-
7/31/2019 10hypertension-100510235019-phpapp01
1/81
Hypertension
Physiology, Pathophysiology and ClinicalManagements
Jun Tao
-
7/31/2019 10hypertension-100510235019-phpapp01
2/81
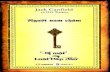
Stro e an Isc emic Heart Disease IHD Morta ityRate in Each Decade of Age, Versus Usual Systolic
BP at the Start of that Decade
Mortality
*
Usual SBP (mmHg)
5059 y
6069 y
7079 y
8089 y
Stroke
Age at risk
256
128
64
32
16
8
4
21
0 120 140 160 180
IHD
Usual SBP (mmHg)
5059 y
6069 y
7079 y
8089 yAge at risk
4049 y
256
128
64
32
16
8
4
2
1
0 120 140 160 180
*Floating absolute risk and 95% CI Reproduced from The Lancet, 360, Lewington et al. pp. 190313Copyright 2002, with permission from Elsevier
-
7/31/2019 10hypertension-100510235019-phpapp01
3/81
Introduction
Primary hypertension is a clinical
syndrome characterized by theincrease in systemic arterial pressure.
-
7/31/2019 10hypertension-100510235019-phpapp01
4/81
95% 0f the patients with hypertension areprimary hypertension with unknowncauses and 5% secondary hypertension
with definitive causes.
-
7/31/2019 10hypertension-100510235019-phpapp01
5/81
Hypertension affects approximately 1billion individual worldwide. In China theincidence of hypertension is about 180
million individuals.
-
7/31/2019 10hypertension-100510235019-phpapp01
6/81
Primary hypertension
-
7/31/2019 10hypertension-100510235019-phpapp01
7/81
Etiology and pathogenesis
Thepathogenesis of primaryhypertension is still unclear. There aremany factors associate with it.
-
7/31/2019 10hypertension-100510235019-phpapp01
8/81
Genetic factors
Sodium intake
Renin agiotensin systems Sympathetic nervous system
Endothelial dysfunction
Insulin resistance Other factors
-
7/31/2019 10hypertension-100510235019-phpapp01
9/81
Genetic factors
The offsprings of the hypertensiveparents are prone to suffering fromessential hypertension compared with thatwithout hypertensive family.
-
7/31/2019 10hypertension-100510235019-phpapp01
10/81
Sodium intake
The mechanisms leading tohypertension are due to increased bloodvolume and the content of the sodium inthe smooth muscle cells enhance followingsubsequent calcium increase.
-
7/31/2019 10hypertension-100510235019-phpapp01
11/81
-
7/31/2019 10hypertension-100510235019-phpapp01
12/81
Sympathetic nervous activation
The activation of Sympathetic nervouscan augment periphery resistant which
increase systemicarterialpressure.
-
7/31/2019 10hypertension-100510235019-phpapp01
13/81
-
7/31/2019 10hypertension-100510235019-phpapp01
14/81
Insulin resistance
Increased absorbability to sodium
Increased sympathetic nervous activationIncreased cellular contents in sodium andcalcium
Caused vascular wall hypertrophy
-
7/31/2019 10hypertension-100510235019-phpapp01
15/81
-
7/31/2019 10hypertension-100510235019-phpapp01
16/81
-
7/31/2019 10hypertension-100510235019-phpapp01
17/81
-
7/31/2019 10hypertension-100510235019-phpapp01
18/81
This is a result of ageing as well ashypertension : both processes thereforecause loss of the normal elastic reservoir
funtion of the aorta and large arteries.
-
7/31/2019 10hypertension-100510235019-phpapp01
19/81
-
7/31/2019 10hypertension-100510235019-phpapp01
20/81
This explains one curious feature ofelderly hypertensive patients. Diastolicblood pressure in patients with isolated
systolic hypertension is inversely related toprognosis.
-
7/31/2019 10hypertension-100510235019-phpapp01
21/81
-
7/31/2019 10hypertension-100510235019-phpapp01
22/81
-
7/31/2019 10hypertension-100510235019-phpapp01
23/81
-
7/31/2019 10hypertension-100510235019-phpapp01
24/81
-
7/31/2019 10hypertension-100510235019-phpapp01
25/81
-
7/31/2019 10hypertension-100510235019-phpapp01
26/81
Hpertrophy of left ventricle
-
7/31/2019 10hypertension-100510235019-phpapp01
27/81
-
7/31/2019 10hypertension-100510235019-phpapp01
28/81
Central nervous system
Cerebral infarction in a hypertensivepatient is usually attributable to atheromaof one of the larger cerebral arteries(usually the middle cerebral artery) andaccounts for about 80 percent of the
strokes which these patients suffer.
