1 MANAGING ASSETS MANAGING ASSETS

1 MANAGING ASSETS. FORENSIC ASPECTS GERO PSYCHIATRY Howard H. Fenn, MD Associate Clinical Professor, Stanford University Medical Director, Acute Geropsychiatry.
Dec 29, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
MANAGING ASSETSMANAGING ASSETS
FORENSIC ASPECTS GERO PSYCHIATRY FORENSIC ASPECTS GERO PSYCHIATRY
Howard H. Fenn, MD
Associate Clinical Professor , Stanford University
Medical Director, Acute Geropsychiatry Unit
Palo Alto Veterans Affairs Medical Center
3

4
FORENSIC ASPECTS FORENSIC ASPECTS of of GEROPSYCHIATRYGEROPSYCHIATRY
o Competency overviewo Assessment of competencyo Specific competencies in geriatric patientso Other:
Elder AbusePersonal injury and malpracticeEnd of life issues
5
TOP 10 REASONS PHYSICIANS SUED TOP 10 REASONS PHYSICIANS SUED
o Informed consent not obtained/documentedo Informed refusal not obtainedo Weak, undocumented patient educationo Inattention to doctor-patient relationshipo Overlooked lab resultso Poor inter-professional communicationso Medication problemso Weak medical recordso Inadequate history-taking or documentationo Inattentive follow-up
6
PREVALENCE PREVALENCE ofof DECISIONAL IMPAIRMENT DECISIONAL IMPAIRMENT
o Diagnosis of dementia by itself does not determine incapacity
o 80-90% of mild-to-moderate Alzheimer’spatients are decisionally impaired
o 44%, 45%, 67%, 69% of nursing home patients are decisionally impaired
7
CATEGORIES CATEGORIES of of INCOMPETENCEINCOMPETENCE
Category Settingo Judicial (de Jure) courto De Facto court-orderedo Informal clinical settings
o Retrospective after an act

8
4 “D”s 4 “D”s of of De JURE De JURE INCOMPENTENCEINCOMPENTENCE
o Diagnosis: not sufficient o Deficit (psychiatric) & lack of functiono Defined by codeo Decision-making ability (specific)
--1995: California (DPCDA)

9

10
PROCESS PROCESS of of ASSESSMENTASSESSMENT
o Orthopedist examines injured player’s abilities =competence evaluation
o Team orthopedist determines capacity to perform =de facto competence
determination
o NHL officials set rules for scoring =Legal code Referee decides if goal made =de Jure
11
ASSESSMENT INSTRUMENTSASSESSMENT INSTRUMENTS
o MacArthur Competence Assessment tool (MacCAT) (Grisso et al, 1997)
o Hopkins Competency Assessment Test(Janofsky et al, 1992)
o Mini-Mental State Exam (Molloy et al 1996) Kim SYH et al., 2000
12
ASSESSMENT ASSESSMENT ofof DECISIONAL CAPACITY DECISIONAL CAPACITY
o A forgetful physician was fretting: o “Maybe Dx is a DAT* I am getting.”o Her recall declined, whereupon she opined,o “I forgot what I found so upsetting.”
13
TESTS TESTS ofof CAPACITY CAPACITY for for MEDICAL TREATMENTMEDICAL TREATMENT
o Evidencing a treatment choice (LS1)o Making a reasonable treatment choice (LS2)o Appreciating consequences of choice (LS3)o Providing rational reasons for choice (LS4)o Understanding treatment situation (LS5)

14
EVIDENCE EVIDENCE aa CHOICE (LS1) CHOICE (LS1)
o Normal 100% competento Mild AD 87% competento Moderate AD 79% competent

15
APPRECIATE APPRECIATE the the CONSEQUENCES (LS3)CONSEQUENCES (LS3)
o Normal 93% competento Mild AD 52% competento Moderate AD 36% competent
16
UNDERSTAND TREATMENT SITUATION UNDERSTAND TREATMENT SITUATION and and CHOICES (LS5)CHOICES (LS5)
o Normal (MMSE >24) 100% competento Mild AD (MMSE 20-23) 0% competento Moderate AD (MMSE 9-19) 0% competent

