© Copyright 2013 Elsevier, Ltd. All rights reserved. 2 Pressure on nerves CHAPTER CONTENTS Anatomy 21 Roots . . . . . . . . . . . . . . . . . . . . . . . . . . 22 Nerve plexus and nerve trunk . . . . . . . . . . . . . 23 Small peripheral nerve . . . . . . . . . . . . . . . . . 23 Terminology 23 Pain originating from the peripheral nerve system 23 Nociceptive pain . . . . . . . . . . . . . . . . . . . . 23 Neuropathic pain. . . . . . . . . . . . . . . . . . . . 24 Superficial dysaesthetic pain . . . . . . . . . . . . . 24 Behaviour of nervous tissue during pressure 24 Pain . . . . . . . . . . . . . . . . . . . . . . . . . . 24 Paraesthesia . . . . . . . . . . . . . . . . . . . . . . 25 Loss of function . . . . . . . . . . . . . . . . . . . . 25 Clinical syndromes 25 Small peripheral nerves . . . . . . . . . . . . . . . . 25 Nerve trunk/plexus . . . . . . . . . . . . . . . . . . . 25 Compression of the nerve root . . . . . . . . . . . . 26 Spinal cord . . . . . . . . . . . . . . . . . . . . . . . 26 Anatomy Peripheral nerves contain both neural and supportive elements. A large multifascicular nerve is composed of a number of dif- ferent bundles of nerve fibres or fasciculi (Fig. 2.1). These are bound together by the epineurium, a condensation of areolar connective tissue derived from the mesoderm. In humans, the epineurium normally constitutes 30–50% of the total cross- sectional area of the nerve bundle: it contains fibroblasts; col- lagen (types I and III); variable amounts of fat (possibly to cushion the nerve fibres it surrounds); lymphatic; blood vessels (vasa vasorum); and free nerve endings. In a monofascicular nerve, the epineurium only surrounds the fasciculus and is fused with the perineurium. The perineurium surrounds and protects one fascicle. It has two different layers; an outer collagen-rich connective one and an inner epithelial layer of contiguous cells. The perineurium has an important role in maintaining the osmotic milieu and fluid pressure within the endoneurium and also acts as a barrier against chemical and bacterial invasion. 1 The connective tissue of peri- and epineurium possesses blood and lymph vessels – the so-called vasa vasorum. 2,3 Also free nociceptive nerve endings which come from the related multifascicular nerve trunks are embedded in the perineurium and epineurium. 4,5 Enclosed in the perineurium is the fasciculus – a bundle of nerve fibres bound together and protected by the endoneu- rium. The latter consists of long collagen fibres running with the nerve fibres. The fibrous and cellular components of the endoneurium are bathed in endoneural fluid. 6 The nerve fibres are axons – the distal offshoots of nerve cells (Fig. 2.2). Most axons are surrounded by a myelin sheath formed from the compressed and concentric Schwann cell membranes. Axons range in diameter from 0.2 µm (small non- myelinated nociceptive axons) to 20 µm (large and myelinated efferent motor axons) and in length from 1 to 100 cm. They contain most of the cell volume. From central to peripheral, the nervous system can be clini- cally divided into four zones (Fig. 2.3): • The spinal cord • The spinal nerve, which contains fibres belonging to one segment • In the brachial and sacral area, and distal from the spinal ganglion, the different spinal nerves form a nerve plexus, from which originate the large multifascicular nerve trunks • Further distally the trunks split into peripheral nerves, with motor, sensory or combined function.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© Copyright 2013 Elsevier, Ltd. All rights reserved.
2 Pressure on nerves
CHAPTER CONTENTS
Anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Roots. . . . . . . . . . . . . . . . . . . . . . . . . . 22Nerve plexus and nerve trunk . . . . . . . . . . . . . 23Small peripheral nerve . . . . . . . . . . . . . . . . . 23
Terminology . . . . . . . . . . . . . . . . . . . . . . . . . 23
Pain .originating .from .the .peripheral .nerve .system . . . . 23
Nociceptive pain . . . . . . . . . . . . . . . . . . . . 23Neuropathic pain. . . . . . . . . . . . . . . . . . . . 24Superficial dysaesthetic pain . . . . . . . . . . . . . 24
Behaviour .of .nervous .tissue .during .pressure . . . . . . . 24
Pain . . . . . . . . . . . . . . . . . . . . . . . . . . 24Paraesthesia . . . . . . . . . . . . . . . . . . . . . . 25Loss of function . . . . . . . . . . . . . . . . . . . . 25
Clinical .syndromes . . . . . . . . . . . . . . . . . . . . . 25
Small peripheral nerves . . . . . . . . . . . . . . . . 25Nerve trunk/plexus. . . . . . . . . . . . . . . . . . . 25Compression of the nerve root . . . . . . . . . . . . 26Spinal cord. . . . . . . . . . . . . . . . . . . . . . . 26
Anatomy
Peripheral nerves contain both neural and supportive elements. A large multifascicular nerve is composed of a number of dif-ferent bundles of nerve fibres or fasciculi (Fig. 2.1). These are bound together by the epineurium, a condensation of areolar connective tissue derived from the mesoderm. In humans, the epineurium normally constitutes 30–50% of the total cross-sectional area of the nerve bundle: it contains fibroblasts; col-lagen (types I and III); variable amounts of fat (possibly to
cushion the nerve fibres it surrounds); lymphatic; blood vessels (vasa vasorum); and free nerve endings. In a monofascicular nerve, the epineurium only surrounds the fasciculus and is fused with the perineurium.
