1 15-F 2t -isoprostane exacerbates myocardial ischemia-reperfusion injury of isolated rat hearts Authors: Zhengyuan Xia 1,2 , Kuo-Hsing Kuo 1;3 , David V. Godin 1 , Michael J Walker 1 and Michelle C.Y. Tao 1* , David M. Ansley 1 Affiliations: 1 Centre for Anesthesia & Analgesia, Dept. of Anesthesiology, Pharmacology & Therapeutics, The University of British Columbia, Vancouver, BC, V6T 1Z3, Canada; 2 Anesthesiology research laboratory, Dept of Anesthesiology, Renmin Hospital of Wuhan University, Wuhan, China; 3 Dept. of Anatomy and Histology, University of Northern British Columbia, Canada; * Summer student Running title: Isoprostane exacerbates cardiac reperfusion injury Word counts: 3912 words (Text). Address correspondence and request for reprints to: Dr. David M. Ansley University of British Columbia Department of Anesthesiology Room 3200, 3 rd Floor JPP 910 West 10 th Ave Vancouver, BC Canada V5Z 4E3 Phone: 604-875-4575 Fax: 604-875-5344 Email: [email protected] Presented in part at the First Global Conference on Cardiovascular Clinical Trials and Pharmacotherapy incorporating the 2 nd World Heart Federation Global Conference on Cardiovascular Clinical Trials and 13 th International Society of Cardiovascular Pharmacotherapy Congress, Oct 1-3, 2004. Hong Kong, China. Published in abstract form in Cardiovasc Drugs Ther 2004;18(supplement 1): A63. Articles in PresS. Am J Physiol Heart Circ Physiol (June 3, 2005). doi:10.1152/ajpheart.00042.2005 Copyright © 2005 by the American Physiological Society.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
15-F2t-isoprostane exacerbates myocardial ischemia-reperfusion injury of isolated rat hearts Authors: Zhengyuan Xia1,2, Kuo-Hsing Kuo1;3, David V. Godin1, Michael J Walker1 and Michelle C.Y. Tao1* , David M. Ansley1
Affiliations: 1Centre for Anesthesia & Analgesia, Dept. of Anesthesiology, Pharmacology & Therapeutics, The University of British Columbia, Vancouver, BC, V6T 1Z3, Canada; 2Anesthesiology research laboratory, Dept of Anesthesiology, Renmin Hospital of Wuhan University, Wuhan, China; 3 Dept. of Anatomy and Histology, University of Northern British Columbia, Canada; *Summer student
Running title: Isoprostane exacerbates cardiac reperfusion injury Word counts: 3912 words (Text). Address correspondence and request for reprints to: Dr. David M. Ansley University of British Columbia Department of Anesthesiology Room 3200, 3rd Floor JPP 910 West 10th Ave Vancouver, BC Canada V5Z 4E3 Phone: 604-875-4575 Fax: 604-875-5344 Email: [email protected] Presented in part at the First Global Conference on Cardiovascular Clinical Trials and Pharmacotherapy incorporating the 2nd World Heart Federation Global Conference on Cardiovascular Clinical Trials and 13th International Society of Cardiovascular Pharmacotherapy Congress, Oct 1-3, 2004. Hong Kong, China. Published in abstract form in Cardiovasc Drugs Ther 2004;18(supplement 1): A63.
Articles in PresS. Am J Physiol Heart Circ Physiol (June 3, 2005). doi:10.1152/ajpheart.00042.2005
Copyright © 2005 by the American Physiological Society.
2
Abstract Background: 15-F2t-isoprostane is a specific marker of in vivo lipid peroxidation induced by
reactive oxygen species (ROS) whose formation is increased after myocardial ischemia and
during the subsequent reperfusion. 15-F2t-isoprostane possesses potent bioactivity under
pathophysiological conditions. However, it remains unknown whether 15-F2t-isoprostane, by
itself, can influence myocardial ischemia-reperfusion injury (IRI).
Methods: Adult rat hearts were perfused by the Langendorff technique with Krebs-Henseleit
solution (KH) at a constant flow rate at 10 ml/min. 15-F2t-isoprostane 100 nM (IsoP), SQ 29548
1µM (SQ), a thromboxane receptor antagonist that can abolish the vasoconstrictor effect of 15-
F2t-isoprostane, or their combination (IsoP+SQ) in KH or KH alone (vehicle control) were
applied for 10 min before inducing 40 min global ischemia, followed by 60 min of reperfusion.
During ischemia, saline (control), IsoP, IsoP+SQ or SQ in saline was perfused through the aorta
at 60 µl/min. Either IsoP, IsoP+SQ or SQ in KH were infused during the first 15 min of
reperfusion. Results: Coronary effluent endothelin-1 (ET-1) concentrations in the IsoP group
were significantly higher than those in the control group during ischemia and also in the later
phase of reperfusion (P<0.05). Infusion of 15-F2t-isoprostane resulted in increased release of
cardiac-specific creatine kinase (CK-MB) and reduced cardiac contractility during reperfusion
and also increased myocardial infarct size relative to the control group. SQ 29548 abolished
the deleterious effects of 15-F2t-isoprostane. Conclusion: 15-F2t-isoprostane exacerbates
myocardial IRI, and may therefore act as a mediator of IRI. 15-F2t-isoprostane induced ET-1
production during cardiac reperfusion may represent a mechanism underlying the deleterious
actions of 15-F2t-IsoP.
Key words: 15-F2t-isoprostane; myocardial; ischemia-reperfusion injury
3
Myocardial ischemia-reperfusion injury (IRI) and its sequelae, cardiac depression and
arrythmogenesis, have been shown experimentally to result, at least in part, from the
disruptive action of reactive oxygen species (ROS) on membrane lipids and intracellular
proteins required for cellular integrity and function. (12;15;26) The release of high levels of
ROS during ischemia-reperfusion can overwhelm endogenous antioxidant defenses, a crucial
event determining the onset of irreversible cellular necrosis secondary to extensive lipid
peroxidation.(17)
A recent advance in free radical biology has been the discovery of isoprostanes, which
are stable in vivo end products of arachidonic acid peroxidation.(22) Of the variety of
isoprostanes detected, 15-F2t-isoprostane (15-F2t-IsoP) (28) has been found to be a specific,
reliable marker of oxidative stress. This has facilitated investigation of the role of ROS in a
variety of disease states, most notably cardiovascular disease. Of interest, 15-F2t-IsoP
possesses potent biological activity, including vasoconstriction and platelet activation under
pathophysiological conditions.(21) 15-F2t-IsoP has no effect on coronary flow in the absence
of ischemia in the isolated rat hearts (up to a concentration of 256 nM), but significantly
reduces coronary flow in the hypoxic or post-ischemic reperfused rat heart (at 30 nM).(14)
Clinically we identified an inverse correlation between the speed of decay of plasma
15-F2t-IsoP concentrations during the early phase of reperfusion and post-operative cardiac
functional recovery in patients undergoing coronary artery bypass surgery utilizing
cardiopulmonary bypass (CPB).(1) The characteristics of 15-F2t-IsoP production and its
effects under conditions of ischemia and reperfusion are similar to those of endothelin-1 (ET-
1). Endothelin-1 is one of the most potent vasoconstrictors known, and it has been postulated
to contribute to post-ischemic myocardial dysfunction (25;27). ET-1 release has been shown

4
to increase during and after myocardial ischemia (3) and its vasoconstrictor effect appears to
be potentiated during post-ischemic reperfusion in isolated hearts. (23;38)
We hypothesized that 15-F2t-IsoP can exacerbate myocardial ischemia-reperfusion
injury and that the mechanism of 15-F2t-IsoP action may involve the release and/or enhancing
the production of ET-1 during cardiac ischemia and reperfusion. Our hypothesis was tested in
an isolated rat heart model, using SQ 29548, a thromboxane A2 receptor (TXA2) antagonist
used to abolish the vasoconstrictive actions of 15-F2t-IsoP.(13)
Methods
Heart preparation
This study was approved by the Committee of Animal Care of the University of
British Columbia. Animals were cared for in accordance with the principles and guidelines of
the Canadian Council on Animal Care. Male Sprague-Dawley rats (280~320g) were
anesthetized with pentobarbital (70mg/kg intraperitoneally) and heparinized with sodium
heparin (1000 IU/kg, intraperitoneally). After median thoracotomy, hearts were quickly
excised and immersed in ice-cold Krebs-Henseleit (KH) solution to stop contractions. Hearts
were gently squeezed to remove residual blood to prevent clot formation. Hearts were
retrogradely perfused via the aorta in a non-working "Langendorff" preparation at a constant
flow rate of 10 ml/min using a peristaltic pump. The perfusion fluid (pH 7.4; temperature,
37°C) was KH solution that contained (in mM): NaCl 118; NaHCO3 24; KCl 4.63; MgCl2 1.2;
CaCl2 1.25; KH2 PO4 1.17; glucose 11. The perfusate was bubbled with a mixture of 95% O2
and 5% CO2. Temperatures of the perfusate solution and of the chamber in which the hearts
were rested were maintained at 37°C using a thermostatically controlled water circulating

5
system. Coronary perfusion pressure (CPP) was measured via a side arm of the perfusion
cannula connected to a pressure transducer (Statham p23 ID, Gould Electronics, Cleveland).
