Hirsutism Dr Fida Al-Asali

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
HirsutismDr Fida Al-Asali
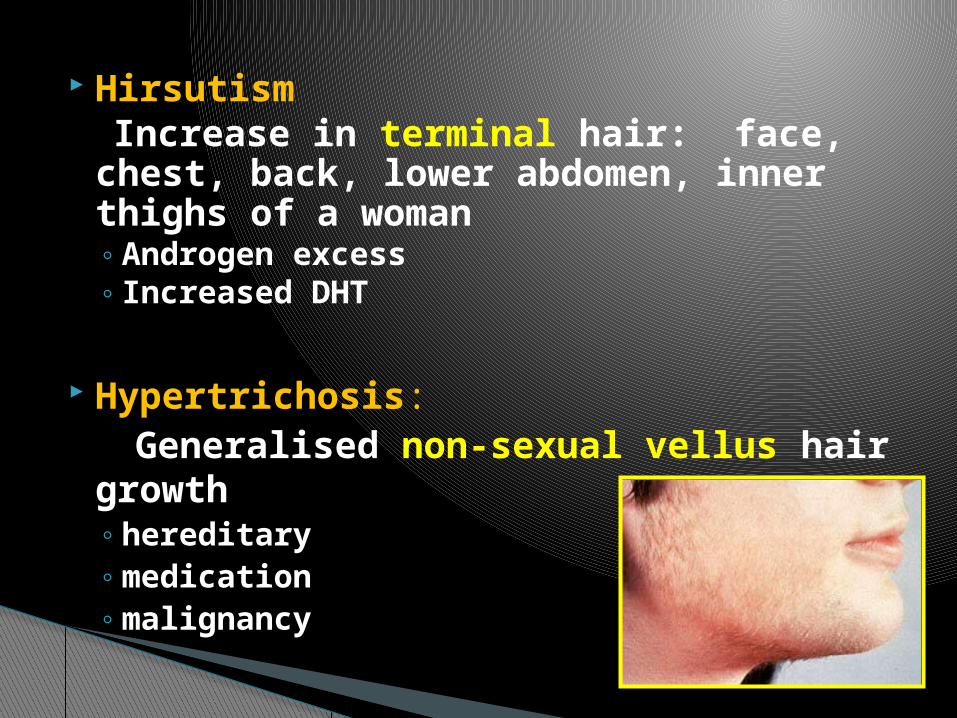
Hirsutism Increase in terminal hair: face, chest,
back, lower abdomen, inner thighs of a woman◦Androgen excess◦ Increased DHT
Hypertrichosis: Generalised non-sexual vellus hair
growth◦hereditary◦medication◦malignancy
Male features: Deepening voice, frontal balding, incr.
Muscle mass, clitoromegaly, breast atrophy, male body habitus
◦ Androgen excess◦ Adult onset CAH “21-hydroxylase
deficiency”◦ XY females◦ Iatrogenic◦ Cushing’s syndrome and acromegaly
Virilization

Adult hair 2 types Hair growth is dynamic Anagen - growing phase active mitoses in basal matrix e.g. scalp hair, face Catagen – rapid involution phase Telogen –Resting phase
Physiology