The perineurium surrounds and protects one fascicle. It has two different layers; an outer collagen-rich connective one and an inner epithelial layer of contiguous cells. The perineurium has an important role in maintaining the osmotic milieu and fluid pressure within the endoneurium and also acts as a barrier against chemical and bacterial invasion.1
The connective tissue of peri- and epineurium possesses blood and lymph vessels – the so-called vasa vasorum.2,3 Also free nociceptive nerve endings which come from the related multifascicular nerve trunks are embedded in the perineurium and epineurium.4,5
Enclosed in the perineurium is the fasciculus – a bundle of nerve fibres bound together and protected by the endoneu-rium. The latter consists of long collagen fibres running with the nerve fibres. The fibrous and cellular components of the endoneurium are bathed in endoneural fluid.6
The nerve fibres are axons – the distal offshoots of nerve cells (Fig. 2.2). Most axons are surrounded by a myelin sheath formed from the compressed and concentric Schwann cell membranes. Axons range in diameter from 0.2 µm (small non-myelinated nociceptive axons) to 20 µm (large and myelinated efferent motor axons) and in length from 1 to 100 cm. They contain most of the cell volume.
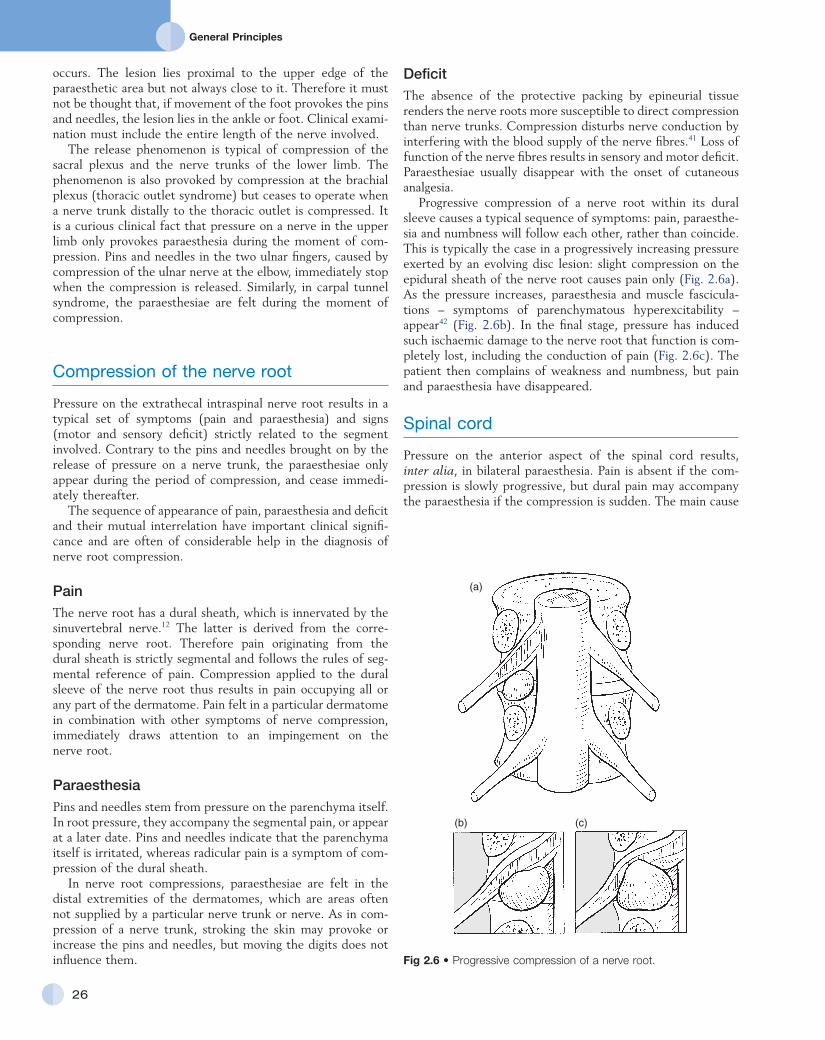
From central to peripheral, the nervous system can be clini-cally divided into four zones (Fig. 2.3):
• The spinal cord• The spinal nerve, which contains fibres belonging to one
segment• In the brachial and sacral area, and distal from the spinal
ganglion, the different spinal nerves form a nerve plexus, from which originate the large multifascicular nerve trunks
• Further distally the trunks split into peripheral nerves, with motor, sensory or combined function.
General Principles
22
Although the fasciculi, from their exit from the central nervous system to the distal extremity of the nerve, exhibit the general morphology summarized above, the structure and behaviour of the connective supportive elements differ consid-erably. This may explain the different clinical behaviour of a compressed cord, a compressed nerve root (within or without its dural sleeve), a compressed nerve trunk and a compressed small peripheral nerve.
