1 Transplantation - Immunosuppression A Case-based Approach January 20, 2009 Paul D. Greig, MD, FRCS(C) Paul D. Greig, MD, FRCS(C) Professor of Surgery Professor of Surgery University of Toronto University of Toronto

1 Transplantation - Immunosuppression A Case-based Approach January 20, 2009 Paul D. Greig, MD, FRCS(C) Professor of Surgery University of Toronto.
Jan 01, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Transplantation - Immunosuppression
A Case-based ApproachJanuary 20, 2009
Paul D. Greig, MD, FRCS(C)Paul D. Greig, MD, FRCS(C)
Professor of SurgeryProfessor of Surgery
University of TorontoUniversity of Toronto
Saint Cosmas & Saint Damian
perform the first transplant
280 CE

Alexis Carrel (1875-1944)
“I have started research into the procedure of vascular
anastomoses in order to be able to transplant certain
organs…” 1901
Sir Peter Medawar (1915-1987)Recognized that lymphocytes were the “immunocompetent cells” that were responsible for rejection – Nobel prize, 1960
Joseph E. Murray, MD
First successful organ transplant: 1954, Brigham Hospital, Boston, Mass.
Kidney transplant between dizygotic twins (recipient
received sub-lethal dose of total body X-radiation)
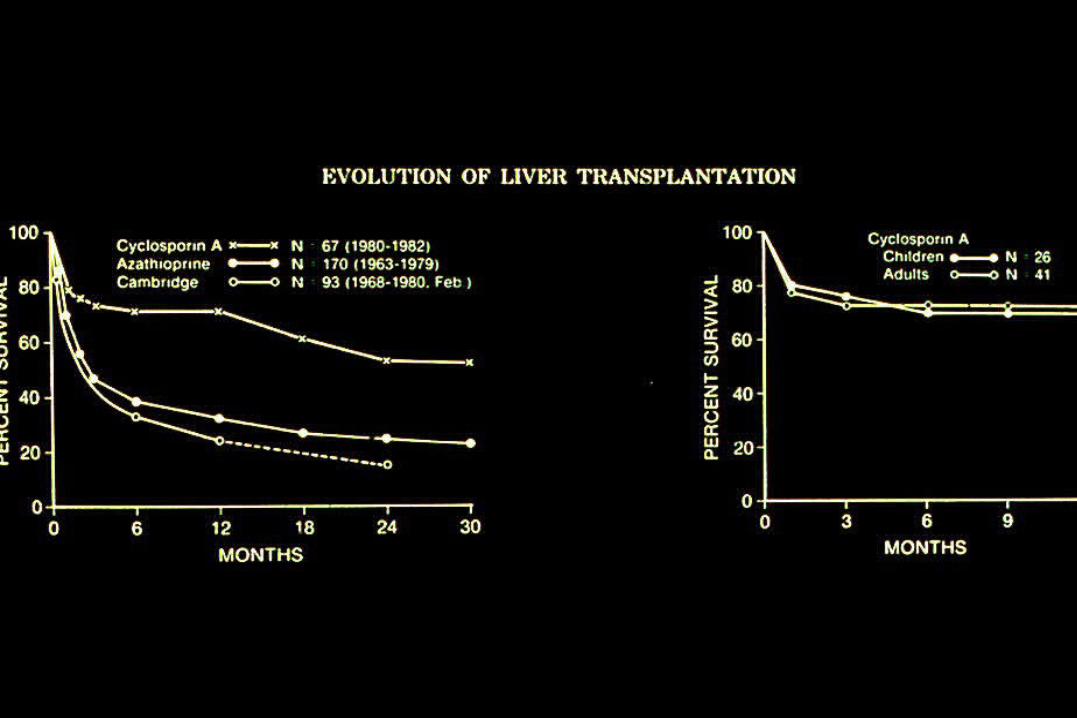
The Pioneers of Liver Transplantation
Sir Roy Calne Thomas E. Starzl, MD
0
20
40
60
80
100
120
140
160
180
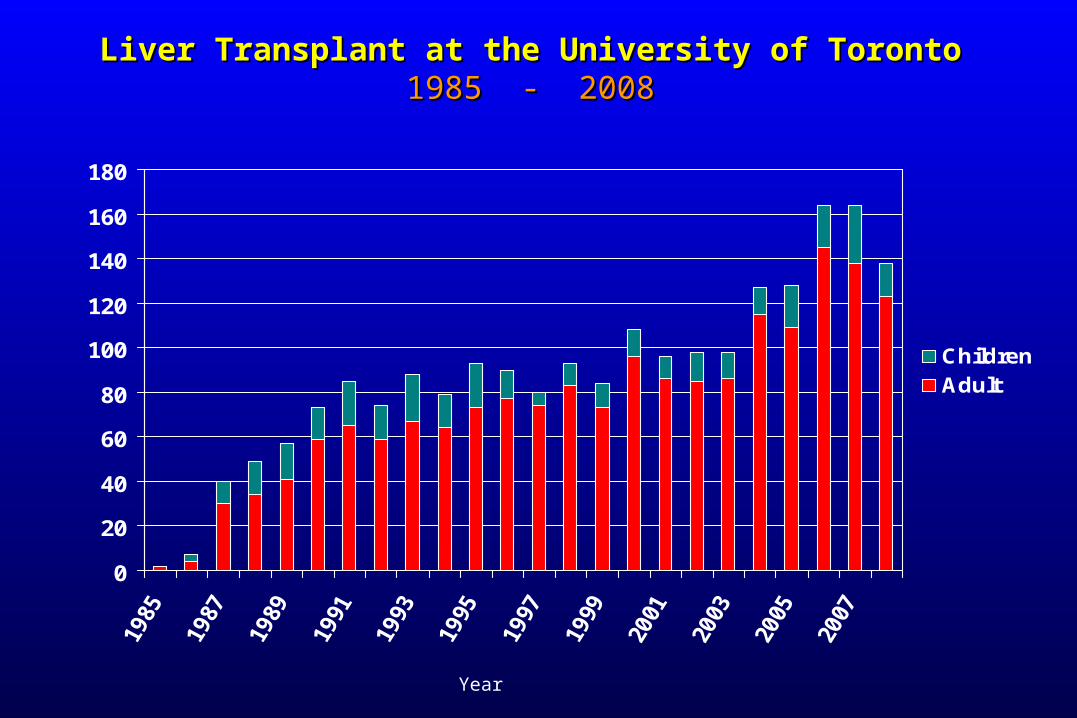
ChildrenAdult
Liver Transplant at the University of TorontoLiver Transplant at the University of Toronto1985 - 20081985 - 2008
Year
11
Transplantation - Immunosuppression
Case 1
• 52 y.o. male– Hepatitis C +ve cirrhosis, ascites (paracentesis q
2-3 weeks)– Liver transplant
• conventional vascular reconstruction• conventional biliary reconstruction: CBD-CBD
– ? Initial postoperative immunosuppression
12
Transplantation - Immunosuppression
Question 1
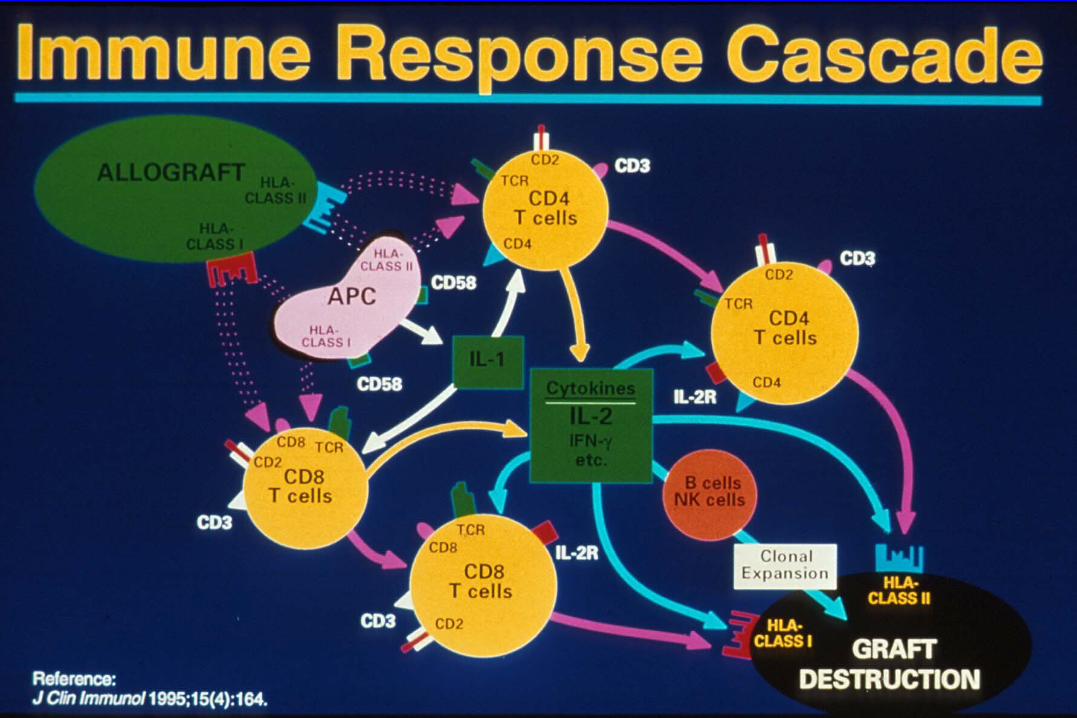
• why is immunosuppression necessary?
• Corollary– what are the immunologic mechanisms of
allograft rejection?• what are the targets of the allo-immune response?• what are the “steps” of this response?

17
Transplantation - Immunosuppression
Question 2a
• what are the immunosuppression options?
