1 Telligen Quality Innovation Network- Quality Improvement Organization Ventilator Associated Events –VAE June 26, 2015 This material was prepared by Telligen, Medicare Quality Innovation Network Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOW-OL-C1-6/2015-11086

1 Telligen Quality Innovation Network- Quality Improvement Organization Ventilator Associated Events –VAE June 26, 2015 This material was prepared by Telligen,
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Telligen Quality Innovation Network-Quality Improvement OrganizationVentilator Associated Events –VAEJune 26, 2015
This material was prepared by Telligen, Medicare Quality Innovation Network Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOW-OL-C1-6/2015-11086
Ventilator Associated Events (VAE)
Boulos (Paul) Nassar, MD MPHAssistant Professor
University of Iowa Hospitals and Clinics
Objectives
• Departure from the 2002 CDC definition of Ventilator Associated Pneumonia (VAP)
• Definition and algorithms of VAE• Limitations of VAE• VAE diagnosis with case studies• Proven strategies to prevent VAE
Ventilator associated pneumonia (VAP)
• >300,000 patients receive mechanical ventilation each year in the US
• VAP is an important cause of morbidity, mortality, and increased health-care costs in patients who are mechanically ventilated
• VAP is a nosocomially acquired infection• VAP is a complication of mechanical ventilation
patient safety measure
• Incidence rates: 0-6 per 1000 ventilator-daysMuscedere-Chest 13

