https://theses.gla.ac.uk/ Theses Digitisation: https://www.gla.ac.uk/myglasgow/research/enlighten/theses/digitisation/ This is a digitised version of the original print thesis. Copyright and moral rights for this work are retained by the author A copy can be downloaded for personal non-commercial research or study, without prior permission or charge This work cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given Enlighten: Theses https://theses.gla.ac.uk/ [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
https://theses.gla.ac.uk/
Theses Digitisation:
https://www.gla.ac.uk/myglasgow/research/enlighten/theses/digitisation/
This is a digitised version of the original print thesis.
Copyright and moral rights for this work are retained by the author
A copy can be downloaded for personal non-commercial research or study,
without prior permission or charge
This work cannot be reproduced or quoted extensively from without first
obtaining permission in writing from the author
The content must not be changed in any way or sold commercially in any
format or medium without the formal permission of the author
When referring to this work, full bibliographic details including the author,
title, awarding institution and date of the thesis must be given
Enlighten: Theses
https://theses.gla.ac.uk/
>
Smt/iARY
KPIDKMIOLOGIGAL AMD UORMONS STUDIED IM EARLY H U m N PREGNANCY - NORMAL AND ABNORMAL
By> MeC# Mappaughtoïî M.E* Ch*B*(Glas») F*r ,c «o *0*
€ In apt or I* Introduction to tRo Thesis #Chapter 2* Epidemiological studieo in abortion* and
subsequent reproductive performance.
K Nomen who start childbearing with Î or 2 consecutive abortions are compared with those who start with 1 or 2 normal pregnancies♦
2. Women who start childbearing with 2 abortions aro olderp shorter and of lowor socio-economic status than the other 3 groups*
3* In the first continuing pregnancy these womenhave a higher incidence of threatened abortionand premature labour. Their perinatal mortality is increased due mainly to ^prematurity * and ®foetal deformity®. They also have an increased incidence of operative delivery *
4. The group with 2 previous abortions have atendency to poor foetal growth and this is
ProQuest Number: 10662677
All rights reserved
INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a com p le te manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uesL
ProQuest 10662677
Published by ProQuest LLO (2017). Copyright of the Dissertation is held by the Author.
All rights reserved.This work is protected against unauthorized copying under Title 17, United States C ode
Microform Edition © ProQuest LLO.
ProQuest LLO.789 East Eisenhower Parkway
P.Q. Box 1346 Ann Arbor, Ml 48106- 1346
2*
associated with premature laboiir*5# Worn cm v/ho abort in their first pregnancy have
an increased risk of abortion in their subsequent reproductive life*
0;# The recurrent abortion risk increases withsuccessive consecutive abortions from 2 5;.. after 1 abortion to SB% after 3 abortions*.
7# One third of abortions occur before 2 monthsgestation and 00% by 3 months#
8# In abortion studies the ®primary recurrent abortcr*with 2 or more consecutive abortions should be studied* Observations must start before 8 weeks of gestation or earlier if a previous abortion has occurred before this time*
Chapter 3* Hormone assays in normal early pregnancy» in abortion and in hydatidiform male*
Î* Urinary pregnanodiol and oestriol assays are madein 3 groups of women ( 0 Normal pregnancy (2) Nomen with at least 2 previous abortions and no successful pregnancies and (3) Women who aborted in the pregnancy studied*
2# There is no significant difference in oestrioland pregnanedioi excretion between the women who

aborted and those in which the pregnancy continued successfully » until after 16 weeks of gestation*
3. These 2 assays are of no value in forecasting abortion until after 16 weeks of pregnancy*
4* The assays were perforned in 5 cases ofhydatidiform mole. In these cases the urinary pregnanediol and oestriol levels may be normal but are more likely to be low. There may be some change in steroid metabolism in this type of case.
Chapter 4. Conversion of progesterone to pregnanediol*
1. After the injection of lOOpc. tritiated progesterone the percentage radioactivity excreted as pregnanediol was measured in 4 groups of women(1) Non-pregnant (2) Early pregnancy (3) Late pregnancy (4) Abnormal pregnancy.
2. There was a significant difference between theresults in abnormal pregnancy and the other 3 groups. The percentage conversion was less in abnormal pregnancy especially in cases of hydatidiform mole.
3. There was no difference in conversion in thesame subject, non-pregnant and pregnant.

T 4 ■*
Chaptos'* 5* Progesterone metabolism in the human proviable foetwo*
1. Perfusion of previabio foetuses with 4-C^^progesterone for M and 45 min.* showed that40% of the radioactivity is present in the liverat 14 min* mainly as 20a dihydroprogesterone andin the adrenal 3*4% of radioactivity^ is present»mainly as polar compounds* After 45 min* themain compound in the liver was pregnanediol andin the adrenals* polar compounds probablycorticosteroid s.
2* The foetal liver is the chief site of progesteronemetabolism and this organ produces mainly reduced metabolites. The adrenal motabolises progesterone to corticosteroids.
3. Progesterone from the placenta is used by thefoetus to produce corticosteroids for its own homeostasis ®
Chapter 6* Steroid studies in a case of hydatidiform mole.
1. Th€ urinary pregnanediol: pregnanetriol ratio inmolar pregnancy is 2 s 1 compared with 20s1 in normal pregnancy.
5
2* Mole tissue v/as Incubated vilth [4 - ^ G ] pregnenoloneas precursor p and 17co liydroxypregnenolone, progesterone» 16a hycU'^OKyprogeoterone and 10(3 h yd r o xy prog eat ero ne v/er e Isolated*
o* ChoXestorolp pregnenolone* 17a hydroxyqjrcgnenoione, pregnanediol* pregnanetrio! and androstenedlonc v/ere isolated from extracts of mole tissue ami theca lutein cyst fluid: 17a hydroxyprogesteronewas isolated from cyst fluid but not from mole tissue*
4* Mole tissue is capable of steroidogenesis but there was leas synthesis of progesterone than normal•
5* The increase of 17a hydroxylation indicated bythe elevation of urinary pregnanetriol excretion is ovarian in origin.
Chapter 7* Urinary steroid excretion after gonadotrophin therapy*
Î* There is a significant increase in pregnanediol excretion in the luteal phade of the menstrual cycle due to the ovarian pa'oduction of 17o. hydroxyprogesterono*

r»
if6*
2* Urinary pregnanetriol excretion also E^ieea in the luteal phase of gonadotrophin stimulated cycles and in gonadotrophin Induced pregnancies until G - 8 weeks#
3v Measurement of this metabolite may be a valuable parameter of corpus luteurn function in the menstrual cycle, ami in early pregnancy#
4# This assay may bo of value in detectinghyperstimulation of the ovaries by gonadotrophins. It may also indicate when the corpus lutcum of pregnancy is deficient and be of help in forecasting early abortion#
EPIiJEMIOLOOlCÀL AKü HORMONE STUDIES ÏH EARLY HUMAN PREOWAf^CY • NOar.îAi AND ABKOMiAL
A THESIS
SUBMITTED TOR THE DKOftSB OF DOCTOR. OF MEDICINE
by
MALCÜUÎ CAMPBSLl, MACNAUOBTOM, M.a. Ch.B.(Glas) .t F.R.C.O.Q.
Department of Obstetrics &Gynaecology,
The University,Dundee. December 1989.

INDEX
CHAPTER 1#CHAPTER 2,
INTRODUCTION TO THE THESISEPIDEMIOLOGICAL STUDIES ON ABORTION AND SUBSEQUENT REPRODUCTIVE ' PERFORMANCE Introduction Incidence of Abortion Epidemiological characteristics and obstetric performance of women who abort
Sources of DataEpidemiological characteristics 1 * Age 2* Height3® Husband's Social Class 4* Duration of marriage and
number of children Obstetric performance in first continuing pregnancy 1. Threatened abortion 2» Antepartum haemorrhage 3# Prematurity
PageU
4, Perinatal Mortality5® Performance in labour
Fertility following first pregnancy Recurrent Abortion
Gestation period of abortion Interval between pregnancies Age and duration of marriage
8#8.
10#
IS#13#18#16#17#18#
ID.
20#
20#
2 1 #
2 1 #
24#26#28#
33#35#36#
PageRelation of results to the design of abortion studies 3 7*1. Type of patient 3 7#2* Gestation period to be
studied 39#CHAPTER 3# HORMONE STUDIES IN NORMAL EARLY
PREGNANCY IN ABORTION AND IN H YD AT ID I FORM MOL E 43 .Normal early piegnancy and abortion 43.
Pregnanediol 44#1# Organs producing
pregnanediol precursor in pregnancy 4$.
2# Pregnanediol excretion innormal pregnancy 46*
oestriol 47*1# Biogenesis of oestrogens
in pregnancy 47*2# Clinical signifieanco 52#3# Urinary oestriol excretion
In normal preg&iancy 54#Present Study 55#
Method of assay of urinary pregnanediol 55*Method of assay of urinary oestriol 55*Subjects 56.Results 57.I# Pregnanediol excretion 57#
- 2* special cases 57#
PageS. Oestriol excretion 58#4# Prognanedlol/oestrlol ratio GO#
Discussion 63#Urinary excretion of oestrogen and pregnanediol In hydatidiform mole 66#Introduction 66#Methods of assay of the hormones 68*Ullnlcal Summaries 69#Results 71#
1# Pregnanediol 71#2# Oestriol 72#3# Oestrone and Oestradloi 72#
Discussion of mole results 7Z#CHAPTER 4# THE CONVERSIUN OF PROGESTERONE TO
PREGNANEDIOL 75#Percentage recovery of Injected progesterone as urinarypregnanediol 76.Present Study 77#
1# Metabolism of progesterone 77,2# Assay of urinary
pregnanediol 80#3# Measurement of the radio
activity present in the urinary pregnanediol following intravenous injection of progesterone 81#
Results $3#1# The radioactivity recovered
as urlnary pregnanedlo1
PageResults oontd#
followl:)g intravenous injection of tritiated progesterone 83#
2# Specific activity of thepregnanediol isolated 86.
3# Urinary pregnanediolexcretion, and percentage conversion of progesterone to pregnanediol in a hyste:ectomlsed woman 88.
4# Excretion by same patientsnon-pregnant and pregnant 88*
Discussion 8D.GHAPTBR S# PROGESTERONE METABOLISM IN THE HUMAN
PREVIABLE FOETUS 94#Introduction 04.Present Study D6#Materials and Methods 86.Results 98#
1. Radioactivity in foetal tissues 14 min. after injection of [4-^'^c] progesterone 98.
2. Radioactivity present in foetal tissues after perfusion with [4-^^^c] progesterone for 45 min. 99»
Discussion 100.

PageCHAPTER 6* STEROID STUDIES IN A CASE OF
HYDATIDIFORM MOLE 107.Clinical History 108.Detcrmixiation of Urinary Steroids 108.Injection of radioactivity 109*Determination of steroids in mole tieene and ovarian cyst fluid 109.Urinary pregnanetriol excretion 111.Résulta 112.Discussion 113.
1. Incubation of mole tissue 113.2. Steroids of the mole
tissue 115.3. Steroids in ovarian cyet
fluid 118.Conclusions 121*
CHAPTER 7* URINARY STEROID EXCRETION AFTERGONADOTROPHIN THERAPY 123.Steroidogenesis in the human ovary 124.Oestriol 125.Control of ovarian biogenesis 126*Pregnanetriol 128.The ovarian production of a pregnanetriol precursor 128.Pregnanetriol excretion in human pregnancy 131*Clinical histories of patients 134Assay methods 13/Results 137Discussion 140
#
PageDiscussion
1# Pregnanetriol excretion in the gonadotrophin stimulated cycle 142*
2# Pregnanetriol excretion in early gonadotrophin stimulated pregnancy 146*
Mote on the functional life of the corpus luteum of pregnancy 146*
CHAPTER 8* SUm^ARY AND CONCLUSIONS 163*1* Summary 163*2* Conclusions 162*3. Further worZt arising from
th18 thes1s 163*Acknowledgements 164*
APPENDIX
1, Plates2, Diagrams 3# Tables4* References5. Publications
u
CMAPfBR t, .
iuetlea to t W Theela
The theme of this thesis la "oorly prognaney^'# that la from ooooeptloa until obout 20 iveeke of ge&tatlon# This period Includes Implantation, placentation, the early development of tho footuo
and of the footo-plaoontal unit#
The %vrltor*8 original Interwt, %vhloh led to thle study, was oonoorned tvlth abortion ana. In particular, %/lth the study of rootxrrent abortion* Much had been written, ohout mothoda whereby abortion eould be foreeaat but the reeulta were eo Ineoneleteiat that further Investigation eeomiod nooeeam'y. Although mueh resonroh had been devoted to the et%My of abortion, and a great volume of writings on the aubjeot had oeoumulated, undei^standlng of the proeeao had expanded little#Thoi^o are a number of reaoone for this, not least of ivhleh, la the fact that much of the study had had, of neeeealty, to be oonduotod %vlthln the oontoxt and limitations of ollnleal medlolne* The selentlfie prlnelploe of oxmet definition of metorial, and of eontroia, have been largely ignored* Although widely

2
h c e o p t W definitions of abortion,^Inovltabio* aboa'tion, rnloood* abortion and *roeurMOt* abortion liave existed for dooadeo those categories have mot boon rigidly eeparated, and# In %vrltlng$ on the snbjdot thofo hoe boon inmfflolont dloorlmlnatlon between those ontltlw* For example# the moaning of r e o w r o n t abortion 1$ not clear from the lltmatnre# and It ooomod probable that limitation of study of foonrrent abortion material to patienta %vho have had throe (rather than two) eonaeentlve ahortlow# %/ae an nnnoeeosarlly aevero reatrletlon ivhleh wan hamed on a taelt aoeeptanee of Malpas* (193$) formula#
It aoemod therefore* Important* In t&%e rirat Inetanoe to InveetlgnW the general Ineldenoe of abortion * ond ti%en to deter&WLne the reprodiactlve history of women wiio began ehlldbearlng with an abortion# This w o o M give factual Information about the number %Yho aborted again and again* Indicate %vhether there was generally poor reproduction In these %mmcn* and the particular aspeeto of their 8%%bsoquent pregnnncloe to y^leh attention should ho paid during the period of antenatal care* It would# In imrtleular# help to define the type of woman moot liable to abort

I ,
again and also give information about the gestation period at which abortion oeenrred* It waa felt by the writer, that frequently, In therapeutic trials of drugs In reeuM^ont abortion# the drugs were given long past the gestation period at which abortion wao likely and that the pregnancies were already highly eoleeted by virtue of having already progressed passed this period*
The results of an Investigation Into these proh3.eais are reported In Chapter 2$ In this chapter some description of the oha%aeterlstlcs of the ivomen concerned, such as age, height and socio-economic group are discussed, and the problems associated with their next pregnancy are assessed with particular reference to perinatal mortality# Their later reproductive pattern Is reviewed, and the number of subsequent abortions Is compared with that In a normal group of women# The question of the gestation period at which abortion and especially recurrent abortions take place Is surveyed, and the chapter concludes with a dissertation on the implication of the results to the design of studies on abortion with particular relation to the gestation period at which therapy, if any, should be started and the women who should be studied#
4#
T W demlgn evolved In Chapter 2 is then applied to tlw atudy of a group of mWrtlon prone women and a s W d y la made to discover If the mea.surement of two steroid hormones# oestriol and prognanedlel. In the maternal w i n e In pregnancy# will give any helpful Information about the likelihood of abortion occurring In these women* The reaeon why those two sterolde are moot likely to W of value 1$ dlacueeed along with Information aho%:t their derivation and the metabollom of their precuraor## The chapter conclude# with u m m observations on another abnormality of early pregnancy - hydatidiform mole - whloh is of particular Interest duo to the absence of the foetua In theae caoes#
The result# obtained In Chapter 3 pose a number of question# concerning progesterone metabolism and two of those are selected for further investigation In Chapter# 4 and 5*
In Chapter 4 the conversion of progesterone to pregnanediol la examined# The work in Chapter 3 Bhowed a groat variation in pregnanediol excretion# and one of the poeelble explanations of thlo was that
there was a variability in conversion from the parent steroid to the urinary metabolite* The results of previous work on this aspect were confusing* The chapter begins with a review of progesterone metabolism in early human pregnancy* A description of the methodology involved is then given and the results are discussed*
The other appcct selected for intensive study is discussed in Chapter 6 on progesterone metabolism in the human previahle foetus* On a previous occasion the writer and D r , Klopper (klopper â 'Maenaughton 1069) had found pregnanediol in the liquor amnii* and the question of the metabolism of progesterone and the production of pregnanediol by the foetal compartment was another possible factor affecting maternal excretion* There %vas little information available at the 'time on this aspect, and perfusion experiments of previahla foetuses with radioactive progesterone were undertaken to elucidate the problem* The technique of the experiments and the results are discussed in this chapter*I
As a result of the work on conversion of progeeter-
one to pregnanediol described in Chapter 4, women with hydatidiform mole were found to have lower conversions than normal women# The question of a different pathway of eteroldogenesla in these caaea was thought to be a posaible explanation# Steroid studies in hydatidiform mole were then unilartaken and are reported In Chapter 6» In these studios molar tlseue v/as incubated with precursor pregnenolone to determine the steroidogenic pathways In this tissue and ©taroids were extracted directly from the molar tissue itself.The steroid content of the theca lutein ovarian cysts v/hioh are frequently present in cases of hydatidiform mole was examined and the origin of certain steroids such as hyd ro xyprogee terone ascertained# The results here do show a change in emphasis of the Steroid pathway in these women#
The findings of Chapter 6 are then applied to the measurement of the ovarian response in amenorrhoeic women being treated with human menopausal gonadotrophins# Chapter 7 discusses an investigation into urinary steroid excretion after gonadotrophin therapy# The stimulation of the ovary caused by gonadotrophins is not unlike that found in some cases of hydatidiform
molo a W the particular use of pregnanetriol excretion in meoBuring corpus Intoum ftmotion in the monotruai cycle, end aioo in early pregnancy is ovaluateu# Thechapter conolWoa ivith a roforonoo to the poesiblo w o of this oeany in forooaoting abortion# the original starting point of this thooia#
In each ohaptor t W relevant litoraturo ia reviewed o%w tho relation of the ivork to that in the literature iB shown* Booh chapter diaouaaea a different aapoot of the overall theme and the relevant litoratnro and dleonaalon have W e n inolWed ia% each chapter rather than in an overall introduction# In t%$i$ %my ropotition la avoided and the thoughts on each napset are kept together#
The purpose of this iE%troduetion is to show the relationship of the chapters to each other and to the overall theme of ea%*ly prognanoy# This theme i# illustrated by plates I VI# ivhleh are taken from *hr* aranvllle*a Graphic Illustrations of Abortion and %he Oiaeaaos of Menstruation* (1633)*

h
CHAPTER 2 »
studies on abortion and
Introduction
Much has been written on the probiem of abortion and ItB incidence (Malpao 1938} Bovis 1051} etc.) and there is confusion in the literature on the probability of abortion occurring in a subsequent pregnancy particularly in women who have experienced recurrent abortions*^ The theoretical calculations made first by Maipas ( 1038) and later revised by Eastman (1056) estimate the risk of spontaneous abortion occurring in women with a history of a given number of abortions.Maipas considered that, after one previous abortion, the risk was 12 , after % previous abortions 38% and after 3 previous abortions 73%. These were revised by Eastman to 13, 37 and 84% respectively. These figures have been subjected to much criticism on the grounds that certain assumptions on which the calculations were based were faulty (Warburton â Fraser 1050} Qoldzieher ê ienigno 1068). Malpas (1038) for example, assumed that spontaneous abortions occur
0
either for a eauee* or for a *non-recurront*cause 1,0. that C % $ 0 0 of abortion can be divided Into a group with 100% chance of recnrrance and a grcnp with a chance of recurrance equal to the incidence of abortion (excluding habitual abortion) In the general population,
The gestation process depends upon such a complex interaction between maternal and foetal factors# both genetic and environmental# that it must be susceptible to Intorferonco by a very large number of agents and therefore Malpas* aeaumptlon is not valid. Results from these calculations have been v/lclely quoted # and have been used as controls in studies concerned with the prevention of habitual, abortion, James (1902) suggested that these calculations should be abandoned as they have been shown to be based on unreliable estimates of the parameters used.
It is the p%%rpoBC of this chapter to discuss the question of the incidence of abortion and to describe an investigation into the characteriptios of women who abort and their subsequent reproductive performance,This investigation describes some characteristics of
10*
women who are more liable to abortion and indicates the important points in their subsequent reproductive life# As a result women at particular risk can be identified and attention directed to prevention of the special risks of their subsequent pregnancies such as# threatened abortion or premature labour# The Chapter concludes with a discussion on the relationship of the results to the design of studies on abortion and the particular pitfalls which should be avoided in such studies#
;0 of abortion
It is difficult# if not impossible# to obtain accurate information about the incidence of abortion for a number of reasons -a)# In early abortions, before the placenta is well defined, the products of conception may easily be passed with little or no discomfort especially in a multiparous patient, and any bleeding may be mistaken for a menstrual period* There are considerable numbers of women who come to the gynaecological department with menorrhagia, discharge or staining, and are shown to have a *mi#»ed* or incomplete abortion

n
preeenoe of villi aml/or deoiduai reaction in the endometrium when material, recovered at curettage ie examined hletoiogically^b)# A numter of women# particulariv# it is prceumed# multiparae# have an abortion# usually early# which they recognise as ouch; but they are not ill and do not eeek advice*c)# A number of women# with abortions# are treated at home by their own doctors and no record or notification of the event is made#d)* There may be deliberate ooncealment in a number of cases %vhere the woman is not married or where the abortion is criminally induced#
It is thought# in the series described here# where the patients^ fi%*st pregnancies end in abortion# and who have recurrent abortions with no live children# that the information concerning the abortions ie likely to be more accurate than abortion information in general because the %vomen presumably want children# The exception to this may be the abortions which occur in later pregnancy numbers in which the question of induced abortions cannot always be ruled out#
32
Some data on the range of abortion incidente from U m literature is given in Table I* Here the lowest ineidenoe is 7#<% (Tietzo et al# 1D50) and the highest IB*0;S (Mai pas# lûsa)* Mer tig and Livingstone(1044) give a proportion of 1 0 * ^ ending in abortion of 1100 pregnanelea in private practice# Tietze and Martin (1957) found a rate of I7 & spentanooiie and t9f
induced abortions in a sample of white married women of rather superior education* in the United States# Baird (195?) says that *the incidence of abortion relative to births at term is probably 1(% if criminal abortions are excluded* and Stallworthy (1955) gives a similar figure# Whitehouse (1929) in an invest- igation of SOOO hospital and private patients attending for gynaecological complaints found that 1972 of 11*430 patients (1?#2$) had ended in abortion and the Interdepartmental Committee on Abortion (1939) estimated that for every 600*000 live births in the 5 years proceeding their report between 110*000 and 150*000 abortions occurred; of these the Committee estimated that 40)6 were induced#
Probably the most accurate incidence is that reported by Stevenson et al* (1959) from
IS
Belfast* In this study total hospital abortion admiseions wore obtained and to this waa added the numbers treated at home* aeeertained from information from fûiilwlvofâ and health visitors* and from the claims Of doctors for fees for treatment of abortions under the Northern Ireland Health Services Scheme# A most comprehensive sample was therefore obtained and an estimate of M $ 8 # of all pregnancies terminating in identifiable abortions was arrived at# The writers# however# thought that the real frequency was probably somewhat greater than this# This magnitude of abortion frequency is Somewhere about the middle of the ranges shown in Table i # It is clear that there will be a wide fluctuation of rates depending on how a sample is obtained#
emiological characteristics and obstetricper formance .. of wom^n v/ho ,abort
Boureoe of Bata
In this study a number of different sources of data have been used ami these have been collated to make the resultant information as comprehensive as possible# While it is recognised that the main
diffiolilties discussed previously obtain* it is thought that the results given here are as aecurate as possible# By considering abortions occurring in the early pregnancies of women with no live children the points mentioned above are greatly obviâtod since the women are anxious to have a successful pregnancy# In the following series* however* where abortions are noted* it is possible that some of these may be induced and not spontaneous*
Five main sources of data have been used:- Group 3# Maternity Records of v/omcn having first
(7391) or second (53 70) pregnancies have been scrutinised# This group has been used as controls* Their obstetric performance has been compared with women who began their obstetric life with one or more abortions#
Group 2. series of ivomen (911)* obtained from Maternity Records* wliose childbearing life began with an abortion* The performance of this group in the second pregnancy has been compared with that of groups 1 and B»
Group 3* A series of women (104) taken from
a
gyaaeeological reeoNs* where the first pregnancy emlecl in abortion* These women have been foil.owed up for at least B years to determine their aubeequont obatetrio history and to compare it with group 4*
A oerieo of women (S3)* taken from obstetric records# v/ho began childbearing with a normal pregnancy and who were followed iip for a period of 10 yeara# This group hasbeen used aa a normal control for comparisonwith group 3#
A aeries of women (129)# having their 3rd* pregnancy where the first too ended in abortion* This group has been used to illustrate any changes in obstetric performance comparedwith groups 1 and 2#
In the tables# it v/ill he seen that the numbers in some of the groupe are not always complete* Thisis due to certain aspects of the data being incompletein individual cases# These are relatively few in number and this does not alter the main trend of the results*
Group 04

Î 6 *
EpiclemiologAcal. Characteristics
In order to compare women who start childbearing with abortions and those who start with normal pregnancies the factors of age# height and husband*s Social Class are compared first#
Age - Table 2#The group of women whose first 2 pregnancies
ended in abortion contain a higher proportion of women over 30 years than any of the other groups#This group and that with 2 normal pregnancies resemble each other most closely# The risk of abortion is said to be greater among older than among younger women (Tietze et al 1960)# Foetal loss in general tends to increase with increasing age of the mother after 20 years (Shapiro et al 1962) and these workers also showed that women whose last pregnancy ended in a foetal death have twice as high a loss rate in their next pregnancy as other women# When the incidence of abortion is related to marriage duration and age an increase is found in women over 26 years (Table 3)* and the National Statistics for England and Wales show a steady increase of childlessness with rising age at
17.
marriage* ChilcUessnass in this sense includes women who have both abortions and foetal deaths and who have no living children* The classical studies of Louis Henry (1953) showed that* in a society not using modern contraceptive methods - nineteenth century England - the probability of having another child was related to the ago of the woman and not to the number of pregnancies she had already had* More recently McKeown and Record (1957) have shown that the proportion of women becoming pregnant again within Z years of their first baby diminished with increasing age* There is much accumulated data showing the dilaterions effect of age on the reproductive process and this effect is again shown here in connection with women who start their childbearing with 2 abortions (Baird et al 1958)* The association of age and abortion was recognised many years ago by Burns (1843) who stated that ’*advancement in life, before marriage* is another cause of frequent abortion, the uterus being then somewhat imperfect in its action*
Height - Table 4*The features of this table are the differences in
18
stature between the women who have 2 abortions and those in the other 3 groups# one third of women with 2 initial abortions are under 5*1" compared with one fifth in the other 3 groups* At the other end of the scale ZQfa of those women are over 5*4" compared with at least 26$ in the other 3 groups*
Husbands Social Class - Table 5*
This table shows that women in the 2 abortiongroup have a higher proportion in social class 4 & 6 than in the other groups*
Height and social clues taken together are awell recognised measure of physique and general health*A persorfs height is determined by both genetic and environmental factors; to attain one’s potential# adequate nourishment is required at all stages of growth including that in utero* Maternal stature has a strong association with social class and Table 6 taken from the Perinatal Mortality Survey shows the distribution of maternal height within socio-economic groups* The proportion of women under 62" is greater in social class IV and V and least in social class I and II so that there are more short
19#
women as one goes down the social scale* The effect of height and soclo-econqmic group on perinatal mortality is also ivell known and Table 7 from the 2nd# Report of the Perinatal Mortality Survey (1969) aho%ys this clearly* The lowest perinatal mortality is in tall tvomen in Social Cl as a 1 and the highest in small ivomen in Social Class IV and V*
The results of this study indicate that women starting their childbearing with 2 abortions are likely to he smaller and of lower socio-economic status than those in the other @ groups shown*
t a c a i t e ™ Q l . M E i l M â ^ i â « œ i ? a L » â L j i y M m ' U 8 ' e 8 forwomen having their first normal pregnancy and a series of women whose first pregnancy ended in abortion# taken from group B$ are compared by duration ofmarriage (Table 8 )•
Almost half (49$) the %vomen v/ho begin xvith an abortion complete this pregnancy within one year of marriage compared ivith 42$ of women who have a legitimate first birth# The cumulative total shows
20
that there Ib little difference between the two groups at the 6 year period# These findings are not surprising# The majority of women# whatever their social class Conceive within 1 year of marriage (Ilisley 1056) and if abortion should occur it will he completed within the year# whereas if the pregnancy continues the delivery will not occur within the year from marriage#
Obstetric performance in first continuing pregnancyThe next aspect to he considered is how women# who
have started their childbearing with an abortion behave in their first continuing pregnancy# In Table 0 the two groups of women who begin with Ï or Z abortions are compared with 2 normal groups# The particular aspects considered are# threatened abortion# antepartum haemorrhage# prematurity and perinatal mortality#
Threatened Abortion#The table shows that there is more threatened
abortion in these continuing pregnancies in the abortion groups than in the normal groups# This is particularly marked in women whose first two pregnancies both end in abortion suggesting that in these women
21
t h w o is a particular tendency to early pregnancy blooding#
Antepartum Haemorrhage#There is little difference in the incidence of
antepartum haemorrhage in the groups# The figure of 3fl$ found In women having a third pregnancy after two previous abortions is very close to that of 3#0$ found in a survey of single pregnancies byPaintin (1002)#
Prematurity,There is also a tendency for the number of
premature births to ho greater in the women ivith % previous abortion and this trend is more marked in vfomen having their third pregnancy where the first two ended in abortion, Prematurity is therefore commoner in pregnancy when abortion has occurred in the previous pregnancy# To distinguish between prematurity due to the "small for dates" or poorly groivn baby# and the baby that is normally grown for the gestation period# but is delivered early# the weights of babies at various gestation periods in the four groups of cases were examined (Table; W ) # Babies born to women in
22
both previous abortion groups up to 35 ivoeks of gestation seam to be smaller than in the other two groups# This may mean that pregnancies in these groups terminate at an earlier stage of gestation* However# women in their third pregnancy with Z previous abortions have babies at least half a pound lighter than any of the other groups at the 3 6 - 3 7 week period#
Thé proportion of deliveries occurring before 36 weeks of gestation is considered in Table 11#There are more deliveries before 3 6 weeks in both abortion groups than in the normal groups and this is particularly so in the group with & previous abortions where it is double that found in normal primigravidae#
These results show that women who begin their Childbearing life with two abortions have an increased risk of premature labour* The women who have premature labour also have email babies for the gestation period and these babies are therefore *small for dates’# There are a number of possible actiClogieai factors#In some cases a uterine factor may operate# This may be a uterine abnormality which can be easily detected

234
on hystcrography# Another possible explanation la that of Inadequate uterine accommodation which is well documented In animals Reynolds (1959) but very difficult to prove in the human subject* There is a Very constant relation b e W e e n the uterus# on one hand# and the size of its contents on the other* The uterus affects the also of the offsp&^lng and the size of the offspring affects the uterus* Reynolds (1959) noted that# as the last phase of uterine accommodation becomes established the contents of the uterus outgrow the confines of an increasingly unfavourable uterine environment and either parturition or foetal death is the inevitable climax* It seems possible that In this group of women there may be a fault in uterine accommodation leading to inadequate foetal grotvth and premature labour*
It has also been sho^m (Baird I§5.3;) that the incidence of prematurity is related to social class being highest in the# lower socio-economic groupe*This seems to be a factor in women having two initial abortions. It is not the whole answer since a number of women with a good #oeio-economic history also have premature labours and poorly gro%vn babies*
24
Here the effect of age on the reproductive process may be important since these women are on the whole o M e r than those in the lower socio-economic groups* fioM (1061) has shown that some mothers repeatedly have premature babies# The tendency to repeat unsuccessful pregnancies is also higher in women who begin childbearing with one or two abortions. It is of prime importance to monitor foetal growth wlth care during these pregnancies. Although poor foetal growth can be detected clinically the use of urinary steroid analysis (Macnaughton 1067) or ultrasonic techniques (Willocks et al 1067) are particularly helpful in management of these cases. If deficient foetal growth is detected it ia these women who are also more likely to have premature labour,
£LÇ.âBââSjLE2£È8MIZ
The main difference between the abortion and normal groups in Table 0 is in perinatal mortality.In the abortion groups# the rates for one previous abortion and two previous abortions are 43,2/1000 and 38,8/1000 respectively compared with 30,7 and 20,9 in the first and second normal pregnancy group.
25,
flio aaueée of these deaths have been analysed and classified by the method of Baird et ai (1064) and the results are shown in Table 12* In the ease of the group of third pregnancies with 2 previous abortions# numbers only are given since these are too small to make percentages meaningful. There are two main causes for the increased perinatal mortality, file number of deaths due to prematurity and foetal deformity are considerably greater in both the previous abortion groups, Seven of 26 deaths in the I previous abortion group and I of B in the 2 previous abortion groups were due to prematurity and 7 of 26 deaths in the former group were due to deformity. In the latter group 3 of B deaths were due to foetal deformity - a high proportion.
The cause of most foetal abnormalities is obscure. Indirect evidence suggests that foetal defects may be brought about by inadequate intrm uterine environment. Abnormalities of implantation are associated with a high incidence of malformation (Hertig 1967) and it is well known that in many early abortions the foetus or the fertilized ovum are abnormal (Hertig and Rock 1944),
26,
There is an Increased Incidence of foetal abnormality if bleeding has occurred In the early months of pregnancy (Turnbull and Walker 1956), It seems likely that the faulty intrauterine enviroiiiment ivhlch leads to deficient implantation and development with resultant abortion in the first one or two pregnancies In the abortion groups may be present to a lesser extent in the next pregnancy* It may be insufficient to precipitate abortion hut sufficient to Interfere with normal foetal development thus resulting in foetal abnormality.
Performance in labour
The four groups are considered by Incidence of Caesarean Section# forceps delivery# assisted delivery and spontaneous delivery (Table 13 ), There is a slight increase in the number of Caesarean sections in the 1 previous abortion group and this rate of 5,9$ is doubled in the 2 previous abortion group. More forceps deliveries (19,6$) were done in the 1 previous abortion group than in the normal group but this %va8 not 80 in the 2 previous abortion group ivhere the main difference was in the number of Caesarean sections
27 *
performed* Table |4 the indications forGaosarcan section in the third pregnancy of the2 provioun abortion group are given* Fourteen women were delivered by CaeearOan section# In 7 of thoBC (50$) the operation was elective and 0 wereoyer 30 years of age# Other reasons for aeetion wereplacenta praevia CO.# Breech presentation (1)# Foetal distress (3)# Incoordinate uterine action (1) and Disproportion (1)#
These increased operative delivery rates.reflect the desire of the attendant to minimise delay in labour and not to ’take any chances’ with the baby#In most cases where the obstetric history is poor there is an increased incidence of operative delivery#
In the Caesarean Section group the factor of age is particularly evident and 8 out of the total of 14 women were over the age of 30 years. In all but one of these ivomen the Caesarean section %vas elective because of the combination of bad obstetric history and age*The other interesting feature of these women is that only 2 of the total were over 5 ’4" in height# They were almost all medium (S’f* - 5*4") or small (under 5*1")*
28
Thi8 is a highly selected group %vith a large proportion of short women# The combination of small stature# relatively old age and a history of previous abortion make the likelihood of Caesarean Section very great in these immen#
There are still# in spite of the adverse history# a relatively large number of women in botli abortion groups who had a spontaneous delivery although the number is lov/er than in the normals#
Fertility following first pregnancy
In Tables 15 16 the fertility of women followinga normal first pregnancy is compared with that of women whose first pregnancy ended in abortion# In the first table (15) the number of subsequent children# the number of unsuccessful pregnancies over 28 iveeks and the number of women who had abortions only following the initial pregnancy are shoim# The detailed data about abortions are shown in the second table (
Nearly 8$ of women who aborted in their first pregnancy had abortions in all their subsequent pregnancies # whereas no woman whose first pregnancy was
29
normal had abortions In all tbelr subsequent pregnancies* Two women In the first group did carry pregnancies past 28 weeks but these were unsuccessful# Therefore 10$ of women in the abortion grotip had no subsequent successful pregnancy compared with none in the normal group* The number of women in the normal group who hod no further pregnancies after the first one was double that in the abortion group* The total number of women having abortions during subsequent childbearing in the abortion group is 36*6$ compared with 20*5$ in the normal group*
There eeems little doubt that when a woman begins childbearing with an abortion a greater number of her subsequent pregnancies will end in abortion than when her initial pregnancy ended with a live child. Very little information is available on the subsequent pregnancies of women who initially miscarried. According to the data of Whelpton and Kiser (1948) approximately 75-80$ of women having an initial miscarriage will eventually have a potentially viable foetus of 20 or more iveeks gestation. This is not very different from the figure of 83$ obtained in this

so#
study# The remaining 17$ consists of approximately
7}<i who had no further pregnancies, 8$ who had nothing but abortions, and 2$ whose pregnancies continued past 28 weeks, but where the baby did not survive.
Eighty-five percent of women whose first pregnancy was normal had further live children but the remainder had AO more pregnancies# None of the 83 patiente in tills group had any subsequent abortions or premature labours. The fact that 14#5$ had no further pregnancies is unusual. The reasons are not clear.It is not solely an age phenomenon since of the 12 women, 6 were over 30 years and 6 were under 30 years at the time of their first pregnancy# This 50s 50
ratio does show that an unusually large number were in fact older at the time of their first pregnancy and may not have desired or been able to have another child These women were all followed up for 10 years so it is unlikely that they would have another pregnancy# It is of interest here to recall the views of Matthews Duncan (1871) who enunciated what he called his * Law of relative sterility’# This was# of course, in an age of no contraception but it may be still partially true# The law states that *a wife, who, having had
SI
ohlldran# hao ceased for 3 years W exhibit fertility# ham p*;*obably become relatively mterilo; that is will probably Oaor no more children# and the probability inereaoos am time elapses’#
The %voman with repeated abortions does not have difficulty in becoming pregnant but in ’holding on’ to the pregnancy# The findings in thia study support the view of Javort (#957) who also said that fertility wee not redneed in theme women# They do not hear out a oommogily held opinion that women %vith a history of repeated or spontaneon# abortion have a lox/ overall fertility (Donnelly and Locke 1053)# The repeated abortion rate in sterility patiente (((%) reported by simhcig at al ( 1952) is not very much above that in ’non-eterile’ patients#
It does not eoem that there is a general close relationship between abortion and sterility#
The number in the abortion group who aborted again in aaecoseive pregnanciee io oho%m in Table 17# Analysio of these résulta ehowe that there is an
32
increasing abortion rate in this type of woman# In the second pregnancy with one previous abortion the rate was 25$ which is not so very much greater than the incidence of abortion for first pregnancies, in the third pregnancy with two previo%is abortions the rate is almost doubled to and more than half(58.3$) of those women who have aborted three timee aborted again in their fourth pregnancy,
The results show that the main increase in abortion probability occurs after 2 successive abortions and therefore# if abortion prone women are being selected for study it is unwisc to restrict the study to women who have had 3 or more recurrent abortions as suggested by Malpas (IMG), This view is alsoexpressed by the Council on Pharmacy and Ohemistry of the American Medical Association (1940), Ooldaiehcr and Uenigno (1966) and Roberts (1964)# There is# however# a wide scatter of probabilities in the literature (Table 18). This wide range of recurrent abortion frequency suggests that the published material is quite heterogeneous and that for more accurate studies individual control groups must be
used. James (1963) noted the high varlanees seen In the observed distributions and sitggested that the abortion probability ohouid remain relatively constant within each woman; if it had varied thia would have reduced the variance (Edwards I960). It aeeras likely that abortion pi^obabilitiea do# in fact# vary from one woman to another although not appreciably within a given woman# This, of course# does not deny that in a few cases abortions are asoociated with blood group incompatibility and that the probability of ieo-immuniaation increaeea ivith gravidity (Glass 1040)#
Gestation Period of Abortion
The results of an analysis of the gestation periods at which abortion occurs are shown in Tables 10# 20 and 21# About one third of abortions take place before 2 months gestation and 60$ have occurred by 3 months# It seems iiZcely that many of these early abortions may have a chromosome anomaly. Carr (19G7) found that the mean duration of pregnancy for 44 abortion specimens with chromosome anomalies was 85.9 days from the first day of the last menstrual period to the day of abortion* The mean gestational
34#
eg© for 144 abortions with normal chronioeomes vms 106.7 days. It is probable that women who abort early in pregnancy are more likely to do bq ûite to a foetal or ovular abnormality and those abortions which occur later are more likely to be due to some utérine or environmental factor. When therapy is considered it should be remembered that 50$ of women abort after the third month and that the clangor of abortion ia not over by this time.
Women who abort in succeasiva pregnancies show the same pattern except that those having a third auceesBive abortion tend to continue their pregnancy for slightly longer. It ie possible that these women are subjected to more care during this pregnancy in view of their previous obstetric history# and that continuation of their pregnancy for a longer period may be due to this care#
If the gestation period of the second abortion is compared with the first (Table 22) in the same woman, between one half and two thirds of the women will abort at the same time in the second pregnancy as in the first. This means that there is a strong
3 5 ,.
teudenoy for women v/ho are abortion prone to abort at the same gestation period in a subsequent pregnancy.
The relevance of these roBults to the design of studies and the use of therapy in recurrent or habitual abortion will be discussed later.
Interval between pregnancies
The interval between pregnancies in women whose first pregnancy is normal compared with women whose first pregnancy ends in abortion is shown in Tables 23 and 24. Half of the woEien (50$) in the abortion group have a second pregnancy within a year from the time of the abortion and 80$ have a third pregnancy within Z years compared with 17$ and SB$ respectively for the normal women. In the abortion group 92$ of women have had a second pregnancy within 5' years whereas only 73$ of women starting with a normal pregnancy have a second child within this time. The picture is the same when the interval between second and third pregnancies is considered (Table 24).
@6*
beare out; the ( rovJLous finding that women who abort are not Infertile^ Indeed their fertility Is,If anything# Increased# It la not that they are nnable to become pregnant ae enggeated by Qottmaeher (19 86) but that when they do achieve a pregnancy It does not continue to viability*
Age a%id Duration of Murrlage
The incidence of first abortion Is greater over the age of yenro than under ^8 years for all mar&'lago durations (Table 3 ) #. but particularly so after marriage has lasted for over 5 years whan the rate is more than double that under years for the same marriage duration* Guttmacher (H98G) shov/ed that when Contraception Is not practised **There Is a detrimental effect of Increasing age on fertility"* These findings substantiate the results discussed on page #Gsho%vlng the del^eterlous effect of age on the reproductive pro^gess* Guttmacher {#986) has also shown# that age and a prolonged state of matrimony were separate anti** fertile factors* no was surprised to find that the time required for a first conception Increased by seven hundredths of a month for each year of the wife^s

37.
age and almost tv/o fifths of a month for each year of marriage# The explanation of the effect of age and cUiration of marriage on abortion and fertility are no doubt compicK and certainly obscure*
Relation of results to the design of abortion studies
There is so much variation in the design of studies on abortion that the results are seldom comparable*One comrrton error is that ’Primary habitual aborters*# women who have had 2 or 3 consecutive spontaneous abortions beginning with the first pregnancy are confused with ’Secondary habitual abortors’# a term which designates those women who have had throe or more consecutive spontaneous abortions following delivery of one or more ionuature# premature or full-term infants (Javert et al 1949)*
The two main points brought out by the presentwork are -(1) The typo of patient that should be studied and
The gestation period which should be studied*
a . fy.m. of pafcionfe
The classification of patients liable to abortion

38
has given rise to mueh discussion (Goidziehcr and Bonigno 1958). The term ’recurrent abortion’ is frequently used to describe ivomen %vlio have had three or more successive abortion$(e*g* Maipae 1838# Speert #884# and others)* it ia# however# apparent from the present work that immen who have had two abortions are likely to abort again in 40^ of cases and that these %vomen should be termed ’recurrent aborters’ and placed in the ’abortion prone’ group (James 3963)#It is important to exclude women who have had only one abortion# Many first pregnancies end in abortion after which further pregnancies are successful (over SÛ|â) * Subjects with only one previous abortion are therefore a heterogeneous group in which the recurrent element is minimally represented# Subjects who have had one or more viable pregnancies interspersed with abortions (secondary recurrent abortion) are likeivise a mixed group and unsuitable for comparative study# Ideally subjects with four or more abortions are the most suitable group to study as the abortion rates in this group are considerably higher than those with two or three previous abortions and the results of therapy would therefore be easier to evaluate# The numbers of
39*
tliese patients# however# v/liich present at any one clinic are very small*
Threatened abortion may# in practice# be verydifficult to distinguish from inevitable or miseed abortion* Studies on threatened abortion (Colvin ot ai #50; Goldzleher and Beriigno 1058) have not proved very useful in diseriminating between successful or indifferent treatment or supplying information as to the cause of abortion* Much the more promising group in this respect would appear to be the primary recurrent abortion group with two or more previous abortions*
2)* Gestation period to be studied«STirajiqt’OtïAa S:i«mtnaaiUFiit K«»a>anwjw*iu»"(5»
Little attention has been paid to defining this aspect of the problem* In his monograph on ’spontaneous and habitual abortion’ Javert (1957) barely mentions gestation period even although the question of therapy in habitual abortion is widely discussed*
Most workers have commenced studying patients at varying stages of gestation without any raferenco being

