2015-B Event N Ques Imp PT – Resu uppe Spe BactiReg3 Notes stions or comm ortant Info –Central Upd 90% of pa General in Event Nam Single SA Data subm ult form and er right corner Results ca paper resu The Repo mailed to Please not your data ecific Samp Mo 50 50 50 52 52 52 50 ments should ormation: dates: Enhan articipants are nstructions ar me now appe AVE function mission report Report Deliv r of your PT C an be entered ult forms will ort Delivery op facilities that tify us at PTS entry or repo ple Notes: odule 90 Gram Sta 30 Bacteriol 40 Bacteriol 50 Throat / U 60 Throat / U 70 Urine Cu 80 Enteric P Mark Yo Re-en 2 Ship d be directed t ncements will e reporting re re located onli ars on your h with results e t now contain very options: Central home online or by not be sent w ption is set to t are not set u Service@slh.w ort settings. ain (GS) ogy Compreh ogy Limited ( Urine Bacterio Urine Bacterio lture (UC) athogens Cul our Calend nrollment l re-e P 2015-BactiR pment Date to Amanda W continue to b sults online a ine at www.w home page nex editable until ns attestation : The setting page. fax. Online d with your PT o Email attach up to receive e wisc.edu or u hensive (MCP (MCL) ology (TU) ology Limited lture (NP) dars Now! N letters hav enroll to rec Page 1 of 21 2601 Agricult Reg3 Even : Septemb Weiss at 800-4 be added. at PT-Central. wslhpt.org . xt to result en the due date. signature. s for your fac data entry is en sample shipm hment, Email emails. se the “Conta P) d (TUL) Next Event ve been ma ceive sam ture Drive Mad nt Notes ber 14, 2015 62-5261 x51 . Thank you! ntry. . cility are note ncouraged. I ments. notification, act Us” option t Ships: F ailed. Parti ples in 201 dison, WI 53718 5 or amanda.w ed in the demo If the data ent or Paper. Pap n on the webs Pag 3 4 - 9 4 - 9 10 - 10 - 14 - 19- ebruary 15 cipants MU 16! (800) 462-526 w[email protected]s ographic infor try option is s per reports wi site if you wis ge(s) 9 9 - 13 - 13 -18 21 5, 2016 UST www.wslhpt.o 1 (608) 265-11 sc.edu. rmation in the set to “web,” ill only be sh to change rg 11 e

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2015-BEvent N
Ques Imp PT –
Resuuppe
Spe
BactiReg3 Notes
stions or comm
ortant Info
–Central Upd 90% of pa General in Event Nam Single SA Data subm
ult form and er right corner Results ca
paper resu The Repo
mailed to Please not
your data
ecific Samp
Mo
50
50
50
52
52
52
50
ments should
ormation:
dates: Enhanarticipants arenstructions arme now appe
AVE function mission report
Report Delivr of your PT Can be entered ult forms willort Delivery op
facilities thattify us at PTSentry or repo
ple Notes:
odule
90 Gram Sta
30 Bacteriol
40 Bacteriol
50 Throat / U
60 Throat / U
70 Urine Cu
80 Enteric P
Mark Yo
Re-en
2Ship
d be directed t
ncements will e reporting rere located onliars on your hwith results e
t now contain
very options:Central home online or by not be sent wption is set tot are not set [email protected] settings.
ain (GS)
ogy Compreh
ogy Limited (
Urine Bacterio
Urine Bacterio
lture (UC)
athogens Cul
our Calend
nrollment lre-e
P
2015-BactiRpment Date
to Amanda W
continue to bsults online aine at www.w
home page nexeditable until ns attestation
: The settingpage. fax. Online d
with your PT o Email attachup to receive ewisc.edu or u
hensive (MCP
(MCL)
ology (TU)
ology Limited
lture (NP)
dars Now! N
letters havenroll to rec
Page 1 of 21
2601 Agricult
Reg3 Even: Septemb
Weiss at 800-4
be added. at PT-Central.wslhpt.org . xt to result enthe due date.signature.
s for your fac
data entry is ensample shipm
hment, Email emails. se the “Conta
P)
d (TUL)
Next Event
ve been maceive sam
ture Drive Mad
nt Notes ber 14, 2015
62-5261 x51
. Thank you!
ntry. .
cility are note
ncouraged. Iments.
notification,
act Us” option
t Ships: F
ailed. Partiples in 201
dison, WI 53718
5
or amanda.w
ed in the demo
If the data ent
or Paper. Pap
n on the webs
Pag
3
4 - 9
4 - 9
10 -
10 -
14 -
19-
ebruary 15
cipants MU16!
(800) 462-526
ographic infor
try option is s
per reports wi
site if you wis
ge(s)
9
9
- 13
- 13
-18
21
5, 2016
UST
www.wslhpt.o
1 (608) 265-11
sc.edu.
rmation in the
set to “web,”
ill only be
sh to change
rg
11
e
Page 2 of 21 2015-BactiReg3 Event Notes
Please review your reports carefully before filing with the rest of your PT records. Documentation of all decisions and actions concerning incorrect responses should be maintained with your event reports to satisfy regulatory requirements. After trouble-shooting or corrective actions are completed and documented, all reports should be reviewed, signed/initialed by the appropriate personnel, and filed with your proficiency testing records to document your participation. Event Specific Information:
Module 5000 (Bacterial Antigens—for meningitis)
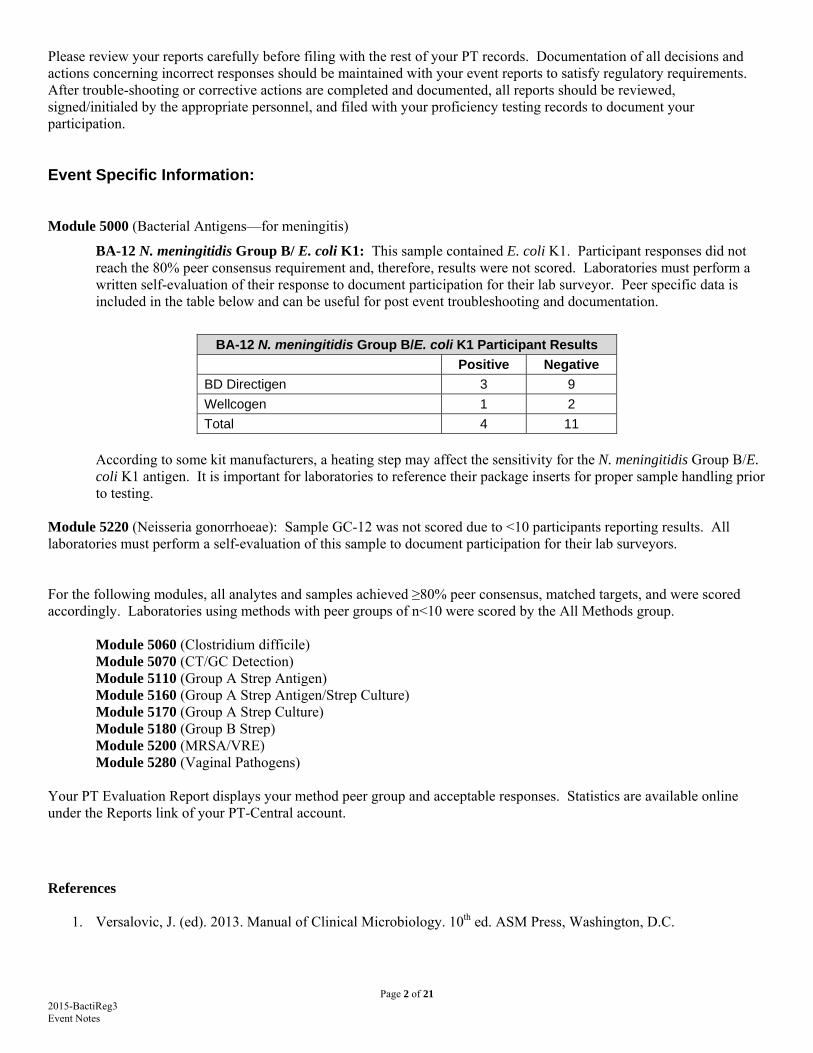
BA-12 N. meningitidis Group B/ E. coli K1: This sample contained E. coli K1. Participant responses did not reach the 80% peer consensus requirement and, therefore, results were not scored. Laboratories must perform a written self-evaluation of their response to document participation for their lab surveyor. Peer specific data is included in the table below and can be useful for post event troubleshooting and documentation.
BA-12 N. meningitidis Group B/E. coli K1 Participant Results
Positive Negative
BD Directigen 3 9
Wellcogen 1 2
Total 4 11
According to some kit manufacturers, a heating step may affect the sensitivity for the N. meningitidis Group B/E. coli K1 antigen. It is important for laboratories to reference their package inserts for proper sample handling prior to testing.
Module 5220 (Neisseria gonorrhoeae): Sample GC-12 was not scored due to <10 participants reporting results. All laboratories must perform a self-evaluation of this sample to document participation for their lab surveyors. For the following modules, all analytes and samples achieved ≥80% peer consensus, matched targets, and were scored accordingly. Laboratories using methods with peer groups of n<10 were scored by the All Methods group.
Module 5060 (Clostridium difficile) Module 5070 (CT/GC Detection) Module 5110 (Group A Strep Antigen) Module 5160 (Group A Strep Antigen/Strep Culture) Module 5170 (Group A Strep Culture) Module 5180 (Group B Strep) Module 5200 (MRSA/VRE) Module 5280 (Vaginal Pathogens) Your PT Evaluation Report displays your method peer group and acceptable responses. Statistics are available online under the Reports link of your PT-Central account.
