Essential Revision Notes in Paediatrics for the MRCPCH Second edition

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Essential Revision Notes
in Paediatrics
for theMRCPCH
Secondedition

Contents
Contributors vii
Preface to the Second edition xi
Preface to the First edition xii
1. Cardiology 1Robert Tulloh
2. Child Development, Child Psychiatry and Community Paediatrics 65Joanne Philpot and Ruth Charlton
3. Clinical Governance 131Robert Wheeler
4. Clinical Pharmacology and Toxicology 143Steve Tomlin and Michael Capra
5. Dermatology 163Helen M Goodyear
6. Emergency Paediatrics 195Serena Cottrell
7. Endocrinology 229Heather Mitchell and Vasanta Nanduri
8. Ethics and Law 281Vic Larcher and Robert Wheeler
9. Gastroenterology and Nutrition 307R M Beattie
10. Genetics 353Louise Wilson
11. Haematology and Oncology 379Michael Capra
12. Hepatology 427Nancy Tan and Anil Dhawan
v
13. Immunology 469Waseem Qasim and Bobby Gaspar
14. Infectious Diseases 497Katy Fidler, Nigel Klein and Karyn Moshal
15. Metabolic Medicine 559Michael P Champion
16. Neonatology 601Grenville F Fox
17. Nephrology 659Christopher J D Reid
18. Neurology 711Neil H Thomas
19. Ophthalmology 769William H Moore and Ken K Nischal
20. Orthopaedics 821Vel K Sakthivel and N M P Clarke
21. Respiratory 843Jane C Davies
22. Rheumatology 889Nathan Hasson
23. Statistics 919Angie Wade
24. Surgery 937Merrill McHoney, Vivien McNamara and Robert Wheeler
Picture permissions 975
Index 977
vi
Contents
Chapter 1
CardiologyRobert Tulloh
CONTENTS
1. Diagnosis of congenital heart disease 51.1 Fetal cardiology1.2 Epidemiology1.3 Cardiac anatomy1.4 Nomenclature for sequential segmental arrangement1.5 Examination technique1.6 Innocent murmurs
2. Basic cardiac physiology 152.1 Physiology of adaptation to extrauterine life2.2 Physiology of congenital heart disease2.3 Physiology of heart muscle and heart rate
3. Left to right shunt 173.1 Atrial septal defect (ASD)3.2 Ventricular septal defect (VSD)3.3 Persistent ductus arteriosus (PDA)3.4 Aortopulmonary window3.5 Others
4. Right to left shunt 224.1 Tetralogy of Fallot4.2 Transposition of the great arteries4.3 Pulmonary atresia4.4 Ebstein anomaly4.5 Eisenmenger
5. Mixed shunt 265.1 Complete atrioventricular septal defects5.2 Tricuspid atresia5.3 Others
1
6. Obstruction in the well child 286.1 Aortic stenosis6.2 Pulmonary stenosis6.3 Adult-type coarctation of the aorta6.4 Vascular rings and slings
7. Obstruction in the sick newborn 307.1 Coarctation of the aorta7.2 Hypoplastic left heart syndrome7.3 Critical aortic stenosis7.4 Interruption of the aortic arch7.5 Total anomalous pulmonary venous connection
8. Non-bypass surgery for congenital heart disease 358.1 Shunt operation8.2 Coarctation of the aorta repair8.3 Pulmonary artery band8.4 Arterial duct ligation
9. Bypass surgery for congenital heart disease 369.1 Switch operation9.2 Fontan9.3 Norwood9.4 Rastelli9.5 Other operations
10. Syndromes in congenital heart disease 3810.1 Isomerism10.2 Trisomy10.3 William syndrome10.4 Noonan syndrome10.5 Di George syndrome10.6 Alagille syndrome10.7 Turner syndrome10.8 VACTERL10.9 Holt–Oram/Thrombocytopenia and Absent Radius (TAR)/Fanconi syndromes10.10 CHARGE10.11 Pentalogy of Cantrell10.12 Dextrocardia10.13 Other syndromes
11. Syncope in childhood 44
12. Pulmonary hypertension 4512.1 Persistent pulmonary hypertension of the newborn12.2 Increased pulmonary blood flow12.3 Chronic hypoxia12.4 Pulmonary venous hypertension
2
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
13. Drug therapy for congenital heart disease 4813.1 Heart failure13.2 Anticoagulation13.3 Pulmonary hypertension13.4 Antiarrhythmia
14. Acquired heart disease 4914.1 Kawasaki disease14.2 Dilated cardiomyopathy14.3 Hypertrophic cardiomyopathy14.4 Suspected bacterial endocarditis14.5 Rheumatic fever14.6 Pericarditis
15. ECG 5515.1 The ECG and how to read it15.2 Tachycardias15.3 Bradycardias
16. Chest X-rays 6016.1 Cardiac outlines
17. Cardiac catheterization 6117.1 Diagnostic cardiac catheterization17.2 Interventional cardiac catheterization
18. Imaging 6318.1 Echocardiography18.2 Magnetic resonance imaging18.3 Positron emission tomography18.4 Radionuclear angiography
19. Further reading 63
3
Cardiology

Cardiology
1. DIAGNOSIS OF CONGENITAL HEART DISEASE
1.1 Fetal cardiology
Diagnosis
In the south of England, most children (. 70%) who require infant surgery for congenitalheart disease (CHD) are diagnosed during pregnancy at 16–20 weeks’ gestation. This givesa significant advantage to the parents who are counselled by specialists who can give arealistic guide to the prognosis and treatment options. A few undergo termination ofpregnancy (depending on the diagnosis). Most continue with the pregnancy and can beoffered delivery within the cardiac centre if there could be neonatal complications or iftreatment is likely to be needed within the first 2 days of life. Surgical intervention duringfetal life is not yet routinely available.
