2-3 OTTOBRE 2009 IL LABORATORIO NELLE URGENZE ED EMERGENZE Gestione POCT: punto di vista clinico. Università degli Studi di Roma TOR VERGATA Dott.ssa Manuela Moresco Anestesia e Rianimazione

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2-3 OTTOBRE 2009
IL LABORATORIO NELLE URGENZE ED
EMERGENZE
Gestione POCT: punto di vista clinico.
Università degli Studi
di Roma
TOR VERGATA
Dott.ssa Manuela Moresco
Anestesia e Rianimazione


Modern concept of coagulation

The Cell-based Model of Coagulation
VIIIaIXa
Hoffman M & Munroe DM. A cell-based model of hemostasis.Thromb Haemost 2001; 85: 958-965
+ activates various factors
Initiation
Amplification
Propagation

Haemoscope Thrombelastograph® Haemostasis
Analyser (TEG®)

Historical notes
• Developed by Hartet in Heidelgerg, Germany 1948
• Clinical practice by Kang in the setting of liver
transplantation at Pittsburg, USA 1985

Relationship between conventional
tests and post-operative bleeding
Predictive values for post operative
bleeding & re-operative rates
Activated clotting time = 30 %
Coagulation profile = 50 %
Thrombelastograph® = 87 %
Spiess et al. J.Clin Monitor 1987; 3

TEG® Applications
– Liver transplants
– ICU
– Cardiac Surgery
– Vascular Surgery
– Cath lab
– Trauma
– Orthopedics
– Obstetrics
– Gyneacology
– Burn wound unit
– Etc...

Detection of
– Heparin Effect
(Hepcon HMS-plus or Hemocron-response)
– LMWH Effect
– Warfarin Effect
– rFVIIa Effect
– ATIII Deficiency
(heparin-resistance; Hepcon HMS-plus or Hemocron-response)
– Functional Fibrinogen & Platelet Contribution
– Fibrinolysis (primary and secondary)

TEG® Technology

TEG is a global assessment of hemostatic
function
Parameters of TEG analysis
• r = coagulation activation
• k = dynamics of clot formation
• angle = kinetics of fibrin cross-linking
• MA = strenght of a clot
• Ly 30,60 = stability of the clot

R R é il tempo di latenza dal momento di inserimento del campione di sangue
nel TEG® fino alla formazione iniziale di fibrina.
L’angolo misura la rapidità (cinetica) di formazione di fibrina e del cross-
linking, cioé della velocità con cui si rinforza il coagulo.
K K é il tempo necessario a raggiungere un certo livello di forza del coagulo
MA MA, o Massima Ampiezza, é funzione diretta delle massime proprietà
dinamiche dell’aggregazione fibrine-piastrine via GPIIb/IIIa e rappresenta la forza
finale del coagulo.
LY30 LY30 misura la percentuale di riduzione dell’ampiezza 30 minuti dopo
l’MA. Questa misura indica la stabilità del coagulo.
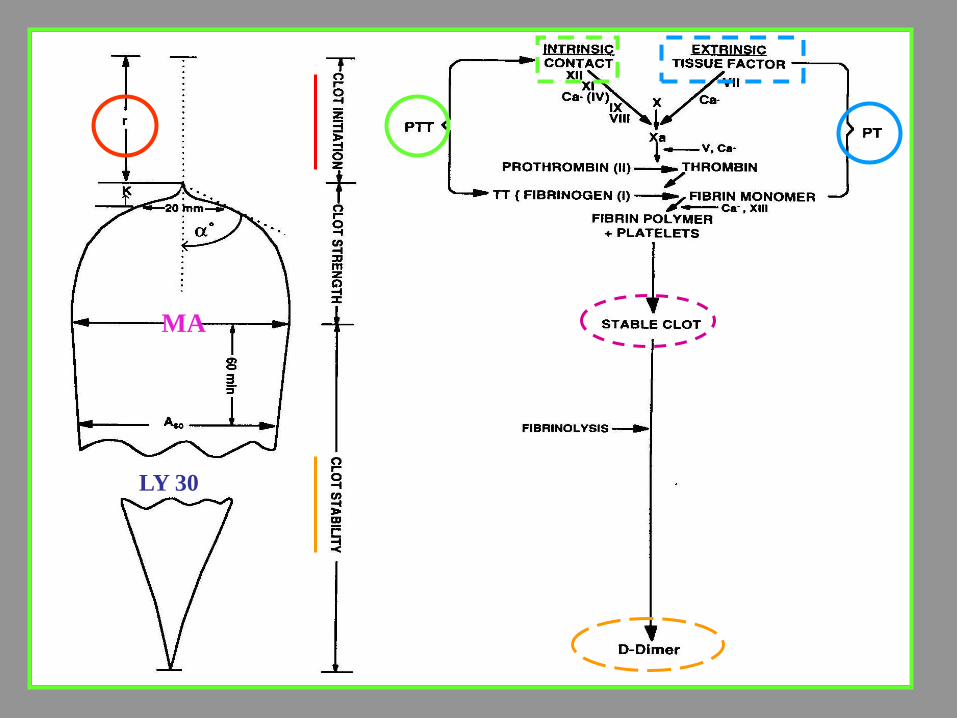
PARAMETRI DEL TEG

