Dept. of Pathology Dept. of Pathology Medical College Medical College Hunan Normal University Hunan Normal University ( ( 湖湖湖湖湖湖湖湖湖湖湖湖湖湖湖 湖湖湖湖湖湖湖湖湖湖湖湖湖湖湖 ) ) 1 Chapter 11 Chapter 11 Respiratory Failure Respiratory Failure 湖湖湖湖湖 () 湖湖湖湖湖 ()

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dept. of PathologyDept. of Pathology
Medical CollegeMedical College
Hunan Normal UniversityHunan Normal University
(( 湖南师范大学医学院病理学教研室湖南师范大学医学院病理学教研室 )) 1
Chapter 11Chapter 11
Respiratory FailureRespiratory Failure(呼吸衰竭)(呼吸衰竭)
22
Respiratory FailureRespiratory Failure
①① IntroductionIntroduction
②② Etiology and Classification Etiology and Classification
③③ Pathogenesis Pathogenesis
④④ Alterations of Metabolism and Alterations of Metabolism and
Function Function
⑤⑤ Pathophysiological Basis of Prevention Pathophysiological Basis of Prevention
and Treatmentand Treatment
Normal Process of Respiration
Air Lungs Blood Tissue
External respiration
Internal respiration
Transportation
Ventilation Diffusion Perfusion
3
Respiratory Failure: Definition
Respiratory failure (RF) is a syndrome in which the
respiratory system fails to adequately oxygenate the
venous blood w/ or w/o retention of carbon dioxide.
PaO2: 60 mmHg (when breathing room air)
PaCO2: Normal (type I) or 50 mmHg (type II)7

Running a race at 12,000 feet
Is This Respiratory Failure?
8

99
Respiratory FailureRespiratory Failure
①① IntroductionIntroduction
②② Etiology and Classification Etiology and Classification
③③ Pathogenesis Pathogenesis
④④ Alterations of Metabolism and Alterations of Metabolism and
Function Function
⑤⑤ Pathophysiological Basis of Prevention Pathophysiological Basis of Prevention
and Treatmentand Treatment
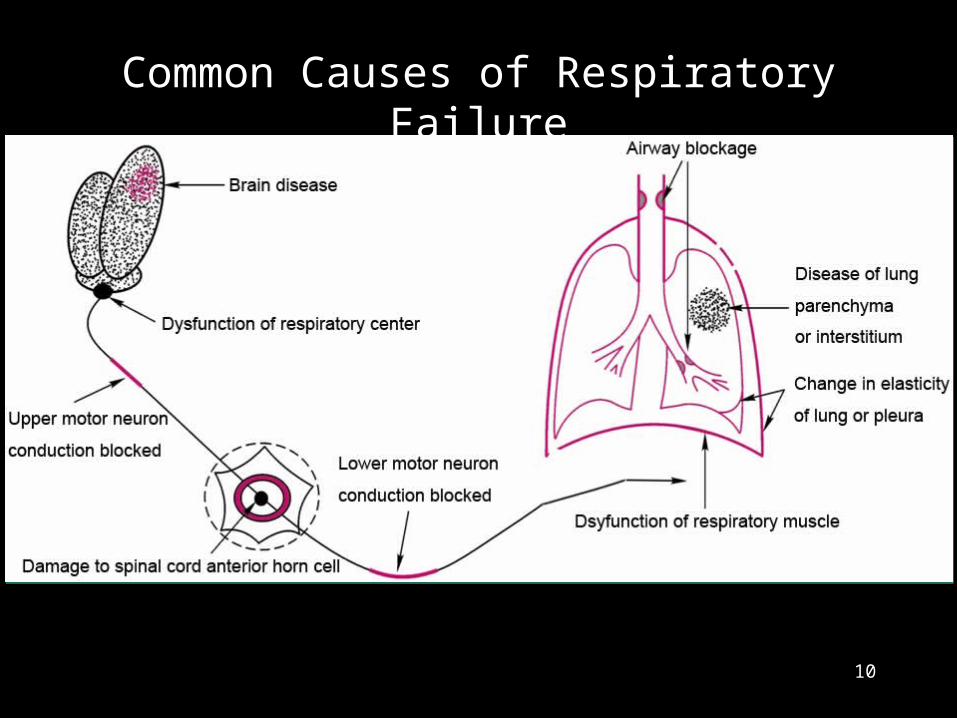
Common Causes of Respiratory Failure
10

EtiologyRespiratory pump damage
Brain disease (trauma or tumor)
Cephalitis
Pleural Effusion
Pneumothorax ( 气胸 )
Lung solid lesionPneumonia
Emphysema ( 肺气肿 )
Atelectasis ( 肺不张 )
Airway obstructionLaryngeal edema
Chronic bronchitis
Foreign body (or tumor)
Gas-exchanging problemPulmonary edema
11

(气胸 )(胸腔积液 ) Pleural Effusion Pneumothorax
Emphysema (肺气肿 ) 12
Classification According to blood gas changes
Type I:
PaO2 60 mmHg
Type II:
PaO2 60 mmHg + PaCO2 50 mmHg
According to pathogenesisVentilation
Gas-exchanging
According to durationAcute
Chronic
According to primary site
Central
Peripheral13

1414
Respiratory FailureRespiratory Failure
①① IntroductionIntroduction
②② Etiology and Classification Etiology and Classification
③③ Pathogenesis Pathogenesis
④④ Alterations of Metabolism and Alterations of Metabolism and
Function Function
⑤⑤ Pathophysiological Basis of Prevention Pathophysiological Basis of Prevention
and Treatmentand Treatment
Pathogenesis of Respiratory Failure
①① Dysfunction in ventilationDysfunction in ventilation
Restrictive hypoventilation Restrictive hypoventilation
Obstructive hypoventilationObstructive hypoventilation
②② Gas-exchange dysfunctionGas-exchange dysfunction
Diffusion impairmentDiffusion impairment
Ventilation/perfusion imbalanceVentilation/perfusion imbalance
Increase of anatomic shuntIncrease of anatomic shunt