Ventilator associated pneumonia (VAP)
• VAP is a hospital acquired infection (HAI)• Public reporting is mandated for HAI
• Surveillance programs attempt to identify events and analyze the circumstances surrounding their occurrence
• Surveillance programs are fundamental for effective prevention of future cases
CDC VAP definition (2002)
1. New or progressive and persistent radiographic abnormality developing in a patient on mechanical ventilation
2. >=1 systemic sign (fever, leukopenia or leukocytosis, or altered mental status)
3. Selected pulmonary criteria (change in respiratory secretions, worsening oxygenation, new onset of cough, dyspnea or rales)
Illustrative case #1
• 57 year old male patient is admitted with acute pancreatitis
• He is orally intubated and started on mechanical ventilation
• He is receiving aggressive fluid resuscitation• 72 hours into his illness, he becomes febrile and
his FiO2 requirements increase from 50% to 70%• A chest radiograph is obtained
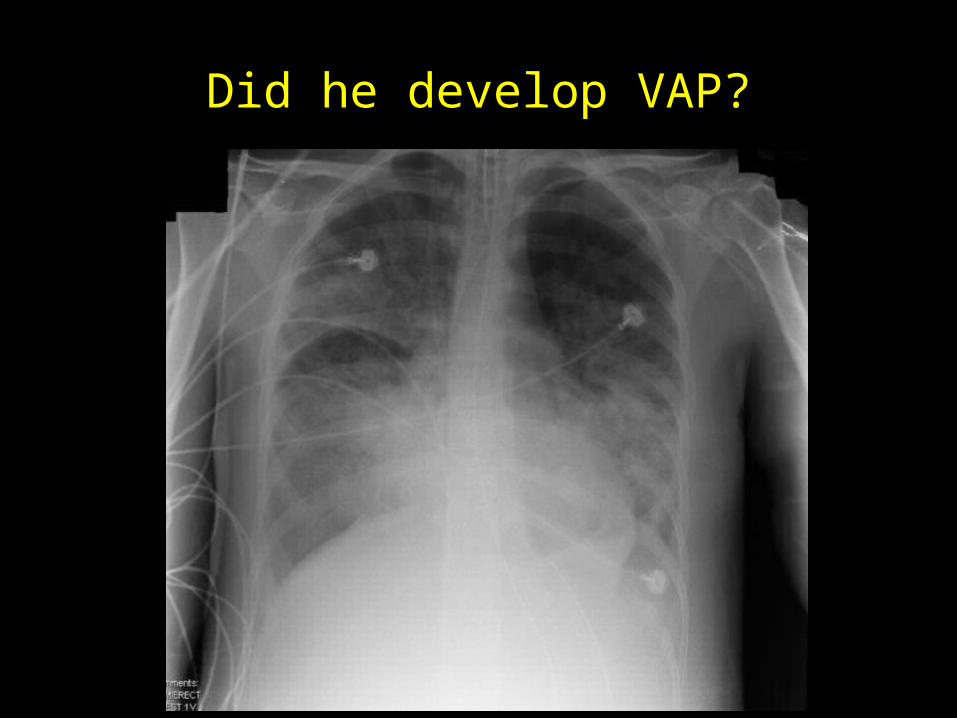
Did he develop VAP?
Polling Question
Did this patient develop VAP?1) Yes2) No3) I don’t know
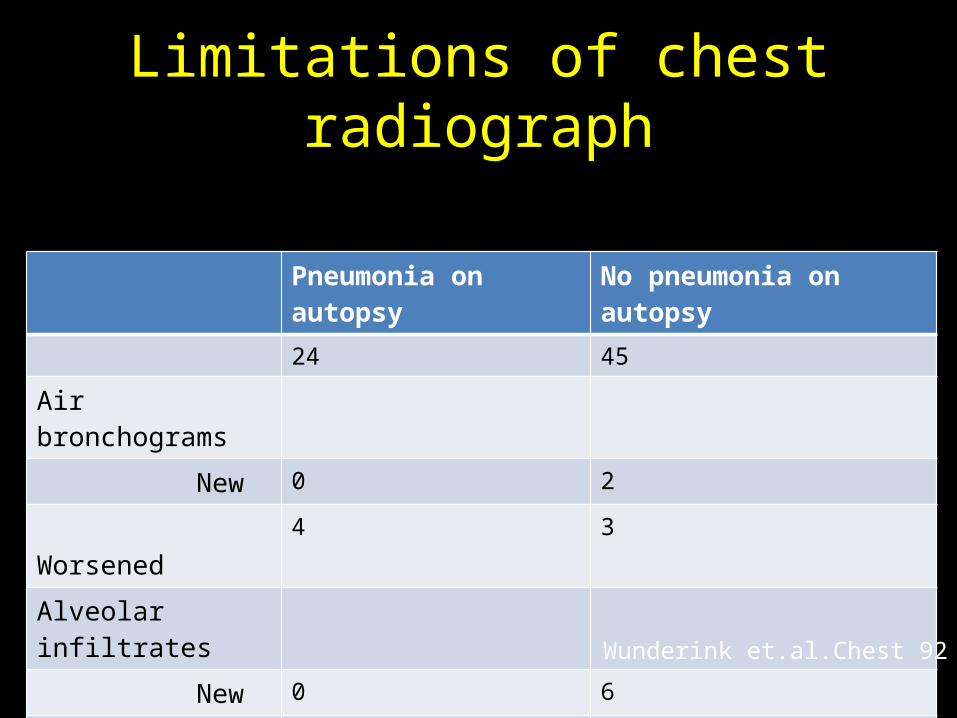
Limitations of chest radiograph
Pneumonia on autopsy No pneumonia on autopsy 24 45
Air bronchograms New 0 2
Worsened 4 3
Alveolar infiltrates New 0 6
Worsened 7 15
Wunderink et.al.Chest 92
Limitations of chest radiograph
• A chest radiograph may demonstrate a haziness that could be pneumonia, atelectasis, or pleural effusion
• Chest radiograph could represent pulmonary edema or ARDS
• Findings are more challenging to characterize on a portable film
• Inter-observer variability in interpretation
Other limitations in the definition
• Clinical signs and symptoms are unreliable for surveillance purposes
• Microbiological evidence is problematic because it is difficult to distinguish between colonization and infection– 22% of 95 intensive care unit patients became
colonized within 24 hours
• The 2002 CDC definition was found to be neither sensitive nor specific for VAP and cannot be accurately used for surveillance
• Definition met through different pathways• Burdensome to capture data
New definition
• Centers for Disease Control and Prevention’s new surveillance paradigms for patients who are mechanically ventilated
• This new VAE definition promotes surveillance in a uniform and consistent manner at all hospitals
New definition
• Uses objective data1. deterioration in respiratory status after a period
of stability or improvement on the ventilator2. evidence of infection or inflammation3. laboratory evidence of respiratory infection
• Chest radiograph is no longer part of the definition
New definition
• Reliable and standardize reporting
1. Public reporting2. Comparison among institutions 3. Pay-for-performance calculations
New VAE approach
• VAE groups all the conditions that result in a significant and sustained deterioration in oxygenation– > than 20% increase in the daily minimum FiO2
or – > 3 cm H2O in the daily minimum positive end-
expiratory pressure (PEEP)