A latex water-filled balloon fixed to a pressure transducer was inserted through the mitral
valve into the left ventricle for the determination of left ventricular (LV) developed pressure
(LVDP), which was calculated by subtracting end-diastolic pressure (LVEDP) from LV peak
systolic pressure (LVSP). LVEDP was adjusted to approximately 5 mmHg before the start of
the experiment by adjusting the volume in the intraventricular balloon.
Experimental Protocol
All hearts were initially equilibrated for 10 min (BS10). They then were randomly
assigned to a sham group or one of the four experimental groups (n=7 per group): ischemia-
reperfusion untreated control (control), 15-F2t-IsoP (IsoP), 15-F2t-IsoP plus SQ 29548 (IsoP-
SQ) or SQ 29548 (SQ) alone . After BS10, 15-F2t-IsoP 100 nM/L (IsoP), SQ 29548 1µM/L
(SQ) or 15-F2t-IsoP 100 nM/L plus SQ 29548 1µM/L (IsoP+SQ) were applied for 10 min
respectively in the corresponding groups, before global ischemia (40 min) was induced by
stopping perfusion. Control hearts underwent an additional 10 min period of equilibration
before global ischemia was induced. During ischemia, saline (control), 15-F2t-IsoP 100 nM/L
(IsoP), SQ 29548 1µM/L (SQ) or 15-F2t-IsoP 100 nM/L plus SQ 29548 1µM/L (IsoP+SQ) in
saline was perfused through the aorta at 60 µl/min using a mini-pump. KH was perfused
during 60 min of reperfusion in the control group. Either 15-F2t-IsoP, SQ 29548 or 15-F2t-
IsoP plus SQ 29548 in KH was perfused for the first 15 min of reperfusion. Hearts were
electrically paced at a rate of 300 beats/min, prior to and following, but not during the
ischemic period when hearts ceased to beat spontaneously.
6
The perfusion flow rate was based on the result of a pilot study which showed that
sham isolated hearts perfused at 10 ml/min with KH beat well and remain hemodynamically
stable for 120 min (the duration of the experiment) in our experimental set-up. The
concentration of 15-F2t-IsoP applied in the current study was based on: 1) prior reporting that
15-F2t-IsoP 100 nM did not affect coronary flow in sham-perfused rat hearts but significantly
reduced coronary flow in ischemic-reperfused rat hearts (13); and 2) our own pilot study
which showed that 15-F2t-IsoP at 30 nM did not cause significant reduction in post-ischemic
LVDP (n=3) compared to control, but when 300 nM 15-F2t-IsoP was given in our
experimental set-up, hearts were not able to resume beating during reperfusion (n=2). Studies
have shown that SQ 29548, a thromboxane A2 (TXA2) receptor antagonist (24), abolished
15-F2t-IsoP (56 nM)-induced reduction in coronary flow in ischemic-reperfused rat hearts at a
concentration of 0.1µM (13) and abolished 15-F2t-IsoP (>300 nM) -induced reduction in
coronary flow in isolated perfused guinea pig heart at 1µM.(20) Therefore, 1µM SQ 29548
was applied in the current study to ensure blockade of 15-F2t-IsoP action in our model.
Effluent perfusate was sampled at BS10, the first 30 min of ischemia (isch) and at 1
(Re-1), 5 (Re-5), 30 (Re-30) and 60 (Re-60) min of reperfusion in the four experimental
groups or at the corresponding time points in the sham group. Aliquots of the effluent samples
were immediately stored at -70 °C until analysis for cardiac specific creatine kinase (CK-MB)
in all study groups and for 15-F2t-IsoP in the sham, control and SQ groups. Another portion of
the effluent sample was initially concentrated (see below) and then stored at -70 °C for
analysis of ET-1 concentration. At the end of the 60 min of reperfusion, 37ºC 1% 2,3,5-
triphenyltetrazolium in buffer (0.1 M phosphate buffer adjusted to pH 7.4) was pumped into
7
the heart at 1 ml/gm/min for 15 min until the epicardial surface became deep red. The hearts
were then stored in 10% formaldehyde for later analysis of myocardial infarct size.
Measurement of Endothelin-1
Enzyme immunoassays (EIA) of ET-1 concentrations in the coronary effluent were
performed in duplicate according to the manufacturer’s instruction (human ET-1 EIA kit 900-
020, Assay Designs, Inc. Ann Arbor). The Assay kit detects ET-1 levels in biological fluids of
human, bovine, canine, murine, porcine and rat (32) samples. Based on pilot studies, ET-1
concentrations in our samples were often below the ET-1 sensitivity of the assay (0.14pg/ml).
Therefore effluent samples were concentrated 4-fold by evaporation of solvent (i.e. the KH
solution) at room temperature under a stream of dry nitrogen. ET-1 concentration was
calculated as 1/4 of the measured ET-1 level in the concentrated sample. The accuracy of this
approach was confirmed by prior testing using known ET-1 standards. The assays plates were
read at 450 nm and the values of the unknowns were expressed as picograms ET-1 per
milliliter effluent.
Measurement of CK-MB
Measurement of CK-MB was determined by enzyme immunoassay (Catalog number:
BC-1121, BioCheck, Inc, Burlingame, CA). The unknowns were expressed as nanograms
CK-MB per milliliter effluent.
8
15-F2t-IsoP Assays
Enzyme immunoassay of free 15-F2t-IsoP was performed according to the methods
provided by the manufacturer (Cayman Chemical, Ann Arbor) as previously described
(33,34). The values of the unknowns were expressed as picograms 15-F2t-IsoP per milliliter
effluent.
Infarct size measurement
The measurement of infarct size was essentially identical to that described by Downey
(8) except for the method of quantification. After the 2,3,5-triphenyl-tetrazolium chloride
(TTC) reaction, the hearts were sectioned transaxially, and size of infarct was evaluated as
percentage of sectional area of infarcted tissue to the sectional area of the whole heart in 1
mm layers (five layers, LG scanner). Morphometric measurements of infarct size were
performed with a LG scanner and 6.0 CE software. The histogram counts of the red (viable
tissue) and white (infracted tissue) were recorded. The percent infarction was calculated as
white counts divided by the sum of the red plus white counts.
Statistical analysis
All data are presented as means ± SEM. Cardiac variables and chemical assay
parameters were compared by two-way analysis of variance (ANOVA) with repeated
measures. One-way ANOVA was used to test for differences in infarct size between groups.
The correlation between effluent ET-1 and 15-F2t-IsoP concentration was evaluated by the
Pearson test. P<0.05 was considered statistically significant.
9
Results
Endothelin-1 release and its relation with 15-F2t-IsoP
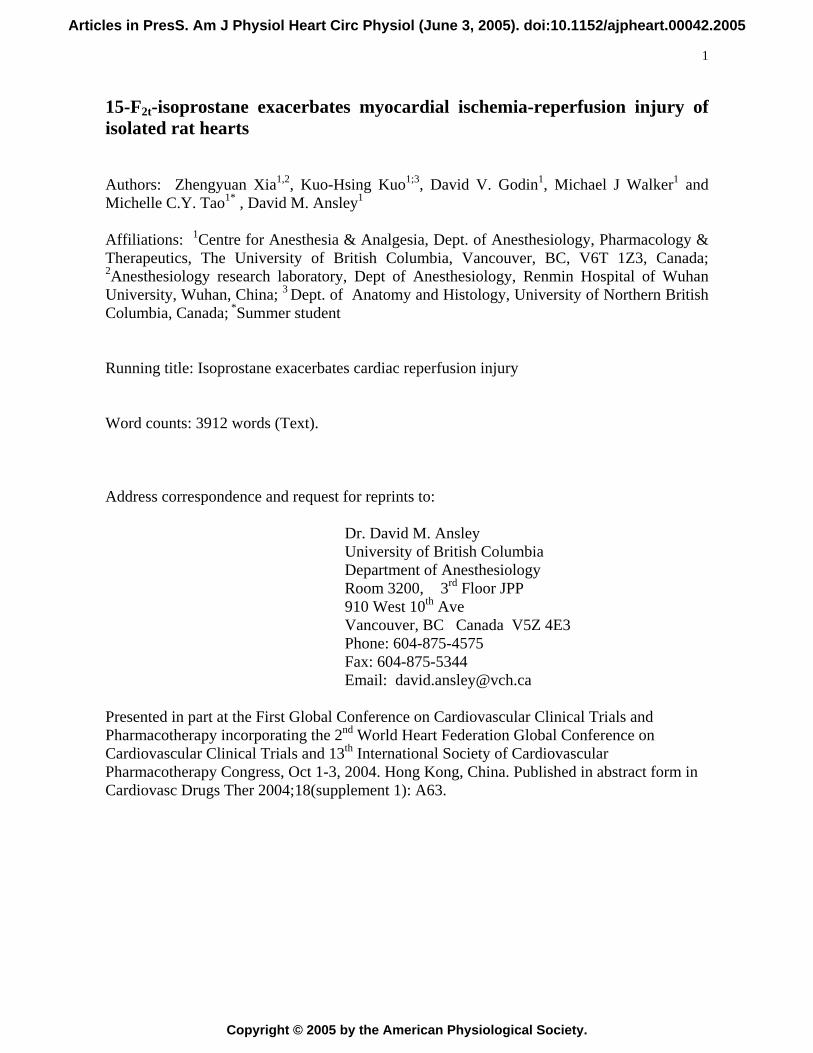
Baseline effluent ET-1 concentrations did not differ among the experimental groups
(Fig 1A). Effluent ET-1 did not significantly change over time in the sham group (data not
shown). ET-1 increased in the control group during ischemia (Fig 1A, P <0.001 vs baseline)
and increased further in the Iso-P group compared to control (P<0.05). ET-1 increased by
approximately 20% at Re-1 and by 32.8±26.9% at Re-30 compared to baseline (BS10) in the
control group. These changes did not reach statistical significance (P>0.1). Effluent ET-1
concentration in the IsoP group was significantly higher than that in the control group (P<0.05)
at reperfusion 60min (Re-60). Effluent ET-1 concentrations in both the IsoP-SQ and the SQ
groups did not differ from those found in the control during ischemia and reperfusion. A weak
but statistically significant positive correlation (r = 0.77, P =0.04, Fig 1B) was noted between
effluent concentrations of 15-F2t-IsoP and ET-1 during ischemia, but not during reperfusion,
in the control (i.e., untreated) group.
