1 Oxygen Delivery Devices and Strategies for H1N1 Patients Pandemic Planning Education Subcommittee October 2009

1 Oxygen Delivery Devices and Strategies for H1N1 Patients Pandemic Planning Education Subcommittee October 2009.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Oxygen Delivery Devices and Strategies for H1N1 Patients
Pandemic Planning Education Subcommittee October 2009
2
Outline
Introduction
Oxygen Delivery Devices
Optimization of Oxygenation
3
Introduction
Oxygen is a drug– Has a Drug Identification Number (DIN)– Colorless, odorless, tasteless gas– Makes up 21% of room air– Is NOT flammable but does support combustion.

4
Indications for Oxygen Therapy
Hypoxemia– Inadequate amount of oxygen in the blood
– SPO2 < 90%
– PaO2 < 60 mmHg
Excessive work of breathingExcessive myocardial workload
5
What does hypoxemia look like?
TachycardiaAgitationDiaphoresisCyanosis
*Tachypnea*DyspneaAccessory
muscle use
*Adult response – pediatric and neonatal patients experience bradycardia
6
Hazards of Oxygen Therapy
Absorption atelectasis– Likely with high FIO2 in presence of partial or
complete small airway obstruction
Oxygen toxicityRetinopathy of prematurityOxygen induced hypoventilation
– Rare condition manifesting in some COPD patients with chronic high plasma bicarbonate
7
Oxygen Therapy Devices2 Types
