158 Endocrine System 2. Assess for changes in mental or emotional status. 3. Evaluate reflexes and neuromuscular response to stimuli. 4. Evaluate serum calcium levels. D. Pancreas problems. 1. Evaluate changes in weight, particularly increase in weight in the adult and decrease in weight in the child. 2. Evaluate alterations in fluid balance. 3. Evaluate changes in mental status. 4. Evaluate serum glucose levels. 5. Evaluate pancreatic enzyme studies. 6. Evaluate the abdomen for epigastric pain and abdominal discomfort. E. Adrenal glands. 1. Adrenal medulla. a. Evaluate changes in blood pressure. b. Assess for changes in metabolic rate. 2. Adrenal cortex. a. Evaluate changes in weight. b. Evaluate changes in skin color and texture, and in the presence and distribution of body hair. c. Assess cardiovascular system for instability as evidenced by labile blood pressure and cardiac output. d. Evaluate GI discomfort. e. Assess status of potassium and sodium levels. f. Assess for changes in glucose metabolism. g. Assess for changes in reproductive system and in sexual activity. h. Evaluate changes in muscle mass. Hyperpituitary: Acromegaly Acromegaly is most often the result of a benign slow ✽ growing tumor (pituitary adenoma) that secretes growth hormones. It occurs after the closure of epiphyses of the long bones. Data Collection A. Enlargement of the hands and feet and hypertrophy of the skin. B. Changes in facial features: protruding jaw, slanting forehead, and an increase in the size of the nose. PHYSIOLOGY OF THE ENDOCRINE SYSTEM A. Pituitary gland - Often referred to as the “master gland” because it secretes hormones that control hormone se- cretion of other endocrine glands. B. Thyroid gland - Primary function of thyroid hormone is to control the level of cellular metabolism by secreting thyroxin (T 4 ) and triiodothyronine (T 3 ). C. Parathyroid gland - Four small parathyroid glands are located near or embedded in the thyroid gland, which secrete parathyroid hormone (PTH) that is primarily involved in the control of serum calcium levels. D. Pancreas - Produces the enzymes trypsin, amylase, and lipase, which are necessary for the digestion and absorption of nutrients; contains the islets of Lang- erhans, which contain beta cells that are responsible for the production of insulin. Insulin is necessary for maintaining normal carbohydrate metabolism and glucose utilization. E. Adrenal glands – Main body is the adrenal cortex that is responsible for the secretion of glucocorticoids, mineralocorticoids, and adrenal sex hormones (andro- gens and estrogen); adrenal cortical function is essential for life. The adrenal medulla secretes catecholamines, epinephrine, and norepinephrine; under the influence of the sympathetic nervous system. System Data Collection A. Pituitary problems. 1. Assess for growth imbalance. 2. Assess for secondary characteristics appropriate for age. 3. Assess for hormonal imbalances throughout the en- docrine system organs. B. Thyroid problems. 1. Assess for changes in weight and appetite: increased or decreased. 2. Assess for intellectual development and mental changes: increased irritability, excitability, nervous- ness, altered mood and affect, confusion, and coma. 3. Assess for changes in hair and skin, altered general appearance, and sexual dysfunction. C. Parathyroid problems. 1. History of problems of calcium metabolism and thyroid surgery.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

158 CHAPTER 8 Endocrine System
158
Endocrine System
2. Assess for changes in mental or emotional status. 3. Evaluatereflexesandneuromuscularresponseto stimuli. 4. Evaluate serum calcium levels.D. Pancreasproblems. 1. Evaluatechangesinweight,particularlyincreasein weightintheadultanddecreaseinweightinthe child. 2. Evaluatealterationsinfluidbalance. 3. Evaluate changes in mental status. 4. Evaluate serum glucose levels. 5. Evaluatepancreaticenzymestudies. 6. Evaluatetheabdomenforepigastricpainand abdominaldiscomfort.E. Adrenalglands. 1. Adrenalmedulla. a. Evaluatechangesinbloodpressure. b. Assessforchangesinmetabolicrate. 2. Adrenalcortex. a. Evaluate changes in weight. b. Evaluatechangesinskincolorandtexture,and inthepresenceanddistributionofbodyhair. c. Assesscardiovascularsystemforinstabilityas evidencedbylabilebloodpressureandcardiac output. d. EvaluateGIdiscomfort. e. Assessstatusofpotassiumandsodiumlevels. f. Assessforchangesinglucosemetabolism. g. Assessforchangesinreproductivesystemandin sexualactivity. h. Evaluate changes in muscle mass.
Hyperpituitary: AcromegalyAcromegaly is most often the result of a benign slow ✽
growing tumor (pituitary adenoma) that secretes growth hormones. It occurs after the closure of epiphyses of the long bones.
Data CollectionA. Enlargementofthehandsandfeetandhypertrophyof theskin.B. Changesinfacialfeatures:protrudingjaw,slanting forehead,andanincreaseinthesizeofthenose.
PHYSIOLOGY OF THE ENDOCRINE SYSTEM
A. Pituitarygland-Oftenreferredtoasthe“mastergland” becauseitsecreteshormonesthatcontrolhormonese- cretionofotherendocrineglands.B. Thyroidgland-Primaryfunctionofthyroidhormoneis tocontrolthelevelofcellularmetabolismbysecreting thyroxin(T
4)andtriiodothyronine(T
3).
C. Parathyroidgland-Foursmallparathyroidglandsare locatednearorembeddedinthethyroidgland,which secreteparathyroidhormone(PTH)thatisprimarily involvedinthecontrolofserumcalciumlevels.D. Pancreas-Producestheenzymestrypsin,amylase, andlipase,whicharenecessaryforthedigestionand absorptionofnutrients;containstheisletsofLang- erhans,whichcontainbetacellsthatareresponsible fortheproductionofinsulin.Insulinisnecessaryfor maintainingnormalcarbohydratemetabolismand glucoseutilization.E. Adrenalglands–Mainbodyistheadrenalcortex thatisresponsibleforthesecretionofglucocorticoids, mineralocorticoids,andadrenalsexhormones(andro- gensandestrogen);adrenalcorticalfunctionis essentialforlife.Theadrenalmedullasecretes catecholamines,epinephrine,andnorepinephrine; undertheinfluenceofthesympatheticnervoussystem.
System Data CollectionA. Pituitaryproblems. 1. Assessforgrowthimbalance. 2. Assessforsecondarycharacteristicsappropriatefor age. 3. Assessforhormonalimbalancesthroughouttheen- docrinesystemorgans.B. Thyroidproblems. 1. Assessforchangesinweightandappetite:increased ordecreased. 2. Assessforintellectualdevelopmentandmental changes:increasedirritability,excitability,nervous- ness,alteredmoodandaffect,confusion,andcoma. 3. Assessforchangesinhairandskin,alteredgeneral appearance,andsexualdysfunction.C. Parathyroidproblems. 1. Historyofproblemsofcalciummetabolismand thyroidsurgery.

CHAPTER 8 Endocrine System 159
TreatmentSurgicalinterventionisprimarymethodofcorrectingprob-lem;hypophysectomymaybeaccomplishedbythetrans-sphenoidalapproach.
Nursing Interventionv Goal: Toprovidesupportivepreoperativecare(seeChapter3).v Goal: Toensurethattheclientwillnotexperiencecomplicationsafterhypophysectomy.A. Elevatethehead30degrees.B. Discouragecoughing,sneezing,orstrainingatstoolto preventcerebrospinalfluidleak.C. Assessforsymptomsofincreasingintracranialpressure (seeChapter15).D. Evaluateurineforexcessiveincreaseinvolume (greaterthan200mL/hr)orspecificgravityless than1.005(i.e.,developmentofdiabetesinsipidus).E. Frequentoralhygienewithnonirritatingsolutions.v Goal: Toassistclienttoreestablishhormonebalanceafterhypophysectomy(adrenalinsufficiencyandhypothy-roidismaremostcommoncomplications).A. AdministercorticosteroidsandADH-regulating medications(seeAppendix5-7).
Diabetes InsipidusDiabetes insipidus (DI) is a problem of the posterior ✽
pituitary characterized by a deficiency of ADH (or kidney’s inability to respond to ADH). When it occurs, it is most often associated with neurological conditions, surgery, tumors, head injury, or inflammatory problems.
Data CollectionA. Excretionofexcessiveamountsurine(greaterthan 200mL/hr)(Polyuria).B. Polydipsia,weakness.C. Lowurinespecificgravity(1.001to1.005).D. Severedehydration(tachycardia,poorskintugor,dry mucousmembranes).E. Increaseinserumsodiumlevel(greaterthan147mEq/L).
Nursing Interventionv Goal: Tomaintainfluidandelectrolytebalances(seeChapter6).A. Encourageintakeoffluidscontainingelectrolytesfor clientswithDI.B. Monitorintakeandoutputcarefully.Weighdaily.C. Evaluateurinespecificgravityforchanges.D. Assesshydrationstatus.
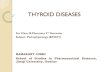
HyperthyroidismHyperthyroidism (also called Graves’ disease) or thy- ✽
rotoxicosis (the signs and symptoms caused by hyperme-tabolism) is characterized by excessive output of thyroid hormones. (Figure 8-1)
Data CollectionA. Intolerancetoheat.B. Significantweightloss,despiteincreasedappetiteand foodintake.C. Tachycardia,increaseinsystolicbloodpressure.D. Increasedperistalsis,leadingtodiarrhea.E. Handtremorsatrest.F. Visualproblems. 1. Exophthalmos(bulgingeyeballs). 2. Changesinvision,eyelidretraction(lidlag).G. Changesinmenstrualcycle-amenorrhea.H. Enlarged,palpablethyroidgland.I. Moodfluctuations.J. Diagnostics(seeAppendix8-1)-increaseinT
3, T
4,
andfreeT4serumlevels,decreaseinTSH,radioactive
iodineuptaketest(I123)greaterthan50%.
ComplicationsA. Thyroidstormorcrisis:mayoccuraftersurgeryor treatmentwithradioactiveiodine. 1. Systolichypertension,tachycardia. 2. Increasedtemperature(greaterthan102oF). 3. Increasedagitationandanxiety.
FIGURE 8-1 Graves’ Disease. (From Zerwekh J, Claborn J, Miller CJ: Memory notebook of nursing, vol 1, ed 3, Ingram, 2007, Nursing Education Consultants, Inc.)

