1 Community Case Management Of Serious, Common, Childhood Infections in High Mortality Countries: Rationale, Experience, and Opportunities Global Business Coalition on HIV/AIDS, Tuberculosis and Malaria Non-Governmental Organization Teleconference April 7, 2011 David R. Marsh, MD, MPH Senior Advisor, Child Survival Global Team Leader, Community Case Management

1 Community Case Management Of Serious, Common, Childhood Infections in High Mortality Countries: Rationale, Experience, and Opportunities Global Business.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Community Case ManagementOf Serious, Common, Childhood Infections in
High Mortality Countries: Rationale, Experience, and Opportunities
Global Business Coalition on HIV/AIDS, Tuberculosis and MalariaNon-Governmental Organization TeleconferenceApril 7, 2011
David R. Marsh, MD, MPHSenior Advisor, Child Survival
Global Team Leader, Community Case Management
2
Outline
• Rationale and definition
• Experience– Programs– Research
• Opportunities

3
Rationale

"Protect, Prevent, Treat" African Regional Workshop on coordinated approaches to pneumonia and diarrhoea prevention and control4 |
Causes of Child Death – 2008*Causes of Child Death – 2008*
Globally, pneumonia, diarrhea, and malaria account for 41% of 8,000,000 deaths (3.3 million) annually.
In Africa they account for 53% of the 4,200,000 deaths in (2.2 million) annually.
WHO CHERG estimates, Black et al Lancet 2010
Global
*Slide courtesy of S Qazi and T Cherian, WHO/CAH

"Protect, Prevent, Treat" African Regional Workshop on coordinated approaches to pneumonia and diarrhoea prevention and control5 |
Source: WHO CAH department; WHO-UNICEF immunization coverage estimates
Uneven coverage patterns across interventions* Coverage levels for countdown interventions and approaches, 68 priority countries
Uneven coverage patterns across interventions* Coverage levels for countdown interventions and approaches, 68 priority countries
Though the global average immunization coverage is high, coverage with Hib vaccine is low and pneumo and rotavirus vaccines have to be introduced and scaled up
Coverage with other interventions is low and in some instances declining
*Slide courtesy of S Qazi and T Cherian, WHO/CAH
%

6
Irrawaddy Delta “Highway” (Myanmar)

7
Socio-economic Impact of Childhood Infection
• Infection predisposes to malnutrition, which increases risk of more infection, more malnutrition...
• Children miss learning (pre-school or school): short-term effects on the child, long-term effects on society– Malnutrition further compromises learning
• Caregivers miss work, reducing earnings and productivity
• Families spend resources on treatment and transport, reducing ability to purchase other goods and services
• CCM (1) saves time, money and human capital, (2) halts the progression of disease and (3) interrupts the infection-malnutrition cycle

8
Definition

9
CCM is a strategy in which…
• A health system trains, supplies and supervises front-line workers in communities without access to health facilities to treat children using evidence-based protocols for common, serious infections:– Mainly diarrhea, pneumonia, and malaria – And sometimes dysentery, newborn sepsis
and acute malnutrition.

10
Sick Child Recording Form
ASK
LOOK
DECIDE
ACT: REFER
ACT: TREAT
AT HOME

11
Drugs & Equipment (Nicaragua)
Antibiotic, zinc, ORS, antipyretic
Spoons, timer, mixing containers, counseling cards, raincoat, forms

12
Encounter (Nicaragua)Counting respirations.
Treatment Register

13
Supervision (Nicaragua)
Supervision Checklist
Health Worker with her Supervisor and her Supervisor’s Supervisor

14
Programs

15
Projects, Programs, and/or Technical Assistance to Governments (22)
• Asia (8): Afghanistan, Bangladesh, China, India, Indonesia, Myanmar, Nepal, Pakistan
• Africa (9): Angola*, Ethiopia, Mali, Malawi, Mozambique, Nigeria, South Sudan, Uganda, Zambia
• Latin America (5): Bolivia*, Dominican Republic, Guatemala, Haiti, Nicaragua
*closed