References
1. Versalovic, J. (ed). 2013. Manual of Clinical Microbiology. 10th ed. ASM Press, Washington, D.C.
Page 3 of 21 2015-BactiReg3 Event Notes
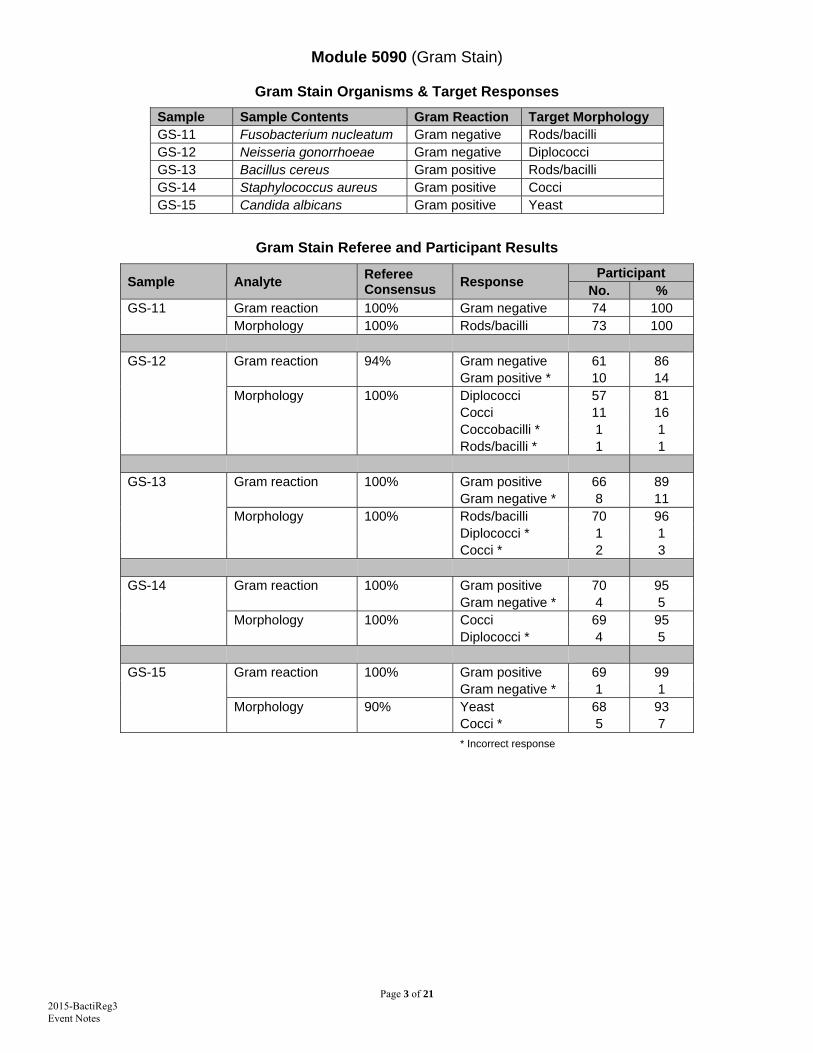
Module 5090 (Gram Stain)
Gram Stain Organisms & Target Responses
Sample Sample Contents Gram Reaction Target Morphology GS-11 Fusobacterium nucleatum Gram negative Rods/bacilli GS-12 Neisseria gonorrhoeae Gram negative Diplococci GS-13 Bacillus cereus Gram positive Rods/bacilli GS-14 Staphylococcus aureus Gram positive Cocci GS-15 Candida albicans Gram positive Yeast
Gram Stain Referee and Participant Results
Sample Analyte Referee Consensus
Response Participant
No. % GS-11 Gram reaction 100% Gram negative 74 100 Morphology 100% Rods/bacilli 73 100 GS-12 Gram reaction 94% Gram negative 61 86 Gram positive * 10 14 Morphology 100% Diplococci 57 81 Cocci 11 16 Coccobacilli * 1 1 Rods/bacilli * 1 1 GS-13 Gram reaction 100% Gram positive 66 89 Gram negative * 8 11 Morphology 100% Rods/bacilli 70 96 Diplococci * 1 1 Cocci * 2 3 GS-14 Gram reaction 100% Gram positive 70 95 Gram negative * 4 5 Morphology 100% Cocci 69 95 Diplococci * 4 5 GS-15 Gram reaction 100% Gram positive 69 99 Gram negative * 1 1 Morphology 90% Yeast 68 93 Cocci * 5 7
* Incorrect response

Page 4 of 21 2015-BactiReg3 Event Notes
Modules 5030 and 5040 (Bacteriology—Comprehensive and Bacteriology—Limited)
Sample ID
Requested Procedure/Analyte(s) Target Organism/Result
MC-19 Group A streptococcus antigen Positive for Group A streptococcus antigen MC-20 Group A streptococcus screen Positive for Group A streptococcus MC-21 Neisseria gonorrhoeae screen Positive for Neisseria gonorrhoeae
MC-22 Aerobic culture (wound) Staphylococcus aureus Susceptibility testing Appropriate antimicrobials & susceptibilities
MC-23 Urine culture Enterococcus faecium Gram stain Gram positive cocci Susceptibility testing Appropriate antimicrobials & susceptibilities
MC-24 Gram Stain Gram positive yeast MC-25 Anaerobic culture Actinomyces meyeri MC-26 Aerobic culture (eye) Bacillus cereus MC-27 Stool Culture Shigella boydii Please note: Samples MC-24 through MC-27 are not included in module 5040 (Bacteriology Limited).
MC-19 (Group A streptococcus antigen detection), MC-20 (Group A streptococcus culture), and MC-21 (Neisseria gonorrhoeae screen): All analytes and samples achieved ≥80% peer consensus, matched targets, and were scored accordingly. Laboratories using methods with peer groups of n<10 were scored by the All Methods group. MC-22 (Aerobic wound culture): Sample contained Staphylococcus aureus >100,000 CFU/Loop and Staphylococcus epidermidis <10,000 CFU/Loop. Referee consensus: 100%
Primary Organism Responses Participants
No. % Staphylococcus aureus 69
99 Staphylococcus coagulase positive 1 Gram positive cocci 1 Growth observed (would refer) 1 Staphylococcus aureus - MRSA * 1 1
* Incorrect response
Page 5 of 21 2015-BactiReg3 Event Notes
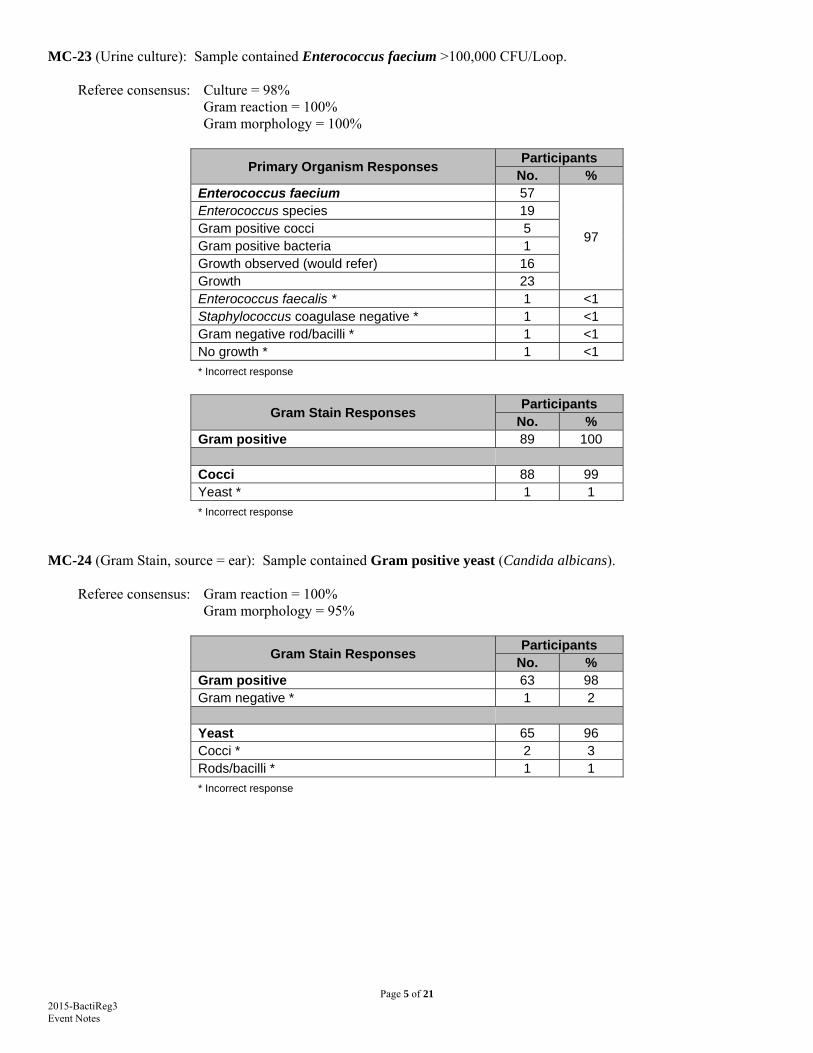
MC-23 (Urine culture): Sample contained Enterococcus faecium >100,000 CFU/Loop. Referee consensus: Culture = 98% Gram reaction = 100% Gram morphology = 100%
Primary Organism Responses Participants
No. % Enterococcus faecium 57
97
Enterococcus species 19 Gram positive cocci 5 Gram positive bacteria 1 Growth observed (would refer) 16 Growth 23 Enterococcus faecalis * 1 <1 Staphylococcus coagulase negative * 1 <1 Gram negative rod/bacilli * 1 <1 No growth * 1 <1
* Incorrect response
Gram Stain Responses Participants
No. % Gram positive 89 100 Cocci 88 99 Yeast * 1 1
* Incorrect response
MC-24 (Gram Stain, source = ear): Sample contained Gram positive yeast (Candida albicans). Referee consensus: Gram reaction = 100% Gram morphology = 95%
Gram Stain Responses Participants
No. % Gram positive 63 98 Gram negative * 1 2 Yeast 65 96 Cocci * 2 3 Rods/bacilli * 1 1
* Incorrect response
Page 6 of 21 2015-BactiReg3 Event Notes
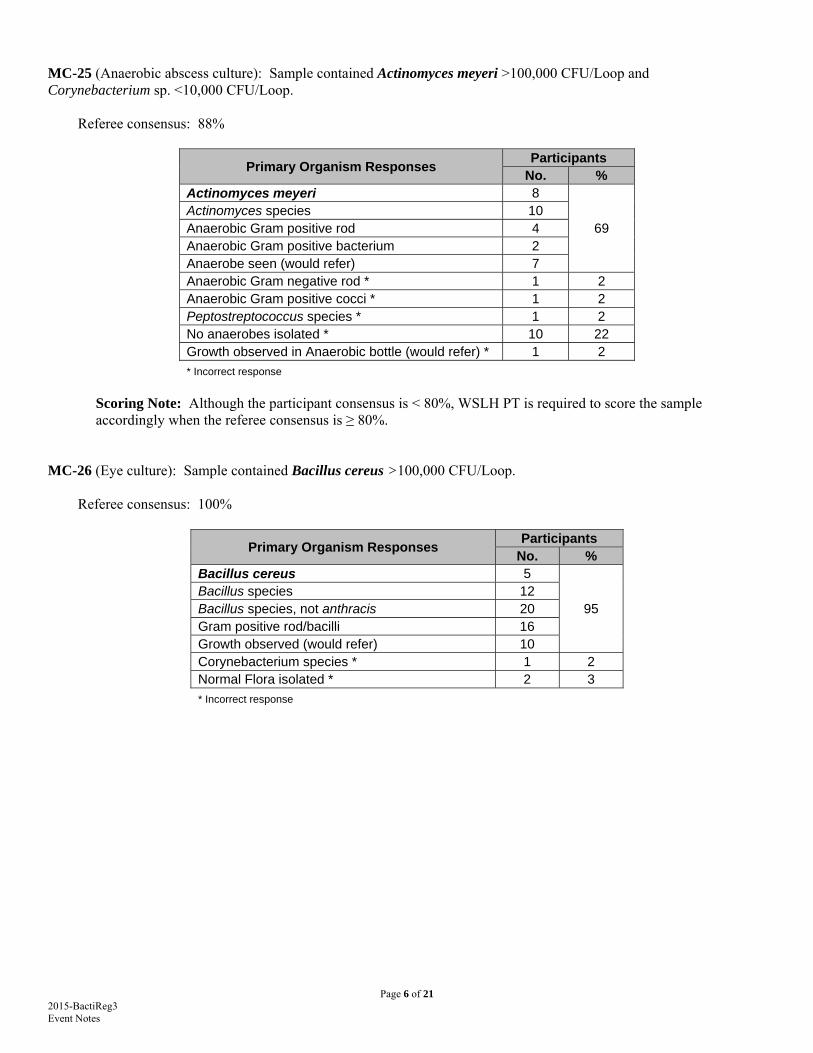
MC-25 (Anaerobic abscess culture): Sample contained Actinomyces meyeri >100,000 CFU/Loop and Corynebacterium sp. <10,000 CFU/Loop. Referee consensus: 88%
Primary Organism Responses Participants
No. % Actinomyces meyeri 8
69 Actinomyces species 10 Anaerobic Gram positive rod 4 Anaerobic Gram positive bacterium 2 Anaerobe seen (would refer) 7 Anaerobic Gram negative rod * 1 2 Anaerobic Gram positive cocci * 1 2 Peptostreptococcus species * 1 2 No anaerobes isolated * 10 22 Growth observed in Anaerobic bottle (would refer) * 1 2
* Incorrect response
Scoring Note: Although the participant consensus is < 80%, WSLH PT is required to score the sample accordingly when the referee consensus is ≥ 80%.
