1 HIV and Infant Feeding: Knowledge, Gaps, and Challenges for the Future by Ellen G. Piwoz Jay Ross Academy for Educational Development

1 HIV and Infant Feeding: Knowledge, Gaps, and Challenges for the Future by Ellen G. Piwoz Jay Ross Academy for Educational Development.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
HIV and Infant Feeding:
Knowledge, Gaps, and
Challenges for the Future
by
Ellen G. Piwoz
Jay Ross
Academy for Educational
Development

2
Overview of the Presentation
• Context of the presentation
• Overview of HIV transmission during breastfeeding
– risk factors
– timing of transmission
– feasibility of feeding alternatives
• Challenges for the future

3
Timing of Mother-to-Child HIV Timing of Mother-to-Child HIV Transmission with Breastfeeding and Transmission with Breastfeeding and
No ARVNo ARVEarly Antenatal(<36 wks)
Late Antenatal(36 wks to labor)
Late Postpartum(6-24 months)
Early Postpartum(0-6 months)
Adapted from N Shaffer, CDC
5-10% 10-20% 10-20%
Labor and Delivery

4
MTCT in 100 HIV+ Mothers by Timing of Transmission
0
20
40
60
80
100
# uninfected
# infected duringBF for 2 yrs
# infected duringdelivery
#infants infectedduring pregnancy
63
uninfected
15
157
5
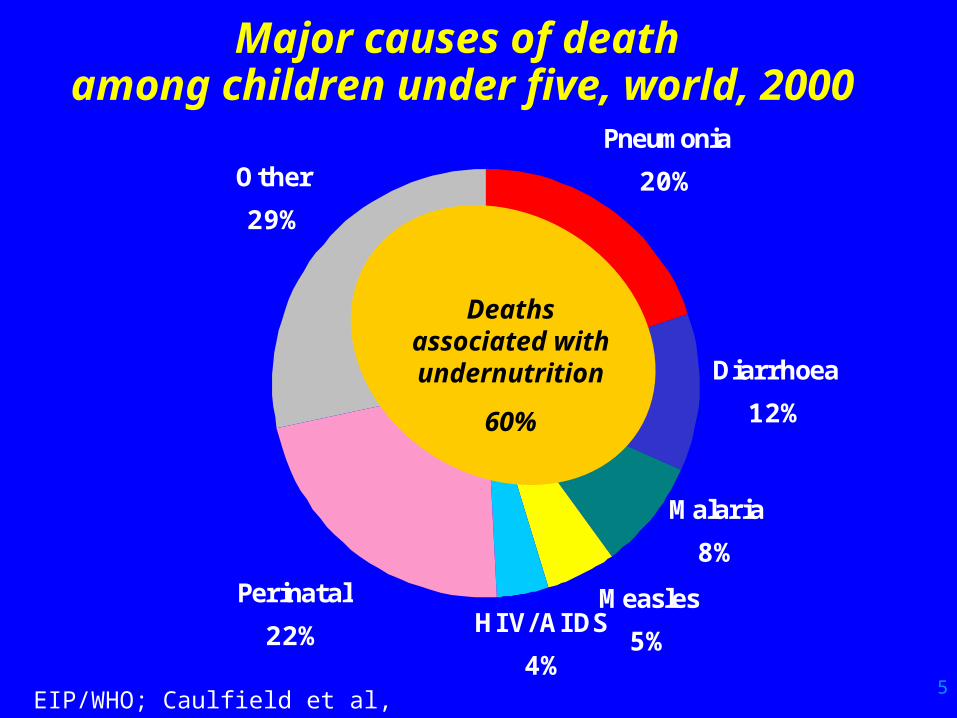
Other
29%
Diarrhoea
12%
Pneumonia
20%
Malaria
8%
Measles
5%HIV/AIDS
4%
Perinatal
22%
Deaths associated with undernutrition
60%
Major causes of death among children under five, world, 2000
