1 Diabetes Management in Diabetes Management in the Older Adult the Older Adult Presented by Carolyn Jennings, MPH, RD, CDE SouthEast Michigan Diabetes Outreach Network (SEMDON) www.diabetesinmichigan.org

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Diabetes Management in the Diabetes Management in the Older AdultOlder Adult
Presented by
Carolyn Jennings, MPH, RD, CDE
SouthEast Michigan Diabetes Outreach Network
(SEMDON)
www.diabetesinmichigan.org
2
Myths: DM in the Older AdultMyths: DM in the Older Adult
• High prevalence of diabetes in older adults is inevitable
• Hyperglycemia in older adults is usually a benign condition
• Reduced life expectancy makes the consequences of uncontrolled diabetes irrelevant
• The majority of older adults with type 2 DM are obese and need to lose weight
• Older adults are less capable of self-monitoring their blood glucose
3
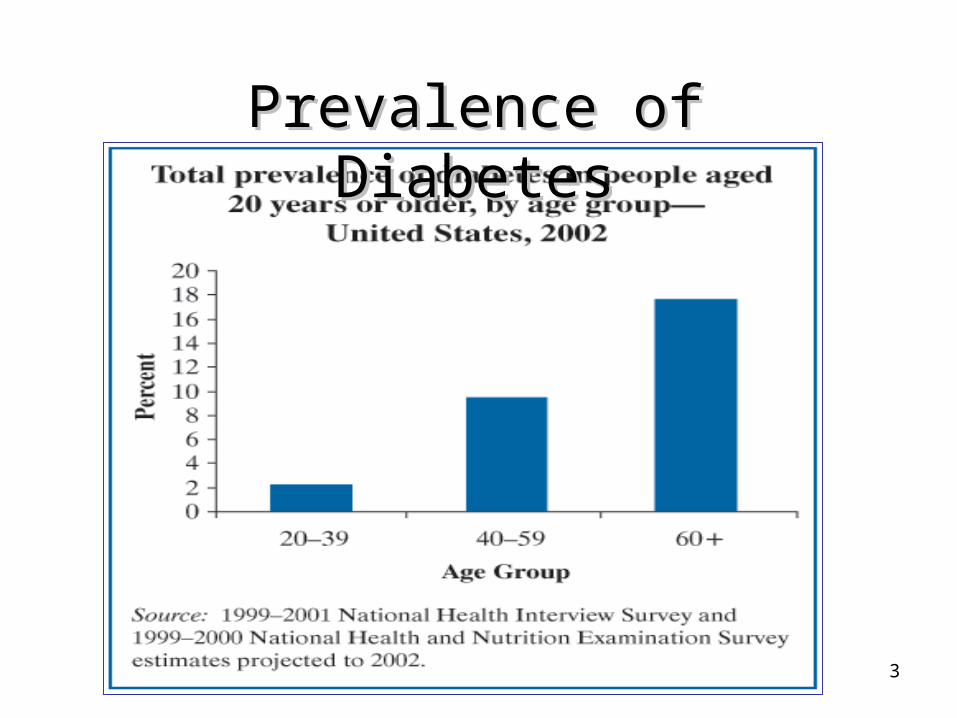
Prevalence of Prevalence of DiabetesDiabetes
4
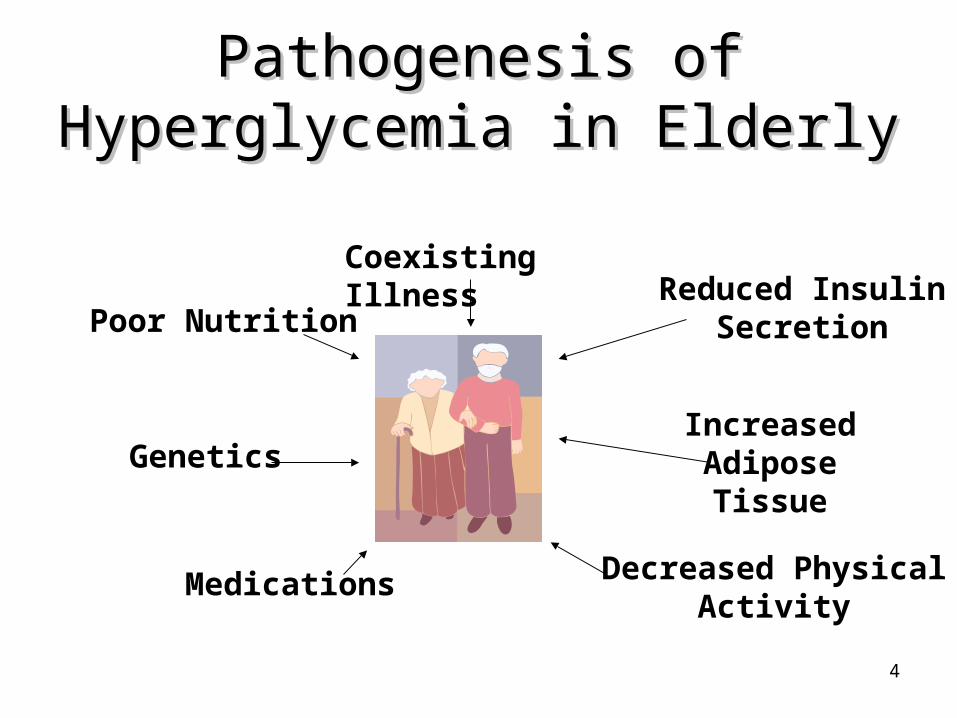
Pathogenesis of Hyperglycemia Pathogenesis of Hyperglycemia in Elderlyin Elderly
Poor Nutrition
Coexisting Illness Reduced Insulin
Secretion
Increased AdiposeTissue
Decreased PhysicalActivity
Medications
Genetics
5
Diabetes in Older AdultsDiabetes in Older Adults
• 50% under-diagnosed – WHY??• Early signs: Metabolic Abnormalities
– Insulin resistance 1st phase insulin release PPG with normal FPG
• Early symptoms: (if any)– Often gradual onset– Commonly mistaken for signs of normal
aging

