CHEST / 88 / 6 I DECEMBER, 1985 829 Hypoxemia in Acute Pulmonary Embolism Yann Huet, M.D.;* Francots Lemaire, M.D.;* Christian Brun-Buisson, M.D.;* William A. Knaus, M.D.;*t Bernard Teisseire, Ph.D.;1: Didier Payen, M.D.;* and Didier Mathieu, M.D. Most patients with severe, acute pulmonary embolism (PE) have arterial hypoxemia. To further define the respective roles of ventilation to perfusion (VA/Q) mismatch and in- trapulmonary shunt in the mechanism of hypoxemia, we used both right heart catheterization and the six inert gas elimination technique in seven patients with severe, acute PE (mean vascular obstruction, 55 percent) and hypoxemia (mean Pa08, 67±11 mm Hg). None had previous cardiopul- monary disease, and all were studied within the first ten days of initial symptoms. Increased calculated venous ad- mixture (mean QVt/QT 16.6 ± 5.1 percent) was present in all patients. The relative contributions of VA/() mismatching and shunt to this venous admixture varied, however, accord- ing to pulmonary radiographic abnormalities and the time elapsed from initial symptoms to the gas exchange study, cute pulmonary embolism (PE) remains one of the more common diagnoses of acutely ill, hospi- talized patients and one of the more frequent complica- tions to occur during hospitalization for other disor- ders.’2 Hypoxemia is a consistent and important clinical feature of PE Its pathophysiology and pre- cise clinical significance in man, however, have not been clearly established. Ventilation/perfusion (VA/a) abnormalities,45 impaired diffusion,3 and intrapulmon- ary shunting, as well as right-to-left intracardiac shunts,4’6’7 all have been implicated, but the exact role of each remains unclear. Although hypoxemia has been related to the degree of pulmonary vascular obstruction (PVO),8 there are reports of massive PE with normal arterial oxygen tension (Pa02).#{176}No clear relationship between other clinical characteristics and the PaO, has been found. Variations in the timing and methods used to assess hypoxemia in previous studies may have contributed to this confusion. The major gas exchange studies in humans were performed long, frequently months, *SeMce de Reanimation M#{233}dicale, H#{244}pital Henri Mondor and Universit#{233} Paris-Val de Mane, France. tICU Research Unit, The George Washington University Medical Center, Washington, DC. Laboratoire des echanges gazeux (INSERM U 138), H#{244}pital Henri Mondor and Universit#{233} Paris-Val de Mane. §Service de Radiologie, H#{244}pital Henri Mondor and Universit#{233} Paris-Val de Marne. This work was supported in part by a grant from the D#{233}partement de Pharmacologie Clinique, H#{244}pital Henri Mondor, Creteil. Presented at the Annual Meeting of the American Thoracic Society, Anaheim, Calif, May, 1985. Manuscript received April 2; revision accepted July 15. Although all patients had some degree of VA/(I mismatch, the two patients studied early (ie, <48 hours following acute FE) had normal chest x-ray film findings and no significant shunt; VA/ mismatching accounted for most of the hypox- emia. In the others a shunt (3 to 17 percent of cardiac output) was recorded along with radiographic evidence of atelec- tasis or infiltrates and accounted for most of the venous admixture in one. In all patients, a low mixed venous oxygen tension (27 ± 5 mm Hg) additionally contributed to the hypoxemia. Our findings suggest that the initial hypoxemia of acute FE is caused by an altered distribution of ventilation to perfusion. Intrapulmonary shunting contributes signifi- cantly to hypoxemia only when atelectasis or another cause of lung volume loss develops. after the PE. In one of these, Wilson et al’#{176} suggested that atelectasis and shunt accounted for most of the hypoxemia, whereas Kafer2 attributed the major role to VA/Q mismatching. In these studies the investigators were unable to examine directly the relative contribu- tions of “A/a mismatching vs shunt at different times after the embolus. Both studies also used the oxygen method to assess hypoxemia, and the degree of in- trapulmonary shunting was not measured but inferred using the alveolar-arterial oxygen difference. Today, bedside right heart catheterization gives an accurate evaluation of the contribution of cardiac factors to the hypoxemia.” The recent introduction by Wagner et al’2 of the multiple inert gas elimination technique allows a more precise evaluation of VA/ distributions than was possible using the oxygen method alone. In this study, we combined these two techniques to study seven patients with recent, angiographically documented acute PE. Our aim was to determine the mechanism of their hypoxemia by relating the timing of our investigation and each patient’s chest x-ray abnormalities to the results of their gas exchange study. Patients PATIENTS AND METHODS Seven consecutive patients admitted to our Intensive Care Unit (ICU) for hemodynamic monitoring and treatment of acute PE were studied. Their individual clinical characteristics are in Table 1. None had any significant preexisting cardiopulmonary disease. One pa- Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CHEST / 88 / 6 I DECEMBER, 1985 829
Hypoxemia in Acute Pulmonary EmbolismYann Huet, M.D.;* Francots Lemaire, M.D.;*
Christian Brun-Buisson, M.D.;* William A. Knaus, M.D.;*t
Bernard Teisseire, Ph.D.;1: Didier Payen, M.D.;* and
Didier Mathieu, M.D.�
Most patients with severe, acute pulmonary embolism (PE)
have arterial hypoxemia. To further define the respectiveroles of ventilation to perfusion (VA/Q) mismatch and in-
trapulmonary shunt in the mechanism of hypoxemia, weused both right heart catheterization and the six inert gas
elimination technique in seven patients with severe, acutePE (mean vascular obstruction, 55 percent) and hypoxemia(mean Pa08, 67±11 mm Hg). None had previous cardiopul-monary disease, and all were studied within the first ten
days of initial symptoms. Increased calculated venous ad-mixture (mean QV�t/QT 16.6 ± 5.1 percent) was present inall patients. The relative contributions of VA/() mismatching
and shunt to this venous admixture varied, however, accord-ing to pulmonary radiographic abnormalities and the timeelapsed from initial symptoms to the gas exchange study,
cute pulmonary embolism (PE) remains one of the
more common diagnoses of acutely ill, hospi-
talized patients and one of the more frequent complica-
tions to occur during hospitalization for other disor-
ders.’2 Hypoxemia is a consistent and important
clinical feature of PE � Its pathophysiology and pre-
cise clinical significance in man, however, have not
been clearly established. Ventilation/perfusion (VA/a)
abnormalities,45 impaired diffusion,3 and intrapulmon-
ary shunting, as well as right-to-left intracardiac
shunts,4’6’7 all have been implicated, but the exact role
of each remains unclear.