EIP/WHO; Caulfield et al, forthcoming
6
Technical Overview of HIV Transmission
during Breastfeeding
7
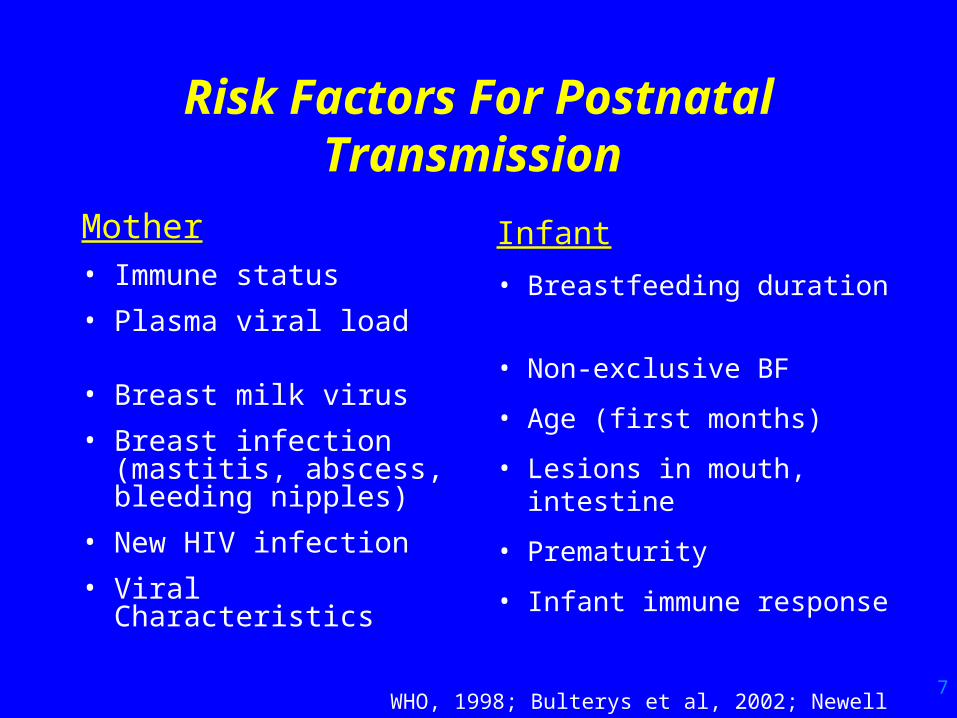
Risk Factors For Postnatal Transmission
Mother• Immune status
• Plasma viral load
• Breast milk virus
• Breast infection (mastitis, abscess, bleeding nipples)
• New HIV infection
• Viral Characteristics
Infant
• Breastfeeding duration
• Non-exclusive BF
• Age (first months)
• Lesions in mouth, intestine
• Prematurity
• Infant immune response
WHO, 1998; Bulterys et al, 2002; Newell et al, 2002
8
How does HIV transmission during breastfeeding occur?
• Exact mechanisms unknown
• HIV virus in blood passes to breast milk– cell-free, cell-associated virus observed
– virus shed intermittently (undetectable ~ 25-35%)
– levels vary between breasts in samples taken at same time (Willumsen et al, 2001)
• Infant consumes HIV– enters/infects through permeable mucosal surfaces, lymphoid tissues,
lesions in mouth, intestine
• Although BF infant may consume >500,000 virons, >25,000 infected cells per day, majority don’t become infected (Lewis et al, 2001)
– immune factors in BM may play a role (Sabbaj et al, 2002)
9
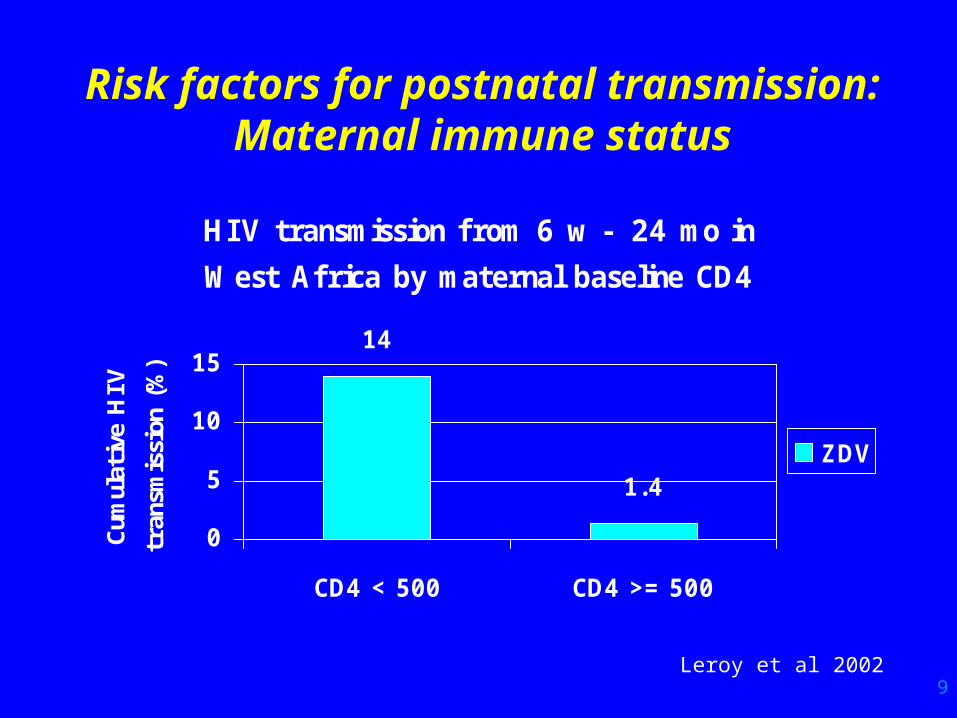
Risk factors for postnatal transmission: Maternal immune
statusHI V transmission from 6 w - 24 mo in
West Africa by maternal baseline CD4
14
1.4
0
5
10
15
CD4 < 500 CD4 >= 500
Cum
ulat
ive
HIV
tran
smis
sion
(%
)
ZDV
Leroy et al 2002