4 0 #
made to the gestation period at which previous abortions had occurred. It has been shown hero that one third of abortions take place before two months of gestation and 50/j have occurred by the end of the third month. Furthermore between one half and two thirds of women abort at the same gestation period in subsequent pregnancies. This suggests that initial observations; in abortion studies must be made at the latest by 8 weeks g and any therapy being used should have started by this time. If a previous pregnancy has ended in abortion at an earlier stage than 8 weeks# thisearlier period should be taken as the time by whichinitial observations should be made. If# for instance# observations# and/or therapy# are started as late as the 14th week of gestation (Goldxieher 1964) it is highly probable that these subjects are already naturally selected against abortion and this tends to vitiate the trial of therapy*
A. further point which has to be noted is the timeat which women normally present themselves at theantenatal clinic for the first visit. Scott et al (1956) have given some information on this aspect* They found that# in Aberdeen# 35 6 of women with two living children
41
attended for the first time after the 20th week of pregnancy as compared ivlth of women with one child and 12^ of childless women* Women with the eame number of children attended earlier if their previous pregnancies had ended in abortion or etillhirth showing that patients who have reason to fear complications consult a doctor earlier in pregnancy# This tendency was found $e he amre pronounced among women who had had previous pregnancies ending in abortion than in women %vho had stillbirths or whose children had died auksequently,In spite of previous abortion# however# the average week of first attendance in multigravidae ivith no living children was 12*6 weeks* It is quite evident therefore# that special arrangements muot he made to see cases for abortion studies early in pregnancy before they normally attend the antenatal clinic*
This study shows that when a %voman a tarte child"* hearing ivith an abortion her subsequent reproductive behaviour is different# with more complicated pregnancies and a higher rate of foetal loss than a woman who starts with a normal pregnancy* These women therefore# form a group requiring strict antenatal supervision in all
42 k
.subsequent pregnancies so that the foetal loss can bo lessened*
43.
CîlAPTEli 3,
hormone assays in normal early prej^nenoy;» in abortion and la hydatidlform mole
la compter 2 it woe aoggomted that once a woman had had w o obortiona %vithout any 3.ive ohlldi- en she ahould W placed In an abortion*" pro no group* This ohaptex* %vhlob deal® ivlth steroid aseaya In abnormal early pregnaney# atemo directly from this %voTk* The objeet h w e to dlsoovor the value of certain 8tm old assays In the management of rooora'ent abortion and to agacer tain what happens to the hormone levels In thla type of oame*
The two main storoida to be oonalderod in the flrüt Inatanee a%*a ( U p&'^ognanadlol {Sp prognano' ' G,"" ^Oo.' diol) and (2) ooeW'lol# one of the three elaaoloal 0eBtroge*%e (ooetradlol IZp# ooatrono and ooetriol)*
Both thogge aubota;ieos are excreted In the urine In pregnancy and some Initial observations will bo made on their derivation and metabollem#
4-4" #
1. Progaancdlol
This compound is a ciharaeteri^tic metabolite of proge.atcrono and v-ms Isolated from lato pregruiaey urine by Marrian in 1D29# In 1034 Butenandt and Schmidt domonatrated a connection hetwoon pregsuniedioi m û tyl'io activa hormone progcatcrono by aysithosieing tho latter from progaaiiadiol* _ In 1030 Odell m û
Mar.rino oxtraotcd a combined form of pregnanodiol from pregnancy urine# They noted that the free storeid CO aid be obtained By hyclroiysie of this compound with hot acid# In the oamc year Vanning and Browne ( 1030) isolated the sellable combined form ofprcgnanodiol from butanol extracts of into pregnancy urine# They wore able to show that It v/aa present as the monosodium aalt of prcgnancdlol glucuronic acid#
In 1837 Vennixig et al demonstrated a physiological connection between progesterone and prcgnanediol by isolating the latter from the urine of subjects injected with progostaroac and of normal women in the luteal phaso of thoir menstrual cycle*
The relationship of progoatcrono to prcgnancdiol
in the human and the recovery of urinary piognanedlol
40#
after t W Injection of p r o g w W r o a o will be dlecussedin detail In chapter 4*
O M a w prodnelng pregnanedlol precursor la pregnanev* Orgaw producing pregnanedlol precursor la pregaancy*
A* Ovary* Progesterone la produced by the corpus lutearn la the ovary and ha® been Isolated from this tissue* (Batcaaadt ot al $934g Bhort 1902)#
Placenta# Prcgesteroae hae been Isolated from W m a a placentas (Pwrlmaa and Oercco# #02b)#Tlsauc culture eapei'^lmeats eaggeet tliat It is p%^oducW by the syacytlotrophoblast and most of the pregaaaedlol found in late prcgaaacy urine originates from placental pi'^ogeeterone# Some metEiholiam of progesterone occurs la the foetus (see Ghapter 8)^ and pregnenWlol he$ been isolated from the foetal livw# That the foetua might exwete pregnanediol in the 'urino seemed likely following the finding of this compound la the liquor amni by Klopper and Macnaughton (1959)* Borne of the pregnonediol in the maternal urine in late pregnancy is almost certainly of foetal origin hut eiace foetal death i^eeults in very little if any reduction in pregnanediol excretion in the
46*
In t W maternal the amotmt must be small(Bolomoa #9 66 "* poMonal communication)*
C* Adrenal* A significant, fraction of theprognanedlol normally present In the urine has been shovm to come fromi the adrenal gland# and %o r e la an association between the levels of %%rlnary pregnanedlol and the physiological activity of the adrenal (Klopper ot al #807)* In fact most of the pregnanedlol preecnt In the urlno of poet menopauoel women comes from the adrenal gland*
Pregnanedlol la therefore' derived from prccnrgior $yntW$lscd In these three eltee and the quantitative rolatlonahlp howeea progesterone p^-'oduetlon and motabollte excretion will be dlocueaed In Chapter 4 together with further notea on the metabollom of pr
^egnanedlol exc»'otlon In normal pregnancy
Tahle^^ from the pa%>er by Klopi^or ^ Blllewloa (##63) ehowa the steady rise In pregnanedlol exorotloMi throughout a o M a l pregnancy* in the present context only the levolo up to #0 %meko gestation have been
47
given as this is t w period of prognancy beingparticuiarly stWiod* Those M s u i t s agree iveii with these of shearman ( 1950) using the seme aesny technique*
2 * oe@triei
During pregnancyg ineroaaing amonnte of oestrogew ere excretw in the maternai wi n e end it has been eatebiiahed that the piaeentn is the mein eoweo of urinary oestrogen In the pregnant woman* The evidence for this view is adequately summrioed by Dic!sfaitmy & Trooa (#6#)* Although a large mmber of different oeetrogons are found in pregnancy urine (Brouer #064)# not all of these appear to he manufactured in the placenta and consideration 1® tmually centred on the on onllod cluaalcal ooetrogena oeetrone ocnt%^adloI #70 and oc$trlol# These aubstancee» and particularly ooatriolf^ have been most iatenulvoly studied in practice*
It waa assumed at first that the human placenta# like the ovary# could mynthesiae ocatrogen® from
4*6 «
acotato# S M m o tho conversion of aeetate to urinary ocatrogan had W e n domonetratod in tîio pregnant mare (iVarlKin at ai 1057} arul tlto conversion of radioactive oholeatarol to urinary aoatrogon In a pregnant woman had also been reported (tevlta at al 1902)* It is not poaaihlo# however $ to domonatrato in vitro tho placental eonvorsioii of acetate to ooatrogen# and thQ clioproportionatoiy large amunnta of oostrlol found in late pregnancy cannot be explained by the placental metaholiam of oootrono or oestradlol heaannc the necessary 16a hydroxylation reaction ia inefficient in th.o p 1 a0 onta (hevita et a 1 1062} * Fnrthermere it has become evident from tho atudios of Fraudéon and 8takeman (19 03) and Caoemor (1909) that the foetus ie ossantJLal for maximum oestrogen production*
It aoaiïio true limvcvar# that the placenta does secrete oostriol' aince the concentration of total ooBtrio.1 is higher in uterine venona blood than in maternal arm vein blood (Eoy 10(>2)« The increaaeti urinary excretion of oestrogens during pregnancy closely parallels the increase in placental weight and^ after removal of the placenta the oestrogen excretion
48*
rapidly (Brown #907) # The %)lac0nta produce® the three ’elaesleal’ oMtrogon®# oe$trane$ oe^trWlel #70 and oeetrlol ^ t W laat eompound Being m a n n f a e t w W In the largest amount*
The placenta appeara to be capable of producing
oastriol 1 B J Ü Ü & ii»Siî£S. (Rya« 1»60)» but not by ^yntheela from acetate and eholeatorol* placental perfusion or Inenbatlen %vlth labelled acetate and eWleatorol (tevlt)% ot al #062) did not ehow the formation of oeatrogona; but after perfwelon of term placentae 1^ (Warren & Tlmberlake# #964;Oodard et al #002) and midterm plaeentaa ln.^8,(^q (Balte et al #0B4a & b)# teatooterone and othei^ neutral C^#B aterolda have Bean transformed Into the oorreapondlng oeetrogmia# The eomblnod aetl%^ltles of foetus and placenta convert non oeotrogenlc oterolde to oeatro&ens and this ia on Important oource of oestrogen in prognanoy# (Mltcholl# #907)*
garly In normal prognoney a largo fraction of the amall total amoant of oeatrlol present la derived f»x)m aoureea aueh aa ovarian ooatradlol* Aa pregnancy proeooda this fraction deereasea and at team amounts
50*
to only about 10;% of total oeotrlol production (Siiterlaua UacBmntlii 1900)#
PrmiûBon atiû Stakamon ( #00# # 1D63) first suggest act
that tho foetal adrenal might supply an oestrogen proaarsor to the placenta* fho work of Bauliou and Bray ( ID63)# SiltorA and MacDonald (1065) and dolte et ai (S864i>) oh owed that dohydroopiandroateroiio
railphato (l>IIAB) which is ciranlating in pregnant women
is converted to urinary oostrogeno $ High concentrât*"ion G of DEI AS have heoii found in cord blood ( Simmer ct al #064; {^borloin 1965)# supporting the oaggestloa that this oestrogen precursor may bo produced in the foetal adrenals* The DHAS ivhlch roachon the placenta via the umhiiloal circulation is converted to urinary
oontrogen (Delto ot al# 1D04B); it ie reduced at G""17 anû 10% hydroKylatod mainly in the foetal liverp (little
16a, hydroxylation take® place in the placenta)*
Once aostriol has been formed by the placenta some reaches the foetus# where it is converted into the corresponding 5-nulphato* The oostrlol-s-
aiilplmto formed is returned to the placenta# where it
io# in part# hyclrolyned by the aryleulphataoe ai

51#
liberated oeetrlol lo returned te the foetal and maternal compartment®* In the mother thle oeetrlol I® conjugated ivlth the 3«^8ulphate and glueoslduroEiate ^and excreted* The metahollam of oestrlol in both maternal and foetal eompartments Is characterised mainly by GhaEnge® In conjugation and not in the ateroid moiety (Dlc%faluay ê Benagiano #D6G)#
Haynoa et ai ($964) otudied the metaboliam of ooatrmdiol"'4-G^'^ in %)crf%med footuaea and found that the major motabolitoe were oest%"adiol»»g'^0Ulphate and oeatrono*^3'"aulphatao They were not a$)ie to demonstrate the formation of oostrioi from oeatradiol in the foetus, FurW%ormore# t$ie perfusion of t$ie footo^piacental unit
did not reveal the p&^eeence of any significant amount of oestriol# Ooetradlol# therefore# which reae$%eo the foetuo via the tmbillcal circulation# is not metabolized to oestriol to a$iy extent* Tliere la aiao little eonveralon of owtrone to oeetrlol alnoe# when the Isolated footna we# perfused ivltfi oeetronQ«»3"« oulphate# OEtly % small amount of oeotrlol was isolated (Bmerman et al $965).
Oeetrlol is man%%factured by the placenta from both
02
foetal mid maternal p M c w s o r ® # A foeto*»placental# eeBtrlel""3.«Guiphate cycle Is oatablishcd consisting of footal anlplmrylation and placental doznlphurylatlon (aoaiielemmnn et al# 1060)$ Soma ocstrlol**3"*aulphatc la oxoratad By the feetua In the n&mlotla sac (Troen 1D01g Dlcafaluw at al 18#3; Kat% et ni 1985); It reaches the membranes tvhore It Is hydrolysed# the oeztrlol le liberated# and tranaferred to the maternal and foetal organleoa# The metaWllo pat W a y a of ooatrogon motabollBm which occur in the footo^'piacental unit are haaloally duo to difforonooe in onxyme distribution between the foetue and placenta.
As a M B u l t of the part played by the foetal tWrenal glande in supplying procorzor hydroxy#* dehydroopiandromtorone onlphato (DIIAB) for the placental olalmratlon of oeotriol# much of which is excreted in increasing mmounta throughout pregnancy in the maternal w i n e # the moaaurement of ocstriol in the urine has provided a w o f u l tool for measuring foetal vitality. Maternal u%\6 contriilmtee a relatively minor proportion of the total oeetriol throughout pregnancjf via both
03
noutraJl anü phenolic pathways#
Bariy in normal pregnancy a large proportion ofthe total rvuiouat of oer:;triol lo derived from other aources poooihiy ovarian* with lengthening pregnancy this source decreases in importance# and attore BCp of the ocstriol ie formed in the placenta# mainly from neutral proeorsoro arising la the foetiia ($iitori & MacDonald 1906)* If# therefore# t h w e is any abnormality of the foetus# this may l:>o reflected in the oestriol excretion In the maternal urino*
This is supported hy^ the finding that ail theoostrio.l formed by a woman with an an encephalic foetus appears to bo derived from maternal OliAS primarily via oestradlol (Siiterl atid MacDonald %D00)* When the foetUB in anoncephalic# the matornnl urinary aoatriol operation is one*-tenth of that found in normal pregnancy (Prahdecn and Stakoman 1903)# In these footuaeo tiic foetal cone of the adrenal gland ia small or absent*
Maternal ocatriol excrotion has also been shown to eorrciato with baby weight (Coyle & brown 1903;F rand eon & V> t a hcman 1 i) 00) *
,04
main e W product of the oeetregenG isoej8tr,Wl and many worker® have been interested in the urinat^y entrât of thi® oterold in pregnency (Brown 1956; Zondek â Goldberg 1957; tantore 1808; Kellar et al 195D; F r a W e o n & ztakeman 1D60; Nobkirk at al i960; Kaiser 1060; Berth #eO; Klopper et al #001; Greene ot al 1061; Oorth 1061; Bnnerjen 1B02; Kobkirk & Nileen 1062;Doling 1003; %Vray & Russell 100$; Ooyle ^ Brown 1003)# It i® difficult to compare the valnea obtained by different workers me their aeeay mothode# their criteria for normal p&^egnaney and thoi$^ experimental deeigno have been different# The paper® quoted repeint mean value® during the last month of pregnancy varying fro#^ U m g (%ondek &Oaldbm''g #57) to 32îo$* (Keiiar et al 1059) per 24 hr®. It is not poeaible on the baeia of these publications to apeeify with any exactitude the ohangee in oestriol excretion during pregnancy W t only the extent of variation to bo OXpOOtod* Ae with prognanediol the swinge of exorotioti from day to day in the same patient may bo wide (Kleppor #02)*
55# .
F r0 s 01 & t ytuûy
Method of asoay of urinary pregaonedioi
The aaaay method iiood in the preoont invoetigationla that of Kloppcr et al (1050)# All as a ays w^erc made o« 24 hr# urino collciefelona which vmro performed at weekly intervale*
Method of cipsay of tifJjmry oootriol
In the prooont invootigationo two methoda of assay v/ero il sod# For very onriy pregnancy the classical method of Brorm (1055) was used hut after 12 weeks of gestation the ehorter method of Kloppor A AMlson (19 02) was preferrod# In the latter method the first four steps of the Brown {1850) method# acid hydrolysis# extraction# solvent partition# and hot alkali treatment are used and the ocatrial content of the residue is dotormined by the Kohôr reaction as in the Brown method# Bccamoc in early pregnancy more than 5 m l # of urine has to he used in order to got enough eestriol for accurate 0 p u c trophotometrio mensuroment suf f1cient impurlty remains in the eestriol fraction to produce an appreciable increase in the background colour# A further purification step is# therefore# necessary with early

56.
prognanoy urine. This is achieved by methylating tli0 oeatrloi fraction froui the chromatographic column and then recovering tUo S-methyi other by a secondchromatographi.o step «
Urinary ocstrlol was studied, in three groups of womeifi ( i) IMormally pregnant women (2 ) iVomon with no successfui pregnancy and at least two abortions none of v/hich had exceeded 24 weeks go station* The pregnancy studied ended successfully*• (3) Women who aborted inthe pr egn a n cy stu d i o cl.
Urinary pregnaaodiol excretion was also studied in groups t and 3 and the levels compared with those reported for normal pregnancy by Klopper & Billewicg (lOOS)* Urine collections from women in groups 2 and S wore always started before the gestation time at which any previous abortion had occurred* This io important# since as pointed out in Chapter 2 # abortion tends to occur at the same time In ouocessive pregnancies# and trends of excretion might be missed if collections are begun after this time# furthermore the individuals would then be selected toward continuation of the pregnancy.
57
ResultsCii crv-K3: tc:." .era
P r e g n a noûi o1 exc r etlon
Tables 2 0# 26 â 27 show the mean excretion of pregnaBcdiol with standard deviation in the three groups from 5 * 16 weeks of pregnancy. There is no statistically signifieanfc difference between the three groups at similar stages of gestation. The moan of the " successful two previous abortion" group tends to be slightly higher at each stage than the normal group which was composed mainly of prijnigraviclae. This . suggested that they were behaving# as far as pregnaneclioi is concerned# like multiparous women. Kloppor and ilillewxcx (19 63) showed that primigravld women excreted significantly less pregnanoctiol than multigravldae during pregnancy and these findings support this obserV€ition* Shearman (19 69) did not give sufficient data in his paper but (Personal communication 1968) did say that other date, he had confirmed this view*
Spécial Gases
Two individual cases where pregiianodiol excretion had been measured in the luteal phase of the menstrual

56.
oy€ie before a pregnancy had occurred have alno been «tmUotU Figure 1 * in one woman the prognanecllol level rose te 14mg/24hr# at II week® of pregnancy# well within the normal range# It then dropped to 4mg/24lir# at Î0 weekfô# the normal non pregnant luteal level for this individual# Thereafter it rose steadily until term when the patient waa delivered of a normal child# At no time during the low level of pregnanedioi were any signs of abortion present#
The second subject had a rise in urinary pregnanediol level to I9mg/24hr# at 10 weeks# The lovol then fell to 2#5mg/24hr# at 25 weeks# the normal luteal level for this patient# Spontaneous abortion occurred shortly after# These serial results indicate that even this type of measuroment in individual women may give little indication of the outcome of the pregnancy#
Tables 28# 29 & 30 show the urinary oestriol excretion in the S groups from 5 - IS weeks of pregnancy# Again no aignificant difference in excretion is evident# Figure 2 shows that up until IS weeks some

womoit v4'io are going to abort show a remarkmbly normal aoGfcriol excrotlon# serial roacliiige in these women give little indication of impending abortion#
The gestation period studied in those siihjocts was hotwoan $ anû 16 weeks of pregnancy and little indication of impending abortion can he gained from these studio»* However# in later abortion» some information may he gained by the measurement of oostriol excretion in a similar way in which it lu used to give information in late pregnancy# Oestriol excretion in the urine in late pregnancy has given inf0 $uHaticm as to the well being of the foetus# After ZO vmolio the excretion of oeetriol in the maternal urino gives information about the growth of the baby# Goylc and Brown (1003) studied the excretion of OGstriol in 51 women who were delivered of hahias weighing under 3000g# after a gestational period of more than 3 7 weeks# In this series the oestriol Values wore normal until about IB weoks but thereafter the rise was two thirds of the normal level after 30 weeks# oostriol excretion appears to correlate with the weight of the hahy# a finding also reported by Frandsen and Btakemmn (1060)#

,60
In a patient being studied as a casa of normal pregnancy# oeatriol emeretion remained lew for 3 month» before abortion finally occurred at 26 weeks (Fig* 3)# pasiSibly reflecting the decline in foetal vitality ami eventual foetal death# ■ Pregnanediol excretion dill not fall until shortly before the abortion and presumably remained at normal levels until placental death irrespective of the state of the foetus# Those findings therefore support the contention of Kloppor aiKl Oiilcwicfls (1063) that up to 20 weeks of pregnancy or 00 the urinary oestriol excretion represents oestrogen pTOdnctioii by the tropliohlast from maternal precursors and perhaps the ovary# while later in pregnancy the effects of the foetal production of precursor»# proviousiy discussed# become important#
It has bocir eiiggcsted that differences in horsaonal concentration between oestrogen ami progesterone influence myométrial contractility in the human (Bcngtsson I8G2)# This suggestion ia baaed on iavootigatians of the hormonal coîitrol of the rabbit myoïeetrium and Csapo (1901b) was able to produce in

G*,
aïiimal condition a resainïillng nUsaed alsortAon t m m m of progi^0teronù iûJeotAoîiB at^tor romoval of the ovary and reparation of the placenta# Csapo ( IP G Ia) Bt%Bgont0 û that p r o g e s t e r o n e b y effecting the membrane potential of the myométrial ceil might block the PMpagotion of contraction wavco through the uterus * Kuriyama and Csnpo {lOOO claimed that the myomotrial block MBS most pronounced in the immediate vicinity of the placenta9 supporting the view that the roatraining factor was-derived from the placenta# A second hormonal factor concerned in myométrial activity may be oestrogen. Corner aiul Csapo ( *DGS) in a study of the contractile Byutern of uterine muscle found that the concentration of the contractile protein actomysing could be increased by oestrogen#
K1 o p3>er an<i B111 owIcs (19 Gg ) a t ud i ecl oe s tr Io 1 excretion during pregnancy and suggested that this particular oestrogen might be concerned in the onset of labour#
If# therefore# one measures the excretion of a progesterone metabolite (prognanodiol) and ocstriol in women who abort# the ratio of these hormones present at the time of abortion may be obtained.

Gat
Fow vmrkor^s have Iti fact measurac! the pragnanodioi/ ôcifïtrioi ratio.# Kaiser (tBûù) considered this aspect but made monthly measurements in only one woman#Eioppor üUû îUllewicn (?063| macie some observations on this sulijeet (Pig# 4)# they fourni that in early pregnancy about 100 times as much pragnanodiol as 0 es trio 1 is being excreted # l)y 30 weaüîB the ratio has fallen to about S?î# They u I b q ehserved that subsequent to 30 weeks the ratio continued to fall althoughI more slowly# and by term the amounts of the W o motoholitoe were approximately equal#
frognanodiol/oeatriol ratio in the nreaent study#**###*## VI Ik Ww#'»jw "I «!#.«# wti'U nr
Table© 31# 32 and 33 ©how the ratio of excrotion of liriaary prognanedioi and ooetriol in the three groiipg# Thera are great variations within the groups and this may he clue to the small niimhm's at some weeks of gestation# However# there is no significant difference between the groups#
Tlio r0snit.s shown here suggest that there is no significant difference in urinary excretion of oostriol and pregnanedioi An abortion and An normal pregnancy#
63.
There are many reports of urinary pregnanedioi levels An tlu'oatenod and habitual abortion and reBult» vary greatly* Borne reports ouggeot that a decreasing or constantly low excretion is followed by abortion (borglin IDUdi Rawlings a Krieger 105Oj and others). Other investigators have found pregntmedlol doterminationo of little progsîostic value (Russell et al 19^7). Measurement of urinary pregnanediol in case© of threatened and recurrent abortion has sometime© heon used as a criteria for-'-'^progostin therapy. In somereports therapy has been based on the results of single ae 1-3ay8 (Kupperman et al iGGOj Morgan et al I960).It ie evident from the series reported here that this ia not juatifiahla.
It ia interesting that great variations occur in pregnanedioi excretion in the same patient. This is very evident in the case shown in Fig* f# where thepregnaaodiol excretion fell to luteal levels at 1? weeksand then rose normally to term without any clinical evidence of abnormality in the pregnancy. It could hesuggested that the fall was duo to the failing corpus

0 4 #
lut m m * However# it lias been shown hy ûicsgfaiuayand Bereii (laoi) that the ovarian contribution to the excretion of both oestrogen and pregnanocUoi at this ©tag# of pregnancy Ib very email if indeed there is any at all* In pregnancy variahie amounts of administered progesterone are converted to pregnanedioi (see Chapter 4) and# furthermore# prognanodioi has been isolated from the faeces during pregnancy as mentioned already (ICIopper and Macnaughton 1059)*It ii clear# therefore# that changea in pregnanediol excretion may he due to alterations in mmtaholism and may not entirely reflect progesterone production* It l@ plain from the results that pregnanediol excretion gives little indication of the prognosis,
file same is true of oestrlol measurements up to tê weeks of pregnancy* Thereafter when the production of foetal precursor hecomes evident oestrlol results may he more meaningful# as In the case mentioned when oestrlel output was depressed for # months before abortion occurred at ZM weeks, The findings are In agreement with those of Kloppor and hlllcwicz (lOOS)*A Similar picture is reported hy Coyle and Brown (19631
06,
whea îBeasurcîmcmt of oostriol excretian proved of great value Am aweseimg ttm viability of the footiio im üaaea with compile at ions mtcli m pre-eelampsla and poor foetal growth syndrome# ll^îmol and r/lartln (t004) have also found that ttw ooetrogom osoretiam. lu easea of threatomod abortion oontlmiimg to term wao not oignlfieamtly different from normal hut that la eaaea of Inevitable 'ahortlom the urinary exeroticîn of oastrtKliol I7p and ooatrono was mlgniflemntly lower thmi In the normal groupa probably duo to the troplio- biastie and foetal production being eat off by this tima.
The ratio of prognunodiol to oostrlol in normal pregnancy has been eonoiderod by Kaiser (I960) and Klopper and billmvleg ($06$)# It IG clear from the roDuits of this study that there is no significant change in this ratio before abortion ocours# flere It s h o u M also be remembered that both oostriol and prcgnauodloi are the end results of a series of metabolic prooeesos and may not reflect events occurring at the cellular level# Short and Meoro (IBS#) m û
rkilker (t065) found no change in blood progoatorone levels at the onset of labour and £3ton and Short (3ÛC0) could find no constant relationship between blood
06.
pragestorone ievata ona the outcome of throatonod abortion* Fig* ti #ho%m tho relationship of bloodppogeatcroria lev ole in pregnancy (Bton m û Short 1060) mid urinary excrotioa of progaaooctiol (Eioppar m û
Mli e w i o g liOS# asid Shearman ÎOSO)*
A # Urinary excretion of ûestrogpii and Pragoaoodlol inll5*datidifor2ii Mole
It is well ostabliohed that the urino of patienta with liydntidiforii mol# contain© high concentratione of chorionic gonadotrophin (Hamburger 1043) imt there aro few reports on the excretion of other hormones * rigeam! and Bnrthiaiiit (îOiî) found that seme patient© with hydatidiforra mole euerotocl increased amounts of prognancclioi# some normal and some diminished amounts* : îûiidor and von Umretovmann ( reported that moletisaiio had almost the same concentration of progesterone ao normal placental tissue. Payne (U)4i) fount! a normal excretion of ocstrogens in two casco of hydmtidiform mole and Uingimis and lilngloia ( 1049) reported a similar finding An 10 ecieco* la both these investigations a biological assay method was used#
67.
In five 00009# however# Smith m û Smith ( 1035) fourni eiior0 fcioft of oestrogen which correopomicd to aon^ pregaoiit levels# Brb et al ( 30G1) ropertocl on two cases of hyclatidlform mole a n d found that one patient excreted normal amounts of the three classical eoBtrogena# east rone# o estradiol and ooetriol I m t lev; amouuto of pregnanedioJ, v/liorea$ the other cMcretecI sraall amouûtû of oestrogen *■ the lower l i m i t of the normal rango « hut normal amounts of prognanecUol#
Framloen and Stahomaii (10 04) have reviowocl eomo of the information eoncorning tho excretion of theochormonea In liyûiitlûifùm mole -and have -ûmcvibQû their fiiiclirigo in 10 caeee. They conciiidod that g aa far as prognanodiol excretion was eoncerned only one out of five caoea had an excretion level similar to that found in normal pregnancy# whoroao ail the others had n lower excretion level- like that found In tho non*" pregnant subject*
far as oeatrlol excretion v/as concerned they found that this wae# In general# much lower than in normal pregnancy of the game gestation period* In addition the ratio of excretion of oesfcrlol to ooatradlol
mul oüstrona corresponded to that found in the non- pregnant woman* Theee workers concluded that oestrogen metabolism In cases of hydatldlform mole resembled that found In the non-pregnant woman *
It waa thought that# since there was some confusion In the literature about the excretion of oestrogen» and pregnanedlol In cases of hydatldiforra mole further Information was desirable as this would help to elucidate the hormone picture In early pregnancy there being no foetal component In cases of hydatAdiform mole*
A small number of suitable cases became available and wore studied from this aspect*
Methods of Assay of the Hormones
In eases I and 2 ocatrone# oestradloi and oestrlol were moaaurod by the method of Brown ( îOB'g) anti In eases $i 4 end 5 oostrlol was measurod by the method of Bpom% ami Cay le {#003) #
Prognonedlol was measured by the method of Kloppar ofe ul (IS5G)*
Gaee #flifâ patient was a priraigraviila aged 21# who was
admitted with vaginal bleeding at the 10th week of pregnancy♦ fhe îlogberi test was positive in a dilution of U ÏOÛ but negative in $?200* The uterus was enlarged to the expeotod at 14 weeks ofgoetation an# continued to grow more rapidly than normal# Intermittent hlcacîiiitg continued and a mole was imsaed at 17 wooks*
Game 2mThe patient was a primigravida aged 24 years# who
was admitted at the I1th week of pregnancy with vaginal bleeding# The utoruu wao of normal also for the gestation period# The iloghen teat wan positive in a dilution of I g 100 and negative 1:200# Intermittent, bleeding continued and a mole was pnaood at IP weeks# Three weeks later the patient was ro-admitted to hospital with severe vaginal bleeding# flie uterus was hiiIJcy and soft and a blue vascular nodule was present ill the lower vagina# Froaen sections of cwettings and Qf the nodule suggested chorio-carcinoina so
70,
hyotoroGtomy cmd excision ef ' nadiiio were pur formed.At oliquation two thuqa iutoin qyoto vioro found rsoaouring ? x 5 n 4cm® and B x 7 u lorn, roppectivcly* Histology of tho utorus and vaginal module uuggastcd that tlio condition was ohorlo-adonomn doo.truoiie am! not Churio^onrcAn m m * Follow up over the next tea yaaro ohowod no evidence of recurranee and the titre
of gonadotrophins in the nrino romainod noraai,
SSiiLlTiiQ patient ivaa aged 2 6# para 2 # admitted at
l‘B weekG gestation with yaginai bleeding, flio uterinealso vaiB -normal for the gestation period. The pregnancycontinued with intermittent bleeding until tlio 10th
when the blood proaoure rose to 200/ $20mmUg and the urine contained 12g/l of albumen, Spontanoouo delivery of a hydatldlform mole followed the aente rise
in blood proaeuro. The patient has since had anormal prognanoy.
;aeoThe patient was a prlmigravida aged %B years# who
wao admitted at SO woolts of pregnancy with vaginal b l m é i n g * The utoruB waa small for thcî gestation period#
It
TilO llogbep tfôsfc wao weakly piisitivo Is 10 dilution# later mit tant bleed in# eontlnuW and a mole was paesocl at 20 waeke,
0a©0.6flm patient waa aged 26# para 2$ and was admitted
with intermittent vaginal bleeding at It weeks gestation, The uterine sisse waa normal for the gestation period# flte Hogbon test was positive Is 10 dilution hot negative Is 100 dilution# intermittent Weeding continued anda mole was paeoed at 16 weeke#
Rerolto
fahlo 34 B h m m the urinary excretion of hormone© in the B eaaea# Fregnanecliol excretion and ocetriolexcretion were measured in all oaooo and the three ^olnooioal^ oestrogono and prognanodio1 in two oubjocto#
PfQgnangdioiIn Q t m m î and @ the levels are higher than in
normal pregnancy wlieroaB in Cases 2# 4 and B the levels are much lower than normal and indeed approximate more to thaoo found in the non-pregnant state#

72
GrxitrlOl0(11S»
Oaeo I* The levels of oeatrlol exorotlon t^emalned normal until N lyooka thereafter flattening out In a manner found In Intra uterine death already mentioned*
Gaae 3$ Only a single reading at # weeke was available* This was lower than normal but consldei'ably higher than those fmmd In Caeos 2 and 4 %vWro rooult# wore available at 19 %veoka#
Cnees 2# 4 and 6* The levels of oeatrlol excretion in these oubjecto wore much below the nojrmal for the gestation period and wore almllar to the levels reported by Frandocn and stakemen ($004) fo%* hydatidiform mole#
r,Bjslïfc.=!k*T-s*fe‘»SAa!-s;'ÿr'4.5si!ss4tt
The levels of these {eWroldo tended to follow those of oeetrlol# being high la Caae I and loiv in Case 2$ The oeetrloliooatrone plus oestradiol ratioVaried from i to 4,7*
A0 has been mentioned before it aoema almost eartain timt the plaoenta produooa progesterone and
73,
In Case I Ml thin ©orics# the lovelB of oostriol romainod high until the letli week of pregnancy# while tUoBii of pguignanedioX were above those of normal oubjeoto nt the same goatation period* In this subject at iaaet until the 16th week# the ooBtrogen production v/ao v/ithin normal limits in spite of the absence of a foetus*
It 0ooriK> posalble> therefore to have normal oestrogen production in the first B month0 of pregnancy without - a foe to** placent ai circulation*
The oestrogen level might be duo to inoroaocd production by the ovaries# which may he cxcosaivcly stimulated by the largo amounts of gonadotrophin present# This seems doubtful# however# oinco from the data in fable f of the paper of Frondeon & Stakeman (1904) fable 35) the lovol of gonadotrophin was lowest in the patient ivith the higEieat level of oostriol# In the present oaoeo there vms no correlation between the level of gonadotrophin# as measured by the flogbon tost end the hormone excretion# or the presence of theca
74.
lutoiii oyats m û the oxcrstion love,I* The hormone may therefore# either he produe od l>y the ovary or hy the trophoblaot# pooolhly hÿ a different motaholie pathway from that foimd in normal pregnancy# and further vmrk to try to elaoldato this problem la roported in Chapter 0.
2
75.
CHAPTER 4.
The Conversion of Progesterone to Pregnanediol
IB chapter 3 .i, when the origin of pregnaneclioi was discussed the relationship of the amount of progesterone represented by urinary pregnanediol was mentioned#Almost invariably estimates of urinary metabolites aro made to obtain inforaiation about the production of the original hormone. For this purpose it is useful to know the ratio between active hormone and inert metabolite and it is essential that some fairly constant relationship should exist between the two to make results meaningful# Hytton & Loitch (19 64) rightly remark in their book ®The Physiology of Human Pregnancy^ that *Mt is curious that so much research has been expended on polishing the technique for estimating pregnanedloi ami so little on discovering how faithfully it is likely to x^epresent its parent hormone’* # It was with this admonition in viev/ and also because of the rather vax'ied results reported in chapter 2 that it was decided to investigate further the relationship of progesterone to urinary pregnanediol.
76.
Percentage recovery of injected progesterone as urinary pregnanediol
This figure has varied from report to report.XThe foiiowing are some figures from the literature#
7.9^ Qiiiiligan and Rothchild ( 1957) ; 9- 16)& Sommerville and Marri an (I960); 20 6 Klopper and Michie ( 1956) ;approx. 20?S Guterman ( 1963); 20-40J4 Davis and Plotz(1957) and 30-35^ Davis and Fugo (1947), Some workers have also reported that the percentage recovery of administered progesterone as urinary pregnanediol is higher in pregnancy than in the non-pregnant state (Venning and Browne (1940); Sommerville and Marrian (1950); Guterman (1953).
In contrast Pearlman (1957) using tritiated progesterone found that the conversion of administrated progesterone to pregnanediol was lower in the pregnant suhject (6-15/0 than in the oophorectomised/ hysterectomised woman (14-27$)# This latter finding seems more logical ,since some of the administered progesterone could be taken by the foetus and/or the mother whereas in the non-pregnant woman it would overload the system giving rise to increased conversion
77.
and excretion of pregnanediol# It also seems true that the exogenous progesterone can bo converted to pregnanediol in the absence of a uterus and/ef ovaries^IÏ11X ton (1040 ) and Gut or man ( 10 53 ) •
Present Study
In view of the varying résulté obtained and relative lack of information on the conversion of progesterone to pregnanediol it v/as decided to investigate this problem further using tritiated progesterone to study any difference in the conversion betv/een normal, and abnormal pregnancy and to determine whether the conversion values v/ere related to abnormalities of pregnancy# especiaily early pregnancy* Outorman {IS53) had suggested that there was a higher conversion of progesterone to pregnanediol when a Viable foetus was present•
Metabolism of progesterone
Pregnanediol is considered to be the principal urinary metabolite of progesterone# F/eist et al (1958) and ih no report has more than 40> S (average 2i>%) of administered progesterone been converted to pregnanediol. When progestérone was injected Davis et al (1956)
recovered 28.54;;% from the faeces in the next 10 days# t^egjligable amounts are secreted via the skixi (Davis and Plot 15 1057) and although no 0^ could he detected following administration of 4-C^'^ progesterone Og was found in expired air after administration of 2 progesterone ( 18-19;^ In 31 hr.) Davis and Plots {1958), This final report illustrates that the side chain can he broken off in mctahoiism with the possible formation of androgens o*g* androsteuedione# andx^osterone and/or a tiocho1ano ion c•
It has been reported that a large amount of progestox-’one is stored in maternal fat (Kaufman and Zander# 1950) and Plotz and Davis (1957), The latter workers showed that after 12# 24 and 48 hr# 17# 7# 33 #7 and 1D#6A' respectively of injected progesterone was found in maternal fat either as progesterone or its motabolites#
Until radioactive px^oge star one could be administered in the form of tritiated progesterone other urlnax'y metabolites of progesterone could be detected only with difficulty# The use of labelled px"ogestex^one in humans has shown that this hormone can also be metabolised to
7D.
Compoimds which are more polar than pregnanediol.Chang 0t al (1960) found that 2% of the administered dose appeared in the polar fraction and Contractor and Pearlman (1D60) found 0.6 - 2% of the administered dose to appear in the ketonic polar fraction. Since these latter workers used progesterone labelled with tritium at C-10 and also hydrolysed the urine with acid it is likely that many of the polar compounds were destroyed and the figure they quote is therefore much smaller than the true conversion. Greater conversions have# in fact# bean reported by Darkness and Potherby (1063) who found about 6^ of the administered dose in the polar fraction and by Romanoff at al (1963) who found a value of 6 - 7fi. The results of Darkness and Fotherby showed the ketonic fraction to contain a greater proportion of these polar metabolites than the non- ketonic fraction.
It seems likely that a large proportion of the polar fraction is composed of metabolites with an oxygen function at position 6# Kamyab and Fotherby# (1963)# and James and Fotherby (1965) have shown that the administration of progesterone is also associated with an increased excretion of these 6-oxygenatod metabolites.
8 0 .
A number of compounds with a hydroxyl group at position 16 have also been isolated from urine* These compounds arise partly from l6a-»hydroxyprogesteroao#This compound has been isolated from corpora lutea and placental blood after normal delivery (Zander et al 1862)# and also from the peripheral metabolism of progesterone or its metabolites (A^'otharby 1864) *
Therefore# although conversion of progesterone to a number of other metabolites occurs in the human and many of these metabolites can be isolated from human urine following administration of labelled progesterone# pregnanediol is the most characteristic metabolite and has been most commonly used as an index of progesterone production. The radioactivity recovered as urinary pregnanediol following intravenous injection of tritiated progesterone gives a measure of the conversion rate of progesterone to pregnanediol*
The method used for the estimation of pregnanediol. v/as that of Klopper et al (1866). It is considered specific for 6j3-pregnanc-3a-20a-diol since the final purified diacotato is only slightly less pure
I.
U u m the diacetata of the pure compound (Klopper et ai I055| Coyle et al (1956))* The method Involves acid hydrolysis# toluene extraction# a permanganate oxidation step to remove the--decomposition products of pregnanediol following acid hydrolysis# chromatography on a n 'alumina column to isolate the free pregnanediol# acétylation and further chromatography to isolate pregnanediol diacetate# The final assay is by colour development with sulphuric acid« No correction was made for extraction loss # all studies were comparative am! losses occurring during the procedure were known to be constant within the overall error of the method.
Measurement of the radioactivity present In the urinary pregnanediol following the intravenous injection of progesterone
The radioactivity contained in the pregnanediol diacetate produced was measured in a Nuclear Enterprises single channel liquid scintillation counter. The efficiency recorded when tritium was measured was 22*5;à# The radioactivity was measured in counting vials of Î 8 m 1# c a p ac i ty #
The scintillation fluid used consisted of:-
^2.ô
4g, 2#J DApheByloxaaoXfô (PFO) txnû 0,05g# p-bls[2-(5- phenyioxaxa.lyi) 3 benzene (POA^OP) .litre of toluene(Seintillation grade)#
The components of the scintillâtion fluid were all pur chased f rom Nueleav En t er prises.
To remove any errors in radioactivity measurement cUve to the background urinary material extracted g a sample of urine obtained prior to the radioactive injection was also extracted. Since the dally percentage recovery of injected progesterone as pregnanediol falls off marlcedly after the first two days # larger volumes (ISO mi.) from the 3rd* # 4th and 5 th days had to be extracted to give sufficient counts for accurate measurement#
pTiplleate analyses were performed in all cases and cluplicato samples were also extracted for direct measurement of the pregnanediol present#
The overall findings are expressed as results under the following headings -1), The absolute amount of pregnanediol excreted each
day in mg/24 hr. pregnanediol diacetate*

2). The amount of radioactivity recovered each day and hence the percentage of tritiated pi^ogesteroiic injected ivhich ia converted to pregnanediol and excreted on each of the 6 days*
The amount of radioactivity loft in the syringes and ampoule» after injection was measured in a number of eases# The average amount remaining in these was 1 #19*10 (sn t 0.20) in Î4 cases# This means that an average amount of 98#8lpc was injected# In view of the very small error involved results were calculated on a basis of 1O0?4 injection of the progesterone#
R esults
The patients studied ?/ere separated into fouri main groups: non-pregnant# early pregnancyt late pregnancyand women with abnormal pregnancies# One hundred microeurioa of tritiated progesterone dissolved in ethanol were given by intravenous injection into the antaciihital vein and urine collected in 24 hour periods for 6 days after the injection#
The daily percentages recovered as pregnanediol on
84 «
the first 5 days are tabulated in Tables 36# 37# 30 & 39#It is clear that the majority of the radio-
active pregnanediol was recovered in the first 24 hour urine specimen after injection of the labcliod steroid* The excretion of radioactivity fell to very low levels by Day 5# Tabic 3 6 Illustrâtes the recoveries in the non-pregnant subject. In Casa No, 3, it should he pointed out that the probable reason for high recovery on Bay 2 was due to post operative renal retention.On Day urine volume3 creatinine excretion^ and pregnanediol excretion were all sub-normal• The percentage recovered as pregnanediol in the group of non-pregnant subjects varied from 5*69 - 14,2 1% - a fairly wide scatter*
Table 3 7 illustrates recoveries for subjects in early pregn ancy *
Case 11 had tritiated progesterone injected into the Uterine muscle Just before hystcrectomy and the first 48 hour urine sample was pooled* In the 11 cases of apparently normal early pregnancy studied it can be seen from the table that the total percent recovered as urinary pregnanediol varied from 6*8 1 - 15*14, There
86,
appeared to be no difference from the 7tb to 19tb week# the amount recovered depending on the Individual# In Gaee 11 where an Intrauterine Injection was performed the percentage recovered was 10.79 and fell within the range repoa^ted after Intra venoue Injection#
Table 38 ebows the conversion in the late pregnancy aubjecte (all three are in the last 2 iveeks of pregnancy)# The total percentage recovered in these women varied from 6*74 - 16#36 and again it appeared thtit any difference seemed to depend on the Individual rather than on the stage of geatatlon#
Table 39 includes a number of clinically abnormal Casas showing their conversion over the five day period#In this group the percentage recovered as m'inary pregnanediol ranged from 1*42 to 9*90 (Case 22 had only a three day recovery period but assuming that she Aiad a similar fall in percentage recovex^y as is present in all other cases the total recovery should hardly be influenced)# Although there is a wide range in the total percentage activity recovered as pregnanediol the average In the abnormal cases appeared lower#
80#
Table 40 iXiustrate© the variation between thefour groi,ipo# Testing for significance by the testthere was no significant difference between the non- pregnant^ early pregnant and the late pregnant subjects# Howeverp there v/as a significant difference between abnormal pregnancy and the other three groups and it seems likely that there may be some altered metabolism of progesterone to urinary pregnanediol In these abnormal cases, Further work on this oubJect will be described in chapter 6,_
Specif i c A c fc ivi ty o f t h e p r egn a n ed J. o 1 i so 1 a ted
The specific activity of the pregnanediol diacetateisolated from the urine was calculated for each ofB urines# The pregnanediol excretion in jug/24 hr# wasdetermined as pregnanediol dlacetate#
( radloactivity in pregnanediol diacetate )( Specific Activity muc/24hr# % 1000
mg, pregnanediol diacetate/24hr# )
Table 4| illustrates the daily specific activity of the isolated pregnanediol diacetate. The results may be separated into two main groups. The first group contains all the patients whose specific activity of
o 7 #
pregnanediol diacetate is above 460mpc/mg on the first day and above ïüOmpc/rng on the second day* The second group contains the remainder although there is possibly a small third groi%p present which does not fit either category *
The n o p r e g n a n t cases all fell into the first group together with 5 out of 11 of the early pregnant cases » No late pregnane 3 or abnormal cases were in this group. In the second groupp all but one of the late pregnancy cases were présente The third group contained a mixture of early pregnancy and abnormal cases•
Since the radioactivity^ excreted in the urine as Pregrianedid xvab aImost constant^ i• e* there xvcre no significant differences in the percentage recovery between the early g late and non^pregnant subjectsÿ when the pregnanediol was low - the non-pregnant and early^ pregnant women - the specific activity was high. Conversely, in late pregnancy, when there was an increase in the pregnanediol excretion the specific activity was low*
These results do not suggest that specific activity

88#
per se gave any particularly useful additional information about the various typos of pregnancy studied#
conversionaxcretwoman
The results are shown in Table 42*
The percentage conversion pregnanediol fell within the usual range for a non-pregnant subject hut the specific activity was extremely high due to the very low absolute amount of pregnanediol excreted dally.
Excretion hy same patienta non**pregnant and pregnantw *** 1IMwiwiii'u I u * m iMW#Mumiwwiwiiowmmniiwtwioei wM**wmn**'.itwii,
Two patients were studied in these two states to determine whether pregnancy changed the conversion in the same individual*
Cases 5 and 21 were the same patient in the nonpregnant and then the pregnant state - before abortion* Similarly Case 4 and Case 8 were the same patient in the non-#pregnant and then the pregnant state. Direct comparison of these results is shown in Table 43*
When both women becmma progaaat the radio0 Ct ivlty rcoovox'W a$ pregnanediol dropped olightly and ÿ sli'KTü the at solute amount of progaoaedloJl rose with pregnancyÿ In both ooocs the apoclflc activity Uocroaood*
DiùcusAion*S:iV•lXirJ’■s‘:MllJ*StS*»IS,!SiH
The average amount of radioactivity recoveroU as urinary prcgnanodioi over l> days after iotrnvonouo injection of tritinted progootcrono in nomoi non** pregnant and pregnant subjects worn lOÿl with a range of 6*221% one #0*68^# This roauit compared favourably with previous reports Quiiiigan & Rothahiid (#057)$ Bo^worviiie & Marrinn (#050) nnd Gutormcn ( $983) aitho%;gh not 06 high m Davis A Plotz (105?)& Noweverp contrary to Ve*%ning and Browne ( $040) and Bommorvilio and Wnrricn ( 1050) ivho found highcr levelo of rocovery in progooncy than in non*pregnancy# and to roarimon ((067)$ who# oonvoroeiy» found higher levela of recovery In non- pregnant vfomen# this work cuggoato that there la no difference in the percentage recovery between the pregnant# (early or late) and the non*prognant women * Kloppcr and Miehic (1800) also found no difference in
oo*
recovery# ÎIcmce It would appear that the proseoco of a foetus does not make any difference to the percentage of progesterone that is converted to pregnanediol# In one case# in the present study# in which abortion occurred the percentage recovered as pregnanediol was low# This result is inaccordance with the view of Outerman (1053) who euggOBtod that the percentage recovered as pregeanedioi was higher whon a viable foetus was present* It is clear that this matter io not finally resolved and further work is required to clarify this point# In contrast to this# patients with abnormal pregnancies# for example hydatidiform mole and pre-eelamptic toxaemia# toncl to have a lower percentage conversion (average 5#32#) # The production of progesterone in those cases is lower than normal since the absolute urinary pregnanediol levels tend to he low also* In the hysterectomised patient# (Table 42)# the percentage recovered as pregnusiodioi was within the normal range and this confirmed previous reports that the uterus and/or ovaries were not necessarily required for the normal conversion of progesterone to pregnanediol# Romanoff (1002) in fact# found t4% of administered progesterone
91 *
Converted to urinary pregnanediol in men.
Although a viable foetus was delivered in Case 30# an extremely^ low conversion to urinary pregnanediol (0#4%^) p and absolute urinary pregnanediol exçretiori (2•5mg/24hr0) were found# neither apparently inconsistent with a successful pregnancy* It seems likely that the metabolism or excretion in this case must be different, The total urinary radioactivity In this case was only 1 @ on dàÿ 1 suggesting - (I) alternative excretion route (2) some alteration in metabolism or (5) increased maternal fat storage or of ^bound progesterone « (Table 44)*
fhe first suggestion is quite possible and is supported by the work of Klopper and â^lacruiughton (î95i>) who isolated pregnanediol from the faeces in late pregnancy. This pregnanediol was in the free form ami these workers suggested that the alimentary excretion of pregnanediol might depend on hydrolysis of its Conjugate in the gut, The '- also suggested that the possible alimentary' lose of a variable proportion of the pregnanediol production of the body might explain the considerable variation in urinary output pregnanediol

92#
as in the case cited.
An alteration in metabolism may be found in liver disease when disappearance of progesterone from blood plasma takes much longer (Patrini 1964)# probably duo to interference with the conjugation reaction-of pregnanediol (Rogers 1956)# Since the urinary pregnanediol excretion was low# the formation of progesterone was probably low and hence the increased requirement for exogenous progesterone which may bo ^hotmd® to protein for transport and readily available# Hooker & Forbes .(1949)# or stored in the fat# Kaufman & Zander ( 1956) and Plotss and Davis (I9S7)#
The first 24 hour urine specimen after the intravenous injection of progesterone contained most of the labelled pregnanediol but over the next 4 days measurable amounts were still preao.nt. These findings are similar to those of RothehiId (l§53)# Harknees & Fotherby (1063)# Davie & flotss ( 1068) who showed that after a sharp rise there was a levelling off in the cumulative pregnanediol recovered 48 hr# after intravenous injection# Van do Wiolc et al (I960) reported that most of the pregnanediol was excreted in the first
9@.
!2 houTB v/lth some throughout the next 36 hr, and Quiliigan & Rothchild (19 5?) found that the majority v/as excrctofi as early as 4 - 12 hr, showing a very rapid metabolism to pregnanediol glucosicluronate*
Sommerville & Marrian (1960) detected a ’priming effect^ i.e. a stepwise rise in excretion of pregnanediol following administration of progesterone# which required the presence of a uterus* However# the results of Roth child { 195*3) gave no indication of this priming effect in the post menopausal female and this was later confis’med by Marri an et al (19 54) and Klopper & Michie (19 56). In the present study only the first 5 days urine were collected and therefore this effect was not studied.
The results discussed in this chapter are generally rather inconclusive and a much larger series of eases would be required to obtain more concrete results.The change in conversion of most interest is perhaps that obtained in hydatidiform mole. It was decided to examine this situation further and the results of this Investigation are reported in Chapter 0.
0 4 .
Progesterone metabolism in the human previable foetus
When the metabolic pathways to and origins o.f pregnanediol were being discussed earlier in this thesis allusion was made to the foetal metabolism of progesterone# and foetal production of pregnanediol as a possible factor in altering pregnanediol excretion in the mother# This chapter describes work undertaken to ascertain the role of the foetus in progesterone metabolism and the foetal production of pregnanediol#
Introduction
There is good ovidenae that the foetus receives'
progesterone from the placenta and metabolises this hormone# it had formerly been thought that the foetus itself was a source of progesterone wh en Forbes (1956) found that the level of the hormone in the umbilical artery was higher than in the umbilical vein. however# the method used (Hooker and Forbes 1947) was nonspecific and it was later shown that 20a-dihydro- progesterone (%Oa-hydroxypr0gn-4-en-3-one) had a higher potency in this test than progesterone (Zander et al 1958)#

95
Ruimebaum and Zander (1962) showed that the .level of progesterone in the nmhilioal arteries was conoiderahiy .lower than that in the umbilical vein # whereas the concentrations of 17a-hydroxyprogestorone# 20a and 20p-dihydroproge6terono were higher in the arteries.This v/as confirmed by Oroig et al (1962) who showed that the rati^ of progesterone in the arterial to that in the venous mmbilical vessels waa 1$1,8 and this finding was substantiated by Van dor Molen (1963) and ilarbet et al (19 64),
■ In view of the differences in progesterone levels In the umbilical vessels (see Fig, G) it seemed therefore likely that the foetus metabolized some of the progesterone it received from the placental circulation,
Solomon at al (1965) perfused foetuses of gestational age 1 7 - 2 1 weeks with p r o g e s t e r o n e - 4 - ^ a n d isolated pregnanediol from the liver. This compound contained approximately 25/-S of the radioactivity perfused into the foetus. It was concluded from this and later work# by the same group (Bird et al 1965)# showing the pregnanediol was in the form of the sulphate as well as the glucosiduronate# that the function of
9 8 ,
the foetal liver was to produce reduced metabolites while the adrenal gland of the foetus at mid term utilized circulating progesterone for the production of corticosteroids.
Present Study
Materials and Methods
Several experiments were performed. The results of two# indicating the short and long term metabolism of progesterone are described,
O * A foetus of 18 weeks gestational ago was obtained at thorapautic termination of pregnancy, A formalin soaked wad of cotton wool was placed over the urnbilical cord to prevent spasm of the vessels during cannulation, Progoatarone (2pc)dissolved in two drops of alcohol and 1ml, of 0.9JI Sodium Chloride solution was injected through the umhilical vein. The heart stopped 14 minutes after the injection, The foetus was dissected at once# the organs removed# weighed and stored at -20^ until extracted.
97.
A foetus of 18 v/eeka gestational age was obtained at therapeutic abortion as in experiment 1*Group Op ilh positive blood diluted 3s I (v/v) with
dextrose in Ringer solution and oxygenated by bubbling oxygen through it# was used to perfuse the foetus by a modification of the method of Westin et al (1958). The composition of the perfusion fluid (pH 6.6) wasi glucose# 400mg/ 100ml| Oxygen saturation; Cl GOm-eqiiiv/l • and COg content# 10.6m-equiv/i# After cannulation of the umbilical vesse3,s the foetus was immersed in B% dextrose in Ringer solution in a perfusion chamber completely filled with solution. In this way preasure changea due to increaa# or decrease in blood volume could be detected on a manometer. The blood dripped into the umbilical vein at a rate of 5 - 20 drops/min.
Progesterone ( lOpc) vms injected and the arterial outflow collected for 3 x 16 mln, periods. The blood was centrifuged and stored as in experiment I* The accompanying diagram^ Fig# 7# illustrates the appearance of the apparatus used in the perfusions.
1■v-i .iV "
88,■l\
The identification of radioactive metabolites and extraction procedures used have already toeen pishiiehed '■(Greig' and Macnaughton 1967) and will not ho described hero in detail* A flow sheet is appended# Fig# 8 which shows the outline of the procodures.uscd*
asauife
ati±:i!£l,f:.go&gaiigy,a»«.
After 14 min# 40% of the radioactivity was present in the liver and Z*4% in the adrenals# . In both the liver and adrenals the radioactive material extracted was mainly * free * steroid# Bt% â 82#6>t respectively* After hydrolysis w'ith the enzyme preparation from j atella yul. at,a.# which contains mainly B-gluouroniclase, OmB% of the conjugated material in the liver and QB% of that in the adrenal was extractable*
The identification techniques showed that the radioactivity was present mainly as 20a-dihydro- progesterone in the liver# whereas almost half of that in the adrenals was present in the form of polar material# (Table 45)# A similar distribution of