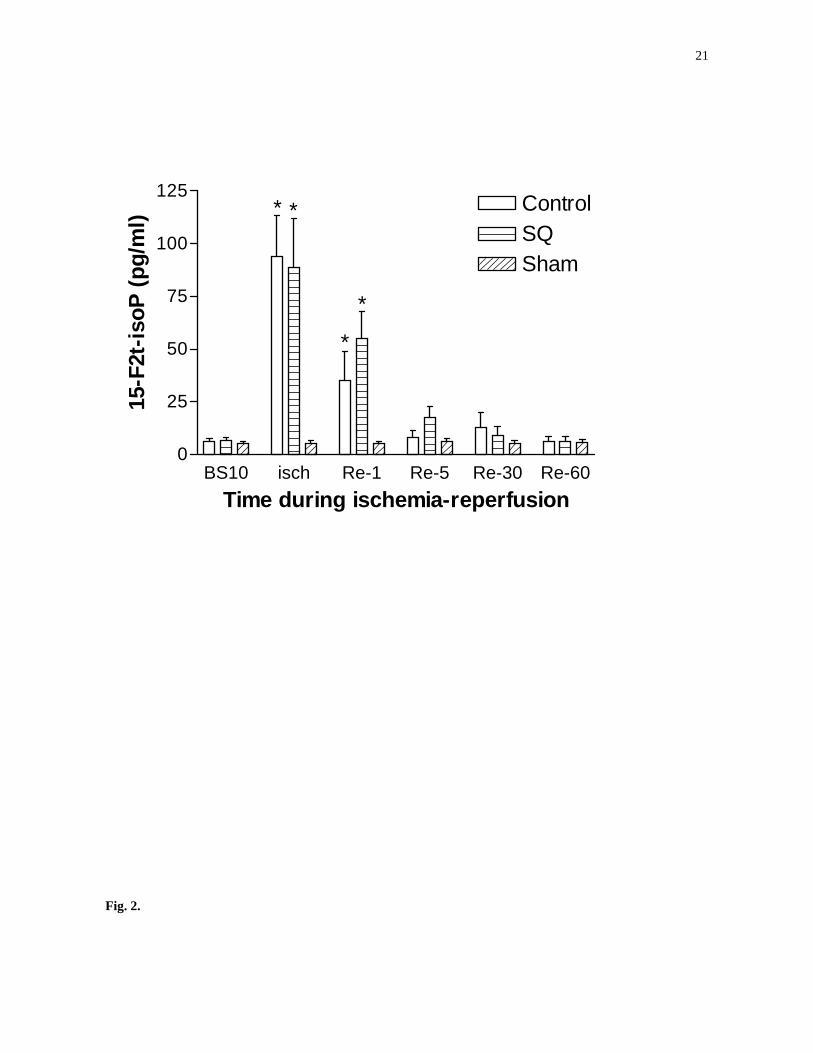
15-F2t-IsoP generation during ischemia-reperfusion
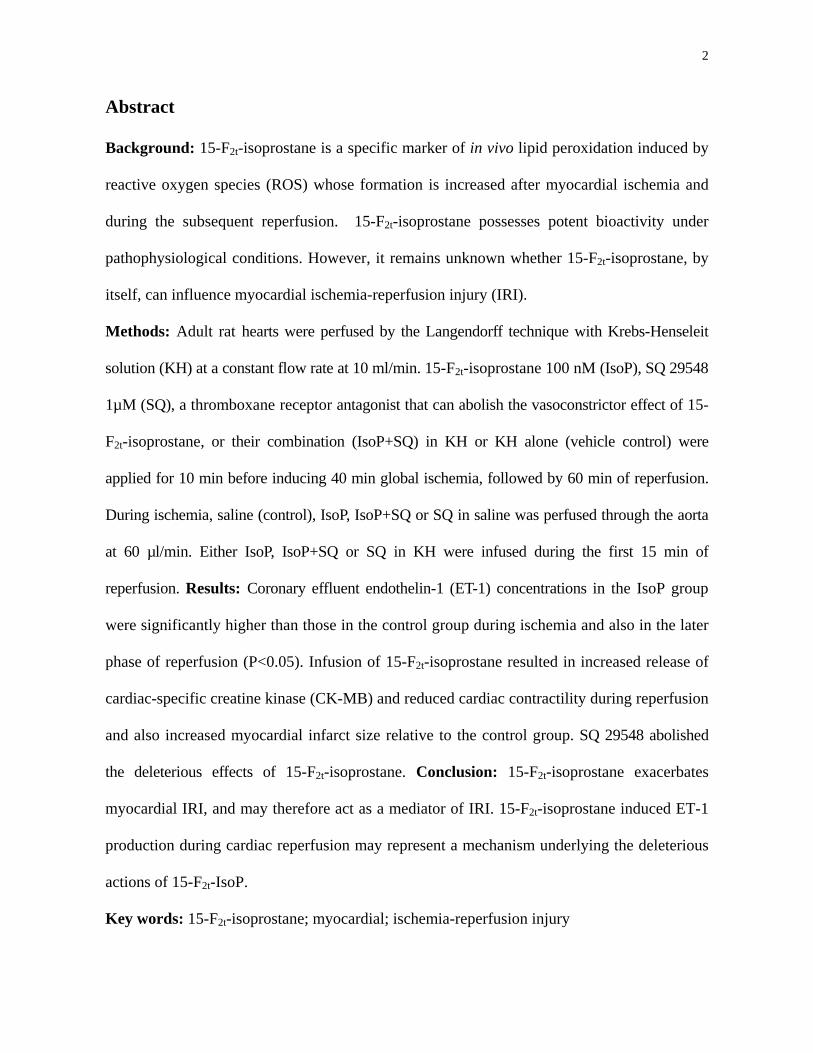
Effluent 15-F2t-IsoP release in the sham group did not change over a 120 min
perfusion period (Fig 2). As shown in Fig 2, effluent 15-F2t-IsoP levels increased during
ischemia (P < 0.001 vs BS10) and remained elevated at Re-1 (P<0.05 or P<0.01 vs BS10) in
the control and SQ groups. Effluent 15-F2t-IsoP release during ischemia and reperfusion did
not significantly differ between the control and SQ groups.
