Tri- and Bi-modality Therapy for N2(+) NSCLC Yong Chan Ahn, MD/PhD Dept. of Radiation Oncology Samsung Medical Center, Sungkyunkwan University School of Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Tri- and Bi-modality Therapy
for N2(+) NSCLC
Yong Chan Ahn, MD/PhD Dept. of Radiation Oncology
Samsung Medical Center, Sungkyunkwan University School of Medicine

Modalities in Treating Cancer
• Loco-regional:
– Surgery
– Radiation therapy
• Systemic:
– Chemotherapy
– Immunotherapy


Radiation and Surgery
Radiation usually fails in tumor center, and
rarely doses at periphery
Surgery usually fails at periphery because of
microscopic tumor cells left behind
Less radical surgery + RT
Organ and function preservation
Improved quality of life

Radiation and Chemotherapy
Synergy/sensitizer/potentiator: drugs directly
modifying radiation survival curve
Hypoxic cell sensitizer: drugs specifically
affecting tumor response
Decreased toxicity: drugs with independent
action or additivity
Theoretic Rationales of Combined Modality
Spatial cooperation
Toxicity independence
Reduction of toxicity
Enhanced tumor response
Prevention of emergence of resistant clones

Treatment Selection Factors
Treatment-related factors
Tumor-related factors
Patient-related factors
Physician-related factors
知彼知己, 百戰百勝
Knowing oneself and one's opponent,
invincibility!


Management of N2(+) NSCLC

N2 disease
• N2 disease is a very heterogenous, and at the
same time, important prognostic factor in
NSCLC.
– Remarkable improvements in diagnosis of N2 disease
(CT, FDG PET-CT, mediastinoscopy, video-assisted
thoracoscopy, and EBUS)
– A few different ways of classifying N2 disease
(clinical vs surgical, minimal vs bulky etc…).
• Still there is no single right answer in treating N2
disease.

Backgrounds

What do they say on role of surgery?

Van Meerbeeck et al (EORTC), JNCI, 2007
Van Meerbeeck et al (EORTC), JNCI, 2007

Response rate to CDDP-based
Ind CTx = 61%
Van Meerbeeck et al (EORTC), JNCI, 2007

Van Meerbeeck et al (EORTC), JNCI, 2007

Resection vs RT after Ind CTx (EORTC)
• In pathologic N2(+) NSCLC and response to Ind
CTx, surgical resection did not improve OS or
PFS compared with RT.
• RT should be considered preferred locoregional
Tx in view of low morbidity and mortality.
• Lobectomy, pN down-staging, R0 resection were
associated with better outcomes!
Van Meerbeeck et al (EORTC), JNCI, 2007
Albain et al (NCI), Lancet, 2009
Albain et al (NCI), Lancet, 2009

45 Gy 61 Gy
Albain et al (NCI), Lancet, 2009

45 Gy 61 Gy
Albain et al (NCI), Lancet, 2009
RT compliance to protocol:
193 (96%) in Group 1 vs 154 (79%) in Group 2 (p<0.0001)

PFS
CT/RT/S
(N=202)
CT/RT
(N=194)
Median PFS 12.8 mo
(5.3~42.2)
10.5 mo
(4.8~20.6)
HR=0.77
(0.62~0.96)
Dead of progression 159 (79%) 172 (89%) p=0.008
Dead PF 36 (18%) 19 (10%) p=0.02
PF at 5 years 32 (22%) 13 (11%) P=0.017
1st failure site CT/RT/S CT/RT
Local only 21 (10%) 43 (22%)
Primary only 5 (2%) 28 (14%)
N1-3 only 14 (7%) 6 (3%)
Both 2 (1%) 9 (5%)
Brain only 12 (11%) 29 (15%)
Other distant sites 75 (37%) 81 (42%) Albain et al (NCI), Lancet, 2009

OS
CT/RT/S
(N=202)
CT/RT
(N=194)
Median OS 23.6 mo
(9.0~)
22.2 mo
(9.7~52.7)
HR=0.87
(0.70~1.10)
Dead 145 (72%) 155 (80%)
Alive at 5 years 37 (27%) 24 (20%) OR=0.63
(0.36~1.10)
Albain et al (NCI), Lancet, 2009