r

Parameters of TEG analysis
R (or R-Time) = Reaction time
• time from start of measurement until the beginning of
clot formation
• explores the enzimatic part of coagulation
• prolonged by anticoagulants and factor
deficiencies
• shortened by hypercoagulable conditions

r k
20mm

Parameters of TEG analysis
K (or K-time) = Clot growth kinetics
• time from the beginning of clot formation until a fixed
level of clot firmness (amplitude of 20 mm) is reached
• explores the kinetics of clot formation
• is related to platelet function and plasma components
• prolonged by anticoagulants that affect fibrinogen
and
platelet function
• shortened by increased levels of fibrinogen and
platelet function

r k

Parameters of TEG analysis
(or angle)
• explores the rate of clot growth
• function of rate of polymerization
• expression of fibrinogen level
• prolonged by anticoagulants that affect fibrinogen and
platelet function
• shortened by increased levels of fibrinogen and
platelet function

r
MA
k

Parameters of TEG analysis
MA = Maximum Amplitude
• maximum strenght of the developed clot
• ability of the clot to form hemostasis
• depends
- on adequate fibrin formation and polymerization
in a 3D network and
- on its interaction with platelet via the Gp IIb/IIIa
receptor

Parameters of TEG analysis
MA = Maximum Amplitude
• conventional coagulation tests (PT, aPTT) are based
only on the time of onset of clot formation
• blood clot firmness is an important parameter
for in-vivo haemostasis because the clot must
stand the shear stress at the site of vascular injury

Parameters of TEG analysis
G
• 5000 A / (100 - A) dyn/cm2
• elastic shear modulus
• measures the resistance of clot to deformation

Parameters of TEG analysis
CI = Coagulation Index
• derived from r, k, MA and
• describes global balance of coagulation
• CI > + 3 = hypercoagulation
• CI < - 3 = hypocoagulation