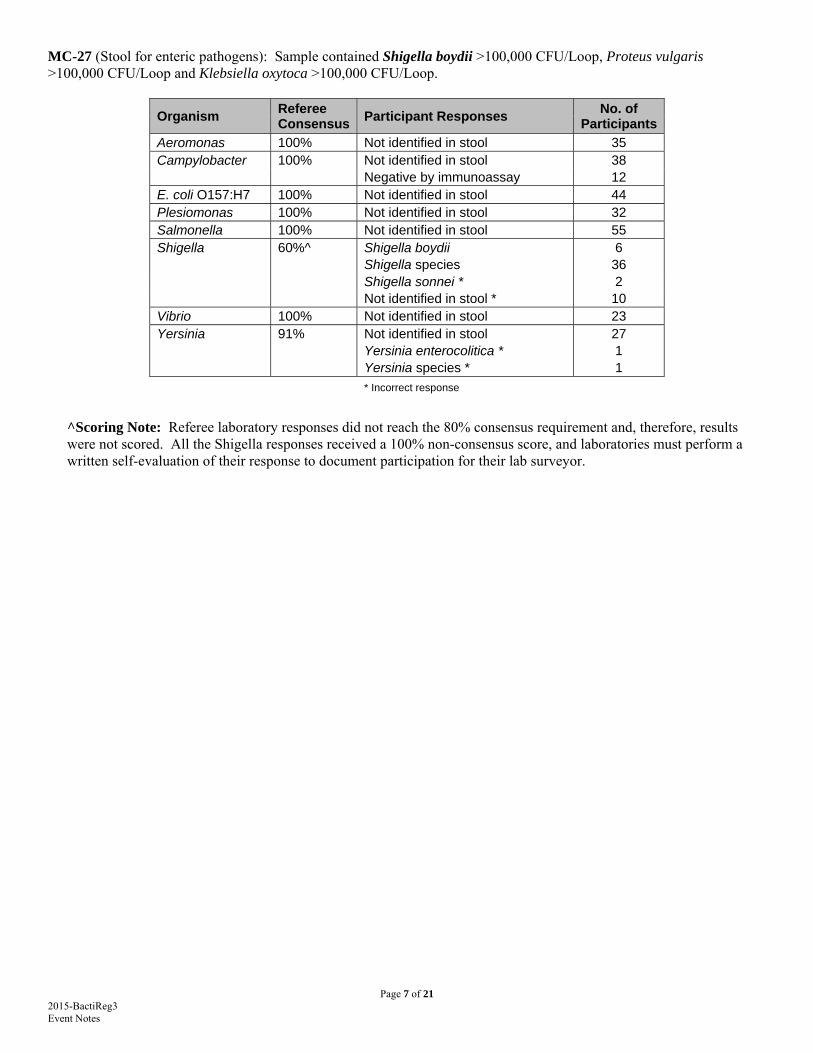
MC-26 (Eye culture): Sample contained Bacillus cereus >100,000 CFU/Loop. Referee consensus: 100%
Primary Organism Responses Participants
No. % Bacillus cereus 5
95 Bacillus species 12 Bacillus species, not anthracis 20 Gram positive rod/bacilli 16 Growth observed (would refer) 10 Corynebacterium species * 1 2 Normal Flora isolated * 2 3
* Incorrect response
Page 7 of 21 2015-BactiReg3 Event Notes
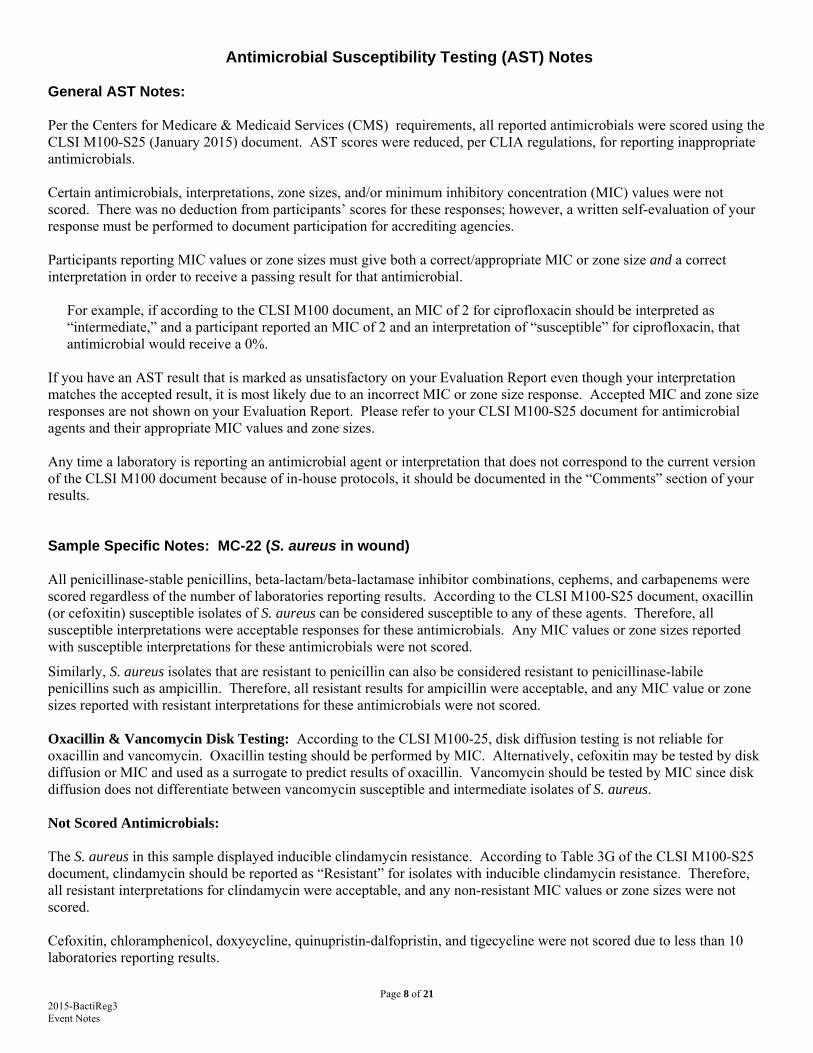
MC-27 (Stool for enteric pathogens): Sample contained Shigella boydii >100,000 CFU/Loop, Proteus vulgaris >100,000 CFU/Loop and Klebsiella oxytoca >100,000 CFU/Loop.
Organism Referee Consensus
Participant Responses No. of
Participants
Aeromonas 100% Not identified in stool 35 Campylobacter 100% Not identified in stool 38 Negative by immunoassay 12 E. coli O157:H7 100% Not identified in stool 44 Plesiomonas 100% Not identified in stool 32 Salmonella 100% Not identified in stool 55 Shigella 60%^ Shigella boydii 6 Shigella species 36 Shigella sonnei * 2 Not identified in stool * 10 Vibrio 100% Not identified in stool 23 Yersinia 91% Not identified in stool 27 Yersinia enterocolitica * 1 Yersinia species * 1 * Incorrect response
^Scoring Note: Referee laboratory responses did not reach the 80% consensus requirement and, therefore, results were not scored. All the Shigella responses received a 100% non-consensus score, and laboratories must perform a written self-evaluation of their response to document participation for their lab surveyor.
Page 8 of 21 2015-BactiReg3 Event Notes
Antimicrobial Susceptibility Testing (AST) Notes General AST Notes: Per the Centers for Medicare & Medicaid Services (CMS) requirements, all reported antimicrobials were scored using the CLSI M100-S25 (January 2015) document. AST scores were reduced, per CLIA regulations, for reporting inappropriate antimicrobials. Certain antimicrobials, interpretations, zone sizes, and/or minimum inhibitory concentration (MIC) values were not scored. There was no deduction from participants’ scores for these responses; however, a written self-evaluation of your response must be performed to document participation for accrediting agencies. Participants reporting MIC values or zone sizes must give both a correct/appropriate MIC or zone size and a correct interpretation in order to receive a passing result for that antimicrobial.
For example, if according to the CLSI M100 document, an MIC of 2 for ciprofloxacin should be interpreted as “intermediate,” and a participant reported an MIC of 2 and an interpretation of “susceptible” for ciprofloxacin, that antimicrobial would receive a 0%.
If you have an AST result that is marked as unsatisfactory on your Evaluation Report even though your interpretation matches the accepted result, it is most likely due to an incorrect MIC or zone size response. Accepted MIC and zone size responses are not shown on your Evaluation Report. Please refer to your CLSI M100-S25 document for antimicrobial agents and their appropriate MIC values and zone sizes. Any time a laboratory is reporting an antimicrobial agent or interpretation that does not correspond to the current version of the CLSI M100 document because of in-house protocols, it should be documented in the “Comments” section of your results. Sample Specific Notes: MC-22 (S. aureus in wound) All penicillinase-stable penicillins, beta-lactam/beta-lactamase inhibitor combinations, cephems, and carbapenems were scored regardless of the number of laboratories reporting results. According to the CLSI M100-S25 document, oxacillin (or cefoxitin) susceptible isolates of S. aureus can be considered susceptible to any of these agents. Therefore, all susceptible interpretations were acceptable responses for these antimicrobials. Any MIC values or zone sizes reported with susceptible interpretations for these antimicrobials were not scored.
