1 Downloaded from www.cozaar.ae The Losartan Intervention For Endpoint reduction in hypertension study An investigator-initiated, prospective, community- based, multinational, double-blind, double-dummy, randomised, active-controlled, parallel-group study from 945 centres Dahlöf B et al Lancet 2002;359:995-1003. Steering Committee Chair: Co-chair: B. Dahlöf R.B. Devereux

1 Downloaded from The L osartan I ntervention F or E ndpoint reduction in hypertension study An investigator-initiated, prospective,
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Downloaded from www.cozaar.ae
The Losartan Intervention For Endpoint reductionin hypertension study
An investigator-initiated, prospective, community-based, multinational, double-blind, double-dummy, randomised, active-controlled, parallel-group study from 945 centres
Dahlöf B et al Lancet 2002;359:995-1003.
Steering Committee Chair: Co-chair:B. Dahlöf R.B. Devereux

2
Downloaded from www.cozaar.ae
Clinical Experience with Losartan
• Losartan is a leader in comprehensive clinical trials, encompassing– 30,000 patients– 4 mega-trials (LIFE, OPTIMAAL, ELITE II, RENAAL)– > 4500 publications
• Losartan and losartan-based regimen have been prescribed to 12 million patients worldwide
• Losartan has proven excellent tolerability
Dahlöf B et al Am J Hypertens 1997; 10: 705713; Dickstein K et al Am J Cardiol 1999; 83: 477481; Pitt B et al Lancet 2000; 355: 15821587; Brenner BM et al N Eng J Med 2001; 345(12): 861869; Bloom BS Clin Ther 1998;20(4):671-681; Goldberg et al Am J Cardiol 1995;75:793-795.
3
Downloaded from www.cozaar.ae
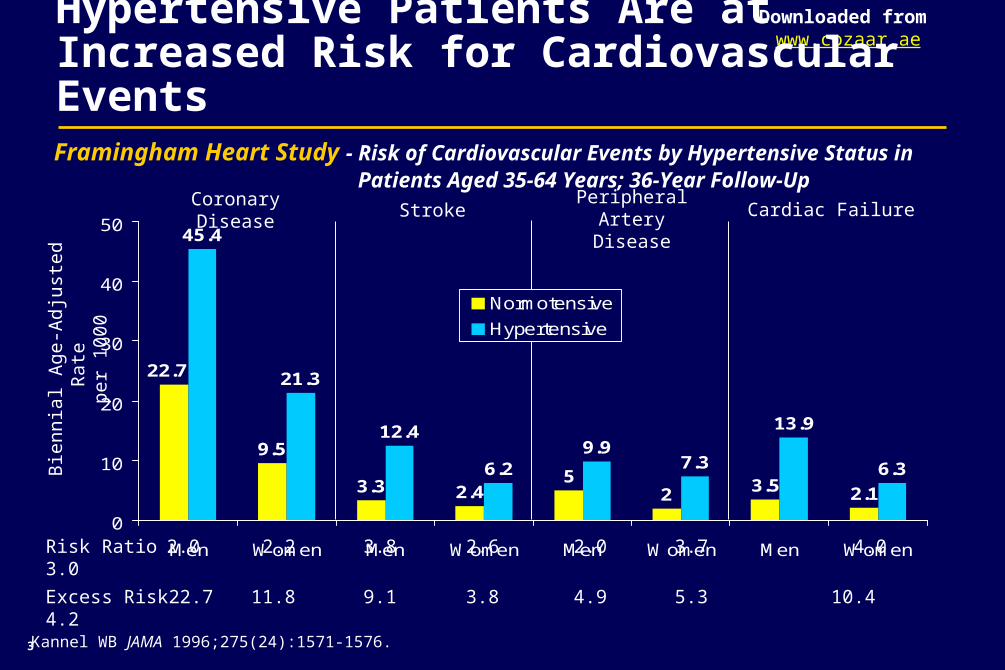
Hypertensive Patients Are at Increased Risk for Cardiovascular Events
Framingham Heart Study - Risk of Cardiovascular Events by Hypertensive Status in Patients Aged 35-64 Years; 36-Year Follow-Up
9.5
3.3 2.45
2 3.5 2.1
45.4
21.3
12.4
6.29.9
7.3
13.9
6.3
22.7
0
10
20
30
40
50
Men Women Men Women Men Women Men Women
Normotensive
Hypertensive
Risk Ratio 2.0 2.2 3.8 2.6 2.0 3.7 4.0 3.0
Excess Risk 22.7 11.8 9.1 3.8 4.9 5.3 10.4 4.2
Coronary Disease Stroke Peripheral ArteryDisease
Cardiac Failure
Bie
nni
al A
ge-A
djus
ted
Rat
e pe
r 10
00
Kannel WB JAMA 1996;275(24):1571-1576.
4
Downloaded from www.cozaar.ae
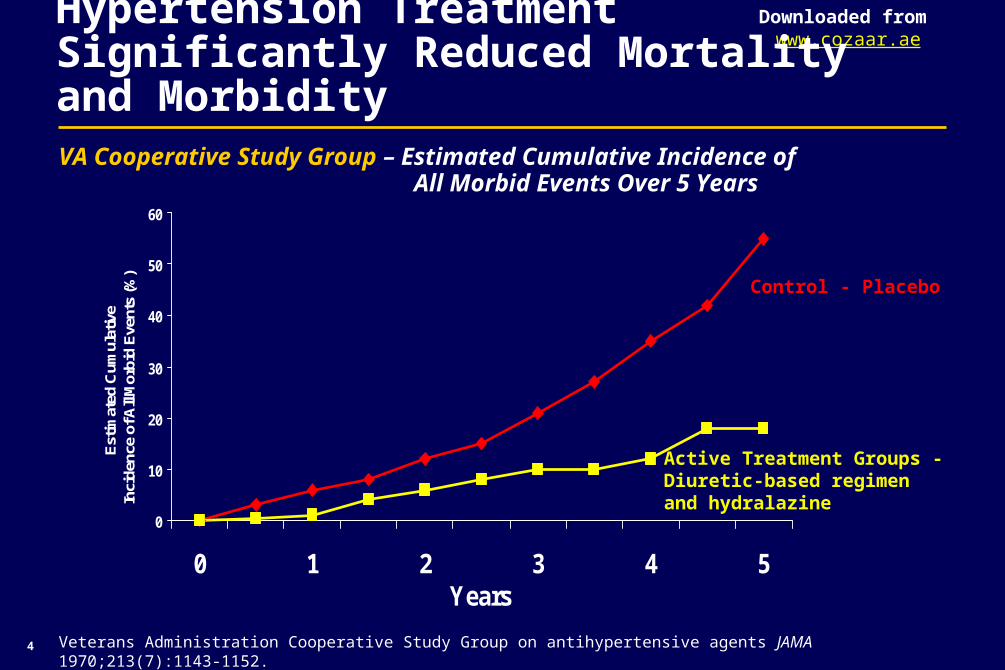
Hypertension Treatment Significantly Reduced Mortality and MorbidityVA Cooperative Study Group – Estimated Cumulative Incidence of
All Morbid Events Over 5 Years
Veterans Administration Cooperative Study Group on antihypertensive agents JAMA 1970;213(7):1143-1152.
0
10
20
30
40
50
60
0 1 2 3 4 5Years
Est
imat
ed C
umul
ativ
e In
cide
nce
of A
ll M
orbi
d E
vent
s (%
)
Control - Placebo
Active Treatment Groups - Diuretic-based regimen and hydralazine
5
Downloaded from www.cozaar.ae
Beta Blockers and Diuretics Lower Risk of Cardiovascular Events
• In hypertension, beta blockers and diuretics have proven risk reduction in cardiovascular morbidity and mortality vs. placebo
– STOP, HEP, MRC Trials
• Hypertension guidelines recommend beta blockers or diuretics as one of the initial treatments for hypertension
– JNC-VI, WHO/ISH Hypertension Treatment Guidelines
Dahlöf B et al. Lancet 1991;338:1281-85; Coope J et al Brit Med J 1986;293:1145-51; MRC Working Party Brit Med J 1985;291:97-104; JNC-VI Treatment of High Blood Pressure Guidelines,1999 WHO/ISH Hypertension Guidelines.