r
MA
k
30 min
LY30

Parameters of TEG analysis
LY30, LY60 = Clot stability
• measures the percentage change in clot strenght at 30
or 60 min after MA
• refers to the potential of the clot to redissolve as a
result of circulating fibrinolytic activators which activate
the plasminogen incorporated in the clot
• LY30 > 7,5% hyperfibrinolysis
MA
LY 30
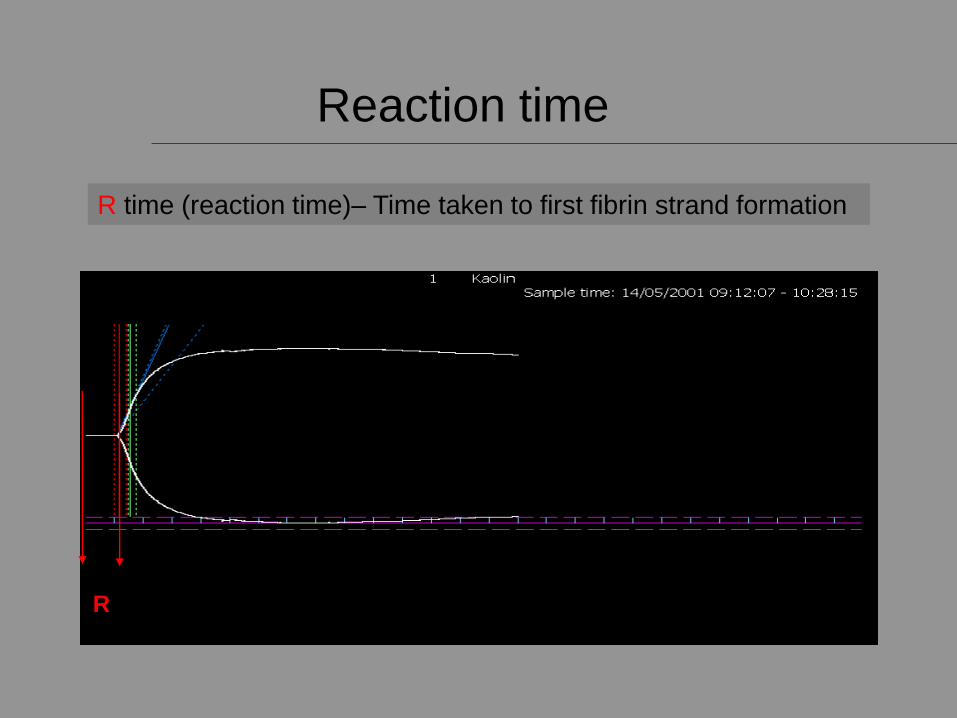
R time (reaction time)– Time taken to first fibrin strand formation
Reaction time
R

K & Angle
K & – Reflect the kinetics of the interaction of fibrin/fibrinogen with platelets
K=Time to reach amplitude of 20mm

MA
MA, maximum clot strength
MA- Maximum Amplitude – Reflects the ultimate strength of the clot due to fibrin/fibrinogen interaction with the GPIIb/IIIa receptor on
functioning platelets

Normal Tracing

Elongated R

Elongated R
• Intrinsic contact pathway inibition (aprotinin)
• Tissue factor inibition
• Warfarin therapy
• FXa inibition (LMWH)
• Low prothrombin level
• Thrombin inibition (HMWH; r-irudin; etc.)
• Low fibrinogen level
• Hypothermia
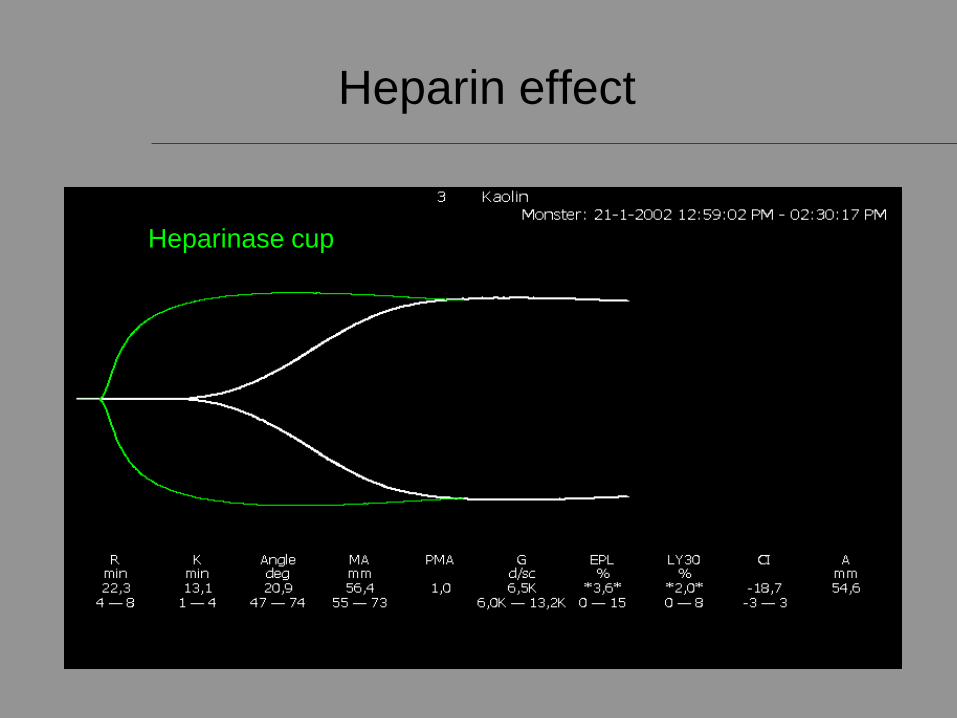
Heparinase cup Plain cup
Heparin effect

