STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH TITLE: Research Documentation Last Revised: 5/2017 Prior Version: None SOP NUMBER: SC- 403 Page 1 of 9 Developed by the UH Clinical Research Center SOP Committee 1 1. PURPOSE: To establish documentation standards for clinical research projects to ensure applicable safety, compliance, and billing requirements are met. 2. SCOPE: All entities conducting clinical research within the University Hospitals Health System. 3. RESPONSIBLE INDIVIDUALS: Clinical and research personnel who interact or care for clinical research participants. 4. DEFINITIONS/ACRONYMS: DOS - Date of Service EMR – Electronic Medical Record Enrollment/enrolled - generally means a research subject has been consented and screened, with eligibility verified GCP - Good Clinical Practice. Good Clinical Practice (GCP) is an international ethical and scientific quality standard for the design, conduct, performance, monitoring, auditing, recording, analyses and reporting of clinical trials. It also serves to protect the rights, integrity and confidentiality of trial subjects HIPAA - Health Insurance Portability and Accountability Act ICF - Informed Consent Form ICH - International Conference on Harmonization. Launched in 1990, ICH is a unique undertaking that brings together the drug regulatory authorities and the pharmaceutical industry of Europe, Japan and the United States. Licensed Medical Provider – An individual, such as a, physicians, nurse practitioners, or other health care professional with documented qualifications and/or licensure to perform medical related tasks (i.e. medical exam, review safety reporting, writing orders for procedures, prescribing medications, etc.) Medical Record - Paper or electronic source document repository of care provided to and patient status. Includes, but not exclusive of, the following: Allscripts Sunshine Enterprises [UHCare Ambulatory –Ambulatory Electronic Medical Record (aEMR)] & UHCare Acute– In Patient Electronic Medical Record; Community Record; Ensite; Mosaic (Radiology); Physician Portal Research - A systematic investigation, including research development, testing, and evaluation, designed to develop or contribute to generalizable knowledge. 45 CFR 46.102

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 1 of 9
Developed by the UH Clinical Research Center SOP Committee 1
1. PURPOSE:
To establish documentation standards for clinical research projects to ensure applicable
safety, compliance, and billing requirements are met.
2. SCOPE:
All entities conducting clinical research within the University Hospitals Health System.
3. RESPONSIBLE INDIVIDUALS:
Clinical and research personnel who interact or care for clinical research participants.
4. DEFINITIONS/ACRONYMS:
DOS - Date of Service
EMR – Electronic Medical Record
Enrollment/enrolled - generally means a research subject has been consented and screened,
with eligibility verified
GCP - Good Clinical Practice. Good Clinical Practice (GCP) is an international ethical and
scientific quality standard for the design, conduct, performance, monitoring, auditing,
recording, analyses and reporting of clinical trials. It also serves to protect the rights,
integrity and confidentiality of trial subjects
HIPAA - Health Insurance Portability and Accountability Act
ICF - Informed Consent Form
ICH - International Conference on Harmonization. Launched in 1990, ICH is a unique
undertaking that brings together the drug regulatory authorities and the pharmaceutical
industry of Europe, Japan and the United States.
Licensed Medical Provider – An individual, such as a, physicians, nurse practitioners, or
other health care professional with documented qualifications and/or licensure to perform
medical related tasks (i.e. medical exam, review safety reporting, writing orders for
procedures, prescribing medications, etc.)
Medical Record - Paper or electronic source document repository of care provided to and
patient status. Includes, but not exclusive of, the following: Allscripts Sunshine
Enterprises [UHCare Ambulatory –Ambulatory Electronic Medical Record (aEMR)] &
UHCare Acute– In Patient Electronic Medical Record; Community Record; Ensite;
Mosaic (Radiology); Physician Portal
Research - A systematic investigation, including research development, testing, and
evaluation, designed to develop or contribute to generalizable knowledge. 45 CFR 46.102

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 2 of 9
Developed by the UH Clinical Research Center SOP Committee 2
Source Data - All information in original records and certified copies of original records of
findings, observations, or other activities in a clinical trial necessary for the
reconstruction and evaluation of the trial. Source data are contained in source documents
(original records or certified copies)
Source Document - Original documents, data, and records (e.g., hospital records, clinical
and office charts, laboratory notes, memoranda, subjects' diaries or evaluation checklists,
pharmacy dispensing records, recorded data from automated instruments, copies or
transcriptions certified after verification as being accurate and complete, microfiches,
photographic negatives, microfilm or magnetic media, x-rays, subject files, and records
kept at the pharmacy, at the laboratories, and at medico-technical departments involved in
the clinical trial)
5. POLICY STATEMENT:
Accurate and complete documentation is the cornerstone of Good Clinical Practice (GCP)
and permits an observer to recreate a subject’s participation in a research study and to
account for the use of any investigational products.
Source documentation must be kept in accordance with FDA regulations (21 CFR 11, 21
CFR50.25, 21 CFR 312.62 (b), 21 CFR 812.140 (a) (3) guidelines), Guidance for Industry:
Electronic Source Data in Clinical Investigations, FDA BIMO Chapter 48-Biomedical
Monitoring Program 7348.811, and ICH GCP E6.
6. PROCEDURES:
A. Medical Record Access
1. Access to the medical record is based on job function.
2. If your entity utilizes an EMR, access to the medical record is granted when
an employee’s UH Manager submits an e-security request. The type of access
granted is dependent on the employee’s job function, UH Policy CP-44 -
UHCare Training for Clinical Staff.
3. Training must be completed prior to accessing or documenting in the medical
record. See Training and Job Aids UHCare Home Page
4. Orders can only be written by medically qualified and authorized study
personnel, in accordance with UH Research SOP GA – 104 Scope of Practice.