10
Risk factors for postnatal transmission: Maternal viral load
• Viral RNA is an important predictor of intra-partum MTCT (Leroy et al, 2001; Semba et al, 1999; Thea et al, 1997)
• Plasma viral load may also be a risk factor during breastfeeding
– 29% transmission risk among women infected postnatally (Dunn et al, 1992)
– risk of infection after 2 months associated with plasma viral load > 43k copies/ml (John et al, 2001) (OR=2.6)
– predicted MTCT by 12 months, after taking into account maternal immune status, Na+ in breast milk (Semba et al, 1999) (Adj OR=1.71 log HIV load)
11
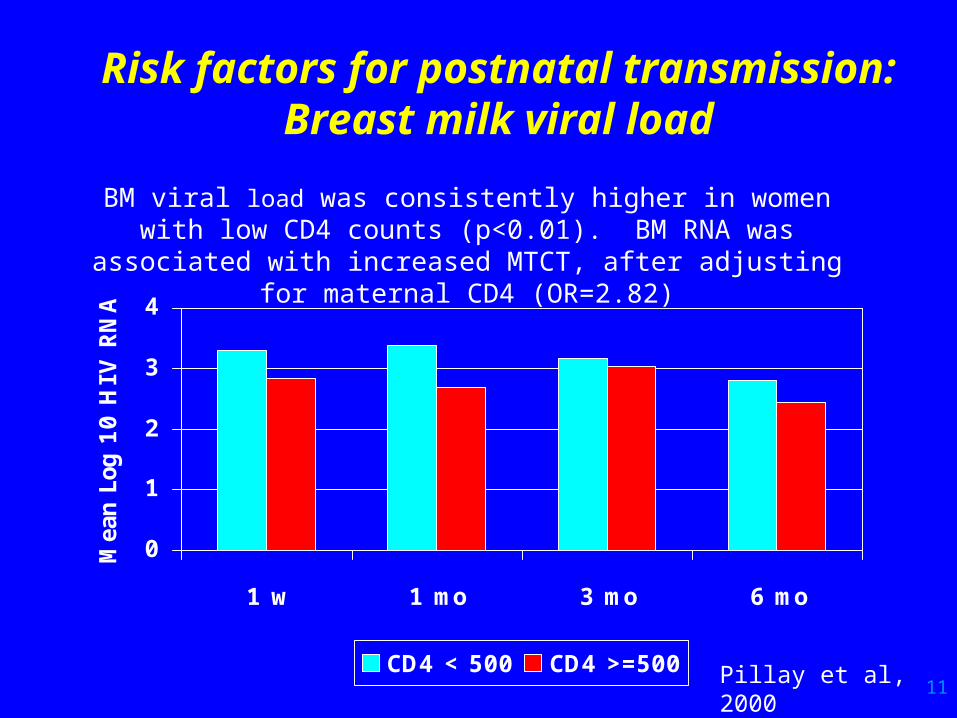
Risk factors for postnatal transmission:
Breast milk viral load
0
1
2
3
4
1 w 1 mo 3 mo 6 mo
Mea
n Lo
g 10 H
IV R
NA
CD4 < 500 CD4 >=500 Pillay et al, 2000
BM viral load was consistently higher in women with low CD4 counts (p<0.01). BM RNA was associated with increased MTCT, after adjusting for maternal CD4
(OR=2.82)
12
Prevalence of breast pathologies in HIV+ women in Africa
• Mastitis (clinical or sub-clinical):– Clinical exam: 7-11% (Embree, 2000; John et al, 2001)
– Na+/K > 1.0: 11-12% at 6, 14 wk (Willumsen et al, 2000)
– Na+ > 12 mmol/L: 16.4% at 6 wk (Semba et al, 1999)
• Nipple lesions:– Clinical exam: 11-13% (Embree, 2000; John et al, 2001)
– Clinical exam: 10% (Ekpini et al, 1997)
– Hospitalized infants: 11% (Kambarami et al, 1997)
• Breast abscesses:– Clinical exam: 12% (John et al, 2001)
– Clinical exam: 3% (Ekpini et al, 1997)