9 9 ,
Compound0 was fotmd in the 'eonjugatod^ fractions(see Table 46)« the principal conjugated steroid inthe liver was pregnanediol whereas the adrenals containedmainly polar compounds* Table compares thepercentage of free and conjugated steroids in the liverand adrenals 14 min* after injection of [4- ' Cî)progesterone*
SI.MAMcMx4M-iCeseB.t_An foeMi„MMuea.^affcer gJiâ^JliJlisîASij2£2imst.gi^^with [4-* ol prog eat erono for 46 min*lirai»*. gat t «WKtia#;*# (»ï***ik.-îï «Sat's*
The total radioactivity recovered from the foetuswas 15$3f&*
The compounds detected in the free fi' action are shown la Table " ** The main compound in the liver was pregnanediol and this was confirmed after recrystail- isation of the diacetate to constant specific activity* The Table shows that in many cases# progesterone was still the major ’free* steroid# particularly in the blood t where it accounted for 06# of the radioactivity In the first 16 min # sample and 51)4 in the 30 - 45 min* period* Pregnanediol was found both in intestine and liver ami a little radioactivity was present as progesterone in the liver* In the plasma samples#
#00,
$8 the omouat» of progesterone and polar material deoreaoed the amount of 20a-dlhydroprotestorone# the prlnolpal Initial metabolite of progesterone# rose#In the liver and plasma# the polar fraction separated into several oompoundo one of which was probably I6a hyclroxyprogoBterone and another probably ## hydroxyprogestorone*
Therefore the main * free’ steroid in the liver in the first experiment was 20a-dlhydroprogesterone and In the second experiment pregnanediol - see fables 4lJ ê 4S In the adrenals most of the radioactivity was present as polar material in both experiments#
1 senssion
These experiments show that a large proportion of administered progesterone was metabolised in the foetal liver and this accords with the résulté of other workers (Solomon et al 196?)# liver deactivation of progesterone has been reported in vivo (Forbes & Hooker 1949) although not jln yi(;ro. Engel (1044)# It is not really surprising that the liver is one of the main sites of metabolism in the foetus since# in the adult a large proportion of the metabolites of progesterone have been
Î O I
cleteotecl in the bile (Sandberg ê\ Slaunwhite 195S|
WeiBt ot al 1958), Zander (1981) also injectedprogesterone into the umbiiieal vein at termin
ation of pregnancy and found that the majority of radioactivity vms present in the liver#
In both foetuses investigated the percentage of conjugated steroids v/as much loss than that of free steroids (liver oxpt# 1# 9 fo free; expt# 2# free)#In cxporiment I# of the conjugated material in the liver and adrenals 80 5 and 74% v/as hydrolysed by the enzyme preparations used# In experiment 2# ail the radioactivity was roleasod by enzymic hydrolysis except for small amounts in the liver# Enzyme hydrolysis was performed us 1 n g Bince this enzyme contains greater p-glucuronidase activity than sulphatase activity (toon et al Î9 00) it suggests that the conjugates were principally giucosiduronates particularly in the case of the liver# This seems reasonable since conjugated pregnanediol in the urine is composed almost entirely of pregnanediol glucoaiduronate (Cr%py at ai Î9G2) although Zander (1964) has found principally sulphate conjugation* Solomon et al (196?) isolated both pregnanediol glucosidtironate and the sulphate from

102
the foetal liver after perfusion with labelled progesterone. The liver has been known to have a principal role in progesterone metabolism# In the rabbit it waa ahown to have a major role in the deactivation of progesterone (Maoeon & Hoffman 1945)#In women^ it has been shown that when liver cLieease was present# the dlaappearanoe of added progesterone from the plasma took much longer and this was attributed to ■slower Intrahepatic metabolism of the liver (Patrini##@64)# In the liver of the foetal and newborn guinea pig Pulkinen et al (196i| found that half the progesterone was metabolised and about one tenth could be Identified ae a pregnanediol-type metabolite#
In the present study* 14 minutes after injection of labelled progesterone the principal steroid Identified was 20a-dihydroprogesterone (30#5#) with approximately equal amounts of polar compounds * pregnanediol* 20p-dihydroprogesterone and unchanged progesterone#A small amount ($$) of pregnanolone was also detected#
In the second experiment 45 minutes after injection of the progesterone was present as pregnanediol and almost equal amounts of polar compounds and progesterone#
103#
The presence of 20a,-dihydroprogesterone and other 3a$20a* dio.l0 was expected after the finding by Vi.lleo and toring (1903) of the presence of 20a hydroxy- dehydrogenase and 3a hydroxy-dehydrogenase in the human foetal liver* They had'found 20a#*dl hydro prog es t crone and pregnanediol ao .products of progesteronei a finding supported by Zander (1901)$ The latter* however* also detected Gg hydroxyps’ogesterone*17a hydroxyprogesterono and 200 dihydroprogestorone as V'iQll as a large amount (2Q%) of polar steroids*.Solomon et al ( 1905) detected progea.t erono*. pregnane lone* 20a-dihydroprogesterone and chiefly pregnanediol present in the liver# There was no radloactivity in the 17a hyd ro %yprog es t Crone area in the presont study or in that of Solomon et al (1965) hut since it was detected by Zander (19G1) 1 min# after injection it may he produced in the very early stages of the metabolism of progesterone*
4
In the adrenals there seemed to he more active metaholiem and conjugation of the radioactive progesterone This view is supported hy the results of Solomon et al ( 1967)* After 14 min#* 47g& of the free "imdioactlvity extracted was polar material although pregnanediol*
104
and unohangod progoaterone were also present with a email amount (6#Zj%) of 20p- dlhydroprogoatorono* In experiment 2* after 45 min*60^ was present In the polar steroid fraction with the rest of the radioactivity a$ unohanged progesterone* Solomon et al (1958) after Incnhating human foetal adrenals with progesterone* isolated 17a-hydroxy- progesterone and androetenedione* and Weliky and Bngel (1065) found 16a-hydro%yprogesterone on ineuhatlon of human hyperplaatie adrenoeortieal elicee with progesterone* In a study of the metaholiam of progeeterone hy foetal testee in * Aeevodo et alCtÔiS)* detected 16a-hydro%yprogeaterone* 17o,-hydroxy- progesterone* 20% end 20@ dlhydroprogeeterone and deoxyoorticooterone*
It is therefore evident that extensive metabolism of progesterone oooure in the foetus. In the liver reduction produoto form the main oompoundo and pregnanediol is a major metabolite in thia situation* In the adrenal glands polar compounds are formed and these have been shown (Solomon et al 1967) to be mainly eortiooids* The foetus therefore uses the progesterone it obtains from the placenta to manufacture its own corticosteroide*
105,
Since prognmnodiol has been shown to ho present Anl iq u o r aiJîBÜ (Kloppor â Alacmaughton 1950) i t eeomc very
l i k e l y that tn ia comes from f o e t a l u r in e and i # th e re fore a r e e i i i t o f th e f o e t a l metahoilom o f prog 00 to rone#
It la probable that foetal progiianediol passes to the maternal clreolettion either across the aranlotle aae or via the placental circulation go that a proportion of the pregnanediol oxer et eel in the maternal urine originatoa in the foetus# it is not known what proportion of matepgml pregnanediol this foetal component forms# In early pregnancy it must bo very small since there io little change v/hon foetal death occurs at abortion unlike oestrioi excretion which falls very steeply,
Some Information * however* is given on this aspect hy Klopper et al (1906) who found that* when salino abortion was performed* pregnanediol output did not fall greatly. In seven patients the average onlyfell to 78% of the prc-injection luweie with a range of 44 l05;oô Two patienta in fact showed no fall inaverage pregnanodiol output at ail. during the injcetioa- abortion perIod.
Î06.
Qîimisea in pregi'ianediol excretion are not easy to interpret# It may be that the foetus is responsible for some 20fa of the pregnanocliol which appears in the mothers urine# The fact that oestriol output falls much more steeply than pregnanediol output in the first 40 hr# after saline abortion (iclopper et al 2066) makes it unlikely that foetal raotaboliam of precursors is as important a step in the production of pregnanediol in the mothers urine as it is v/lth the production of oeatrial#
It seems therefore that the foetal metabolism of progesterone and the foetal production of pregnanediol may ho relatively unimportant as far as the maternal excretion of pregnanediol is concerned* The changes in conversion of progesterone to pregnanediol discussed in Chapter 4 arc probably of more importance# It v/as found in these investigations that particularly low Conversions accompanied the presence of a hydatidiform mole and it v/as decided to look at steroidogenesis in a case of hydatid!form mole in detail# Some observations on this subject are reported and discussed in the next chapter#
107.
CHAPTER 6.
steroid S tudieg in,, a case of, 1>y<l at ij if ora mole
It has beoe already shown in Chapter 4* that* in certain abnormal pregnancies* of which one variety is hydatidiform mole* the conversion of progesterone to pregnanediol is lower than in normal pregnancy, The question then arises as to what other pathways of metabolism could be occurring in these women# Stitch èt ai (1966) observed a considerable increase in the production of urinary pregnanetrio! in a case of hydatidiform mole suggesting that an alternative pathway might be favoured in this type of case*It was therefore decided to investigate this problem by -( O determining the urinary steroids in hydatidiform
mole and a suitable case of molar pregnancy was used for this purpose*
iz) investigating the steroids present in mole tissue and theea lutein cyet fluid*
(3) iocuaation of a homogonatc of the mole tissue withpregnenolono* to determine its steroid
ogenic capacity#
Î08
Qllnioal Histwy?
A woman 4 months pregnant in her second pregnancywas admitted to hospital with persistent vaginalbleeding# At examination* the uterus v/as found tobe considerably larger than expected for the gestationperiod# A Hogheti test was poA^formed and found to hepositive in a dilution of 1/200# A diagnosis ofhydatidiform mole was made and laparotomy performed.At this operation a typical hydatidiform mold wasev£icuated from the uterus; bilateral ovarian lutealcysts were found and 200 ml# of cyst fluid was aspirated
0and stored at -20 for later examination.
II i.0 to logical examination of the mole confix'med thediagnosis and examination of a biopsy specimen ofovarian tissue showed that the cysts were of the thecalutein type#
I)etermination of Urinary Steroidsnwrmm» «*u i* i.WMMWWtRHgailia»
I)etermination of Urinary Steroids
The urinary levels in mg/24hr# of pregnanediol and pragnanetriol wore determined by the methods of Kiopper et al (1856) and Stern (1957)#
109#
Injection of Radioactivity
Conversion of injected progesterone to pregnanediol and pregnaxietriol wao measured by using the technique described ear .lier in Chapter 4# Fifty micro curies of [ 7%-^irj prog OB tore no wore injected into the an te cubital vein of the mother and the steroids v/cro isolated from the maternal urine for 3 days after the injection# The tritium content of these fractions was then determined* These déterminations were made before laparotomy and evacuation of the uterus and after a provisional diagnosis of molar pregnancy had boon made*
Deter mi xi at ion of steroids In mole tissue and ovarian£i«CAlfi.wi\TJ ti.iiKa«ï>s*aWitrr»\-B»to««#»«titt>wwÈW»sw wwtoieriMBieiMiyi • rtw«a «Ker*wwwiiewww
Fifteen grams of mole tissue were incubated with [ 4 - ^ C] pregnenoloxie as precursor* Steroids wore extracted from the incubation mixture the remainder of the mole tissue and the ovarian cyst fluid once with ethanol and a further throe times with BOjâ ethanol; the combined eKtA‘‘actB wore then evaporated to dryness#
The dried extracts wore partitioned betvjeen ether and watOT and the ether fraction from the extracts was examined for neutral storoids# Preliminary fractionation
ilo
v/as perforated by column adsorption and column partition chromatography and zones of individual steroids v/ere isolated by thin layer chromatography* Spots on thin layer chromatograms were Identified by spray colour reagents* ultra-violet absorption and gas liquid chromatography after elution*
The Individual metabolites fro# each of the extracts were chromatographed until racLio-chemically pure and characterised by isotope dilution or reverse isotope dilution* All metabolites and derivatives were crystallised to constant specific activity through at least three crystallisation steps* Where no high specific activity radioactive standards wore available identification of steroids isolated from the mole tissue and cyst fluid was performed using some or all of the following criteria^ chroraatographic mobility* derivative formation* ultraviolet absorption j, colour reactions (Zimmerman chromogens * sulphuric acid ehr#mogens)* and gas liquid chromatography* Quantitive estimations of the amounts of each material isolated from the mole tissue and cyst fluid were made on tiio basis of crystalline weights * isotope dilution studies* colour chromogens and ultraviolet abeorption and are
1 1
expressed as (ig/100m.l» (cyst fliLid) and pg/lOOg v/ct v;t* (mole tissue)* Radioactive ssones on thin-layer plates wore located using a Nueleor-Ohicago Actigraph III Strip Scanner with a thin layer attachment « Samples forquantitation of radioactivity were counted in henzane solution in a Nuclear«*Ühj.cago Uniltix Mark I Liquid Scintillation Spectrometer in a Bcintiliatlon fluid GOritain 1 ng Sg. 2 , 1 phenyloxasio 1 e (PPO) and SOmg af‘2 2 - pa r a ph ony 1 hie 5 p h onyl o xa m I e ( POP OP )/111 re to i-uone •
The ahove is a summary of the main stops of the methodology involved and the full details of the extraction procedures^ isolation and characterioation of steroids^ quantitative determination of Isolated steroids and determination of radioactivity are given in the paper by Goutte et al (1BG0)#
Üx^inary pregnanetrlol ezceretion
% e urinary excretion of pregnanetriolthe excretion product of Î7a-hydroxyprogOBteroxie is only slightly elevated in normal pregnancy (Fotherhy et al IS6,5) measured weeks until term# The wholesubject of pregnanetrioi excretion in pregnancy is discussed fully in Chapter ?•
M2#
Resuitn
The levels of urinary pregnanediol and pregnanetriol were 16*0 and 10* 7mg/24lir* when determined by colorimetric methods; 0*43 and 2*84; conversions respeclively from injected progesterone were found#
By both methods the ratio pregnanediolspregnanetriol in this subject was approximately 2:1 whereas that in normal pregnancy is 20$1 (Harkness & Love i960)* Since the pregnanediol levels are within the normal range (Goyie et al 1950) this ratio signifies a greater excretion of pregnanetriol than occurs normally^ indicating increased secretion of 17*hydroxylated steroids
Table 49 shows the metabolites isolated after incubation of [4#*^^C] pregnenolone with mole tissue*As well as unchanged p r e c u r s o r 1 7 a hydroxyprcgnenolonci, progesterone^ 10a hydroxyprogesterone and 10p hydroxy* progesterone were isolated#
Table 50 shows concentrations of steroids and steroid precursors found in the extracts of mole tissue and cyst fluid.
Cholesterol, pregnenolone, 17# hydroxypregnenolone,
113
pregnanedlol, pregnanetrlol and androatenedlone v/ore Isolated from both extracts# Progesterone and Its 17a hydroxylated derivative were isolated from cyst fluid but not from the mole tissue in mea9%%roablo amount8$
Detectable quantities of oeetrogena were not observed in either of the extracts but colour reactions suggested the presence of traces of them in the cyst fluid extract. The maternal urinary excretion of oestriol was low (2$0pg/24hr*) in this patient before laparotomy determined by the method of Brown & Coyle (1903)*
.ISi
In a caoo of hydatidiform mole accompanied by ovarian theca lutein cysta a greatly increased urinary excretion of pregnanetriol was observed. Stitch et al (1900) made the same observation in a similar case and characterised this pregnanetrlôl as Sp"prQgnane"3a#17a, 20a4.triol, the excretion product of 17a hydroxyprogcstcrone
Incubation of mole tissue
On incubation of the mole tissue with pregnenolone under conditions suitable for steroid*

1 1 4 , .
ogéaesis 17a hydroxypregnonolone, progesterone,Hlo, hjdroxyprogeaterone and ISp hyclroxyprogesterone
v/erc formed* Although a search was made for 17a hydroxy- progesterone, none v/as’téund* It would appear however, that since mole tissue was able to form progesterone and 17a hydroxypregnenolone it should have the capacity
for synthesising 17a hydroxypx’ogesterone* Perhaps on production 17a hydroxyprogesterone is metabolised at
a similar rate to its synthesis thus preventing isolation#
It therefore seems evident from the lack of accumulation of 1?a hydroxyprogesteroii© that the increased excretion of p r e g n a n e loi Is unlikely to be a function of the mole tissue#
lOo. hydroxylation is an important step in the
biosynthetic pathway to oestriol# Ci.irrent views on the foeto-plaoental steroid relationships at mid term (Solomon et al 196?) indicate that 1@a*hydroxylation Is a function of the foetal liver and adrenal and that this hydroxylated progesterone is then transported to the placenta# llo yevor, this abnormal placenta is capable of forming the precursor of oestriol# Tliia hydroxylation may only occur in the abnormal tissue because larger

1 1 5 .
quantities of precuroor than normal are being formed or possibly as an alternative to normal pathways which are ah à ont * HO 20-dihyclro progesterone a vmro f o rm ed #
The rosuits of this ineuliation shows that hydatidiform mole tissue:;.le active la steroWogonesls; it la able to form progesterone and to perform hydroxylations of steroids.
Steroids of the mole tlssw .»,T«tewu t t ) e-*toti<WfSW6M«i:'«œs*es«««*tniei
kevit?5 et ai C19 02) showed that the human placenta could not form the store.W nucleus from acetate but depended upon preformed precursors for feho oyntheeis of progesterone. In the placenta both cEnolcsterol (Solomon 1900) and pregnenolone (Palmer ot al 1966) can act as progesterone precursors. It is postulated that these substances are transferred to the placenta in the maternal blood and are retained by that organ for synthesis of progesterone and related hoavnooes.From the levels of cholesterol and pregnenolone found in maternal blood, cholesterol would appear to ho the preferred precursor. In this case the synthesis of progesterone will p*oceed by way of pregnenolone (Solomon 1900}»
n o .
As well as forming progesterone the placenta has been shovm by studies in vitro, to contain enzyme systems capable of metabolising progesterone .to 30a* d ihyd ro prog e s t eron e and Î 7a*liyd ro xyp ro ge s t e rone {tittle et ill 1959; tittle & Shaw 1961), 16a*hydro30 * progesterone and androstenedlone (Little et al 19 63; Warren & Cheatum 1904) and 6p*hydroxyprogesterone (Berliner & Oalhaniek 1956)#
From the abnormal trophoblastic mole tissue
cholesterolp prognenoione, 17a hydroxyprognenolone, pregnaaediol, pregnanetriol, aadrostenedione and a trace of progestérone were Isolated* Although Pearlman and C'erceo (1052b) observed that successful extraction of progesterone from placental tissue required a high pH, it is not felt that poor extraction was responsible for the low level of progesterone found, since Qreig and Maonaiighton (19 67) * . see chapter 5 * used à similar extraction method to that used here and also because progesterone was isolated from the ovarian cyst fluid by the same methods* Failure to extract a substance from a tissue does not necessarily indicate lack of synthesis of it hut in the light of the amounts of progesterone isolated from placental tissue in previous
117*
studies (Chamberlain et al 1906a) it ia concluded that in thiB hydatid!foi'm mole there was a decreased Gynthesis of placental progesterone* This might reflect a lowered placental function or could mean that part of the placenta had regressed or separated from the uterine wall and that only the remainder was capable of producing steroids. The lowered progesterone production must be equated with the normal pregnanediol levels found in this patient end this will be discussed later. 20o,*Dihydroprogesterone was not found In the 'mole tissue and neither was 17a*hydro%yprogesterone although 17a*hydro#ypr0gnenolone was identified. Pregnanediol and pregnanetriol, the saturated reduction products of progesterone and 17a*hydroxyprogesterone respectively# were both identified. Pregnanediol is a normal constituent of placental tissue (Pearlman and Cerceo 19S2o) and the presence of pregnanetriol was not surprising since the patient excreted large quantities of this substance in her urine#
It is concluded from these studies that the mole tissue wae capable of steroidogenesis but there was less synthesis of progesterone than is normal; there
l i a .
was also an accompanying lack of the normaJ* hydroxy*
1 at8(1 derivatives of progestérone • Chamberlainet ai (lS68b) using gaB*J.iqiiid chromatography have at ml led extracts from three separate moios* Although these workers found more progesterone than observed in
this study they also eoneluded that the abnormal tissue
produced less progesterone than normal. Mo 1 7ci*hydroxy- progesterone was extracted from the mole tissue and only a small amovjnt of 17o»*hydroxypregnenolone.Although a smoJJ. amount of pregnanetriol was isolated
these findings lend support to the conclusion drawn from the incubation experiments that the increased urinary excretion of pregnanetr1oÎ in this case of hydatidiform molo did not originate from the mole tissue.
3toroids in ovarian cyst fluid
Cholesterol, pregnenolone, 1 7ci*hydroxypregncno 1 ono, progesterone , 1 7a*hydro)syprogestorono, pregnanediol, pregnanetriol and androstenecllone were Isolated from the ovarian cyst fluid. The compounds isolated from the
C5 st fluid were the same as those found in the mole tissue with the addition of measurcable amounts of
119
protestoron© and 17#*hydroxyprogestcrone. Apart from the precursors choleaterol and pregnenolone, all other GUhstancos isolated were found in much larger quantities than in the mole tissue, (Table 50>*These results suggest that the increase in l7*hydro;iylation which was signified by an increased urinary excretion of pregnanetrlol, is ovarian in origin# This conclusion would he in agreement with the findings of Stitch et ai (Î90O) who observed that pregnaneti'^.iol excretion remained high after evacuation of the uterus until regression of the cysts*
In hydatid iform mole the trophoblast produces large quantities of human chorionic gonadotrophin (l!«CsG«) - the Hog ben test was positive in a dilution of 1&20Q * and it is probably as a result of over* stimulation by this hormone that the ovaries became cystic# These ovaries were stimulated to produce 17a*hydroxyprogeGterone* Evidence for the secretion of a pregnanetriol precursor by the ovary is given by Fotherby (|9G2) and this will bo discussed in the next Chapter when the ovarian production of hormones is considered following stimulation with human menopausal gonado tro phin#

120
CllîoXostoroi from the maternal blood or ovary le probably need ao the precursor of 17««hydro%y storoidsand overs Simulation would reeislt in increased productionof all the intermediates in this pathway ^ pregnenolona^ $7a*hydroxypregnenolone and progesterone «• as well as
the excretory product, pregnanetriol# - Fig. 0*
The polycyotic avaries produced m m l l quanti ties of onoro8tonedione hut -no traco of tootostorone wasfamid in the o.yot fluid@ The fact that the ovarios arc not stimulated to produce oestrial is in agreement with the findings of Frandoen (1005) and the lowered urinary cxcrotion of oestrioi frequently found in many cas03 of hydntidiform mole, also observed In this caoo and doscribed in oomc detail in chapter 8* This is a further factor which supporte the hypothceia that the proeonco of foetal proourooro of oestrioI are ncceaeary for the increased production of oostriol in pregnancy#
Ttio .normal pregnanediol levels found in such a case may be misleading since they may reflect normal placental function^ or may indicate Imvorcd placental function at the same time as an increased ovarian production of progesterone which may mcplain the

1Z1
findings reported in chapter 3, where' the pregnanecliol love Is in cases of hydatidiform mole vary from low to normal *
Oonei Its ions
From these investigations the following concluslone may he drawn (1) there was an increased urinary excretion of pregnanetriol (2) the mole tissue was active in steroid metabolism producing î7a-hydroxy* pi’egnonolonej progesterone, 16a--hydroxyproge6terone,
and 16p*hydroxyprogoaterone from pregnenolone, but
apparently less progesterone than a norraal placenta#The increased urinary excretion of pregnantetriol is not a function of the mole tissue (3) the high urinary level of pregnanetriol is probably of ovarian origin (possibly
ae a result of overstimulation by the high levels of H*C*G# present).
The effect on the ovary of the high levels of
il#0*G# produced by the molar tissue is of particular interest# In the therapy of some amoriorrhooic women
combinations of follicle stimulating hormone and H.C#0# are now in regular use for the induction of ovulation* One of the most troubleoeme complications of this

1 2 2 .
thürapy is hyperstimulation of the ovary* The
fiyndrome, as far as the ovary is concerned. Is analogous to that produced by the II*C*G* from a hydatidiform mole* fhe results of this molar Investigation arc now applied, in the next chapter, to women being treated with human menopausal gonadotrophin and their relevance to the measurement of corpus lutcum function in those women is discussed*

12ù *
ürlnaryBteroM exeretlon after
In the previous chapter It %vas suggested that the high level of pregnanetriol In the urine of women with hydatidiform mole has it$ origin in the ovary* It la produced in the theea lutein cyete of the ovary ivhich are caueed by the large quantities of II.G.G# present in the circulation of these women and does not result from metabolism occurring in the trophohlast itself# These findingo are relevant to early pregnancy induced by human menopausal or pituitary gonadotrophins where hyper stimulat ion of the ovary frequently occurs# due to excessive dosage of gonadotrophin* This is a very similar situation to that found in the hyperstimulated ovaries in hydatidifo rm mole*
The information obtained in the previous chapter has been applied to the study of a small number of women in whom ovulation was induced by human menopausal gonadotrophin and this work forms the basis of this
i?A>
chapter# These results are as yet ratlier preliminary but are of coneldarable Interest and It Is felt they are worthwhile discussing in this thesis# They both help to round o#' the work reported and at the same time pose a number of problems for future work* To put the position of pregnanotriol into perspective some aspects of steroidogenesis in the human ovary ivill first be discussed#
Sterqidogenesis in the human ovarz
The iMsman ovary is capable of synthesising cholesterol from acetate probably by the same route as that established for hepatic cholesterol synthesis (Popjak and Gornforth 1900)# Pregnenolone is formed by splitting off the side chain and progesterone is formed from pregnenolone by removal of 2 hydrogen atoms and the shift of the double bond from the delta 5 to the delta 4 position# The steps of the biosynthetic pathway to oestrogens are shown in the diagram (Fig# 9 )$ The relative importance of the several alternative routes from pregnenolone to ocstradiol are not known in any detail# There is some evidence that in the follicle# oestradlol may be formed by a pathway not
Î 2 5 .
Involving progesterone# whereas in the corpus luteum a pathway involving progeatorone may predominate (Ryan and Petro $006).
c^strioi.i As has been said earlier in this thesis oestriol is present in .large quantities in human urine and if oestradioi is given to a woman a considerable pro portion of this material is excreted, in the urine me oestrioi# The conversion of oestradioi into oestrioi occurs in the maternal liver and oestriol has usually been considered to bo a catabolic product of oestrone or oestradiol* It has also been thought to be a detoxication product because its oestrogenicity is loiver and it is more soluble in wator than the other two classical oestrogens* There is, however# evidence that the ovary does secrete oestriol# especially during the lt:teal phase of the cycle (Barlow and Logan $966) and the ovary has been shown to contain a Ida hydroxylase Oestriol may therefore be considered an ovarian oestrogen in its own right. It is not yet cloar whether# as in the liver this ovarian oestriol is formed from oestrone and oestradiol or whether# as in the placenta from $6% hydroxy dehydroepiandrostorone.

120#
Oontrol of ovarian biogonesis
The pituitary gland secretes trophic hormoneo which stimulate the endocrine glando to produce their reapeetive hormones * Follielo stimulating hormone (F*8$II#) atimuiatea follicular growth and results in incroaaed oestrogen excretion# In this sense F#S#h# stimulates oestrogen production but it is not cloar that it has any specific effect on steroidogenesis#At the menopause# for example# high levels of F#S#H# are associated %vith lo%v oeatrogen levels because of the absence of growing follicles#
In ,vitrp preparations of F#8*tl# have been reported to stimulate the rate of conversion of cholesterol to pregnenolone in non pregnant bovine corpora lutea (ichii et al 1903)# but these results could not be reproduced (Yago et al 1967)# It is also impossible to obtain pure F#$#H# i#e# not containing a proportion of Luteinising hormone (LH) and it cannot therefore be Said that any action due td this F#S#h# is due to this material alone since it might be due to the Lh Contamination#
In contrast there is considerable evidence that
127#
Loll* can specifically influence ateroidogeneais (Bavard, et al I060I Channing and Short 19 66)• It has the effect of increasing both the rate of conversion of cholesterol into progectorone and the de-novoproduction of the latter*
In early pregnancy, it may be a specific action of chorionic gonaclotropUin on steroidogenesis that maintains production of progesterone and oestrogen by the corpus lute urn* Tho L.IÎ* peak in the inenstrual cycle (see Fig*10) is of short duration and occurs near the time of ovulation and not in the luteal phase of the cycle (Midgley and Jaffe 1966)* It appears to bo associated with ovulation and possibly with corpus luteum formation but does not appear to maintain steroid secretion during the luteal phase* There does not scorn to be a sharp decline in L*H. associated with the decline of the luteal steroidogenesis and it is difficult to explain how rising levels of chorionic gonadotrophin continue the life span and steroid secretion of the corpus lutoum when conception occurs# The presence of a uterine luteolytic factor, for which there is evidence in several animal species (Short 1966)
U B .
does not seem to obtain in the human and removal ofthe uterus appears to prolong the life of the corpus lut cum by only a few clays (Andreoii 1965)*
The effoet of gonadotrophins on ovarian cellular metabolism vlvq is almost completely unknown although the resultant steroid excretion is well documented, e*g# Loraine and Bell (19 68), at any rate as far as oestrogen and prognanecllol are concerned# Where other steroids and particularly pregnanetriol are concerned evidence is much more scanty*
The other steroid of particular interest is pregnanetriol (5p-prognanG-3o.# I7a,20a--triol) and its origin and excretion in the menstrual cycle and in pregnancy will now he discussed#
In the biosynthesis of the steroid hormones 17c. hydroxyprogesterona is an important intermediate (Samuels 1960)# The principal urinary metabolite of 17(& hydroxyprogGstorono is pregnanetriol (Axelrod and Gold si eh or 1960; Fukiishlma ot al 1961)#
There are three possible precursors of pregnaaetrioi namely, 11-#deoxycortl8ol, 17a Eiydroxypregnenolbne, and $7o, hydroxyprogesterone# Fotherby and Love (1DG0) studied the conversion of these precursors to pregnanetriol and found that by far the greatest conversion occurred when 17a hydroxyprogesteronewas injected# These worke%*s concluded that pregnanetriol %vas therefore the main metabolite of 17a hydroxyprogesterone#
îiie«.21ar|jin^gî;;od«ctAos^,,|_a
It has been suggested (Brown 1050) that ovulation occurs at about the time that the excavation of oestrone and oestradiol reached a maximum towards the end of the follicular phase of the menstrual cycle* The data of potherby (1062) showed that there was a significant rise in pregnanetriol excietion on the day that the excretion of oestrone and oestradiol reached a peak#The magnitude of the rise suggests that the precursor responsible in the second half of the menstrual cycle was 17a hydroxyprogesterone since oestrogen levels are lower at this time* I7a Hydroxyprogesterone is kno%vn to be secreted by the adrenal cortex and the majority
130*
of pregnanetriol in the urine may arise from this source* From the day of ovulation this adrenal prcgnanetrloi is supplemented by some arising from precursors secreted by the ovary $
Although the evidence (Fatherby 1962) suggests that the increase in prognanetriol excretion in the menstrual cycle (Fig# 11) is due to an increased secretion of precursor from the ovary it could possibly he due to increased adrenal production at this time* llowever, that the ovary is responsible, is supported by the fact that the biosynthesis of oestrogens from cholesterol involves 17a hydroxyprogesteronc as an intermediate (see Fig* 9 ) (gyan and Smith 19 65') and this steroid has been identified in extracts of human ovaries (bander 19 58) and in human follicular fluid (Short and London 1961)* Further support for the ovarian secretion of a pregnanetrioi precursor is provided by Fotherb^^ (19 62) who administered nor- ethisterone to normally menstruating women and found that the rise of pregnanetriol excretion in the second half of the cycle did not occur* Since the second oestrogen peak and the pE^egnanediol peak did not

131.
occur in these women® Fotherby (10 62) concluded that the decrcase in the excretion of pregnanetriol during the administration of the synthetic steroids was due to a suppression of procursors from the ovary which are metabolised to prognaaotrlol viz 17a hydroxyprogestorone in the cor pus lutcum#
It would appear, therefore, that the excretion of pregnanetrial in the urine might give some estimate of the corpus lutcum activity of the ovary and that this might be a valuable steroid to measure In the urine in early pregnancy#
Pregnanetriol excretion in human pregnancy
The most reliable estimates of urinary pregnanetriol output dux'ing normal pregnancy are probably those of Harkness and Love (19 06)# Previous methods i#e#Potherby and Lovo (19 60) wore probably not specific for the determination of pregnanetriol in the urine of pregnant v/omen (Fotherby et al 1905)* These previous methods (Bongiovanni and Clayton 1954; Stern 1957) used a sulphuric acid colour reaction for estimating the steroid and there arc compounds present in the urine of vmmen during pregnancy that interfere with this colour
132
reaction. Those interfering sulphuric acid chromogens in pregnancy urine increased with duration of the pregnancy and Fotherhy et al (1965) found that at least some of the interfering compounds in pregnancy urine are polar metahoiitea of progesterone* In non-pregnant women and in early pregnancy the method of Fotherhy aEid Love (10 60) is suitable since the amount of interfering substances is minimal *
In their paper Harkness and Love (1060) measured urinary pregnanetriol excretion in the urine after the 22nd week of pregnancy and Fig * 12 is taken from their results. This shows an increase in the last trimester reaching a maximum at about 30 - 3 7th weeks of pregnancy* There were large variations between individual patients*The increase found by these workers was not so great as that described by Herrmann and Silverman (1953) and Honan et al (i960)* llarkriess and Love ( 1966) also estimated pregnanetriol excretion during pregnancy in an adrenalectomisod woman and found that the level also increased. They suggested that the focto-placontal unit is probably the source of the increased amounts of urinary pregnanetriol in the adrenalatomisad pregnant
133
woman and presumably it is also the origin of some of the increase observed in normal pregnant women in the second and third trimesters* The occiirrance of the rise in the last trimester of pregnancy suggests that the foetal component of the foeto-placentai unit may be the more important sonrco of the increase in tu .tnary pregnanetriol* This suggestion is consistant with the scheme proposed by liiczfainsy ( 10 64) for the steroid metabolism of the focto-placental unit at t)ld pregnancy*
All the workers already referred to have measured the urinary excretion of prognanetriol from raid pregnancy and there is no information as to what happens' in very early pregnancy#
It is well Known how difficult it is to obtain information at very early stages of human pregnancy hut the advent of gonadotrophin therapy for stimulation of ovulation in amenerrhoeic women has meant that a number of women are under observation at the time of conception and during the very early stages of pregnancy« It istherefore possible to measure urinary steroids in these patients in the cycle in ^vhieh pregnancy occurs and
134*
observa the changes which take place in steroid excretion at this very early stage of pregnancy, wheiip in fact impIan tation and the growth of the blastocyst are talcing place* It is at this time that the corpus Inteiim of pregnancy, in the h u m a n i s of some importance Since after 3 5 days, it has been shown by Tu 1 sky and Koff (1957) that human pregnancy can continue even If the corpus luteum has been removed*
Gi.i nieal II1 b to ri eg of Patients
Oaae Mo* 1* f*ll« Age 34, Secondary ameriorrhoea for8 years*
The menarChe occurred at the age of Î4 years and the menstrual cycle v/as regular at first* At the age of 18 years it became .less regular and finally stopped when the patient was 20 years old#
She was first seen at the age of 34 years and tested for suitability for gonadotrophin therapy* The details of this investigation are not pertinant to the aspect of the subject be.lug discussed and will not be given here* She was Judged to be suitable for the induction of ovulation v/ith human menopausal gonadotrophin*

135.,
This patient became pregnant after treatment and abortion occurred at about 2-3 months of pregnancy *In a second pregnancy twins wore conceived* This pregnancy proceeded to term when she was successfully delivered by Caesarean Section*
The results of steroid excretion assays during the aborted and W i n pregnancy will he discussed*
Case Mo# 2* II* dl F* Age 27 yrs* Secondary aimenorrhaaa for 4 years following the birth of her only child*
the menarchè occurred at age lo years and hermenstrual cycle was regular until her first pregnancy occurred at ago 23 years* The pregnancy was uneventful and she had a normal delivery at term with nocomplications* Menstruation did not return and after4 years Btie was tested for suitability for gonadotrophin thcrapy and found to be suitable*
She was treated with human menopausal gonadotrophin In a number of cycles before a pregnancy occurred* In the first half of this pregnancy she had intermittent vaginal bleeding and rested in hospital for prolonged ariods at this time* She remained well during the
ÎS6»
middle trimester of her pregnancy and then had further bleeding and v/as admitted to hospital again for rest and supervision at 34 weeks# She was delivered successfully by Caesarean Section at S9 weeks of pregnancy. The results of steroid excretion in a cycle and during the early part of pregnasiey will be discussed #
Case No# 3# 3#F# Age 52 years# Secondaryamenerrhoon for 7 years#
The menarcho occurred at the age of 13 years and the menstrual cycle continued to be fairly regular until the age of 25 when the amount of bleedingbecame scanty and menstruation finally ceased altogether#
!
This patient v/as 'foimd to be suitable for gonadotrophin therapy and several cycles of treatmexit have been given#
The results of steroid excretion during these cycles will be diecussed.
Case No # 4# G#H# Age 35 years# Nullipara#
This patient suffered from severe endometriosis and total hysterectomy and bilateral salpingo-
137.
oopherectomy wore performecU She kindly agreed to cooperate In an experiment to determine the effect of administered F.S #H# and t.O* to an oopho recto raised . v/oman® She was given 760 lU# plus' $000 ID.Sl.C.O# and her urinary steroids were measured for 14 days thereafter. The object of this experiment was to find out whether pregnanetrioi excretion rose after gonadotrophin stimulation in the absence of the ovary i.e. ivhother aome of the increase was due to the adrenal•
Assay methods; Urinary prognanedlol was measured by the method of Klopper et al i^9B5)p and urinary oeatriol by the method of Drown (1055) as modified by B row» e t a 1 ( Î 0 5 7) » P regaa ne t r io 1 wa s me a a nr ed by the method of Fotherhy and Love (1000)'which- is.8uitable for measuring this substance In the non- pragEiant state and in early pregnancy where there is little interference with the sulphuric acid colour reaction.
Results:
Fig. 13 shows the pregnancdiol excretion and the oestriol excretion in 48 hour urine specimens in Case
1S8» «
No. I .in the pregnancy in wh.ich abortion occurred.The levels of both hormones rose to above nou"pregnancy levels until bleeding occurred (Bj after which time there was a gradual fall in both eteroids^ the ^Oravindex* pregnancy test became negative and abortion finail,y took place.
Fig. 14 shows the first 20 weeks of a twin pregnancy which resulted in a successful conclusion* In this pregnancy the excretion of oestriol and pregaanedioi rose in the usual manner associated with early pregnancy and the hormone pattern in the urine remained normal till tcx*m«
Fig. 15 shows the excretion of pregsianecUoi^ pregnanetriol and oestriol in a gonadotrophin stimulated cycle in Case No. 2. Only I oestrogen pealc ispresent in this cycle and there are peaks of pregnanediol and prcgnanetriol after ovulation thereafter the levels falling toward the end of the cycle*
Fig* 16 shows the excretion of these three steroids in the urine of Case No. tp in the cycle in ;vhich pregnancy occurred and the .excretion thereafter till 30 weeks gestation. There is a fall in ocstriol

159.
after 5-0 weeks of pregnancy but the level then begins to rioo again to normal pregnancy levels. Pregnanedialexcretion follows t he.oame pattern with a fall to relatively low levels at about 12 weeks - it was during this time that bleeding occurred and there may have been deficient steroid biosynthesis in the trophoblastic tiaaiie around this time accounting for the fall in the urinary excretion of steroid metabolites.
The excretion of pregnanotrioi in this case also rose pare passu with pregaanediol up to 6 weeks of pregnancy and then foil to the levels usually reported for human p regnan ey•
■ Figs# t?p 18 and 18 show the excretion of prognanediolÿ pregnanetriol and oestriai in 3 consecutive cycles stimulated by gonadotrophin therapy in Case No# 3. In the 1st. and 3rd * cycles the response is more marked than in the 2nd. cycle and this confirms the variability of response by the same woman to the same dose of gosiiadotrophin in different cycles that has been commented upon by Grooke et al (19 86) and others.
Fig. 20 showB the urinary excretion of the three hormones in the urine in Oaao No. 4# where the ovaries
140.
wore absent. There is a little rise in oestriol exeretxoa but little change in the excretion of pregnanediol ami pregnanetricl.
EU£M£8|^0B
In Fig. Î3 where abortion occurred the initial levels of oestriol and pregnanodiol rose as would be expected in normal pregnancy. At about 60 days gestation there was some bleeding and thereafter the levels of hormone excretion fell. It seems probable that when bleeding occurred there was some disruption of the trophoblast which resulted in death and subsequent falling of the levels of urinary metabolites of the hormones manufactured by the trophoblastic tissue#
This ease confirms the results discussed in Chapter 8 p and shows that measurement of these two metabolites, vis, preguanediol and oestriol, in the urine during pregnancy, is not likely to give an indication of impending abortion. This result would indicate that, at this stage of pregnancy when abortion occurred the ovarian contribution to the level of these
Î41
steroids in the maternal urine must be minimal# Dlesfalusy and Boreil (10 01) measured the output of ooBtrogens and pregnanediol before and after removal of the ovary seventy eight days after the date of the last menstrual period# In the removed ovary theye workers found a fully mature corpus iuteum of pregnancy. Since the level of both the oestrogens and pregaanediol remained the same after oophorectomy • indeed that of pregnanediol actually rose after the operation - it v as concluded that during the third month of pregnancy a histologically mature corpus lutcum of pregnancy did not seem to be a significant source of urinary oestrogen and prognanedioi.
It may be true, and seems likely, that at even earlier stages of pregnancy the ovarian contribution may be significant^ but this would appear to be at very early stages only.
The pattern of excretion in the twin pregnancy is shoxvn in Fig# 14 . There is a steady rise in hormone level# The levels in this case are rather higher than those reported for twin pregnancy* Gem%ell and lioos (Î960) found the average excretion of prognanodioi to
Î 4 2 » .
he almost the sarae in those women who conceived a single infant or twins bmt was ©ignifioantiy higher only iu those women ooncoivlng triplets or more foctiisos# On the other hand the avoroge excretion Of oestrogen has been found by these workers to be somewhat lower in those women who gave birth to a single infant than in those who gave birth to twins, triplets or wore foetuses# The findings in the present patient would support this view# Unfortunately the level0 of prognanotriol wore not available in this woman#
PregnanetrioI excretion in the gonadotraphia
SMSElâÊJ.l»£iaM
fho origins and precursors of urinary pregnanetriol have already boen discussed# Very little information is available in the literature about the excretion of pregnanotrlo1 in the urine of women being treated with gonaclotrophino although much has boon %vritten about 0estrogens and prognanodioi (toraino and Beil $968)# Lorain0 ot ai (1060) have reported a few cycles of pregnanetriol excretion in women who havo been given clomiphene for induction of ovulation# and the pattern

14S.
in those cycles has been of the same order as that found in the normal cycle where stimulation has been by endogenous gonadotrophin#
Four gonadotrophin stimijilated cycles are shown where the levels of pregnanetriol have been measured in the ux'lno. Figs# 15, 17, 18 & 19. Three 'of these ( 17# 18 & 19) v/ero successive cycles la the same woman and the fourth ( 15) was in m patient who became pregnant in a subsequent cycle#
The results show that in the gonadotrophin stimulated cycle the urinary excretion of pregnanetriol rises during follicle growth and is greatest Just after ovulation i.e. betv/een day 14 and 16 when the corpus luteum is most active*,
As has been mentioned before the principle precursor of Pregnanetrio1 is I?a-hydroxyprogesterone {Fotherby 1962)# Strott and Lipsett (1968) have shown that there is a significant clifferance in plasma 17a-hydroxy- progesterone levels between women in the follicular and luteal phases of the menstrual cycle# These workers indicate that the higher 1 ?G,-hydroKyprogesterono levels
1 4 4 -
during the luteal phase of the cycle suggest that the corpus iutemn la the source of the 17a-hydroxy- progestorono* There is no doubt that this steroid is accreted by the ovary and Mikhail et al (1963) showed that the levels of 17a-hydroxyprogeoterone in ovax'.ian venous blood were 60 times those found in
peripheral blood thereby proving ovarian secretion of 17a-hydroxyprogesterone* It is notable that in Case 4, where the ovaries are absent, there is no rise in the level of pregnaoetriol following administration of F*S*lî* and Loll. This gives further support io the ovarian origin of the increased amounts of this Bubstance found in prâno daring the menstrual cycle*
The suggestion therefore is that the corpus lutcum does in fact seerete moderate amounts of 17a--hydroxyprogesterone and this accords with the findings reported in Chapter 0, where this cooipoimd was detected in the theea lutein cyst fluid from a woman with hydatidiform mole* 'That the secretion is from the corpus lutcum is further supported by the fact that in men, where the levels of 1?a-hydroxyprogeBtoronO are higher than those in the follicular phase of the
145#
cycle in women, there .is a substantial increase in urinary pregnanetrio1 following the administration of Human Chorionic Gonadotrophin to normal men (Jaylo 1965; Landau and Lanes 1959). There appears to he a gradual decline in steroid synthesis in the corpus Xnteum during the luteal phase of the cycle since the level of both pregnanediol and prognanetrio.l fall together# other evidence that this ie so is based on the progesterone content of the tissue, and the progesterone content of ovar.I.an and peripheral venous bleed (Zander et ai, 1958; Mikhail et al, 1963)#On the other hand recent work by Le Maire et al (1968) on measurement of progesterone synthesis in the corpus lutcum failed to reflect the expected gradual decline through later phases of the menstrual cycle# These v/orkers found that only the abrupt complete failure of corpora .latea, 14 days and over, to incorporate 140 acetate, accorded with previous observations of cessation of fonction of the corpus lutcum at the end of the cycle# The reasons for this latter finding are not clear but an obvious shortcoming of in vitro studies of the type performed by Le Maire et al (1908) is the great variability in the synthetic capacities
#46-
of imlivldtiaJt from different patients# afactor which lg$ absent from oeqnontial stiWiea conductedin the saue patient-# flüs of courso is Impassible
do in the human out je et-*
W i m m s M â R i .
ISY. ■' ■ '
Xîï the paf.iG'fits who "feocamo pregnatît the .levels g I ‘
oaatrioiÿ prognanetriol mid prognanodioi rooo together following ovarian stimalatimi by PoO.Ho and
intorc$6Ling features are that y tiw prognonotrlol iavel rooo to over iOmz/?A hr#, vory much lUgUep than any previouai^^ reported in prognancys Theievci of aii throe hormones thoa foil and at this time the patient was resting in hospital with threatened abertiei'%t% The lovoi of oestriol and pr#gnaaedloi thoroaftcr rose to the ncnmi figuras found in pregnancy and tho iQVol of prognsnota'iol remained at that ropot^tW for progiiaaoy hy ps'Wioim authors and dAseuosed curliar#
The suggestion is therefore made that this high MluetiOR of pregnanet.rlol at this very early stage of
147,
pregnancy is a function of the corpus Xoteum of
pregnancy and that the amount found does, in fact, give a measurement of this corpus lutcum activity.A second patient (Case 3) has recently become pregnant and has shown the same findings in very early pregnancy.
. It has been difficult to assess clireetly the
function of the corpus luteum of pregnancy* Ovarian and peripheral venous progesterone levels have been measured at intervals throughout pregnancy (Mikhail and Allen 19 67) and this data suggested that the corpus
lutcum was the important source of pragesterono during the first 12 weeks of pregnancy. More recently Yoshima et al (1960) have mensured plasma 1 7o,-hydro%y- progesterone in women who became pregnant after ovulation v/as induced with gonadotrophin* Since the placenta has no or only very limited capacity for
17o,hydroxy 1 at ion (Palmer ct ai 1966; Jungmann and Scîliweppe 10 67) measurement of plasma 17a-hydroxy- progesterone or its main urinary metabolite pregnanetriol should reflect corpus luteum function*The findings in the present case fit exactly those of Yoshima et a.I (19 69). These workers found that the
peak of plasma 1?a-hydroxyprogesterone vms between

