1 Physiology and Clinical Benefits of Kinetic Therapy and Prone Positioning Frank Sebat, MS, MD, FCCP Kritikus Foundation · Redding, California

1 Physiology and Clinical Benefits of Kinetic Therapy and Prone Positioning Frank Sebat, MS, MD, FCCP Kritikus Foundation · Redding, California.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Physiology and Clinical
Benefits of
Kinetic Therapy and
Prone Positioning
Frank Sebat, MS, MD, FCCPKritikus Foundation · Redding, California

2
Positional Therapy
• Body movement and frequent posture changes are the norm
• The supine position is uncommon and deleterious
• Patients are nursed in the supine position
Will frequent positional changes > 40° rotationWill frequent positional changes > 40° rotationand proning improve patient outcomes?and proning improve patient outcomes?

3
Immobility Is A Disease
• Skin breakdown
• Atelectasis
• Pneumonia
• Decreased gut motility
• Vascular stasis

4
Standard of Practice for the Treatment of Immobility
• Turning q 2 hours by nursing
– Developed by Dr. Monroe in 1940’s to prevent skin breakdown
– Little evidence regarding pulmonary complications
– Compliance is difficult
– Inconsistency to the degree of rotation

5
Mother Nature’s Answer to Positional Changing
Minimum Physiologic Requirement, Studied and Published by Dr. Francis Keane who developed
the first RotoRest
Minimal mobility requirement = 11.6
minutes

6

7
Defined by the CDC
to be Continuous
Rotation > 40°
Kinetic Therapy

8
Alternatives to Immobility in Critical Care
45°45°

9
Alternatives to Immobility in Critical Care
62°
62°

10
Alternatives to Immobility in Critical Care
248°
248°
A Proning Bed WithKinetic
Therapy

11
A Proning Bed

12
No Proven Outcomes In Rotation < 40°
Witerman, K, et al. Effects of Continuous Lateral Rotation Therapy on Pulmonary Complications in Liver Transplant Patients. American Journal of Critical Care, March 1995; 4:133-139.
N=69
Traver, GA, et al. Continuous Oscillation: Overcome in Critically Ill Patients, Poster presented at the 1993 ALA/ATS International Conference, San Francisco, California.
N=103
Macintyre, N., MD, et al. Automated Rotational Therapy for the Prevention of Respiratory Complications during Mechanical Ventilation. Respiratory Care, December 1999; Vol. 44, No. 12
N=104Macintyre, N., MD, et al. Automated Rotational Therapy for the Prevention of Respiratory Complications during Mechanical Ventilation. Respiratory Care, December 1999; Vol. 44, No. 12