Fixed– A device that meets all the patients inspiratory flow
demands.– Designed to deliver a specific oxygen concentration to
patientVariable
– Does not meet all inspiratory demands of the patient so some room air is breathed in
– Oxygen concentration will vary with changes in the depth and rate of breathing
– in general, the oxygen concentration is by the size of the reservoir
8
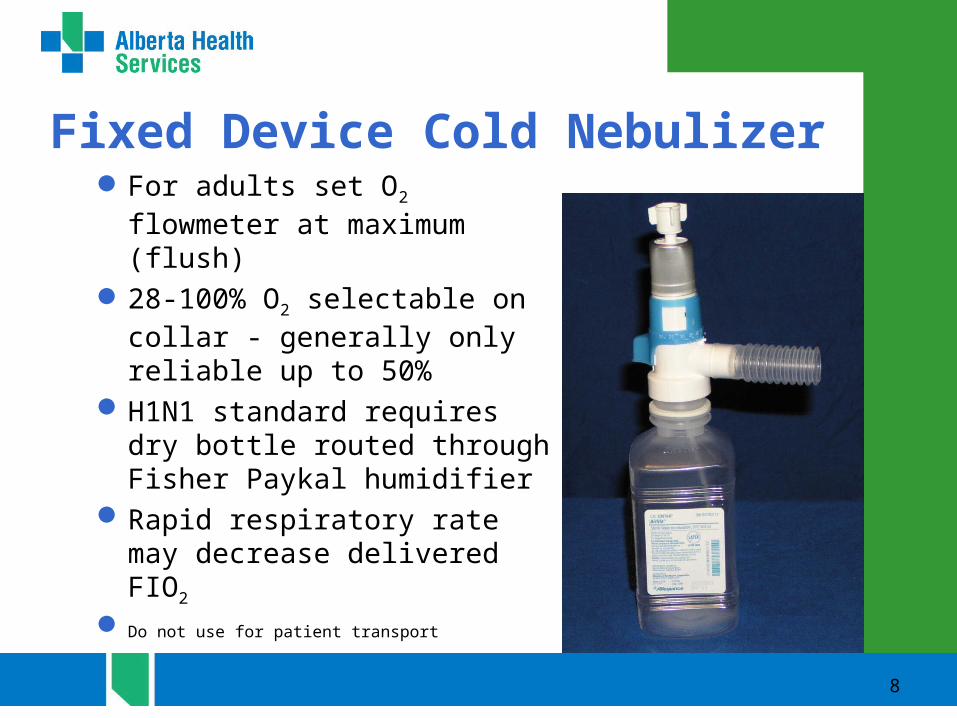
For adults set O2 flowmeter at maximum (flush)
28-100% O2 selectable on collar - generally only reliable up to 50%
H1N1 standard requires dry bottle routed through Fisher Paykal humidifier
Rapid respiratory rate may decrease delivered FIO2
Do not use for patient transport
Fixed Device Cold Nebulizer
9
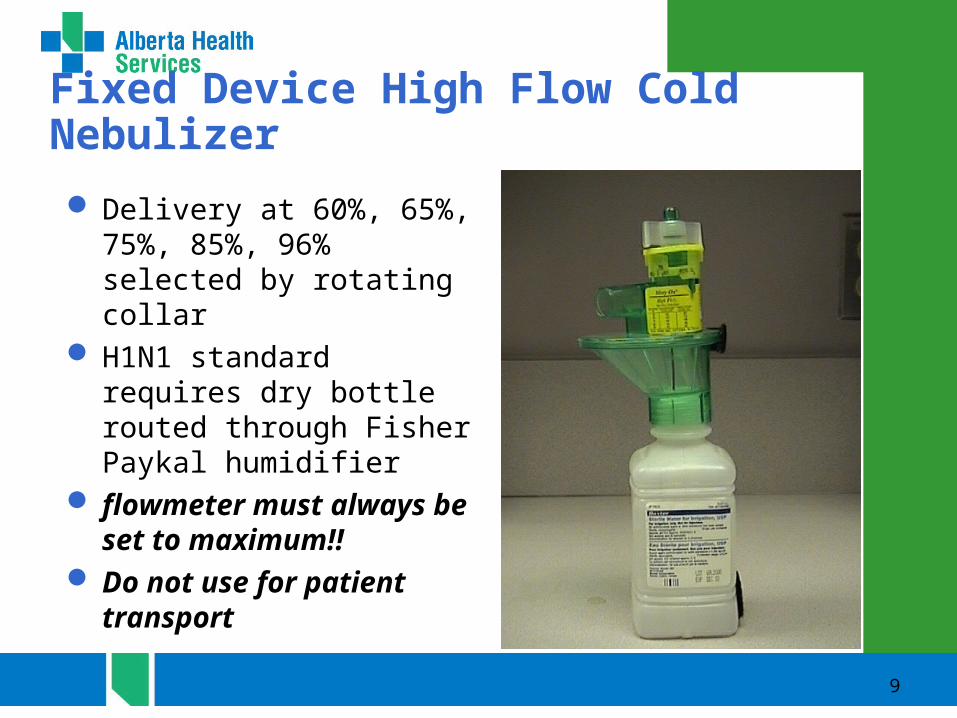
Fixed Device High Flow Cold Nebulizer
Delivery at 60%, 65%, 75%, 85%, 96% selected by rotating collar
H1N1 standard requires dry bottle routed through Fisher Paykal humidifier
flowmeter must always be set to maximum!!
Do not use for patient transport
10
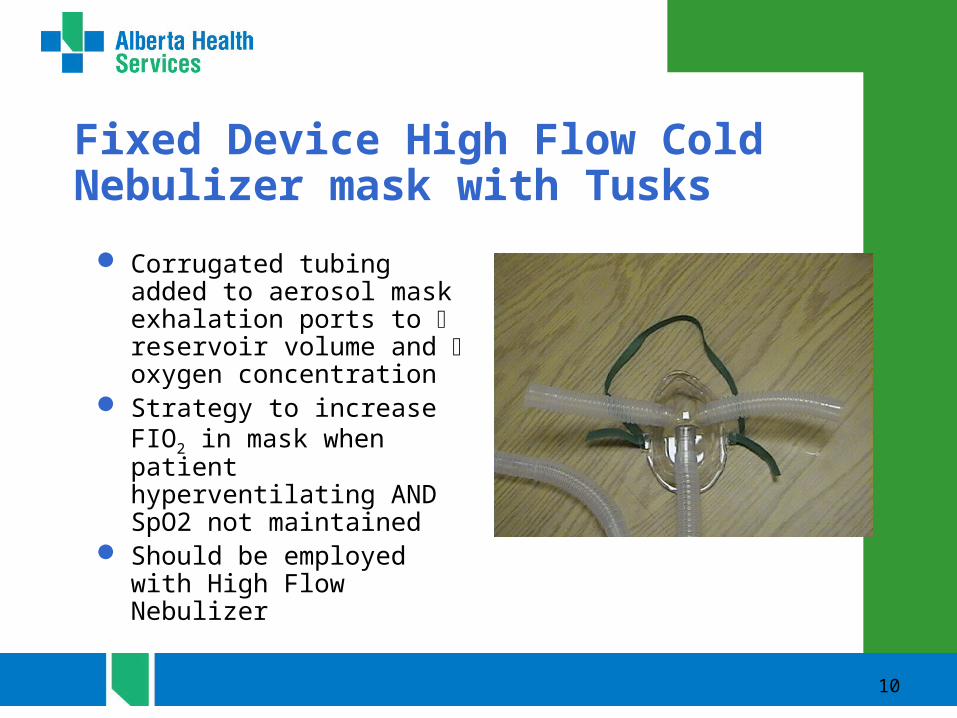
Corrugated tubing added to aerosol mask exhalation ports to reservoir volume and oxygen concentration
Strategy to increase FIO2 in mask when patient hyperventilating AND SpO2 not maintained
Should be employed with High Flow Nebulizer
Fixed Device High Flow Cold Nebulizer mask with Tusks