1 4 8 .
4 and B weeks of gestation and by 12 weeks this compound had stabilised to a level which was
maintained for the remainclor of the pregnancy (Fig. 21). Plasma progesterone, on the other hand rose to a peak about 3 - 4 weeks aftex' H.C.G. The level then
fell reaching a nadir at six to eight weeks. This was foilov/ed by increasing levels, almost certainly due
to placental production of progesterone.
Koto on the functional life of the corpus iuteuBi of
The functional life of the corpus lut cum ofpregnancy in man has given rise to controversy over the years. Scattered reports indicate that its function may not be important to the continuation of pregnancy after 6 weeks, (Deansly 196G), but as has been suggested earlier in this chapter the work of Tulalty and Koff (1957) and Froov/is (19 63) indicate that abortions tend to occur after removal of the corpus lutcum during the fifth to sixth week after conception whereas after the sixth week there were no
t.pontaneoiis abortions. These data are consistent
with an early important role for the corpus luteum.
1 4 9 .
It does not, however, help v/i,th respect toContinuing corpus inteiim function in pregnancy* Histological studios of the corpus lutcum of pregnancy showed the persistence of granulosa lutein cells throughout pregnancy (Oillman et al 1941). These seemed to reach their greatest development between the second and third month and to disappear shortly thereafter, Nelson and Greene (1958) after extensive study concluded that the corpus lutemi of pregnancy actively flourished and was functional during the first six weeks of pregnancy, deteriorated markedly from the 8th to the 16th week and was passively maintained from then on until the termination of the pregnancy# These workers concluded that the ovary during the larger portion of pregnancy appeared from
a histological point of view, to act only as an end organ influenced hy extrinsic substances probably of placontal or1g1n.
Elevated plasma 1 ?a*»hyciroKyprogeBterone levels wore found In the luteal phase of the cycle (Yoshima Ct al 10 69) and these workers found that the plasma I'/a-hydroxyprogesterone level was a good index of
150.
follicular development and luteal function* Theysuggested that they could examine one aspect of steroid production by the corpus luteum in the presence of a functional placenta* They estimatedfrom the divergence of curves of plasma progesterone and Î?a-hydroxyprogcsterone (Fig. 22), that the life of the corpus lutetim of pregnancy was about 10 weeks.
I f t h e r e f o r e , the pi as m a 1 hyd r o xy p ro g este ro no does monitor the early corpus lutem^, and the evidence that it does seems good, then the main metabolite pregnanetriol could also be used in this way. The
evidence of the present two cases suggests that it does and therefore it is put forward that the measurement of pregnanetriol in the urine in very early pregnancy may be helpful in monitoring abnormalities of early ■pregnaBicy clue to deficiency of corpus iiiteum function such as early abortion*
During the first six weeks of gestation the
corpus lutcum is the predominant source of progesterone and after the nadir of plasma progesterone is reached the placenta assumes the important role in progesterone production. The occurrence of the nadir in the plasma
151.
progostorone curve suggests that this should be a critical period in pregnancy since cither an unusually rapid fall in progesterone production by the corpus luteom or a too slow increase in placental progesteroin production could result in plasma progesterone levels incompatible with the continuation of pregnancy* The value of urinary pregnanediol measurements in early pregnancy have been shown earlier in this work to be unreliable In forecasting abortion and giving information about the corpus lutcum, and it is now suggested that urinary prognanetriol estimations
ohould be used instead unless suitable methods of assay of pXtisma levels of hormones can be developed for this, but this involves more complex methodology and repeated veni puncture*
One point which must be noted, however, is that urinary pregnanediol excretion is well known to be greater after induced ovulation than after normal oVulatioa {Geinzell 1965) * The levels of 1 7-hyd ro xy progesterone and progesterone noted one week after ovulation induced by gonadotrophins were higher than those seen at a comparable time of the normal luteal
152
phase and the levels of pregnanetrlol seen in the
lULine in the present cases are also higher than those previously reported•
These higher levels may be due to multiple corpora lutea, or perhaps to a larger corpus lutcum and are most probably attributable to the dose of gonadotrophin used to induce ovulation.
It is impossible, therefore, to consider gonadotrophin induced ovulation as noxvnal and the high excretion of pregnanediol and oestrogens noted by
many investigators attests to this* There is however no reason to suppose that the time relationships of corpus luteum growth and persistence are altered by the pre%fious injection of gonadotrophins. The increased
excrétion of pregnanetriol in gonadotrophin stimulated cycles where the level is higher than that normally reported are similar to those seen in cases of hydatid!form mole where there is also excessive stimulation as described in Chaptex^ 5#
103
CHAPTER 8 .
Summary and ConeXu9Ions#
1. Summary
Chapter I# ïntrodyctiou to the Thesis#r j r
The introduction discusses the thoughts leading to the studies and shows the relationship of the different chapters to each other#
Chapter 2# Epidemiological studies on abortion andsubsequent reproductive performance#
1# Women who start childbearing with 1 or 2consecutive abortions are compared v/ith those %vho start with 1 or 2 normal pregnancies in respect of age, height, husband’s social class, obstetric performance in subsequent continuing pregnancy and later reproductive performance#
2# Women starting childbearing life with 2 abortions are older, shorter and of lower socio-economic status than the other 3 groups* Their problem is not ’fertility* but the difficulty of ’holding o n ’ to the pregnancy#
154*
3* In the first oositieuing pregnancy these women have a higher incidence of threatened abortion and premature labour* The perinatal mortality is increased mainly due to ’’prematurity’* and ’''foetal deformity” * There is also an increased rate of operative delivery, of forceps after I previous abortion and of Caesarean Section after 2 previous abortions*
4* In the group with 2 previous abortions there is an increased tendency to poor foetal growth and the women with poor foetal growth also have premature labour* Meticulous antenatal care isindicated in these women *
5# Eight percent of women who abort in their first pregnancy aborted in all their subsequent pregnancies and lOjS of this group had no subsequent successful pregnancy*
6# The recurrent abortion risk increases withcoaaecutivc abortions from tB% after 1 previous abortion to BBfo after 3 previous abortions#
7# One third of abortions take place before 2 months

155*,,
gestation ami have occurred by 3 monthe*
8* The results suggest that in abortion studies thetypo of patient who should he studied is the ’primary recurrent ahorter* with two or more previous consecutive abortions and no pregnancies which have progressed past 28 weeks*
0* Initial observations 1ft abortion studies shouldbe made, at the latest, by 8 weeks of gestation*If a previous abortion has ended at an earlier stage than 0 weeks the initial observations must be made before this time#
Chapter 3* Hormone assays in normal early pregnancy,in abortion and in hydatidAform mole*
1* The metabolic pathways from precursors topregnanediol and oestriol are discussed.
2* Urinary pregnanediol and oestriol assays aremade in 5 groups of women (l) Normal pregnancy#(2) Ifomon with at least 2 previous abortions and no stîcceasful pregnancies and (3) Women who aborted in the pregnancy studied*
156#
3# Thoro la no significant difference in oestrioland pregnanediol excretion between the women who aborted and those in which the pregnancy continued successfully until 16 weeks gestation# Thereafter, %Aen the foetal component of oestriol production takes effect low oestriol excrotion is significant# There is no difference in the pregnanediol/oestriol ratio between successful and unsuccessful cases#
4# Urinary oestriol and pregnanediol assays areof no value in forecasting abortion until after16 v/eeke of pregnancy#
5* These two assays are performed in 5 cases of hydatidiform mole where the trophoblast is abnormal and the foetus is absent# Urinary pregnanediol levels are higher than normal in 2 oases and lower in 3# The level of oestriol was normal until. 16 weeks in t case and then flattened out# In the other 4 cases it was low*
6* In hydatidiform mole urinary pregnanediol andoestriol levels may bo normal but are more likely to be low# There may be some change in steroid metabolism in this type of case#

157.
Chapter 4, Conversion of progesterone to pregnanediol.
1. Pregnanediol is the characteristic urinary metabolite of progesterone but other more polar mat abolîtes are also excreted in the urine
. especially 6 and 16 hydroxylated compounds*
2. After I.V# injection of lOOpc. tritintedprogesterone the percentage radioactivity excreted as pregnanediol v/as measured in 4 groups of women (Î) Non-pregnant (2) early pregnancy (3) late pregnancy <4) abnormal pregnancy*
3. fhere was no significant difference between the ûûsi^prognant, earljf pregnancy and late pregnancy subjects, but there was a significant difference between abnormal pregnancy ami the other 3 groups* In particular the conversion in cases of hydatid if orm mole v/as low#
4# There was no difference in conversion in the same subject - pregnant and non-pregnant.
158.
Chapter 5# Progesteroïxe metabolism la the humanproviable foetus.
1# The levels of progesterone In the umbilicalVOS sels indicate that the human foetus raetabolises this hormone.
2* Perfusion of pro viable foetuses with 4-0^'^progesterone for 14 and 45 raiautes followed hy extraction of the tissues and identification of metabolites shows that 40?S of the radioactivity is present in the liver after 14 minutes mainly as 20a dihydroprogesterono. The adrenals at 14 rainutes contain 3.4?^ of the radioactivity mainly in the form of polar compounds. After 45 minutes the main compound in the liver was pregnanediol and in the adrenals polar compounds - probably co rtico st oroi d s.
3* The foetal liver ia the chief site of metabolism of progesterone and this organ produces mainly reduced metabolites. The adrenal also metabolises progostorono to polar compounds, sueh as corticosteroids.
ISQ#
4. Progestorona from the placenta is used by the foetus to produce cortieostoroids for its ovm homeostasis#
Chapter 6* Steroid studies in a case of hydatidiformmole# .
I« fho increase in urinary pregnanetriol excretion in cases of hydatidiform mole suggests nn alternative metabolic pathway in these cases.The prognanediolî pregiianetriol ratio in molar pregnancy is as 1 compared with that of 20s î in normaI pregn an ay.
2* Mole tissue was incubated v/ith [4-*^o3 pregnenolone ae precursor, and 17a. hydroxypregnonolone, progesterone# 10a hydroxyprogesterone and I6p hydroxyprogesterona were isolated.
3• Cholesterol# pregnenolone# Î7a hydroxypregnenolone# pregnanediol# pregaanetriol and androatenedione
■ -V > .were isolated from extracts of mole tissue and theca lutein cyst fluid. t?a Hydroxyprogesterone was isolated from cyst fluid but not from mole tissue.
1 W .
4* Mole tissue is capable of atoroidogenesis but there was less eynthesis of progesterone than normal*
5. The increase in 17a, hydroxylation indicated hy the elevation Of the urinary excretion of pregnanetriol, is ovarian in origin# perhaps due to stimulation hy the large amounts of H*C«0*circulating in these eases#
Chapter 7# Urinary steroid excretion aftergonadotrophin therapy#
Io ovarian steroid hiogenesis is controlled hyand I.#11# It ia not clear that F#S*II*
has any specific effect on steroidogenesis hut L#H# can increase the rate of conversion of cholesterol into progesterone and the do-novo production of the latter#
2» The major precursor, of prognanotriol is 17a-hydroxyprogestcrone and there is a significant increase in the excretion of this metabolite in the luteal phase of the menstrual cycle# This is due to ovarian production of Î7a hydroxy-
16t.
progesterone#
5. Urinary pregnane trio 3. excretion also rises in the luteal phase of gonadotrophin stimulated oyoles and this may he a valuable measure of corpus luteum'function#
4# The excretion of this substance also rises Inearly pregnancy during the grov/th of the corpus
i y"luteum of pregnancy and folle to normal pregnancy levels after 6 - 0 v/eehs of gestation when the main function of the corpus lutcum of pregnancy appears to he past.
$. The pattern of urinary pregnane.trlol levels Invery early pregnancy agrees with that of the plasma levels of precursor 17a hydroxyprogesterone.
6. Urinary pregnanetrlol excretion up to 0 - 8 weeks of pregnancy may he valuahle in detecting the hyperstlmulatIon syndrome after gonadotrophin therapy# and also In monitoring the corpus luteum of pregnancy# It may indicate v/hen the latter is deficient wit# the resultant possibility of earl^r abortion.

3 02.
2. 0onelusi,ono
tm Women who begin childbearing with one or twoabortions have a relatively poor subséquentreproductive performance.
2. Urinary oestrioi and pregnanedioi assays do not ' help in forecasting abortion up to Hi v/eeks of
gestation and may not be helpful in diagnosing hydatldiform mole.
3. The conversion of progesterone to prognanediolis low in abnormal pregnancy.
4. The foetus uses progesterone to manufacture adrenal atoroids for its own homooatasis.
5* The increased I "/-hydroxylation which takes placein hydatid!form mole occurs in the ovaries probably due to stimulation by E.Q*G.
d., Urin'hry pregnanetriol excretion is a measureof corpus luteum function in the menstrual cycle and of the corpus luteum Of early pregnancy.
363
Fur the r work arising from this thesio#
U Investigation into the control of steroid metabo-liom Isi the human 3'oetue and footo-plac ont ai uni t #
2# Measeromcnt of other steroid motabolîtes e.g.ê and 16 hyclroxylated mctabalitos of progesterone in the urine in pregnancy# normal and abnormal.
Ù «
4.
Further investigation into the use of pregnanetrioX and also of plasma 3?a liydroxyprogesteronc in early pregnancy to assosa corpus luteum function and its possible use in forecasting abortion.
The use of these assays in the prevention of ovarian hyperstimulation with subsequent multiple ovulation and multiple pregnancy in tlierapy witti human gonadotrophins.

64
AcknowletÎKQmenfcs
The author owoa a particular debt of gratitude to the following people.
1* To ProfOBBor Sir Dugaid Baird who Initiallyprovided the environment for the first of theae studies and who encouraged the author andprovided the necessary facilities.
2* To Professor James Walker who has# during thepast 8 years provided every necessary facility and help for this work* Me has been a continuous guide and encouragement v/ith his interest and constructive criticism.
3. To Dr. Arnold Klopper who initially stimulatedinterest in steroid biochemistry and trained the author in steroid laboratory techniques.
4. To Mrs* Eileen Mlchle# B.Se.# for her help with the assays in Chapter 3 ami for many discussions.
5. To Dr* Marion Bluck (nee Greig) B.Sc.(ilons)# Ph.D. for her technical expertise ia Chapters 4 and 5.
165.
6. To Or. JolUT* CouttBj, B.Sc* Ph.D.# forhio toehnical vmrk la the inveetigation in Chapter Q and for contimsiiig education of the author in 8toroid biochemistry.
?. To Miss M.C.K# Brcnniingf B.Sc. (Hone)# for some of the assay results reported in Chapter 7.
8* TO Mr# W# Cooper# Chief Technician# Department of Ohs te trice and Gynaecology:^# for help with the assay0 reported in Chapter 7.
§. To Mies Carol Howat and Mrs. Catherine Gibson for their help v/ith the preparation of this thesis.
B P m m i O l O G I C A L AND HORMONE STUDIES IN EARLY HUMAN PRBGNANOY - N O m A L AND ABNORMAL
APPENDIX
I# PlatOG*2* Diagrams3. Tables*4# References* 5* Pnbilcatione
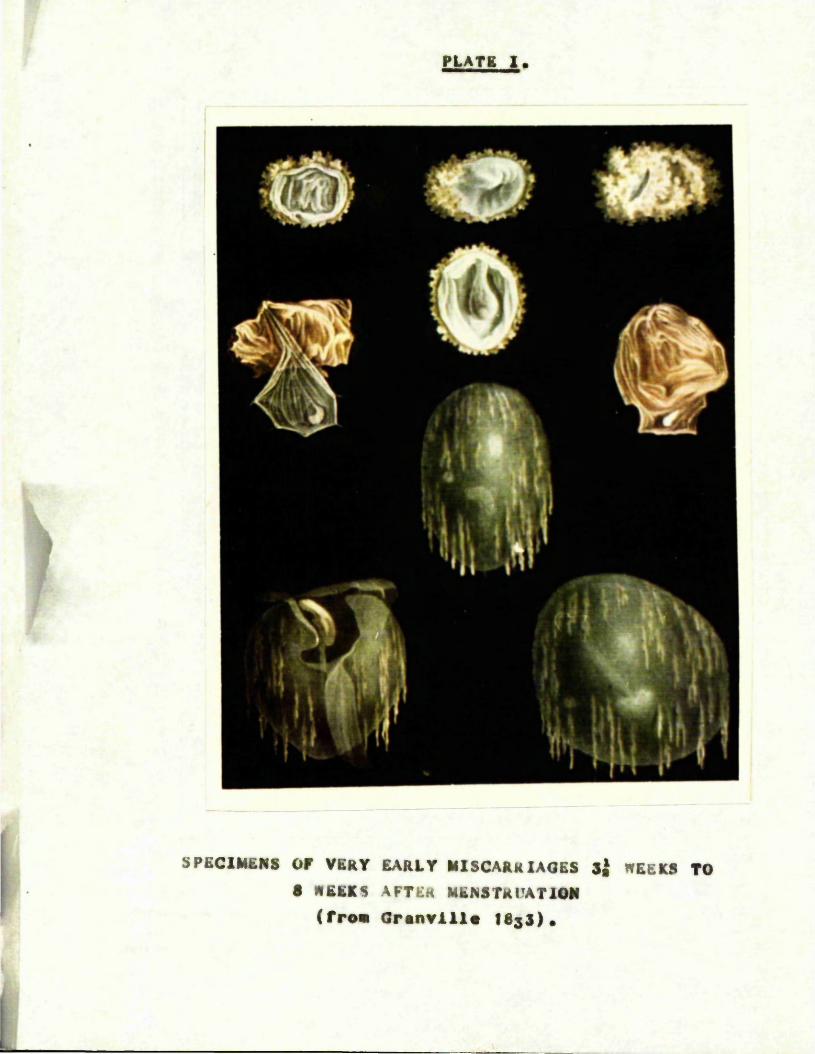
PLATE 1.
4
s
SPECIMENS OP VERY EARLY MISCARRIAGES Sj WEEKS TO 8 WEEKS AFTER MENSTRUATION
(from Oranvill* ISgS)«

PLATE II,
i|)j VboruftHA
SPECIMENS OF MISCARRIAGE 9 AND 10 WEEKS AFTERMENSTRUATION
(from Granville ISsS),
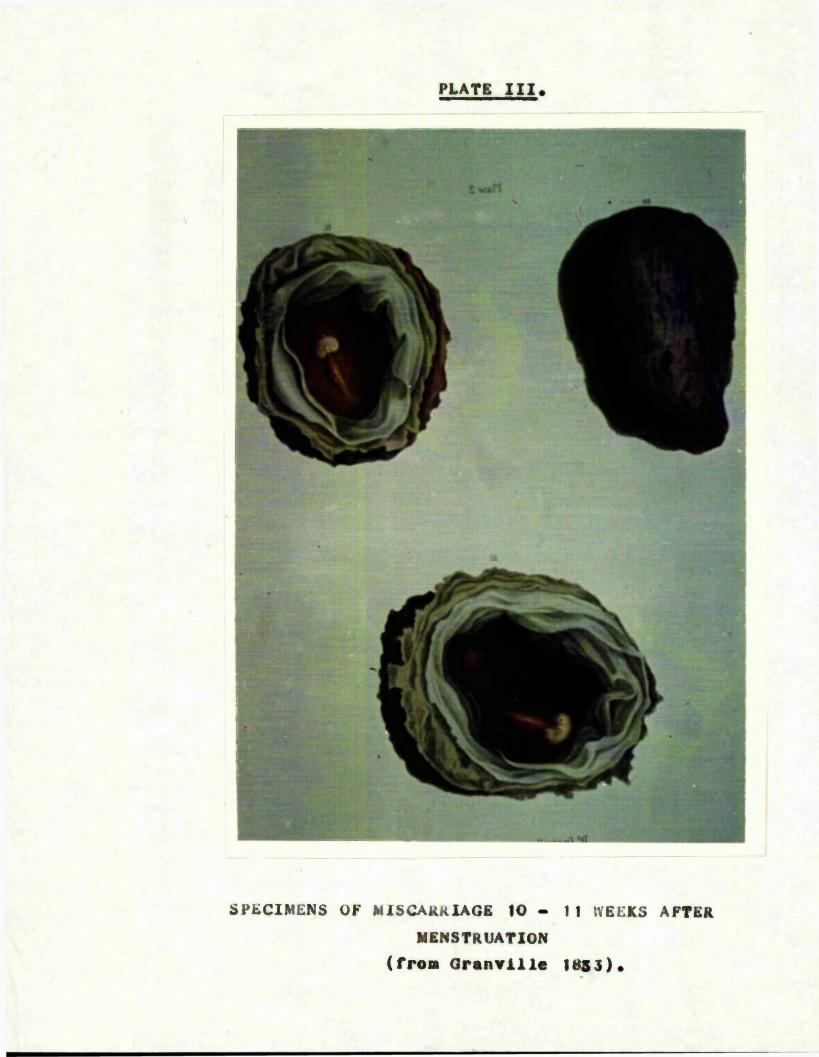
PLATE III.
IK
F
i M
rSPECIMENS OF MISCARRIAGE 10 - 11 WEEKS AFTER
MENSTRUATION (from Granville 1853).
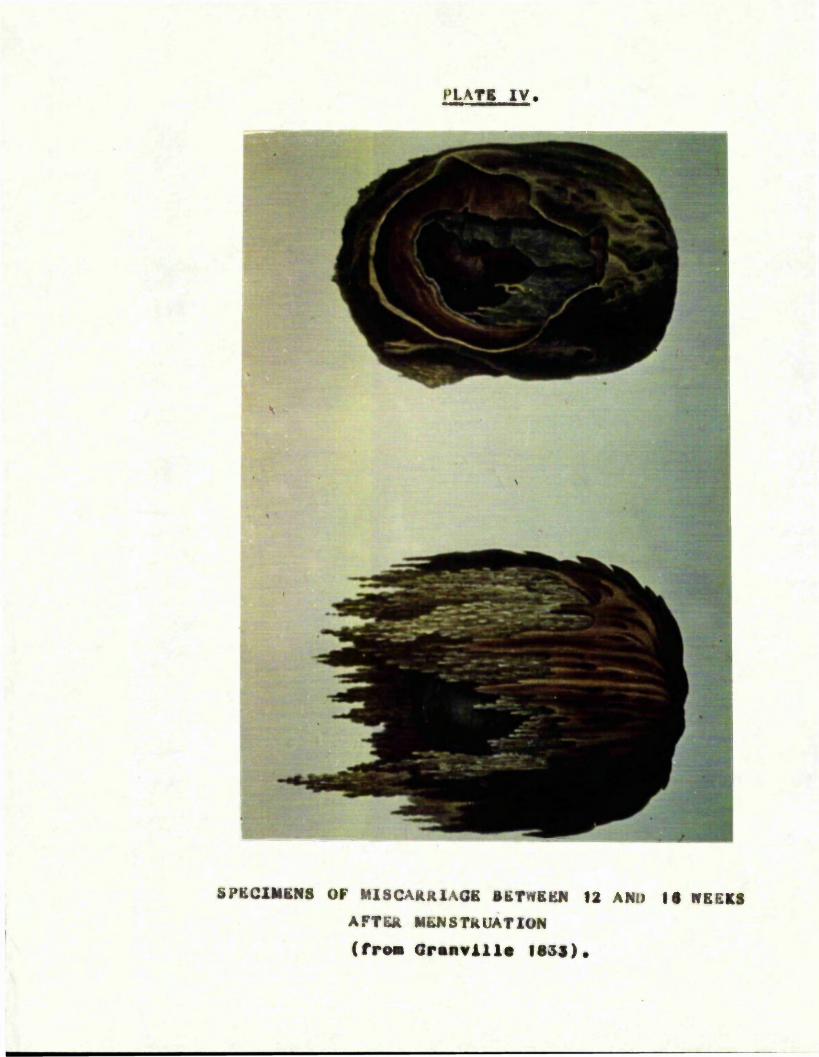
PLATS IV.
è
- I
SPBCXMKNS OF MISCARRlAOB BBTWBKN 12 AND IS WBEBS AFTER MENSTRUATION ( from Oranvill* less).
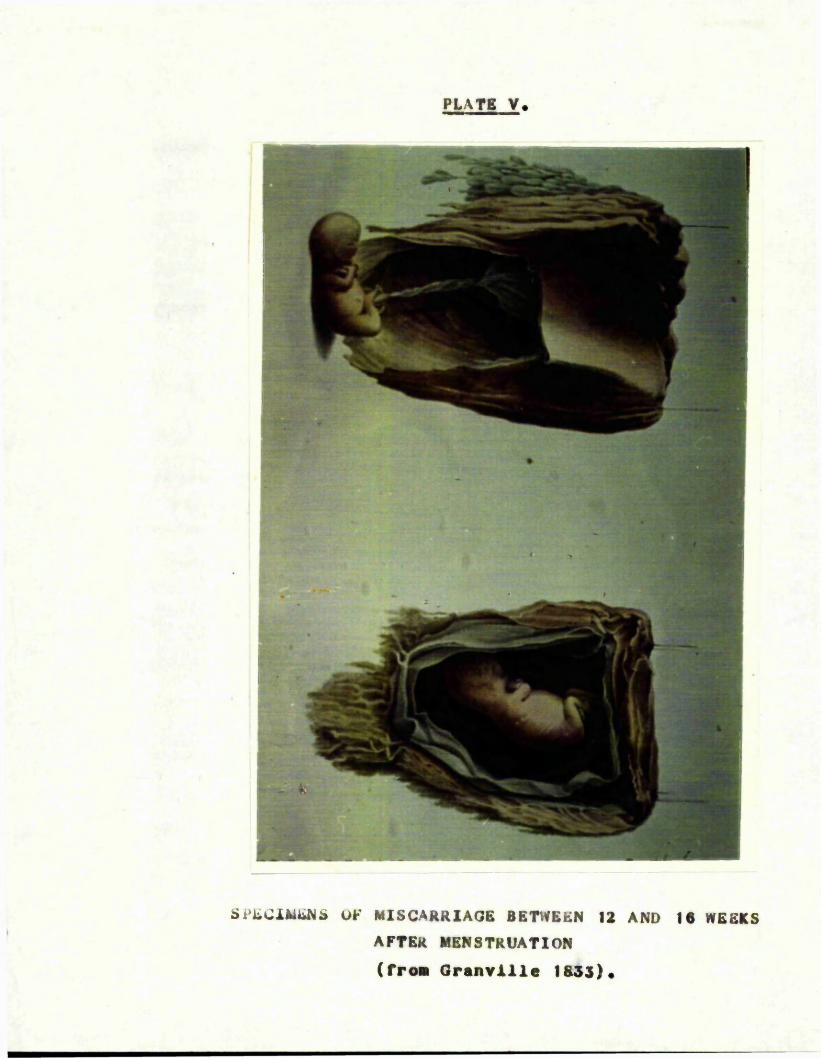
PLATE V.
ü
SPECIMENS UK MISCARRIAGE BETWEEN 12 AND 18 WEEKS AFTER MENSTRUATION (from Oranvlllo 1833).
PLATE VI.
L
SPECIMEN OF A MISCARRIAGE AT FIVE MONTHS (fro. Granville 13s3)
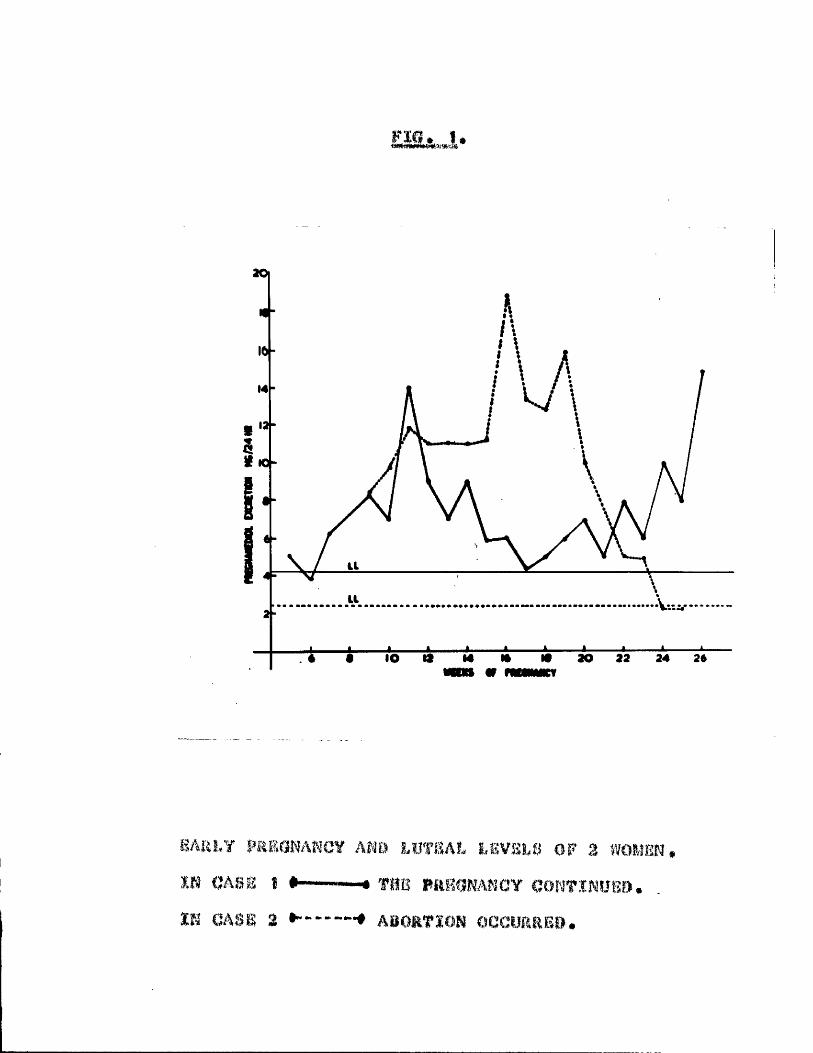
20|
16-
2 -
lO 20 22 24 26
m a L v AND iL8V! L8 3 w o m m .IN 0A8gg $ #---- — # Tim m a m W N C Y qONTINUSD.IN CASE a ABORTION OCCURRED.
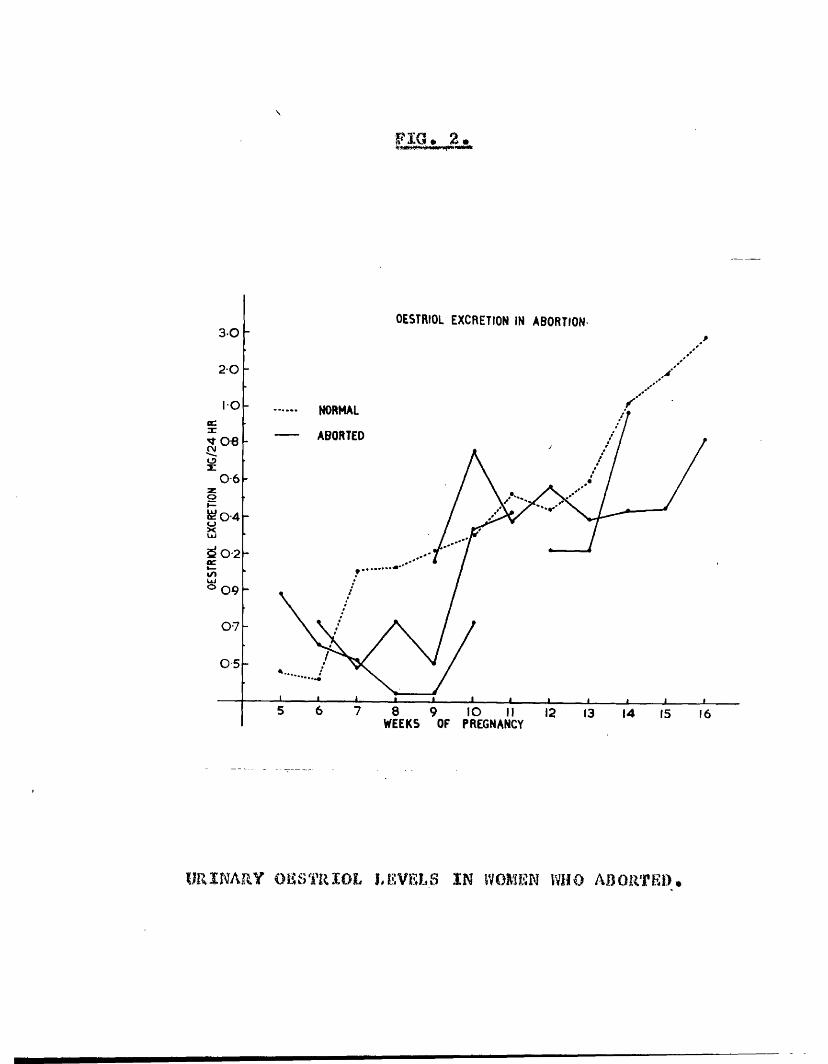
‘1 0 . a .
OESTRIOL EXCRETION IN ABORTION3 0
20
NORMAL
ABORTED
0 6
d02
0 7
0 5
8 9 lO IIWEEKS OF PREGNANCY
URINARY OESTRIOL LEVELS IN WOMEN WHO ABORTED.

FIG O
St«fO>d Ekcrction in Vitr«utcr><x Ocoth
15 ■
8 -
4 -
3«4
PREGN4SeDtO13 -4
TTTT8 lO 12 14 16 It 30 33 34 3«
*44» of prifiMncy
OSSTRÏOJ. ÂK» p r s o m a n e d i o l b x g r k t i o n in aWOMAN WHO ABORTED AT 26 WEEKS

FIGo 4,
mean
I ' I ' I ""I ' I ' I ' y Ie 12 16 20
PREGNANEMOL/OESTRIOL RATIO IN NORMAL PREGNANCY. ABSCISSA AXIS - WEEKS OF PREGNANCY.ORDINATE AXIS - PREONANEDIOL/OESTRIOL RATIO,
(From Kloppor and Blllewlcz 1063)
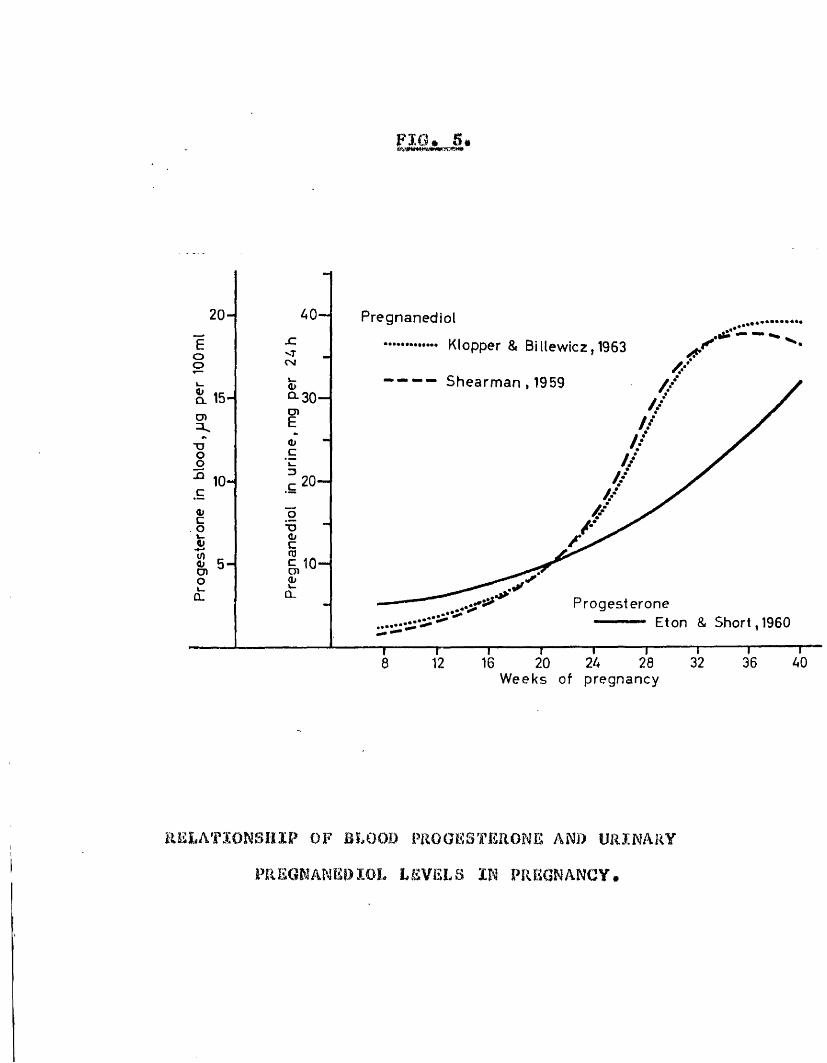
FIG. 5.
20- Pregnanediol
Klopper & Billewicz,1963<rCMoo
Shearman , 1959Û. 15- cn
TJ-Q 10-
O)O-
ProgesteroneEton & Short, 1960
16 28 32 36 40208 12Weeks of pregnancy
R E L A T IO N S H IP OF BLOOD PROGESTERONE AND U R IN A R Y
PREGNANE*)lOL LE V E L S IN PR EG N A N C Y•
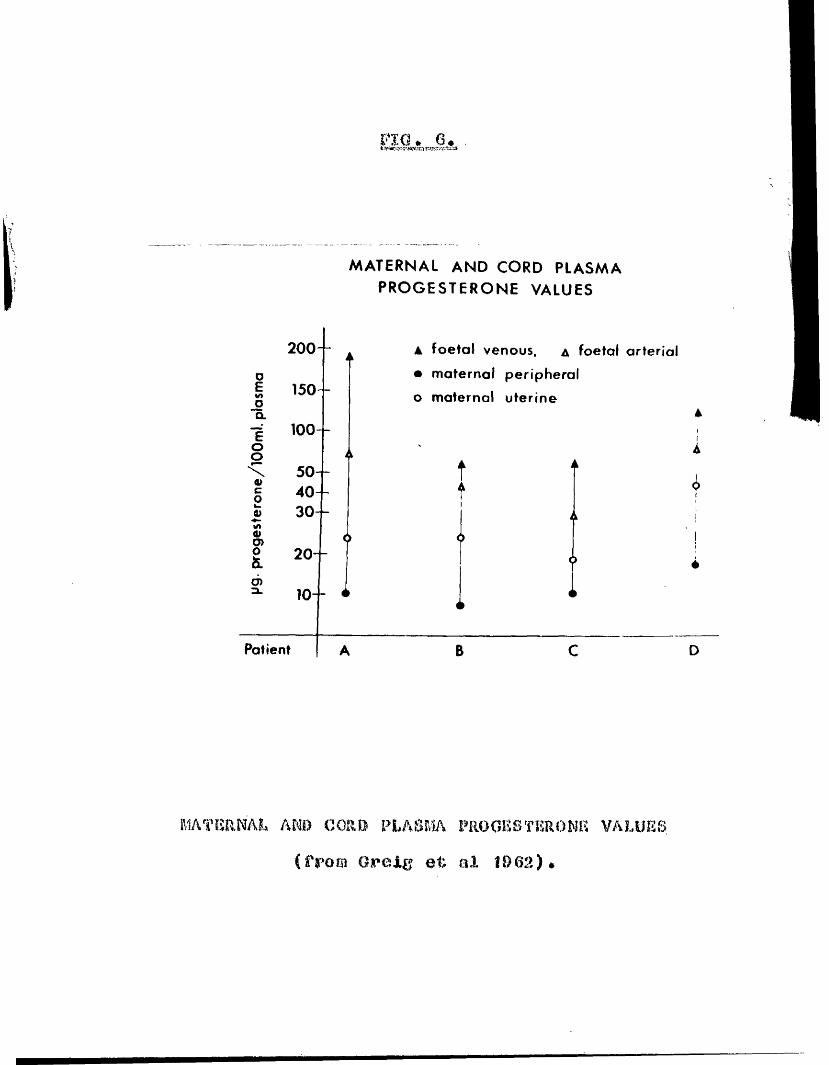
F i a . 6 .
MATERNAL AND CORD PLASMA PROGESTERONE VALUES
200- . ▲ foetal venous, a foetal arterial
o • maternal peripheralE 150-o o maternal uterine"5. 4-g 100- 1oo i\ 50- f i
1o>§ 40- t t1 30- éL 1
s> (> <> ' !o 20- <> AO) 10- i < <
*>
Patient A B C D
MATERNAL AND CORD PLASMA PROGESTERONE VALUES (from Oreig et al 1962).

FIG. 7*
F O E T A L P E R F U S I O N A P P A R A T U S
T o u m b . v n .
F r o m u m b .
H e p a r i n i s e d o x y g e n a t e d t yp e " 0 " adul t b lood pH 7.4
P e r f u s i o n C h a m b e r wi th foetus in 50% H a r t m a n n ’ s so lu t ion .
FOEÏAL PERFUSION APPARATUS.
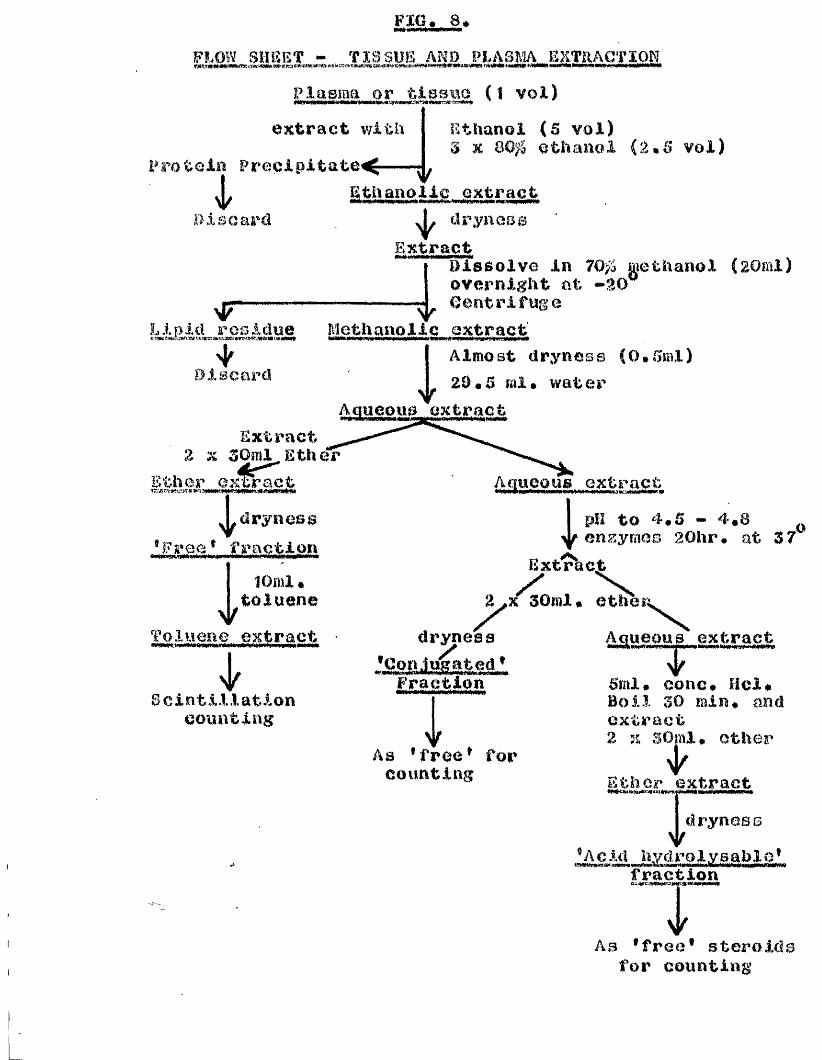
FIG, 8,FLOW SHEET - TISSUE ANO PLASMA EXTRACTIONWW«Wi WVII' I i«MI WMMaMMt
Plasma or. tlasw (Î voi)extract with Ethanol (S vol)
3 K 800 ethanol (2*5 voi)Protoiïi Precipitates^
^thanolic extractPisoarcl clryncBs
Extract
1
Dissolve in 700 methanol (20ml) overnight at -20Centrifuge
L1pid residue Methanolic extracttsvie l a m w m M f H , * s . | i w < » i> i i » i n « iw w i i | i W « « i m a i « H M « i * » ^ i i m I n w j i j W i W M i m #
I Almost dryness (0#5ml) I 2BmB ml. water M u e p u a extract
Discard
Extract 2 X ^Oml_Ether
Ether extract
iAaueous extract
dryness ® Free * fraction ipH to 4*5 - 4.8 enzymes 20hr. at 37o
Ex turbot10ml.
tolueneToluene extract
Idryness
niu^jte^ * Fraction
ettîfeîA queaus extract
Scintillationcounting iAs •free * for
counting
5ml. conc. Hcl. Boil 30 min. and extract2 n 30ml. other
4 ^Ether extract dryness
’Aoici nyai«WMgaagarjwMM taerfWVjittCTaii . ...fraction
VAs *free* steroids
for counting
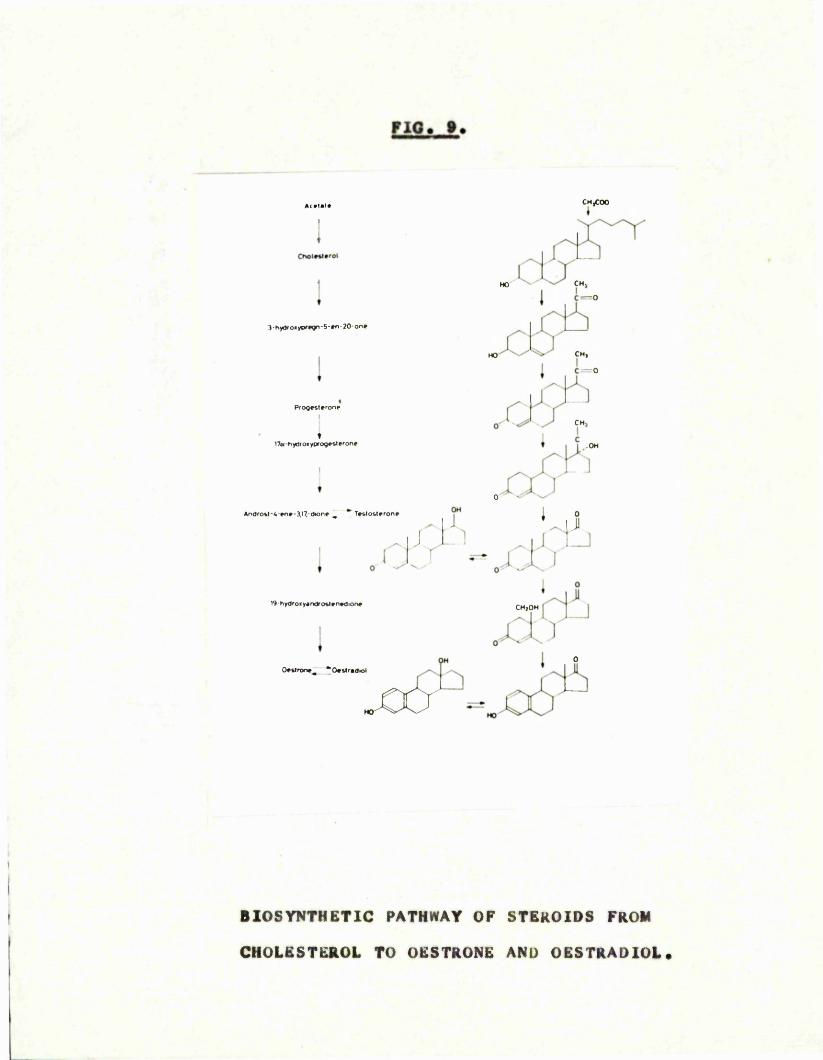
PIO. 9.
CMfOO
3 - hydr o« ypftgn - 5 - »n - 20-on »
P ro q e s l* ro n »
♦17b hydroiyprogv&lFron»
I
♦
Andro» t-4 -»n*-3 ,17 .-(lionF _ * T e t lo s l f r o n r
CH,HOC— 0
CHjc
« •OH
0
19-hydroiy«ndro&l»nFdionF
O F U ro n *^ * 0 * & lr » d io l
; OHiI . J
• * .i i, ICHjOHh ' j
. .X. L 1
^ r i i
BIOSYNTHETIC PATHWAY OF STEROIDS FROM CHOLESTEROL TO OESTRONE AND OESTRADIOL