160 CHAPTER 8 Endocrine System
B. Calciumdeficitmayoccurasaresultoftraumatothe parathyroid(seeHypoparathyroid).
TreatmentA. Surgical:thyroidectomy.B. Medical. 1. Reducethyroidtissue:irradiationofthyroidgland withradioactiveiodine(I131),eventuallyresultingin hypothyroidstate. 2. Medicationstodecreasethyroidsynthesisandre- lease(seeAppendix8-2).
Nursing Interventionv Goal: Todecreaseeffectsofexcessthyroidhormone.A. Decreaseenvironmentalstress(lights,visitors,noise, etc.).B. Cool environment.C. Sedatives,ifappropriate.D. Well-balancedmeals(highincaloriesandhighin vitamins);smallmealsserved4to6timesperday.v Goal: Toprotecteyesofclientexperiencingcomplica-tionscausedbyeyechanges.A. Eyedropsorointment.B. Assessforexcesstearing,asignofdrycornea.C. Eyepatchesormaskmaybenecessaryatnight.v Goal: Tomaintainhomeostasisinclientexperiencingthyroidstorm(orcrisis).A. Decreasebodytemperatureandheartrate. 1. Hypothermiablanket. 2. Acetaminophentodecreasefever. 3. Propranolol(Inderal)anddigitalistotreatcardiac issues.B. Oxygentomeetincreasedmetabolicdemands.C. IVfluids.D. Antithyroidmedicationsandiodinepreparationsto decreaseT
4output.
v Goal: Toprovidepreoperativenursingmeasuresifsurgeryisindicated.A. Demonstratetoclienthowtoprovidenecksupportafter surgery.B. Administeriodinepreparationstodecreasevascularity ofthethyroidgland.v Goal: Tomaintainhomeostasisafterthyroidectomy.A. Maintainsemi-Fowler’spositiontoavoidtensiononthe suture line.B. Administeranalgesicsforpain.C. AdministerIVfluidsuntilnauseaandswallowing difficultysubside.D. Checkdressingsonthesideandbackoftheneckfor bleedingandreportanybleeding.E. Applyicecollartodecreaseedema.F. Checkcalciumlevels;parathyroidmayhavebeendam- agedoraccidentallyremoved.G. Evaluatetemperatureelevations;temperatureincrease maybeearlyindicationofthyroidstorm.
TEST ALERT: Monitor status of client who has under-gone surgery (hemorrhage, airway, wound).
v Goal: Topreventcomplicationofrespiratorydistressafterthyroidectomy.A. Assessclientfrequentlyfornoisybreathingandin- creasedrestlessness.B. Evaluatevoicechanges;increasinghoarsenessmaybe indicativeoflaryngealedema.Reportanychangesim- mediately.C. Keeptracheotomysetreadilyavailable.v Goal: Todecreaseradiationexposureinclientbeingtreatedasanin-patientwithradioactiveiodine(I131).A. Allbodysecretionsarecontaminatedbecausethisisa systemictypeofradiation.B. Advisefamilymemberstoavoidoralcontactbecause salivaiscontaminated.C. Foranybodyfluidspills(urine,vomitus,etc.),contact theradiationsafetyofficerforthefacility.Donotclean upthespill.D. Generalguidelineistomaintain1meter(alittlemore than3feet)distancefromtheclientunlessdirect contactisnecessary.E. Infantsandpregnantwomenshouldavoidcontactwith clientforapproximately2days.F. Allhealthcarepersonnelprovidingdirectcaretoclient shouldweararadiationbadge.G. Monitorclientforatransientperiodofseveraldaysto weekswhenthesymptomsofhyperthyroidismmay actuallyworsenafterradioactiveiodinetherapy.
TEST ALERT: Observe client for side effects of chemotherapy or radiation.
Home CareA. Thyroidlevelscheckedannually.B. Lifelongthyroidreplacement.C. Ifexcessivefatigueortachycardiaandtremorsbecome aconsistentproblem,notifyhealthcareprovider.
Hypothyroidism Hypothyroidism is characterized by a slow deteriora- ✽
tion of thyroid function. It occurs primarily in older adults and five times more frequently in women (ages 30 – 60) than in men. Myxedema coma is a life-threatening form of hypothyroidism
Data CollectionA. Earlyclinicalmanifestations. 1. Extremefatigue,menstrualdisturbances. 2. Hairloss,brittlenails,anddryskin. 3. Intolerancetocold,anorexia. 4. Constipation,apathy.

CHAPTER 8 Endocrine System 161
morefrequently;thyroidpreparationsmayaltereffects ofhypoglycemicagents.C. Continue to reinforce teaching information as client beginstomakeprogress;earlyinthedisease,theclient maynotcomprehendimportanceofinformation.
Hyperparathyroidism
✽ Hyperparathyroidism is characterized by excessive secretion of parathyroid hormone (PTH), resulting in hy-percalcemia. Excessive PTH leads to decalcification of the bones, as the calcium moves from the bones into the serum, hypercalcemia results and possible kidney damage.
Data CollectionA. Bonecystsandpathologicalfractures.B. Renalcalculi,azotemia. 1. Hypertensioncausedbyrenalfailure. 2. Repeatedurinarytractandrenalinfections.C. Centralnervoussystemproblemsoflethargy,stupor, andpsychosis.D. GIproblems. 1. Anorexia,nauseaandvomiting. 2. Constipation,developmentofpepticulcer.E. Diagnostics-increasedlevelofserumtotalcalcium; decreasedlevelofserumphosphorous;increasedPTH.
TreatmentA. Decrease level of circulating calcium.B. Parathyroidectomy.
Nursing Interventionv Goal: Todecreasethelevelofserumcalcium.A. Highfluidintaketodiluteserumcalciumandurine calcium levels.B. Encouragemobility,becauseimmobilityincreases demineralizationofbones.C. Limitfoodshighincalcium.v Goal: Toassessclient’stoleranceofandresponsetoincreasedPTHlevel.A. Assessforskeletalinvolvement–presenceofbone pain.B. Assess for renal involvement. 1. Strain urine for stones. 2. Evaluateforlowbackpain(renal). 3. Checkforhematuria. 4. Assessintakeandoutputcarefully.C. Monitorforcardiacarrhythmiasduetoincreased calcium.v Goal: Toprovideappropriatepreoperativemeasuresifsurgeryisindicated(seeChapter3).v Goal: Topreventpostoperativecomplicationsofpara-thyroidectomy.A. Careofclientwhohasundergoneparathyroidectomyis sameasthatforclientwhohasundergonethyroid- ectomy.
B. Lateclinicalmanifestations. 1. Subnormaltemperature. 2. Cardiaccomplications(bradycardia,congestive heartfailure,hypotension). 3. Weightgainandedema,thickenedskin. 4. Changeordecreaseinlevelofconsciousness.C. Pediatricimplications:cretinism. 1. Identifiedafterbirthbymandatorystatescreening tests. 2. Hypotonia,hyporeflexia,poorfeeding. 3. Hypotonicabdominalmusculature–constipation, protrudingabdomen(umbilicalhernia).D. Diagnostics-decreaseinserumT
3andT
4 levels,
increaseinTSHlevel.
TreatmentA. Medicalmanagement. 1. Replacementofthyroidhormone. 2. Low-caloriediettopromoteweightloss. 3. Decreaseincholesterolintake. 4. Pediatric-Ifreplacementthyroidhormoneisac- complishedshortlyafterbirth,itispossiblethatthe childwillhavenormalphysicalgrowthandintel- lectualdevelopment.
ComplicationsA. Thyroidhormonereplacementwillincreasethework loadoftheheartandincreasemyocardialoxygen requirements.B. Observeclientfordevelopmentofcardiacfailure.
Nursing Interventionv Goal: Toassisttheclienttoreturntohormonebalance.A. Beginthyroidreplacementandevaluateclient’s response;adviseclientthatitwillbeabout7days beforeheorshebeginstofeelbetter.B. Provideawarmenvironment.
NURSING PRIORITY: ✔ Administer sedatives and hypnotics with caution because of increased susceptibility. These medications tend to precipitate respiratory de-pression in the client with hypothyroidism.
C. Preventand/ortreatconstipation.D. Assessprogress. 1. Decreaseinbodyweight. 2. Intakeandoutputbalance. 3. Decreaseinvisibleedema. 4. Energylevelandmentalalertnessshouldincrease in7to14daysandcontinuetoriseuntilnormal.E. Evaluatecardiovascularresponsetomedication.v Goal: Toassistclienttounderstandimplicationsofdiseaseandrequirementsforhealthmaintenance.A. Needforlifelongdrugtherapy.B. Diabeticclientneedstoevaluatebloodsugarlevels

