1 Imaging session Haematology MBChB V Session 1 MJ Coetzee

1 Imaging session Haematology MBChB V Session 1 MJ Coetzee.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Imaging sessionHaematology
MBChB V
Session 1MJ Coetzee
2
Normal blood picture
3
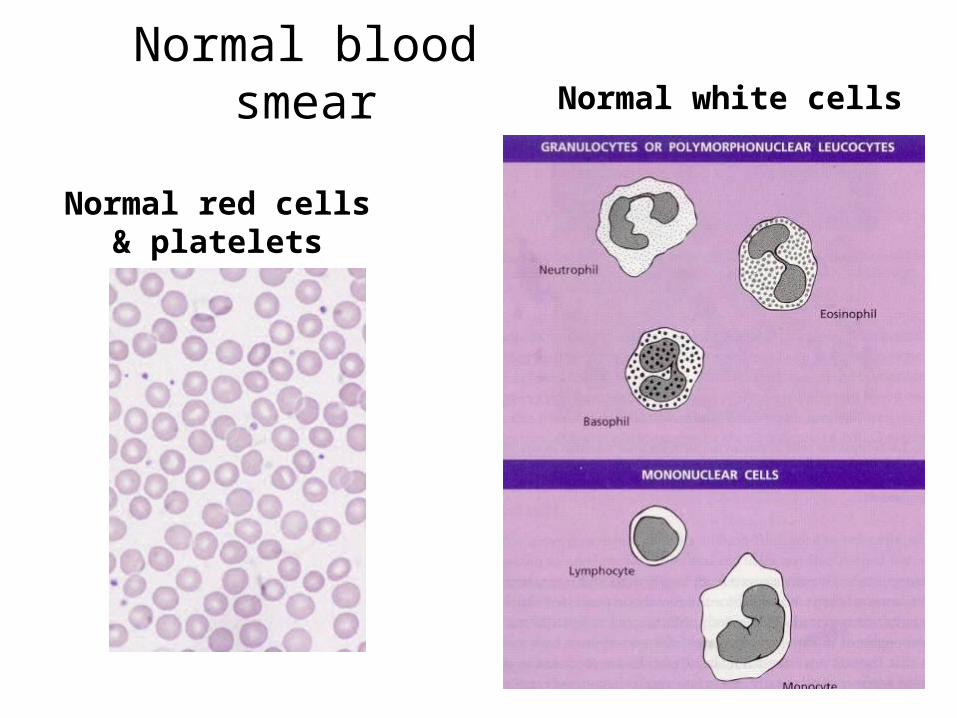
Normal blood smear
Normal red cells& platelets
Normal white cells
4
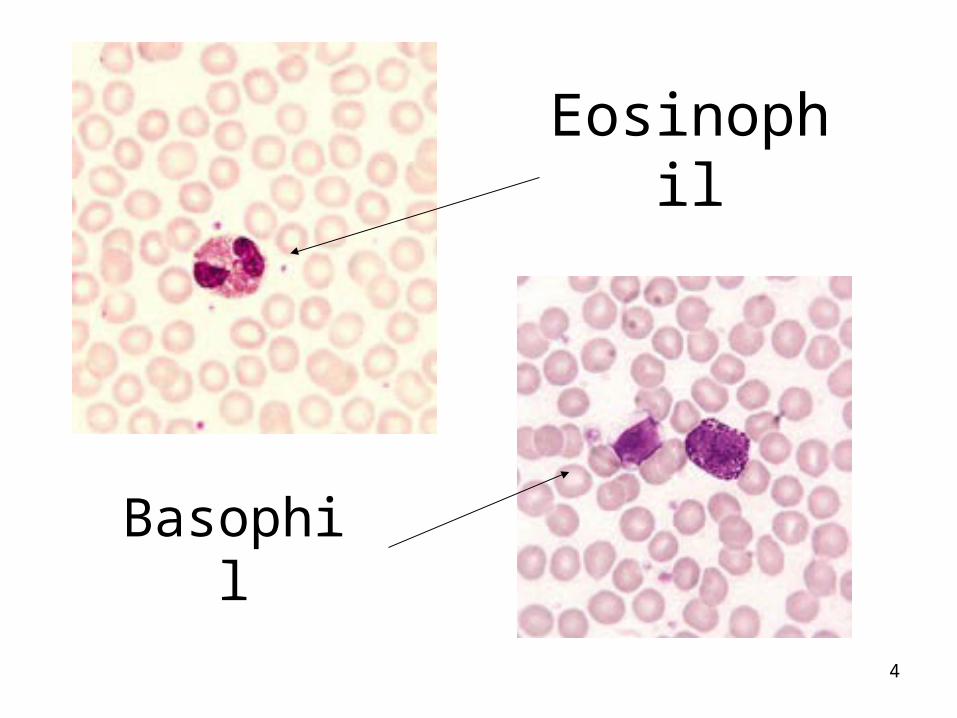
Eosinophil
Basophil