• Corollary– what points in the allo-immune response are the targets
of current immunosuppressive drugs?– What are the current (new) immunosuppressive drugs
available?– What is the mechanism of action of each of these
drugs?
Transplantation - Immunosuppression IMMUNOSUPPRESSIVE DRUGS
• Traditional DrugsTraditional Drugs– Steroids– Cyclosporine A– Azathioprine– Anti-lymphocyte
antibodies: • polyclonal or
monoclonal (OKT3)
• Newer DrugsNewer Drugs– Neoral– Tacrolimus– Mycophenolate
Mofetil– Sirolimus– anti- IL2R antibodies


20
Transplantation - Immunosuppression
Question 2b
• what are the toxicities of these immuno-suppression drugs?
• Option– balance the immunosuppressive activity with toxicity
with different combinations– summary of each drug:
Transplantation - Immunosuppression CORTICOSTEROIDS
• Mechanism of action– inhibition of cytokine production by APCs
• Toxicity– infection, poor wound healing,osteoporosis, aseptic necrosis,
hypertension, DM, hyperlipidemia, obesity,cushinoid facies
• Currently– minimize dose, alternate day therapy– early steroid withdrawal
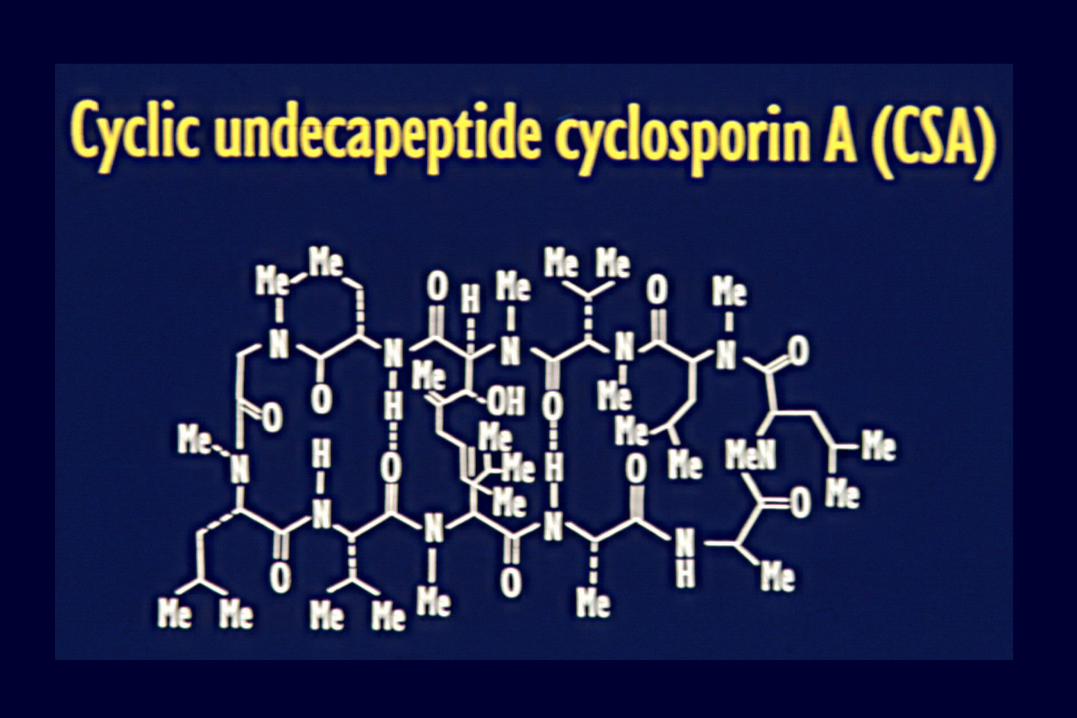
Transplantation - Immunosuppression MICROEMULSION CYCLOSPORINE A
NEORAL• Mechanism of Action
– inhibits calcineurin --> inhibits IL2 production– Microemulsion CsA (NEORAL)
• improved absorption, avoid IV dosing
• Toxicity– Nephotoxicity, hypertension– Neurotoxicity (tremor, headache, direct CNS)– DM, hyperlipidemia, hirsutism, gingival hyperplasia
• Currently– 10 agent
– ? Optimal monitoring using C2 (peak level) not C0 (trough levels)
Transplantation - Immunosuppression TACROLIMUS, formerly FK506 - PROGRAF
• Advantages– lower incidence of acute rejection than CsA?– useful for refractory or chronic rejection– less hyperlipidemia, hirsutism, gingival hypertorphy than CsA
• Toxicity– same as Cyclosporine A, possibly higher incidence– More DM,
• Currently– primary immunotherapy, esp. those at high risk– for steroid resistant or refractory rejection
Transplantation - Immunosuppression AZATHIOPRINE
