Virtual Geometry and Three- Virtual Geometry and Three- dimensional mapping system: dimensional mapping system: how is really how is really useful for ablate AF ? useful for ablate AF ? Stefano Nardi MD, PhD “ “ SANTA MARIA” GENERAL HOSPITAL - TERNI SANTA MARIA” GENERAL HOSPITAL - TERNI THORACIC SURGERY AND CARDIOVASCULAR DEPARTEMENT ARRHYTHMI THORACIC SURGERY AND CARDIOVASCULAR DEPARTEMENT ARRHYTHMI ELECTROPHYSIOLOGIC CENTER ELECTROPHYSIOLOGIC CENTER AND CARDIAC PACING UNIT AND CARDIAC PACING UNIT Progress in Progress in Clinical Pacing ‘06 Clinical Pacing ‘06

2006 roma, progress in clinica pacing 2006. i sistemi di mappaggio 3 d nel trattamento della fibrillazione atriale
Aug 12, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Virtual Geometry and Three-Virtual Geometry and Three-dimensional mapping system: how dimensional mapping system: how is really useful for ablate is really useful for ablate AF ?AF ? Stefano Nardi MD, PhD
“ “SANTA MARIA” GENERAL HOSPITAL - TERNISANTA MARIA” GENERAL HOSPITAL - TERNI THORACIC SURGERY AND THORACIC SURGERY AND
CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOGIC CARDIOVASCULAR DEPARTEMENT ARRHYTHMIA ELECTROPHYSIOLOGIC CENTER AND CARDIAC PACING UNIT CENTER AND CARDIAC PACING UNIT
Progress in Progress in Clinical Pacing ‘06Clinical Pacing ‘06

RF
Atrial Fibrillation MechanismsAtrial Fibrillation Mechanisms
• PVs as TRIGGER and PERPETUATORS
• SUBSTRATE with CRITICAL MASS
• GANGLIONIC PLEXI affecting vagal innervation
• ROTOR sites critical to the maintenance of reentry
How does it work?

Pulmonary Vein triggers
Haissaguerre, NEJM ‘’98
Firing from PVs
RF

Role Of Pulmonary Veins in AFRole Of Pulmonary Veins in AF
Dominant source of triggers Dominant source of triggers
Role in the maintenanceRole in the maintenance• Sustained focal firingSustained focal firing (Ja(Jaïïs)s)
• Intermittent focal firing Intermittent focal firing (O’Donnell, Kumagai, Oral)(O’Donnell, Kumagai, Oral)
• Reentry Reentry (Arora, Hocini, Wu, Mansour, Jais)(Arora, Hocini, Wu, Mansour, Jais)
IIIIIIIIIIIIVIVI
MapMap
PV1-2PV1-2
PV10-1PV10-1
CSCS

Different TechnologiesDifferent TechnologiesMappingMapping• Point by pointPoint by point
• LassoLasso• SpiralSpiral• BasketBasket
TrackingTracking• XrayXray
• CARTOCARTO• LocaLisaLocaLisa• NavXNavX• RPMRPM
• ICEICE
AblationAblation• ConventionalConventional
• 8 mm tip8 mm tip• Irrigated tipIrrigated tip• InvestigationalInvestigational(balloon, cryo...)(balloon, cryo...)
- Framework for ablationFramework for ablation
- Mapping guidanceMapping guidance
- Anatomic localizationAnatomic localization
- Tagging of ablation - Tagging of ablation sitessites
- Determine Determine catheter contactcatheter contact
- Improved Improved efficiency of efficiency of power deliverypower delivery
How we can approach to AF ablation ?