11
Face Tent
Use with a cold nebulizerThe “tent” portion is
directed upwardsUses: children and any
patients who find mask claustrophobic or have had facial/nasal surgery
Not optimal for high FIO2 requirements
12
Tracheostomy Collar
Provides humidity & oxygen for tracheostomy patients via cold neb
adults - 10-15 LPM up to ‘flush’
O2 adjusted on cold neb but maximum is usually 50%
13
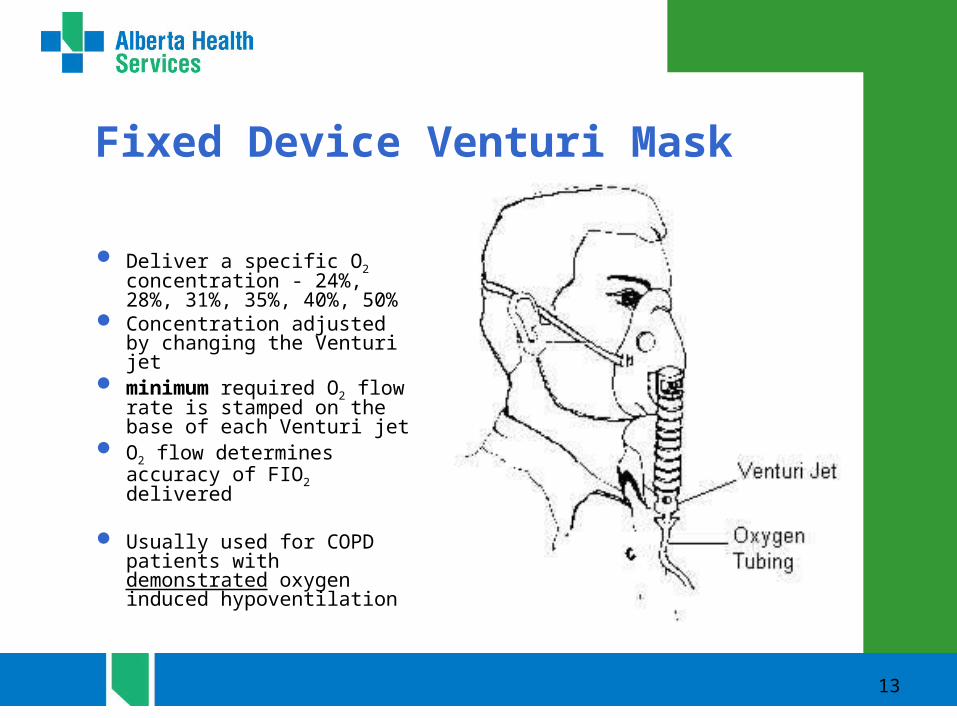
Deliver a specific O2 concentration - 24%, 28%, 31%, 35%, 40%, 50%
Concentration adjusted by changing the Venturi jet
minimum required O2 flow rate is stamped on the base of each Venturi jet
O2 flow determines accuracy of FIO2 delivered
Usually used for COPD patients with demonstrated oxygen induced hypoventilation
Fixed Device Venturi Mask
14
Variable Flow Nasal Cannula
22% - 40% Stable is FIO2 based on:
– Respiratory rate– O2 flowrate– Reservoir capacity of
nasopharynx adults 6 LPM infants/toddlers 2 LPM children 3 LPM FIO2 is not affected by
mouth breathing
15
Flow rates from 6-15 LPMFor patients that require >
6 LPM O2 but cannot tolerate a mask
Larger tubing inner diameter permits higher O2 flow
Tubing is always green
Variable Device High Flow Nasal Cannula