P M . 10.
99
9 8
ffi 9 7
4 0 n
:3o-
T 2 0 .
CM
DA Y S F R O M L H - P E A K
MEAN SERUM L.ll. LEVELS t S.E. ÏN 10 NORMAL MENSTRUAL CYCLES,
(from Mlclsley and Jaffo 1966).
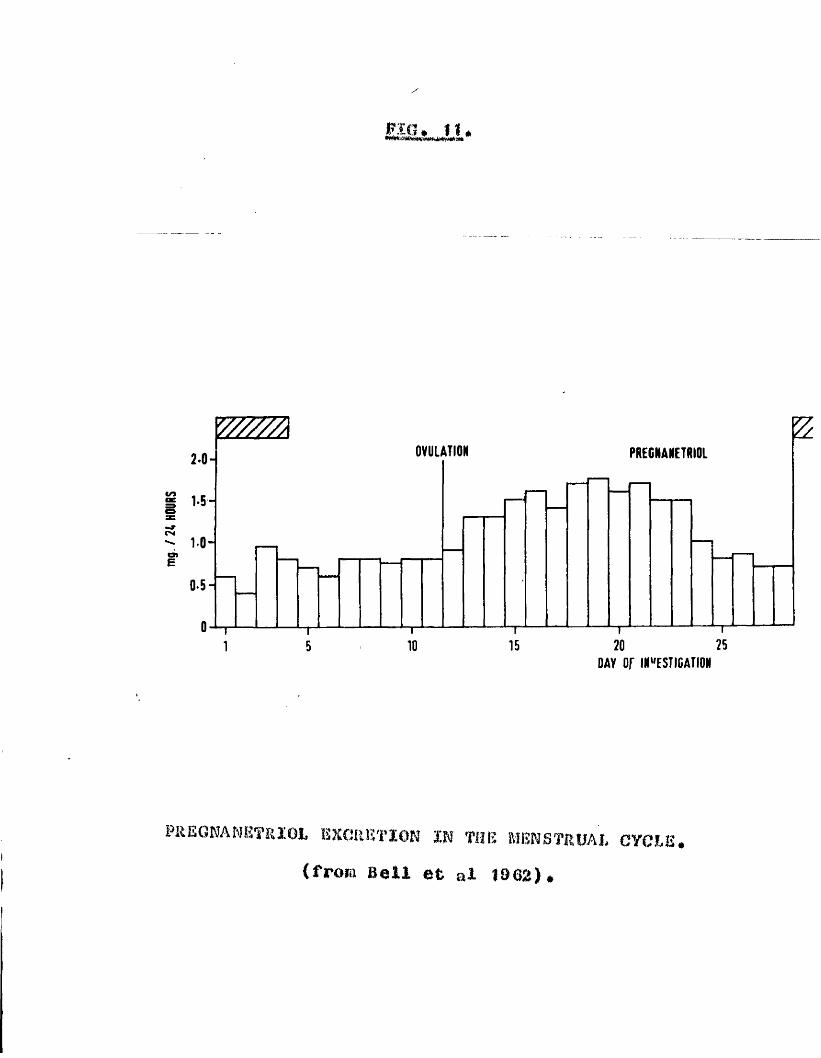
PIG, I I ,
2*0“
1- 5 -
1 0 -
I*0*5 -
O-r 1
OVULATION PREGNANETRIOL
1-------------------------------r
20 25DAY o r INVESTIGATION
FREGWAMKTRIOI, EXCRETION IN THE MENSTRUAL CYCLE# (froia Beil et al 1902)#
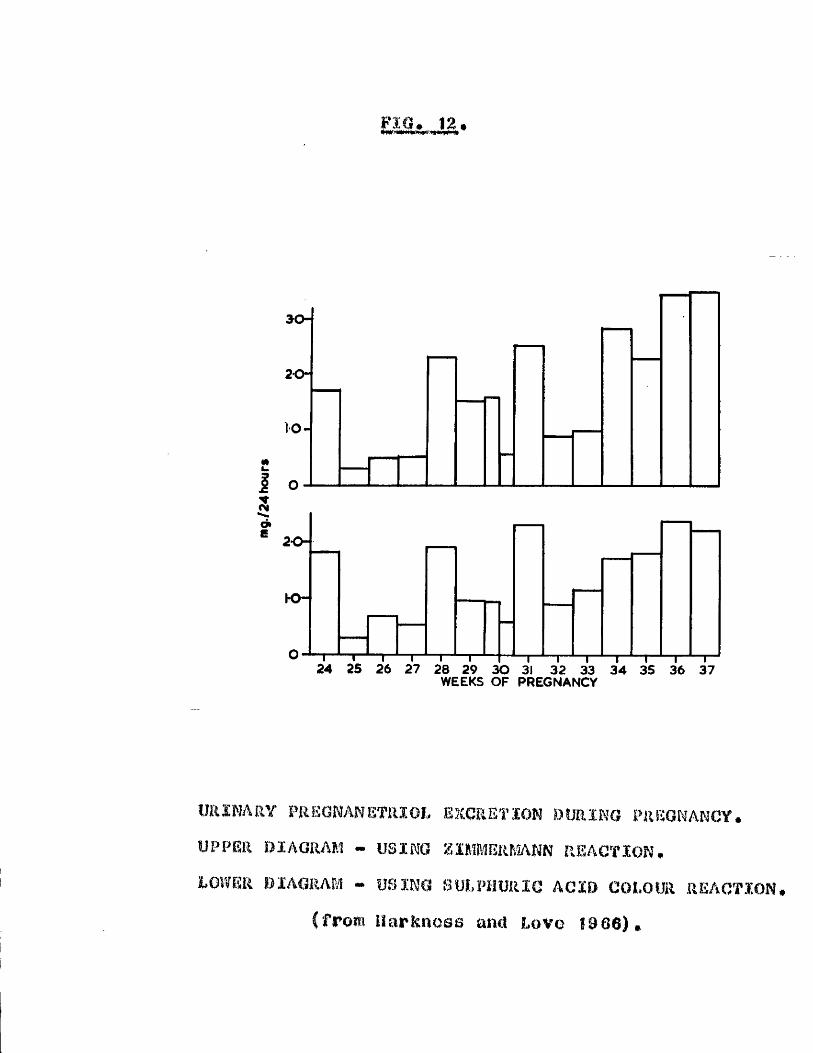
3 0 -
20-
O-c1 o-$o*E 20-
T ~ - ~ f24 25 26 27 28 29 30 31 32 33 34 35 36 37
WEEKS OF PREGNANCY
imXNARY FRSONANETMOL excretion DURING MlEGMANCY. UPPER DIAGRAM - USING %IMMERMANN REACTION#LOWER DIAGRAM - USING SULPHURIC ACID COLOUR REACTION#
(from Harkncss and Love 1906)»
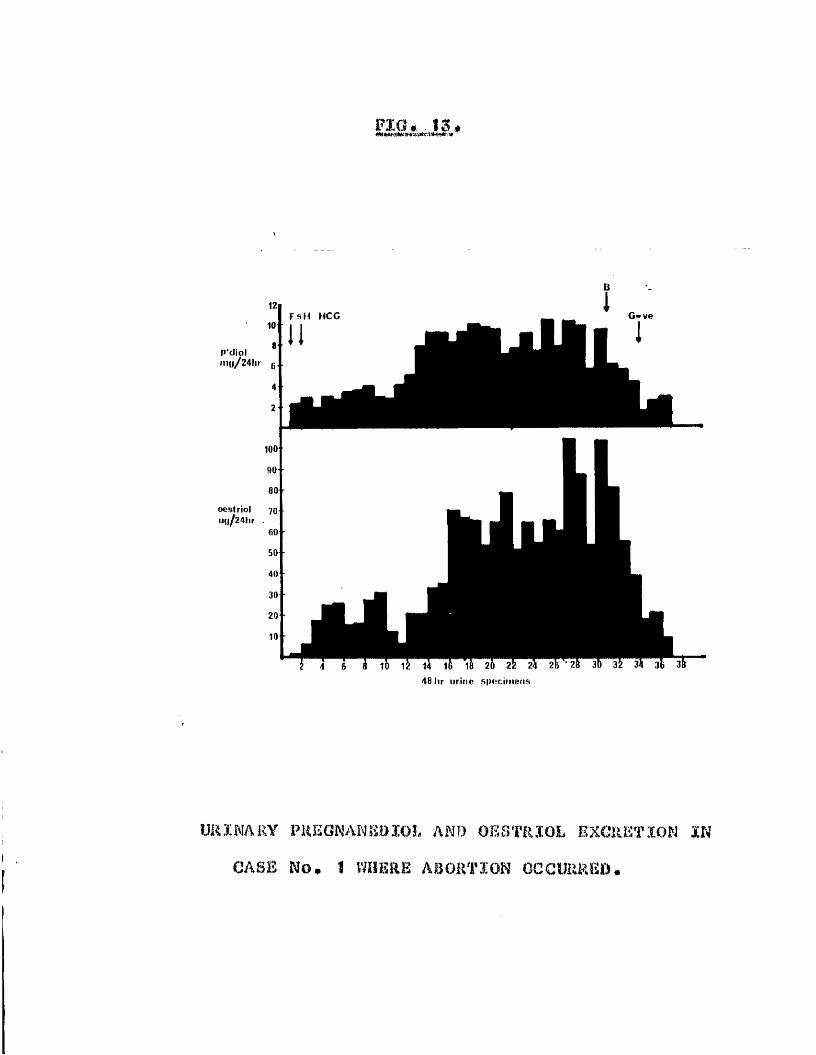
P'dtol ino/24hr g
oeslriol 70 iiwflAUr .
FIO,.15.
G " veFsH HCG
48 hr urine .specimens
URÏNARY PUKONANSÎUÏOL AND OESTRIOL EXCRKT.ÏON IN CASE No. 1 WHERE ABORTION OCCURRED.
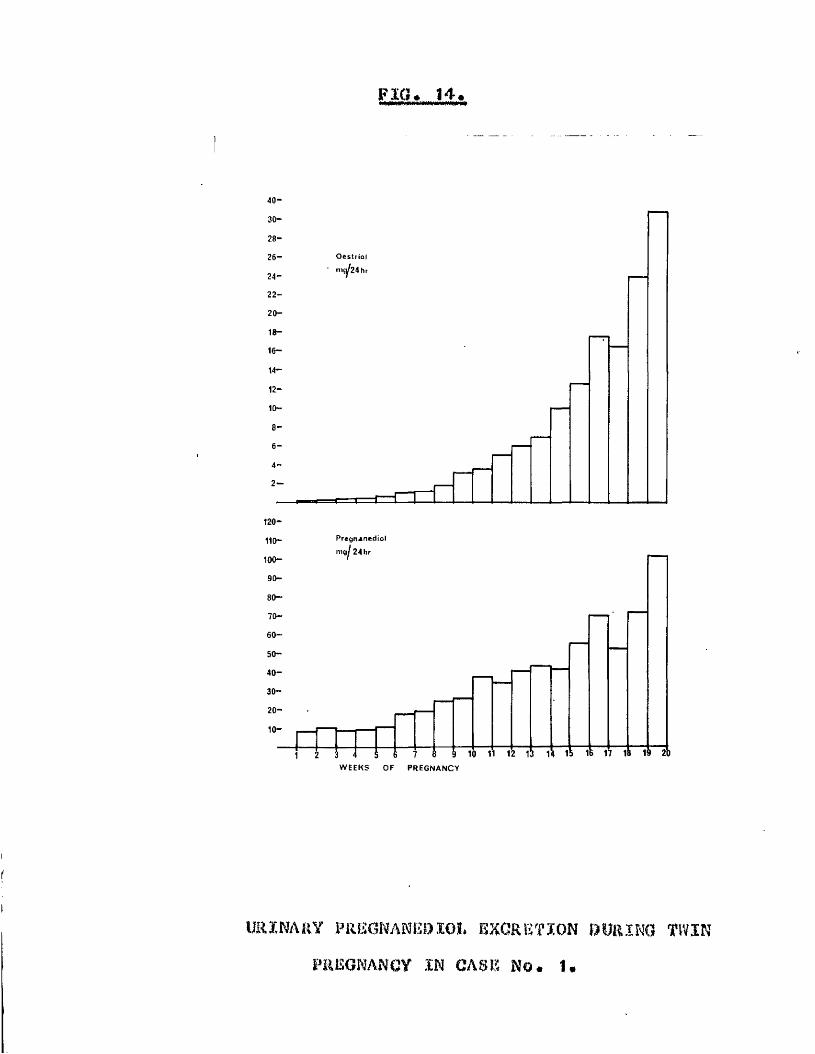
PIC. 14.
O e & t n o l 24 hr
120-
110- P r e g n a n e d i o l
100“
90-80-
60-50-40-30-
10-
W E E K S O F P R E G N A N C Y
IJRÏNARY PREGNANE!).ÏOL EXCRETION DURING W I N PREGNANCY IN CASE No. 1.

FIG.. IS.
200“
ug/24h100+
P ’diol
10-mg/24h
P'triol
2*5Hmg/24h
F T - K t - n 1 I---L I-- L3 9 10 iV 12 131 2 3 4 5 B 7 Ô 9 10 1'1 12 l3 14
48 hr URINE SPECIMENS AFTER INJECTION
URINARY OESTRIOLt PREGNANSDXOL AND PREGNAMETRIOL EXCRETION IN THE CYCLE IN CASE No. Z BEFORE THE CONCEPTION CYCLE

FIG# I f -
IS
14
13
1211109
87
654
3
21
40-
30PD
PT
2010|-
10-
8-64
D T n T -
5 10WEEKS OF
15 2PREGNANCY
URINARY PREGNANEDIOL, PREONANETRlOL, AND OESÏRIOÏ. EXCRETION IN CASE No. 2# IN
p r e g n a n c y u n t i l 30 WEEKS OF GESTATION

45'-40-
3 5 -
3 0 -
25-20-15—10-5-
5-
4-—
3-
2-1-
O Z L
OESTRIOLus/24hr
Pregnanediolmg^24hr
2-1-
Pregnanetrîol>ng/24hr
2 4 6 8 10 12 14 16 18 20 2Z 24 26 26 30Days a f t e r In je c t io n
tlRÎNAR? i»RSaNAt'mOÏOL* PftSCîmHBffaOI. AND OKSTIUO!. BxeREfîON IN m m ? a m M u m î O P & m s v m m A ' m B
c m s 0AS8 No* 3.
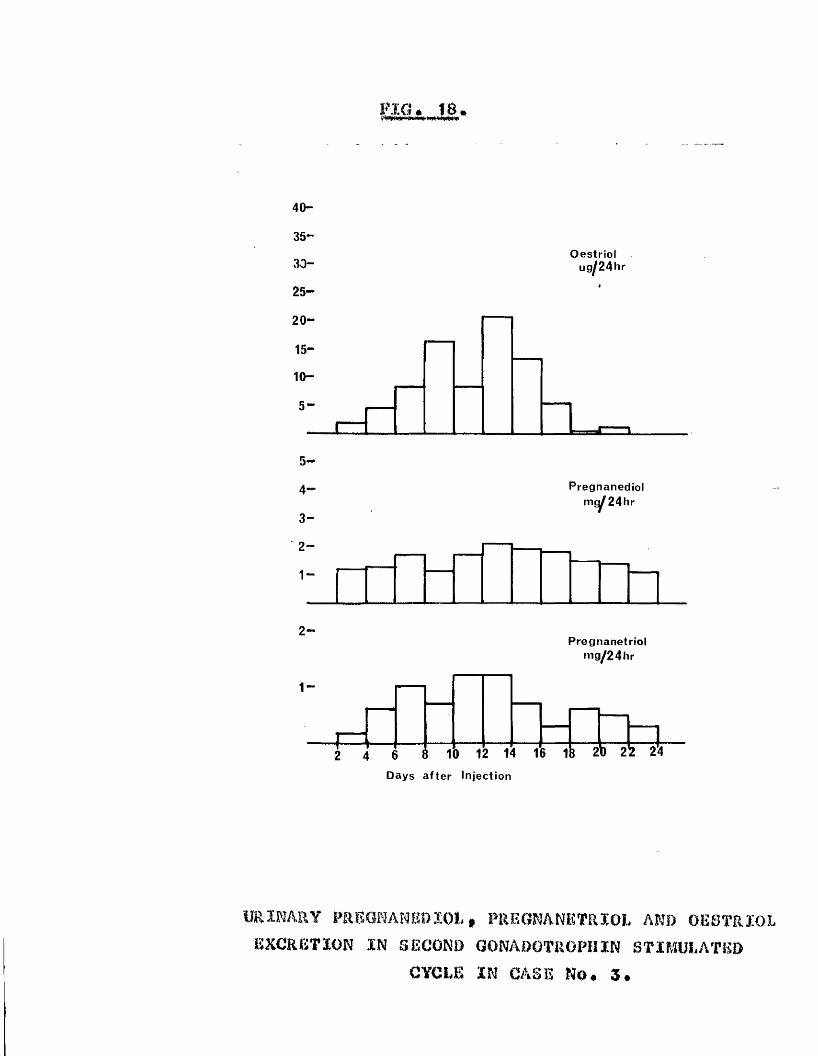
MO* IS*
40-
3 5 -
3 0 -
2 5 -
20-1 5 -
10-5 -
O estriotu g /2 4 h r
5 -
4 —
3 -
2-1-
Pregnanediol i 24hrm(
2-
1-
Pregnanetrio lm g /2 4 h r
i 2 2!2 4 6 8 10 12 14 16 18 20 2 2 !4
Days a fte r In jection
URIRAftY PREGNAMEBÏOL, PllEGRARETRÏOL AND OESTRIOL EXCRETION IN SECOND GONADOTROPHIN STIMULATED
CYCLE IN CASE No. 3.

FIG. 19.
110“ /
Oestrio)
8“7“
6*-5“
4“
3“2“1“
Pregnanediol myg 4 hr.
--
-r— 1— 1— i—
Preonanstriolmg/24hr
I 1-- 1— f— 1— 1— 1— 2 4 6 8 1a 12 1 1 1B 20 22 24 26
Days aflci Injection
URINARY PREGNANEDIOL, PRISGNANSÏRIOL AND 0E13TRÏ0L EXCRETION IN THIRD GONADOTROPHIN STIMULATED
CYCLE IN CASE No. 3.

PIG. 20.mtaemriimmimmmixfà ■
5 -
4 -
3 -
2 " 1-
Oestriolug^24hr
HCG
g .. Pregnanediol j mg 2 4 h r
2 1 -
1-0-0-80*60-40*2
P re g n a n e tf io l^ mg 2 4 h r
FA F ï F ü4 5 ID A Y S
1b 1
URINARY EXCRETION OF OESTRIOL, PREGNANEDIOL AND PRSGNANEÏRÏOL IN AN OOPHORECTOMISED, HYSTERECTOMISED WOMAN AFTER STIMULATION WITH F.S.ÎI. AND H.C.G.
CASE No. 4,

HCG
oo HMG
3,0
CO
o
3224 2820128 160 4WEEKS
PLASMA 17a HYDROXYPROGKSTERONE LEVELS DURING GONADOmOPHIN INDUCED PREGNANCY.
(from Yoshtei et a I 1969),

n o * 2 2 .
? 10hEOO«y
UizoaaUJ 5♦—*/>wooacCL<f%</>_ja. 0
'T" T HCG T— r
HMG
/
0 4 B 12 16
too
to
10
i 01
0 01
u*5oo
nI
20 (/)
10
T3%)oRt/iozm*1:•oso3
WEEKS
170, AND PLASMAiniOGEBTBRONE LEVELS DURING GDHAOOTROPHIN INDUCED PRECmNCY. s m w i W DIVBRGENCB OE TDK
CURVES AT 0 " a WEEKS CESTAT3:0N (from YoihiwC eL ai ID60)
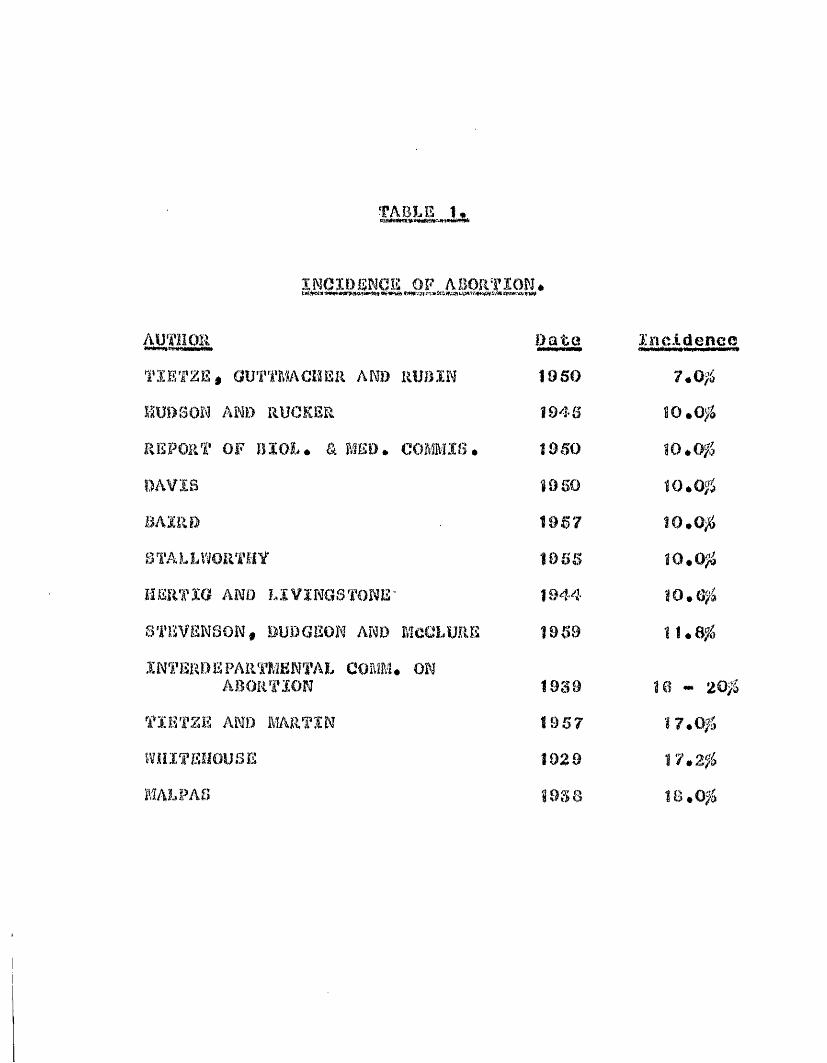
•FABLE 1.
i n c i d e n c e o f a b o r t i o n .
AUTHORTIETZE, aUT'i'MACISER AND RUB INHUDSON AND RUCKERREPORT OF BIOL. & MED. COMMIS.DAVISBAIRDSTALLViORTHVHERTJG AMD LIVINGSTONESTEVENSON, DUDGEON AND MCCLUREINTER!)EPARTMENTAL COMM. ON
ABORTIONTIETZE AND MARTINÎÏHÏTEHOUSE MALPAS
Date19S0Î94SÎ9S0Î950196719SS194419S9
1939198719298938
Incidence7.0#10.0#80.0#10.0#10.0#10.0#10.6#11.8#
18 - 20# 17.0# 17.2# 18.0#
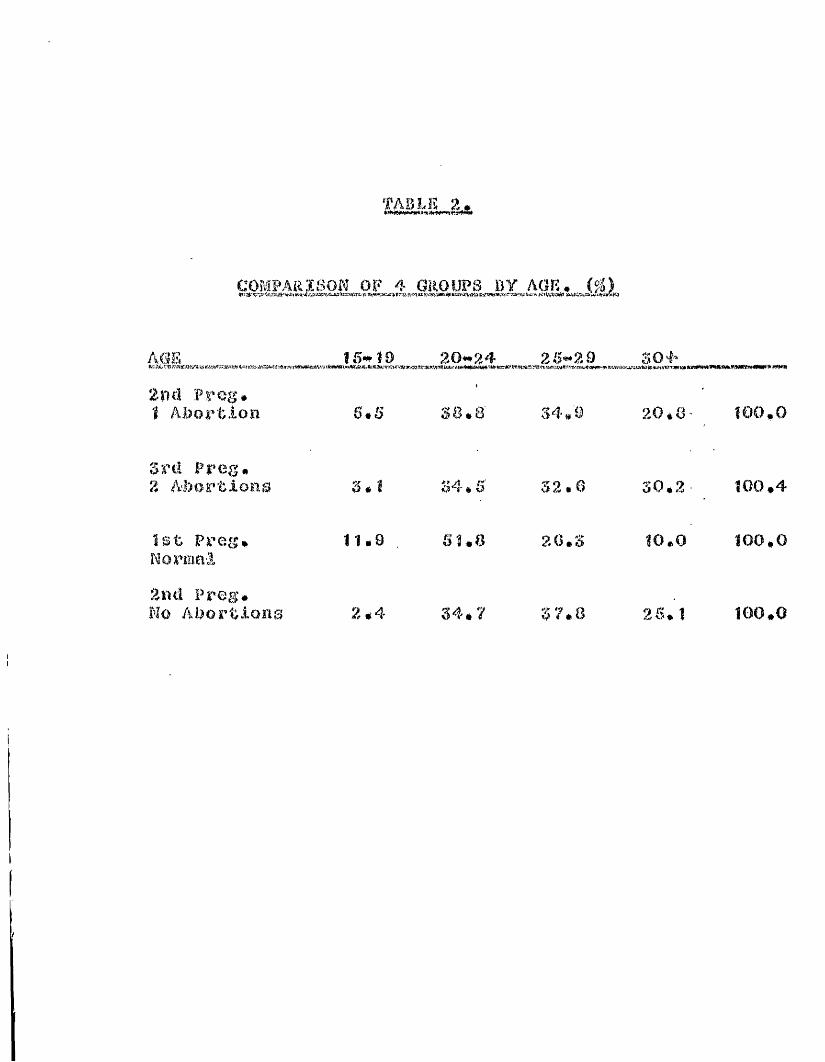
TABLE 2,
COMPARISON OF 4 GROUPS BY AGE. (#)
m IS* 19 20-24 28-29 304'
2nd Preg.1 Abortion 6.5 38.8 34,9 20.8 100,0
3rd Ppeg.2 Abortions 3.1 34,6 32.8 30.2 100.4
1st Preg, 11.9 51.8 20.3 10.0 100,0Normal2nd Preg.No Abortions 2.4 34*7 3 7.8 26.1 100,0
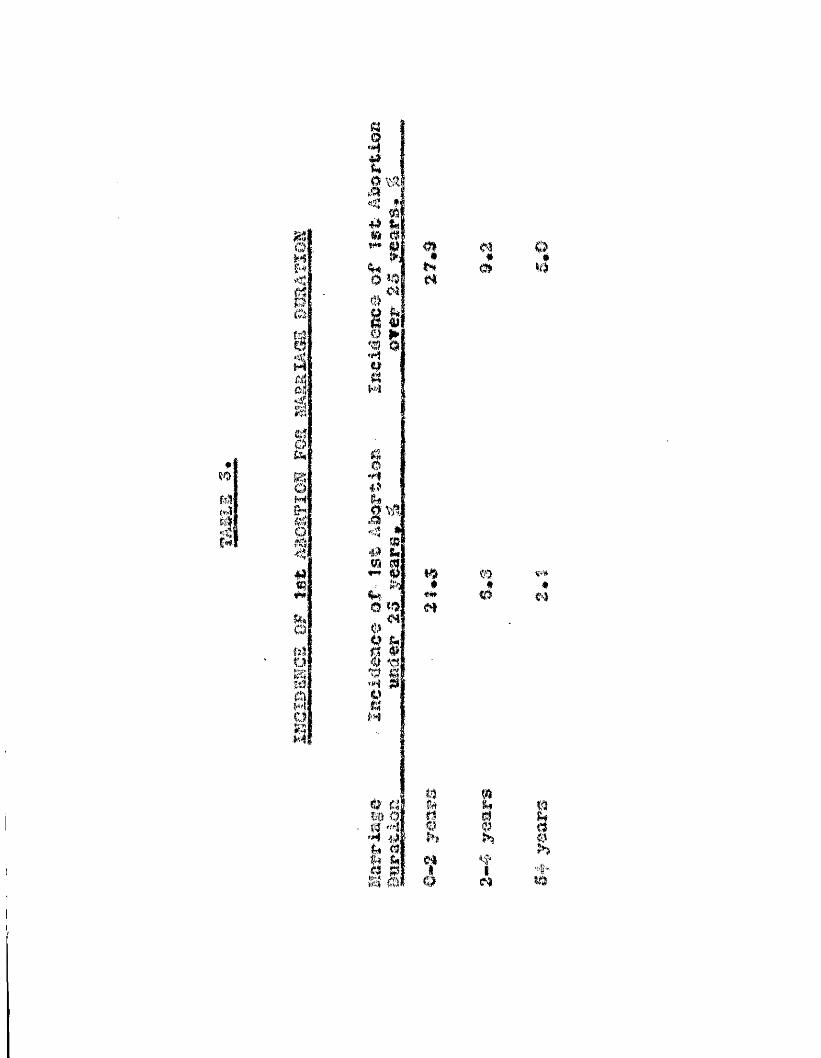
«
m(Mg
ma0MH<fôî
1Klej
mMlQrai4
iNiOisSO
tgî®!> :# (% ^ p. *
6* : _ 0E&i 0 >*•'Mg0•14.V0.a#m
#m
4 ' o(%
f)4 <03 1sM
#Nm*o
oll
m Çï'** # ##* 0 mm
^ # w o
d ,,itm
I
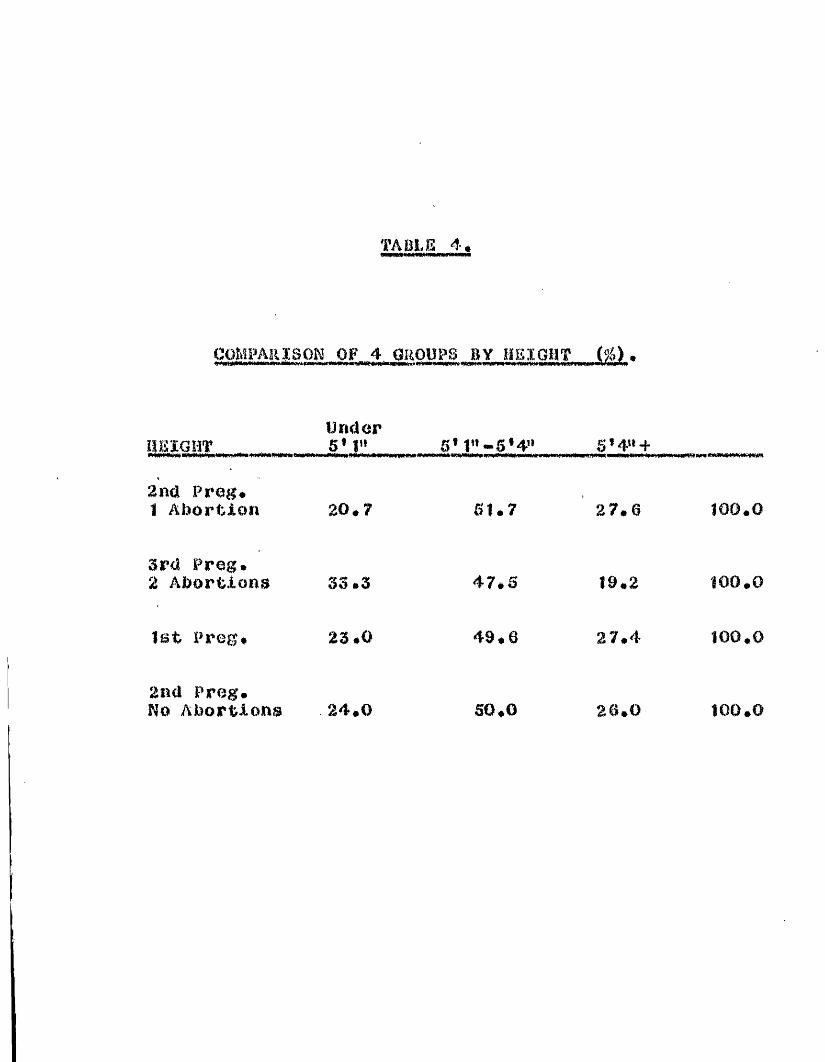
TABLE 4.
COMPARISON OP 4 GROUPS BY HEIGHT (#>.
UnderH E I G H T ________5* I"______ 5* 5,411 +
2nd Prog.1 Abortion 20.7 61.7 27.0 100.0
3rd Prog.2 Abortions 33.3 47.S 19.2 100,0
1st Preg. 23*0 49.0 27.4 100.0
2nd Preg.No Abortions 24.0 30.0 26.0 100.0

'■ At
COMPARISON OP 4 GROUPS BY HUSBANDS SOCIAL CLASS (#).
SOCIAL CLASS 1 & % 3 4 6 5(,l Preg.
1 Abortion 12.4 64.1 23.5 100.0
3rd Prog.2 Abortions 14.7 56.0 30.3 100.0
1 Prog. 11.1 64.9 24.0
2nd Preg.No Abortions 9.6 62.5 27.8 99.9
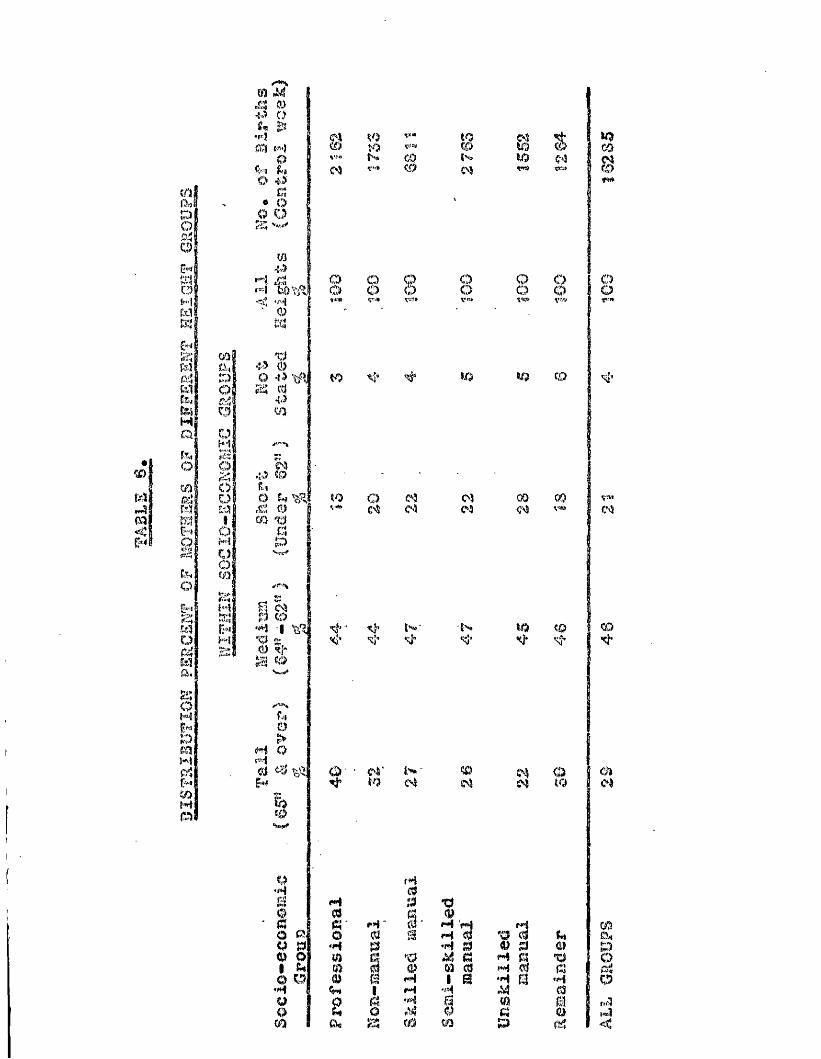
m M4.: o
m t«>) 0
O *5m • oQ Q z;
w'î',
0î%3
e% to T"* to 03 1m to çjm W co 1 ^N co w 10 05 i ^O) V-» aù 04 t-S> 1 ©
I f *
M f. O o gr -j i o o o< «"'i Kf 8 O O O O ooT"'*
mÊi,:DIuH'îOO0 M1oOom'
43 0o 43 "AlS 04.) 10 '
M <0UO S*IR|et'.! Ojm g
to
to OC>S (S
lo
mtM
00 OO
<sj*
m
!îwH'I
f-3 © ,'M #%ï g:# <'|-tf' ‘ îi; V
■{v**<;* m # m
f I0M Q M ,<!i ^1*1
O C4‘ N ' W (4 0sM
a f40
0H03 1« eî' M 0* H 'HO 0, o 0 û H 0 "00 K> ‘H P •H 0 0
0 O m "O cî M1 A* m m 0 m 0 f«4o o 0 M 1 H •H
H 1 M M A#u o '## a mo O 000 0@ h ; fû 00 p
tQ
Tîm
'3i
ChCh
09&,§Oi«3

mm
<
Ï<<!Ma<53 IÏ»SIm53
Cl5'00i'4<£[531moC/ÎmCQil
ll-'sS<S'
0i qO 3 M O* êuom
,"-4, ffa,*to o © 't 0 o o* # • * * * I #N V" to I aM C>3 to to t. w 1 to'Vii,' Vt?r V=iJ* W;* iO 1*» o m ÏO IfSK»to (0 00 N to i to© © tf) 5*1* to Mto
I'fi'id’0#4W PW'I0r*J B 00 a0 00 a 0 a# m3 0 MO 0 m M•H fj »MM
0m a '0 mj0 W 0 m mi0 a r»| 1 "44*y 1 M MO q0 a toU .i4 0 f*itu © © P
0I"4I03
Tj I ,m?r* <**«» filn01 ca Ch s». to ÇVO431 • 0 • « # « •0 t to o M N © ©4*3 t> GO m tO. 0Ï ODCO S,!»" w v-v» ««(jtJf 'tew Vkj*>E3 to © (0 ' QO; tiO w © %l* © © 1 m4% m Ç!» ©
/*•** ,!«*>5 00 to © m tom ♦ • « # ♦ « 1 «
4-3 © N 00 to V*» CO fw I (DM N to toO im s*y \tz Sr,-V V«!.CÎ 0 to0 *0 a v m 1' o0> <>3 xim o SOrj"*w/ çse <0 to m toXifi
(««'■*to !1 to o xj' to M !“ !1 * * # * # # •fi tMi to !,Q S3 vw O i m0 toI m CO to to to e)
•f4 1 jI "'tW Vçu' VJUT? Vw<* V(4;(, VsTf'0 s: m0 p $0 0> to CO O^ © N to «*w © N oN e4 r-» to N ©<M
Li /**■'%O I O N N to to> • * « « * « «M O m to © © VB» m 10•*“•3 V-* N M to m0 Vïr w ■'■Jfciïü,!
i: r* to Ô M m MÎ0 o m to to C4© C4 KO 05 ¥11* sj*
tf*JI'■4
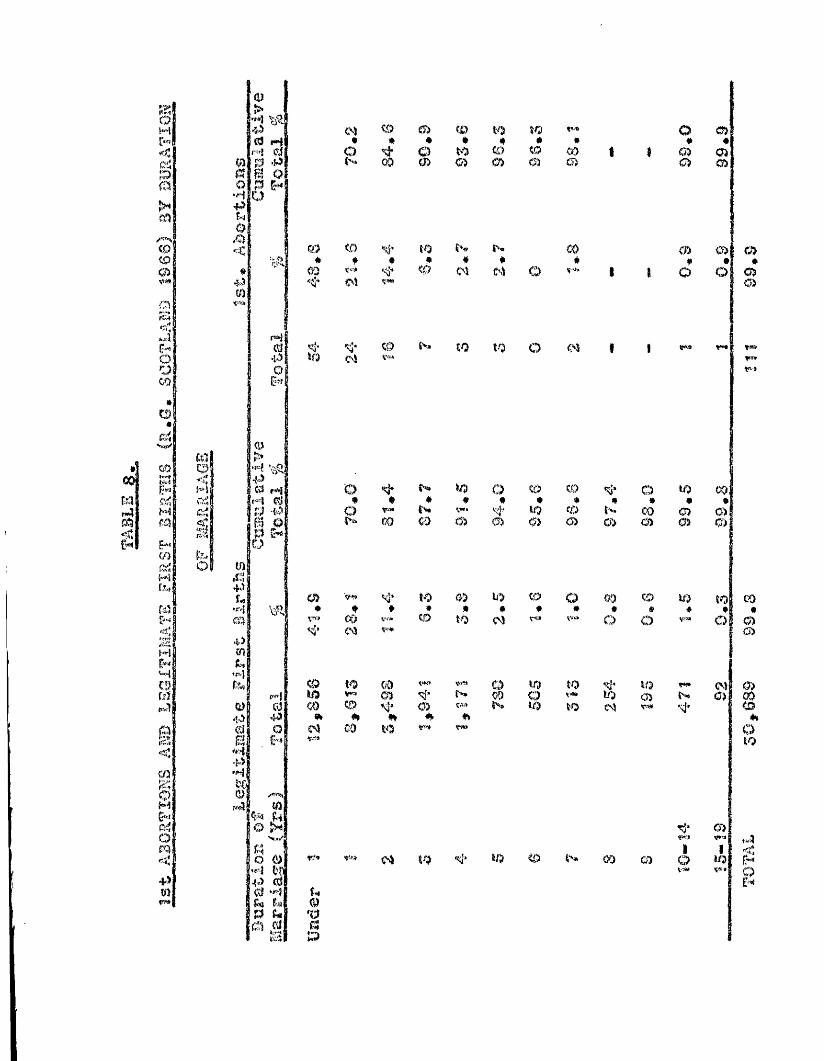
QOm
m
êHIfiîîi IÙi
§mcomo
Ooco
fôll00ZpMj&!ÎHmme:{Mil
*%îHÎw?i| I
SIP%1@i<wSiQiOm
•P ■mw*
'liN
o 0fnmX*cD
m C0 m CD to ÎO * * O %« * • * * • # # «P Q to m to Où 1 0) 0300 m (S) 0) 0) m 0) 03
<0 <0 to CO CD o> a>• f $ * # * • # • #00 0 oî G4 O r*" 1 1 O O 03oï 03
c:'OS m W ÎO o m
CD to 0) KO (O O 00 © K)* * ♦ » # # f » « # ♦\Wf COCM CD to CM o O V!W
<9 to 00 O KO ÎO 10 fi*to m * N CO o v«. K) o> NCO#»CMCD#CO #»10
0)4k A K) to CM r*# si'
m ï/? (0 W CO O)
O to (:) CD m O MO %# * * # * # * # * • #o f* N fn tf> CD CO 0) CDÿkn 00 CO 03 03 0> CD o> d> 0) O'J
to$
<MO
tsa
CO#a05
m00o&oso
Tj’ G)SfHO fa H1 f <O M3;; £HÇS»i p

M *%.OSd•H4m (S
mÆJ 0{ O 0 O dCM#10
COêcôso
*o
03
0M
«<Ats'rrt3f4
m\u
ù i \£'g|Q-tOjh !mt-4mmof-7OCOk:Uu■a14§
PO■ïD'M•Pigcs.
m îïf-p; o0 'M& P40 Ou æjad <Ft4
to$CO
*MO
O4fw»fa
#ÔCM
M3fW
t.Ù«01
CO4
0^ to rs 0PCfl C40 Ci (0 f m CDB R'ta .• . • ••P 0 ja 01:
CM to CM ’C'rt
CM
f4 # ObO'M 0 Pfïl0 .d '0 < «CM
m a # ohù M0 -PC*i f#i01 O ,0*0 <iîto CM
0a,43m
So# 'Mt)9 4 > 0 ^ ^ Ùa, A <'O#4 OCM Sr.

t/5m %o w 10 10« # # • *M m N (9
mg0 <?.) •î4 0.î|m m m
0> o VF» 00 %)Q m Oi
# # • • #10 O <s> N
%) o 1004 fO o U3 |x*f # * * #
ÎO m N
00 ÈO U) w cùm O N N# * • # *m tiO W w
:at;:mm
NM
#tCO¥> o'?3*
QJ>'ÇJg
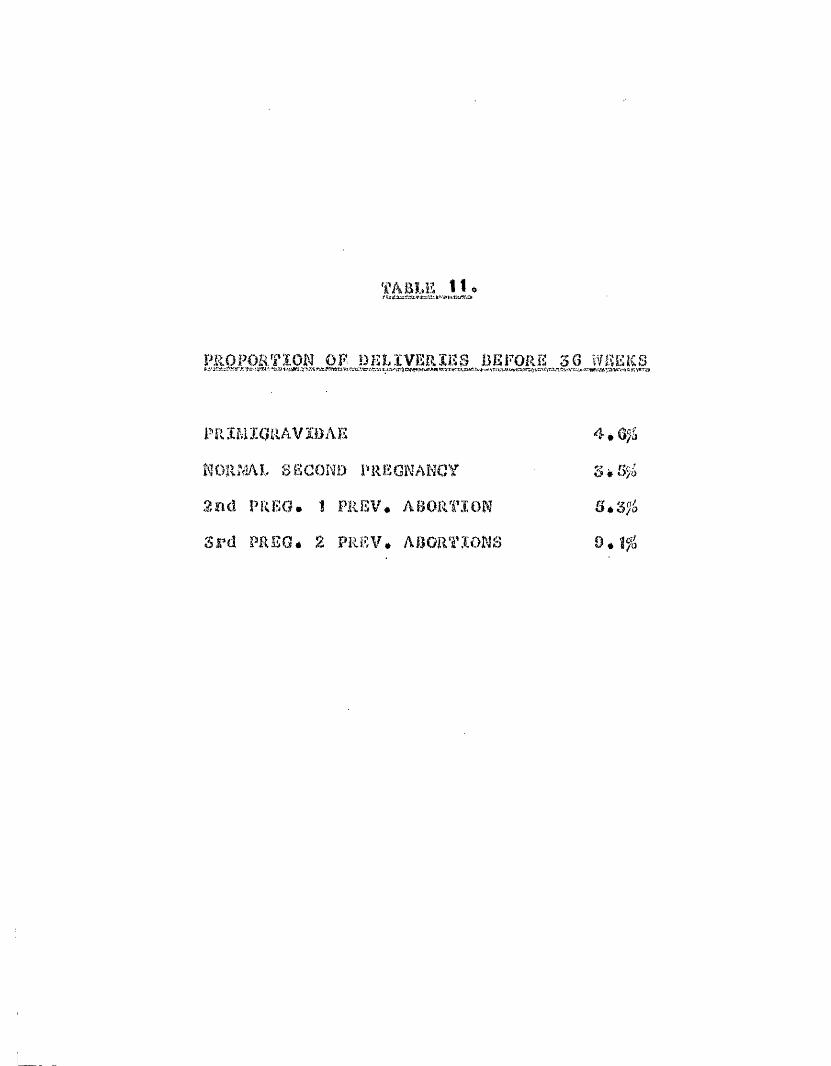
'I'ASl.E 11.
PROPORTION OP iJEMVERIlîS ÜEFORE 36 ΟHEKS
PRBIIGRAVÏBAE 4*6;4KORÎ.ÎAL SECOND PREGNANCY Sè55*2nd PR PO. 1 PREV, ABORTION 5*3Ji3S‘d PREQé 2 PREV, ABORTIONS 9.î?i
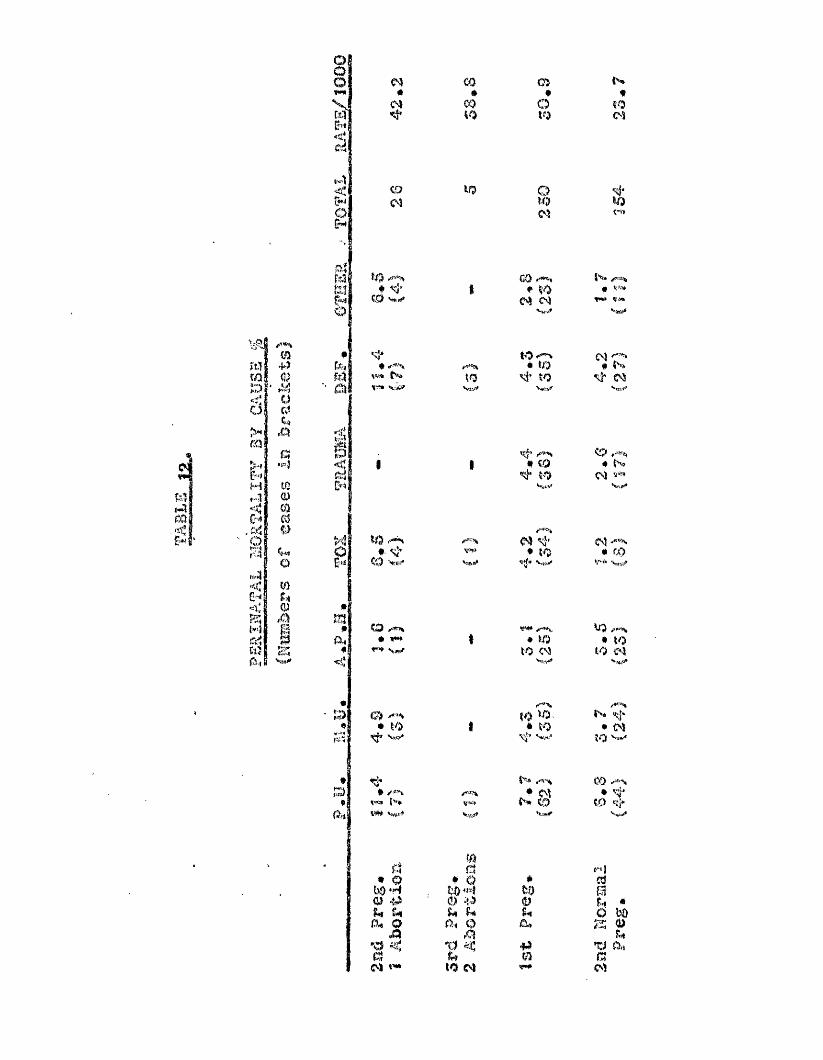
M#m
03»m40
C i*
Otoo*
fîOm
iQ(N
KO g si"KO
*to '««J*(%) (lfiw«f KO 04 oî
Vwtlf
t'’*'*t«î> Ç-»
'■«f*’
«V«iS*t=» KO
Vjrf
to * to to C'5a
S<feî
# to^ toVsvl'
<0 *. «4♦ Nç\ï
pto#■ si"to Vs,-'
04 s}’ * to•if» Vfi.»
C4* tO
*1ÎS I
4| to >fm KOA,| # #W* 1 • to • to
#8 *=** to ("4 KO 04< 1 w ,^
*1t'1>pH *P^« © <^4 to ^ t>* <î '• KO 1 * to • 04
’wv* Si" V.I.’ to
tl t -® ,^ ’' \ 0304 • m;]-
f-W t'W* V'S to m si*Odl 1*1 *MWLS-il 'r-Si
q • o(0 44u u 0M otiO0o) «'*
q • 0O 40 1 ^ 0:i O
to oi
#to0U&)44#
(.nj
iè w
î«(TJ 0.1f304

lit#
ciaet ar atif4àmttion.. iiifli'ÿ
4.0 ie.1
Aos4«$«sdBqiivei'y Spontané,OB#
znû* PiHig» îst-1* Wepmmi a*« 3.0 0.9 94,5
aijtî# pp@s. Ï A&opfcion e,9 #9.8 3.» 7t,&
8 N . r*P0g* ,$::A#pt4en# i i * 7 t $ , t 71,8
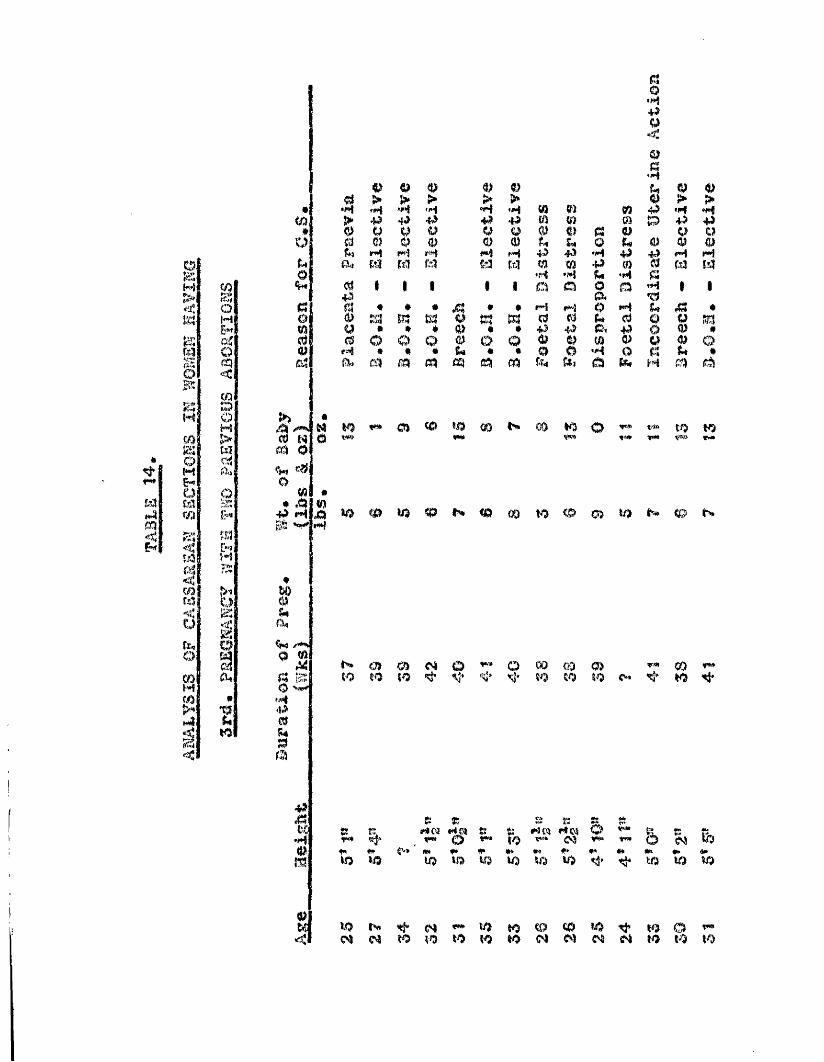
«
O.
M>im
mo
N
soMm
s0i<§15[f,0
NWpf*w$
1
§ofHI£**GîOcq<%OMWCSÎA.)8ÎH•f*î
eu
V.m\K)i
03 03 03 03 00 > > > > ># •4 M "4 'M *4 «H m m mm* > .p 4.) 4*3 # *P m m m<3 ü P U 0 Qt
03 a 030 0 Oî P 03 0 0 0 PfU M 14 f# M H 4»K # •H 4)tw Ot M m m W M m m # 0O; ♦H '4 fU •40 « # 1 • 1 0 0 0 044 a.a « * • A • # p»î f*>J 0 H# m m ta V m m 0 0 dm u # • « 03 * * 4 4> p-, #ttj es 0 0 0 0 0 0 0 0 w 003 r«î # # # &* * • 0 0 '4 0f?4 Rk m m m cq m r?4 &Ki a K&
b*dl /**>*(0 McA O<wo• A# «4 jQifî
é*#/**%
fg O »*#$44mS4!3m
44:,CtJÛ•HM
9><
§•444Q
4 à44 «H *4P 44 +4W Cî O 03 O44 #4 H03 W WH I I
1
Y#f4
tî mo **'* ^ m O)
)w> 1x5 tp
P 03f** î>
S ' îP ott •m
K3 o 'P* tf) M)VW» K<« VB» V®» f*
m 10 <P m KO <D
KO 10 to SÎ* Sj* si* to KO KO 'ti' KO <*
Ç! K4® fi:*>4 OS ÎS*1P » % #4(9 n S ?sVMÉ 5 e &r# «w» 0 to 1WW (N# 4* «M f* # •» #* #* ## #> •*KO KO KO m KQ 10 10 to fâ' 4» KO 10 10
*0 w 4“ N «M> to to (0 m tO 4» to © <tmN ro ÎO to to to m M N N to to to