10
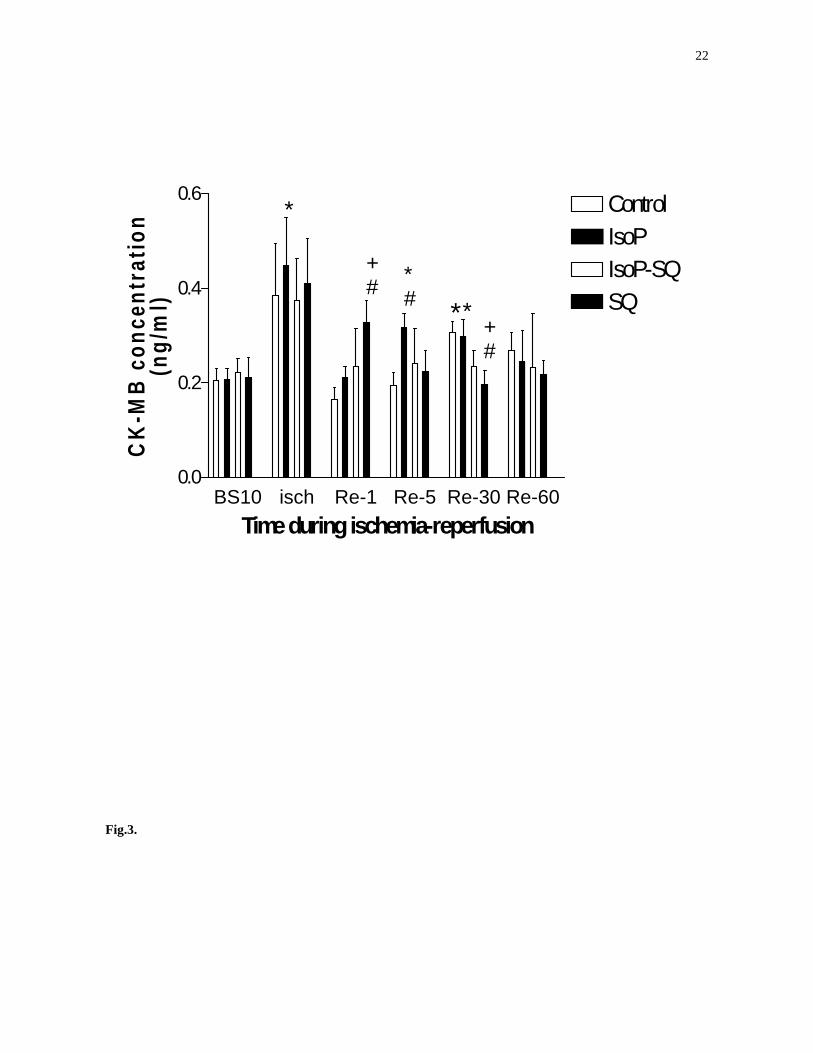
CK-MB release during ischemia-reperfusion
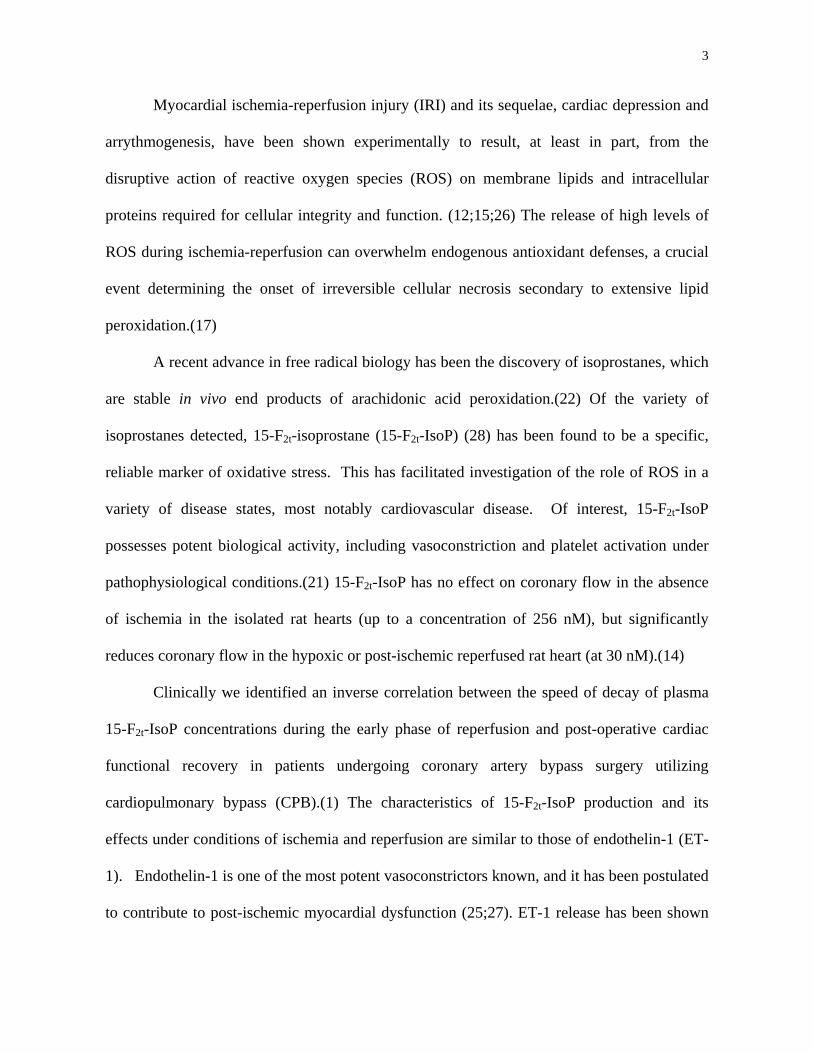
Baseline CK-MB release was detectable in this model and did not differ among groups
(Fig 3). Effluent CK-MB release did not significantly change over time in the sham group.
During ischemia, CK-MB increased significantly from baseline values only in group iso-P
(p<0.05).
During reperfusion, CK-MB increased gradually and was significantly higher than
baseline at Re-30 in the control group (P<0.01). Effluent CK-MB concentration in the IsoP
group increased more rapidly during reperfusion and was significantly higher at Re-5 than its
baseline value (P<0.05). This was also significantly greater than values measured in control
hearts at the same time interval (p<0.05). CK-MB levels in IsoP-SQ were similar to values
measured in untreated control hearts during ischemia and reperfusion. At Re-1, CK-MB level
in SQ was higher than in the control group and the IsoP group (<0.05) but then decreased
quickly thereafter.
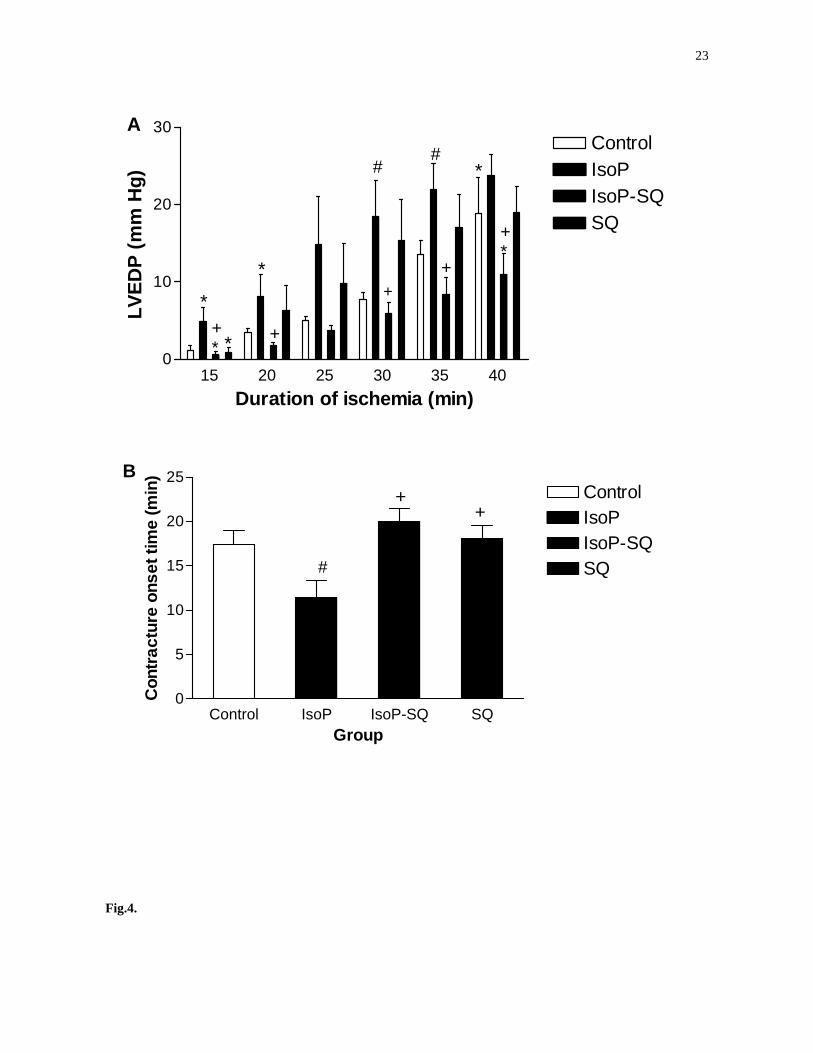
Contracture development during ischemia
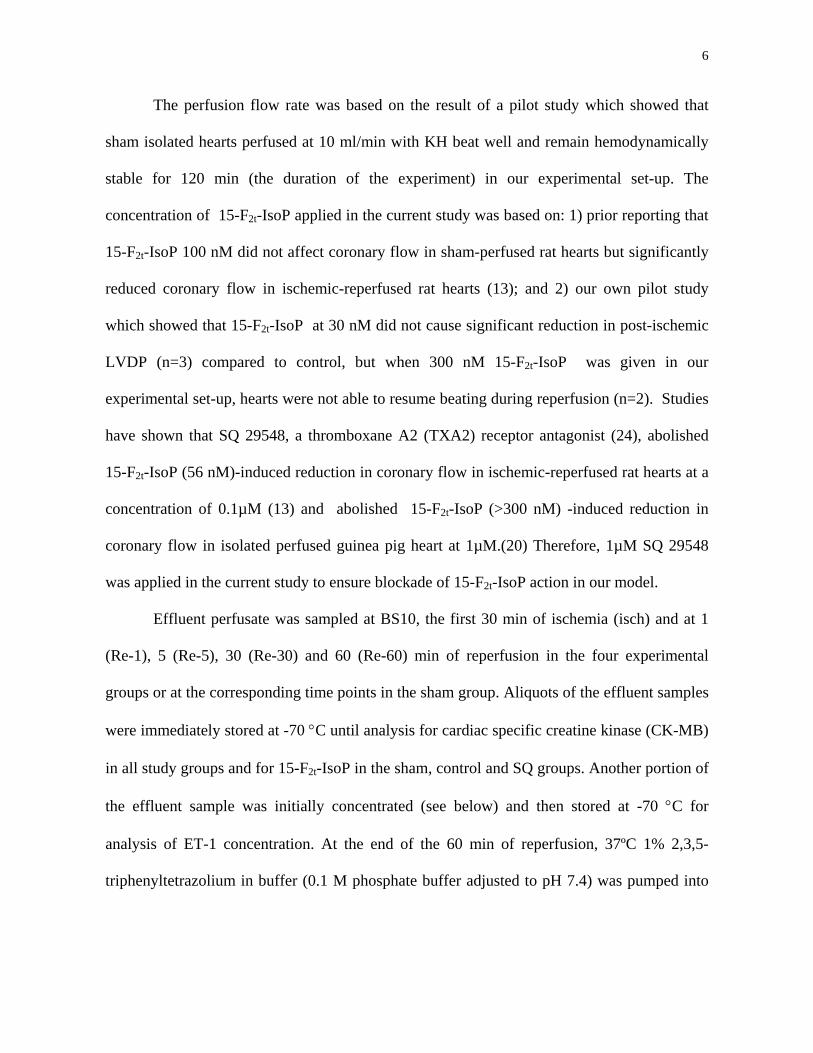
The LVEDP increased progressively during ischemia in the control group (Fig 4A).
