Surgical/Orthodontic Treatment of Mandibular Asymmetries Pamela R. Hanson, DDS, MS, and Michael B. Melugin, DDS, MS The management of a mandibular asymmetry requires a combined surgical and orthodontic approach. Orthodontic and orthopedic management in a growing patient can sometimes fully correct an emerging minor mandibular asymmetry. Moderate to severe asymmetries can usually be minimized but not fully corrected with early orthodontic and orthopedic intervention. Sometimes the severity of associated dysfunction or the presence of devel- opmental compensations that are occurring with growth require early sur- gical intervention. Early surgical asymmetry correction (during growth), as well as surgical treatment at growth cessation, has the same requirements with respect to selecting the proper treatment approach. Ideally, the se- lected treatment should optimize symmetry, while minimizing morbidity and treatment duration and maximizing long-term predictability. (Semin Orthod 2009;15:268-278.) © 2009 Published by Elsevier Inc. T he timing and method of treatment is de- termined by the magnitude of mandibular asymmetry, the skeletal age of the patient, and the presence of functional deficits. Minor asymmetries can be corrected with growth modification through orthopedic and orthodontic forces. Asymmetric forces delivered during growth can result in resolution of asym- metry in mild cases. In more moderate to severe asymmetries, effective growth modification may only be enough to improve, but not fully correct, asymmetry. An assessment of the nature and magnitude of the mandibular asymmetry must be com- pleted as the first step toward management. Data gathering for this assessment includes a thor- ough clinical and radiographic evaluation, pos- teroanterior and lateral cephalometric studies, and a dental occlusal evaluation. The orthodontic and orthopedic manage- ment of mandibular asymmetry falls into 2 cate- gories: orthodontic correction of the occlusal asymmetry, or correction of the underlying skel- etal discrepancy by combined orthodontic and orthopedic means. The correction of occlusal asymmetry may include several treatment methods, including asymmetric extraction therapy, asymmetric func- tional appliance therapy, asymmetric elastic trac- tion (Fig. 1), asymmetric force delivery using fixed or removable appliances, and others. A successful outcome with treatment of this type is the creation of a more symmetric and functional occlusion while accepting the underlying skele- tal disharmony. Sometimes, however, the correction of an oc- clusal asymmetry allows for improvement in skel- etal symmetry. In a patient with unilateral Class II malocclusion and maxillary transverse defi- ciency, for example, correction of the unilateral posterior crossbite will allow the mandible to take a Class I position on the affected side, im- proving symmetry 1 (Fig. 2). The management of mandibular asymmetry in the skeletally immature patient may take sev- eral courses: (1) fully addressing the asymmetry From the Division of Oral and Maxillofacial Surgery, Medical College of Wisconsin, Milwaukee, WI, Cleft and Craniofacial Teams, Children’s Hospital of Wisconsin, Milwaukee, WI, Depart- ment of Orthodontics, School of Dentistry, Marquette University, Milwaukee, WI, and Department of Dentistry, Children’s Hospital of Wisconsin, Milwaukee, WI. Address correspondence to Pamela R. Hanson, DDS, MS, 15855 West National Avenue, New Berlin, WI 53151; Phone: (262) 784-4050, Fax: (262) 784-3189; E-mail: [email protected] © 2009 Published by Elsevier Inc. 1073-8746/09/1504-0$30.00/0 doi:10.1053/j.sodo.2009.07.006 268 Seminars in Orthodontics, Vol 15, No 4 (December), 2009: pp 268-278

1-s2.0-S1073874609000413-main
Dec 10, 2015
jj
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SMP
Tat
godmaoa
opgo
CTmMW
W7
2
urgical/Orthodontic Treatment ofandibular Asymmetries
amela R. Hanson, DDS, MS, and Michael B. Melugin, DDS, MS
The management of a mandibular asymmetry requires a combined surgical
and orthodontic approach. Orthodontic and orthopedic management in a
growing patient can sometimes fully correct an emerging minor mandibular
asymmetry. Moderate to severe asymmetries can usually be minimized but
not fully corrected with early orthodontic and orthopedic intervention.
Sometimes the severity of associated dysfunction or the presence of devel-
opmental compensations that are occurring with growth require early sur-
gical intervention. Early surgical asymmetry correction (during growth), as
well as surgical treatment at growth cessation, has the same requirements
with respect to selecting the proper treatment approach. Ideally, the se-
lected treatment should optimize symmetry, while minimizing morbidity
and treatment duration and maximizing long-term predictability. (Semin
Orthod 2009;15:268-278.) © 2009 Published by Elsevier Inc.
ta
mgaeo
iattfistot
ceIcptp
i
he timing and method of treatment is de-termined by the magnitude of mandibular
symmetry, the skeletal age of the patient, andhe presence of functional deficits.
Minor asymmetries can be corrected withrowth modification through orthopedic andrthodontic forces. Asymmetric forces delivereduring growth can result in resolution of asym-etry in mild cases. In more moderate to severe
symmetries, effective growth modification maynly be enough to improve, but not fully correct,symmetry.
An assessment of the nature and magnitudef the mandibular asymmetry must be com-leted as the first step toward management. Dataathering for this assessment includes a thor-ugh clinical and radiographic evaluation, pos-
From the Division of Oral and Maxillofacial Surgery, Medicalollege of Wisconsin, Milwaukee, WI, Cleft and Craniofacialeams, Children’s Hospital of Wisconsin, Milwaukee, WI, Depart-ent of Orthodontics, School of Dentistry, Marquette University,ilwaukee, WI, and Department of Dentistry, Children’s Hospital ofisconsin, Milwaukee, WI.
Address correspondence to Pamela R. Hanson, DDS, MS, 15855est National Avenue, New Berlin, WI 53151; Phone: (262)
84-4050, Fax: (262) 784-3189; E-mail: [email protected]© 2009 Published by Elsevier Inc.1073-8746/09/1504-0$30.00/0
edoi:10.1053/j.sodo.2009.07.006
68 Seminars in Orthodontics, Vol 15, No
eroanterior and lateral cephalometric studies,nd a dental occlusal evaluation.
The orthodontic and orthopedic manage-ent of mandibular asymmetry falls into 2 cate-
ories: orthodontic correction of the occlusalsymmetry, or correction of the underlying skel-tal discrepancy by combined orthodontic andrthopedic means.
