1 Pathology of Malaria David P. Humber School of Biosciences University of East London

1 Pathology of Malaria David P. Humber School of Biosciences University of East London.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Pathology of Malaria
David P. HumberSchool of BiosciencesUniversity of East London
2
Learning Outcomes
Know the parasites, vector & epidemiology
Understand of the life cycle Know the principal clinical features
and pathology and the basis of diagnosis
Appreciate the difficulties of control
3
The Problem
At Risk• More than 40% of the world population
Deaths• More than 2 million per year
Chemotherapy• Limited Drugs & drug resistance
Vector control Vaccination

4
The Parasite - Taxonomy
• Phylum - Apicomplexa (Sporozoa)• Class - Haemosporidea (Sporozoea)• Order - Haemosporidia• Genus - Plasmodium
5
Species Infecting Humans
Plasmodium falciparum• Malignant tertian (Cerebral)
Plasmodium vivax• Tertian
Plasmodium ovale• Tertian
Plasmodium malariae• Quartan
Common & Severe
Rare & Mild
6
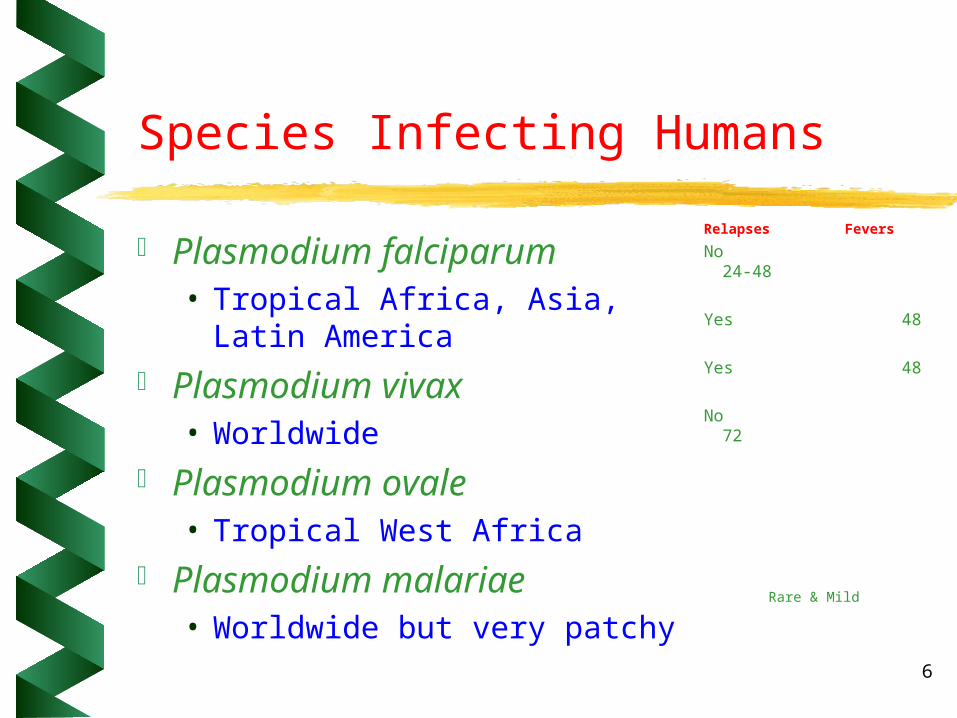
Species Infecting Humans
Plasmodium falciparum• Tropical Africa, Asia, Latin
America Plasmodium vivax
• Worldwide Plasmodium ovale
• Tropical West Africa Plasmodium malariae
• Worldwide but very patchy
Relapses Fevers
No 24-48
Yes 48
Yes 48
No 72
Rare & Mild
7
Epidemiology
>400 million cases annually3 million deaths
majority 2-5 years103 endemic countries
most in Africamost due to P.falicparum
Need 15oCfor 4 weeks <300m64oN to 32oS