①① Dysfunction in ventilationDysfunction in ventilation
Restrictive hypoventilation Restrictive hypoventilation
a)a) Dysfunction of respiratory pump activityDysfunction of respiratory pump activity
b)b) Decrease of lung compliance (solid lesions)Decrease of lung compliance (solid lesions)
Pathogenesis

Pathogenesis of Respiratory Failure
①① Dysfunction in ventilationDysfunction in ventilation
Restrictive hypoventilation Restrictive hypoventilation
Obstructive hypoventilationObstructive hypoventilation
②② Gas-exchange dysfunctionGas-exchange dysfunction
Diffusion impairmentDiffusion impairment
Ventilation/perfusion imbalanceVentilation/perfusion imbalance
Increase of anatomic shuntIncrease of anatomic shunt

Causes:
Asthma
Chronic Obstructive Pulmonary Disease (COPD)
(Chronic bronchitis)
Types:
Central airway obstruction
Peripheral airway obstruction
Obstructive Hypoventilation
22

Outside of chest
Inside of chest
Central Airway Obstruction
Trachea crotch
23
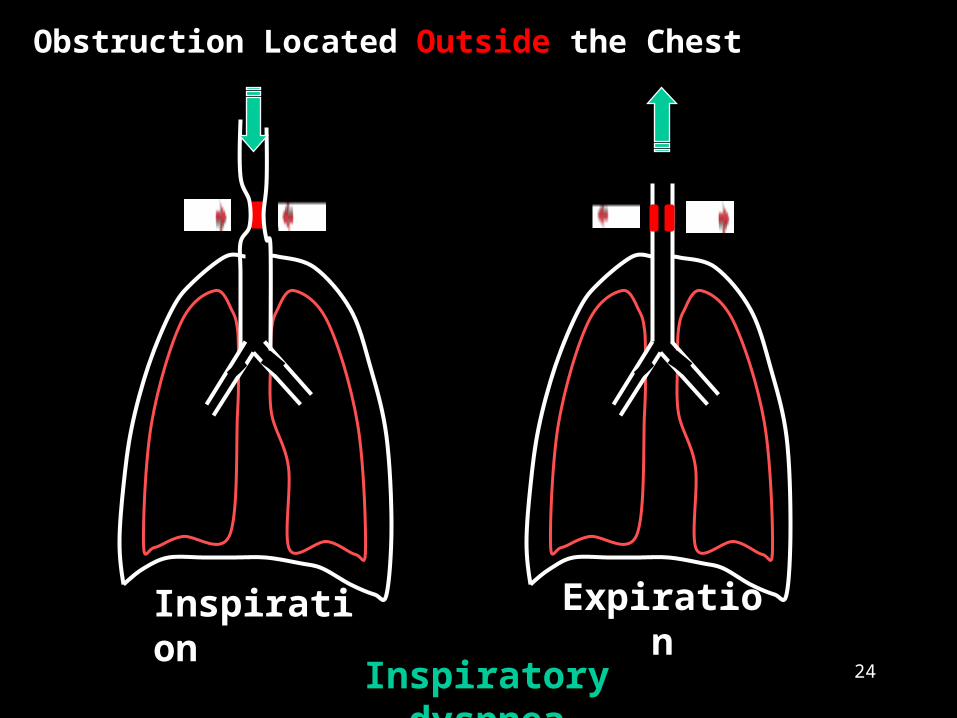
Inspiration
Obstruction Located Outside the Chest
Inspiratory dyspnea
Expiration
24

ExpirationInspiration
Expiratory dyspnea
Obstruction Located Inside the Chest
25

Alveolus
Inspiration
Bronchiole
Elastic tissue
Expiration
Expiratory dyspnea
Alveolus
Bronchiole
Elastic tissue
Peripheral airway obstruction
27