13
Risk factors for postnatal transmission:
Breast health -1• Sub-clinical mastitis is associated with higher viral load
in BM (Willumsen et al, 2000; Semba et al, 1999)
• Mastitis is associated with increased risk of postnatal transmission:
Kenya (Embree; > 3 mo) OR=2.3 (1.1-5.0)
Kenya (John; overall) RR=3.9 (1.2-12.7)
Kenya (John; >=2 mo) RR=21.8 (2.3-211)
Malawi (Semba; overall) OR=2.3 (1.2-4.3)
Malawi (Semba; > 6 wk) RR=3.7 (NS)
• Nipple lesions and breast abscesses also associated with increased transmission

14
Risk factors for postnatal transmission:
Breast health -2• 18-20% of overall MTCT may be attributable to
mastitis (estimated from mastitis prevalence and adjusted risk estimates):
– 18% of all transmission in first year in Malawi (Semba et al, 1999)
– 20% of transmission up to 2 years (John et al, 2001)
• If BF accounts for 40% of all transmission, then mastitis (breast health problems) may be the cause of 50% all postnatal transmission (20/40)

15
Risk factor for postnatal transmission: Duration of
breastfeeding• Risk of transmission persists for as long as
breastfeeding is practiced• Some studies indicate that the risk of HIV
transmission may be higher in the first 6 months of life (Miotti et al, 1999; Nduati et al, 2000; John et al, 2001)
• Several possible explanations – higher prevalence of mastitis, breastfeeding problems
– infant gut more immature, vulnerable/permeable
– more breast milk consumed