162 CHAPTER 8 Endocrine System
HypoparathyroidismHypoparathyroidism is characterized by a decrease ✽
in the PTH level, resulting in hypocalcemia and elevated serum phosphate levels. Severe hypocalcemia results in tetany.
Data CollectionA. Mayoccurwithinadvertentremovalofparathyroid glandduringthyroidectomyorradicalneckdissection.B. Muscleweakness/spasms.C. Overt/acutetetany(potentiallyfatal). 1. Bronchospasm,laryngospasm. 2. Seizures,cardiacdysrhythmias.D. Diagnostics-decreasedserumcalciumandPTHlevels, increasedserumphosphatelevels.
TreatmentA. VitaminDtoenhancecalciumabsorption.B. Increasedcalciuminthediet.
TEST ALERT: Adjust food and fluid intake to improve fluid and electrolyte balances.
C. Acute. 1. ReplacecalciumthroughslowIVdrip(calcium gluconate,calciumchloride). 2. Sedatives,anticonvulsants.
Nursing Interventionv Goal: To assist client to increase serum calcium levels.A. Administercalciumpreparations.B. Evaluateincreasesinserumcalciumlevelsand decreasesinserumphosphatelevels.v Goal: Topreventcomplicationsofneuromuscularir-ritability.A. Quiet environment.B. Lowlights.C. Seizureprecautions(Appendix15-5).v Goal: Tohelpclientavoidcomplicationsofrespiratorydistress.A. Bronchodilators.B. Tracheotomysetreadilyavailable.C. Frequentassessmentofrespiratorystatus.Immediately reportanysignificantchanges.
Diabetes MellitusDiabetes mellitus is a complex, multisystem disease ✽
characterized by the absence of or a severe decrease in the secretion or utilization of insulin.A. Pathophysiology. 1. Theprimaryfunctionofinsulinistodecreasethe bloodglucoselevel.
2. Insulinissecretedbythebetacellsintheisletsof Langerhansinthepancreas. 3. Insulinallowsthebodytousecarbohydratesmore effectivelyforconversionofglucoseforenergy. 4. Ifcarbohydratesarenotavailabletobeusedfor energy,cellswillbegintobreakdownthefatsand proteinstores. a. Breakdownoffatresultsintheproductionof ketonebodies. b. Proteiniswastedduringinsulindeficiencyand isbrokendown. c. Whenfatsareusedastheprimaryenergy source,theserumlipidlevelrisesandcontri- butestotheaccelerateddevelopmentofathero- sclerosis. 5. Whencirculatingglucosecannotbeutilizedfor energy,thelevelofserumglucosewillincrease (hyperglycemia).B. Classification. 1. Type1:absolutedeficiencyofinsulinsecretion (Figure8-2). a. Onsetisfrequentlyinchildhood;mostoften diagnosedbeforetheageof18years.Most commonagerangeis10to15years. b. Previouslycalledjuvenilediabetesorinsulin- dependentdiabetesmellitus. c. ClientwillhaveType1diabetesfortherestof his or her life.
FIGURE 8-2 Diabetes, type 1. (From Zerwekh J, Claborn J, Miller CJ: Memory notebook of nursing, vol 1, ed 4, Ingram, 2008, Nursing Education Consultants.)

CHAPTER 8 Endocrine System 163
2. Type2:combinationofinsulinresistanceandinad- equateinsulinsecretiontocompensate(Figure8-3). a. Insulindeficiencycausedbydefectsininsulin productionorbyexcessivedemandsforinsulin; clientisnotdependentoninsulin. b. Onsetispredominatelyinadulthood,generally aftertheageof40years,butitmayoccuratany age. c. Previouslycalledadultonsetdiabetes(AODM) ornoninsulin-dependentdiabetesmellitus (NIDDM). d. Associatedwithobesity;overweightpeople requiremoreinsulin. e. Mayrequireinsulinforcontrol. 3. Gestationaldiabetes. a. Developsduringpregnancy;usuallydetectedat 24-28weeksgestationbyoralglucosetolerance test. b. Glucosetoleranceusuallyreturnstonormal soonafterdelivery. c. Commonlyoccursagaininfuturepregnancies; clientisatincreasedriskfordevelopmentofglu- coseintoleranceandType2diabeteslaterinlife. d. Infantmaybelargeforgestationalageandmay experiencehypoglycemiashortlyafterbirth.
Data CollectionA. Clinical manifestations. 1. Types1and2. a. ThreeP’s:polyphagia,polydipsia,polyuria. b. Fatigue. c. Increasedfrequencyofinfections. 2. Type1. a. Weightloss,excessivethirst. b. Bed-wetting,blurredvision c. Complaintsofabdominalpain. d. Onsetisrapid,generallyoverdaystoweeks. 3. Type2.(mostclientsasymptomaticfirst5to10 years).
a. Weightgain(obese),visualdisturbances. b. Onsetisslow;mayoccurovermonths. c. Onsetusuallyaftertheageof40years;peaks around45to50years. d. Fatigueandmalaise. e. Recurrentvaginalyeastormoniliainfections -frequentlyinitialsymptominwomen. f. Olderadultassessmentconsiderations(Box8-1).B. Diagnostics(thecriteriafordiagnosisaretwoormore abnormaltestresultswithtwoormorevaluesoutside thenormalrange)(seeAppendix8-1). 1. Fastingbloodglucoselevelisabove126mg/dl (normalglucoserange70-100mg/dl). 2. Glucosetolerancetest:2-hourglucosevaluesare greaterthan200mg/dl. 3. Randomglucosegreaterthan200mg/dlwithsymp- toms(threeP’s,weightloss). 4. Prediabetes–intermediatestagebetweennormal anddiabetes. a. Impairedglucosetolerance(IGT):greaterthan 140mg/dlandlessthanorequalto200mg/dl. b. Impairedfastingglucose(IFG):fastingblood glucosegreaterthan100mg/dl,butlessthan 126mg/dl. 5. Glycosylatedhemoglobin(HbA
1c)isincreased.
(Lessthan7%isconsideredgoodcontrolfor diabetic;isnotatesttodiagnosediabetes).
• Determinementalstatusandmanualdexteritytohandle injections.• Determineifclientcanaccesstheinjectionsites.• Isclientalertandmentallycapableofmakingjudgments onmedications?• Determineiftheclientcanpayforsupplies.• Whatistheclient’sattitudeaboutneedlesandinjections?• Assesshowmanyothermedicationstheclientistaking; problemswith“polypharmacy”(toomanymedications).• Determinefamily’sorclient’sabilitytoaccurately performserumglucosetesting.• Whatistheclient’ssupportsystem?
BOX 8-1 OLDER ADULT CARE FOCUS Diabetic Assessment Considerations and Care
FIGURE 8-3 Diabetes, type 2. (From Zerwekh J, Claborn J, Miller CJ: Memory notebook of nursing, vol 2, ed 3, Ingram, 2007, Nursing Education Consultants.)

164 CHAPTER 8 Endocrine System
TreatmentA. Hypoglycemicagents.High Alert Medications 1. Insulin:maybeusedinbothtypesofdia- betes.Primaryfunctionofinsulinistotrans- portglucoseintomuscleandfatcells(Figure8-4: ProfileofInsulins). a. Combinationpremixedinsulintherapyelimi- natesproblemofmixingdifferenttypes (example:NPH/regular70/30–numberrefersto percentageofeachtypeofinsulin). b. Responsetoinsulinmixturesvarieswithindi- viduals. 2. Oralhypoglycemicagentsfornoninsulin-dependent clients(seeAppendix8-2).B. Diabeticdiet. 1. Decrease calories for weight loss. 2. Diettomeetnutritionalneedsandmaintainopti- mumglucoselevel.Avoidsimplesugarsandin- creasedietaryfiber. 3. Decreaseincholesterollevel–reducesaturatedand transfatfoods. 4. Decreaseproteinforadultduetostressthatmoder- atetohighproteinplacesonthekidneys).C. Exercise-plannedexercise;sporadicexerciseisdis- couraged.
NURSING PRIORITY: ✔ Metabolic effects of exercise: 1. Reduces insulin needs by reducing the blood glucose. 2. Contributes to weight loss or maintenance of normal weight. 3. Assists the body to metabolize cholesterol more efficiently. 4. Promotes less extreme fluctuations in blood glucose level.5. Decreases blood pressure.
Complications of Insulin TherapyA. Hypoglycemia(Table8-1).B. Lipoatrophy(tissueatrophy)andlipohypertrophy(accu- mulationofextrafatatthesiteofmanysubcutaneous injectionsofinsulin).C. Somogyieffect. 1. Reboundhyperglycemiafromanunrecognizedhy poglycemicstate. 2. Mostoftenoccursatnightandtreatedbydecreasing theeveninginsulindoseorbyincreasingthecalo- riesinthebedtimesnack.D. Dawnphenomenon 1. Results from nighttime release of growth hormone andcortisol. 2. Bloodglucoseelevatesat5:00to6:00AM(predawn hours).
FIGURE 8-4 Insulin Profiles (Adapted from Lewis S, Heitkemper M, Dirksen S: Medical-surgical nursing: assessment and management of clinical problems, “Commercially available insulin preparations showing onset, peak, and duration of action,” St Louis, 2007, Mosby).
HIGH
ALERT
Nursing Implications (intermediate acting) 1. Hypoglycemia tends to occur in mid to late afternoon. 2. Never give IV. 3. May be mixed with regular insulin.
Nursing Implications (long acting) 1. Glargine has low pH (4); CANNOT be mixed with other insulins. 2. Usually given once a day at bedtime, but can be administered during the day.
Nursing Implications (rapid acting) 1. Should be used in combination with longer acting insulin.
NURSING PRIORITY: Because of quick onset of action, client must eat immediately.
Nursing Implications (short acting) 1. Usually given 20 - 30 minutes before meals. 2. May be given alone or in combination with longer-acting insulins. 3. Given for sliding scale coverage.
NURSING PRIORITY: When administering injections: 1. May mix regular insulin with other insulins. 2. Only regular insulin may be given IV.
FIGURE 8-4 Profile of Insulins
TEST ALERT: Intervene to control hypoglycemia/ hyperglycemia. Know various insulins and nursing implications. Specifically, know when to anticipate reaction and what to teach the client about his or her insulin.