The correction of occlusal asymmetry maynclude several treatment methods, includingsymmetric extraction therapy, asymmetric func-ional appliance therapy, asymmetric elastic trac-ion (Fig. 1), asymmetric force delivery usingxed or removable appliances, and others. Auccessful outcome with treatment of this type ishe creation of a more symmetric and functionalcclusion while accepting the underlying skele-al disharmony.
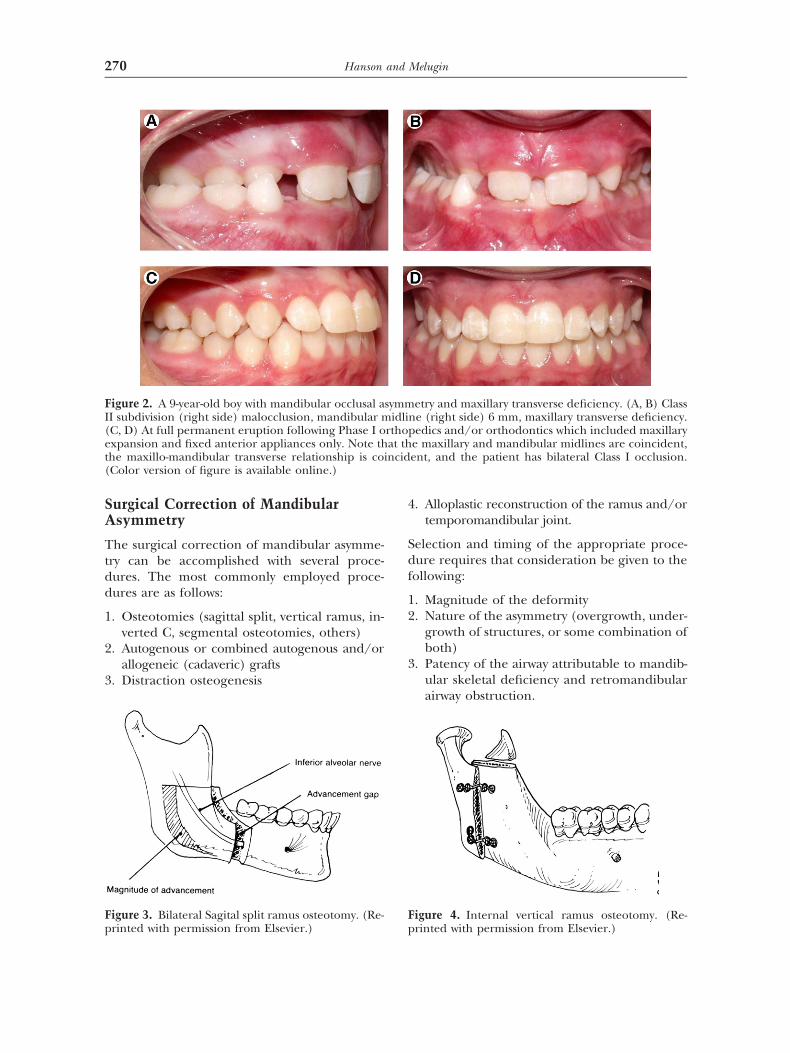
Sometimes, however, the correction of an oc-lusal asymmetry allows for improvement in skel-tal symmetry. In a patient with unilateral ClassI malocclusion and maxillary transverse defi-iency, for example, correction of the unilateralosterior crossbite will allow the mandible toake a Class I position on the affected side, im-roving symmetry1 (Fig. 2).
The management of mandibular asymmetryn the skeletally immature patient may take sev-
ral courses: (1) fully addressing the asymmetry4 (December), 2009: pp 268-278

bsmmftgmsacmrrairc
tirg
pwdtmeofmiserrb
amailm
FAcaNsFi
269Treatment of Mandibular Asymmetries
y orthopedic and/or orthodontic means, (2)urgically addressing the asymmetry on skeletalaturity, (3) orthodontic and/or orthopedicanagement during the years of facial growth
ollowed by definitive surgical and/or orthodon-ic correction on completion of facial skeletalrowth, or (4) surgical correction of the asym-etry during growth and, if needed, again at
keletal maturity. If early treatment objectivesre met from the standpoint of function, oc-lusion, and/or facial symmetry, the patientust be retained and monitored through the
emainder of growth to ensure that the cor-ection was stable. Reinstitution of orthopedicnd/or orthodontic treatment may be neededf asymmetry reemerges with growth. A long-ange plan that includes surgery at growthessation may be elected.
Patients with an asymmetry that is moderateo severe and with no significant functional lim-tations may wait until skeletal maturity iseached for a definitive orthodontic and/or sur-
igure 1. Orthopedic and/or orthodontic managemesymmetric malocclusion in the mixed dentition, Claoincident, occlusal cant to the mandibular dental arfter maxillary expansion, full fixed appliances, and eote that the maxillary and mandibular midlines are
ymmetry of occlusion (Class I bilaterally) and the maxinal skeletal and occlusal result with correction of the
s available online.)
ical correction. This approach is best used for i
atients with reasonable function and cosmesis,ho will not be negatively affected by waiting forefinitive treatment. If the patient is being nega-
ively affected functionally, psychosocially, or cos-etically, the decision to address the asymmetry
arly and then possibly again later may be the bestption. The intent of this approach is to optimizeunction and cosmesis during growth, providing a
ore normal interim status for the patient. Earlynterventions will likely decrease the magnitude ofurgical correction that might be necessary at skel-tal maturity. An early intervention that results in aeduction of the severity of skeletal deformity willesult in a definitive surgical procedure that maye less extensive and more stabile.
In the skeletally immature patient with severesymmetry, the option to treat early might be theost appropriate choice, especially if there are
ssociated functional, psychosocial, or estheticssues that demand early intervention. Again,ater treatment will likely be needed, but the
agnitude of subsequent treatment is dimin-
f a young patient with asymmetric malocclusion. (A)(left side) and Class III (right side), midlines are not(B) Improved symmetry in the permanent dentition
traction. (C) Continued asymmetric elastic traction.ident, the occlusal cant is corrected, and right-to-leftandibular transverse dimension are in harmony. (D)
etal and occlusal disharmony. (Color version of figure
nt oss IIch.
lasticcoincillo-mskel
shed by early intervention.