Although hypoxemia has been related to the degree
of pulmonary vascular obstruction (PVO),8 there are
reports of massive PE with normal arterial oxygen
tension (Pa02).#{176}No clear relationship between other
clinical characteristics and the PaO, has been found.
Variations in the timing and methods used to assess
hypoxemia in previous studies may have contributed to
this confusion. The major gas exchange studies in
humans were performed long, frequently months,
*SeMce de Reanimation M#{233}dicale, H#{244}pital Henri Mondor and
Universit#{233} Paris-Val de Mane, France.tICU Research Unit, The George Washington University Medical
Center, Washington, DC.�Laboratoire des echanges gazeux (INSERM U 138), H#{244}pitalHenri
Mondor and Universit#{233} Paris-Val de Mane.§Service de Radiologie, H#{244}pital Henri Mondor and Universit#{233}
Paris-Val de Marne.This work was supported in part by a grant from the D#{233}partementde Pharmacologie Clinique, H#{244}pital Henri Mondor, Creteil.Presented at the Annual Meeting of the American Thoracic Society,Anaheim, Calif, May, 1985.
Manuscript received April 2; revision accepted July 15.
Although all patients had some degree of VA/(I mismatch,the two patients studied early (ie, <48 hours following acute
FE) had normal chest x-ray film findings and no significantshunt; VA/� mismatching accounted for most of the hypox-emia. In the others a shunt (3 to 17 percent of cardiac output)was recorded along with radiographic evidence of atelec-
tasis or infiltrates and accounted for most of the venousadmixture in one. In all patients, a low mixed venous oxygentension (27 ± 5 mm Hg) additionally contributed to thehypoxemia. Our findings suggest that the initial hypoxemia
of acute FE is caused by an altered distribution of ventilationto perfusion. Intrapulmonary shunting contributes signifi-
cantly to hypoxemia only when atelectasis or another cause
of lung volume loss develops.
after the PE. In one of these, Wilson et al’#{176}suggested
that atelectasis and shunt accounted for most of the
hypoxemia, whereas Kafer2 attributed the major role to
VA/Q mismatching. In these studies the investigators
were unable to examine directly the relative contribu-
tions of “A/a mismatching vs shunt at different times
after the embolus. Both studies also used the oxygen
method to assess hypoxemia, and the degree of in-
trapulmonary shunting was not measured but inferred
using the alveolar-arterial oxygen difference.
Today, bedside right heart catheterization gives an
accurate evaluation of the contribution of cardiac
factors to the hypoxemia.” The recent introduction by
Wagner et al’2 of the multiple inert gas elimination
technique allows a more precise evaluation of VA/�
distributions than was possible using the oxygen
method alone.
In this study, we combined these two techniques to
study seven patients with recent, angiographically
documented acute PE. Our aim was to determine the
mechanism of their hypoxemia by relating the timing
of our investigation and each patient’s chest x-ray
abnormalities to the results of their gas exchange
study.
Patients
PATIENTS AND METHODS
Seven consecutive patients admitted to our Intensive Care Unit
(ICU) for hemodynamic monitoring and treatment of acute PE were
studied. Their individual clinical characteristics are in Table 1. None
had any significant preexisting cardiopulmonary disease. One pa-
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

Table 1-Clinical Features and Chest X-ray Findings in 7 Patients with Acute Pulmonary Embolism
830 Hypoxemla In Acute Pulmonary Embolism (Huet of a!)
Clinical Features
. Studyl-
Patient Age,
Hours Since
Occurrence Precipitating
.
Pulmonary
Vascular
X-ray Fi ndings at Time of
..