CHAPTER 8 Endocrine System 165
3. Maybetreatedbyincreasinginsulinforovernight period.E. Insulinrequirementincreaseswhen: 1. Seriousillnesses,physicaltrauma,andinfections. 2. Surgicalproceduresandgrowthspurtsduring adolescence.
NURSING PRIORITY: ✔ Intensive control of blood glucose levels in clients with type 1 diabetes can prevent or ameliorate the complications. Intervene to control symptoms of hypoglycemia or hyperglycemia.
Complications Associated with Poorly Controlled DiabetesA. Diabeticketoacidosis. 1. Asevereincreaseinthehyperglycemicstate. 2. Occurspredominatelyintype1diabetes.B. Clinicalmanifestationsofdiabeticketoacidosis(see Table8-1). 1. Onset-maybeacuteoroccuroverseveraldays. a. Mayresultfromstress,infection,surgery,or lackofeffectiveinsulincontrol. b. Resultsfrompoorlycontrolleddiabetes. 2. Severehyperglycemia(bloodglucoselevelsof300- 800mg/dL). 3. Presenceofmetabolicacidosis(lowpH[6.8-7.3]and serumbicarbonatelevellessthan15mEq/L).
4. Hyperkalemia,hypokalemia,ornormalpotassium level,dependingonamountofwaterloss. 5. Urineketoneandsugarlevelsareincreased. 6. Excessiveweakness,increasedthirst. 7. Nausea,vomiting,dehydration. 8. Increasedtemperaturecausedbydehydration. 9. Fruity(acetone)breath,Kussmaulrespirations. 10.Decreasedlevelofconsciousness.C. Hyperosmolarhyperglycemiasyndrome(HHS).Also knownasNonketoticHyperosmolarComaand/or HyperosmolarHyperglycemicState(seeTable8-1). 1. Occursintheadult(olderadult)withType2 diabetes. 2. Characterizedbyextremehyperglycemia(400-1200 mg/dl)withoutacidosis.
Complications of Long-Term DiabetesA. Angiopathy:prematuredegenerativechangesinthe vascularsystem. 1. Mayaffectlargevesselsasinperipheralvascular disease:decreasedcirculationtolowerextremities. 2. Mayaffectsmallervesselsofthekidney,resulting innephropathyandrenalfailure. 3. Mayaffectsmallvesselsoftheretina,resultingin blurredvision,retinopathy,cataracts. 4. Accelerationofatheroscleroticprocess,resultingin hypertension.
TABLE 8-1 COMPARISON OF DIABETIC KETOACIDOSIS (DKA) AND HYPOGLYCEMIA DKA Hypoglycemia Age Allages,increasedincidenceinchildren. Allages
GI Abdominalpain,anorexia,nausea,vomiting,diarrhea Normal;maybehungry
Mentalstate Dull,confusionincreasingtocoma Difficultyinconcentrating,coordinating; eventuallycoma
Skintemperature Warm,dry,flushed Cold,clammyPulse Tachycardia,weak TachycardiaRespirations Initiallydeepandrapid;leadto Shallow Kussmaulrespirations Breathodor Fruity,acetone NormalUrineoutput Increased Normal
Lab Values: Serum Glucose Greaterthan300(upto1500mg/dL) Below70mg/dLKetones High/large NormalpH Acidotic(lessthan7.3) NormalHematocrit Highduetodehydration Normal
Lab Values: Urine Sugar High NegativeKetones High NegativeOnset Rapid(lessthan24hr) RapidClassificationofdiabetes PrimarilyType1;Type2inseveredistress Type1andtype2
DKA,Diabeticketoacidosis;GI, gastrointestinal

166 CHAPTER 8 Endocrine System
C. Thereisanincreasedtendencytowardthedevelopment ofmetabolicacidosis.D. Thereisatendencytointensifytheexistingcomplica- tionsofdiabetes.E. Oralhypoglycemicagentsarenotusedtocontroldiabe- tesinthepregnantclient–insulinisused.
Nursing Intervention (All Types)v Goal: To return serum glucose to normal level.A. Initiallyadministerregularinsulinonaproportional basisaccordingtoneed(Box8-2).B. Administerinsulin30minutesbeforeamealorsnack.C. Maintainadequatefluidintake.D. Evaluateserumelectrolytelevels,especiallypotassium.E. Evaluatehydrationstatus.F. Evaluate and report clinical manifestations of hypogly- cemia and hyperglycemia.
TEST ALERT: Monitor hydration status and electrolyte balance.
v Goal: Toplanandimplementateachingregimen.A. Assesscurrentlevelofknowledgeregardingdiabetes.B. Evaluateculturalandsocioeconomicparameters.C. Evaluateclient’ssupportsystem(family,significant others).D. Instructregardingsick-dayguidelines(Box8-3).
TEST ALERT: Determine ability of family/support systems to provide care for client. Identify client’s and family’s strengths.
E. Administrationofinsulin(seeBox8-2). 1. Correctinjectiontechniques. 2. Rotateinjectionsite(Figure8-5). 3. Checkexpirationdateontheinsulin. 4. Durationandpeakactionofprescribedinsulin. 5. Allowforamplepracticetime. 6. Administeratthesametimeeachday.
B. Nervedamageresultinginneuropathy. 1. Peripheralneuropathy:painandtinglinginlegsand feet;mayprogresstopainlessneuropathy. 2. Verycommoncomplication.C. Infections:Immunesystemisaltered;persistent glycosuriapotentiatesurinarytractinfections.
NURSING PRIORITY: ✔ Painless peripheral neurop-athy is a very dangerous situation for the diabetic. Severe injury to the lower extremities may occur, and the client will not be aware of it. Clients should be taught to visually inspect their feet and legs.
Clinical Implications of Diabetes in PregnancyA. Duringthesecondandthirdtrimester,thenormalre- sponseisfortheinsulinneedstoincreaseasmuch as70%to100%.B. Failureofinsulinneedstoincreasemaybeindicativeof placentalinsufficiency.
1. Donotadministercoldinsulin;itincreasespainand causesirritationatinjectionsite.
2. Anopen10-mLvialofunrefrigeratedinsulinshouldbe discardedafter30days,regardlessofhowmuchwas used.
3. Donotallowinsulintofreezeandkeepitawayfromheat andsunlight.
4. Insulinpens(NPHand70/30)shouldbediscardedafter 1weekofstorageatroomtemperature.Regularcartridges, whichdon’tcontainpreservatives,maybeleftunrefriger- atedforupto1month.
5. Extremetemperatures(lessthan36°Forgreaterthan 86°F)shouldbeavoided.
6. Rollthevialbetweenthepalmsofthehandstodecrease theriskofinconsistentconcentrationofinsulin.
7. Theabdomenistheprimarysiteforsubcutaneousinjec- tionsofinsulin.Rotateinjectionsites;injectionsites shouldbe1inchapart.
8. Abdomenareaprovidesmostrapidinsulinabsorption.9. Useonlyinsulinsyringestoadministerinsulin.10. Checkexpirationdateoninsulinbottle.11. Whendrawingupregularinsulinwithalong-acting insulin,drawuptheregular(clear)insulinbeforethe longer-acting(cloudy)insulin.
12. Regularinsulinisusedforadministrationbyslidingscale andperiodswhenbloodsugarisunstableanddifficultto control.
13. Usingalcoholtocleansetheskinbeforeinjectionisnot recommended.Ifused,holdalcoholpadinplacefora fewsecondsbutdonotmassage.
14. Aspiratingisnotrecommendedforself-injection.15. Checkdosewithanothernursepriortoadministering.
BOX 8-2 IMPLICATIONS IN THE ADMINISTRATION OF INSULIN
HIGH
ALERT
• Avoidcannedfruitsthatareinheavysyrup;selectfruit packedinwater.• Includefreshfruitsandvegetablesandwhole-grain cerealsandbreadstoprovideadequatedietaryfiberto preventconstipation.• Avoidcasseroles,friedfoods,saucesandgravies,and sweets.• Fats(oils,margarines)thatareliquidatroomtemperature arebetterthanthosethataresolid.• Readfoodlabels:thehighest-contentingredientislisted first.• Selectfoodsinwhichthemajorityofcaloriesdonotcome from a fat source.
BOX 8-3 OLDER ADULT CARE FOCUS Guidelines for Food Selection