5
Normal band cell
6
Normal bone marrow
7
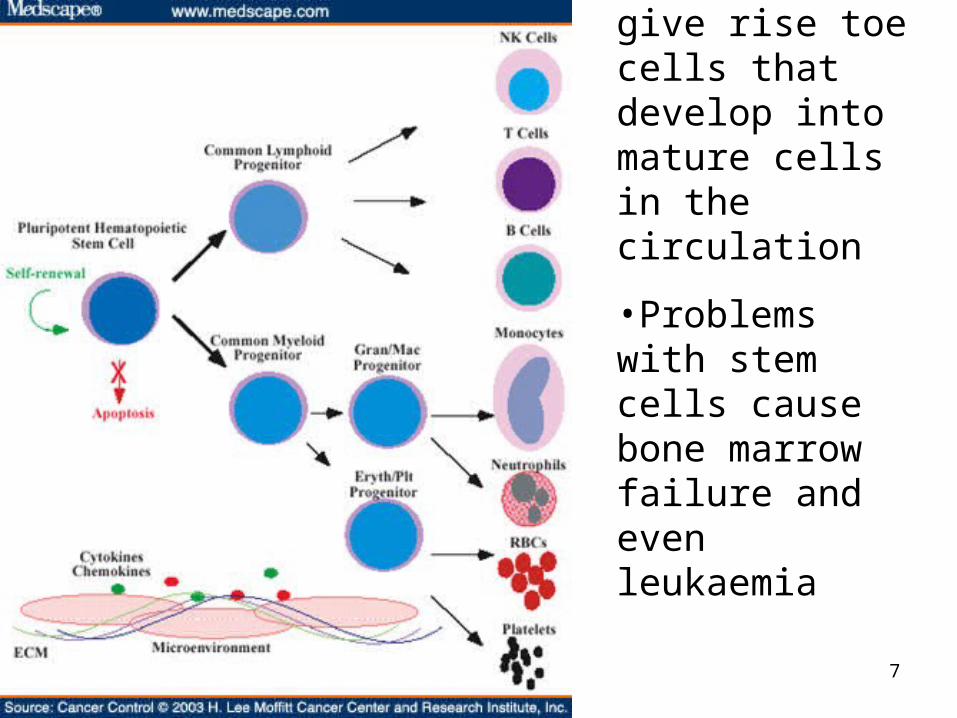
•Stem cells give rise toe cells that develop into mature cells in the circulation
•Problems with stem cells cause bone marrow failure and even leukaemia
8
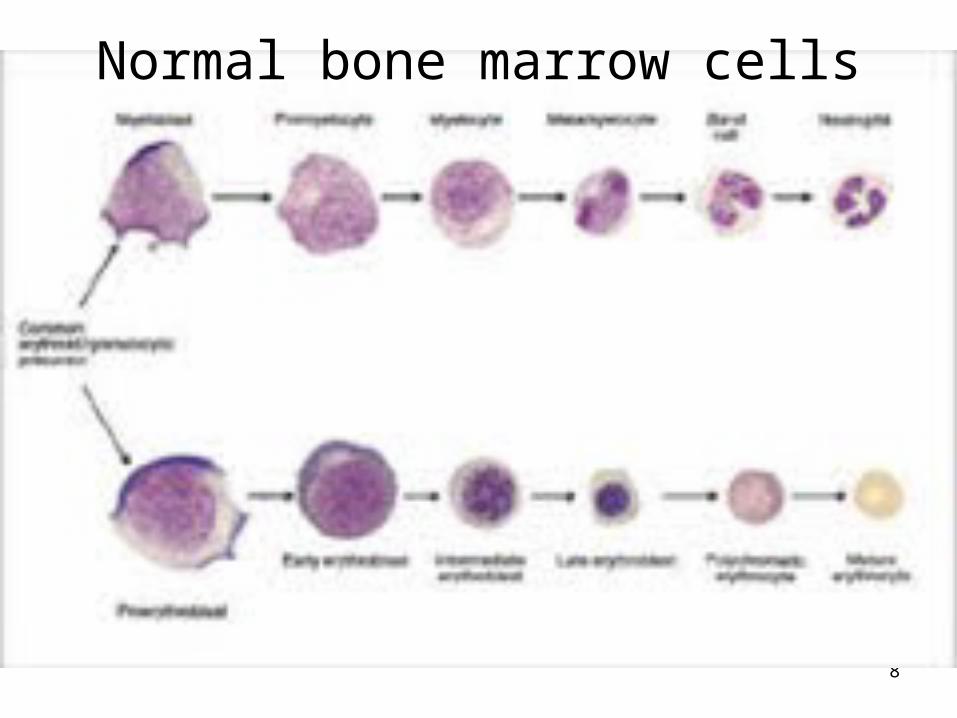
Normal bone marrow cells
9
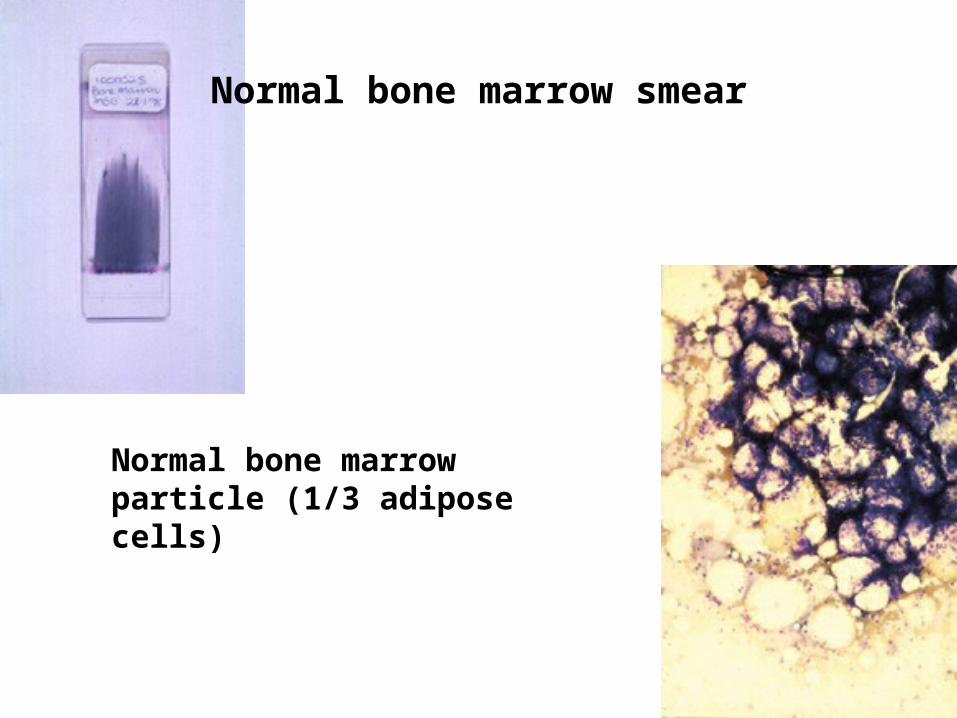
Normal bone marrow smear
Normal bone marrow particle (1/3 adipose cells)
Marius Coetzee
Get normal biopsy picture
10
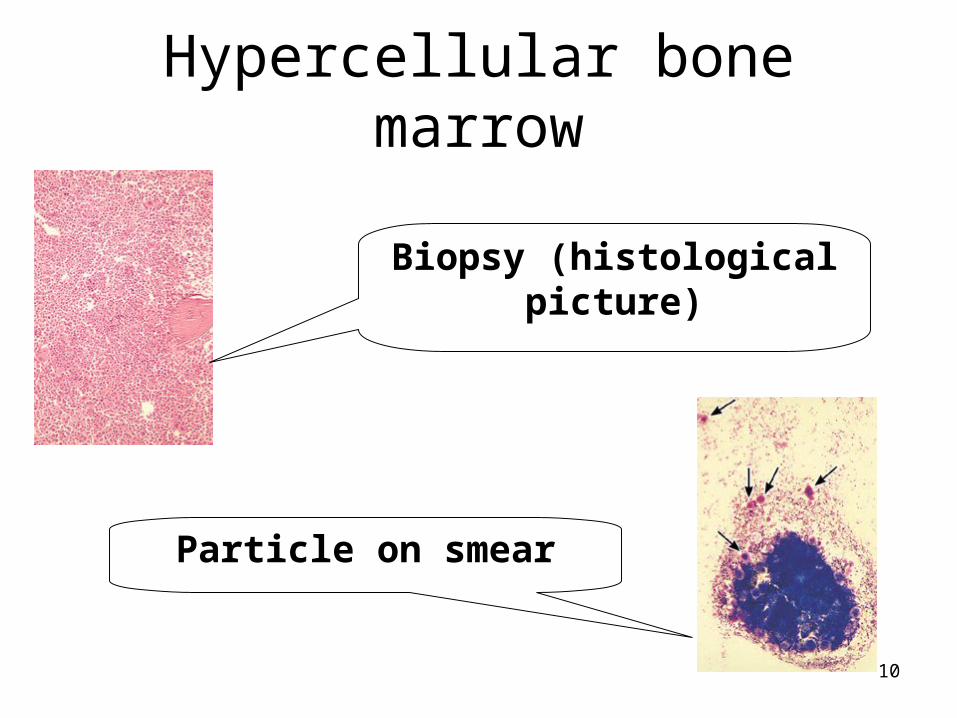
Hypercellular bone marrow
Particle on smear
Biopsy (histological picture)
11
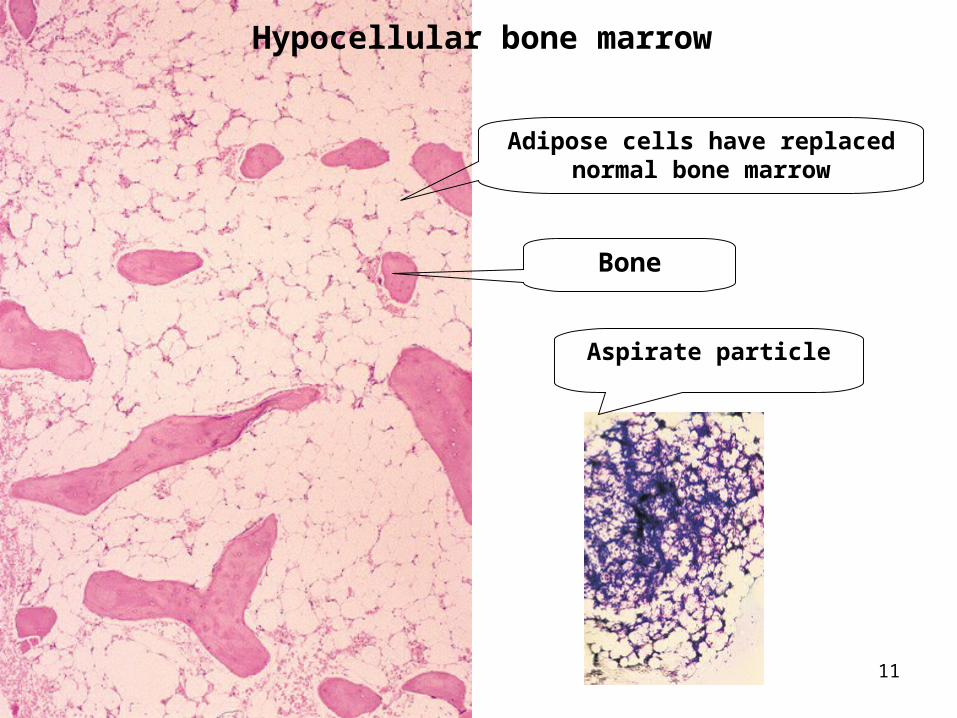
Hypocellular bone marrow
Adipose cells have replaced normal bone marrow
Bone
Aspirate particle
12
Full blood count
13
Full blood count-1• The FBC is a group of tests that
provides us with information about:– Red cells and their properties– Total white cell count and concentrations
of types of white cells (differential count)– Concentrations of platelets
• A blood smear is made and the morphology of the blood cells are reported
• Often the ESR is done simultaneously
14
Full blood count -2
• Blood for a FBC is drawn into a purple tube, that contains the anticoagulant EDTA
• The tube should reach the lab. within 2 hours - otherwise artifacts can occur
• Manual blood counts entails involves pipetting by mouth and involves a risk of infection
• Automated cell counters count red cells, white cells & platelets, en does Hb and red cell indices

15
Haemoglobin-1
• Normal Hb varies with age, sex & height above sea level
• In Bloemfontein (1300 m) the normal Hb for adults is:– Men: 14,5-18,5 g/dl
– Women: 12,5-16,5 g/dl
16
Haemoglobin-2
• Hb can also be measured in g/l and mmol/l
• World Health Organisation– At sea level– Definitions of anaemia by experts
• Children < 10 j < 9 g/dl
• Adult men < 13 g/dl
• Adult women < 12 g/dl
• Pregnant women < 11 g/dl

17
Red cell indices-1
• The Hb shows the presence/absence of anaemia
• The red cell indices show the type of anaemia
• The MCV (mean. corpuscular volume) is usually between 80-100 fl– MCV < 80 fl: microcytic– MCV 80-100 fl: normocytic– MCV > 100 fl: macrocytic

18
Red cell indices-2• The haematocrit reflects the portion of
the blood that consists of RBCs.– It is used exstensively in the USA as an
indicator of anaemia, but not elsewhere
• The MCH (mean cell haemoglobin) reflects the amount Hb/RBC
• The MCHC gives an idea of the colour of the RBCs
• Nowadays the MCV is accurately measured and it is the most important

19
FBC direct from the cell counter

20
Haematocrit
21
White cell count• The total WCC is 4,0-11,0 x 109/l• Most of the white cells are neutrophils• A leucopenia is mostly caused by a
decreased number of neutrophils, but not always
• A leucocytosis is mostly caused by an increased number of neutrophils, but not always
• Therefore it is important to know the absolute count of individual types white cells

22
Report of the blood smear
• Although one can obtain a lot of information from the FBC, always read the comments on the blood morphology
• The morphology can give information about e.g. malaria, left shift, activated lymphocytes, etc, while most machines cannot do this– Comments put the counts in perspective
and lead one to determine the cause of an anaemia, etc.
23
Red cell shapes