OS matched lobectomy candidates (N=90) OS matched pneumonectomy candidates (N=51)
CT/RT/S CT/RT
Median survival 33.6 mo 21.7 mo p=0.002
Alive at 5 years 21 (36%) 10 (18%)
CT/RT/S CT/RT
Median survival 18.9 mo 29.4 mo
Alive at 3 years 17 (36%) 22 (45%)
Alive at 5 years 7 (22%) 10 (24%)
Albain et al (NCI), Lancet, 2009

RT + CTx +/- Surgery (NCT-2550)
• CRT with or without resection (preferably
lobectomy) are options for stage IIIA(N2)
NSCLC.
– Similar OS, improved PFS in trimodality arm.
– Better OS by trimodality in lobectomy candidates, but
not in pneumonectomy candidates.
Albain et al (NCI), Lancet, 2009

Comparison ERTOC NCI
Study
- period
- No. of pts.
1994-2002
582
1994-2001
429
Scheme ind. CT RT
ind. CT S
def. CCRT
ind. CCRT S
CTx CDDP (80 mg/m2)
Gemzar or Taxane
CDDP (50 mg/m2)
Etoposide (50 mg/m2)
TRT 60-62.5 Gy/30-32 Fx’s
none
61 Gy/33 Fx’s
45 Gy/25 Fx’s
Surgery
- % pneumonectomy
- % R0 resection
- Tx-related death
47%
50%
2%
31%
71%
8%

Comparison
ERTOC NCI
C+RT vs. C+S CRT vs. CRT+S
OS
- median (mo)
- 5-year
17.5 vs 16.4
14.0% vs 15.7%
22.2 vs 23.6
20.0% vs 27.0%
PFS
- median (mo)
- 2-/5-year
11.3 vs 9.0
(2-year) 24.0% vs 27.0%
10.5 < 12.8
(5-year) 11.0% < 22.0%
Site of 1st relapse
- Locoregional
- Distant
55% < 32%
39% vs 61%
22% < 10%
57% vs 48%
Summary RT is safer than surgery Better OS by trimodality
in lobectomy candidates

Based on the same data, different interpretations are possible!
What have we experienced at SMC?

Therapeutic Decision at SMC
• Work-up’s:
– Standard: Chest CT, PET-CT, PFT, Bronchoscopy…
– Optional: Brain MR (especially if AD)
– Mediastinoscopy and/or EBUS for all potential surgical candidates
• Staging:
– Localized vs loco-regionally advanced vs metastatic
– Operable vs inoperable
– Resectable vs potentially resectable vs unresectable

Tx Scheme at SMC (since mid-90’s)
T
T1 T2 T3 T4
N
N0 IA-IIB
1. Op ± RT/CTx/CRT
2. Def. RT IIIB
1. Def. CCRT
2. RT alone
3. Seq CTx + RT
N1 IIIA (T3N1)
N2
IIIA
1. Preop. CCRT + Op ± RT
2. Def. CCRT
3. RT alone
N3

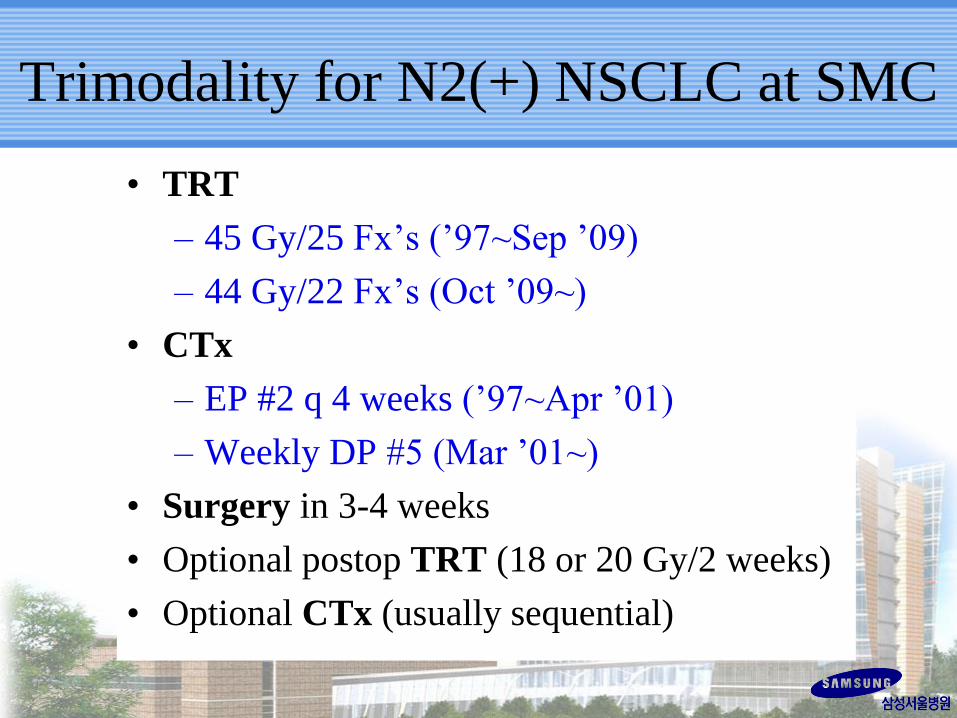
Trimodality for N2(+) NSCLC at SMC
• TRT
– 45 Gy/25 Fx’s (’97~Sep ’09)
– 44 Gy/22 Fx’s (Oct ’09~)
• CTx
– EP #2 q 4 weeks (’97~Apr ’01)
– Weekly DP #5 (Mar ’01~)
• Surgery in 3-4 weeks
• Optional postop TRT (18 or 20 Gy/2 weeks)
• Optional CTx (usually sequential)


