A competitive analysis justifying expansion into the Single‐Port Laparoscopic Surgery market with a Single‐Port Access Device ii Table of Contents 1.0 Abstract...................................................................................................................................1 2.0 Laparoscopic Surgery .............................................................................................................1 2.1 Single-Port Laparoscopic Surgery...................................................................................1 2.2.1 Advantages ...............................................................................................................2 2.2.2 Disadvantages ..........................................................................................................3 2.2.3 Failure Modes...........................................................................................................3 3.0 Single-Port Access Devices................................................................................................4 3.1 Current Products..............................................................................................................4 3.1.1 Covidien SILS Port Multiple Instrument Access Port..............................................4 3.1.2 Ethicon Endo-Surgery SSL Access System .............................................................5 3.1.3 dalimSurgNET OCTO-Port System .........................................................................5 3.1.4 KARL STORZ Endocone ........................................................................................6 3.1.5 Applied Medical GelPOINT Access Platform .........................................................6 3.1.6 Advanced Surgical Concepts TriPort Access System ..............................................6 3.1.7 TransEnterix SPIDER ..............................................................................................7 3.1.8 Surgiquest AirSeal Trocar ........................................................................................8 4.0 Device Design Proposal .....................................................................................................8 4.1 Proposed Solutions ..........................................................................................................8 4.1.1 Visualization and Triangulation ...............................................................................8 4.1.2 Internal Retraction and Range of Motion .................................................................9 4.1.3 External Interference ................................................................................................9 4.1.4 Surgical and Operational Failure............................................................................10 4.1.5 Training and Learning Curve .................................................................................10 4.2 Functional Specifications ..............................................................................................10 4.3 Regulatory Aspects .......................................................................................................11 4.4 Manufacturing Processes...............................................................................................11 5.0 Conclusion........................................................................................................................11

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

AcompetitiveanalysisjustifyingexpansionintotheSingle‐PortLaparoscopicSurgerymarketwithaSingle‐PortAccessDevice
ii
TableofContents
1.0 Abstract ................................................................................................................................... 1 2.0 Laparoscopic Surgery ............................................................................................................. 1
2.1 Single-Port Laparoscopic Surgery................................................................................... 1 2.2.1 Advantages ............................................................................................................... 2 2.2.2 Disadvantages .......................................................................................................... 3 2.2.3 Failure Modes........................................................................................................... 3
3.0 Single-Port Access Devices ................................................................................................ 4 3.1 Current Products.............................................................................................................. 4
3.1.1 Covidien SILS Port Multiple Instrument Access Port .............................................. 4 3.1.2 Ethicon Endo-Surgery SSL Access System ............................................................. 5 3.1.3 dalimSurgNET OCTO-Port System ......................................................................... 5 3.1.4 KARL STORZ Endocone ........................................................................................ 6 3.1.5 Applied Medical GelPOINT Access Platform ......................................................... 6 3.1.6 Advanced Surgical Concepts TriPort Access System .............................................. 6 3.1.7 TransEnterix SPIDER .............................................................................................. 7 3.1.8 Surgiquest AirSeal Trocar ........................................................................................ 8
4.0 Device Design Proposal ..................................................................................................... 8 4.1 Proposed Solutions .......................................................................................................... 8
4.1.1 Visualization and Triangulation ............................................................................... 8 4.1.2 Internal Retraction and Range of Motion ................................................................. 9 4.1.3 External Interference ................................................................................................ 9 4.1.4 Surgical and Operational Failure ............................................................................ 10 4.1.5 Training and Learning Curve ................................................................................. 10
4.2 Functional Specifications .............................................................................................. 10 4.3 Regulatory Aspects ....................................................................................................... 11 4.4 Manufacturing Processes............................................................................................... 11
5.0 Conclusion ........................................................................................................................ 11
iii
ListofFigures Figure 1: The total number of single-port laparoscopic procedures is compared to the number of
traditional laparoscopic procedures [4]. .......................................................................................................... 2 Figure 2: This illustrates the current and anticipated market size for specialized single-port trocars
from 2009 to 2014 [4]. .................................................................................................................................... 2 Figure 3: These are mean score results from simulated surgery using traditional laparoscopy
methods and single-port access, demonstrating that SILS experience is still beneficial to surgeons with prior multiple-port laparoscopy experience [5]. .............................................................................................. 3
Figure 4: This illustrates the final insertion of the Covidien SILS device [15]. ............................... 4 Figure 5: This is a diagram of the Ethicon Endo-Surgery SSL set of devices [16]. ......................... 5 Figure 6: This is the OCTO-Port system, which consists of a wound retractor, attachment ring,
and port cap [17]. ............................................................................................................................................ 5 Figure 7: The seal cap for the OCTO-Port system is interchangable to accomodate varying
instrument configurations [17]. ....................................................................................................................... 5 Figure 8: This is the KARL STORZ Endocone [18]. ....................................................................... 6 Figure 9: This is a picture of Applied Medical's GelPOINT product [19]. ...................................... 6 Figure 10: This illustrates the correct method necessary to introduce the distal ring to the
abdominal cavity [21]. ..................................................................................................................................... 7 Figure 11: This is a diagram of the ASC TriPort Access System [21]. ............................................ 7 Figure 12: This is a diagram and cross-section view of the TransEnterix SPIDER device [10]. ..... 7 Figure 13: The AirSeal forces air into the cannula, maintaining relatively constant pressure and air
circulation [24]. ............................................................................................................................................... 8 Figure 14: The open nature of the device permits insertion of multiple tools simultaneously [24]. 8 Figure 15: This illustration demonstrates the internal crossing of hand tools while using a
GelPOINT single-port access device [20]. ...................................................................................................... 9
ListofTables Table 1: This is an abbreviated list of functional requirements for a single-port access device. ... 10
Page 1
AcompetitiveanalysisjustifyingexpansionintotheSingle‐PortLaparoscopicSurgerymarketwithaSingle‐PortAccessDevice
Edwin Chung August 9, 2010
1.0Abstract Single-Incision Laparoscopic Surgery
(SILS) is being rapidly accepted as an alternative to multiple-site laparoscopic surgery. The primary benefit cited is the improved cosmetic result due to the single incision being made inside the umbilicus. This presents an opportunity for market growth, which can come from the development of new products as well as re-branding of current products.