13
45° Combined Kinetic Therapy and Percussion Therapy on the Resolution of Atelectasis on Critically Ill Patients. • Recruitment of Segmental lobar or whole-lung
atelectasis with reduced need for bronoscopy. Raoof, Suhail, MD, FCCP; et al.. CHEST, 1999; 115; 1658-1666.
40-62°Kinetic Therapy in Critically Ill Patients; Combined ResultsMeta Analysis n= 419
• 24% reduction in ICU stay p < .02
• 35% reduction in hours intubated p < .04
• 50% reduction in ICU-acquired pneumonia p < .002
Choi, SC: Nelson. LD.. Journal of Critical Care, March 1992.
Benefit of Rotation > 40°
n=24test-17control-7
14
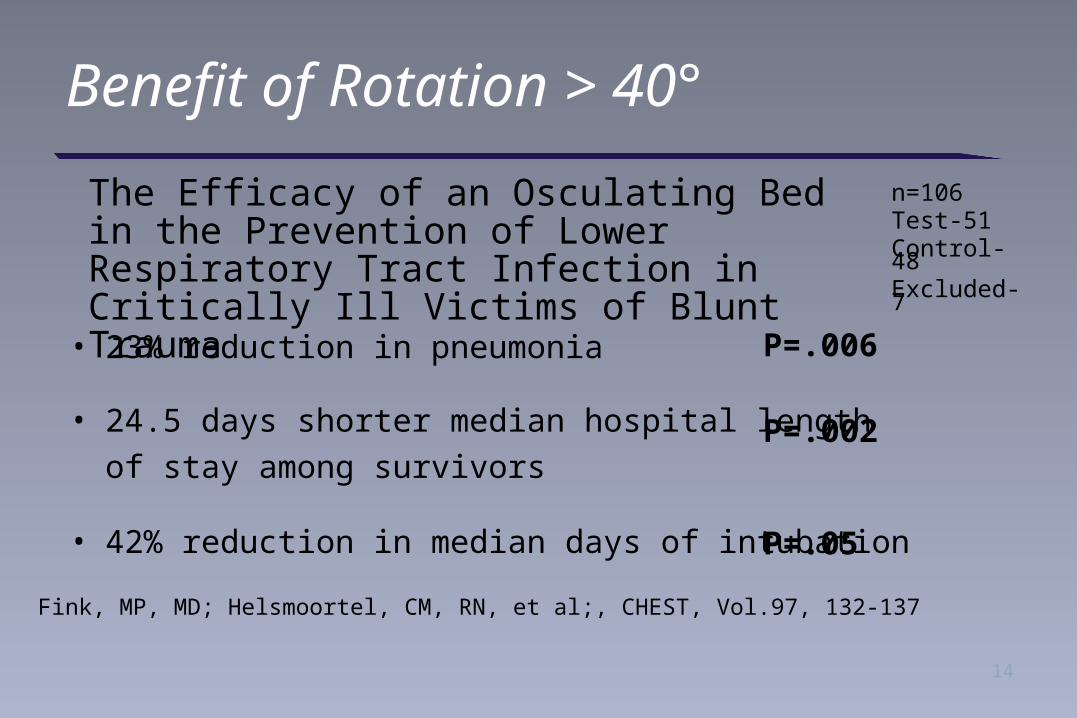
• 23% reduction in pneumonia
• 24.5 days shorter median hospital length
of stay among survivors
• 42% reduction in median days of intubation
Fink, MP, MD; Helsmoortel, CM, RN, et al;, CHEST, Vol.97, 132-137
n=106Test-51Control-48Excluded-7
P=.006
P=.002
P=.05
Benefit of Rotation > 40°
The Efficacy of an Osculating Bed in the Prevention of Lower Respiratory Tract Infection in Critically Ill Victims of Blunt Trauma
15
Physiology of Positional Therapy
• Pleural gradient
– Triangular shape of lung with more mass posterior than anterior
– Position of the diaphragm
– Position of the heart

16
Physiology of Positional Therapy
• Mobilization of secretions
• V/Q matching
• Restriction of anterior chest (proning)

17
Pleural Gradient
-10
0 + 1

18
Proning -- Just Good Horse Sense

19
Pleural Gradient
-10
-5

20
Pleural Gradient
-10
+10 to +15

21
Pleural Gradient
-5 to -10
-5

22
Redding California’s Introduction to Kinetic Therapy 1992
Dr. Johnson’s
ARDS Patient
on RotoRest

23
• Apx. 1000 patients with ALI/ARDS treated with RotoRest with 62° rotation in the last 12 years
– Increase need of sedation
– Minimal to no hemodynamic instability
– RNs request RotoRest prior to physicians
– 14 Intensivists, 90 critical care beds in community all use RotoRest and now RotoProne for management of ALI/ARDS
Redding California’s Experience with Kinetic Therapy 1992-2004

