Winter 1999 ❤ ❤ Get Pumped! Get Pumped! ~ HEART Health Information Inside ~ ~ HEART Health Information Inside ~ Take the road to a healthy heart Take the road to a healthy heart

1999 - Winter
Mar 11, 2016
Heart Health
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Winter 1999
❤❤Get Pumped!Get Pumped!
~HEART Health Information Inside~~HEART Health Information Inside~
Take the roadto a
healthy heart
Take the roadto a
healthy heart

In the past several months, the U.S. Senate and the
U.S. House of Representatives have passed their own
versions of so-called Patients’ Bill of Rights legislation.Much of the debate in Washington has been fueled
by anecdotal HMO (health maintenance organization)
horror stories and accusations that the insuranceindustry opposes any legislation benefiting consumers.
Actually, there are several matters addressed in proposed
legislation with which Arkansas Blue Cross and BlueShield agrees in concept. They include: a grievance
process, mandatory Point-of-Service, direct access to
certain specialists, internal and external appeals, accessto emergency care, coverage for participation in clinical
trials, patient access to information, prohibitions on gag
clauses, and improper incentive arrangements.In general the House and Senate bills have major
differences both in scope and impact. Each bill is
hundreds of pages long and clearly subject to differinginterpretations. Following is a short explanation of some
of the highlights of each measure:
• Senate VersionMany provisions contained in the Senate measure,
called the Patients’ Bill of Rights Plus Act, apply to the
48 million Americans covered by plans regulated only
by federal law. These are called ERISA (EmployeeRetirement Income Security Act) plans and are provided
through employers. The Senate and House bills both
require plans to have an internal appeals process. Underthe Senate bill, enrollees also would have access to an
independent external review of certain questions of
medical necessity, experimental and investigationaltreatments. The decision of the independent reviewer
would be binding on the insurance plan. The Senate
measure does not expand the right to sue health plans,as does a controversial provision contained in the
House measure.
• House VersionOn the House side, the Bipartisan Consensus
Managed Care Improvement Act of 1999 applies to allindividuals with private health insurance and expands
the right to sue health plans on a wide range of issues.
Patients could sue in state or federal courts for unlimiteddamages. If the current pre-emption for ERISA plans is
removed as proposed, lawsuits could be filed in state or
federal court for unlimited damages. Because ERISAplans are regulated only under federal law they currently
are exempt from state actions. Employers are concerned
that the cost of providing insurance for their employeesmay increase substantially because of the direct or
indirect cost of increased legal liability. The increased
costs may cause employers to stop offering such benefitsand result in more uninsured workers.
In addition to various access issues, both bills also
would allow self-employed individuals to deduct the cost
of health insurance. A new deduction for long-term careand the expansion of medical savings accounts also are
among the provisions contained in both measures.
Because the bills are quite different, a conferencecommittee comprised of members appointed by the
House and Senate leadership has been created. These
lawmakers are charged with attempting to work out acompromise measure, a process that may not begin until
after Congress returns in January. Two members of the
Arkansas Congressional delegation, Republican Sen.TimHutchinson and Democrat Rep. Marion Berry have been
selected to serve on the conference committee.
If you would like further information on theseimportant bills, please contact us at (501) 378-2131.
On the “Patients’ Bill of Rights”On the “Patients’ Bill of Rights”
CONGRESSIONAL UPDATE

3
is published four times a year by theArkansas Blue Cross and Blue ShieldAdvertising and CommunicationsDivision for the company’s mem-bers, health care professionals andother persons interested in health
care and wellness. Opinions expressed herein do not necessar-ily reflect the views of Arkansas Blue Cross and Blue Shield orany of its publics.
Vice President of Advertising and CommunicationsPatrick O’Sullivan
EditorKelly Whitehorn
DesignerGio Bruno
ContributorsMark Carter, Damona Fisher, Kathy Luzietti and Greg Russell
Customer Service Numbers
Little Rock Toll-freeCategory Number (501) Number
State/Public School Employees 378-2437 1-800-482-8416
e-mail: [email protected]@arkbluecross.com
Medi-Pak (Medicare supplement) 378-3062 1-800-338-2312
Medicare (for beneficiaries only): Part A (hospital benefits) 378-2173 1-800-482-5525 Part B (physician’s benefits) 378-2320 1-800-482-5525
UniqueCare, UniqueCare Blue, Blue Select® (individual products) 378-2010 1-800-238-8379
Group Services 378-5579 1-800-421-1112
BlueCard® 378-2127 1-800-880-0918
Federal Employee Program (FEP) 378-2531 1-800-482-6655
Health Advantage 221-3733 1-800-843-1329
Medi-Pak HMO (Health Advantage) 954-5200 1-800-354-9904
USAble Administrators 378-3600 1-800-522-9878
Numbers to call for information about obtainingcoverage:
Little Rock Toll-freeCategory Number (501) Number
Medi-Pak (Medicare supplement) 378-2937 1-800-392-2583
UniqueCare Blue, Blue Select® (individual products) 378-2937 1-800-392-2583
Medi-Pak HMO (Health Advantage) 378-6987 1-800-588-5706
Regional Office locations:Central Little RockNortheast JonesboroNorthwest FayettevilleSouth Central Hot SpringsSoutheast Pine BluffSouthwest TexarkanaWest Central Fort Smith
Customers who live in these regions may contact theregional offices or call the appropriate toll-free telephonenumber listed above.
INSIDETHIS ISSUE
~WINTER 1999~
Risks and signs of a heart attack ................ 4The brain attack (or stroke) ............................ 5Heart-healthy eating .................................... 6Exercise for your heart ................................ 7High blood pressure/cholesterol info ........... 8How to kick the smoking habit .................... 9Focus on Heart Health (dental care, aspirin,congestive heart failure) ................................... 10Children’s health tips................................. 11Shot Dodgers ............................................. 11Women’s Health and Cancer Rights Act ..... 11Preventive Health Guidelines................ 12-13Can we afford escalating drug costs? ....... 14Health Advantage scores well on survey ... 15Leading the Way(get to know some of Arkansas’ legislators) ....... 16-17MENTOR program ....................................... 18Hansel and Gretel ...................................... 18Blue & Your Community ............................. 19Clearly Blue(a guide to health insurance terminology) ............... 20
4
The heart health information for this issueof Blue & You was provided by the AmericanHeart Association. For more information onheart disease — and heart health — pleasecontact the nearest chapter of the AmericanHeart Association or call 1-800-AHA-USA1(1-800-242-8721) or visit them on-line atwww.americanheart.org.
HEART ATTACK WARNING SIGNS
If you experience one or
more of these heart attack warning
signs, get help immediately.
• Uncomfortable pressure,
fullness, squeezing or pain in
the center of the chest lasting
more than a few minutes.
• Pain spreading to
the shoulders, neck or arms.
• Chest discomfort
with lightheadedness,
fainting, sweating,
nausea or shortness
of breath.
You are having trouble breathing. You have a shooting pain in your left arm. You feellike an elephant is sitting on your chest. Chances are, you are having a heart attack.
Each year, approximately 1.5 million people in the United States have a heart attack —and 500,000 of those die. Heart attacks claim more lives than any other single cause.
There are some risk factors for a heart attack that you can’t control. They are increasingage, gender (men are more at risk than women), race (African-Americans and otherminority groups are more likely to have high blood pressure than white Americans),diabetes, and family medical history.
Risk factors you can control include smoking, high cholesterol, high blood pressure,obesity, physical inactivity and diet.
What is a heart attack?Heart attacks result from blood vessel disease in the
heart. A heart attack occurs when the blood supplyto part of the heart muscle itself is severelyreduced or stopped. If the blood supply iscut off severely or for a long time, musclecells suffer irreversible injury and die.Disability or death may result. Butheart attacks may be stopped inprogress and muscle damagereduced if they’re treated within afew (usually one to three) hours.
To reduce your risk of a heartattack, remember the following:• Do not start smoking. If you smoke, quit.• Recognize and treat high blood pressure and diabetes.• Don’t drink too much alcohol.• Be physically active.• Eat a healthful diet.• Have regular medical checkups. ❤
The heart attackTelltale risks and signs can help you detect this potential killer
W O M E NAND HEART DISEASE
Each year, cardio-vascular diseases killmore women than allforms of cancer, chroniclung disease, pneumonia,diabetes, accidents andAIDS combined.
There are some riskfactors you cannotcontrol, such asincreasing age, familyhealth history andrace.Your risk of heartdisease is greater ifclose members of yourfamily have had heartdisease. African-Americans have agreater risk ofdeveloping heart diseasethan white Americansbecause they typicallyhave higher bloodpressure levels. African-American women, infact, have a death ratefrom high blood pres-sure that is almost fivetimes higher than therate for white women.
The risk factors youcan change are smoking,high cholesterol, highblood pressure andphysical inactivity.