Development of new and innovative devices will propel adoption of SILS procedures by minimizing disadvantages. The primary issues inhibiting adoption are: the reduced movement range in the intracorporeal space and the adaptation to limited viewing angles from the laparoscope.
Current products being utilized in traditional laparoscopic procedures can be marketed unilaterally for enhancing SILS procedures, earning an additional share of the laparoscopic hand tool market.
In conclusion, marketing and training programs combining our superior and well-established camera technology with a complimentary single-port access device can establish our initial share of the SILS market.
2.0LaparoscopicSurgery Laparoscopic surgery is a minimally
invasive technique used to treat condition in the abdomen. Traditionally, this is done by making three to five incisions and inserting trocars – hollow metal tubes – through the skin and muscle. An insufflation tube is introduced
through one of the trocars and used to create a pressure “bubble”, ultimately lifting the muscle wall up and providing an internal space for the surgeon to use during the procedure. Next, various instruments are inserted into the cannulas, starting with a laparoscope. The laparoscopic camera (laparoscope) is an integral part of any minimally invasive surgery since it provides the doctor with vision inside the body cavity. Other tools used include graspers and cutters and come in varying shapes and sizes. Depending on the circumstances, another incision might be necessary to rescind an organ or tissue matter.
Laparoscopy has been very popular due to its clear benefits over open surgery. Patients receiving this kind of operation typically recover in a few days, which has an additional benefit of reducing costs for the hospital or medical professional.
2.1Single‐PortLaparoscopicSurgery Single-Port Laparoscopic Surgery, often
referred to as “Single Port Access (SPA) Surgery” or “Single Incision Laparoscopic Surgery (SILS)”, is rising in popularity only recently despite the first reported SILS being done by Navarra et al. in 1997 [1]. “The guiding principle [of SILS] is operating through a single transumbilical incision” [2]. After an incision between 15mm and 25mm long is made, multiple cannulas are inserted through the opening [3] to permit insertion of equipment. Typically, this involves use of a laparoscopic camera and two hand tools, sometimes requiring reinsertion and alternating equipment. If necessary, such as during a cholecystectomy, the
Page 2
specimen is removed through the same transumbilical incision upon completion of the surgery.
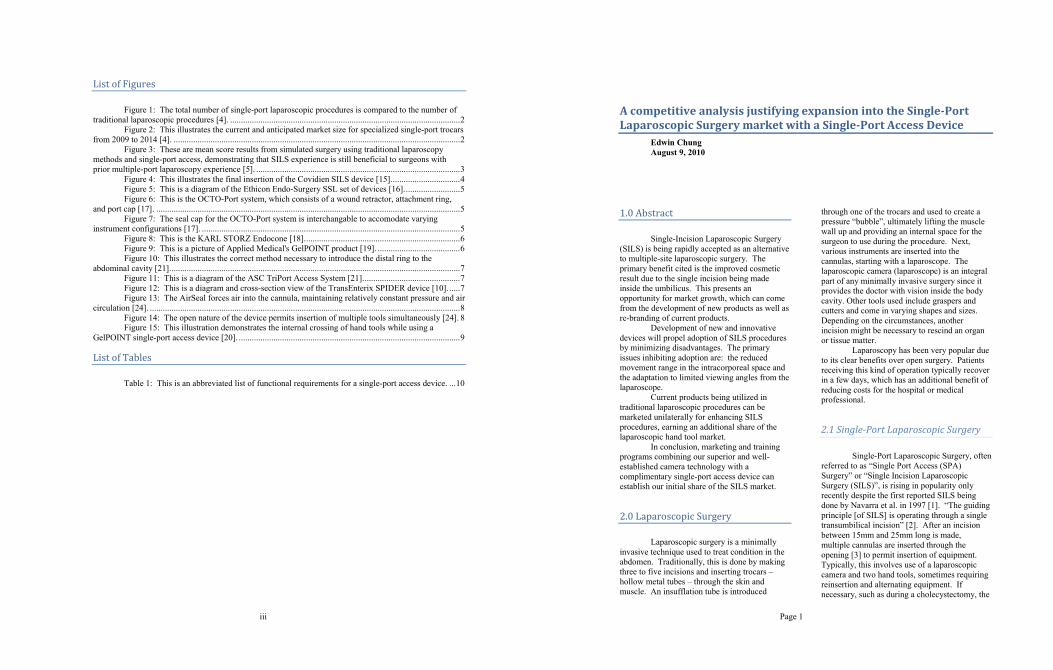
Although only 0.4% of laparoscopic surgery used a single-port method in 2009, it’s expected that almost 24% of laparoscopic surgeries will use some form of SILS in 2014. Millennium Research Group anticipates this will equate to an approximately $138M market by 2014, as illustrated in Figures 1 and 2 [4].