Different Approach

Electro-physiologic ApproachSOCA of all 4 veins

Pulmonary vein anatomy the first challenge
Left common trunk 3 right lower veins
Normal

• Inadeguate Mapping of complex anatomical substrates
IIIIII
PV 1-2
PV 10-1
V1
CSP
Limitation of Limitation of
EP EP SOCASOCA
• PVs potential that run along the LA posterior wall could be
missed with a purely EP approach
• Too complex design for transection between anatomical structures

Limitation of EP SOCALimitation of EP SOCA
• FLUOROSCOPY has a limited use (poor soft-tissue resolution and relatively high exposure to ionizing radiation).
• SUCCESS RATE depends on the ability to place ablation lesions at predefined
anatomic targets site, and the identification of all PVs fascicule could be challenging especial in complex anatomy.
3 right lower veins Left common trunk

Limitations of EP criteria
• Repeated the procedure provides a significant clinical benefit and suggest that
if permanent PVI is an important “END POINT” a different strategies may be required to improve long-term efficacy.
• Recovery of conduction after a previously successful PVI could be due to a “SUB-OPTIMAL” identification of all PVs pot.

Wide complex and articulate anatomy.Irregular myocardial sleevers Miocardial fibres extend from LA to PVs (HO, J CV El. ‘99; HO, Heart ‘01; SAITO, J CV El. ‘00; Moubarak, P. Cl. El. ‘00).
Irregular disposition of fibres (Circular, Longitudinal, Oblique, Spiral)
Prevalent extension into Upper PVs
Hocini M, Card. Res ’02 Hocini M, Circulation ‘02
The Antral Zonethe second challenge

• Fractioned EGM, with slow conduction and heterogeneous repolarization represent the “IDEAL” substrate for reentry mechanism (Hocini, Circulation `02; Arora, Circulation `03)
• Intense periodic electrical activity in AF with high frequency” electric potential able to create stable micro-reentry around the junction (Mandapati, Circulation `00)
• The PVs antrum could be functionally considered as a “BROAD BAND”
• Possible Arrhythmogenic Nature due to EMBRIONAL origin
The Antral Zonea 2nd challenge

3D mapping system in AFib 3D mapping system in AFib What is really usefull?

What is really usefull?3D mapping system in AFib3D mapping system in AFib
RPV
LPV
Cutaneous patches and conventional catheter
for tracking (NavX)
Superimposed EM field With a dedicate mapping
catheter (CARTO)

Anatomical Approach Anatomical Approach CLAACLAA
• 251 Patients• 54±12 min of RF
End Point: (75%)• PVP < 0.1 mV• Delay > 30 ms
Success off AADs:• 148/179 PaAF (83%)• 40/72 PeAF (55%)Pappone, Circulation ‘01Pappone, Circulation ‘01

Anatomical CLAA: Incomplete PVI in ~ 60%Anatomical CLAA: Incomplete PVI in ~ 60%
70 ms70 ms
IIIIIIIIIIIIV1V1
PV1-2PV1-2
PV10-1PV10-1
CSDCSD
CSPCSP

LIMITATIONS
Ernst, JACC ‘03Ernst, JACC ‘03
Complete LesionsComplete Lesions
A – 5% A – 5% B – 21% B – 21% C C – 50% – 50% D - 58-65% D - 58-65%OutcomeOutcome
• Complete lesion 74% Complete lesion 74% arrhythmia free w/o AADsarrhythmia free w/o AADs
• Incomplete lesion – Incomplete lesion – almost almost all recurrent all recurrent arrhythmiaarrhythmia
Anatomical Approach Anatomical Approach CLAACLAA

Challenge of CLAAChallenge of CLAA• Complete linear lesions are
analogous to surgical incisions
• They are challenging to achieve (with increased procedural risk)
• Incomplete linear lesions are pro-arrhythmic

Limitation of CLAA• Which substrate is “real target” for AF ablation ?• Almost 60% of pts no PVI • Which is the % success rate ?• It’s so effective in PeAF as PaAF ?• No PV stenosis• Extensive LA damage• LA flutters more common (20%)
V1V1
RF probeRF probe(ostial)(ostial)
LIPV 1-2LIPV 1-2
2-32-3
3-43-4
4-54-5
5-65-6
6-76-7
7-87-8
8-98-9
9-109-10
10-110-1
LA appLA app
Discrete Residual PV Fascicle - Producing Discrete Residual PV Fascicle - Producing ArrhythmiaArrhythmia

Evolution over the time3D mapping system in AFib3D mapping system in AFib

Bazaz & SchwartzmanBazaz & Schwartzman
3D mapping system in AFib3D mapping system in AFib