LVEDP in the IsoP group increased more quickly. At 30 and 35 min of ischemia, the
magnitude of LVEDP in the IsoP group was significantly higher than that in the control group
(P<0.05). SQ 29548 attenuated the effect of 15-F2t-IsoP on ischemic contracture. LVEDP was
significantly lower in the IsoP-SQ group than the IsoP group at ischemia 30 min and onwards.
LVEDP in the IsoP-SQ and the SQ group did not differ from that measured in the control
group during ischemia.
Time to the onset of ischemic contracture was significantly shorter in the IsoP group
(11.4±1.9 min) compared to control (17.4±1.6 min, P <0.05, Fig 4B). The latency to ischemic
11
contracture in the IsoP-SQ (20.0±1.5 min) and the SQ (18.1±1.5 min) groups was
significantly increased compared to that in the IsoP group (P<0.01 or P<0.05), but did not
differ from that in the control group (P>0.05, Fig 4B).
Functional response to ischemia/reperfusion
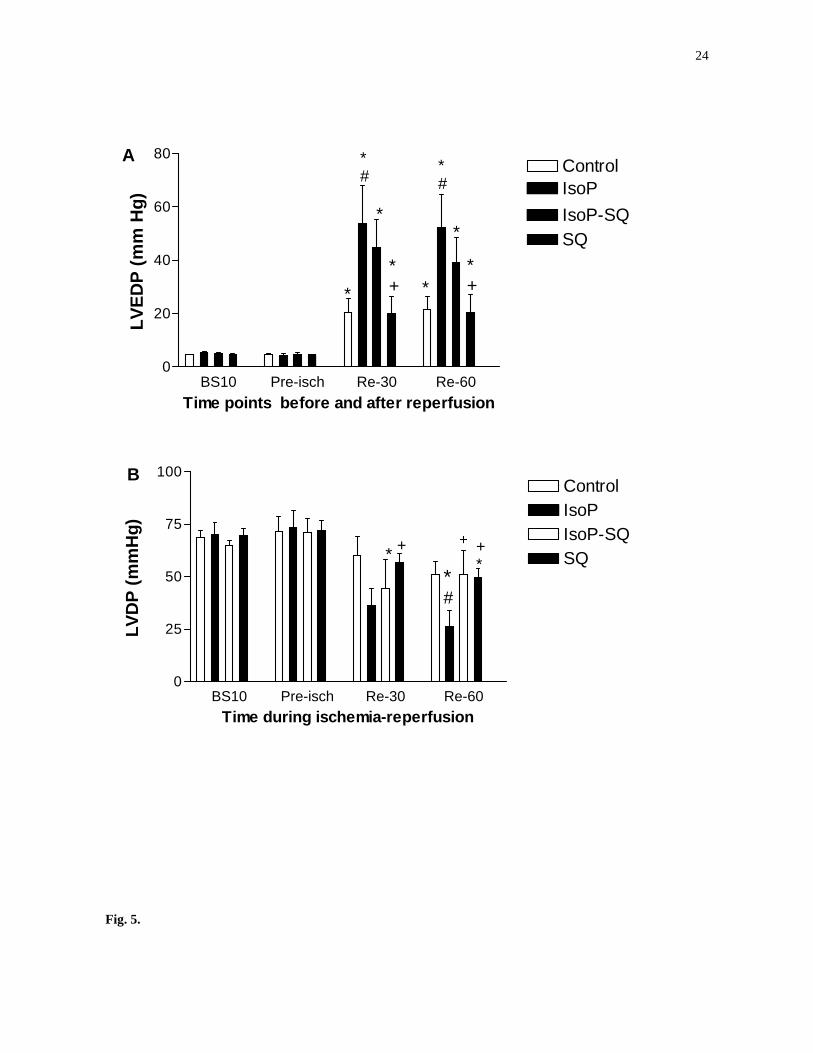
During reperfusion, LVEDP in the control group was significantly higher than that at
baseline (Fig 5A). 15-F2t-IsoP significantly augmented the increase of LVEDP during
reperfusion at Re-30 and Re-60 (P<0.01). SQ 29548 attenuated the 15-F2t-IsoP-induced
increase in LVEDP. The magnitude of LVEDP in the IsoP-SQ and the SQ groups did not
significantly differ from that in the control group during reperfusion.
The LVDP in the sham group did not change significantly over time during the
experimental period. The LVDP in the control group recovered to a maximum of 87.0±11.6 %
of its baseline value at Re-30 (P>0.05 vs BS10, Fig 5B) and decreased thereafter. The LVDP
in the IsoP group recovered to a maximum of 56.5±13.5% of its baseline value at Re-30
(P<0.05 vs BS10) and decreased quickly thereafter. At Re-60, LVDP in the IsoP group was
lower than that in the control group. The LVDP values in the IsoP-SQ and the SQ group did
not differ from those in the control group at Re-60. SQ 29548 exacerbated 15-F2t-IsoP
induced reduction in LVDP relative to control group at Re-10.
Coronary perfusion pressure (CPP)
Neither 15-F2t-IsoP, SQ 29548, nor their combination affected CPP before ischemia.
CPP did not increase significantly until after 60 min of reperfusion in the untreated control
group (80.4±11.0 mmHg at Re-60 vs 51.3±1.1 mmHg at BS10, P<0.05). CPP in the IsoP
group increased more quickly during reperfusion relative to the control group. At Re-30, the
12
CPP value in the IsoP group (100.4±13.9 mmHg) was higher (P<0.05) than its baseline value
(52.1±3.9 mmHg) and higher (P<0.05) than the corresponding value in the control group
(65.6±4.6 mmHg). SQ 29548 did not significantly affect CPP as compared to the control
group. At Re-60, CPP values did not significantly differ among the control (80.4±11.0
mmHg), the IsoP (110.4±14.9 mmHg), the IsoP+SQ (115.4±14.9 mmHg) and the SQ
(84.8±13.5 mmHg) groups (P>0.05).
Myocardial infarct size
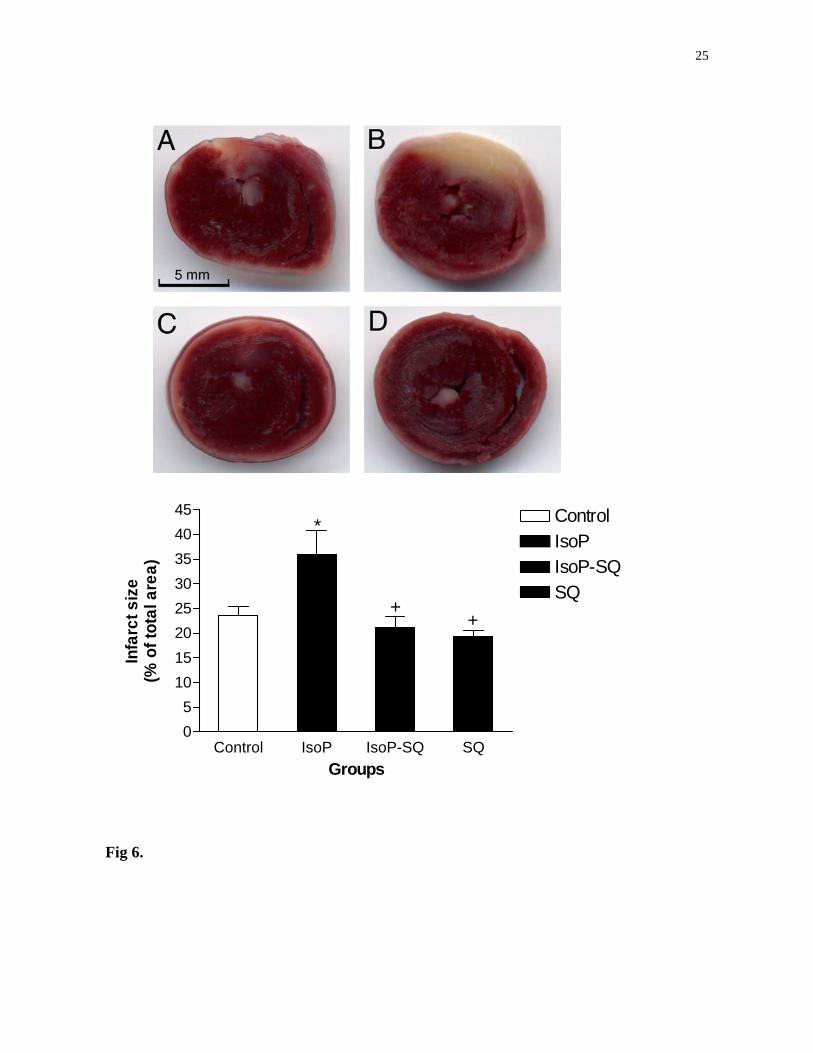
As shown in Figure 6, myocardial infarct size in the IsoP group is significantly larger
than that of the control (untreated) group (P<0.05). The myocardial infarct sizes in the IsoP-
SQ and SQ groups are significantly smaller than those in the IsoP group (P<0.05 or P<0.01).