Screening (by a fetal cardiologist) is offered to those with:
• Abnormal four-chamber view on routine-booking, antenatal-anomaly ultrasound scan• Increased nuchal translucency (thickness at back of the neck), which also increases the
risk of Down syndrome• Previous child with or other family history of CHD• Maternal risk factors, such as phenylketonuria or diabetes• Suspected Down, or other, syndrome
Important normal findings on fetal echocardiography include echodensities:
• Used to be called ‘Golf-balls’• Found on anterior mitral valve papillary muscle• Thought to be calcification during development• No importance for CHD• Positive association with Down syndrome• Do not need echocardiogram after delivery
Arrhythmias
• Diagnosed at any time during pregnancy: an echocardiogram is required to confirmnormal anatomy and to confirm type of arrhythmia. Fetal electrocardiogram (ECG) is notyet a routine investigation
• Multiple atrial ectopics are usually not treated• Supraventricular tachycardia is usually treated with maternal digoxin or flecainide
5
• Heart block may be treated with maternal isoprenaline or salbutamol• Presence of hydrops is a poor prognostic sign
1.2 Epidemiology of congenital heart disease
Eight per 1,000 live births have CHD, of which the commonest are:
• Ventricular septal defect 30%• Persistent arterial duct 12%• Atrial septal defect 7%• Pulmonary stenosis 7%• Aortic stenosis 5%• Coarctation of the aorta 5%• Tetralogy of Fallot 5%• Transposition of the great arteries 5%• Atrioventricular septal defect 2%
Incidence is increased by a positive family history, so the proportion of live births with CHDwill be:
• Previous sibling with CHD 2%• Two siblings with CHD 4%• Father with CHD 3%• Mother with CHD 6%
Incidence also increased by
• Presence of other anomaly or syndrome• Parents with an abnormal genotype• Maternal ingestion of lithium (Ebstein anomaly)• Third-trimester enterovirus or coxsackievirus infection (myocarditis, dilated
cardiomyopathy)• Maternal systemic lupus erythematosus (anti-ro, anti-la antibodies leading to congenital
heart block)
6
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
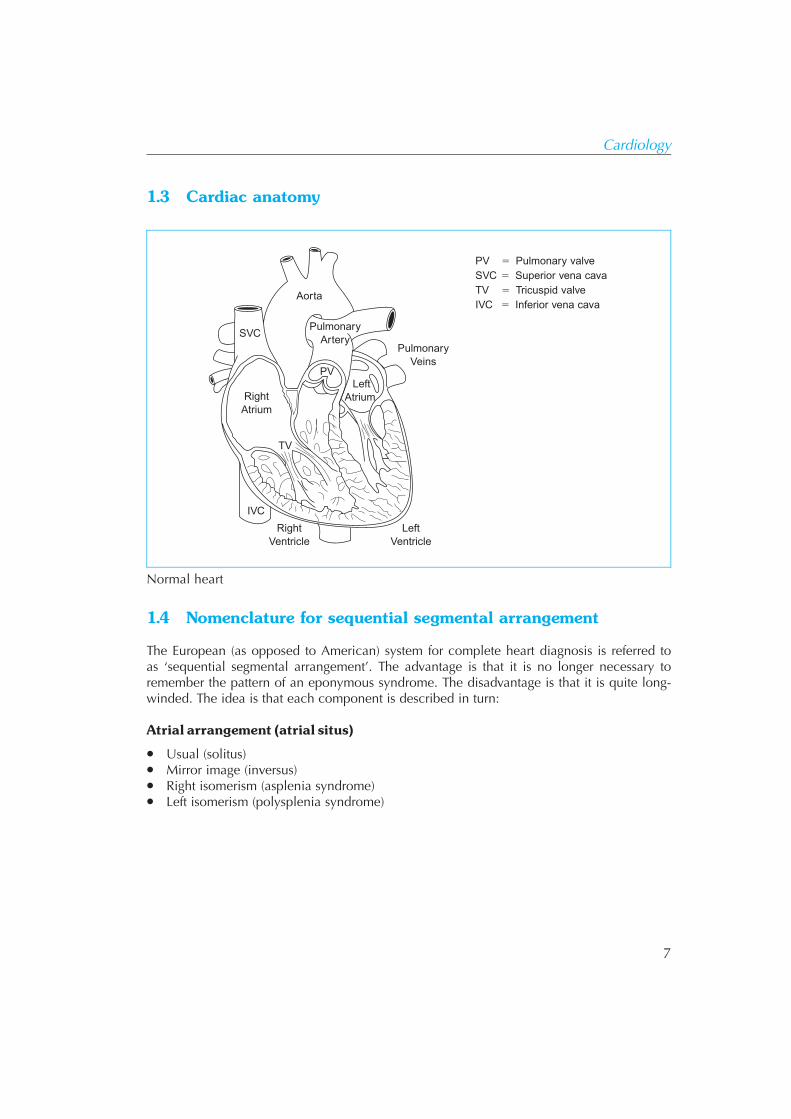
1.3 Cardiac anatomy
Right
Atrium
Left
Atrium
PV
TV
IVC
Right
Ventricle
Left
Ventricle
SVCPulmonary
ArteryPulmonary
Veins
Aorta
PV 5 Pulmonary valve
SVC 5 Superior vena cava
TV 5 Tricuspid valve
IVC 5 Inferior vena cava
Normal heart
1.4 Nomenclature for sequential segmental arrangement
The European (as opposed to American) system for complete heart diagnosis is referred toas ‘sequential segmental arrangement’. The advantage is that it is no longer necessary toremember the pattern of an eponymous syndrome. The disadvantage is that it is quite long-winded. The idea is that each component is described in turn:
Atrial arrangement (atrial situs)
• Usual (solitus)• Mirror image (inversus)• Right isomerism (asplenia syndrome)• Left isomerism (polysplenia syndrome)
7
Cardiology
Atrioventricular (AV) connection
Type of atrioventricular connection
• Biventricular• Concordant• Discordant• Ambiguous (with atrial isomerism)
• Univentricular• Absent left AV connection• Absent right AV connection• Double inlet AV connection
Mode of atrioventricular connection
• Two AV valves• Common AV valve• Straddling right or left AV valve• Imperforate right or left AV valve• Overriding right or left AV valve
Ventricular topology
• Right-hand (normal) or left-hand topology
Ventriculoarterial connection
Type of ventriculoarterial connection
• Concordant• Discordant• Double outlet• Single outlet:
• Common arterial trunk• Solitary arterial trunk• With pulmonary atresia• With aortic atresia
Mode of ventriculoarterial connection
• Two perforate valves• Left or right imperforate valve
Infundibular morphology
Arterial relationships
Associatedmalformations
• Position of heart in the chest — left, right or middle• Systemic and pulmonary veins
8
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
• Atrial septum• Atrioventricular valves• Ventricular septum• Semilunar valves• Anomalies of great arteries (e.g. double aortic arch)
Surgical or interventional procedures
Acquired or iatrogenic lesions
1.5 Examination technique
To many candidates the diagnosis of congenital heart disease is daunting. Certainly, if thecandidate examines the child, listens to the heart and then tries to make a diagnosis, thiswill prove difficult. The following system should be used instead.
History
The history-taking is short and to the point. The candidate needs to know:
• Was the child born preterm?• Are there any cardiac symptoms of:
• Heart failure (breathlessness, poor feeding, faltering growth, cold handsand feet)
• Cyanosis• Neonatal collapse
• Is it an asymptomatic heart murmur found on routine examination?• Is there a syndrome such as Down syndrome?• Is there any family history of congenital heart disease?• Did the mother have any illnesses or take any medication during pregnancy?
Examination
• Introduce yourself to mother and patient. Ask if you can examine the child.• Position child according to age:
• For a 6-year-old — at an angle of 45 degrees• For a toddler — upright on mother’s knee• For a baby — flat on the bed
• Remove clothes from chest• Stand back and look for:
• Dysmorphism• Intravenous infusion cannula• Obvious cyanosis or scars
The following examinations sbould be performed.