Elevated Platelike
No. * yr/Sex of PE Cause Obstructiont Diaphragm Atelectasis Infiltrates
1 4IJF 24 Immobilization
Pelvic surgery
58 + 0 0
2 41/M 48 Lower limb
fracture
60 0 0 0
3 40/F 84 Immobilization
Hepatic cancer
65 + + + + 0
4 69/F 102 Lower limb
fracture
56 0 + +
5 50/M 128 Immobilization
Neurosurgery
35 + + + + +
6 61/M 192 Immobilization
Abdominal surgery
65 + + + + + +
7 50/M 216 Lower limb
fracture
50 ++ ++ ++
*Numbering according to time elapsed since initial symptoms of embolism.
tIn % of pulmonary vascular bed, estimated according to index described by Tibutt et al.#{176}
�Notation as follows: 0 sign absent; + minimal changes; + + marked and/or multiple changes.
tient had suffered a pulmonary embolism five yeas before but had no
residual effects. The diagnosis of PE was made on clinical history andthe results of a pulmonary angiogram perfurmed within a few hoursof ICU admission. The degree of PVO was determined using the
index described by Tibutt et al.#{176}A Swan-Ganz catheter and radialartery line were already in place. The gas exchange study was
perfbrmed on the first day in the ICU, approximately two hours after
the pulmonary angiogram. The delay between the first symptom ofPE (acute chest pain and/or dyspnea) and the inert gas study was
carefully determined and ranged between one and nine days (Table1). The patients were receiving only heparin therapy at the time ofthe study. No vasoactive drug was used. After the study, we gave
urokinase to all except patient 5, who was recovering from recentneurosurgery.
Methods
The gas exchange study was done with patients in a semirecum-
bent position. All were breathing spontaneously via a face mask with
humidified room air or supplemental oxygen (patients 3 and 7) as
required to maintain an adequate oxygen arterial partial pressure.
The masks were tightly fitted to the patient’s face so that no air leaks
occurred. Patients breathed through a circuit consisting of an 0,
blender, a humidifier, and a specially designed heated mixing box via
a one-way valve. The expiratory tubing was also heated to prevent
condensation and extraction of the more soluble gas, ie, acetone.
In each patient, the following measurements and calculations
were made: (1) minute ventilation WE) and tidal volume (VT) using a
calibrated Wright spirometer; (2) fraction of inspired 0, (Flo,) by
sampling gas in the inspiratory line of the circuit; (3) right atrial,
pulmonary, and systemic arterial pressures (Statham P23 DB trans-
ducer and Honeywell recorder); (4) cardiac index (CI), derived from
cardiac output (CO) measured by the thermodilution technique
perfurmed in triplicate (CO computer 9520, A. Edwards Laborato-
ries); (5) arterial and mixed venous oxygen tension and carbon
dioxide tension (PaO,, P�O,, PaCO,) (ABL 30, Radiometer
Copenhagen) and 0, saturation (SaC), and S�O,) (OSMII; Radi-
ometer); (6) total pulmonary resistance (TPR) calculated as mean
pulmonary arterial pressure (PAP) divided by cardiac index (pulmo-
nary capillary wedge pressure measurements were possible only in
two patients, most likely because of extensive pulmonary arterial
obstruction); (7) venous admixture (QVAJQT) using the oxygen
method and computed with the standard equation of Berggren; (8)
physiologic dead space assessed by the Bohr dead space for carbon
dioxide calculated as (arterial-mixed expired) divided by PaCO,.
Anatomic dead space was assumed from body weight (1 mI/Ib) plus
instrumental dead space (80 ml); (9) distribution of”.&/(� ratios using
the multiple inert gas elimination technique, as described by Evans
and Wagner.’4
A brief summary of this last technique follows. Six inert gases
(sulfur hexafluoride [SF61, ethane, cyclopropane, halopropane,
ether, and acetone) were equilibrated in a 5 percent dextrose
solution and infused intravenously (IV) at a constant rate of 5 mI/mm
for 25 minutes. Then, simultaneous 15-mI blood samples were drawn
from the pulmonary artery and a systemic artery for analysis of the
inert gas concentrations. At the same time, 50 ml of expired gas was
sampled. The blood samples were equilibrated with nitrogen in a
heated bath for 45 minutes.
The equilibrated blood and the expired gas samples were analyzed
for SF6 by an electron capture detector (Packard 429; Packard
Instrument Co) and for the five other gases by a flame ionization
detector (Packard). The blood solubility coefficient of each gas wasdetermined for each patient. The relative concentrations of the inert
gases in arterial and mixed venous samples were derived from the
equilibrated samples and the measured solubilities. The error of
measurement of SF6 determined in our laboratory was 1.3 percent.
and less than 1.8 percent for the other five gases.�S
Retention-solubility and excretion-solubility curves were then
constructed. From these, the best approximation of the ventilation-
perfusion distributions was determined, using the ridge regression
technique.’4 The mean residual sum of square was 3.2 ± 2.0, indicat-ing compatibility between the distribution curves and the inert gas
ram data.’4 A computer-assisted analysis of the distribution of the
VA/Q ratios allowed the determination of shunt (Qs/Qt); ie, Y..�JQ
<0.005; low VA/Q; ie, 0.005<VA/Q<0.1; high VA/Q; je, 10<VA/Q
<100; and dead space (Vu/VT); ie, VA/Q<100. The mean peak valuesof blood flow and ventilation distribution were determined, as well as
the SD of the distribution calculated with a natural log scale for the
abcissa (log SD), which is taken as an index of dispersion of blood flow
and ventilation. The ventilation to perfusion distributions were
combined with the mixed venous blood gases, cardiac output, VE,
and PaO, in the 50-compartment model’4 to predict the arterialpartial pressure of oxygen.
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

Patient
No.
HR,
beats/mm
RAP
mm Hg
PAP
mm Hg
SAP
mm Hg
CI,
Limin#{149}m’
TPR,
mm Hgfmin/m’/L
1 105 2 20 100 4.76 4.2
2 110 12 24 70 1.91 12.5
3 145 15 29 60 2.58 11.2
4 90 10 32 87 2.54 12.6
5 103 2 24 76 2.25 10.7
6 84 3 20 103 2.65 7.5
7 110 3 19 106 3.2 5.9
Mean 107 7 24 86 2.84 9.2
±SD 20 5 5 18 0.94 3.3
*HR = heat rate; �XP = mean right atrial pressure; = mean pulmonary arterial pressure; = mean systemic arterial pressure; CI =
cardiac index; TPR = total pulmonary resistance.