16
Flow rate of 5-10 LPM35% -50% O2
O2 flow and respiratory rate determine stability of delivered FIO2
CAUTION Set flow rate must be > 5 LPM (adult and children) to flush exhaled carbon dioxide from mask
Variable Device Simple Oxygen Mask
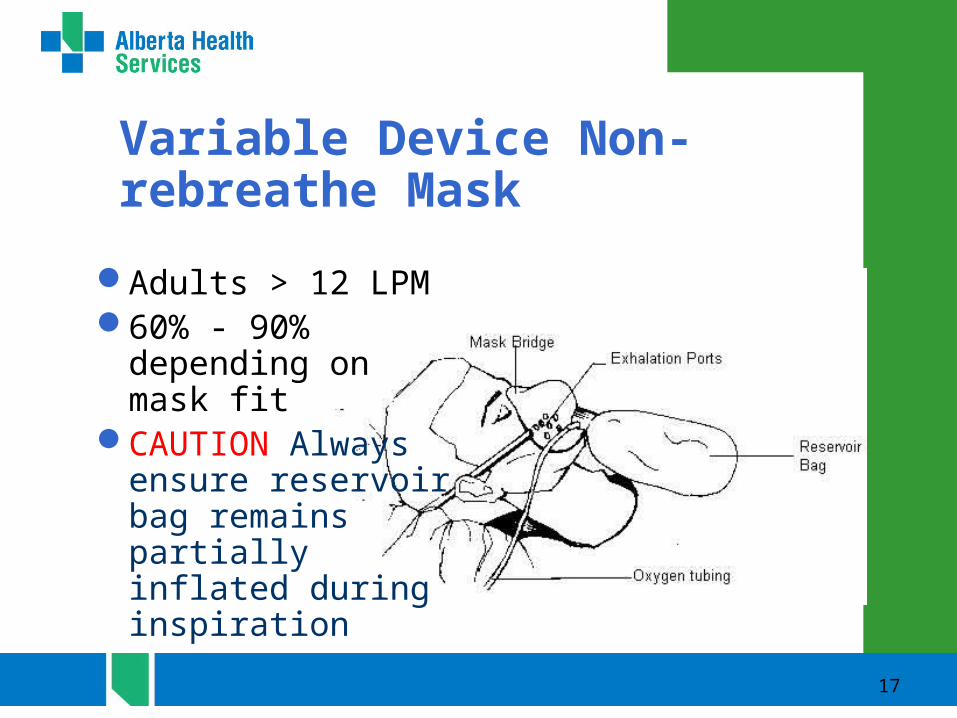
17
Adults > 12 LPM60% - 90%
depending on mask fit
CAUTION Always ensure reservoir bag remains partially inflated during inspiration
Variable Device Non-rebreathe Mask