SA
Ttdd
1
2
3
4
Sdf
12
3
FI(et(
Fp
F
270 Hanson and Melugin
urgical Correction of Mandibularsymmetry
he surgical correction of mandibular asymme-ry can be accomplished with several proce-ures. The most commonly employed proce-ures are as follows:
. Osteotomies (sagittal split, vertical ramus, in-verted C, segmental osteotomies, others)
. Autogenous or combined autogenous and/orallogeneic (cadaveric) grafts
. Distraction osteogenesis
igure 2. A 9-year-old boy with mandibular occlusal aI subdivision (right side) malocclusion, mandibular mC, D) At full permanent eruption following Phase I oxpansion and fixed anterior appliances only. Note thhe maxillo-mandibular transverse relationship is coiColor version of figure is available online.)
igure 3. Bilateral Sagital split ramus osteotomy. (Re-
rinted with permission from Elsevier.) p. Alloplastic reconstruction of the ramus and/ortemporomandibular joint.
election and timing of the appropriate proce-ure requires that consideration be given to theollowing:
. Magnitude of the deformity
. Nature of the asymmetry (overgrowth, under-growth of structures, or some combination ofboth)
. Patency of the airway attributable to mandib-ular skeletal deficiency and retromandibularairway obstruction.
etry and maxillary transverse deficiency. (A, B) Classne (right side) 6 mm, maxillary transverse deficiency.
edics and/or orthodontics which included maxillarye maxillary and mandibular midlines are coincident,ent, and the patient has bilateral Class I occlusion.
igure 4. Internal vertical ramus osteotomy. (Re-
symmidli
rthopat thncid
rinted with permission from Elsevier.)
45
MAittsiottltgitattl
lsvIntt
wrbtsct(mpfifi
ado
FfaiIs
271Treatment of Mandibular Asymmetries
. Skeletal age
. Psychosocial and functional needs of thegrowing patient that may require early (non-definitive) surgical intervention
andibular Osteotomiesn osteotomy is a “bone cut” or a sectioning
nto 2 or more pieces of the bone (in this case,he mandible). Bone can then be removed athe osteotomy site to reduce the mandibularize, or bone can be grafted interpositionallynto the osteotomy site to lengthen the bone,r the osteotomy can be structured such thathere is a planar section of overlap that allowshe bone halves to slide over one another toengthen the bone (the sagittal osteotomy orhe inverted “C” osteotomy) (Fig. 3). At sur-ery, with the osteotomy technique, the bones made shorter or longer by a specific lengthhat is planned before surgery, using clinicalnd cephalometric evaluation. In general,he magnitude of mandibular lengtheninghrough osteotomy techniques is limited byong-term data that suggest stability for moves
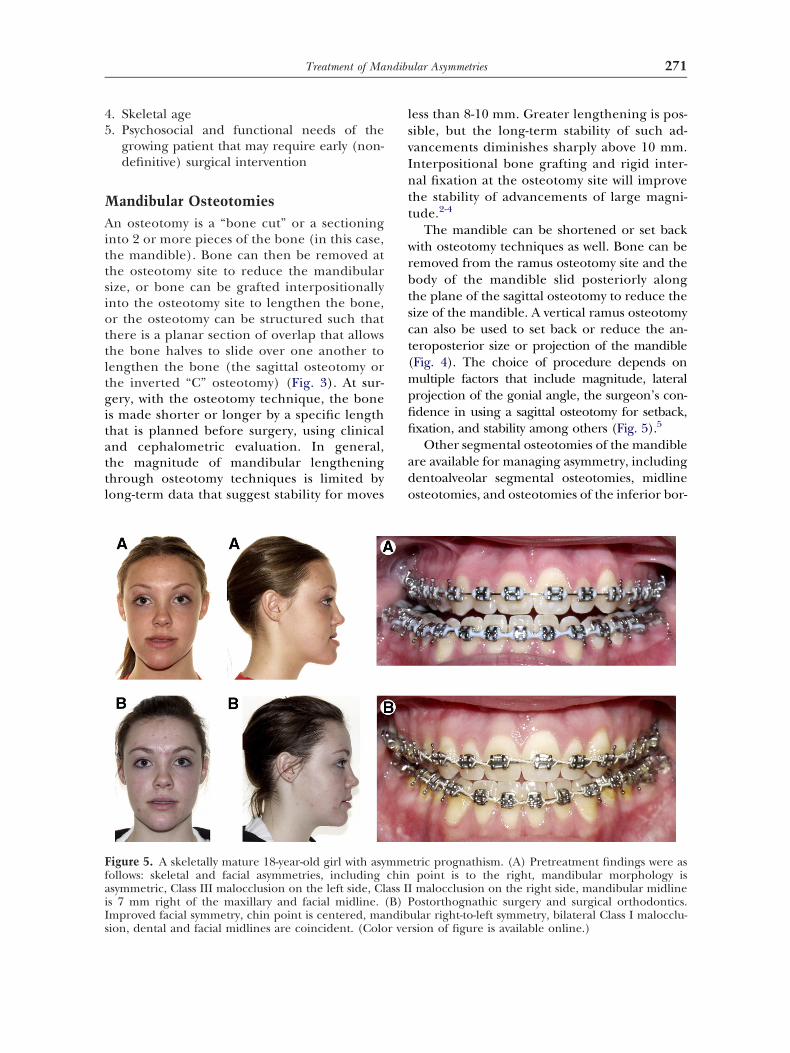
igure 5. A skeletally mature 18-year-old girl with asyollows: skeletal and facial asymmetries, includingsymmetric, Class III malocclusion on the left side, Cls 7 mm right of the maxillary and facial midline. (mproved facial symmetry, chin point is centered, ma
ion, dental and facial midlines are coincident. (Color veress than 8-10 mm. Greater lengthening is pos-ible, but the long-term stability of such ad-ancements diminishes sharply above 10 mm.nterpositional bone grafting and rigid inter-al fixation at the osteotomy site will improve
he stability of advancements of large magni-ude.2-4
The mandible can be shortened or set backith osteotomy techniques as well. Bone can beemoved from the ramus osteotomy site and theody of the mandible slid posteriorly alonghe plane of the sagittal osteotomy to reduce theize of the mandible. A vertical ramus osteotomyan also be used to set back or reduce the an-eroposterior size or projection of the mandibleFig. 4). The choice of procedure depends onultiple factors that include magnitude, lateral
rojection of the gonial angle, the surgeon’s con-dence in using a sagittal osteotomy for setback,xation, and stability among others (Fig. 5).5
Other segmental osteotomies of the mandiblere available for managing asymmetry, includingentoalveolar segmental osteotomies, midlinesteotomies, and osteotomies of the inferior bor-
tric prognathism. (A) Pretreatment findings were aspoint is to the right, mandibular morphology ismalocclusion on the right side, mandibular midlineostorthognathic surgery and surgical orthodontics.