Table 2-Hemodynamic Data*
CHEST I 88 I 6 I DECEMBER, 1985 831
A standard chest x-ray film was also obtained on the day of the
study. Analysis of the films was made by two independent observers
who did not know the patient’s clinical characteristics. According to
Fleischner,” they described each film with emphasis on the follow-
ing: (1) elevated hemidiaphragm were marked present or absent; (2)
platelike atelectasis and areas of consolidation (“infiltrates”) were
scored 0 for no abnormality, + for slight opacities, and + + for
marked and/or multiple opacities. There was close agreement
between the two observers on all films.
All the data are expressed as mean ± SD.
RESULTS
In all tables and figures the patients are listed from 1
to 7 corresponding to the time elapsed from initial
symptoms of PE to the gas exchange study. The chest
x-ray findings are recorded in Table 1. The two patients
studied within two days of initial symptoms had no
parenchymal radiographic abnormalities. Localized
atelectasis and/or small infiltrates were common in
patients studied later. Pulmonary arterial obstruction
was substantial in all patients (mean value, 55 percent
of the pulmonary arterial vascular bed). There was no
obvious geographic relationship between radiologic
findings and site of embolus.
The standard hemodynamic data are shown in Table
2. Right atrial pressure ranged from 2 to 15 mm Hg.
Mean pulmonary arterial pressure was only moder-
ately increased (24 ± 5 mm Hg). Cardiac index was
moderately low (2.84±0.96 L/minm’) and notably
depressed in patient 2 (1.91 L/min#{149}m’). Total pulmo-
nary resistance was markedly elevated (9.2 ± 3.2
mmHg/L.min.m’). The hemodynamic impact of PE
was further evidenced by the increased arteriovenous
oxygen difference (mean 5.7 ± 1.5) with a calculated
mean oxygen consumption of 165±39 mllminm’. No
patient, however, had a systolic blood pressure less
than 90 mm Hg.
Standard gas exchanges are presented in Table 3. A
mild hypoxemia (mean 67 ± 11mm Hg) was recorded in
all patients. The alveolar-arterial 02 difference wasenlarged, but did not correlate to the degree of pul-
monary vascular obstruction or to the PaO,. Calculated
venous admixture (0, method) was elevated in each
patient, and ranged from 10.5 to 25.6 percent of cardiac
output (mean, 16.6 ± 5.1). Mixed venous oxygen partial
pressure and saturation were low (mean, 27 ± 5 mm Hg
and 52 ± 10 percent, respectively), as could be ex-
pected from the decreased cardiac index. The Bohr
dead space was markedly high, ranging from 44 to 75
percent of minute ventilation. All of the patients had an
arterial hypocarbia, and respiratory alkalosis was noted
in five of seven patients (mean pH, 7.47±0.04).
The inert gas study revealed different patterns of
VA/Q distribution in relation to the timing of the study
and the presence of x-ray abnormalities. Shunt, ie,
Table 3-Standard Gas Exchange in 7 Patients with Acute Pulmonary Embolism
Patient
No.
Weight,
kg
Height,
cm
PaO,,*
mm Hg
SaO,,
%
PaCO,,
mm Hg pH
P(A-a)0,,
mm Hg
P�O,,
mm Hg
S�O,,
mm Hg
(>VA/(>r,
%
VD/VT
(Bohr), %
1 45 162 66 94 34 7.45 42 34 65 19.3 57.6
2 73 180 60 93.5 27 7.52 55 25 45 15.8 66
3 71 170 90 95 29 7.40 88 25 43 10.5 75
4 62 157 62 92.5 26 7.49 53 21 44 15.3 62
5 68 180 65 92.5 31 7.49 43 25 45 15.8 47
6 72 170 57 89.5 37 7.42 44 29 57 25.6 62
7 80 171 70 93.5 26 7.51 112 32 65 18.5 44
Mean 67.3 170 67 93 30 7.47 - 27 52 16.6 59
±SD 10 8 11 2 4 0.04 - 5 10 5.1 10
*�4.ll patients breathing room air, except 3 and 7 (FIo,= 0.30). Abbreviations: PaO, = arterial partial pressure of oxygen; SaO, - arterial
oxyhemoglobin saturation; PaCO, = arterial carbon dioxide tension; P(A-a)O, = alveolar-arterial oxygen tension difference; P�O, = mixedvenous partial pressure of oxygen; Sc�o, = Mixed venous oxyhemoglobin saturation; QVA/QT = venous admixture (oxygen method); VD/VT
dead space (Bohr).