Roots
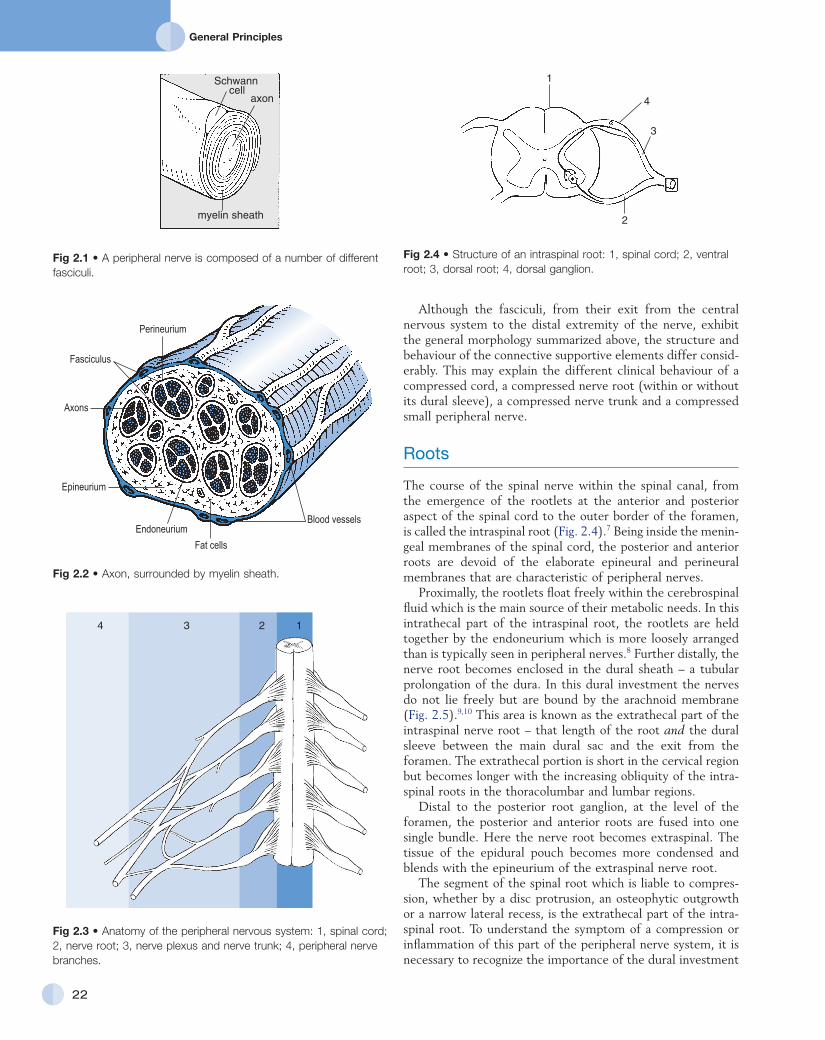
The course of the spinal nerve within the spinal canal, from the emergence of the rootlets at the anterior and posterior aspect of the spinal cord to the outer border of the foramen, is called the intraspinal root (Fig. 2.4).7 Being inside the menin-geal membranes of the spinal cord, the posterior and anterior roots are devoid of the elaborate epineural and perineural membranes that are characteristic of peripheral nerves.
Proximally, the rootlets float freely within the cerebrospinal fluid which is the main source of their metabolic needs. In this intrathecal part of the intraspinal root, the rootlets are held together by the endoneurium which is more loosely arranged than is typically seen in peripheral nerves.8 Further distally, the nerve root becomes enclosed in the dural sheath – a tubular prolongation of the dura. In this dural investment the nerves do not lie freely but are bound by the arachnoid membrane (Fig. 2.5).9,10 This area is known as the extrathecal part of the intraspinal nerve root – that length of the root and the dural sleeve between the main dural sac and the exit from the foramen. The extrathecal portion is short in the cervical region but becomes longer with the increasing obliquity of the intra-spinal roots in the thoracolumbar and lumbar regions.
Distal to the posterior root ganglion, at the level of the foramen, the posterior and anterior roots are fused into one single bundle. Here the nerve root becomes extraspinal. The tissue of the epidural pouch becomes more condensed and blends with the epineurium of the extraspinal nerve root.
The segment of the spinal root which is liable to compres-sion, whether by a disc protrusion, an osteophytic outgrowth or a narrow lateral recess, is the extrathecal part of the intra-spinal root. To understand the symptom of a compression or inflammation of this part of the peripheral nerve system, it is necessary to recognize the importance of the dural investment
Fig 2.1 • A peripheral nerve is composed of a number of different fasciculi.
axon
myelin sheath
Schwanncell
Fig 2.2 • Axon, surrounded by myelin sheath.
Blood vessels
Perineurium
Fasciculus
Axons
Epineurium
Endoneurium
Fat cells
Fig 2.3 • Anatomy of the peripheral nervous system: 1, spinal cord; 2, nerve root; 3, nerve plexus and nerve trunk; 4, peripheral nerve branches.
3 2 14
Fig 2.4 • Structure of an intraspinal root: 1, spinal cord; 2, ventral root; 3, dorsal root; 4, dorsal ganglion.
2
4
3
1

C H A P T E R 2Pressure on nerves
23
The fasciculi of plexus and trunks do not differ significantly from those of the roots or the peripheral nerves. The connec-tive support tissue, however, has some anatomical particulari-ties. Because the monofascicular spinal nerve changes into a multifascicular structure, there is an increased amount of epineurial tissue, forming a protective packing for the nerve tissue. The perineurium is also reinforced by elastin fibres. The fasciculi have an undulating course, whereas the collagen fibres run more longitudinally. This structure ensures that the nerve fibres are protected from mechanical deformation (compres-sion and elongation) during normal movements of the limbs.16 Although the epi- and perineurium contain nociceptive nerve endings, these seem to be relatively insensitive.17
Small peripheral nerve
A small peripheral nerve is the distal termination of a branching nerve trunk. The nerve ending is often monofascicular. The epineurium is then fused with the perineurium. Peripheral nerves can either have only a motor or a sensory function, or both can be combined. They all have nociceptive nerve endings in their supporting connective tissue.