Androgens initiate growth and increase rate of
mitoses in all but scalp hair Estrogens : slow rate & initiation of
growth Progestins : minimal direct effect Pregnancy : can increase the
synchrony of hair growth, periods of growth & shedding
Endocrine
Factors influence Hair Growth
Local skin temperature Blood flow Summer > Winter
Non hormonal factors
Dehydroepiandrosterone (DHEA)-a weak carbon-5 androgen secreted principally by the andrenal gland
DHEAS almost 100% by adrenal gland Androstendione (A) - a weak carbon-4 androgen
secreted in equal amounts by the adrenal glands and ovaries
Testosterone (T)- a potent carbon-4 androgen secreted by the adrenal glands and ovaries and produced in adipose tissue from the conversion of androstendione
Dihydrotestosterone (DHT)-even more potent than testosterone.The conversion from testosterone is the result of action of 5 -a reductase
Main androgens
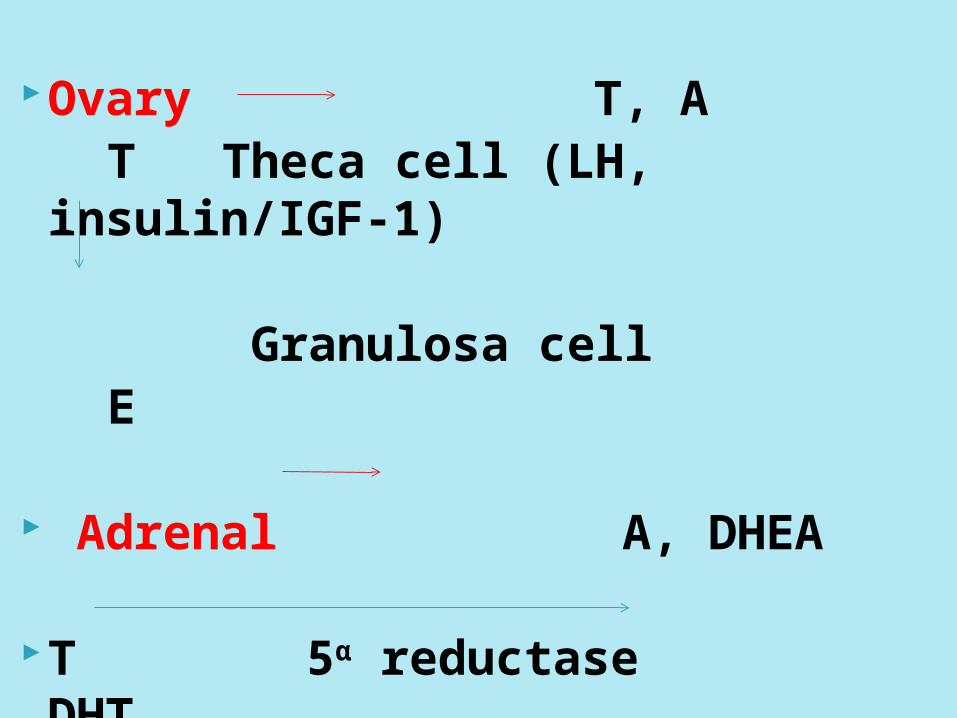
Ovary T, A T Theca cell (LH, insulin/IGF-1) Granulosa cell E
Adrenal A, DHEA
T 5α reductase DHT

Production rate in the normal female is 0.2 to 0.3 mg/day
Normal total testosterone concentration in serum is below 0.8ng/ml
◦50% peripheral conversion◦25% ovary( midcycle)◦25% adrenal
Testosterone
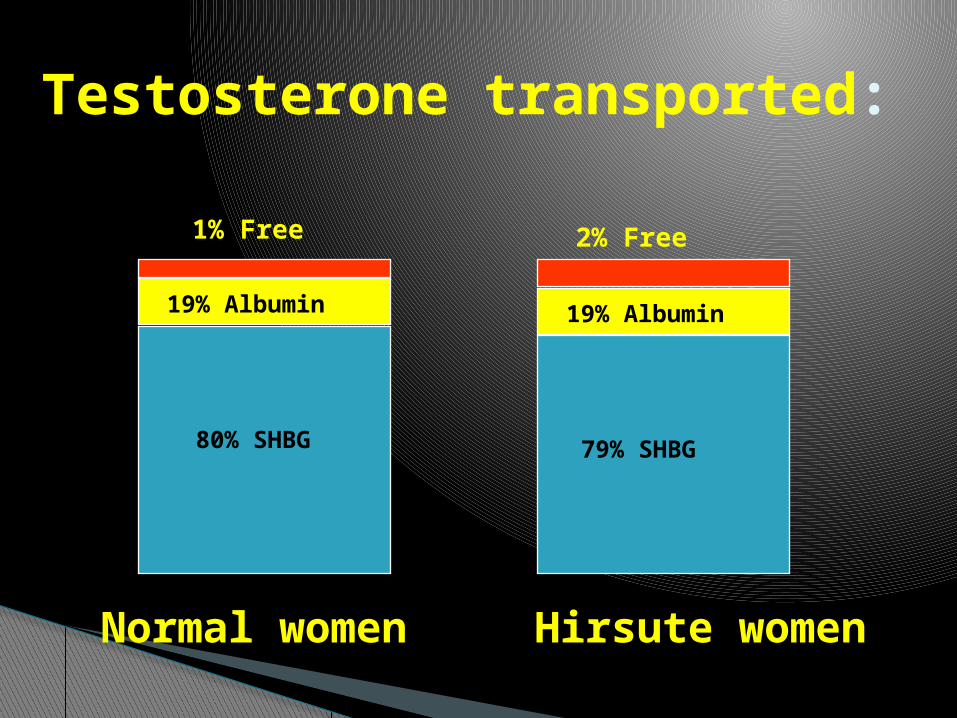
Testosterone transported:
Normal women Hirsute women
80% SHBG 79% SHBG
19% Albumin 19% Albumin
1% Free 2% Free