OPS
s&<cio
dIHICiom44»
I§4*3gÎH5M&**Êfuç«»Sifï3»O’wwf4P,m:
%4)a0H440aO
I%a0"444fWs<44Æ5rai3zm$?K% -a
4*:§
1
to Né s
10«8
sotoGO
0 d" ■ 'ch N N 0 CO« # * # # # # *CO © to to 0 CP Ifw*to o>
I
âto03I
&§IAHI0O2;440
to to C4 05 00* # * ♦ # # «op to h# Ch 0 0 0>to C4 «#t G>
4oKS
©3 O CO N s;as!3i?*S3îrt«rcsïiCL !7S':3LtkaT*%JS(fW!fa-K*
CO 0 05# * # #to V# 00 toC£3 N CO
Mto (N O <0 CO N O o tom
0u a
£« 0 00 % > K3fU iH 0XI
§H 0 00 ,q
a H W& ^ to S|* to -H c U 0
:à 0 S3 ^•H d 00 t
« 0 0tfO ^ >
# 0 0 HI
âA<
S# <30 HA, C4 0
3
o
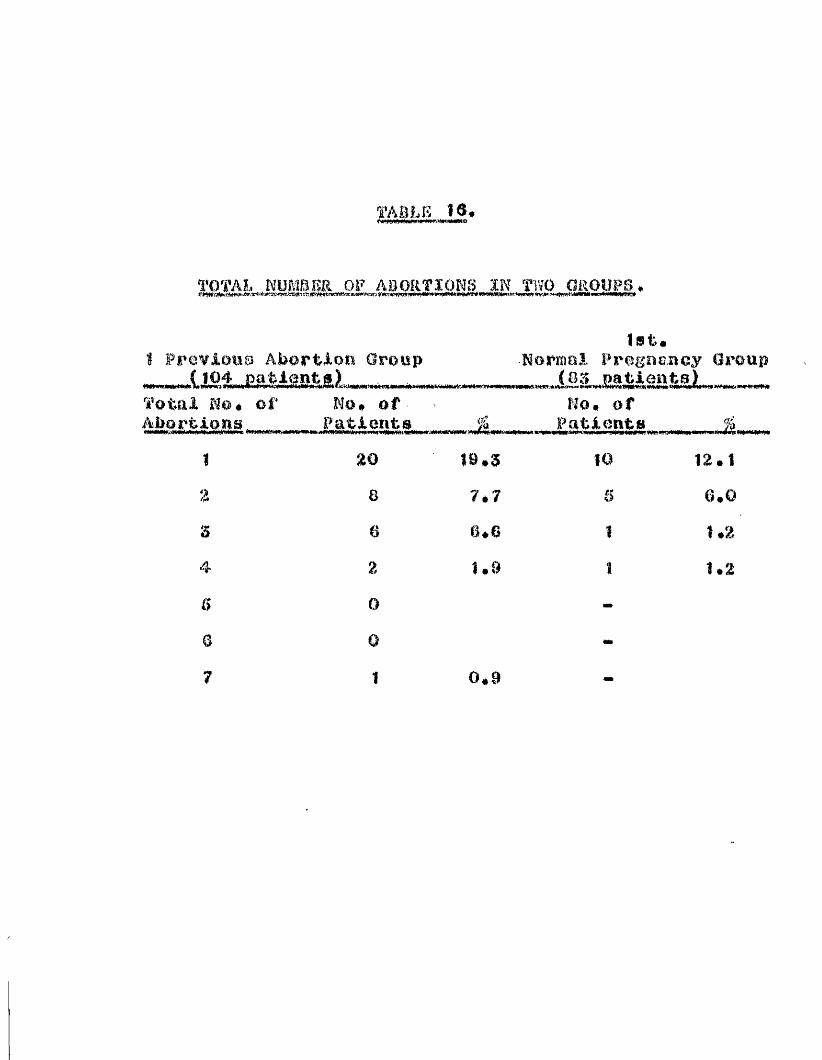
TABLE 18,
TOTAL NUMBER OF ABORTIONS IN TlïO GROUPS.
Previous Aioortioû Group
'â’otal of Ho# of AMrti-ons
list#-Normal Pregaancy Group
,iâ3„ESJBâ«ÈsL.no. of
.WW<«rW«HI6WWe
Paticut » % Patients Jk
I
s
B
a7
2 0
8620
Î9.S7*76*6Î . 8
10 12*1
6.01*2
1.2
0*9

Ï A 8 L E 17.
OTIMBKRS WHO ABORÏKO IN SUBSEQUENT 1PRE0NANG.IES gQLiOWÏNG 1st. ABORTION (TOTAL 83)
No. of women who aborted In 2nd Pregnancy -* 26 (2,$%)No. of women who aborted in 3rd Pregnancy
after 2 previous abortions *• 12$ of those who aborted in 2nd Pregnancy * 46j
No. of women who aborted in 4th Pregnancyafter 3 previous abortions - 7 (6.7%)
% of those who aborted in 3rd Pregnancy - 38*3%
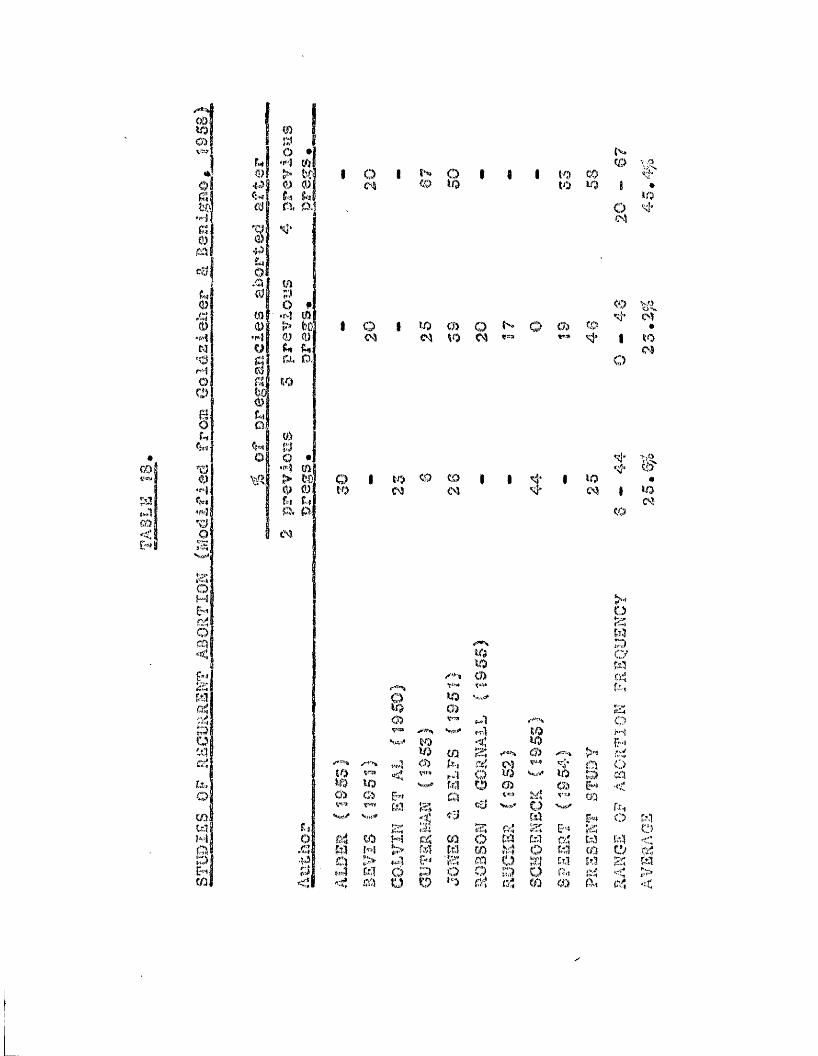
GO
mg
mÎXÎo •]fnji (0> t'441 0 0h ulm ' m,o..]
TJa)
/.I(Utctj m
•r«.'î Iu
§■aw0uQ
f{tj(o
10po #:•i>î ui> fco(U (Ü r»t. D.
y>o •'M m> to]O 0fi-i fvjà a
N\Ro 1 ï*'»» p 1 1 1 to CO ç.j.
%> i-O to Ü3 9 *toO
<0|Vij,o 1 to m Q O o> C0 •
so m 9*3 1 to
Qto to to m to I I si" toM
o
\j'Ito
#toC'
80)SOC O
t ot o
C A mm
at ,
gM*z
0 m M CÏÎ/ 4
O
{«{ 'a70 > t4l0 ■ i 4 m P< : < ffO a O
o%tï35O '
V ) mm c4
to V-ïi>0>
O
<10to
Mr -
to Z; CA >->1p i VJJ> si* o C.)
O to to D cqw P G5 CD &*< <<:fô ti«i m-n.»* Qcci
£5W C) N
&-* k% C)COtt3
Om
[z3o a
wto
r4o S
o 59 Ct.1 tû :s: STrip q IT,) O fhi ir4 >to (4 to % a.i q <

TABLE 19
GESTATION PERIOD AT WHICH ABORTION OCCURS
1st. Pregnancy ending in abortion
Time of Abortion»j!*iv.wtt'in'c«j«*wpe<#t>irww«» MWM IM unm»W I***»#*»*- Number Up to 2 months 283 32.82 months « 3 months 13} 18.13 months •• 4 months 29 6 34. 1Over 4 months 137 18.1TOTAL 869 100.1
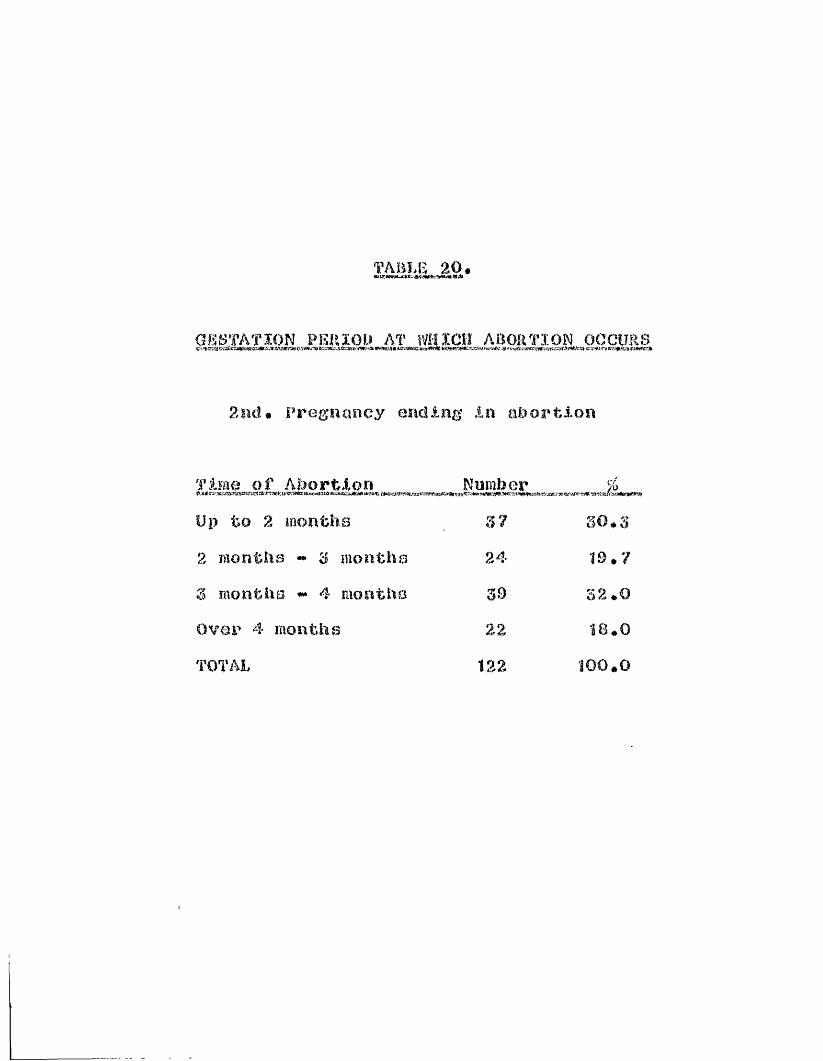
TABLE 20.
GESTATION PERIOD AT WHICH ABORTION OCCURS
2nd# Pregnancy ending In abortion
Time of Abortion Number %feiHlCi‘Ha.aaV?gsiH?a*'?a:»;a‘iW«faaTCa«j:0c=j»»zaa»Mn’*-aMiia\tEratjjjiaggyaacira>i!ng!,*KiJriigjW'»g"5iiwwiiae--agJ!B0p.v
Up to 2 months 37 80#32 months - 8 mouths 24 19# 78 months ## 4 Eiontha 39 32 #0Over 4 months 22 !8#0TOTAL 122 100#0
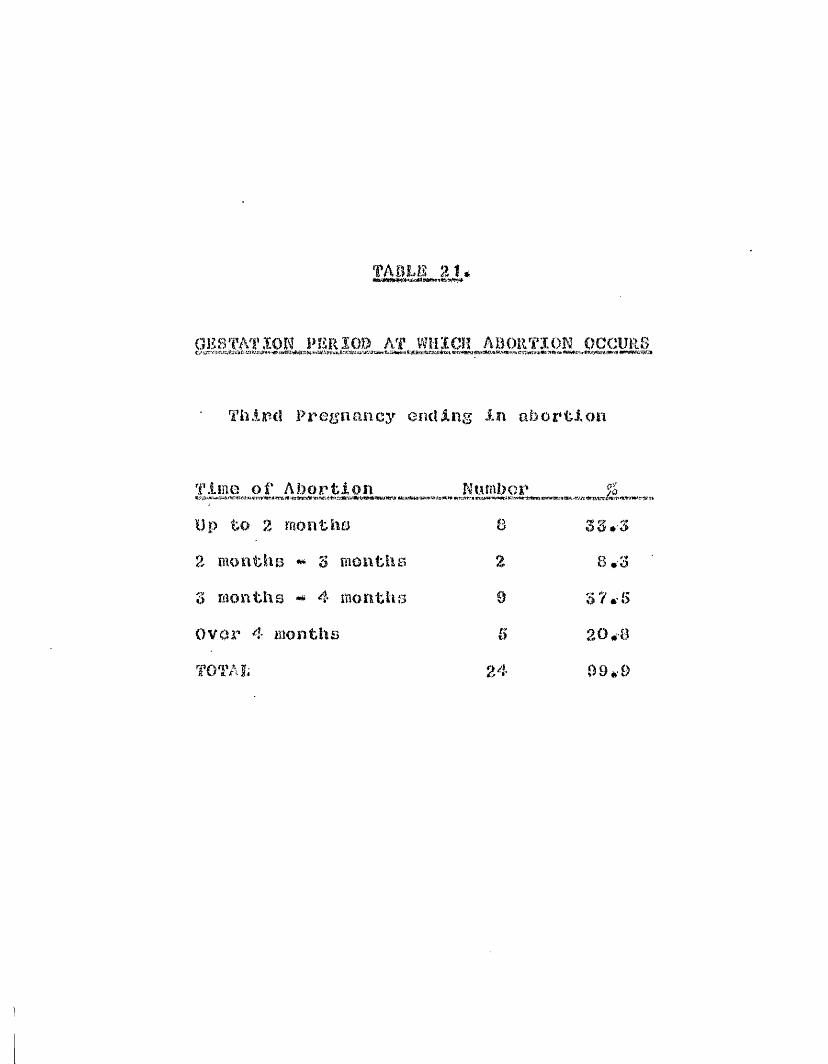
TAOLfâ 21.
GESTATION PERIOD AT WHICH ABORTION OCCURS
Third Pregnancy ending in abortion
Time of Abortion Number %
Up to 2 months B 33*32 months ** 3 months % 8.33 months 4 months 9 37*5Over 4 months 5 20*8TOTAL 24 09.-9
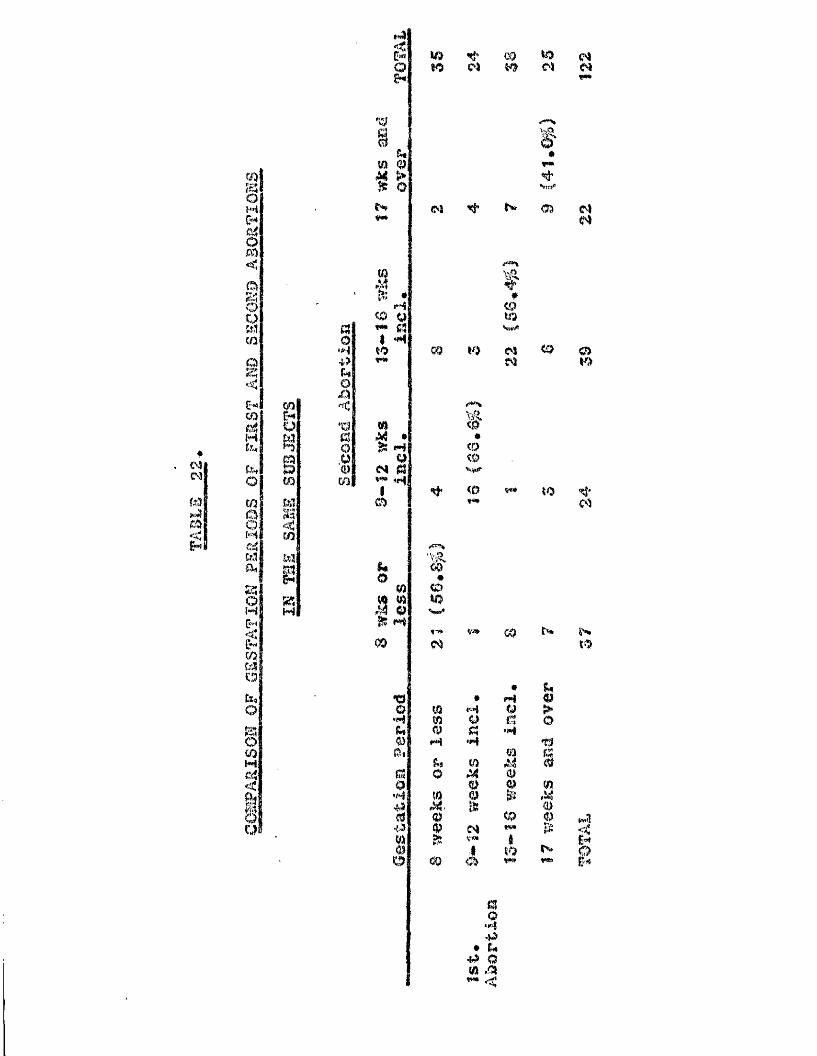
#
WW
ë!
m%oC"*o<ABCOQ2:<
fsi!Mkt14
§Mic4ia.
11M|pm-*!S'ëtî-ijQ§U"3Mg
Ê
impm
M
<ro13
ZM
aO
• H-(f)U0
X »<* deî1m
gg
Sm 0 M >
N
aM9^ Cl
I «M
M •^ H
9<M qV*> 4r«|m
&*o
1C#0fôi
a
24«ï.d4'5I
W )80
(M
#
%Q%aw»
m
to§M
0
1dO
m
8 0
'ê•CDC 9■Hiim**<0
M9«M
a1c\$v«»&
c o8 0
v®**»f*
CDV )
OSN
0#
*M9
M
S0I(ptV*(8 0
■S♦ c# •p o m ,cs
too s
mos
m
<0
so
N
|3>
%
m
îo »tW9
NOS
O80
'CÎ'm
to
imtt!
I

TABLE 23.
INTERVAL BETWEEN 1st. & 2nd. PREGNANCY (to noapost year)
Intervalin Years No* %6y:rj<Wv«i>»*vtrtwwriii.amF!iflwci!»et»«.(ieKtKE»aeJ-iti-eiïsta™iTr»Wif"si5!SaiKM<«wir«ïe:
1st* Abortion No. .. %; n #Mt 3» fjT'KAMTAK?# ' Hi fH V
1 14 17*1 64 50.117 21*0 38 50.0
3 16 20*0 9 7,04 8 10*0 2 1.05 4 5.0 5 3,9
i 4 5.0 07 3 3*7 1 0,8a 4 5*0 00 1 1*2 0Î0 0 0
Nil Î0 12*4 8 6.3
TOTAL 81 100.4 12? 99.7
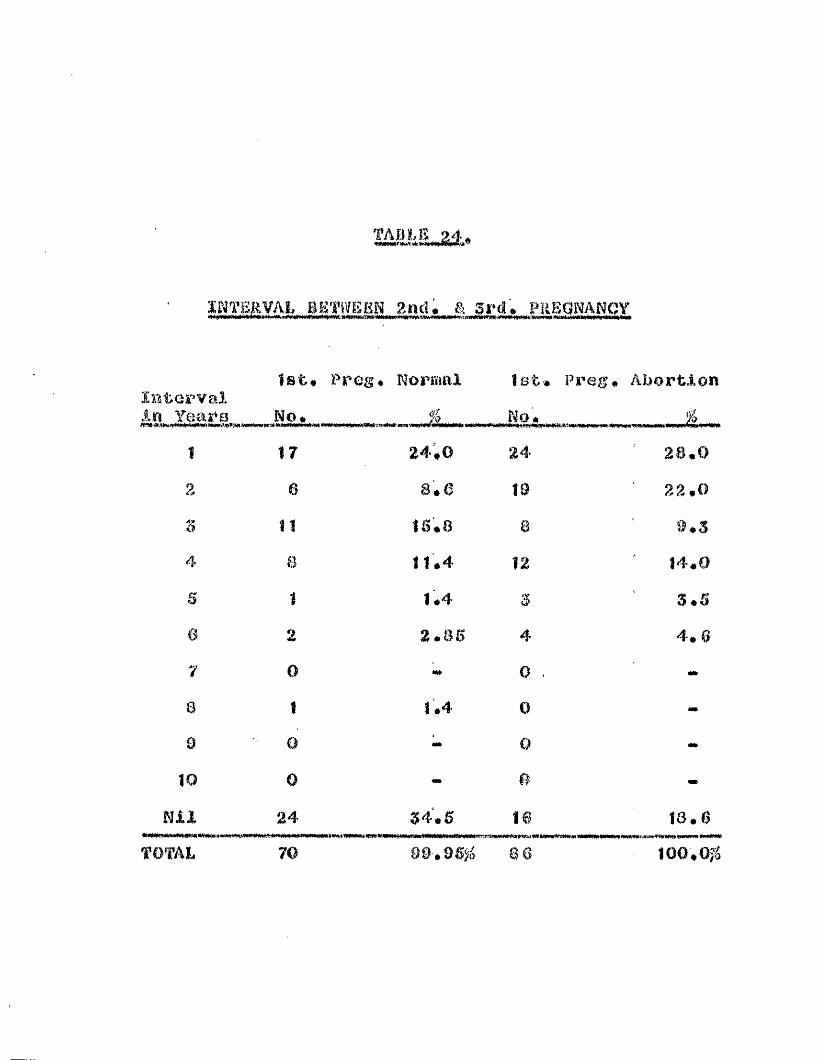
TAB L E M ,
INTERVAL BETWEEN 2nd, & 3rd, PREGNANCY# #*#ww
1st* Prog# Normal 1st* Preg# AbortionInterval
28.0 22.09.5 Id'.O3.54.6
in Years No# %. .No,fpA# îOl *fWMÎ 17 24#0 242 0 a#6 W
n 11 15.8 84 a 11.4 12S Ï 1 #4 36 2 2.85 47 0 M» 08 Î 1 .4 0B 0 •t* 010 0 e
Nil 24 34.5 16TOTAL 70 90.95% 8 6
18.6100,0^
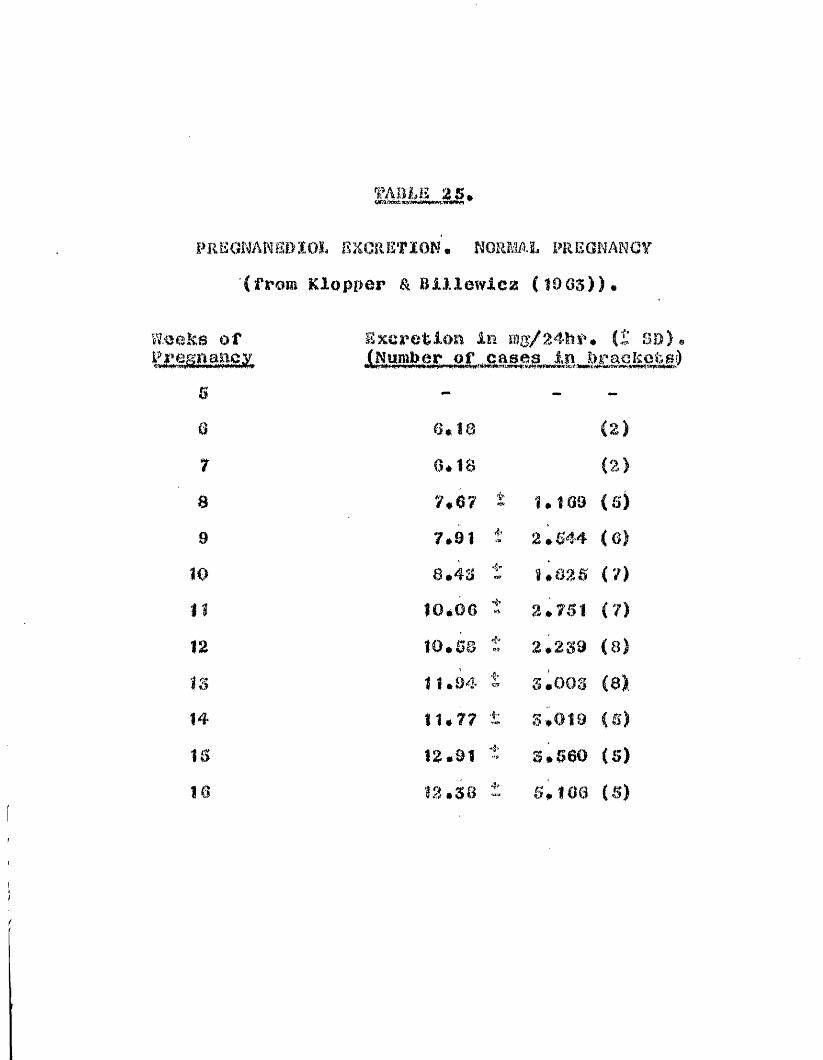
i H i E o n m m i o h ekore?ion • normal piieonancy (from Klopper & Blllmviez (I0G5))#
w.eeRs of Excretion in mg/24lir. (£ so)®(Number of cases in bracketeO
B — - -0 3*18 <2)7 3*18 (2)8 7*3? 1.169 (S)8 7.91 t’ 2.544 (6)10 8.48 4’" 1.826 (7)II 10.06 2*761 (7)12 10.58 4. 2.289 (8)IS 11.04 t 8.008 (8)14 11.77 ■V 3,019 (S)15 12.91 8,660 (6)la 12.38 4s 6* 168 (6)

EiaMANEDÎOL EXCRETIOW <- SO) IN PATIENTS 'iîXTH 2 OR. r.îORE PREVIOUS AS0RTÏ0NE1,
PRESENT PaSGRANCy SUCGBSS*'””(HUMBEa OF CASES Sfl miA
la A
WookÉ» ofÉr»i
•Ü7
12
Î4
PregnanocLiol oxerofclooIf *-!»Fïse*5WWS>:
e»e* vse.oB #4 8,8*S i
10,2
11.7
12,0
14,1
C 3) 2.9S < 4) U 0 O ( e) 2.3S ( 8) 2,49 (11)2.!3,26 S. OS 4*2?
5.
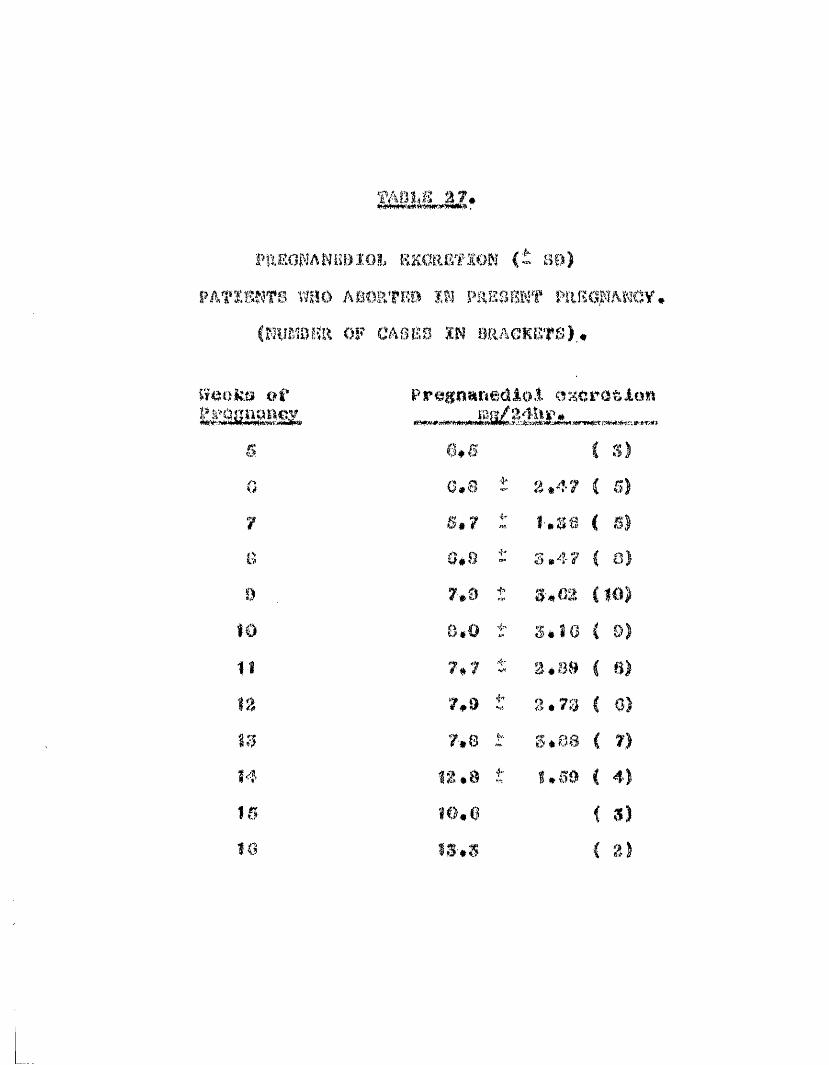
( BO
PATESNT8 Wî!Ô ASORTRO ÏW PaKSBKT PftRS.WANCV, (NUMBER OF CASKS IN üflAGKCTS).,
W«oks of excretion
1510
5.s 6*50 0.8 4® 2,477 S,7 4® f.ss0 0.8 s.47
0 , 7,9 i-" 3,08to 8.0 s . t a
It 7*7 3*8918 7,9 i* 8.73
7,8 k. ÎÎ.0S%4 m *8 t 1*69
«0.C
»*'
i 3)■'♦o
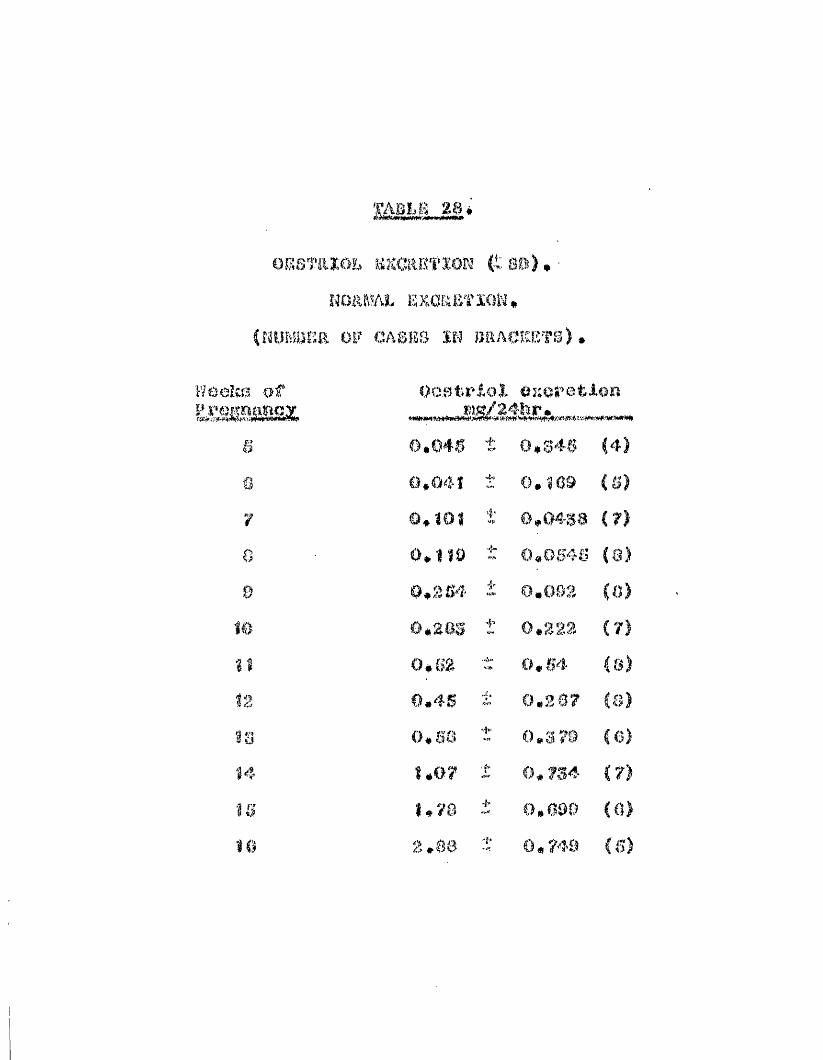
' R m e 28*
iESTRÏÔl. SKeSF'P' (t 8») ,HO&MAL SSCKE'i’IOK,
NlBlsiKR OF CASES IN BllACKETS)
lïôeîîB -of
5 0*040 t 0,046 (4)
5 0*041 ’f»
y 0*101 ■'I'- 0,04sa (?)0 0*110 •Î®- 0,0.546 (8)0 0*204 0,063 (0)# 0,2.23 (7)$1 0*52 ■; 0,64 (&)
0.40 ic 0.307 (s)
98 0.06 t 0,3 79 (0)1.0? j; 0,734 (73
15 1*76 0.090 (0)10 %.ee 0,749

o ABORT]oES'mïoî. EseftBTSow $ s»).If f ‘s" tüîia 4A
FüBSEKT PEKONAN0’/ S CNURtSfîE or PAflKRITS ÏN PRACKBT8)
U *
$
ê
f
ê
n
14
B a
0.216
0.400
0.790
2.06 :
r 0*0184. 0*040i- 0,03 ît 0.126
0.134i" 0,107i" 0,304i 0,200t 0,002J.. 0,340Vf* 0.S994' 0,620
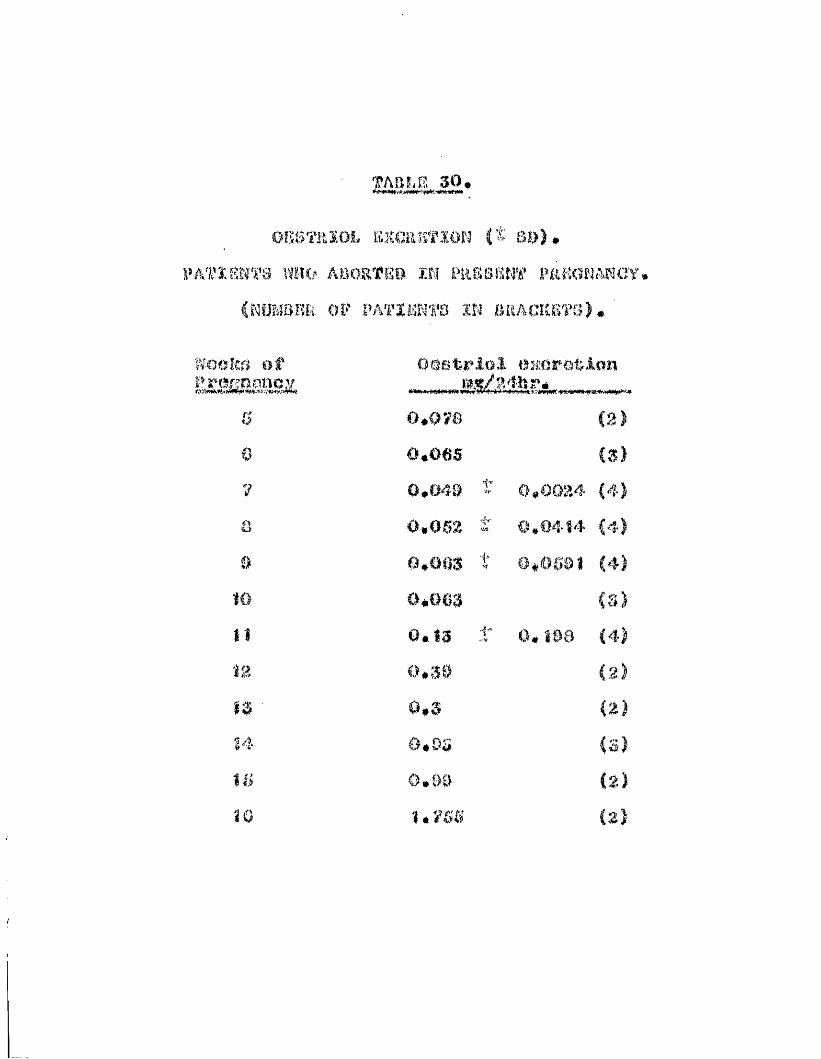
TABLE 30,
OKS'fftîOi, BXCaSTlON (t 30),PATÏ.8WT3 WHO ABOETEB Î.R PRSSBN'ff FkKGMARCY.
CKüMsrîîi OF Ph'mmt'Q m bracicbts),
tïoùkfi ai Oestrioî amip&uiatim s î B z ___M*f/24hï"«
& ©,0?8 (2)0 0,065 (3)? 0,040 t 0,0024 (4)Ô 0,052 t 0,0414 (4)B 0,803 t 0,0681 (4)
10 0,803 es)t1 0 .1 3 ■t 0, Î90 (4)12 0,30 (2)m 0,3 (2)14 Ô.ÔÏÏ (3)16 0,09 (&)10 1,755 (2)

TAB LU
RATIO OF BXCaUTION OF FRRGNAMBDIOL & OESTRIOLN O a m L RATIO#
(NUMBEtlOF CASES IN BRACKETS)..
Weeks ofRatio
0 181*7 f 93.8 (4)a 147*9 64.2 (5)7 92*0 32. Î (7)a 0S#4 ■4e 20,6 (8)# 01*1 33,4 (8)Ω 40*0 i* 1?,2 (7)It S6.4 "4* 29,2 (6)12 S7*8 t 33 ,S (8)IS S4*0 i-» 4Î.1 (6)14 22*0 24,1 (7)IS 7.5 4" 6,71 (6)10 5*2 4’ 3,16 (s)
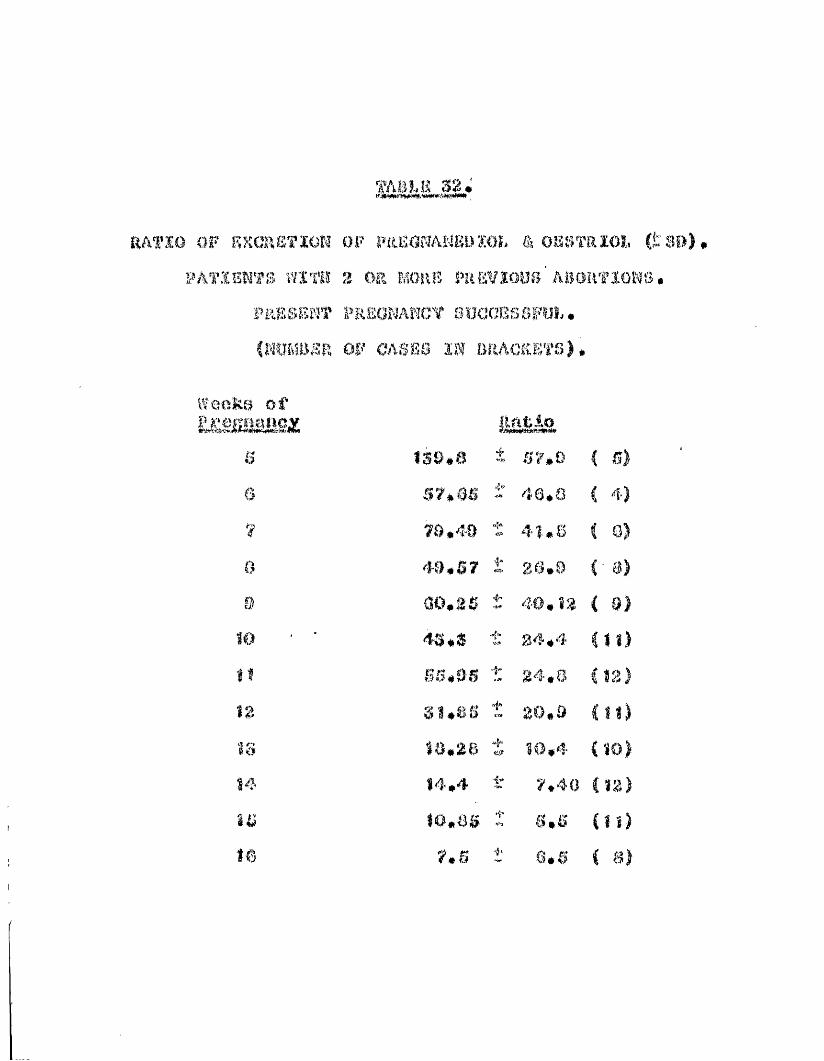
TABLE 32
R A T IO O F R S G R S T IO K O F PREONAMEI) ÏO L â O K S T R ÏO Î,. ( t SB
P A T ÏB N ’f S W IT H 3 OR MOHiî P R E V IO U S ' A B O R T IO N S .
P l A B B l î m ' P R E O R A H C t S O C C E S S F O L .
iSP, OF CASSS I N B R A C K E T S ).
Weeks of lirjiHliBS; Ratio
0 139,8 67*06 48.8? 79,40 48,60 40,57 1* 26.99 00,26 40,83
4S*S t 34,4II BS,0S 34,0
S U S S t 20,018 88.28 10,484 14,4 "|w 7,4015 80.85 s,sΩ 7.6 i' e.®
S
B)a)
8)
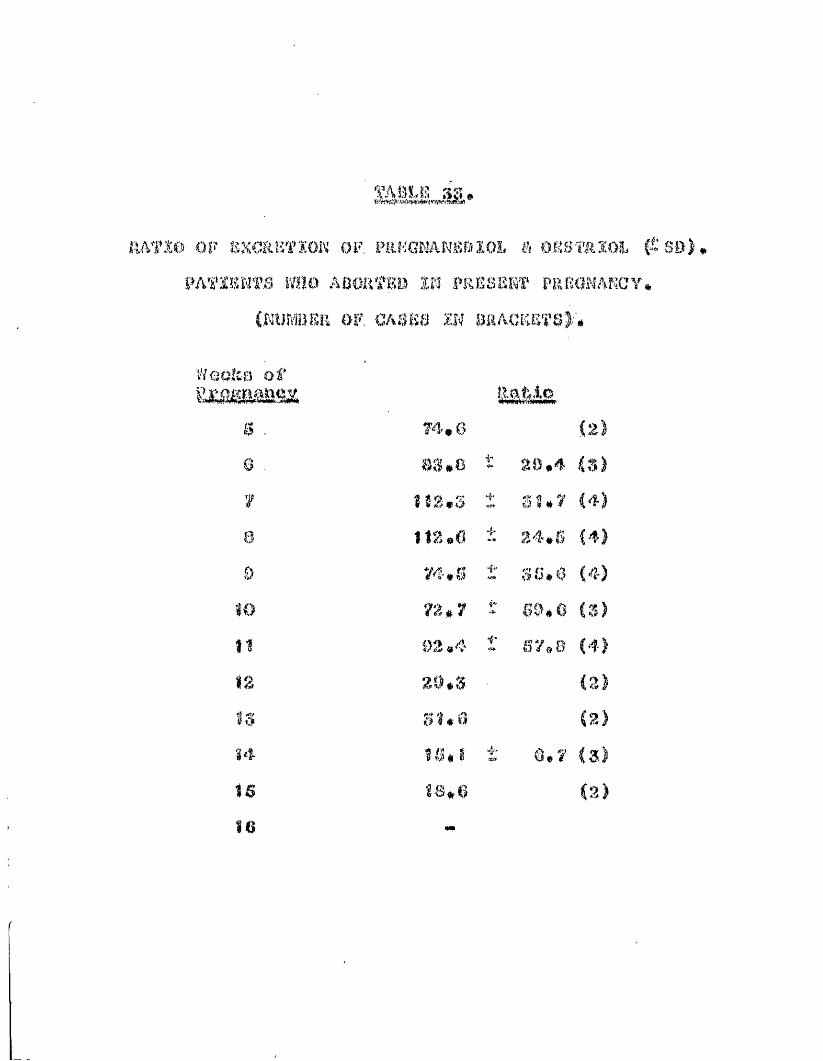
m S L E S3,
HAfli) OF SXC&KTIOK OF. FaEGNANAîBÏOL ê OESTftSOi # SB)PATIEKfO WHO ABORTEO SK W4ËSSIOT FREGflAKCY
ill OF, CASK8 IN BRACKeTS);',
s . 74,0Q os*c ’t 80,4 iT,)
f 113,3 t SI,7 (4)& 112,0 4- 34,6 (4)9 74. S so.o
72*7 SQ*& C3)ÎÎ 93 ,4 i' 67,8«2 29,3 c ^
31,0 C2)14 16,8 0,7 (3)16 18,6 (2)16 ##
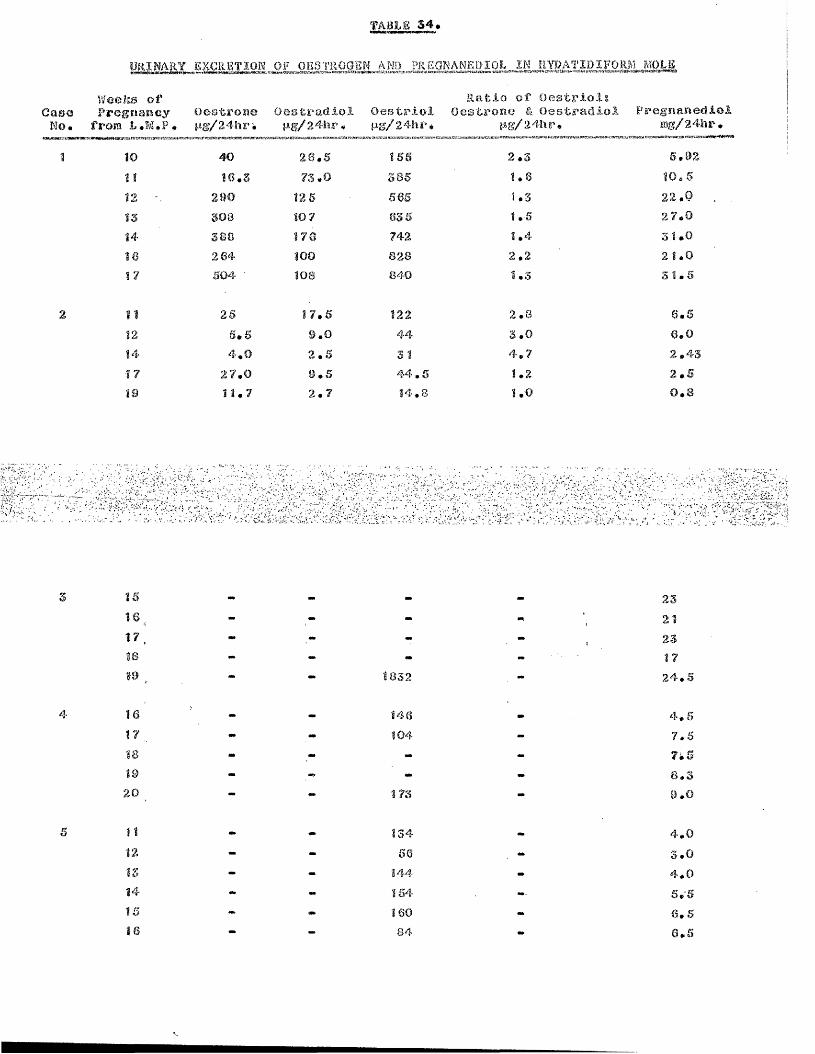
TA8L6 $4.EXCRETION OF OESTROGEN AMD PREGMAMEDIOL IN HYDATIDIFORA] MOLE
Weeks oÉ' R a t io o f O e a t r io l iCase Pregnancy o ea tro n e O e a tra d io l O e a t r io l O estrone & O estradioJ
No. from L .M .P # M g/24hrk n g /2 4 h r , P 8 /2 4 h r*MwmmfKtawwwKKui
1011
1213
14
16
1Z
4 0
1 6 . 3
2 9 0
3083 8 8
2 6 4
5 0 4
2 6 . 5
7 3 . 0
12 5
10 7
1 7 6
100 108
*Ag/24hr. P re g n a n e d io im8/24hr#Ç-iiv'39's»3aFC7a#gi£5itc:ra>; «WS Wîï
1 5 6
3855 6 5
6 3 5
7 4 2
8 2 8
8 4 0
2 . 3
1 . 6
1 . 3
1 . 5
1 . 4
2.2 1 . 3
5 . 9 2
1 0 . 5
22.02 7 . 0
3 1 . 0
2 1 .0
51.5
111214
1719
2 5
5 . 5
4 . 0
2 7 . 0
1 1 . 7
1 7 . 5
9 . 0
2 . 5
9 . 5
2 . 7
1224 4
31
4 4 . 5
1 4 . 8
2.83 . 0
4 . 7
1.21 .0
6 . 5
6.0 2 . 4 3
2 . 5
0.8
15161718
19 18 3 2
2 3
212 3
17
2 4 . 5
16
17
18
19
20
14 6
10 4
173
4 . 6
7 . 5
7k58 . 3
9 . 0
11
1213
14
15
16
1 3 4
5 6
14 4
15 4
16 0
8 4
4 . 0
3 . 0
4 . 0
5 . 5
6.6 6 . 5