Infarct sizes in the SQ group and IsoP-SQ groups were somewhat smaller than those in the
control group, but the differences did not attain statistical significance.
Discussion
This is the first study providing evidence that 15-F2t-IsoP exacerbates myocardial IRI
in isolated perfused rat hearts. Our findings include the following: (1) 15-F2t-IsoP did not
affect pre-ischemic cardiac mechanics and coronary perfusion pressure but did reduce cardiac
tolerance to ischemic insult, as manifested by an early onset and higher magnitude of
ischemic contracture; (2) 15-F2t-IsoP stimulated the release and/or production of ET-1 during
ischemia which was accompanied by an increased severity of myocardial cellular damage as
evidenced by increased CK-MB release; (3) 15-F2t-IsoP increased myocardial infarct size and
13
exacerbated post-ischemic myocardial dysfunction, which may be attributable, in part, to
stimulation of ET-1 production and/or release during reperfusion.
Endothelin-1 has potent vasoconstrictor properties and is known to reduce myocardial
contractility and contribute to the progression of the heart failure.(27) Plasma levels of ET-1
increase during cardiac operations requiring cardiopulmonary bypass (CPB)(2;31). A high
plasma ET-1 level during the early postoperative period has been associated with prolonged
pharmacologic management (i.e., inotropic support), longer intensive care unit stay, and
complicated recovery.(2;7). The present study clearly demonstrates that 15-F2t-IsoP, whose
formation increased in the myocardium and coronary artery during CPB surgery,(18) can
increase the release and/or production of ET-1 during myocardial ischemia-reperfusion. This
might be a mechanism whereby 15-F2t-IsoP exacerbates myocardial IRI. The positive
correlation between effluent concentrations of 15-F2t-IsoP and ET-1 during ischemia in the
control (untreated) group suggests that endogenous 15-F2t-IsoP may act to stimulate increased
ET-1 release during ischemia.
We observed a reduction in ET-1 concentration at 30 min of reperfusion (Re-30), but a
statistically significant increase by 60 min of reperfusion (Re-60) in the IsoP group compared
to control (Fig 1A). 15-F2t-IsoP may have triggered an increased formation of ET-1 during
late reperfusion. In the IsoP group, the infusion of 15-F2t-IsoP was terminated at 15 min of
reperfusion. Sequestration of a significant amount 15-F2t-IsoP in the heart tissue 45 min after
the termination of exogenous 15-F2t-IsoP infusion is unlikely in this study, since the 15-F2t-
IsoP decay half-life in this model is about 4 min (data not presented). 15-F2t-IsoP stimulation
of ET-1 formation during late reperfusion could represent an important mechanism
responsible for post-ischemic myocardial dysfunction in the clinical setting. Whereas we
14
previously found that plasma free 15-F2t-IsoP levels increased during ischemia-reperfusion for
approximately 30 min during cardiac surgery, the 15-F2t-IsoP decay pattern during early
reperfusion correlated with early postoperative cardiac recovery.(1) Plasma ET-1 levels may
remain elevated at least 24 hours after cardiac surgery.(35) Recent study conducted in isolated
rat cardiomyocytes has shown that 30 min of ischemia with or without 30 min of reperfusion
is sufficient to rapidly stimulate the gene expression of myocyte ET-1 as well as the ET-1
receptors. (9) It is possible that high levels of 15-F2t-IsoP during ischemia and/or early
reperfusion may have induced ET-1 gene expression resulting in increased ET-1 production
during late reperfusion. Further study is merited to address the underlying mechanism.
Based on our results we postulate that 15-F2t-IsoP may increase ET-1 release into the
coronary circulation relative to the myocardial tissue during ischemia. It has been previously
shown that the ratio of ET-1 secretion to the interstitial transudates versus secretion to
coronary effluent is about 6.6 at baseline in isolated perfused rat hearts (3). This ratio is
reduced to about 2.5 during the period of low-flow ischemia and the first 30 min of
reperfusion.(3) The relative reduction of ET-1 concentration observed in the IsoP group at 30
min of reperfusion, 15 min after the termination of 15-F2t-IsoP infusion, indicates 15-F2t-IsoP
may have primarily stimulated ET-1 release rather than its production during ischemia and
early reperfusion.
Despite 15-F2t-IsoP’s bioactivity as a vasoconstrictor,(21;29) reduction of coronary
flow is not likely a major mechanism of 15-F2t-IsoP action during myocardial IRI, at least in
this model. In the current study, hearts were perfused at a constant flow rate. In addition, CPP
at Re-60 did not differ significantly among experimental groups although LVDP in the IsoP
group was significantly lower than that in the control, IsoP-SQ and the SQ groups. It is
15
possible that 15-F2t-IsoP aggravates myocardial IRI by a complex mechanism involving the
activation of Na+-H+ exchange indirectly through ET-1.(4;11). Alternatively, 15-F2t-IsoP may
act by reducing the intrinsic activity of nitric oxide,(19) an endogenous vasodilator. This may
explain why the CPP value at Re-30 was higher in the IsoP group relative to control
irrespective of the similar effluent levels of ET-1 at this time point.
Despite abolishing the deleterious effects of high concentration exogenous 15-F2t-IsoP,
SQ 29548 did not confer any beneficial effect in attenuating myocardial IRI compared to the
control in this model. This is in keeping with previous findings describing the effect of
exogenous 15-F2t-IsoP on the isolated guinea pig heart. (20) The relatively high concentration
of CK-MB at Re-1 in the SQ group is likely due to rapid release of CK-MB from the ischemic
tissue rather than the result of more intense tissue damage, since the infarct size of the SQ
group was comparable to that in controls. The inability of SQ 29548 to attenuate myocardial
ischemia-reperfusion injury in the isolated perfused heart model may suggest the following: 1)
endogenous 15-F2t-IsoP production in the myocardium during ischemia and reperfusion is
relatively low under the current experimental condition, and it is mainly a marker (i.e., the
result of lipid peroxidation) rather than a mediator of oxidative damage; 2) TXA2 may play
little role in myocardial IRI in rat, a finding similar to that found in gene knock-out mice. (37)
Given that TXA2 may stimulate rat heart smooth to generate ET-1(6), we can not exclude the
possibility that SQ 29548 blockade of endogenous TXA2 action may have contributed to the
decrease in ET-1 release at Re-60 seen in the isoP-SQ group. It seems apparent that, SQ
29548 blockade of 15-F2t-IsoP action rather than the blockade of TXA2 action represents a
major mechanism of myocardial protection seen in the current study.
16
It is intriguing that SQ blocked the effects of 15-F2t-IsoP on LVEDP during ischemia
but not during reperfusion. It appears that the concentration of 15-F2t-IsoP may be a
determinant of the effectiveness of SQ. At ischemia 40 min (Fig. 4A), the magnitude of
LVEDP in group IsoP-SQ was not only significantly lower than that in group IsoP, but was
also about 40% lower than the corresponding values in the control or SQ groups (P=NS). The
effluent level of ET-1 during ischemia in the IsoP-SQ group was about 20% lower than the
corresponding values in the control or SQ groups. It is possible that this slight 20% difference
in ET-1 concentration during ischemia caused the 40% difference in the magnitude of LVEDP
mentioned above. Study has shown that ischemia may cause time-dependent externalization
of ET-1 receptor binding sites in rat cardiac membranes (16), which may sensitize and
exacerbate ET-1 deleterious effects, such as the exacerbation of ischemic contracture (4).
Further study is merited to address why SQ could act differently, during myocardial ischemia,
in the presence or absence of 15-F2t-IsoP.
It is should be noted that ET-1 has been shown to exert a cardioprotective or
preconditioning-like effect in both in vivo (10) and in vitro (5)models of myocardial ischemia-
reperfusion in the rat, when applied prior to ischemia. Of interest, our most recent study
suggests that ET-1 may confer post-preconditioning-like effect as well in the isolated
ischemic-reperfused rat hearts (36). We found that the ET-1 A and B receptor antagonist
bosentan, when applied during the first 15 min of reperfusion worsened post-ischemic
myocardial dysfunction in the rat heart, and unmasked any potential beneficial effects of ET-1
blockade during ischemia (36). However, when ET-1 receptor blockade was applied only
during later phase of reperfusion, post-ischemic myocardial infarct size was reduced. Hence,
as observed in the current study, an 15-F2t-IsoP induced ET-1 increase during ischemia, and
17
especially during later reperfusion, may represent a major mechanism underlying the
deleterious actions of 15-F2t-IsoP.