24
Round macrocytosis(e.g. alcohol)
Oval macrocytes (e.g. megaloblastic anaemia
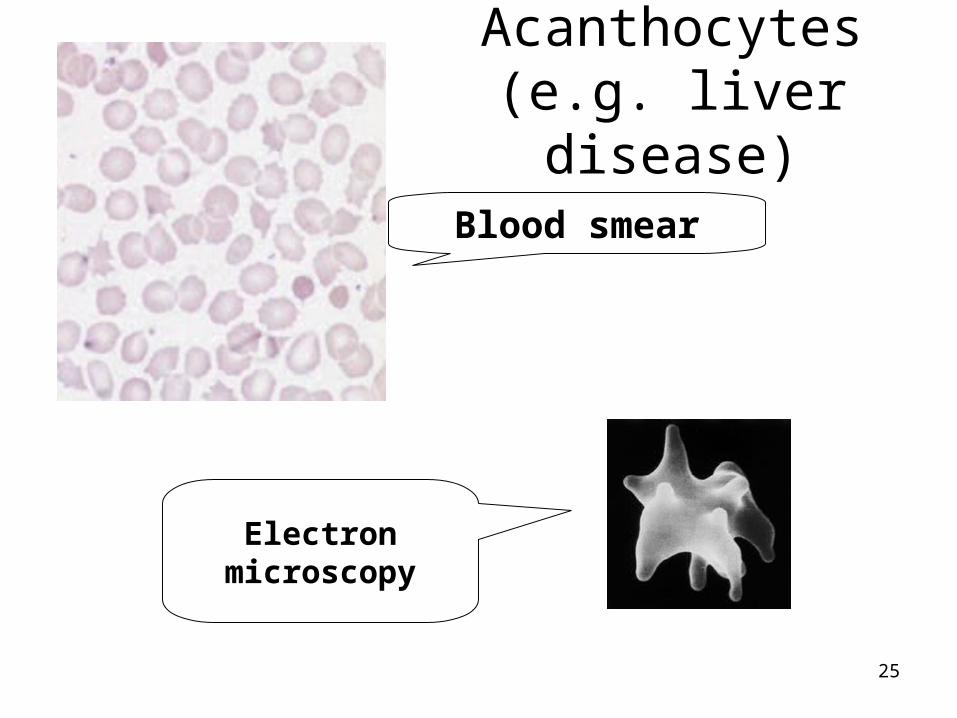
25
Acanthocytes(e.g. liver disease)
Blood smear
Electron microscopy
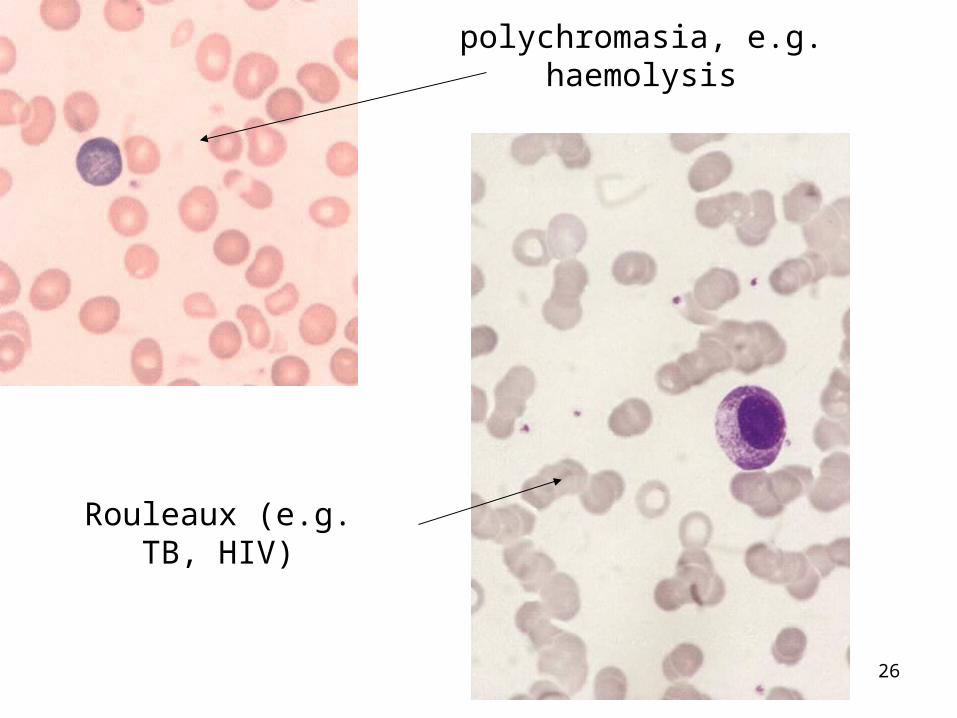
26
polychromasia, e.g. haemolysis
Rouleaux (e.g. TB, HIV)
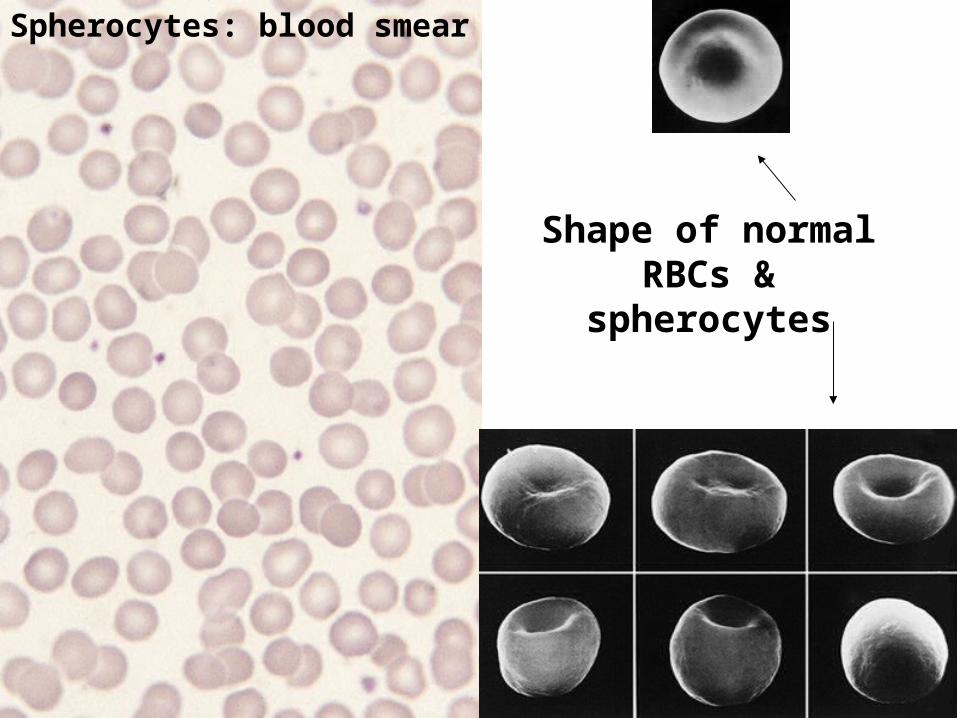
27
Spherocytes: blood smear
Shape of normal RBCs & spherocytes
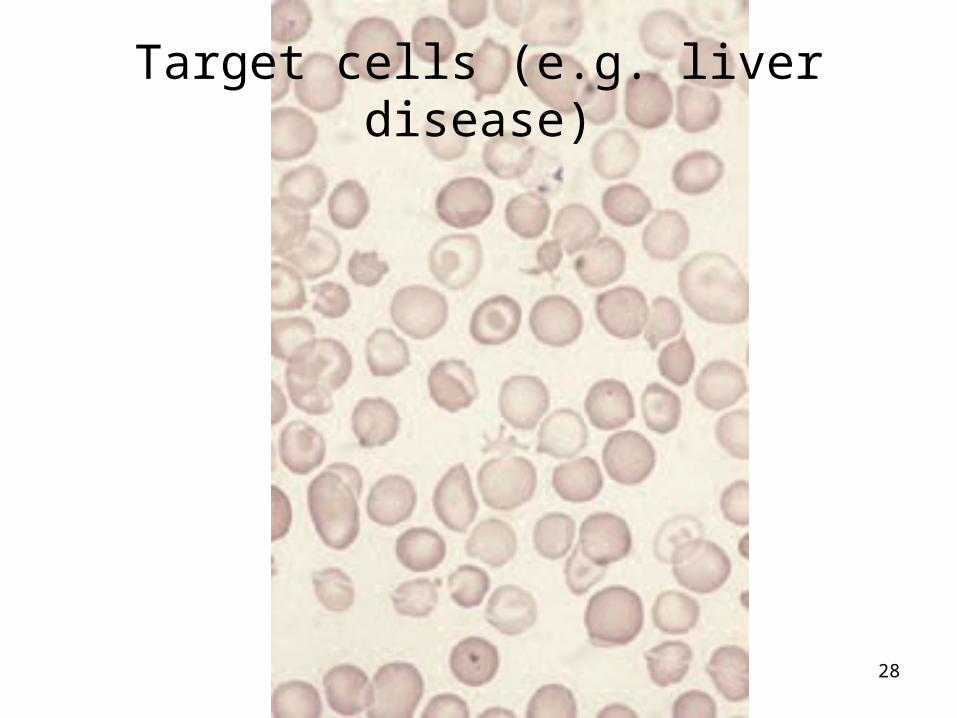
28
Target cells (e.g. liver disease)
29
Common white cell disorders
30
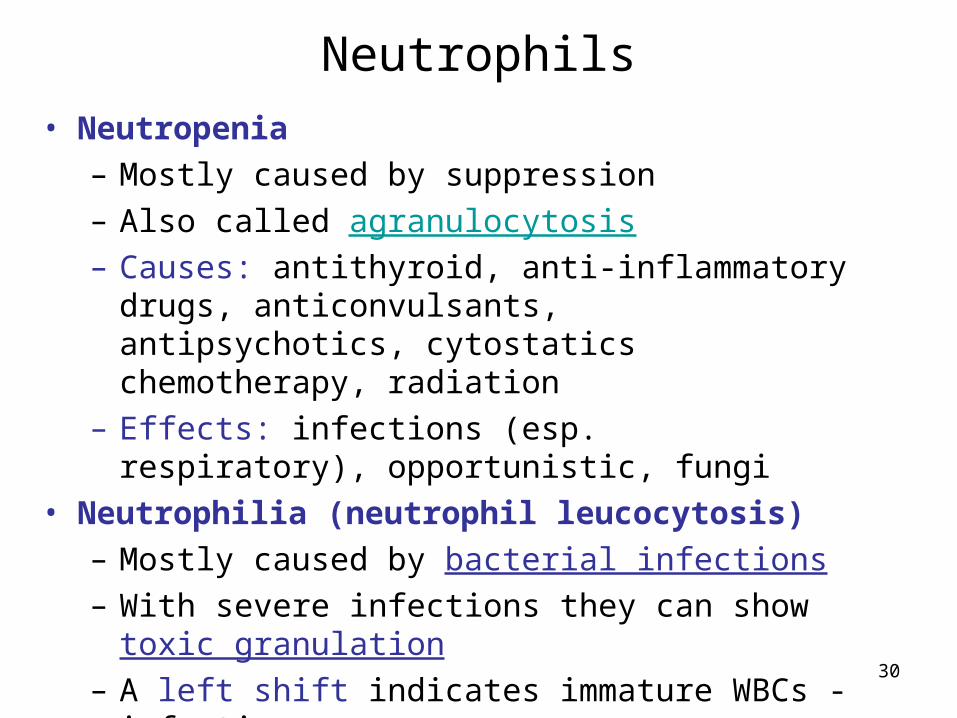
Neutrophils• Neutropenia
– Mostly caused by suppression– Also called agranulocytosis– Causes: antithyroid, anti-inflammatory drugs,
anticonvulsants, antipsychotics, cytostatics chemotherapy, radiation
– Effects: infections (esp. respiratory), opportunistic, fungi
• Neutrophilia (neutrophil leucocytosis)– Mostly caused by bacterial infections– With severe infections they can show toxic
granulation– A left shift indicates immature WBCs - infection
31
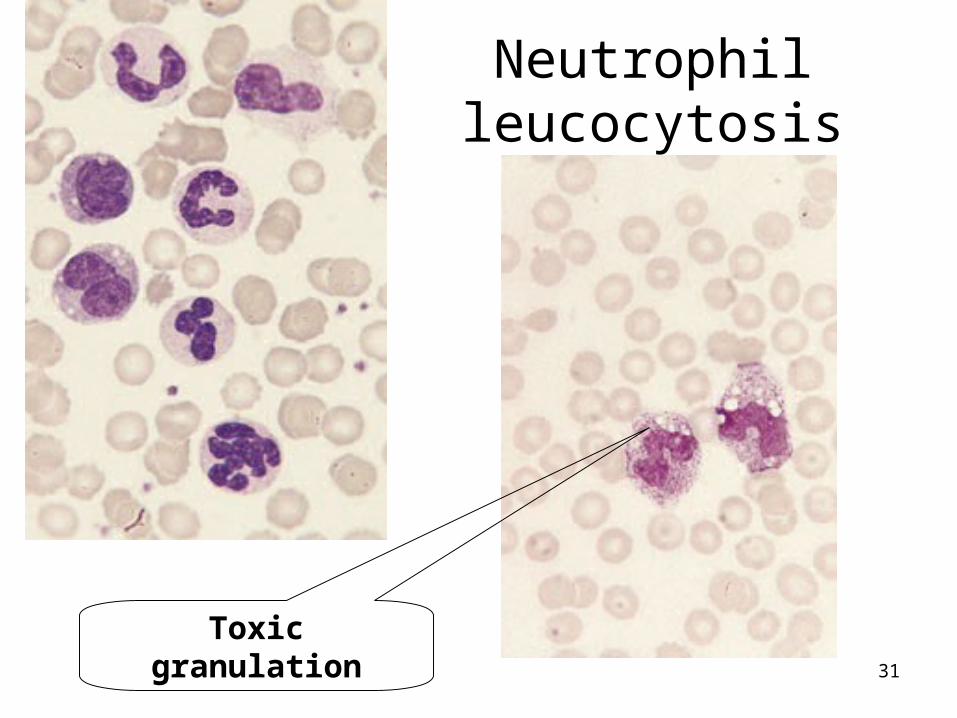
Neutrophil leucocytosis
Toxic granulation