ular right-to-left symmetry, bilateral Class I malocclu-
mmechinass IIB) P
ndib
sion of figure is available online.)
dat
rwmidas
mtlocmti
B
Bot
dinstsmwfnplcmtfccoclhcsTf
Fidoasa
272 Hanson and Melugin
er of the mandible with advancement, setback,symmetry correction, or some combination ofhe above mentioned osteotomies.6,7
Osteotomies are usually fixated rigidly or semi-igidly with plates, screws, mesh, pins, and/orires. Rigid fixation can be combined with inter-axillary fixation. After healing of the osteotomies
s completed, the new size and shape of the man-ible will change only as a result of relapse, latend unexpected skeletal growth, or additionalkeletal surgery.
When orthognathic surgery is used to addressandibular asymmetry, presurgical orthodontic
herapy is used to remove dental compensations,evel, align, and coordinate arches. The orth-dontist and surgeon must agree on the final oc-lusal and skeletal outcome. The orthodontistust provide a presurgically adjusted dentition
hat allows the surgeon to place skeletal segmentsn the predetermined position (Figs. 5 and 6).
one Grafts
one grafts may be used in combination withsteotomies to improve the stability of large sagit-al advancements of the mandibular body. In ad-
igure 6. An 18-year-old girl with hemifacial micrommediate presurgery findings were as follows: softiscrepancies between the maxillary, mandibular, andrthodontics. Orthognathic surgery included Le Fortdvancement and bilateral sagittal split ramus osteotomymmetry, occlusal cant corrected, coincident midline
vailable online.)ition, allogeneic (cadaveric) bone can be usednterpositionally, or in combination with autoge-ous (harvested from the hip, calvarium, rib of theame patient) to reconstruct large deficiencies ofhe mandible. Before the advent and wide-pread use of distraction osteogenesis, largeagnitude deficiencies could be managedith an allogenic hollowed-out mandibular
orm filled with autogenous bone, or alter-ately, an autogenous rib or hip bone strutacked with particulate autogenous bone. Al-
ogeneic bone by itself does not transfer boneells. Therefore, it has limited applications forandibular lengthening. The addition of au-
ogenous bone involves a separate surgical siteor bone harvesting. This involves additionalost, time, and morbidity. In addition, rib andlavicle may be used to reconstruct the ramusf the mandible for large magnitude deficien-ies that include absence of a normal articu-ating condylar surface. These bone grafts arearvested in continuity with their articulatingartilage, which then serves as the articulatingurface within the temporomandibular joint.hese costochondral grafts have the potential
or growth when used in a growing patient.
ia. (A) After presurgical orthodontic preparation,e and skeletal left-sided deficiencies, occlusal cant,l midlines. (B) Postorthognathic surgery and surgicalling by differential impaction and down grafting andost-treatment findings include soft tissue and skeletald good overall occlusion. (Color version of figure is
somtissufaciaI leve
y. Ps, an
Tmosst
DTtccitsslapanottb
dabftp
aolttcttgtss
ttmlt
Fc
273Treatment of Mandibular Asymmetries
his growth, however, is not predictable anday exhibit undergrowth or, more rarely,
vergrowth. These grafts may also be rigidly oremirigidly fixated to the mandible, and areubject to the volume limitations of the soft-issue bed at the site.
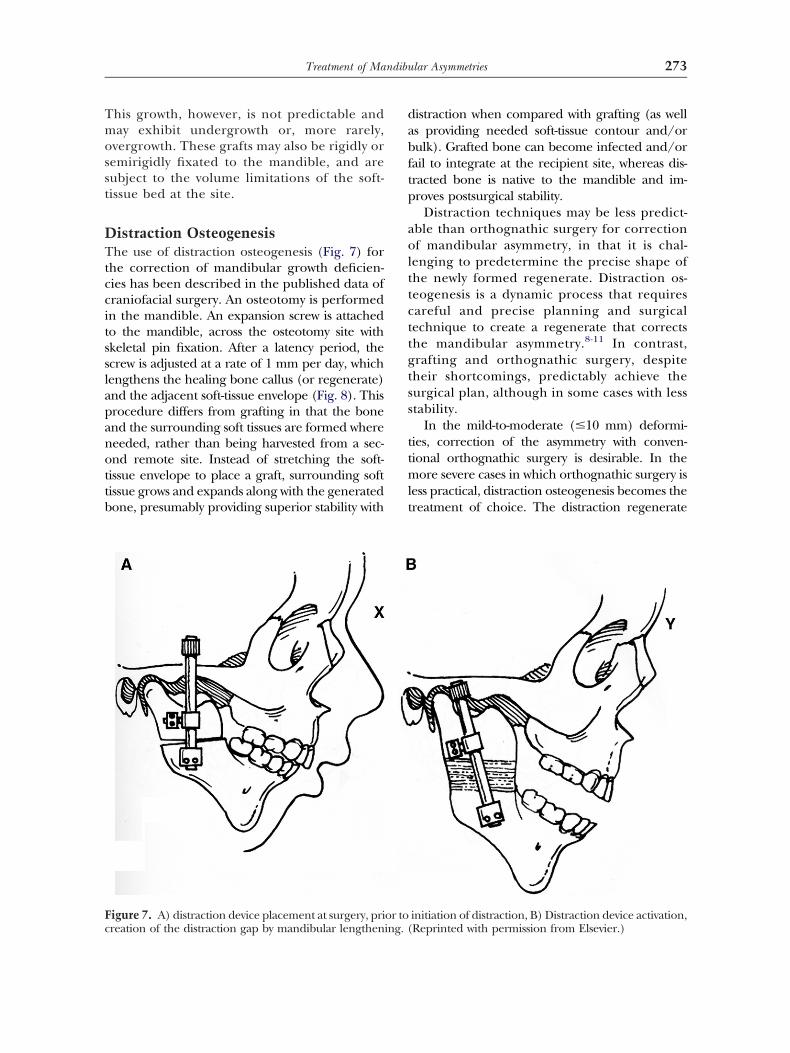
istraction Osteogenesishe use of distraction osteogenesis (Fig. 7) for
he correction of mandibular growth deficien-ies has been described in the published data ofraniofacial surgery. An osteotomy is performedn the mandible. An expansion screw is attachedo the mandible, across the osteotomy site withkeletal pin fixation. After a latency period, thecrew is adjusted at a rate of 1 mm per day, whichengthens the healing bone callus (or regenerate)nd the adjacent soft-tissue envelope (Fig. 8). Thisrocedure differs from grafting in that the bonend the surrounding soft tissues are formed whereeeded, rather than being harvested from a sec-nd remote site. Instead of stretching the soft-issue envelope to place a graft, surrounding softissue grows and expands along with the generatedone, presumably providing superior stability with
igure 7. A) distraction device placement at surgery, pri
reation of the distraction gap by mandibular lengthening. (istraction when compared with grafting (as wells providing needed soft-tissue contour and/orulk). Grafted bone can become infected and/orail to integrate at the recipient site, whereas dis-racted bone is native to the mandible and im-roves postsurgical stability.