Pathogenesis of Respiratory Failure
①① Dysfunction in ventilationDysfunction in ventilation
Restrictive hypoventilation Restrictive hypoventilation
Obstructive hypoventilationObstructive hypoventilation
②② Gas-exchange dysfunctionGas-exchange dysfunction
Diffusion impairmentDiffusion impairment
Ventilation/perfusion imbalanceVentilation/perfusion imbalance
Increase of anatomic shuntIncrease of anatomic shunt
Pathogenesis
Diffusion Impairment Diffusion Impairment
a)a) Increase of thicknessIncrease of thickness
b)b) Decrease of gas-exchange areaDecrease of gas-exchange area
c)c) Shortening of diffusion timeShortening of diffusion time
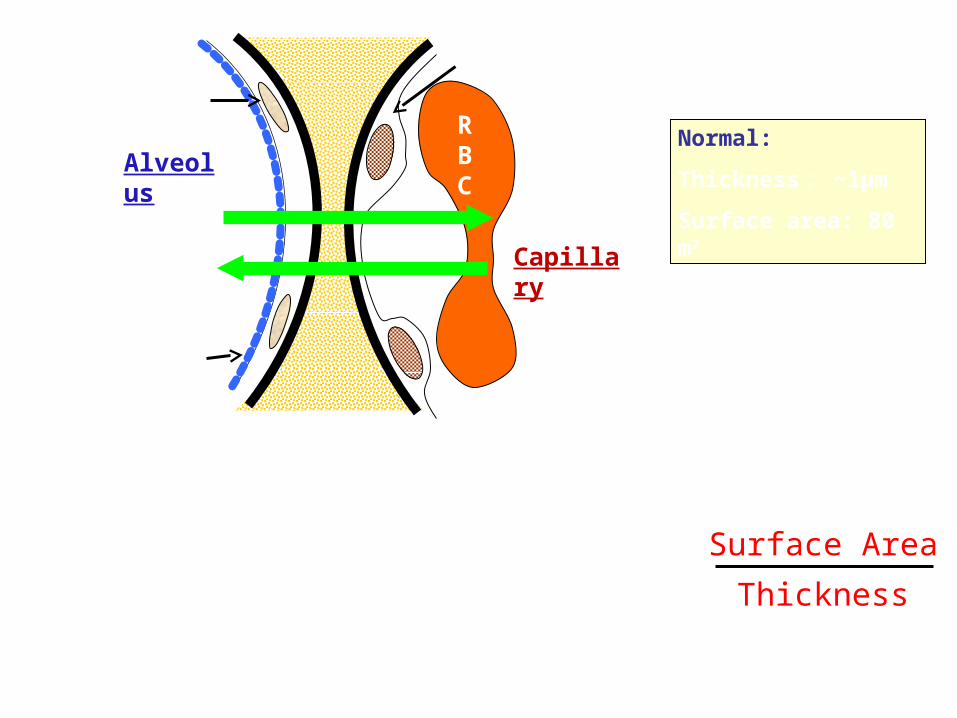
Structure of Alveolar-Capillary Membrane(Diffusion Membrane)
Diffusion Speed∝ Surface Area
Thickness
Alveolus
RBC
Capillary
Normal:
Thickness : ~1µm
Surface area: 80 m2
O2
CO2
Epithelium
Surfactant
Endothelium
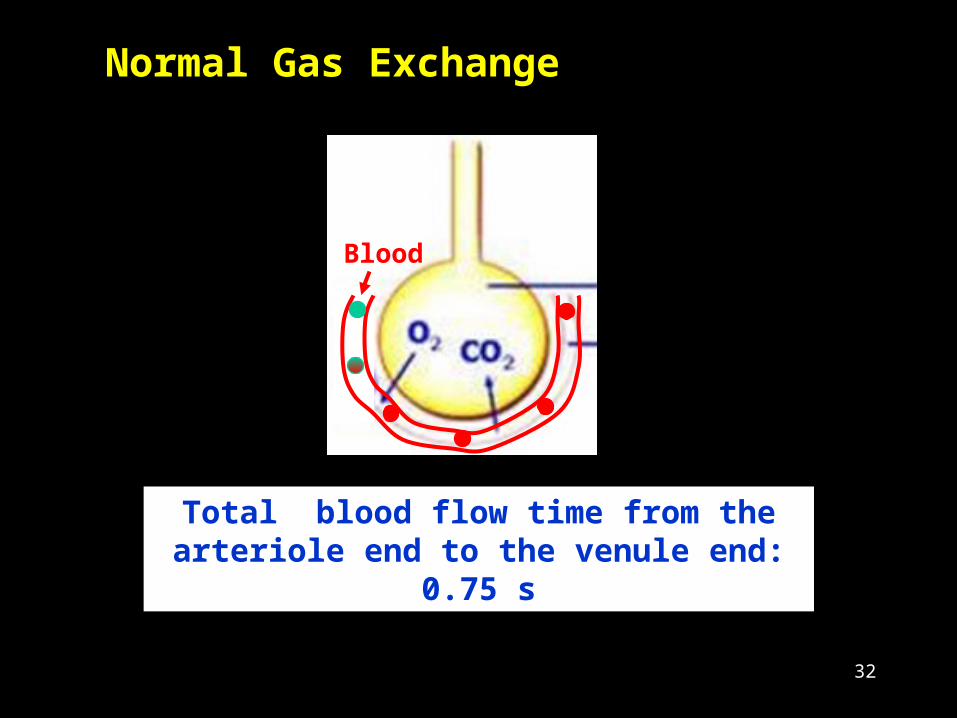
Normal Gas Exchange
Blood
Total blood flow time from the arteriole end to the venule end:
0.75 s
32

Prolonged Time for Gas Exchange
PO2
100
80
60
40
20
0s 0.25s 0.50s 0.75 s
PCO2
46
PaO2
PaCO2
40
Time of Blood Flow Through Capillary
Dotted lines showing thickened diffusion membrane.
CO
2
Epithelium
Surfactant
33