32
Band cell (left shift)
Döhle bodies (infection)
33
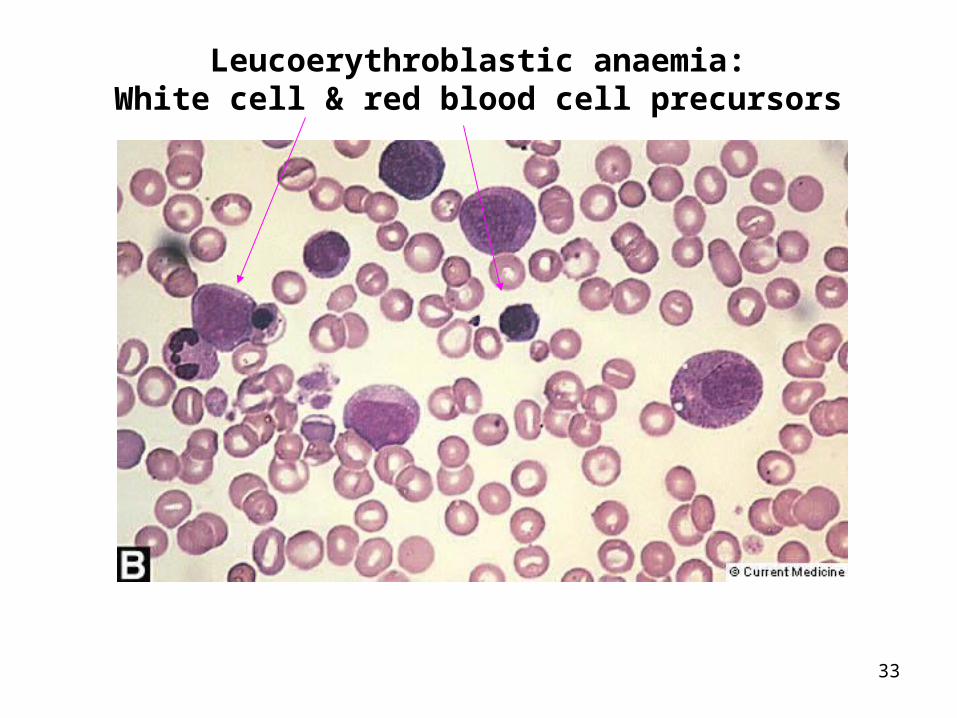
Leucoerythroblastic anaemia:White cell & red blood cell precursors

34
Leucoerythroblastic anemia:bone marrow infiltrate by cancer cells
35
Lymphocytes
• Lymphopenia– Mostly caused by drugs, e.g. steroids
• Lymphocytosis– Mostly caused by viral infections– With severe virus infections the lymphocytes
can appear activated

36
The leucocyte in viral infection:reactive lymphocytes
37
Monocytes & eosinophils
• Monocytosis– Mostly caused by chronic infections, e.g.
TB
• Eosinophilia– Parasitic infections, allergies, skin
conditions, neoplasia
38
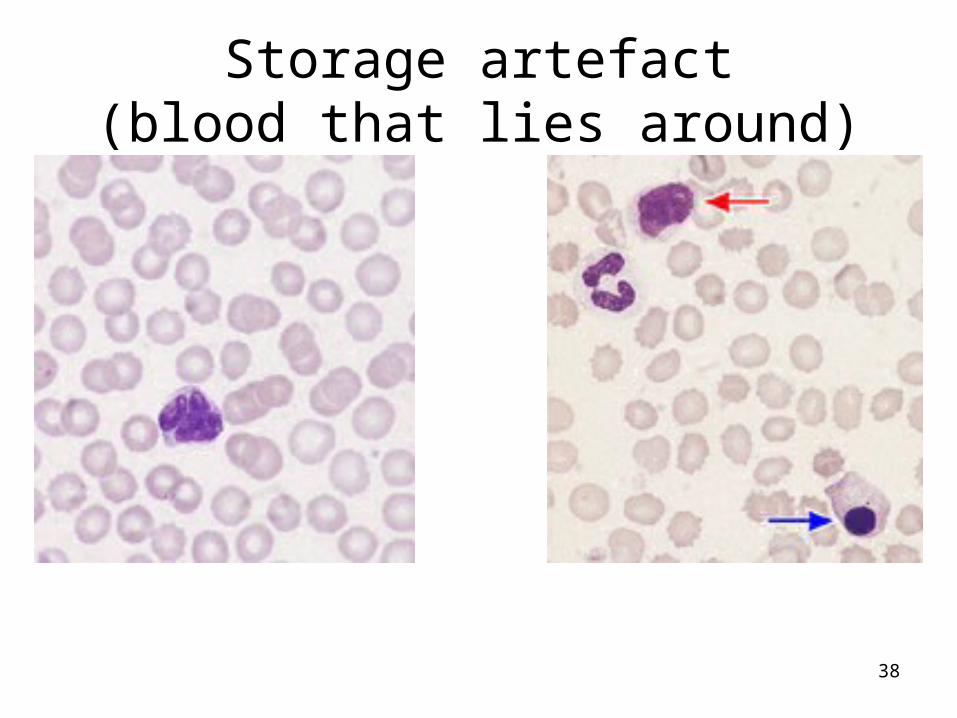
Storage artefact(blood that lies around)

