1 Chapter 5 Respirat ion Liu Yuhong Department of Physiology Ji Ning Medical College E-mail: [email protected]

1 Chapter 5 Respiration Liu Yuhong Department of Physiology Ji Ning Medical College E-mail: [email protected].
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Chapter 5 Respiration
Liu Yuhong Department of PhysiologyJi Ning Medical College
E-mail: [email protected]
2
The gas exchange between the body and the external environment is named respiration.
The goales of respiration are:
uptake oxygen (O2)
output carbon dioxide(CO2)

3
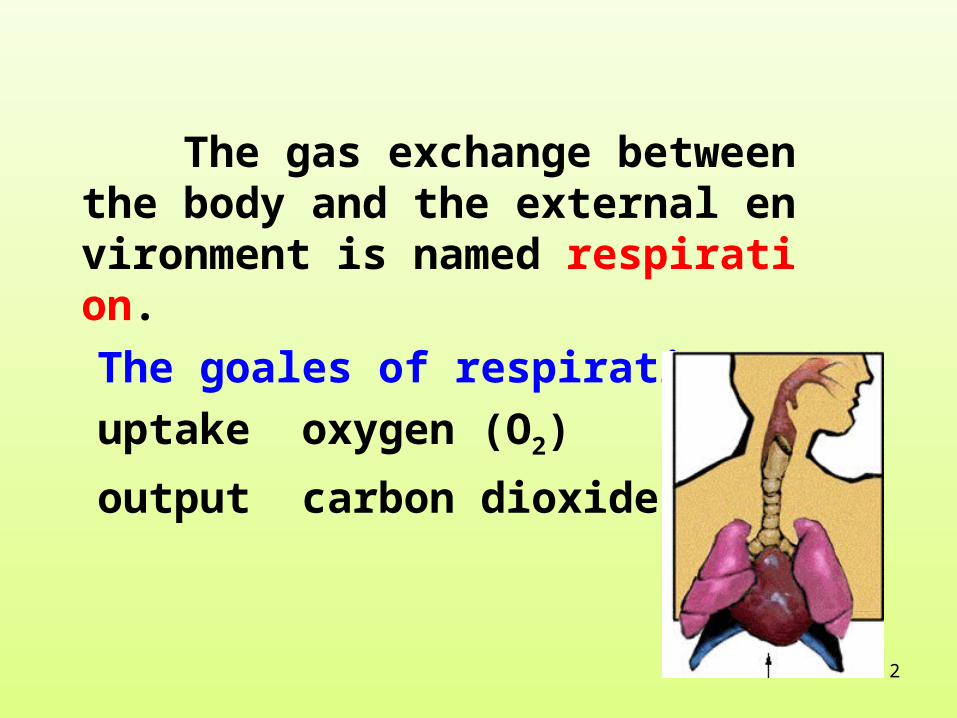
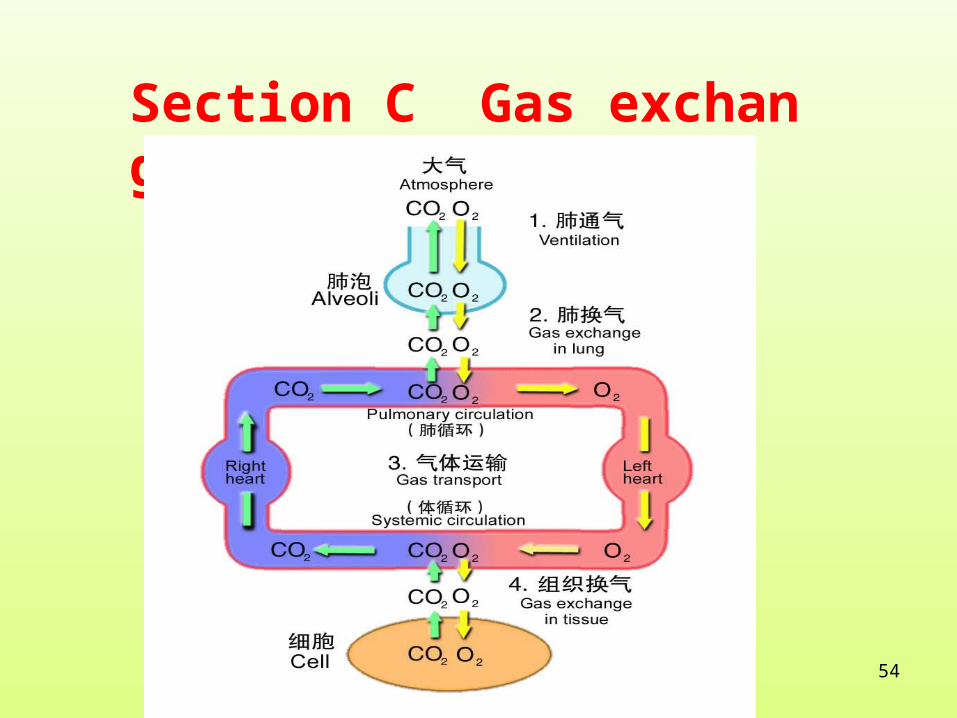
Respiration is consisted of three major functional events:
①
④③②
gas transport
CO2O2
4
5
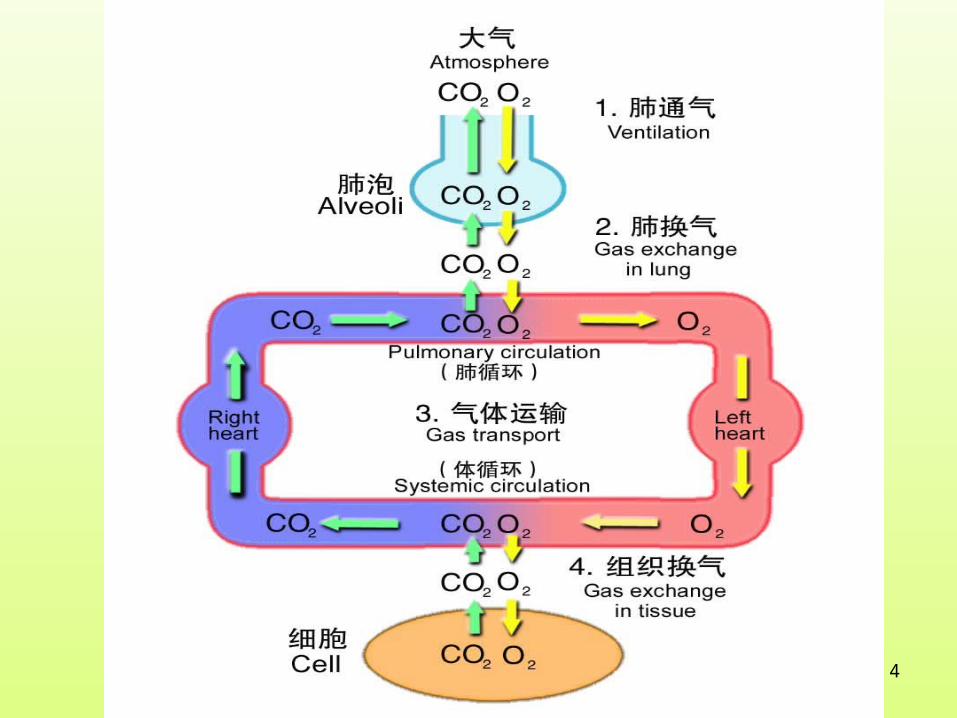
atria
ventricle

6
Section A Organization of the Respiration System
nose
bronchioles
alveolus
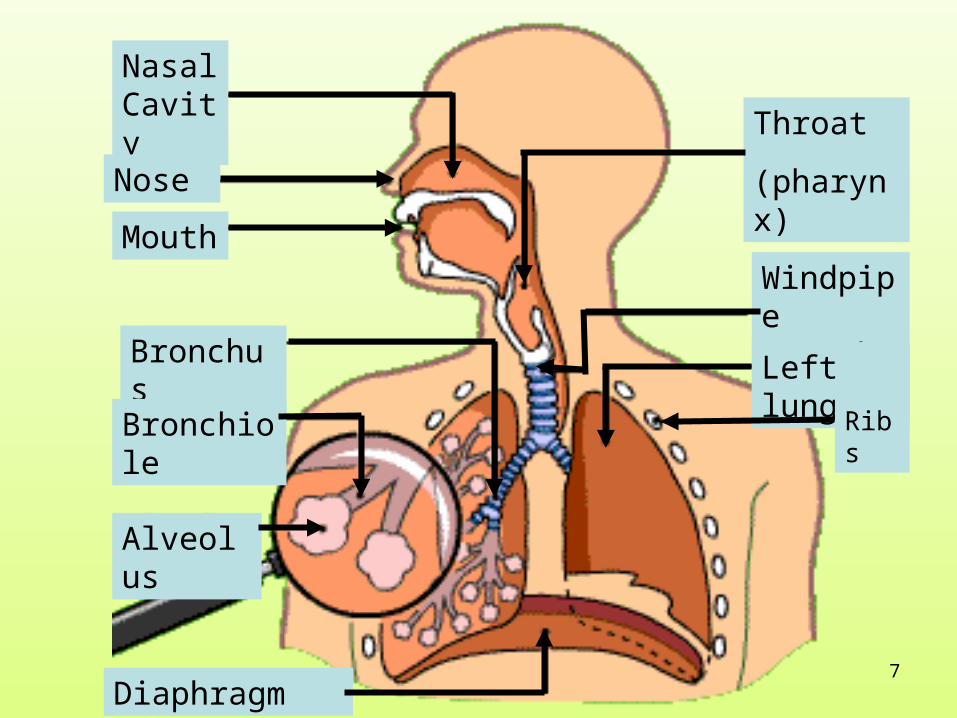
7
Nasal Cavity
Nose
Mouth
Bronchus
Bronchiole
Alveolus
Diaphragm
Throat
(pharynx)
Windpipe (Trachea)
Left lungs
Ribs

8

9
sternum
ribs
diaphragm
external intercostal
muscles internal intercostal muscles
abdominal muscles
The thorax/chest
Expand
Recoil

10
• When intercostal muscles contract or relax, the volu
me of chest expand or recoil, then the volume of lun
gs expand or recoil. Why?

11
• Pleural cavity is made up of two layers of pleura.One is
visceral layer stick to the surface of lung and the other is
parietal layer stick to thorax .
• There is only little liquid in the pleural cavity but not gas.
• The effect of this layer of liquid is :( 1 ) The power between liquid molec
ules pastes two layers of pleura to make them tightly.
( 2 ) Lubrication effect between two layers of pleura.

12
Section B Pulmonary ventilation
Pulmonary ventilation is the gas exchange process between lungs and environment.
13
Mechanics of Pulmonary Ventilation:Mechanics of Pulmonary Ventilation:
Two factors:
• One is the power to push gas flowing.• The other is resistance to prevent gas flowing.
• The former must overcome the latter , and then
pulmonary ventilation can be completed.
14
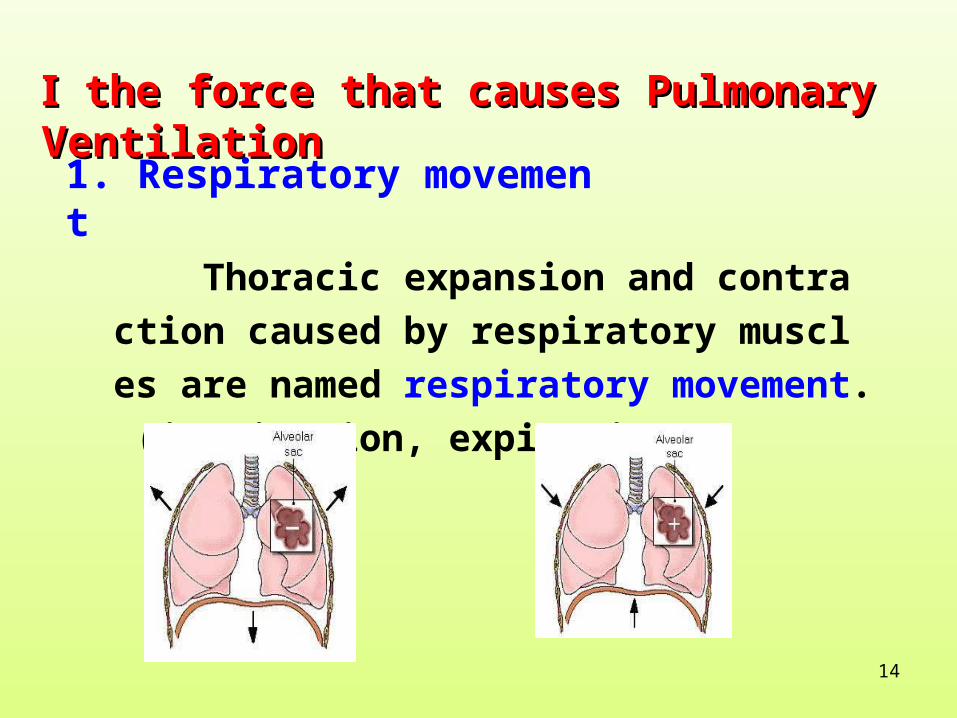
Ⅰ Ⅰ the force that causesthe force that causes Pulmonary VentilationPulmonary Ventilation
1. Respiratory movement
Thoracic expansion and contraction caused
by respiratory muscles are named respiratory
movement. (inspiration, expiration)