Figure 1: The total number of single-port laparoscopic procedures is compared to the number of traditional laparoscopic procedures [4].
Figure 2: This illustrates the current and anticipated market size for specialized single-port trocars from 2009 to 2014 [4].
Demand for SILS procedures will
continue to increase due to the inherent advantages [4]:
Superior cosmetic results Reduced postoperative pain Decreased blood loss and Fewer complications.
It is also important to point out that additional studies which demonstrate the efficacy of SILS procedures and improved training curricula will
increase surgeon acceptance of this new class of procedure [5].
Demand for specific SILS access devices, on the other hand, will be dependent on the marketing, research, and development of devices that resolve the disadvantages of SILS procedures [6]:
Triangulation difficulties Reduced intracorporeal work space Instrument collision Hand collision and A steep learning curve.
2.2.1AdvantagesThe primary and most consistent benefit
of SILS procedures is the cosmetic outcome [7]. The “cosmetic results of SILS are due… to the fact that… the scar can be hidden in the umbilicus” [8].
Furthermore, having a “single midline fascial incision minimized trauma to the abdominal muscles, epigastric arteries, and parietal nerves” [2]. This reduction in physical damage results in decreased postoperative pain and shorter recovery time [2] compared to multiple-site incisions, although some research indicated that the larger incision may increase the risk of hernia or infection [9] [10].
Lastly, cost is a significant factor contributing to the adoption of SILS compared to other types of minimally invasive surgery. Rawlings et al. reported that they “were able to use existing equipment with an additional material cost compared with conventional [laparoscopy surgery] of approximately $410” [7].
Initially, surgeons used multiple trocars inserted into the single incision simultaneously. Although this contributed to limited maneuverability of the tools, problems maintaining pneumoperitoneum, and issues for the operators, it demonstrated that the procedure could be done using standard, inexpensive laparoscopic instruments [7]. In fact, surgeons found familiar and ergonomic laparoscopic instruments reduced the learning curve for technical and complex procedures [2] [11]. Because no major capital investment was required, it was easier to adopt SILS procedures in the hospital [8], despite the disadvantages.
Page 3
2.2.2DisadvantagesThe initial impression surgeons reported
was that the “difference between the single and standard laparoscopic technique is the absence of instrument triangulation” [8]. The reduced triangulation of movement is inherent with working around a single point of entry. Rawlings et al. found that by “placing… instruments through a single umbilical incision, triangulation between the camera and the working ports is lost. Parallel instrument alignment [results in an] ‘in-line’ view of the anatomy and field of dissection” [7]. For experienced surgeons, the absence of familiar instrument triangulation may have resulted in confusion or hesitation. Pryor et al. specifically stated, “A practical single-port system, which could effectively replicate multi-port laparoscopy and potentially replace it, will need to enable triangulation and have effective retraction capabilities” [10].
A severely limited range of motion inside the abdomen inhibits retraction and caused movement of the instruments to be “jerky at times” [12]. Because of the close proximity of the insertion ports, “‘sword fighting’ of instruments can restrict freedom of movement and viewing, as well as dissecting angles” [7]. In addition, movement would often deflect the camera [12], causing disruption in the current action.
Additionally, users reported that external interference negatively impacted results as well. This included interactions between the laparoscopic instrument handles, as well as the surgeon’s hands, during an operation [8]. It also included interference with the camera shaft, camera handle, or camera operator who was assisting in the procedure [8], complicating “the holding of the laparoscope for the assistant” [2].
Finally, there is an additional training requirement due to the differences between standard and single-port laparoscopic surgery. Leblanc et al. indicated that the “prolonged learning curve had led to [a] low adoption rate” [2]. Solomon et al. later determined that “the learning curve… is approximately ten cases” [3]. This is further complicated by the fact that SILS procedures, due to the proximity of the hand tools, are “suited to a single operator, [which] may hinder the training of surgeons in SILS” [2].