Ann Surg Oncol, 2014

Patients (May ’97~Aug ’11)

Patients’ Characteristics (N=355)

Preop Tx
TRT 45 Gy in 25 Fx’s (1997’ ~ Oct 2009’)
44 Gy in 22 Fx’s (Sep 2009’ ~ )
258 (72.7%)
97 (27.3%)
CTx EP q 3 weeks (1997’ ~ Jul 2001’)
Weekly DP (Jul 2001’ ~ )
38 (10.7%)
317 (89.3%)
Surgery
Sublobar resection
(Bi-)Lobectomy
Pneumonectomy
2 ( 0.6%)
301 (84.8%)
52 (14.6%)
Postop Tx
TRT No or incomplete
Yes (18-20 Gy in 10 Fx’s)
144 (40.6%)
211 (59.4%)
CTx No
Yes
271 (76.3%)
84 (23.7%)
Treatment Characteristics (N=355)

Pathologic Findings (N=355)
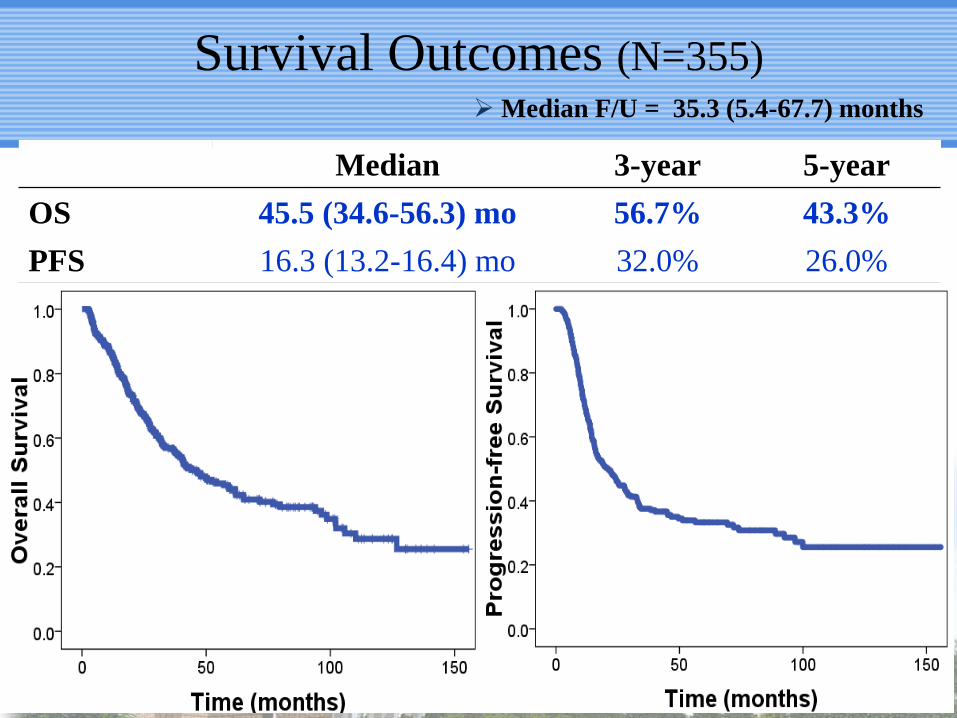
Median 3-year 5-year
OS 45.5 (34.6-56.3) mo 56.7% 43.3%
PFS 16.3 (13.2-16.4) mo 32.0% 26.0%
Survival Outcomes (N=355) Median F/U = 35.3 (5.4-67.7) months