15
• Muscles of inspiration : diaphragm and
external intercostal muscles
• Muscles of expiration : internal intercostal muscles
and abdominal muscles
Eupnea
deep breathing

16
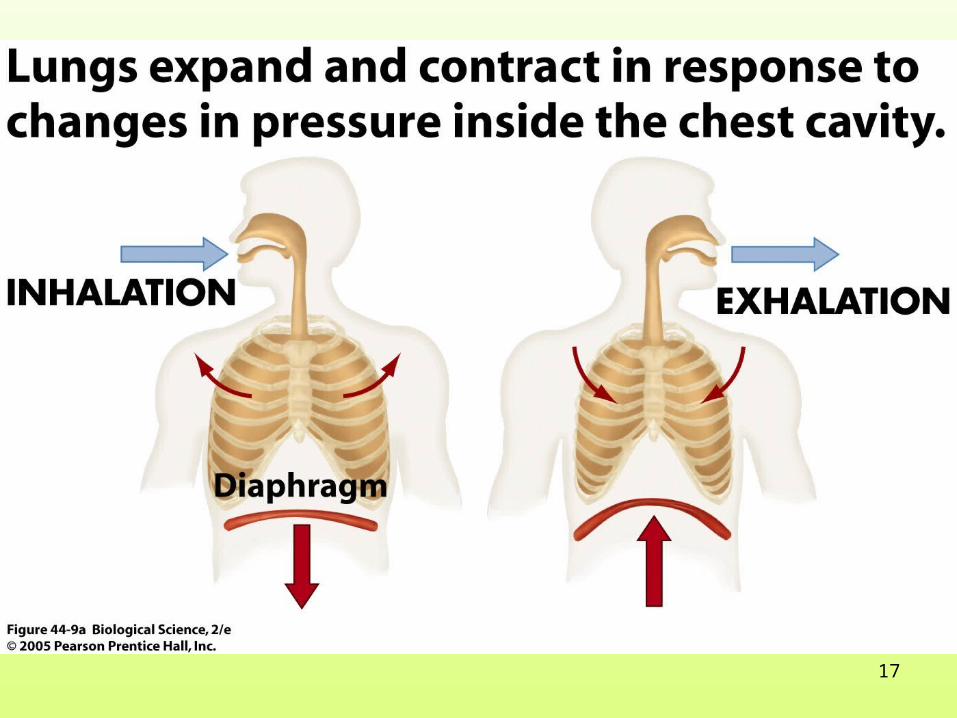
The Process of eupnea:
Inspiration: inspiration muscles contract thoraxes expand lungs expand lung volumes increase intrapulmonary pressure decreases gas enters lungs
Expiration: diaphragm and external intercostal muscles relax thorax recoils lung recoils intrapulmonary pressure increases gas is removed.
17
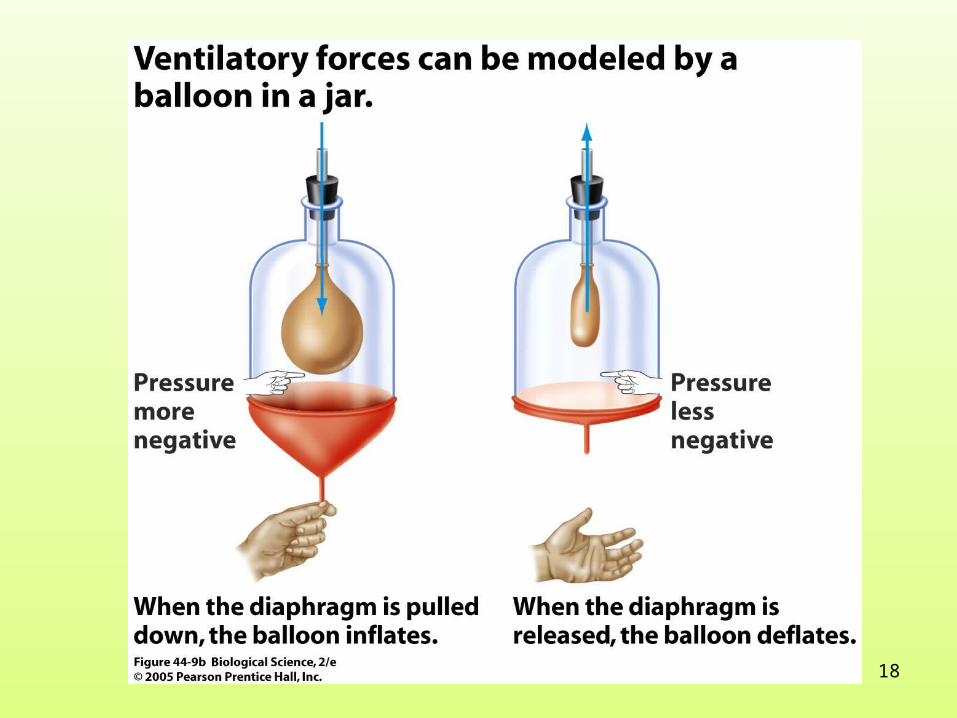
18
19
patternspatterns :
Abdominal breathing
Thoracic breathing
Eupnea
deep breathing
Normal quiet breathing is accomplished almost entirely by movement of the diaphragm.
Breathing caused primarily by the movement of external intercostal muscles.
Breathing at rest is calm.
Respiratory movement is greatly enhanced.
20
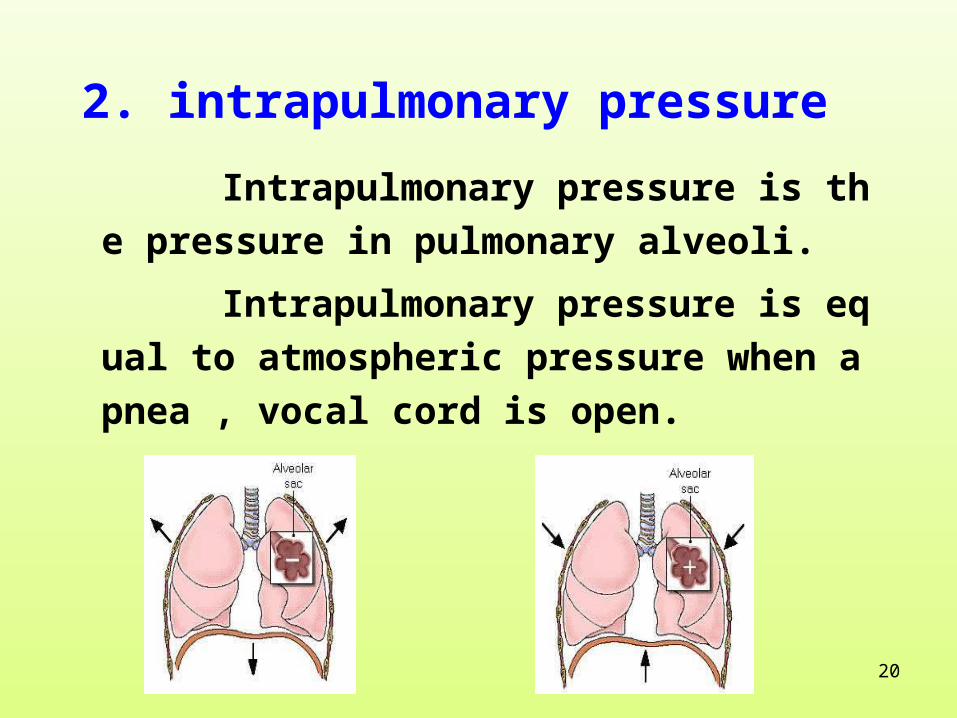
2. intrapulmonary pressure
Intrapulmonary pressure is the pressure in pul
monary alveoli.
Intrapulmonary pressure is equal to atmosphe
ric pressure when apnea , vocal cord is open.

21
At the first of inspiration, lung volume increases an
d intrapulmonary pressure decreases below atmosph
eric pressure. Air enters alveoli under the pressure di
fference. Intrapulmonary pressure increases as the in
creasing of gas in lung. At the last of inspiration, intr
apulmonary pressure is equal to atmospheric pressur
e and the air flow stops.

22
At the first of expiration, lung volume decreases an
d intrapulmonary pressure increases until it exceeds
atmospheric pressure. Air outflows lungs and intrap
ulmonary pressure decreases by and by. Intrapulmo
nary pressure is equal to atmospheric pressure at th
e last of expiration.
23
Artificial respiration: once respiration stops, int
rapulmonary pressure can be changed factitiously .
Pressure difference between intrapulmonary pres
sure and atmospheric pressure can be created to
maintain pulmonary ventilation .

24
Intrapleural pressure is u
sually negative pressure.
At the end of expiration o
f eupnea,the pressure is a
bout -5~ -3mmHg.
At the end of inpiration o
f eupnea, the pressure is
about -10~ -5mmHg.
3. Intrapleural pressure

25
Intrapleural pressure = intrapulmonary pressure - lungs recoil
At the end of respiration or inspiration, intrapulmonary pressure equals atmospheric pressure
intrapleural pressure= - lungs recoil

26
If pleura breaks, pleural cavity will be open to
atmosphere and air will enter pleural cavity . This
is called pneumothorax. At this time , two layers o
f pleura separate and lungs contract for the elasti
c recoil.

27
Power of Pulmonary Ventilation (Summary)
Expansion and contraction of respiration muscles e
xpansion and contraction of thoracic cage (lungs c
hange with the moving of thoracic cage)lung volumes
change pressure differences between lung volume
and atmospheric pressure gas enters or is removed
out of lungs.
28
Ⅱ Ⅱ Resistances to Pulmonary Ventilation Resistances to Pulmonary Ventilation
one is elastic resistance (70 % ) ( the main resistance of eupnea )
elastic resistance of lung
elastic resistance of thorax
the other is non- elastic resistance( 30 % )
airway resistanceinertial resistanceviscous resistance of organization

29
1. Elastic Resistance and Compliance
The ability of an elastic structure to resist stretching or distortion is named elastic resistance.
Compliance is the expandability of elastic tissue when acted on by foreign forces.
Relationship between compliance and elastic resistance C = 1 / R
☆
☆
☆
Compliance is inversely proportional to elastic resistance, that is, the larger the compliance, the less elastic properties, and vice versa.
E.g. an elastic band

30
(( 11 )) Elastic Resistance of Lungs and ComplianceElastic Resistance of Lungs and Compliance change of lung volume (△ V )lungs compliance = change of transpulmonary pressure ( △P )
transpulmonary pressure is the difference between intrapulmonary pressure and pleural pressure.
(L/cmH2O)

31
injector
Water manometer
Connect tracheal intubation
Three-way tap
32
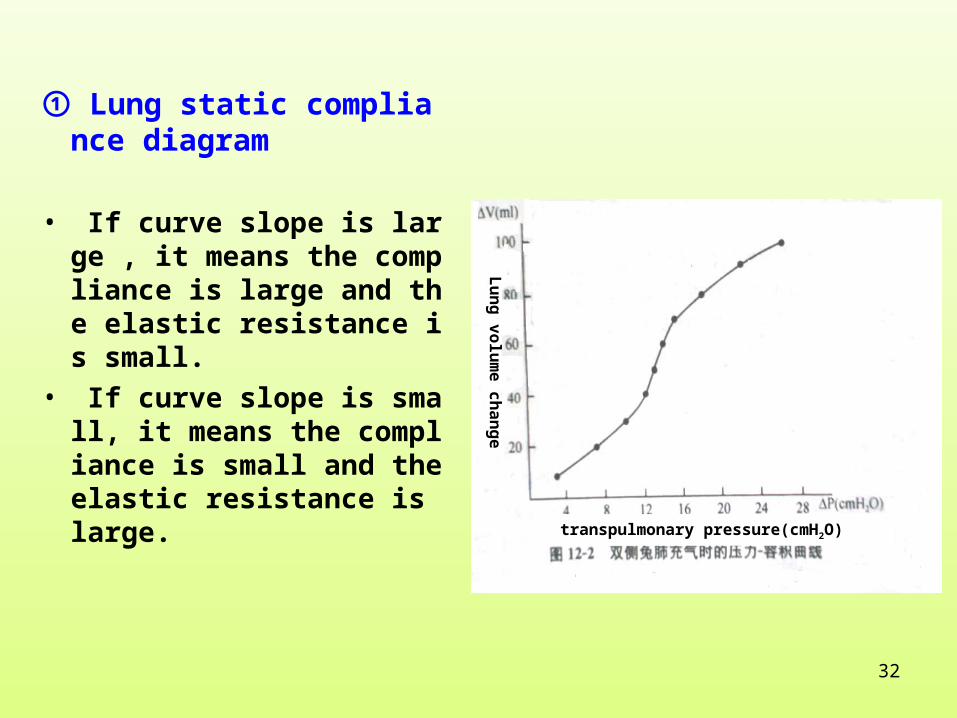
① Lung static compliance diagram
• If curve slope is large , it means the compliance is large and the elastic resistance is small.
• If curve slope is small, it means the compliance is small and the elastic resistance is large.
transpulmonary pressure(cmH2O)
Lu
ng
vo
lum
e c
ha
ng
e