6
Downloaded from www.cozaar.ae
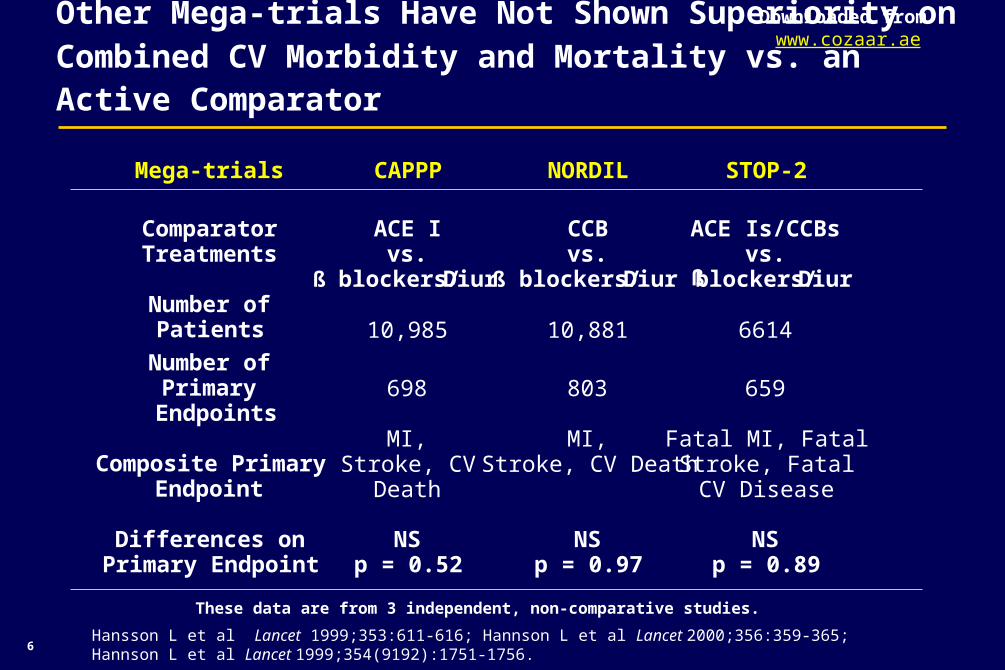
Mega-trials CAPPP NORDIL STOP-2
ComparatorTreatments
ACE Ivs.
ß blockers/Diur
CCBvs.
ß blockers/Diur
ACE Is/CCBsvs.
ßblockers/DiurNumber of
Patients 10,985 10,881 6614
Number ofPrimary
Endpoints698 803 659
Composite PrimaryEndpoint
MI,Stroke, CV
Death
MI,Stroke, CV Death
Fatal MI, FatalStroke, FatalCV Disease
Differences onPrimary Endpoint
NSp = 0.52
NSp = 0.97
NSp = 0.89
Other Mega-trials Have Not Shown Superiority on Combined CV Morbidity and Mortality vs. an Active Comparator
These data are from 3 independent, non-comparative studies.
Hansson L et al Lancet 1999;353:611-616; Hannson L et al Lancet 2000;356:359-365; Hannson L et al Lancet 1999;354(9192):1751-1756.
7
Downloaded from www.cozaar.ae
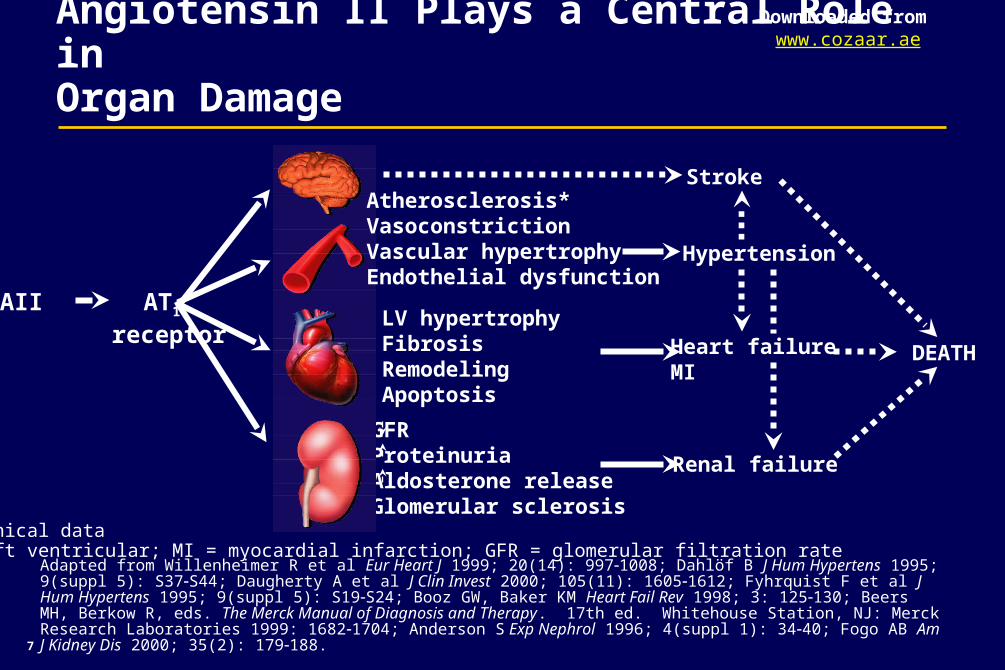
GFRProteinuriaAldosterone releaseGlomerular sclerosis
Angiotensin II Plays a Central Role inOrgan Damage
Adapted from Willenheimer R et al Eur Heart J 1999; 20(14): 9971008; Dahlöf B J Hum Hypertens 1995; 9(suppl 5): S37S44; Daugherty A et al J Clin Invest 2000; 105(11): 16051612; Fyhrquist F et al J Hum Hypertens 1995; 9(suppl 5): S19S24; Booz GW, Baker KM Heart Fail Rev 1998; 3: 125130; Beers MH, Berkow R, eds. The Merck Manual of Diagnosis and Therapy. 17th ed. Whitehouse Station, NJ: Merck Research Laboratories 1999: 16821704; Anderson S Exp Nephrol 1996; 4(suppl 1): 3440; Fogo AB Am J Kidney Dis 2000; 35(2): 179188.
Atherosclerosis*VasoconstrictionVascular hypertrophyEndothelial dysfunction
LV hypertrophyFibrosisRemodelingApoptosis
Stroke
DEATH
*preclinical dataLV = left ventricular; MI = myocardial infarction; GFR = glomerular filtration rate
Hypertension
Heart failureMI
Renal failure
AII AT1 receptor
8
Downloaded from www.cozaar.ae
LIFE: Rationale
• To date, no treatment of essential hypertension has proven additional protective benefits for prevention of combined CV morbidity and mortality beyond lowering blood pressure with beta blockers and diuretics
• LVH is a strong risk factor for cardiovascular events
• Selective AII antagonism with losartan may reduce the risk of cardiovascular morbidity and death beyond blood-pressure lowering in patients with HT and LVH
Adapted from Dahlöf B et al Lancet 2002;359:995-1003; Dahlöf B et al Am J Hypertens 1997; 10: 705713; Levy D Drugs 1988; 35(suppl 5): 15; Verdechhia et al Circulation 2001;104:2039-2044; Kannel WB Am J Med 1983;
75(suppl 3A): 411.
9
Downloaded from www.cozaar.ae
Hypothesis
Losartan will reduce the incidence of the primary composite endpoint of cardiovascular morbidity and mortality (defined as stroke, MI or cardiovascular death) to a greater extent as compared to atenolol in patients with essential hypertension and LVH
Dahlöf B et al Am J Hypertens 1997; 10: 705713.
10
Downloaded from www.cozaar.ae
LIFE: Choice of Atenolol as Comparator
• A rigorous test of the study hypothesis required a comparator that had already been shown to reduce the risk of cardiovascular morbidity and mortality
• Beta blockers have well established beneficial cardiovascular effects in higher-risk patients
• Atenolol is the most widely prescribed beta blocker
Dahlöf B et al Am J Hypertens 1997; 10: 705713; MacMahon S, Rodgers A J Vasc Med Biol 1993; 4: 265271; Collins R et al Lancet 1990; 335: 827838; Dahlöf B et al Am J Hypertens 1995; 8: 578583; IMS 2002, MAT Patient Days of Therapy - Beta Blocker Market Share.