18
CAUTION Always ensure reservoir bag remains partially inflated during inspiration Ensure bag does not deflate during inspiration
Valving system directs exhaled gas through bacterial filter
May be used for transport of H1N1 isolation patients
Must be assembled from stock Y’s, one way valves
Variable Device Non-rebreathe Mask with Filter
19
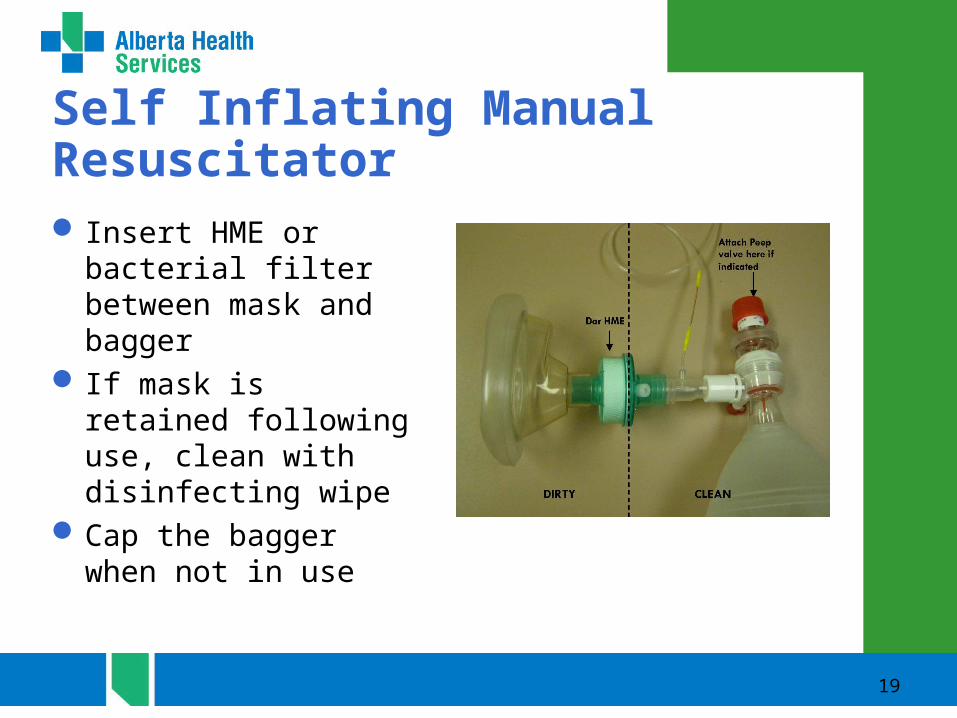
Self Inflating Manual Resuscitator Insert HME or bacterial
filter between mask and bagger
If mask is retained following use, clean with disinfecting wipe
Cap the bagger when not in use

20
Manual VentilationFor Respiratory Arrest:
– Deliver 1 breath every 5 to 6 seconds (10 to 12 breaths per minute).
– For cardiac arrest deliver 2 breaths after every 30 compressions - deliver 8 to 10 breaths per minute without interrupting CPR once airway secured
– Ensure that you have attached the EtCO2 sampling line to the correct port on the HME. The EtCO2 sampling port has ridges to screw on the sampling line male

21
Avoid hyperventilation which may result in:
– Impaired hemoglobin function with reduced O2 delivery to tissues
– Gastric distension– Increased intra thoracic pressure causing:
– decreased venous return to the heart and diminished cardiac output.
– Increased intracranial pressure

Complications
Gastric distension is the most common adverse event in manual ventilation
Distension may impair lung expansionPalpate the abdomen at commencement of
baggingWatch for visual distension and recheck
palpation - request gastric tube placement if abdominal rigidity is noted
22
23
Optimization of Oxygen Therapy
24
Hypoxemia
Hypoxemia is defined as:– Low levels of oxygen in the blood
PaO2 of less than 60 mmHg (moderate)
SpO2 of less than 90%
25
Manifestations of Hypoxemia
Hypoxemia will affect vital signs by:– Increased heart rate– Increased blood pressure– Increased respiratory rate– CAUTION tachycardia is the adult response to hypoxemia –
children and neonates will react to hypoxemia with bradycardia that may rapidly deteriorate to cardiac arrest
– Hypoxemia in neonates and children requires rapid intervention and correction