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH TITLE: Research Documentation
Last Revised: 5/2017 Prior Version: None
SOP NUMBER: SC- 403 Page 3 of 9
Developed by the UH Clinical Research Center SOP Committee 3
B. Research Registration/Scheduling 1. All research subjects seen onsite at UH facilities must be registered and given
a medical record number if they don’t already have one. “Research insurance” must be placed in the primary insurance position for any clinical study-related DOS, in accordance with UH Policy R-2 Patient Billing under Research Grants.
i. The registration process for a new UH patient assigns them a singleunique medical record number in accordance with UH Policy GM-71 – Patient Access Service (PAS).
2. Research related appointments must be scheduled in the hospital or entityscheduling system.
i. Scheduling at University Hospitals Cleveland Medical Center(UHCMC) must occur in Athena and/or Soarian, depending uponwhether technical or professional patient care services will beprovided.
ii. Registration and scheduling instructions are located in Appendix C –“Registration Workflow: Athena/ Soarian Research Documentation”.
C. HIPAA and Research 1. Parts of the Health Insurance Portability and Accountability Act (HIPAA)
regulations are designed to ensure research patients’ privacy and the security of the information we use and retain within UHCMC and regional offices.
2. Researchers accessing, using or retaining protected health information (PHI) ofUHCMC patients must abide by the UHCMC’s HIPAA-related policies.
3. Restricted/Confidential Records follow organizational guidelines for restrictedrecords (i.e., Browns players, public figures, infectious disease and psychiatricpatients).
In accordance with UH Policy GM-61 Accessing Medical Records (Section 12.3 research records), PH-3 - Permitted Uses/ Disclosures of PHI (Section 2.11 – for research), PH-4 Authorizations for Use and Disclosure of PHI (Section 7.1 – Research), PH-23 – Psychotherapy Notes, R-3 Uses & Disclosures of PHI for Research.
E. Research Documents 1. All original source and essential research documents must be retained.
Measures should be taken to prevent any premature or accidental destruction.

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 4 of 9
Developed by the UH Clinical Research Center SOP Committee 4
2. A copy of research records should be maintained in the EMR if applicable per
institutional policy or at the discretion of the investigator to ensure adequate
subject safety.
3. When original observations are entered directly into a computerized system, the
electronic record is the source document. This requirement applies to the
retention of the original source document, or a copy of the source document.
In accordance with UH Policy GM-1 Records Management, ICH E6 4.9.4.b,
21CFR312.62 Investigator Record Keeping and Record Retention – Case histories, FDA
Guidance for Industry - Computerized Systems Used in Clinical Investigations: Source
Documentation and Retention.
D. Required Medical Record Documentation
In accordance with UH Policy CP50 – Worklist Documentation (including eMAR),
UH Policy EMR-1 Integrated Interdisciplinary Documentation and Charting in the
EMR, UH Policy GM-49 Medical Records Completion and UH Policy GM-93 –
Timely Completion of Transactions in the Ambulatory EMR.
1. All clinical study related tasks must be documented on a timely basis by the
clinician and/or delegate who performed the task.
2. Include secondary diagnosis code Z00.6 (research) on billing charge capture
documents for all care provided as documented below.
3. Assure that the following elements are documented in the patient medical
record:
i. Informed consent (IC).
In accordance with FDA 21 CFR 50.27: “Documentation of Informed
Consent”, and UH IRB Policy “Informed Consent”.
The IC process must be documented in the subject’s medical
record.
Refer to Appendix E: UH Clinical Research Tools and Templates
Informed Consent Documentation Checklist Informed Consent
Documentation Checklist for suggested IC process documentation
content.

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 5 of 9
Developed by the UH Clinical Research Center SOP Committee
5
Original fully executed (signed) IC forms must be maintained in
the research records.
A copy of the fully executed (signed) IC document must be added
to a paper medical record or scanned into an EMR.
Refer to UH Policy GM68 - “Medical Record Content”. For
instructions on how to scan see Appendix D: Ambulatory Scan
Job Aid. See EMR Standard Filing Guide Master (The table
provides a roadmap for placement of scanned documents into
folders within the patient’s EMR) and Guide to Clinical Data
Location (Clinical Data Matrix-The ability to connect with patient
data across the UH system and affiliated hospitals is vital to
continuity of care and patient safety. The table provides a roadmap
for patient data by source, type and location.
Any subsequent changes to the IC form must be discussed with the
study subject and the study subject re-consented. This process
must also be documented as a narrative note in the subject’s
medical record, indicating that the subject has been re-consented
and wishes to continue in the study.
Additional versions of the IC document must be maintained as is
the original versions.
ii. Enrollment* note source documentation must contain the following:
Date
Narrative of visit
Phraseology must include the following: “patient has been
enrolled/participating in the (insert IRB approved short study
name) research study” (or “research database” or “research
registry” if applicable) written by or signed by PI or designee.
* “Enrollment/Enrolled" generally means "consented and screened,
with eligibility verified."
iii. Orders
Research study related clinical procedures and tests must be
ordered by a licensed medical provider and documented as a
written order in the study subject’s medical record. In accordance

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 6 of 9
Developed by the UH Clinical Research Center SOP Committee
6
with UH Policies: EMR-2 – Master UHCare Order Management
and MM-2 – Medication Orders.
iv. Administration or Implant of Investigational Product
Drug or biologic administration should be documented by the
person administering item, according to their scope of practice.
Implant of an investigational product must be documented in the
procedure note by a physician.
a. Phraseology must include the following: “Patient met
eligibility requirements and has been enrolled in the (insert
IRB approved short study name) research study and
received (insert investigational device product name).
b. Must include IDE number
When applicable, investigational study medications must be
managed by Investigational Drug Services (IDS) in accordance
with UH Policy: MM-4 - Investigational Drugs.
v. Visit Progress Notes (Initial and follow-up visits)
The Investigator and/or delegate will document progress notes for
each visit the participant makes to the clinic or hospital.
Documentation should include but not limited to the following:
purpose of visit, any ICF changes information, subjects status of
study involvement (i.e. still receiving study medication, not
receiving study medication, terminated from study, etc.), whether
or not the research subject had an adverse event or any health
changes since last study visit, date of next study visit, any other
important information or conversations, and the identity of person
completing the note.
Update any medication changes, enter new vitals, and add/update
any new medical conditions, as necessary.
vi. Telephone Encounter Note
The Investigator or delegate will be expected to document
telephone contact notes for relevant research study related calls to
the participant.
Documentation should include: the purpose of call, information on
whether or not the research subject had an adverse event or any
changes in health since last study visit/telephone call, date of next
study visit, any other important information or conversations, and
the identity of person completing the note.