EXCRETION OF( fro m F p and s en & S t a keman , 19 64)
Weeks of 0R% OEg OEgCase Amenorrhooa M $ /2 4 h r , p g /2 4 h r . p g /2 4 h r ,
OEo/ Q POEfi OEa IU /2 4 h r . m g /24hr
K .K . 19 * « 85 *20 - 2 10 -
I . N . 25 21 12 104 3 .1 132#000 3 .226 26 12 138 3 .1 6 5 0 ,0 0 0 3 .2
A .O . 16 - - 260 700,^000
Il *A • 16
17
106 4 6 219280
1 .9 6 0 0 ,0 0 0 3 .6
G .8 . 16 - ' - 525 -
18 - - 1100 -
K .8 . 18 - - 1100 2 4 ,0 0 0
L .M . 20 43
■r - ■■sv'A î i S i '
' S Ê Ê M m M - i S i t l ; .
L . 8 . 12 117 29 126 0 .9 8 5 4 ,0 0 0 7 .613 - - 132 2 4 7 0 ,0 0 014 77 66 130 1 .0 2 6 0 0 ,0 0 0 7 .715 2 62 187 240 0 .6 2 6 4 0 ,0 0 0 5 .618 - - 194 6 7 0 0 ,0 0 017 - - 425 8 4 0 0 ,0 0 0
B .n . 11 - - 184 -15 62 19 102 1 .3 2 4 0 ,0 0 0 1 .9
I . E . 32 (? ) 94 68 335 2 .2 4 6 ,0 0 0 3 .4
OEj_ - o e s t r ô n e
0K<5 » O e s t r a t l i o l
OE-} * O o s t r io l G » G o n ad o tro p h inP » P r e g r i a n o d i o l
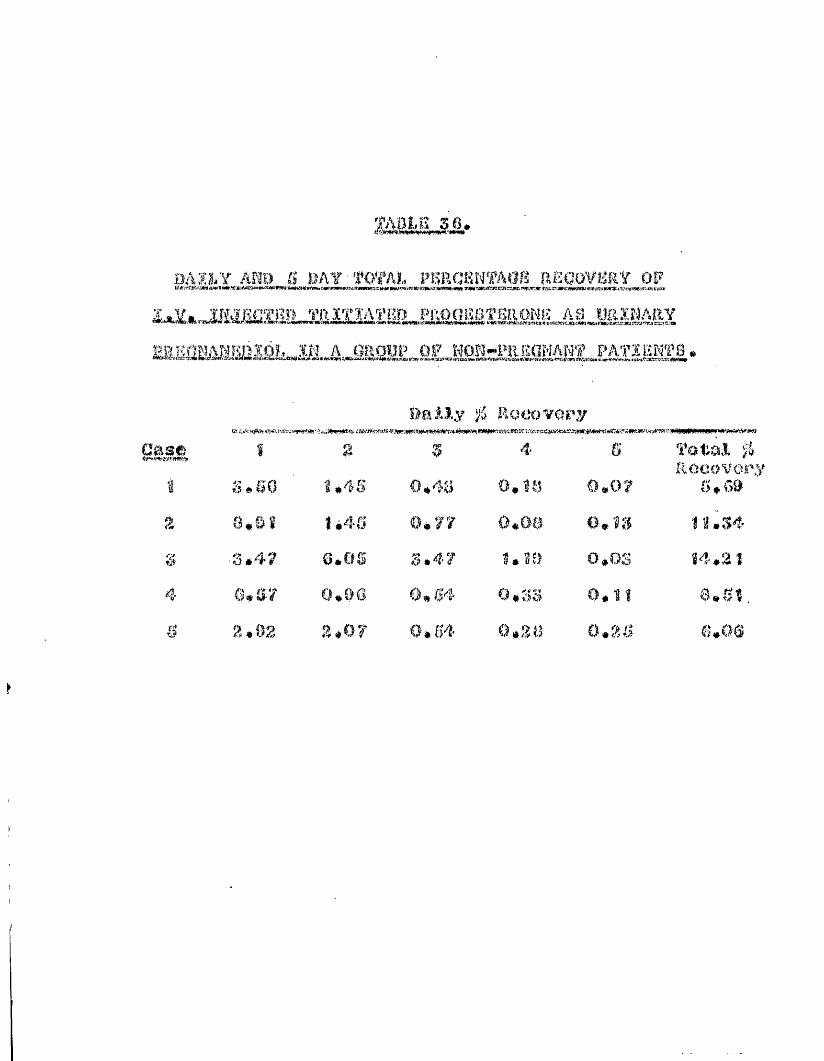
TABLS 36.
BAILY AND S BAY TOTAL PERCENTAGS REGOVSRV OF
i^.,.jjiiSüsia^ciimA2î»_iiâSM
0aAî.y % Recovery4&&%Ê î g 5 4 S Tota.1 1
RGCOVOi1 S»60 1 »4S 0.48 O.s!» 0,0? 6, G»Ê Ô,SÏ l é4S @*y? 0.08 O.îîf IUS4S 8.4? 0.OS s. 4? UÏ9 o.os Î4.2Î■ 0,a? 0.00 0,04 0.3S 0.1Î a.Sîs 2.02 2.0? 0.64 0,28 0,25 6,06
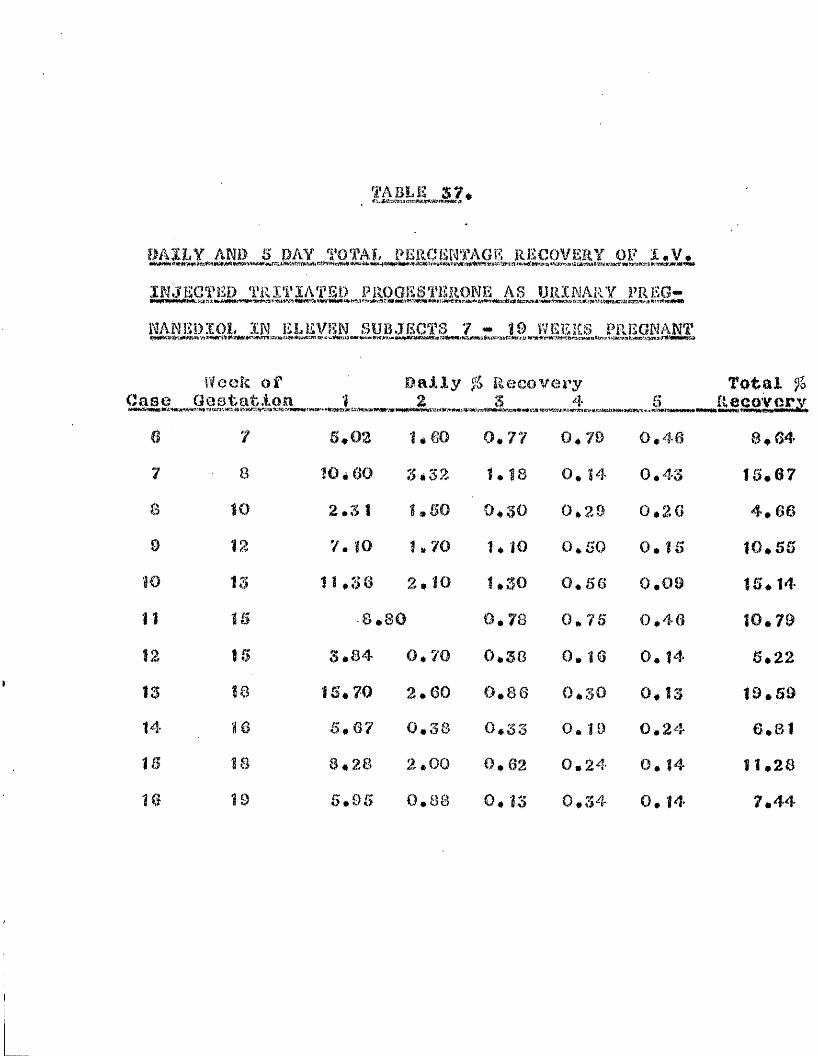
TABLE S?*
DAILY AN» S DAY TOTAL PERCENTAGE RECOVERY OF X.V, INJECTED TRÏTJATED PROGESTERONE AS URINARY FREQ- KANEDÏOL m ELEVEN SUBJECTS 7 - 1 9 WEEKS PREGNANT■WWlSîîSrtjiiïïWiiïi vt #Ki!##i:#PwArn eigia*iiiiRttCti<*i:i*î4iÉiMt*>eiL’ütoWi6‘Xî5p<tt#<s,Wj-u.W*ie*ï*w.59»iiîï><tt
Week of Bally fo Recovery Total %ase Gestation % 2«Wstme wwi*. W1» svjMES-a*3s-»«(trHw»'»»«9KiT«ris,-WcwiiM.;,T» ^ _ ___. ^^RecQVcry0 7 6*03 i # m 0.77 0*79 0*46 8*647 8 10*60 S.32 1.18 0. 14 0.43 15.67a 10 2.3 1 1*60 o.so 0.29 0*26 4*669 12 7. 10 1.70 1.10 0.50 0.15 10*55m IS Î U S O 2*10 1.30 0.66 0.09 15*14n 16 ■8.80 0.73 0.76 0.46 10.7912 16 3.84 0*70 0*38 0. 16 0. 14 5*22IS 18 16*70 2.60 0.66 o.so 0*13 19*5914 16 6*67 0.38 0*33 0. 19 0.24 6.8116 18 8*28 2.00 0.62 0.24 0. 14 11*2810 19 6.95 0.88 0. IS 0*34 0. Î4 7.44

TABLE 38.fl.*s3y*iH™wi»c*s3raer*s'»i
DAILY AND S DAY TOTAL PERCENTAGE RECOVERY OF Ï.V.' ' ' ' .INJECTED TRÏTIATEO PROGESTERONE AS URINARY PREG- MAW D I O L IN SUBJECTS S9 and 40 WEEKS PREGNANT
Week of Pally % keoovery total %Case Gestation 1- 2 3 4 5 Recover:
0.11 5.800.07 18.360.07 8.08
17 39 4.G8 0.34 0.45 0.22Î8 40 13.00 2.24 0.28 0. 1019 40 6.23 1.07 0.53 0.18

t'?)!wjIm;i
m#Wjî'4<1f-i [t«ïÿ î>''N aîi-î 2r:
0a SUj f,0
t4c.) ù.w 1T3 ■ iM ?!
0u:e m
M <su'1 a01
0k.!î )4> #%0 ?4U HIL: <K'';
0o'i0 (%*< %,ai >*tq ciq <w0V,
Q
ë (n<
K " m
a
§SMsi
1ef?.I
%% HwM ÛH>] # Ql
O U|fi,uf.!&l
W
O(5,a
é $
#
Q m 03 0 0 ya 010 0- 0'> 0 OS 4'* # # 0 * 4 * « tt\é Çîtt w e& tQ 0* N
5"% i'â 0 CM 30 m m0 N ## Q g# # # * * # # * #Q 0 0 0 0 0 0
m m o> ÏO m to 30# 0 M M oâ 0 V’ia 03» # i # 9 « # « #0 0 0 0 0 0 0 0
<a CO (%) i/4 U)m (G ÿv* 04 W3 CM os m# # # * * « # é #a 0 0 0 Q # 0 0 0
# m 1# U7 w OS to m 03# M O'i N m N 0 &- # '« 9 » <* 4 « * «0 0 0 Vf# V--» 0 0
9 04 # m ÎÔ M Oï VJ|.# 0 Q <% 30 m (0 m ¥4»# ■* * 9 # 9 » #(4 Oî to 03 m (0
* # «p. *
s H » G ,q0 ù q %) C‘> m M Ci',1 à,i«i M M t#') C'A* « g 0 m& 44 g 9 0 fei &4 a, 0fe w # m S# üff' « A 0 <p1*. > G
0 y a? <m m CO
Q Ow. v«i*O SÎ' 03 ^ 0 N<*" r# i:Ç' CQ (O
êOB
P%.*<yW#0'aî>)
*mU
OMî>MMmEXm
%m<
twl0:00mmc
or î-jBmmHByMa«5mfHo080t.ci,03g01
I I I*#£Ü.O4
i
O (M # ^ f» Q:)03 03 05 Ci 05 01 OS Oî 01
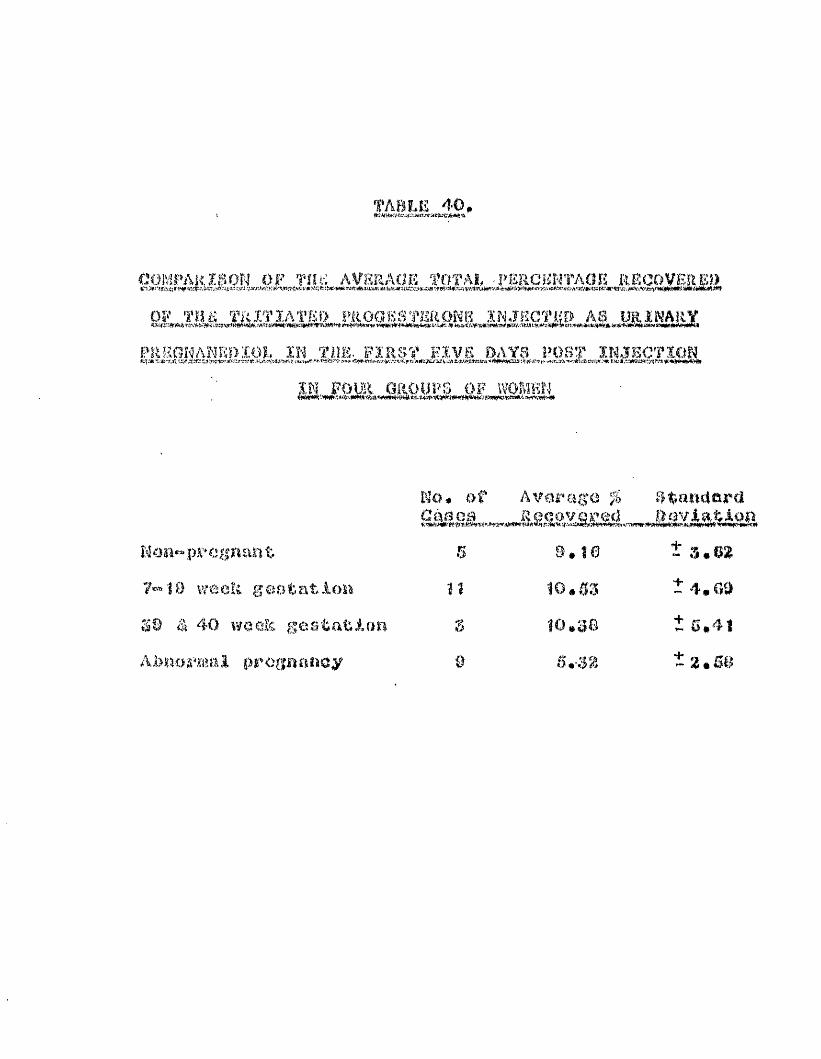
TABLE 40,
c o m p a r i s o n o f TIU-: a v e r a g e t o t a l î'ERCSiNTAOfi RECO VERED
P R B tlH A N R O IÜ L Ï N T iU î. F IR S T H IV E OAYS PO ST IN J E C T IO NKV-*-,®-.j" % « . % * : ! Æ<»lrtï.ï.r,7®'.;v;tils,KltJJKJiïtiCAfcrt/Ja.-Wît'st‘##«siî3sf rtîïli- Jlrttv:,ML'a,*1rtSÏ«!Xnj W
M F o m GROUPS OF WOMEN
Wo# of Average % standardC m o B Recovered Baviatii
U q u ^ prcgriau t n 9. 10 Î 3.62week g coûtât ion 10,53 t 4,09
30 ê 40 woelG gestafcian 10,38 Î 0,41Abnormal pregnancy 9 6,32 tz,B&

*0
«s»A wm* mA mAc o « *0£ > f j o c o < » o G o < e • • • • « • * • -« O W « 3 w » 4 > .C f lO > 0 3 O f * Q 4 % O l O & N
03 «Hi N
£SC»CO«0W C O O M O 1 • * « • » • • • •— o o N O W " * c n m t o(O N M 0 « 0 0 3 0 0«
w —* »*M 4 « 3 fei 05 00 ©2 0 O O i - * C f » - » 4 M C 0 Mw o o s e s t ^ c o O i ^ » *
W —* —* —a W O M O)
NI «* —* —* «aM 45, «3 W O 03 to M
Z os en 63“ # 1ta —* 0 os“ * Os 4k ©
m 4k o* N On03 -# M «3I •
4k N> çn w
r**0
N —*O .Pk M • ♦ •<0 Crt <£) (n 4k N>
03 <0 M % (%>o en 03O 4k N
O SI N) 4k «O «. • * «-to w 4ko CO NI
en 00 M 4k en oi—t 03 0 3co 03 en
en CD MNI o —*CD SI 4k N NI NI
tq
*9 D
(S 03 SI o>cn4kefiw-»©c£>03si03 en 4k en N w
s i SI N (n O * ♦ • • •03 en 03 NI 4k 4k 03 O O O
00 ® en en SI © &i »# s i en
^ W O s i 03 O O 4fk (n 4k
& Nen 03
M SIa& M
O
NI -» WO 00 O en SI • * • • •s | -* © M 00eo CD e» O 00
w» mm mm ma.CD (n © —* en 4k w g) si « • • • • • * » « •N) GO 4k (D w © N) w en 0300 m (A SI en w N O O <o
—A S* NI —* atnic n - * c o N i C K ) © © s i î n © N i e n N i s i e o ®# # # * « # # * * * # # # # # #s j o i m © e n ç n c n ç o © - * c » oo s i © © O)C n 4 k N C 0 N > O c » O c n 4 k O © s | © N G
—* «A M «I» nt *Wk —AA e n O N iç n O o ïO o e n O N 4k w en w en. î k C f 0 O O G o e n - ,o i« * c i3îo o < x3c n e n 0 30 o e D 4 ko o w SI O) en w
s i SI en to en
s* N —rt» «w, ##M G G O s c n G o c n c n G c n N i w Di w 4k en( \ a s i - * e o - * w © O s | s i ©M O C D - ^ t O M s i ^ O C n ©
<50 en SI Di en0 3 4k O Crt S|
M
en
IN?t
’O2<§ia5"
Q.H'B)OOCTPet-<&
CfloH
:
o>MM«500"OtaoHïj59HMtata§
iIr*|taj4k
t'i en '*■' ta H.J c4 TOt NI os N> ls> to CCI m ta @34k ta ta ta -A en co oo • • • • • • • « •to -»i co ta o s| o (n
B.-.V OS
Ù1
t a t a t a s iOS en SI CfS O ë a s
o 4^ 03 en tnv-A o OS 4k (O CD
I •en taCD GO
«A taen en os to eo oo C3 en»#*##* # # #s| en ta O (n oi en oi
E 3 g “ta (0 ta
( n c 0 e n W " . t o t a O ©irt'i Cfl ,}x »ik ta Os ta 03 • « • • • • • • » • « »o to »A os 03 63 4k en en en
01 ta 01«.3 ta co
taW os "A • « « 01 en O
W - * 03 » • • 0 1 (D Si
- •••> © en # * *01 03 «*
4k SI 4k 03 OI8 8 3 K S
.p,j CÎ3 taî j a a s
4k O ta O ta o os 0 63 CO ta
ta 4'k 4k ta Où
OS ta OS 4» ta (ïj .-ik co ta 03(O w 4k si en os ta ta co =*# * * * * # * # # * #,5s. SI %) 03 © <0 © ta VVA
K»' OS os «a .jk si OS {53 en caSi ta en os 01 4k 4k '■Av ta 01 ta • • • • • • • • • • •03 03 S) fî> 00 4k ta êrf Ifs. © s j
■s* ta œv en ta «-A ta c.'iO 4k SI en CD ta o i (D en si 03© SI ", 4k os ta CD CO &) 01 en
ta ta « en O 4k ta 03SI ta03 en 03 00 r» % * • *. *co os 03 <0
ta - * ta - , en -|k en ta bco 4k ta ta — ta Os OS GCD OS ta 0 os ta » , 0 os ta 00
TJ41, GO CD 03 (0 ta ta 03 ta
Os CD CO 00 CJJ <0 en «»' «si en
CD O en 01 ta
fCA os
ta os osco 0> =.4 *fk
s , ôa © SI :(k
co os «1 os•A,J KJ, c«» o ta • « « « •4k © G
Os
©pH'
>oetl„.
f
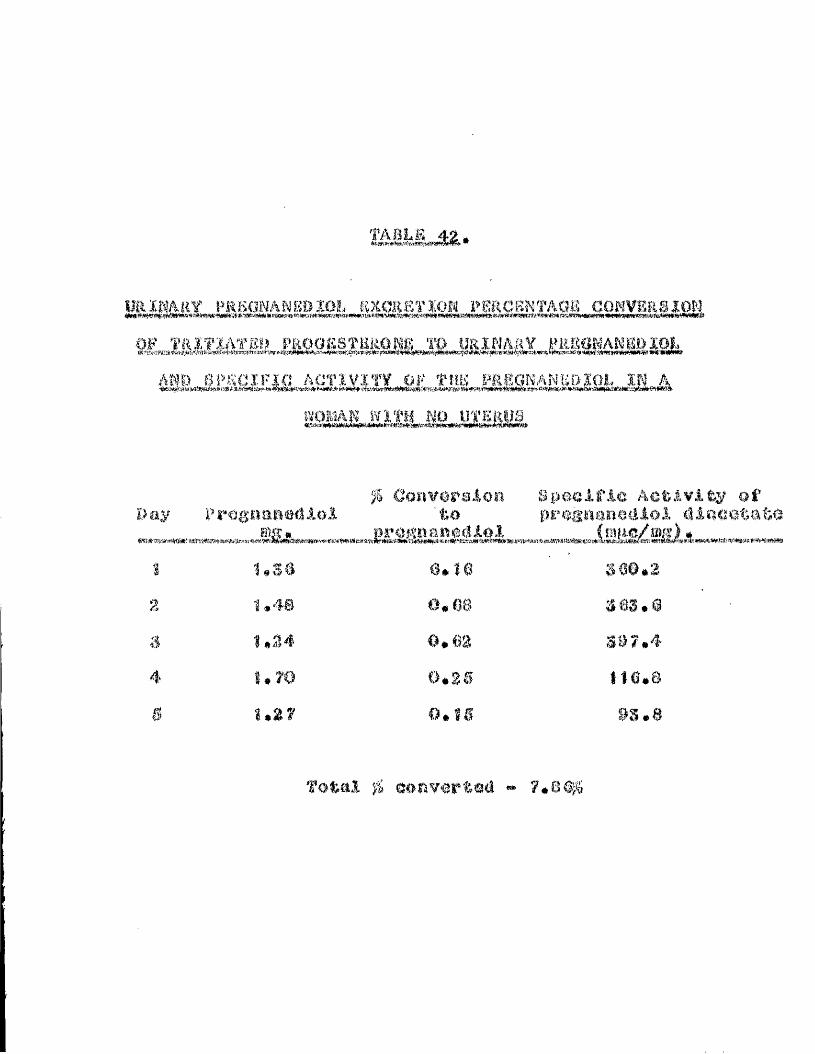
TABLiS 42.
PRÎiOKANgDÏOL gXCREÏÏOK l»mCBNTAQB CONVgRSlONOF TRiTXATSIJ FP.OO£STBkOP3g TO URINARY FiiSOWANBOIOJ,
AND SPSCIFifl ACTIVITY OF fllB PR80NANB0Ï01. IS AWOMAN WITH NO UTERUS
Day P M g a a n W l o lOonveralon
to:gpoGlfjle Activity olT Dr%:%oneUio3, d l ooataW
Î 1.S8 a,10 360.22 1,48 0.08 363.0a 1,24 0*62 S97.44 1.70 0.3S 116.8s 1.27 O.ÎS as.8
1TG#;6&& 33» Gk&#rv<eHri&@(& «» ip*c;<&g;
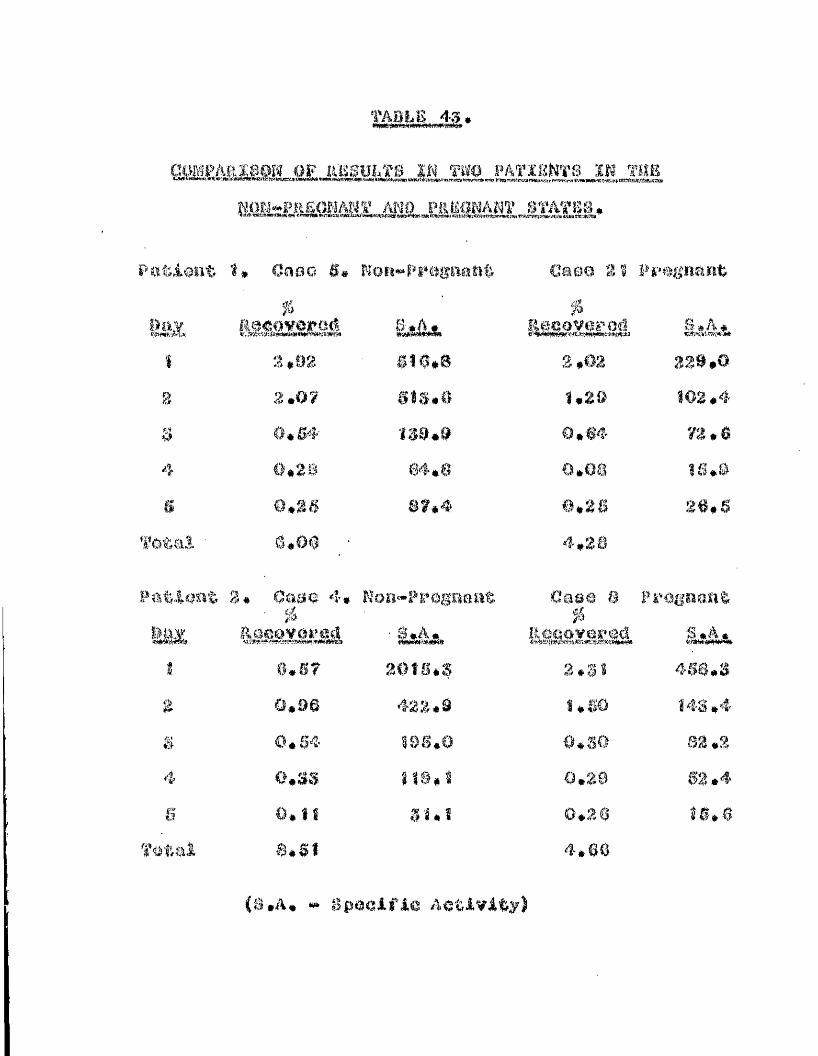
TABLE 43.
m m s â u m m m
Patient 1» Oasct S. WoiJ-PiHigaaîife Case 2! Fî'0gna«t%
HÜîSXSEiâ Ê&&& i ê s s m s â SaiÔsÆ.1 2 #92 610.8 3,02 329.0i 2.07 SÎ3.0 1,20 162.4S 0.64' 139.9 0,64 73.64 0.26 64.8 0.08 16,0
0,38 87.4 0,26 26,6Totai ' §#0# 4,28
Patient 0* Oaae 4*' ^
Ror»™>Ppsgaaat Ü0PO 8
&iSËXS£iâ
Pî'Ogaasit
&&&*1 0,67 20ÎS.S 2.31 468.3
0,96 422.9 1,60 I4S.4& 0.S4 Î9S.0 o.ss 82 .24 o.ss J 1S.Î 0.29 02.4S 0,1! 3Î.Î 0.20 Î6.6
Total 8.61 4.6Ô
(s,A, » SpaeAfie ActAvAty)
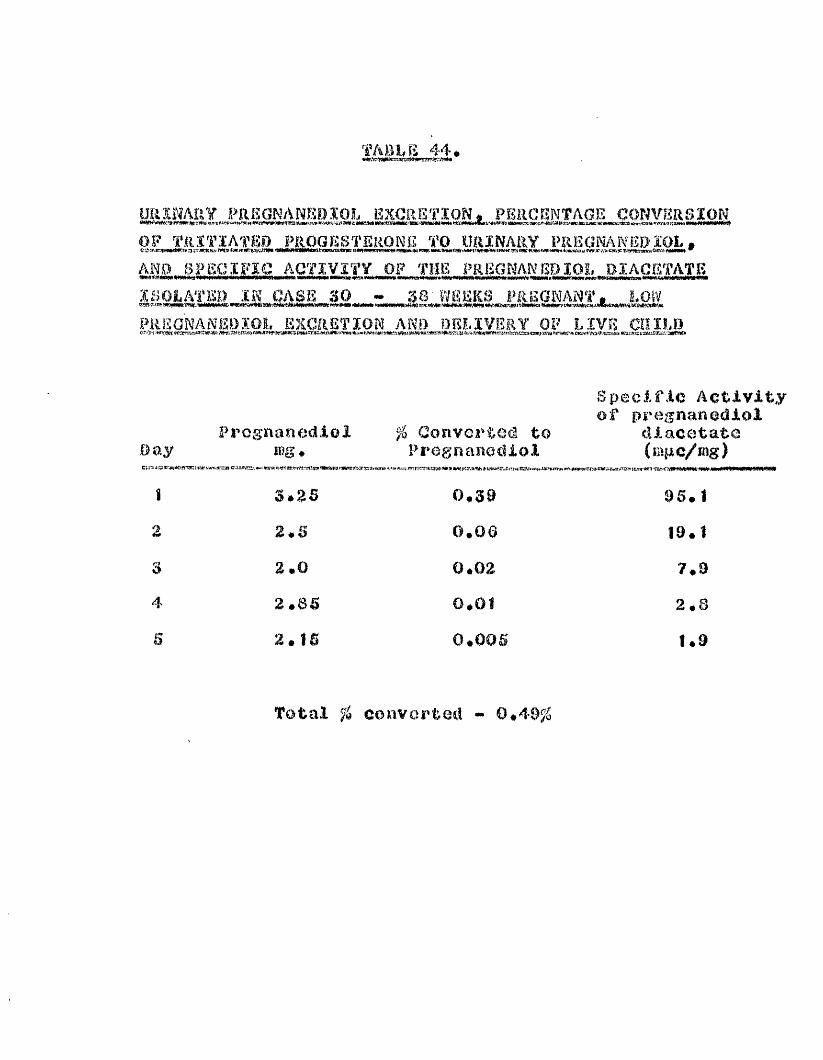
TABLE 44,
UîlîflAîl? PRKGNANKBÎOL EXCRETION, PERCENTAGE CONVERSION OP TRÏTÏATE» PROGESTERONE TO URINARY PREGNANEDïOL,11.11 Uif ME-’«fîi3j(nv wt> qnwa, #w*i .w»i u# *** iMMtrRi «#r#ü#g w# */#«%[ &i w.r 7.71 fcy-jc y?sfn:s sesR wamw
AND SPECIFIC ACTIVITY OF THE PRBGNANBPlOI, DIACETATE
PRSONANE0ÏO1. EXCRETION AND DELIVERY OP LIVE CHILD
Specific Activity of pre^nanediol
Prog'nanediol % Converted to diacetateDay4i'iJ fww,wr=3) c
mg # P rog n a no ci i 0 1 ( mp c/mi
Ï 3$%6 0*$9 05. 1z 2.S 0.06 10.10 &.0 0.02 7.D4s 2*8$ 0*01 2.8B 2*t$ 0.005 1.0
Total % converted - 0*40^6

p ï s t r ï b u t: rs COMPOUNDS ÏN TUS *FREE14 m m # AFTEE INJECTION
m o Q m m m m . INTO A HUMAN FC»BTUS
% of Total RadioactivityMetaDo.iitc .esent in
tivër ' " U S i l iFûlar Material 16,6 47.0Pregnanediol 19.2 13.3aûa«*ditiydr0progeaterone 36,5 17,820p«-diliydroprûgesterone 1t.0 6,7
I Pragnaaolene 3.2 0Progestérone 13.4 15,6
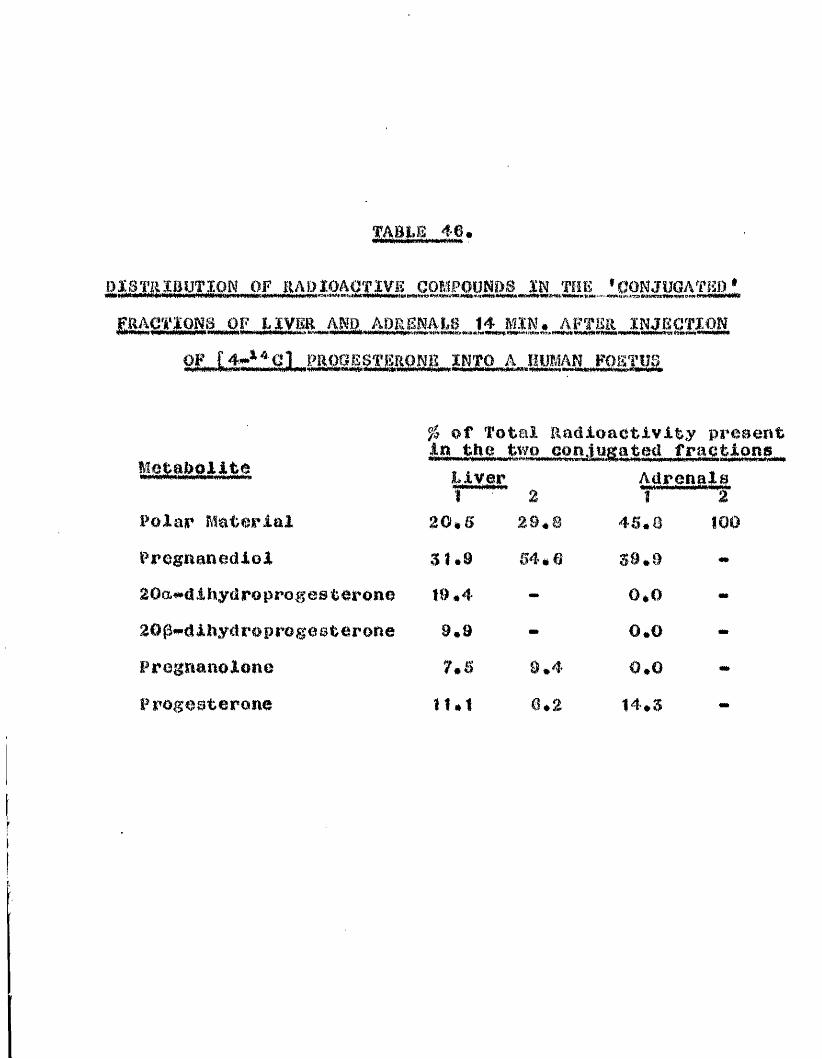
DISTRIBUTION OF RADIOACTIVE COMPOUNDS IN THE 'CONJUGATKO'FRACTIONS OF LIVER AND
A HUMAN FOETUS—^8 I, IMM
# of Total Radioactivity present in the tw<
W a g e1 2Adrenals Î "T
Polar Material 20,S 29.8 45.8 100Pregnanediol 31.9 54.6 S0.920aë»dlihydroprogest6roiia 19.4 0.02Op*^dlhy<ir0prog0sterone 9.9 0.0Frogrianolone 7.5 0 #4" 0.0Progesterone 11.1 0*2 14.5 -

0
1wl>
la;!w
iK.'tûmm
mAMOiAÜmEnca#
<gI*Z'
mMe4ÈÏH
#m
m
W:NAg<Ilog
r*iu#*ftasmti
fe(
gümz
IfiSs*mM
14Om£:'■**mmMmgI.m<
âmmgw
■an.(4m
m
iw8
#te3Pfat,RS<c»!R3
W
Sfw,ww§Gi04
SgWfôS
s*H 0 [(w M 0°,g£g$ c & m #
I *aSi %1 $12U
WS
© p>i"40 0 *4à >0 «*îII
Jg "Ils<a *H
0"4MI
09
# <0 0)0 en 0Î •<P O W% 8 uR)fhi SL0 >* ## -w0 *4m > . o0 •i 0> NS o A, m< # %W V"
##
m*
u»m
#î0M
Nm
:@4♦
O
IN#
#
eo00
M#
m 10 10 O N0 # # • # 1 *tm <0m N O*# *0 00
<0*Î0
:<0#K
N N» #m 00m o
: g0 ou u0 00 00 §to toM p o© & £#H HI A, 0 0QO o 0 00 '4 u &# q Og*0 T) V •0 Hl0 0 &lE (3 H Xî I 0%## f>"O •ü & 00 1 1 »0 bOH 0 6 m. 0 ôQ &# O o Ri è,a, &$ m m 0W a*

*<x>
w
Î
§Mam
<
w?a,a#mBwm1*4
Img%M
IW
IImw
I%M
a*o
3
I 00 ^^ • 30 *o A#04
0, §W K#2 SCü w 0
08 1m & 00 0 q'4 d 0Ch W M0 ©a $4*404•0 0O 1 8U P 00 k U0 0m >> 0a mtm 4 0O n m©o !?CM a
&a #4
Î-#4
^ • 2H 0 O 0 Ctl
00mmlel
I I » I I
I I
*§ i
I 0 Ma m m
Ï© m N• * # # *m O m
##CM# *
I I I I IN W) o to
* # • •.CM K© to 1.tw* CM CM
I I I I I
m m o« * * *4* I 1 %) 1 ^ CAto w to C0
smm*p40
ma &•H 0 "0k 'H
4-.
<
m 0 feO Ê#
*o
to CM O CM to ©) -f# to o o* # # * * # * * • # #10 N O to <0 o to CM w toCD to V*w m* CO <0 to
I I «
CM 00 m <0 ## o* • # # * # • *
Q 00 " t CD N CDYsw tw CM 10
I I I
00 Q 4* 09 VM CM 0) to o. ' # # # « # #M § # 00 00 to Ci Nto ** CM
M # ♦ #0 0 a c© '4 •4 #4"© 8 i fii
Hm to o too *"» to 4*m um w* 1 # 1•H
0 m 0 O to O% © m vm 10o © 0 m0 > © 0q *4 © MH 0 0#
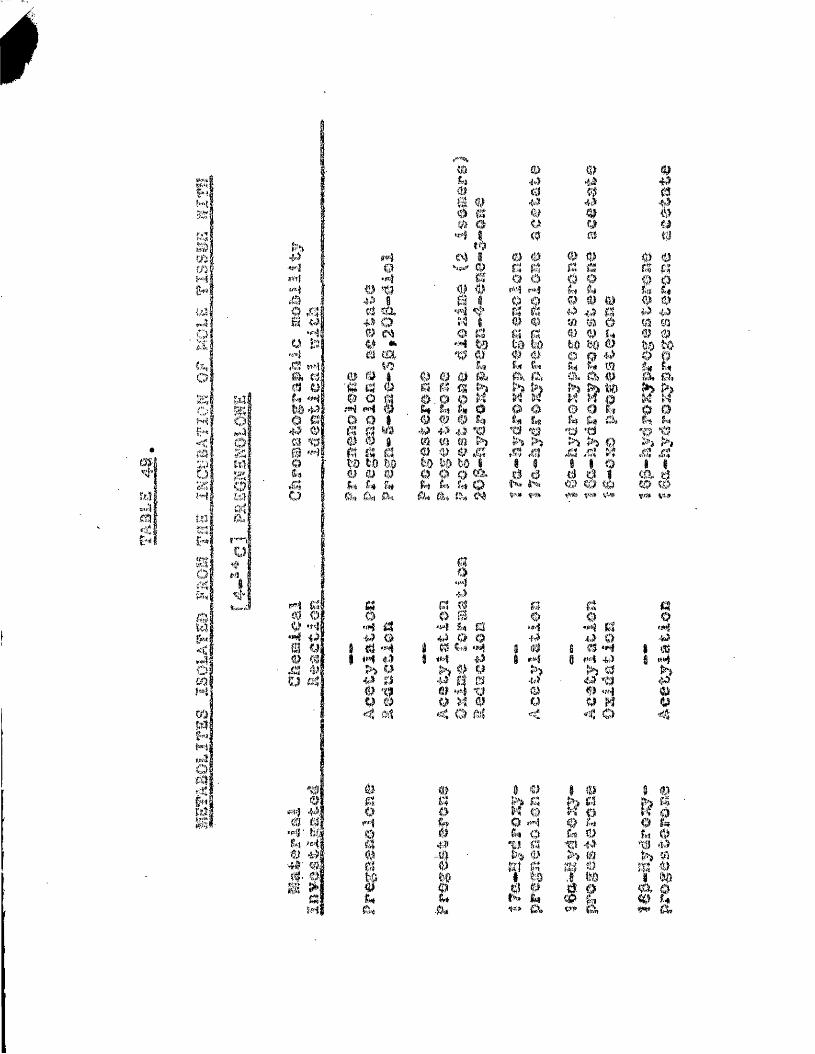
EM
Stos&<W0
A4O
KoM
<#m %)4 ”| U1 z ;
3 i5 ( w<%# Sîrn H
mo
SoùQM
mMsi
w
iMmgo
©S
1II© 4')# 0' ©.# 0- ©%«aM
O«4 o %3 0W .+» o# M 0 «* m (%©© q d © oH <4
d 0 W# m 0 0 d d to LD b6 © © © A» g* &*fôfl fèrj 0h
0"3.v500mum
© 0 0 q q ©M f'î# . © ©
m.
w©m© # &# 0 0 *0m m >i 4) © ,g%6* f.
ik a, %
0 ©fisS'U lea
# #itâ
0 m4à 0Î4 R4i© 4#©© U# #
© © 0 ©q d d q22 2 2© 0 m © ©0 0 # 0 0m m o m me © © ©bO KO © O O 0&4 R4 mq. f% © lî â© a ft q ot*% ^ a k k.T*% >> 0 >) >#X3 X! X3 /3A A ?iêé CD (O*>,ih %W, ç«» 4»,
I*1*11di d q © G d qO: O ^ 0 8 O ow|: '4 q '4 U q •4 •4 # «#0 0 m 0 0 6 •f*j a 0 0■y 1 # '4 # 0 *H 0 i m *4 s 0(3 1 «4 $9 1 #4 i «f*î 0 #4 0 É «M'# w >> >) 0 h# # 0 ë 19 0 0 'tl 0
0 %# m *4 "U © 0 *4 ©y # o ){ © Q U ^ ©< ùi < o M < < O <s
Sî§#4
t
00I4î?-é0W
#(# © iZ* 4»» >* (A&
ê%v> Q,
g
h <0 &, V# &
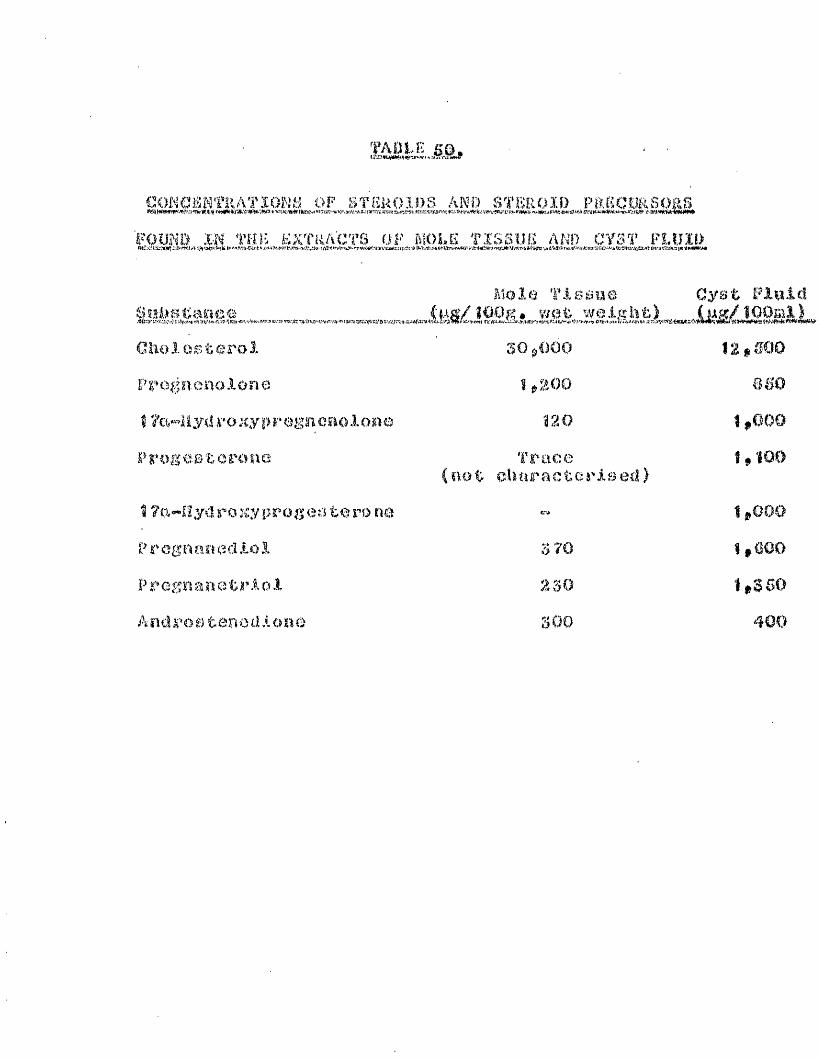
fAEtE
GOKCaMTRATÏOKH OF STEUOIOS AND SÏBROI» PâBCORvSOgS FOUND m THîi EXTRACTS OF MOLK TISSUE AND CYST FLUID
SjlllgtaggOGlioiesteroi Prognenolone I ZcwRyd ro xy p r egn eiiolona Progeeteronfâ
17%«"Hyd ro xy prog CM.’i te ro ne Pr eg nan eel.loi
Pregnanetrioi A n cl r Ù e t e n c d i o n q
Mole T-iasue Cyst Finie!CfAg/îWg# wot weight) (#g/iOOmi)
SOjOOOS ,200
Î20Trace
(not charactGs'ised)
5 70 230 300
12»@00 a SO
1,000
1,100
1,000 1,600 1,350 400
Aqevade^ AMolrod# &,#&*» lahlkawa# a. & Takmki#f# |l003)t Sfcuclies in fetal metahollam#II * M e t a W l i s m of praxesteron0*4«*^'^(; and prmgnenelene"*yaî*^ in the human fetal testes*1 # eiin* (Sndow* Metah# ::5# 885*
Alderÿ R# (#85S); Pregnenedlel e%eretien and eerpu# luteum therapy in habitual abortlen*
rtll# star11* 4» 170#
Andreelly G* (1905)# Corpuo ILuteum Activity afterRyetereetemy In %wmen* Aeta ondeer* Cepnh* 50# 00#
Axelrod# t#a# and Ooid%leher# (1900); Themetabolism of l?o liydroxyprogesterone mû It# relation to congenital adrenal hyporplaela#J# Giln# Bndoor* Metab* %0# MO*
nalN# D* (1953): The Prevention of Prematurity#Proe* a. 900# Med. 40# 877*
palrd# D# (1957)$ Combl%%ed Textbook of Obstetric#and Oynaoeology* *&# & 8* Llvlngiz^tone# Edinburgh#

I ml ÿ D # # W ai ke r# J* ê T h om eon# A# M * ( 1954) : ?h oCauses and Prevention of St,illbirths and first woek deaths-# Pt# III# A Classification of Doaths by clinical causes tho effect of ago# parity and length of gestation on death rates by cause*Jo Obstet# Gynaoc. Or. Emp# 61# 4S3.
Baird# D*# llytton# F.E» & Thomson# A.M-# ( 195$)s Agoand Unman O.eproduetlon. J. Obstot# Cynaee. Or# Emp# 9# 805#
Oanerjea# B-.K* (1052): index of placental function byeadoerine assay and its clinical application in obstetrical practice# J# O W t e t # Oynoec# Or#Commo nw # # # B 03 #
Bor low# J* J, m û Logan # ü#M# < î966)s Estrogen Secretion § Biosynthesis and Metabolisms Their Relationship to the Menatrual Cycle# Steroids 7# soo#
Batiliou# E#E# and Dray# F# ( 196$); Conversion of
'«dchydroisoandrostcronc (30"*8ydroA^ «^androsten-'17«»one) sulphate to II® estrogens in Normal Pregnant ivomen# J# Clin. K W o c r # Motab# M # #208#
Beling# C*Q* (1063)s Gel Filtration of ConjugatedUrinary Oastrogena and its Application in Clinical Aaanya* M#0* Thesia. Periodica# Copenhagen*
Beil# E*T*f Brown# J *B ,# Fotherby# K* & Loraine# J*A* (1862): Effect of a derivative of dithio-oarbnmoyihydrazine on hormone excretion during
the menstrual cycle* Lancet ii# 528*
Bengtsaon# L* Ph* (ï962)î Mieeed Abortion* The
Aetiology# Endocrinology and Treatment*Lancet 1# 339*
Berliner# B.L. and Baltianlck# O.A* ( 1956): The
presence of 6p-hydroxylase in human placenta* j* Clin* Endocr* Metah* 16# BÛ3*
Be vis # l>«€#A* (1051)s Treatment of habitual abortion*
Lancet 2# 207*
Bird# 0*E*, Solomon# 8# # Wiqvist# U* à Oicssfalusy# IS*(1965)3 Formation of 0-21 steroid sulphates and glueosidurenates by previable human foetuses perfused with [4-140] progesterone. Biochiœ* Biophys* Acta 104# 623*
BI im b e rg § G.n* # 8 h or l> or # D * A * & h Lvi ng o to a# S#H# (10 52 ) :
The ProvontIon of iMisoarriage# M.Y* Bt* J# Mod#
52# 720$
lioltog E*# liitmowso# S## Eriksaon# Cl$# wicivifit# W# & DlO/sfaiusy# E* (I904a)s StiKlioo on tho Aromatisation of Neutral itoroids in pregnant Nomon; I Aromatloation of G-19 Steroids by placoatao parfuaod in oita# Acta oadocr#
C*o pal'i $ 4‘5 gt 5 *
Boito# E#t Manoiisots 8 »# ErlWeoa# Cf## Wlqvlot# N* a Blc% fa3.usy # E$ (1994b| i S tiicl loo on the Aromatisation of Neutral. Bteroida in Pragiiant iVomon; 8 - overall Aroma tie at Ion of Pohydro- opiai'Mlrootorone Sulphate circulating in the Foetal and Maternal Compartmente$ Acta endocr* Copah# 46# 570$
Bongiovanni# A.$M$ and Clayton# Q»W# Jr# ( 1954):BimpXlfi^û method for routine déterminâtion of prognanedlol and prognanQtk'lol in urine# Bull#John Hopkino Hos»* 94# 180#
EorgiiU^-^UB» (1006) S The excretioti of prognanedlol All the urine in threatened abortion# Acta Qndoer*.Connh$ 22» 49*
Morth# a# ( $DW); Gomparioon of oont: ioi andpregnanedio.1 excretion In ooloetod oaooo of
prognancy* tn Pmmnt-txl üaro*NoordUoff# Groningen p$ S7*
Berth g II# (I06î)« Mofcaboiisme et closogo <leo oestrogène# mt cours de la grossesse# Bull# Fed* Clyn* et (Unytùt* 13# lîU
Brcuerÿ vu (1864)g' Oeciirronoo and Déterminationof the Wewor Oestrogens In Human ürino* In ResQureli On -Steroltlo# Vol I» p I3S* Romos Il Ponslore Gclontifioo#
Bmmïp t i.O» C19551? A C h e m ic a l m o tîu u l f o r t l ie
determination of oeatriol# oestrone and oostracliol in human urine. Biochem# J. 00/2@ 185.
Ercm ïiÿ JoBq C1US0)s U r i n a r y e x c r e t i o n o f ooetrogono during pregnancy lactation and the re-oatabliah#' ment of menstruation. tanoet 1# 704*

Brown# J.B. (1957)$ Relationship between Urinaryoeatrogen# and oeatrogena produced In the body.Jq Bndocr# 10# 202*
Brown # J * B * # Bui broo k $ li *D* ê Greenwood # F * C * ( 1967) ;An evaluation of a qhemleal method for the estimation of ooatriol# oestrone and oestradlol 170 in human urine# J# Bndoer, 16# 41*
Brown# J#B* and Goyle# M*G* (1963): Urinary exoretionof oestrlol during pregnancy* J. Ohatet* Gynaee#IS r • Commonw * 70# 219*
Burns# J# (1643): Principles of Mldv/lferyg includingdlseaoea of ivomen and children* Longman# Brown# Green and Longmane# London# p 520*
Butenandt# A. and Bchmidt# J* (1934): Oherfuhrung de$pregnanediole in eorpua-luteum-hormon^*Ber# dtech* ehem* Ges* 67# 1901*
Bukton# C*L* (1940): Pregnanediol determinationsas an aid in clinical diagnosis* Am* J. Ohstet# Gynee* 40# 202*

Carr g D .H @ (îd(i7)t Oytogaiotiee of Abortions* In
Comparative Aspects of Roproductivo Fdlluro,
eclq E,® Bqnirschko» Springor-Verlfg; Berlin* p D6*
Casomor#-Oft (1D6D)( Hormono Production of the Isolated Placenta* Acta crulocr* Copnh# 32# Suppl. 45.
Oedard g i » $ Varangot # J# ê ¥aito111 # S * C1962) ?Hsiosyrithcae cic i*ocBtrio,l ilana loe placentae humains porfaooa In vitro: Formation a partirèe certain ©teroiiln noiitreo phenoliqnos hydroxy.100 Bar. ie qarbqn J 0 % 0#r. hebcU Beano* Acad* Sol*Paris# 254# 3B90#
Chamberlain# J## Morris# N#F# â Smith# N,C. (l90Sa)$
ilaa chromatographic onal.yaia of the ancon jugeât cd# neutral# non polar otoroidB of human placenta*J# EiKlacr. 40# D U
Chamberlain# J#* Morris# W,F# â'-Smith,# N.C# ( 1968b);StoroMa in hydatidiform mole#* J, Endocr* 41» 209#
Chang# E#£> aianrnvhitc# W.R* Jr. » ê SandDorg# A .A# ( 1060); Biliary and urinary motaholitos of 4-CM-prog0eterone in h m m m subjects# J. 01 in# Endoer* Me tab* SO# 1568#
Ghannlng» # and Sliort$ R*V# (1066)i TheBiosynthesis of Progosterone in Tiasue Culture by Equine Granulosa cells. In Proceedings of 2nd. International Oongreaa on Hormonal Steroids p 26Î.
Colvin# E.D.# Bartholomew# R.A.# G^'^imea# W.H# & Fish»J.8. (1950): Salvage possibilities in threatenedabortion# Am# J# Ohstet. Gynec. 59# 1208.
Contractor# B * F. » and Fearlman# W.li. ( i960) : ( 16-^11)progesterone metabolism in advanced pregnancy and 00 pho rectomised-hyg ter ectoraiseci women ; urinary ketonic metabolites. Biqohem. J# 76» 36.
Corner# G.W. and Csapo, A. (1953): Action of ovarianhormones on uterine muscle. Brit. Med# J# i# 687.
Council on Pharmacy and Chemistry (1940): Treatmentof Habitual Abortion with Vit E. J# Am. mod.Ass* 14 1 » 2214.
CouttSf J.R.T.# Macnaughton, M#C#» Eosa# F*E. t Walker» J* (1969): atcroidogoncsis in a ease ofHydatidiform mole. J. Bndocr. 44# 355.