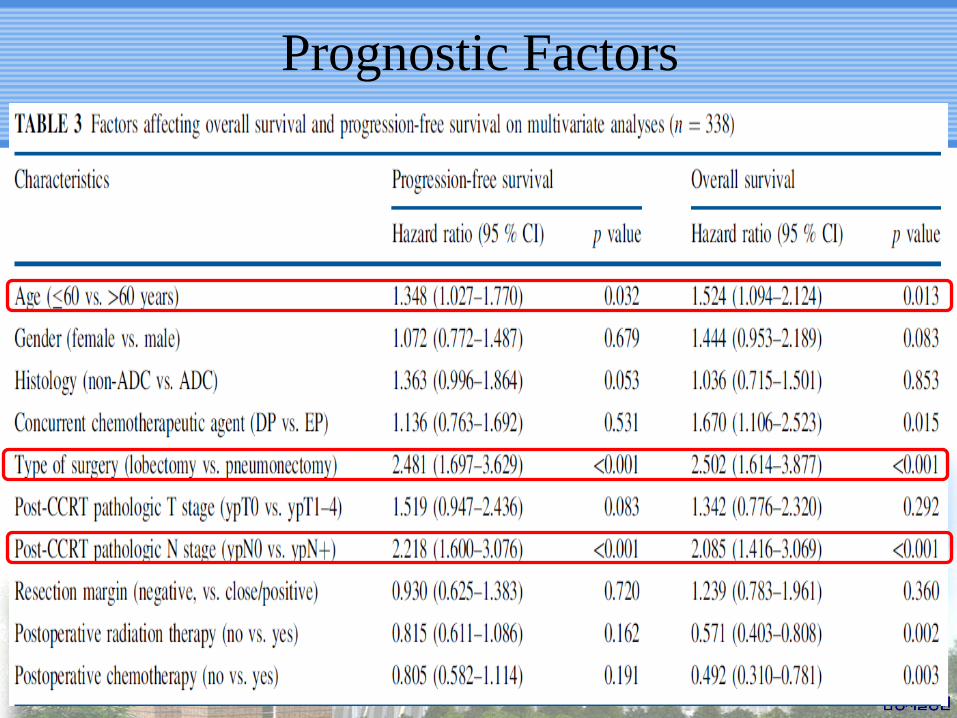
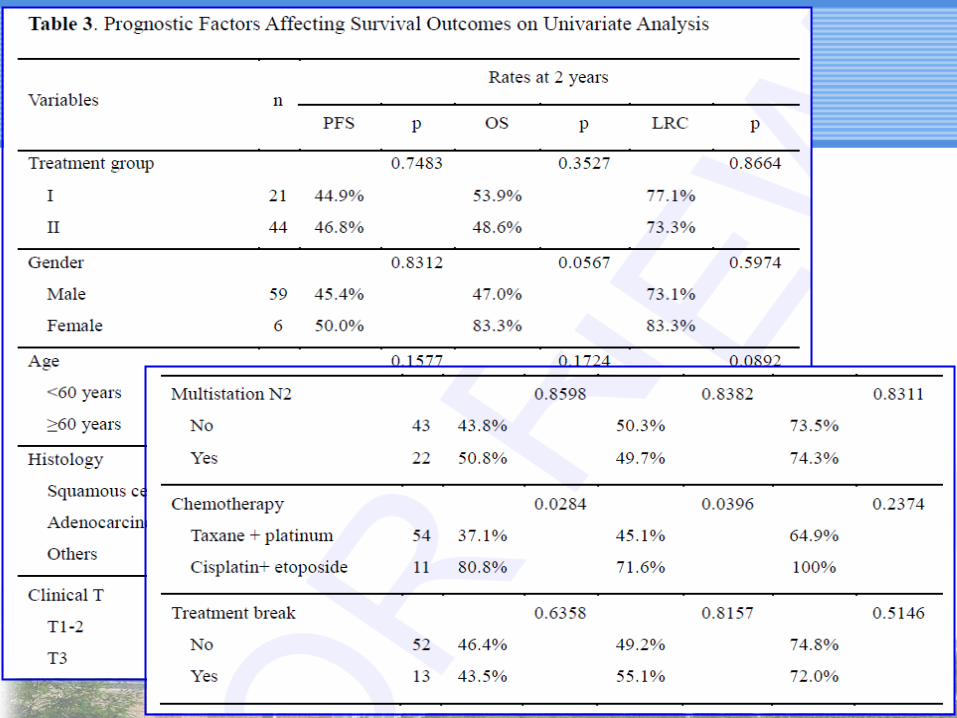
Prognostic Factors