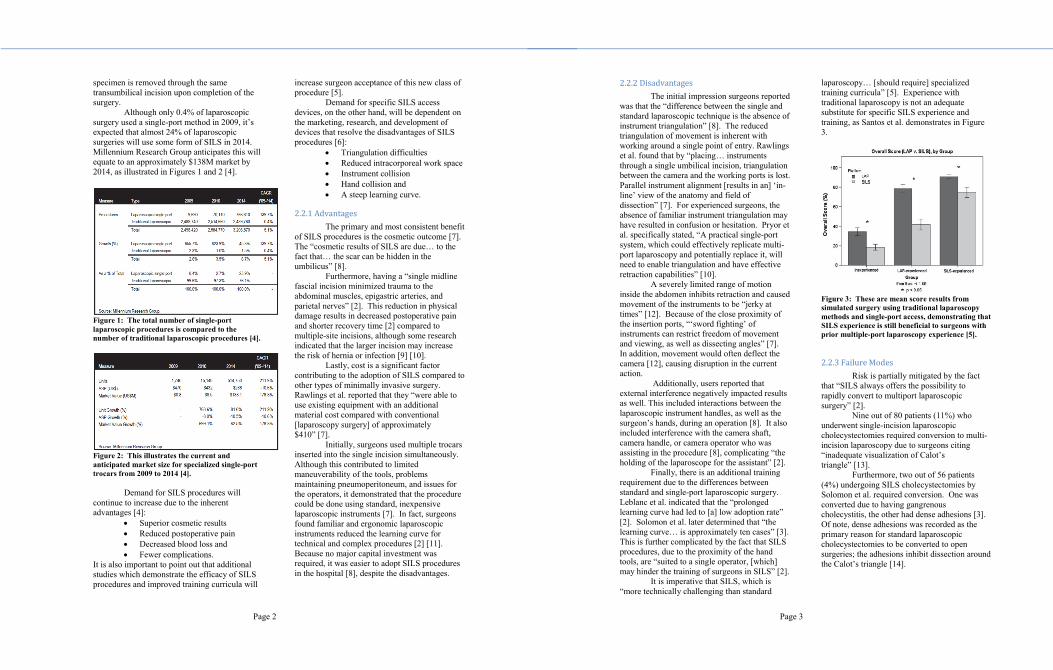
It is imperative that SILS, which is “more technically challenging than standard
laparoscopy… [should require] specialized training curricula” [5]. Experience with traditional laparoscopy is not an adequate substitute for specific SILS experience and training, as Santos et al. demonstrates in Figure 3.
Figure 3: These are mean score results from simulated surgery using traditional laparoscopy methods and single-port access, demonstrating that SILS experience is still beneficial to surgeons with prior multiple-port laparoscopy experience [5].
2.2.3FailureModesRisk is partially mitigated by the fact
that “SILS always offers the possibility to rapidly convert to multiport laparoscopic surgery” [2].
Nine out of 80 patients (11%) who underwent single-incision laparoscopic cholecystectomies required conversion to multi-incision laparoscopy due to surgeons citing “inadequate visualization of Calot’s triangle” [13].
Furthermore, two out of 56 patients (4%) undergoing SILS cholecystectomies by Solomon et al. required conversion. One was converted due to having gangrenous cholecystitis, the other had dense adhesions [3]. Of note, dense adhesions was recorded as the primary reason for standard laparoscopic cholecystectomies to be converted to open surgeries; the adhesions inhibit dissection around the Calot’s triangle [14].

Page 4
3.0Single‐PortAccessDevices New products have been developed to
alleviate the disadvantages of Single-Incision Laparoscopic Surgery (SILS). This is due to the market demand for a product that is cost-effective and safe. As more solutions are introduced, we expect almost 1 in 4 laparoscopic operations will be done using a SILS method – that’s 770,000 SILS procedures – in 2014 [4] and, as a result, will be purchasing and using specific equipment designed and optimized for SILS.
Although doctors such as Iannelli et al. state that we should “rapidly provide surgeons with better instrumentation such as flexible scopes and articulating instruments to overcome the problems” [8] associates with using SILS techniques, other research shows that straight or traditional curved instruments can be effective in surgery and may even be preferable due to the cost of purchasing replacement hand tools, especially more-expensive energy-based dissecting devices [11].
Access devices, however, are required for all laparoscopic procedures. Companies have developed products designed specifically for use in SILS procedures, and have already established products and market share. Covidien, for example, has launched studies to assess the feasibility and safety of performing SILS procedures using their access device which will conclude in 2011 [4].
Currently, advanced devices for single-port surgery are more expensive, costing an average of US$400 compared to the US$55 cost of a traditional access device [4]. This is somewhat mitigated by the need for fewer devices per surgery – one single-port access devices versus three or four trocars for traditional minimally invasive surgery [4].
The bare minimum requirements for a single-port access device are:
Maintains pneumoperitoneum (CO2 pressure) inside the abdominal cavity
Allows visual access into the abdomen, typically using a laparoscope
Permits manipulation of tissue and organs inside the body
using laparoscopic hand tools and
Facilitates removal of an organ or tissue from the abdominal cavity.
3.1CurrentProducts
3.1.1CovidienSILSPortMultipleInstrumentAccessPort
The Covidien SILS Port Multiple Instrument Access Port was launched in April of 2009. It’s a soft, disposable product that is inserted through the umbilicus and into the abdomen wall using forceps. There are two ports for 5mm hand tools and one 12mm port, in addition to the insufflation connector [15].
The Covidien system was the first on the market and current enjoys an 89.5% share of the single-port device market [4].
Figure 4: This illustrates the final insertion of the Covidien SILS device [15].
DeviceAnalysisDisposable devices offer great
convenience due to not having risk of biocontamination.
Boni et al. reported that, while using the Covidien SILS port, “surgeon’s hands often are crossed and the use of articulated instruments… is recommended to obtain a virtual triangulation” [11]. As a result, Covidien’s Reticulator passive articulating hand instrument was used in the majority of SILS procedures in 2009 [4].
Page 5
Covidien offers courses on single-port laparoscopic surgery using their own SILS Port [4].