Terminology
Lesions of the peripheral nervous system are characterized by a pathognomonic sensation: paraesthesia (‘pins and needles’). Although all tissues in the human body which contain nocicep-tive structures can be a source of pain, pins and needles will only arise when some part of the peripheral nervous system is at fault. Hence, the medical world tends to use the term ‘neu-ritis’ when pain is accompanied by pins and needles. Strictly, however, the suffix ‘-itis’ implies inflammation. Therefore the word neuritis should only be used when the peripheral nerve is affected by infectious or toxic irritation – i.e. there is an intrinsic disorder of the nervous parenchyma. Classically, these lesions are classified into mono- and polyneuritis. They are not discussed in this book, except in the shoulder region, where the clinical appearance of three mononeurites and neuralgic amyotrophy of the shoulder girdle is reviewed (see online chapter Nerve lesions and entrapment neuropathies of the upper limb).
When external pressure is applied to a normal nerve, pins and needles arise, although the nerve tissue is initially not inflamed. If the compression is not severe, the nerve continues to conduct normally. This situation of extrinsic pressure on a normal nerve is not a ‘neuritis’ and requires a totally different therapeutic approach. In this situation, the terms ‘pressure on nerve’ or ‘entrapment neuropathy’ are preferred.
Pain originating from the peripheral nerve system
Nociceptive pain
Peripheral nociceptors in the connective tissue of the periph-eral nerves are stimulated, and via Ad and C fibres of the nervi
– the nerve root sheath. The dural sheath has considerable sensitivity:11 it has many nociceptive nerve endings, especially at the anterior aspect where it receives its innervation from the sinuvertebral nerve belonging to the same segment.12–14 Pain arising from the dural sheath is segmental and obeys the rules of segmental reference of pain (see Ch. 1). There is no evidence that root pain arises from involvement of the axons. For example, pressure at the extraspinal nerve root, which misses the nerve root sleeve, as happens in some types of spondylolytic compression, causes not pain but only paraesthe-sia and neurological deficit.
From a clinical point of view, it is important to consider this structural duality: the outer investment is responsible for seg-mental pain, whereas the parenchymatous content is responsi-ble for the paraesthesia and the conduction deficits.
Nerve plexus and nerve trunk
Immediately distal to the foramen, the single fasciculus of the extraspinal root is enclosed in a thin, but strong, perineurial sheath, external to which is the epineurial areolar connective tissue. Within a few millimetres of its formation, the single fasciculus of the spinal nerve divides into several bundles which form the plexuses. Motor and sensory fibres of one nerve root mix, and more distally there is a redistribution of the fasciculi of various consecutive nerve roots.15 The brachial plexus is thus formed of the anterior rami of roots C5–T2, and the sacral plexus of the roots L2–S5. Distally, the fasciculi continue in the large nerve trunks of the limbs.
Fig 2.5 • Course of spinal nerve: A, intrathecal part of the nerve root; B, extrathecal part of the nerve root; 1, spinal cord; 2, ventral and dorsal rootlets; 3, spinal ganglion; 4, dura mater; 5, arachnoidea.
B A
1
4
2
3
4
5
4

General Principles
24
elements or any combination of these. Depending on the degree and the duration of compression, the effects can be subtle or can lead to displacement, deformity and morphologi-cal changes in the compressed tissue (neural tissue or neural support tissue).30
The clinical effects of nerve compression are pain, paraes-thesia and loss of function (see Box 2.2 for an overview of pressure on nerves).
Pain
The pain mechanism in entrapment phenomena is usually noci-ceptive: free nerve endings in the connective tissue of the nerve or in the dural investment of the nerve root are depolarized by application of mechanical forces or after exposure to irritating chemical substances, released from inflamed tissues.31 The pain stems from irritation of the support tissue enclosing the nerve fibres and only exceptionally does it result from pathological processes in the nerve tissue itself (neuropathic and dysaes-thetic pain). This has the following clinical consequences.
The pain will depend largely on the density of the nocicep-tive receptors in the support elements. It follows that the intensity of the pain depends not only on the intensity of compression but also on the localization along the course of the peripheral nerve. Pressure on a nerve root, for instance, will be more painful than an equal degree of force applied on a nerve plexus.
Because an external force acts first on the outer supporting structures of the nerve, pain will usually be the first symptom and it sometimes appears before involvement of the paren-chyma is present. A chronic but moderate pressure that is insufficient to impair conduction solely influences the outer structures and results in pain only. It is thus possible to have a completely normal examination of the peripheral nervous system, even though the patient does have nerve compression.32
nervorum conducted to the spinal cord and thence to the pain projection areas in the cortex.18 There are indications that most of the pain that stems from direct irritation of the peripheral nervous system is of nociceptive origin.19,20 ‘Nerve pain’ thus behaves identically to other peripheral pain,21 obeys exactly the rules of referred pain and is not to be distin-guished from pain of ligamentous, tendinous or arthrogenic origin (see Ch. 1).
Neuropathic pain
This type of pain, also called ‘de-afferentation or neuralgic pain’ is less common than nociceptive pain and results from prolonged damage to peripheral nerve tissue, such as avulsion, dissection or amputation.22 The pain is felt in the anaesthetic area, is continuous and burning and is independent of posture or movement, although local pressure can increase the pain considerably.23
Chronic damage or formation of scar tissue seems to provoke pain mechanisms without involvement of peripheral nocicep-tion. Also, the formation of a neuroma leads to increased sensitivity and spontaneous pain.24 Research on experimental neuromata has shown that regenerating axons have a spontane-ous excitability and an increased sensitivity to mechanical stimuli. An action potential in one axon probably leads to an impulse in a nearby axon. This mechanism of ‘cross-talking fibres’ accounts for the repetitive train of action potentials in a bundle of regenerating axons.25 A small stimulus thus leads to a self-perpetuating series of action potentials, and excessive and long-standing pain.26
Another mechanism that may account for neuropathic pain is the loss of inhibitory effects of the large diameter mechano-receptor afferents in a traumatized nerve. This leads to a relative increase of the activity from the small nociceptive afferents, and thus an opening of the gate at the dorsal horn.27 (see Ch. 1).