• Mechanism of action– antimetabolite, inhibits PRPP amidotransterase
• Toxicity– marrow: esp. neutropenia, thrombocytopenia– liver: cholestasis
• Currently– routine “triple therapy”– added to reduce calcineurin inhibitor– added for rejection despite adequate calcineurin inhibitor levels
Transplantation - Immunosuppression MYCOPHENOLATE MOFETIL
CELLCEPT or MYFORTIC
• Advantages– no nephro- or neuro-toxicity– MoA more lymphocyte-specific than azathioprine – reduced acute rejection
• Toxicity– marrow, GI tract
• Currently– primary “triple immunotherapy”– add to CsA or FK monotherapy following rejection or to reduce
dose for CNI toxicity
Transplantation - Immunosuppression Toxicities - in - Common
• Infection– esp. viral and fungal
• Malignancy– all cancers with time
• importance of surveillance
– Lymphoproliferative Disease (LPD)• + Epstein Bar Virus (EBV-LPD)• --> monoclonal LPD --> lymphoma
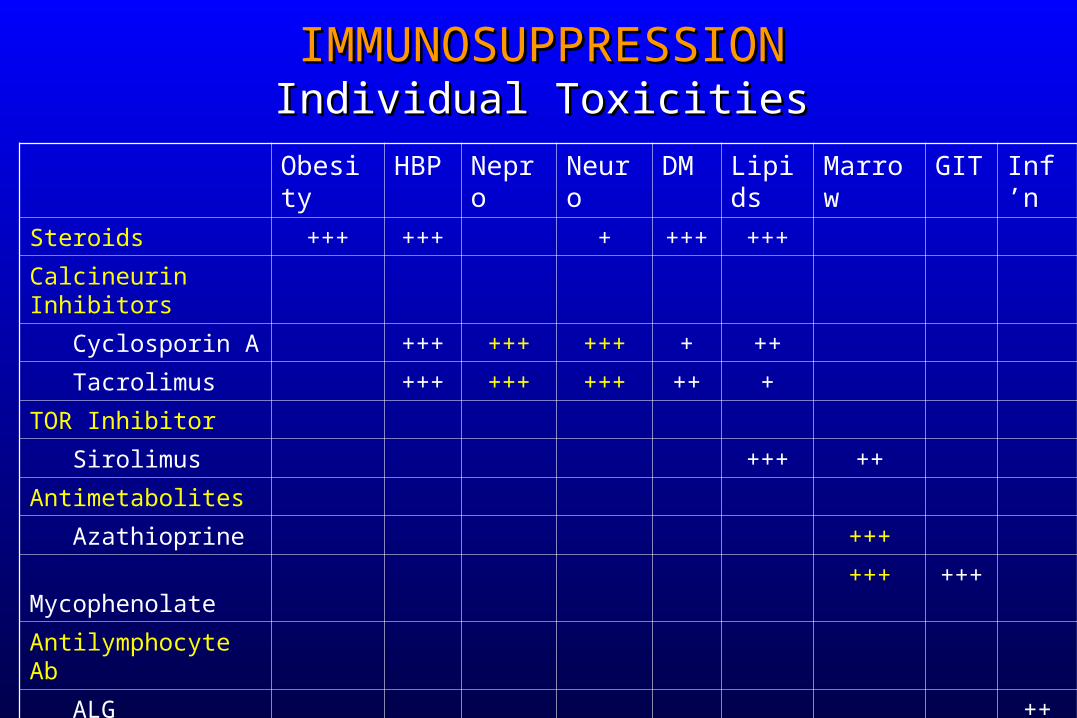
IMMUNOSUPPRESSIONIMMUNOSUPPRESSIONIndividual ToxicitiesIndividual Toxicities
Obesity HBP Nepro Neuro DM Lipids Marrow GIT Inf’n
Steroids +++ +++ + +++ +++
Calcineurin Inhibitors
Cyclosporin A +++ +++ +++ + ++
Tacrolimus +++ +++ +++ ++ +
TOR Inhibitor
Sirolimus +++ ++
Antimetabolites
Azathioprine +++
Mycophenolate +++ +++
Antilymphocyte Ab
ALG ++
OKT3 ++
IL2R-Ab

Transplantation - Immunosuppression “Standard Combinations”
• Calcineurin-inhibitor based– Corticosteroids
• Solumedrol 500 mg pre-op, then taper form 200 mg/d to 20 mg/d during 1st week
– Cyclosporin A (NEORAL)• CsA 10 - 15 mg/kg/d divided BID, orally
OR
– Tacrolimus (PROGRAF)• FK 1 - 1.5 mg/kg/d divided BID, orally
– Third agent• MMF (Cellcept) 2 gm/d divided BID• Azathioprine 1-2 mg/kg/d
30
Transplantation - Immunosuppression
Question 2c• Do all patients require the same degree and type of
immunosuppression?• Rephrased:
– what are the risk factors for acute rejection?• Who needs more immunosuppression, who needs less?
– What are the risk factors for toxicity?• Any alternates without Nephro/Neuro-toxicity?