8
Distribution of Malaria

9
Life Cycle
Sporozoite Liver Schizont
Oocyst
Ookinete
Trophozoite
Merozoite
Gametocytes
RBC

10
Infected Liver CellHepatocyte
Pre-erythrocytic schizonts

11
Erythrocytic forms (signet)
Young ring form trophozoites
12
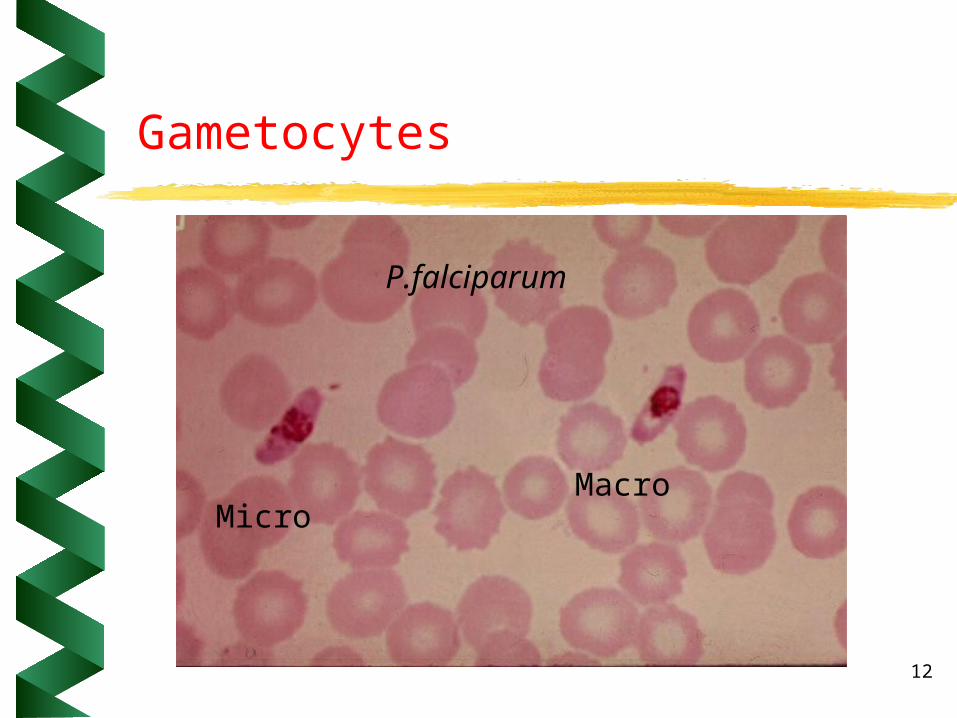
Gametocytes
MicroMacro
P.falciparum

13
Exflagellation
P. vivax produces 8 microgamentes in mosquito’s midgut
14
Clinical Features
Pre-patent Period• Time taken from infection to
symptoms– P. falciparum 6-12 days– P. vivax 10-17days– P ovale 14 days– P. malariae 28-30 days
15
Clinical Features of Malaria
Prepatent period Flu-like initially Intermittent fever Recurrence Coma/death
Chronic infection Relapses
Cold stage hr• Headache/shiver/rapid
weak pulse Hot stage 6hrs
• Intense headache/nausea/thirst/distress
Sweating stage 4hrs• Profuse sweatingSleep!

16
Tertian Malaria - P. vivax & P. ovale
Rarely fatal- relapses common Prodrome
• myalgia, headache, chilliness, low grade irregular fever (no sync maturation cycle)
Synchronisation @ 5-7 days - paroxysms on alternate days
Spleen palpable 10-14 days P. ovale milder with shorter initial
attacks
17
Qartan Malaria - P. malariae
Paroxysms every third day Mildest and most chronic of the 4 immune complex nephropathy seasonal variation with P.f (wet
season)

18
Falciparum Malaria
Cause of virtually all malaria deaths• asynchronous cycle• onset insidious - fever variable• Rapid onset of splenomegaly
Severe anaemia, jaundice, hyperventilation, cns dysfunction (delirium, stupor, coma) . . . . . . . . .

19
Fever Charts

20
Untreated P. falciparum malaria
Sequestration - (schizogony completed)
• Bind to endothelia cells surface receptors eg ICAM1 - via membrane “knobs” with histidine rich protein
• Reduced in some individuals - splenectomy & genetic background
• Clumping also occurs (platelets involved?)