Increase of Thickness of Diffusion Membrane
Normal Edema
CO
2
34
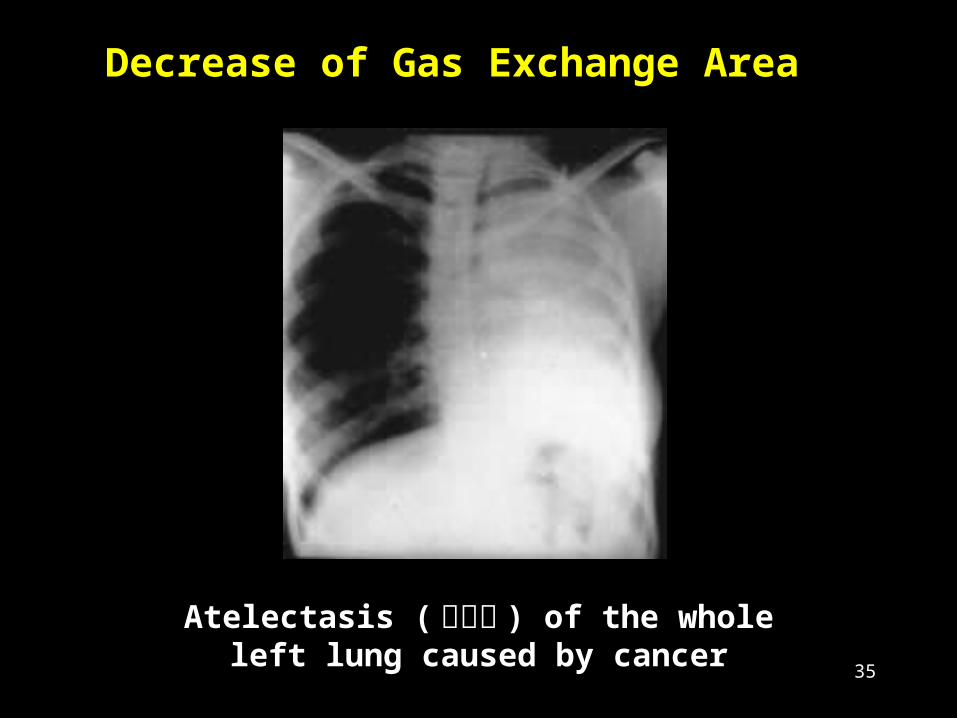
Decrease of Gas Exchange Area
Atelectasis (肺不张 ) of the whole left lung caused by cancer
35
Pathogenesis of Respiratory Failure
①① Dysfunction in ventilationDysfunction in ventilation
Restrictive hypoventilation Restrictive hypoventilation
Obstructive hypoventilationObstructive hypoventilation
②② Gas-exchange dysfunctionGas-exchange dysfunction
Diffusion impairmentDiffusion impairment
Ventilation/perfusion imbalanceVentilation/perfusion imbalance
Increase of anatomic shuntIncrease of anatomic shunt
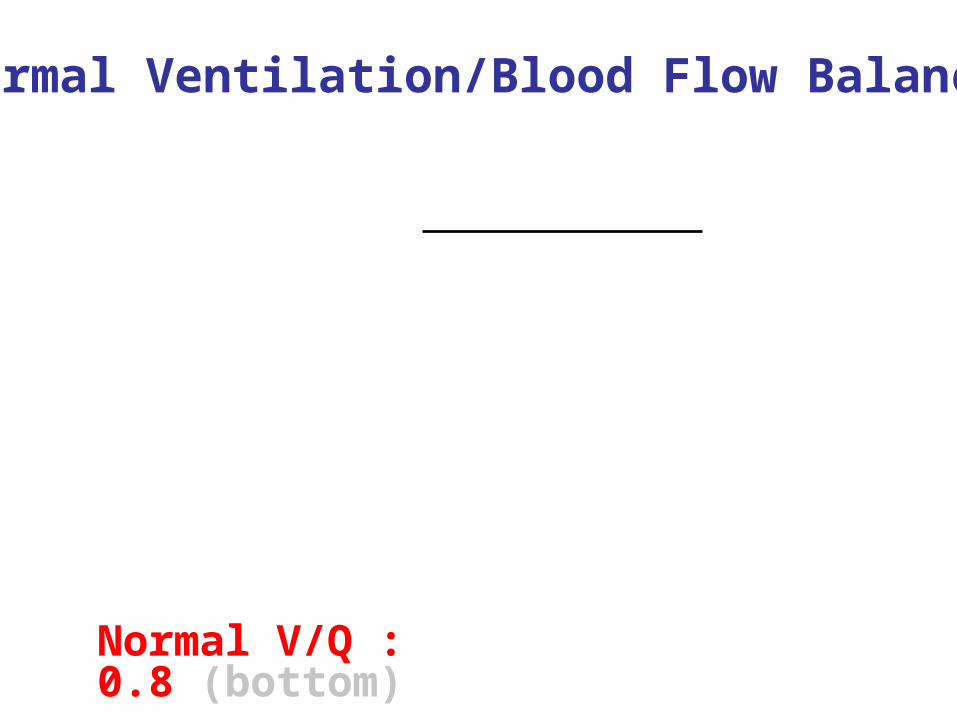
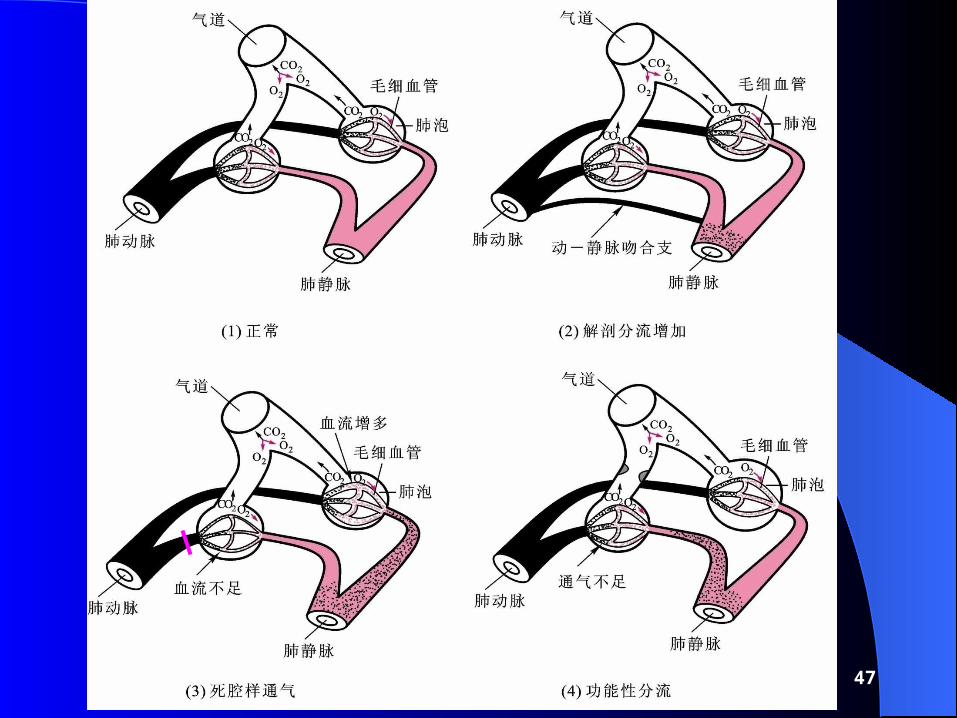
Normal Ventilation/Blood Flow Balance
V: Alveolar ventilation (N: 4 L/min)
Q: Pulmonary blood flow (N: 5 L/min)
Normal V/Q : 0.8 (bottom)
V/Q ratio = Ventilation (V)
Blood flow (Q)