5
STROKE WARNING SIGNS
• Sudden weakness or numbness
of the face, arm or leg on one side
of the body.
• Sudden dimness or loss of vision,
particularly in one eye.
• Loss of speech, or trouble talking
or understanding speech.
• Sudden severe headaches with
no known cause.
• Unexplained dizziness,
unsteadiness or sudden
falls, especially
along with any of
the previously
mentioned
symptoms.
When considered separately from other cardiovascular diseases, stroke (or brainattack) ranks as the third-leading cause of death — behind diseases of the heart and cancer.On average, someone in the United States has a stroke every 53 seconds.
While the elderly population account for the majority of stroke deaths, stroke ranksthird as a cause of death among middle-aged people.
However, there is some good news, thanks to improvements in medical care for strokesurvivors. The age-adjusted death rate for stroke in the United States has been steadilydeclining, dropping from 89 per 100,000 in 1950 to 18 per 100,000 in 1990.
Some risk factors for a stroke are genetically determined, others are simply a function ofnatural processes, but still others result from a person’s lifestyle.
Factors that can’t be changed include: increasing age, gender, race, diabetes, a prior stroke and heredity. Risk factors that can be changed include: smoking, elevated blood cholesterol and lipids, physical inactivity and obesity, drinking too much alcohol and drug abuse.
What is a stroke? Stroke is the No. 1 cause of disability and the third leading cause of death in the United States. A stroke is similar to a heart attack, but it happens in the brain. It occurs when a blood vessel bringing oxygen and nutrients to the brain bursts or is clogged by a blood clot or some other particle. The affected part of the brain doesn’t get the blood it needs and in minutes begins to die. Approximately 10 percent of brain attacks are preceded by “temporary strokes” or transient ischemic attacks (TIAs). These may occur days, weeks or even months before a major stroke. TIAs result when a blood clot temporarily clogs an artery and part of the brain doesn’t get the supply of blood it needs. The symptoms may occur rapidly and last a relatively short time, usually from a few minutes to several hours. The usual symptoms are like those of a full-fledged brain attack, except that they are temporary, lasting 24 hours or less. ❤
The brain attackA stroke can strike anyone: know your risk factors
Stroke is
the third
leading cause
of death
in the
United States.

6cream has 2-3 grams per serving, as opposed to 10-18 gramsin a serving of ice cream. Pudding made with skim milk hasno fat; pudding made with whole milk has 5-6 fat gramsper serving.• Switch to low-fat breads, cereals and pastas.
A bagel has 2 grams of fat per serving. A doughnut has14 grams of fat. Try substituting hot cereal for pastries or aDanish (2 grams of fat as opposed to 38 grams or more).Also, baked potatoes and pasta have almost no fat, but youmust be sure to choose low-fat toppings.• Use egg whites or egg substitutes.
You can indeed enjoy eggs as part of a heart-healthydiet, but the American Heart Association recommends nomore than three to four egg yolks per week. Use egg whitesor egg substitutes when scrambling eggs (try poached eggsinstead of fried eggs); in nonfat cooked frostings; in makingcakes, cookies and muffins, and in making bread me-ringues. A general guide to follow is to use two egg whitesfor each whole egg or use egg substitutes.• Use less fat in cooking.
Try to limit the amount of fat you eat to no more than5-8 teaspoons per day, including what is used in cooking.Helpful tips include baking, broiling, boiling, steaming,poaching, or microwaving foods instead of frying them;using nonstick vegetable oil cooking sprays; and trying toenjoy the taste of foods without sauces or gravies or usinglow-fat or nonfat versions.
The American Heart Association recommends you limityour fat intake to less than 30 percent of your total dailycalories. For example, if you consume 1,500 calories per dayor less, you should eat foods with 50 grams of fat or lessdaily; 2,000 daily calories, 65 grams of fat or less; and 2,500calories, 80 grams of fat or less.
Remember, choices you make can help you lead alonger, heart-healthy life. ❤
Eating heart-healthy foods doesn’t have to be achore. Taking a little effort to eat foods with less fat andcholesterol can not only make you feel better but could helpyou live a longer, healthier life.
The American Heart Association says that a diet low infat and cholesterol may reduce the risk of heart attack. Hereare some tips to help you get started:• Use nonfat products.
Eat more fruits and vegetables to help reduce your fatintake. Most fruits and vegetables are low in fat and high invitamins and minerals.• Choose low-fat products.
Compare products when shopping. For example, trybaked tortilla chips instead of fried tortilla chips or pretzelsand low-fat potato chips instead of regular or corn chips.• Use lean meats.
The food that adds more fat to the American diet thanany other is also the most popular — burgers. Try choosingfish, chicken, turkey and lean cuts of beef and pork insteadof hamburger.• Switch to skim, nonfat or fat-free milk.
Whole milk has up to 8 grams of fat per serving. Fat-free milk has less than half a gram per serving. Try gradu-ally reducing the fat content of the milk you drink. If youdrink whole milk now, try switching to one percent milk,then half-percent, and finally fat-free (skim) milk.• Use low-fat and nonfat cheeses and dairy products.
Try nonfat and low-fat cheeses instead of regularcheeses, and low- and nonfat sour creams and yogurts.• Try nonfat and low-fat puddings and frozen desserts.
Frozen fruit bars have zero grams of fat per serving, asopposed to 11-20 grams in an ice cream bar. Low-fat ice
A “hearty” appetite
7Exercise. The mere word makes some people
cringe. But a little exercise can help make you look andfeel better.
Benefits of regular exercise include:• More energy.• The ability to cope better with stress.• Improved self-image.• Increased resistance to fatigue.• Stronger resistance to anxiety and depression.
• More relaxationand less tension.• Improved abilityto fall asleepquickly and sleepwell.• Easy way toshare an activitywith family mem-bers and friends,and an opportunityto meet new friends.Exercise also canmake you lookbetter. It can:
• Tone your muscles.• Burn off calories to help you lose extra pounds or stayat your desired weight.• Help control your appetite.
You need to burn off 3,500 calories more than youtake in to lose one pound. If you want to lose weight,regular physical activity can help you in two ways.First, you can eat your usual amount of calories butbe more active.
For example, a 200-pound man who keeps eating thesame amount of calories but decides to walk briskly eachday for a mile and a half will lose about 14 pounds inone year.
Or, you could eat fewer calories and be more active.This is an even better, and quicker, way to lose weight.
Exercise also may help you work better. It can:• Help you be more productive at work.• Increase your capacity for physical work.• Build endurance for other physical activities.• Increase muscle strength.• Help your heart and lungs work more efficiently.
Consider the benefits of a well-conditioned heart.In one minute with 40 to 45 beats, the heart of a well-conditioned person pumps the same amount of bloodas an inactive person’s heart pumps in 70 to 75 beats.Compared to the well-conditioned heart, the averageheart pumps up to 36,000 more times per day, or13 million more times per year.
Feeling, looking and working better — all thesebenefits from regular physical activity can help youenjoy life more fully. ❤
Exercise: Your heart’s best friend