Superficial dysaesthetic pain
This type of pain is also rare, and is typical of diffuse polyneuri-tis, for example in diabetes,28 vitamin B1 deficiency or chemical irritation. Damage to small C fibres leads to sprouting of small offshoots in the regenerating axons. This leads to increased excitability, which results in unpleasant painful sensations during normal stroking of the skin (allodynia).29 The patient also complains of a burning feeling and ‘electrical sensations’ when the skin is gently touched (dysaesthesia), and there is also some analgesia (see Box 2.1 for an overview of neuro-genic pain).
Behaviour of nervous tissue during pressure
Entrapment of peripheral nerve tissue is defined as mechanical compression of the nerve, which includes the reduction of radial dimensions in the neural cells, the neural support
Box 2.1
Neurogenic pain
Nociceptive .pain• Common• Irritation of nociceptive structures in the connective support
tissues of the nerve• ‘Normal’ pain sensation, obeys the rules of segmental
reference
Neuropathic .pain• Rare• Results from damage to the nerve tissue• Intense pain, sharp, burning
Superficial .dysaesthetic .pain• Rare• Polyneuritis: irritation of C fibres• Dysaesthesia, allodynia and anaesthesia in the innervation area
of the peripheral nerve

C H A P T E R 2Pressure on nerves
25
Small peripheral nerves
Pressure on a small peripheral sensory nerve results in pain, paraesthesia and numbness. Pain is usually moderate and the main symptom is numbness. Together with some paraesthesia, these symptoms occupy the appropriate area of supply, which is usually well defined with clear-cut borders. The patient can tell precisely where the cutaneous analgesia is felt and where sensation is still normal. The centre of the region is often completely anaesthetic. A typical example is ‘meralgia paraes-thetica’, which results from compression of the lateral cutane-ous femoral nerve of the thigh.
Nerve trunk/plexus
Minor and intermittent pressure on a nerve trunk or a plexus causes paraesthesia and numbness. Sudden and serious tissue damage may provoke neuropathic pain. Constant pressure on a nerve trunk leading to parenchymatous damage does not usually provoke pain nor paraesthesia but only loss of motor and sensory function.
If the pressure is intermittent, a neurological deficit does not appear, even after many years. Paraesthesiae do not appear during the time of compression but only when the pressure on the nerve trunk has been released. It is common knowledge that pressure on the sciatic nerve while sitting causes only vague analgesia in the affected area or no symptoms at all. The shower of pins and needles then only appears when the subject relieves the pressure by standing up. The interval between the cessation of the pressure and the onset of the tingling depends on the duration of the compression: the longer the pressure is applied, the longer is the interval between the relief of pressure and onset of symptoms.
There is also a relation between the duration of compression and the duration of paraesthesia. Thus, after 15 minutes of pressure, the pins and needles appear 20–60 seconds after the release and last only 1 or 2 minutes. After release from 15 hours’ compression, paraesthesiae will probably appear only after an interval of some hours, then persist for 1 to 2 hours before recovering spontaneously. Cyriax39 calls this strange and hitherto unexplained phenomenon the ‘release phenomenon’ (see his p. 37). Lundburg and Rydevik have demonstrated that fluctuations in membrane permeability of the structures within the endoneurium are more noticeable when compres-sion on the nerve trunk is released and oedema appears, than during the compression of the nerve and its supplying blood vessels.40 This might explain the release phenomenon.
Another characteristic of paraesthesia induced by compres-sion at the level of the plexus is that active movements of the limb or the digits, or stroking over the analgesic area of skin usually brings on or increases the pins and needles. It is a common experience that the paraesthesia in the feet that comes on after relieving pressure on the sciatic nerve increases when the subject walks around or stamps the feet on the ground.
Paraesthesia and numbness are usually felt in the distal part of the cutaneous area supplied by the compressed plexus or nerve, no matter at what point in its course the compression
Paraesthesia
Pins and needles are pathognomonic of involvement of the peripheral nervous system in that the sensation cannot be produced in any way other than compression or inflammation of nerve tissue.33 Paraesthesiae are always felt in the cutaneous area supplied by the nerve tissue involved and distal to the site of the lesion. It is therefore extremely important to ascertain the precise site of the symptom, in that this helps to determine the site of compression.
Provocation of pins and needles by movements (distant movements or local pressure) or by stroking over the affected skin demonstrates an external origin for the symptoms. In primary afflictions of the peripheral nerve (neuritis), the pins and needles come and go spontaneously and movements do not influence them.
Loss of function
The epineurium and perineurium initially buffer the fasciculi from constrictive effects, but with a greater amount of compression, structural changes of the elements within the endoneurium follow.34 Recent research has demonstrated that the intraradicular oedema caused by alteration of the blood–nerve barrier is the most important factor in the nerve root dysfunction of chronic compression.35,36
Sometimes only the Schwann cells are affected, without damage to the axons. Destruction of the myelin sheath then results in loss of conduction. This type of lesion (lesion of Schwann cells without lesion of the axon fibre) is termed ‘neuropraxis’. If the compression has been only temporary, recovery of the Schwann cells will not take more than 2 weeks. This is the type of lesion responsible for the ‘Saturday night palsy’ seen after prolonged pressure on the radial nerve, or the ‘gardener’s palsy’ seen after prolonged traction on the peroneal nerve.