Pathological V/Q Imbalance
Hypoventilation (↓V)
- V /Q? (< 0.8)
- Also called “Functional shunt” or
“Venous admixture”
Hypoperfution (↓Q)
- V /Q ? (> 0.8)
- Also called “Dead space-like ventilation”40

Normal
Functional Shunt
Hypoventilation (functional shunt) : V/Q ↓
Seen in asthma, COPD, edema, fibrosis

Pathological V/Q Imbalance
Hypoventilation (↓V)
- V /Q? (< 0.8)
- Also called “Functional shunt” or
“Venous admixture”
Hypoperfution (↓Q)
- V /Q ? (> 0.8)
- Also called “Dead space-like ventilation”42

Normal
Dead Space-like
Hypoperfusion (dead space-like ventilation) :V/Q ↑Seen in pulmonary artery embolism, pulmonary vasoconstriction, pulmonary DIC
Pathogenesis of Respiratory Failure
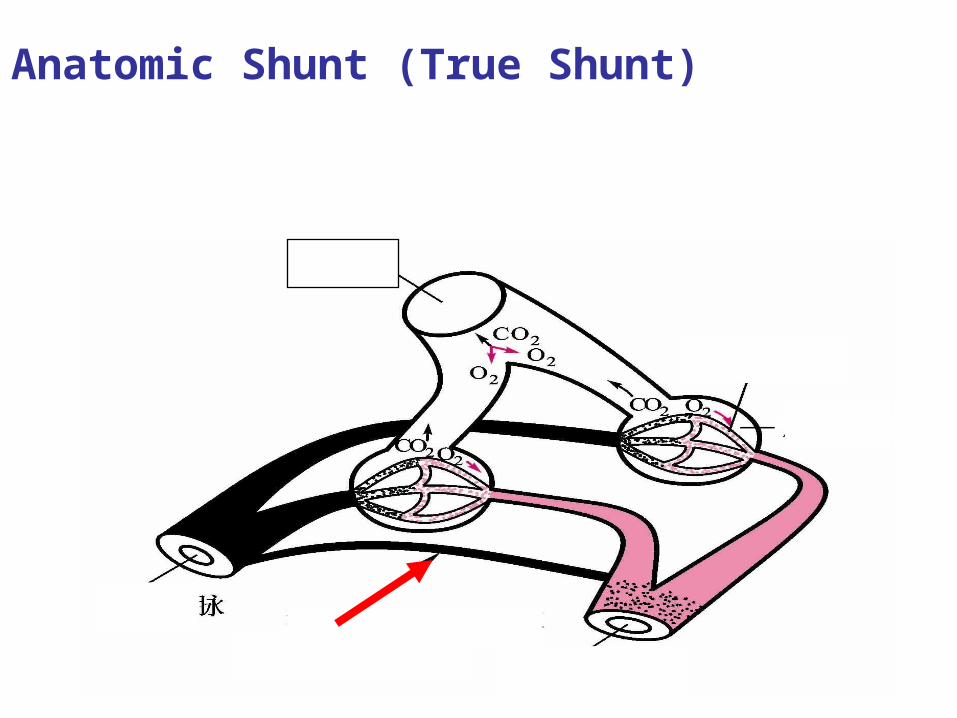
Anatomic Shunt (True Shunt) Part of venous blood directly flows into the pulmonary vein through the bronchial vein or arterio-venous fistula.
Airway
Capillary
Alveolus
vein
Artery
Arterio-venous fistulas
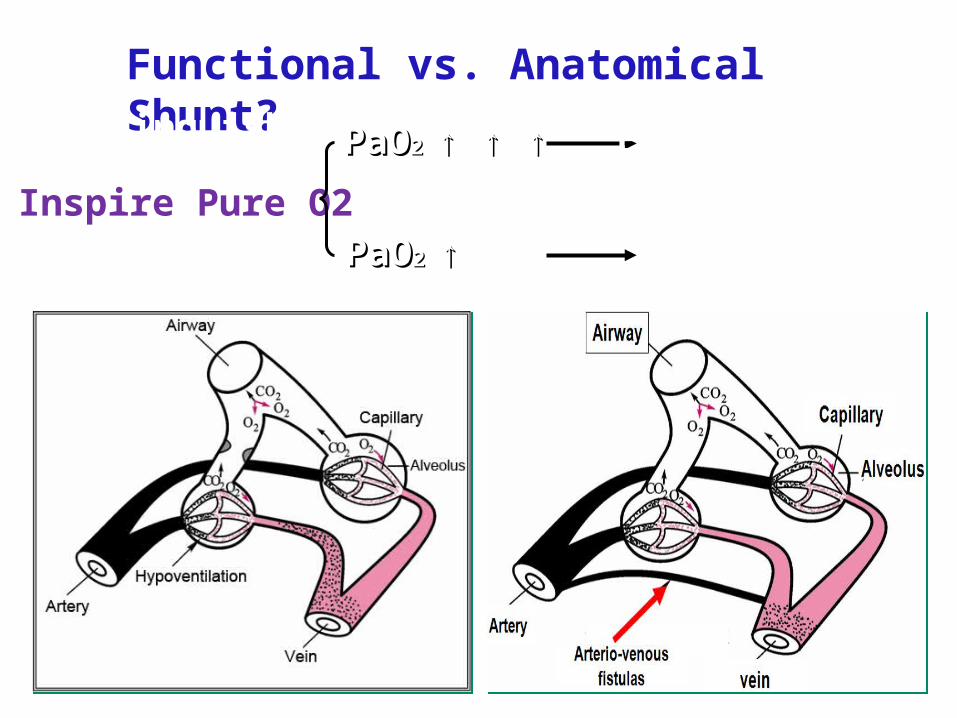
Functional vs. Anatomical Shunt?Distinquish:
Inspire Pure O2
PaOPaO2 2 ↑ ↑ ↑↑ ↑ ↑
PaOPaO2 2 ↑↑ Anatomical
Functional
47
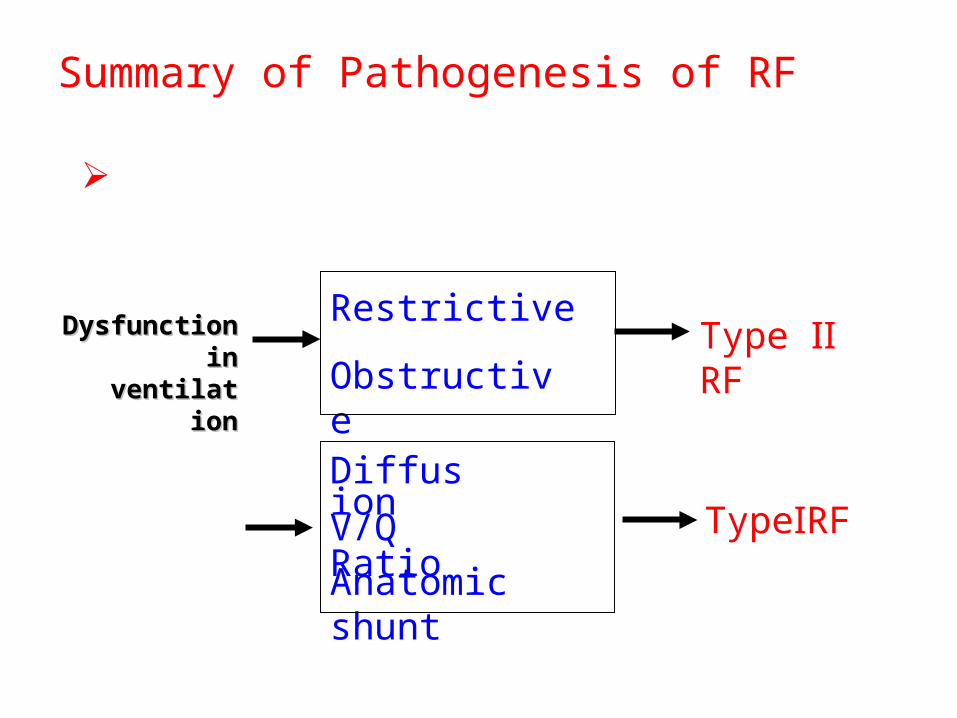
Summary of Pathogenesis of RF
Caused by dysfunction of external respiration.
Dysfunction Dysfunction in in
ventilativentilationon
Restrictive
ObstructiveType Ⅱ RF
Dysfunction in gas-
exchange
Diffusion V/Q RatioAnatomic shunt
TypeⅠRF