8It’s called the “silent killer” because there are no
symptoms. You may look and feel fine while your bloodpressure is rising to dangerous levels. So what can youdo? Learn what causes high blood pressure and whatyou can do to decrease your risk of having highblood pressure.
What is high blood pressure?Two numbers are being measured when you have
your blood pressure checked by a medical professional.The first number (systolic pressure) measures thepressure in your arteries while your heart beats. Thesecond number (diastolic pressure) measures thepressure while your heart rests between beats.
Normal blood pressure falls within a range; it’s notone set of numbers. It should be less than 140/90 if youare an adult. If your blood pressure goes above thisthreshold and stays there, you have high blood pressure.
High blood pressure can kill you before you know it
The Silent Killer
What causes high blood pressure?In 90 to 95 percent of high blood pressure cases, the
cause is unknown. You could have it for years withoutknowing it. In the other five percent of cases, there isusually an underlying problem such as a kidneyabnormality or congenital heart defect.
What can you do about high blood pressure?• Maintain a normal, healthy weight.• Decrease salt intake.• Take medications as prescribed by your physician.• Don’t start smoking and, if you are a smoker, quit. ❤
The good, the badand the healthy
There is good news and bad news aboutcholesterol.
The good news is that the “good” cholesterolcan actually lower cholesterol levels in your body. Thebad news is that the “bad” cholesterol is no friend toyour heart.
The “good” cholesterol is HDL (high-densitylipoprotein) which actually helps to clear cholesterol outof your system. High levels of HDL lower your risk ofheart disease. The “bad” cholesterol is LDL (low-densitylipoprotein), which deposits cholesterol on artery walls,increasing plaque buildup.
It is important to haveyour blood levels of totaland HDL cholesterolchecked, especially if you oryour family have a historyof high cholesterol.
The chart below outlines the good and the bad aboutcholesterol levels.
If your total cholesterol or HDL levels are in theborderline-high risk or high-risk category, you shouldtalk to your family physician about:• Having your LDL cholesterol checked.• When to re-check your cholesterol levels.• How to reduce your risk by eating less fat, saturated
fat and cholesterol; increasing your physical activity;losing weight (if needed) or maintaining a healthyweight; and avoiding tobacco smoke.
• Taking medication, if needed. ❤
Cholesterol levels Desirable (low-risk) Borderline-High risk High risk
Total cholesterol less than 200 200-239 240 or higherLDL or “badcholesterol” less than 130 130-159 160 or higherHDL or “goodcholesterol” 35 or higher less than 35 less than 35

9G iving up a habit is hard. Whether you twist
your hair, bite your nails or smoke cigarettes, it is hard tobreak a habit. Although twisting your hair may leave youwith a head covered with ringlets, smoking is a habitthat can damage your heart and lungs and affect yourquality of life.
With the year 2000 just around the corner, quittingsmoking would be a great New Year’s resolution if youare trying to kick the habit. It won’t be easy, but withsome willpower and planning, you can do it.
Have a plan. Write down the reasons that you wantto quit. Examples might be:• Smoking is bad for my health.• Smoking makes my clothes and hair smell bad.• I want to be in control of my life, not a slave to a habit.
Read your list each day. Add other reasons to yourlist as you think of them.
Your plan should include the following: commit toquit; set a target date to quit; talk to your physicianabout nicotine replacement therapy; and take better careof yourself by starting an exercise program, drinkingmore fluids and getting plenty of rest. Try to smokefewer cigarettes. Encourage your family andfriends to support your decision to quit. Switchcigarette brands to a brand you don’t like.
Now put your plan into action.Do the following:• Stop smoking entirely. Throwout all your cigarettes and matches.• Buy yourself a treat or do something special tocelebrate.• Go to the dentist and have your teeth cleaned.• Find a cigarette substitute (deep-breathing exercises,chewing gum, etc.)
Remember to avoid those things that might trigger anurge for a cigarette. Think about when and where youprefer to smoke and avoid those situations and places.You will get the urge to smoke, so be ready to resist thetemptation. Studies show that the hardest place to resistthe urge to smoke is home. Other risky places are at
work and in social situations. Theactivities most closely linked tosmoking are eating, attendingparties and drinking. Mosturges occur when anothersmoker is present. Learn to copewith the urges and resist smoking.
Ways to cope includethe following:• Know your triggers and avoid those situations.• Keep your hands busy (fiddle with a pencil, knit, docrossword puzzles, etc.).• Use oral substitutes (chew gum, munch carrots orapples, etc.).• Find activities that make smoking difficult (gardening,washing the car, walking the dog, meditation, etc.).• Start an exercise program.• Change your habits (if you always have a cigarette witha cup of coffee, switch to tea or water for awhile, etc.)• Choose nonsmoking environments and spend timewith friends and family who do not smoke.• Avoid smokers.• Drink lots of water and fruit juices.• Keep your mouth feeling fresh and clean.• Review your reasons for quitting.• Seek social support.• Think positively.• Learn to relax.• Reward yourself for not smoking.
OK, so you decided to quit, created a plan, avoidedthe triggers, used your new coping skills and … guesswhat, you had a slip and smoked a cigarette. Don’tblame yourself and don’t feel guilty. One slip is not theend of all your hard work. Identify what triggered yourslip and think about how to cope with that situation thenext time.
As the new year approaches, makea commitment to a better, healthiernon-smoking you. ❤
Where there’s smoke, there’s fire