CHAPTER 8 Endocrine System 167
7. Clientsfollowinganintensivediabetestherapypro- grammaychoosetouseaninsulinpumporto monitorbloodglucoselevelsfourtosixtimesaday andtakeinjectionsatthosetimes. a. Theinsulinpumpisbatteryoperated;insertion siteischangedevery2to3days;pumpisre- filledandreprogrammedwhensiteischanged. b. Deliverscontinuousinfusionofshort-acting insulinovera24-hourperiod,allowingfortight glucose control. c. Candeliverbolusofinsulinbasedonexcessive carbohydratesingested. d. Monitorinsertionsiteforrednessandswelling. 8. Insulinpenisacompactportabledevicethatis loadedwithinsulin;needtochangeneedlewith eachinjection.F. Oralhypoglycemicagents. 1. Takemedicationasscheduled;donotskiporadd dose. 2. Signsandsymptomsofhypoglycemia. 3. Anticipatechangeinmedicationwithpregnancy.G. Monitoringbloodglucose. 1. Self-monitoringofbloodglucose(SMBG)–not necessarytousealcoholtocleansesite. 2. Usesideoffingerpadratherthannearthecenter. Ifalternativesiteuse(i.e.,forearm),mayrequire differentequipment.
3. Needonlyalargedropofblood.H. Exercise. 1. Establishanexerciseprogram. 2. Avoidsporadicexercise. 3. Reviewinstructionsregardingadjustmentofinsulin andfoodintaketomeetrequirementsofincreased activity. 4. Extremitiesinvolvedinactivityshouldnotbeused forinsulininjection(e.g.,armswhenplaying tennis).I. Diet(Box8-4). 1. Regularlyscheduledmealtimes. 2. Understandingoffoodgroupsandbalanced nutrition. 3. Incorporatefamilytendenciesandculturalpatterns intoprescribeddietaryregimen. 4. Provideclientandfamilywithwritteninstructions regardingdietaryneeds.J. Infectioncontrol. 1. Reportinfectionspromptly. 2. Insulinrequirementsmayincreasewithseverein- fections. 3. Increasedproblemswithvaginitis,urinarytractin- fections,andskinirritation.K. Avoidinjury. 1. Decreasedhealingcapabilities,especiallyinlower extremities. 2. Maintainadequatebloodsupplytoextremities; avoidtight-fittingclothingaroundthelegs. 3. Properfootcare(seeChapter11).v Goal: Topreparethediabeticclientforsurgery.A. Oralhypoglycemicagentsshouldnotbegiventhe morningofsurgery.B. ForclientswithNPO(nothingbymouth)statuswho requireinsulin,anIVof5%dextroseinwater(D
5W)is
frequentlystarted.C. Obtainabloodglucosereadingaboutanhourbefore sendingtheclienttosurgerytomakesureheorsheis notdevelopinghypoglycemia.
NURSING PRIORITY: ✔ Evaluate intake; do not give client on NPO status insulin unless IV is in place.
v Goal: Tomaintaincontrolofdiabeticconditioninthepostoperativeclient.A. IVfluidsandregularinsulinuntilclientisabletotake fluidsorally.B. Frequentbloodsugarlevelassessment.C. Observeforhypoglycemiaimmediatelyaftersurgery.v Goal: Toidentifydiabeticketoacidosisandassistcli-ent to return to homeostasis.A. Frequentmonitoringofvitalsignsandserumglucose checks(normallyhourly).B. Hourlyurinemeasurements:Donotadministerpotas- siumifurineoutputislowordropping.
FIGURE 8-5 Sites Used for Insulin Injection. The injection site can affect the onset, peak, and duration of action of the insulin. Insulin injected into the abdomen (area I) is absorbed fastest, followed by insulin injected into the arm (area II) and the leg (area III). (From Black J, Hawks, J: Medical surgical nursing: clinical management for positive outcomes, ed 8, St Louis, 2009, Mosby.)

168 CHAPTER 8 Endocrine System
Home CareA. Maintainoptimumweight.B. Continuetoreceivelong-termmedicalcare.C. Notifyallhealthcareprovidersofdiagnosisofdiabetes; wearmedicalalertidentification.D. Recognizeproblemsofthecardiovascularsystem. 1. Peripheralvasculardisease. 2. Decreasedhealing. 3. Increasedriskofstroke. 4. Increasedriskofmyocardialinfarction.
5. Presenceofretinopathy. 6. Increasedriskofrenaldisease.E. Recognizeproblemsofperipheralneuropathy.
OLDER ADULT PRIORITY: ✔ Assess client’s ability to take medications correctly and/or client’s manual dexterity to handle insulin syringe and visual acuity to measure correct dose.
v Goal: Toassistthediabeticclienttomaintainhomeo-stasisthroughoutpregnancy.A. Prevent infection.B. Frequentevaluationofglucoselevelsandmonitoringof changesininsulinrequirements.C. Maintainoptimumlevelofweightgain;labormaybe inducedorcesareandeliverymayberequiredifcompli- cationsareevident.
Hypoglycemia (Insulin Reaction)Hypoglycemia is a condition characterized by a ✽
decreased serum glucose level, which results in decreased cerebral function.
Data CollectionA. Labilityofmood.B. Emotional changes, confusion.C. Headache,lightheadedness,seizures,coma.D. Impairedvision,tachycardia,hypotension.E. Nervousness,tremors,diaphoresis.F. Serumglucosebelow50mg/dL.G. Negativeurineacetonetestresult.
TreatmentA. Carbohydratesbymouthifclientisalertandcanswal- low. 1. Milkpreferredinchildrenwithamildreaction;it providesimmediatelactose,aswellasproteinand fatforprolongedaction. 2. Simplesugarsforimmediateresponse:orangejuice, honey,candy,glucosetablets.B. Glucagoncanbegivenintravenouslyifclientisuncon- scious.
Nursing Interventionv Goal: To increase serum glucose level.A. Administerglucose/carbohydratepreparationsasindi- cated.
NURSING PRIORITY: ✔ When in doubt of diagnosis of hypoglycemia versus hyperglycemia, administer car-bohydrates; severe hypoglycemia can rapidly result in permanent brain damage.
If you do not feel well (not eating regularly, fever, lethargy, nausea and vomiting, etc.):1. Checkyourbloodglucoseevery3to4hoursandurine ketoneswhenvoiding.2. Increaseyourintakeoffluidsthatarehighincarbohy- drates;everyhour,drinkfluidsthatreplaceelectro- lytes:fruitdrinks,sportsdrinks,regularsoftdrinks (notdietbeverages).3. Ifyoucannoteatandyouhavereplacedfourtofive mealswithliquids,notifyyourhealthcareprovider.4. Getplentyofrest;ifpossible,havesomeonestaywith you.5. Donotomitorskipyourinsulininjectionsororal medicationsunlessspecificallydirectedtodosobyyour healthcareprovider.6. Followyourhealthcareprovider’sinstructionsregarding bloodglucoselevelsandinsulinororalhypoglycemic agents.7. Staywarm,stayinbed,anddonotoverexertyourself.8. Callyourhealthcareproviderwhen: a. Youhavebeenillfor1to2dayswithoutgettingany better. b. Youhavebeenvomitingorhaddiarrheaformorethan 6 hours. c. Yoururineself-testingshowsmoderatetolarge amountsofketones. d. Youaretakinginsulinandyourbloodglucoselevel continuestobegreaterthan240mg/dlafteryouhave takentwotothreesupplementaldosesofregular insulin(pre-arrangedwithyourprovider). e. Youaretakinginsulinandyourbloodglucoselevelis lessthan60mg/dl. f. YouhaveType2diabetes,youaretakingoraldiabetic medications,andyourpremealbloodglucoselevels are240mg/dlorgreaterformorethan24hours. g. Youhavesignsofseverehyperglycemia(verydry mouthorfruityodortobreath),dehydration,or confusion. h. Youaresleepierormoretiredthannormal. i. Youhavestomachorchestpainoranydifficulty breathing. j. Youhaveanyquestionsorconcernsaboutwhatyou needtodowhileill.
BOX 8-4 DIABETIC “SICK DAY” GUIDELINES