33
34
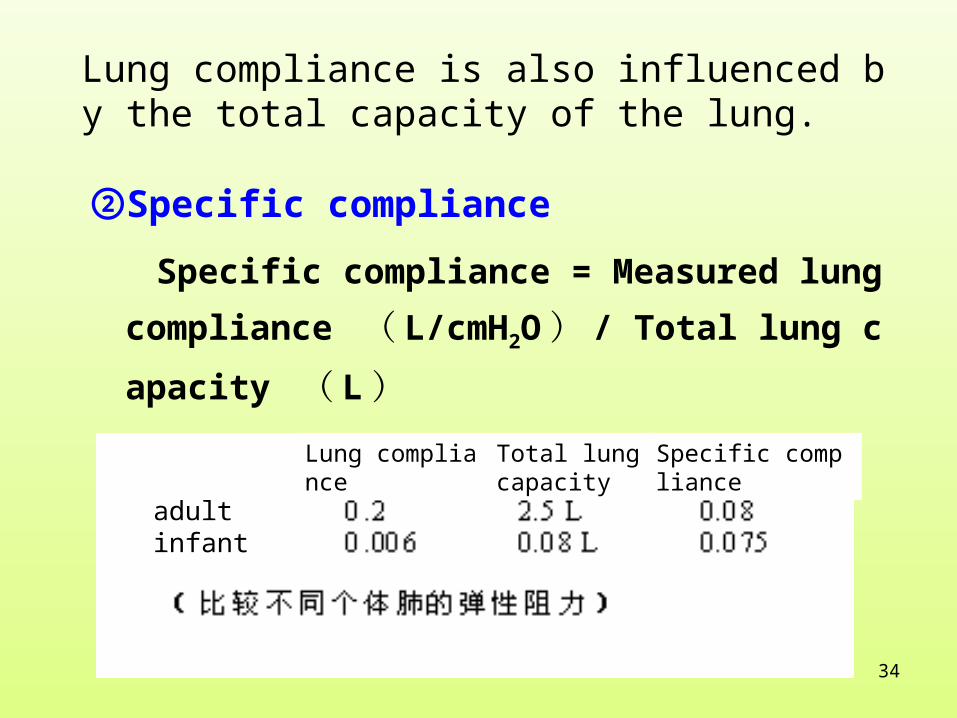
②Specific compliance
Specific compliance = Measured lung compliance
( L/cmH2O ) / Total lung capacity ( L )
adultinfant
Lung compliance
Total lung capacity
Specific compliance
Lung compliance is also influenced by the total capacity of the lung.
35
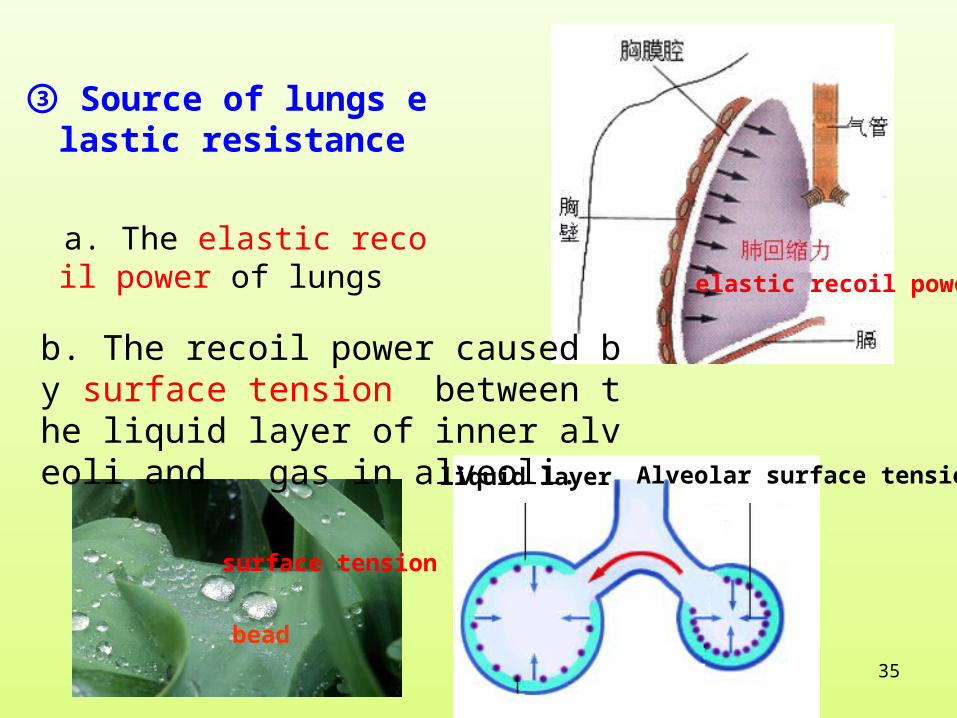
③ Source of lungs elastic resistance
a. The elastic recoil power of lungs elastic recoil power
surface tension
bead
liquid layer Alveolar surface tension
b. The recoil power caused by surface tension between the liquid layer of inner alveoli and gas in alveoli.
36
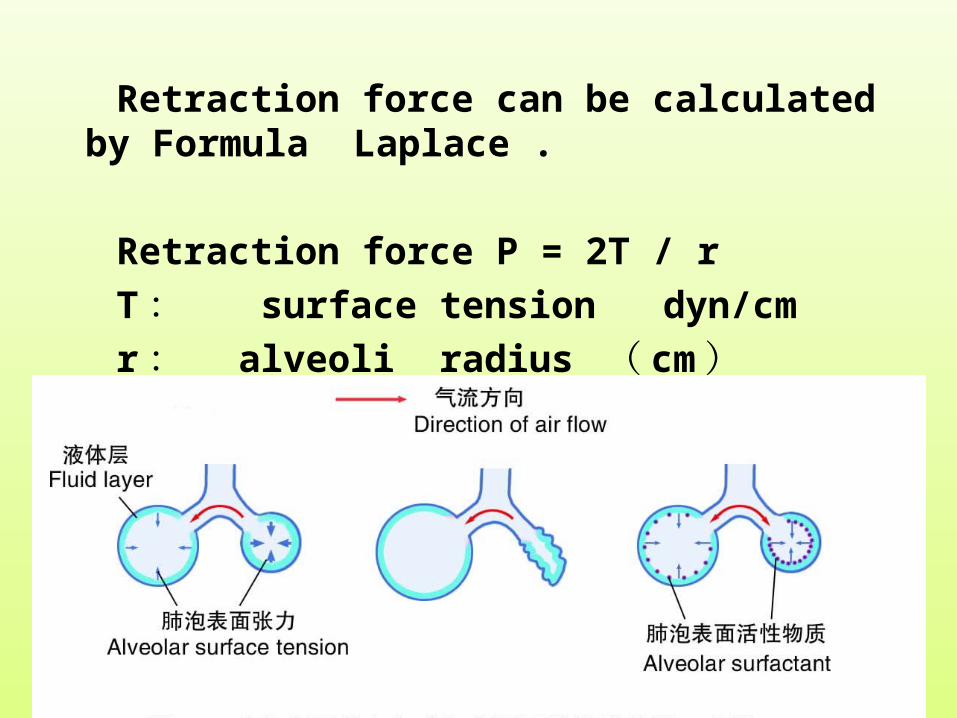
Retraction force can be calculated by Formula Laplace .
Retraction force P = 2T / r
T : surface tension dyn/cm
r : alveoli radius ( cm )

37
(2) Pulmonary Surfactant
DPPC
DPPC is an important p
ulmonary surfactant in the
the liquid layer of inner al
veoli, DPPC binding to a
polipoprotein exist as lip
oprotein.
liquid layer Alveolar surface tension

38
• DPPC is synthesised by alveoli cells.Ⅱ

39
physiological effect of pulmonary surfactant
( 1 ) Lower alveolar surface tension and reduce inspiration
resistance.
( 2 ) Accommodate surface tension and stable alveolar pres
sure.
( 3 ) The effect of suction is reduced. Reduce the producin
g of alveolar liquid and prevent pulmonary edema.
40
development of Pulmonary surfactant
occurent from cyesising 25 - 30 weeksat the high point in cyesising 40 weeks
Premature may get respiratory distress syndrome even to death for deficiency of pulmonary surfactant and formation of pulmonary atelectasis.

41
2. non-elasrtic resistance
Learn by yourself.
42
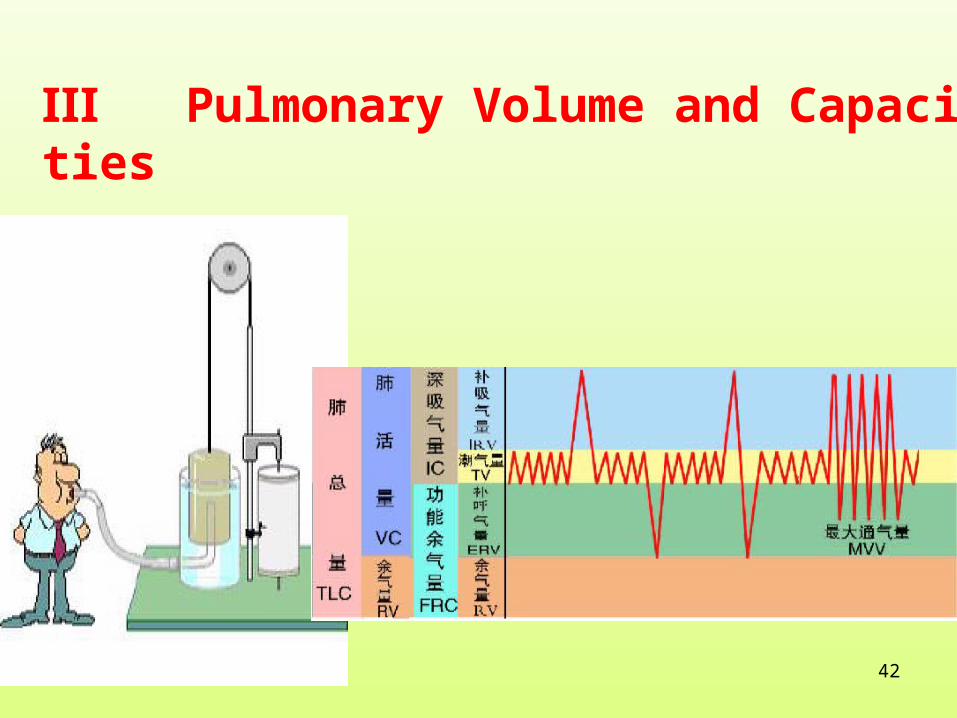
Ⅲ Pulmonary Volume and Capacities
43
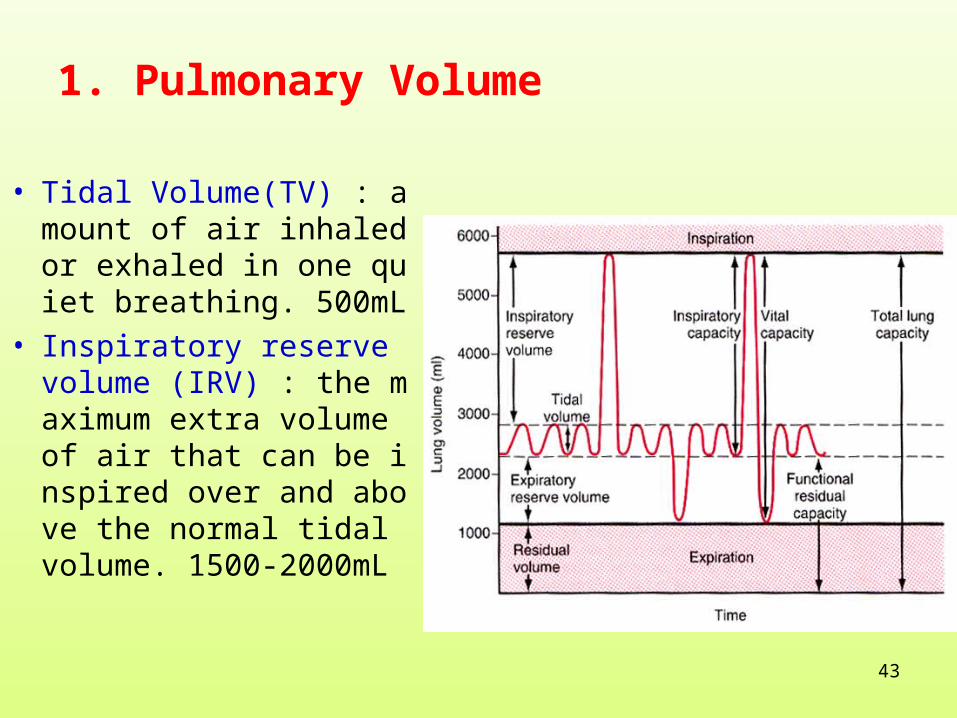
• Tidal Volume(TV) : amount of air inhaled or exhaled in one quiet breathing. 500mL
• Inspiratory reserve volume (IRV) : the maximum extra volume of air that can be inspired over and above the normal tidal volume. 1500-2000mL
1. Pulmonary Volume

44
● Expiratory reserve volume (ERV ): the maximum extra volume of air that can be exspired by forceful expiraton after the end of a normal tidal expiraton . 900-1200mL● RV(residual volume): amount of air remaining in the lungs after maximum expiraton. 1000-1500mL