11
Downloaded from www.cozaar.ae
LIFE: A Landmark Study
• 9193 hypertensive patients with LVH, aged 55-80 years
• Mean 4.8-year follow-up
• 44,119 patient-years of follow-up
• 945 study sites in 7 countries
• 1096 patients with primary endpoints
Investigator-initiated, prospective, double-blind, active-controlled, intention-to-treat, community-based study
Dahlöf B et al Lancet 2002;359:995-1003.
12
Downloaded from www.cozaar.ae
Dahlöf B et al Am J Hypertens 1997;10:705713.
LIFE: Inclusion Criteria
• Age 55–80 years
• Previously treated or untreated hypertension
• Diastolic BP 95–115 mmHg or systolic BP 160–200 mmHg
• ECG-confirmed LVH
– Cornell Voltage Product > 2440 mm X msec
– Sokolow-Lyon > 38 mm
13
Downloaded from www.cozaar.ae
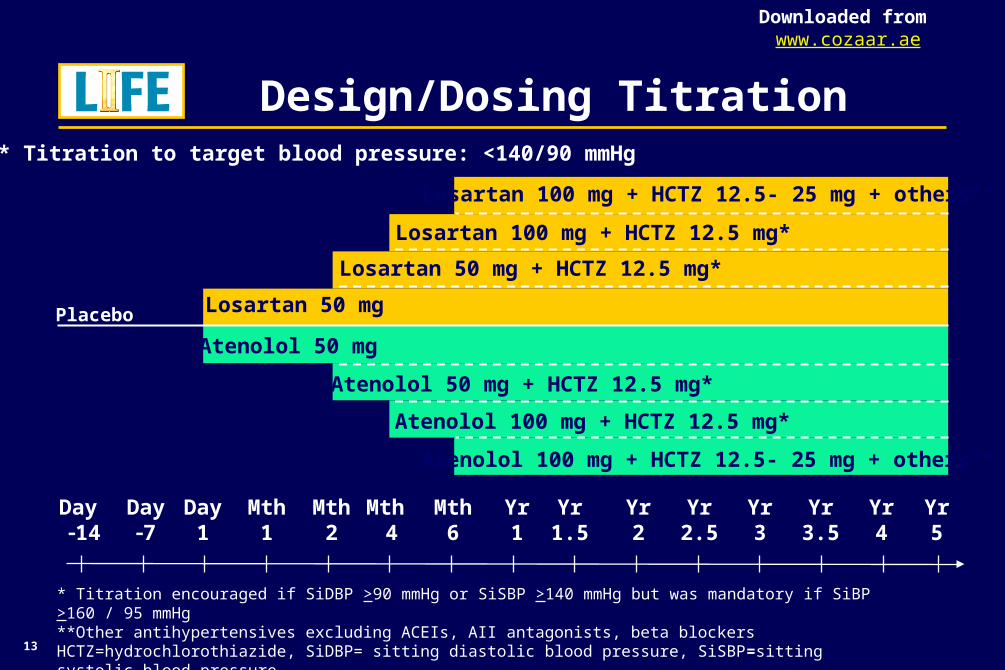
* Titration encouraged if SiDBP >90 mmHg or SiSBP >140 mmHg but was mandatory if SiBP >160 / 95 mmHg**Other antihypertensives excluding ACEIs, AII antagonists, beta blockersHCTZ=hydrochlorothiazide, SiDBP= sitting diastolic blood pressure, SiSBP=sitting systolic blood pressure Dahlöf B et al Am J Hypertens 1997;10:705713.
LIFE: Design/Dosing Titration
Day 14
Day7
Day1
Mth1
Mth2
Mth 4
Mth6
Yr1
Yr1.5
Yr2
Yr2.5
Yr3
Yr3.5
Yr4
Yr5
* Titration to target blood pressure: <140/90 mmHg
Placebo Losartan 50 mg
Atenolol 50 mg
Losartan 50 mg + HCTZ 12.5 mg*
Losartan 100 mg + HCTZ 12.5 mg*
Losartan 100 mg + HCTZ 12.5- 25 mg + others**
Atenolol 50 mg + HCTZ 12.5 mg*
Atenolol 100 mg + HCTZ 12.5 mg*
Atenolol 100 mg + HCTZ 12.5- 25 mg + others**
14
Downloaded from www.cozaar.ae
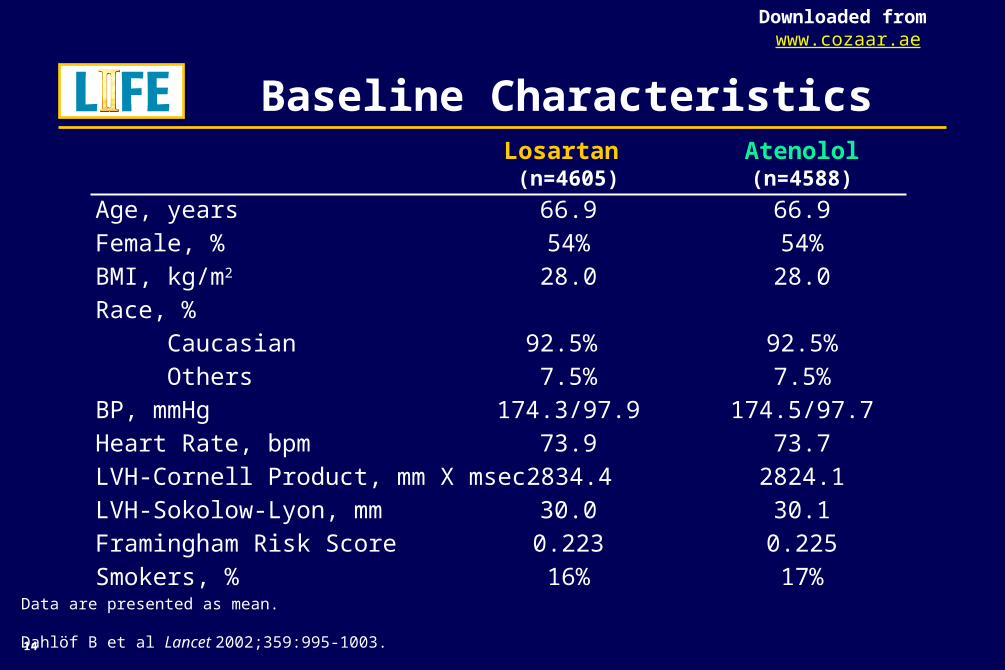
LIFE: Baseline CharacteristicsLosartan Atenolol(n=4605) (n=4588)
Age, years 66.9 66.9Female, % 54% 54%BMI, kg/m2 28.0 28.0Race, % Caucasian 92.5% 92.5% Others 7.5% 7.5%BP, mmHg 174.3/97.9 174.5/97.7Heart Rate, bpm 73.9 73.7LVH-Cornell Product, mm X msec 2834.4 2824.1LVH-Sokolow-Lyon, mm 30.0 30.1Framingham Risk Score 0.223 0.225Smokers, % 16% 17%
Data are presented as mean.
Dahlöf B et al Lancet 2002;359:995-1003.