In conclusion, our finding that 15-F2t-IsoP can increase myocardial infarct size and
exacerbate myocardial IRI may have important clinical implications. During cardiac surgery,
systemic production of ROS occurs during CPB and may exceed production arising from
reperfusion of the ischemic heart. The plasma level of 15-F2t-IsoP has been observed to
dramatically increase shortly after the start of CPB.(30) These high levels of 15-F2t-IsoP could
enter the heart either before aortic cross-clamping (the beginning of global myocardial
ischemia) or at the time of aortic declamping, triggering and/or exacerbating myocardial IRI.
The findings of the current study combined with our previous work on the effect of
antioxidant supplementation with propofol suggest that combined therapy with antioxidant
and 15-F2t-IsoP antagonism during ischemia and early reperfusion could offer a promising
approach to attenuate myocardial IRI.
Acknowledgements
This study is supported in part by internal department development funding (to D. Ansley) and
in part by the National Natural Science Foundation of China (No: 30471659, to Z. Xia). D. Ansley
received a Clinical Scholar Research Award from the International Anesthesia Research Society. Z.
Xia received a research fellowship from the Centre for Anesthesia & Analgesia, Dept. Pharmacology
& Therapeutics, The University of British Columbia, Canada.
18
Figure legends
Fig.1. A. Effluent Endothelin-1 (ET-1) concentrations during myocardial ischemia-
reperfusion. BS10 and isch indicate 10 min after stabilization and 30 min during global
myocardial ischemia, respectively; Re-1, Re-5, Re-30 and Re-60 indicate 1, 5, 30 and 60 min
after reperfusion, respectively. * P<0.001 vs BS10; # P<0.05 or P<0.01 vs control. (n=7 for
each group). B. Relationship between 15-F2t-isoprostane (15-F2t-isoP) and ET-1
concentration during the first 30 min of ischemia in the control group. ET-1 release is
positively correlated with 15-F2t-isoP concentration (r = 0.7695, 95% CI: 0.0389 – 0.9640,
n=7, P (two-tailed) = 0.043).
Fig. 2. Effect of SQ 29548 (SQ) on 15-F2t-isoprostane (15-F2t-isoP) release during myocardial
ischemia-reperfusion. BS10 and isch indicate 10 min after stabilization and 30 min during
global myocardial ischemia, respectively; Re-1, Re-5, Re-30 and Re-60 indicate 1, 5, 30 and
60 min after reperfusion, respectively. * P<0.001 or P< 0.05 vs BS10. # P< 0.001 vs control. P
>0.05 SQ vs control, n=7 per group.
Fig.3. Effluent CK-MB concentration during myocardial ischemia-reperfusion. BS10 and isch
indicate 10 min after stabilization and 30 min during global myocardial ischemia, respectively;
Re-1, Re-5, Re-30 and Re-60 indicate 1, 5, 30 and 60 min after reperfusion, respectively. *P<
0.05 vs BS10; #P<0.05 vs control; +P<0.05 vs isoP group. (n= 7 for each group)
19
Fig. 4. A: Development of left ventricular end-diastolic pressure (LVEDP), reflecting
myocardial contracture, during ischemia. B: Ischemic contracture onset time. # P<0.05 vs
control; +P<0.05 or P<0.01 vs IsoP (15-F2t-isoprostane) group; *P<0.05 or P<0.01 vs
ischemia 30 min within the same group (n=7 per group).
Fig. 5. A: Variations of left ventricular end-diastolic pressure (LVEDP), reflecting
myocardial stiffness, during reperfusion. BS10 and Pre-isch indicate 10 min after stabilization
and the time immediately prior to ischemia, respectively; Re-30 and Re-60 indicate 30 and 60
min after reperfusion, respectively. *P<0.05 or P<0.01 vs BS10; # P<0.05 or P<0.01 vs
control; +P<0.05 or P<0.01 vs IsoP (15-F2t-isoprostane) group. B: Recovery of left
ventricular developed pressure (LVDP), reflecting effective myocardial contractility, during
reperfusion. BS10 and Pre-isch indicate 10 min after stabilization and the time immediately
prior to ischemia, respectively; Re-30 and Re-60 indicate 30 and 60 min after reperfusion,
respectively. *P<0.05 vs BS10; # P<0.05 vs control; +P<0.05 or P<0.01 vs IsoP (15-F2t-
isoprostane) group (n=7 per group).
Fig. 6. Myocardial infarct size. Top: representative images showing myocardial infarction
(white) in the control (A), 15-F2t-isoprostane plus SQ 29548 (IsoP+SQ, C) and SQ 29548
(SQ, D) groups. Bottom: Percentage infarction (Mean ± SEM, n=7 per group): *P<0.05 vs
control; +P<0.05 or P<0.01 vs IsoP group.

20
BS10 isch Re-1 Re-5 Re-30 Re-600.00
0.25
0.50
0.75
1.00 ControlIsoPIsoP.SQ
A
*
#
* * SQ
*
Time during ischemia-reperfusion
ET-1
con
cent
ratio
n (p
g/m
l)
0 50 100 150 2000.00
0.25
0.50
0.75
1.00B
15-F2t-isoP release during ischemia incontrol group (pg/ml)
ET-1
rel
ease
dur
ing
isch
emia
in c
ontr
ol g
roup
(pg/
ml)
Fig. 1.
21
BS10 isch Re-1 Re-5 Re-30 Re-600
25
50
75
100
125 ControlSQ
* *
*
*
Sham
Time during ischemia-reperfusion
15-F
2t-is
oP (p
g/m
l)
Fig. 2.
22
BS10 isch Re-1 Re-5 Re-30 Re-600.0
0.2
0.4
0.6 ControlIsoPIsoP-SQSQ
*
+# *
# *+#
*
Time during ischemia-reperfusion
CK
-MB
con
cent
ratio
n(n
g/m
l)
Fig.3.
23
15 20 25 30 35 400
10
20
30ControlIsoPIsoP-SQSQ
##
++
*
+*
+
*+* *
*
A
Duration of ischemia (min)
LVED
P (m
m H
g)
Control IsoP IsoP-SQ SQ0
5
10
15
20
25ControlIsoPIsoP-SQSQ
B
#
++
Group
Con
trac
ture
ons
et ti
me
(min
)
Fig.4.
24
BS10 Pre-isch Re-30 Re-600
20
40
60
80ControlIsoPIsoP-SQ
*#
*
*+ *
*#
*
*+*
A
SQ
Time points before and after reperfusion
LVED
P (m
m H
g)
BS10 Pre-isch Re-30 Re-600
25
50
75
100ControlIsoPIsoP-SQSQ* + +
*+
B
*#
Time during ischemia-reperfusion
LVD
P (m
mH
g)
Fig. 5.
25
Control IsoP IsoP-SQ SQ05
1015202530354045 Control
IsoPIsoP-SQSQ
*
++
Groups
Infa
rct s
ize
(% o
f tot
al a
rea)
Fig 6.

26
Reference List
1. Ansley, D. M., Z. Xia, and B. S. Dhaliwal. The relationship between plasma free 15-F2t-
isoprostane concentration and early postoperative cardiac depression following warm heart
surgery. J Thorac Cardiovasc Surg 126: 1222-3, 2003.
2. Bond, B. R., B. H. Dorman, M. J. Clair, C. A. Walker, M. L. Pinosky, S. T. Reeves, S. Walton, J.
M. Kratz, J. L. Zellner, A. J. Crumbley 3rd, M. M. Multani, and F. G. Spinale. Endothelin-1
during and after cardiopulmonary bypass: association to graft sensitivity and postoperative
recovery. J Thorac Cardiovasc Surg 122: 358-64, 2001.
3. Brunner, F. Cardiac tissue endothelin-1 levels under basal, stimulated, and ischemic conditions.
J Cardiovasc Pharmacol 26 Suppl 3: S44-6, 1995.
4. Brunner, F. and L. H. Opie. Role of endothelin-A receptors in ischemic contracture and
reperfusion injury. Circulation 97: 391-8, 1998.
5. Bugge, E. and K. Ytrehus. Endothelin-1 can reduce infarct size through protein kinase C and
KATP channels in the isolated rat heart. Cardiovasc Res 32: 920-9, 1996.
6. Chua, C. C., R. C. Hamdy, and B. H. Chua. Regulation of endothelin-1 production by a
thromboxane A2 mimetic in rat heart smooth muscle cells. Biochim Biophys Acta 1313: 1-5,
1996.
7. Dorman, B. H., B. R. Bond, M. J. Clair, C. A. Walker, M. L. Pinosky, S. T. Reeves, J. M. Kratz,
J. L. Zellner, A. J. Crumbley 3rd, M. M. Multani, and F. G. Spinale. Temporal synthesis and
release of endothelin within the systemic and myocardial circulation during and after
cardiopulmonary bypass: relation to postoperative recovery. J Cardiothorac Vasc Anesth 14:
540-5, 2000.