Distraction techniques may be less predict-ble than orthognathic surgery for correctionf mandibular asymmetry, in that it is chal-
enging to predetermine the precise shape ofhe newly formed regenerate. Distraction os-eogenesis is a dynamic process that requiresareful and precise planning and surgicalechnique to create a regenerate that correctshe mandibular asymmetry.8-11 In contrast,rafting and orthognathic surgery, despiteheir shortcomings, predictably achieve theurgical plan, although in some cases with lesstability.
In the mild-to-moderate (�10 mm) deformi-ies, correction of the asymmetry with conven-ional orthognathic surgery is desirable. In the
ore severe cases in which orthognathic surgery isess practical, distraction osteogenesis becomes thereatment of choice. The distraction regenerate
initiation of distraction, B) Distraction device activation,
or to Reprinted with permission from Elsevier.)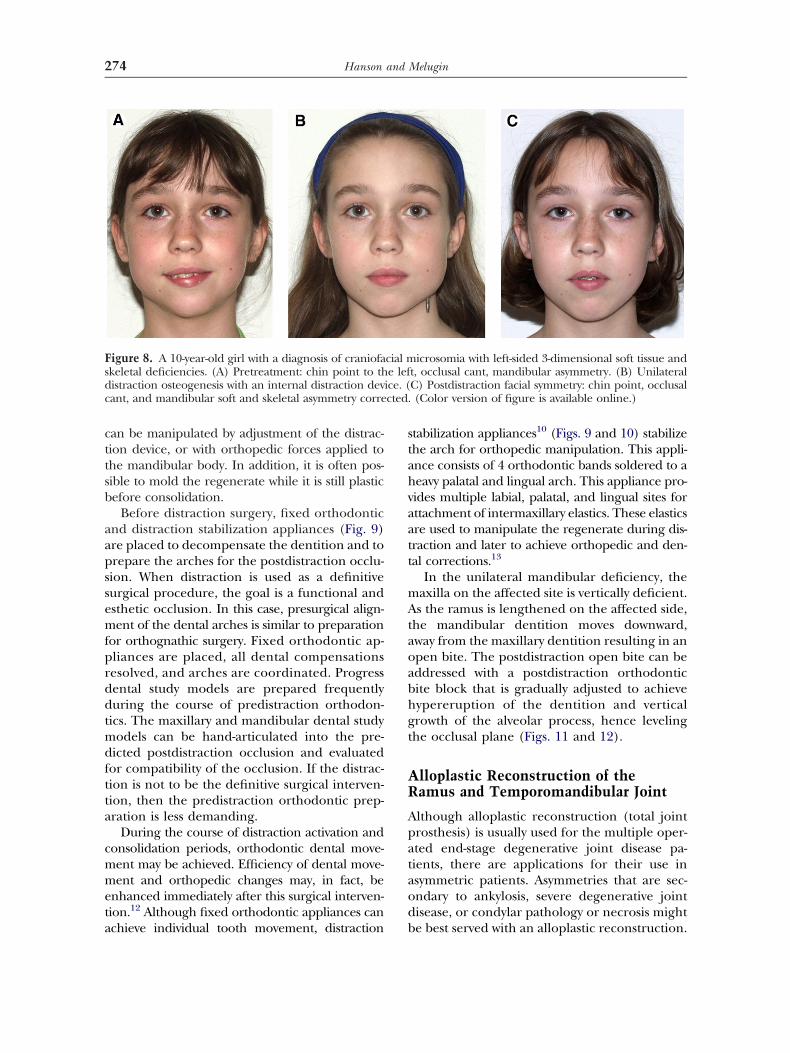
cttsb
aapssemfprddtmdftta
cmmeta
stahvaatt
mAtaoabhgt
AR
Apataod
Fsdc cted.
274 Hanson and Melugin
an be manipulated by adjustment of the distrac-ion device, or with orthopedic forces applied tohe mandibular body. In addition, it is often pos-ible to mold the regenerate while it is still plasticefore consolidation.
Before distraction surgery, fixed orthodonticnd distraction stabilization appliances (Fig. 9)re placed to decompensate the dentition and torepare the arches for the postdistraction occlu-ion. When distraction is used as a definitiveurgical procedure, the goal is a functional andsthetic occlusion. In this case, presurgical align-ent of the dental arches is similar to preparation
or orthognathic surgery. Fixed orthodontic ap-liances are placed, all dental compensationsesolved, and arches are coordinated. Progressental study models are prepared frequentlyuring the course of predistraction orthodon-
ics. The maxillary and mandibular dental studyodels can be hand-articulated into the pre-
icted postdistraction occlusion and evaluatedor compatibility of the occlusion. If the distrac-ion is not to be the definitive surgical interven-ion, then the predistraction orthodontic prep-ration is less demanding.
