1 Court-Based Interventions and Co- Occurring Disorders Florida Partners in Crisis 2012 Annual Conference and Justice Institute Orlando, Florida, July 13, 2012 Presented by Roger H. Peters, Ph.D., University of South Florida, and Fred C. Osher, M.D., Council of State Governments Justice Center

1 Court-Based Interventions and Co-Occurring Disorders Florida Partners in Crisis 2012 Annual Conference and Justice Institute Orlando, Florida, July 13,
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Court-Based Interventions and Co-Occurring Disorders
Florida Partners in Crisis 2012 Annual
Conference and Justice Institute Orlando, Florida, July 13, 2012
Presented by Roger H. Peters, Ph.D., University of South Florida, and
Fred C. Osher, M.D., Council of State Governments Justice Center

2
Workshop Outline
I.I. Overview of workshopOverview of workshop
II.II. Integrated screening and assessmentIntegrated screening and assessment
III.III. Modifications to court program Modifications to court program structure and treatmentstructure and treatment
IV.IV. Clinical Considerations: Principles of Clinical Considerations: Principles of care for CODscare for CODs
V.V. Linking to EBP’s in the communityLinking to EBP’s in the community
VI.VI. Q & AQ & A

(GAINS Center, 2004; Steadman et al., 2009)

4
Co-Occurring Substance Use Disorders
74% of state prisoners with mental problems also have substance abuse or dependence problems
(U.S. Department of Justice, 2006)

5
Persons with CODs
Repeatedly cycle through the criminal justice Repeatedly cycle through the criminal justice and treatment systemsand treatment systems
Experience problems when not taking Experience problems when not taking medications, not in treatment, experiencing medications, not in treatment, experiencing mental health symptoms, using alcohol or drugsmental health symptoms, using alcohol or drugs
Small amounts of alcohol or drugs may trigger Small amounts of alcohol or drugs may trigger recurrence of mental health symptomsrecurrence of mental health symptoms
Antisocial beliefs similar to other offendersAntisocial beliefs similar to other offenders More criminal risk factors than other offendersMore criminal risk factors than other offenders

Conceptual Model of COD Treatment Services in Specialty Courts
6

Integrated Screening and Assessment
• Routine screening for both sets of disordersRoutine screening for both sets of disorders• Identify acute symptomsIdentify acute symptoms• Focus on areas of functional impairment that Focus on areas of functional impairment that
would prevent effective drug court participationwould prevent effective drug court participation• Examine longitudinal interaction of disordersExamine longitudinal interaction of disorders• Assess participant motivationAssess participant motivation

8

9

10
Features of COD Treatment
• Highly structured treatment servicesHighly structured treatment services• Destigmatize mental illnessDestigmatize mental illness• Focus on symptom management vs. cureFocus on symptom management vs. cure• Education regarding individual diagnoses Education regarding individual diagnoses
and interactive effects of CODsand interactive effects of CODs• ““Criminal thinking” groups Criminal thinking” groups • Basic life management and problem-solving Basic life management and problem-solving
skills skills

11
COD Program Phases
• OrientationOrientation
• Relapse prevention/transitionRelapse prevention/transition
• Intensive treatment Intensive treatment

Treatment Modifications - I
• Higher staff-to-participant ratioHigher staff-to-participant ratio• Increased length of services:Increased length of services:
• Pace of treatment slowerPace of treatment slower• Flexible progression through treatment allowedFlexible progression through treatment allowed• Ongoing tracking and case monitoringOngoing tracking and case monitoring• Extended exit and re-entry policies Extended exit and re-entry policies • Treatment may last for more than one yearTreatment may last for more than one year

Treatment Modifications - II
• Integrated treatment to address MH and SA issuesIntegrated treatment to address MH and SA issues• More emphasis on education and support rather More emphasis on education and support rather
than compliance and sanctionsthan compliance and sanctions• Motivational interventions in both group and Motivational interventions in both group and
individual settingsindividual settings• Cognitive and memory enhancement strategiesCognitive and memory enhancement strategies• Case management and outreach servicesCase management and outreach services• Focus on housing, employment, medication needsFocus on housing, employment, medication needs

14
Modifying Treatment for Cognitive Impairment
• Minimize need for abstraction (e.g., Minimize need for abstraction (e.g.,
use concrete, specific scenarios) use concrete, specific scenarios)
• Have demonstrate skills Have demonstrate skills
• Keep instructions brief Keep instructions brief
• Use audiovisual aids Use audiovisual aids • Keep role plays short and focusedKeep role plays short and focused
(Bellack, 2003)(Bellack, 2003)