6
Case of Mistaken IdentityCase of Mistaken Identity
• Blurred Vision• Polyuria and nocturia• Fatigue• MI and CVA’s 2 times
more common• High Blood Pressure• Neuropathy and foot
deformities• Restlessness/confusion
with high and low BG.
• Needing glasses• More frequent urination• Can’t do things like you
did when you were 20• Atherosclerosis• High Blood Pressure• Change in gait• Restlessness, confusion,
slower cognition.
Signs of DiabetesSigns of DiabetesSigns of Signs of AgingAging

7
Aging and DiabetesAging and Diabetes
• Poor diabetes control exacerbates the aging process.
• Poor diabetes control causes age related disease to develop earlier.
• Poor diabetes control makes co-morbid conditions worse and harder to manage.

8
OBJECTIVESOBJECTIVES• State three areas of assessment for State three areas of assessment for
the older adult with diabetes.the older adult with diabetes.
• State two recommendations for the care of the older adult with diabetes.
• List education strategies appropriate for the older adult with diabetes.
9
Diabetes AssessmentDiabetes Assessmentin the Older Adultin the Older Adult
• Physical Assessment
– Mobility/ Physical Activity
– Nutritional Assessment
• Neurological Assessment
• Psychosocial Assessment
• Other Areas
10
Diabetes AssessmentDiabetes Assessmentin the Older Adultin the Older Adult
Common Geriatric “Syndromes”• Depression
• Polypharmacy
• Cognitive Impairment
• Urinary incontinence
• Injurious falls
• Persistent pain

11
Physical AssessmentPhysical Assessment
• Ophthalmic– Higher rates of cataracts, glaucoma and
macular degeneration.
• Auditory
• Renal– Thickening of basement cell membranes.
• Immune system• Flu, herpes zoster, cancer

12
Physical AssessmentPhysical Assessment Cardiovascular System
– Reduction in CVD risk factors may have greatest impact on morbidity and mortality
• Hypertension• Lipids
– Increased risk of CVA’s and MI’s. – Heart rate in response to exercise reduced.– Thickening of basement cell membranes.– 50% of newly diagnosed people with T2DM
have CVD.

