service delivery is whether every local government andcommunity has equal capacities to absorb the resources efficiently and effectively, or getequal access to goods and services. Despite increased efforts to channel goods, services andinvestments to rural areas, some communities constrained by low knowledge, expertise,technological capacities, shortage of skilled manpower and isolation - have not benefitedequally. Having access to services does not alone indicate use of services.19 In addition, somesectors have not been able to deliver the same level of services as others. The PovertyAnalysis Report (2004) mentions that the services by the industry and agriculture sectorshave been chronically affected by low levels of labour productivity. Certain communitiesalso lack behind in terms of socio-economic indicators, either because they are isolated orface shortage of personnel to deliver services.
The administrative capacity is crucial for a successful decentralization and for properlyimplementing development programme and service delivery activities. After 2002, theadministrative set-up saw the increase in the number of staff in district administrations (50-70 at dzongkhag head quarter with 20-40 extension staff excluding teachers and healthworkers). But, the technical staff continue to have a dual line of reporting both to thedzongdag and the centre thus creating confusion. There is no devolved authority over cadresize at dzongkhags. It is still done centrally. The dzongkhag has only the authority to
appoint general service cadre of grade below 13 and elementary service posts. Thegups andthe GYT members are far less educated, have lesser remunerations than the gewog sectorstaff, which makes it difficult to put a check-and-balance against them.
The dzongkhag administration needs more qualified staff than support staff but the situationin most dzongkhags is otherwise. This is a reflection of the lack of a comprehensive andcoordinated human resource development policy in tune with the decentralisation policy. Insupport of devolution, the Royal Civil Service Commission (RCSC) has deployed HumanResource Officers (HRO) at dzongkhags. In 2004, the first batch of district HROs wereappointed. This initiative was seen as a forerunner of further human resource developmentinitiatives at the local level but so far there has not been any visible impacts, since these
19 Rapid Rural Impact Assessment p. 23.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
26/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 23
officers lack experience and are neither supported by a district HRD plan nor have sufficientfunds to implement HRD development programmes. This leaves HRD plans highlydependent on donor funding.
The DYT and GYT members were given both short and long-term training on routine
administration but the fact that they serve in their posts for only a certain number of yearshas set a requirement for the continued need to train newly elected leaders. Many of themget replaced in the next elections, that too, after making considerable investments in trainingthem. Until now, this kind of training has been externally funded but whether suchinitiatives can continue with the phasing out of support programmes by various donoragencies is a critical question. The Royal Institute of Management has been providingtraining courses for the DYT and GYT members, but absence of partnership and involvementof other ministries led to these courses being delivered without actually capturing theessence of sector-based decentralised service reforms.
The GYTs are auditable and accountable units of the Government. The gups act as both
political and executive heads. They have to serve the double roles of GYT administration andoverall governance, putting them under tremendous pressure. There is a need to strengthenexecutive staff capacity in the GYTs, otherwise, there is immense risk of comprising thedecentralisation reform. The recent initiative to post gewog administrative officers (GAO)and accounts officers is a move towards strengthening the executive capacity of the GYTs.However, as long as the variation in the size of gewog administrations exist, larger GYTs arelikely to remain constrained by shortage of executive staff as these GYTs have moreadministrative works comparing to the smaller ones.
What came up clearly during the Joint Evaluation Missions (2009 December) focus groupdiscussions with the dzongkhag officials of Punakha was the issue of shortage ofprofessional staff. There is a heavy reliance on the dzongkhag administration to undertakeall technical support work including scheme estimation, design, tendering, contractmanagement, supervision and monitoring.
The dzongkhag administrations too face the severe constraints of technical staff. Forexample, the engineers who are the most demanded professionals for the construction andmaintenance of roads, irrigation channels, water supply schemes, schools and dispensariesare based in the district headquarters while the actual activities take place in the gewogs.They cannot cater to every local demand [for technical assistance] as the district engineeringunits have one or two engineers, who are further constrained by lack of adequate transportfacilities, travel budgets and other incentives to travel to construction sites. Though most ofthe construction works are outsourced, these engineers cannot participate and monitor the
construction quality. The results are poor standard infrastructures for the local people.
Besides, the rural areas fail to attract central staff due to lack of incentives and opportunitiesfor higher training. Most of the professionals and civil servants are concentrated in thecentral ministries. They defy rural postings due to difficulties of livelihoods, lack ofincentives, less training opportunities, etc. The local governments have no authority to hireor fire the local officials like community teachers, health assistants, foresters, RNR staff, etc.They are placed by the central government and their remuneration is determined centrally.