Program Modifications for CODs
• Supplementary servicesSupplementary services (COD treatment (COD treatment groups, medication clinic, case groups, medication clinic, case management/crisis intervention)management/crisis intervention)
• TracksTracks within specialty court programs within specialty court programs
• COD docketsCOD dockets• TransferTransfer between drug courts, mental between drug courts, mental
health courts, COD dockets health courts, COD dockets
• Extended program Extended program durationduration (e.g., 18 mos.) (e.g., 18 mos.)
• Blended Blended screening and assessmentscreening and assessment
• Specialized supervision teamsSpecialized supervision teams15

16
• Community partnerships for COD/MH servicesCommunity partnerships for COD/MH services• Recovery-oriented treatment planning and case Recovery-oriented treatment planning and case
managementmanagement• Dually credentialed staffDually credentialed staff• Focus on incentives and non-punitive sanctionsFocus on incentives and non-punitive sanctions• Specialized supervision teamsSpecialized supervision teams
Other Modifications for CODs
Modifying Court Hearings
• More frequent court hearings may be neededMore frequent court hearings may be needed• Hearings provide a good opportunity to recognize Hearings provide a good opportunity to recognize
and reward positive behavioral changeand reward positive behavioral change• Less formal, smaller, more privateLess formal, smaller, more private• Greater interaction between judge and participantsGreater interaction between judge and participants• Include mental health professionalsInclude mental health professionals

18
Community Supervision and CODs
• Specialized caseloadsSpecialized caseloads (MH/COD)
• Smaller caseloads (e.g., < 45)
• Sustained and specialized Sustained and specialized officer trainingofficer training
• Active engagement in Active engagement in SA and MH treatmentSA and MH treatment
• Dual focus Dual focus on treatment and surveillanceon treatment and surveillance
• Specialized caseloads more effective w CODsSpecialized caseloads more effective w CODs- Lower rates of revocation, arrest, incarcerationLower rates of revocation, arrest, incarceration- Better linkage with community treatment servicesBetter linkage with community treatment services

Community Supervision and CODs
• Problem-solvingProblem-solving approachapproach- Higher revocation thresholdHigher revocation threshold- Wide range of incentives and sanctionsWide range of incentives and sanctions- Flexibly apply sanctionsFlexibly apply sanctions- Avoid sanctions that remove participants Avoid sanctions that remove participants
from treatmentfrom treatment• Relationship quality important Relationship quality important (trust, (trust,
caring-fairness, avoid punitive stance) – caring-fairness, avoid punitive stance) – “firm but fair”“firm but fair”
(See Skeem et al., 2006, 2009)(See Skeem et al., 2006, 2009) 19

Court Based Interventions: Clinical Considerations
Fred Osher, M.D.