24
Results of Proning Studies
• A large number of small studies demonstrate:
– Improved P/F ratio
– Patient safety
– Requires 4-5 nurses and 1 physician
– Often used as a rescue method when other methods fail
– Convincing data lacking regarding morbidity and mortality
25
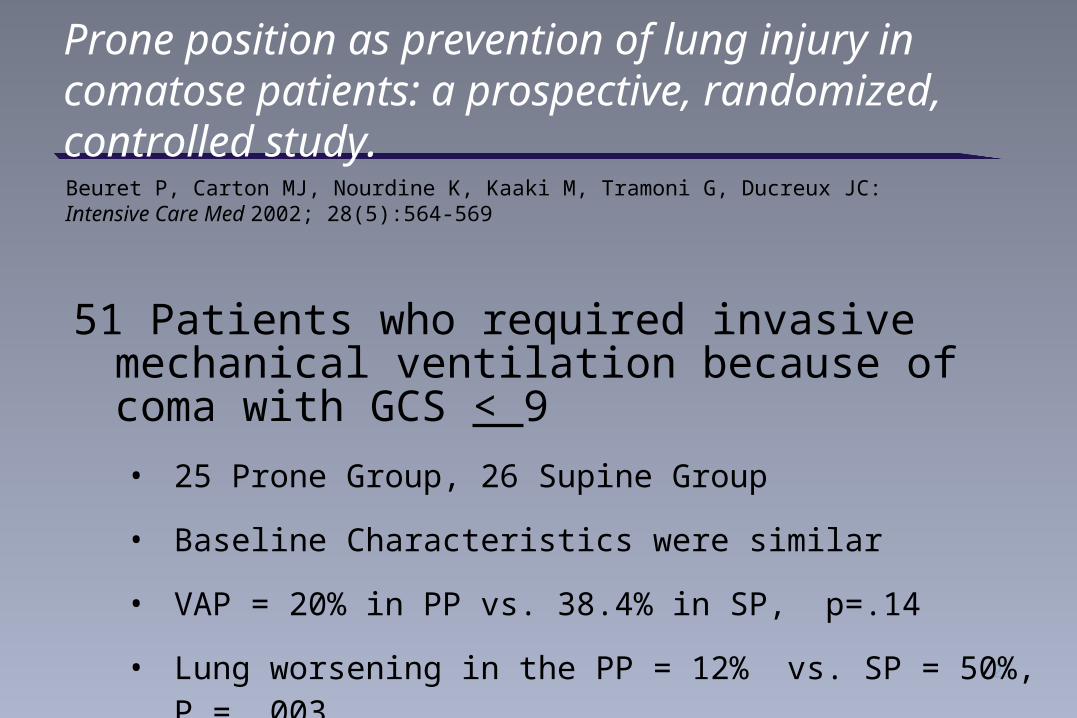
Prone position as prevention of lung injury in comatose patients: a prospective, randomized, controlled study.
Beuret P, Carton MJ, Nourdine K, Kaaki M, Tramoni G, Ducreux JC: Intensive Care Med 2002; 28(5):564-569
51 Patients who required invasive mechanical ventilation because of coma with GCS < 9
• 25 Prone Group, 26 Supine Group
• Baseline Characteristics were similar
• VAP = 20% in PP vs. 38.4% in SP, p=.14
• Lung worsening in the PP = 12% vs. SP = 50%, P = .003

26
Prone vs. Supine Position in ARDS Patients. Results of a Randomized Multicenter Trial[A094] [Poster: 920] J. Mancebo, G. Rialp, R. Fernndez, F. Gordo, R.K. Albert. Hospital de Sant Pau and the Spanish ARDS RCT on PP vs SP, Barcelona, Barcelona, Spain; Denver Health Medical Center, Denver, CO
Supine (n 58) Prone (n 75)
Age 54±17 55±17
SAPS II 38±15 43±15
PaO2 (mmHg) 128±95 108±66
FiO2 .77±.25 .83±.22
PaCO2 (mmHg) 43±11 45±9
Time Proned 0/24 hrs 20/24 hrs

27
Prone vs. Supine Position in ARDS Patients Results of a Randomized Multicenter Trial
[A094] [Poster: 920] J. Mancebo, G. Rialp, R. Fernndez, F. Gordo, R.K. Albert. Hospital de Sant Pau and the Spanish ARDS RCT on PP vs SP, Barcelona, Barcelona, Spain; Denver Health Medical Center, Denver, CO
Supine (n 58) Prone (n 75)
RR (bpm) 19±4 20±4
PEEP (cmH2O) 12±2 12±2
VT (ml/kg) 8.1±1.4 8±1.7
Pplat (cmH2O) 32±4 33±5
ICU Mortality 58.6% 44.4%
Conclusion: A 14.2% absolute and a 25% relative reduction in mortality after adjusting for the difference in severity of illness p=.017

28
Proning Pilot Study
• 19 patients randomized:– 2 hr Sup/ 2hr Pro……………..…..…12 hr prone
– 45 min Sup/ 3 hr 15 min Pro……….19.5 hr prone
• Purpose:– Feasibility– Safety– Segregation of responders
The utility of an automated proning and kinetic therapy-unit with intermediate versus long proning time and its effect on lung recruitment and ventilator days in patients with acute lung injury (ALI)