Low platelet function

Fibrinolysis

Secondary Fibrinolysis

Hypercoagulability

Timing for the use of heparinase and
TEG in cardiac surgery
• Pre-CPB
• Shortly before the termination of CPB (with heparinase)
• 10 minutes and 60 minutes after protamine administration (with and without heparinase)
In case of elongated R-time TEG with heparinase or HMS-plus for detection of HMWH!
Ho AM et al. 2003 Jun;17(3):413-14

TEG Pattern Recognition

TEG trace in cardiac surgey
Pre-CPB
During CPB (test without heparinase)
During CPB (test with heparinase)
Colella D, MD

LMWH and TEG
12 h after LMWH withdrawal
Colella D, MD

Coumadin
Coumadin BaseCoumadin Base

Coumadin 24 ore

Coumadin 36 ore

Summary
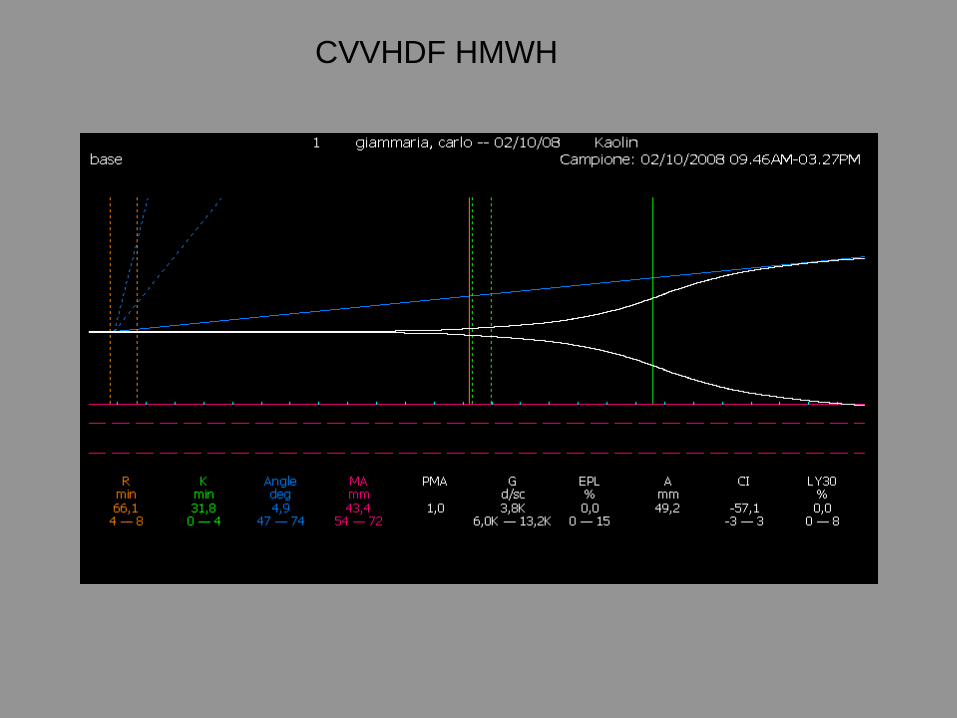
CVVHDF HMWH




Elongated R (test with heparinase: neg)
Hepcon HMS-plus: no residual HMWH
PT= 60% (15’’) INR= 1,45
APTT= 32,5’’ RATIO= 0,9
Fibrinogen= 254 mg/dl
PLT= 294000/mmc
ACT= 145’’
Postoperative bleeding

Post infusion of 5 units of platelets
Still bleeding!
4 units of FFP

Post infusion of 1000 IU prothrombin complex concentrate
(VII, IX, X)
Stop bleeding!