45
2. pulmonary capacities
● Inspiratory Capacity (IC):maximum amount of air that can be inhaled after a normal tidal expiration. = TV + IRV 2000 - 2500 mL
● Functional residual capacity (FRC): amount of air remaining in the lungs after a normal tidal expiration .
= RV+ERV 2500 mL
46
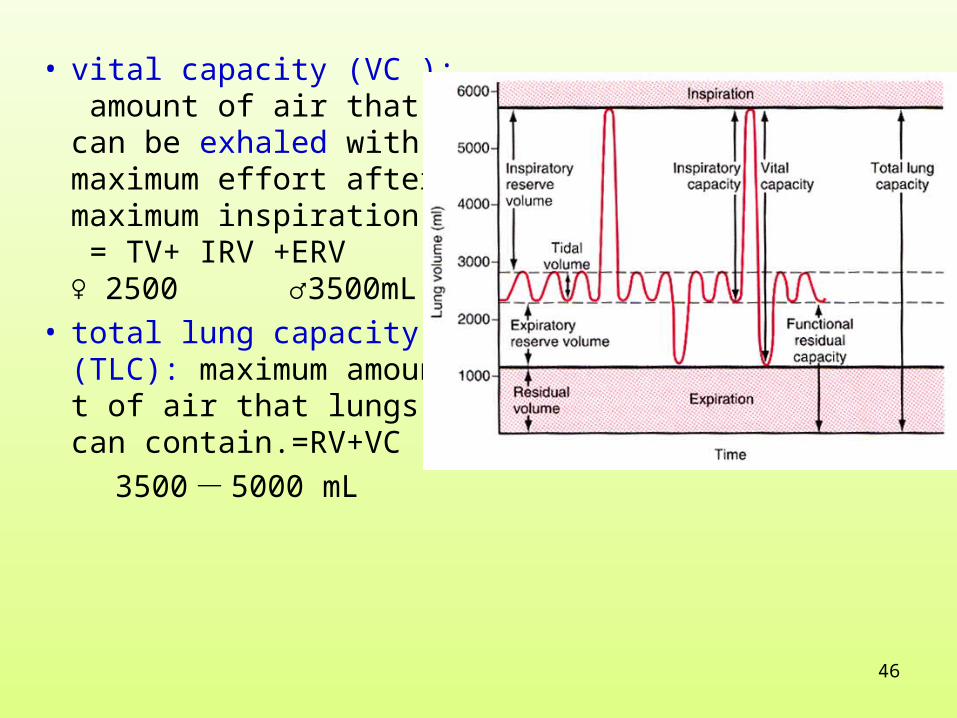
• vital capacity (VC ): amount of air that can be exhaled with maximum effort after maximum inspiration. = TV+ IRV +ERV ♀ 2500 ♂3500mL
• total lung capacity (TLC): maximum amount of air that lungs can contain.=RV+VC
3500 - 5000 mL

47

48
• timed vital capacity (TVC)• expired 80% of all vital capacity at the first second• expired 96% of all vital capacity at the second second• expired 99% of all vital capacity at the third second

49
3. lung ventilation volume
Minute ventilation volume=
Tidal Volume×respiratory rate 6-8L
Maximal voluntary ventilation :70 - 120L/min
It is expressed ventilation reserve.
500ml 12-18 times/min

50
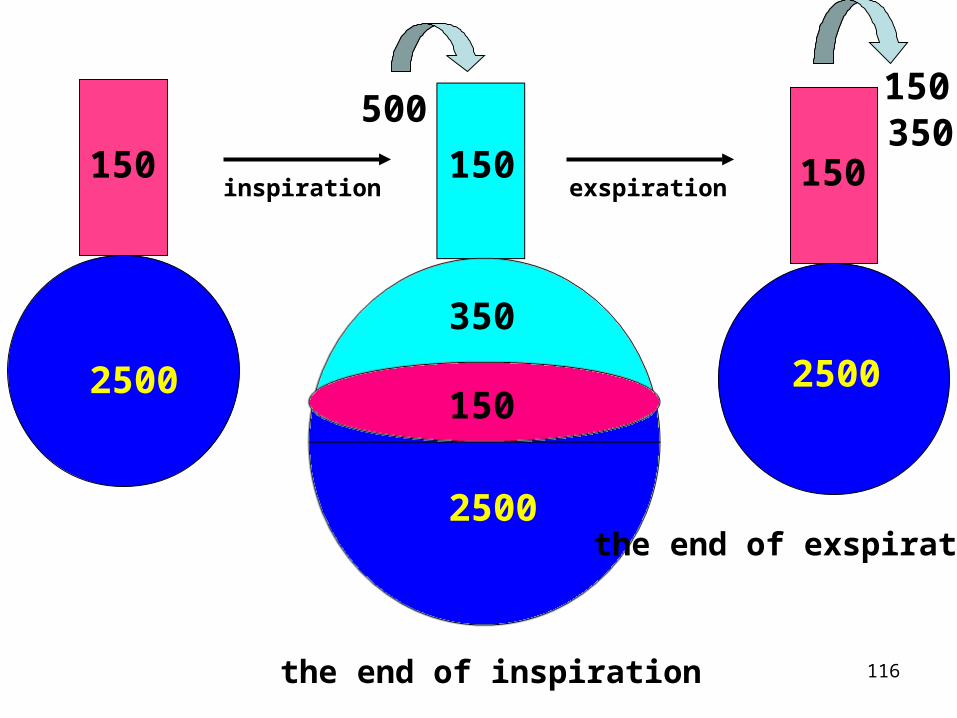
4.Dead space and Alveolar Ventilation
dead space
anatomic dead space
alveolar dead space
physiologic dead space:

51
150 150150
2500
2500 2500150
350
the end of inspiration
the end of exspiration
500150350
inspiration exspiration
52
alveolar ventilation = (tidal volume- dead space)× resp
iratory rate
( 500mL - 150mL ) ×12 次 / 分 =350 ×12= 4200 L
53
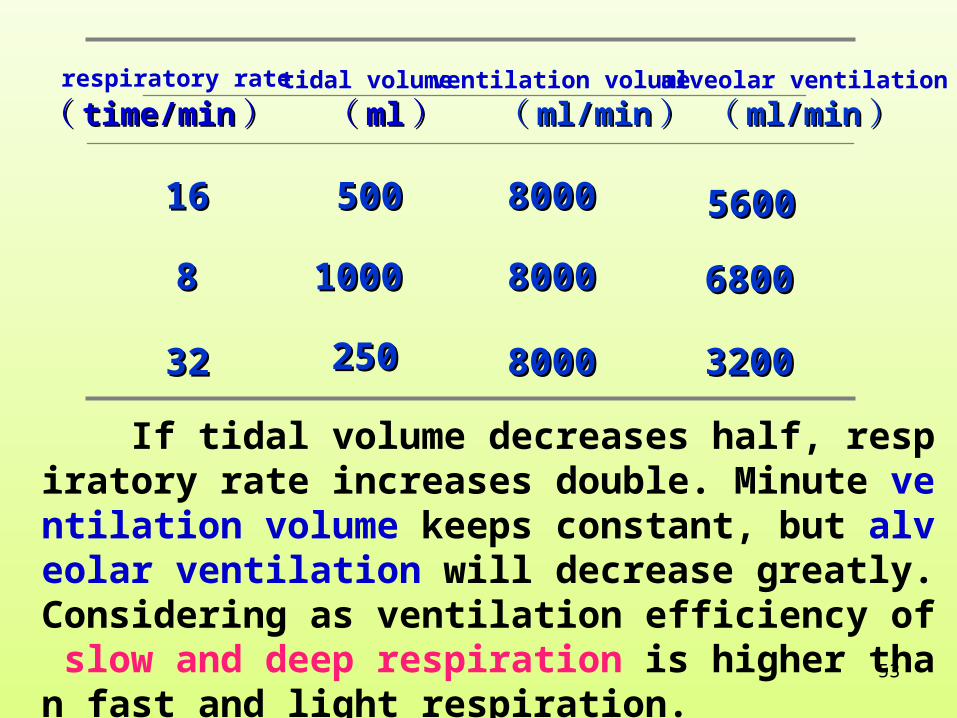
respiratory rate
(( time/mintime/min ))tidal volume
(( mlml ))ventilation volume
(( ml/minml/min ))alveolar ventilation
(( ml/minml/min ))
1616 500500 80008000 56005600
88 10001000 80008000 68006800
3232 250250 80008000 32003200
If tidal volume decreases half, respiratory rate increases double. Minute ventilation volume keeps constant, but alveolar ventilation will decrease greatly. Considering as ventilation efficiency of slow and deep respiration is higher than fast and light respiration.
54
Section C Gas exchange
55
Ⅰ principle of gas exchange
gas diffusion:
Gas molecules move freely among one another. The
result is gas molecules diffuse from high-pressure area
toward low-pressure area. The process is called gas diff
usion.
Exchange of gas in alveoli and tissues are physical d
iffusion processes .
56
The volume of gas diffusion in unit time is called diffusion rate. It is effected by the following factors
D∝△P*T*A*S
d*√MW
△P is the pressure difference between the two ends of the
diffusion pathway, T is the temperature, A represents the
cross-sectional area of the pathway, S is the solubility of t
he gas, d is the distance of diffusion, MW stands for the m
olecular weight of the gas.
57
1. Gas partial pressure difference: gas partial pressure diff
erence is larger—diffuses faster
2. Gas molecular weight and solubility:
when solubility is high, it diffuses fast
when molecular weight is large,it diffuses slowly.

58
3. Diffusion area of alveolar membrane : when diffu
sion area of alveolar membrane is large,it diffuses fas
t
★diffusion area of alveolar membrane is 40m2 in no
rmal quiet state.
★ diffusion area of alveolar membrane is 70m2 duri
ng sports.

59

60
4. Diffusion distance—thickness of alveolar membrane(inverse ratio relationship)
★ Pulmonary fibrosis
★ Pulmonary edema
5. Temperature of fluid increases
Solubility increases—Diffuses fast
Averages 0.6 μm
61
Ventilation/perfusion ratio is the rate between alveolar ventilation and pulmonary blood flow.
VA: alveolar ventilation per minuteQ : pulmonary perfusion per minute
VA/Q (value of normal quiet state) = 4.2L/5L = 0.84
If blood flow decreases and gas exchange are normal--the exchange total amount decreases. Soalveolar ventilation and blood flow must keep anappropriate ratio.
6. Ventilation /Perfusion Ratio(VA/Q )

62
★ventilation /perfusion ratio increases:it means partial alveolar gas can not exchange fully with the blood =physiological dead space increases.
★ventilation /perfusion ratio decreases:it means partial blood flow through hypoventilation alveoli. They can not get fully exchange. And it equals functional arteriovenous shunt.
63
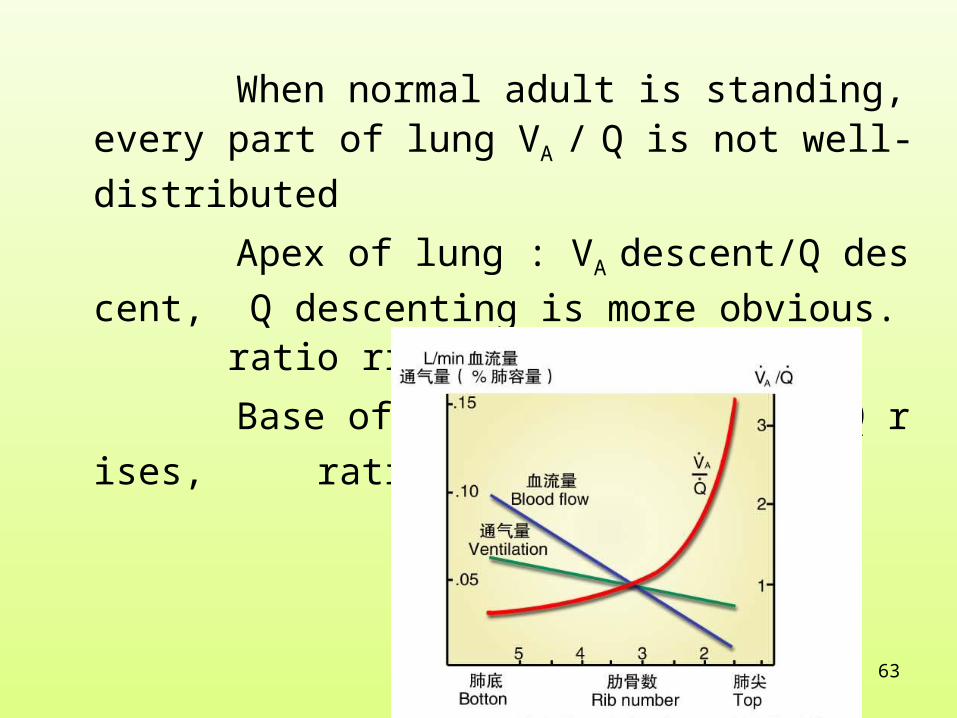
When normal adult is standing, every part of lung V
A / Q is not well-distributed
Apex of lung : VA descent/Q descent, Q descenting
is more obvious. ratio rises(more than 3)
Base of lung: VA descents/Q rises, ratio descents
(0.6).