Hypoxemia and H1N1
Decompensation in hospitalized H1N1 Patients often begins with a decrease in SpO2 and increased oxygen demand
Be alert - and communicate even minor increases in oxygen flows or requirements for higher FIO2 devices
26
27
Causes of Hypoxemia
Shunt Hypoventilation
– As carbon dioxide increases oxygen falls V/Q mismatching (ventilation/perfusion) serious complications
of H1N1 produce V/Q mismatch– Pneumonia– Pulmonary edema– ARDS
Increased diffusion gradient– asbestosis– Early pulmonary edema
28
Oxygen Therapy
Goal of therapy is an SPO2 of >90% or for documented COPD patients 88–92%
As SPO2 normalizes the patients vital signs should improve”– Heart rate should return to normal for patient– Respiratory rate should decrease to normal for patient– Blood pressure should normalize for patient
29
Optimization
My SpO2 is < 90%, what next?– Is the pulse oximeter working/accurate
Do I have a good signal?Heart rate plus/minus 5 bpm?Is there adequate perfusion at the probe site?Can the probe be repositioned?Do other vital signs or clinical manifestations give
evidence of hypoxemia?

30
Optimization cont.
Check my source!– Ensure the O2 delivery Ensure the O2 delivery
device is attached to device is attached to oxygen not medical air.oxygen not medical air.
– Follow tubing back to Follow tubing back to source and ensure source and ensure patencypatency
– Are all connections tight?Are all connections tight?
Is the flow set high Is the flow set high enough?enough?– All nebs especially high All nebs especially high
flow large volume nebs flow large volume nebs need to be run at the need to be run at the highest rate.highest rate.
– Turn flow meter to Turn flow meter to maximum for large maximum for large volume nebs.volume nebs.
31
Optimization cont.
Reposition patient.– Avoid laying patient flat
on back.– Raise head of bed.– Encourage deep
breathing/coughing
Listen to chest.– Wheezing?
Do they need a bronchodilator?
– Crackles?Encourage deep
breathing/cough.Are they fluid
overloaded?
32
Optimization cont.
Can I improve the mechanics of breathing?– Patient position
– Pursed lip breathing
– Abdominal breathing.
– Anxiety relief?

33
Optimization cont.
Increase the flow:– With nasal prongs, increase the flow rate by 1 -2
lpm increments until target SpO2 is reached.– High flow nasal prongs can be maximally set at
15 lpm.– Call for physician assessment Medical if high
oxygen flows are required.
34
Optimization cont.
What do I do if my patient is really hypoxemic (on low flow oxygen)?– Assess patient to determine cause of increasing oxygen
requirements.– Best short term solution is non-rebreathe mask at 15 lpm.
(reservoir stays inflated)– Goal saturation is still 88 – 92%.– Increase flow as required until re-assessed by physician
35
Optimization cont.
What do I do if my patient is really hypoxemic (on high flow oxygen)?– Assess patient to determine cause of increasing
oxygen requirements.– Adjust FIO2 upwards in 10% increments titrating
for target SPO2.– Call physician for further assessment

H1N1 points of emphasisH1N1 decompensation requiring ICU
admission usually begins with a systemic inflammatory response and pulmonary edema
CXR may not correlate with degree of oxygenation impairment
Gradually increasing oxygen requirement is a sentinel sign of impending respiratory failure
36

H1N1 points of emphasis
H1N1 Patients with escalating O2 needs warrant frequent monitoring for signs of impending respiratory failure
If a critical care triage system is operative, know the patient’s classification and prepare equipment accordingly – endotracheal intubation may not be an option
37
Related Documents