Similarly, S. aureus isolates that are resistant to penicillin can also be considered resistant to penicillinase-labile penicillins such as ampicillin. Therefore, all resistant results for ampicillin were acceptable, and any MIC value or zone sizes reported with resistant interpretations for these antimicrobials were not scored. Oxacillin & Vancomycin Disk Testing: According to the CLSI M100-25, disk diffusion testing is not reliable for oxacillin and vancomycin. Oxacillin testing should be performed by MIC. Alternatively, cefoxitin may be tested by disk diffusion or MIC and used as a surrogate to predict results of oxacillin. Vancomycin should be tested by MIC since disk diffusion does not differentiate between vancomycin susceptible and intermediate isolates of S. aureus. Not Scored Antimicrobials: The S. aureus in this sample displayed inducible clindamycin resistance. According to Table 3G of the CLSI M100-S25 document, clindamycin should be reported as “Resistant” for isolates with inducible clindamycin resistance. Therefore, all resistant interpretations for clindamycin were acceptable, and any non-resistant MIC values or zone sizes were not scored. Cefoxitin, chloramphenicol, doxycycline, quinupristin-dalfopristin, and tigecycline were not scored due to less than 10 laboratories reporting results.
Page 9 of 21 2015-BactiReg3 Event Notes
Inappropriate Antimicrobials: Appropriate antimicrobials for S. aureus are listed in Table 2C, Staphylococcus spp., of the CLSI M100-S25 document. Antimicrobials that are considered inappropriate according to this table received a 0% score. Please note that nitrofurantoin should only be reported on urine sources.
Sample Specific Notes: MC-23 (E. faecium in urine) Clindamycin, trimethoprim-sulfamethoxazole, all cephalosporins, and all aminoglycosides (except for synergy screens) were scored regardless of the number of laboratories reporting results. According to the CLSI M100-S25 document, Enterococcus isolates should not be reported as susceptible to any of these agents. Therefore, all resistant interpretation results were acceptable for these antimicrobials. Any MIC values or zone sizes reported for these antimicrobials were not scored since there are no breakpoint values listed in Table 2D of the CLSI M100-S25 document.
Please note that these agents are not clinically effective against Enterococcus species even though they may appear susceptible in vitro. Doxycycline was scored based on the consensus results of tetracycline. Not scored antimicrobials: According to the CLSI M100-S25 document, penicillin results may be used to predict the susceptibility of ampicillin, ampicillin-sulbactam, amoxicillin, amoxicillin-clavulanic acid, piperacillin and piperacillin-tazobactam. Similarly, the results of ampicillin may be used to predict the susceptibility of amoxicillin, amoxicillin-clavulanic acid, ampicillin-sulbactam, piperacillin and piperacillin-tazobactam. Therefore, these antimicrobials were scored based on the consensus response for penicillin and/or ampicillin. Any MIC values reported for the predicted antimicrobials were not scored since there are no breakpoint values listed in Table 2D of the CLSI M100-S25 document. Norfloxacin, rifampin, and tigecycline were not scored due to less than 10 laboratories reporting results. Nitrofurantoin interpretation responses did not reach the required ≥ 80% consensus for the Vitek2 and All Methods peer groups. All nitrofurantoin responses in these peer groups were not scored due to non-consensus. The table below shows the nitrofurantoin responses by method.
The nitrofurantoin interpretation responses in the Microscan peer group reached 82% consensus and were therefore scored accordingly.
Antimicrobial Susceptibility Interpretations by Method for Sample MC‐23
Antimicrobial Agent Interpretation Disk
Diffusion Microscan Vitek2
Nitrofurantoin Susceptible 6 22 20
Intermediate ‐ 5 13
Resistant 1 ‐ 2
Inappropriate antimicrobials: Appropriate antimicrobials for E. faecalis are listed in Table 2D, Enterococcus spp., of the CLSI M100-S25 document. Antimicrobials that are considered inappropriate according to this table received a 0% score. Please note that erythromycin is not recommended for reporting on urine sources. Quinupristin-dalfopristin (Synercid) should only be reported on vancomycin-resistant E. faecium.
Page 10 of 21 2015-BactiReg3 Event Notes
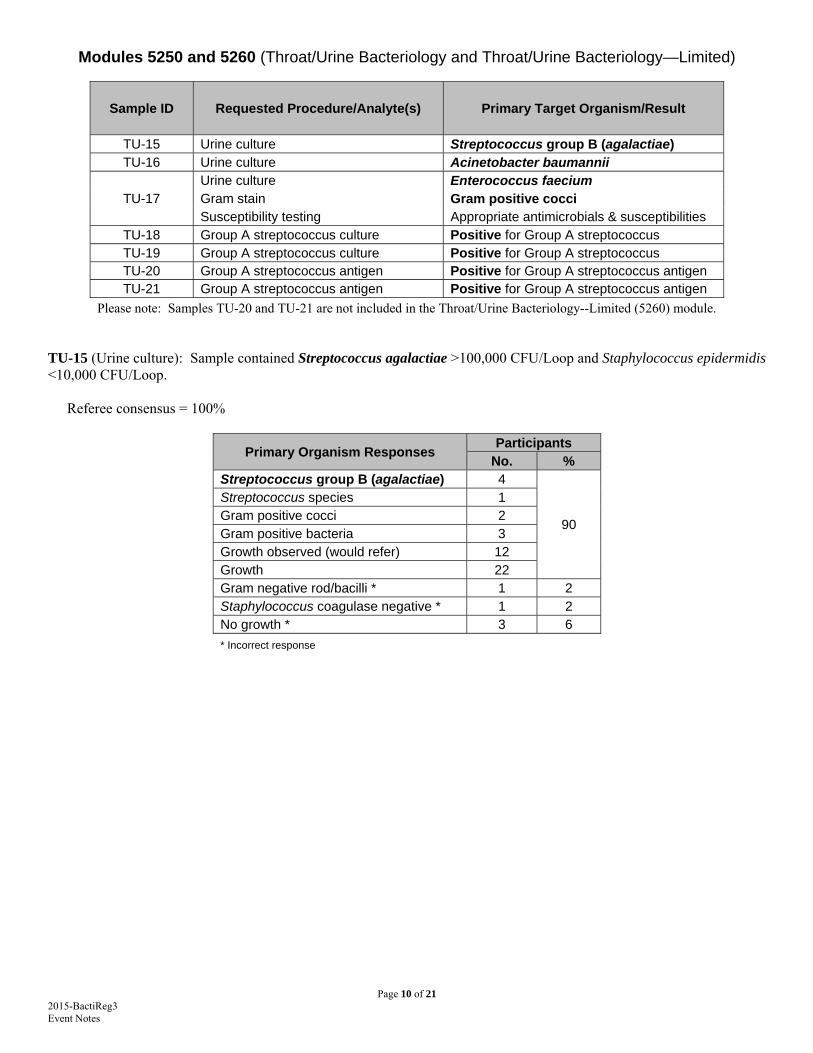
Modules 5250 and 5260 (Throat/Urine Bacteriology and Throat/Urine Bacteriology—Limited)
Sample ID Requested Procedure/Analyte(s) Primary Target Organism/Result
TU-15 Urine culture Streptococcus group B (agalactiae) TU-16 Urine culture Acinetobacter baumannii
TU-17 Urine culture Enterococcus faecium Gram stain Gram positive cocci Susceptibility testing Appropriate antimicrobials & susceptibilities
TU-18 Group A streptococcus culture Positive for Group A streptococcus TU-19 Group A streptococcus culture Positive for Group A streptococcus TU-20 Group A streptococcus antigen Positive for Group A streptococcus antigen TU-21 Group A streptococcus antigen Positive for Group A streptococcus antigen
Please note: Samples TU-20 and TU-21 are not included in the Throat/Urine Bacteriology--Limited (5260) module. TU-15 (Urine culture): Sample contained Streptococcus agalactiae >100,000 CFU/Loop and Staphylococcus epidermidis <10,000 CFU/Loop.
Referee consensus = 100%
Primary Organism Responses Participants
No. % Streptococcus group B (agalactiae) 4
90
Streptococcus species 1 Gram positive cocci 2 Gram positive bacteria 3 Growth observed (would refer) 12 Growth 22 Gram negative rod/bacilli * 1 2 Staphylococcus coagulase negative * 1 2 No growth * 3 6
* Incorrect response
Page 11 of 21 2015-BactiReg3 Event Notes
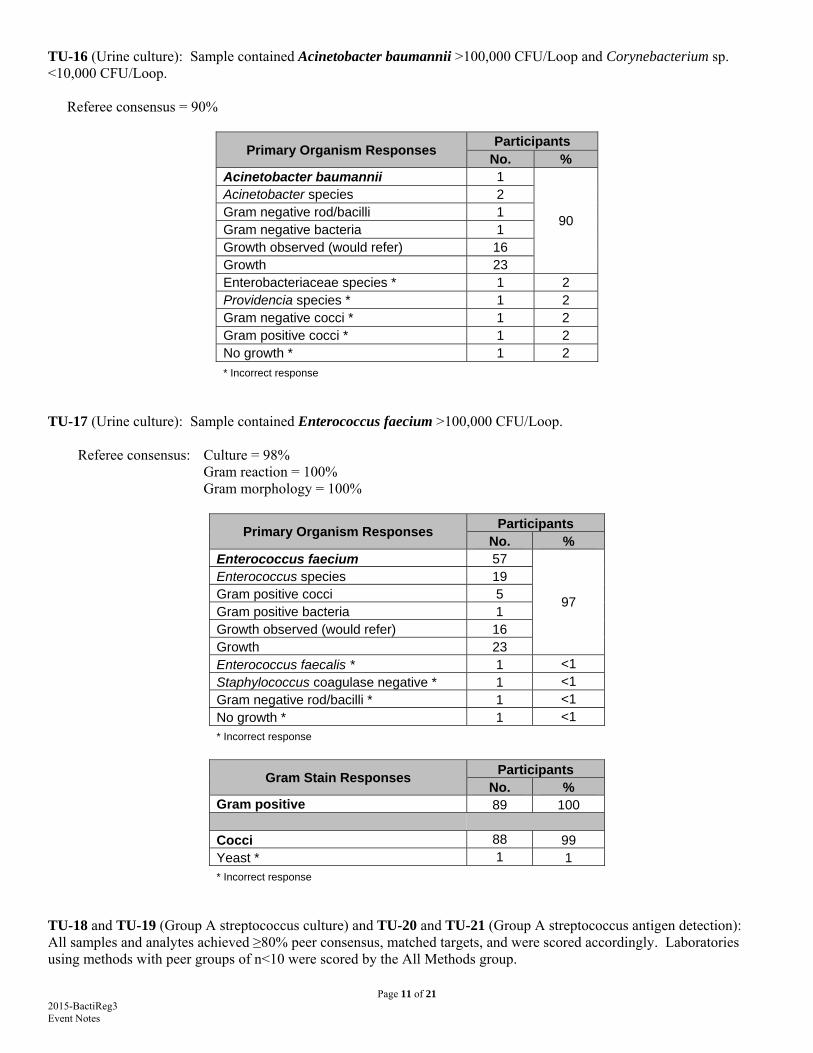
TU-16 (Urine culture): Sample contained Acinetobacter baumannii >100,000 CFU/Loop and Corynebacterium sp. <10,000 CFU/Loop.