64
7. pulmonary diffusion capacity
When all kinds of gas is under unit partial pressure difference,the gas volume(ml) passing through respiratory membrane per minute is called pulmonary diffusion capacity. It is the physiological index to test the diffusion ability of respiratory membrane.
DL
V
PA PB

65
CO2 diffusibility/ O2 diffusibility= √O2 molecular
weight/ √CO2 molecular weight=√32/√44 = 5.6/6.
6
But because CO2 solubility/ O2 solubility= 0.592/0.0
244=24.3/1.0(Herry’s law )CO2 diffusion velocity/ O2 diffusion velocity =
( 5.6/6.6 ) × ( 0.592/0.0244)=20.6/1.0 From all above ,we know that the diffusion velocity of CO2 is much more than that of O2. There is no diffusion disturbance of CO2 in clinical.
66
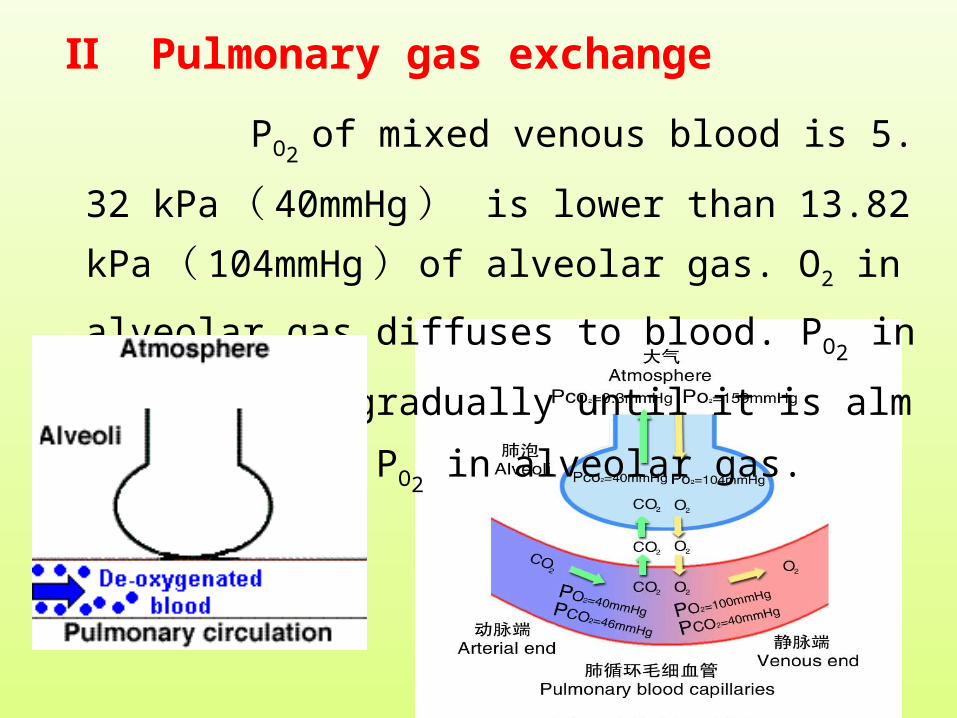
Ⅱ Pulmonary gas exchange
PO2 of mixed venous blood is 5.32 kPa ( 40mmH
g ) is lower than 13.82 kPa ( 104mmHg ) of alveo
lar gas. O2 in alveolar gas diffuses to blood. PO2 in bloo
d rises gradually until it is almost equal to PO2 in alveol
ar gas.
67
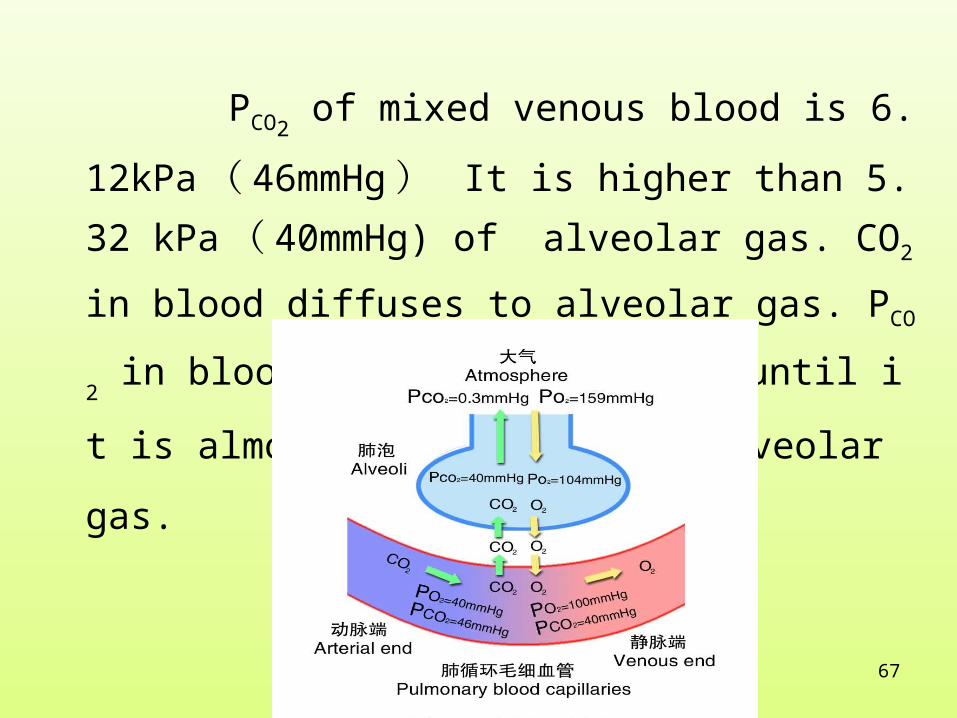
PCO2 of mixed venous blood is 6.12kPa ( 46mmH
g ) It is higher than 5.32 kPa ( 40mmHg) of alveol
ar gas. CO2 in blood diffuses to alveolar gas. PCO2 in bl
ood descents gradually until it is almost equal to PCO2 i
n alveolar gas.

68
69
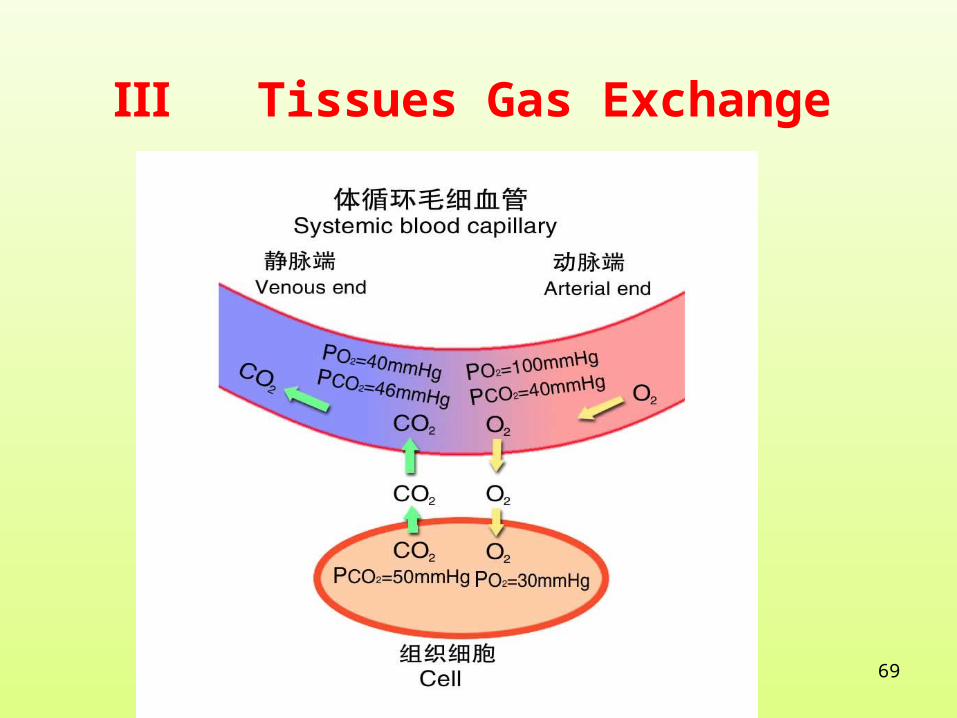
Ⅲ Tissues Gas Exchange
70

71
72
Section D Gas Transport
Ⅰ Existing forms of O2 and CO2 in the blood
chemical combination(primary)
physical dissolution(medium)two forms
O2 physical dissolution combination physical dissolution O2
lung tissue
CO2 CO2 physical dissolutioncombination physical dissolution

73
Ⅱ oxygen transportation
oxygen transportation
98.5 % binding to Hb
1.5 % physical dissolution
74
75
Maximum capacity of hemoglobin binding with O2 (in every 100ml blood ) is named oxygen capacity.
When normal Hb is in 15g/100ml blood , 1g Hb
binds with 1.34ml O2.
Oxygen capacity= 15×1.34 = 20ml
The volume of hemoglobin binding with oxygen (in fact or really) is called oxygen content.
arterial blood: 20ml O2
venous blood: 15ml O2

76
The percentage of oxygen content to oxygen capaci
ty is called oxygen saturation.
oxygen content
oxygen capacity
In arterial blood, oxygen content equals 20ml and o
xygen saturation is 100%.
In venous blood , oxygen content equals 15ml and o
xygen saturation is 75%.
×100%)(=

77
form
O2 partial pressure is higher(lung)
Hb + O2 HbO2
O2 partial pressure is lower(tissues)
reduction 、 royal blue oxygenation 、 red
break
relaxationtension
(一)

78
character
1. Reversible binding. Without enzyme. Fast. Effected b
y PO2.
2. O2 binds with Fe2+ of hemoglobin . The iron value is
permanent. So the process is called oxygenation but n
ot oxidation.
PO2↑
PO2↓HbO2Hb + O2
79
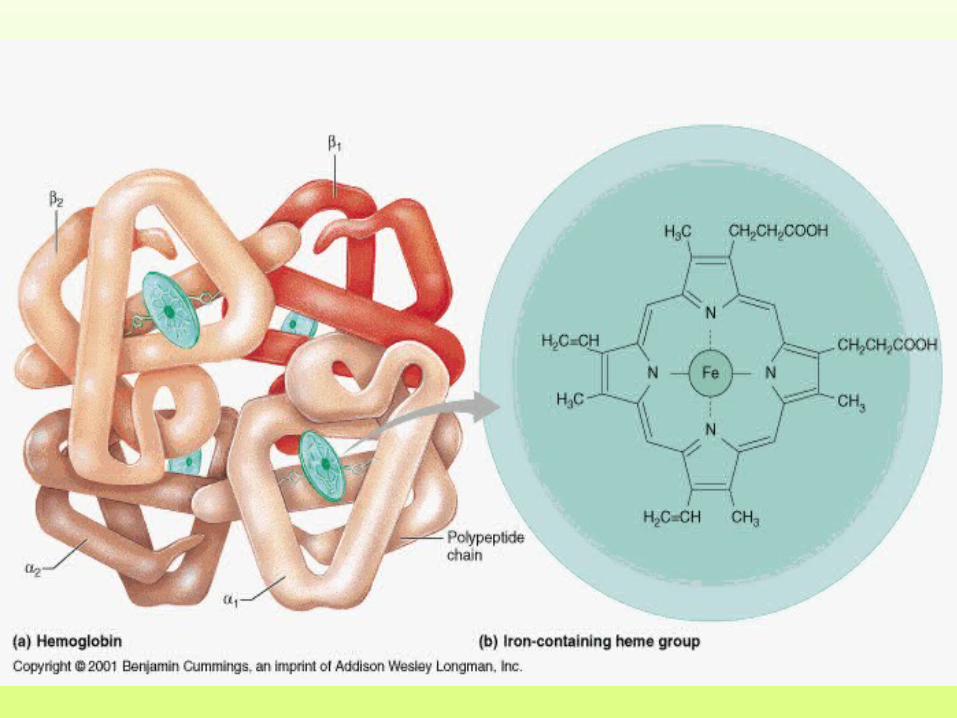
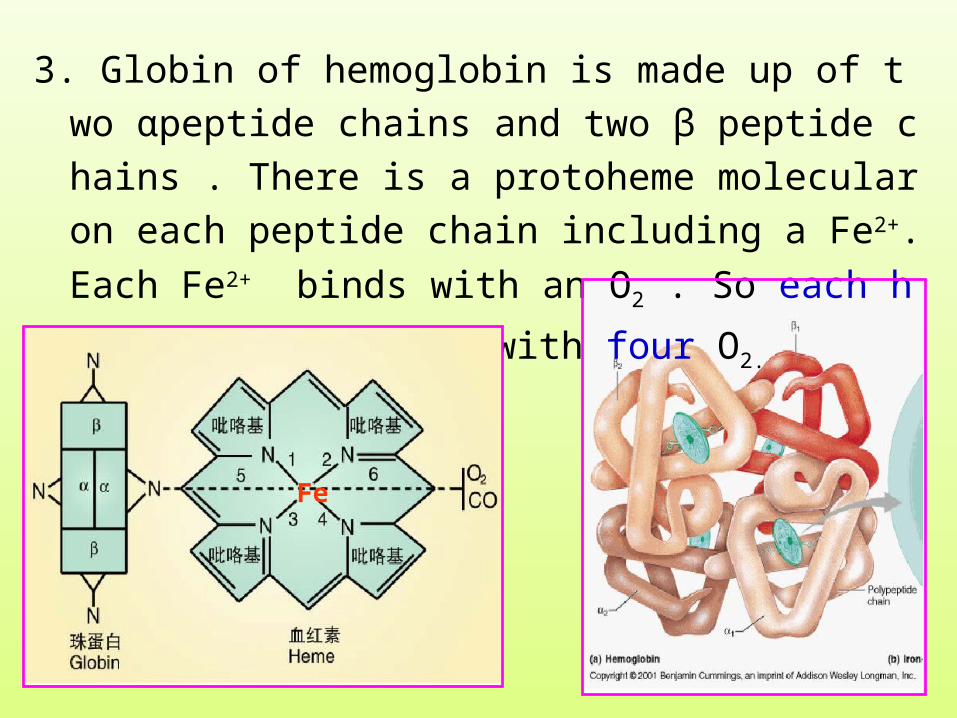
3. Globin of hemoglobin is made up of two αpeptide chains
and two β peptide chains . There is a protoheme molecul
ar on each peptide chain including a Fe2+. Each Fe2+ bind
s with an O2 . So each hemoglobin can bind with four O2.
Fe