Summary • Current study strongly supports that trimodality Tx can
provide remarkable survival benefit in IIIA-N2 NSCLC
patients.
• Initial bulk and extent of N2 node involvement do not
influence prognosis.
• Sterilization of mediastinal LN remains the most important
factor for prognosis.
• Well-designed prospective clinical trials may be required.
SWOG 8805 RTOG 0229 INT 0139 SMC
Median 13 months 26.6 months 23.6 months 45.5 months
OS 27% (3-Yr) 54% (2-Yr) 27% (5-Yr) 43.3% (5-Yr)

Conclusions
• There definitely is positive role of surgical
resection following CCRT in cN2 disease.
• Benefit of surgery is summarized as improved
loco-regional control at no excess morbidity.
• Without loco-regional control,
“real cure” cannot be
expected, and surgery should
remain essential under multi-
disciplinary spirit.

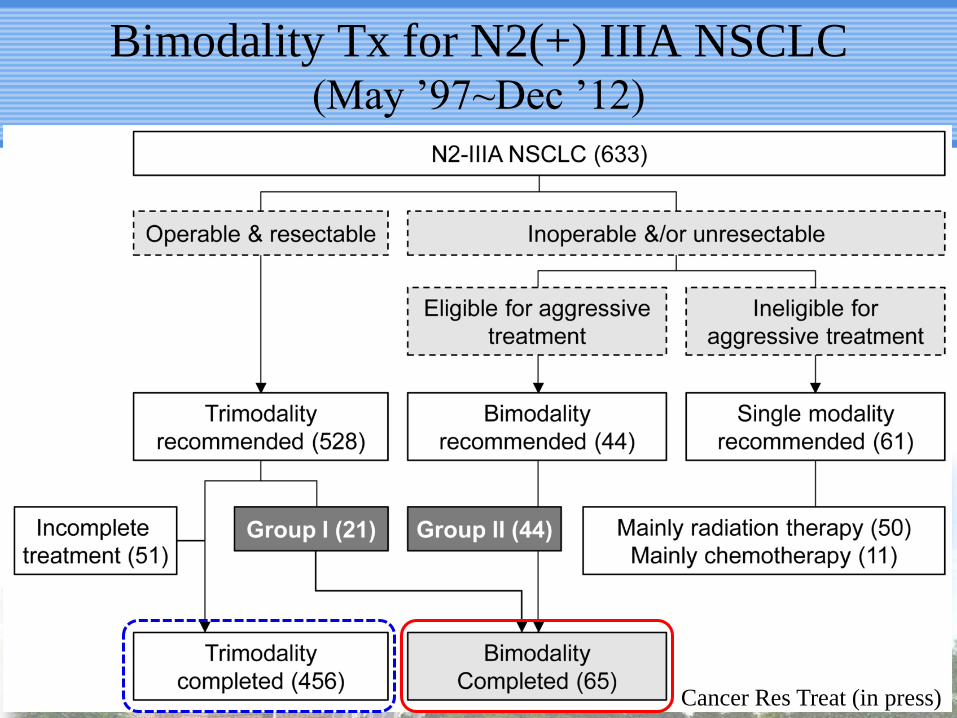
Bimodality Tx for N2(+) IIIA NSCLC (May ’97~Dec ’12)
Cancer Res Treat (in press)
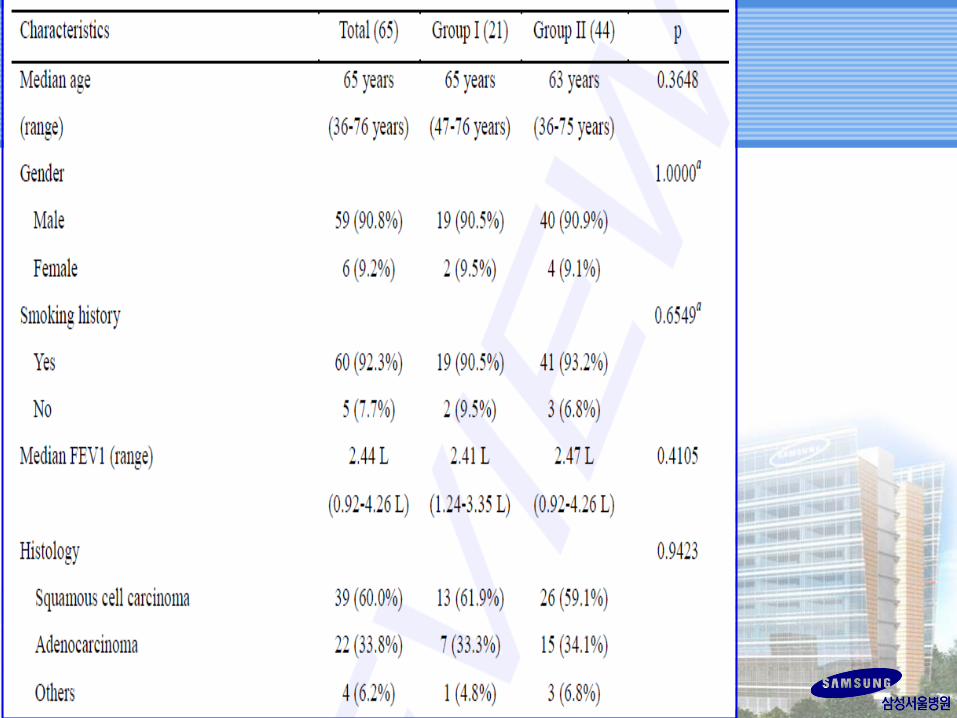