Referee consensus = 90%
Primary Organism Responses Participants
No. % Acinetobacter baumannii 1
90
Acinetobacter species 2 Gram negative rod/bacilli 1 Gram negative bacteria 1 Growth observed (would refer) 16 Growth 23 Enterobacteriaceae species * 1 2 Providencia species * 1 2 Gram negative cocci * 1 2 Gram positive cocci * 1 2 No growth * 1 2
* Incorrect response
TU-17 (Urine culture): Sample contained Enterococcus faecium >100,000 CFU/Loop. Referee consensus: Culture = 98% Gram reaction = 100% Gram morphology = 100%
Primary Organism Responses Participants
No. % Enterococcus faecium 57
97
Enterococcus species 19 Gram positive cocci 5 Gram positive bacteria 1 Growth observed (would refer) 16 Growth 23 Enterococcus faecalis * 1 <1 Staphylococcus coagulase negative * 1 <1 Gram negative rod/bacilli * 1 <1 No growth * 1 <1
* Incorrect response
Gram Stain Responses Participants
No. % Gram positive 89 100 Cocci 88 99 Yeast * 1 1 * Incorrect response
TU-18 and TU-19 (Group A streptococcus culture) and TU-20 and TU-21 (Group A streptococcus antigen detection): All samples and analytes achieved ≥80% peer consensus, matched targets, and were scored accordingly. Laboratories using methods with peer groups of n<10 were scored by the All Methods group.
Page 12 of 21 2015-BactiReg3 Event Notes
Antimicrobial Susceptibility Testing (AST) Notes General AST Notes: Per the Centers for Medicare & Medicaid Services (CMS) requirements, all reported antimicrobials were scored using the CLSI M100-S25 (January 2015) document. AST scores were reduced, per CLIA regulations, for reporting inappropriate antimicrobials. Certain antimicrobials, interpretations, zone sizes, and/or minimum inhibitory concentration (MIC) values were not scored. There was no deduction from participants’ scores for these responses; however, a written self-evaluation of your response must be performed to document participation for accrediting agencies. Participants reporting MIC values or zone sizes must give both a correct/appropriate MIC or zone size and a correct interpretation in order to receive a passing result for that antimicrobial.
For example, if according to the CLSI M100 document, an MIC of 2 for ciprofloxacin should be interpreted as “intermediate,” and a participant reported an MIC of 2 and an interpretation of “susceptible” for ciprofloxacin, that antimicrobial would receive a 0%.
If you have an AST result that is marked as unsatisfactory on your Evaluation Report even though your interpretation matches the accepted result, it is most likely due to an incorrect MIC or zone size response. Accepted MIC and zone size responses are not shown on your Evaluation Report. Please refer to your CLSI M100-S25 document for antimicrobial agents and their appropriate MIC values and zone sizes. Any time a laboratory is reporting an antimicrobial agent or interpretation that does not correspond to the current version of the CLSI M100 document because of in-house protocols, it should be documented in the “Comments” section of your results. Sample Specific Notes: TU-17 (E. faecium in urine) Clindamycin, trimethoprim-sulfamethoxazole, all cephalosporins, and all aminoglycosides (except for synergy screens) were scored regardless of the number of laboratories reporting results. According to the CLSI M100-S25 document, Enterococcus isolates should not be reported as susceptible to any of these agents. Therefore, all resistant interpretation results were acceptable for these antimicrobials. Any MIC values or zone sizes reported for these antimicrobials were not scored since there are no breakpoint values listed in Table 2D of the CLSI M100-S25 document.
Please note that these agents are not clinically effective against Enterococcus species even though they may appear susceptible in vitro. Doxycycline was scored based on the consensus results of tetracycline. Not scored antimicrobials: According to the CLSI M100-S25 document, penicillin results may be used to predict the susceptibility of ampicillin, ampicillin-sulbactam, amoxicillin, amoxicillin-clavulanic acid, piperacillin and piperacillin-tazobactam. Similarly, the results of ampicillin may be used to predict the susceptibility of amoxicillin, amoxicillin-clavulanic acid, ampicillin-sulbactam, piperacillin and piperacillin-tazobactam. Therefore, these antimicrobials were scored based on the consensus response for penicillin and/or ampicillin. Any MIC values reported for the predicted antimicrobials were not scored since there are no breakpoint values listed in Table 2D of the CLSI M100-S25 document. Norfloxacin, rifampin, and tigecycline were not scored due to less than 10 laboratories reporting results. Nitrofurantoin interpretation responses did not reach the required ≥ 80% consensus for the Vitek2 and All Methods peer groups. All nitrofurantoin responses in these peer groups were not scored due to non-consensus. The following table shows the nitrofurantoin responses by method.
Page 13 of 21 2015-BactiReg3 Event Notes
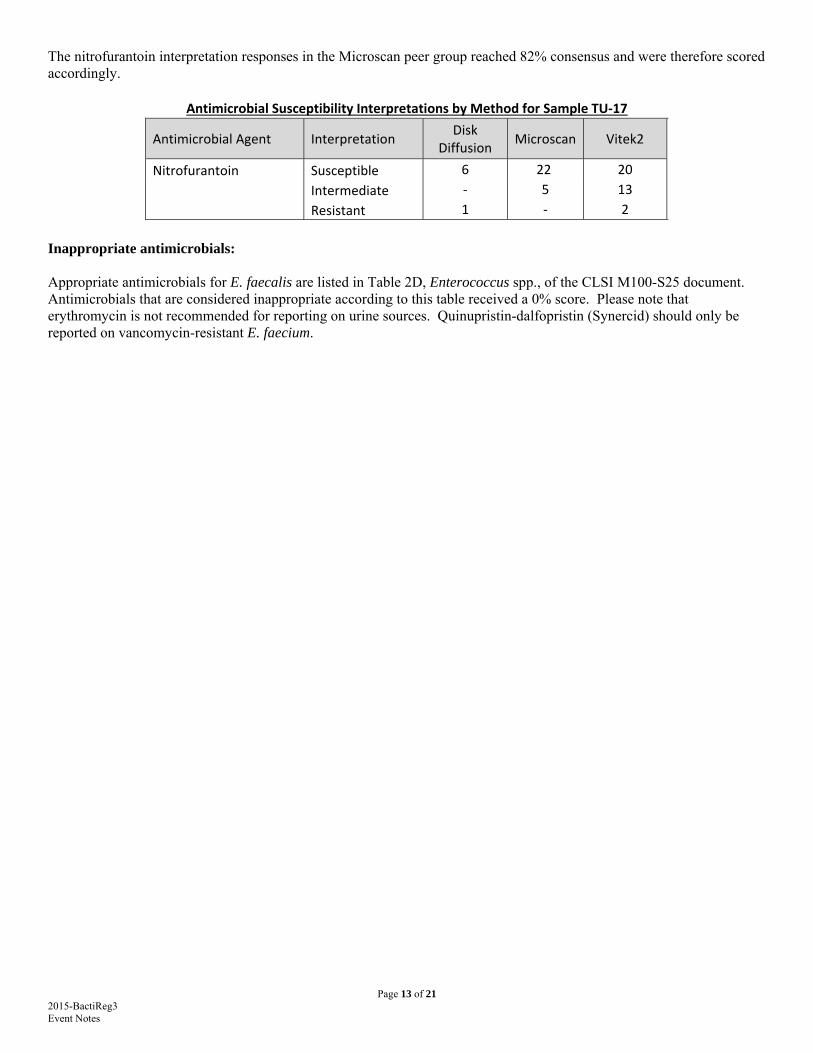
The nitrofurantoin interpretation responses in the Microscan peer group reached 82% consensus and were therefore scored accordingly.
Antimicrobial Susceptibility Interpretations by Method for Sample TU‐17
Antimicrobial Agent Interpretation Disk
Diffusion Microscan Vitek2
Nitrofurantoin Susceptible 6 22 20
Intermediate ‐ 5 13
Resistant 1 ‐ 2
Inappropriate antimicrobials: Appropriate antimicrobials for E. faecalis are listed in Table 2D, Enterococcus spp., of the CLSI M100-S25 document. Antimicrobials that are considered inappropriate according to this table received a 0% score. Please note that erythromycin is not recommended for reporting on urine sources. Quinupristin-dalfopristin (Synercid) should only be reported on vancomycin-resistant E. faecium.
Page 14 of 21 2015-BactiReg3 Event Notes
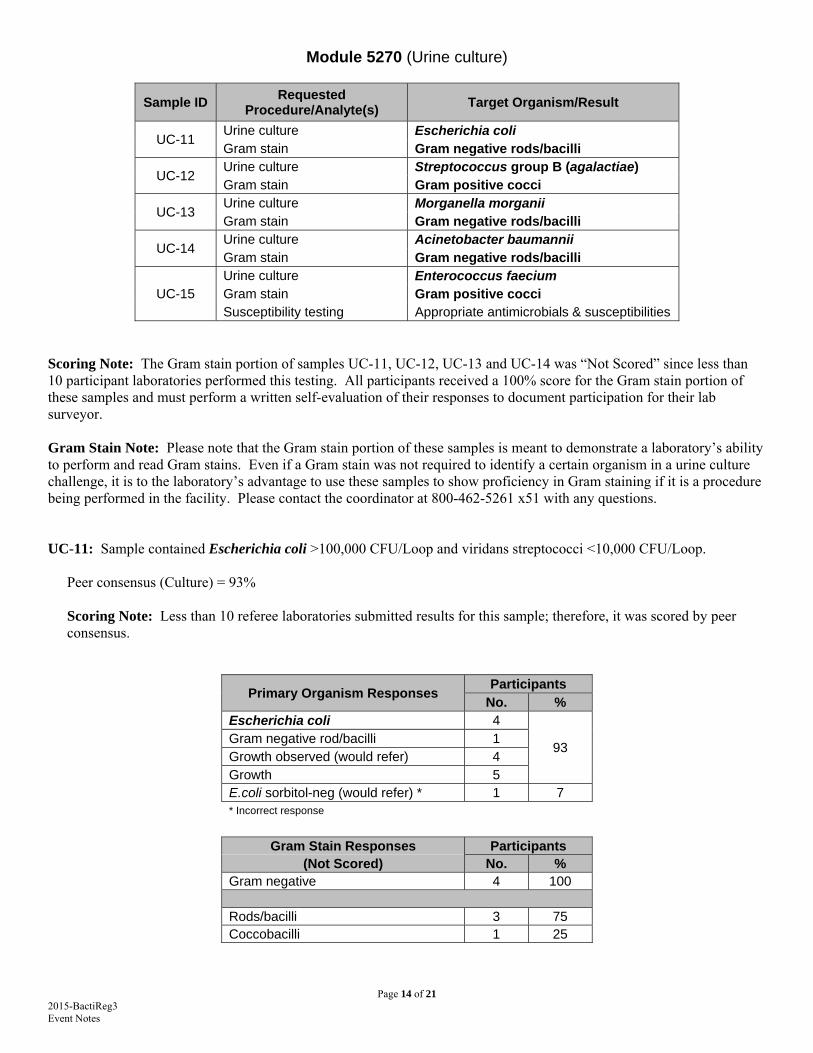
Module 5270 (Urine culture)
Sample ID Requested
Procedure/Analyte(s) Target Organism/Result
UC-11 Urine culture Escherichia coli Gram stain Gram negative rods/bacilli
UC-12 Urine culture Streptococcus group B (agalactiae) Gram stain Gram positive cocci
UC-13 Urine culture Morganella morganii Gram stain Gram negative rods/bacilli
UC-14 Urine culture Acinetobacter baumannii Gram stain Gram negative rods/bacilli
UC-15 Urine culture Enterococcus faecium Gram stain Gram positive cocci Susceptibility testing Appropriate antimicrobials & susceptibilities
Scoring Note: The Gram stain portion of samples UC-11, UC-12, UC-13 and UC-14 was “Not Scored” since less than 10 participant laboratories performed this testing. All participants received a 100% score for the Gram stain portion of these samples and must perform a written self-evaluation of their responses to document participation for their lab surveyor. Gram Stain Note: Please note that the Gram stain portion of these samples is meant to demonstrate a laboratory’s ability to perform and read Gram stains. Even if a Gram stain was not required to identify a certain organism in a urine culture challenge, it is to the laboratory’s advantage to use these samples to show proficiency in Gram staining if it is a procedure being performed in the facility. Please contact the coordinator at 800-462-5261 x51 with any questions. UC-11: Sample contained Escherichia coli >100,000 CFU/Loop and viridans streptococci <10,000 CFU/Loop.