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

Perfusion Distribution, Ventilation Distribution,
Perfusion to Ventilation Anatomic
%CO %VE. . �,
Pa02/PaO,, Unventilated to Unperfused Dead Log SD of Log SD of
VE, VT, CO, Meas/Pred, Lung,t Lung,1 Space,* Mean VAJQ Blood Flow Mean VA/Q Ventilation
Limn ml L/mn mm Hg % % % Ratio Distribution Ratio Distribution
1 11 730 5.3 66/72 0 56.8 23.3 0.58 0.838 1.58 1.129
2 20 910 3 60/56 0.3 53 24.8 1.65 1.235 5.45 0.877
3 31 910 4.4 90/106 4.6 63.4 24.4 1.22 1.163 5.01 1.031
4 21 820 5.7 62168 3.2 55.1 24.5 1.39 1.142 2.19 0.877
5 14 700 6.1 65/63 4.2 40.5 30.8 1.03 0.842 1.96 0.723
6 13 650 5.4 57/66 8.8 58.4 32.5 0.89 0.815 1.26 0.494
7 17 770 6.3 70/66 16.9 35.4 31.2 1.66 0.691 2.68 0.676
Mean 18 784 5.2 67/71 5.4 51.8 1.20 0.950 2.88 0.83±SD 7 101 1.1 11/15 5.9 10.1 0.40 0.210 1.67 0.22
#{176}Abbreviations: iTE = expired ventilation; VT = tidal volume; CO = cardiac output.
t’7A/( 0.005.�‘A/() 100.§Anatomic dead space assumed from weight (1 ml/lb) plus instrumental dead space.
a
Sc
[
0
Atelectasis
o 0 ++ + + ++ ++
Infiltrat#{149}s ++ �1+
o 0 0 + ++
.15
.10 -
.fl.ii.flI I I I I I F I
1 2 3 4 5 6 7 8 9 Days
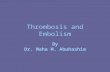
FIGURE 1. Association between shunt measured with the six inert gas technique and x-ray findings in relation
to time elapsed since the occurrence of PE. X-ray changes scored as: 0 = no abnormality; + = slightopacities; + + = marked and/or multiple opacities. It is clear that a significant shunt is present only when
chest x-ray is abnormal. Conversely, normal chest films were obtained in patients with no detectable shunt
and studied within 48 hours after embolism.
Table 4-Inert Gas Data#{176}
832 Hypoxemla In Acute Pulmonary Embolism (Huot of a!)
perfusion to the unventilated lung, was negligible in
patients 1 and 2 but accounted for a low but significant
part of cardiac output (3.2 to 8.8 percent) in patients 3
to 6, and to as much as 17 percent of cardiac output in
patient 7 (Table 4). There was no relationship between
venous admixture measured with the 02 method and
Qs/�t (six inert gases method).
Figure 1 correlates the shunt to the x-ray abnormali-
ties, and shows that a significant shunt occurred only
when atelectasis and/or infiltrates were seen radio-
graphically. Figure 2 shows the VAJQ distribution for
each patient and a normal control. Analysis of the \TA/�
distribution shows that the mean peak of blood flow,
although not markedly different from 1 (1.2 ± 0.4), had
a large dispersion (0.95 ± 0.21). Thus, a significant part
of perfusion was distributed to lung units with “A/(�
ratios lower than 1 (between 1 and 0.1), despite the
absence of a definite zone of very low VAJQ ratios. The
measured PaO, values were closely related to the PaO,
values predicted from the PiIO, and the VA/�
distributions (Table 4).
In all patients, ventilation to the unperfused areas
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

CO 4.4
SHUNT
1.1%1.4
YE 74
©DEAD SPACE
26.5%
C
E
IS0
000
0z4
I0,01 01 10
1.4
1.0
1.4
1.0
0.6
0.2
IA
1.0
o.e
0.2
/.‘
/ / \\�1/ .�‘.__J�
ii” 001 0.1 10 100
VE 31DEAD SPACE
63.4%
1�
/�‘��OI O�I�’ � 10 500
E
SHUNT
4.2%
0.6
0.2
1.4
1.0
0.6
0.2
1.4
1.0
0.8
0.2
YE 14
DEAD SPACE
40.5%
0
CO 5.7 (�) VE 21
SHUNT DEAD SPACE3i% 55.5%
W. I I ‘I I0 0.01 0.1 1 10 100
CO 5.4 © YE 13
SHUNT DEAD SPACE8.8% 58.4%
1.4
to
08
0.2
1.4
1.0
0.6
0.2
CO 6.3 YE I?
SHUNT DEAD SPACE
16.9% 35.4%
0:01 � � i#{243}o10 100
I.8
CHEST I 88 I 6 I DECEMBER, 1985 833
IS0
000
0z4
C03 VE 20
SHUNT DEAD SPACE0.3% 53.0%
I’
001 0.1 1 1�O tOO
CO 5.3
SHuNT0.0%
CO 4.4
SHUNT4.6%
VENTILATION - PERFUSION PATIO
A
1/III
-�V� #{149}#{149}‘t Io 0.01 0.1
YE 11DEAD SPACE
56.8%
VENTILATION-PERFUSION RATIO
FIGURE 2 (A, upper, and B, lower). Distribution of ventilation and perfusion, according to the ventilation!
perfusion ratios in a normal subject (0) and 7 patients with acute PE (ito 7). Co = cardiac output (Llmin); VE
= minute ventilation (Limmn). Normally, perfusion and ventilation are distributed to VA1Q around 1, with
tall and narrow unique peak. No shunt exists. By contrast, patients 1 and 2, studied within the 48 first hours,
have no shunt but a marked enlargement of the perfusion peak. Thus, a significant part of perfusion isdistributed to VA/Q between land 0.1. The ventilation peak is shifted to the right. Dead space is markedly
increased. Patients 6 and 7, studied later, have a normal mode of VAJQ ratio distribution, with a narrowed
perfusion peak around 1 and a shunt of 9 and 17 percent, respectively.