80
4. O2 can facilitate binding or releasing.
In lungs, increasing of PO2 promotes combination.
In tissues, decreasing of PO2 promotes releasing.
PO2↑
PO2↓HbO2Hb + O2

81
5. The binding or releasing curves of Hb and O2 appear S
form.This is related to the allosterism effect of Hb.
Hb binds with O2—salt bond breaks, R form
Hb releasing with O2—salt bond forms,T form
The affinity of T form to O2 is smaller.
The affinity of R form to O2 is larger.
relaxationtension
Hb HbO2
82
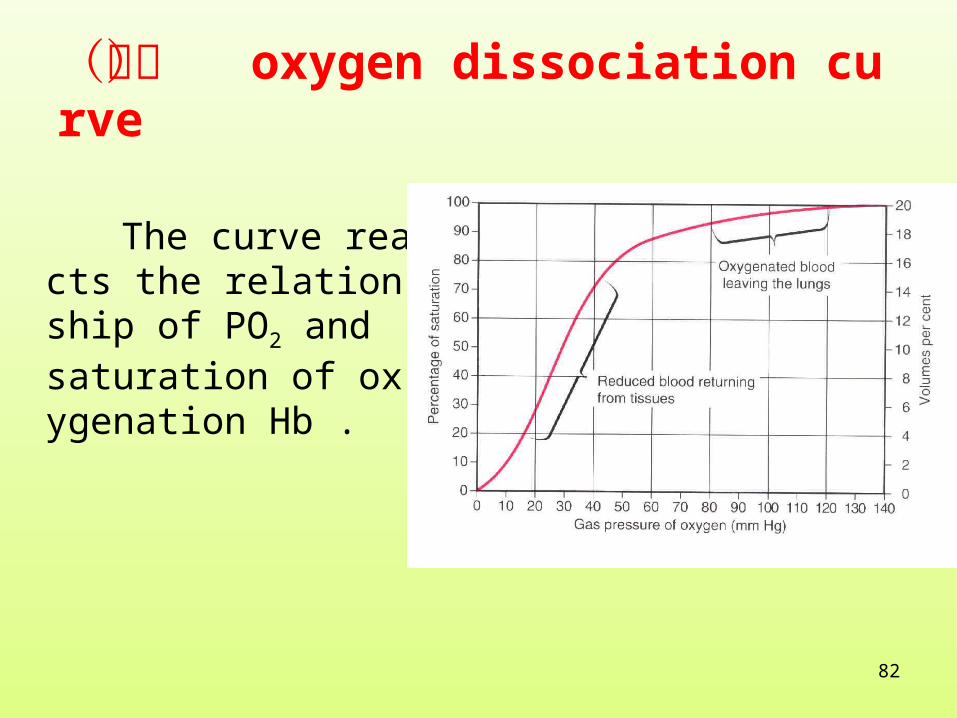
(二) oxygen dissociation curve
The curve reacts the relationship of PO2 and saturation of oxygenation Hb .

83
oxygen dissociation curve character
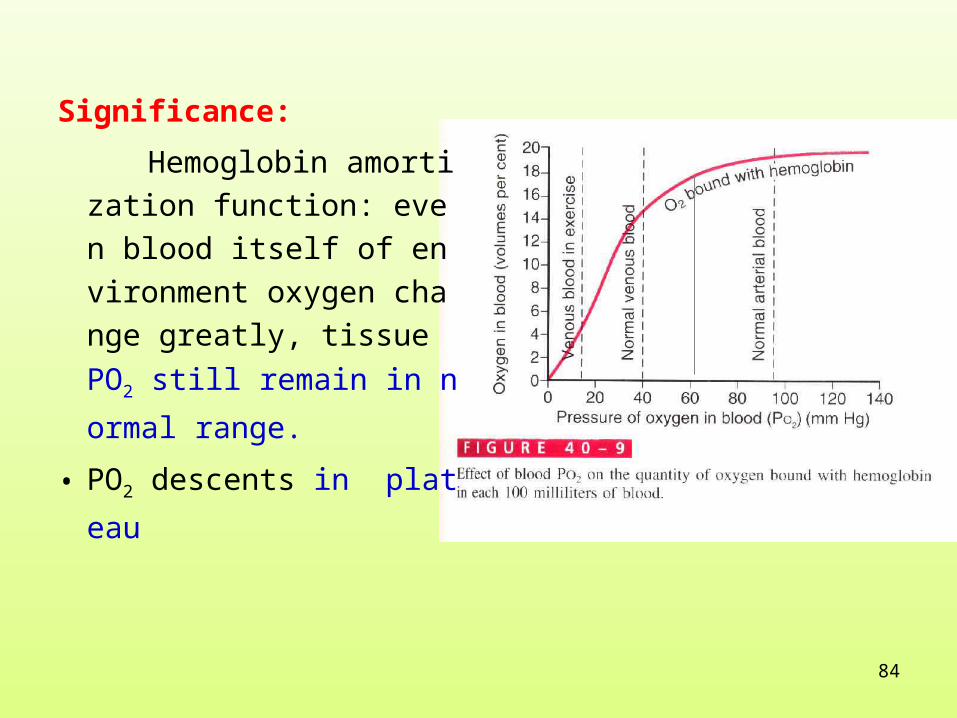
1. Superior segment of curve: PO2 60 - 100mmHg.
Slope is flat.
Partial pressure of oxygen c
hanges greatly. But oxygen sa
turation changes little—even
PO2 of environment or alveoli
descents, oxygenation saturat
ion will maintain high level.
84
Significance:
Hemoglobin amortizati
on function: even blood
itself of environment ox
ygen change greatly, tis
sue PO2 still remain in n
ormal range.
• PO2 descents in plateau
85
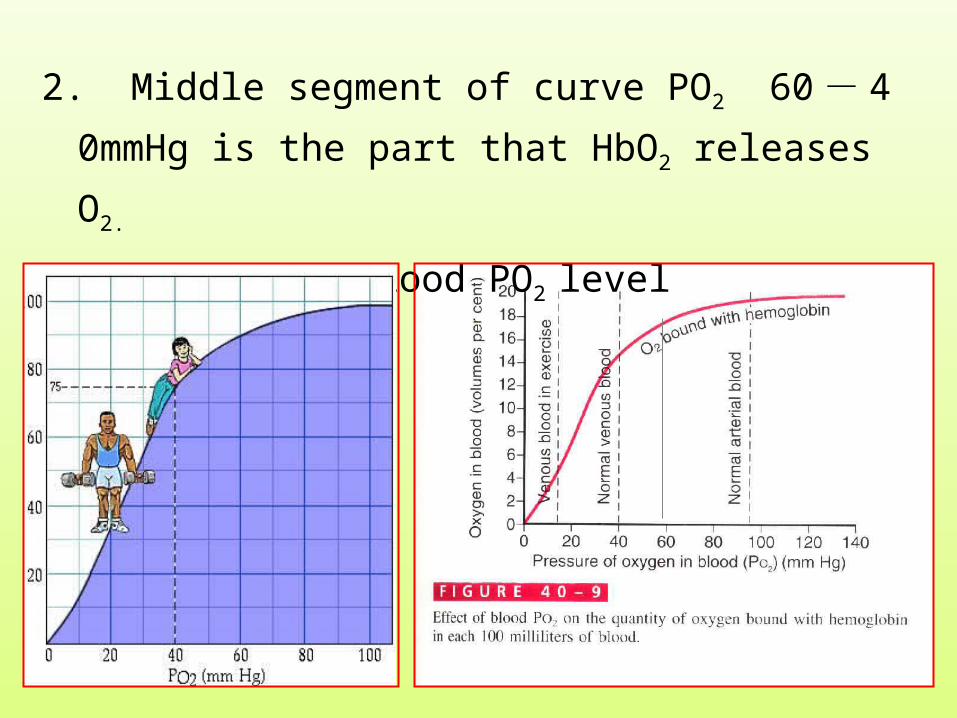
2. Middle segment of curve PO2 60 - 40mmHg is the p
art that HbO2 releases O2.
e.g. venous blood PO2 level

86
3. Inferior segment of curve . PO2 10 - 40mmHg . Th
e slope is steep.
PO2 descents a little. It makes oxygen saturation desc
ent greatly. This is benefit to supplying oxygen for tissue activity.
87
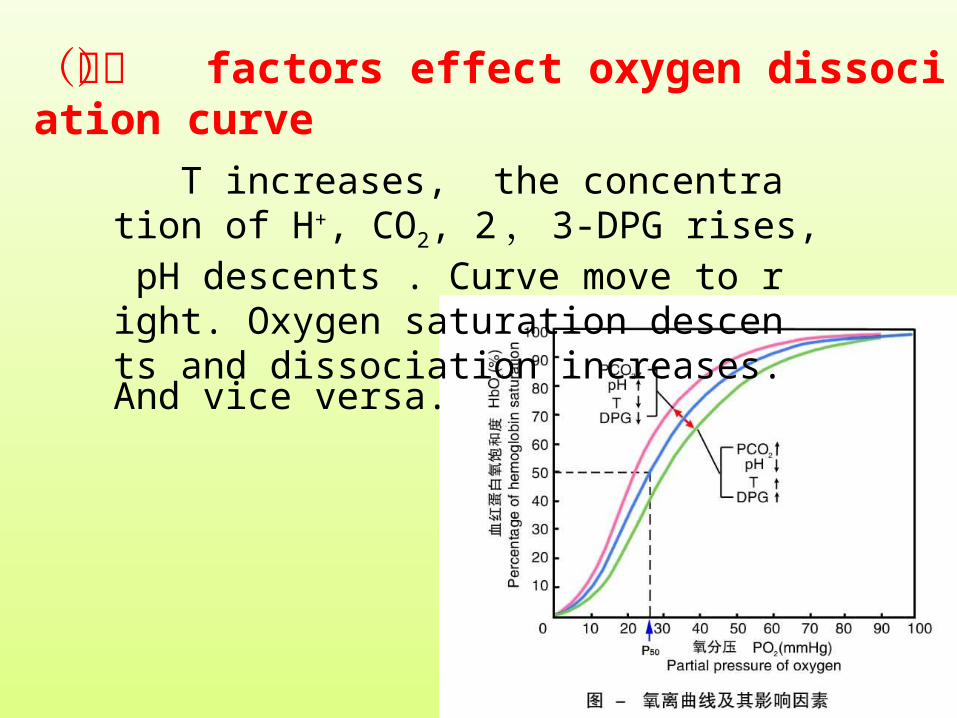
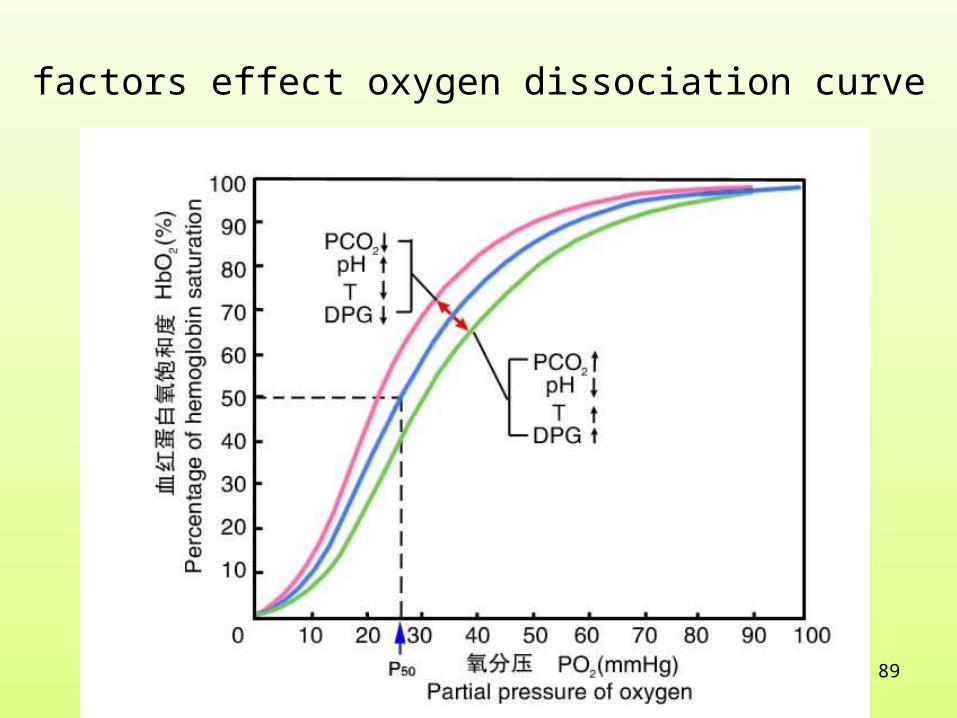
(三) factors effect oxygen dissociation curve
T increases, the concentration of H+, CO2, 2 ,3-DPG rises, pH descents . Curve move to right. Oxygen saturation descents and dissociation increases.
And vice versa.