9
Cardiology
Heart failure
The delivery of oxygen to the peripheral vascular bed is insufficient to meet the metabolicdemands of the child. Usually because of left to right shunt with good heart pump function.
• A thin, malnourished child (Faltering growth)• Excessive sweating around the forehead• Tachycardia• Breathlessness +/– subcostal or intercostal recession• Poor peripheral perfusion with cold hands and feet• A large liver• Never found with ventricular septal defect (VSD) or other left to right shunt in first week
of life• An emergency if found up to 7 days of age. Implies a duct-dependent lesion, e.g.
hypoplastic left heart syndrome or coarctation
Cyanosis
• Mild cyanosis is not visible — use the pulse oximeter
Clubbing
• Visible after 6 months old• First apparent in the thumbs or toes• Best demonstrated by holding thumbs together, back to back to demonstrate loss of
normal nail-bed curvature• Disappears a few years after corrective surgery
Pulse
• Rate (count for 6 seconds 3 10)• Rhythm (only ‘regular’ or ‘irregular’, need ECG for ‘sinus rhythm’)• Character at the antecubital fossa with the elbows straight, using the thumbs — on both
arms together
Head and neck
• Anaemia — for older children only — ask the patient to look up and examine theconjunctivae (not appropriate in a baby)
• Cyanosis — the tongue should be examined for central cyanosis. If in doubt ask thechild to stick out their tongue and ask the mother to do the same. This will detectoxygen saturations of , 85%
• Jugular venous pressure — the head is turned towards the candidate so that the otherside of the neck (the left side) can be seen with the jugular venous pressure visible,outlined against the pillows. In a child who is under 4 years, the jugular venous pressureshould not be assessed
• Carotid thrill — essential part of the examination, midway up the left side of the neck,felt with the thumb, proof of the presence of aortic stenosis
10
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
Precordium
Inspection
• Respiratory rate• Median sternotomy scar (¼ open heart surgery — see Section 9)• Lateral thoracotomy scar (Blalock–Taussig (BT) shunt, patent ductus arteriosus (PDA)
ligation, pulmonary artery (PA) band, coarctation repair)• Additional scars, e.g. on the abdomen
Palpation
• Apex beat ‘the most inferior and lateral position where the index finger is lifted by theimpulse of the heart’. Place fingers along the fifth intercostal space of both sides of chest(for dextrocardia) and count down apex position only if patient is lying at 45 degrees
• Left ventricular heave• Right ventricular heave at the left parasternal border• Thrills at upper or lower left sternal edge
Auscultation
• Heart sounds and their character• Additional sounds• Murmurs, their character, intensity and where they are best heard
Heart sounds
First heart sound is created by closure of the mitral and then tricuspid valves. It is notimportant for the candidate to comment on the nature of the first heart sound.
Second heart sound, however, is more important, created by closure of first the aortic andthen the pulmonary valves.
• Loud pulmonary sound — pulmonary hypertension• Fixed splitting of second sound (usually with inspiration the sounds separate and then
come together during expiration). Listen when patient is sitting up, at the mid-left sternaledge in expiration• Atrial septal defect• Right bundle-branch block
• Single second sound in transposition of great arteries (TGA), pulmonary atresia, orhypoplastic left heart syndrome
• Quiet second sound may occur in pulmonary valve stenosis or pulmonary artery band
Additional soundsAdded sounds present may be a normal third or fourth heart sound heard in the neonate orthese sounds can be pathological, for example in a 4-year-old with a dilated cardiomyo-pathy and heart failure. An ejection click is heard at aortic valve opening, after the firstheart sound, and is caused by a bicuspid aortic valve in most cases.
11
Cardiology

Murmurs
Before listening for any murmurs, the candidate should have a good idea of the type ofcongenital heart disease, which is being dealt with. The candidate should know whetherthe child is blue (and therefore likely to have tetralogy of Fallot) or is breathless (likely tohave a left to right shunt) or has no positive physical findings before auscultation of themurmurs (and therefore more likely to either be normal, have a small left to right shunt ormild obstruction). By the time the murmurs are auscultated, there should only be two orthree diseases to choose between, with the stethoscope being used to perform the finetuning. It is best to start at the apex with the bell, and move to the lower left sternal edgewith the diaphragm. Then on to the upper left sternal edge and upper right sternal edgeboth with the diaphragm. Additional areas can be auscultated, but provide little additionalinformation. Murmurs are graded out of 6 for systolic, 1 ¼ very soft, 2 ¼ soft, 3 ¼ moderate,4 ¼ loud with a thrill, 5 ¼ heard with a stethoscope off the chest, 6 ¼ heard as you enterthe room. Murmurs are out of 4 for diastolic, again 2, 3 and 4.