Peer consensus (Culture) = 93% Scoring Note: Less than 10 referee laboratories submitted results for this sample; therefore, it was scored by peer consensus.
Primary Organism Responses Participants
No. % Escherichia coli 4
93 Gram negative rod/bacilli 1 Growth observed (would refer) 4 Growth 5 E.coli sorbitol-neg (would refer) * 1 7 * Incorrect response
Gram Stain Responses Participants (Not Scored) No. %
Gram negative 4 100
Rods/bacilli 3 75 Coccobacilli 1 25
Page 15 of 21 2015-BactiReg3 Event Notes
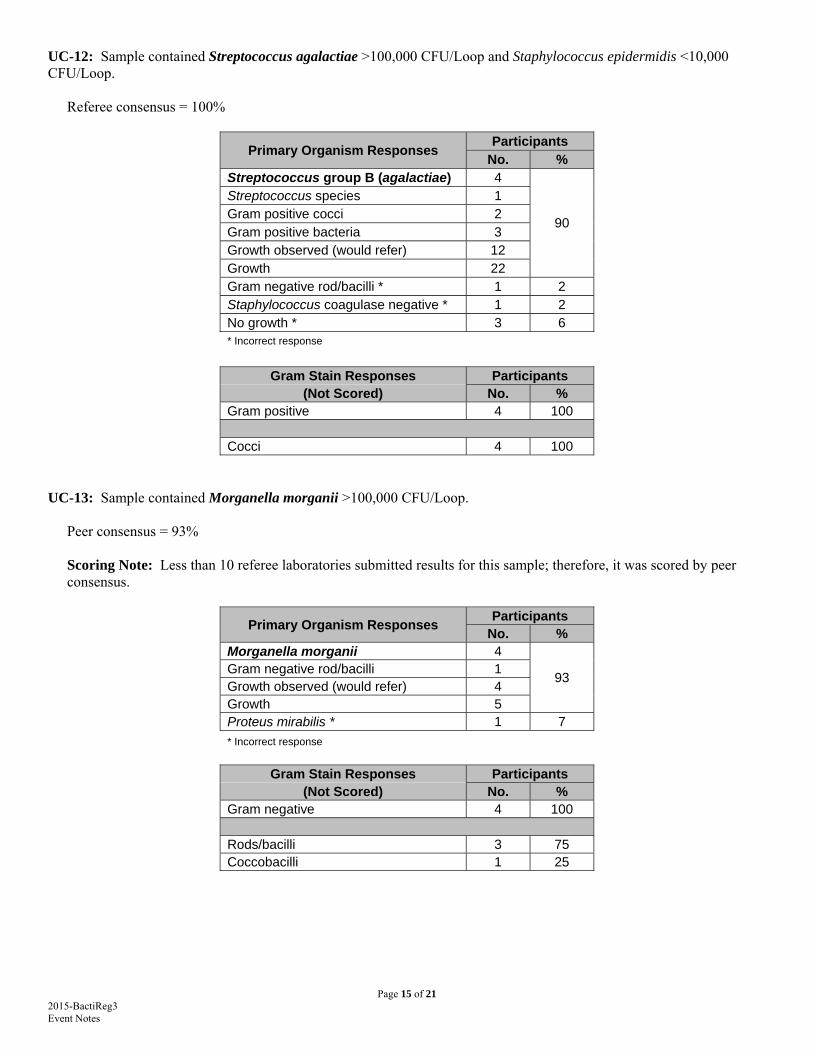
UC-12: Sample contained Streptococcus agalactiae >100,000 CFU/Loop and Staphylococcus epidermidis <10,000 CFU/Loop.
Referee consensus = 100%
Primary Organism Responses Participants
No. % Streptococcus group B (agalactiae) 4
90
Streptococcus species 1 Gram positive cocci 2 Gram positive bacteria 3 Growth observed (would refer) 12 Growth 22 Gram negative rod/bacilli * 1 2 Staphylococcus coagulase negative * 1 2 No growth * 3 6 * Incorrect response
Gram Stain Responses Participants (Not Scored) No. %
Gram positive 4 100
Cocci 4 100 UC-13: Sample contained Morganella morganii >100,000 CFU/Loop.
Peer consensus = 93% Scoring Note: Less than 10 referee laboratories submitted results for this sample; therefore, it was scored by peer consensus.
Primary Organism Responses Participants
No. % Morganella morganii 4
93 Gram negative rod/bacilli 1 Growth observed (would refer) 4 Growth 5 Proteus mirabilis * 1 7
* Incorrect response
Gram Stain Responses Participants (Not Scored) No. %
Gram negative 4 100
Rods/bacilli 3 75 Coccobacilli 1 25
Page 16 of 21 2015-BactiReg3 Event Notes
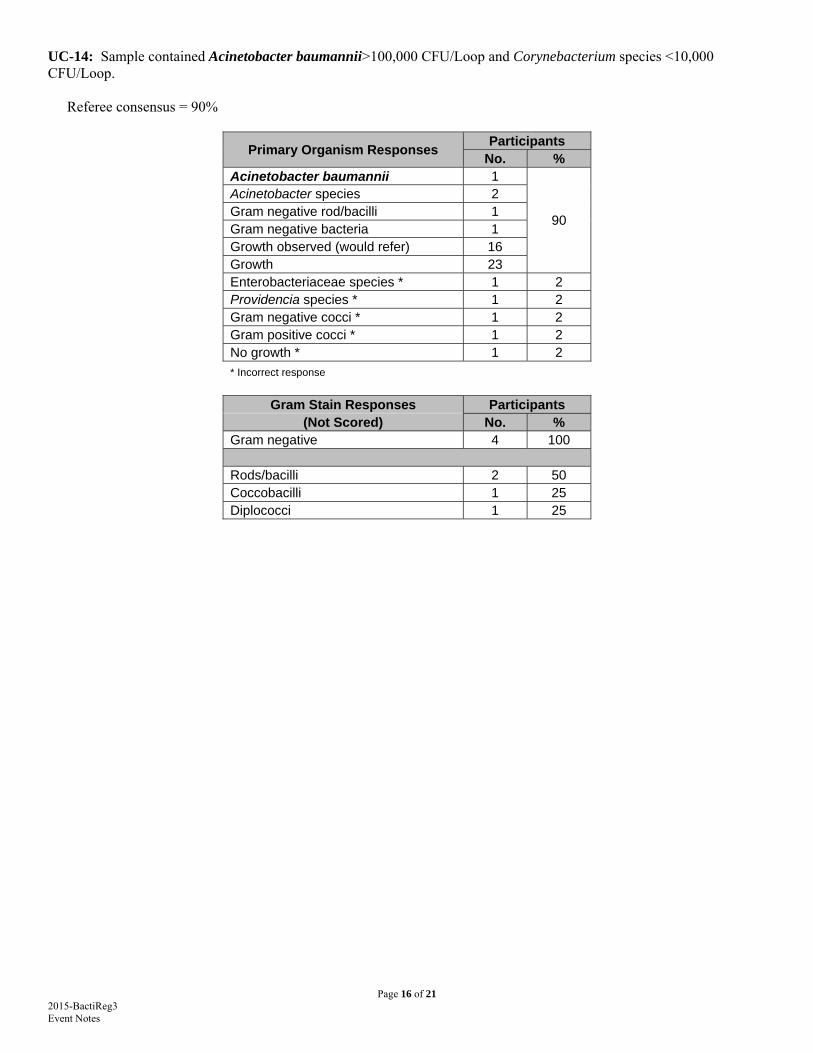
UC-14: Sample contained Acinetobacter baumannii>100,000 CFU/Loop and Corynebacterium species <10,000 CFU/Loop.