10Dental care for adults with heart disease
If you have heart disease, you need specialconsideration when you get dental treatment, and it isimportant that you establish and maintain a healthymouth. You need to make sure your dentist knows youhave a heart problem. And, you must carefully followyour physician’s and dentist’s instructions when theyprescribe special medications such as antiobiotics.
Several heart problems require that you and yourdentist take special precautions. These include: heartattack, irregular heartbeat, heart failure, angina pectoris,heart murmur, artificial heart valve, heart pacemaker,bypass surgery and vascular surgery. Also, remember totake special care when you are taking antiobiotics toprevent bacterial endocarditis or when taking otherheart medications. ❤
Aspirin and cardiovascular diseasesStudies suggest that aspirin helps prevent and treat
heart attack, stroke and some other blood-vesseldiseases. It works by making it harder for blood clots toform. Although much has been written about takingaspirin to reduce the risk of heart attack and stroke, noteveryone should use aspirin for this purpose.
Data clearly shows that the vast majority of peopleshould be treated with aspirin after a heart attack.Studies show that taking aspirin protects against laterheart attacks. Taking aspirin also reduces the chance thatvessels will reclog after heart bypass surgery or coronaryangioplasty. Aspirin also helps in treating chest pain(angina pectoris).
Despite these favorable findings, people withhealthy heart and brain vessels should not take aspirinto prevent a heart attack or stroke without their
doctor’s specific recommendations.Why? Because aspirin lowers the riskfrom clots but increases the risk ofintestinal bleeding. ❤
What is congestive heart failure?It sounds pretty scary. But it doesn’t mean your
heart has stopped beating or death is imminent. Itmeans that your heart isn’t pumping as well as itshould be.
In cases of congestive heart failure, the heart keepsworking. As a result, the body’s needs for oxygen-richblood (both during exercise and rest) aren’t fully met.Congestive heart failure is a condition in which aweakened heart exists along with a buildup of fluid inthe body. It can be caused by many forms of heartdisease. Common causes of congestive heart failure areas follows:
1.Narrowed arteries that supply blood to the heartmuscle.
2.Past heart attack.3.High blood pressure.4.Heart valve disease due to past rheumatic fever or
other causes.5.Primary disease of the heart muscle itself.6.Defects in the heart present at birth.7. Infection of the heart valves and/or heart muscle
itself.If you are diagnosed with congestive heart failure,
it can almost always be managed. With treatment andadjustments in daily life, patients usually feel a lotbetter. The first way to treat this disease is to limit saltintake, maintain potassium and magnesium at normallevels and control weight. Additional ways to managecongestive heart failure include prescriptionmedications and surgical treatment. ❤
H E A R T
The heart health information for thisissue of Blue & You was provided by theAmerican Heart Association. For moreinformation on heart disease — andheart health — please contact thenearest chapter of the American HeartAssociation or call 1-800-AHA-USA1(1-800-242-8721) or visit themon-line at www.americanheart.org.
Shot Dodgers
Good healthis child’s play 11To promote the health of the approximately 78
million children and teen-agers in the United States, theCenters for Disease Control (CDC) recommends thatchildren should do the following:• Wash hands to prevent infection.• Eat breakfast before going to school.• Not smoke and avoid the smoke of others.• Exercise and play safely and appropriately use
protective gear.And parents should do the following to promote the
health of their children and teen-agers:• Read to and be actively involved with their children.
• Get their children vaccinated.• Get health care insurance for their children.• Check for health hazards in their home and eliminate
them.• Place children weighing less than 40 pounds in child
safety seats and all other children in safety belts in therear seats of automobiles.
• Seek medical advice if their child is slow to learn.• Avoid tobacco use and limit alcohol use.
In addition, women of childbearing age should takevitamins with folic acid to prevent certain birth defects.
Good healthis child’s play
In accordance with the Women’s Health and CancerRights Act of 1998, all group and individual health plansthat provide medical and surgical benefits for mastec-tomy cover reconstructive breast surgery, if elected bythe covered individual following mastectomy, including:• Reconstructive surgery on the breast on which the
mastectomy was performed.• Reconstructive surgery on the unaffected breast
needed to “produce a symmetrical appearance.”• Prostheses and treatment of complications of any stage
of a mastectomy, including lymphedema.
~ Women’s Health and Cancer Rights Act reminder ~These provisions apply to all policies issued by
Arkansas Blue Cross and Blue Shield, Health Advantageand to all health plans administered by USAble Adminis-trators and are subject to the applicable co-payments, co-insurance, benefit limitations, exclusions and benefitmaximums.
If you have questions about your insurance coverage,contact your group benefits administrator or a customerservice representative at your local Arkansas Blue Crossoffice.
More than 29 percent of Medicare beneficiaries inthe United States reported that they did not receive eitherthe influenza or pneumococcal vaccine prior to cold andflu season, according to the 1996 Medicare CurrentBeneficiary Survey.
When asked why they did not receive thevaccinations, most Medicare beneficiaries reported theydid not know they needed the vaccine (19 percent for theflu and 57 percent for pneumonia). More than 40 percentof those who did not receive the vaccines reported that
Shot Dodgersthey had concerns about the vaccine, and 13 percent ofthose who did not receive the pneumococcal vaccinecited the lack of a doctor’s recommendation.
In the United States, the flu causes an average of20,000 deaths per year, and 90 percent of these deathsare among persons aged 65 or older. Annual flu andpneumococcal vaccines can prevent complications fromthese diseases in persons aged 65 or older.
Information for this article was obtained from theCenters for Disease Control.
Imm
uniz
ation L
egend:
DTP -
Dip
hth
eria-t
eta
nus-
pert
uss
isHib
- H
aem
ophilus
infl
uenzae T
ype b
conju
gate
vaccin
e
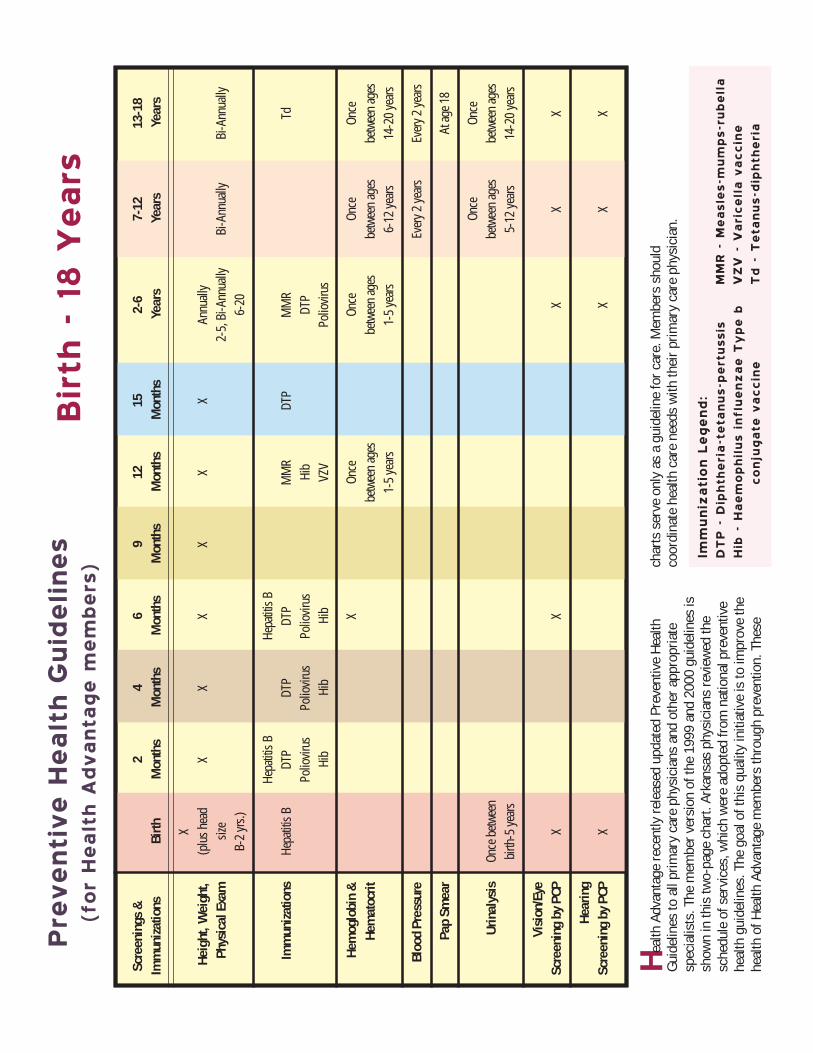
Pre
ventive H
ealth G
uid
elines
(for
Health A
dvanta
ge m
em
bers
)
Scre
enin
gs &
24
69
1215
2-6
7-12
13-1
8Im
mun
izat
ions
Birth
Mon
ths
Mon
ths
Mon
ths
Mon
ths
Mon
ths
Mon
ths
Year
sYe
ars
Year
s
XHe
ight
, Wei
ght,
(plu
s hea
dX
XX
XX
XAn
nuall
yPh
ysic
al E
xam
size
2-5,
Bi-A
nnua
llyBi
-Ann
ually
Bi-A
nnua
llyB-
2 yr
s.)6-
20
Hepa
titis
BHe
patit
is B
Imm
uniz
atio
nsHe
patit
is B
DTP
DTP
DTP
MM
RDT
PM
MR
TdPo
liovir
usPo
liovir
usPo
liovir
usHi
bDT
PHi
bHi
bHi
bVZ
VPo
liovir
us
Hem
oglo
bin
&X
Once
Once
Once
Once
Hem
atoc
ritbe
twee
n ag
esbe
twee
n ag
esbe
twee
n ag
esbe
twee
n ag
es1-
5 ye
ars
1-5
year
s6-
12 ye
ars
14-2
0 ye
ars
Bloo
d Pr
essu
reEv
ery 2
year
sEv
ery 2
year
s
Pap
Smea
rAt
age 1
8
Once
Once
Urin
alys
isOn
ce b
etwee
nbe
twee
n ag
esbe
twee
n ag
esbi
rth-5
year
s5-
12 ye
ars
14-2
0 ye
ars
Visi
on/E
yeSc
reen
ing
by P
CPX
XX
XX
Hear
ing
Scre
enin
g by
PCP
XX
XX
MM
R -
Measl
es-
mum
ps-
rubella
VZV -
Varicella v
accin
eTd -
Teta
nus-
dip
hth
eria
Heal
th A
dvan
tage
rece
ntly
rele
ased
upd
ated
Pre
vent
ive
Heal
thGu
idel
ines
to a
ll pr
imar
y ca
re p
hysi
cian
s an
d ot
her a
ppro
pria
tesp
ecia
lists
. The
mem
ber v
ersi
on o
f the
199
9 an
d 20
00 g
uide
lines
issh
own
in th
is tw
o-pa
ge c
hart.
Ark
ansa
s ph
ysic
ians
revi
ewed
the
sche
dule
of s
ervi
ces,
whi
ch w
ere
adop
ted
from
nat
iona
l pre
vent
ive
heal
th g
uide
lines
. The
goa
l of t
his
qual
ity in
itiat
ive
is to
impr
ove
the
heal
th o
f Hea
lth A
dvan
tage
mem
bers
thro
ugh
prev
entio
n. T
hese
Birth
- 18 Y
ears
char
ts s
erve
onl
y as
a g
uide
line
for c
are.
Mem
bers
sho
uld
coor
dina
te h
ealth
car
e ne
eds
with
thei
r prim
ary
care
phy
sici
an.