CHAPTER 8 Endocrine System 169
B. Thoroughassessmentofthediabeticclientforthe developmentofhypoglycemia.v Goal: Toassistclienttoidentifyprecipitatingcausesandactivitiestopreventthedevelopmentofhypoglycemia.A. Instructthediabeticclienttocarrysimplecarbohy- drates.B. Administerbetween-mealsnacksatthepeakactionof insulin.C. Between-mealsnacksshouldlimitsimplecarbohydrates andincreasecomplexcarbohydratesandprotein.D. Clientshouldcarrysometypeofmedicalalertindenti- fication.
Pancreatitis ✽ Pancreatitis is an inflammatory condition of the
pancreas that results in autodigestion of the pancreas by its own enzymes.
Data CollectionA. Severeconstantmidepigastricpain. 1. Radiatestothebackorflankarea. 2. Exacerbatedbyeating.B. Acute. 1. Persistentvomiting,low-gradefever. 2. Hypotensionandtachycardia. 3. Jaundice,ifcommonbileductisobstructed. 4. Abdominaldistention.C. Chronic. 1. Decreaseinweight,mildjaundice. 2. Steatorrhea(fattystools),hyperglycemia. 3. Abdominaldistentionandtenderness.D. Increaseinserumamylaseandlipaselevels.
TreatmentA. Opioidanalgesics.B. Antibiotics,smoothmusclerelaxants.C. Decreasepancreaticstimulus. 1. NPOstatus;IVfluids. 2. Nasogastricsuction,bedrest. 3. Diet:(ifnotNPO)low-fat,high-carbohydrate.D. Surgicalinterventiontoeliminateprecipitatingcause (biliarytractobstruction).
Nursing InterventionNursing intervention is the same for the client with acute pancreatitisandfortheclientwithchronicpancreatitisexpe-riencinganacuteepisode.v Goal: Torelievepainanddecreasepancreaticstimula-tion.A. Administeranalgesics;paincontrolisessential(rest- lessnessmaycausepancreaticstimulationandfurther secretionofenzymes).B. Placeclientonsideinknee-chestorinsemi-Fowler’s position.C. Evaluateprecipitatingcause.
D. MaintainNPOstatusinitially.E. Maintainnasogastricsuctioning.F. Smallfrequentfeedingswhenfoodisallowed.v Goal: Topreventcomplications.A. Monitorfluidandelectrolyteimbalancesespecially hypocalcemiaandhydration.B. Maintainrespiratorystatus;problemsoccurbecauseof painandascites.C. Assessforhyperglycemiaanddevelopmentofdiabetes.
Home CareA. Avoidallalcoholintake.B. Knowsignsofdevelopmentofdiabetesandwhento returnforevaluationofbloodsugarlevel.C. Blanddiet,lowinfat,highincarbohydrates(protein recommendationsvary).D. Replacementofpancreaticenzymes.
Cancer of the PancreasThe majority of tumors occur in the head of the ✽
pancreas. As tumors grow, the bile ducts are obstructed, causing jaundice. Tumors in the body of the pancreas frequently do not cause symptoms until growth is advanced. Cancer of the pancreas has a poor prognosis; the 5 year survival rate is low.
Data CollectionA. Dull,achingabdominalpain.B. Ascites, nausea, vomiting.C. Anorexiaandprogressiveweightloss.D. Jaundice,clay-coloredstools,E. Dark,frothyurine.
TreatmentA. Surgery:Whipple’sprocedure(radicalpancreaticduo- denectomy).B. Radiationtherapy.C. Chemotherapy.
Nursing Interventionv Goal: Tomaintainhomeostasis(seenursinginterven-tionforpancreatitis).v Goal: Toprovidepreoperativenursingmeasuresifsurgeryisindicated.A. Maintainnasogastricsuctioning;assessforadequate hydration.B. Controlhyperglycemia.C. Assesscardiacandrespiratorystability.D. Assessfordevelopmentofthrombophlebitis.v Goal: Topromotecomfort,preventcomplications,andmaintainhomeostasisinclientwhohasundergoneWhipple’sprocedure.A. Generalpostoperativecare(seeChapter3).

170 CHAPTER 8 Endocrine System
B. Evaluateforbleedingtendenciescausedbydecreased prothrombinactivity.C. Monitorforfluctuationinserumglucoselevels.D. MaintainNPOstatusandnasogastricsuctionuntilperi- stalsis returns.E. Encourageadequatenutritionwhenappropriate. 1. Decreasefatsandincreasecarbohydrates. 2. Small,frequentfeedings.
Home CareA. Evaluateforboutsofanxietyanddepressioncausedby severityofillnessandprognosis(seeChapter6).B. Assist client in setting realistic goals.C. Encourage ventilation of feelings.
PheochromocytomaPheochromocytoma is a rare disorder of the adrenal ✽
medulla characterized by a tumor that secretes an excess of epinephrine and norepinephrine.
Data Collection
NURSING PRIORITY: ✔ Clients experiencing prob-lemsof theadrenalmedullahaveseverefluctuations inblood pressure related to the levels of catecholamines.
A. Persistentorparoxysmalhypertension.B. Palpitations,tachycardia.C. Hyperglycemia,headache.
TreatmentA. Medications-antihypertensivemedications.B. Surgery:removalofthetumoristhetreatmentof choice.
Nursing Interventionv Goal: Todecreaseclient’shypertensionandprovidepreoperativenursingmeasuresasappropriate(seeChapter3).A. Decreaseintakeofstimulants.B. Assessvitalsignsfrequently.v Goal: To assist client to return to homeostasis after adrenalectomy.A. Maintainnormalbloodpressurethefirst24to48hours aftersurgery;clientisatincreasedriskforhemorrhage orseverehypotensiveepisode. 1. Assessforbloodpressurechangescausedbycat echolamineimbalance(bothhypertensionand hypotension). 2. Administeranalgesicsjudiciously. 3. Administercorticosteroidsasindicated.v Goal: Tomaintainhealthafteradrenalectomy.A. Continuedmedicalfollow-upcare.B. Ifbothadrenalsareremoved,clientwillrequirelifelong replacementofadrenalhormones.
Addison’s Disease (Adrenocortical Insufficiency/Adrenal Hypofunction)
Addison’s disease is caused by a decrease in secretion ✽of the adrenal cortex hormones.
Data CollectionA. Fatigue,weakness.B. Weightloss,bronzepigmentationoftheskin.C Posturalhypotension.D. Hyponatremia,hyperkalemia.E. Hypoglycemia.F. Adrenalcrisis(Addisoniancrisis)–maybecausedby clientfailingtotakemedications. 1. Profoundfatigue,dehydration. 2. Vascularcollapse(seecyanosisandsignsofshock: pallor,anxiety,weak/rapidpulse,tachypnea,and lowbloodpressure).
TEST ALERT: Determine if vital signs are abnormal (e.g., hypotension, hypertension); notify others of change in client’s condition.
TreatmentA. Replaceadrenalhormones.B. Mayrequirelifelongreplacementofadrenalhormones.
Nursing Interventionv Goal: To return to homeostasis.A. InitiateandmaintainIVinfusionofnormalsaline solution.B. AdministerlargedosesofcorticosteroidsthroughIV bolusinitially,thentitrateinadilutedsolution.C. Frequentevaluationofvitalsigns.D. Assesssodiumandwaterretention.E. Evaluateserumpotassiumlevels.F. Keepclientimmobilizedandquiet.
NURSING PRIORITY: ✔ If any client is experiencing difficultywithmaintainingadequatebloodpressure,donot move him or her unless absolutely necessary. Avoid all unnecessary nursing procedures until the client’s condition is stabilized.
v Goal: Tosafelytakesteroidreplacements(seeAppen-dix5-7).A. Administersteroidpreparationswithfoodoranantacid.B. Evaluateforedemaandfluidretention.C. Assessserumsodiumandpotassiumlevels.D. Checkdailyweight.E. Increaseintakeofproteinandcarbohydrates.F. Evaluateforhypoglycemia.G. Observeforcushingoidsymptoms.

CHAPTER 8 Endocrine System 171
Home CareA. Lifelongsteroidtherapyisnecessary.B. Dosageofsteroidsmayneedtobeincreasedintimesof additionalstress.C. Infection,diaphoresis,andinjurywillnecessitatean increaseintheneedforsteroidsandmayprecipitate a crisis state.D. Reportgastricdistressbecauseitmaybecausedby steroids.E. Carryamedicalidentificationcard.
Cushing’s Syndrome (Adrenal cortex hypersecretion/Hypercortisolism)
Cushing’s syndrome occurs as a result of excess levels ✽of adrenal cortex hormones.
NURSING PRIORITY: ✔ The most common cause of Cushing’s syndrome is long-term steroid therapy for chronic conditions. Many chronic conditions necessitate the use of long-term steroid therapy. The symptoms of the syndrome are the same regardless of the origin of the problem.
Data CollectionA. Markedchangeinpersonality(emotionallability), irritability.B. Changesinappearance. 1. Moonface. 2. Depositoffatontheback. 3. Thinskin,purplestriae. 4. Truncalobesitywiththinextremities. 5. Bruisesandpetechiae.C. Persistenthyperglycemia.D. GIdistressfromincreasedacidproduction.E. Osteoporosis.F. Increasedsusceptibilitytoinfection.G. Sodiumandfluidretention;potassiumdepletion.H. Hypertension.I. Changesinsecondarysexualcharacteristics. 1. Amenorrhea(females). 2. Hirsutism(females). 3. Gynecomastia(males). 4. Impotenceordecreasedlibido.
TreatmentTreatmentdependsonthecauseoftheproblem.Cushing’ssyndromismostoftencausedbytheintakeofsteroidmedi-cationsrequiredtotreatachroniccondition(e.g.,arthritis,pulmonaryinflammation,transplants),andcontrolofthecon-ditionrequirestheclienttostayonthemedications.Atthatpoint,treatmentoftheconditionissupportive.
Nursing Interventionv Goal: Toassistinreturntohormonebalance.A. Restrictsodiumandwaterintake.B. Monitorfluidandelectrolytelevels.C. Evaluateforhyperglycemia.D. AssessforGIdisturbances.E. Prevent infection.v Goal: Topreventcomplications.A. Excessivesodiumandwaterretention:monitorfor edema,hypertension,heartfailure.B. Potassiumdepletion:monitorforcardiacarrhythmias.C. Evaluateclient’sabilitytocopewithchangeinbody image.D. Predisposedtofractures;promoteweightbearing; monitorforjointandbonepain;promotehomesafety.
Home CareA. Stresstheneedforcontinuoushealthcare.B. Encourage continuation of activities.C. Haveclientdemonstrateanunderstandingofthemedi- cation regimen.D. Assistclienttoidentifymethodsofcopingwithprob- lemsoftherapy.E. Haveclientdemonstrateanunderstandingofspecific problemsforwhichheorsheneedstonotifythe physician.