Ejection systolic murmurUpper sternal edge — implies outflow tract obstruction. Right or left ventricular outflowtract obstruction can occur at valvar (+ ejection click), subvalvar or supravalvar level.
• Upper right sternal edge (carotid thrill) ¼ Aortic stenosis• Upper left sternal edge (no carotid thrill) ¼ Pulmonary stenosis or atrial
septal defect (ASD)• Mid/lower left sternal edge ¼ Innocent murmur (see below)• Long harsh systolic murmur + cyanosis ¼ Tetralogy of Fallot
Pansystolic murmur
• Left lower sternal edge (+/– thrill ) ¼ VSD• Apex (much less common) ¼ Mitral regurgitation• Rare at left lower sternal edge (+/– cyanosis) ¼ Tricuspid regurgitation
(Ebstein anomaly)
Continuous murmur
• Left infraclavicular (+/– collapsing pulse) ¼ Persistent arterial duct• Infraclavicular (+ cyanosis + lateral thoracotomy) ¼ BT shunt• Any site (lungs, shoulder, head, hind-quarter) ¼ Arteriovenous fistula
Diastolic murmurs
• Unusual in childhood• Left sternal edge/apex (+/– carotid thrill or VSD) ¼ Aortic regurgitation• Median sternotomy (+/– PS (pulmonary stenosis) murmur)
¼ Tetralogy of Fallot, repaired• Apical (+/– VSD) ¼ Mitral flow/(rarely stenosis)
NB Listening to the back gives little diagnostic information, but is useful thinking time.
12
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
Presentation of ¢ndings
Few candidates pay enough attention to the case presentation. This should be done after theexamination is complete. The candidate should stand, look the examiner in the eye, puthands behind his/her back and present. The important positives and negatives should bestated quickly and succinctly with no ‘umms’ or ‘errrs’. It is important to judge the mood ofthe examiner, if he/she is looking bored, then go faster. Practise with a tape recorder orvideo-recording.
To complete the examination you would:
• Measure the blood pressure• Measure the oxygen saturation• Feel the femoral pulses• Feel the liver edge
The presentation should be rounded off with the phrase ‘the findings are consistent with thediagnosis of . . .’.
13
Cardiology
Patient
Cyanosed Acyanosed
Femoral Pulses
No YesCoarctation
No other pulses
Critical Aortic StenosisHLHS
Absent Left CarotidInterrupted Aortic Arch
YesCarotid thrill AS
No
Apex in left chestNoYes
YesPrecordial thrill VSD or PS
No
Murmur
Yes No Normal Heart
?Kartagener with
normal heart
?Abnormal heart
Murmur
Yes No
Fallot TGA VSD
Mitral regurgitation
(AVSD is not visibly
cyanosed and may have
apical murmur of left AV
valve regurgitation)
Split S2 ASD
Not split PS
AS 1 Carotid thrill
Valvar AS or PS
Sub- or supra valvar
Pulmonary hypertension
Left
Apex
Left
Right
Loud
PSM Lower S.E.
ESM Upper S.E.
Ejection click
No ejection click
Pulmonary sound
HLHS
L
AS
VSD
PS
TGA
ASD
PSM
ESM
AVSD
AV
hypoplastic left heart syndrome
Left
aortic stenosis
ventricular septal defect
pulmonary stenosis
transposition of great arteries
atrial septal defect
Pan Systolic murmur
ejection systolic murmur
atrioventricular septal defect
atrioventricular
KEY
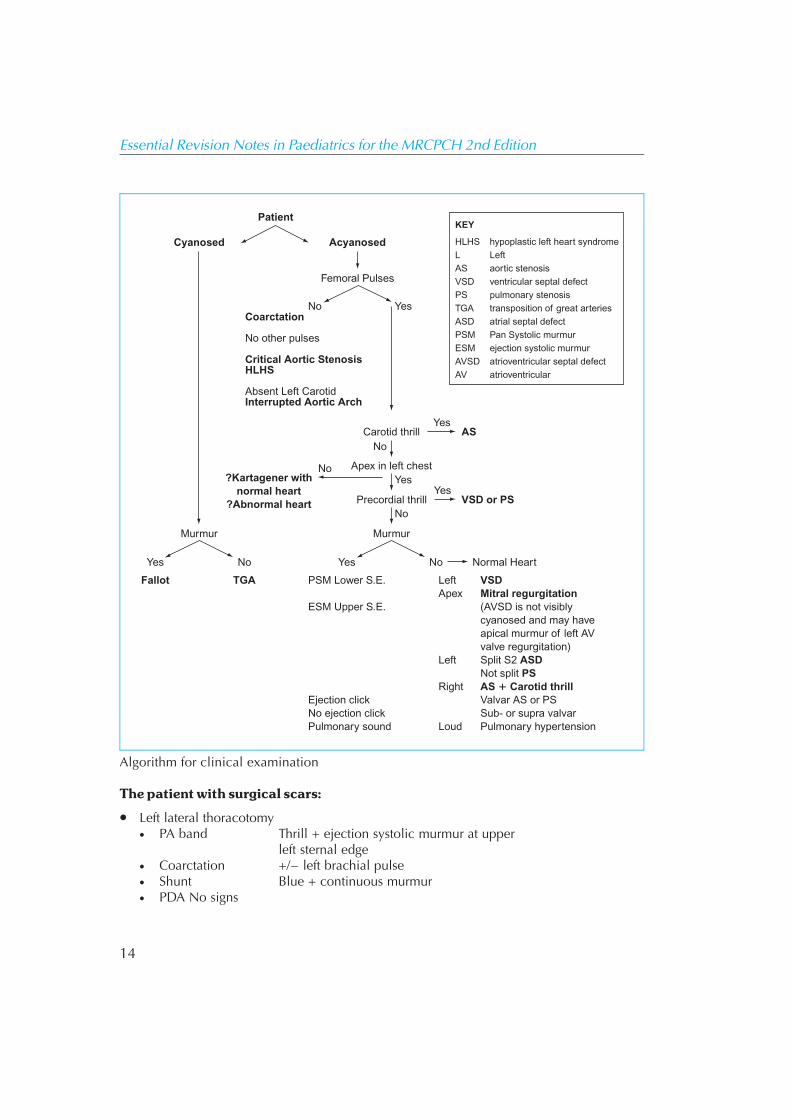
Algorithm for clinical examination
The patient with surgical scars:
• Left lateral thoracotomy• PA band Thrill + ejection systolic murmur at upper