During the course of distraction activation andonsolidation periods, orthodontic dental move-ent may be achieved. Efficiency of dental move-ent and orthopedic changes may, in fact, be
nhanced immediately after this surgical interven-ion.12 Although fixed orthodontic appliances can
igure 8. A 10-year-old girl with a diagnosis of craniofakeletal deficiencies. (A) Pretreatment: chin point to thistraction osteogenesis with an internal distraction devant, and mandibular soft and skeletal asymmetry corre
chieve individual tooth movement, distraction b
tabilization appliances10 (Figs. 9 and 10) stabilizehe arch for orthopedic manipulation. This appli-nce consists of 4 orthodontic bands soldered to aeavy palatal and lingual arch. This appliance pro-ides multiple labial, palatal, and lingual sites forttachment of intermaxillary elastics. These elasticsre used to manipulate the regenerate during dis-raction and later to achieve orthopedic and den-al corrections.13
In the unilateral mandibular deficiency, theaxilla on the affected site is vertically deficient.s the ramus is lengthened on the affected side,
he mandibular dentition moves downward,way from the maxillary dentition resulting in anpen bite. The postdistraction open bite can beddressed with a postdistraction orthodonticite block that is gradually adjusted to achieveypereruption of the dentition and verticalrowth of the alveolar process, hence levelinghe occlusal plane (Figs. 11 and 12).
lloplastic Reconstruction of theamus and Temporomandibular Joint
lthough alloplastic reconstruction (total jointrosthesis) is usually used for the multiple oper-ted end-stage degenerative joint disease pa-ients, there are applications for their use insymmetric patients. Asymmetries that are sec-ndary to ankylosis, severe degenerative jointisease, or condylar pathology or necrosis might
icrosomia with left-sided 3-dimensional soft tissue andt, occlusal cant, mandibular asymmetry. (B) UnilateralC) Postdistraction facial symmetry: chin point, occlusal(Color version of figure is available online.)
cial me lef
ice. (
e best served with an alloplastic reconstruction.
Tcwagsirlsal
eogatoacasaf
Fict olor
FpscdpR
275Treatment of Mandibular Asymmetries
otal joint prosthesis is an alternative for costo-hondral or sternoclavicular grafting for patientsho require a replacement of large condylend/or ramus segments. Although autogenousrafts confer the ability to grow, they require aecond surgical site for harvest. In the nongrow-ng patient, the alloplastic total joint prosthesisequires no harvest, might better resist reanky-osis (heterotopic calcification), and is not asusceptible to the resorption or failure as can begraft at the site of significant soft-tissue enve-
ope stretch that can occur when trying to re-
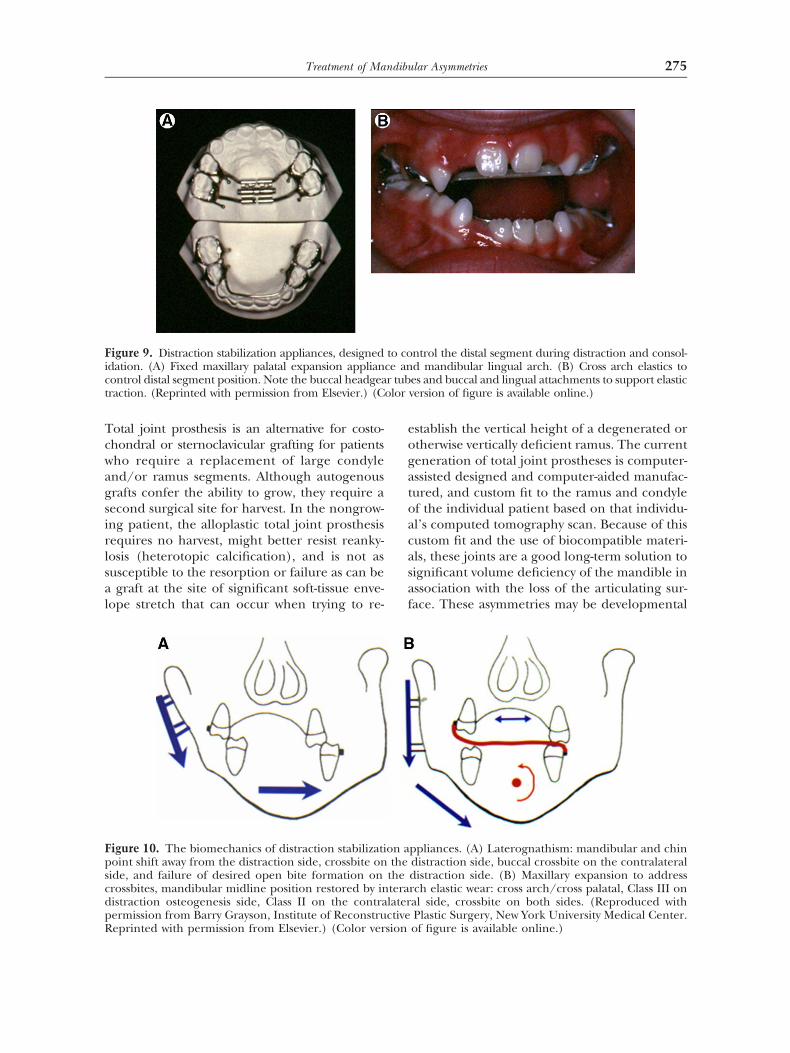
igure 9. Distraction stabilization appliances, designeddation. (A) Fixed maxillary palatal expansion applianontrol distal segment position. Note the buccal headgearaction. (Reprinted with permission from Elsevier.) (C
igure 10. The biomechanics of distraction stabilizatioint shift away from the distraction side, crossbite onide, and failure of desired open bite formation onrossbites, mandibular midline position restored by inistraction osteogenesis side, Class II on the contraermission from Barry Grayson, Institute of Reconstru
eprinted with permission from Elsevier.) (Color versionstablish the vertical height of a degenerated ortherwise vertically deficient ramus. The currenteneration of total joint prostheses is computer-ssisted designed and computer-aided manufac-ured, and custom fit to the ramus and condylef the individual patient based on that individu-l’s computed tomography scan. Because of thisustom fit and the use of biocompatible materi-ls, these joints are a good long-term solution toignificant volume deficiency of the mandible inssociation with the loss of the articulating sur-ace. These asymmetries may be developmental
ntrol the distal segment during distraction and consol-d mandibular lingual arch. (B) Cross arch elastics toes and buccal and lingual attachments to support elasticversion of figure is available online.)
ppliances. (A) Laterognathism: mandibular and chindistraction side, buccal crossbite on the contralateraldistraction side. (B) Maxillary expansion to addressrch elastic wear: cross arch/cross palatal, Class III onal side, crossbite on both sides. (Reproduced withPlastic Surgery, New York University Medical Center.
to coce anr tub
on athe
theteralaterctive
of figure is available online.)