3.1.2EthiconEndo‐SurgerySSLAccessSystem
Ethicon Endo-Surgery has the largest market share for trocars and access devices [4], giving them an established marketing and sales network for their SSL platform.
The SSL Access System is inserted by hand similar to the Covidien SILS device. However, the SSL is a seal cap and attachment ring, allowing removal and replacement of the access device.
Figure 5: This is a diagram of the Ethicon Endo-Surgery SSL set of devices [16].
DeviceAnalysisAlthough there is no published and
reported case using the Ethicon Endo-Surgery SSL system, certain technical usage aspects can be inferred from the design.
The Seal Cap acts as the cannula, but does not have a long shaft. This permits insertion of bent or rounded hand tools.
The Seal Cap is rotatable separately from the attachment ring without violating the pneumoperitoneum seal [16]. This allows a surgeon to reorient the hand tools during surgery, providing an additional degree of freedom if desired.
The Seal Cap is removable, allowing for specimen removal without having to remove the Retractor.
3.1.3dalimSurgNETOCTO‐PortSystemThe dalimSurgNET OCTO-Port
consists of a wound retractor and a separate “cap”. The cap attaches to maintain the pressure seal, but is also sold in varying configurations to
permit the use of a differing quantity or sizes of instrumentation.
The OCTO-Port has CE certification, but has not been approved by the FDA for use or sale in the United States.
Figure 6: This is the OCTO-Port system, which consists of a wound retractor, attachment ring, and port cap [17].
Figure 7: The seal cap for the OCTO-Port system is interchangable to accomodate varying instrument configurations [17].
DeviceAnalysisThere were no available reports
demonstrating usage of this device. The removable port cap permits
flexibility with instrument usage. The silicon ports are flexible and positioned with varying heights, which will help to reduce external clashing between device handles. The entire cap is rotatable, allowing a surgeon to maximize available triangulation.

Page 6
The port cap also permits extraction of specimens or tissue without removal of the wound retractor.
The dual insufflation connectors permit recycling of CO2, allowing for automatic and constant smoke evacuation when using powered (RF) devices.
3.1.4KARLSTORZEndoconeThe Endocone is a reusable, rigid
device with six 5-mm ports, one 10-mm port, and one 12-mm port. It is only intended to be used with four instruments simultaneously, but the additional ports were intended to provide flexibility with instrument placement.
Figure 8: This is the KARL STORZ Endocone [18].
DeviceAnalysisThe curved edge is intended to ease
initial insertion, but it might cause tissue damage during introduction of the device.
The tall height and crossing cannulas will reduce the external clashing between devices.
KARL STORZ provides specifically designed coaxial curved instruments. Used with the Endocone system, this provides better intra-abdominal triangulation without the need for crossing the surgeon’s hands [11].
3.1.5AppliedMedicalGelPOINTAccessPlatform
Applied Medical’s product was released in October of 2009. It consists of a hard, plastic “cap” – the GelSeal Cap – connected to a plastic chute, the Alexis Wound Retractor, with a ring on the distal end. The cap can be separated and reattached to the Alexis Wound Retractor multiple times. After insertion through the skin, pull the plastic up to tighten it against the abdomen wall and establish your pressure seal.
Figure 9: This is a picture of Applied Medical's GelPOINT product [19].
DeviceAnalysisThe GelPOINT sits a few inches above
the abdomen, increasing internal working diameter [19]. This allows wider placement of the instrument ports, reducing coaxial alignment [20] and allowing greater triangulation between instruments.
“The laterally-placed insufflation port alleviated potential loss of pneumoperitoneum during instrument exchanges, repositioning, and excessive torqueing” [20].
Removal of the GelSeal Cap allows specimen extraction without removal of the entire access device [20].
3.1.6AdvancedSurgicalConceptsTriPortAccessSystem
This product, being marketed and sold by Olympus / Gyrus-ACMI since April of 2009, is unique because it is inserted using a blunt trocar “introducer”. This is necessary due to the lack of rigidity of the distal ring. It has three permanent “gel ports” for two 5-mm and one 12-
Page 7
mm device, in addition to the insufflator connection [21].
Figure 10: This illustrates the correct method necessary to introduce the distal ring to the abdominal cavity [21].
Figure 11: This is a diagram of the ASC TriPort Access System [21].
DeviceAnalysisThe low-profile valves on the flexible
TriPort permit insertion of bent instruments [22], such as the Olympus EndoEye Articulating Video Laparoscope [21].
There is a thermoplastic elastomer covering each valve to maintain the pneumoperitoneum seal intended to permit smooth introduction of instruments [23]. However, Henckens et al. found that it was beneficial to make a small incision into each
valve cover so that instrument introduction does not tear the gel [22].
Maneuverability is inhibited in the gel valves due to the seal. Henckens et al. state, “Lubrification of the ports provide more easy manipulating” [22], while Patel et al. confirm that “[The TriPort] device can be stiff, requiring copious lubrication through surgery” [12].
3.1.7TransEnterixSPIDERThe TransEnterix SPIDER – “Single-
Port Instrument Delivery Extended Research” – is a disposable system that combines the graspers and cannula into a single device. There is a retractable sheath used to cover the distal end during insertion [10]. One of the unique design aspects included is the distal-end center arm, which is designed to add unique articulation angles by moving the pivot close to the distal-end of the device.