16
Research

17
Evaluation of a CCM Demonstration (2005-06) in Liben District, Oromiya
Region, Ethiopia
Total Population: 138,000 (2001)Under five mortality: 161/1000 live births
18
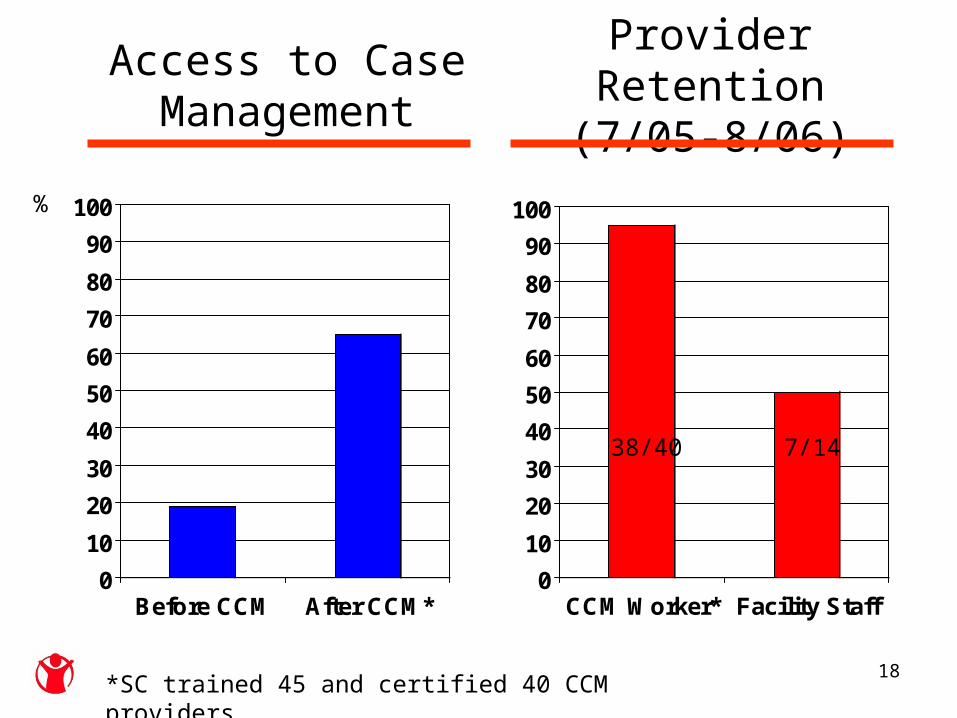
Access to Case Management
0
10
20
30
40
50
60
70
80
90
100
Before CCM After CCM*0
10
20
30
40
50
60
70
80
90
100
CCM Worker* Facility Staff
Provider Retention (7/05-8/06)
%
38/40 7/14
*SC trained 45 and certified 40 CCM providers
19
0
1000
2000
3000
4000
5000
Facility Staff CCM Worker
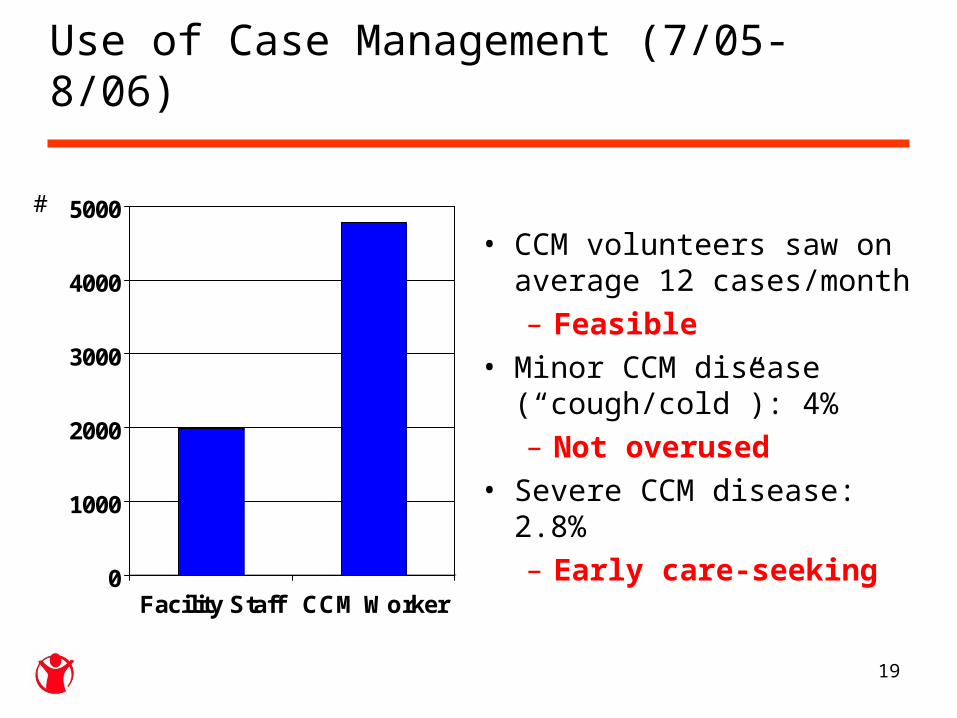
• CCM volunteers saw on average 12 cases/month – Feasible
• Minor CCM disease (“cough/cold”): 4% – Not overused
• Severe CCM disease: 2.8% – Early care-seeking
#
Use of Case Management (7/05-8/06)