31
Transplantation - Immunosuppression
Risk Factors for Acute Rejection
• Increased Risk– ABO incompatibility (preformed anti- A or B antibodies)
– presensitized (+ve crossmatch)• From previous blood transfusions or pregnancy
– high PRA• Variable levels of preformed antibody
– previous immunologic graft loss (chronic rej’n)– underlying autoimmune disease
• PSC, Autoimmune CAH
– younger patients
• Lower risk– Uremia– Malnourished patient– older patient– critically ill
32
Transplantation - Immunosuppression
Risk Factors for Early Toxicity
• Increased Risk– renal failure
• Rx: avoid CsA or FK by using antibody therapy * 5 - 10 days, introduce low dose CN-inhibitor with MMF or Azathioprine
– preop coma, postop depressed LOC• Rx same as above
– CMV -ve recipient of CMV +ve organ• Rx, lower immunosuppression or antiviral prophylaxis
– EBV naïve recipient • surveillance
33
Transplantation - Immunosuppression
Risk Factors for Early Toxicity
• Options for patients at Increased Risk– in general: it is the nephro- or neuro-toxicity– avoid (or minimize calcuneurin (IL2) inhibition
• i.e. avoid cyclosporin or tacrolimus
– use anti-lymphocyte antibodies• for 5 - 10 days • combine with MMF or Aza • introduce low dose CsA or Tac ~ POD 7
34
Transplantation - Immunosuppression
Anti-Lymphocyte Antibodies
• Polyclonal Products: RATS, ATG, ALS– cocktail of anti-bodies to antigens on activated t-cells– Toxicity: 1. Fever 2. Cross-react with platelets (thrombocytopenia)
• Monoclonal Antibody: OKT3– murine antibody to the CD3 receptor– Toxicity: 1. Cytokine storm 2. Anti-murine antibodies
• Anti-IL2R Antibodies – anti-CD25 antibody to the -chain of IL2R– chimerized or humanized – toxicity: fever– ? Efficacy without CNI

IMMUNOSUPPRESSIVES BACKGROUND
What’s The Problem?• Toxicity
– major barrier to effective immunosuppression– variable spectrum of toxicities
• specific to each drug– objective
• juggle the toxicities of the available agents to achieve the lowest doses necessary for each patient
– problem• no objective measure of the net immunosuppressive effect in any one
individual
Transplantation - Immunosuppression Toxicities - in - Common