17
ASSESSMENT ASSESSMENT ofof COMPETENCE COMPETENCE by by PHYSICIANSPHYSICIANS
o Physicians did NOT agree in mild AD o Physicians agreed in cognitively intacto Highest agreement--least stringent standardso Competency assessment instruments enhance
judgment of competency
--Marson et al., 1996_
18
PREDICTORS of DECISIONAL IMPAIRMENT in ADPREDICTORS of DECISIONAL IMPAIRMENT in AD
o Auditory comprehension predicted LS 1o Word fluency predicted LS3o Conceptualization predicted LS5o Confrontational naming predicted LS5
o --Marson et al. 1996
19
PRESUMPTION PRESUMPTION of of COMPETENCECOMPETENCE
No person may be presumed to be incompetent because he or she has been evaluated or treated for mental disorder or chronic alcoholism, regardless of whether such evaluation or treatment was voluntarily or involuntarily received. Any person who leaves a public or private mental health...
--Sec. 5331 W&I Code
20
DEFICIT+LACK OF FUNCTIONDEFICIT+LACK OF FUNCTION
o A determination that a person is of unsound mind or lacks the capacity to make a decision or do a certain act, including, but not limited to, the incapacity to contract, to make a conveyance, to marry, to make medical decisions, to execute will, or to execute trusts, shall be supported by evidence of a deficit in at least one of the following mental functions…and evidence of a correlation between the deficit…and the decision or acts in question
o --Sec. 811 Probate Code

21
CAPACITY= COMMUNICATE CAPACITY= COMMUNICATE
o The rights duties and responsibilities created by, or affected by the decision
o The probable consequences for the decision maker and, where appropriate, the persons affected by the decision
o The significant risks, benefits, and reasonable alternatives involved in the decision. SEC 812 PROBATE CODE
22
SPECIFIC COMPETENCIESSPECIFIC COMPETENCIES
o Provide food, clothing, shelter sec. 5250 W&I Refuse psychotropic meds sec. 5332 W&I Manage assets sec. 812 PROBATE Informed consent--medical sec. 813 PROBATE Informed consent-dementia Rx sec. 2356.5 PROBATE Execute a will sec. 6100.5 W&IAdvance Directive sec. 4609 PROBATE Informed consent for ECT sec. 5352 W&I CODEFor research sec. 24178 H&S CODE

23
CAPACITY--REFUSE PSYCHOTROPICS CAPACITY--REFUSE PSYCHOTROPICS
o Riese v. St. Mary's Hospital 243 Cal Rptr 241 (Cal App. 1 Dist l987)
o Able to participate in treatment decision by means of rational thought processes.
o In absence of a clear link between patient's delusional or hallucinatory perceptions and his ultimate decision to consent or refuse treatment, court should assume that patient is utilizing rational modes of thought.

24
CONSERVATORSHIP DISTINCTIONS CONSERVATORSHIP DISTINCTIONS
Mental Health / LPSo Treatment as goalo Involuntary commitmento Beyond reasonable
doubto Grave disability +
mental illnesso Reviewed yearly o Mental health
professional
Probate o Estate as goalo No civil commitmento Clear and convincingo Financial incompetence
and/or dementiao Reviewed every 2 yearso Petitioner: anyone

25
CONSENT-MEDICAL TREATMENTCONSENT-MEDICAL TREATMENT
o 1. Respond knowingly and intelligently to queries about that medical treatment
o 2. Participate in that treatment decision by means of a rational thought process
o 3. Understand all of the following terms of minimum basic medical treatment information with respect to... treatment: sec. 812 and sec. 813 Probate Codesec. 812 and sec. 813 Probate Code