4949
Respiratory FailureRespiratory Failure
①① IntroductionIntroduction
②② Etiology and Classification Etiology and Classification
③③ Pathogenesis Pathogenesis
④④ Alterations of Metabolism and Alterations of Metabolism and
Function Function
⑤⑤ Pathophysiological Basis of Prevention Pathophysiological Basis of Prevention
and Treatmentand Treatment

Alterations of Metabolism and Function
①① Acid-base imbalanceAcid-base imbalance
②② Electrolyte disturbanceElectrolyte disturbance
③③ Organ system dysfunctionOrgan system dysfunction
Pulmonary systemPulmonary system
Circulatory systemCirculatory system
Central nervous systemCentral nervous system
Urinary and digestive systemUrinary and digestive system
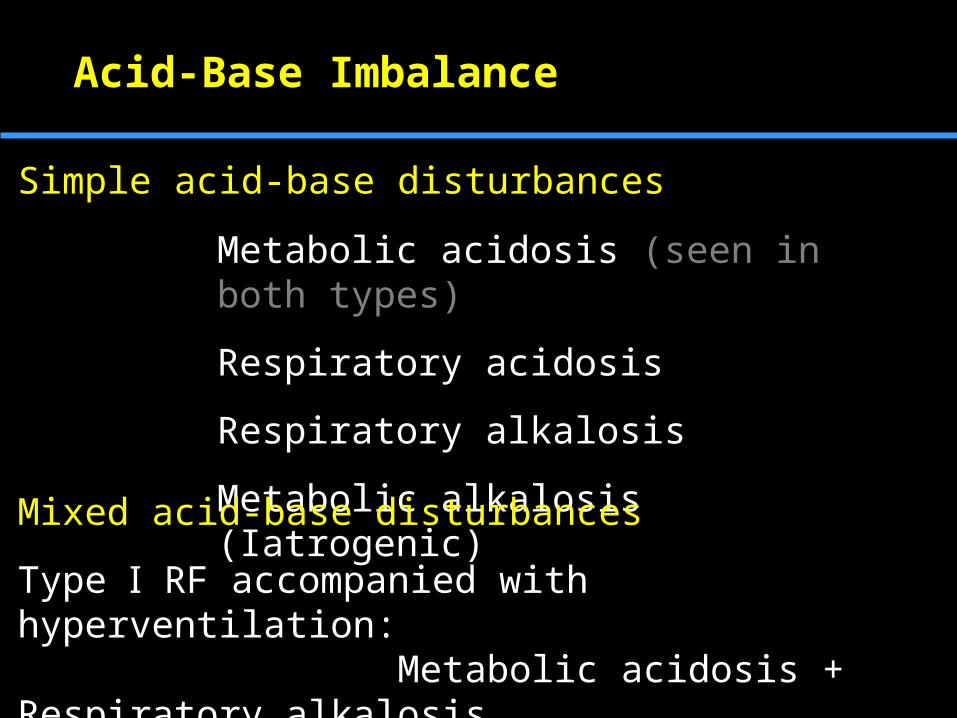
Acid-Base Imbalance
Metabolic acidosis (seen in both types)
Respiratory acidosis
Respiratory alkalosis
Metabolic alkalosis (Iatrogenic)Mixed acid-base disturbances
Type Ⅰ RF accompanied with hyperventilation: Metabolic acidosis + Respiratory alkalosis
Type Ⅱ RF: Metabolic acidosis + Respiratory acidosis
Simple acid-base disturbances

