1 Adverse Event Review as Mandated by the Best Pharmaceuticals for Children Act Presented at the Psychopharmacologic Drugs Advisory Committee & Pediatric Subcommittee of the Anti- Infective Drugs Advisory Committee Meeting February 2, 2004 Solomon Iyasu, MD, MPH Hari Cheryl Sachs, MD, FAAP Division of Pediatric Drug Development Center for Drug Evaluation and Research Food and Drug Administration

1 One Year Post Exclusivity Adverse Event Review as Mandated by the Best Pharmaceuticals for Children Act Presented at the Psychopharmacologic Drugs Advisory.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
One Year Post Exclusivity Adverse Event Review as Mandated by the
Best Pharmaceuticals for Children Act
Presented at the Psychopharmacologic Drugs Advisory Committee
& Pediatric Subcommittee of the Anti-Infective Drugs Advisory Committee Meeting
February 2, 2004
Solomon Iyasu, MD, MPHHari Cheryl Sachs, MD, FAAPDivision of Pediatric Drug DevelopmentCenter for Drug Evaluation and Research Food and Drug Administration

2
Best Pharmaceuticals for Children Act (BPCA)
Jan 4, 2003
• Section 17: Adverse Event (AE) Reporting– review all AEs for one year after granting
pediatric exclusivity– report to the Pediatric Advisory Sub-Committee
for review

3
Data Source for Drug Adverse Data Source for Drug Adverse EventsEvents
• FDA’s Adverse Event Reporting System (AERS)– spontaneous and voluntary reporting system– electronic database of postmarketing reports of
adverse drug reactions– reporters include health care providers,
pharmacies, consumers, and pharmaceutical manufacturers

4
ParoxetineParoxetine
Pediatric Psychiatric Adverse Pediatric Psychiatric Adverse EventsEvents
5
Background Drug InformationBackground Drug Information
• Moiety: Paxil®, Paxil CR® (paroxetine)• Therapeutic Category: Antidepressant• Sponsor: GlaxoSmithKline • Adult Indications: Major depressive disorder,
obsessive compulsive disorder, panic disorder, social anxiety disorder, generalized anxiety disorder, posttraumatic stress disorder – adult dose range: 20-60 mg/day
• There are NO approved pediatric indications• Original market approval: December 1992• Pediatric exclusivity granted: June 27, 2002
6
• Pregnancy Category C
• Precautions: – Suicide risk inherent in MDD– Suicide risk present in co-morbid conditions– Activation of mania– Seizures– Adverse events with abrupt discontinuation
• agitation, anxiety, dizziness, sensory disturbance, nausea and sweating
Relevant Safety LabelingRelevant Safety Labeling
7
Drug use trends: paroxetineDrug use trends: paroxetine• Second most commonly used SSRI in children.1
• Both pediatric & adult prescriptions have increased steadily between 1999 and 2003. 1
• Pediatric Diagnosis (off label): depression, anxiety and obsessive-compulsive disorders 2
• Pediatric patients account for approximately 3.5 % of total U.S. prescriptions of Paxil® between Jul 2002 – Jun 2003 (1.1 million).1,3*
1IMS Health, National Prescription Audit Plus, On-Line Source Year Aug 1999 – Jul 2003, Data Extracted Aug 20032IMS Health, National Disease and Therapeutic Index, CD-Rom, Source 3 Year Jul 2000 – Jun 2003 3AdvancePCS Dimension Rx, On-Line*Calculation based on application of proportions of pediatric paroxetine prescriptions in AdvancePCS to IMS Health, National Prescription Audit Plus to estimate number of paroxetine prescriptions dispensed nationwide to pediatric population

8
Adverse Events 1992-2003: Adverse Events 1992-2003: General Overview (raw counts)General Overview (raw counts)
• Total: over 17,000 adult and pediatric reports (68 % domestic)
• < 5 % of total are pediatric
• Top 20 pediatric AEs
– similar to those reported in adults
– majority labeled
– unlabeled events related to maternal exposure
• Number of pediatric adverse event reports increased in 2002 compared with prior years

9
Raw Counts* of Pediatric Adverse Raw Counts* of Pediatric Adverse Event Reports by Year Event Reports by Year (Dec 1992 to Jul 2003)(Dec 1992 to Jul 2003)
* * includes duplicate reports