39
Other infections
40
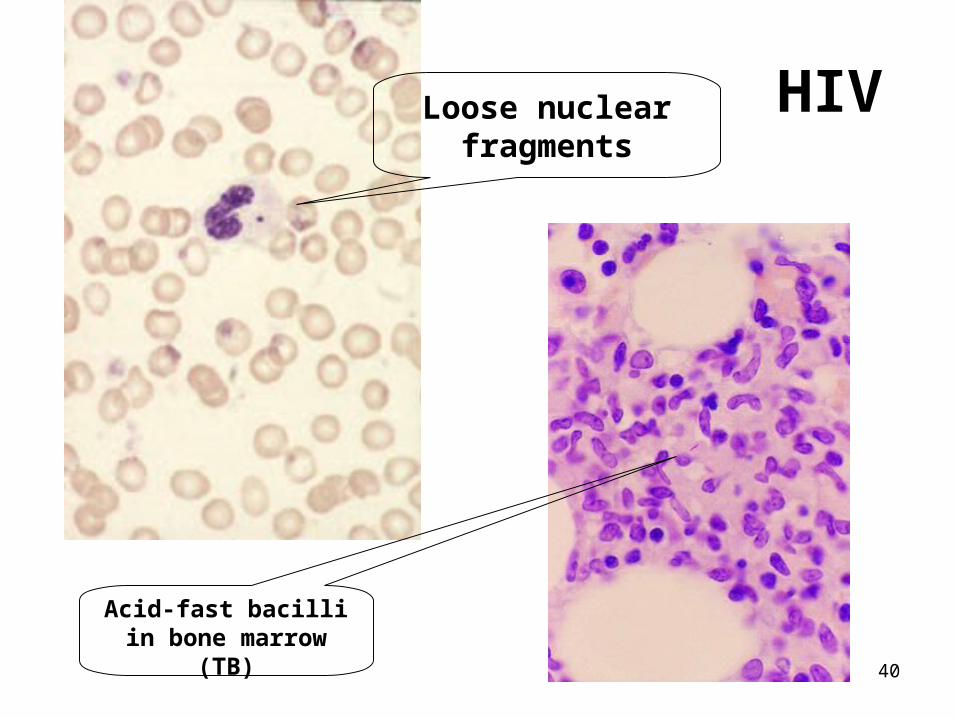
HIV
Acid-fast bacilli in bone marrow (TB)
Loose nuclear fragments
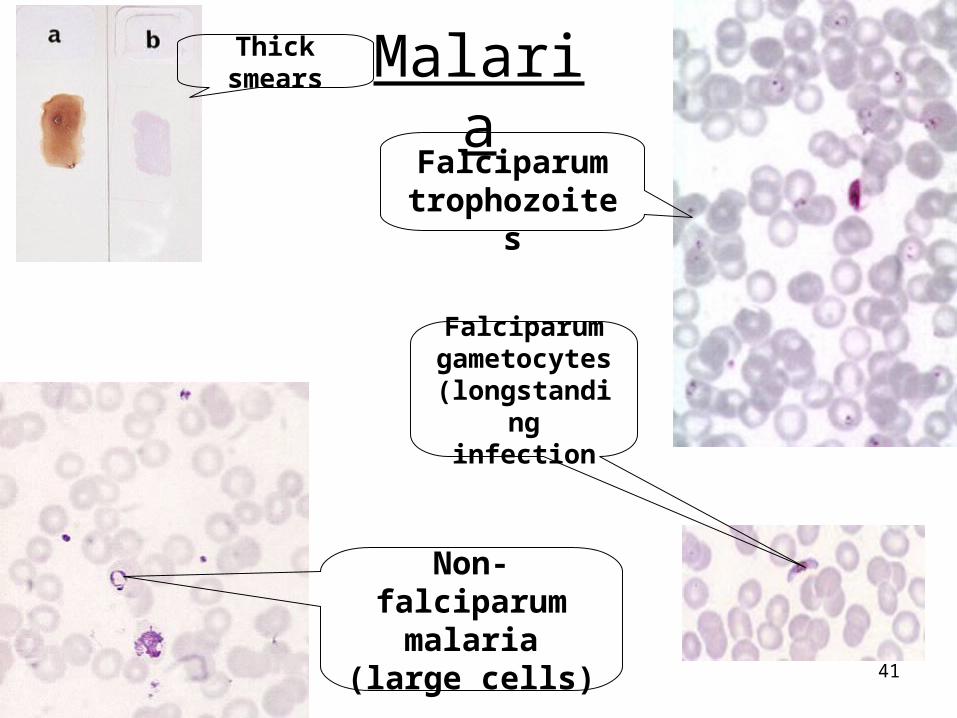
41
MalariaThick
smears
Falciparum trophozoites
Falciparum gametocytes(longstanding
infection
Non-falciparum malaria (large
cells)
42
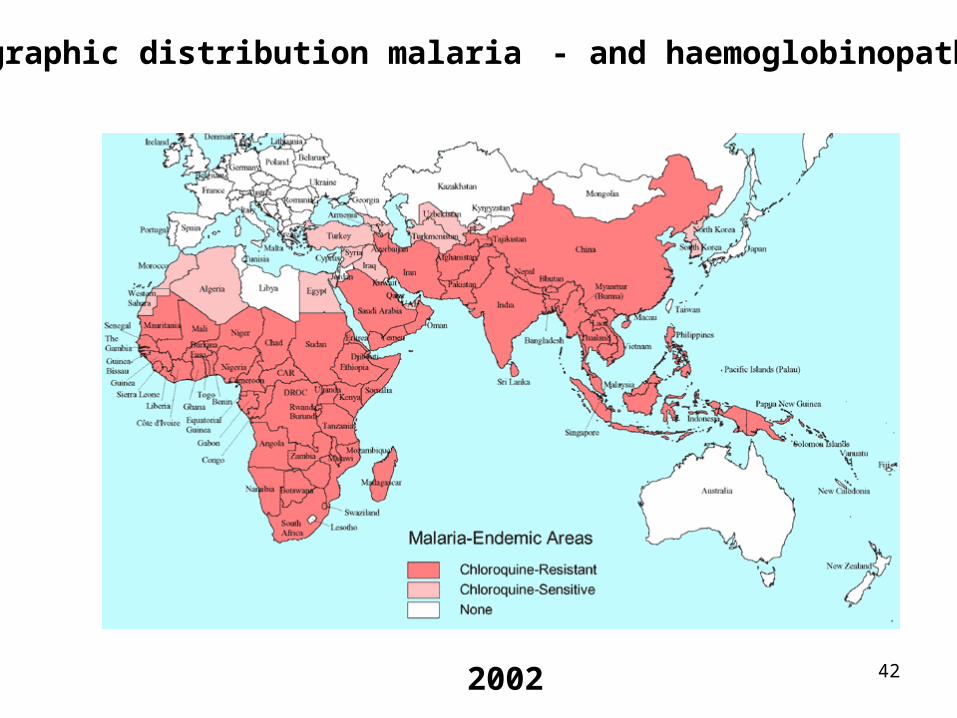
Geographic distribution malaria - and haemoglobinopathies
2002
43
Fe deficiency