If considerable compression is maintained for a longer period, atrophy of the nerve tissue occurs and is followed by Wallerian degeneration of the distal part of the axon. Oedema, cellular proliferation and ingrowth of connective tissue also follows.37 If the compression is maintained for long periods, fibrotic degeneration appears at the site of the lesion, which makes recovery most unlikely.38
Clinical syndromes
Cyriax39 (see his pp. 37–39) distinguished four different syn-dromes in entrapment phenomena, corresponding to the site of compression along the peripheral nerve: at the small periph-eral sensory nerve, at the nerve trunk/plexus, at the nerve root and at the spinal cord (see Fig. 2.3).
Depending on the localization of compression, the periph-eral nervous system behaves differently. These differences are a major help to the clinician trying to ascertain the precise site of the lesion.
General Principles
26
DeficitThe absence of the protective packing by epineurial tissue renders the nerve roots more susceptible to direct compression than nerve trunks. Compression disturbs nerve conduction by interfering with the blood supply of the nerve fibres.41 Loss of function of the nerve fibres results in sensory and motor deficit. Paraesthesiae usually disappear with the onset of cutaneous analgesia.
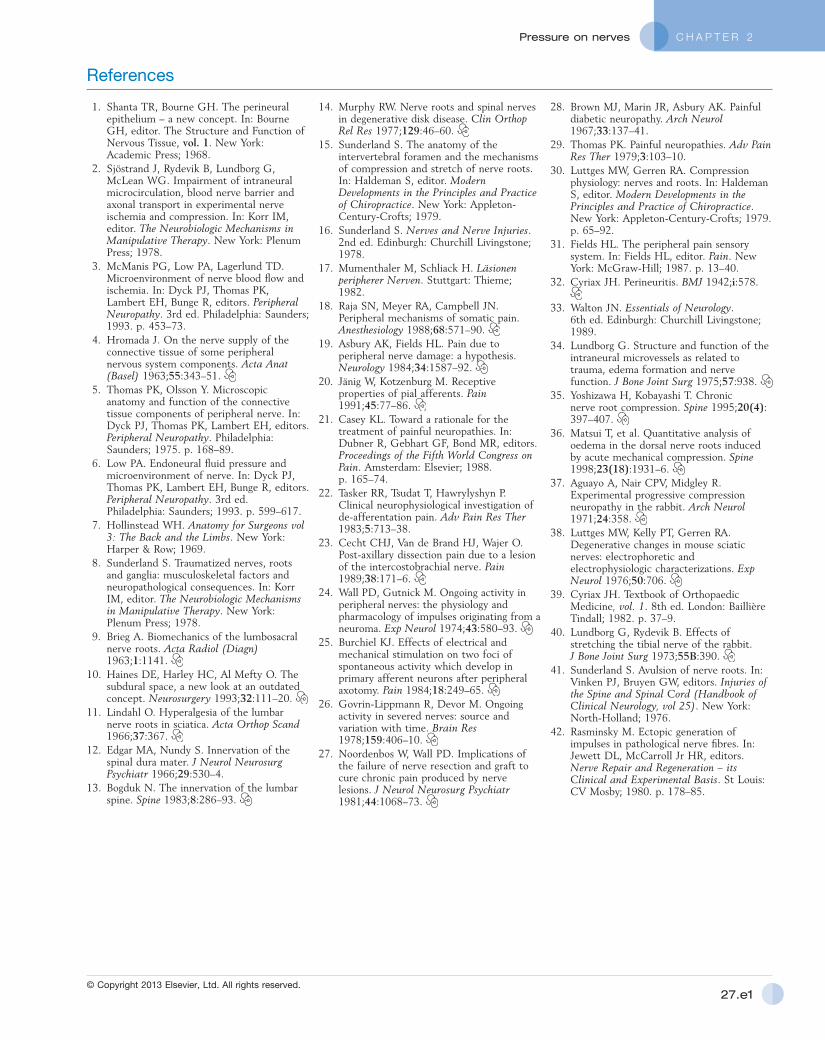
Progressive compression of a nerve root within its dural sleeve causes a typical sequence of symptoms: pain, paraesthe-sia and numbness will follow each other, rather than coincide. This is typically the case in a progressively increasing pressure exerted by an evolving disc lesion: slight compression on the epidural sheath of the nerve root causes pain only (Fig. 2.6a). As the pressure increases, paraesthesia and muscle fascicula-tions – symptoms of parenchymatous hyperexcitability – appear42 (Fig. 2.6b). In the final stage, pressure has induced such ischaemic damage to the nerve root that function is com-pletely lost, including the conduction of pain (Fig. 2.6c). The patient then complains of weakness and numbness, but pain and paraesthesia have disappeared.
Spinal cord
Pressure on the anterior aspect of the spinal cord results, inter alia, in bilateral paraesthesia. Pain is absent if the com-pression is slowly progressive, but dural pain may accompany the paraesthesia if the compression is sudden. The main cause
occurs. The lesion lies proximal to the upper edge of the paraesthetic area but not always close to it. Therefore it must not be thought that, if movement of the foot provokes the pins and needles, the lesion lies in the ankle or foot. Clinical exami-nation must include the entire length of the nerve involved.