172 CHAPTER 8 Endocrine System
1. Thenurseisevaluatingaclientwithdiabeticketoacido- sis.Thenursewouldnotewhichrespiratorypatternas indicativeofcomplicationsassociatedwiththis condition? 1 Rapidanddeeprespirations. 2 Rapidandshallowrespirations. 3 Normalwithsleepapnea. 4 Cheyne-Stokesrespirations.2. Aclientintheemergencydepartmenthasabloodglu- coseof40mg/mL.Thenursewouldanticipatewhich medicationtobeordered? 1 NPHinsulin. 2 Metformin(Glucophage). 3 Regular insulin. 4 Glucagon.3. Aclientisplacedoninsulinslidingscale.Thenurse wouldanticipatewhichmedicationneedingtobe administered? 1 Lenteinsulin. 2 Regular insulin. 3 NPHinsulin. 4 Glargineinsulin.4. Whilegatheringinformationonadiabeticclient,the nursesmellsasweet,fruityodor.Whatwouldbe importantforthenursetocheck? 1 Serumbloodglucoselevel. 2 Bloodureanitrogenlevel. 3 Ketostixoftheurine. 4 Urinaryoutput.5. Aclienthasanorderforaglycosylatedhemoglobintest tobedone.Thenurseunderstandsthatthepurposeof this test is to: 1 Determinetheglucoselevelsoverthepast120days. 2 Evaluatethebloodglucoselevelaftera24-hour fasting. 3 Determinethelevelofinsulinpresentinthebody. 4 Evaluatethefunctionofthepancreas.6. Whatwouldbenotedontheassessmentofaclientwith hyperthyroidism? 1 Dryskin,bradycardia,andhypertension. 2 Difficultystayingawake,increasedappetite,and weight gain. 3 Markedweightgain,hypertension,andtachycardia. 4 Increasedactivity,difficultysleeping,andweight loss.7. Thenurseiscaringforaclientwhois8-hourspost- thyroidectomy.Whatareimportantnursinginterven tionsforthisclient?Selectallthatapply:____ 1 Havetheclientspeakevery2hourstodetermine ____ increasing level of hoarseness.____ 2 Provideahigh-calciumdiettoreplacecalciumlost ____ duringtheprocedure.____ 3 Evaluatebehindtheneckforthepresenceofblood ____ from the incision.
____ 4 Assistclienttoperformrange-of-motionneckexer ____ cisestopreventcontractures.____ 5 Maintaintheclientinsemi-Fowler’sposition.____ 6 Checktheincisionforformationofahematoma.8. AclientisadmittedwithadiagnosisofCushing’ssyn- drome.Whatisanimportantconsiderationforthenurse tomakeincaringforthisclient? 1 Theclientisgoingtobeintolerantofheat,andpulse rateandbloodpressurewillbeincreased. 2 Duetodecreasedinflammatoryresponse,theclient willbeatincreasedriskforinfection. 3 Itisimportanttomaintainstrictintakeandoutput duetohypovolemia. 4 Duetoactivityintolerance,theclientwillbekept onbedrestandahigh-sodiumdietwillbe prescribed.9. ThenurseiscaringforaclientwhohasAddison’sdis- ease.Howwillthenurseevaluatetheclientforcompli- cationsassociatedwiththiscondition? 1 Evaluatetheclientforthepresenceoffluctuating bloodpressurereadings. 2 Assessforthedevelopmentoffeverandpurulent drainage. 3 Performfrequentrespiratorychecksfordecreased movement of air. 4 Maintainstrictintakeandoutputrecordstodeter- minecompromisedrenalfunction.10. Adiabeticclientcomesintotheemergencydepartment withadiagnosisofdiabeticketoacidosis.Thenurse wouldanticipatewhatsymptomswiththisclient? 1 Shallowrespirations,bradycardia,confusion. 2 Pallor,diaphoresis,tachycardia. 3 Lowbloodpressure,diaphoresis,nauseaand vomiting. 4 Rapidanddeeprespirations,tachycardia,confusion.11. Whichclientwouldbemostlikelytobeabletocontrol theirdiabetesthroughdietandexercise? 1 A10-year-oldchild. 2 A30-year-oldwomanwithonsetatage11years. 3 A1-year-oldchild. 4 A60-year-oldwomanwithonsetatage45years.12. Whenaclientreturnstohisroomfollowingathyroid- ectomy,whatequipmentisimportantforthenurseto havereadilyavailable? 1 Oralairway. 2 Tracheotomytrayandsuction. 3 Paperandpencil. 4 Asmallcassettetaperecorder.
Answersandrationalestothesequestionsareinthesectionatthe end of the book titled Chapter Study Questions: Answers and Rationales.
Study Questions: Endocrine System

CHAPTER 8 Endocrine System 173
Appendix 8-1 ENDOCRINE DIAGNOSTICS Diagnostic Test Normal Clinical/Nursing Implications THYROIDThyroxine(T
4) 5-12mcg/dl 1. Increasedinhyperthyroidism,decreasedinhypothyroidism
Triiodothyronine(T3) 70-220ng/dl 2. WhenT
3 & T
4arelow,TSHsecretionincreases.
Thyroid-stimulatinghormone(TSH) 0.2-5.4mIU/L 3. TSHisincreasedinhypothyroidismanddecreasedinhyperthyroidism.
PANCREASSerumglucose 60-110mg/dl 1. Testistimedtoruleoutdiabetesbydeterminingrateofglucoseabsorption from serum.Oralglucosetolerancetest 1hr:lessthan200mg/dl 2. Inhealthyperson,insulinresponsetolargedoseofglucoseis immediate. 2hr:lessthan140mg/dl 3. Insulinandoralhypoglycemicagentsshouldnotbeadministered beforetest.Glucosefastingbloodsugar(FBS) Sameasserum 1. Usedasascreeningtestforproblemsofmetabolism.Alsocalled:fastingbloodglucose glucose(consistentlygreater 2. Maintainclientinfastingstatefor12hoursuntilbloodisdrawn.(FBG)andfastingplasmaglucose than126mg/dlisdiagnostic 3. Ifclientisaknowndiabeticandexperiencesdizziness,weakness,or(FPG) fordiabetes) fainting,drawbloodfordeterminationofglucoselevel.Glycosylatedhemoglobin(HbA
1c) Nondiabeticusually 1. Moreaccuratetestofdiabeticcontrol,becauseitmeasuresglucose
4%-6%.2%-6.4% attachedtohemoglobin(indicatesoverallcontrolforpast90-120days, consideredgooddiabetic whichisthelifespanoftheRBC). control(goalis7%orless) greaterthan8%consideredpoor diabeticcontrol
2-Hourpostprandialbloodsugar 65-139mg/dl 1. Involvesmeasuringtheserumglucose2hoursafterameal;resultsare significantlyincreasedindiabetic.Serumamylase 30-200U/L 1. Usedtoevaluatepancreaticcelldamage. 2. Otherintestinalconditionsandinflammatoryconditionscauseincrease.Serumlipase Normalvaluesvary 1. Appearsinserumafterdamagetopancreas. withmethod;elevated isabnormalUrinesugar(Clinistix, Clinitest, Negativeforglucose 1. Usefreshdouble-voidedspecimen.Labstix) 2. Aroughindicatorofserumglucoselevels. 3. Resultsmaybealteredbyvariousmedications.Ketonebodies(acetone) Negative 1. Ketonebodiesoccurintheurinebeforethereissignificantincreasein serumketones. 2. Usefreshlyvoidedurine.
PITUITARYGrowthhormone(GH) Lessthan5ng/mLinmen 1. NPOaftermidnight. Lessthan18ng/mLinwomen 2. Maintainbedrestuntilserumsampleisdrawn.
ADRENAL MEDULLAUrinaryvanillylmandelicacid(VMA) Lessthan8mgin24hr 1. Dependingonhowtestismeasured,theremaybedietaryandmedication Increasedwith restrictions. pheochromocytoma 2. 24-hrurinecollection.ACTHstimulationtest Increaseinplasma 1. ACTHisgivenasIMorIVbolusandsamplesaredrawnat30and60minto cortisollevelsby evaluateabilityofadrenalglandstosecretesteroids. morethan7-10mcg/dl abovebaseline
ADRENAL CORTEXACTHsuppression Normalsuppression; 1. Anovernighttest:Asmallamountofdexamethasoneisadmin- (dexamethasonesuppressiontest) 50%decreaseincortisone isteredintheevening,andserumandurineareevaluatedinthe production(cortisollevel morning;extensivetestmaycover6days. lessthan3mcg/dl) 2. Cushing’ssyndromeisruledoutifsuppressionisnormal.Plasmacortisollevelsfordiurnal Secretionhighinearly 1. Elevationinplasmacortisollevelsoccursinthemorningandvariations morning,decreasedin significantdecreaseineveningandnight—adiurnalvariation. evening. 8:00AM:5-23mcg/dl 4:00PM:3-13mcg/dl24-Hoururinefor17-hydroxycorti- Male:3-10mg/24hr 1. Increaseinurinelevelsindicateshyperadrenalfunction.costeroidsand17-ketosteroids Female:2-8mg/24hr 2. Keepspecimenrefrigerated Childunder15yr: lessthan4.5mg/24hr
ACTH,Adrenocorticotropichormone;ADH,antidiuretichormone; NPO,nothingbymouth;RBC,redbloodcell.
TEST ALERT: Frequently, the level of the FBS is given in a question, and it is necessary to evaluate the level and determine the appropriate nursing intervention.