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 7 of 9
Developed by the UH Clinical Research Center SOP Committee
7
Update any medication changes, and add or update any new
medical information, as necessary.
vii. Investigational Medication or Product Reconciliation
If required by the research protocol, document use, return and
destruction of investigational product in accordance with UH
Policy EMR-3 UHCare Medication Administration Record.
viii. Withdrawal / Early Termination / Study Completion
The Investigator or delegate must document in the subject’s
medical record when a research subject terminates participation in
a research study.
Include all pertinent information for the continuation of care.
Enter a progress note of study termination, document the date and
purpose of the study termination and identify person completing
the note. The EMR must be updated to indicate the research
subject is no longer participating in the research
In accordance with Ohio Code 4731-23-02 - Delegation of Medical
Tasks, UH Policy EMR-2 Master UH Care Order Management
and EMR-3 UHCare Medication Administration Record.
Refer to Appendix A: UHCare Inpatient EMR Workflow and/or Appendix B: UHCare
Ambulatory EMR Workflow on how to complete required steps outlined in section 6D.
7. APPENDICES:
Appendix A: UHCare Inpatient EMR Workflow
Appendix B: UHCare Ambulatory EMR Workflow
Appendix C: Registration Workflow (Athena/Soarian Research Documentation)
Appendix D: Scanning Workflow
Appendix E: UH Informed Consent Documentation Checklist
8. REFERENCES:
DHHS 45 CFR 46: Protection of Human Subjects
EMR Standard Filing Guide Master (Where to file scanned documents in the subjects’ EMR) https://intranet.uhhospitals.org/ClinicalProfessional/PhysicianServices/docs/UHCare_Policies/Sta
ndard_Filing_Guide.xlsx FDA Guidance for Industry: Electronic Source Data in Clinical Investigations
FDA 21 CFR 11: Electronic Records and Electronic Signatures

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH
TITLE: Research Documentation
Last Revised:
5/2017
Prior Version: None
SOP NUMBER: SC- 403 Page 8 of 9
Developed by the UH Clinical Research Center SOP Committee
8
FDA 21 CFR 50.25: Elements of Informed Consent
FDA 21 CFR 50.27: Documentation of Informed Consent
FDA 21 CFR 312.62: Investigator Record Keeping and Record Retention
FDA 21 CFR 812.140: General Responsibilities of Sponsors
GCP ICH E6: 1.51: Source Data
GCP ICH E6: 1.52: Source Documents
Guide to Clinical Data Location (Clinical Data Matrix) (How to connect with patient data across
UH systems and affiliated hospitals for continuity of care and patient safety)
https://intranet.uhhospitals.org/ApplicationsPortal/System/UHCareAmbulatory/docs/Document_
Matrix/ Clinical_Data_Matrix.pdf#search=clinical%20data%20matrix FDA BIMO Chapter 48: Biomedical Monitoring Program 7348.811
Ohio Code 4731-23-02 - Delegation of Medical Tasks
UHCare Link (Information for UHCare training manuals and job aids): https://intranet.uhhospitals.org/ApplicationsPortal/System/UHCare/Training2_Home.aspx
UH IRB Policy: Informed Consent
UH IRB Policy: Records
UH Policy CP-44: UHCare Training for Clinical Staff
UH Policy CP-50: Worklist Documentation (including eMAR)
UH Policy EMR-1: Integrated Interdisciplinary Documentation and Charting in UHCare
UH Policy EMR-2: Master UH Care Order Management
UH Policy EMR-3: UHCare Medication Administration Record
UH Policy GM-49: Medical Records Completion
UH Policy GM-61: Accessing Medical Records (Section 12.3 Research Records)
UH Policy GM-68: Medical Record Content
UH Policy GM-71: Patient Access Service (PAS).
UH Policy GM-93: Timely Completion of Transactions in the Ambulatory EMR
UH Policy MM-2: Medication order
UH Policy MM-4: Investigational Drugs
UH Policy PH-3: Permitted Uses and Disclosures of PHI (Section 2.11 – For Research)
UH Policy PH-4: Authorizations for Use and Disclosure of PHI (Section 7.1 – Research)
UH Policy PH-23: Psychotherapy Notes
UH Policy R-2: Patient Billing Under Research Grants
UH Policy R-3: Uses and Disclosures of PHI in Research
UH Research SOP GA-104: Scope of Practice

STANDARD OPERATING PROCEDURE (SOP) FOR CLINICAL RESEARCH TITLE: Research Documentation
Last Revised: 5/2017 Prior Version: None
SOP NUMBER: SC- 403 Page 9 of 9
Developed by the UH Clinical Research Center SOP Committee
9
APPROVALS
Approved by Dr. Grace McComsey, Associate Chief Scientific Officer, University
Hospitals Health System, Director, UH Clinical Research Center– June 16, 2017

1
EMR Research Work Flow –Inpatient
Version 05/23/2017
Appendix A
Electronic Medical Record
Research Workflow - Inpatient EMR
Patient List Display_____________________________________________________________
Research staff will not see new patient lists. Lists will need to be created via finding a patient, or
via a Criteria List.
Finding a Patient_______________________________________________________________
1. Click the Find Patient icon located on the icon toolbar.
2. Click the Name, Identification, Provider or Other tab.
3. Type your search request. (e.g., Last Name>Smith.)
4. Click Search.
5. Select the patient from the Search Results.
6. Click the Show visit.
7. Highlight the correct visit.
8. Click Save Selected Patients to save to a Personal List.
OR
9. Click OK to save to a Temporary List
Flag a Patient as Research (Adding Research Participant to the Header)______________________
1. Click on the Patient info Tab.
2. Under Data Entry click on Comment.
3. Under the Type choose HEADER 1.
4. Under Comments, type in, Research Participant.
5. Click OK (Research Participant will show up on the Header).
If the patient is no longer in a research study than this will need to be removed from the
Header
2
EMR Research Work Flow –Inpatient
Version 05/23/2017
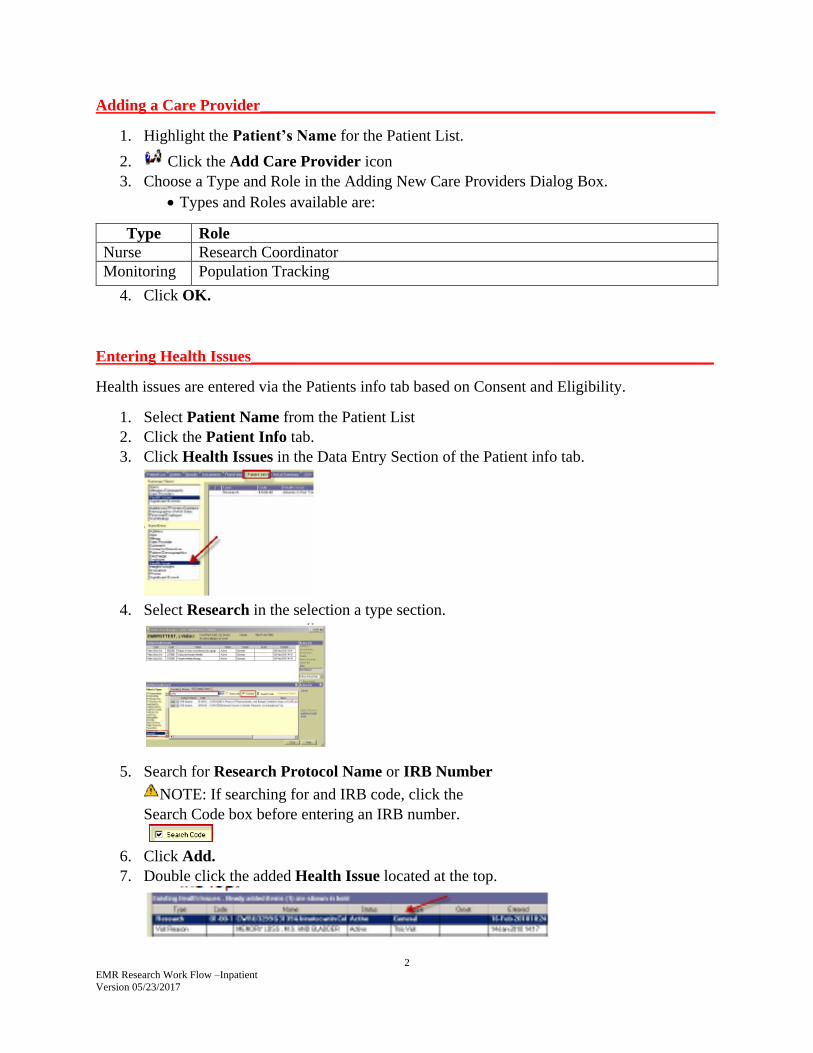
Adding a Care Provider_________________________________________________________
1. Highlight the Patient’s Name for the Patient List.
2. Click the Add Care Provider icon
3. Choose a Type and Role in the Adding New Care Providers Dialog Box.
Types and Roles available are:
Type Role
Nurse Research Coordinator
Monitoring Population Tracking
4. Click OK.
Entering Health Issues__________________________________________________________
Health issues are entered via the Patients info tab based on Consent and Eligibility.
1. Select Patient Name from the Patient List
2. Click the Patient Info tab.
3. Click Health Issues in the Data Entry Section of the Patient info tab.
4. Select Research in the selection a type section.
5. Search for Research Protocol Name or IRB Number
NOTE: If searching for and IRB code, click the
Search Code box before entering an IRB number.
6. Click Add.
7. Double click the added Health Issue located at the top.