• Infection– esp. viral and fungal
• Malignancy– all cancers with time
• importance of surveillance
– Lymphoproliferative Disease (LPD)• + Epstein Bar Virus (EBV-LPD)• --> monoclonal LPD --> lymphoma
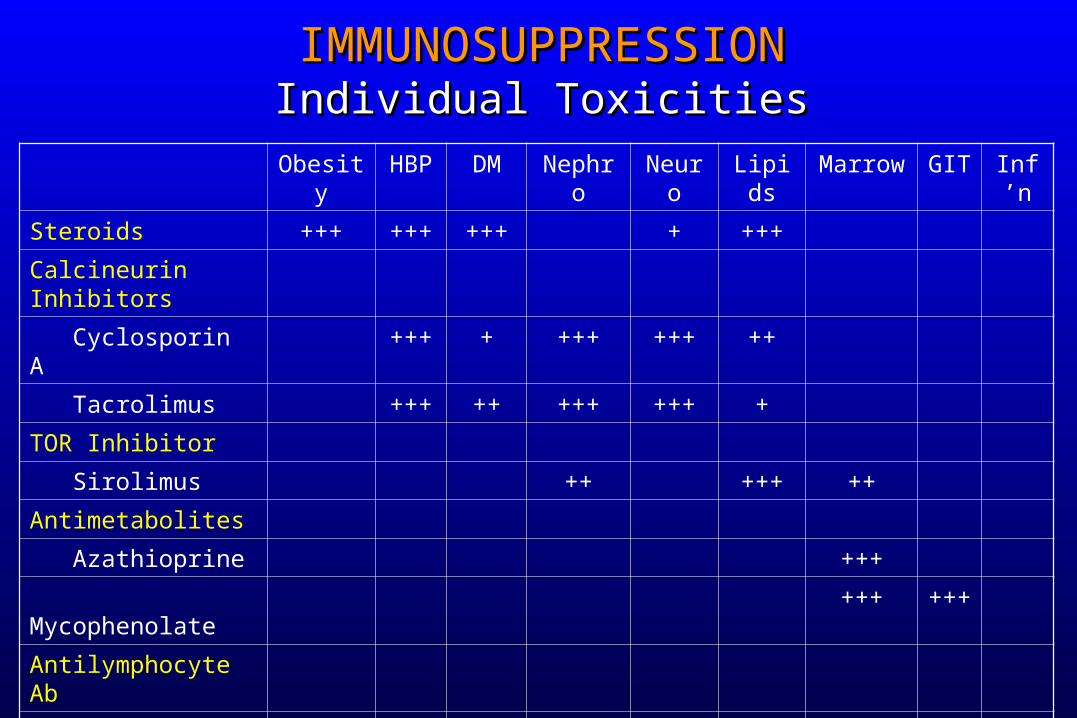
IMMUNOSUPPRESSIONIMMUNOSUPPRESSIONIndividual ToxicitiesIndividual Toxicities
Obesity HBP DM Nephro Neuro Lipids Marrow GIT Inf’n
Steroids +++ +++ +++ + +++
Calcineurin Inhibitors
Cyclosporin A +++ + +++ +++ ++
Tacrolimus +++ ++ +++ +++ +
TOR Inhibitor
Sirolimus ++ +++ ++
Antimetabolites
Azathioprine +++
Mycophenolate +++ +++
Antilymphocyte Ab
ALG ++
OKT3 ++
IL2R-Ab
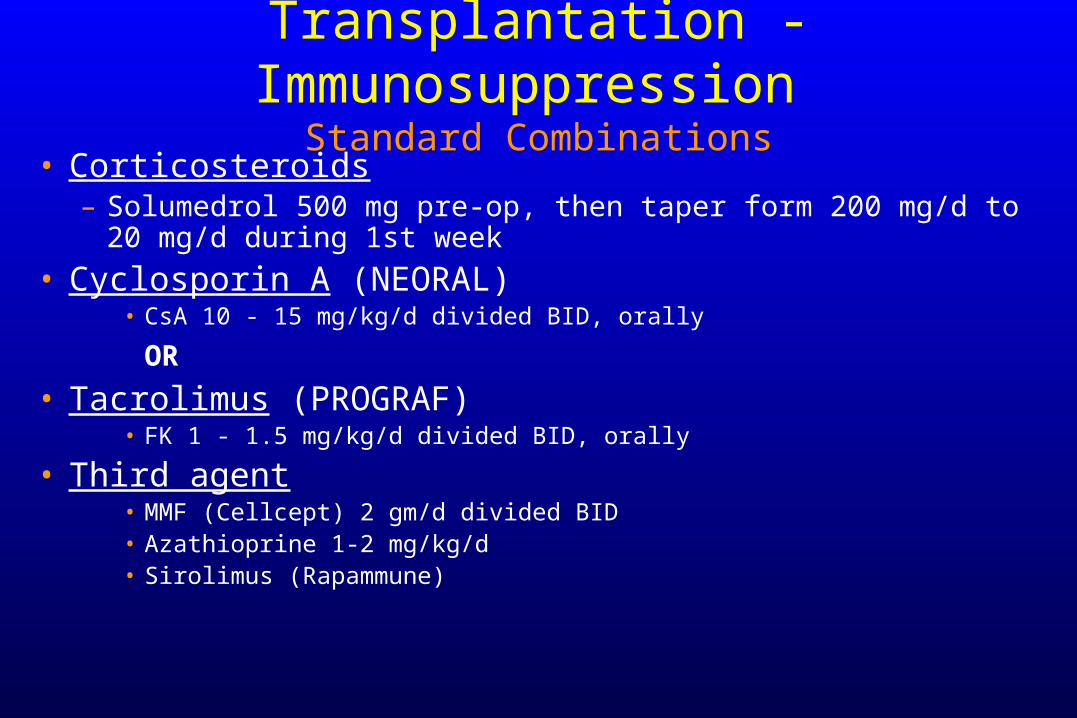
Transplantation - Immunosuppression Standard Combinations
• Corticosteroids– Solumedrol 500 mg pre-op, then taper form 200 mg/d to 20 mg/d
during 1st week
• Cyclosporin A (NEORAL)• CsA 10 - 15 mg/kg/d divided BID, orally
OR
• Tacrolimus (PROGRAF)• FK 1 - 1.5 mg/kg/d divided BID, orally
• Third agent• MMF (Cellcept) 2 gm/d divided BID• Azathioprine 1-2 mg/kg/d • Sirolimus (Rapammune)
39
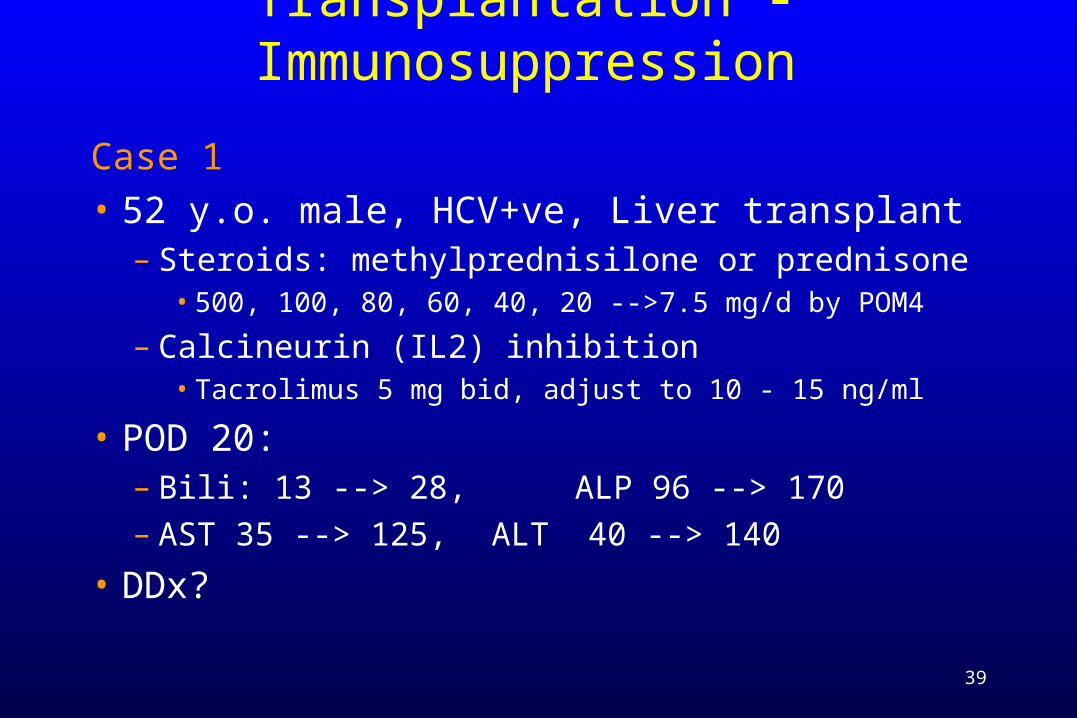
Transplantation - Immunosuppression
Case 1• 52 y.o. male, HCV+ve, Liver transplant
– Steroids: methylprednisilone or prednisone• 500, 100, 80, 60, 40, 20 -->7.5 mg/d by POM4
– Calcineurin (IL2) inhibition• Tacrolimus 5 mg bid, adjust to 10 - 15 ng/ml
• POD 20: – Bili: 13 --> 28, ALP 96 --> 170– AST 35 --> 125, ALT 40 --> 140
• DDx?
40
Transplantation - Immunosuppression
Case 1
• DDx:– Hepatic artery thrombosis
• U/S liver & Doppler, CT & arterial phase, Angiogram
41
Transplantation - Immunosuppression
Case 1
• DDx:– Hepatic artery thrombosisHepatic artery thrombosis
• U/S liver & Doppler, CT & arterial phase, AngiogramU/S liver & Doppler, CT & arterial phase, Angiogram
– Biliary Stenosis, Leak• U/S, MRCP, ERCP
42
Transplantation - Immunosuppression
Case 1
• DDx:– Hepatic artery thrombosisHepatic artery thrombosis
• U/S liver & Doppler, CT & arterial phase, AngiogramU/S liver & Doppler, CT & arterial phase, Angiogram
– Biliary Stenosis, LeakBiliary Stenosis, Leak• U/S, ERCPU/S, ERCP
– Infection• CMV --> CMV antigenemia, Liver Bx• recurrent HCV --> Biopsy
43