13
Physical AssessmentPhysical Assessment• Dexterity/coordination
– History of injurious falls
• Mobility/Physical Activity – Joint disease/ Bone mass Aerobic capacity Lean body mass Fat mass – Activity
Current level? Limitations, preferences

14
Nutritional AssessmentNutritional Assessment
• Preferences and Lifelong habits
• Meal Planning considerations
• Food Preparation
• Lifestyle changes
• Mobility issues
• Dentition
• High Risk considerations
15
Nutritional AssessmentNutritional Assessment
• Malnutrition– Altered nutrient absorption
– Vitamin deficiencies (B12)
– CHO intolerance– Decline in renal function
• Depression
• Cognitive Impairment
16
Nutritional AssessmentNutritional Assessment• Nutritional status
– Change in nutrient needs– Change in body composition– Hydration status– Alcohol use/abuse– Supplement/herbal use
• Gastrointestinal tract Absorption– Gastroparesis Appetite

17
Neurological AssessmentNeurological Assessment
• Cognitive Impairment– Increased rate in PWD
• Mini-mental status exam recommended
• Check for reversible causes:– B12 levels– Thyroid hormone– Neuroimaging– Depression screening– Blood glucose control
18
Neurological AssessmentNeurological Assessment• Autonomic and peripheral neuropathies:
– Heart
– Incontinence
– Sexual function
– Protective sensation
– Hypoglycemia unawareness
– Body Temperature regulation
– Reduced ability to sense:• Thirst, Smell, Taste
19
Psychosocial AssessmentPsychosocial Assessment
• Depression
• Support systems
– Loss of peers
– Change in family role
• Health Beliefs
• Locus of Control
– Internal vs. External
20
Other Areas of Assessment
• Co-morbidities
• Pain
• Polypharmacy– Diabetes medications appropriate?– Drug interactions– Ability to administer medications
• Safety
• Finances
21
OBJECTIVESOBJECTIVES• State three areas of assessment for
the older adult with diabetes.
• State two recommendations for the State two recommendations for the
care of the older adult with diabetes.care of the older adult with diabetes.
• List education strategies appropriate for the older adult with diabetes.
22
Treatment Recommendations
• Glycemic Control• Hypertension• Lipids• Tobacco cessation• Eye care• Foot care• Nephropathy• Diabetes Self-Management Training
23
Treatment Recommendations
• When and how to prioritize interventions?
• Stratifying older adults:– Comorbities– Complications– Risks vs. benefits of (intensive) therapies
24
Glycemic ControlGlycemic Control
• A1c- – <7% in healthy adults with good functional
status– <8% appropriate in:
• Frail older adults
• Life expectancy less than 5 years
• Those whom risk of intensive glycemic control outweighs benefits
– Frequency

