HIV Treatment Update Todd Correll, PharmD, BCPS Clinical Pharmacy Specialist, Infectious Diseases/HIV University of North Carolina Hospitals November 2006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HIV Treatment Update
Todd Correll, PharmD, BCPSClinical Pharmacy Specialist, Infectious Diseases/HIV
University of North Carolina HospitalsNovember 2006

Objectives
• Provide an update on DHHS HIV treatment naïve guidelines
• Discuss the currently approved antiretrovirals
• Describe treatment options for opportunistic infections

HIV Life Cycle
Illustration by David Klemm

Goals of Therapy & Strategies to Achieve Goals
Improvement of quality of life
Reduction of HIV-related morbidity and mortality
Restoration and/or preservation of immunologic function
Maximal and durable suppression of viral load
Selection of ARV regimen Preservation of future
treatment options Rational sequencing of
therapy Maximizing adherence Use of resistance testing
in selected clinical settings
StrategiesStrategiesGoalsGoals

Indications for Antiretroviral Initiation
Clinical Category
CD4 cell count
HIV RNA
Recommendation
Symptomatic (AIDS)
Any value Any value TREAT
Asymptomatic AIDS
<200 cells/mm3
Any value TREAT
Asymptomatic 200 to 350 cells/mm3
Any value Offer treatment;
pros vs cons
Asymptomatic >350 cells/mm3
>100K c/mL
TREAT
Asymptomatic >350 cells/mm3
<100K
c/mL
Defer therapy

Antiretroviral Combinations Not Recommended as Initial Therapy
Reason for Avoidance Medication/Regimen
↑ rate of virologic failure • ddI + TDF + NNRTI
Inferior antiviral activity • Delavirdine• Unboosted SQV
↑ incidence of toxicities • d4T + ddI• RTV 600 mg Q12h
↑ pill burden/dosing frequency • APV (w/ or w/out RTV)• Unboosted IDV• NFV + SQV
Lack of treatment-naïve data • TPV• DNV• T-20

Antiretroviral Combinations Not Recommended Anytime
• Monotherapy– Except for the perinatal HIV transmission prevention
• Dual NRTI• 3 drug regimens not recommended
– ddI + TDF + NNRTI– ABC + TDF + 3TC– ddI + TDF + 3TC
• NNRTI-based regimens– Efavirenz in pregnancy → category D– Nevirapine initiation → ↑ risk of hepatotoxicity
• women with a CD4 count > 250 cells/mm3• men with a CD4 count > 400 cells/mm3
High rates of virologic failure

Antiretroviral Combinations Not Recommended Anytime
• NRTI backbone– ddI + d4T → toxicities– d4T + AZT → drug antagonism– FTC + 3TC → drug antagonism
• PI combinations– APV + FPV → FPV is the prodrug of APV– APV oral solution in children, pregnancy, renal/hepatic
failure– APV oral solution + RTC oral solution → propylene
glycol toxicity– ATV + IDV → ↑ risk of elevated total bilirubin

Antiretroviral Components in Initial Therapy: NNRTIs
ADVANTAGES• Less fat
maldistribution and dyslipidemia than in PI-based regimens
• PI options preserved for future use
DISADVANTAGES• Resistance - single
mutation• Cross-resistance
among NNRTIs• Rash; hepatotoxicity• Potential drug
interactions (CYP450)

Antiretroviral Components in Initial Therapy: PIs
ADVANTAGES• Longest prospective
data• NNRTI options
preserved for future use
DISADVANTAGES• Metabolic complications
(fat maldistribution, dyslipidemia, insulin resistance)
• Greater potential for drug interactions (CYP450), especially with ritonavir

ART Options
NRTIs (Nucleoside OR Nucleotide Reverse Transcriptase Inhibitors, aka “Nukes”)
NNRTIs (Non-Nucleoside Reverse Transcriptase Inhibitors, aka “Non-Nukes”)
PIs (Protease Inhibitors)
Fusion (or Entry Inhibitors)
ART agents in additional classes currently in development
-Integrase Inhibitors-CCR5 Antagonists-CXCR4 Antagonists