Cutaneus manifestation of hyperandrogenism
Women have male-pattern hair growth In areas :
upper lip chinsideburn area upper neck chestupper armlower abdomenintergluteal regionperineumthigh
Hirsutism
Hirsutism rating scale by Ferriman Gallwey>8 points - hirsutism
Variable – ethnic Higher in Africans & Mediterranean 5-10% of reproductive age
Hirsutism: Incidence
NOT a diagnosis but
a manifestation
Hirsutism
PCOS 75% Idiopatic hirsutism 15%Adrenal hyperplasia 3%Cushing’s disease 1%Hyperprolactinemia 1%Tumor of the ovary 1%Tumor of the adrenal 0,1%After medications 1%
Causes of hyperandrogenism:
Non Neoplastic vs Neoplastic
oCushing’s Syndrome Glucocorticoid excess by excessive ACTH
secretion with concomitant rise in androgen intermediates. adenomas, paraneoplastic syndromes,
adrenal tumors. SX: hirsutism, acne, menstrual irreg, etc…..
oCAH 21-alpha-hydroxylase = no GC/aldo, salt
wasting and adrenal insuff at birth. Female infants – ambig genitalia Adult onset – mild virilization and menstrual irreg
Adrenal Disorders

◦3B-hydroxylase & 3B-HSD Precursors shunted to testosterone & androstenedione
Females = hirsutism/virilization/cortisol def. & varying degrees MC excess/deficiency with respective enzyme deficiencies
Adrenal Disordres Cont
Non-neoplasticPCOS
Cycle of excess androgenic stimulation of LH cystic ovarian changes, chronic anovulation/amenorrhea, virilization, hirsutism, obesity,
LH-FSH ration > 2:1
Theca Lutein CystsTheca internal cells normally Androstenedione & TCysts excess androgens during nl or molar pregnancyHirsuitisms & ocassional virilization
Stromal Hyperplasia & HyperthecosisHyperplastic stroma or foci increased activityHirsuitism & virilizatoin with increased ovarian size
Ovarian Disorders
Neoplastic Functional Ovarian Tumors• Produce variable amounts of androgen Sex-cord mesenchymal tumors, Sertoli-Leydig
tumors, granulosa-theca tumores, hilar cell tumors, luteomas…..
Non-functional Ovarian Tumors Do not secrete androgens themselves but may stimulate proliferation in adjacent ovarian stromaKrukenberg’s tumor, cystademona…
A variety of drugs decrease SHGB, resulting in increased levels of free T to interact at cellular level.
Androgens and corticosteroids also SHBG
Examples: anabolic steroids, minoxidil, phenytoin, diazoxide, cyclosporin, danazol.
Drugs & Exogenous Hormones

History-detailed• Onset-duration, severity• Other symptoms of virilization• Menstrual hx• Infertility• Hx suggestive of other medical
conditions- • Cushing’s syndrome or hypothyroid
Medications
Clinical assessment of hirsutism
Evaluate severity using Ferriman-Gallwey scoring system
Signs of virilization Acanthosis nigricans Pelvic exam
P/E

Ferriman–Gallwey scoring system
Used to quantify the amount of hair growth.
Each area of the body is scored for the amount of hair.
6–8 :mild 8–15: serious > 15: overt

T, androstenedione, DHEAS ◦ adrenal source◦ Abdominal CT & medical tests r/o CAH or Cushings
DEAHS normal or minimally elevated◦ Ovarian source◦ Pelvice U/S r/o tumor
Elevated LH-FSH ratio◦ Ratio>3 suggests PCOS
Rapid Onset Virilization w/ T>200ng/dL◦ May indicate ovarian neoplasm
Investigations

Baseline 17-OH progesterone Dexamethasone suppression test Pelvic imaging
If androgen excess NOT readily evident: MRI, venous blood draws, Free T, 5-alpha reductase activity to check for peripheral T conversion
Diagnosis & Evaluation
Women with greater activity of 5 -a reductasein in the skin
Normal ovulationRegular menstrual cycleNormal hormone concentrations
Constitutional hirsutism
Mechanical removal of hair
◦ Shaving, plucking, bleaching, depilation◦ Electrolysis achieves permanent hair
removal. If done poorly, it maybe associated with scarring.
◦ Laser depilation is most effective in women with pale skin and dark hair.
Treatment
Adrenal nonneoplastic: pharmacological androgen suppression◦ Prednisone 5mg qhs◦ Antiandrogens such as spirinolactone
Ovarian nonneoplastic:◦ OCPs suppress LH/FSH and SHBG◦ Progesterone alone suppresses LH and T
catabolism◦ Gonadotropin releasing hormone agonists
suppress LH/FSH but requires estrogen replacement
Treatment