3
EMR Research Work Flow –Inpatient
Version 05/23/2017
8. Select the Research Type from the status drop down box.
9. Type any notes that you will need for this s in the Description box.
10. Click Close.
Research Order Entry__________________________________________________________
DCRU Order Set (Only the DCRU nurses can/should document in the DCRU Research section)
Research Workflow
Role Work Flow
DCRU Nurses
Sign into the EMR
Find a Patient
Create patient lists by finding a patient, or by creating Criteria Lists.
Add a Care Provider to each patient.
Add Health Issue to each patient.
Be sure to mark each Health Issue as it is related to the Research Status
Admission Checklist
General Information
Health and Illness
Home Medications/Allergies
Additional information
Vital Signs
Pediatric Assessment
Pediatric Screens
Narrative Notes
All other DCRU Research documentation (physician order, study flow sheets) are
still hard copy source documents
Investigational Medicines
Role WorkFlow
Inpatient
Fax Order to Investigational Pharmacy
Investigational Drug Services (IDS) enters into the system
eMAR – sign off medications
Outpatient Fax Order to Investigational Drug Services (IDS)
eMAR – sign off medications
Other Areas Remains on paper

4
EMR Research Work Flow –Inpatient
Version 05/23/2017
eMAR________________________________________________________________________
The Worklist Manager displays a list of your selected patient(s) tasks and medications for the
displayed period.
Anything currently documented an inpatient medication administration, continue that in EMR.
Outpatients will remain the same for now.
The standard eMAR view timeframes are:
12 hour shift (+2 hours before and 2 hours after)
24 hour shift
8 hour shift (+2 hours before and 2 hours after)
The filters at the top of the window allow you to change the worklist view in a number of ways
to display the information you wish to see. Click the drop-down arrow for the files you wish to
filter and select the appropriate options(s).
Update patient Information______________________________________________________
Research staff will enter or update the following patient information as appropriate:
Allergies
Significant Events
Home Medications
Worklist Manager_______________________________________________________
The Worklist Manager is used to view tasks that have been done and those that need to be done
for patients. This is also where tasks are documented against, such as “marked as done” or “not
done”.
Colors Used in the Worklist Manger
Color Description
Cyan background indicates a continuous task.
Magenta background indicates a PRN task.
Yellow background indicates a scheduled task
Red background indicates an overdue task.
Green background indicates it is an unscheduled task.
Blue background indicates a manual scheduled task.

5
EMR Research Work Flow –Inpatient
Version 05/23/2017
Purple background indicates a conditional order/task.
√ White background and a check mark indicate all occurrences are recorded.
White background without a check mark indicates no occurrence within the designated time frame.
Green trough indicates unscheduled tasks.
Yellow trough indicates provisional tasks where the order was placed after the last scheduled time for
today. The trough enables you to perform the task sometime within the trough time frame if desired.
Magenta trough indicates scheduled or non-scheduled PRN tasks.
White task description cell with a single line through it indicates a discontinued / canceled task.
References____________________________________________________________________
UHCare Training including Job Aids
Training and Job Aid information on UHCARE Acute and Ambulatory settings for allied health,
nurses and physicians/providers.
https://intranet.uhhospitals.org/ApplicationsPortal/System/UHCare/Training2_Home.aspx

1
EMR Research Work Flow – Ambulatory
Version 05/23//2017
Appendix B
Electronic Medical Record
Research Workflow – Ambulatory EMR
Finding a Patient______________________________________________________________________
Application opens to daily schedule, select patient. If patient is not on the schedule, “select patient”, “last
name” or “MRN #” or “DOB”. The clinical desktop = home page for patient chart.
Flag a Patient as Research______________________________________________________________
There are two ways to flag a research subject (please use both ways), from the clinical toolbar:
1. Select the “FYI” icon in the patient banner; enter free text regarding research study. The
FYI button will turn from white to yellow when a comment has been added.
2. Select the “i” icon in the patient banner to “Add an Alert”, select “Research Study Patient”
this will mark an alert in the patient banner in a very noticeable red font. Alerts can be removed
when patient has completed study.
Add Care Provider/Assigning Research Care Provider(s)____________________________________
From the clinical toolbar, select the “i” icon in the patient header, in the demographic section, select
“Patient Care Team” tab. Enter the following: names of the research team caring for the patient (e.g. PI,
Co-I, study coordinator, study nurse…), role, relationship (e.g. research coordinator). Select “Comment”
section to enter additional data or free text (e.g. research study name, IRB number), and contact numbers.
Entering a Health Issues/Research Diagnosis ______________________________________________
From the clinical toolbar, select the “Problem” icon, select “Research” diagnosis code Z00.6. Select
“Comments” section to enter additional data or free text (e.g. study start and stop dates).
Creating a Research Visit and/or Research Telephone Note(s)________________________________
1. For a generic Visit Notes: from the clinical toolbar, select the style as “note authorizing” icon, and
then select a “visit type as “office note” and complete requested details.
2. For a Nursing Visit Note: Select “visit type” as “nursing visit”, and then select the following:
“Nurse Note” - REQUIRES MD/Licensed Medical Provider sign off.
“Nurse Note - Per Protocol” - No need for MD/Licensed Medical Provider signs off but can
forward to doctor, will appear on task list.
Some fields (current medications list, date of birth, allergies) will auto populate.