44
Pallor
“Strawberry” tongue:Fe deficiency
Hands useful, regardless of ethnicity
45
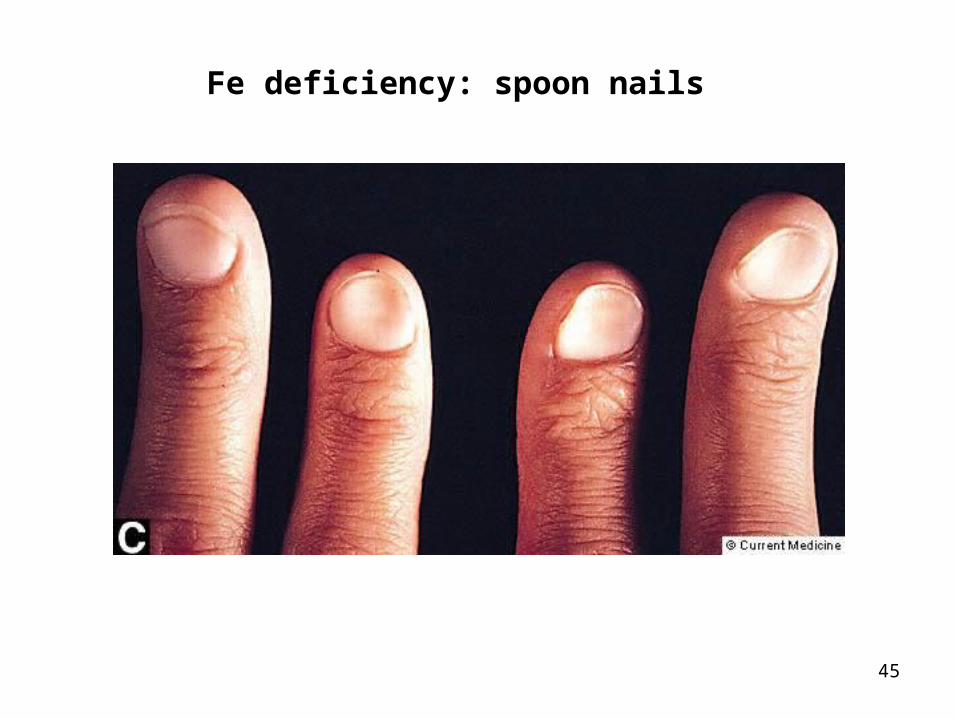
Fe deficiency: spoon nails
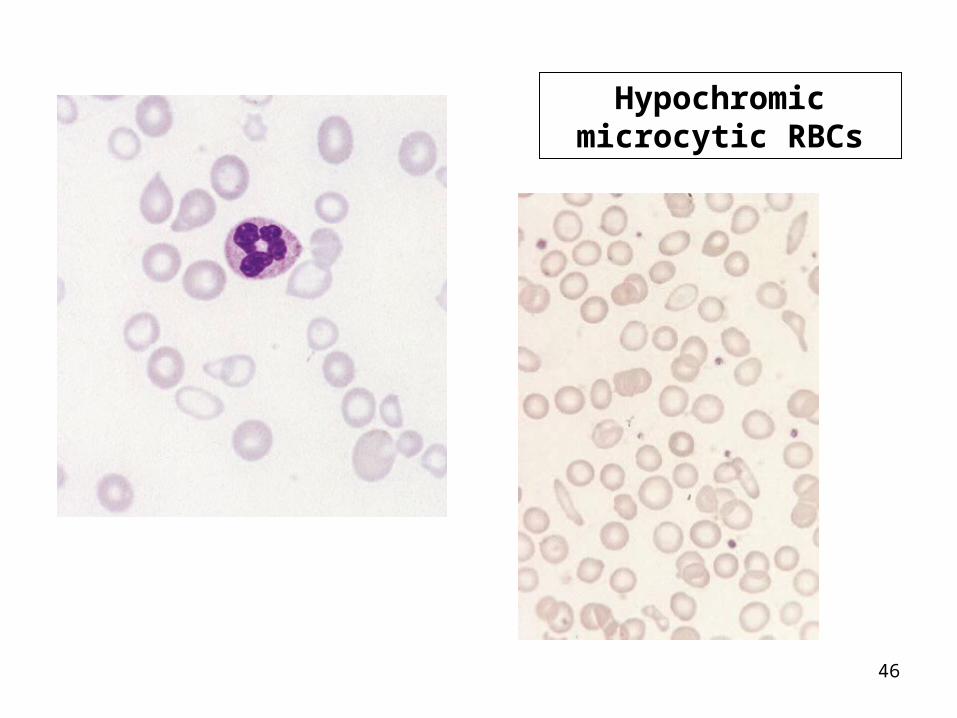
46
Hypochromic microcytic RBCs
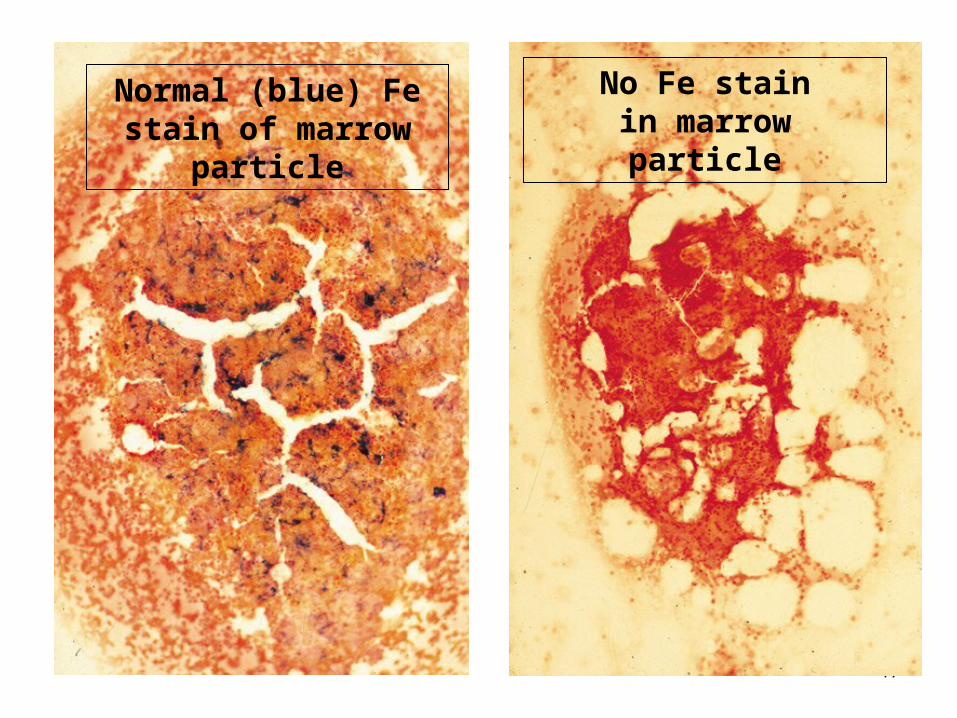
47
Normal (blue) Fe stain of marrow particle
No Fe stainin marrow particle
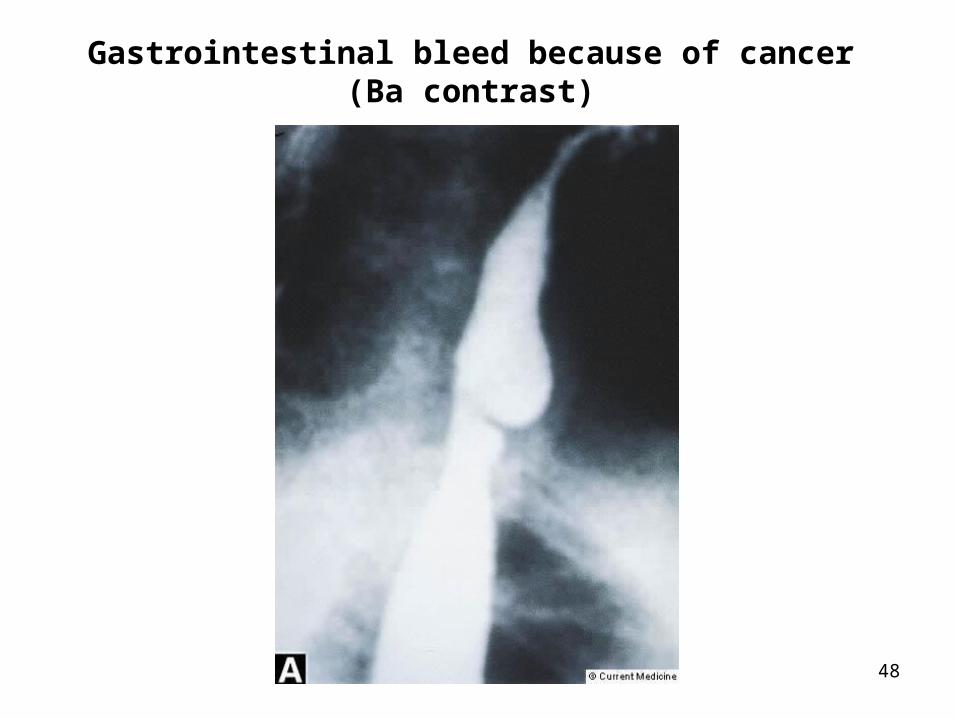
48
Gastrointestinal bleed because of cancer(Ba contrast)