Referee consensus = 90%
Primary Organism Responses Participants
No. % Acinetobacter baumannii 1
90
Acinetobacter species 2 Gram negative rod/bacilli 1 Gram negative bacteria 1 Growth observed (would refer) 16 Growth 23 Enterobacteriaceae species * 1 2 Providencia species * 1 2 Gram negative cocci * 1 2 Gram positive cocci * 1 2 No growth * 1 2
* Incorrect response
Gram Stain Responses Participants (Not Scored) No. %
Gram negative 4 100
Rods/bacilli 2 50 Coccobacilli 1 25 Diplococci 1 25
Page 17 of 21 2015-BactiReg3 Event Notes
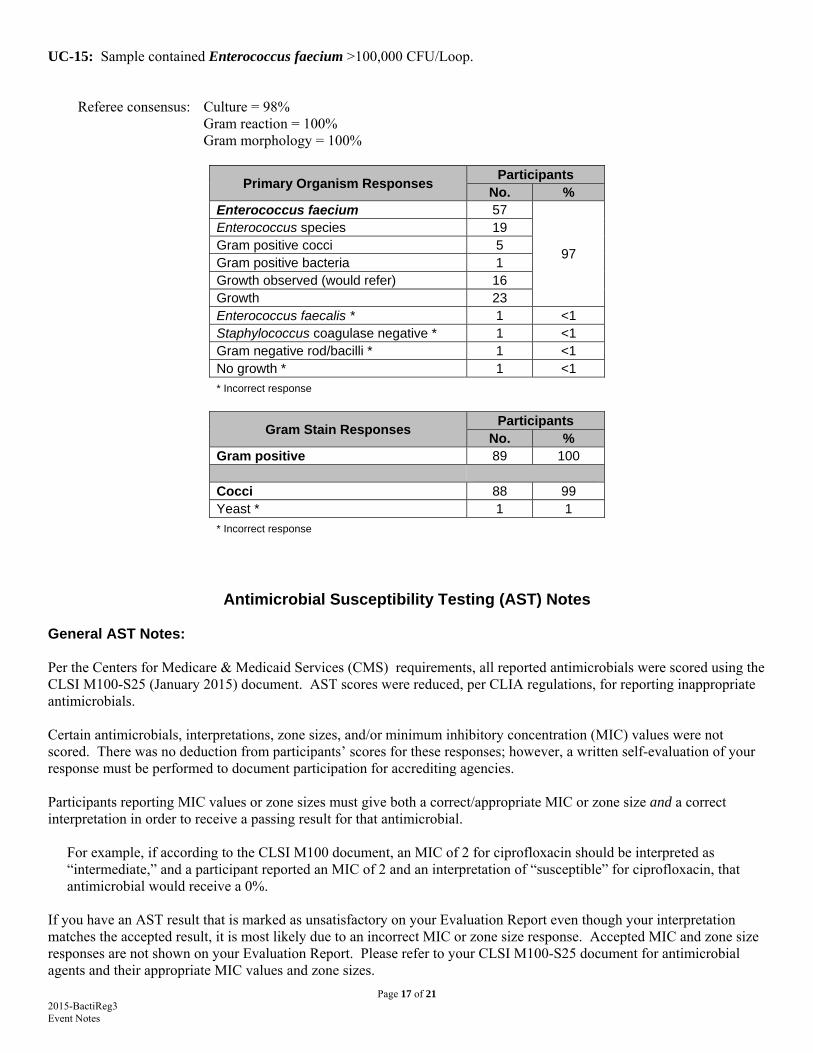
UC-15: Sample contained Enterococcus faecium >100,000 CFU/Loop. Referee consensus: Culture = 98% Gram reaction = 100% Gram morphology = 100%
Primary Organism Responses Participants
No. % Enterococcus faecium 57
97
Enterococcus species 19 Gram positive cocci 5 Gram positive bacteria 1 Growth observed (would refer) 16 Growth 23 Enterococcus faecalis * 1 <1 Staphylococcus coagulase negative * 1 <1 Gram negative rod/bacilli * 1 <1 No growth * 1 <1
* Incorrect response
Gram Stain Responses Participants
No. % Gram positive 89 100 Cocci 88 99 Yeast * 1 1
* Incorrect response
Antimicrobial Susceptibility Testing (AST) Notes General AST Notes: Per the Centers for Medicare & Medicaid Services (CMS) requirements, all reported antimicrobials were scored using the CLSI M100-S25 (January 2015) document. AST scores were reduced, per CLIA regulations, for reporting inappropriate antimicrobials. Certain antimicrobials, interpretations, zone sizes, and/or minimum inhibitory concentration (MIC) values were not scored. There was no deduction from participants’ scores for these responses; however, a written self-evaluation of your response must be performed to document participation for accrediting agencies. Participants reporting MIC values or zone sizes must give both a correct/appropriate MIC or zone size and a correct interpretation in order to receive a passing result for that antimicrobial.
For example, if according to the CLSI M100 document, an MIC of 2 for ciprofloxacin should be interpreted as “intermediate,” and a participant reported an MIC of 2 and an interpretation of “susceptible” for ciprofloxacin, that antimicrobial would receive a 0%.
If you have an AST result that is marked as unsatisfactory on your Evaluation Report even though your interpretation matches the accepted result, it is most likely due to an incorrect MIC or zone size response. Accepted MIC and zone size responses are not shown on your Evaluation Report. Please refer to your CLSI M100-S25 document for antimicrobial agents and their appropriate MIC values and zone sizes.
Page 18 of 21 2015-BactiReg3 Event Notes
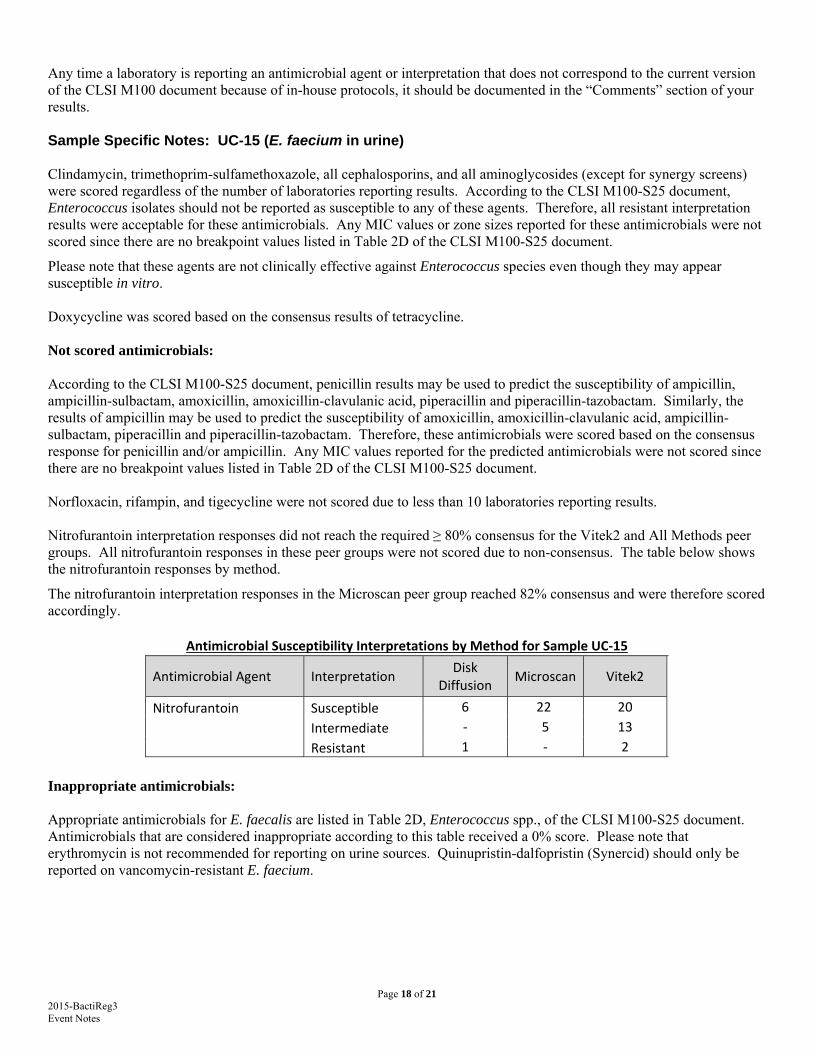
Any time a laboratory is reporting an antimicrobial agent or interpretation that does not correspond to the current version of the CLSI M100 document because of in-house protocols, it should be documented in the “Comments” section of your results. Sample Specific Notes: UC-15 (E. faecium in urine) Clindamycin, trimethoprim-sulfamethoxazole, all cephalosporins, and all aminoglycosides (except for synergy screens) were scored regardless of the number of laboratories reporting results. According to the CLSI M100-S25 document, Enterococcus isolates should not be reported as susceptible to any of these agents. Therefore, all resistant interpretation results were acceptable for these antimicrobials. Any MIC values or zone sizes reported for these antimicrobials were not scored since there are no breakpoint values listed in Table 2D of the CLSI M100-S25 document.
Please note that these agents are not clinically effective against Enterococcus species even though they may appear susceptible in vitro. Doxycycline was scored based on the consensus results of tetracycline. Not scored antimicrobials: According to the CLSI M100-S25 document, penicillin results may be used to predict the susceptibility of ampicillin, ampicillin-sulbactam, amoxicillin, amoxicillin-clavulanic acid, piperacillin and piperacillin-tazobactam. Similarly, the results of ampicillin may be used to predict the susceptibility of amoxicillin, amoxicillin-clavulanic acid, ampicillin-sulbactam, piperacillin and piperacillin-tazobactam. Therefore, these antimicrobials were scored based on the consensus response for penicillin and/or ampicillin. Any MIC values reported for the predicted antimicrobials were not scored since there are no breakpoint values listed in Table 2D of the CLSI M100-S25 document. Norfloxacin, rifampin, and tigecycline were not scored due to less than 10 laboratories reporting results. Nitrofurantoin interpretation responses did not reach the required ≥ 80% consensus for the Vitek2 and All Methods peer groups. All nitrofurantoin responses in these peer groups were not scored due to non-consensus. The table below shows the nitrofurantoin responses by method.
The nitrofurantoin interpretation responses in the Microscan peer group reached 82% consensus and were therefore scored accordingly.
Antimicrobial Susceptibility Interpretations by Method for Sample UC‐15
Antimicrobial Agent Interpretation Disk
Diffusion Microscan Vitek2
Nitrofurantoin Susceptible 6 22 20
Intermediate ‐ 5 13
Resistant 1 ‐ 2
Inappropriate antimicrobials: Appropriate antimicrobials for E. faecalis are listed in Table 2D, Enterococcus spp., of the CLSI M100-S25 document. Antimicrobials that are considered inappropriate according to this table received a 0% score. Please note that erythromycin is not recommended for reporting on urine sources. Quinupristin-dalfopristin (Synercid) should only be reported on vancomycin-resistant E. faecium.
Page 19 of 21 2015-BactiReg3 Event Notes
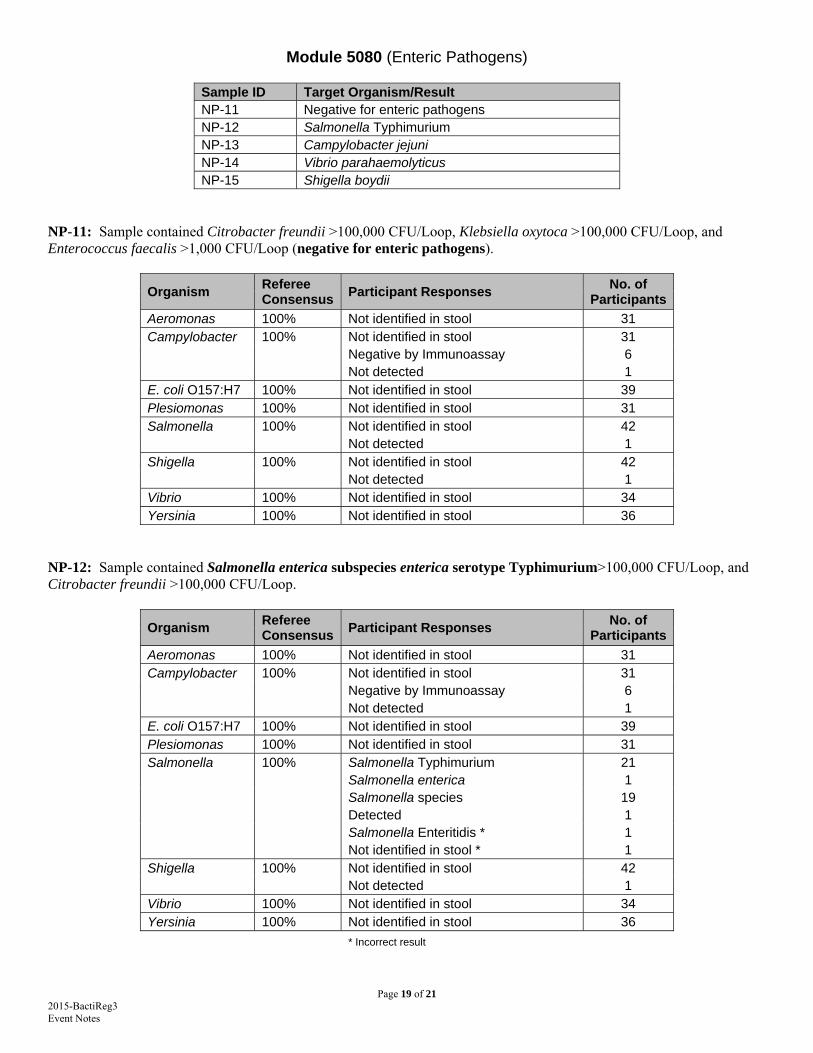
Module 5080 (Enteric Pathogens)
Sample ID Target Organism/Result NP-11 Negative for enteric pathogens NP-12 Salmonella Typhimurium NP-13 Campylobacter jejuni NP-14 Vibrio parahaemolyticus NP-15 Shigella boydii
NP-11: Sample contained Citrobacter freundii >100,000 CFU/Loop, Klebsiella oxytoca >100,000 CFU/Loop, and Enterococcus faecalis >1,000 CFU/Loop (negative for enteric pathogens).