2
EMR Research Work Flow – Ambulatory
Version 05/23//2017
3. For a Telephone Note – Select “communication” than select “telephone note”.
Research Order Entry________________________________________________________
1. Order Entry: from the clinical toolbar, access the “Add Clinical Item” icon and select the
appropriate tab based on the type of order you wish to enter (i.e. Rx, lab, Proc, Rad, etc.) and
complete requested information.
For research orders, complete the following “Select the order detail tab, scroll down past the
details section to the question section, select “yes” to Research and enter the grant number and
the IRB number of the research study.
3. Resulting Orders: can be documented by selecting the clinical desktop and select the “HMP or
Orders tab" and enter result details.
4. Authorizing Orders – based on your workscope, orders may need to be signed off by the
provider.
5. Orders Completion - may occur automatically or may need to be done manually.
Documentation and Sign Off on Investigational Drugs_______________________________________
There are two places to add medications to the chart, from the clinical toolbar, select:
1. “Rx” tab – Not recommended. This choice sends a message to the physician to approve the
medication
2. “Medical History” tab – Free text box – can add anything, unspecified medication,
investigational product
Select “Unspecified Research Medication” from the medication dictionary. Comments can be added
(e.g. study drug name/placebo).
*Please note, the system cannot check for drug to drug interactions when using medications listed as
“Unspecified Research Medication”.
Scanning of Research Informed Consent and Other Research Document______________________
Scanning documents is a separate application but makes documents available in UHCare. Once
documents are scanned they can be put into patient specific folders. Documents can be filed in the
“Research” or other folders.
Ambulatory Scan Job aid Job aid for scanning documents into the EMR.
https://intranet.uhhospitals.org/ApplicationsPortal/System/UHCareAmbulatory/docs/Provider/ScanGuide
FINAL.pdf
EMR Standard Filling Guide Master The table provides a roadmap for placement of scanned documents into folders within the patient’s EMR.
https://intranet.uhhospitals.org/ClinicalProfessional/PhysicianServices/docs/UHCare_Policies/Standard_F
iling_Guide.xlsx

3
EMR Research Work Flow – Ambulatory
Version 05/23//2017
Guide to Clinical Data Location (Clinical Data Matrix) The ability to connect with patient data across the UH system and affiliated hospitals is vital to continuity of care and patient
safety. The table provides a roadmap for patient data by source, type and location.
https://intranet.uhhospitals.org/ApplicationsPortal/System/UHCareAmbulatory/docs/Document_Matrix/C
linical_Data_Matrix.pdf#search=clinical%20data%20matrix
References___________________________________________________________________________
UHCare Training including Job Aids Training and Job Aid information on UHCARE Acute and Ambulatory settings for allied health, nurses and
physicians/providers.
https://intranet.uhhospitals.org/ApplicationsPortal/System/UHCare/Training2_Home.aspx

Appendix C
Registration for Athena and Soarian

Registration v Scheduling
• Corporate Compliance mandate: all clinical
research participants must be registered with a
MRN
• Outpatient departments register own patients
• At CMC, Patient Access Services (PAS) registers:
– Radiology
– Seidman
– Dahms Clinical Research Unit (DCRU) visits for
both RB&C and Coleman Clinical Research Suite

• Patients must be scheduled for billable
research services
– Hospital/technical (UHC, PMC, SJMC etc)
– Professional (UHMG)
– Not necessary to formally schedule
research personnel time only visits (e.g.
Study Coordinator or research nurse)
Registration v Scheduling – cont.

Research Registration - Athena
Registration team adds research “insurance”

Research Registration - Soarian
9/2014

February 7, 2012
Be the Difference.
Scan 1
UHCare Ambulatory Scan
UHCare Ambulatory Scan Overview
The Scan module is an electronic imaging and chart management application. It is used to transfer written documents such as consults, some test results, journal articles (for reference), and other pertinent chart information into an electronic format.
Scanned documents are indexed to the appropriate patient for the appropriate visit and under the correct document type.
Scanned documents may then be viewed from the Clinical Desktop.

UHCare Ambulatory Scan
Job Aid UHCare Ambulatory 2
Logging In to Scan
1. From the desktop, double-click the UHCare Ambulatory Scan icon.
The UHCare Ambulatory Scan Sign On page displays.
2. Enter your User Name and Password.
Your User Name is your UH Network User ID.
Your initial password is welcome01.
Note ► You must change your password manually the first time you access UHCare Ambulatory Scan by clicking Configure and Change Password.
3. Click Login.
4. Accept the Licensing Agreement, if necessary.
Note ► The User (or User Group) rights govern what is available to the Scan user. Certain buttons or pages may be grayed out or unavailable based on these rights.

UHCare Ambulatory Scan
UHCare Ambulatory Job Aid 3
Searching for Patients in UHCare Ambulatory Scan
1. From the Scan toolbar, select the Search Menu.
2. Select Patient Charts from the drop-down menu.
3. Complete the Patient and Type fields in the Patient Search page.
4. Click Search.
Tip ► Users may search for patients by Name, MRN, DOB, Phone, Other, or Bar Code.
5. On the Pick Patient page, select a patient name.
6. Click Select.
The Patient Chart displays with the Chart Group in the middle of the page.
7. To view a document in a chart, select the appropriate folder from the Chart Group.
8. Double-click the folder to open it.
Notes Regarding Folders
Empty Folders are gray.
Parent folders with content are gray/yellow.
Sub-folders with content are yellow.
System folders have a blue diamond.