(dead space) was markedly high (52±10 percent) and
accounted for as much as 63 percent of YE in patient 3
(Table 4). Anatomic dead space assumed from body
weight was markedly smaller than inert gas dead space
(27 percent vs 52 percent, respectively). As a conse-
quence of the increased dead space, minute ventilation
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

834 Hypoxemla in Acute Pulmonary Embolism (Huet of a!)
(‘�‘E) was consistently increased (mean VE 17±7 L/min)
and was above 20 IJmin in patient 2. The mean peak of
ventilation was also consistently shifted to the high
VA/� ratios (mean, 2.88 ± 1.67), with a large dispersion
of the distribution (.83 ± .22).
The VA/Q diagrams in Figure 2 make it possible to
contrast these different patterns of VA/� distribution
and to compare them to normal. For example, in
patient 1, who was studied within 24 hours of the
embolic event and had normal chest x-ray film find-
ings, there is substantial dispersion of the perfusion
peak but no shunt. In patient 6, studied one week afterthe onset of symptoms and presenting with atelectasis
and infiltrates chest x-ray film, we found a shunt of 9
percent. His VA/Q distribution, however, is close to
normal, with a mean value centered on a VA/Q ratio of
approximately 1.
DIscUssIoN
Hypoxemia has been consistently demonstrated in
acute PE,345’#{176}but its etiology remains unclear. We
believed that part of the difficulty in discovering its
cause was related to variations in the selection of
patients or in the severity of the embolism and to the
long delay between initial symptoms and clinical
investigation.5 In addition, past studies have in-
terpreted hypoxemia in regard to associated changes in
P(A-a)0, and venous admixture.’#{176} The clinical signifi-
cance of these measurements are difficult to deter-
mine, since they are influenced by shunt, VAJ�
mismatching, and impaired diffusion.’7
In this study, we examined a group of patients with
large (mean vascular obstruction 55 percent) but
nonlethal acute pulmonary embolism shortly after
their first symptoms. All were hypoxemic (mean PaO,,
67 ± II), and each had moderate hemodynamic depres-
sion from the acute embolism, but none required
vasoactive drugs. We combined right heart catheteri-
zation with the multiple inert gas elimination tech-
nique to determine the relative impact of pulmonary
shunt, ‘s’A/Q mismatch, impaired diffusion, and cardiac
factors on the hypoxemia. We found that their hypox-
emia was caused by different pulmonary mechanisms,
depending on chest x-ray findings and on the time
elapsed since the PE. In patients studied early follow-
ing embolism, hypoxemia was mainly due to perfusion
of lung units with low VA/C ratios (ie, VA/�
mismatching), without a significant contribution from
perfusion of blood through unventilated lung units, ie,
shunting (Fig 1 and 2). Shunt became a significant
contributor to hypoxemia only if atelectasis or other
causes of lung volume loss developed. In our series
these characteristics were found in patients studied 48
hours or more after the initial symptoms.
Three major mechanisms have been proposed to
explain the pulmonary contribution to the hypoxemia
following acute PE: (1) a decreased 0, diffusing capac-
ity across the pulmonary membrane;3’8 (2) ventilation
to perfusion mismatching;46 and (3) shunting of blood,
at either the intracardiac or the intrapulmonary
level.�7’#{176} An embolus could theoretically cause a
decrease in diffusing capacity by reducing the surface
area of the alveolar capillary membrane available for
gas exchange or by decreasing the transit time of blood
flow through a reduced pulmonary vascular bed. But
the measured PaO, values were nearly identical to the
PaO, values predicted from the actual ‘,�A/�
distributions. This suggests that impaired diffusion was
not a cause for hypoxemia in our patients, a finding in
agreement with several recent experimental and clini-
cal studies.’�”
In contrast, in most of our patients an increased
venous admixture (0, method) in the absence of a
parallel increase in Qs/�t (inert gases method) indi-
cated that VAIQ mismatching accounted for a substan-
tial portion of their hypoxemia. This was most apparent
in patients studied early, eg, 1 and 2, in whom virtually
no shunt was found despite a venous admixture of 19
and 16 percent of cardiac output. The inert gas study
confirmed the VA/� mismatching in these patients by
documenting increased dispersion of perfusion, with-
out a definite zone of very low � (Fig 2). The low
VA/� ratios may be explained on the basis of an
increased perfusion to the nonembolic lung.” This was
the conclusion from a recent automated computer
analysis of ventilation-perfusion lung scans in II pa-
tients with acute pulmonary emboli and normal chest
x-ray findings.” In each of these patients the analysis
showed lung areas remote from those affected by the
emboli that had an abnormal matching of ventilation to
perfusion with relative overperfusion.
It has also been suggested that this \TA/� mismatch
could be caused by selective pneumoconstriction in
areas contiguous to the embolic lung that remain per-
fused.” This has been demonstrated in experimental
canine thromboembolism and is attributed to reflex
bronchoconstriction or pneumoconstriction.’4 Bron-
choconstriction has also been consistently shown in
human pulmonary embolism,4 and a shift of ventilation
away from the unperfused lung has been demonstrated
in man after the temporary occlusion of one pulmonary
artery.” This bronchoconstriction or pneumoconstric-
tion may then be responsible for subsequent loss of
lung volume in the embolic lung.9
Our data suggest that when such volume loss occurs,
shunt enters the clinical picture. The high incidence of
discoid atelectasis in patients with measurable shunts
has already been emphasized.’#{176} In experimental PE
studies, shunt as a major contributor to hypoxemia is
usually reported when alveolar collapse is seen at
autopsy. Wilson et al’#{176}found that they could tem-
porarily lower their patients’ P(A-a)O, if they were
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

CHEST I 88 I 6 I DECEMBER, 1985 835
encouraged to breathe 80 to ifi percent of their
predicted inspiratory capacity, thus decreasing the
amount of focal alveolar collapse. Similarly, no shunt
was demonstrated in the study by Caldini6 when
mechanical ventilation with periodic sighs was used. In
the patients we studied, clinically significant shunting
was found only in those with atelectasis and infiltrates
(Fig 1). It may be that significant loss of lung volume
and alveolar collapse developed in lung areas corre-
sponding to those of pulmonary vascular obstruction
and that early reperfusion of these zones produced
shunting.