The local governments capacity to deliver services effectively is constrained by the lack ofan institutional framework for coordination among different sectors. RNR tries to deliveragriculture sector service in a package comprising of forestry, livestock and agriculture
services, but when it comes to actual delivery, it happens independently. The GYT members
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
27/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 24
spearhead the local service delivery plans and programmes, but they lack knowledge onresource analysis, prioritisation of services and activities and financial management foreffective service delivery planning (RIARD, 2007).
Even if the facilities like BHUs and schools are set up, there are many cases of these facilities
being understaffed, especially in rural areas. This represents the case of creating the servicecentres with inadequate number of skilled service providers. Decentralisation is not just amatter of devolving power and responsibilities to the GYTs, but to seek to define the specificroles and responsibilities and provide appropriate staff to the local sector offices to make anoptimal use of limited resources. The local agencies should have adequate and appropriatestaffing strength to fulfil local goals and objectives while the central government fulfils thenational objectives.
Decentralisation reforms have given considerable degree of discretionary powers to the localadministrations in relation to the budget implementation, procurement, expenditure, etcwhich has contributed to the general efficiency in the service delivery. The issue here is
whether there are enough people at the GYTs (personnel) to operate these funds.The community schools are under the management of the community, though staffed by thecentrally placed staff. One of the challenges facing community schools is that the local peoplefail to see the immediate benefits of education for their children, and therefore, get littleincentives to cooperate and support the school management. When the community schoolsmanagement refers such cases to the DYTs and district education sector, they take leastinterest in the matter because the community schools do not fall within its purview. Thisleads to the poor service quality, in the form of ill-maintained school infrastructures.
What is the policy pattern of production and provision of local services? There seem to besome ambiguities in functions among the providers. For example: Goenshari gewog one of
the most inaccessible gewogs has most of its lands under Jigme Dorji National Park. Thispark is managed by the Park Office located at Damji under Gasa dzongkhag. The villagerstravel all the way to Punakha dzongkhag headquarter to get the permits only to be sent backto the park office. This creates lot of confusion and problems for the people. There are toomany complications to avail services including filling up forms which sometime is not soconducive to illiterate people, and those who provide services are helpless as they are boundby practices and rules.
5.3 Participatory planning
The community members are involved in the process of designing and implementing planswith technical backstopping from the civil servants. However, the participation of themembers of different groups is complex, as the knowledgeable and influential, and withsome exposure to government, and therefore vocal members tend to dominate the planningdiscussions and decisions.20 This indicates a need to improve planning process to preventelite capture; otherwise it defeats the purpose of grass-roots participatory planning anddevelopment. Lack of literacy, numeracy and access to information are major inhibitors ofthe mass participation.
Another pertinent area in the planning process is transparency. The planning is done in thepublic meeting, but people are mostly not aware of budget allocations for activities to beimplemented or deferred.21 The planning process carried out is a one-off event and
20
Rapid Rural Assessment (p. 48).21 Rapid Impact Assessment for the Rural Development, pp.56.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
28/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 25
commences at village level. Once the plans are made, a system for farmers to check the plansdoes not exist as monitoring is done by the GYT, not chiwogs, though the latter is thesmallest unit headed by tshogpas who have direct contact with the local people22. The extentof decentralised planning is limited by the sector-wise budgeting system and, although
communities are empowered to identify and select activities for priority funding, the overalldesign of the plan activity lies with the respective sectors. There is a tendency for the plan tobecome an offshoot of the budget rather than the plan shaping the budget allocation. This isin contrast to planning for activities under the DSP or Local Government DevelopmentProgramme supported block grants mechanism where the gewog has full discretion todecide on any activity, scheme or sector in line with the local priorities and needs.
The level of participation and submission of requests by different communities also dependon the dynamics between various groups and level of cooperation and conflict among themin executing development or service delivery programmes. Some communities often cannotcome to terms on the location of the common development or service centres. The localcapacity, context and nature of settlements matters much in this case. The arbitrators, whoare usually civil servants of the dzongkhag administrations, make the decisions on theirbehalf, whose decisions often lead to wrong locations of service centres.