The SPIDER provides only two ports for insertion of 5-mm hand tools, but it also permanently provides the two distal-pivoting arms.
Figure 12: This is a diagram and cross-section view of the TransEnterix SPIDER device [10].
DeviceAnalysisThe distal end is controlled by the
gimbal arms. This represents a training necessity for surgeons new to the product.
The insertion tube is only 18mm in diameter, making it the thinnest access device intended specifically for use with SILS. This

Page 8
will minimize fascial insult and muscle damage [10].
The primary advantage of this device is to “allow surgeons to… [use] a combination of proprietary flexible instruments and common ‘off-the-shelf’ laparoscopic instruments” [10].
3.1.8SurgiquestAirSealTrocarThe Surgiquest AirSeal uses a constant
influx of directed CO2 to maintain pneumoperitoneum without physically sealing the entry port.
In 2009, Surgiquest entered an agreement with Intuitive Medical Devices to develop a disposable AirSeal-type device for use with the DaVinci Surgical Robot.
Figure 13: The AirSeal forces air into the cannula, maintaining relatively constant pressure and air circulation [24].
Figure 14: The open nature of the device permits insertion of multiple tools simultaneously [24].
DeviceAnalysisThe lack of a physical seal on the
cannula permits insertion and removal of multiple instruments or cameras [24]. Working from a single opening with no motion
restrictions results in a “learning curve [that] was short and easily surmountable” [25].
Furthermore, the unsealed opening permits “additional adjuncts, such as [a] hemostatic sponge or compressive tampon, could be placed into and withdrawn from the peritoneal cavity” [25]. This is the only device discussed which allows withdrawal of a specimen without deflating and re-establishing the pressure cavity.
However, Leroy et al. also reported that he experienced instrument crowding at the atrium and ineffective retraction with three devices inserted due to their proximity. They were able to partially overcome this issue by using micro-instruments of differing lengths and curvatures [25].
4.0DeviceDesignProposal It is possible to design an access device
that is superior to the products already on the market. Rapid design and prototyping will lead to 510(k) approval for our product, and previously-established insurance codes will ensure acceptance of our superior device into the market. A structured design exercise can be done to maximize the advantages of our new design while minimizing research and development costs.
Furthermore, specific design considerations can be made to accommodate other products we market. This synergistic approach will demonstrate the quality of our products as a platform for this market which will grow almost 180% in the next four years [4].
4.1ProposedSolutions
4.1.1VisualizationandTriangulationResearchers agreed that a small-
diameter laparoscope with a 30-degree angular or flexible tip would improve visualization and performance [2]. A camera with a 45-degree angle “allows the end of the scope to be placed farther above the working instruments inside the abdomen, to reduce intracorporeal collision” [6]. A scope with a flexible tip would “reduce clashing of the [other] instruments with the camera” [5].
Page 9
Our micro laparoscopes with 45-degree viewing angle would be ideal for this circumstance.
Placement of the 5-mm access ports may impact the ability to visualize the Calot’s triangle during a cholecystectomy procedure.
4.1.2InternalRetractionandRangeofMotionUsing “instruments of different length
and low profile ports improved the degree of freedom” [8]. Furthermore, reducing the size of the instruments is important to minimize interference between devices internally.
Although articulating instruments would seem to improve dissection angles, Marietti et al. described “articulating instruments [as] difficult to manipulate” [6], implying the necessity for additional training or experience. Crossing of instruments facilitated internal triangulation by allowing greater retraction and tension ranges [12].
Figure 15: This illustration demonstrates the internal crossing of hand tools while using a GelPOINT single-port access device [20].
“Innovative instrumentation may allow
surgeons to more closely match their [traditional Laparoscopy] performance while using a SILS approach” [5]. Henckens et al. suggest using devices with two bends: one on the intraperitoneal end and one on the handle. This would increase the range of motion to improve retraction while reducing instrument interference [22].
One procedure done by Marietti et al. even found that using our
alligator grasper inserted percutaneously in the right subcostal region significantly aided in retraction without causing additional scarring [6].
Low-profile, flexible access ports will allow the surgeon more flexibility when manipulating the hand tools.
The access device should reduce internal interference by maximizing the distance between access ports.
Small-diameter, straight tools of varying length will encourage adoption of the device by surgeons experienced with current laparoscopic tools.
The device must be able to accept curved or other non-straight hand tools.
There may be synergy with our line of micro-laparoscopic tools because it maintains the primary advantage of SILS surgery (superior cosmetic results).
4.1.3ExternalInterferenceAgrawal et al. suggest using standard
tools and bariatric tools simultaneously to reduce external clashing [23]. Marietti et al. confirmed that the increased length of the bariatric scope helps to eliminate the camera holder from extracorporeal collision [6].
Others found that a “smaller diameter laparoscope with an angular tip and an incorporated light source” [2] or a “laparoscopic camera-scope combination with an in-line light cord and a low-profile camera head… would cause less tangling externally and yield more working space” [8].
Marietti et al. also commented that “hand collision was minimized if the instruments were of varying lengths” [6]. Collision between device handles led to an inhibited intracorporeal space.
Using our Bariatric laparoscope will reduce external clashing between operators and assistants.
A camera with an integrated light source would reduce external tangling.

Page 10
Placement of the access cannulas should be oriented outwardly from the center to reduce external interference between devices.