Pulmonary edema from alteration of pulmonary
alveolar-capillary permeability or from increased blood
flow to the still-perfused lung is an alternative explana-
tion for shunting in acute PE, and alveolar edema has
repeatedly been shown in animal experiments.’6’7
However, convincing clinical reports of PE with acute
pulmonary edema in patients free of left heart disease
are distinctly rare.” None of our patients had x-ray
evidence of acute edema in nonembolic areas of the
lung. Subclinical focal pulmonary edema, however,
cannot be excluded in the areas of consolidation.
Remaining explanations for right-to-left shunting in
acute PE are intracardiac shunts from the opening of a
patent foramen ovale6’7 or intrapulmonary shunts from
the opening of precapillary shunts.3 The opening of a
patent foramen ovale cannot be entirely ruled out in
our patients, but their right atrial pressures were in the
normal range, especially in those with the largest
shunts. The opening of precapillary shunts never has
been demonstrated in patients or in recent experimen-
tal studies,” and no relationship was found between
shunt and PAP in our patients.
As already mentioned, however, the magnitude of V
A/� mismatching and shunt were moderate and dispro-
portionate to the degree of hypoxemia recorded in our
patients. This suggests that an additional factor may
worsen the hypoxemia. Except patient 1, all of our
patients suffered from hemodynamic changes associ-
ated with their acute PE. Because of their low cardiac
output, they had low P�O, (27 ± 5 mm Hg), and this no
doubt contributed to their hypoxemia. The potential
role of a low P�O, for any level of shunt or low VA/� has
recently been emphasized by Dantzker and Bower.’6
Assuming that VA/� distributions would remain un-
changed, these authors calculated that a marked in-
crease in predicted PaO, would result from an increase
of Pi�O, to 40mm Hg. This explains why PaO, values in
this study were significantly reduced despite relatively
mild degrees of’�/� mismatch and shunt. Therefore,
depression of cardiovascular function is a major con-
tributor to the hypoxemia in acute PE.
Dead space was consistently increased in all pa-
tients. Consequently, minute ventilation was mark-
edly increased, up to 31 L in patient 3, and the peak of
ventilation shifted to the right, with a mean value of
2.88. Measured dead space, using both the expired
CO, (Bohr, 59 ± 10 percent) and the excretion of
soluble gases (inert gas dead space, 52±10 percent)
was higher than the predicted anatomic dead space
(27 ± 4 percent), corresponding to the ventilation of
unperfused lung. In addition to the dead space,
patients studied within the first 48 hours following PE
had a supplemental mode of ventilation, with high
VA/Q ratios (Fig 2). In dog experiments, Dantzker et al
have already demonstrated the early occurrence of
such a high mode, with VA/Q between 10 and 100, that
disappeared after a few hours.
The major limitation to our findings is the small
number of patients studied and that, for practical
reasons, the inert gas study could not be repeated
within individuals to document changes in VA/Q and
shunt over time. A larger number of patients would
have permitted the use of stronger statistical testing to
demonstrate the relationship between atelectasis and
shunting. Repeated determinations of gas exchange in
the same patient would have further supported the
observations made between individuals. Neverthe-
less, we believe that the results in these individuals are
firm enough to suggest that when an acutely ill patient
has acute PE, initial hypoxemia is caused by VA/Qmismatch. Only when atelectasis or other indications
of lung volume loss develop should the hypoxemia be
attributed to shunting. Initial therapeutic measures
therefore should be aimed at preserving or, if possible,
increasing the functional residual capacity.” Depend-
ing on the clinical circumstances, rapid initial support
of cardiovascular function may also be a critical part of
management.
CONCLUSION
The primary cause of the initial hypoxemia in acute
pulmonary embolism appears to be a disturbed pat-
tern of ventilation to perfusion. Simultaneous depres-
sion of cardiac function further contributes to hypox-
emia, but intrapulmonary shunting does not become
important until atelectasis or another cause of lung
volume loss develop.
ACKNOWLEDGMENT: We are indebted to Robert Herigault andFrancoise Veyssi#{232}re for her excellent technical assistance, and toMrs. Fiorella Delcampe and Maryse Gu#{233}rinfor preparation of themanuscript.