-
7/31/2019 10hypertension-100510235019-phpapp01
29/81
-
7/31/2019 10hypertension-100510235019-phpapp01
30/81
-
7/31/2019 10hypertension-100510235019-phpapp01
31/81
-
7/31/2019 10hypertension-100510235019-phpapp01
32/81
The kidney
The long-term renal damageproduced by glomerular hypertensionprobably accountd for progressiveglomerulosclerosis in essentialhypertension.
-
7/31/2019 10hypertension-100510235019-phpapp01
33/81
-
7/31/2019 10hypertension-100510235019-phpapp01
34/81
X
-
7/31/2019 10hypertension-100510235019-phpapp01
35/81
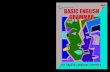
Malignant hypertension:Fibrinoid necrosis of damaged arteriole of kidney
-
7/31/2019 10hypertension-100510235019-phpapp01
36/81
-
7/31/2019 10hypertension-100510235019-phpapp01
37/81
-
7/31/2019 10hypertension-100510235019-phpapp01
38/81
-
7/31/2019 10hypertension-100510235019-phpapp01
39/81
-
7/31/2019 10hypertension-100510235019-phpapp01
40/81
-
7/31/2019 10hypertension-100510235019-phpapp01
41/81
Nocturia
this is one of the most frequent clinicallyapparent consequences of blood pressureelevation resulting from reduction in urine-concentrating capacity.
-
7/31/2019 10hypertension-100510235019-phpapp01
42/81
-
7/31/2019 10hypertension-100510235019-phpapp01
43/81
Symptoms associated with target organ damage
Cardiovascular system
Effort dyspnoea and orthopnoeasuggest cardiac failure. Increased leftventricular mass is associated withdecreased compliance and impairedcardiac output response to exercise.
-
7/31/2019 10hypertension-100510235019-phpapp01
44/81
-
7/31/2019 10hypertension-100510235019-phpapp01
45/81
-
7/31/2019 10hypertension-100510235019-phpapp01
46/81
Retinopathy
Scotomas suggest fundal haemorrhagesor exudates, whilst blurring of vision isassociated with papilloedema.
-
7/31/2019 10hypertension-100510235019-phpapp01
47/81
-
7/31/2019 10hypertension-100510235019-phpapp01
48/81
-
7/31/2019 10hypertension-100510235019-phpapp01
49/81
-
7/31/2019 10hypertension-100510235019-phpapp01
50/81
CategorySystolic blood
pressure (mmHg)
Diastolic blood
pressureOptimal blood pressure
-
7/31/2019 10hypertension-100510235019-phpapp01
51/81
CVD Risk Factors
Hypertension* Cigarette smoking
Obesity* (BMI >30 kg/m2)
Physical inactivity
Dyslipidemia*
Diabetes mellitus*
Microalbuminuria or estimated GFR
-
7/31/2019 10hypertension-100510235019-phpapp01
52/81
-
7/31/2019 10hypertension-100510235019-phpapp01
53/81
-
7/31/2019 10hypertension-100510235019-phpapp01
54/81
-
7/31/2019 10hypertension-100510235019-phpapp01
55/81
-
7/31/2019 10hypertension-100510235019-phpapp01
56/81
Lifestyle Modification
Weight reduction:
the trial of hypertension preventionproduced an average weight loss of 3.8
kg at 18 months, reduction of SBP andDBP by 2.9 and 2.3 mm Hg.
-
7/31/2019 10hypertension-100510235019-phpapp01
57/81
Exercise:
Following increased physical activity,BP falls up 6-7 mm Hg for both SBP and
DBP.
-
7/31/2019 10hypertension-100510235019-phpapp01
58/81
Algorithm for Treatment of
-
7/31/2019 10hypertension-100510235019-phpapp01
59/81
Algorithm for Treatment ofHypertension
Not at Goal Blood Pressure (100 mmHg)
2-drug combination for most (usuallythiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 Hypertension(SBP 140159 or DBP 9099 mmHg)
Thiazide-type diuretics for most.May consider ACEI, ARB, BB, CCB,
or combination.