Transplantation - Immunosuppression
Case 1• DDx:
– Hepatic artery thrombosisHepatic artery thrombosis• U/S liver & Doppler, CT & arterial phase, AngiogramU/S liver & Doppler, CT & arterial phase, Angiogram
– Biliary Stenosis, LeakBiliary Stenosis, Leak• U/S, ERCPU/S, ERCP
– InfectionInfection• CMV --> CMV antigenemia, Liver BxCMV --> CMV antigenemia, Liver Bx• recurrent HCV --> Biopsyrecurrent HCV --> Biopsy
– Acute Rejection• Biopsy

•Rejection Activity Index:• infiltrate, phlebitis, ductitis
45
Transplantation - Immunosuppression
Risk Factors for Acute Rejection
• Increased Risk– ABO incompatibility (preformed anti- A or B antibodies)
– presensitized (+ve crossmatch) - ** not with liver– high PRA - ** not with liver– previous immunologic graft loss (chronic rej’n)– underlying autoimmune disease
• PSC, Autoimmune CAH
– Younger, well nourished patients
• Lower risk– malnourished, older patient– critically ill

10
100
0 1 2 3 4 5 6 7 8 9 10Years PosttransplantP
erc
en
t G
raft
Su
rviv
al (l
og
)
63585247
01-23-45-6
HLA mm16.013.211.1
9.8
8,1967,835
23,77613,173
n t1/2
Cecka, Clinical Transplants 2002 (p.10)
HLA Matching Effect (1995-2001)
50 16%
47
Transplantation - Immunosuppression
Risk Factors for Early Toxicity
• Increased Risk– renal failure
• Rx: avoid CsA or FK by using antibody therapy * 5 - 10 days, • introduce low dose CN-inhibitor with MMF or Azathioprine
– preop coma, postop depressed LOC• Rx same as above
– CMV -ve recipient of CMV +ve organ• Rx, lower immunosuppression plus antiviral prophylaxis
– EBV naïve recipient • surveillance
48
Transplantation - Immunosuppression
Risk Factors for Early Toxicity
• Options for patients at Increased Risk– in general: it is the nephro- or neuro-toxicity– avoid (or minimize calcineurin (IL2) inhibition
• i.e. avoid cyclosporin or tacrolimus
– use anti-lymphocyte antibodies• for 5 - 10 days • combine with MMF or Aza • introduce low dose CsA or Tac ~ POD 7

49
Transplantation - Immunosuppression
Case 1
• 52 y.o. male, HCV+ve, Liver transplant
• POD 20: – Bili: 13 --> 28, ALP 96 --> 170– AST 35 --> 125, ALT 40 --> 140
• Bx = Acute Rejection – Grade 5-6 / 9
• Treatment?