26
TESTAMENTARY CAPACITYTESTAMENTARY CAPACITY
o An individual is not mentally competent to make a will if at the time of making the will either of the following is true:
o A) cannot understand the nature of the testamentary act
o B) cannot understand and recollect the nature and situation of the individual’s property, or
o C) cannot remember and understand the individual’s relations to living descendants, spouse, and parents, and those whose interests are affected by the will. (Probate Code Sec 6100.5)
27
ECTECT
o No convulsive treatment as defined in Section 5325 of the Welfare and Institutions Code may be performed on a ward or conservatee under this division.
o Affective indications of incompetence: Pessimism, hopelessness, helplessness, giving up, and worthlessness
o Cognition may remain intact

28
CAPACITY TO CONTRACTCAPACITY TO CONTRACT
o A person entirely without understanding has no power to make a contract of any kind—CC 38

29
COMPETENCE TO STAND TRIALCOMPETENCE TO STAND TRIAL
o A defendant is mentally incompetent for purposes of this chapter if, as a result of mental disorder, he/she is unable to understand the nature and purpose of the proceedings taken against him/her and to assist counsel in the conduct of a defense in a rational manner.”

30
DURABLE POWER DURABLE POWER ofof ATTORNEY ATTORNEY for for HEALTH CAREHEALTH CARE
o Capacity to contracto Attorney-in-fact makes substituted judgmento Attorney-in-fact cannot consent to civil commitment,
ECT, psychosurgery, sterilization, abortiono Principal’s assent required for end of life treatment o -- Sec. 4724 Probate Code
31
ADVANCE DIRECTIVEADVANCE DIRECTIVE
Informed consentInformed consent Advance DirectiveAdvance Directive
Treatment now Treatment in future Capacity now Capacity in futureNo trigger Trigger: incapacityActual choice Hypothetical choiceNo choice=a choice Can always choose
32
INABILITY OF CONSERVATEE TO GIVE INFORMED INABILITY OF CONSERVATEE TO GIVE INFORMED CONSENT; JUDICIAL DETERMINATIONCONSENT; JUDICIAL DETERMINATION
o “the court may take into consideration the frequency, severity, and duration of periods of impairment.”
--(Sec.1890)
33
WILLS & TRUSTSWILLS & TRUSTS
o Sec.6100.5 Probate Codeo 1)The individual does not have sufficient mental
capacity to be able to o A)understand the nature of the testamentary acto B) understand and recollect the nature and situation
of the individual’s property , or o C)remember and understant the individual’s relations
to living decendants, spouse, and parents…o 2) The individual suffers from a mental disorder with
symptoms including delusions or hallucinations, which delusions or hallucinations result in the idnvidual’s devising property in a way which, except

34
DEFICITS in MENTAL FUNCTIONS DEFICITS in MENTAL FUNCTIONS (SEC.811 (SEC.811 PROBATE CODE)PROBATE CODE)
o Alertness and attention, including level or arousal or consciousness
o Ability to attend and concentrateo Orientation to time, place, person, and situationo Information processing, including short-and long-term memoryo Ability to understand or communicate with others, either verbally
or otherwiseo Recognition of familiar objects and familiar personso Ability to understand and appreciate quantititieso Ability to reason using abstract conceptso Ability to plan organize, and carry out actions in one’s own
rational interesto Ability to reason logicallyo Thought processes. Deficits: severely disorganized thinking,
hallucinations, delusions, uncontrollable, repetitive or intrusive thoughts, ability to modulate mood and affect.