Scre
enin
gs &
19-3
940
-49
50-6
465
Imm
uniz
atio
nsYe
ars
Year
sYe
ars
Year
s &
Up
Heig
ht, W
eigh
t, Ph
ysic
alEx
am, B
lood
Pre
ssur
e
C
linica
l disc
retio
n
Teta
nus-
diph
ther
ia (T
d)
O
nce e
very
10
year
s
Influ
enza
Vac
cine
Annu
ally
Pneu
moc
occa
l Vac
cine
Once
-boo
ster i
n 5-
10 ye
ars
at cli
nica
l disc
retio
n
Non-
Fast
ing
Tota
l Blo
odCh
oles
tero
l
Cl
inica
l disc
retio
n
Urin
alys
isOn
ce b
etwee
n 14
-20
year
sCl
inica
l disc
retio
n
Visu
al A
cuity
, Hea
ring
& H
earin
g Ai
dsCl
inica
l disc
retio
n
Pap
Smea
r
Ever
y 1-3
year
s
Clin
ical
Bre
ast E
xam
Pe
riodi
c eva
luati
on, a
nnua
lly o
r as a
ppro
priat
e
Mam
mog
ram
Ever
y 1-2
year
s
A
nnua
lly
Sigm
oido
scop
yEv
ery 3
-5 ye
ars
Ever
y 4 ye
ars
Feca
l Blo
od O
ccul
t
Ann
ually
➙➙
➙
19 Y
ears
& U
p
Not
e:Pr
even
tive
hea
lth
serv
ices
are
cov
ered
acc
ordi
ng t
o th
e pa
tien
t’s
indi
vidu
al h
ealt
h ca
re b
enef
its
wit
h H
ealt
h A
dvan
tage
.