UHCare Ambulatory Scan
Job Aid UHCare Ambulatory 4
Batch Scan with Tasking
The Batch Basket workflow is the preferred method when scanning similar document types for multiple patients.
Similar documents may be placed in a pile upon receipt and scanned in as a Batch Basket by anyone at the end of the day. Once all documents are scanned, they must be sorted to the appropriate patient chart.
Recommended batch size is less than 50 pages.
1. From the Scan toolbar, click Batch.
2. Select Scan.
3. From the Batch Scan Documents page, enter a name for the batch.
Note ► Batch names should be intuitive to the document type and contain your 4 letter code for your practice. (This is the same code as entered into ImpactMD and Athena).
Tip ► The Default Document Name and Default Document Date are default values and may be changed while sorting to a patient’s Chart Group folder.
4. Set the Access Group to limit access to this batch to specific groups of users, if necessary.
5. Click Scan to begin scanning the batch.
6. Click Sort to Chart to sort images to patient charts.
7. Manipulate the image as necessary to identify the document type and identify the patient.
8. Enter Name of the Patient (Last Name first) in Patient field.
9. Click Search.
10. Select the patient.
11. Click on ellipsis next to the Current Folder field to display the Folder Tree Window.
12. Click the appropriate folder to file this document.
13. Click OK.
14. Enter the Document Date, if not, enter today’s date.
15. Verify that the owner of the document is the Provider.
UHCare Ambulatory Scan
UHCare Ambulatory Job Aid 5
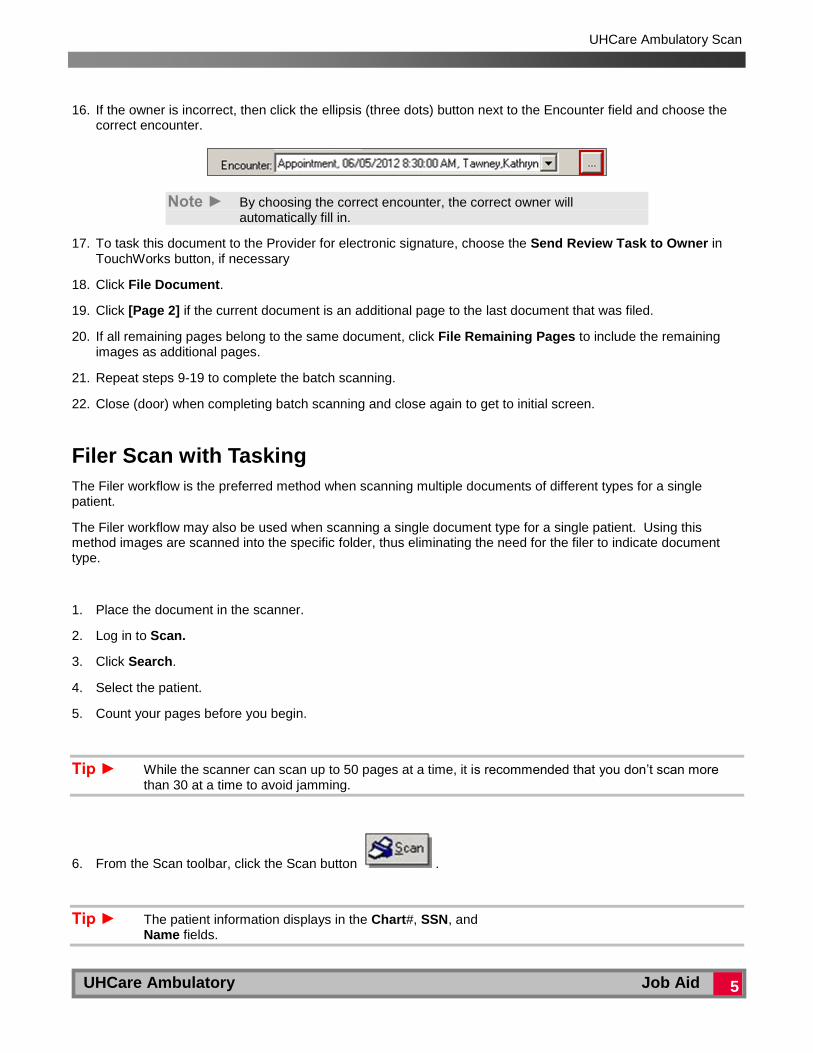
16. If the owner is incorrect, then click the ellipsis (three dots) button next to the Encounter field and choose the correct encounter.
Note ► By choosing the correct encounter, the correct owner will automatically fill in.
17. To task this document to the Provider for electronic signature, choose the Send Review Task to Owner in TouchWorks button, if necessary
18. Click File Document.
19. Click [Page 2] if the current document is an additional page to the last document that was filed.
20. If all remaining pages belong to the same document, click File Remaining Pages to include the remaining images as additional pages.
21. Repeat steps 9-19 to complete the batch scanning.
22. Close (door) when completing batch scanning and close again to get to initial screen.
Filer Scan with Tasking
The Filer workflow is the preferred method when scanning multiple documents of different types for a single patient.
The Filer workflow may also be used when scanning a single document type for a single patient. Using this method images are scanned into the specific folder, thus eliminating the need for the filer to indicate document type.
1. Place the document in the scanner.
2. Log in to Scan.
3. Click Search.
4. Select the patient.
5. Count your pages before you begin.
Tip ► While the scanner can scan up to 50 pages at a time, it is recommended that you don’t scan more than 30 at a time to avoid jamming.
6. From the Scan toolbar, click the Scan button .
Tip ► The patient information displays in the Chart#, SSN, and Name fields.

UHCare Ambulatory Scan
Job Aid UHCare Ambulatory 6
Note ► All documents will be scanned into the To be filed folder. The Document Name and Date fields default to the system date and folder.
7. Select the Duplex option if scanning double-sided documents.
Note ► If using a flatbed scanner, the user is prompted to continue scanning after each page.
8. Click Scan.
Note ► When scanning is complete, the application returns to the patient chart and the To Be Filed folder contains the scan job.
9. Click Filer to file documents to the Chart Group folders for the patient.
10. Manipulate the image as necessary to identify the document type and identify the patient.
11. Confirm that the document type and date are correct.
12. Change the date to match the date of the document being scanned.
Note ► The document date defaults to the scan date.
13. If the document needs to be electronically tasked to the Provider for an electronic signature, complete the following steps:
a. Click New Task (icon with the circular arrow) on the Scan Toolbar
The Create New Task window displays.
b. From the Category drop-down, select Verify or Sign.
c. Click To .
d. In the Type Name field, enter the Provider’s name.
e. Click once on the Provider’s name.
f. Click To-> in the middle.
Note ► The Provider’s name should show on the right side.