88
2 , 3 - DPG is a kind of organophosphate in RBC.
缺氧、贫血 hypoxia, anemia
长时间运动 long time sports
RBC 2 , 3DPG increases
89
factors effect oxygen dissociation curve

90
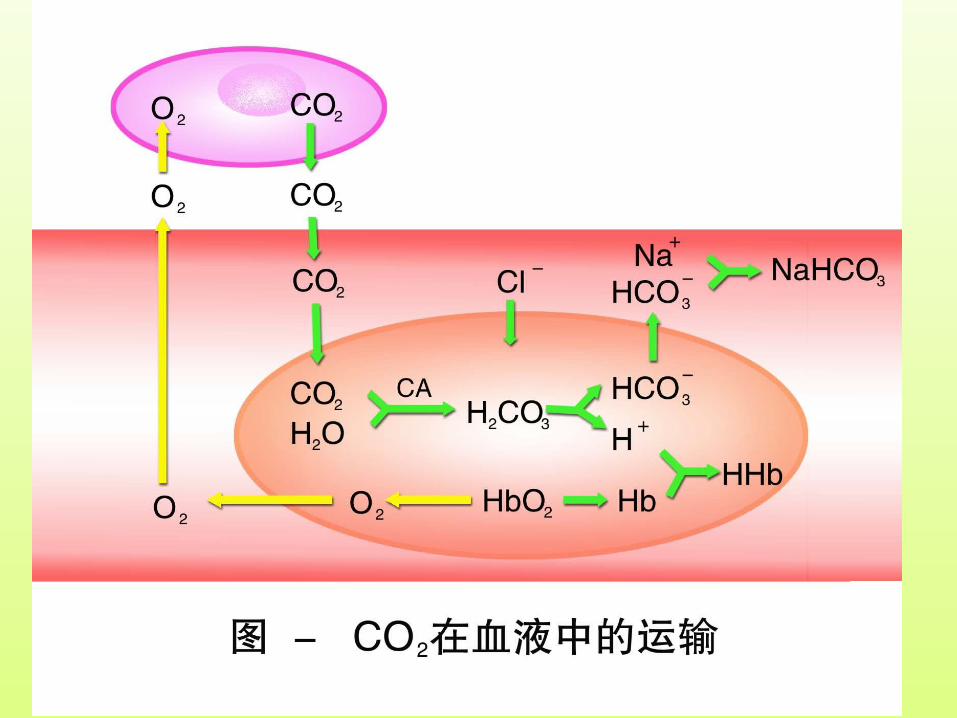
Ⅲ Transportation of CO2
transportation of CO2
physical dissolution( 5% )
combination( 95% )
bicarbonate( 88% )
Carbaminohemoglobin( 7% )
91
92
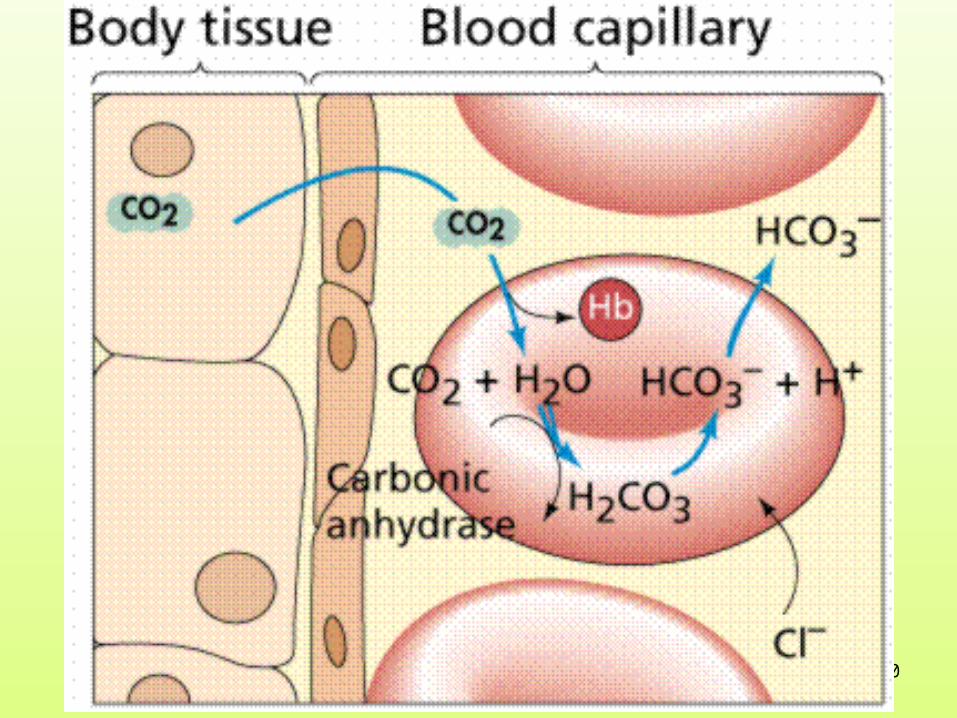
(一) Transport in bicarbonate pattern
character:
1. Reaction is reversible. But it need the help of enzyme(C
A).
2. Conjugation or dissociation is decided by partial pressure
difference of CO2.
3. There is the transfer of Cl - in the reaction.
93
(二) Transport in carbaminohemoglobin pattern
in tissues
HbNH2+CO2 HbNHCOOH
lung
HbNHCOO - + H +

94
character
1. Reaction is reversible and need not the help of enzyme.
2. Conjugation or dissociation is decided by the
oxygenation effect of Hb.
Much Deoxy Hb binds with CO2.
Little Hb binds dissociation is much.
3. The effect of partial pressure difference is not obvious.
in tissues HbNH2+CO2 HbNHCOOH lung HbNHCOO- + H+
carbaminohemoglobin

95
Section E Regulation of Respiration

96
Ⅰ respiratory center Respiratory center is composed of several groups
of nerve cells which produce and regulate respirator
y movement in central nervous system.
97
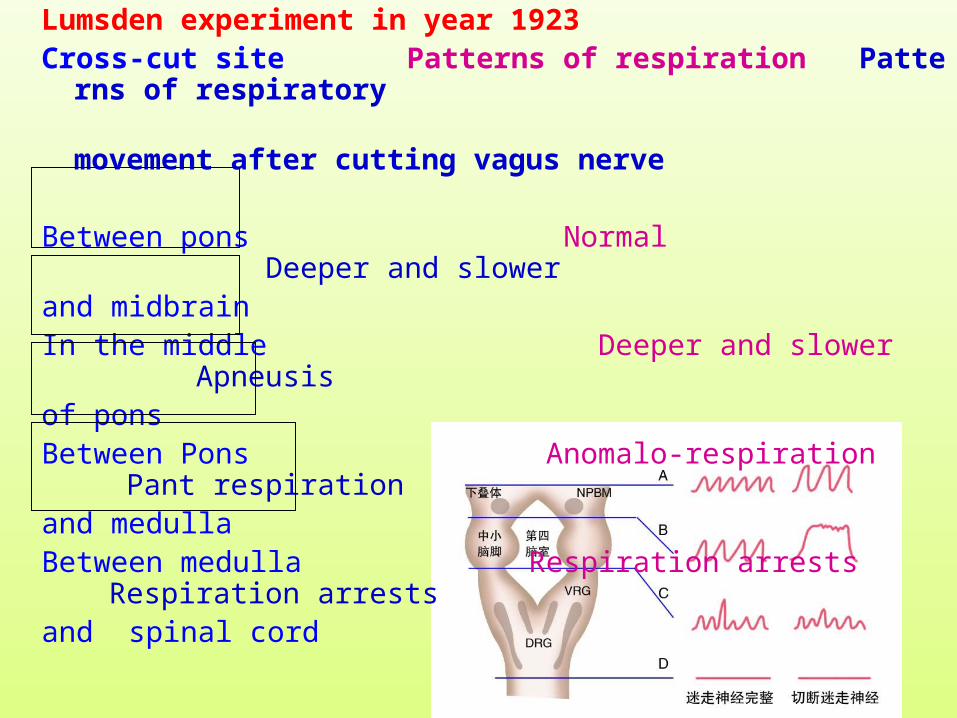
Lumsden experiment in year 1923 Cross-cut site Patterns of respiration Patterns of respiratory movement after cutting vagus nerve
Between pons Normal Deeper and slowerand midbrainIn the middle Deeper and slower Apneusisof ponsBetween Pons Anomalo-respiration Pant respirationand medullaBetween medulla Respiration arrests Respiration arrests and spinal cord

98
Conclusion:
Superior part of pons -- pneumotaxic respiratory center
medulla --basic respiratory center
spinal cord--primary respiratory center

99
Regulation of Cerebral Cortex to Respiration
1. Liberty Regulation and Creation of
respiration Conditioned reflex.
2. Coordination with the process of la
nguage activity.
Clinical: Descending pass of spinal c
ord pro-Lateral funiculus is damage
d.---Autonomous breathing arrests.
Regulate through voluntary breathin
g. Use breathing machine during sl
eeping . Oden’s curse
100
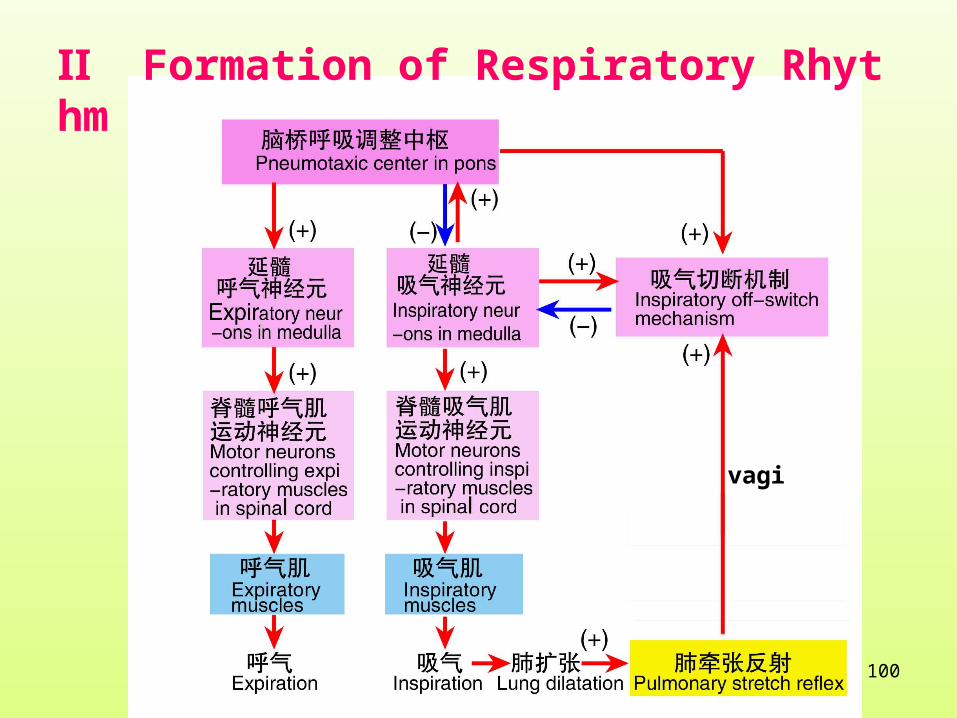
Ⅱ Formation of Respiratory Rhythm
vagi

101
Reversion inhibition theory(part neuronal cir
cuit feedback and controling theory)
1 ) Central inspiratory activity
2 ) inspiratory off-switch mechanism central inspirato
ry activity inspiration-initiative process
expiration-passive -process

102
3 ) The mechanism of changing from expiratory phase
to inspiration—there are probably a group of cutting of
f expiratory neurs.
Imagining the process of expiration phase is probabl
y controled by a mechanism of inhibiting inspiration a
bility during respiration phase. The ability degree of th
is mechanism is getting weaker during the expiration p
hase.once reaching the critical level, the inhibition of i
nspiration ability is relieved and the next inspiration w
ill begin.