Without CompellingIndications
Not at GoalBlood Pressure
Optimize dosages or add additional drugsuntil goal blood pressure is achieved.
Consider consultation with hypertension specialist.
-
7/31/2019 10hypertension-100510235019-phpapp01
60/81
-
7/31/2019 10hypertension-100510235019-phpapp01
61/81
Diuretics
Indications : cardiac failure
elderly patients
systolic hypertension in elderly
-
7/31/2019 10hypertension-100510235019-phpapp01
62/81
-
7/31/2019 10hypertension-100510235019-phpapp01
63/81
-
7/31/2019 10hypertension-100510235019-phpapp01
64/81
-
7/31/2019 10hypertension-100510235019-phpapp01
65/81
-
7/31/2019 10hypertension-100510235019-phpapp01
66/81
-Adrenergic blockers
Indications: prostatism
Contraindications: urinary incontience
-
7/31/2019 10hypertension-100510235019-phpapp01
67/81
Compelling and possible indications, contraindications, and cautions forthe major classes of antihypertensive drugs
Class of
drug
Compelling
indications
Possible
indications Caution
Compellingcontra-
indications
Alpha-blockers
Benign prostatichypertrophy
Posturalhypotension,heart failure
Urinaryincontinence
ACE-inhibitors
Heart failure,LV dysfunction, post
MI or established CVD,Type I diabeticnephropathy, 2o strokeprevention
Chronic renaldisease,
Type II diabeticnephropathy,proteinuric renaldisease
Renal impairment
PVDPregnancy,renovascular
disease
ARBs ACE inhibitor-intolerance,Type II diabeticnephropathy,hypertension with LVH,heart failure in ACE-intolerant patients, postMI
LV dysfunctionpost MI, intol-erance of otherantihypertensivedrugs, proteinuricrenal disease,chronic renaldisease,
heartfailure
Renal impairmentPVD
Pregnancy,renovasculardisease
-
7/31/2019 10hypertension-100510235019-phpapp01
68/81
-
7/31/2019 10hypertension-100510235019-phpapp01
69/81
-
7/31/2019 10hypertension-100510235019-phpapp01
70/81
-
7/31/2019 10hypertension-100510235019-phpapp01
71/81
Other medications for hypertensive patients
-
7/31/2019 10hypertension-100510235019-phpapp01
72/81
Other medications for hypertensive patients
Primary prevention(1) Aspirin: use 75mg daily if patient is aged 50 years with blood pressurecontrolled to
-
7/31/2019 10hypertension-100510235019-phpapp01
73/81
Lipid targets
-
7/31/2019 10hypertension-100510235019-phpapp01
74/81
Targets for lipid lowering
Ideal - TC
-
7/31/2019 10hypertension-100510235019-phpapp01
75/81
Some key points of the 2007 ESHand ESC guidelines
-
7/31/2019 10hypertension-100510235019-phpapp01
76/81
CVD Risk Factors
There are some new risk factors :
fasting blood glucose 5.66.9mmol/L ;
pulse pressure (in the elderly)
-
7/31/2019 10hypertension-100510235019-phpapp01
77/81
f
-
7/31/2019 10hypertension-100510235019-phpapp01
78/81
ESH - ESC Guidelines, J Hypertens 2008
-BP < 140/90 mmHg in all hypertensive
patients
< 130/80 mmHg in hypertensive patients
with diabetes or renal disease
-Control of all cardiovascular risk factors
Goals of treatment
b d
-
7/31/2019 10hypertension-100510235019-phpapp01
79/81
About drug treatment
Diuretics, Blockers, Calcium channel blockers,ACE inhibitors and Angiotensin II receptorblockers can be used in onset and maintenanetherapy.
Diuretics combined with Blockers is notsuitable for metabolic syndrome or high-riskdiabetes patients.
Low-dose combination therapy as first linetreatment of mild-to-moderatehypertension
-
7/31/2019 10hypertension-100510235019-phpapp01
80/81
-
7/31/2019 10hypertension-100510235019-phpapp01
81/81