UHCare Ambulatory Scan
UHCare Ambulatory Job Aid 7
g. Click OK.
h. In the Reply To drop-down, verify that the sender’s name displays.
i. Enter a short description of the document or message being sent, if desired.
j. Click Send to send the task and return to the Document Viewer.
Note ► Once the task is sent, it displays on the Task List in UHCare Ambulatory for follow-up.
k. Set the status of the task using the buttons at the top of the window:
The default is set to Normal, no icon required.
The red exclamation point denotes Urgent.
The blue arrow means Low Priority.
14. Click the sub-folder button to file the scanned image as the selected document type.
15. Click [Page 2] if the current document is an additional page to the last document that was filed.
16. If all remaining pages belong to the same document, click File Remaining Pages to include the remaining images as additional pages.
Note ► The association between the image and selected document type is not finalized until the page is closed.
Tip ► Any images not filed will remain in the To Be Filed folder.
Searching for a Document in UHCare Ambulatory Scan
1. From the Scan toolbar, select the Search Menu.
2. Select Documents from the drop-down menu.
3. In the Document Search window, enter your search criteria.
The Document tab enables a user to enter document specific search criteria by: Document Number, Document Date, Document Name, Acquire (Scan) Date, Last Change, Chart Group, and Folder.
The Chart tab enables a user to enter patient specific search criteria by: Site, Patient, and Type.
4. Click Search.
5. Click Clear to clear the search tabs and search again.
Tip ► To re-access recent patient charts, from the top toolbar select Chart Lists and then Recent from the drop-down menu.

UHCare Ambulatory Scan
Job Aid UHCare Ambulatory 8
Viewing a Document in UHCare Ambulatory Scan
1. To work with a document in Scan, bring a patient into context.
2. Select the appropriate folder from the Chart Group.
3. Double-click a document to open it in the Document Viewer.
4. To manipulate the scanned image, use the toolbar at the top of the Document Viewer.
Document Viewer Toolbar Options

Informed Consent Documentation Checklist
Protocol Title:
IRB Number: Principal Investigator:
Version 5/2017
Study ID: _______________________ Study Visit Date: _____________________________ (Month /Day/Year)
Date of first contact with participant regarding study: __________________________________
Informed Consent (ICF) Obtained by: ______________________________________________
Date Signed: _____________________ Time Signed: _________________________ (Month/Day/Year) (Military time format)
Individuals present during the informed consent process: ________________________________________
Date and Time research activities began: _____________________________________________________
Did the participant verbalize an understanding of the main purpose Yes No
of the study, procedures, follow-up, risks, etc.)
*If no, what additional procedures were used to ensure understanding? (Please list): ______________________________
The participant was consented in a private location, e.g. exam room, private office. Yes No
*If no, what additional procedures were used to ensure privacy? (Please list): _____________________________________
Were the participant’s questions answered to his/her satisfaction? Yes No
Were others involved in the decision making? Yes No
If yes, who? / Relationship: __________________________________________________________
Was the participant given a current, stamped copy of the ICF? Yes No
Version Date/Number ___________________________ Expiration Date: ________________________________
ADDITIONAL DOCUMENTATION
The participant signed and dated the ICF before any study procedures were performed. Yes No
The participant was given adequate time to review the ICF and ask questions. Yes No
The participant was entered on the Enrollment Log. Yes No
A copy of the consent form is filed in the UH medical record. Yes No
The current UHCMC IRB consent template version is being used and appropriate signature Yes No
blocks are present (i.e., LAR, next of kin, one parent, two parents, etc.)
FORM COMPLETED BY: __________________________________________ DATE: ____________

Master Master
To Be Filed To Be Filed Documents in this folder are not viewable in the EMR
Scanned documents that have not yet been filed
Clipboard Clipboard System folder. Please do not scan
Imported Documents Imported Documents System folder. Please do not scan
HITECH RESTRICTIONS HITECH RESTRICTIONS PHI Restriction Request form
PATIENT NOTES Office Notes Office Notes
ACOG ACOG documentation
Psych Clinical Documents Beck Depression Inventory - pre and post score
Psychological evaluations and documentation
History & Physicals EPSDT form
Growth Chart
History and Physical Exam documentation
Medicare Initial Physical form
Physical Exam form
Well Child Care form
Past Medical History ASQ Information summary
Athena Physical History Form
Gap Survey
Past Medical Information Sheet
Patient Questionnaire
Problem List
Phone Messages Parent Communication Log
Phone message sheet
Phone Messages
Rainbow Advice Center messages
Triage Call Documentation Report/Nurse Triage
Backfill Information Storage area for UHCare Ambulatory backfill forms
Procedure Notes Documentation related to procedures
Urodynamics
Hospital Notes Hospital Notes
Devices Devices other than Cardiac and Hearing Aid
OP Reports OP reports and documentation
H&P (Hospital) H&P documentation
Discharge Summary Patient Discharge Summaries documentation
ED Report ED Visit documentation
Health Maintenance CONNERS/ ADHD Assessment Form
Diabetic Flow SheetHealth Maintenance documentation, such as Logs and wellness documents

NICHQ Vanderbilt Assessment Scale
Vaccine and Immunization forms
Medication Refills Medication Refill requests
Ritalin Summary
Notes/Alerts - Impact MD Notes/Alerts - Impact MD
Chart Notes - ImpactMDChart Notes brought over during ImpactMD conversion. Do not scan
Alerts - ImpactMD Alerts brought over during ImpactMD conversion. Do not scan
Referral/Consult Professional correspondence
Prenatal Do Not Scan into this folder ‐ use ACOG folder
LABORATORY Blood Work Blood Work documentation and results
PT/INR Anticoagulation/Protime Flowsheet
Blood Work documentation and results
Pathology Pathology documentation and results
PAP Pap results
Other Lab ResultsLaboratory documentation and results other than blood work and pathology
Urine Urine results
RADIOLOGY/IMAGING Breast Imaging Breast Imaging images and impressions
CT + CTA CT and CTA images and impressions
Intervential Radiology Interventional Radiology images and impressions
MRA + MRI MRA and MRI images and impressions
Nuclear Medicine Nuclear Medicine images and impressions
Radiography + Fluoroscopy Radiography and Fluoroscopy images and impressions
Ultrasound Aortic or Venous Duplex scans.
Carotid or Vascular reports/studies
PVR – Pulse Volume Recordings
US, Sonograms
Other Radiology *
Drawings/Diagrams Drawings/Diagrams
Tumor Map Tumor Map
DIAGNOSTIC TESTING Cardiovascular Testing Cardiology
Angiogram Angiogram documentation and results
Catheterization Catheterization documentation and results
Doppler Doppler documentation and results
Echo Echo documentation and results