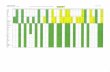
NNRTI
’’8787 ’’9191 ’’9292 ’’9494 ’’9595 ’’9696 ’’9797 ’’9898 ’’9999 ‘‘0000’’8888 ’’8989 ’’9090
NRTINRTI
PIPI
Approved Antiretrovirals
NorvirNorvir
InviraseInvirase
CrixivanCrixivan
FortovaseFortovase
KaletraKaletraViraceptViracept
ZiagenZiagen
CombivirCombivir
VidexVidex
HividHivid
ZeritZerit
EpivirEpivir
TrizivirTrizivir
Rescriptor
SustivaViramune
’’0101
VireadViread
EmtrivaEmtriva
FuzeonFuzeon
ReyatazReyataz
‘‘0202 ‘‘0303’’9393
AgeneraseAgenerase
LexivaLexiva
TruvadaTruvada
EpzicomEpzicom
FIFI
AZTAZT
AptivusAptivus
PrezistaPrezista
AtriplaAtripla

Mechanism of Action
Nucleoside analogs (like AZT below) are activated after being phosphorylated so that they can be incorporated into the viral DNA strand by reverse transcriptase.
Since TDF is a nucleotide, it does NOT have to be phosphorylated prior to being incorporated into the growing viral DNA strand.
After incorporation of
the NRTI, viral DNA
synthesis will be
terminated.

FDA Black Box WarningsNRTI Warning
AZT■ Lactic acidosis and steatosis.■ Hematologic toxicities including neutropenia & anemia.■ Myopathy
ddI■ Fatal and nonfatal pancreatitis; hold ddI if pancreatitis suspected; D/C if confirmed.■ Lactic acidosis and steatosis.■ Fatal lactic acidosis in pregnant women with ddI + d4T.
d4T■ Lactic acidosis and steatosis.■ Fatal lactic acidosis in pregnant women with ddI + d4T.■ Fatal and nonfatal pancreatitis with ddI + d4T+ HU.
3TC ■ Lactic acidosis and steatosis.■ Acute HBV exacerbation upon discontinuation.
ABC
■ Fatal hypersensitivity reactions reported.■ S/S are fever, rash, fatigue, and GI and respiratory Sx. If suspected, ABC should be D/C and should NOT be restarted.■ Lactic acidosis and steatosis.
TDF ■ Lactic acidosis and steatosis.• Acute HBV exacerbation upon discontinuation.
FTC ■ Lactic acidosis and steatosis.■ Acute HBV exacerbation upon discontinuation.

NRTIsDrug Standard
Dose*Dosage forms
Combos Common Side Effects
Zidovudine (ZDV/AZT) Retrovir
300mg bid* 300mg tab, 100mg cap, iv oral soln
Combivir, Trizivir
Fatigue, malaise, HA, myalgia, anemia, GI
Lamivudine (3TC) Epivir
150mg bid* or 300mg qd
150, 300mg tab, oral soln
Combivir, Epzicom, Trizivir
Well tolerated
Emtricitabine(FTC) Emtriva
200mg qd* 200mg cap Truvada,Atripla
Well tolerated
Didanosine (ddI) Videx
400mg EC qd*†
125,200,250,400mg cap, pwdr for soln
Pancreatitis, peripheral neuropathy, LA/HS
*dose reduce for renal dysfunction† dose reduce for weight <60 kg

NRTIs
Drug Standard Dose*
Dosage forms
Combos Common Side Effects
Stavudine (d4T) Zerit
40mg bid*† 15,20,30,40 mg cap,oral soln
Peripheral neuropathy, Dylipidemia, LipodystrophyPancreatitis, LA/HS
Abacavir (ABC) Ziagen
300mg bid, 600mg qd
300mg tabs, oral soln
Trizivir, Epzicom
hypersensitivity
Tenofovir(TDF) Viread
300mg qd* 300mg tabs Truvada,Atripla
Few SEs, potential renal dysfxn.
* dose reduce for renal dysfunction† dose reduce for weight <60 kg

NRTI Combination Products
Drug Standard Dose Dosage Form
Combivir(AZT + 3TC)
1 tablet BID* 300/150 mg tablet
Trizivir (AZT + 3TC + ABC)
1 tablet BID* 300/150/300 mg tablet
Epzicom(ABC + 3TC)
1 tablet QD* 600/300 mg tablet
Truvada(TDF + FTC)
1 tablet QD* 300/200 mg tablet
*Use of individual components instead of combination products may necessary in patients with renal dysfunction.

Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) Inhibit reverse transcriptase by a mechanism that is
different from that of NRTIs nevirapine (NVP)
delavirdine (DLV)
efavirenz (EFV)
Use caution when coadministering PIs (modify dose and closely monitor in order to minimize P450 interactions and complications)
X
I can stop that HIV reverse transcriptase!
RT

Mechanism of Action
These agents directly bind to reverse transcriptase to inhibit its making DNA from the HIV’s RNA.
NEVER use NNRTIs as monotherapy in order to ↓
development
of rapid
resistance!
RT
X

FDA Black Box Warnings
NNRTI Warning
NVP
■ Severe, life-threatening hepatotoxicity including fulminant and cholestatic hepatitis, hepatic necrosis & hepatic failure.■ Severe, life-threatening, and even fatal skin reactions. Monitor intensely during the first 12 wk to detect hepatotoxicity and skin reactions.
DLV ■ None
EFV ■ None
http://aidsinfo.nih.gov/guidelines/adult/AA_032304.pdf

NNRTIs
Drug Standard Dose
Dosage forms
Combos Common AEs
Delavirdine (DLV) Rescriptor
400 mg tid 100mg tab, 200mg cap
Suboptimal data on efficacy; potent CYP3A inhibitor
rash
Nevirapine (NVP) Viramune
200 mg qd x 14 d then200 mg bid
200mg tabs, Oral susp
CYP3A inducer, auto inducer
rash, hepatotoxicity
Efavirenz (EFV) Sustiva
600 mg qhs 50, 100, 200mg cap, 600mg tab
CYP3A inducer, potency similar to PIs
Vivid dreams, drowsiness, CNS SEs, rash (including Stevens Johnson)

Atripla
• Triple combination tablet containing:– Emtricitabine 200 mg – Tenofovir 300 mg– Efavirenz 600 mg
• Bilayer tablet– Do not crush– Do not cut in half
• First “complete regimen” tablet• Dose: 1 tablet at bedtime

Atripla Bioequivalence
TFV
0 12 24 36 48 60 725
50
500
1000
TestReference
Time (hrs)
TF
V P
lasm
a C
on
cen
trat
ion
(ng
/mL
)
FTC
0 24 48 72 961
10
100
1000
5000
Test
Reference
Time (hrs)
FT
C P
lasm
a C
on
cen
trat
ion
(ng
/mL
)
EFV
0 72 144 216 288 360 432 50410
100
1000
5000
Test
Reference
Time (hrs)
EF
V P
las
ma
Co
nc
en
tra
tio
n(n
g/m
L)

Protease Inhibitors:Mechanism of Action
Protease cleaves HIV precursor proteins (gag/pol polyproteins) into active proteins that are needed to assemble a new, mature HIV virus. This enables new viral particles to “break off” from infected host cells.
PIs prevent this cleavage and inhibit the assembly of new HIV viruses within infected host cells.
PI
HIV-1 Protease
XHIV

FDA Black Box WarningsPI Warning
SQV ■ None
RTV ■ Co-administration with certain medications may cause serious or life-threatening events.
IDV ■ None
NFV ■ None
APV ■ Large amount of the excipient propylene glycol in oral soln (contraindicated in pregnant women, pts< 4y, pts with renal or hepatic failure, and pts treated with disulfiram or metronidazole)
LPV ■ None
ATV ■ None
TPV ■ Reports of clinical hepatitis & liver decompensation including some fatalities have occurred; risk of intracranial bleeding
DNV None
FOS ■ None
http://aidsinfo.nih.gov/guidelines/adult/AA_032304.pdf