4.1.4SurgicalandOperationalFailureBecause SILS procedures involve a
single access port with larger size, there is “added risk of infection, delayed healing, and herniation” [10] compared to traditional laparoscopic surgery. Using low-profile trocars result in smaller fascial defects [4], and reducing the size of the initial incision from 20-mm will reduce the chance of port hernia [9].
The access device must be usable with a 15-mm transumbilical incision.
4.1.5TrainingandLearningCurveCurrently, “SILS is not a standard
component of the widely adopted FLS curriculum, nor are there any ACGME requirements for SILS training” [5]. As a result, the burden of training and educating surgeons lies on the manufacturers of the devices.
4.2FunctionalSpecifications For sake of brevity, Table 1 is a partial
list of relevant functional specifications. A complete analysis should be done before development is initiated. Table 1 is an abbreviate example of the functional specifications necessary for this device.
Defined User Needs
(DUN) Design Input (DI)
Regulatory Compliance
FDA FDA Safety & Efficacy Requirements
ISO ISO Quality Requirements
Device Effectiveness
The operator must be able to use the device to perform single-port
laparoscopic surgery
The device must be insertable into a 15-mm
abdominal incision
Device must maintain pneumoperitoneum
throughout procedure
Device must have port(s) for insufflator attachment
Device must seal and hold pressure up to 25 psi
Seal must hold during insertion and removal of
hand instruments
Access ports must facilitate use of up one, two, or three laparoscopic instruments
Device must allow usage of a single hand tool
Device must allow simultaneous usage of two
hand tools
Device must allow simultaneous usage of
three hand tools
Device must maximize intracorporeal movement
range
Placement of access ports must be at least 15mm from the center of the
device
Access ports must allow internal crossing of tools
Device must maximize external movement range
Access ports must be directed outwardly from
center
Surgical Safety
Device must be safe for patient and surgeon contact
Device must meet biocompatibility risk
requirements
Device must not cause excessive tissue trauma
during use
Device must be free of sharp edges
Device must be reasonably sized for insertion into 15-
mm incision
System Compatibility
Device should permit insertion and removal of
other commonly available products
Device must be compatible with our laparoscope
Device must be compatible with 3.0-mm straight
laparoscopic instruments
Device must be compatible with 5.0-mm straight
laparoscopic instruments
Device must be compatible with 5.0-mm bent
laparoscopic instruments
Table 1: This is an abbreviated list of functional requirements for a single-port access device.
Page 11
After the functional specifications are established, we can utilize internal testing (Verification) to ensure we have met our requirements or to acquire additional data necessary to modify our requirements.
Once we have completed our internal verification, we can invite surgeons to our site to provide us with user feedback (Validation).
4.3RegulatoryAspects We will be able to obtain regulatory
approval by means of 510(k) for this Class II device.
Insurance reimbursement codes for single-access-port devices have already been established by competitive products.
4.4ManufacturingProcesses Manufacturing will be dependent on
final product specifications. However, assuming that the completed product is a single-use polymeric device, we can hypothesize on some of the manufacturing concerns we may encounter.
If possible, there are manufacturing and cost advantages to developing our device as a single, moldable plastic device. If necessary, way may consider a two-piece system consisting of a disposable section and a reusable cap.
We may be using some form of compression molding for production of our device. It will be of utmost importance to identify and acquire a biocompatible material that meets all of our Functional Requirements, including storage, packaging, and sterilization. Quality is of utmost importance for maintaining or establishing our competitive advantage.
5.0Conclusion The information presented clearly
establishes the growing market size for Single-Port Laparoscopic Surgery: the market is expected to grow 179% to US$268 million by 2014 [4]. Furthermore, synergy with hand devices will permit us to increase our market
share in that field simultaneously with increased adoption for our SILS products.
The adoption of Single-Port Laparoscopy in the operating room is dependent on resolving the disadvantages associated with these procedures. These disadvantages can be partially or completely rectified through the design of innovative devices:
Limited movement range due to intracorporeal collision and
Limited movement range due to external collision
Reduced or altered visual acuity due to reduced movement range of the laparoscopic camera.
Development of solutions and products must consider the user’s actions and ergonomic requirements during development. This includes other people in the operating room, such as the camera-wielding assistant, in addition to the surgeon.
Additionally, many of the problems identified by surgeons can be resolved through the application of current products on the market.
Possible solutions include: Curved or shaped laparoscopic
instruments Thinner hand tools Hand tools with varied length Smaller handles on hand tools Laparoscopic cameras with angled
tips and viewing angles Laparoscopic cameras with
articulating viewing windows Flexible access ports that remove
fewer degrees of freedom Finally, it’s important to recognize the
need and advantage of SILS-specific training programs. Covidien, for example, has established a 90% market share for their SILS device partially due to their established weekend training courses being offered to surgeons interested in observing and learning optimal methods and procedures when using the Covidien SILS Access Port.
Training programs combining our superior and well-established camera technology with a complimentary single-port access device can establish our share of the Single-Port Laparoscopic Surgery market.

Page 12
WorksCited
[1] G Navarra, E Pozza, S Occhionorelli, P Carcoforo, and I Donini, "One-wound Laparoscopic Cholecystectomy," British Journal of Surgery, no. 84, p. 695, 1997.