EKG EKG documentation and results
Monitors Cardiovascular Monitoring data and documentation
Stress Test Stress Test documentation and results
CV Devices Cardiovascular device documentation
Initial Interrogation Report
Mechanical Assist Device and Lead Information sheet
PST Meter Training
Pulse Width Threshold Test
Other CardiovascularCardiovascular Testing documentation and results other than those categorized above
Gastro Testing Gastro Testing
Colonoscopy Colonoscopy documentation and results
Endoscopy Endoscopy documentation and results
Barium Swallow Barium Swallow documentation and results
EGD EGD device documentation
Other GastroGastro Testing documentation and results other than those categorized above
Neurology Neurology
EEG EEG documentation and results
EMG EMG documentation and results
Other NeurologyNeurology documentation and results other than those categorized above
Pulmonary Testing Pulmonary Testing
Bronch Bronch documentation and results
Sleep Study Epworth Sleepiness Scale/ ESS
Sleep Questionnaire
Sleep Study documentation and results
PFT/Spirometry PFT and Spirometry documentation and results
Other Pulmonary Pulmonary Testing documentation and results other than those categorized above
Other Testing Speech Therapy
Testing information that doesn't go into any other folder listed.
Voice evaluations
Vision Vision testing documentation and results
Advanced Diagnostic tests Advanced Diagnostic testing information
Audiology Hearing test documentation and results
Hearing Aid/Spec Devices Hearing aid and device information
Cochlear Implant Cochlear Impact information

Allergy Allergy
Skin Testing Skin Testing documentation
Patient Formula Immunotherapy form RX
Patient Formula sheet
Shot Chart Antigen Shot Record
Immuno-Progress sheet
Shot Reaction Record
Venum Shot record
Xolair/ IVIG Xolair/ IVIG forms
PATIENT INFORMATION ABN Patient ABN Consent Forms
Consent Forms Contract for Controlled Substance Prescriptions
Other Patient Consent Forms
DNR/DNI/Directives Advanced Directives
HIPAA HIPAA-related documentation
Living Will Patient's living will
POA Power of Attorney
Registration Forms Patient Registration Forms
ROI Release of Information Forms
Other Patient Information Other patient forms that do not match any of the above folders
CORRESPONDENCE Patient Patient
FMLA FMLA case documentation
Physical Forms Patient Physical documentation
Disability Disability Claim forms and documentation
Insurance Patient insurance documentation
Medical Records/Record ReleasMedical Record Release Forms and requests
Legal Legal forms and documentation
BWC Miscellaneous BWC documents not listed below
C9 C9 Forms
First Report of Injury First Report of Injury Forms
Medco 14 Work Ability Frm Medco 14 Forms
C23 Change Phys of Record C23 Forms
Medco 31 Prior Auth Meds Medco 31 Forms
DOT Forms DOT Forms
BWC Clinical Notes BWC Visit Notes/documentation
MRO Verification MRO Verification Forms
Incident Report BWC Incident Reports

Miscellaneous Miscellaneous Correspondence
Surgery Reservation Request
Rehab/Home Health Home Health Visit Notes
PT/OT
DME Certification DME Certification forms
Multidisciplinary Notes Craniofacial notes
Social Work Social Work
Dietary Dietary
OLD RECORDS OLD RECORDSTransfer records sent from a different practice. Usually proceeded by an Authorization to release information
MISFILED MISFILEDDocuments in the wrong patient's chart that have been electronically signed by the physician

DATA SOURCE DATA TYPEPhysicianPortal
Community Record*
State HealthInformationExchange (HIE)
UHCare Acute EMR
UHCare Ambulatory
EMR
UH PersonalHealth
Record (PHR) OTTR
Demographics (ADT) ‐ Downtime Only x x xAllergies x x x
History & Physical x x xProgress Notes x
Consults x x xDischarge Summary x x x
Oncology Notes (Ambulatory) x x xCoordinated Care Notes x x xMedication Reconciliation x x
C‐CDA x x
CCD x x xOffice Visit,
Health Maintenance,Dietitian, Medicare, PharmD,
PPD Result, Procedure Notes
x x x
Athena Registrations (ADT) x x x x x xCardioLab (PRUKA) Adult Electrophysiology x x x x
CoPath Pathology x x x x x xSyngo Peds ECHO x x x X xEmbla Sleep Lab Studies x xHeartlab Adult Cath/Vascular/Stress x xSyngo Adult ECHO X X X X XIDX Rad Radiology Reports (textual) x x x x x x xMedgis Genetics Reports x x
MedQuist Transcriptions (unsigned) x x x xMeta Demographics, Dx, Px x x x
Meta (eSig) Transcriptions (signed) x x xMuse EKG wave reports x x
Provation GI Documents x x x (select results) x x xSoarian Demographics (ADT) x x x x xSoftlab Lab Results x x x x x x xSoftlab Microbiology x x x x xSpheris Transcriptions x x x x
Viewpoint Ultrasounds x x x
The ability to connect with patient data across the UH system and affiliated hospitals is vital to continuity of care and patient safety. The table below provides a roadmap for patient data by source, type and location. If you have any questions, please contact the Clinical Portals team at [email protected].
DATA RESIDES IN:
UHCare Acute EMR
UHCare Ambulatory EMR
Revised: 10‐15‐15
UHCare Acute EMR
UHCare Ambulatory EMR
UH Ancillary Systems

DATA SOURCE DATA TYPEPhysicianPortal
Community Record*
State HealthInformationExchange (HIE)
UHCare Acute EMR
UHCare Ambulatory
EMR
UH PersonalHealth
Record (PHR) OTTR
DATA RESIDES IN:Revised: 10‐15‐15
Orchard Harvest Lab Results x
McKesson Demographics (ADT) xCerner Lab Results and Microbiology xSeris RIS Radiology Reports X
Dictaphone/Horizon Transcribed Notes X
Demographics (ADT) xRadiology Reports xTranscriptions x
Lab Results and Microbiology x
Soarian Demographics (ADT) xDictaphone Radiology Notes xSiemens EDM Transcriptions x
SoftLab Lab Results and Microbiology x
Demographics (ADT) xRadiology Notes xTranscriptions x
Lab Results and Microbiology x
Demographics (ADT) xLab Results x
Transcribed Notes xMedications x
Demographics (ADT) xLab Results x
Transcribed Notes xMedications x
Demographics (ADT) xLab Results x
Portage Medical Center
Data from Other FacilitiesUniversity Suburban Health Center (Green Rd.)
Parma Medical Center
Mercy Medical Center
Meditech
Meditech
Meditech
Elyria Medical Center
Southwest General Health Center
Cerner
St. Vincent Charity Hospital
St. John Medical Center
Meditech

DATA SOURCE DATA TYPEPhysicianPortal
Community Record*
State HealthInformationExchange (HIE)
UHCare Acute EMR
UHCare Ambulatory
EMR
UH PersonalHealth
Record (PHR) OTTR
DATA RESIDES IN:Revised: 10‐15‐15
Transcribed Notes xMedications x
* In the UHCare Ambulatory EMR, access Community Record by selecting the “Community” button at the bottom on the Clinical Desktop. In the UHCare Acute EMR, select the “Community Record” tab.
Meditech
Related Documents