Organism Referee Consensus
Participant Responses No. of
Participants
Aeromonas 100% Not identified in stool 31 Campylobacter 100% Not identified in stool 31 Negative by Immunoassay 6 Not detected 1 E. coli O157:H7 100% Not identified in stool 39 Plesiomonas 100% Not identified in stool 31 Salmonella 100% Not identified in stool 42 Not detected 1 Shigella 100% Not identified in stool 42 Not detected 1 Vibrio 100% Not identified in stool 34 Yersinia 100% Not identified in stool 36
NP-12: Sample contained Salmonella enterica subspecies enterica serotype Typhimurium>100,000 CFU/Loop, and Citrobacter freundii >100,000 CFU/Loop.
Organism Referee Consensus
Participant Responses No. of
Participants
Aeromonas 100% Not identified in stool 31 Campylobacter 100% Not identified in stool 31 Negative by Immunoassay 6 Not detected 1 E. coli O157:H7 100% Not identified in stool 39 Plesiomonas 100% Not identified in stool 31 Salmonella 100% Salmonella Typhimurium 21 Salmonella enterica 1 Salmonella species 19 Detected 1 Salmonella Enteritidis * 1 Not identified in stool * 1 Shigella 100% Not identified in stool 42 Not detected 1 Vibrio 100% Not identified in stool 34 Yersinia 100% Not identified in stool 36 * Incorrect result
Page 20 of 21 2015-BactiReg3 Event Notes
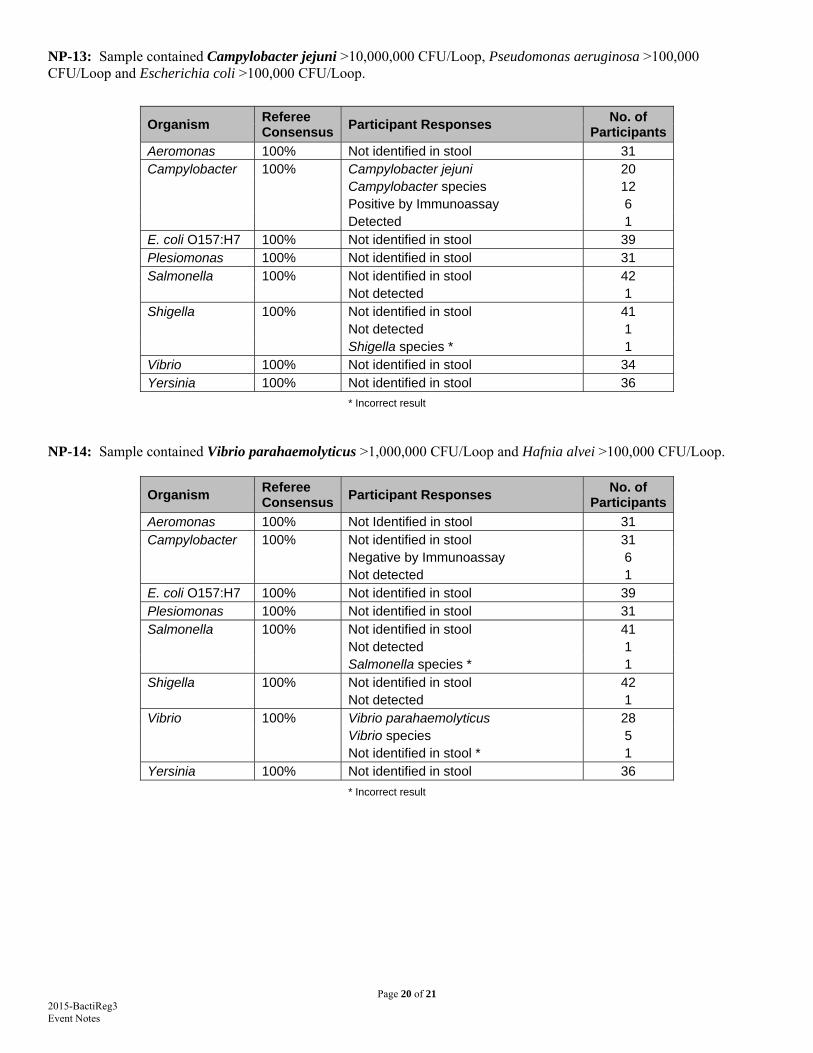
NP-13: Sample contained Campylobacter jejuni >10,000,000 CFU/Loop, Pseudomonas aeruginosa >100,000 CFU/Loop and Escherichia coli >100,000 CFU/Loop.
Organism Referee Consensus
Participant Responses No. of
Participants
Aeromonas 100% Not identified in stool 31 Campylobacter 100% Campylobacter jejuni 20 Campylobacter species 12 Positive by Immunoassay 6 Detected 1 E. coli O157:H7 100% Not identified in stool 39 Plesiomonas 100% Not identified in stool 31 Salmonella 100% Not identified in stool 42 Not detected 1 Shigella 100% Not identified in stool 41 Not detected 1 Shigella species * 1 Vibrio 100% Not identified in stool 34 Yersinia 100% Not identified in stool 36
* Incorrect result
NP-14: Sample contained Vibrio parahaemolyticus >1,000,000 CFU/Loop and Hafnia alvei >100,000 CFU/Loop.
Organism Referee Consensus
Participant Responses No. of
Participants
Aeromonas 100% Not Identified in stool 31 Campylobacter 100% Not identified in stool 31 Negative by Immunoassay 6 Not detected 1 E. coli O157:H7 100% Not identified in stool 39 Plesiomonas 100% Not identified in stool 31 Salmonella 100% Not identified in stool 41 Not detected 1 Salmonella species * 1 Shigella 100% Not identified in stool 42 Not detected 1 Vibrio 100% Vibrio parahaemolyticus 28 Vibrio species 5 Not identified in stool * 1 Yersinia 100% Not identified in stool 36 * Incorrect result
Page 21 of 21 2015-BactiReg3 Event Notes
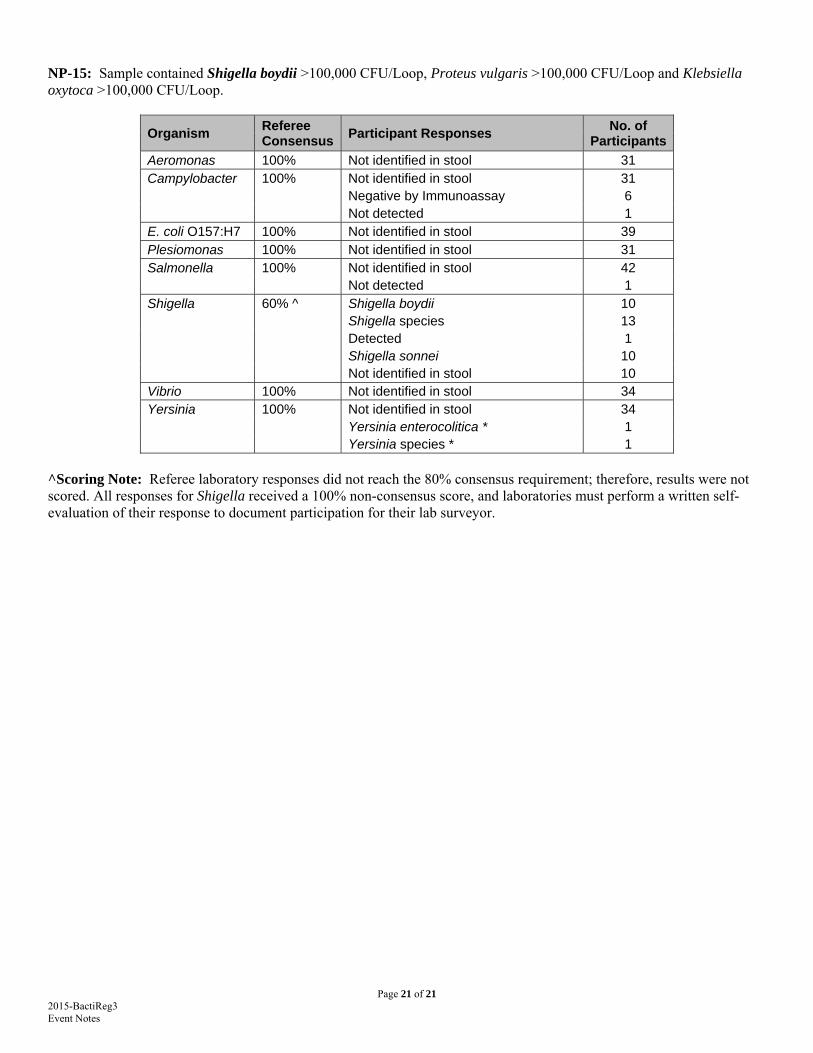
NP-15: Sample contained Shigella boydii >100,000 CFU/Loop, Proteus vulgaris >100,000 CFU/Loop and Klebsiella oxytoca >100,000 CFU/Loop.
Organism Referee Consensus
Participant Responses No. of
Participants
Aeromonas 100% Not identified in stool 31 Campylobacter 100% Not identified in stool 31 Negative by Immunoassay 6 Not detected 1 E. coli O157:H7 100% Not identified in stool 39 Plesiomonas 100% Not identified in stool 31 Salmonella 100% Not identified in stool 42 Not detected 1 Shigella 60% ^ Shigella boydii 10 Shigella species 13 Detected 1 Shigella sonnei 10 Not identified in stool 10 Vibrio 100% Not identified in stool 34 Yersinia 100% Not identified in stool 34 Yersinia enterocolitica * 1 Yersinia species * 1
^Scoring Note: Referee laboratory responses did not reach the 80% consensus requirement; therefore, results were not scored. All responses for Shigella received a 100% non-consensus score, and laboratories must perform a written self-evaluation of their response to document participation for their lab surveyor.
Related Documents