Hyperkalemia (↑ K+)
Acidosis
Increased tissue catabolism
Hypochloremia (↓ Cl-) or Hyperchloremia (↑ Cl-)
Depending on types of acid-base disturbance
RAc: Hypochloremia
RAl: Hyperchloremia
Electrolyte Disturbance
52
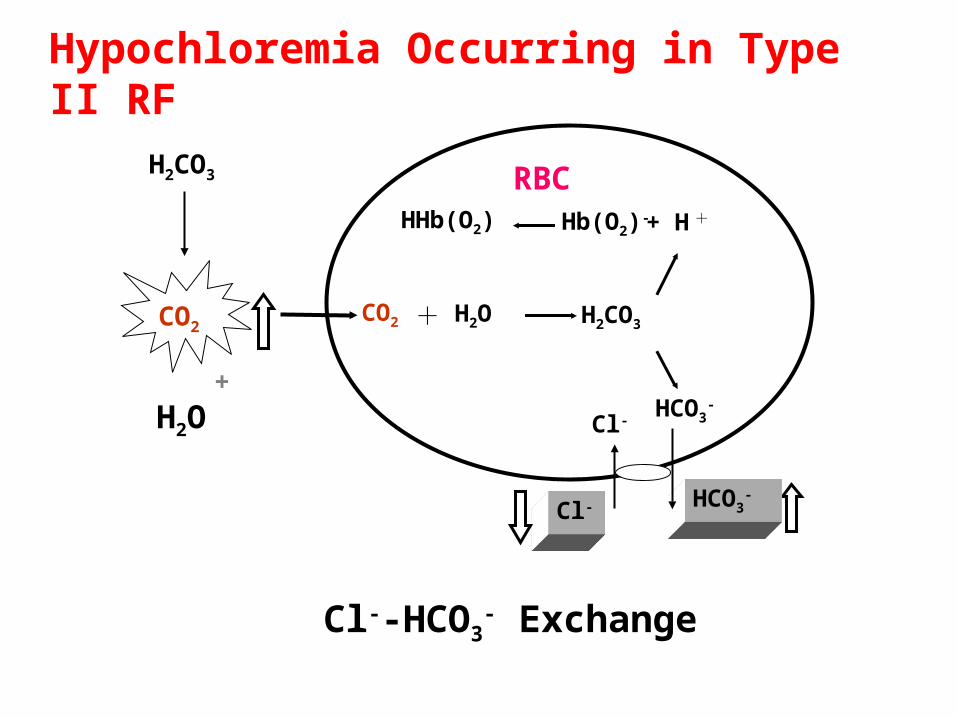
Cl--HCO3- Exchange
+ H +Hb(O2)-HHb(O2)
RBC
HCO3-
CO2 H2CO3+ H2O
Cl-
Cl- HCO3-
CO2
H2CO3
+
H2O
Hypochloremia Occurring in Type II RF
53

Alterations of Respiratory System
PaO2
<60 mmHg: ↑ respiratory movement
<30 mmHg:↓respiratory center
PaCO2
>50 mmHg: ↑ respiratory movement
>80 mmHg:↓respiratory center
54
Alterations of Circulatory System
Compensatory responses
Hypoxia and hypercapnia → ↑ vasomotor center
Increase HR, CO, myocardial contraction, BP; blood redistribution
Injurious responses
Hypoxia and hypercapnia → ↓vasomotor center
decrease HR, CO, myocardial contraction, BP;cor pulmonale

Pulmonary Heart Disease (cor pulmonale)
58
Alterations of central nervous system
CNS is the most sensitive organ to hypoxia.
PO2<60 mmHg: gentle impairment of intelligence and vision
PaCO2>80 mmHg: CO2 narcosis
PO2<50 mmHg: appearance of nervous and psychiatric symptoms
61

Alterations of urinary and digestive system
Functional acute renal insufficiency:
Excitement of sympathetic nerve leads to renal vessel constriction and RBF and GFR reduction.
Gastro-intestinal insufficiency:
Excitement of sympathetic nerve leads to GI organ vessel constriction → erosion, necrosis, hemorrhage, ulcer.
62
6363
Respiratory FailureRespiratory Failure
①① IntroductionIntroduction
②② Etiology and Classification Etiology and Classification
③③ Pathogenesis Pathogenesis
④④ Alterations of Metabolism and Alterations of Metabolism and
Function Function
⑤⑤ Pathophysiological Basis of Prevention Pathophysiological Basis of Prevention
and Treatmentand Treatment
Prevention and Treatment
1. Remove the factors that cause RF
2. Raise PaO2 via oxygen therapy
3. Reduce PaCO2 through improving ventilation
4. Others:
Correct acid-base imbalance
Correct electrolyte disturbance
Protect against heart and brain failure
64
Type II RF:
Low concentration (30% O2)
Low flow (1 - 2 L/min)
- Avoid too rapid correction of hypoxia
Oxygen Therapy
Type I RF:
High concentration (40% O2)
65
Introduction
Etiology and Pathogenesis
ARDS
Alterations of Metabolism and Function
Principle for Treatment
Contents
66