What fulfills this new VAE definition?
What fulfills this new VAE definition?
1. Infectious conditions (tracheitis, tracheobronchitis, and pneumonia)
2. Noninfectious conditions (atelectasis, pulmonary embolism, pulmonary edema, ventilator-induced lung injury)
Timeline for VAE
• The day of intubation and initiation of mechanical ventilation is day 1
• Patients must be mechanically ventilated for more than 2 calendar days
• The earliest date of event for VAE (the date of onset of worsening oxygenation) is day 3
• The earliest day on which VAE criteria can be fulfilled is day 4
Timeline for VAE
D2D1 D3 D4
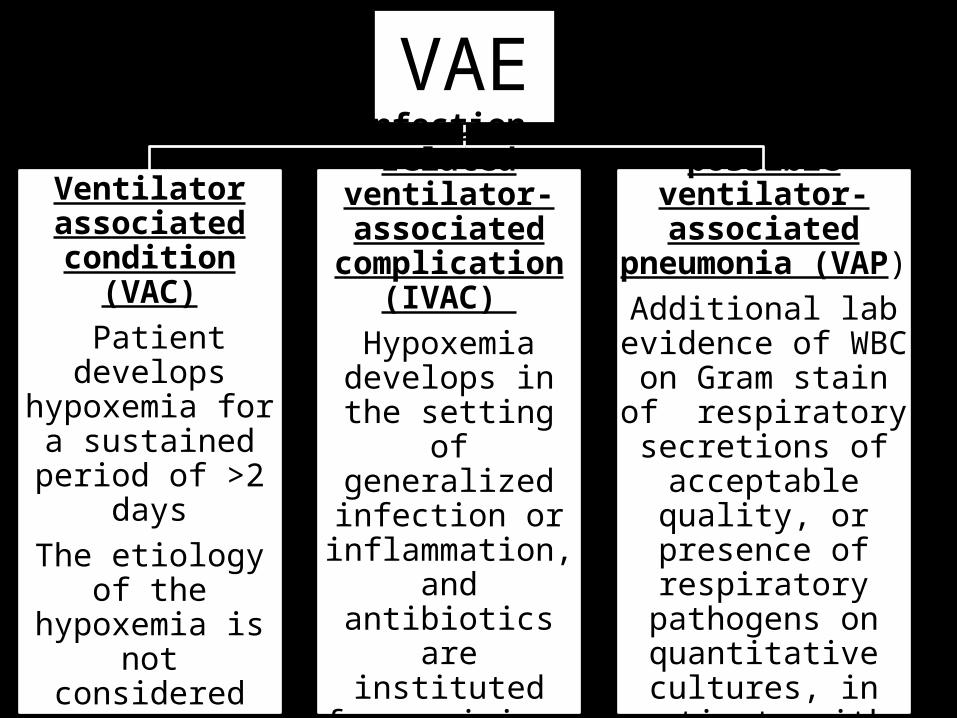
VAE
Ventilator associated
condition (VAC) Patient develops hypoxemia for a
sustained period of >2 days
The etiology of the hypoxemia is not
considered
Infection-related ventilator-associated
complication (IVAC)
Hypoxemia develops in the
setting of generalized infection or
inflammation, and antibiotics are instituted for a
minimum of 4 days
Probable or possible ventilator-associated
pneumonia (VAP) Additional lab
evidence of WBC on Gram stain of
respiratory secretions of acceptable quality,
or presence of respiratory pathogens
on quantitative cultures, in patients
with IVAC
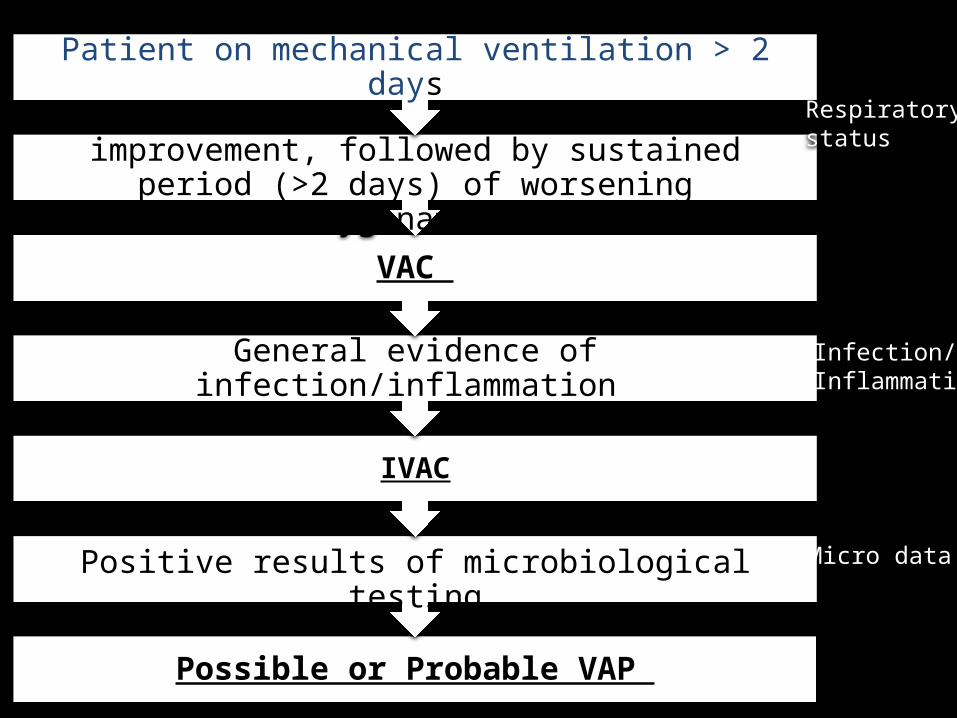
Possible or Probable VAP
Positive results of microbiological testing
IVAC
General evidence of infection/inflammation
VAC
Baseline period of stability or improvement, followed by sustained period (>2 days) of worsening oxygenation
Patient on mechanical ventilation > 2 days Respiratory status
Infection/Inflammation
Micro data
Tier 1: Ventilator associated condition (VAC)
• VAC is defined by a sustained period of worsening oxygenation that immediately follows a baseline period of stability or improvement
• Captures both infectious and non-infectious condition and complication occurring in mechanically ventilated patients
• Detects variety of conditions, not all of which are preventable; hence they are called conditions not complications
Tier 2:Infection-related ventilator-associated complication (IVAC)
• Identifies the subset of VACs that are potentially related to infection1. Abnormal WBC2. Abnormal Temperature3. Initiation of a new antimicrobial agent
• IVAC will likely capture patients with pulmonary infections and extrapulmonary infections of sufficient severity to trigger respiratory deterioration
Tier 3: Probable or possible ventilator associated pneumonia (VAP)
• Patient who met 1 and 2 with • respiratory infections as manifested by
objective evidence of purulent respiratory secretions and/or positive results of microbiological tests performed on respiratory specimens
Tier 3: Probable or possible ventilator associated pneumonia (VAP)
• Possible VAP– presence of purulent secretions or a positive lower
respiratory tract culture• Probable VAP
– purulent secretions in addition to a positive lower respiratory tract culture meeting certain quantitative or semiquantitative thresholds of pathogen growth
– presence of a positive pleural fluid culture, lung tissue with histopathological evidence of infection, or positive diagnostic tests for Legionella or respiratory tract viruses
Limitations• Limited science to truly define VAP• Surveillance definitions don’t always align with
clinical events• Only 21% of “traditional” VAP are detected by
VAC and 17% by IVAC – Definition criteria– VAC does not equal VAP
• Minimum of duration of mechanical ventilation could miss a fraction of patients
Lilly et.al.Chest 13
Limitations• Measure physician behavior rather than
physiologic parameters or pathologic patient conditions – The measure can improve with changes in
behavior to game the system that do not reflect improvement in the condition of the patient
Lilly et.al.Chest 13
Pointers
• Acknowledge the limitations of the current definition• Cost of this surveillance program might be less• Avoid “manipulating” data to avoid detection of
events and lower the rates without improving delivery of care
• Opportunity of partnership between infection preventionist and other stakeholders – Tumor board model?
• Use VAC flag to make sure all VAP preventive measures are in place