[2] F Leblanc et al., "Single Incision Laparoscopic Colectomy: TechnicalAspects, Feasibility, and Expected Benefits," Diagnostic and Therapeutic Endoscopy, vol. 2010, 2010.
[3] Daniel Solomon, Robert L Bell, and Andrew J Duffy, "Single-port Cholecystectomy: Small Scar, Short Learning Curve," Surgical Endoscopy, April 2010.
[4] Millennium Research Group, "US Markets for Laparoscopic Devices," Toronto, 2010.
[5] Byron F Santos, Daniel Enter, Nathaniel J Soper, and Eric S Hungness, "Single-incision Laparoscopic Surgery (SILS(tm)) Versus Standard Laparoscopic Surgery: A Comparison of Performance Using a Surgical Simulator," Surgical Endoscopy, June 2010.
[6] Sarah Marietti, Marvalyn DeCambre, Timothy Fairbanks, Karen Kling, and George Chiang, "Early Experience with Laparoendoscopic Single-Site Surgery in the Pediatric Urology Patient Population," Journal of Endourology, pp. 1321-4, 2010.
[7] Arthur Rawlings et al., "Single-Incision Laparoscopic Cholecystectomy: Initial Experience with Critical View of Safety Dissection and Routine Intraoperative Cholangiography," Journal of the American College of Surgeons, pp. 1-7, 2010.
[8] Antonio Iannelli, Anne Sophie Schneck, Giovanna Ioia, and Jean Gugenheim, "Single Incision Laparoscopic Surgery Cholecystectomy A Preliminary Experience," Surgical Laparoscopy Endoscopy & Percutaneous Techniques, pp. e89-e81, 2010.
[9] Kai He, Hao Chen, Rui Ding, Rong Hua, and Qiyuan Yao, "Single Incision Laparoscopic Totally Extraperitoneal Inguinal HerniaRepair," Hernia, 2010.
[10] Aurora D Pryor, John R Tushar, and Louis
R DiBernardo, "Single-Port Cholecystectomy With the TransEnterix SPIDER: Simple and Safe," Surgical Endoscopy, no. 24, pp. 917-923, 2010.
[11] Luigi Boni et al., "Single Incision Laparoscopic Right Colectomy," Surgical Endoscopy, May 2010.
[12] Ameet G Patel et al., "Single-Incision Laparoscopic Left Lateral Segmentectomy of Colorectal Liver Metastasis," Surgical Endoscopy, July 2010.
[13] Chris Edwards et al., "Single-Incision Laparoscopic Cholecystectomy is Feasible: Intial Experience with 80 Cases," Surgical Endoscopy, 2009.
[14] Waseem Memon, Tariq Wahab Khanzada, Abdul Samad, and M Hussain Laghari, "Laparoscopic Cholecystectomy: Conversion Rate and its Causes at Isra University Hospital, Hyderabad," Isra University Hospital, Hyderabad, Surgical Report 2008.
[15] Homero Rivas, SILS(TM) Port Insertion. Norwalk: Covidien AG, 2009.
[16] Ethicon Endo-Surgery, Inc., Introducing the SSL Access System from Ethicon Endo-Surgery., 2009.
[17] dalimSurgNET. octo-port. [Online]. http://www.octo-port.com/
[18] KARL STORZ. (2010, August) CUSCHIERI ENDOCONE. [Online]. http://www.karlstorz.com/cps/rde/xchg/SID-D7194388-20722622/karlstorz-en/hs.xsl/8878.htm
[19] Applied Medical, GelPOINT Advanced Access Platform., 2010.
[20] Madhu Ragupathi, Diego I Ramos-Valadez, Rodrigo Pedraza, and Eric M Haas, "Robotic-Assisted Single-Incision Laparoscopic Partial Cecectomy," The International Journal of Medical Robotics and Computer Assisted Surgery, 2010.
Page 13
[21] Advanced Surgical Concepts. (2010) Triport Instructions For Use. [Online]. http://www.advancedsurgical.ie/TriPort/Default.166.html
[22] Tom Henckens et al., "Laparoendoscopic Single-Site Gastrectomy for a Gastric GIST Using Double-Bended Instruments," Journal of Laparoendoscopic & Advanced Surgical Techniques, 2010.
[23] Sanjay Agrawal, Anna Slovick, and Yuen Soon, "Single-Port Laparoscopy for the Drainage of Abdominal Infected Fluid Collections in Children, With the TriPort System: Initial Experience of 2 Cases," Surgical Innovation, 2010.
[24] SurgiQuest, Inc. AirSeal for Laparoscopy. [Online]. http://surgiquest.com/?q=node/49
[25] Joel Leroy, Ronan A Cahill, Silvana Peretta, and Jacques Marescaux, "Single Port Sigmoidectomy in an Experimental Model With Survival," Surgical Innovation, pp. 260-5, 2008.
[26] United States Department of Health & Human Services, Food and Drug Administration, Laparoscopic Trocar Injuries: A Report From a U.S. Food and Drug Administration (FDA) Center for Devices and Radiological Health (CDRH) Systematic Technology Assessment of Medical Products (STAMP) Committee. Washington: GPO, 2003.
[27] TransEnterix. (2010) The SPIDER(R) Surgical System. [Online]. http://spidersurgery.com/
Related Documents