29
Responds to Proning?

30
Baseline Characteristics of Rotoprone Trial
Group 1
12 hours of proning
Group 2
19.5 hours of proning
p value
Patients 10 9
Age 61 57.8 .70
APS-Day 1 60.9 54.3 .52
APACHE III-Day1 72.7 64.7 .49
LIS 3.2 (10) 3.1 (9) .58
P/F Ratio 125.5 (10) 131.0 (9) .77
Compliance 33.7 (10) 35.3 (9) .77

31
Results
Group 1
12 hours of proning
Group 2
19.5 hours of proningp value
Goal: Proning Time 50% 81.25%
Actual: Time proned 41.7% 63.5%
Hospital length of stay 36.2 29.1 .571
Mortality 40.0% (4) 22.2% (2) .631
Predicted mortality 36% 30%
1After accounting for difference in severity of illness

32
Lung Injury ScoreLung Injury ScoreGroup 1: 12 Hr of proning / 24 hr / 2 hr intervalsGroup 2: 19:30 hrs proning / 24 hrs /:45 m supine vs. 3:15 hr prone
Initial Day Day 3
Group 1
Group 2
2.8
2.3
3.2
3.1
2.0
2.5
3.0
3.5
4.0
P = 0.13

33
P/F Ratio and Compliance
200-
100-
50-
25-
P/F Ratio and ComplianceGroup 1: 12 Hr of proning / 24 hr / 2 hr intervalsGroup 2: 19:30 hrs proning / 24 hrs /:45 m supine vs. 3:15 hr prone
166.7
188.5
125.5
131.0
Initial Day Day 3
Group 1
Group 2
P/F Ratio
31.6
41.0
33.7
35.3
Compliance
P=0.55
P=0.25

34
Bed, Ventilator, ICU Days
Group 1: 12 Hr of proning / 24 hr / 2 hr intervalsGroup 2: 19:30 hrs proning / 24 hrs / :45 m supine vs. 3:15 hr prone1After accounting for difference in severity of illness
5.1
19.9
24.2 23.7
3.7
10.5
15.6
10.9
0
10
20
30
Therapy Unit Days Ventilation Days ICU Length of Stay Ventilation Days of
Survivors
Group 1
Group 2
P value .251 .131 .191 .171

35
Homo vs. Hetero ALI by CT Distribution
Homo1 Hetero2 p value
Patients CT Scans at Enrollment 5 14
APS-Day 1 43.8 62.8
APACHE III-day1 53.8 74.3 .11
Actual Mortality (%, n ) 60.0 (3)21.0
(3) .054*
Repeat CT Findings-Improved 3 of 3 9 of 9
* After accounting for difference in severity of illness1heterogeneous i.e., dorsal consolidation generally with ventral sparing2homogeneous i.e., diffused pan-lung infiltrates

36
Adverse Events
• Facial edema 100%
• Right mid auxiliary line/chest skin breakdown (1 patient)
• Self Extubation (1 patient)
• Poorly functional groining CVVH catheter (1 patient)
• Scleral hemorrhage (2 patients)
• No hemodynamic or respiratory instability requiring discontinuation of proning
• Rapid mobilization of copious endotracheal secretions in patents with pneumonia