49
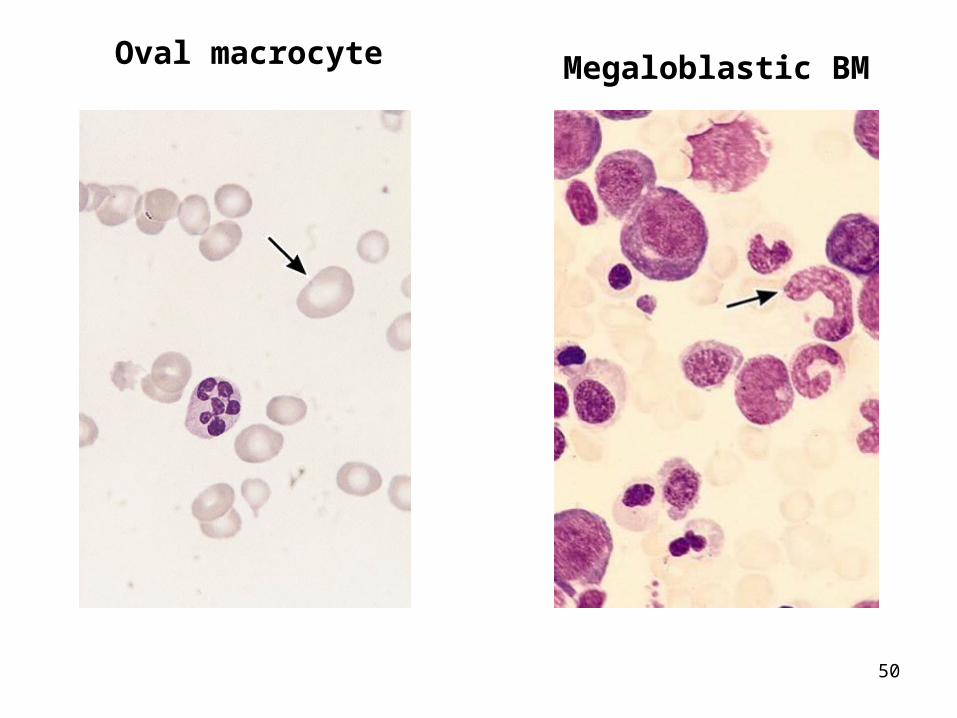
Megaloblastic anaemia
50
Oval macrocyte Megaloblastic BM
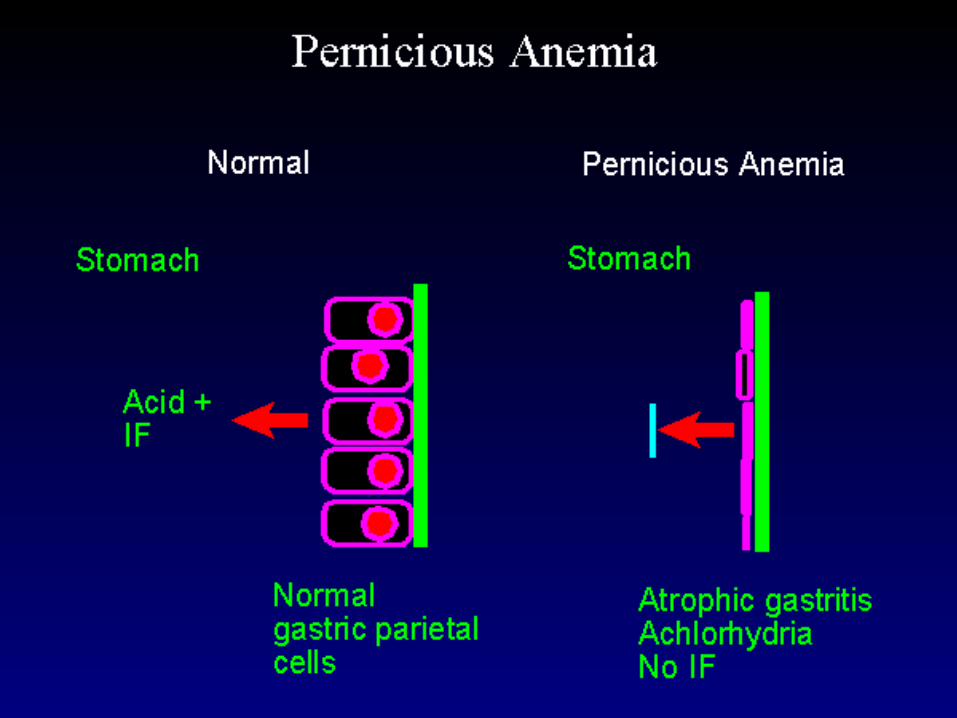
51
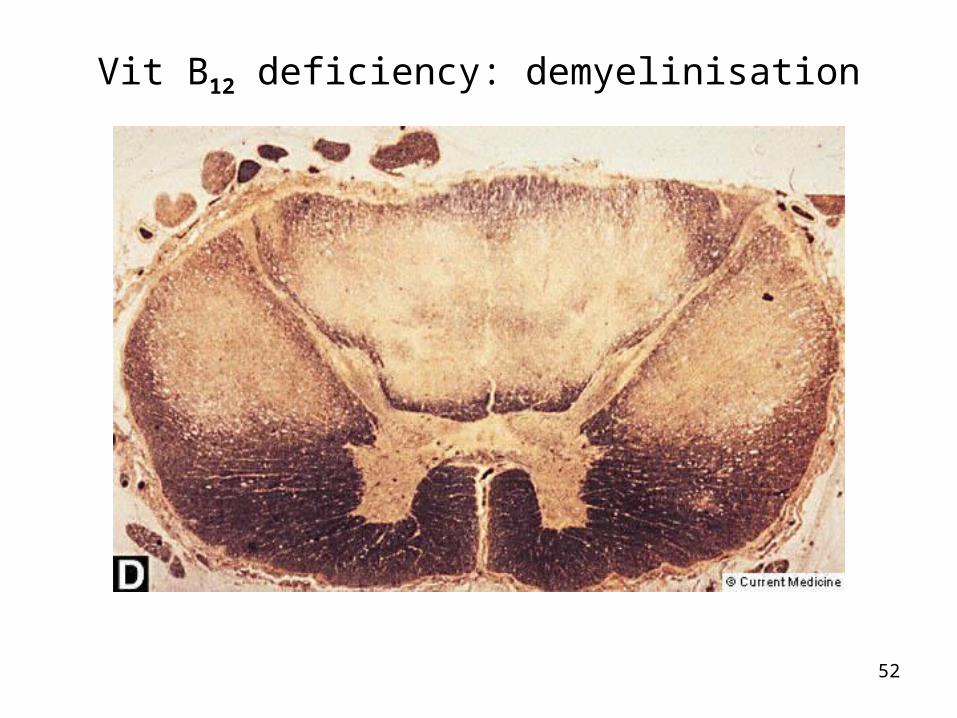
52
Vit B12 deficiency: demyelinisation
53
Haemolytic anaemias

54
Jaundice of haemolysis

55
Warm (IgG) AIHA:pherocytosis,
polychromasia, normoblasts
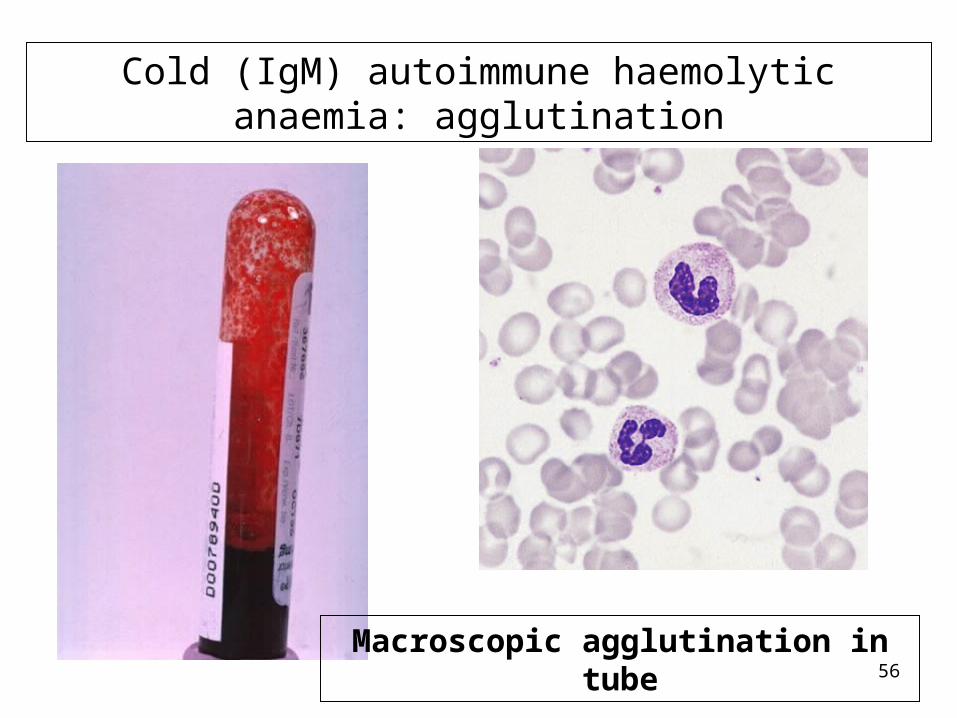
56
Cold (IgM) autoimmune haemolytic anaemia: agglutination
Macroscopic agglutination in tube

57
Mechanical haemolysis (schistocytes)
58
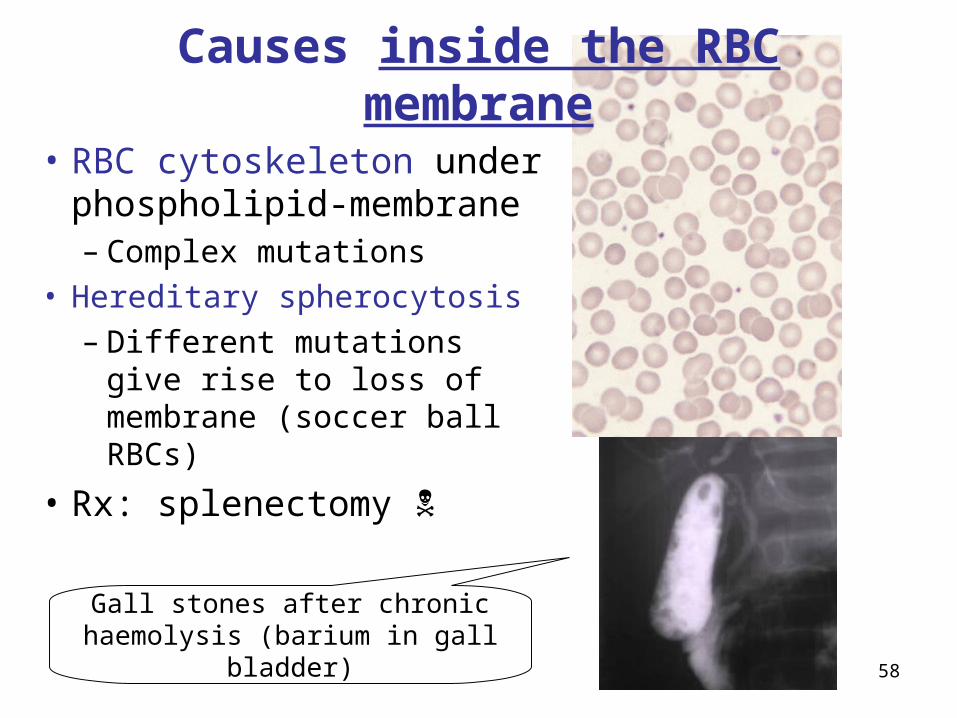
• RBC cytoskeleton under phospholipid-membrane– Complex mutations
• Hereditary spherocytosis– Different mutations give
rise to loss of membrane (soccer ball RBCs)
• Rx: splenectomy
Causes inside the RBC membrane
Gall stones after chronic haemolysis (barium in gall bladder)