16
Postnatal transmission of HIV:Duration of breastfeeding Ghent meta-analysis -2
(Read et al, 2002)
4
9
16
0
5
10
15
20
4 w to 6 mo up to 12 mo up to 18 m
Cumulative rates of late postnatal HIV infection (> 4 wks)
17
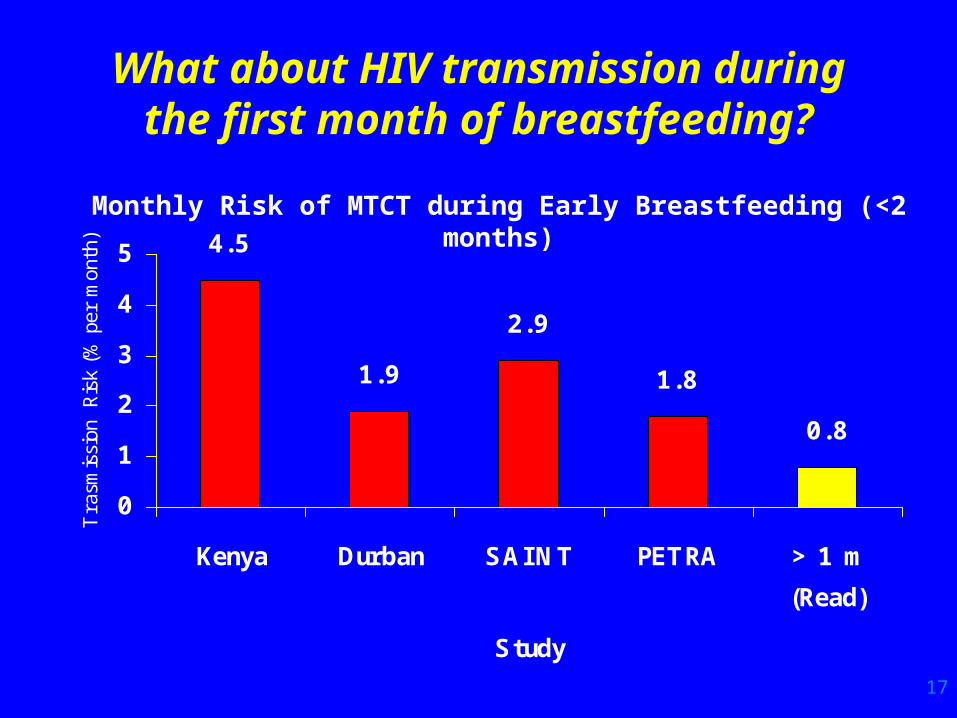
What about HIV transmission during the first month of
breastfeeding?
4.5
1.9
2.9
1.8
0.8
0
1
2
3
4
5
Kenya Durban SAINT PETRA > 1 m
(Read)
Study
Tra
smis
sion
Ris
k (%
per
mon
th)
Monthly Risk of MTCT during Early Breastfeeding (<2 months)
18
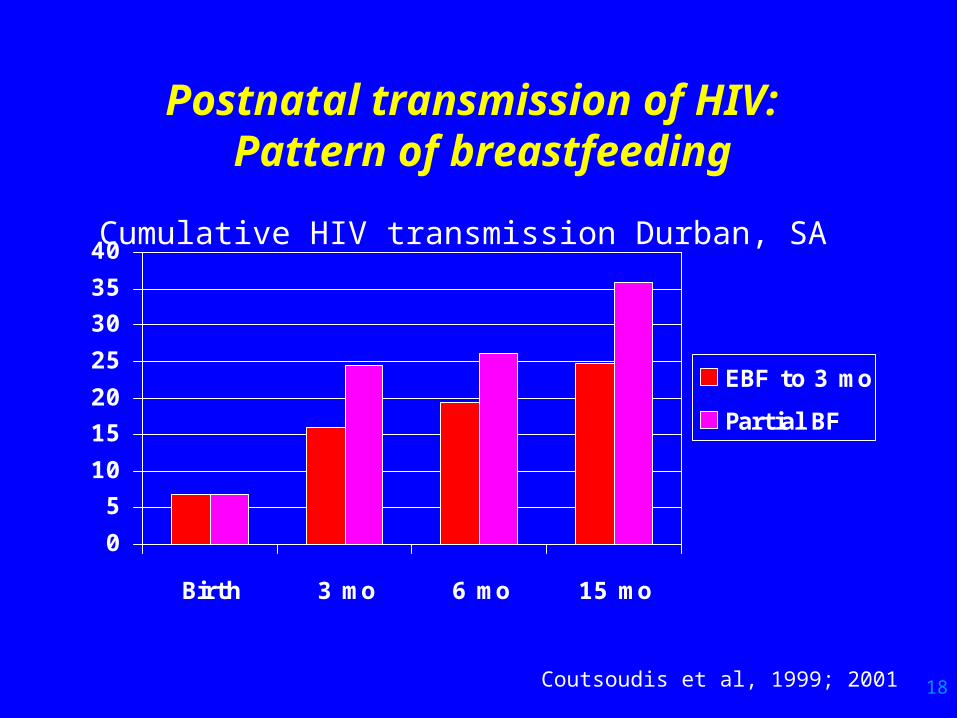
Postnatal transmission of HIV: Pattern of breastfeeding
0
5
10
15
20
25
30
35
40
Birth 3 mo 6 mo 15 mo
EBF to 3 mo
Partial BF
Coutsoudis et al, 1999; 2001
Cumulative HIV transmission Durban, SA