How can we do a “ good mapping “ ? Importing the CT/MRI 3D Model
Digital Image Fusion
CT/MRI Scanner
DICOM 3 Slice Data
Worstation
Segmented 3D ModelSegmentation Module
User Interface

Virtual Reality Today

Esophageal contiguity with LA3D mapping system in AFib3D mapping system in AFib
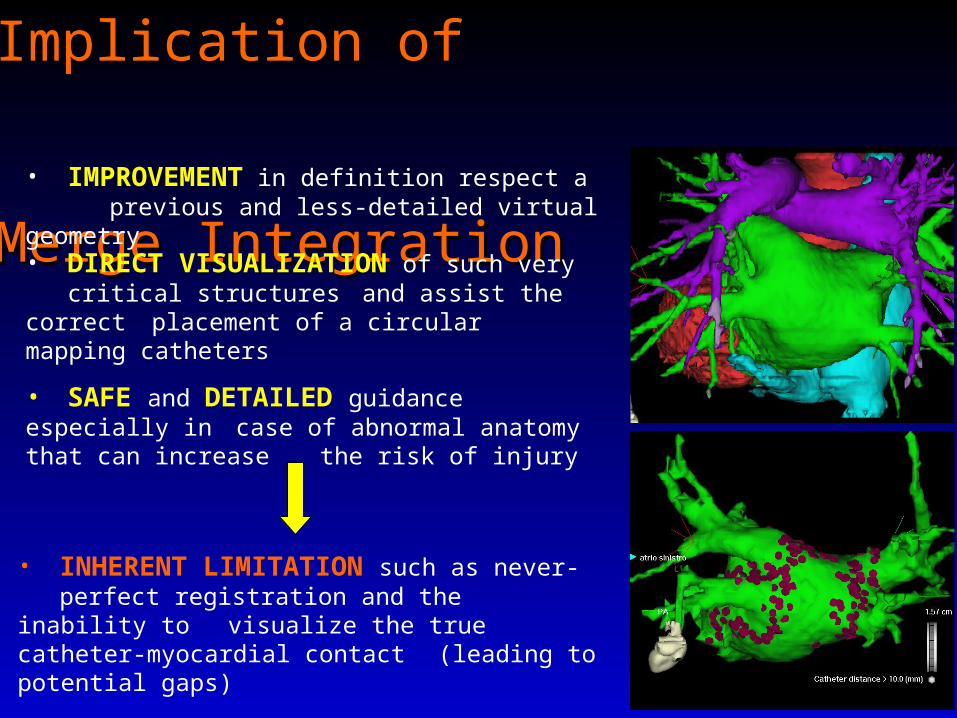
Implication of Implication of
Merge IntegrationMerge Integration
• SAFE and DETAILED guidance especially in case of abnormal anatomy that can increase the risk of injury
• DIRECT VISUALIZATION of such very critical structuresand assist the correct
placement of a circular mapping catheters
• IMPROVEMENT in definition respect a previous and less-detailed virtual geometry
• INHERENT LIMITATION such as never-perfect registration and the inability to
visualize the true catheter-myocardial contact (leading to potential gaps)

• POSITION ERROR of the EM location system.
• SEGMENTATION process of 3D imaging and EXTRACTION is dependent on CT quality and on individual threshold determination (additional source of error).
• The selected REGISTRATION METHOD significantly affects the resulting accuracy
Differences in cardiac anatomy or contractility, as well as respiratory, cardiac,
and body motion, are only partially compensated
Implication of Implication of
Merge IntegrationMerge Integration

Limitation of Limitation of Virtual Geometry Virtual Geometry“ STRETCHING EFFECT ”
• Possible loose of correspondence between RF displayed and the ”TARGET POINT”
• The tip of catheter can get “hung up” on the trabecular sleevers and a further deflection
could stretch and can “pull down” the wall. Moving the tip position on the map to the “next spot” the tip could be still in contact with the same point. When the tip is freed, the elasticity moves the sleevers “back up” resulting in a gap between the last ablation site and the current “next spot” indicated by the system.
• SEVERAL GAPS could be found within the ablation lines, ranging from 2 to 4 mm, when we explore the “encircling line”.