15
Downloaded from www.cozaar.ae
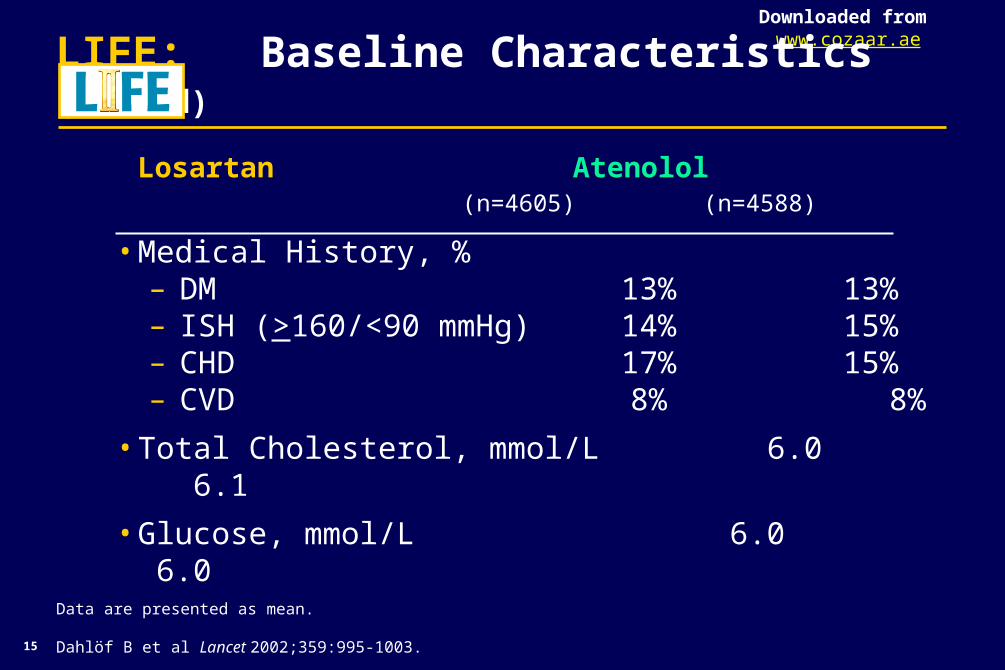
LIFE: Baseline Characteristics (cont’d)
Losartan Atenolol (n=4605) (n=4588)
• Medical History, %– DM 13% 13%– ISH (>160/<90 mmHg) 14% 15%– CHD 17% 15%– CVD 8% 8%
• Total Cholesterol, mmol/L 6.0 6.1
• Glucose, mmol/L 6.0 6.0
Data are presented as mean.
Dahlöf B et al Lancet 2002;359:995-1003.
0
2
4
6
8
10
12
14
16
Pro
po
rtio
n o
f p
ati
en
ts w
ith
fir
st
ev
en
t (%
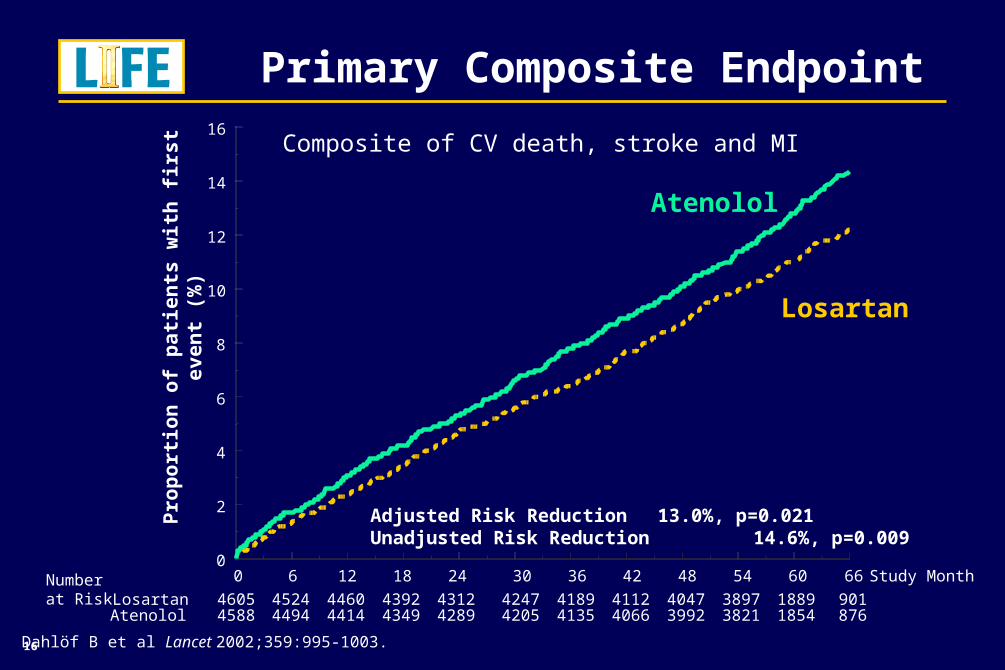
)Composite of CV death, stroke and MI
Losartan
Atenolol
LIFE: Primary Composite Endpoint
Study Month0 6 12 18 24 30 36 42 48 54 60 66
Losartan 4605 4524 4460 4392 4312 4247 4189 4112 4047 3897 1889 901Atenolol 4588 4494 4414 4349 4289 4205 4135 4066 3992 3821 1854 876
Adjusted Risk Reduction 13.0%, p=0.021Unadjusted Risk Reduction 14.6%, p=0.009
Dahlöf B et al Lancet 2002;359:995-1003.
Number at Risk
16
17
Downloaded from www.cozaar.ae
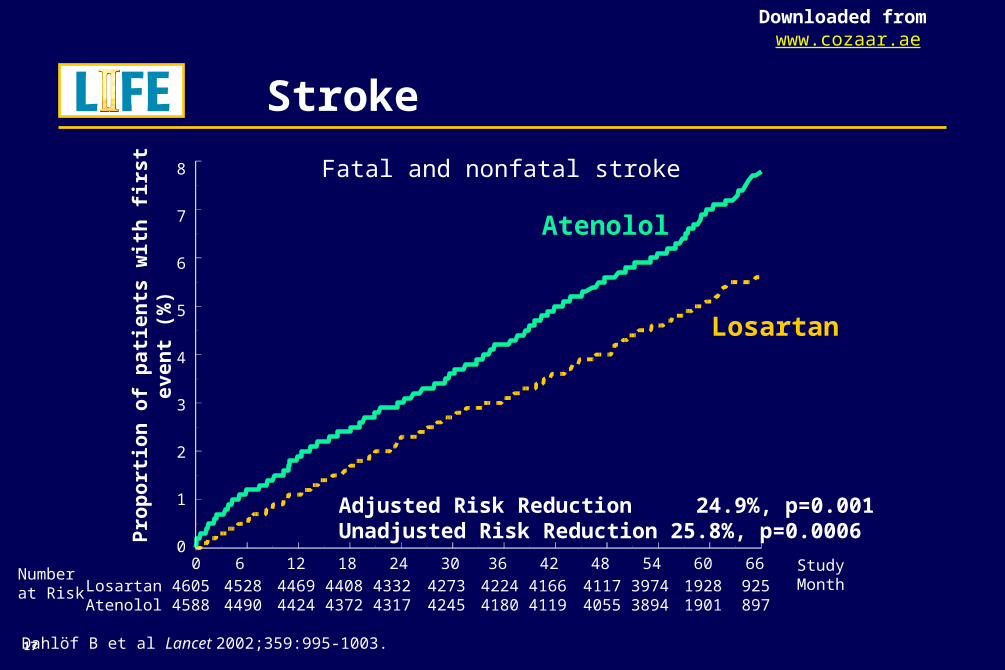
Stroke
Losartan
Atenolol
Adjusted Risk Reduction 24.9%, p=0.001Unadjusted Risk Reduction 25.8%, p=0.0006
Study Month0 6 12 18 24 30 36 42 48 54 60 660
1
2
3
4
5
6
7
8
Dahlöf B et al Lancet 2002;359:995-1003.