50
Transplantation - ImmunosuppressionTreatment of Acute Rejection
1 Treat Rejection– Increase CNI
• If RAI < 4
– Corticosteroids • methylprednisilone 500 mg/d * 3
2 Prevent Recurrence– depends on reason for AcR– if Tac or CsA levels sub-therapeutic
• increase Tac or CsA
– if Tac or CsA levels adequate• add a third agent: MMF or Rapamycin
51
Transplantation - ImmunosuppressionTreatment of Acute Rejection
• Outcome– normalization of liver biochemistry– + liver Bx confirmation
• For high RAI
• Steroid - Resistant Rejection– antilymphocyte anti-body therapy:– Polyclonal anti-lymphocyte antibodies
• RATS, ATG, ALS
– Monoclonal ALG• OKT3

52
Transplantation - ImmunosuppressionTreatment of Acute Rejection
• Sequelae of an episode of AcR– treatment increases risks of all immunotherapy related complications
• viral infections– CMV, EBV
• DM, psychosis,
– Renal Tx• reduced graft 1/2 life• Also Lung & Heart• “Cumulative graft injury”
– Liver• Increase recurrence of Hepatitis C• fewer long term sequelae• ? Induce tolerance
53
Transplantation - Immunosuppression
Case 1
• 52 y.o. male, HCV+ve, Liver transplant
• POD 20: – Acute Rejection , Grade 5-6 / 9– Treatment: corticosteroid (2 cycles)
• POD 90:– fever (39O), generally unwell– WBC = 2.8, Liver enzymes 25%– PE: unremarkable
• DDX?
54
Transplantation - Immunosuppression
DDx:
1 Bacterial Infection– CXR, Urine C&S, Blood culture– U/S or CT scan abdomen– Treat on speculation?
55
Transplantation - Immunosuppression
DDx:2 Viral Infection
a ) Cytomegalovirus (CMV)• risk in CMV +ve recipients = 25%
• risk in -ve recipients of +ve organ = 50 - 100% (should receive prophylaxis)
• CMV syndrome (antigenemia)
• CMV disease (Bx confirmation)– liver (Bx), lung (BAL), brain (CT or MRI)
– Treatment• reduce immunosuppression
• Gancyclovir (IV --> PO)
56
Transplantation - Immunosuppression
DDx:2 Viral Infection
b ) Epstein Barr Virus (EBV)• presents as lymphoproliferative disease (LPD) • lympadenopathy • CT: head, chest, abdomen• Biopsy• graded: LPD --> monoconal B-cell lymphoma
– Treatment• reduce (stop) immunosuppression• antiviral therapy (Gancyclovir)• chemotherapy for lymphoma

57
Transplantation - Immunosuppression
DDx:
3 Fungal Infection– candida, aspergillosis, cryptococcus,
mucormycosis– image and culture

58
Transplantation - Immunosuppression
DDx:
4 Other Infection– TB– cat-scratch fever– Herpes simplex

59
Transplantation - ImmunosuppressionChronic Rejection
• Advanced graft injury• Secondary to repeated episodes of acute rejection and/or persistent low
grade immunologic injury• Additive to previous injury
• In donor• Preservation/ischemia/reperfusion
• Liver: duct loss: “ductopenic rejection”• Target = duct or small arterioles
• Lung: bronchiolar loss: “Brochiolitis obliterans”• Cumulative injury
• Heart: accelerated atherosclerotic change: “graft vasculopathy”• Kidney: “chronic graft nephropathy”• Probably multifactorial
• Including donor injury, preservation injury, postop injury…
Transplantation - Immunosuppression TOWARDS TOLERANCE
• Partial Tolerance– “adaptation” allows reduction in total immunosuppression during
first 3 months– = microchimerism?
• Tolerizing Strategies– objective
• drug-free, donor-specific hyporesponsiveness
– needs:• stem or dendritic cell• induction therapy with tolerizing antibodies• continuous antigen exposure
Transplantation - Immunosuppression FUTURE
• Multi-drug Regimens– variety of “protocol” therapies– increased patient-specific individualization
• New Drugs– less toxicity
• or non-overlapping toxicities
– increased efficacy• reduced chronic rejection
– more “patient-friendly”• for improved long-term compliance
Related Documents