14
The A.M. Best Company has affirmed the “A-”(Excellent) rating of Arkansas Blue Cross and Blue Shieldfor another year, continuing the rating held since 1994. Arating from A.M. Best represents an independent opinionfrom the leading provider of insurer ratings of acompany’s financial strength and ability to meet itsobligations to policyholders.
The “A-” rating reflects the enterprise’s marketleadership in Arkansas, the ongoing migration of mem-bership into a more structured managed care environ-ment and an adequate level of capitalization, accordingto a news release from A.M. Best.
The news release also stated that Arkansas BlueCross and its affiliates have the largest market share inthe Medicare supplement arena, group health coverage
When used appropriately, prescription medicationprovides an effective means for reducing pain, healinginfections and preventing hospitalizations. Historically,medication costs have been nominal when compared tohospital and other medical costs. Approximately 20 yearsago, the entire charge for a prescription was $12 to $15.This was before prescription cards and drug co-pay-ments; when you paid for the medication and were laterreimbursed by your insurance plan.
Physician services and hospital care traditionallyhave been the high-cost areas, and pharmacy costs havebeen negligible by comparison. However, this haschanged significantly during the past decade. Mostpeople today pay only the co-payment for name-brandprescriptions and do not feel the impact of the alarmingcost of prescription medications. Today, a prescriptioneasily may cost $100 or as much as $1,500. In recentyears, drug costs have increased to the point of becomingunaffordable for some. Compare the growth trends thatshow the annual percentage of cost increase in thefollowing table:
National Health Expenditures — Annual Percentage Growth — 1992-1998
1992 1993 1994 1995 1996 1997 1998EHospital Care 8.2% 5.8% 3.9% 3.4% 3.9% 2.9%Physician Services 8.5% 5.7% 3.8% 4.6% 3.3% 4.4%Nursing Home 9.0% 6.7% 7.0% 6.2% 5.2% 4.3%Prescription Drugs 10.6% 8.7% 9.0% 10.6% 13.2% 14.1% 18.4%E
Escalating prescription costsEscalating prescription costsEscalating prescription costsEscalating prescription costsEscalating prescription costs— — — — — can we afford them?can we afford them?can we afford them?can we afford them?can we afford them?
and HMO (health maintenance organization) marketsand have been able to adapt to the health care coverageneeds of their respective memberships.
A.M. Best also affirmed the “A-” (Excellent) ratingsof USAble Life and the First Pyramid Life InsuranceCompany of America. According to the A.M. Best Report,these companies continue to add value to Arkansas BlueCross’ diverse portfolio, through the offerings of ancillarybenefits. Additionally, A.M. Best rated Health Advantageat “A-” (Excellent) for the first time. This initial ratingreflects Health Advantage’s strategic role in the enter-prise, A.M. Best said. USAble Corporation and BaptistHealth HMO, Inc. each own 50 percent of HealthAdvantage, the largest health maintenance organizationin Arkansas.
Escalating prescription costsEscalating prescription costsEscalating prescription costsEscalating prescription costsEscalating prescription costs— — — — — can we afford them?can we afford them?can we afford them?can we afford them?can we afford them?
Pharmaceuticals cannot claim credit for thesestabilizing hospital and physician costs, but continuousimprovements in disease management — includingmedication therapy — should produce fewerhospitalizations.
Pharmaceutical manufacturers have discovered theeffectiveness of direct-to-consumer advertising forprescription medications and now spend as much ormore on this than calling on physicians. This produceshigher utilization of more expensive drugs, which usuallyare the drugs advertised.
More new drugs are being approved at a faster rateby the federal Food and Drug Administration (FDA) thanever before. Some of these new medications are first-generation, demonstrating marginal effectiveness but afirst step toward final success. This new era of pharma-ceuticals is producing long-awaited treatments forchronic and fearsome diseases (Alzheimer’s, multiplesclerosis, diabetes, migraine headaches, cancer andmore) that have troubled people for centuries. Theseprescriptions will come at a shocking price, and every-
one will be involved in sharingthis cost.
$$$$$$$$$$$$$$$
Among the BestAmong the Best
A-, A-,A-
A-, A-,A-

15
Health Advantage
members —
take note!
Health Advantage strives tomeet the health and wellness needsof its members. According to arecent survey, Health Advantagemembers indicated that they aresatisfied with the health mainte-nance organization’s (HMO)performance and very satisfied withthe physicians in HealthAdvantage’s network.
The 1999 National Committeefor Quality Assurance (NCQA)Health Plan Employer Data Infor-mation Set (HEDIS) MemberSatisfaction Survey results are beingused to identify areas where HealthAdvantage and its providers couldimprove their services to members.
The most recent survey, a newinstrument used for the first time in1999, was mailed to a randomsample of 1,240 of HealthAdvantage’s commercial HMOmembers. A total of 689 respon-dents were certified as “valid”respondents, which gave HealthAdvantage a 65.3 percent responserate from the eligible sample.
Health Advantage receivedhigher-than-average scores in sevencategories — when compared withnational averages — on the survey.Those categories are: rating ofpersonal doctor, courteous andhelpful clinic staff, claims process-ing, customer service, getting carequickly, getting needed care andoverall health care services. Whenmembers rated their experiencewith their health plan, HealthAdvantage received an overallrating equal to the national andregional averages.
“This was the first time thatquestions were asked about thephysicians participating in theHealth Advantage networks, and weare very pleased with the results.Survey participants indicated theyare very pleased with the physi-cians in our network; that thephysicians are listening to theirneeds and that they are happy withtheir personal physicians,” saidDavid Bridges, president and chiefexecutive officer of Health Advan-tage. “Survey participants also saidthey were getting care quickly and
that the approval process throughHealth Advantage was not aproblem. This survey shows that weare on the right track, and I amappreciative of all Health Advantageemployees for their hard work.”
According to the “effectivenessof care” categories, which are basedon claims data information (notsurvey results), Health Advantageand its network of providers shouldfocus on several areas. For example:members said their physicians needto increase their efforts in advisingsmokers to quit (see related articleon Page 9).
In the past few months, HealthAdvantage has sent out “Women’s
Health Alert” reminders for preven-tive tests.
The wide-ranging survey askedmembers to characterize variousaspects of their experiences indealing with the health plan and itshealth care providers (doctors andhospitals). The results of a few keyquestions are as follows:
• A total of 83.3 percent ofrespondents rated their special-ist 8 or higher on a 10-pointscale. A total of 73.7 percentof respondents rated theirpersonal physician 8 or higheron a 10-point scale. Nine outof 10 members rated theirphysician and office staffcommunication as very goodor excellent.
• A total of 86.4 percent ofrespondents said there wasno problem with delays inwaiting for approval from thehealth plan. A total of 85.7percent of respondents saidthere was no problem ingetting the care they or theirdoctor believed necessary.
• A total of 87 percent of respon-dents said their claims werealways or usually handledcorrectly. A total of 85.2percent of respondents saidtheir claims were always orusually handled in a reason-able amount of time.
Health Advantage scores well on member surveyMAKING THE GRADE