21
Site Specific Sequestration
Brain• measurable reduction in blood flow
Intestines• diarrhoea
Placenta• intervillus space

22
Hepatosplenomegaly
Hepatic dysfunction Hyperplasia of splenic/liver
macrophages Normally transient
• related to parasite load Tropical splenomegally
• Proportion of adult develop very large spleens
• Genotype/IR genes

23
Hepato-splenomegaly
10-15% die - survivors partially immuneoften with splenomegaly

24
Cerebral Malaria
Coma 6- 96 hours• shorter in children
20% fatality Hepatoslenomegaly common Retinal haemorrhages
25
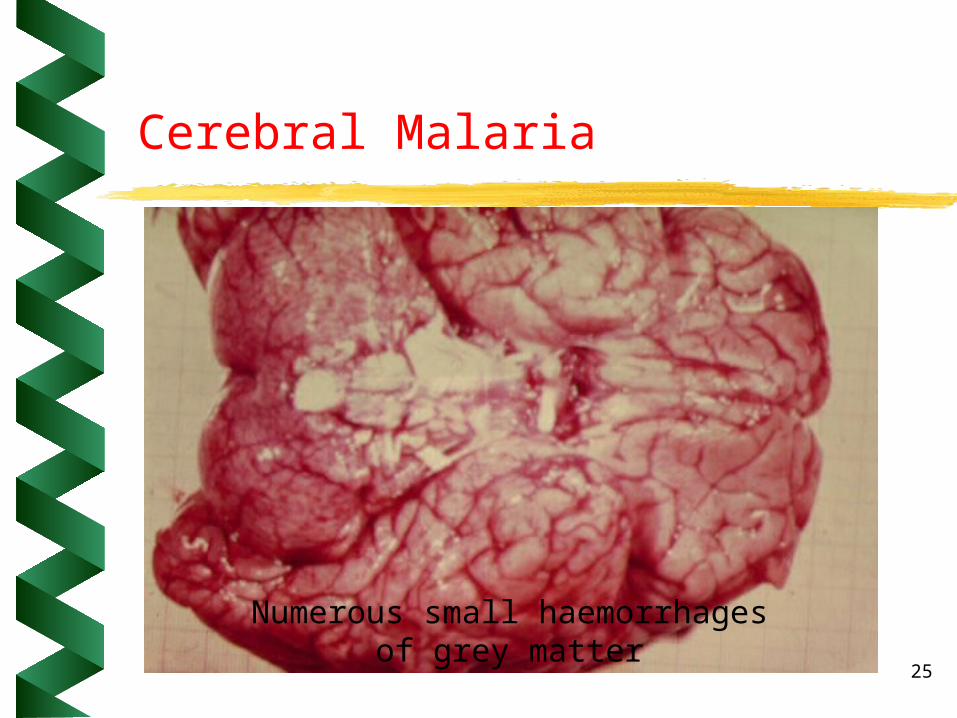
Cerebral Malaria
Numerous small haemorrhagesof grey matter