REFERENCES
1 Dalen JE, Alpert JS. Natural history of pulmonary embolism.
Prog Cardiovasc Dis 1975; 17:259-70
2 Moser KM. Pulmonary embolism. Am Rev Respir Dis 1977;
115:829-52
3 Robin ED, Forkner CE, Bromberg PA, Croteau Jr, Travis DM.
Alveolar gas exchange in clinical pulmonary embolism. N EngI JMed 1960; 262:283-87
4 Sasahara AA, Cannilla JE, Morse RL, Sidd JJ, Tremblay GM.
Clinical and physiologic studies in pulmonary thromboem-
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013

836 Hypoxemia in Acute Pulmonary Embolism (Huef of a!)
bolism. Am J Cardiol 1967; 20:10-20
5 Kafer ER. Respiratory function in pulmonary thromboembolic
disease. Am J Med 1969; 47:904-15
6 Caldini P. Pulmonary hemodynamics and arterial oxygen satura-
tion in pulmonary embolism. J AppI Physiol 1965; 20:184-90
7 Gazzanica AR, Dalen JE. Paradoxical embolism: its pathophysi-
ology and clinical recognition. Ann Surg 1970; 171:137-41
8 McIntyre KM, Sasahara AA. The hemodynamic response to pul-
monary embolism in patients without prior cardiopulmonary
disease. Am J Cardiol 1971; 28:288-94
9 Jardin F, Bardet J, Sanchez A, Blanchet F, Bourdarias JP,
Margairaz A. Massive pulmonary embolism without arterial
hypoxemia. Intensive Care Med 1977; 3:77-80
10 Wilson JE, Pierce AK, Johnson RL, Wings ER, Hazull WR,
Curry CC, et al. Hypoxemia in pulmonary embolism: a clinical
study. J Clin Invest 1971; 50:481-91
ii Jardin F, Gurdjian F, Desfonds P, Fouilladieu JL, Margairaz A.
Hemodynamic factors influencing arterial hypoxemia in massive
pulmonary embolism with circulatory failure. Circulation 1979;
59:909-12
12 Wagner PD, Laravuso RB, Uhl R, West JB. Continuous distribu-
tions of ventilation-perfusion ratios in normal subjects breathing
air and 100 per cent 0,. J Clin Invest 1974; 54:54-68
13 ‘flbutt DA, Fletcher EWL, Thomas ML, Sutton GC, Miller
GAH. Evaluation of a method fur quantifying the angiographic
severity of major pulmonary embolism. Am J Radiol 1975; 125:
895-99
14 Evans JW, Wagner PD. Limits on VA/Q distribution from
analysis experimental inert gas elimination. J Appi Physiol 1977;
42:889-98
15 Matamis D, Lemaire F, Harf A, Teisseire B, Brun Buisson C.
Redistribution of pulmonary blood flow induced by positive end
expiratory pressure and dopamine infusion in acute respiratory
failure. Am Rev Respir Dis 1984; 10:39-44
16 Fleischner FG. Observations on the radiologic changes in pul-
monary embolism. In: Sasahara AA, Stein M, eds. Pulmonary
embolic disease. New York: Crone & Stratton, 1965:206-13
17 Wagner PD, West JB. Ventilation-perfusion relationships. In:
West JB, ed. Pulmonary gas exchange (vol 1). New York:
Academic Press, 1980:219-62
18 Williams MH. Mechanical vs reflex effects of diffuse pulmonary
embolism in anesthetized dogs. Circ Res 1956; 4:325-31
19 Levy SE, Simmons DH. Mechanism of arterial hypoxemia
following pulmonary thrombo-embolism in dogs. J Appl Physiol
1975; 39:41-46
20 Dantzker DR, Wagner PD, Tornabene VW, Alazraki NP, West
JB. Gas exchange after pulmonary thromboembolization in dogs.
Circ Res 1978; 42:92-103
21 D’Alonzo GE, Bower JS, Dettart P, Dantzker PD: The mecha-
nisms of abnormal gas exchange in acute massive pulmonary
embolism. Am Rev Respir Dis 1983; 128:170-72
22 Meignan M, Harf A, Oliveira L, Simonneau C, Cinotti L,
Duroux P, et al. Overperfusion of non embolic lung as a cause of
hypoxemia in pulmonary embolism [Abstract]. Am Rev Respir
Dis 1983; 116:A127
23 Burton CH, Seed WA, Vernon P. Observations on the mecha-
nism of hypoxemia in acute minor pulmonary embolism. Br Med
J 1984; 289:276-79
24 Levy SE, Simmons DH. Redistribution of alveolar ventilation
following pulmonary thromboembolism in the dog. J Appl
Physiol 1974; 36:60-68
25 Even F, Sors H, Reynaud F, Safran D, Duroux F, Ruff F
L’hypoventilation alveolaire r#{233}gionale par constriction hypocap-
nique des voies a#{233}riennes. Bull Eur Physiopathol Respir 1979;
15:145-66
26 Young I, Mazzone RW, Wagner PD. Identification of functional
lung unit in the dog by graded vascular embolization. J AppI
Physiol 1980; 49:132-41
27 Johnson A, Malik AB. Effects of different size microemboli in
lung fluid and protein exchange. J AppI Physiol 1981; 51:461-64
28 Manier C, Mora B, Castaing Y, Guenard H. Oed#{232}me pulmonaire
au cours d’une embolie pulmonaire. Bull Eur Physiopathol
Respir 1984; 20:55-60
29 Cheney PW, Paulin J, Fevens BS, Allen D. Effect of pulmonary
microembolism on arterio venous shunt flow. J Thorac Cardiovasc
Surg 1978; 75:473-77
30 Dantzker DR, Bower JS. Mechanisms of gas exchange abnormal-
ity in patients with chronic obliterative pulmonary vascular
disease. J Clin Invest 1977; 59:203- 16
Downloaded From: http://journal.publications.chestnet.org/ on 08/10/2013
Related Documents