Leading16 As promised in the Autumn 1999 issue of Blue & You, Arkansas BlueCross and Blue Shield will continue to help our customers get to knowthe many state senators and representatives of the Arkansas General
Sen. Gunner Delay (R)(Dist. 11) Fort SmithCommittee on Committees;Revenue & Taxation;Transportation, Aging &Legislative Affairs(O) 501-785-4466(H) 501-782-4727
Sen. Mike Everett (D)(Dist. 23) Marked TreeVice-Chairman, Children &Youth; Agriculture, Economic& Industrial Development;Joint Budget; JointRetirement & SocialSecurity; Judiciary; Rules,Resolutions & Memorials(O) 870-358-5800(H) 870-358-3560
Sen. Jon Fitch (D)(Dist.26) HindsvilleChairman, Transportation,Aging & Legislative Affairs;Vice-Chairman, JointRetirement & SocialSecurity; Agriculture,Economic & IndustrialDevelopment; Efficiency;Joint Budget(O/H) 501-789-2608
Sen. Gary Hunter (R)(Dist. 32) Mountain HomeAgriculture, Economic &Industrial Development;Children & Youth; JointBudget; Joint Retirement &Social Security; Revenue &Taxation; Rules, Resolutions& Memorials; Aging &Legislative Affairs(O) 870-425-6255(H) 870-425-2220
Rep. Gary Biggs (D)(Dist. 85) ParagouldCity, County & Local Affairs;Public Health, Welfare & Labor;Rules(O) 870-239-6084(H) 870- 239-5127
Rep. Herschel Cleveland (D)(Dist. 26) ParisAgriculture & EconomicDevelopment; Education; JointPerformance Review(O) 501-963-8009(H) 501-963-2418
Rep. Joyce Dees (D)(Dist. 76) HermitageAging, Children & Youth,Legislative & Military Affairs;Energy; Judiciary(O) 870-226-7441(H) 870-463-8154
Rep. Dean Elliott (R)(Dist. 62) MaumellePublic Transporation; StateAgencies & Governmental Affairs(O) 501-851-7783(H) 501-851-0062

the Way 17Assembly who spend numerous hours working on health care issues.(Upcoming issues of Blue & You will feature additional profiles ofour legislators.)
Rep. Steve Faris (D)(Dist. 18) MalvernChairman, Joint Retirement& Social Security; JointBudget; Public Health,Welfare & Labor; StateAgencies & GovernmentalAffairs(O) 501-865-3333(H) 501-337-7307
Rep. Boyd Hickinbotham (D)(Dist. 66) SalemAging, Children & Youth,Legislative & Military Affairs;Joint Performance Review;Revenue & Taxation(O/H) 870-895-2319
Rep. John Lewellen (D)(Dist. 58) Little RockAging, Children & Youth,Legislative & Military Affairs;Joint Retirement & SocialSecurity; PublicTransportation(O/H) 501-372-5612
Rep. Sandra Rodgers (D)(Dist. 28) HopeVice-Chairman, Aging,Chidren & Youth, Legislative& Military Affairs; Education;Energy(O) 870-777-0500(H) 870-777-3907
Rep. Harmon Seawel (D)(Dist. 77) PocahontasCity, County & Local Affairs;Education; Joint AdvancedCommunications &Information Technology(O) 870-647-2051(H) 870-647-2571
Rep. Martha Shoffner (D)(Dist. 79) NewportJoint Budget; Joint PerformanceReview; Public Transportation;State Agencies & GovernmentalAffairs(O/H) 870-523-6153
Rep. Roger Smith (R)(Dist. 32) Hot Springs VillageJoint Retirement & SocialSecurity; Revenue & Taxation;State Agencies & GovernmentalAffairs(O) 501-321-1781(H) 501-922-0730
Rep. Bobby Lee Trammell (D)(Dist. 88) JonesboroPublic Health Welfare & Labor;State Agencies & GovernmentalAffairs(O) 870-932-4639(H) 870-919-3315
Rep. Wilma Walker (D)(Dist. 65) College StationAging, Children & Youth,Legislative & Military Affairs;Education(O) 501-490-5811(O) 501-490-0235
18Once upon a time, Arkansas’ medical landscape
was dotted with country doctors. Physicians inrural areas were depended on as integral parts oftheir communities.
Arkansas still depends on rural physicians, butunfortunately, their numbers have been decliningsteadily over the past several decades.
The Arkansas Medical MENTOR Partnership isseeking to reverse that trend. This innovative program,which seeks to cultivate an interest in health-relatedcareers among rural youth, is sponsored by ArkansasBlue Cross and Blue Shield, the Area HealthEducation Centers (AHEC) Program and theRural Hospital Program (both of the Universityof Arkansas for Medical Sciences), the Arkan-sas Academy of Family Physicians, ArkansasFarm Bureau, Arkansas Community HealthCenters, the Electric Cooperatives of Arkansasand the Arkansas State Chamber of Com-merce/Associated Industries Inc.
The MENTOR program is based on the belief(supported by statistics) that health professionalswho were reared in non-urban settings are more likelythan their city-raised counterparts to establish long-termpractices in rural regions. Sadly, though, rural juniorhigh school and high school students often aren’tactively encouraged or counseled to seek a career inthe health professions.
The MENTOR program, through community-basedawareness initiatives and events, seeks to provideresources that expose interested students to the possibili-ties of a career in health care, provide any neededguidance and planning, and make a case for returninghome to practice. The program also targets rural schools,inviting them to open local MENTOR chapters.
The centerpiece of the program is an intensive, two-week summer medical experience program called MASH(Medical Applications of Science for Health). MASH
camps, which are held throughout the state atthe Area Health Education Centers and
affiliates of the Rural Hospital Program,allow 10th-, 11th- and 12th-gradestudents to get hands-on exposure to avariety of health professions. Studentsapply for the camps in the spring.
The MENTOR partnership alsoinvites county Farm Bureaus, local
businesses and civic organizations toprovide $50 co-sponsorships. Otherwise,
the MENTOR partnership pays the full $200tuition for each student.
For more information about the MENTOR partner-ship and/or the MASH program, contact Ken Tillman ofArkansas Farm Bureau at (501) 228-1295 or YvonneLewis, Ed.D., of the UAMS Area Health EducationCenters Program at (501) 686-6557.
MENTOR, MASHinitiatives seek
to remedyrural plight
ss
m
m
H o m e - g r o w n h e a lt h c a r e
For the fourth year, Arkansas Blue Cross and BlueShield is teaming up with Wildwood Park for the Per-forming Arts in an effort to entertain and teach elemen-tary school-aged children through a live theater experi-ence. Performances of “Hansel and Gretel” now are beingbooked for the Spring Tour 2000.
Through the centuries, fairy tales have taughtchildren and adults important lessons in character,conquering fears and overcoming problems. Studentstoday still can learn these life lessons as they experiencethis enchanting story, based on the Grimm Brothers fairy
Teaching through story-tellingTeaching through story-tellingTeaching through story-tellingTeaching through story-tellingTeaching through story-tellingtale, in a musical theater setting — complete with a tastygingerbread house and the delightful tunes of composerEngelbert Humperdinck.
The production comes with a colorful set, charmingcostumes and fully synthesized orchestral accompani-ment. “Hansel and Gretel” is appropriate for students ingrades K-6 or family-oriented community presentations,and is available February through April 2000.
For performance cost, booking availability or moreinformation, call Holly Matthews at Wildwood,(501) 821-7275, ext. 241.
ssssstttttooooorrrrryyyyy