o(tapb
agvn
SPM
CwtrapctqptiAmottiaaitfnitaoeiovc
uccbatbm
Fescomucrpputtobcctcplaa
276 Hanson and Melugin
r secondary to the failure of prior procedureseg, for failed or ankylosed prior rib grafts). Inhe skeletally mature or near skeletally maturesymmetry patient, this form of reconstructionrovides an alternative to distraction and/or
igure 11. An 8-year-old boy with a diagnosis of Gold-nhar Syndrome. (A) Pretreatment findings: right-ided 3-dimensional soft tissue and skeletal deficien-ies, chin point to the right, mandibular midline rightf maxillary dental and facial midlines. (B) Pretreat-ent occlusal cant demonstrating right-sided mandib-
lar vertical and anterior–posterior deficiency andompensatory maxillary vertical and anterior–poste-ior deficiency. (C) Unilateral right distraction deviceositioned perpendicular to the functional occlusallane to provide vertical lengthening of the mandib-lar ramus. Note the correction of the chin point to
he left and correction of the right skeletal and softissue deficiencies and leveling of the mandibularcclusal plane. There is a unilateral open bite createdy the correction of the mandibular vertical defi-iency and the remaining compensatory maxillaryant and vertical deficiency. (D) Postunilateral dis-raction to level the mandibular occlusal plane andorrect the vertical deficiency of the mandible andostorthopedic leveling of the compensatory maxil-
ary occlusal cant by selective eruption and verticallveolar development. (Color version of figure is avail-ble online.)
one reconstruction. Obvious shortcomings of o
lloplasts include infection and/or failed inte-ration, the potential for long-term eventual de-ice failure, and the fact that the alloplast doesot grow, remodel, or adapt.
election of the Proper Surgicalrocedure for the Correction ofandibular Asymmetry
onventional orthognathic surgery, with orithout allogeneic or autogenous interposi-
ional bone grafts, may be indicated for cor-ection of mild to moderate anteroposteriornd vertical deficiencies of the mandible (ap-roximately �10 mm). In the more severeases, interpositional grafting improves long-erm stability. If interpositional grafting is re-uired, bone can be harvested from the sym-hysis, the contralateral ramus, the maxillary
uberosity, the tibia, or calvarium, adding min-mum additional surgical time or morbidity.lternatively, a block of allogeneic materialay be used. Orthognathic surgical correction
f mandibular asymmetry allows immediate in-raoperative assessment and modification ofhe resulting symmetry and occlusion, whereasn distraction osteogenesis these modificationsnd alterations occur during the activationnd consolidation phases.14 In moderate casesn which both orthognathic surgery and dis-raction osteogenesis could be performed, theormer offers several advantages. Orthog-athic surgery achieves the clinical objectives
n a 1-step procedure, whereas distraction os-eogenesis requires an extended period forctivation, consolidation, and surgical removalf the devices. In distraction, there may also bexternal scars and some degree of imprecisionn the correction of mandibular deformity andcclusion. Although orthognathic surgery pro-ides certain advantages in these moderateases, it may be less stable in the long run.
As mentioned previously, osteotomies aresed to reduce hyperplastic structures that areontributing to mandibular asymmetry. Verti-al ramus osteotomies allow setback of theody and ramus and may be completed usingn intraoral, extraoral, and/or endoscopicechnique. Sagittal split osteotomies may alsoe used for the reduction of a hyperplasticandible; however, this procedure for setback
r size reduction exhibits lower long-term sta-
bapp
ati
ioreduw
FboctcttUo
277Treatment of Mandibular Asymmetries
ility because of factors related to techniquend patient selection.4 There is no distractionrocedure for the reduction in size of a hyper-lastic structure.
In addition to ramal osteotomies, segmentalnd symphyseal osteotomies may also be used inhe correction of mandibular asymmetry, provid-
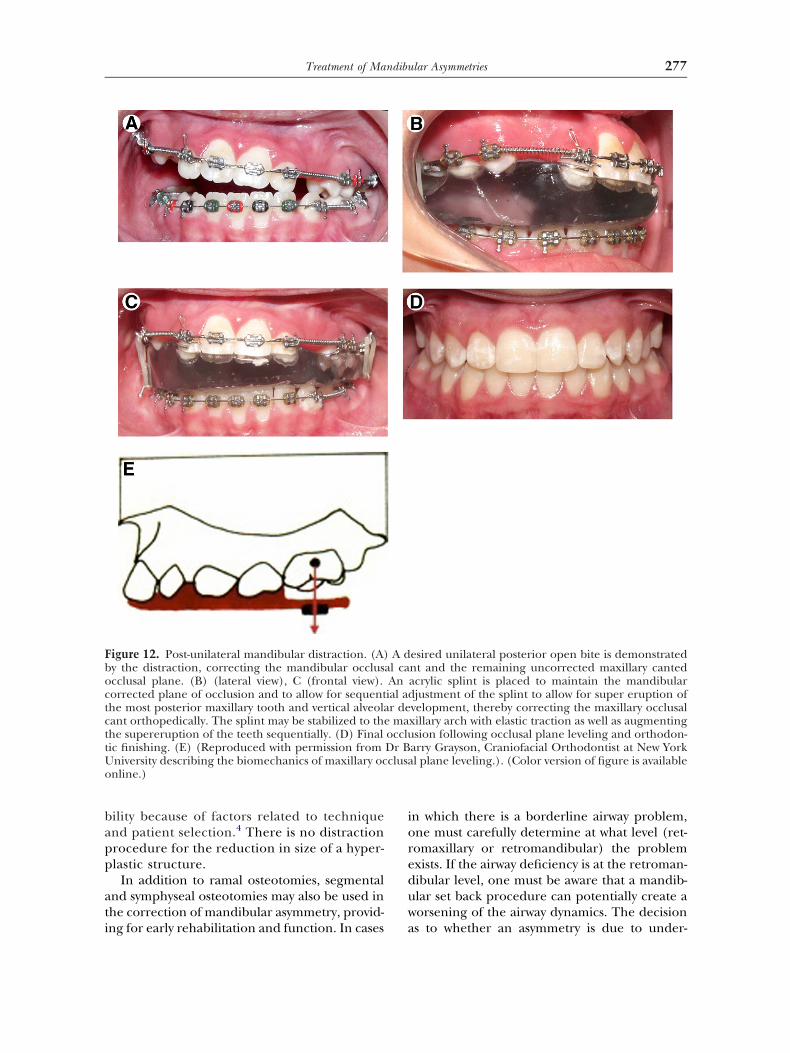
igure 12. Post-unilateral mandibular distraction. (A)y the distraction, correcting the mandibular occluscclusal plane. (B) (lateral view), C (frontal view).orrected plane of occlusion and to allow for sequenthe most posterior maxillary tooth and vertical alveolaant orthopedically. The splint may be stabilized to thehe supereruption of the teeth sequentially. (D) Finalic finishing. (E) (Reproduced with permission fromniversity describing the biomechanics of maxillary ocnline.)