Losartan 4605 4528 4469 4408 4332 4273 4224 4166 4117 3974 1928 925Atenolol 4588 4490 4424 4372 4317 4245 4180 4119 4055 3894 1901 897
Fatal and nonfatal strokeP
rop
ort
ion
of
pa
tie
nts
wit
h f
irs
t e
ve
nt
(%)
Number at Risk
18
Downloaded from www.cozaar.ae
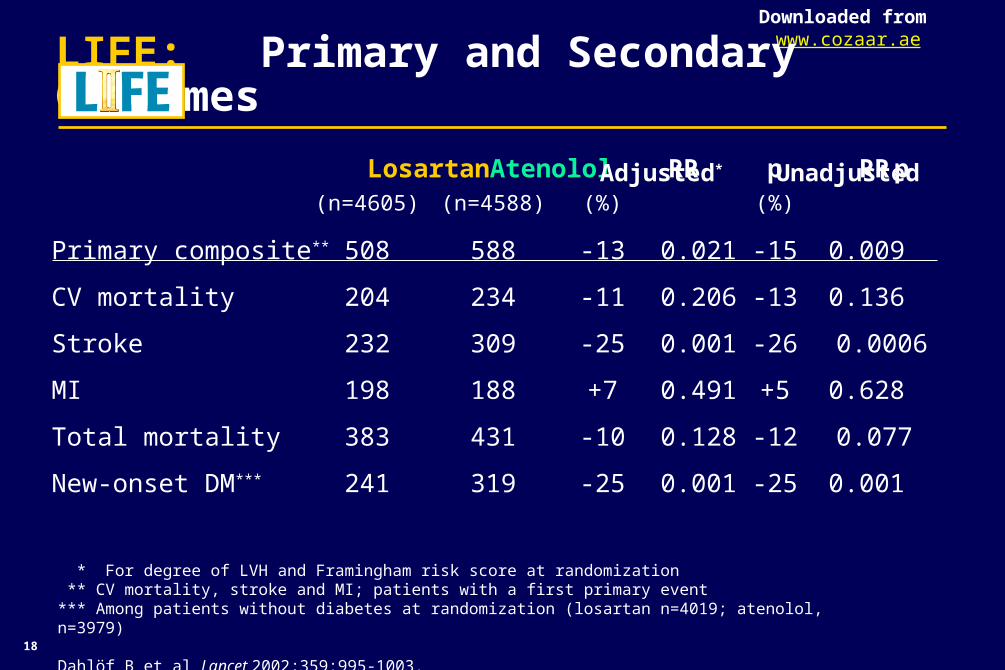
Losartan Atenolol RR p RR p (n=4605) (n=4588) (%) (%)
Primary composite** 508 588 -13 0.021 -15 0.009
CV mortality 204 234 -11 0.206 -13 0.136
Stroke 232 309 -25 0.001 -26 0.0006
MI 198 188 +7 0.491 +5 0.628
Total mortality 383 431 -10 0.128 -12 0.077
New-onset DM*** 241 319 -25 0.001 -25 0.001
LIFE: Primary and Secondary Outcomes
* For degree of LVH and Framingham risk score at randomization ** CV mortality, stroke and MI; patients with a first primary event*** Among patients without diabetes at randomization (losartan n=4019; atenolol, n=3979)
Dahlöf B et al Lancet 2002;359:995-1003.
UnadjustedAdjusted*
19
Downloaded from www.cozaar.ae
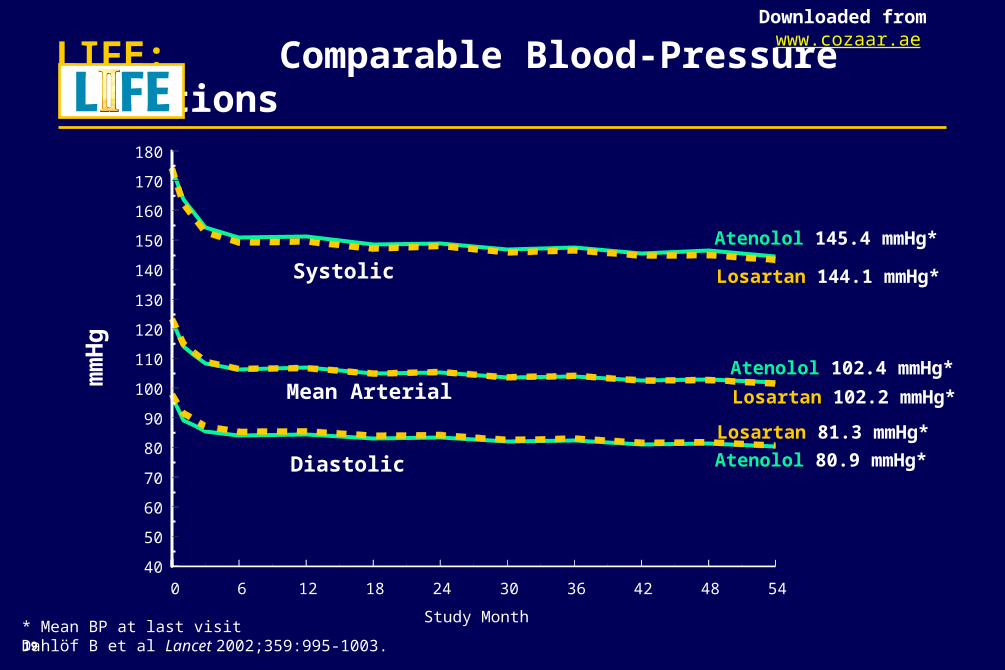
LIFE: Comparable Blood-Pressure Reductions
0 6 12 18 24 30 36 42 48 54
Study Month
40
50
60
70
80
90
100
110
120
130
140
150
160
170
180
Systolic
Diastolic
Mean Arterialmm
Hg
Atenolol 145.4 mmHg*
Losartan 144.1 mmHg*
Atenolol 80.9 mmHg*
Losartan 81.3 mmHg*
* Mean BP at last visitDahlöf B et al Lancet 2002;359:995-1003.
Atenolol 102.4 mmHg*
Losartan 102.2 mmHg*
20
Downloaded from www.cozaar.ae
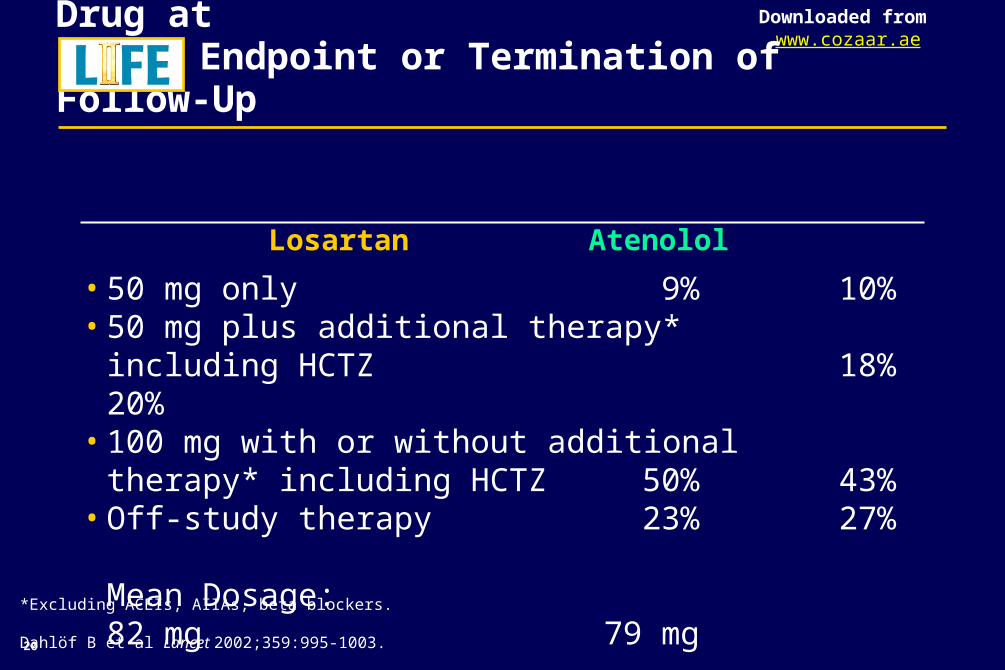
LIFE: Number of Patients on Study Drug atEndpoint or Termination of Follow-Up
Losartan Atenolol
• 50 mg only 9% 10%• 50 mg plus additional therapy*
including HCTZ 18% 20%• 100 mg with or without additional
therapy* including HCTZ 50% 43%• Off-study therapy 23% 27%
Mean Dosage: 82 mg 79 mg
*Excluding ACEIs, AIIAs, beta blockers.
Dahlöf B et al Lancet 2002;359:995-1003.