10
BBC show “The Secret of Seroxat,” aired October 13, 2002 British government
warning issued on June 10, 2003
FDA Talk Paper issued on June 19, 2003
FDA PUBLIC ADVISORY for antidepressants and suicide issued on Oct 27, 2003
Exclusivity Period

11
Pediatric Adverse Events in the Pediatric Adverse Events in the One-year One-year PostPost-exclusivity Period-exclusivity Period
• Total unduplicated reports (N= 127)
• Gender: Female - 61, Male - 59, Unknown - 7
• Age: 0-<2 yrs (n=32), 2-5 yrs (n=6), 6-11 yrs (n=33), 12-16 yrs (n= 55) & unknown (n=1)
• Outcomes: – 10 % of reports were deaths (n = 13)– Approximately 1/3 hospitalizations/ER visit
(n= 43)

12
Pediatric Adverse Events by Gender, Pediatric Adverse Events by Gender, Age & Exposure to Paroxetine (N=127)Age & Exposure to Paroxetine (N=127)
Gender: Female
Male
Unknown
Age: 0-2 yrs
2-5yrs
6-11yrs
12-16yrs
Unknown
Maternal/Breastfeeding
(n=33)
7
19
7
32
0
0
0
1
Direct Pediatric Exposure
(n=94)
54
40
0
0
6
33
55
0

13
Pediatric Adverse Events: Reasons Pediatric Adverse Events: Reasons for Exposure to Paroxetine for Exposure to Paroxetine (N=127)(N=127)
• Prenatal Exposure/Breastfeeding (n= 33)• Direct Pediatric Exposure (n=94)
– Depression/dysthymia - 28
– Anxiety/Panic/PTSD- 15
– ADHD- 2
– OCD- 1
– Multiple Psychiatric diagnosis- 18
– Other- 9
– Unknown - 21

14
Paroxetine: Pediatric Adverse Paroxetine: Pediatric Adverse EventsEvents
• Concomitant medications (n =55), exclusively Concomitant medications (n =55), exclusively paroxetine (n=5), most unknown (n= 67)paroxetine (n=5), most unknown (n= 67)
• Reporters: only 1/3 health professional; 2/3 Reporters: only 1/3 health professional; 2/3 consumer, media, litigation, etc. consumer, media, litigation, etc.
• Dose range 5-60 mg/day (n=65, excludes Dose range 5-60 mg/day (n=65, excludes maternal/breastfeeding exposure)maternal/breastfeeding exposure)

15
Pediatric Adverse Events: Pediatric Adverse Events: Predominant EventsPredominant Events
• Psychiatric adverse events (68)• Discontinuation Syndrome/decrease in
dose (7)• Maternal exposure (33) • Neurologic events (8)• Accidental ingestion (2)• Other (9)

16
Psychiatric Adverse EventsPsychiatric Adverse Events by Labeling Status (n=68 ) by Labeling Status (n=68 )
Labeled• Completed suicide - 9
• Suicidal attempts -17
• Suicidal ideation - 11
• Occurrence of other psychiatric symptoms - 9
Unlabeled • Self-injurious behavior - 10
• Completed homicide - 4
• Aggression/Hostility/ Homicidal ideation - 8
17
Psychiatric Adverse Events (n=68)Psychiatric Adverse Events (n=68)
• Demographics: – Gender: 57% Female– Age: 2-5 yrs. (5%), 6-11 yrs. (35%), 12-16 yrs.
(60%)• Concomitant medications described in only 24
patients– 20 of the 24 on other psychotherapeutic agent
• discontinuation or decrease in dose noted in 11 of the 68 patients with psychiatric events

18
Psychiatric Events with Psychiatric Events with Discontinuation or Decrease in DoseDiscontinuation or Decrease in Dose
• Completed suicide (1 out of 9 )
• Suicidal attempts (5 out of 17)
• Homicide (2 out of 4)
• Aggression/Hostility/Homicidal ideation (3 out of 8)
19
Suicide AttemptsSuicide Attempts(n=17)(n=17)
• Diagnosis: Majority MDD, Bipolar Disorder
• Concomitant medications in approximately one third
• discontinuation or decrease in dose in approximately one fourth

20
Pediatric Deaths (n=13)Pediatric Deaths (n=13)
10 deaths involving direct pediatric exposures– 9 completed suicides– 1 case of Stevens Johnson Syndrome; patient
also received valproic acid
3 deaths among patients with prenatal exposure