Ticlopidine and TEG
Colella D, MD

Aspirin
Colella D, MD
TEG selective analysis of effects of
platelet inhibiting drugs on ADP, AA and
IIb/IIIa receptors
New Developement: Platelet Mapping™

Materials and methods
• Clear “cup and pin” and/or blue
(heparinase) “cup and pin”
• Kaolin
• Novel activator (P1)
• ADP (P2)
• Arachidonic acid AA (P3)
Colella D, MD

Channel 1
•Whole blood
•Kaolin
Channel 2
•Whole blood
• Heparin
•Novel activator
Channel 3
•Whole blood
•Heparin
•Novel activator
•ADP
Channel 4
•Whole blood
•Heparin
•Novel activator
•AA
Max MA using
commonly protocol
with Kaoline
Unique
contribution of
fibrin to MA
Contribution to MA
of fibrin and
uninhibited platelets
by ADP or IIbIIIa
inhibitors
Contribution to
MA of fibrin and
uninhibited
platelets by NSAID
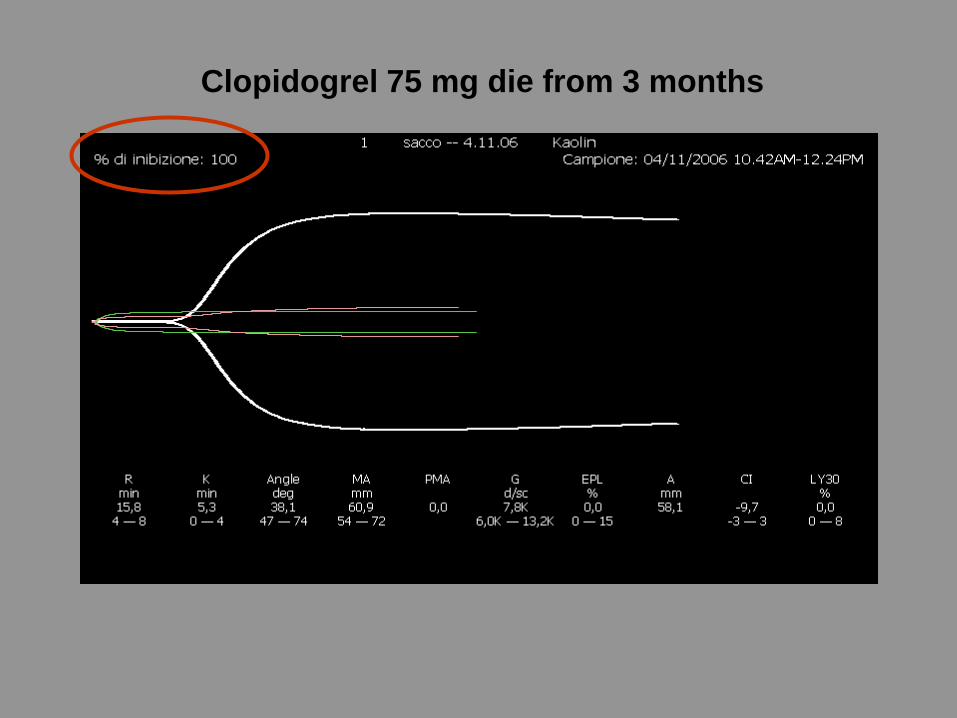
Clopidogrel 75 mg die from 3 months

Case report 1

• 54 years, male, 65 kg, 168 cm
Diagnosis:
• AMI with previous PCI
• CAD: LM with unstable angina
• Type II diabete mellitus
• Dyslipidemia ??

Preoperative therapy
• -blockers
• Ace-inhibitors
• Aspirin 100 mg
• Atorvastin 20 mg
• Clopidogrel 75 mg (for 3 months)
• HMWH 1000 IU/h

Standard coagulation tests
PLT count: 150k
pT: 14,3 s
INR: 1,3
aPTT: 80 s
ACT: 190 s
Fibr: 350 mg/dL
ATIII: 84%

Is clopidogrel really working?
Which kind of tests can we perform?