21
Downloaded from www.cozaar.ae
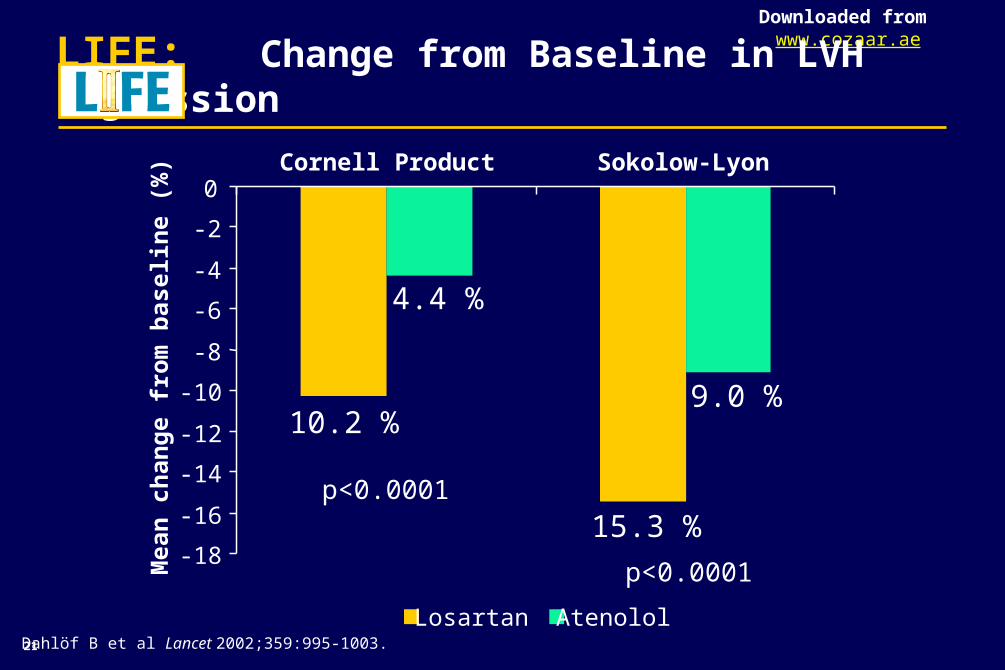
LIFE: Change from Baseline in LVH Regression
-18
-16
-14
-12
-10
-8
-6
-4
-2
0Cornell Product Sokolow-Lyon
Mea
n c
han
ge
fro
m b
asel
ine
(%)
Losartan Atenolol
p<0.0001
Dahlöf B et al Lancet 2002;359:995-1003.
10.2 %9.0 %
15.3 %
4.4 %
p<0.0001
22
Downloaded from www.cozaar.ae
LIFE: Adjustments for Difference
* Unadjusted for Framingham risk score and LVH
B. Dahlöf at the American College of Cardiology, Atlanta, GA, March 17-20, 2002.
• Adjustment none*– Treatment effect -15%
Achieved BP– Adjustment for SBP
• Treatment effect -14%
Regression of ECG-confirmed LVH – Adjustment for Cornell Voltage Duration Product (CVDP) and
Sokolow-Lyon (SL)• Treatment effect -10%
Conclusion: Adjusting for differences in achieved BP and degree of LVH regression only explains part of the study outcome
23
Downloaded from www.cozaar.ae
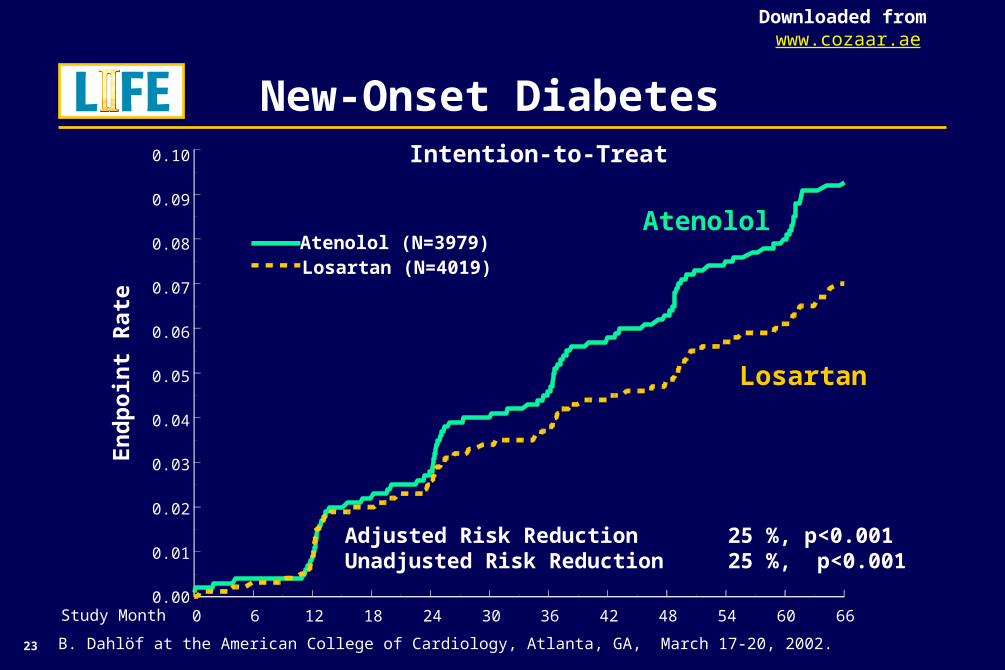
Intention-to-Treat
LIFE: New-Onset Diabetes
Losartan
AtenololAtenolol (N=3979)Losartan (N=4019)
Study Month 0 6 12 18 24 30 36 42 48 54 60 660.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.10
Adjusted Risk Reduction 25 %, p<0.001Unadjusted Risk Reduction 25 %, p<0.001
B. Dahlöf at the American College of Cardiology, Atlanta, GA, March 17-20, 2002.
En
dp
oin
t R
ate
24
Downloaded from www.cozaar.ae
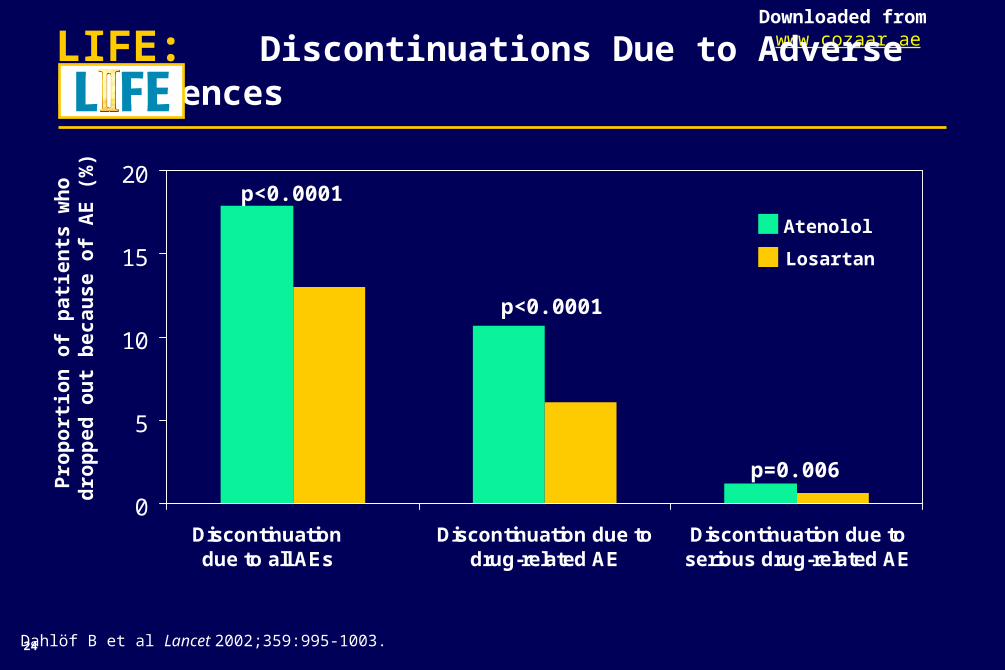
0
5
10
15
20
Discontinuation due to all AEs
Discontinuation due todrug-related AE
Discontinuation due toserious drug-related AE
p<0.0001
p<0.0001
p=0.006
LIFE: Discontinuations Due to Adverse Experiences
Atenolol
Losartan
Dahlöf B et al Lancet 2002;359:995-1003.