Blue team gets ready to race forthe cure.
BlueAnn Ewe takes a heart-healthywalk with Northeast Arkansans.
19Arkansas Blue Cross and Blue Shield is a good
corporate citizen. Our employees raise money and spendmany hours helping those causes near and dear to thehearts of Arkansans.
Blue is in the PinkMore than 300 Arkansas Blue Cross and Blue Shield,
Health Advantage and USAble Administrators employeeswalked and ran to raise awareness and funds for theSusan G. Komen Breast Cancer Foundation in the 1999Arkansas Race For The Cure® on Sept. 25. Employee raceparticipants turned out in their Blue team T-shirts to jointhe more than 22,000people who con-verged on the streetsof downtown LittleRock. The company’sThree Miles of Men®team received the“Team Spirit Award”for its efforts incheering on Raceparticipants at the“Blue Hawaii” blocks located at Arkansas Blue Cross’headquarters at Sixth and Gaines streets.
Cure for the KidsArkansas Blue Cross participated in the Juvenile
Diabetes Foundation’s “Walk to Cure Diabetes,” heldOct. 2, in Little Rock’s River Market. Employees raised$4,608, which was added to a corporate match of $5,000and presented to JDF. Many Arkansas Blue Cross employ-ees joined walkers from throughout the state for thesecond-annual event, which grew significantly from lastyear. A special “thanks” to Dr. David Lupo and SouthArkansas Urology for donating a great door prize whichwas awarded as part of the event.
Milestones for MercyMore than $150,000 was raised during the annual
Mercy Celebrity Classic, held Oct. 1-3 in Fort Smith tobenefit the Phillips Cancer Support House, the Alzheimer’sAssociation Western Arkansas Chapter and the HelpingHands For Children/St. Edward Mercy Auxiliary Project.As part of the festivities, Arkansas Blue Cross sponsoredthe Cancer Awareness Survivors’ Challenge the morning of
Oct. 2 in downtown Fort Smith. Runners and walkers got ascenic tour of historic Fort Smith and helped raise aware-ness of needs in the fight against cancer.
Hearty WorkoutBlueAnn Ewe, Arkansas Blue Cross’ health-and-
wellness ambassador, joined several employees from theArkansas Blue CrossNortheast RegionalOffice in support ofthe American HeartAssociation’s HeartWalk, held Oct. 3 inJonesboro. DaveFerguson of theArkansas Blue CrossNortheast RegionalOffice served asassistant chair of the event, and BlueAnn helped lead thewarm-up activities before the walk. Arkansas Blue Crossemployees also walked in the event to help raise $30,000in support of the agency which benefits residents in thenortheast region of the state.
Breast Center opens inBentonville
With hopes of becoming known as a comprehensivecare program with a reputation as one of the best facilitiesnot only in the region but in the nation, Mercy HealthCenter in Bentonville unveiled the new Mercy BreastCenter on Oct. 10. The opening was held in conjunctionwith National Breast Cancer Awareness Month observed inOctober. The new concept in care is the vision of DouglasFriesen, M.D., who said the center will be evaluating itsperformance against the best breast centers in the country.Mercy Breast Center services include: mammography,ultrasound, stereotactic biopsy, physical therapy, educa-tion, support groups and pastoral care. The Mercy BreastCenter will work closely with the NARTI (North ArkansasRadiation Therapy Institute) care team and the HighlandsOncology physicians. Dr. Friesen said three key compo-nents will set Mercy apart from other health care provid-ers: a nurse coordinator; the partnerships with NARTIand Highlands; and weekly interdisciplinary conferencesby all the physicians to improve the delivery of breastcancer treatment.

Arkansas Blue Cross and Blue ShieldP.O. Box 2181Little Rock, AR 72203-2181
— a guide to health insurance terminology
IIf health care terminology (including abbreviations andacronyms) leaves your head spinning … don’t worry, ArkansasBlue Cross and Blue Shield wants to help you make sense ofall the jargon. We want you to be an informed customer, so ineach issue of this quarterly publication, Blue & You, we willexplain the meaning behind those health insurance words,acronyms and abbreviations that you may encounter whenreading health care-related materials.
Benefit — Services provided or expenses reimbursed in ahealth care policy or contract.
Cost sharing — A general set of financing arrangements, viadeductibles, co-payments and/or co-insurance, in which aperson covered by the health plan must pay some of the coststo receive care.
DRG (Diagnosis Related Group) — A system of groupingmedical/surgical hospital admissions according to major bodysystems and similar consumption of hospital resources. Thegrouping of conditions and procedures is statistically similar,based on resources consumed and the total cost of services.DRGs are used by Medicare and some private, third-partypayers as the unit of payment.
Formulary — A listing of drugs, classified by therapeuticcategory or disease class, that are considered preferred therapyfor a given managed population and that are to be used by ahealth maintenance organization’s (HMO) providers inprescribing medicine.
Managed care — The integration of both the financing anddelivery of health care within a system that seeks to provideinformation on accessibility, cost and services.
Medical Management — A combination of the following:credentialing, education, information, data review, siteappropriateness, policymaking, standard setting, practiceguideline development, provider panel access, etc. aimed atimproving the effectiveness, efficiency and affordability ofservices and benefits.
Point-of-service (POS) — Often known as open-ended healthmaintenance organizations (HMOs), these plans encourage theuse of network providers through benefits reimbursement, butindividuals may choose providers outside the plan at the timeservice is rendered, but at a greater cost.
Physician-Hospital Organization (PHO) — A community-based affiliation of doctors and hospitals.
Preferred Provider Organization (PPO) — A health plan witha network of providers whose services are available toenrollees at lower costs than the services of non-networkproviders. PPO enrollees may self-refer to any networkprovider at any time. PPO enrollees also may go out-of-network at a higher cost.
Preventive medicine — Care that increases knowledge ofnutrition and disease with the aim of promoting health. Thescope of preventive medicine has been extended beyond justwarding off communicable diseases through immunizations.Today, early detection of a disease, especially during the earlychildhood years, as well as the ability to inhibit furtherdeterioration of bodily functions, are among the most fruitfulareas of preventive medicine. The potential for effective long-term cost-containment may be the greatest in this area ofhealth care.
Primary Care — Medical practice based on direct contact withthe patient without referral from another physician. Suchpractice is undertaken by doctors trained in various waysincluding pediatricians, obstetricians, general internists, familyphysicians and general practitioners. In addition, manyspecialists engage in a significant amount of primary care.
Related Documents