Acute Respiratory Distress Syndrome
Definition Clinical concept
defined it as a spectrum of ALI
- Acute onset
- bilateral infiltrates on CXR (“White lung”)
- PCWP =< 18 mmHg
- Hypoxia and PaO2/FiO2 =< 200
( ALI if P/F ratio =< 300 )
-No cardiovascular lesion 67
返回
68
69

ARDS is a severe lung syndrome (not a disease) caused by a variety of direct and indirect issues. It is characterized by inflammation of the lung parenchyma leading to impaired gas exchange
Pathophysiological concept
Alveolar-capillary membrane injury
70

Acute respiratory distress syndrome
Normal
71

ARDS
Acute lung injury
Diffuse alveolar damage (DAD)/Acute respiratory distress syndrome
72
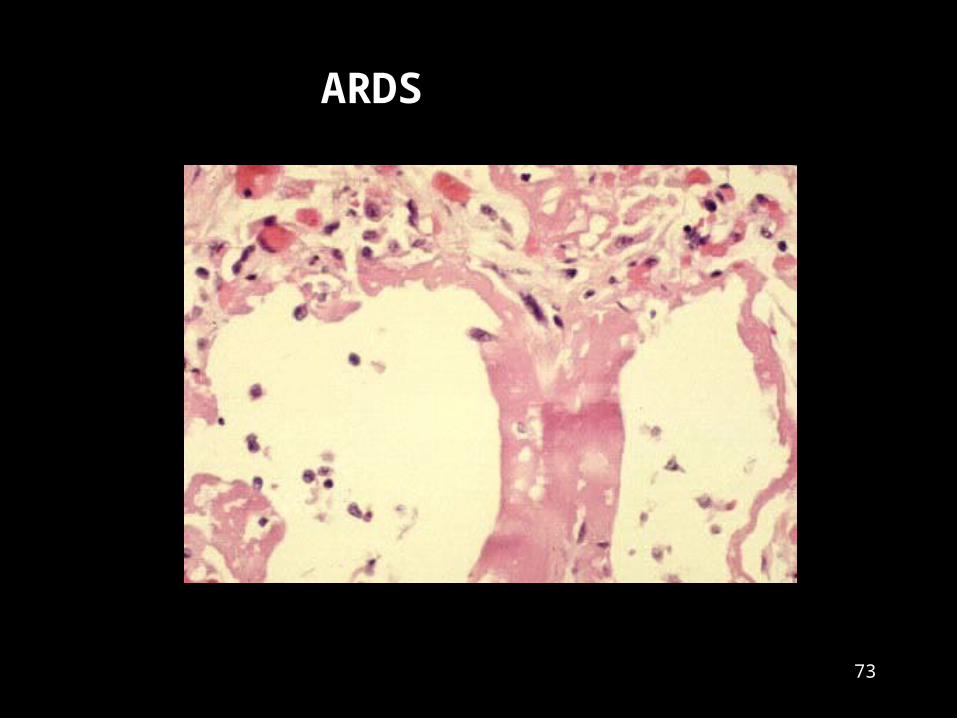
ARDS
73
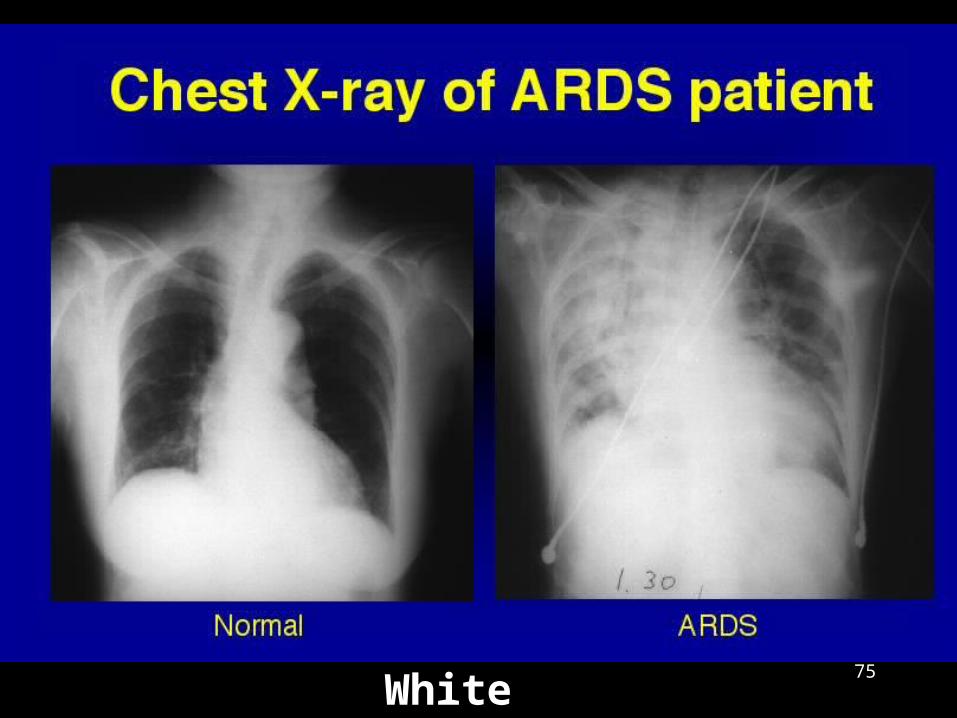
White lung75

Causes
Sepsis and Shock
Severe multiple trauma
Aspiration of gastric contents
Inhalation of toxic gases and fumes
etc.
Insults involved in alveolar capillary membrane injury
76

Pathogenesis
A-Cm injury
Pathogenic factors
PMN activation
Protease release ROS generation Inflammatory mediators
Plt activation aggregation
Thrombosis
Pulmonary edemaBleeding
hyaline membrane
Atelectasis Bronchial spasm
Vaso-constriction
Diffusion dysfunction
ShuntDead space
Hypoxemia 77
Related Documents