The release phenomenon is typical of compression of the sacral plexus and the nerve trunks of the lower limb. The phenomenon is also provoked by compression at the brachial plexus (thoracic outlet syndrome) but ceases to operate when a nerve trunk distally to the thoracic outlet is compressed. It is a curious clinical fact that pressure on a nerve in the upper limb only provokes paraesthesia during the moment of com-pression. Pins and needles in the two ulnar fingers, caused by compression of the ulnar nerve at the elbow, immediately stop when the compression is released. Similarly, in carpal tunnel syndrome, the paraesthesiae are felt during the moment of compression.
Compression of the nerve root
Pressure on the extrathecal intraspinal nerve root results in a typical set of symptoms (pain and paraesthesia) and signs (motor and sensory deficit) strictly related to the segment involved. Contrary to the pins and needles brought on by the release of pressure on a nerve trunk, the paraesthesiae only appear during the period of compression, and cease immedi-ately thereafter.
The sequence of appearance of pain, paraesthesia and deficit and their mutual interrelation have important clinical signifi-cance and are often of considerable help in the diagnosis of nerve root compression.
PainThe nerve root has a dural sheath, which is innervated by the sinuvertebral nerve.12 The latter is derived from the corre-sponding nerve root. Therefore pain originating from the dural sheath is strictly segmental and follows the rules of seg-mental reference of pain. Compression applied to the dural sleeve of the nerve root thus results in pain occupying all or any part of the dermatome. Pain felt in a particular dermatome in combination with other symptoms of nerve compression, immediately draws attention to an impingement on the nerve root.
ParaesthesiaPins and needles stem from pressure on the parenchyma itself. In root pressure, they accompany the segmental pain, or appear at a later date. Pins and needles indicate that the parenchyma itself is irritated, whereas radicular pain is a symptom of com-pression of the dural sheath.
In nerve root compressions, paraesthesiae are felt in the distal extremities of the dermatomes, which are areas often not supplied by a particular nerve trunk or nerve. As in com-pression of a nerve trunk, stroking the skin may provoke or increase the pins and needles, but moving the digits does not influence them. Fig 2.6 • Progressive compression of a nerve root.
(a)
)c()b(

C H A P T E R 2Pressure on nerves
27
of spinal cord compression is spinal stenosis at the cervical or thoracic level. When the cord is compressed over the thoracic region, the paraesthesiae are felt only in the limbs. In compression at the cervical level, pins and needles will be present in all limbs or in the lower limbs only. The paraesthesiae are usually bilateral and extend beyond the borders of the areas of the cutaneous innervation of any spinal nerve, nerve trunk or peripheral nerve. For instance, the patient may complain of pins and needles in both hands and forearms at both aspects or in both legs from the knees to all the toes.
The symptoms are provoked neither by movements of the limbs nor by stroking the skin. Neck flexion is the only way to bring on the pins and needles (L’Hermitte’s sign). Together with the extrasegmental and bilateral dis-tribution of the painless paraesthesiae, positive neck flexion provides the clue to the diagnosis of incipient spinal cord compression.
Box 2.2
Pressure on nerves: SummaryPeripheral nerve Numbness > paraesthesia > pain
Clearly delineated areaNerve trunk Paraesthesia > numbness > pain
Vaguely delineated areaRelease phenomenon:—The pins and needles appear after the compression has ceased—There is a direct relation between the interval of onset and duration of compression
Nerve root Pain > paraesthesia > numbnessSegmental distribution of symptomsChronological sequence of symptomsCompression phenomenon:—The pins and needles appear during the compression
Spinal cord Completely painless (sometimes dural pain)Extrasegmentally and bilaterally distributed paraesthesiaPositive neck flexion Access the complete reference list online at
www.orthopaedicmedicineonline.com
C H A P T E R 2Pressure on nerves
27.e1© Copyright 2013 Elsevier, Ltd. All rights reserved.
References
1. Shanta TR, Bourne GH. The perineural epithelium – a new concept. In: Bourne GH, editor. The Structure and Function of Nervous Tissue, vol. 1. New York: Academic Press; 1968.
2. Sjöstrand J, Rydevik B, Lundborg G, McLean WG. Impairment of intraneural microcirculation, blood nerve barrier and axonal transport in experimental nerve ischemia and compression. In: Korr IM, editor. The Neurobiologic Mechanisms in Manipulative Therapy. New York: Plenum Press; 1978.
3. McManis PG, Low PA, Lagerlund TD. Microenvironment of nerve blood flow and ischemia. In: Dyck PJ, Thomas PK, Lambert EH, Bunge R, editors. Peripheral Neuropathy. 3rd ed. Philadelphia: Saunders; 1993. p. 453–73.
4. Hromada J. On the nerve supply of the connective tissue of some peripheral nervous system components. Acta Anat (Basel) 1963;55:343–51.
5. Thomas PK, Olsson Y. Microscopic anatomy and function of the connective tissue components of peripheral nerve. In: Dyck PJ, Thomas PK, Lambert EH, editors. Peripheral Neuropathy. Philadelphia: Saunders; 1975. p. 168–89.
6. Low PA. Endoneural fluid pressure and microenvironment of nerve. In: Dyck PJ, Thomas PK, Lambert EH, Bunge R, editors. Peripheral Neuropathy. 3rd ed. Philadelphia: Saunders; 1993. p. 599–617.
7. Hollinstead WH. Anatomy for Surgeons vol 3: The Back and the Limbs. New York: Harper & Row; 1969.
8. Sunderland S. Traumatized nerves, roots and ganglia: musculoskeletal factors and neuropathological consequences. In: Korr IM, editor. The Neurobiologic Mechanisms in Manipulative Therapy. New York: Plenum Press; 1978.