174 CHAPTER 8 Endocrine System
HIGH
ALERT
Appendix 8-2 MEDICATIONS USED IN ENDOCRINE DISORDERS
Medications Side Effects Nursing Implications ADH REPLACEMENTDesmopressin(DDAVP): Excessivewaterretention, 1. Monitordailyweight;correlatewithintakeandoutput.nasalspray,PO,IV,SQ headache,nausea,flushing. Vasopressin(Pitressin):IM,SQ 2. VasopressinmorelikelytocauseadversecardiovascularandLypressin(Diapid):nasalspray thromboembolicproblems.
ANTITHYROID AGENT: Inhibits production of thyroid hormone; does not inactivate thyroid hormone in circulating blood. Medi-cations are not reliable for long-term inhibition of thyroid hormone production.
Propylthiouracil(PTU):PO Agranulocytosis;abdominal 1. Mayincreaseanticoagulationeffectofheparinandoralanti- discomfort;nausea,vomiting, coagulants. diarrhea;crossesplacenta. 2. Maybecombinedwithiodinepreparations.Methimazole(Tapazole):PO Same;crossesplacentamore 3. MonitorCBC. rapidly. 4. StoreTapazoleinlight-sensitivecontainer. 5. Maybeusedbeforesurgeryortreatmentwithradioactive iodine.Lugol’ssolution:PO Inhibitssynthesisandrelease 1. Administerinfluidtodecreaseunpleasanttaste.Saturatedsolutionofpotassium ofthyroidhormone.iodide(SSKI) 2. Maybeusedtodecreasevascularityofthyroidglandbefore surgery.
RADIOACTIVE IODINE: Accumulates in the thyroid gland; causes partial or total destruction of thyroid gland through radiation.
Iodine(I123 or I131):PO Discomfortinthyroidarea; 1. Increasefluidsimmediatelyaftertreatment,becauseradioac- bonemarrowdepression. tiveisotopeisexcretedintheurine. Desiredeffect:permanent 2. Therapeuticdoseofradioactiveiodineislow;noradiation hypothyroidism. safetyprecautionsarerequired. 3. Contraindicatedinpregnancy.
THYROID REPLACEMENTS: Replacement of thyroid hormone.
Levothyroxinesodium(Levothroid, Overdosemayresultin 1. Becarefulinreadingexactnameonlabelofmedications;Levoxyl, Levo-T, Novothyrox, symptomsofhyperthyroidism: microgramsandmilligramsareusedasunitsofmeasure.Synthroid):PO,IM,IV tachycardia,heatintolerance, 2. Generallytakenonceadaybeforebreakfast. nervousness. 3. Within3-4days,begintoseeimprovement;maximumeffectinLiothyronine(Cytomel, Triostat) 4-6weeks.
PANCREATIC ENZYMES: Replacement enzyme to aid in digestion of starch, protein, and fat.
Pancreatin(Creon):PO GIupsetandirritationof 1. Clientisusuallyonahigh-protein,high-carbohydrate,low-fat mucousmembranes. diet.Pancrelipase(Pancrease, 2. Enteric-coatedtabletsshouldnotbecrushedorchewed.Pangestyme, Ultrase, Viokase): 3. Pancreatinmaybegivenbefore,during,orwithin1hrafterPOmeals. 4. Pancrelipaseisgivenjustbeforeorwitheachmealorsnack.
ANTIHYPOGLYCEMIC AGENT: Increases plasma glucose levels and relaxes smooth muscles.
Glucagon:IM,IV,SQ Possiblerebound 1. Watchforsymptomsofhypoglycemiaandtreatwithfoodfirst, hypoglycemia. ifconscious. 2. Clientusuallyawakensin5-20minafterreceivingGlucagon. 3. Ifclientdoesnotrespond,anticipateIVglucosetobegiven.
ORAL HYPOGLYCEMIC AGENTS: Stimulate beta cells to secrete more insulin; enhance body utilization of available insulin (see Figure 8-4 for insulin). HIGH ALERT MEDICATIONS
GENERAL NURSING IMPLICATIONS• Doseshouldbedecreasedforelderly.• Usewithcautioninclientswithrenalandhepaticimpairment.• Alloralhypoglycemicagentsarecontraindicatedinpregnantclients.• Allclientsshouldbecarefullyobservedforsymptomsofhypoglycemiaandhyperglycemia.• Medicationsshouldbetakeninthemorning.• Long-termtherapymayresultindecreasedeffectiveness.

CHAPTER 8 Endocrine System 175
Appendix 8-2 MEDICATIONS USED IN ENDOCRINE DISORDERS—cont’d
Medications Side Effects Nursing Implications SULFONYLUREAS: Stimulate the pancreas to make more insulin.
Chlorpropamide(Diabinase): Hypoglycemia,jaundice,GI 1. Tolbutamidehasshortestdurationofaction;requiresmultiplePO disturbance,skinreactions dailydoses. (fewersideeffectswith 2. Glyburidehasalongdurationofaction. 2nd-generationagents). 3. Interactwith:calciumchannelblockers,oralcontraceptives,Glipizide(Glucotrol):PO glucocorticoids,phenothiazines,andthiazidediuretics.Glyburide(Micronase, DiaBeta):PO Glimepiride(Amaryl):PO Gliclazide(Diamicron):POTolbutamide(Orinase):POTolazamide(Tolinase):PO
BIGUANIDE: Decrease sugar production in the liver and help the muscles use insulin to break down sugar.
Metformin(Glucophage):PO Dizziness,nausea, 1. Administeredwithmeals. backpain,possible 2. Hasabeneficialeffectonloweringlipids. metallictaste. 3. Weightgainmayoccur.
ALPHA-GLUCOSIDASE INHIBITOR: Slows down how the body absorbs sugar after eating; also known as “starch blockers.”
Acarbose(Precose):PO Diarrhea,flatulence, 1. Takeatbeginningofmeals;noteffectiveonanemptystomach.Miglitol(Glyset):PO abdominalpain. 2. Acarboseiscontraindicatedinclientswithinflammatorybowel disease. 3. Frequentlygivenwithsulfonylureastoincreaseeffectivenessof bothmedications.
THIAZOLIDINEDIONES: Enhance insulin utilization at receptor sites (they do NOT increase insulin production); also referred to as “insulin sensitizers.”
Pioglitazone(Actos):PO Weightgain,edema. 1. Mayaffectliverfunction;monitorLFTs.Rosiglitazone(Avandia):PO 2. Postmenopausalwomenmayresumeovulation;pregnancymay occur.
MEGLITINIDES: (Non-Sulfonylurea Insulin Secretagogues) Stimulate release of insulin from beta cells.
Nateglinide(Starlix):PO Weightgain,hypoglycemia. 1. Rapidonsetandshortduration.Repaglinide(Prandin):PO 2. Take30minbeforemeals(orrightatmealtime). 3. Donottakeifmealismissed.
DIPEPTIDYL PEPTIDASE-4 (DDP-4) INHIBITORS: Enhances the incretin system, stimulates release of insulin for beta cells, and decreases hepatic glucose production.
Sitagliptin(Januvia):PO Upperrespiratorytract 1. ShouldnotbeusedinType1diabetesorforthetreatmentofVildagliptin(Galvus):PO infection,sorethroat, diabeticketoacidosis. headache,diarrhea.
INJECTABLE DRUGS FOR DIABETES
AMYLIN MIMETICS: Complements the effects of insulin by delaying gastric emptying and suppressing glucagon secretion.
Pramlintide(Symlin):SQ Hypoglycemia,nausea, 1. Teachclienttotakeotheroralmedicationsatleast1hourprior injectionsitereactions. totakingor2hoursafter,becauseofdelayedgastricemptying. 2. Injectedintothighorabdomen. 3. Cannotbemixedwithinsulin.
NURSING PRIORITY: ✔ Can cause severe hypoglycemia when used with insulin; usually occurs within 3 hours following injection.
INCRETIN MIMETICS: Stimulates release of insulin, decreases glucagon secretion, decreases gastric emptying, and suppresses appetite.
Exenatide(Byetta):SQ Hypoglycemia,nausea, 1. Usedinconjunctionwithmetformin. vomiting,diarrhea, 2. Monitorweight. headache,possibleweight 3. Notindicatedforusewithinsulin. loss.
CBC,Completebloodcount;GI,gastrointestinal;IM,intramuscularly;IV,intravenously;LFTs,liverfunctiontests;PO,bymouth(orally);SQ,subcutaneously.
Related Documents






![[PPT]Lab 10 Special Senses and Endocrine System · Web viewLab 11 THE SPECIAL SENSES AND THE ENDOCRINE GLANDS Thyroid & Parathyroid, 100x Thyroid & Parathyroid, 400x Parathyroid Hormone](https://static.cupdf.com/doc/110x72/5aee361c7f8b9a3b2e91b2bd/pptlab-10-special-senses-and-endocrine-viewlab-11-the-special-senses-and-the-endocrine.jpg)