Example 1: VAC or no VAC?
MV day Daily minimum PEEP
Daily minimum FiO2
1 0 100%2 0 50%3 5 50%4 5 50%5 8 50%6 8 50%
Polling Question
Does this case represent VAC?
1) VAC
2) No VAC

Example 2: VAC or no VAC?
MV day Daily minimum PEEP
Daily minimum FiO2
1 8 100%2 6 50%3 5 35%4 5 40%5 6 70%6 6 70%

Polling Question
Does this case represent VAC?
1) VAC
2) NO VAC
How do we prevent VAP?High to moderate evidence
• Use non invasive positive pressure ventilation!• Early discontinuation of mechanical ventilation• Minimize sedation • Daily interruption of sedation• Assess readiness to extubate daily • Early mobilization• Change the ventilator circuit only if visibly soiled• Utilize endotracheal tubes with subglottic secretion
drainage port • Head-of-bed elevation (30º to 45º)
How do we prevent VAP?Less evidence
• Oral decontamination and care with chlorhexidine
• Mechanical tooth brush
How do we prevent VAP?Generally not recommended
• Early tracheostomy• Early parenteral nutrition• Monitoring residual gastric volumes• Stress ulcer prophylaxis• Silver coated endotracheal tubes

Take home points
• New definition is a surveillance algorithm and not a clinical definition
• There is an opportunity to involve multiple stakeholders in addressing VAP
• Surveillance program is an opportunity to signal to the clinician when a VAC has occurred
• Anticipate changes as more data is being collected on the performance of this new algorithm
Questions
40
Contacts
Karen BolandSr. Quality Improvement FacilitatorEmail: [email protected]: 630-928-5828
Debbie CamachoSenior QI ManagerEmail: [email protected]: 630-928-5815
Meghan FoleyProject Assistant II Email: [email protected]: 630-928-5828
Related Documents