At EnrollmentAt 2 Days of Proning
Patient #1

At EnrollmentAt 2 Days of Proning
Patient #1
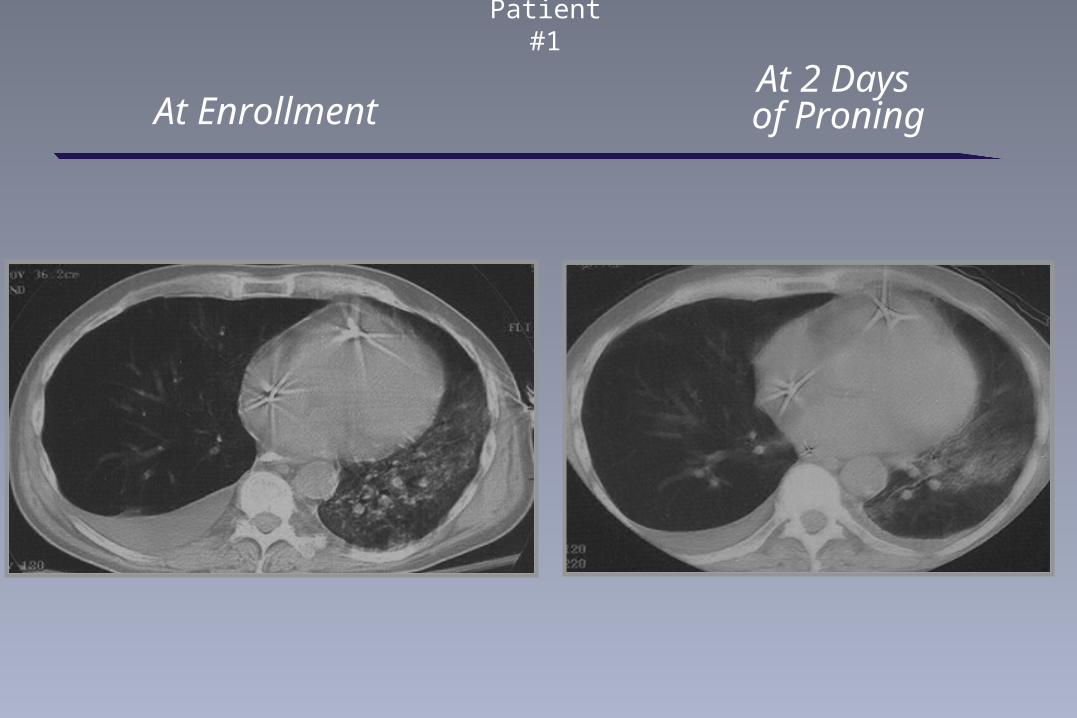
At EnrollmentAt 2 Days of Proning
Patient #1

40
At EnrollmentAt 2 Days of Proning
Patient #2

41
At EnrollmentAt 2 Days of Proning
Patient #2

At EnrollmentAt 2 Days of Proning
Patient #3

43
At EnrollmentAt 2 Days of Proning
Patient #4

44
At EnrollmentAt 2 Days of Proning
Patient #4

45
At EnrollmentAt 2 Days of Proning
Patient #4

46
At EnrollmentAt 2 Days of Proning
Patient #4

47
Before Bed Placement
48 hours After Bed Placement
17 y.o. w/ Tricuspid Endocarditis

48
Before Bed Placement
48 hours After Bed Placement

49
Before Bed Placement
48 hours After Bed Placement

50
Before Bed Placement
48 hours After Bed Placement

Evaluation of Density Area in Dorsal Lung Region During
Prone Position Using Transesophageal Echocardiography
Tsubo T, Yatsu Y, Tanabe T, Okawa H, Ishihara H, Matsuki AUniversity of Hirosaki School of Medicine, Hirosaki, Aomori-ken, Japan

52
AO, ascending aorta CW, chest wall DA, descending aorta
DE, density area ES, esophagus LA, left atrium
LV, left ventricle PE, pleural effusion

53
Transesophageal Echocardiography Image During Prone Position

54
Conclusion: Kinetic Therapy with > 40° Rotation
• Reduction in ventilator associated pneumonia and possibly hospital days
• Reduction in atelectasis and need for bronchoscopy

55
Conclusion: Automated Proning
• Restriction of anterior chest with possible reduction in VILI
• Rapid mobilization of secretions
• Improvement in oxygenation /Rapid recruitment of posterior consolidation
• Accomplished with one nurse
• 20 hrs proning per day well tolerated and trended toward better outcomes compared to 12 /24 hrs

56
Conclusion: Other Possible Benefits
• Reduction of sinusitis
• Reduced skin breakdown
• Increased output from abdominal drains
Related Documents

![MJAT SEBAT: FROM KHEMET & TIMBUKTU A CURRICULUM FOR AFRIKAN DEVELOPMENT [DRAFT]](https://static.cupdf.com/doc/110x72/5477e7b05906b59b318b46ee/mjat-sebat-from-khemet-timbuktu-a-curriculum-for-afrikan-development-draft.jpg)