ng for early rehabilitation and function. In cases a
n which there is a borderline airway problem,ne must carefully determine at what level (ret-omaxillary or retromandibular) the problemxists. If the airway deficiency is at the retroman-ibular level, one must be aware that a mandib-lar set back procedure can potentially create aorsening of the airway dynamics. The decision
esired unilateral posterior open bite is demonstratednt and the remaining uncorrected maxillary cantedacrylic splint is placed to maintain the mandibularjustment of the splint to allow for super eruption of
velopment, thereby correcting the maxillary occlusalxillary arch with elastic traction as well as augmentingsion following occlusal plane leveling and orthodon-
arry Grayson, Craniofacial Orthodontist at New Yorkl plane leveling.). (Color version of figure is available
A dal caAnial adr dema
occluDr Bclusa
s to whether an asymmetry is due to under-

gsrrldt
tpui
cf(ioetmpscmtocsgmg
sdaatmsa
ooectedfiT
osong
R
1
1
1
1
1
1
278 Hanson and Melugin
rowth on one side or overgrowth on the otheride is based on careful clinical and cephalomet-ic evaluation. In addition, increased uptake ofadionuclide in the condylar area of the en-arged ramus might be used to corroborate theiagnosis of condylar hyperplasia (nuclear scin-
igraphy or bone scan).For patients with potential concerns related
o sleep-disordered breathing that is at leastartially attributable to decreased airway vol-me, consideration must be given to preserv-
ng airway space.15
In the growing patient, a definitive surgicalorrection is recommended on completion ofacial skeletal growth. However, functionalpsychosocial, airway, speech, swallowing) def-cits often require early surgical (orthognathicr distraction osteogenesis) intervention. Ifarly surgery is indicated, overcorrection ofhe deficient mandible might be recom-
ended to compensate for the innate growthroblem, with the awareness that a secondaryurgical procedure might be needed at theompletion of facial growth. If a decision isade to wait until growth completion, poten-
ial dental and alveolar compensations mightccur. These could be managed orthodonti-ally and orthopedically before the definitiveurgical correction. In addition, some sur-eons consider the sagittal split osteotomyore difficult when performed in a young
rowing child.The correction of mandibular asymmetry
ometimes requires a different surgical proce-ure on each side of the mandible. For example,vertical ramus osteotomy setback on one side
nd a sagittal split osteotomy advancement onhe other may be indicated. Similarly, a rib graft
ight be used to restore length on the deficientide, combined with a sagittal split osteotomydvancement on the contralateral side.
The patient’s needs can be fully addressednly through the effort of a craniofacial orth-dontist operating within the context of anxperienced interdisciplinary team. Theraniofacial orthodontist carefully describeshe skeletal and/or dental deformity, facialsthetics, and the patient’s stage of growth andevelopment. Other members of the team de-ne critical functional and psychosocial needs.
aking the team’s critical evaluation and rec-mmendations into consideration, the skilledurgeon is best able to select among the vari-us surgical options (conventional orthog-athic surgical procedures, distraction osteo-enesis) to meet the patient’s needs.
eferences1. Chang JY, McNamara JA Jr, Herberger TA: A longitudi-
nal study of skeletal side effects induced by rapid max-illary expansion. Am J Orthod Dentofacial Orthop 112:330-337, 1997
2. Gassmann CJ, Van Sickels JE, Thrash WJ: Causes, loca-tion, and timing of relapse following rigid fixation aftermandibular advancement. J Oral Maxillofac Surg 48:450-454, 1990
3. Bays RA, Bouloux GF: Complications of orthognathicsurgery. Oral Maxillofac Surg Clin North Am 15:229-242,2003
4. Serafin B, Perciaccante VJ, Cunningham LL: Stability oforthognathic surgery and distraction osteogenesis: op-tions and alternatives. Oral Maxillofac Surg Clin NorthAm 19:311-320, 2007
5. Tucker MR: Surgical correction of mandibular excess,technical considerations for mandibular setbacks. AtlasOral Maxillofac Surg Clin North Am 1:29-39, 1993
6. Bloomquist DS: Anterior segmental mandibular osteot-omies for the correction of facial-skeletal deformities.Oral Maxillofac Surg Clin North Am 19:369-379, 2007
7. Alexander CD, Bloomquist DS, Wallen TR: Stability ofmandibular constriction with symphyseal osteotomy.Am J Orthod Dentofacial Orthop 103:15-23, 1993
8. Grayson B, Santiago P: Treatment planning and biome-chanics of distraction osteogenesis from an orthodonticperspective. Semin Orthod 5:9-24, 1999
9. Grayson BH, Santiago PE: Treatment planning andvector analysis of mandibular distraction osteogenesis.Atlas Oral Maxillofac Surg Clin North Am 7:1-13,1999
0. Hanson PR, Melugin MB: Orthodontic management ofthe patient undergoing mandibular distraction osteo-genesis. Semin Orthod 5:25-34, 1999
1. Hanson PR: Treatment planning and orthodontic man-agement of patients undergoing mandibular distractionosteogenesis, in Samchukov ML, Cope JB, CherkashinAM (eds): Craniofacial Distraction Osteogenesis. St.Louis, MO, Mosby, 2001, pp 156-167
2. Frost HM: The regional acceleratory phenomenon: areview. Henry Ford Hosp Med J 31:3-9, 1983
3. Hanson P, Melugin M: Orthopedic and orthodonticmanagement of distal segment position during distrac-tion osteogenesis. Atlas Oral Maxillofac Surg Clin NorthAm 16:273-286, 2008
4. Chigurupati R: Orthognathic surgery for secondary cleftand craniofacial deformities. Oral Maxillofac Surg ClinNorth Am 17:503-517, 2005
5. Leighton S, Drake A: Airway considerations in craniofa-cial patients. Oral Maxillofac Surg Clin North Am 16:
555-566, 2005
Related Documents