Pro
po
rtio
n o
f p
ati
en
ts w
ho
dro
pp
ed
ou
t b
ec
au
se
of
AE
(%
)
25
Downloaded from www.cozaar.ae
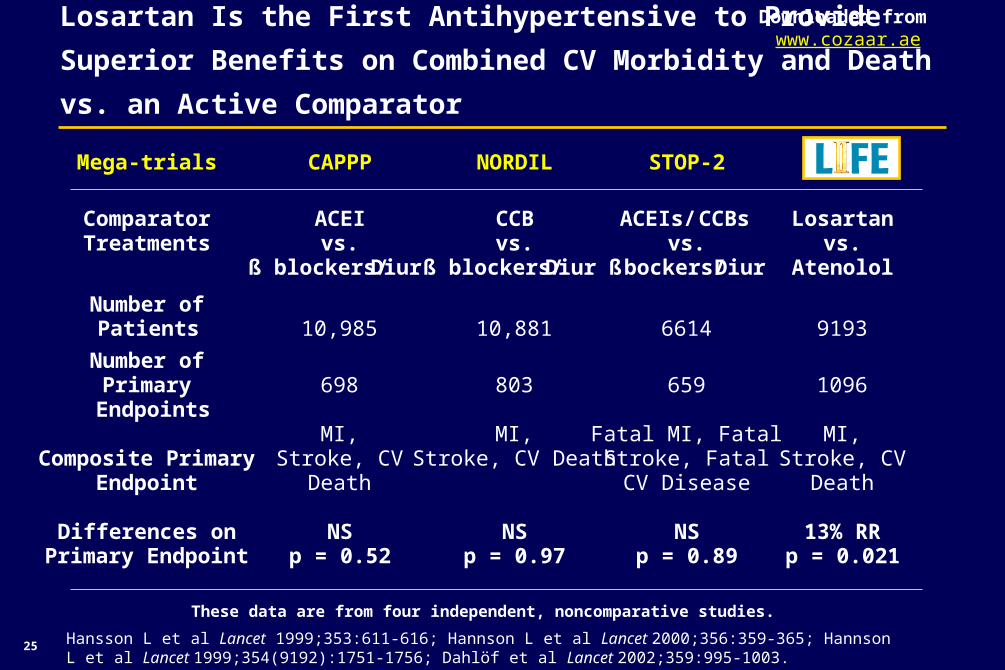
Mega-trials CAPPP NORDIL STOP-2
ComparatorTreatments
ACEIvs.
ß blockers/Diur
CCBvs.
ß blockers/Diur
ACEIs/ CCBsvs.
ß bockers/Diur
Losartanvs.
Atenolol
Number of Patients 10,985 10,881 6614 9193
Number ofPrimary
Endpoints698 803 659 1096
Composite PrimaryEndpoint
MI,Stroke, CV
Death
MI,Stroke, CV Death
Fatal MI, FatalStroke, FatalCV Disease
MI,Stroke, CV
Death
Differences onPrimary Endpoint
NSp = 0.52
NSp = 0.97
NSp = 0.89
13% RRp = 0.021
Losartan Is the First Antihypertensive to Provide Superior Benefits
on Combined CV Morbidity and Death vs. an Active Comparator
These data are from four independent, noncomparative studies.
Hansson L et al Lancet 1999;353:611-616; Hannson L et al Lancet 2000;356:359-365; Hannson L et al Lancet 1999;354(9192):1751-1756; Dahlöf et al Lancet 2002;359:995-1003.
26
Downloaded from www.cozaar.ae
LIFE: Summary
• Losartan-based antihypertensive therapy provided superior benefit on combined cardiovascular morbidity and death vs. atenolol:
– Superior risk reduction in the primary composite endpoint (CV death, stroke, and MI) of 13% (p=0.021)*
– Superior risk reduction in stroke of 25% (p=0.001)
• Losartan and atenolol provided substantial and comparable effective blood-pressure reduction
• Losartan was better tolerated with significantly fewer discontinuations due to adverse events
* No significant differences in cardiovascular death and MI vs. atenolol
27
Downloaded from www.cozaar.ae
LIFE: Conclusions
• Losartan with LIFE is the only antihypertensive that has demonstrated a superior benefit over another active treatment, atenolol, in reducing the risk of combined CV morbidity and death in patients with hypertension and LVH*
• The superior benefit of losartan therapy on combined CV morbidity and death* compared to atenolol was:
– beyond blood-pressure control
* Defined as composite of CV death, MI, and stroke
28
Downloaded from www.cozaar.ae
LIFE: Implications
• The greater clinical benefit and enhanced tolerability demonstrated by losartan in The LIFE Study Group suggest that broader use of losartan may improve outcomes for hypertensive patients with LVH
• “Our results are directly applicable in clinical practice and should affect future guidelines.”1
The LIFE Study Group

29
Downloaded from www.cozaar.ae
LIFE: Committees
• Steering Committee– Björn Dahlöf (Chair), Richard B. Devereux (Co-chair),
Stevo Julius (US Coordinator), Sverre E. Kjeldsen (Secretaryand Scandinavian Coordinator), Gareth Beevers, Ulf de Faire,Frej Fyhrquist, Hans Ibsen, Lars H. Lindholm, Markku Nieminen, Per Omvik, Suzanne Oparil, Ole Lederballe-Pedersen, Hans Wedel, Krister Kristianson (non-voting)
• Endpoint Classification Committee– Daniel Levy (US), Kristian Thygesen (Denmark)
• Data Safety Monitoring Board– John Kjekshus (Chairman, Norway), Lewis Kuller (US),
Pierre Larochelle (Canada), Giuseppe Mancia (Italy), Joël Ménard (France), Stuart Pocock (UK), John Reid (UK), Michael Weber (US)
Dahlöf B et al Lancet 2002;359:995-1003.
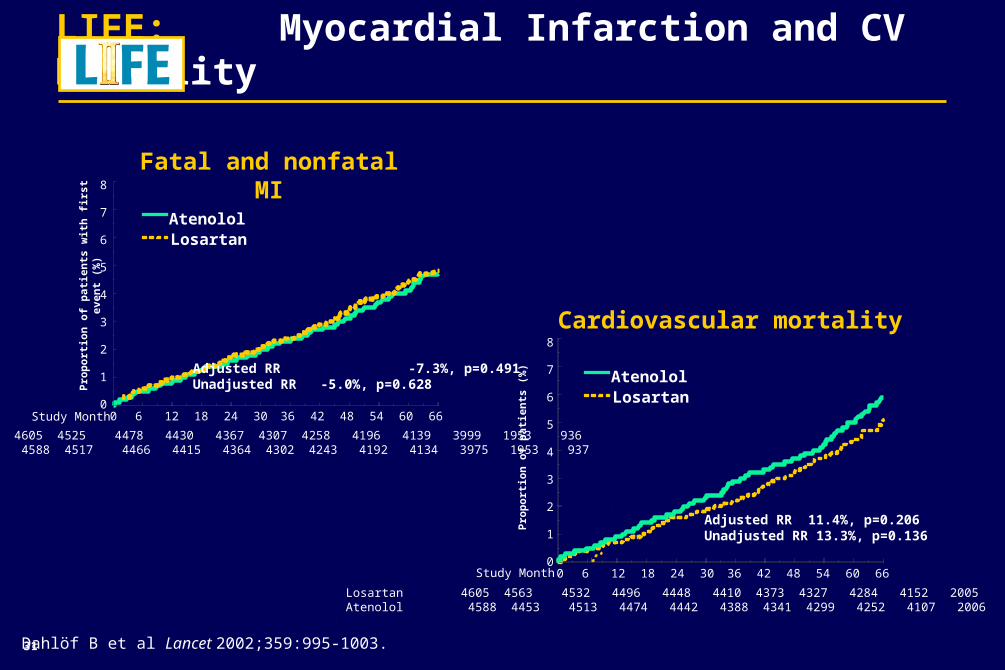
LIFE: Myocardial Infarction and CV Mortality
Dahlöf B et al Lancet 2002;359:995-1003.