9. Brieg A. Biomechanics of the lumbosacral nerve roots. Acta Radiol (Diagn) 1963;1:1141.
10. Haines DE, Harley HC, Al Mefty O. The subdural space, a new look at an outdated concept. Neurosurgery 1993;32:111–20.
11. Lindahl O. Hyperalgesia of the lumbar nerve roots in sciatica. Acta Orthop Scand 1966;37:367.
12. Edgar MA, Nundy S. Innervation of the spinal dura mater. J Neurol Neurosurg Psychiatr 1966;29:530–4.
13. Bogduk N. The innervation of the lumbar spine. Spine 1983;8:286–93.
14. Murphy RW. Nerve roots and spinal nerves in degenerative disk disease. Clin Orthop Rel Res 1977;129:46–60.
15. Sunderland S. The anatomy of the intervertebral foramen and the mechanisms of compression and stretch of nerve roots. In: Haldeman S, editor. Modern Developments in the Principles and Practice of Chiropractice. New York: Appleton-Century-Crofts; 1979.
16. Sunderland S. Nerves and Nerve Injuries. 2nd ed. Edinburgh: Churchill Livingstone; 1978.
17. Mumenthaler M, Schliack H. Läsionen peripherer Nerven. Stuttgart: Thieme; 1982.
18. Raja SN, Meyer RA, Campbell JN. Peripheral mechanisms of somatic pain. Anesthesiology 1988;68:571–90.
19. Asbury AK, Fields HL. Pain due to peripheral nerve damage: a hypothesis. Neurology 1984;34:1587–92.
20. Jänig W, Kotzenburg M. Receptive properties of pial afferents. Pain 1991;45:77–86.
21. Casey KL. Toward a rationale for the treatment of painful neuropathies. In: Dubner R, Gebhart GF, Bond MR, editors. Proceedings of the Fifth World Congress on Pain. Amsterdam: Elsevier; 1988. p. 165–74.
22. Tasker RR, Tsudat T, Hawrylyshyn P. Clinical neurophysiological investigation of de-afferentation pain. Adv Pain Res Ther 1983;5:713–38.
23. Cecht CHJ, Van de Brand HJ, Wajer O. Post-axillary dissection pain due to a lesion of the intercostobrachial nerve. Pain 1989;38:171–6.
24. Wall PD, Gutnick M. Ongoing activity in peripheral nerves: the physiology and pharmacology of impulses originating from a neuroma. Exp Neurol 1974;43:580–93.
25. Burchiel KJ. Effects of electrical and mechanical stimulation on two foci of spontaneous activity which develop in primary afferent neurons after peripheral axotomy. Pain 1984;18:249–65.
26. Govrin-Lippmann R, Devor M. Ongoing activity in severed nerves: source and variation with time. Brain Res 1978;159:406–10.
27. Noordenbos W, Wall PD. Implications of the failure of nerve resection and graft to cure chronic pain produced by nerve lesions. J Neurol Neurosurg Psychiatr 1981;44:1068–73.
28. Brown MJ, Marin JR, Asbury AK. Painful diabetic neuropathy. Arch Neurol 1967;33:137–41.
29. Thomas PK. Painful neuropathies. Adv Pain Res Ther 1979;3:103–10.
30. Luttges MW, Gerren RA. Compression physiology: nerves and roots. In: Haldeman S, editor. Modern Developments in the Principles and Practice of Chiropractice. New York: Appleton-Century-Crofts; 1979. p. 65–92.
31. Fields HL. The peripheral pain sensory system. In: Fields HL, editor. Pain. New York: McGraw-Hill; 1987. p. 13–40.
32. Cyriax JH. Perineuritis. BMJ 1942;i:578.
33. Walton JN. Essentials of Neurology. 6th ed. Edinburgh: Churchill Livingstone; 1989.
34. Lundborg G. Structure and function of the intraneural microvessels as related to trauma, edema formation and nerve function. J Bone Joint Surg 1975;57:938.
35. Yoshizawa H, Kobayashi T. Chronic nerve root compression. Spine 1995;20(4):397–407.
36. Matsui T, et al. Quantitative analysis of oedema in the dorsal nerve roots induced by acute mechanical compression. Spine 1998;23(18):1931–6.
37. Aguayo A, Nair CPV, Midgley R. Experimental progressive compression neuropathy in the rabbit. Arch Neurol 1971;24:358.
38. Luttges MW, Kelly PT, Gerren RA. Degenerative changes in mouse sciatic nerves: electrophoretic and electrophysiologic characterizations. Exp Neurol 1976;50:706.
39. Cyriax JH. Textbook of Orthopaedic Medicine, vol. 1. 8th ed. London: Baillière Tindall; 1982. p. 37–9.
40. Lundborg G, Rydevik B. Effects of stretching the tibial nerve of the rabbit. J Bone Joint Surg 1973;55B:390.
41. Sunderland S. Avulsion of nerve roots. In: Vinken PJ, Bruyen GW, editors. Injuries of the Spine and Spinal Cord (Handbook of Clinical Neurology, vol 25). New York: North-Holland; 1976.
42. Rasminsky M. Ectopic generation of impulses in pathological nerve fibres. In: Jewett DL, McCarroll Jr HR, editors. Nerve Repair and Regeneration – its Clinical and Experimental Basis. St Louis: CV Mosby; 1980. p. 178–85.
Related Documents