25
Risks of Intensive Glycemic Risks of Intensive Glycemic ControlControl
• Hypoglycemia
• Polypharmacy
• Drug to drug interactions
• Drug to disease interactions
26
Who benefits most from Who benefits most from Intensive Glycemic Control?Intensive Glycemic Control?
• Older adults in good health
• Those with microvascular complications
• Frail elderly without microvascular complications will probably not live long enough to develop them
27
HyperglycemiaHyperglycemia• Can cause:
– Delirium– Mood swings and irrationality– Appetite changes– Sleep disturbances
• Increases risk for:
– Diabetic Ketoacidosis
– Hyperglycemic Hyperosmolar State (HHS)
28
HyperglycemiaHyperglycemia• Impairs cognitive ability• Reduces energy• Impairs memory• Decreased wound healing• Increased risk of HHS• Increases urine output
– Impacts incontinence/dehydration
• Increased risk of UTI• Impairs immune system
29
• Aging increases risk of hypoglycemia:Aging increases risk of hypoglycemia:– Reduced hormonal counter regulation– Renal and hepatic changes– Hydration status– Inadequate or irregular nutrition– Decreased intestinal absorption – Autonomic neuropathy– Polypharmacy– Use of alcohol, other sedating meds
HypoglycemiaHypoglycemia

30
HypoglycemiaHypoglycemia
• May cause:– Heart arrhythmias– Increased risk of falls– Signs and symptoms may be masked by
co-morbidities (i.e. Parkinson’s)– Impairs concentration and cognition– Impairs reaction time

31
HypertensionHypertension
• Goal: Less than 140/80 if tolerated
• Less than 130/80 may produce further benefit
• Blood pressure reduction should be done gradually to minimize complications (no more than 20mm/hg reduction in systolic BP/3 mo)
32
Hypertension:Hypertension: Medication Precautions Medication Precautions
• ACE-I or ARB Therapy– Monitor K 1-2 weeks after initiating therapy
and with each dose increase– ACE-I associated with decreased renal
function in elderly– Hyperkalemia common at moderate and high
doses

33
Hypertension:Hypertension: Medication Precautions Medication Precautions
• Thiazide or loop diuretic– Check electrolytes within 1-2 weeks of
initiation and at least yearly– Hypokalemia associated with ventricular
arrhythmias.
34
LipidsLipids
• Secondary to overall health status assessment
• Goals: LDL< 100mg/dl–HDL > 40 men, 50 women–TG < 150mg/dl
• LDL<100 reassess q 2yrs• LDL 100-129: MNT w/ physical activity• LDL > 130 pharmacologic therapy + lifestyle
intervention

35
Lipids: Medication PrecautionsLipids: Medication Precautions
• Increased side effects– Myalgias and myositis– Rhabdomyolysis– Elevated liver function?
• Niacin or Statin: Measure ALT w/in 12 weeks of initiation or dosage change
• Fibrate: evaluate liver enzymes at least annually
– Precaution with reduced renal function

36
Aspirin UseAspirin Use
• The older adult (who is not on any other anticoagulant therapy and has no contraindications to aspirin) should be offered 81-325mg/d.
37
Tobacco CessationTobacco Cessation
12% of PWD over age 65 smoke
• Assess use/willingness to quit
• Offer counseling and/or pharmacologic interventions to assist with cessation
38
Retinopathy ScreeningRetinopathy Screening
• Dilated eye exam at diagnosis
• High risk (symptoms of eye disease, retinopathy, glaucoma, cataracts, A1c>8, T1DM or BP>140/80mm/hg): – at least yearly follow-up exams
• Low(-er) risk : every 2 years
39
Foot ScreeningFoot Screening
• At least annual comprehensive foot exam and at all non-urgent outpatient visits. Assess changes in:– Skin integrity– Loss of protective sensation– Early detection of neuropathy– Decreased perfusion– Bone deformity