Goylc» M.Of» Mitchell » F.L* êausaell» 0*8. (1958):A report on t W ehromatographic aasay of urinary progmmcdlel In pregnancy# J* obstet# Oynaec#Br# Commonw* 63» 560*
Goyle» ^#0#» and Brnwn» ,)*D* (#83): Urinary excretionof oostrlel during pregnancy* II - RoAulto In Normal and Abnormal Pregnancies# J# Obetet*Gynaoc# 8r* Commonw* 70» 225#
Crcpy» 1*» J W a a # 0*» RullcmWieslln» F# ê Jayle» M.F# (#63): Mode do conjugation doa motaholltco dola progesterone dene lea arlnoa de femmes oncclntca* Dull# 8oc* Chlm* blol# Parle 44» $27#
Orooko» A#c*» butt» %v#a#, & Bertrand» r#V* ( # 06): Olinlcal Trial of Human Gonndotrophlna 3:Variation In Banaltlvlty b c W e e n Patients and standardisation of Treatment* Acta ondoct*Copnh# Suppl# 111» 3*
Caapo» A* (1001a): in Frogeotcronc (ed. A#c# Barnoe)*Augusta» Allch*
Csapo, A. (1961b) 2 Defence Mechanism of'Pregnancy#In Progesterone and the Defence Mechanism of Pregnancy {ed. G.E.IV# VVoletenhalme & M.P. Gamer on). J* & A. Churchill Ltd# # London# p3#
Davis# A# (1960): 2605 Oases of Abortion# AClinical Survey# Drit# mod# J# 2# Ï23#
Davis p M#E# and Fiigo# M .N. ( 1947) s Effects of various sex hormones on excretion of pregnanediol early in pregnancy# Proc# Soc# exp# Biol* N#Y. 65# 2BS#
Davie# M.E* and Plot%# E*J* (1957)s The metabolism of progesterone and its clinical use in pregnancy# Recent Prog# îlorm# Ras# 13# 347#
Davie# M#E* and Plots# E*J# (1950)$ Hormones in human P0P product ion# Ft II # Further Investigation of steroid metabolism in human pregnancy# Am# J. Obstet# Gynee* 76# 930#
Davis# M#E#a Plotz# E#J#@ Lo Roy# G#¥* & Gould# G#R.(1956): Hormones in reproduction# Part X#Metabolism of Progesterone# Am# J# Ob at at# C?yn«c# 72# 740#
Deansloy» R. (lOOO)i The Endocrinology of Pregnancy and Foetal life# Xn M a r s h a l l Physiology of Reproduction# ed# /uS# Parkes# Longmans,® Green
Co* London#
Biczfulimyp E# (1004): Endocrine functions of thefoato-plaeental unit# Fedn# Proc# Fedn* Am*Bocs# axp* M o l # 23» 701#
Picsfaiusy» B# and Borell » U# (IBOl): Influence ofoophorectomy on steroid excretion in earX^^ pregnancy# J # Clin# Endear#'Metah. 21 » 1119*
Dic%f ailisy » E # and Troen » P • {1961 ) g Endocri.neFunctioiiG of the Human Placenta# Vit# Uorm# 19» 229#
0ie:^faluey» E# » Tiilinger» K-0#» Wiqviet^ N # , Levitt» M # » Condon» 0*P# & B a n d s » J# (I9 6?i)? Ris|.>ositiori of Intra***amnioticaiiy Administered Estrioi-î6-C*' ami Estrone-16-0 " Sulphate by Women # J # cl la#Eridocr# Me tab# 23» 503#
FIlciÊîfaliisy g* anti Banagiano» G# (1966)? Oestrogen Metabolism in Mid PrcLgnancy* In Research on Steroids» VoX 2» p2 7# Rome? I.l Pensiero Beicntifico#
Donnelly» J.F# and Lock» f.R* (1053): Indicationsthe Sterilisation of Women# Bull» Am# Goll# Surgeons» 3$» 07#
Duncanp J# Matthews (1871): Fecundity» Fertility»sterility and allied topics# Adam & Ghas. Black# Kdinburgh 1871*
Eastman» N#J# (1956)3 Williams Obstetrics* 11th Edition# Appleten-Oentury» New York#
Rberlein» %V#R# (10 85)$ Steroids and Sterols inUmbilical Cord Blood# J# Clin# Endoqr# Metab#25» 1101#
Edwards» A#w#F# (1060): The moaning of binomialdistribution# Nature (bond) 186» 1074#
Emerman» S#$ bancis# J*» Levitz# M#» Wiqvist» M# &Diczfalusy» K# (1065}: Metabolism of Estrone-6»7-li® Sulphate in the Perfused Human Fetus#J# Clin# Endocr# Metab* 25$ 63D#
Engel» P# (1044): A study on inactivation of ovarianhormones by the liver# Notes and Comments# Endocrinology 35» 70#
Krb» H.» Kellcr» M.» Uausorp.a.A® R® (1961):Eetrogon and pregnanodiûl excrétion in ■ •hydafeifjiform mole» Oy uaeco log la (Basel) 15*2» 317»
Eton» iU and Short» R.V* (1900)2 Blood progeatororiolevel a In nbmrmnl prognancAos® J» Obstot» (lynaoc* Sr* Emp# 07g 785»
ForbOBf} T»a», ( 1055): Apparent secretion of progostoroBO' by human and go@t foetiisos# Eniloerifiolag\y 50$ ODD*
Forbesp T®li® and Hooker» C»W# ( 1940)g Inactivity
of bouml plasma pro geetorono# • Froc» 8oc. o%p.Biol» M»y. 70$ 082.
Fothorby» 1C* (1002): The ovarian production of. apregaanodlol precursor. J. Endocr. 25-» 10»
Potherby, li* ( 1904)s The Biochemistry of Progesterone»¥ 11. # Horm« 22 » 15S «
Potherby# K# and Lovo# 0 «N . (1960)$ A modified method
for the estimation of pregnanet&'iol In urine.A® Endocr. 20$ 157,

FotherbYjj IC,# ». Jamas» F#$ Kamyab» B*» Kiopper» A#I#R Wilson» G #11# (1965)$. Excretioaii of 6-oxygenated metabolites of progeeterone and Bp-pregnane-Sa» I7a^20a-t’.iriol during pregnancy* J* Endocr. 33» 135#
Frandsan» V*A* ( 106$) s The site of production of oestrogenic hormones in human pregnancy*Europ. Rev*- Rndoer. I » Z27*
FrandseOÿ V*A* and Stakoman» Cl* (1960): UrinaryExcretion of Oestriol in Pathological Pregnancies*
. mod * Bull » 7* 98*
F r ÜUÛ a en $ ¥ * A * and B t a keman » ( 10 6 1 ) g The Site o fProduction of Oestrogenic Hormones in Human Pregnancy* I - Hormone Excretion in Pregnancy with Anoncephalic Foetus* Acta endocr* Oopnh#58# 585*
Frandaen» V*A* and Stakoman# 0* (10 63): The Site ofProduction of Oestrogenic Hormones in Human Pregnancy. II - Experimental Investigations on theEo I e of th e Foet a 1 A d r eii a I * Acta e nd o c r * Co pnh *43» 184*
FranciGon» V .A . and S tû liem an» Cl® ( 1 9 6 4 ) : E x c r é t i o n o f
ho rm ones i n üaees o f h y d o t l d i fo rm m o le and cIîosvIob
epithelioma® A eta ondocr® Gopnh* suppl 00# p$ 81®
Froewlsg J® (1 003)s Whon does adequate rovereal of
production of the pregnancy-maintaining hormoneof tile pregnancy corpus lut cum for the placenta occm''? A clinical contribution® Wien®, Klin®wschr® 75» 300.
Ftitoeliiraap l>®K®$ Pradlqw» ll.it » Hallman» L#» Znmoff @ D«
R Clailaghor» T*F® Study of 17-hydroxy-progeatcronc-4-C14 in Man® J® Qlin* Endocr® Mctab#2 1» 705®
Oomgell# Co (I060)§ Induction of ovulation wlth human(loiiadotrophind® Roc ont Prog® llora® HO0 ® 2 1» 170®
Gemmoll C«A* and ilooB» P® ( 1006)s Fregnanoien followingtreatment with human gonadotrophins® Am® J®Obetot® Gyneo® 04» 400*
ÛiiUmm^ Jo and Stein » 1.1 oB® ( 1041) 3 Human corpus
lutcum of pregnancy® Surgery# Oyncc# Ohetot*72» 120®

* II* (Î949)î The relation of ïih Incompatibility to abortion. Am. J* Obstet. Clynec* 5?# 323.
Qoobolsmann» tj. » #1 q v i s t » N. » 0 1 c%falusy » B. $ Lévita » M « $ Condon » 0«P « & Danclo» J . (î0G6)s Fate-of Intra- omnlotically Administered Ocstriol ^n-s-sulphato and OQstriol îO-^^C-îO Cllncoolclaronato in Pregnanthhnmm at Mid-term* A eta on doer* Ooprilio 52» S50 #
QoMBiehev p jjh* ( 1964) g Donbl0-blind trial of aprogestin in habitual abortion* J* Am. mod * Asa. $88» 132*
Ooldaleher» J * W @ and Boni.gno» RoB© (1058)? Tho
Treatment of Threatened and Recurrent Abortion:A Critical Review# Am.. J. Obstet. Oynoo# 75# 1202.
Granville» A#B, t$853): Graphic illustrations ofAbortion and The Dieeaooe of Menstruation.W V a t cl y p r i n ted* I. o ado n *
Greenep J.w.$ Touchstone# J.C# and Fiolde# El. ( iBOI)i Urinary estriol ao cm index of placental function.A preliminary report. Qbet. Oyn# (N.Y.) 7$ 340.
g ivï » g Cooper g tVo & iVaIkorp J# ( 1S>62) sPlasma progestérone ifi tho motlu^r and foetus in
the second half of Inman prog^nanoy# J# Gbetet#OynaéCo Dr» Commonw# ODj, 772#
Grelg j) Ma and Macnaughton# M^C.o {'1907) : Radioactive^otaboixtcu in the liver and adreualo of the human foetus after ad mi aist r otion of [4«*’' c3 PragcBteranu# J# Eadoor# 3D# t&8*
G a te rm a n $ H . 8 # ( # 9 8 3 ) : P r o g e s te r o n e m e ta b o l is m In t l i a
human female; Xta significance in relation to r e p r o d u c t i o n # R e c e n t Prog# H o t o « Eea# 0 , 293# ■
Guttmachei’ÎÎ A#F® Cl95C>)s Factoro Affecting normalexpectancy of eonccptioru *1# Am, mad# âes# 10 3, 8611#
g R@ and Martin# J#D# (1064) i Urinary oosferogon eater at ion in Threatoned abortion# J# Obatot#Gynaec# Br# Cùt m m m ^ ?1 g 600*
Hamburgerj, G* ( 1943): Contribution to hormonal<l:iagnosia of hydatidlferm mo 1 o and chorion epithelioma based on 76 cases with hormonal analyooe#Acta Ohs tot o ilynoe# ScancU 24# 45#
# McOaiîghcy# lUS*# Scoggin# w,II* &Thornton# w $i. -( IB#4)% Ceneomtratiun ef
progesterone An nowborn and ;%»cornai oircuiation
at delivery• -Obat# Oyn, N*Y* 23 s» 413#
The motahoiism
and aepuration-RoA# and Fothorby* E#
o f p rogesterone in man* S x tra o t
by counter currant distribution of the metabolitesurine® ia U # V Oil ao8#
Hmlm^BBp R#A# and tovo, D#N* C1906)* Studios on estimation of urinary pregnanotrioi during pregnancy and childhood# Acta ondoor. Copah.
CO# E«C# Jar## Mikhail # G * # Srikoson# <1* # Wiqvlst # K# â Diczfalusy# E*< (1064)8 Oostradiol Metabolism in
i_ Previablc Human Foetus and- in the Foetovpiacenta,Acta ondocr# Gopniu 4 6 %D?#A #
(ï053)i Fécondité des Muringos$ Nouvelles. Mothodô do Meouro* Paria# Presses Univ# Franco*
Herrmann# r/# and Silverman# t* ( 10S7)î Excretion ofpregnanc“*3a# î 7a#20o,«^triol in pregnancy # J# ' clin* E n d o c r # M o t u b # 1 7 ^ 1 4 6 2 *

^fotniiil?o4(l nîüuinif l i t ouoyqo%jj iioBojraso x ts jo nvnmj.mWQ
u o y 3 î 3 O î 2 R A 4 0 C c | o ^ u a C T Y i ^ pun »%| *^*lp|c|Of|
'S09♦ riDopu^ * DuiittSoAAl OY^oqvTi) puc ‘imihmn
wy uoŸ^^'*:0^o _ao^ojî'%s30 9(0D6&)
^ ^opyMUH * * v ^mTCtUTV **%*d
*U';S *To?e *'00G *ouuoB <^omJojT^upiCq eiom
0p (mo un auBuXnduiooou oonbyJUAO eeqs/Tiq op prubfx
up ofcuonktmf ocA'it’Uv *i>maojj'4op-»Cq c f op
e^fcuoaaoii pph^ji $(qwl ) *W ^STB#UYn pun *n ^CffOT^Ufll
*6'H " DoaAo *2@^nqo* r *#V *UAO UUum%3 OTSOtOliqOd pUB PRIU SOU ^
JO uoY^dTJOSDp ' (o%48 RUOTTTAOdd jo 2 8%9%qoqdw$02 eouodojo*^ X?rfOocle q^T/A moAO ucmnq /i!|»,niO
j 0 %ïmmlojùhOp i!o P(lr|/Ol) p u n
' *liU ^02Z * popj * r ^|i?UO M M * 2 u o m 2 B O J 3 p i m
S|S0i3o20if4ud 021 sU€>T2doqv Tun^TUDU PUe pouo2%oa% <^sno©«U2UOds S(i'i>6i ) *Q*U ^Ouoqs^uiATi pun ® j / v
* 1 1 d *tiTt40€| *0î|ï,prAr|îîf5p *|>o
OAj2onpo,MlEn: jo eqoodav oà^%n.mûvâù^
m m uf moMG4(% i i M O A O oiu *J/¥

.ton * JO /:42STUTN Ptic OûTJJO cmO||>^ ( a S û E ) 2^i0do'^i a o i 2 4 o q v im m ^ ^ p n m o Q %02i m u r j . m d o
*9061 *2tWs 112-pl ^40,WTW *m dTqp% ?uo j o qxo^üOO lOTOog 0% : (e 0 G : )
*im 0 r fO 4 0 2 s miUtQO aiiTAOg
jo 0oiÆ2:tiH S u î A O O ï D UTBtiD^opfg 10402^010%aicmicHi'oqci no suîqdcM2O|?OJiiO0 ' j.o 2Doj,ih oa^îA ut
s (8 9 0 1 ) *1*13 p w * T i i 0 M 3 4 0 a ^*(2 ^ ïT % 0 l
* aî’M * d * p46 JXO O0OT2B 0ît<m«i 0 T J î 2 U O T a s ï î a M i | à | ) t t « ^ a o u o i î D J c îiomnii
j o vmoiOTS/Ztpi aq j: puo
*t'PB *sav *pow *mv *r *uoT2'10(1'Vonoouoquods pim * s * ù ^uoepUH
*10 V'F /k^otout400pu^ *|K>Ofq UT UU 04020 00041#j o 2 4 o d 0 œ . J 2 o%l " ( 0 P 6 I ) *1I*& ^ 0 ô q j o / | pite q # 0 *4o:>|00|î
A8oTOUT40opusi * e u w D 2 S o 0 w d j o àqimoum o ^ m t f m
4 0 J A u e s B Ô T q V ^ s o q ja e : p u e # ^ * 0 < ^40}ï0o n
James# (1962)s On the Probability that mhabituai aborter sviii abo&'*t a carrent
pregnancy* J. obatct# CIjmaeo* Br* Gemmcmv# 09# 000
James »V*H* ( 1D05); .Not00 Towards an Qpidomioiogy ofBpoataueouB Abortion# Aftu J* Jam* Genet, 16# 223,
ê'tmoBp F* and Fothorby# II# (I0G6)| A method far the estimation of O-^oxyganatcd metabolites of progesterone in tirlne# Biocltem, J# 96# 469,
Javert# C<?To ( 1067)^ in Spontmioeno and llebitiaal Abortion by €%?# Javnrt# fttcClrav dllll liooh Co,Inc, Now York#
Javert# 0*T,# Finn# W#F# and standor# H#J, (1040): Primary and Secondary Habitual Abortion*Am, J, obotet, Oyncc, 67# 078#
Jayle# M,F, C î9 0S)§ Rtlologloal Hormonal factors ofRepeated Abortions# in Hormonal Steroids# Vol 2# Academic Press New York, ccU Martini, L, acidPcclie# A, p 717*
Jones# 0 #E#s# and Dclfa# is# ( 195'#): Endocrine patternsla term pregnancies following abortion# J* Am,'med#A b s # |4e. ' 1212#
Jtmgrnann# ami Schweppo# ( 1907): Biosynthemioarul metabolism of neutral ateroiilo by himaii mid ter mi
placenta anti fetal liver* J * GlXn, Hndocr^ Mo tan o27# 1151.
Kaiser # r ® (|06O); On the elm ago in the aatrogeii/. p.ra,gaaruKllo.l ratio during pragnanoy# Arch,Oyn^iCRy 19% # 420,
Kamynb? S * and Fotherby# fC, CHHtïlH quoted by
Vit# & Horm, 23# 63#
Kat&# s.R,# Danois# J# a Levitt# M# (#06): RelativeTran a fcr of Gstrioi ami its OonjugatOQ AcrooB the Fetal Membranpa in vitro# Endocrinology 76# 722#
Katsfman# (% and Zander# J# ( 1960)g Progeateron inmenachliohem hint miû gowabe# Klin, WocIh**# $4# 7*
Keller# A#@ Matthew# McKay# R## Brown# &Roy g B«Ja (1B50)s Some clinical applications of oeatrogcn J@ Obotet# Gynnqc, Dr# Emp*OG# 004#
Kloppor^ /%$ (1902)g Variations in Oeatriel outpat inhate Pregnancy# Acta ondoer# Copnh# Suppl# 07# 122#
3f
Kloppar^ Aé# H.A* ami Brown^ J#B* ( 1955}gA' Method for the dotormlnatlon of urinary progs an ôihioÂ# J* EWoer* 13# 209,
Kio'ppar# /w and Mlehiog E,*A, ( 1U6C) s The oxcretiou urinary pregnanoéioi aW%Vr administration of .
progeetorüuoé . J. Eadocr. 13# 360$
Kioppar# A * g strong9 J»A» and Cook# L«R, ( Ï967)s The oxcretion•of prognanedioi and adrenocqrticalactivity* J, Endocr# 16» ISO#
Klopper» A# and Maon&ughton# M#0, (ID60): Theidentification of PregnanodidI in iiqiior- amnii.# bile and faeces# J, Sadoctr# IS# ;|I9#
Klopper » A# » Wmmaughton^ M»C, and Mich le# E.A® ( 1901); oestrloi and orognanodlol oxcrotlon during pregnancy and at the onset of labour. J® Endocr.2 2 ® KiV.
Klopper» A# and Wlf.eon» G.R. ( ID62).% A method for theassay of oestrial la pregnancy urine. J. ohstot. Gynaec# hr. Commons# 89» 633#
ICIopper-îj A* ami ruiiewicz# (1903)s ' Urinaryexcretion of oestriol and prognanediol during normal pregnancy*- J* Obstet* Gynaoc,.Br#Cpramonv/*' 70# 1024,. ,
iClopper» A, #. # A*G, and Anderson# ( 1966) :Changes in Steroid Mormone Excretion during Abortioh'in mid-pregnancy by the Intra amniotic injection of hypertonic saline* J* Ohatet* Gynaec* B r * Commonw, 73@ 390*
Kuppermah# H*S*#'Seidl# J, ü^û Epstein# J*A, (19 60)?Use of progestins in habitual abortion, Notes on salvage and foetal afanormalitlee, Acta endocr, Oopnh. 51, 673,
n
ICurlyaum# H, and Csapo# A* (I9 01)s Placenta andmyométrial block* Am* J* Obstet* Oynoc* 82# 592*
Landau# R*L* and Lanes, M*L, (1950)$ Urinarypregnanetriol of testicular origin* J* Clin* Endocr* Metab# 19# 1399*
1.0 Maire# W.J.# Rico# B*E. and Savard# K*' (1958) sSteroid Hormone Formation in the Human Ovary; V* Synthesis of Progesterone in vitro in Corpora Lutoaduring the lleproductivo Cycle* J. Clin. Bndoer* Metab,
28, 1249
Lontera# "Oeatriolultscheiding in dourlno on do Anhtomioche Toestand van de Placenta"*ivU0s. Thesis# University of Qrooiogen®. JoB#
Walters# Ovoningon#
Loon# YoA.p Dnlbrook# und Gornor# (#960):steroid ouiphataao# aryloislphataao# and p*»gluûnronlûùoo kn mollusoa* B-iechom, J* 75& 01 2 *
Levitîs0 M. » Emoroan# S# â Panels^ J$ C I802)i Bterol Synthoaim in Forfuood Human placenta* Bxcerptamed* Intaroat, Cong# Sor* 51# Z20♦
h J. t tl e 0 l> i iliar 11.ni$# J * ù, Myha Im # B * {III59 ) iConversion of progeotorono to «‘prognen-^Oa^^ol*^ 3-ono by human placenta in vitro* Acta ondocr*Coimh# 30 J, 530,
Little3 % nuû Shav;# A* (ID6 l)g Conversion of progeeter* one to IFcwhyd roxyprog os t or one by human piaean ta In vitro. Acta endoor, Copnh® @G# 455.
Little# B# # Shaw» A* _ A Purdy* R* ( Conversion of progesterone to t r oxy pr ene-3 #20 die noand androat-4-ono-3 » I ?**diono by human placenta in vitro, Acta qndocr, Copnh# 43» 610#
Loraine# # Bell# # Marlmoos# R.A. & llarrieou#M *T# (1900); The effect of clomipheno on hori usno excretion in patients with gaJ,o.ctorrhoea*
Acta on doer# Cîopnh, 52 # 52 7#
Loraine JoA, and Boil# R.T# (l06O)i Fortiiity andContraception in the human female, B,S, Livingstone h til « Ed i nh urgh,
Maipae# F# (I93B); A Study of Abortion Sequences,
J D Ohs tot, Oynaec, hr, Hmp#; 45# 052,
Marrian# a,F# (#029): fhe chemistry of ooatrin*1» rreparation from urine and reparation from an unidentified solid alcohol, Miochem, J ,
23» m w #
Ma r r i a n# G , F # # R ua soil# M • E # oiid A the r den # 5, M . ( 10 54 ) % Urinary exoretien of nr eg n medial in poot mmminmotil m m o n and men during prolonged daily administration of progcatorone# J, Enilacr# 10# 351#
Masson# Cl# and Hoffman# M#M# (1946); Studios on the5role of the liver in the metabolism of progestérone®
Endocrinology 37» III#
Midgioy# ami Jaffe# iUB* ( 1986); HumanIirtoiEtiEing hermene In Bmmi^ during tlio menstrualcycle; determination by radioimmunoao^ay,
/
J, Clin* Emlocr# Metob, 2G# 1376#
Mikhail# 0. s> Zander# J# & Allen# W.M* ( Î963): store idsin human ovarian vein blood# J. Clin# Gndoor#Metab. 23» 128?#
Mikhail » C. and Allen# %V #M. {1007) t ovarian functionIn human pregnancy. Am# J# Obatet, Oynec. 99# 308*
Miteho11# F#L. (19 67)g Steroid Metabolism in the Fotopiaceatal Unit and la early Childhood."Vit# a horm# 200 I© I#
Morgan» J . » a n c k o t tp iV#R. & Hunt# T . ( ( 0 8 0 ) ; The
place of pregustoron# in the treatment of Abortion* J. Obctot* Oynaec# Br# Emp. 07» 323*
McKomm# T# and Record» R#C# ( 1067)§ An examination of fertility of women following pregnancy according to height and weight. Brit# J# prev.ri>Oe a JilOQ g 1 1» 102 *

Maqnaugbtûn» (190?)? Hormone oxerotion os amcasuromont #f fetal growth and development #Ara# J 0 nBt e t o Oyneq, 07» 90B ,
Helsoîtj^ and Greene^ ïiji^ (19SB); Some observationsof the histology of the human ovary duringpregnancy $ Amo J * Obsteto Gynee* 76® 66,
W e l l » A#D* and M a r r i a n » ( 1 9 3 6 ) ; N o te on proBonoe
in human pregnancy urine of acid^hydroXyBablo combined form of pregnonediol, Bieehem, J, 30# I53S#
Paintin » 0.E* (Î062)t The Epidemiology of Antepartumîlaarnorrhage® J , Ohstet® Gynaoc, Br# Commomv,60» 614,
Palmer» R# p Blair» J\A# » HrIksson# 0® & Dlcsfaluoy» E,( #0 0 0 ) S Stud lea on the metaholia'm of C-2 I steroid a
in the human foeto-^placontal unit. 3. Motahoiism of progesterone and 20 a and 20 p d 1 hycî ro prog est or on el>y midterm placentas porfusod In o.iti!* Acta eriéocr. Copnh. 53» 40 7 *
f a trin I» G. it 0 64 ) s T h o cl i b a p pc a r a nc e o f i> rog es ter one from the Blood in normal women and In women with ûlBùiivoB of the liver. Exccrpta Med, Endocr# 18»No. 206,
Payne# (î94î)$ Hormone utuéloB in premonee ofhyilaticllfoTO moio tmû ohorio epithelioma*
, Surgery Gynee. Ohatot, 73» 80*
F ear Ima&i » J * B * ( 1*)67) 2 [16*** b ] p I'og e e t orone m et abo .1X amIn advanced pregnancy and in DOphoroctomiEed-^- Hyoterectcmieed amen* bioeham* 3* 07» I*
PearImam^ , and üorcoo» E* (1952a): isolation of. On I B t er o id o f r op\ h%%man pi ac on ta, J * b io i •
m* 104» 00 7*
faariman» 4*Ho and Ooreeo# E* (IP52fo)g progeaiarono from human placenta.
, Chem* 190» 70,
Isolation of J, hieI*
PlgoaiKl » îl « and BurthXaiilt » li, ( 10 57) s Coritributiana i ' otIÎÛ Q do 1 e 1 imlna11 on upina 1 ro dn ps"egnanclioi dans la inolo et sans le ehorXa«=H;pithi5liosie*Gynec * ot O b n w t . 50 @ 34-î*
P1Qtz 0 B a j 0 illic'l J)aVis » *E 0 ( 1B5 7 ); i) 1 ùtr j.bn11 on ofradioactivity in human maternal and foetal tisanes following administration of 4* progeotoronc#Proc* Socw exp, Biol, ) 96» 92,

Popjaks CI* imû üorsiforth» (îi60)î TheBloayatlieais of Cholestérol# Adv# E.asymol#2 2 » 261#
PulWci%icn g M«0 Lehtinoiip A » ê Hartiaiak» J# (1961)3Mataboilem of progesterone by liver of foetal and newborn gulftoa-^pig# Ann# Mod#• Exp# Penn# SB# 57»
iI i, igan E « J # aud Ro thohiId » I # i t& $7) Kate of preg.ruuied.iol aKcroti.on following intra- portal or X a t r a o y a t em 1 c i n t r a v e ao a s ad m 1 n I s t r a 11 o n o f progesterone in human subjects# Jo Clin, Endocr#
17. 695#
Rawlingsp C#J# and Krieger^ V#I# (1959): The valueof the progunnedloi excretion test in the prognosisof abortion# J* ObBtet# Gynaec# hr# Emp# GO» 805#
Reidp B#M, ( Î90O5 Unexplained Prematurity; Investigation o f I 0 8 s lb 1 o C an s e s * J * l) b b t et • Oy n a o c * B r •Commonw# 6 8» 700,
Report of the Biological and Medical Committoo * Paperof Royal Commision on Population# Vol IV* 10 50#Ilf hi 0 Ï.Î ® 0 ♦ t o n t.l o n #

7iim A N * Y* Acud # b d • 75 ». 09 I,
Roberta» D * F, (iB€>4)t Probability of SpontaneousA Port 1 o n .i n Wn 11 i p a r o o « J, Ro p r o d * F e rt# ■ 7 » 8 9 »
Hobocm» Tcli* and GorouiX» A*0« ( 1966) s Prognanodlolaosays and the abortion ’problem* Canad# Mmu A80# J* 72» 830.
Rogers# J@ (19 50)? Progesterone metabolism in liverdisease* J * Clin. Endacr* Metat * Î6» 114.
Romanoff » B*P, (19 02); Tpo oocration rate ofprogeGtorene and daily OKorotion of prognauedioi 3o,»l7a»20cj, in young men after* administration of pr0goHteror»e - 4 - c « Ëkcorpta MocU {Internat*Cong* Ser)» 5?^ 194,
Romanoff» L®l%p Riorris» C.W. » Welch » P. » Grace» lUPe & P1 n CIÎ s » Q * i i 0 OS ) I ti e t a b 0 11 # m o f pr o g os to r one
in young and elderly men® J, Clin » Endocr. Me tab# 23.» 286.

Eonap » F , F • p Parsons » L ♦ » U amio t » E * & Wo tix » H',II,(1000)3 Studies in steroid metabolism IK* The excretion of prcgnane-Sci» 17%»20o. trioi during pregnancy. J. C ü n * Endocr* Me tab, 20» 365*
Eothchild» I * (1953); On conversion of intravonouaiy administered progesterone to pregnanedioi in human f emale* J * Clin* Endocr * Metab. 13 » Î 2 1S •
Roy» E»J* (I962)s the concentration of oestrogens in maternai and foetal blood obtained at Caesarean Section and the effect of hospitalisation on maternal blood oestrogen levels# J* Ohstet*Oynaec* Or* Commomv* 89» 196*
Rucker» M*P# (1852); Spontaneous abortions; toomany or too few* J * Internat* Coll* 8urg* Î7» 328*
llunnebaum» B# and Zander» J# ( 19 62); Progesterone»tâ -pregnene-ZOa-oI-S-foriO» i/" -pregncn-20fi-ol-S-ono and 17a hydro^cyprogesterone in the plasma of the umbilical vein and arteries* K^in* VVschr* 40» 453*
Russell) C *8*) Coyle» M*G*» Dewhurst» C.S* & Paine» C*G* (1957)$ Prcgnanedioi excretion in normal and abnormal pregnancy. J, Obstet# Oynaec* hr* Emp* 64» (348
Ryan# K, J, ( 10GO) : Motabolâsm ©f oestraneby lliHiian Placenta# Endocrine logy GO» 491#
Ryan» It.J# and Potro» ( 1DGG); Steroid Biosyiithoeis
by IUime.n Ovarian Granuloaa miû Thcoal coils®J 0 C i i n , E nû o c r ® M et ab ® 2 '6 ® 4 6 «
Ryan $ K#J, and S m.l t h » O. W . (19 8 5 ) s B1 og en c s i a of
Steroid Hormones in the Human Ovary # RecentFrogs Harm* Eos. 21» 367#
SamueiBp L.T# {10 60)s In Metabolic Pathways 1#CIrccîiborg B AM , ed® Academic Press» London#
S end be rg » A » A # an d B i aumvhite » w #R. ( 1D 58 ) ; f homet abolie fate of progesterone in human subjects* J, OXin# Rndoor# Motab# IB» 2 55#
8#vardg K#p Marsh» J,M# and Rice» 8#F# ( #85):Gonadotrophins and ovarian ateroidogonoais.Rcooat Prog# Horm# Res# 21» 235#
S ehoon oc k » i‘. J# ( I &&$ ) ; P r egna nc y pa 11 a ini s and foetal, saivageo Obet# R %noe. 1 » 610,
Bcofct* » lilsloy» R * â Thomson» (1050);A pBychoiogiqai investigation af prlmigraviclae* Maternai social class» âge» physique ami .Intelligence, J* Ohstot* Gynaec, Br# Emp# 6 5 » 338#
Shapiro $ 8 # » Jones» E#W# & Bons en» P #M# (1902): A.life table of pregnancy terminations and correlates of fetal loss# Miiihank. Mem. Fond# Quart# 40:7» 145.
Shearman# li.P# ( 1959): Borne aspects of the urinaryexcretion of pregnanocUol in pregnancy. J# Ohstet. aynaec. Br# Emp# 6 6 » I.
Short» R.V# (1062)5 Steroids In the follicular fluid and the corpus luteum of the mare. A. * two-cell type * theory of ovarian steroid oynthesis, j* Endocr. 24» 59.
Short» R#V. (1906)5 Comparative Endocrinology of Early Gestation. In Foetal Homeostasis Vol II# od. Ralph M. Wynn# The Wetv York Academy of
/ sclcncos. Nov/ York.
Short# R.V* and Mocro$ M.W. ( 1950) g Progesterone inblood. V. Progesterone and 2 0 a hydroxypregn-4-on- 5-one in the placenta and blood of er/os. J.Endocr* 19» 288.
rt» R.V* end London# t W O U : OorootlvoBiosynthetyls yf Ovarian Steroid# in the stein^ LcjventhaX Syndrome# Brit, mod * J, Io 1724®
5, * Ù -0 « îSÿ’i p
Sulphate for Entrog SyntîToi^voandro estera nodll ring human
rrognancy. Sfceroltls 2 » 713 «
SiiWri# P.K* and MocUonaXd# F#C#Eatregen Bioaynthoals dwing human pregnancy.J. Clin, a # 4'Vf e t CUil e Z 6 a T l> Î «
r.a Pion# Ro &^964}$ Neutral Steroids and
Slmmor# Eaetocllng#nignam» %V*J.Steroid SluXfatoo In Human Pregnancy: I =Identification of Dchydrooplandrootorone Sulfato In Kotal Blood and Quuntificatioa of thin Hormone In Cord Arterial# Cord Vonoue and Maternal Peripheral blood In Normal Frognanelos at Term# 8toroids 4. #8*
Smith# 0 # and Smith# 0 . ( 18 3 6)% Comparatively low levels of ocf9trin In casos of cliorlo opitholiomamid hydatidiform mole. Proa. Soc. oxp. Biol. (N,Y$)
Solomon# s. Cî960)s in fho placenta and fotal membraneo p 200. tM* Ce A* yillm» Baltimore» Maryland# willlame Û ,Wilkins#
Solomon) S# g Lanman » J@T# » Lind# J . h Lieborman ». 8 ,(I05B); the bloeyntlieeie of A'^^^androetonodlona and 17a, bydroxypro^estorone from p*'ogooterone 3)y surviving human fetal adrenals, J. blol. Chom.235» 1084,
Solomon » S, p Bird# C.E,, Wlioon# II,» Wlqvlst# N* &Hiciîfaiuay p K, ( 1060} : Progeotorono mot aboi lornIn the fatal«‘pXao0ntnl unit#' Proeeedingo of the Second Xntornational Oongrcoa of Bndocrinology» Series Mo, 83» Exeerpta Modioa Foundation p 72t#
Solomon# So# Bird» G,E,» Ling# w, » Ivmmlyap M, &Youngp PsC9We C Î067)s Formation and M etaba1iam of 3 tore .Wo in Potuo and Plaoente# Reeent Prog, norm® flea. 23» 207*
Bommervillo# I#F* and Marrian# G.F# (1050)$ Urinary excretion of pregnanodiol in human oubjocte following the adminletration of progostorone and of pregn ane-Sok: 20a, dial I, 8 loch am, J, 40# 285,

Speert» H# (11)54); Pregnancy Prognosis fol.iow.ingrepoa t eel Abortion. Am * J. Oba te t @ Gynec * 08» 6 65 @
S t a 1 i vm r thy# J* (10 5 5) : I ri B r i t i b ti o b a t e t r i c &Gynaecological Practice Vol I® EU* Holland 'U o u ra e @ ii e i a o m a n ®
8torn3 FUi© (10 67); 7 method for the determination,of 6p-™pregaane-So # 17a,»20c. trio 1 in urino#Jo Endoor® 10» 180*
Stevenson» A*c* » Dudgeon» and McClure» H.I, (1959);ObaervatioftD on the résulta of pregnancies of women resident in Belfast# II. Abortions » hyd a t X ci 1 fo riu mo I o s an d e c to p 1 c pr eg n an cle s ©A an * hum © Genet® 23 » 31) S •
Stitch# 5 oR« 9 Lovoll» M.J.» oakey# R#E, and Scott» J.s.(1006)? Excretion of pregnonetriol In a case of hydatid1form mole associated with theea luteincysts » L ancot 1 » 1344 ®
Strott » C»A* ami Lipsett » .M*B ® {î968 ) s Measurement ofI'/oJI.ydroxyprogesterone in Human Plasma * J# C l i n .
E n a o c r ® M e t a b . 2 8 » H 2 0 *
fiotoe» 0,» Guttmacher» A.F. â Rubin» 8, ( 1950):Unintentional abortion in 1497 planned prognancios,J # Am# mod# A® 8 # 142» 1340#
Tiotise» 0# and Martin# C#E# (1957}$ Foetai deaths# spontaneous and itidacoci in tho urban white population of the United States# Popai* stud#11# 170#
Troen# P* (1961): Perfusion Studies of the HumanPlacenta: II - Metaboiism of c^*-i7p estradiol with ami without added Human Chorionic Gonadotrophin# J# Ciiti# Endocr# Metah* 21# 096#
fuisky# A#S# and Koff# A#K# (1967)$ Some observations on the role of the corpus luteum in early human pregnancy# Fertil# Sterii# 8# 116#
Turnbull# E#P#M# and Walker# J# (1960)$ Outcome of Pregnancy complicated by threatened al^ortion#J# OhBtet# Gynaac# Br# Emp# 63# 663#
Yon der Molen# 1i#J# ( 1903)$ Determination of plasma progesterone during pregnancy# Clinics Chim#Acta a# 943#
V m êo wicïio» kaily» w#â#»Laragh® ùïiû Lieberman# S* ( 1DOO); TheBecrotian rate of progeotorono nnû aléeeteroae in normal and abnormal pregnancy* Advonco abstracts of short Gommnnlostlona prooontod at the First International CongpoQo of Endocrinology p 15D» Copenhagen^ Porlodlea*
Venning» E.H. and Browne# JoS.L* (1038): Isolationof a T7 a t e r - a o 1 ubl e fregnancdiol cojnpIoK from human pregnancy urine* Froe# Soc# oxp, Biol,Med# 34» 702,
Vunning# Henry# J#0* & Brovmu# 3,8,1* (1037);The moaauromont of a prognanocliol complex inlimiuin ÜB'’lne® €arto Med# Ao b, J® 36» 03,
Venning# E,H, and Browne# J*$,L* {1040); A Studyof the laetaboiism of crystalline progestérone,E nc! o c I' I n 01 o gy 2 7 » 70 7 #
V111 ee p C oA # and horing » J#M » Cl©63 ) â 2Do, hydro%y a toroid dehydrogenase and 3o,«"hydro%y otorold dohydrogouasG In the human foetal liver* Eatlacrinology 72 » 324*
Walkor# J# {î965)S' in Free# Initiation of Labor Oonferonca# -U#$# Dopt, of iloalth Education and Ifoifare#
Warburton# D, and Fraser# F.G* (1959): GeneticAspects of Abortion* Clin, OOstct# Gyneo, 2# 22*
Warren# J*G* and Oheatum# 3*0* (1964): Demonstrationof a steroid 17-20 desmoiase in human placenta* üan# J* Diochem* Physiol* 42» 143*
Warren# J#0* and Timberlake# C*E* (1964): Biosynthesisof Batrogona'in Pragnancys Precnreor Role of Plasma Oehydroisoandroaterone* Ohstot* Gynec* N*Y* 23» #9*
Waist# w*G*# Fujimoto# G#i* and Sandberg# A*A, (19 58): Motaholism of progoaterone-4-0^'* in a post menopausal woman with a biliary fistula*J* Glin* Endocr* Metah* 18# 972*
Vfaliky# t and Engel# L.L, (1003)$ Mctaholism of progcaterone-4-G^* and pregitenolone-7a-îl® by human adrenal tissue* J* Bid* Chom* 238» 1302*

Werhin» H*» Plotz# J.» Leroy» G.V. & Davis» E.M. (1957); Cholesterol: A precursor of Estrone in vivo.J . Am* Ghem. 8oc # 79» 1012*
Westin^ B.» Nybert» R* & Enhornlng» 0* (1958); Atechnique for perfusion of the proviable human foetus * Acta paediat* Btoelch* 47 » 359.
Whelptoa » P *K* and Kiser» C.V# (1948): Social andPsychological factors affecting fertility*Ml 1II)ank. Mem* Fund, Quart. 182.
Whitehouae» II* (1029): Habitual Abortion.Proc• R * 8oc. Med. 23» 241*
WiXioclcs» J.» Donald » I * » Campbell » S * & Duns mo re» I*R#(1967): Intrauterine growth assessed byultrasonic foetal cephalometry* J* Obstet. Gynaec. Br* Commonw* 74» 639*
iVray» P.M. and Russell» C.S* (19 63): The Urinaryoestriol in normal pregnancy * J * Obstet*Oynaec * Dr* Commonw* 70» 4.

Yego# M.#.# O0rfttmrit & Fo*pehlelIl#Ef <1907)5 ' NA0lHi InîiibitlQn auû in vitro Effect of Oonadotï'Ophiiüis On the cholestcroi »idc-ohain- ci caving Bn5s,ymc Bystem in Bovine Corpora Lotea#
Biochem# m$ 374.
Voitiimi» T*# Strott# C.A., MmreWii# J.R* ê tipectt#II.B* (10(10)5 Oorpn» tntcnm function in Early Pregnancy. t. Clin# Endocr. MetaO. 20. 220#
Zander# J.* (1058)5' ^toroids in the Human Ovary.J. Biol# Ghcm. 252# 117.
Zander# j# <106l)s' Eclationghip Between progesterone production in the human placenta and the foetus.In Progesterone and the Defence Mechanism of Pregnancy, ed# O.E.if. wolstenholme & M.P. Cameron# d. & A# Churchill# London. ^ p 52#
Zander# J, <1964)5 Progesterone and its aetaholitos in the placental«*foetal unit. Excerpts Med. (Internat. Cong, ser#) 85# 715*
Zander# ,1* and von Munstermann# A.M. < 1950) ; Progesterone in human Blood and tissues* III# Progesterone in plaçante# uterine mucosa and amniotic fluid# Klin# nschr# 34# 944*

Zander# J## Porhea# T.%«# von liunstemane# A#M# &Weher# E# I‘î95t)î ^3*^KeWprognen0**3O&*'Ol and A’^^S«*Eetoprogneii0**20p«0l# two naturally occurring metaBelItem of prcgcatarona# isolation# Idcntifleatlon# Biological activity and concentration in human tissuea. 3* Clin#Enclocr# MotaB# IS# 337#
Zander# J## fliljaacn# *7# & von Munatormann# A.m. ( I003)i Isolation and identification of i€m hydroxy-*» progesterone from human corpora lutea and placental Blood# 3# Olin# iïuîocr# Met ah# 22# #01,
Zondek# B# and ÛnldOcrg# S# (1957)$ ' PlacentalFunction and Foetal Death# J# OBstet# % m w c , ir# Bmp# 64# I#
PuBlleatlong
Î. Some oBaervatlons on the excretion of pregnanediolin the urine of women with a had ohstetric history# (1960)# Advance Ahstract# 1st# International Congress of Endocrinology# Copenhagen#
2# Pregnancy following abortion# (1961)#J# Ohstot# Oynaec* hr* Commonw# 68# 789#
3# Urinary steroids in Spontaneous abortion# (1962)#Acta endoer# Copnh# guppl# 67, 124#
4# The Prohahiiity of Recurrent Abortion # (1964)#J# Ohstet# Cynaee# Br# Commonw# 71# 784#
5# Urinary excretion of oestrogen and pregnanedioi inhydatidiform mole# (1966)# J# Ohstet# Gynaec* Br# Commonw# 72# 249*
6# Some aspects of progesterone metaholism in humanpregnancy# (1965)# (with M# Oreig)# J# Reprod# Fertll# 10# 219#
7# The conversion of progesterone to prognanodlol in human pregnancy # (1965)* (with M. Graig).J# Ohstet* Gynaee# Br* Commeaw* 72# 1029*
a* Urinary oestrogen.and pregnanodiol excretion in recurrent abortion # (1966)* J* Ohstet.Gynaec# Br* Commonw* 73# 290*
9* Radioactive metabolites in the liver and adrenalsof the human foetus after administration of
PjP0g 0gt;erone# ( 1967)* (with M# Oreig)*J* Kndocr* 39# 157*
10* ateroidogenosis in a case of hydatidiform mole (1969), (with J*Il*T* Coutts# P*E* E 0 SS a J# Walker). J# Endoer* 44# 555*
11* Some aspects of gonadotrophin therapy# (1970), Proc* R* 8oc* Med* - in press*
Related Documents