Protease InhibitorsDrug Dose Pill burden Dosing info
Saquinavir (Invirase)
1000 mg + RTV 100 mg BID
2(500mg) caps/1(100mg cap) BID
Take with food
Nelfinavir (Viracept)
1250 mg BID750 mg TID
2(625mg) tabs BID3(250mg) tabs TID
Take with food
Indinavir(Crixivan)
800mg + RTV 100 BID
800 mg TID
2 (400mg) caps +1(100mg cap) BID
2 (400 mg) caps TID
Drink 7-8 glasses of water per day
Fosamprenavir(Lexiva)
1400 mg BID1400 mg + RTV 200 QD
700 mg + RTV 100 mg BID
2 (700mg) tabs BID2 (700mg) tabs + 2 (100 mg) caps QD
1 (700mg) tabs + 1 (100 mg) caps BID
Take with food
Amprenavir (Agenerase)
600 mg + RTV 100 mg BID1200 mg + RTV 200 mg QD
Available as 50 mg capsules and liquid
Liquid contains propylene glycolAvoid concomitant with ritonavir liquid

Protease Inhibitors
Drug Dose Pill burden Dosing info
Lopinavir/ritonavir (Kaletra)
400mg/100mg QD400mg/100mg BID
4 tabs QD2 tabs BID
Take with or without food
Atazanavir(Reyataz)
400mg QD
300mg + RTV 100mg QD
2 (200mg) QD
2 (150mg) + 1 (100mg) QD
Take with food; avoid PPI
Tipranavir(Aptivus)
500mg + RTV 200mg BID 2 (250mg) caps +2( 100mg cap) bid
Take with food
Darunavir(Prezista)
600mg + RTV 100mg BID 2 (300mg) tabs+ 1 (100 mg) caps BID
Take with food

Protease InhibitorsDrug Side
EffectsBioavailability/Protein Binding
Metabolizingenzymes
Saquinavir GI intolerance 4%/98% 3A substrate
Nelfinavir diarrhea 20-80%/99% P450 inhibitor/inducer/ substrate
Indinavir Nephrolithiasis; GI intolerance
30%/60% 3A substrate
Fosamprenavir GI symptoms, rash
Poor/90% 3A inducer/ substrate
Lopinavir/ritonavir GI symptoms, rash
Poor/99% 3A inhibitor/ substrate; 2D6 inhibitor
Atazanavir ↑bilirubinemia good/86% 3A and UGT1A1 inhibitor; 3A substrate
Darunavir N/V, rash, HA ----------- 3A inhibitor, 3A substrate
Tipranavir GI symptoms↑ LFTs, lipids,
rash
Unknown/99% 3A inhibitor/ substrate

Entry Inhibitors Fusion inhibitors [Fuzeon (enfuvirtide, T20)]
Attachment Inhibitors
Chemokine co-receptor antagonists
See Kilby and Eron, NEJM 2003;348:2228-38

Enfuvirtide (T-20) (Fuzeon)
FDA-approved fusion inhibitor; 36 AA peptide
Dose: 90 mg sc bid side effects:
injection site rxn (common); hypersensitivity reactions (uncommon); eosinophilia (10% >700; 2% >1400); ↑increased risk of pneumonia on phase III
studies

Enfuvirtide: Injection Site Reactions
• Painful• Erythematous• Nodular• Pruritic• Last for ~7 days• DO NOT REINJECT
SITE UNTIL NODULE DISAPPEARS!!!!

Common Opportunistic Infections
CD4 cell count Opportunistic Infection
< 500 cells/mm3 Tuberculosis
VZV
HSV
Recurrent bacterial infections
< 250 cells/mm3 Thrush
< 200 cells/mm3 PCP
< 100 cells/mm3 Toxoplasmosis gondii
< 50 cells/mm3 Cryptococcus meningitis
MAC
CMV

Pneumocystis jiroveci (PCP)
• Ubiquitous fungus• Historic mortality of 20-40% in HIV pt• Incidence has declined since HAART• Clinical Presentation
– DOE/SOB fulminate pneumonia– Fever– Nonproductive cough– Poor oxygenation status/respiratory acidosis