• Thoracic RT:
– Median 66 Gy in 33 fractions in all
– Median 72 Gy in 13 patients in Group I who had
median 36 days’ Tx break d/t delayed decision on
resectability
• Chemotherapy:
– Weekly Taxane + Platinum in 54 (83.1%)
– Cisplatin + etoposide q 3 weeks in 11 (16.9%)
• Median F/U = 18.8 (1.6~173.1) months
Treatment




• Phase III trial by NCI (Lancet 2009):
– CCRT+Surgery vs. Definitive CCRT
– Survival benefit was observed following lobectomy
• Lobectomy is better than pneumonectomy following CCRT
– National Cancer Database (J Thoracic Oncol 2013)
– SMC trimodality experience (Ann Surg Oncol 2014)
• Bimodality therapy should be primary treatment in
unresectable lesion or probable pneumonectomy
candidates.
Discussion/Conclusion

’97 may~’11 Nov ’97 may~’12 Dec
Pt number 355 65
OS @ 5Y (Med) 43.3% (45.4 M) 33.3% (28.6 M)
Heavily biased by “selection”

• Thoracic RT concurrent with weekly TP chemo is
better than 3-weekly EP.
• Surgery, if in retrospective nature, has played a key
role in terms of local control and survival at SMC.
• Surgery (<pneumonectomy) is an essential
component for “survival with cure”.
• ypN down-staging following CCRT has proved a
key prognostic factor.
Summary (or Bias @ SMC)?


Evidence-based Pride vs Observational Prejudice
• What was known to be “true” sometimes turns
out to be “false”.
• “Religious belief” might be simple bias if not
based on “scientific evidence”.
• Randomized controlled trial is necessary to
discriminate “prejudice” from “pride”!

Evidence-based Medicine?
BMJ 2003

Natural history of gravitational challenge
• Use of parachutes is associated with morbidity
and mortality.
• Survival has been reported after gravitation
challenges of more than 10,000 meters.
• Are studies required to calculate balance of
risks and benefits of parachute use?

Parachute and healthy cohort effect
• Possibility of selection and reporting bias:
– Jumping from aircraft without parachute
likely to have psychiatric morbidity
– Using parachutes less likely to have
psychiatric morbidity
Apparent protective effect may be “healthy
cohort” effect?.
• It is unclear whether results of industry
sponsored trials are reliable.


• In addition to quantitative parameters (disease
control, survival, Tx duration, cost…), qualitative
impacts following Tx need to be evaluated.
• Development of practical and optimal mediastinal
re-staging tool following CCRT would be desired
to select out ideal surgical candidates.
• Intimate multidisciplinary collaboration is
important.
Future Directions

They are all different! Which weapon do
you need babies?
Give me a knife!
I will irradiate!
I will wait/see!
I need toxin!

Factors affecting treatment selection
Modality-
related
Disease-
related
Patient-
related
Physician-
related

Multidisciplinary
spirit!

Lung Cancer Center @ SMC

Thank you for attention!
Related Documents