• The lesion of RF are displayed at Epicardium whereas the RF lesions are created at the endocardium surface (the epicardial projection point are used to evaluate position error).
Limitation of Limitation of Virtual Geometry Virtual Geometry“ SOURCE of ERRORS ”
• The SEGMENTATION PROCESS is depended and could be negatively affected
by some intramiocardial markers (such as PM)
• The CT scan or MRI are pre-acquired (STATIC IMAGE) and may not accurately reflect the anatomic characteristic in that moment (volume changed by irrigated cooled tip)

Limitation of Limitation of Virtual Geometry Virtual Geometry
How we can do to reduce
the source of error ?
• CT scan/MRI, the endocardial point recording tagging with the MAP at endocardial surface
and the Catheter Icon displayed should be linked at the same phase of the cardiac cycle.
• Performing the image registrations combining two separate internal registration methods
(landmark and surface registrations) to compensate for each other’s intrinsic error.

Does one ablation schema fit all AF
patients?

• 422 pts with symptomatic PaAF and PeAF referred to us between July ‘04 and September ’06. CA performed in
145/422 pts (34%).
TERNI RegistryTERNI Registry
• At least one MONTHLY episode of Persistent symptomatic AF
• At least ONE WEEKLY episode of PaAF or PeAF
• At least Two or More AADs unable to control symptoms
• Age >75 yrs• Contraindications to ACT• Congestive HF• NYHA class III or IV• LVEF ≤35% • LA diameter ≥55mm• CARDIAC THROMBUS• Life expectancy <1 yr• CCH surgery <3 mo or
PROSTHETIC valves
Inclusion criteriaInclusion criteria Exclusion criteriaExclusion criteria

Procedure (min): 14826 14424 151 29
Fluoroscopy (min): 5917 5816
6619 Mapping (min): 158
139 184 Nr. Pulses of RF:
6216 6017 6519
RESULTSRESULTS Global Pz.in SR Pz. in AF
TERNI RegistryTERNI Registry
629 VP treated (145 pts)
Acute Complete Acute Complete BlockBlock
558 VP (89%)558 VP (89%)
Incomplete Incomplete BlockBlock
71 VP (11%)71 VP (11%)

• After a mean FU Overall FREEDOM FROM AF (both PaAF and PeAF) was 60% (69% and 48%), w/o AADs and 72% (80% and 55%) with previous ineffective AADs.
Clinical OUTCOME
• The Kaplan-Meier statistical analysis probability of freedom from arrhythmia was maximal at 9 months
TERNI RegistryTERNI Registry
• Among UNIVARIATE predictors, the variables of age, sex, duration and frequency of AF, LVEF, LA size and structural heart disease, this approach revealed that an increased LA SIZE >50mm is an indipendet
predictor of AF recurrence

Conclusions (1)Conclusions (1)
• Conventional EP mapping is not always a really appropriate strategies for AF ablation because it provides very limited understanding of these complex arrhythmias which are highly variable from one pt to the other.
• The main drawback of a pure EP approach is that the identification of all putative “end point” could be extremely difficult to achieve.
• Viceversa, a pure EA approach, with a CLAA fashion could not to be the treatment of choice, because PVs are still able to conduct into LA.

Conclusions (2)Conclusions (2)
• The implemented use of virtual geometry and a combined approach of EP with EA criteria is able to allow
a realistic reconstruction of the chamber of interest
• An individually tailored approach is needed
• A merge integration could fulfill an important clinical demand for detailed anatomic guidance, especially in case
of abnormal anatomy, condition that can increase the risk of damage if not realized.

• Inherent limitations can lead to a potential potential source of error, however this represents a significant improvement respect to previous less-detailed reconstructed 3D maps
• A combined approach may be useful in the treatment of pts with AF, where CA Rx is primarily both EP and anatomically based.
Conclusions (3)Conclusions (3)

What is success?
• Complete freedom of AF, off drug RX?• No symptoms, but drug Rx required?• Dramatic decrease in symptoms, but
AADs still required?• QoL• How do we detect asymptomatic
episodes?• Anticoagulation ………………...?
QUESTIONSQUESTIONS
Related Documents