26
Brain section - P. falciparum
27
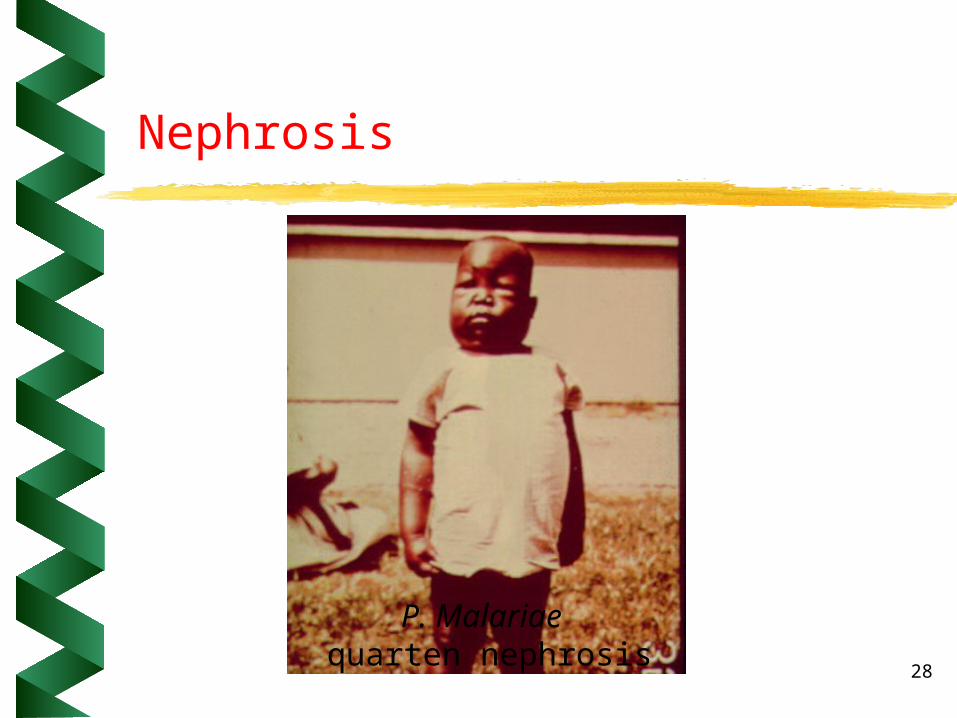
Nephrosis
Renal failure common in adults• poor prognosis
Transient Nephrosis • all species
Nephrotic Syndrome• P. malariae - IC mediated
28
Nephrosis
P. Malariae quarten nephrosis

29
Blackwater Fever
Massive intra vascular haemolysis• haemoglobinuria• acute renal failure
– tubule necrosis
• parasitemia may be absent• nonimmune or G6PD deficiency +
treatment - autoimmuninty? Mortality 20-30%
30
Pregnancy
Serious complication in pregnancy• maternal deaths, foetal death (x10) &
foetal retardation Placental sequestration & clumping
• accumulation of intervillus macrophages & fibrin deposits

31
Section of Placenta

32
Diagnosis
Clinical symptoms– Regular fevers / possible exposure
Stained fixed blood smear– Thick film - presence/absence– Thin film - morphology/species
Blood– Capillary - fluorescence– Antigen capture– PCR/Mabs

33
Chemotherapy
Quinine•Extract of tree bark•used since 17th century•1.3 - 2.0g/day for 7 -10 days•Tonic water!
– Methylene blue– pamaquine– mepacrine

34
Synthetic antmalarials
Chloroquine• Developed by Bayer in 1934 (toxic!)• Rediscoved in the mid 1940’s
– selective uptake by food vacuole– intefers with haem polymersiation/detox
reactive oxygen species
• Resistance in humans early 1960’s

35
Other Antimalarials
Proguanil - 1948 Primaquine - 1951 Pyrimethamine - 1952 Cycloquanil - 1963
Resistant strains by late 1960’s
36
Treatment v Prophylaxis
Monotherapy Treatment
• high dose short term Prophylaxis
• low dose long term

37
Immune Mechanisms
Antibody blocks merozoite infection of RBC’s• passive transfer experiment in the Gambia
Enhance clearance through opsonisation ADCC likely NK activity Decrease in circulating T cells Down regulation of T cell function
Spleen - spleenectomy!

38
Cytokines
IL1
TNF
IL10
39
Stage specific
Anti sporozoite antibodies in adults in endemic areas- blocks liver invasion
Anti sporozoite/merozoite antibodies - block rbc invasion
TNF blocks merozoite development Erythrocyte clearance - liver and
spleen Block cyto-adherence

40
Immunomodulation
Poly clonal T & B activation• auto antibodies - anaemia?
Immunodepression• humoral & cellular - T, B &
macrophage
41
Immunopathology
Fever• correlates with schizont rupture• IL1 & TNF
Anaemia• common complication exceeds
parasitemia & may worsen after treatment
• T cell control of spllenomegally/bone marrow
42
Immunopathology 2
Cerebral malaria• highly reversible• Under T cell control - IL1/TNF
Glomerulonephritis• Not very common - acute nephritis
reversed by treatment• IgM, IgG & C3 - autoimmune?• treatment mediated
Related Documents