What intraoperative interventions
could we perform to optimize the
patient’s coagulation status?
Pharmacologic agents CPB technologies

Heparin effect
R=15,6
TEG trace with heparin
TEG trace with heparinase

Clopidogrel effect (ADP)
Novel activator (no thrombin platelet activity; fibrin contribution only)
ADP (decreased activity 27,1 %)
Thrombin (max platelet activity)

Aspirin effect (AA)
Thrombin (max platelet activity)
AA P3 (decreased activity 95,8 %)
Novel activator (no thrombin platelet activity; fibrin contribution only)

Comments
• Heparin efficacy (prolonged R time; 15.6 min)
• Strong (95.8%) aspirin contribution to % MA
reduction
• Very low efficacy (27.1%) of clopidogrel to % MA
reduction
(statins therapy or genetic resistance)
Clopidogrel resistance is associated with increased risk of recurrent
atherothrombotic events in patients with acute myocardial infarction.
Matetzky S et al. Circulation 2004,109
Contribution of hepatic P450 3A4 metabolic activity to the phenomen
of clopidogrel resistance. Lau WC et al. Circulation 2004,109

Case report 2

• 67 years, male, 70 Kg, 173 cm
• PCI procedure for STEMI
(intra-stent restenosis)

Preoperative therapy
• -blockers
• Ace-inhibitors
• Aspirin 100 mg
• Atorvastin 20 mg

Standard coagulation tests
PLT count: 220k
pT: 12,8 s
INR: 1,1
aPTT: 31 s
ACT: 145 s
Fibr: 380 mg/dL
ATIII: 110%

• Abciximab (Reopro) 18 mg bolus iv
• Abciximab (Reopro) 10 mcg/Kg/hr
Periprocedure therapy

Failed PTA
Need for CABG on CPB(Normothermic CPB, Coated circuits, Heparin dose-
response test, Tranexamic acid 15mg/kg)

Platelet mapping on TEG
Novel activator (no thrombin platelet activity; fibrin contribution only)
Thrombin (max platelet activity)
ADP/Reopro (decreased activity 81%)

• Strong contibution of abciximab to % MA
reduction (81%)
Comments

Suggested treatment (cardiac surgery)
anticoagulant of choiceProthrombotic stateLY30 < 7.5%, C.I. > 3.0
anticoagulant of choiceSecondary fibrinolysisLY30 at 7.5% or greater, C.I. > 3.0
antifibrinolytic of choicePrimary fibrinolysisLY30 at 7.5% or greater, C.I. < 3.0
.06 u/kg cryo fibrinogen levelless than 45
x10 platelet units platelet functionMA at 40 mm or less
x5 platelet units platelet functionMA between 41 -48 mm
0.3mcg/kg DDAVP platelet functionMA between 49 -54 mm
x 4 FFP or 16 ml/kg clotting factorsR greater than 14 min
x 2 FFP or 8 ml/kg clotting factorsR between 11-14 min
x 1 FFP or 4 ml/kg clotting factorsR between 7 - 10 min
Suggested TreatmentClinical causeTEG® value
Treatment protocol
Shore-Lesserson L et al. Anest Analg 1999


• TEG is very sensible to the presence of HMWH
• TEG is a very sensible test but does not identify
any specific alteration of clotting factors
• TEG parameter MA is both a sensible and
specific test for platelet dysfunction
• TEG is both a sensible and specific test for
fibrinolysis

Conclusions II
• Modified TEG
- native whole-blood
- celite
- kaoline
- heparinase
- ADP, AA and novel activator (Platelet Mapping)
- tissue factor (Hemoliance)
- abciximab
- ATIII (heparin resistance detection)
- urokinase
- heparinase/abciximab
- heparinase/fresh frozen plasma
- in vitro effect of colloids, cristalloids, plasma, amniotic fluid etc

LAVORIAMO INSIEME !!!!!!!!!!!!!!!!!!!!!
GRAZIE !!!!!!!
Related Documents