left sternal edge• Coarctation +/– left brachial pulse• Shunt Blue + continuous murmur• PDA No signs
14
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
• Right lateral thoracotomy• Shunt Blue + continuous murmur
• Median sternotomy• Any intracardiac operation
1.6 Innocent murmurs
The commonest murmur heard in children is the functional, innocent or physiological heartmurmur (40% of all children). They are often discovered in children with an intercurrentinfection or with anaemia. These all relate to a structurally normal heart but can cause greatconcern within the family. There are several different types depending on the possible siteof their origin. It is clearly important to make a positive diagnosis of a normal heart. Themurmur should be:
• Soft (no thrill)• Systolic• Short, never pansystolic• ASymptomatic• Left Sternal edge
It may change with posture.
Innocent murmurs do not require antibiotic prophylaxis.
Diastolic murmurs are not innocent.
An innocent murmur is not associated with abnormal or added heart sounds.
Types of innocent murmur include:
• Increased flow across branch pulmonary artery — this is frequently seen in pretermneonates, is a physiological finding and resolves as the pulmonary arteries grow. Themurmur disappears after a few weeks of age, and never causes symptoms
• Still’s murmur — this is vibratory in nature and is found at the mid-left sternal edge. Itmay be caused by turbulence around a muscle band in the left ventricle
• Venous hum — it may be easy to hear the venous blood flow returning to the heart,especially at the upper sternal edge. This characteristically occurs in both systole anddiastole and disappears on lying the child flat
2. BASIC CARDIAC PHYSIOLOGY
2.1 Physiology of adaptation to extrauterine life
During the adaptation from fetal life there are a number of changes in the normal child:
• A fall in the pulmonary vascular resistance, rapidly in the first few breaths, but thiscontinues until 3 months of age
• A resultant fall in the pulmonary arterial pressure• Loss of the placenta from the circulation
15
Cardiology
• Closure of the ductus venosus• Closure of the ductus arteriosus• Closure of the foramen ovale
The arterial duct is kept patent with prostaglandins E1 or E2 infusion in children with duct-dependent circulation such as transposition of the great arteries, or pulmonary atresia.
2.2 Physiology of congenital heart disease
The main principles of congenital heart disease are
• The pressure on the left side of the heart is usually higher than that on the right• Any communication between atria, ventricles or great arteries leads to a left to right
shunt• Pulmonary vascular resistance falls over the first 12 weeks of life, increasing the shunt• There will only be cyanosis if the desaturated blood shunts from the right to left side• Common mixing leads to cyanosis and breathlessness• Duct-dependent conditions usually present at 2 days of life• Prostaglandin E2 or E1 can be used to reopen the duct up to about 2 weeks of life
2.3 Physiology of heart muscle and heart rate
Arterial pulse volume depends on stroke volume and arterial compliance.