40
Nephropathy ScreeningNephropathy Screening
• Screen for microalbumin and GFR at diagnosis and (at least) annually
41
Diabetes Self-Mangement TrainingDiabetes Self-Mangement Training• More likely to include family members
and/or other caregivers• Essential topics:
– Hypoglycemia prevention and treatment– Benefits of MNT and physical acitvity– Medication review– Evaluation of foot care- amputation
prevention– Evaluate Geriatric Conditions
42
OBJECTIVESOBJECTIVES• State three areas of assessment for the
older adult with diabetes.
• State two recommendations for the care of the older adult with diabetes.
• List education strategies appropriate for List education strategies appropriate for
the older adult with diabetes.the older adult with diabetes.
43
The Adult LearnerThe Adult Learner
• Perceives need
• Self-directed
• Experienced
• Problem-oriented
• Task-centered
• Internally motivated
44
Patient Centered EducationPatient Centered Education
• Assessment of where patient is with disease “Health Beliefs”
• Assessing where patient is in regard to “readiness to change” current behaviors to improve (diabetes) health
WITH THIS INFORMATION the patient and
educator can work together to develop individualized self-management plan
45
Patient Centered EducationPatient Centered Education• Patients Role:Patients Role:
– Determine personal self-care goals
– Find solution– Take
responsibility for own health
• HCP’s Role:HCP’s Role:
– Active Listener– Source of accurate
Information– Provide essential
knowledge and skills training
– Understand client’s perspective
– Acknowledge the client’s feelings
– Support Person– Facilitator

46
Education StrategiesEducation Strategies
LISTEN, LISTEN, LISTEN…LISTEN, LISTEN, LISTEN…• Positive attitude
• Provide meaningful practical individualized information.– Prioritize needs with the patient– Assist with problem solving and goal setting– Empowerment Model- Patient CenteredPatient Centered

47
Education Strategies
• Assess baseline knowledge.– Dispel any misinformation– Update information
• Overcome generational barriers.
• Consider financial, accessibility, safety, support systems and the effect on perceived quality of life

48
Education StrategiesEducation Strategies
• Assess functionality and special needsAssess functionality and special needs
• Adaptive teaching strategiesAdaptive teaching strategies
– Visual accommodationsVisual accommodations• Low vision aids• Bright illumination• Large print and bright contrast• Detailed verbal explanations• Use support system.
49
• Auditory AccommodationsAuditory Accommodations– Eliminate distractions– Minimize background noise.– Reinforce with written materials.– Speak slowly in short sentences.– Speak to best hearing side.– If patient reads lips, keep mouth uncovered
and do NOT chew gum.
Education StrategiesEducation Strategies
50
Education StrategiesEducation Strategies
• Cognitive AccommodationsCognitive Accommodations– Simplify instruction.– Frequently summarize.– Focus on single topics.– Teach simple tasks first then move on to
more complex.– Use memory aids.– Evaluate learning often.
51
Education StrategiesEducation Strategies
What is the present degree of Blood Glucose control?
• If currently Hypo or Hyperglycemic:– Teach Survival Skills– Schedule follow-up when BG control
improved– Give educational materials for
reinforcement

52
Education Strategies:Education Strategies:Nursing Care Facilities
• Assess patient’s ability to participate in self care.
• Prioritize care to patient and family.
• Involve family in education.– Appropriate snacks to bring.– Reinforce behaviors that promote optimal
control.
53
Education Strategies:Education Strategies:Nursing Care Facilities
• Safety issues– Hyper/hypoglycemia signs/symptoms
• Adult Learner Guidelines• Evaluate level of control with respect to
quality of life, safety.• Advocate for your patients whose diabetes
control is sub optimal.
54
Summary- Education GoalsSummary- Education Goals• Assist older adults to optimally self-manage
diabetes.– Individualized BG goals to avoid both hyper-
and hypoglycemia.– Prevent or delay progression of
complications.• Promote optimal control for all older PWDs
– Hospitalized •• Residential care– Group living
55
ResourcesResources• Guidelines for Improving Care of the older person with
diabetes AM J Geriatric Soc 51(2003): S265-S280• Geriatric Resource Directory www.bphc.hrsa.gov• Working Together to Manage Diabetes Diabetes Medications Supplement
www.ndep.nih.gov/diabetes/publications • Oral Health Care for Older Adults www.nohic.nidcr.nih.gov• Working with Your Older Patient, a clinician’s handbook
www.nia.nih.gov• Exercise, A Guide from the National Institute on Aging
www.nia.nih.gov
Related Documents