In some other cases, the nature of settlements determines the access to the service centre. InGoenshari gewog, the Gewog Service Centre (RNR, Gups Office, School and BHU) are alllocated together away by a distance of more than two hours from every village in the gewog.This means the peoples accessibility to the gewog service centre has not improved much.
The rural people when discussing development activities are largely concerned with theinputs but think little about the outcomes. One typical example: the communities ofGoenshari gewog, have fought through for road budgets and built two farm roads withoutactually building bridges, and so far, these roads have not been able to improvedevelopment and service outcomes for local residents.
The consultations with the local people by the local staff or district staff normally arepatterned in such a way that in the end, they come up with a long wish-list or list ofunrealistic demands or over-planning. The consultations do not emphasises much on wherethe limited expenditure should be focused-based on the balance between the needs ofcitizens and what the Government can realistically afford, but in most of the consultations,the district administrations or local staff end up saying they would submit it to GNHC orother ministries for further scrutiny thereby creating unrealistic expectations in the minds ofthe local people. The plans are made by the local people, and these plans are normallyambitious, and lack consistency between the plans and adequacy of the resource envelope
and priorities, resulting in non-implementation.
So far, there has been no one-stop services, though the present Government has announcedits plan to set up these facilities. This somehow results in poor inter-agency coordination. Forexample, in order to claim pensions, the pensioners have to travel all the way to districtheadquarters, which otherwise could have been effectively done from the nearest post officeor banks. The process of service delivery in many cases is procedurally long.
5.4 Service delivery
There are no set standards for procedural requirement including time of delivery. There areno quality assurance groups in the ministry or agencies to assess the compliance of service
22Ibid. pp.56.
-
7/27/2019 201002ThematicPaper LocalServiceDelivery Final
29/39
Thematic Paper: Local Service DeliveryJoint Evaluation of Danish-Bhutanese Programme 2000-09
PEMCONSULT/OXFORD POLICYMANAGEMENT 26
providers through internal checks and feedbacks from the public. GG Plus recommendedestablishing such groups, but many agencies do not have the one.
A further challenge is presented in the form of infrastructure and service delivery inenvironmentally protected areas. Bhutan has a strong commitment to environmental
protection especially relating to national parks which have strict controls on the nature andform of infrastructure. At the same time local government needs to be involved in regulationand enforcement of these provisions. There are park management offices, their functionsoften duplicating the functions and authority of the GYTs in the management of theenvironment.
Improving access to clean and safe drinking water through water supply schemes in ruralareas has been given priority since 1974. The major setback is that once the water supplyproject is completed and handed over to the communities, many of them fail to remainoperational because of poor maintenance. The communities lack skills and resources tomaintain the schemes. It was found out, as early as in the 1990s that ineffective community
management of water supply facilities was a real threat to the programmes sustainability.One of the complaints that the people raised during the election campaigns in 2008 was onshortage of drinking water. Sustaining water supply services has become a challenge tohuman development.23
Rural-urban migration is another problem affecting service delivery. The proportion ofpeople living in urban areas has increased from 21% in 2004 to 31% in 200524, putting unduepressure on health and educational facilities in urban areas and leading to under utilisationof those facilities in rural areas set up with higher establishment and operational costs.
While the communicable diseases are common, non-communicable life style related diseasesare increasing, posing a serious double-burden of diseases. The enormous resources
demanded for these double-burden diseases might affect the resource available for theprimary health care services.25 The MDG 2005 Report claims that achieving 4th MDG ofreducing child mortality will require emergency obstetric care services made available andaccessible to every pregnant woman in need. There is lower maternal and newborn careservices in rural areas and low literacy of mothers and caregivers add to poor outcomes forchildren.
Services like rural credit schemes, due to its operation conditions have not reached widely.The loan scheme has not been conducive to poor small farm holders as they lack necessarycollaterals and do not have diverse sources of income to repay the loans. In principle, creditaccess is available to all, but many poor farmers do not avail loans fearing their inability torepay them. Credit provider like Bhutan Development Finance Corporation also does notprovide loans to everyone due to delay in repayment and non-payment of loans.26 Out of1,141 respondents in a sample survey, only 167 (15%) responded they availed rural credit,whereas 90% said they have access to the same.
To decentralise the delivery of goods and services, local government must be given sufficientfiscal discretion, besides giving them clear roles and responsibilities. However, in-depthinterviews with dzongkhag officials and focus group discussion (RIARD, 2007) revealed
23 Kuensel. Bhutan: much vaunted water