• Small pulse volume in• Cardiac failure• Hypovolaemia• Vasoconstriction
• Large pulse volume in• Vasodilatation• Pyrexia• Anaemia• Aortic regurgitation• Hyperthyroid• CO2 retention
• Pulsus paradoxus• Exaggeration of normal rise and fall of blood pressure with respiration, seen in
airways obstruction, such as asthma• Sinus arrhythmia
• Variation of the normal heart rate with respiration. Faster in inspiration and slower inexpiration. Can be very marked in children
Cardiac output is increased by• Adrenergic stimulus• Increased stretch (Starling’s curve)• Increased preload• Reduced afterload
16
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
3. LEFT TO RIGHT SHUNT
(Pink +/– breathless)
General principles
No signs or symptoms on first day of life because of the high pulmonary vascular resistance.Later, at 1 week, infant can develop symptoms and signs of heart failure.
Symptoms of heart failure
• Tachypnoea• Poor feeding, Faltering growth• Cold hands and feet• Sweating• Vomiting
Signs of heart failure
• Thin• Tachypnoea• Displaced apex• Dynamic precordium• Apical diastolic murmur• Hepatomegaly
3.1 Atrial septal defect (ASD)
Types of defect
• Secundum ASD• Primum ASD (partial atrioventricular septal defect)• Sinus venosus ASD• Other
SecundumASD
A defect in the centre of the atrial septum involving the fossa ovalis.
Clinical features
• Asymptomatic• 80% of ASDs• Soft systolic murmur at upper left sternal edge• Fixed split S2 (difficult to hear)
ECG
• Partial right bundle-branch block (90%)• Right ventricle hypertrophy
17
Cardiology
Chest X-ray
• Increased pulmonary vascular markings
Management
• Closure at 3–5 years (ideally)• 90% undergo device closure in catheter laboratory• 10% undergo surgical closure (too large or personal preference)
Partial atrioventricular septal defect (PrimumASD)
A defect in the lower atrial septum, involving the left atrioventricular valve which has threeleaflets and tends to leak.
Clinical features
• Asymptomatic• 10% of ASDs• Soft systolic murmur at upper left sternal edge• Apical pansystolic murmur (atrioventricular valve regurgitation)• Fixed split S2 (difficult to hear)
ECG
• Partial right bundle-branch block (90%)• Right ventricle hypertrophy• Superior axis
Chest X-ray
• Increased pulmonary vascular markings
Management
• Closure at 3–5 years• All require surgical closure (because of the need to repair valve)
Sinus venosus ASD
A defect at the upper end of the atrial septum, such that the superior vena cava (SVC)overrides the atrial septum. The right pulmonary veins are usually anomalous and draindirectly into the SVC or right atrium adding to the left to right shunt.
Clinical features
• Asymptomatic or heart failure• 5% of ASDs• Soft systolic murmur at upper left sternal edge• Fixed split S2 (easily heard)
18
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
ECG
• Partial right bundle-branch block• Right ventricle hypertrophy
Chest X-ray
• Increased pulmonary vascular markings• Cardiomegaly
Management
• Closure at 1–5 years• All require surgical closure and repair to the anomalous pulmonary veins
There are other rare types of ASD, which are similarly treated.
3.2 Ventricular septal defect (VSD)
Small defect
A defect anywhere in the ventricular septum (perimembranous or muscular, can be inlet oroutlet). Restrictive defects are smaller than the aortic valve. There is no pulmonary hyper-tension.
Clinical features
• Asymptomatic (80–90%)• May have a thrill at left lower sternal edge• Loud pansystolic murmur at lower left sternal edge (the louder the murmur, the smaller
the hole)• Quiet P2
ECG
• Normal
Chest X-ray
• Normal
Management
• Review with echocardiography• Spontaneous closure, but may persist to adult life
Large defect
Defects anywhere in the septum. Large defects tend to be the same size or larger than theaortic valve. There is always pulmonary hypertension.
19
Cardiology
Clinical features
• Symptomatic with heart failure after age 1 week• 10–20% of VSDs• Right ventricular heave• Soft or no systolic murmur• Apical mid-diastolic heart murmur• Loud P2
ECG
• Biventricular hypertrophy by 2 months (see Section 15 — ECG)
Chest X-ray
• Increased pulmonary vascular markings• Cardiomegaly
Management
• Initial medical therapy, diuretics +/– captopril + added calories• Surgical closure at 3–5 months
3.3 Persistent ductus arteriosus (PDA)
There is persistence of the duct beyond 1 month after the date the baby should have beenborn.