8. Downey, J. M. Measuring infarct size by the tetrazolium method. Available at:
27
http:/www.usouthal.edu/ishr/help/ttc. [accessed July 15, 2003].
9. Gan, X. T., S. Chakrabarti, and M. Karmazyn. Increased endothelin-1 and endothelin receptor
expression in myocytes of ischemic and reperfused rat hearts and ventricular myocytes exposed
to ischemic conditions and its inhibition by nitric oxide generation. Can J Physiol Pharmacol 81:
105-13, 2003.
10. Gourine, A. V., A. I. Molosh, D. Poputnikov, A. Bulhak, P. O. Sjoquist, and J. Pernow.
Endothelin-1 exerts a preconditioning-like cardioprotective effect against ischaemia/reperfusion
injury via the ET(A) receptor and the mitochondrial K(ATP) channel in the rat in vivo. Br J
Pharmacol 144: 331-7, 2005.
11. Khandoudi, N., J. Ho, and M. Karmazyn. Role of Na(+)-H+ exchange in mediating effects of
endothelin-1 on normal and ischemic/reperfused hearts. Circ Res 75: 369-78, 1994.
12. Kloner, R. A., K. Przyklenk, and P. Whittaker. Deleterious effects of oxygen radicals in
ischemia/reperfusion. Resolved and unresolved issues. Circulation 80: 1115-27, 1989.
13. Kromer, B. M. and J. R. Tippins. Coronary artery constriction by the isoprostane 8-epi
prostaglandin F2 alpha. Br J Pharmacol 119: 1276-80, 1996.
14. Kromer, B. M. and J. R. Tippins. The vasoconstrictor effect of 8-epi prostaglandin F2alpha in
the hypoxic rat heart. Br J Pharmacol 126: 1171-4, 1999.
15. Li, X. Y., P. B. McCay, M. Zughaib, M. O. Jeroudi, J. F. Triana, and R. Bolli. Demonstration of
free radical generation in the "stunned" myocardium in the conscious dog and identification of
major differences between conscious and open-chest dogs. J Clin Invest 92: 1025-41, 1993.
16. Liu, J. J., D. J. Casley, and W. G. Nayler. Ischaemia causes externalization of endothelin-1
binding sites in rat cardiac membranes. Biochem Biophys Res Commun 164: 1220-5, 1989.
17. Meerson, F. Z., V. E. Kagan, Y. u. P. Kozlov, L. M. Belkina, and Y. u. V. Arkhipenko. The role
28
of lipid peroxidation in pathogenesis of ischemic damage and the antioxidant protection of the
heart. Basic Res Cardiol 77: 465-85, 1982.
18. Mehlhorn, U., A. Krahwinkel, H. J. Geissler, K. LaRosee, U. M. Fischer, O. Klass, M.
Suedkamp, K. Hekmat, P. Tossios, and W. Bloch. Nitrotyrosine and 8-isoprostane formation
indicate free radical-mediated injury in hearts of patients subjected to cardioplegia. J Thorac
Cardiovasc Surg 125: 178-83, 2003.
19. Minuz, P., G. Andrioli, M. Degan, S. Gaino, R. Ortolani, R. Tommasoli, V. Zuliani, A. Lechi,
and C. Lechi. The F2-isoprostane 8-epiprostaglandin F2alpha increases platelet adhesion and
reduces the antiadhesive and antiaggregatory effects of NO. Arterioscler Thromb Vasc Biol 18:
1248-56, 1998.
20. Mobert, J., B. F. Becker, S. Zahler, and E. Gerlach. Hemodynamic effects of isoprostanes (8-iso-
prostaglandin F2alpha and E2) in isolated guinea pig hearts. J Cardiovasc Pharmacol 29: 789-
94, 1997.
21. Morrow, J. D., K. E. Hill, R. F. Burk, T. M. Nammour, K. F. Badr, and L. J. Roberts 2nd. A
series of prostaglandin F2-like compounds are produced in vivo in humans by a non-
cyclooxygenase, free radical-catalyzed mechanism. Proc Natl Acad Sci U S A 87: 9383-7, 1990.
22. Morrow, J. D., T. A. Minton, C. R. Mukundan, M. D. Campbell, W. E. Zackert, V. C. Daniel, K.
F. Badr, I. A. Blair, and L. J. Roberts 2nd. Free radical-induced generation of isoprostanes in
vivo. Evidence for the formation of D-ring and E-ring isoprostanes. J Biol Chem 269: 4317-26,
1994.
23. Neubauer, S., S. Zimmermann, A. Hirsch, F. Pulzer, R. Tian, W. Bauer, B. Bauer, and G. Ertl.
Effects of endothelin-1 in the isolated heart in ischemia/reperfusion and hypoxia/reoxygenation
injury. J Mol Cell Cardiol 23: 1397-409, 1991.
24. Ogletree, M. L., D. N. Harris, R. Greenberg, M. F. Haslanger, and M. Nakane. Pharmacological
actions of SQ 29,548, a novel selective thromboxane antagonist. J Pharmacol Exp Ther 234:

29
435-41, 1985.
25. Pearl, J. M., D. P. Nelson, C. J. Wagner, J. P. Lombardi, and J. Y. Duffy. Endothelin receptor
blockade reduces ventricular dysfunction and injury after reoxygenation. Ann Thorac Surg 72:
565-70, 2001.
26. Przyklenk, K. and R. A. Kloner. Is "stunned myocardium" a protective mechanism? Effect of
acute recruitment and acute beta-blockade on recovery of contractile function and high-energy
phosphate stores at 1 day post-reperfusion. Am Heart J 118: 480-9, 1989.
27. Spinale, F. G., J. D. Walker, R. Mukherjee, J. P. Iannini, A. T. Keever, and K. P. Gallagher.
Concomitant endothelin receptor subtype-A blockade during the progression of pacing-induced
congestive heart failure in rabbits. Beneficial effects on left ventricular and myocyte function.
Circulation 95: 1918-29, 1997.
28. Taber, D. F., J. D. Morrow, and L. J. Roberts 2nd. A nomenclature system for the isoprostanes.
Prostaglandins 53: 63-7, 1997.
29. Takahashi, K., T. M. Nammour, M. Fukunaga, J. Ebert, J. D. Morrow, L. J. Roberts 2nd, R. L.
Hoover, and K. F. Badr. Glomerular actions of a free radical-generated novel prostaglandin, 8-
epi-prostaglandin F2 alpha, in the rat. Evidence for interaction with thromboxane A2 receptors.
J Clin Invest 90: 136-41, 1992.
30. Ulus, A. T., A. Aksoyek, M. Ozkan, S. F. Katircioglu, and S. Basu. Cardiopulmonary bypass as
a cause of free radical-induced oxidative stress and enhanced blood-borne isoprostanes in
humans. Free Radic Biol Med 34: 911-7, 2003.
31. Verma, S., A. Maitland, R. D. Weisel, P. W. Fedak, S. H. Li, D. A. Mickle, R. K. Li, L. Ko, and
V. Rao. Increased endothelin-1 production in diabetic patients after cardioplegic arrest and
reperfusion impairs coronary vascular reactivity: reversal by means of endothelin antagonism. J
30
Thorac Cardiovasc Surg 123: 1114-9, 2002.
32. Wang, Y. and D. H. Wang. Prevention of endothelin-1-induced increases in blood pressure: role
of endogenous CGRP. Am J Physiol Heart Circ Physiol 287: H1868-74, 2004.
33. Xia, Z., D. V. Godin, and D. M. Ansley. Propofol enhances ischemic tolerance of middle-aged
rat hearts: effects on 15-F(2t)-isoprostane formation and tissue antioxidant capacity. Cardiovasc
Res 59: 113-21, 2003.
34. Xia, Z., D. V. Godin, T. K. Chang, and D. M. Ansley. Dose-dependent protection of cardiac
function by propofol during ischemia and early reperfusion in rats: effects on 15-F2t-isoprostane
formation. Can J Physiol Pharmacol 81: 14-21, 2003.
35. Xia, Z., J. Gu, D. M. Ansley, F. Xia, and J. Yu. Antioxidant therapy with Salvia miltiorrhiza
decreases plasma endothelin-1 and thromboxane B2 after cardiopulmonary bypass in patients
with congenital heart disease. J Thorac Cardiovasc Surg 126: 1404-10, 2003.
36. Xia, Z., K. H. Kuo, J. H. McNeill, and D. M. Ansley. Endothelin A and B receptor antagonist
bosentan reduces postischemic myocardial injury in the rat: critical timing of administration.
Can J Physiol Pharmacol 83: 259-66, 2005.
37. Xiao, C. Y., A. Hara, K. Yuhki, T. Fujino, H. Ma, Y. Okada, O. Takahata, T. Yamada, T.
Murata, S. Narumiya, and F. Ushikubi. Roles of prostaglandin I(2) and thromboxane A(2) in
cardiac ischemia-reperfusion injury: a study using mice lacking their respective receptors.
Circulation 104: 2210-5, 2001.
38. Zaugg, C. E., P. Zhu, D. Simper, T. F. Luscher, P. R. Allegrini, and P. T. Buser. Differential
effects of endothelin-1 on normal and postischemic reperfused myocardium. J Cardiovasc
Pharmacol 22 Suppl 8: S367-70, 1993.
Related Documents