Cardiovascular mortality
AtenololLosartan
Pro
po
rtio
n o
f p
atie
nts
(%
)Adjusted RR 11.4%, p=0.206Unadjusted RR 13.3%, p=0.136
Fatal and nonfatal MI
0 6 12 18 24 30 36 42 48 54 60 660
1
2
3
4
5
6
7
8
Pro
po
rtio
n o
f p
atie
nts
wit
h f
irst
eve
nt
(%)
Adjusted RR -7.3%, p=0.491Unadjusted RR -5.0%, p=0.628
AtenololLosartan
Losartan 4605 4525 4478 4430 4367 4307 4258 4196 4139 3999 1953 936Atenolol 4588 4517 4466 4415 4364 4302 4243 4192 4134 3975 1953 937
0 6 12 18 24 30 36 42 48 54 60 660
1
2
3
4
5
6
7
8
Losartan 4605 4563 4532 4496 4448 4410 4373 4327 4284 4152 2005 976Atenolol 4588 4453 4513 4474 4442 4388 4341 4299 4252 4107 2006 965
Study Month
Study Month
31
32
Downloaded from www.cozaar.ae
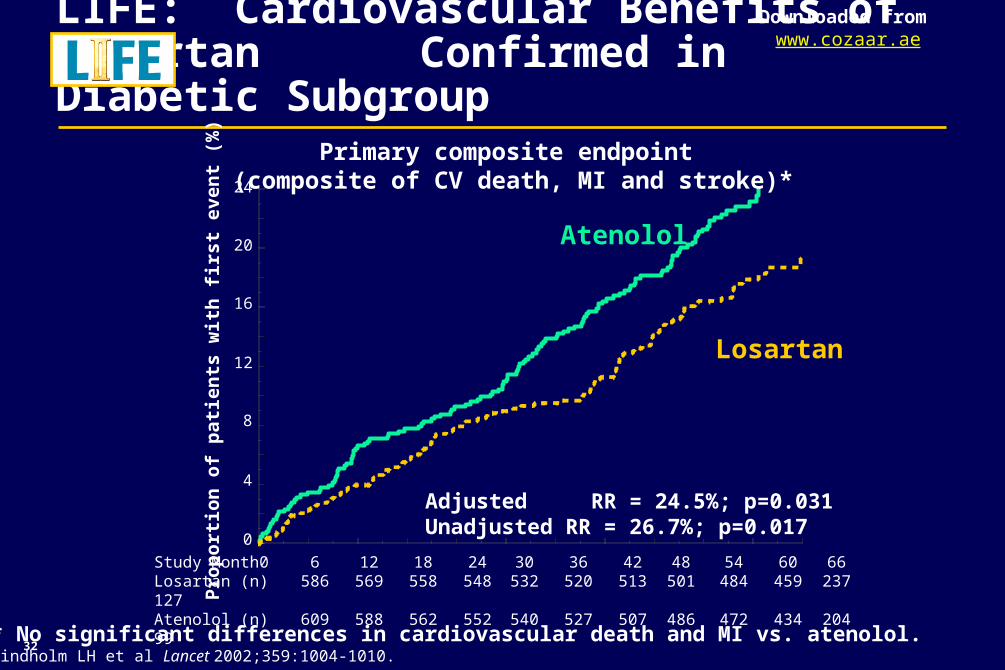
LIFE: Cardiovascular Benefits of Losartan Confirmed in Diabetic Subgroup
Study Month 0 6 12 18 24 30 36 42 48 54 60 66Losartan (n) 586 569 558 548 532 520 513 501 484 459 237 127Atenolol (n) 609 588 562 552 540 527 507 486 472 434 204 99
24
20
16
12
8
4
0Pro
po
rtio
n o
f p
atie
nts
wit
h f
irs
t e
ven
t (%
)
Adjusted RR = 24.5%; p=0.031Unadjusted RR = 26.7%; p=0.017
Losartan
Atenolol
* No significant differences in cardiovascular death and MI vs. atenolol.Lindholm LH et al Lancet 2002;359:1004-1010.
Primary composite endpoint (composite of CV death, MI and stroke)*
33
Downloaded from www.cozaar.ae
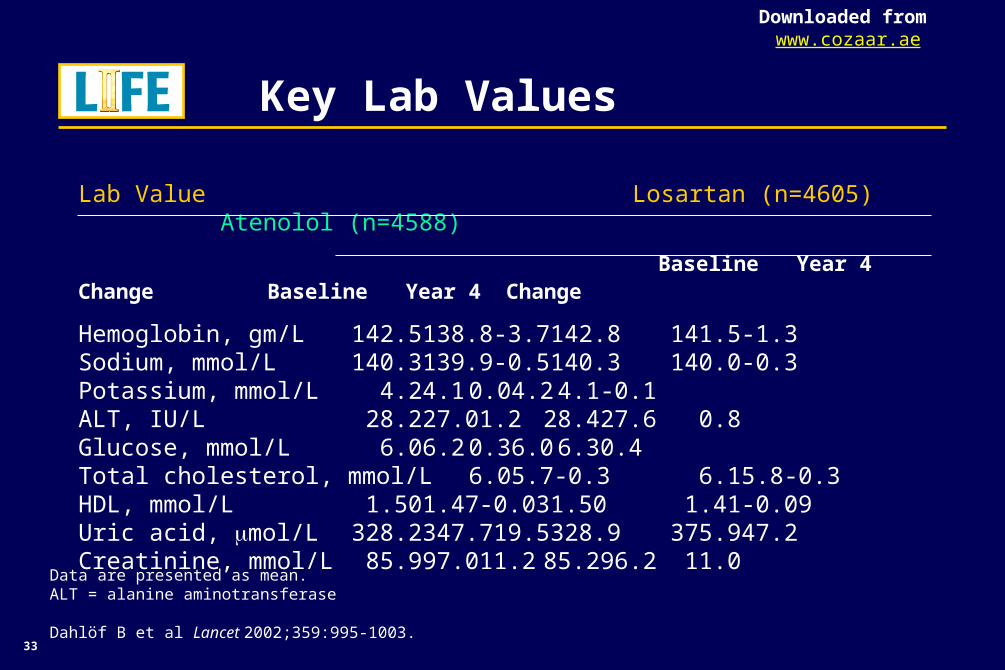
LIFE: Key Lab Values
Lab Value Losartan (n=4605) Atenolol (n=4588)
Baseline Year 4 Change Baseline Year 4 Change
Hemoglobin, gm/L 142.5 138.8 -3.7 142.8 141.5 -1.3Sodium, mmol/L 140.3 139.9 -0.5 140.3 140.0 -0.3Potassium, mmol/L 4.2 4.1 0.0 4.2 4.1 -0.1ALT, IU/L 28.2 27.0 1.2 28.4 27.6 0.8Glucose, mmol/L 6.0 6.2 0.3 6.0 6.3 0.4Total cholesterol, mmol/L 6.0 5.7 -0.3 6.1 5.8 -0.3HDL, mmol/L 1.50 1.47 -0.03 1.50 1.41 -0.09Uric acid, mol/L 328.2 347.7 19.5 328.9 375.9 47.2Creatinine, mmol/L 85.9 97.0 11.2 85.2 96.2 11.0
Data are presented as mean.ALT = alanine aminotransferase
Dahlöf B et al Lancet 2002;359:995-1003.
34
Downloaded from www.cozaar.ae
LIFE: References
Before prescribing, please consultfull product information.
35
Downloaded from www.cozaar.ae
LIFE: References
Before prescribing, please consultfull product information.
36
Downloaded from www.cozaar.ae
LIFE: References
Before prescribing, please consultfull product information.
37
Downloaded from www.cozaar.ae
LIFE: References
Before prescribing, please consultfull product information.
38
Downloaded from www.cozaar.ae
LIFE: References
Before prescribing, please consultfull product information.
39
Downloaded from www.cozaar.ae
Before prescribing, please consultfull product information.
Copyright © 2003-2004 Merck & Co., Inc., Whitehouse Station, NJ, USA.
All rights reserved. 5-05 CZR 2002-W-6783-SS Printed in USA
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com
Related Documents