21
Pediatric Deaths: Completed Pediatric Deaths: Completed Suicides Suicides (n=9)(n=9)
– Ages 12-16 years– Gender Female (5) Male (4)– Initial Diagnosis: MDD (5) Explosive
Disorder (1) Unknown (3)– Duration of treatment- 14 days to 1 year– Discontinuation or decrease in dose (2)– Concomitant medication (4)– Possible substance abuse (4)– History of prior attempts (3)
22
Factors Contributing to Difficulty Factors Contributing to Difficulty in Assessing Causalityin Assessing Causality
• Patient Factors– severity of illness/ underlying disease– prior history of suicide attempts– concomitant medication– substance abuse
• Reporting factors– inadequate detail in describing event– timing of event in relationship to medication– ascertainment of reported events– lack of follow-up
23
Limitations of AERSLimitations of AERS
• Spontaneous and voluntary system– Underreporting – Reporting bias (media publicity, length of time
in market)– Report quality may vary (missing details e.g.
concomitant medications) – Cannot estimate true incidence rate of events or
exposure risk

24
Closing ObservationsClosing Observations
• The psychiatric events described in the adverse event reports may reflect:– underlying disease – drug adverse effect– lack of drug effect
• Evaluation of controlled trials necessary to sort out
25
AcknowledgementsAcknowledgements
ODS reviews prepared by:
Mark Avigan, MD, C. M.
Susan Lu, R. Ph
Carol Pamer, R. Ph
Toni Piazza-Hepp, Pharm.D.
Gianna Rigoni, Pharm.D.
26
Citalopram: Pediatric Psychiatric Adverse
Events
Solomon Iyasu, MD, MPH
Hari Cheryl Sachs, MD, FAAP
Division of Pediatric Drug Development

27
Citalopram:Citalopram: Background Drug InformationBackground Drug Information
• Moiety: Celexa® (citalopram)• Therapeutic Category: Antidepressant• Sponsor: Forest Pharmaceuticals• Adult Indication: Major Depressive Disorder
– Adult dose range: 20-40 mg/day
• There are NO approved pediatric indications• Original market approval: July 17, 1998• Pediatric exclusivity granted: July 9, 2002
28
Relevant Safety LabelingRelevant Safety Labeling
• Pregnancy Category C• Excreted in human breast milk• Precautions:
– Suicide risk inherent in depression– Activation of mania/hypomania– Any psychoactive agent may impair
intellectual or psychomotor functions– Seizures: introduce citalopram with care

29
Relevant Safety LabelingRelevant Safety Labeling(cont.)(cont.)
• Adverse Reactions– Agitation– Pre marketing reports
• Frequent: impaired concentration, depression, suicide attempt, confusion
• Infrequent: aggressive reaction, psychotic reaction, delusion, paranoid reaction, emotional lability, panic reaction
30
Drug use trends: CitalopramDrug use trends: Citalopram• 4th most commonly used SSRI in children1
• Both pediatric and adult prescriptions have increased between 1999 and 20031
• Pediatric patients account for approximately 3.3% (665, 000) of the total U.S. prescriptions of Celexa® during Jul 2002- Jul 20031,2
• Pediatric Diagnosis (off label): depressive disorders, obsessive-compulsive disorder and attention deficit disorder3
1IMS Health, National Prescription Audit Plus, On-Line Source Year Aug 1999 – Jul 2003, Data Extracted Aug 20032AdvancePCS Dimension Rx, On-Line, Jul 2001 – Jun 20033IMS Health, National Disease and Therapeutic Index, CD-Rom, Source 3 Year Jul 2000 – Jun 2003*Calculation based on application of proportions of pediatric citalopram prescriptions in AdvancePCS to IMS Health, National Prescription
Audit Plus to estimate number of citalopram prescriptions dispensed nationwide to pediatric population

31
Overview of Adverse Event Overview of Adverse Event Reports Since Marketing Reports Since Marketing
ApprovalApproval
• Total: over 6,000 reports (79% domestic) • <5 % of total are pediatric• Top 20 AE
– All adverse events related to in utero exposure were unlabeled
– Adverse event reports for children involving direct exposure were generally similar to those reported for adults