Suppression of LH and therefore suppression of androgen production by the ovarian theca cells
Increases production of SHBG, which in turn decreases free circulating androgens
Decreases androgen secretion by the adrenal gland
Progestogens can possess androgen activity in laboratory studies, but clinically there is no
difference in the clinical suppression of androgenic symptoms.
The best hormonal contraceptive is the one that is best tolerated by the individual.
COCP for hirsutism

The combination of drospirenone 3 mg and ethinyl oestradiol 30 mg (Yasmin) given cyclically is also effective for the treatment of hirsutism and acne associated with PCOS
Yasmin
2nd line monotherapy or in combination with OCP in severe cases
Work to suppress hirsutism by competitive inhibition at the level of the testosterone receptor.
All are equally effective. Should be combined with effective
contraceptive to avoid feminization of a male fetus. Cyproterone acetate SpironolactoneFlutamide Finasteride
Antiandrogens
The combination of an anti-androgen, cyproterone acetate (CPA, 2 mg/day) and ethinyl oestradiol (35 µg/day) (Diane) is very effective treatment when given cyclically.
The addition of CPA 10–100 mg/day on the first 10 days of the combined medication has proved effective for more severe cases.
Mechanism of action:1. suppression of LH release by the anterior
pituitary2. Blocks androgen receptors3. as a progestogen in suppressing the action
of 5a reductase4. in combination with ethinyl oestradiol, it
increases SHBG concentrations.
Cyproterone acetate

Blocks androgen receptors Inhibits 5α reductaseDose 50-200mg/day between days 4
and 22 of cycle ; 50-75mg/day- mild to moderate hirsutism; 100-200mg/day severe hirsutism
Effect is dose-dependentS.E diuresis Postural hyptension Menstrual irregularities Hyperkalemia
Spironolactone(aldosteron antagonist)

used in prostate cancer ,It inhibits the binding of 5a-DHT to androgen receptor)
Potent androgen receptor antagonistDose 250 mg or 500 mg/day. S.E hepatotoxicity, which may be
severe and the incidence seems to increase with higher doses.....liver function!.
Flutamide
Inhibitor of 5α reductaseDose :1–5 mg/dayS.E : mild GI disturbances, dry skin,
decreased libidoTeratogenic Consider effective contraception
Finasteride
Tpical antiprotozoal Acts locally to inhibit hair follicle
ornithine decarboxylase enzyme Improvement within few weeks Regrowth of hair when stopped S.E obstruction of sebaceous glands
and hence worsening of acne Enhances effect of laser treatment
Eflornithine(Vaniqa®)
Insulin sensitizing agents Metformin- Studies controversial weight loss GnRH agonists Surgical
•Polycystic ovarian syndrome is one of the most common causes of hirsutism.
•Weight loss in obese patients may improve hirsutism.
•Virilism usually indicates significant pathology.
•The oral contraceptive pill is the most commonly used single therapy for hirsutism.
KEY POINTS
Thank you
Dehydroepiandrosterone sulfate >800 = adrenal tumor 500-800 congenital adrenal hyperplasia adult onset , we
can do basline 17-OH hydroxelase Lesser elevations we should think of PCOS so we must do -FSH/LH ratio , TSH , PRL -free androgen index -FSH and estradiol level for primary ovarian faliure -testosterone studies= radioimmuno assay,
equilibrium dialysis,total T -lipid profile , fasting blood sugar -ovarian ultrasound
Laboratory test

Free cortizol ,,, dexamethasone suppression test
Abdominal imaging … CT scan If pituitary causes are suspected…imaging Think about constitutional hirsutism -MRI , 5-alpha-reducatse activity , free T,
venous blood draws
Related Documents
![Hirsutism (androgen excess) warda [compatibility mode]](https://static.cupdf.com/doc/110x72/559d189d1a28ab64558b469c/hirsutism-androgen-excess-warda-compatibility-mode.jpg)








![Therapeutic Department, Örebro Region County Hirsutism€¦ · hirsutism is controversial, as some experts recommend against . testing [50] and others recommend at least one determination](https://static.cupdf.com/doc/110x72/5ed76ed703f7cc5c8c4631f9/therapeutic-department-rebro-region-county-hirsutism-hirsutism-is-controversial.jpg)