59
• Enzyme deficiencies– G6PD deficiency common
in Africa
• Haemoglobinopathies– Thalassaemias, sickle Hb
• Infections– Malaria
• Falciparum
Causes inside the RBC

60

61
Aplastic anaemia:purpura ofthrombocytopenia
62
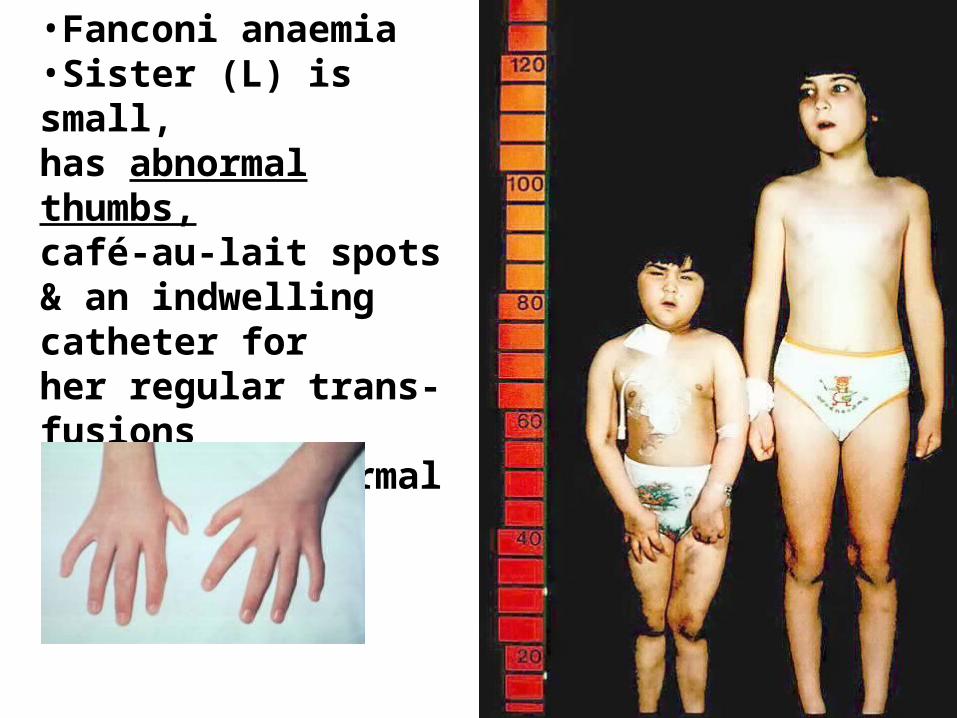
•Fanconi anaemia•Sister (L) is small,has abnormal thumbs,café-au-lait spots& an indwelling catheter forher regular trans-fusions•Sister (R) normal
63
Platelets
• Thrombocytopenia– Decreased production (bone marrow
failure) or increased destruction (ITP)
• Thrombocytosis– Reactive: infections, post-splenectomy
– Thrombocytaemia: essential thrombocythaemia

64Describe the red cells please.
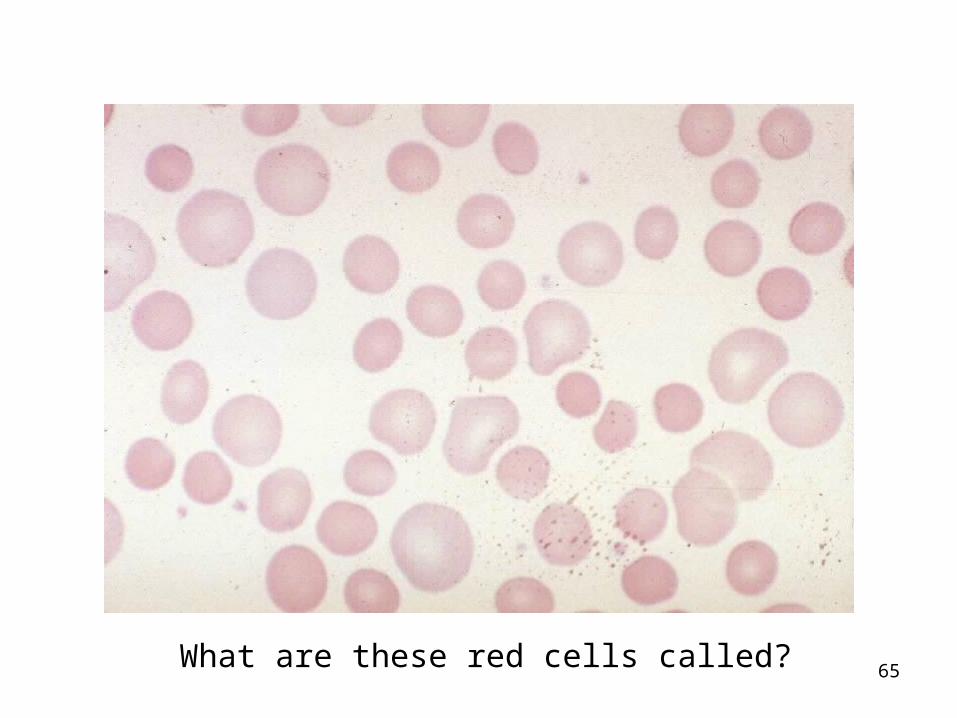
65What are these red cells called?
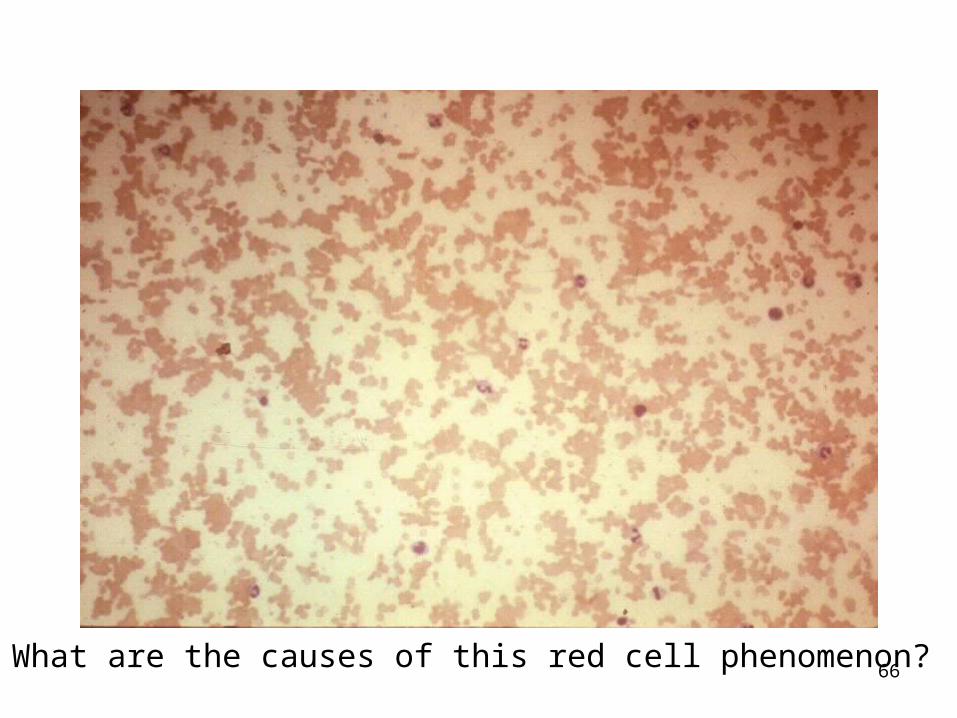
66What are the causes of this red cell phenomenon?

67
What is the naem of this haemoglobinopathy?

68What is the single cause of all these red cell changes?
69
Paper case 1• A. is a forty-five year-old lady that is
prematurely grey. She complains that she has become increasingly tired over the last few months. She can hardly walk around a block. She is also losing her balance. She is pale, slightly jaundiced and has cracks in the corners of her mouth. Her tongue is raw and her pulse is fast. She has lost her sense of vibration in her arms and legs. She has a white cell count of 2.5 x 109/l (normal 4-11 x 109/l), haemoglobin of 6 g/dl (normal 12.5-16.5 g/dl) and platelets of 100 x 109/l (normal 150-400 x 109/l). Her red cells are oval and macrocytic. The nuclei of her neutrophils are hypersegmented.

70
• Paper case 2
• N. is a 50-year old man that presents with exercise intolerance. He eats a balanced diet. He had a partial gastrectomy for a bleeding ulcer, five years ago. His full blood count shows: white cells 4 x 109/l, haemoglobin 9 g/dl and platelets 100 x 109/l. The rapport says that he has oval macrocytes.
71
Paper case 3• Ms H. is 30 years old. She has three
children and is pregnant. Her husband lost his job recently and they live in Joe Slovo informal settlement. She feels increasingly tired and presented at the Polyclinic. She becomes unsteady and complains that her heart beats fast. She has developed a taste for clay.
• She is pale and has slight ankle oedema. Her pulse is 90/min. She is 30 weeks pregnant. Her haemoglobin is 8 g/dl with a mean cell volume (MCV) of 65 fl.

72
Paper case 4T. is an 18-year old woman that has become increasingly pale and tired over the last fortnight. Her eyes are yellow. Her left upper abdomen is tender. Her mother had a similar condition as a youngster and had a splenectomy. After the operation her mother’s symptoms never recurred. T’s FBC shows the following: WBCs 7 x 109/l, haemoglobin 8 g/dl and platelets 250 x 109/l. Her blood smear shows spherocytes and her reticulocyte count is raised.
Related Documents