32
Pediatric Adverse Events in the Pediatric Adverse Events in the One-Year Post-exclusivity PeriodOne-Year Post-exclusivity Period
• Total unduplicated reports (n=42)
• 16 in utero exposures; resulted in unlabeled events and one death
• 26 children involving direct exposure, 8 unlabeled events, no deaths– 16 serious AEs (10 hospitalization, 4 life-
threatening, 2 with disability)– dose 5-60 mg/day, median dose 20 mg/day
33
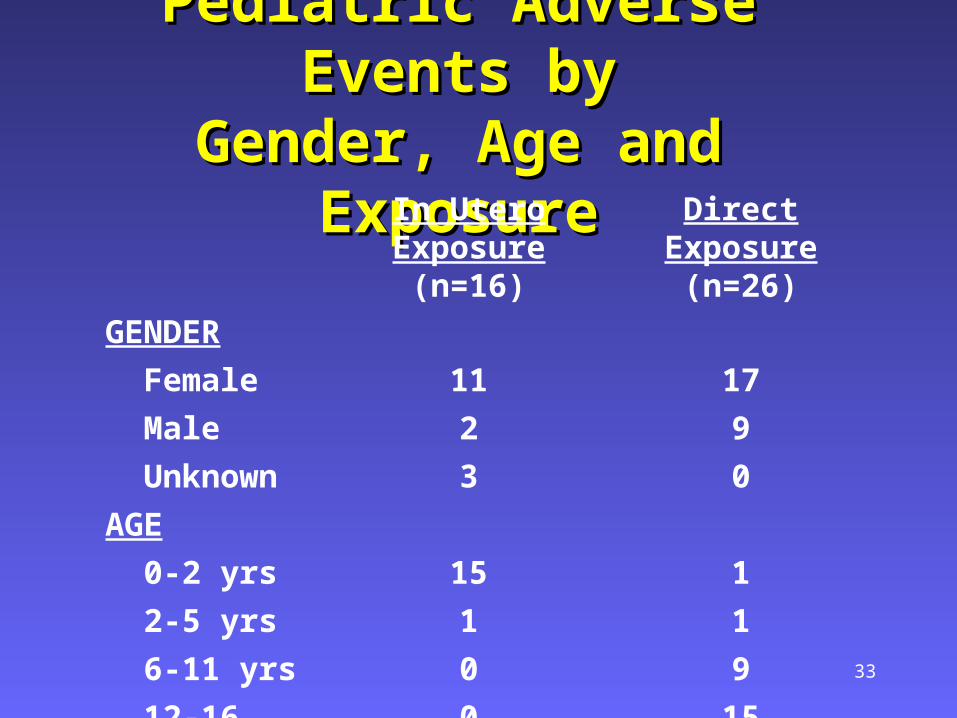
Pediatric Adverse Events byPediatric Adverse Events byGender, Age and ExposureGender, Age and Exposure
GENDER
In Utero Exposure (n=16)
Direct Exposure (n=26)
Female 11 17
Male 2 9
Unknown 3 0
AGE
0-2 yrs 15 1
2-5 yrs 1 1
6-11 yrs 0 9
12-16 yrs 0 15

34
Pediatric Adverse Events:Pediatric Adverse Events:Reasons for Exposure to Reasons for Exposure to
CitalopramCitalopram
• In utero exposures – 16
• Direct Pediatric Exposure – 26– Depression – 13– Ingestion of another person’s prescription – 2– Other – 5– Unknown - 6

35
Citalopram adverse events- Citalopram adverse events- Psychiatric (n= 5)Psychiatric (n= 5)
Labeled• Cognitive impairment• Aggression• Agitation, mania, and
delusions• Suicidality• Psychotic reaction
Unlabeled • Violent/homicidal
behavior

36
Citalopram Adverse Events- Citalopram Adverse Events- Psychiatric Psychiatric (cont.)(cont.)
• Gender: 4 males, 1 female
• Age: 6-11 yrs (2), 11-16 yrs (3)
• Diagnosis: MDD (4), ODD(1)
• Concomitant medications – 2– Prozac®; Keppra®, clonazepam
• Symptoms resolved when citalopram discontinued - 4

37
Closing observationsClosing observations
• Few psychiatric events were reported
• Unable to determine causality due to limitations of AERS
• FDA will continue monitoring these adverse events in children
38
AcknowledgementsAcknowledgements
ODS reviews prepared by:
Mark Avigan, MD
Toni Piazza-Hepp, Pharm.D.
Kathleen Phelan, R. Ph
Gianna Rigoni, Pharm.D.
Related Documents