35
CLINICAL vs. LEGAL CAPACITY CLINICAL vs. LEGAL CAPACITY
o CLINICAL STANDARDSo Evidencing a treatment
choiceo Making a reasonable
treatment choice o Appreciating consequences
of choice o Providing rational reasons
for choice o Understanding treatment
situation
o PROBATE CODE Sec. 813
o Respond knowingly and intelligently to queries about that medical treatment
o Participate in that treatment decision by means of a rational thought process
o Understand all…minimum basic medical treatment information with respect to... treatment:

36
DEMENTIA POWERS DEMENTIA POWERS
o The conservatee has dementia...o …and lacks the capacity to give informed consent to
the placement and has at least one mental function deficit pursuant to subdivision (a) of Section 812, and this deficit significantly impairs the person’s ability to understand and appreciate the consequences of his or her actions pursuant to subdivision (b) of Section 812—
o Section 2356.5 of Probate Code
37
38
TO BOLSTER COMPETENCETO BOLSTER COMPETENCE
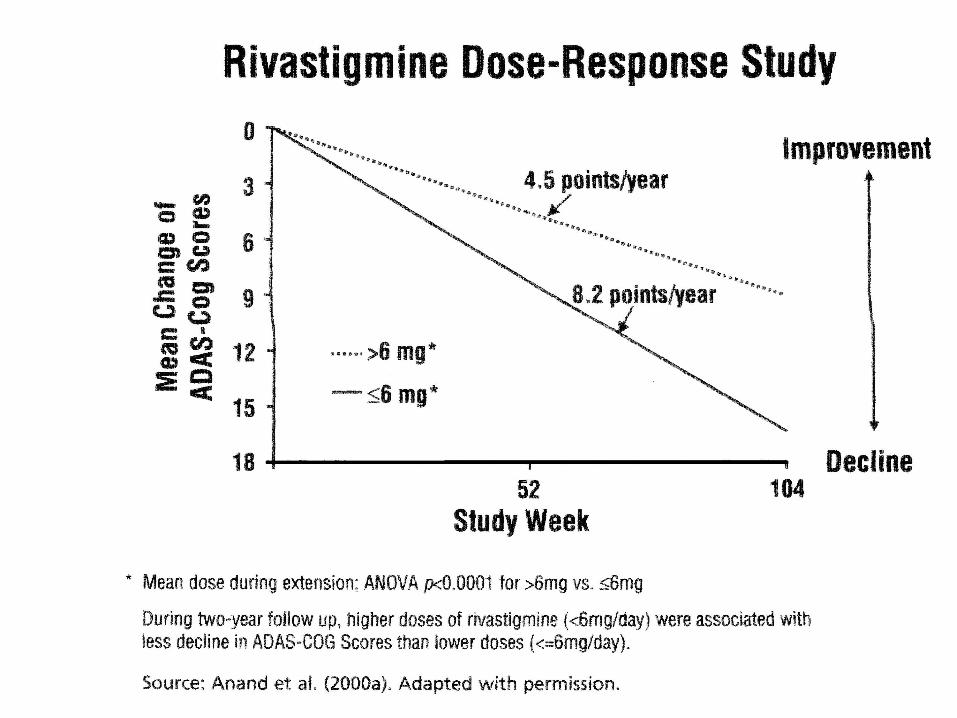
o Present information piece-mealo Try-out research projecto Bypass deficit with written memory aidso Target symptoms with medications (33%-40% with
AD have psychotic symptoms)o Rx with Anticholinesterase inhibitorso Rx with Memantine when available
39

40
INCOMPETENT INCOMPETENT toto MAKE A WILL MAKE A WILL ifif
o cannot understand nature of the testamentary acto cannot understand and recollect the nature and
situation of the individual’s property, or o cannot remember and understand the individual’s
relations to living descendants, spouse, and parents, and those whose interests are affected by the will. Probate Code Sec 6100.5)

41
UNDUE INFLUENCEUNDUE INFLUENCE
o “Will replaced by that of another”o “Coercion or compulsion” not requiredo Facts establish a presumptiono Opportunity (access, dependency, control)o Motive (Influencer to benefit)o Naturalness (relatives favored)o Susceptibility (“weakness of mind”)
42
FORENSIC GEROPSYCHIATRY SUMMARYFORENSIC GEROPSYCHIATRY SUMMARY
o Decision-making capacity is centralo Competency Codes consistent with psychiatric o de Jure incompetence:
o Diagnosis not sufficiento Deficit+loss of functiono Defined by codeo Decision-specific
Related Documents