20
0
20
40
60
80
100
CaseScenarios (3)
Register No Stockout Reporting
%
Quality of CCM Services

21
0
10
20
30
40
50
60
70
80
90
1997 2001 2006
Treatment Seeking for Cough and Difficult Breathing (1997-2006)
% *
* = 200,000 untreated cases of childhood pneumonia, malaria,
and diarrhea every year
17%
58%
84%
Clinic-based treatment of pneumonia
and malaria.
CCM of pneumonia
and malaria.

22
0
10
20
30
40
50
60
70
80
90
1997 2001 2006
Treatment Seeking for Cough and Difficult Breathing (1997-2006)
% *
* = 200,000 untreated cases of childhood pneumonia, malaria,
and diarrhea every year
17%
58%
84%
Clinic-based treatment of pneumonia
and malaria.
CCM of pneumonia
and malaria.
CCM

23
Scale (2009-2011)
• Publication: Degefie T, Marsh DR, Gebremariam A et al. Community case management improves use of treatment for childhood diarrhea, malaria and pneumonia in a remote district in Ethiopia’s Oromiya Region, Eth J of Hlth Dev 2009; 23(2):120-126.
• Stakeholder buy-in: Ethiopian Pediatrics Society recommended Health Extension Workers to treat pneumonia (2009)
• Policy change: 2010• National implementation: Broad partnership to roll
out community-based pneumonia treatment in 100s of districts (2010-2011)

24
CCM Training in Ethiopia (2/11)

25
Current CCM Research
• Effective access in Malawi, Mali, Zambia• Video-based training in South Sudan• Supervision in Malawi and Ethiopia (mHealth)• Teaming CHW and TBA in Zambia • Effect of demand generation in Pakistan• CCM of severe acute malnutrition in Bangladesh • Severe pneumonia in Pakistan• Cost of pneumonia treatment in Pakistan• Costing in Malawi• Global indicator validation in Malawi, Mali

26
Opportunities

27
Corporate Opportunities to Advance the Agenda
• Save the Children will continue to: – Speak for children dying from controllable diseases
• Develop materials: printed, videotaped• Take on “a killer”
– Leverage a seat “at the table” for multilateral policy and implementation
• Sponsor a policy meeting or participation from abroad– Contribute to global and country research
• Support answering a research question from your “corporate community” of national relevance
– Provide technical assistance to governments to test, introduce and/or scale up CCM
• Provide gift-in-kind for CHW kit• CHWs: “adopt” 100, supervise 500, train 1000• Sponsor a district, province or country

28
• Save the Children’s new directions:– Add CCM for neonatal sepsis into child CCM– Test mobile phone applications (“mHealth”)– Develop and test other technologies for
training, supervision, case management– Strengthen facility-based case management– Engage private sector providers
• Motivate private sector• Support testing public-private partnership
Corporate Opportunities to Advance the Agenda

29
Twa to te la 谢谢 (xièxiè)
Photo by Cleis
Related Documents