Awareness: Consequences of Co-occurring Disorders
Increased vulnerability to relapse and rehospitalization
More psychotic symptoms Inability to manage finances Housing instability and homelessness Noncompliance with medications and treatment Increased vulnerability to HIV infection and
hepatitis
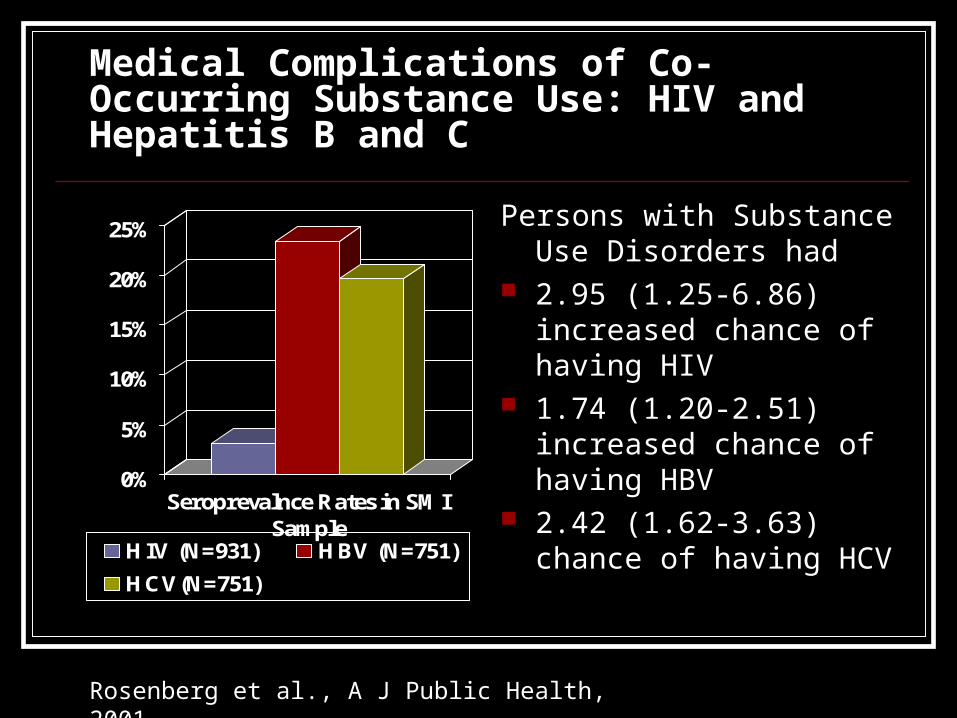
Medical Complications of Co-Occurring Substance Use: HIV and Hepatitis B and C
0%
5%
10%
15%
20%
25%
Seroprevalnce Rates in SMISample
HIV (N=931) HBV (N=751)
HCV(N=751)
Persons with Substance Use Disorders had
2.95 (1.25-6.86) increased chance of having HIV
1.74 (1.20-2.51) increased chance of having HBV
2.42 (1.62-3.63) chance of having HCV
Rosenberg et al., A J Public Health, 2001
Consequences of Co-occurring Disorders (cont.) Lower satisfaction with familial relationships Increased family burden Violence Return to Incarceration Increased depression and suicidality Higher service utilization and costs

Principles of care
1. Integrated treatment2. Screening, Assessment, and Individualized Treatment Planning3. Assertiveness4. Close monitoring5. Longitudinal perspective6. Harm reduction7. Stages of change8. Stable living situation9. Cultural competency and consumer
centeredness10. Optimism

1. Integrated treatment
Traditional models of treatment for dual disorders results in poor outcomes no treatment -- high utilization of E.R., jails, hospitals sequential treatment parallel treatment -- burden of integration on individual Fragmentation
Integrated treatment associated with better outcomes in SMI and perhaps non-SMI

Past Year Mental Health Care and Treatment for Adults Aged 18 or Older with Both Serious Mental Illness and Substance Use Disorder
26
Source: NSDUH (2008)

FIDELITY TO DUAL DIAGNOSIS PRINCIPLES*** If current & subsequent points = 1 then the current score = 1Assessment Points Baseline 6 mo. 12 mo. 18 mo. 24 mo. 30 mo. 36 mo.Hi-Fidelity 0 19.67 26.23 29.51 37.7 42.62 55.74Low-Fidelity 0 3.85 3.85 7.69 7.69 15.38 15.38
Figure 1. Percent of Participants in Stable Remission for High-Fidelity ACT Programs (E ; n=61) vs. Low-Fidelity ACT Programs (G; n=26).
0
10
20
30
40
50
60
Baseline 6 mo. 12 mo. 18 mo. 24 mo. 30 mo. 36 mo.
2. Screening, Assessment, and Individualized Treatment Planning Definition: Screening
A formal process of testing to determine whether a client does or does not warrant further attention at the current time in regard to a particular disorder and, in this context, the possibility of a co-occurring substance or mental disorder.
The screening process for co-occurring disorders (COD) seeks to answer a “yes” or “no” question: Does the substance abuse [or mental health] client being screened show signs of a possible mental health [or substance abuse] problem?
Note that the screening process does not necessarily identify what kind of problem the person might have, or how serious it might be, but determines whether or not further assessment is warranted.