19
Infant mortality among children born to HIV+ mothers by early feeding pattern (0-3 months) in Harare,
Zimbabwe (n=2,892) Tavengwa et al, 2002
50
95 104
210
0
50
100
150
200
250
EBF Predominant
BF
Partial BF BM+NHM
dea
ths/
1000
Adjusted HR for BM+NHM vs EBF = 5.97 (p<0.001); Predominant BF vs EBF=2.52 (p=0.04); Partial BF vs EBF=2.84 (p=0.02)

20
Risk factors for postnatal transmission: Infant oral lesions
• Disruption of the skin or mucous membranes in mouth and intestine believed to increase the risk of HIV transmission during breastfeeding
– epithelial integrity affected by nutritional deficiencies, infection
– feeding pattern, mastitis did not effect intestinal permeability (Rollins et al, 2001; Willumsen et al, 2000)
• Infant oral thrush associated with increased risk of postnatal transmission
– Kenya: OR=2.8 (1.3-6.2) (Embree et al, 2000)
– Cote d’ Ivoire: RR=5.0 (0.5-39.8) (Ekpini et al, 1997)
21
Infant Feeding Options for HIV+ Mothers

22
WHO recommendations on infant feeding for HIV+
women“When replacement feeding is acceptable, feasible,
affordable, sustainable and safe, avoidance of all breastfeeding by HIV-infected mothers is recommended.
Otherwise, exclusive breastfeeding is recommended during the first months of life.
To minimize HIV transmission risk, breastfeeding should be discontinued as soon as feasible, taking into account local circumstances, the individual woman’s situation and the risks of replacement feeding (including infections other than HIV and malnutrition).”
New Data on the Prevention of Mother-to-Child Transmission of HIV and their Policy Implications: Conclusions and Recommendations (WHO 2001)
23
How Can Families Decide? -1
• What is meant by ACCEPTABLE?
– There are social and cultural norms about infant feeding.
– Concerns about stigma associated women who do not breastfeed, suspicion of HIV
• What is meant by FEASIBLE?
– There are economic, behavioral, psycho-social aspects for care-giver and infant
– Resources and skills are required
24
How Can Families Decide? -2
• What is meant by SUSTAINABLE?
– It must be practiced every day and night
– Resources must be available throughout
– It should be exclusive over first 6 months
• What is meant by SAFE?
– Free from contamination
– Nutritious
– Free from stigma
– Does not spillover to general population

25
Infants who do not breastfeed have an increased risk of dying in
the first year of life
5.8
4.1
2.51.8 1.4
0
2
4
6
0- 1 2- 3 4- 5 6- 8 9- 11
Age in months
WHO Collaborative Study Team, 2000
Pooled Odds Ratios
Related Documents