Clinical features
• Asymptomatic usually, rarely have heart failure• Continuous or systolic murmur at left infraclavicular area
ECG
• Usually normal• If large, have left ventricle volume loading (see Section 15 — ECG)
Chest X-ray
• Usually normal• If large, have increased pulmonary vascular markings
Management
• Closure in cardiac catheter laboratory with coil or plug at 1 year• If large, surgical ligation age 1–3 months
NB The presence of an arterial duct in a preterm baby is not congenital heart disease. Ifthere is a clinical problem, with difficulty getting off the ventilator, or signs of heart failure
20
Essential Revision Notes in Paediatrics for the MRCPCH 2nd Edition
with bounding pulses, the problem is usually treated with indomethacin or ibuprofen(, 34 weeks). If medical management fails, surgical ligation is undertaken.
3.4 Aortopulmonary window
A defect in the wall between the aorta and pulmonary artery.
Clinical features
• Rare• Usually develop heart failure• Continuous murmur as for PDA
ECG
• If large, have left ventricle volume loading (see Section 15 — ECG)
Chest X-ray
• If large, have increased pulmonary vascular markings
Management
• If large, surgical ligation age 1–3 months
3.5 Others
There are other rare causes of significant left to right shunt, such as arteriovenousmalformation. These are all individually rare. Medical and surgical treatment is similar tothat for large ducts or VSDs.
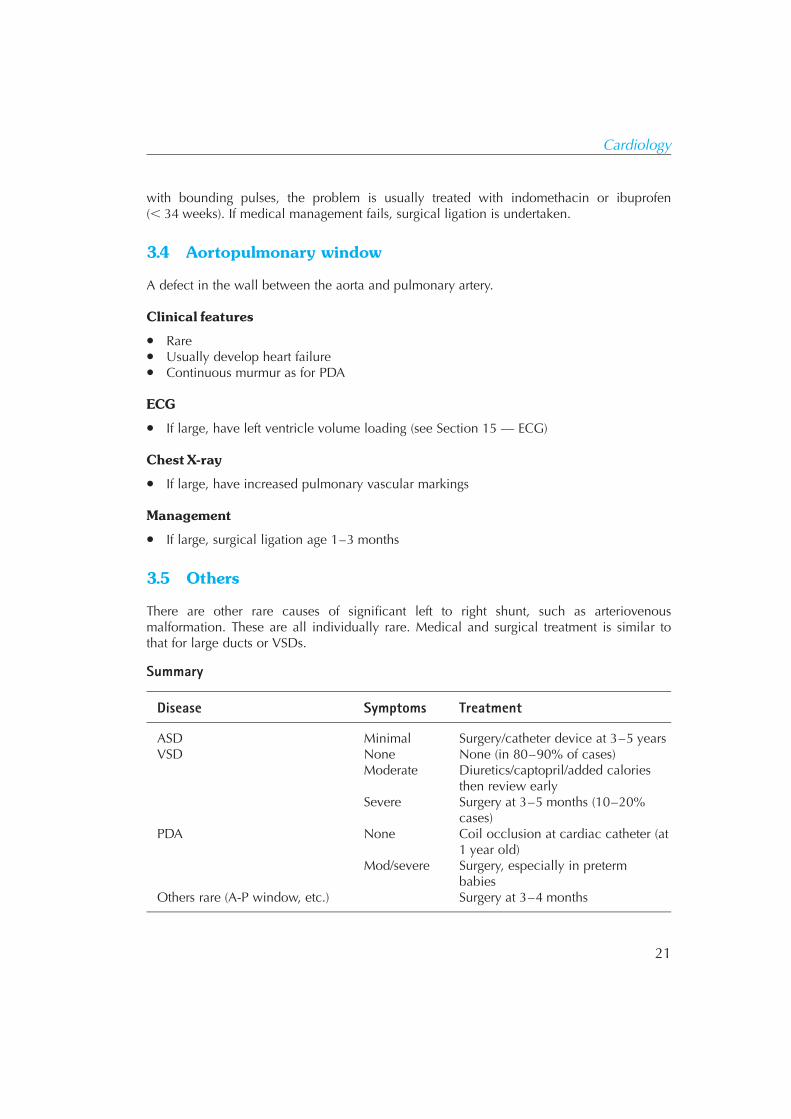
Summary
Disease Symptoms Treatment
ASD Minimal Surgery/catheter device at 3–5 yearsVSD None None (in 80–90% of cases)
Moderate Diuretics/captopril/added caloriesthen review early
Severe Surgery at 3–5 months (10–20%cases)
PDA None Coil occlusion at cardiac catheter (at1 year old)
Mod/severe Surgery, especially in pretermbabies
Others rare (A-P window, etc.) Surgery at 3–4 months
21
Cardiology
Related Documents