Council of State Governments Justice Center 29
A Framework for Prioritizing Target Population
Low Criminogenic Risk
(low)
Medium to High Criminogenic Risk
(med/high)
Low Severity of Substance Abuse
(low)
Substance Dependence
(med/high)
Low Severity of Substance Abuse
(low)
Substance Dependence
(med/high)
Low Severity of
Mental Illness(low)
Serious Mental Illness
(med/high)
Low Severity of
Mental Illness(low)
Serious Mental Illness
(med/high)
Low Severity of
Mental Illness(low)
Serious Mental Illness
(med/high)
Low Severity of
Mental Illness(low)
Serious Mental Illness
(med/high)
Group 1I – L CR: lowSA: lowMI: low
Group 2II – L CR: lowSA: lowMI: med/high
Group 3III – L CR: lowSA: med/highMI: low
Group 4IV – L CR: lowSA: med/highMI: med/high
Group 5I – H CR: med/highSA: lowMI: low
Group 6II – H CR: med/highSA: lowMI: med/high
Group 7III – H CR: med/highSA: med/highMI: low
Group 8IV – HCR: med/highSA: med/highMI: med/high

2. Screening, Assessment, and Individualized Treatment Planning Definition: Assessment
A basic assessment consists of gathering key information and engaging in a process with the client that enables the counselor/therapist to understand the client’s readiness for change, problem areas, COD diagnosis, disabilities, and strengths.
An assessment typically involves a clinical examination of the functioning and well-being of the client and includes a number of tests and written and oral exercises. The COD diagnosis is established by referral to a psychiatrist or clinical psychologist.
Assessment of the COD client is an ongoing process that should be repeated over time to capture the changing nature of the client’s status.
1. Evaluate pressing needs 2. Determine motivation to address
substance use/mental health problems 3. Select target behaviors for change 4. Determine interventions/conditions to achieve
desired goals 5. Choose measures to evaluate the
intervention 6. Select follow-up times to review the plan.
Individualized Treatment Planning - Steps
3. Assertiveness
Responsibility of systems to support outreach and engagement services
Successful interventions: “go wherever the client is” In-reach to institutional settings work with family, landlords and employers
Forensic Assertive Community Treatment (FACT)

4. Close monitoring
Intensive supervision needed until stable Sometimes coercive, always persuasive
representative payeeship mandatory substance abuse treatment urine testing
The essence of court-based interventions

5. Longitudinal perspective Mental health, substance use disorders, and
disease are chronic, relapsing conditions
Treatment occurs continuously over years
Progress measured over time
What is the courts role in the recovery trajectory
6. Harm reduction strategies
Assume: continuum from abstinenceproblematic use
abuse/dependence reducing quantity/frequency of use decreases
likelihood of negative consequences Provide alternatives to traditional abstinence
only philosophies More likely to engage those who don’t yet
have abstinence as a goal Tough concept in drug court context

7. Stages of change Engagement - connecting people to treatment
Persuasion - convincing engaged clients to accept treatment
Active treatment - range of behavioral, psychoeducational and medical interventions
Relapse prevention - prevention and management of relapses

COURSE OF ATTAINING STABLE REMISSION (Drake et al, 1997)QuickTime™ and aGraphics decompressorare needed to see this picture.
0 mo. 6 mo. 12 mo. 18 mo. 24 mo. 30 mo. 36 mo.0
10
20
30
40
50
60
70
80
90
100
Pe
rce
nt
Assessment Point
Pre-engagement
Engagement
Early Persuasion
Late Persuasion
Early Active Treatment
Late Active Treatment
Relapse Prevention
Recovered

8. Stable living situation
Not having a home makes assessment difficult and protracted
Range of safe, affordable housing options are necessary safe havens or low demand residences for engagement and
persuasion alcohol and drug free housing during active treatment and
relapse prevention Separate conditions and treatment from housing Flexibility and tolerance required to retain people in
housing
9. Cultural competency and consumer centeredness
Seek to understand - don’t assume a shared set of values or impose one’s own
Respect cultural differences
Value the consumer’s point of view

10. Optimism
Critical ingredient for recovery
Hope as an antidote to despair Must have courage to connect with the reality of despair Share belief that because the problems are severe, the
person deserves help Create a vision of what a hopeful outcome might be
Peer supervision and training to bolster staff optimism

Integrating Treatment with Supervision

Transformation: Integrated Public Health-Public Safety Court Strategies (NIDA 2006)
Blends functions of criminal justice and treatment systems to optimize outcomes
Community-based
treatment
Opportunity to avoid incarceration or criminal record
Close supervision
Consequences for noncompliance are
certain and immediate

What is the capacity of your community behavioral health providers to serve the target population and willingness to partner with the court diversion efforts?
What is the quality of behavioral health services available to the target population?
What is the priority given to criminal justice involved clients for community behavioral services?
Questions for Discussion

Q&A
51
Related Documents