Pneumocystis jiroveci (PCP)Treatment of
ChoiceAlternative Discontinue
Primary Prophylaxis
Bactrim DS QD
Dapsone 100 mg QD
Atovaquone 750 mg BID
CD4 > 200 x 3 months
Secondary Prophylaxis
Bactrim DS QD
Dapsone 100 mg QD
Atovaquone 750 mg BID
CD4 > 200 x 3 months
Treatment Bactrim 15 mg/kg in divided doses
Moderate-severe
•Pentamidine 4 mg/kg IV QD
Mild-moderate
•Dapsone 50 mg + TMP 15 mg/kg in divided doses
•Primaquine 30 mg base + clindamycin 600 mg Q6h
Treat for 21 days followed by secondary prophylaxis
If PaO2 < 70 initiate prednisone 40 mg BID x 5 days; 40 mg QD x 5 days; 20 mg QD x 11 days

Mycobacterium Avium Complex
• Non-TB Mycobacterium spp• Occurs in highly immunocompromised patients• Clinical symptoms depend on organ system
involved– General fever, malaise, lymphadenoapthy– Pulmonary SOB, cough, DOE– GI colitis, abdominal pain– Bone anemia, bone marrow suppression

MACTreatment of
ChoiceAlternative Discontinue
Primary Prophylaxis
Azithromycin 1200 mg Q week
Clarithromycin 500 mg BID
CD4 count >100 cells/mm3
Secondary Prophylaxis
N/A N/A N/A
Treatment Clarithromycin 500 mg BID + ethambutol 20 mg/kg QD ± rifabutin 300 mg QD*
Fluoroquinolone
Amikacin
D/C therapy if a minimum of 12 months of MAC therapy, pt is asx and CD4 count > 100 cells/mm3 for at least 6 months
Rifabutin has drug interactions with PI; dose reductions may be necessary

Toxoplasmosis gondii
• Protozoa causing reactivation disease– 15% of adults are toxoplasmosis IgG positive– 90% of HIV-infected patients are IgG positive
• Clinically presented as an encephalitis with ring-enhancing lesions on CT/MRI– Seizures, altered MS, coma– Multiple lesions
• Often hard to clinically differentiate CNS lymphoma and toxoplasmosis

Toxoplasmosis gondiiTreatment of Choice Alternative Discontinue
Primary Prophylaxis
Bactrim DS QD •Dapsone 50 mg QD + pyrimethamine 50 mg Q week + leucovorin 25 mg Q week
•Atovaquone 1500 mg QD
CD4 >200 x 3 months
Secondary Prophylaxis
Bactrim DS QD •Dapsone 100 mg QD
•Atovaquone 750 mg BID
CD4 > 200 x 6 months
Treatment Pyrimethamine 75 mg QD + sulfadiazine
1-2 g Q6h + leucovorin 25 mg QD
(clindamycin 600 mg IV q6h may be used in sulfa allergic patients)
• Atovaquone 750 mg BID
• Atovaquone + Pyrimethamine 75 mg QD
+ leucovorin 25 mg QD
• Atovaquone + sulfadiazine 1-2 g Q6h
+ leucovorin 25 mg QD
Treatment for at least 6 weeks; rescan to determine CT/MRI improvement
Bactrim 10 mg/kg IV in divided doses in patients who cannot take PO formulations

Cryptococcus• Fungus- yeast• Commonly presents as meningitis or menigoencephalitis
– Seizures– Altered MS– HA, fever
• CSF results– High opening pressure– Lymphocyte predominance– Normal/slightly low glucose– Mild elevation of protein– Organism growth
• Cryptococcus titers

CryptococcusTreatment of
ChoiceAlternative Discontinue
Primary Prophylaxis
None None N/A
Secondary Prophylaxis
Fluconazole 200 mg CD4 > 100-200 x 6 months
Treatment Amphotericin B 0.7 mg/kg + flucytosine 100 mg/kg/d x 14 days
Fluconazole 400 mg QD x 6 weeks
Fluconazole 800 mg QD

6 Rules to Live By1. Per Gretchen- your job is not to screw these
patients up (she will hunt you down!)2. 2 ART is a bad idea; 1 ART is a REALLY bad
idea; Combination therapy is a GREAT IDEA3. The ID clinic note can help you4. Nexium (aka Purple crack) is WHACK
- SIGNIFICANT interaction with atazanavir
5. If Dr. Van der Horst is your attending, do not pass go, do not collect 200 dollars and just follow instructions
6. When in doubt, call 216-0626
Related Documents