103
Ⅲ Reflex Control of Breathing
Respiratory movement can be regulated , accelerate
d or inhibited by all kinds of stimulus to the body.
104
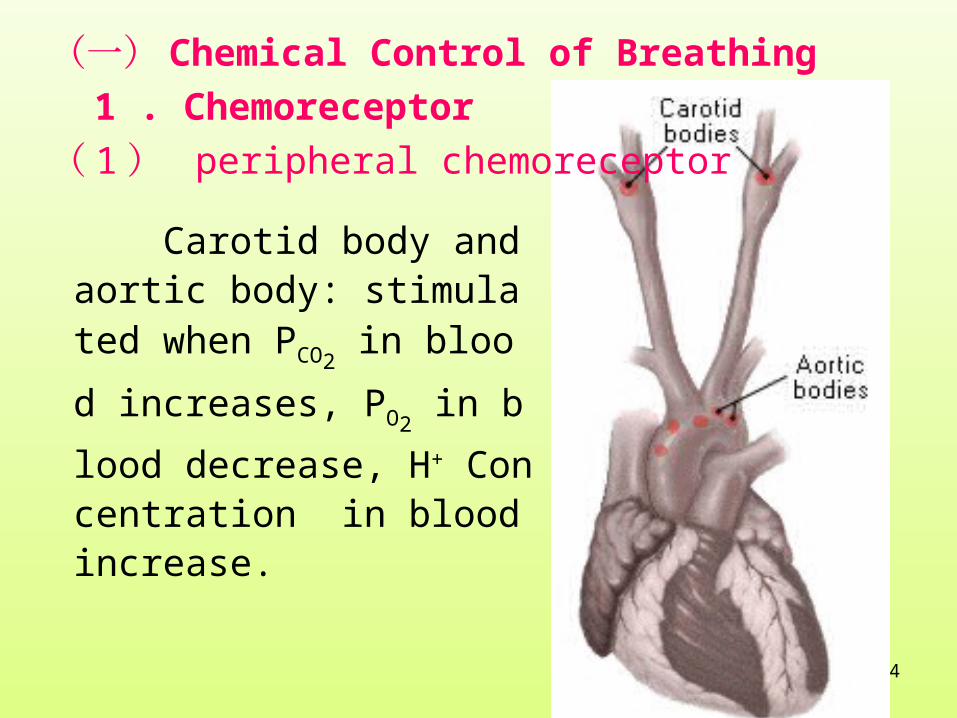
(一) Chemical Control of Breathing
1 . Chemoreceptor
( 1 ) peripheral chemoreceptor
Carotid body and aortic body: stimulated when PCO2
in blo
od increases, PO2 in blood decr
ease, H+ Concentration in blood increase.

105
(2) central chemoreceptor
106
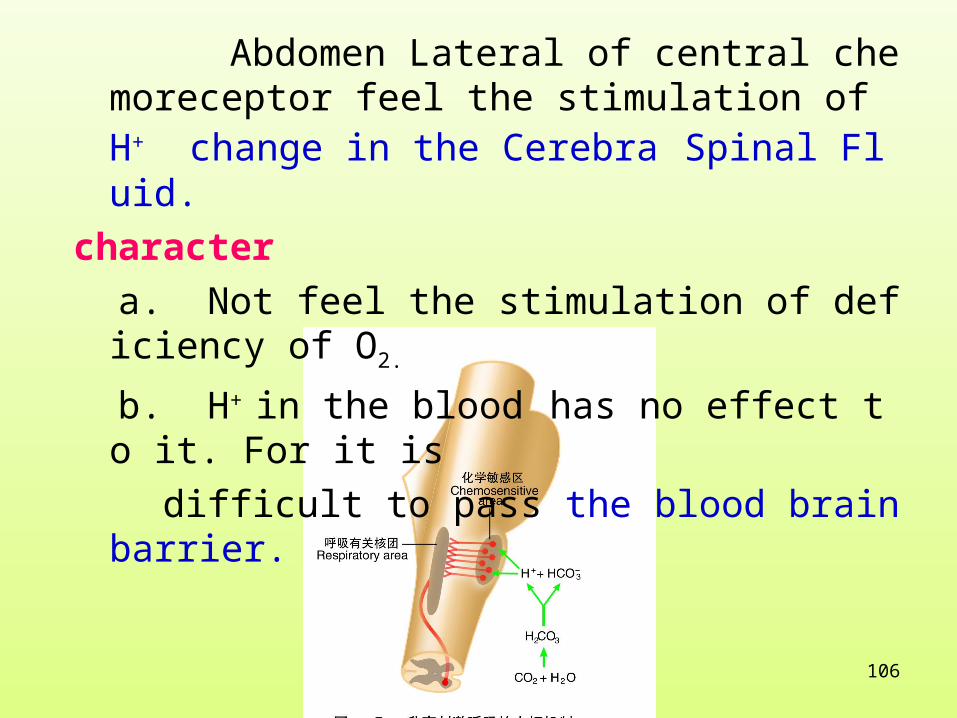
Abdomen Lateral of central chemoreceptor feel the stimulation of H+ change in the Cerebra Spinal Fluid.
character
a. Not feel the stimulation of deficiency of O2.
b. H+ in the blood has no effect to it. For it is
difficult to pass the blood brain barrier.
107
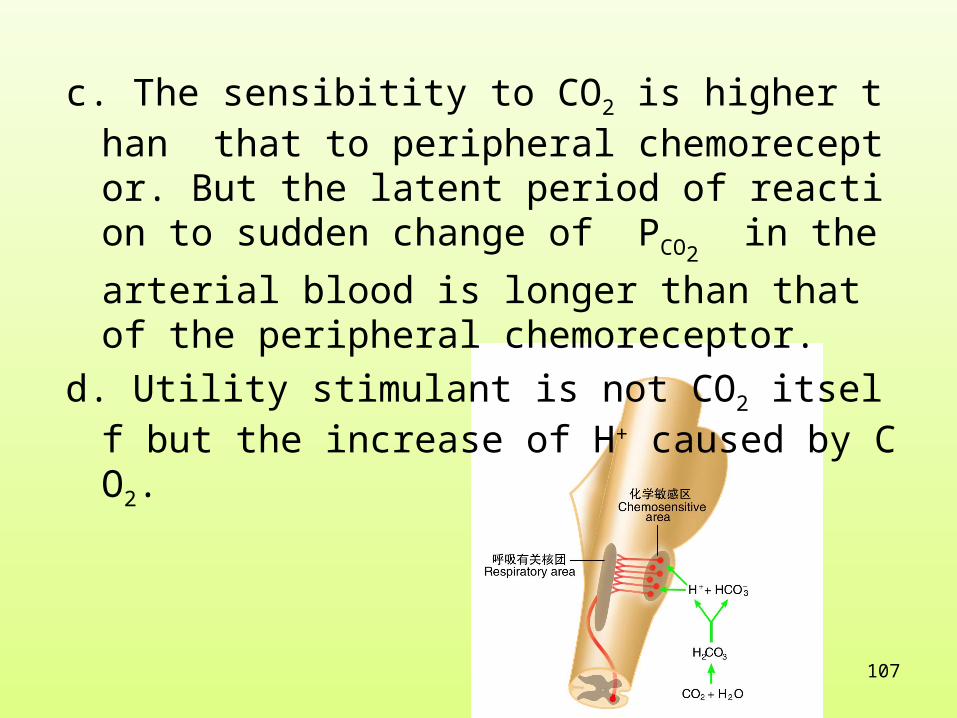
c. The sensibitity to CO2 is higher than that to peripheral chemoreceptor. But the latent period of reaction to sudden change of PCO2
in the arterial blood is longer
than that of the peripheral chemoreceptor.
d. Utility stimulant is not CO2 itself but the increase of H+ caused by CO2.

108
109
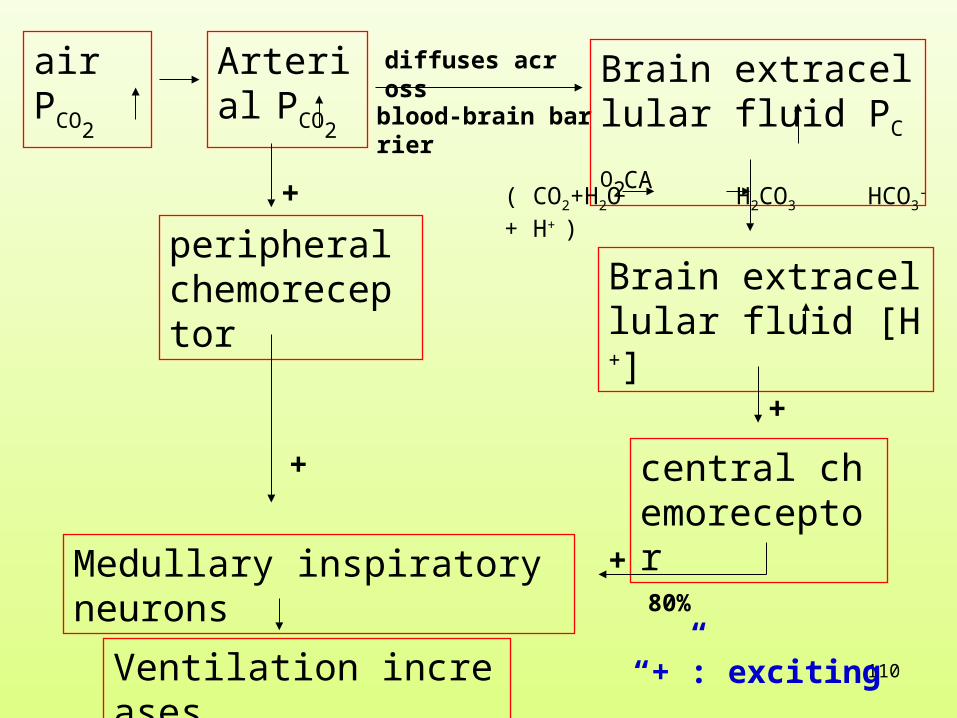
2. Regulation of CO2 、 H+ 、 O2 to respiration( 1 ) Influence of CO2 to respiration
a. Act indirectly to central chemoreceptor(main pathway)
b. Act directly to peripheral chemoreceptor.
The sensibitity of central chemoreceptor to H + is about 25 times of that of peripheral chemoreceptor.
110
air PCO
2
Arterial PCO2
peripheral chemoreceptor
diffuses across
blood-brain barrier
Brain extracellular fluid PCO2
Brain extracellular fluid [H+]
( CO2+H2O H2CO3 HCO3- + H+ )
CA
central chemoreceptor
Medullary inspiratory neurons
Ventilation increases
80%
+
+
+
+
“+”: exciting

111
( 2 ) Effect of O2 to respiration
1 ) character
a. Hypoxia stimulation act through peripheral chemorecep
tor. If the inputing of peripheral chemoreceptor is cut, th
e stimulation effect disappear.
b. The direct effect of hypoxia to center is light inhibition.

112
2 ) The pathway of hypoxia regulating respiration
The main pathway is acting directly on peripheral
chemoreceptor and inputting impulse.respiration ce
nter is excited.
113
( 3 ) Effect of H+ to respiration
1 ) Increasing H+ or decreasing pH can faster respiration.
It is the effective stimulator to chemoreceptor.
2 ) Pathway of H+ regulating respiration
a. H+ in blood increases—excites peripheral chemorecepto
r mainly
b. H+ in Cerebra Spinal Fluid increases-- excites central c
hemoreceptor . Because H+ is very difficult to diffuses
across the blood-brain barrier, so brain extracellular fl
uid [H+] increased very little.

114

115
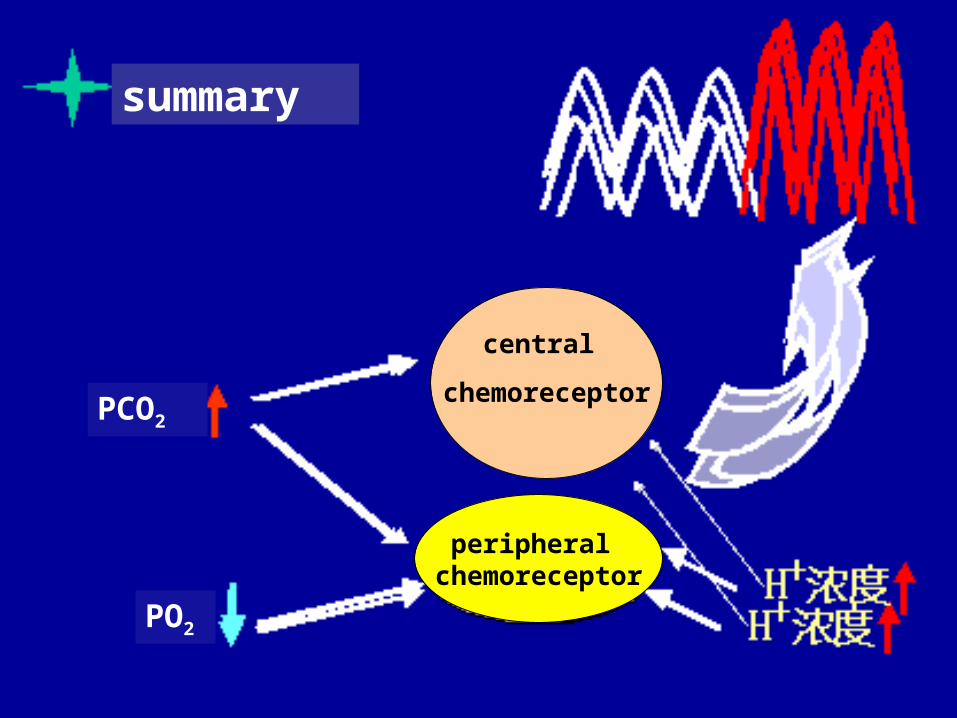
( 4 ) Interface of PCO2 、 H+and PO2 effect respiration
1 ) PCO2 does main role in normal respiration regula
tion.
2 ) When any of the three factor changes ,it can induce the continued change of the other factors.and it can change the respiration effect of the first factor changing .
3 ) Hypoxia and increasing of H+ concentration can strengthen the stimulation effect of PCO2 increasing
to respiration.
116
150 150150
2500
2500 2500150
350
the end of inspiration
the end of exspiration
500150350
inspiration exspiration

117
the alveolar ventilation reaction of changing any of the factors of PCO2
, PO2, PH in Arterial blood but not control
ing the other two factors
118
PCO2
PO2
summary
central
chemoreceptor
peripheral chemoreceptor

119
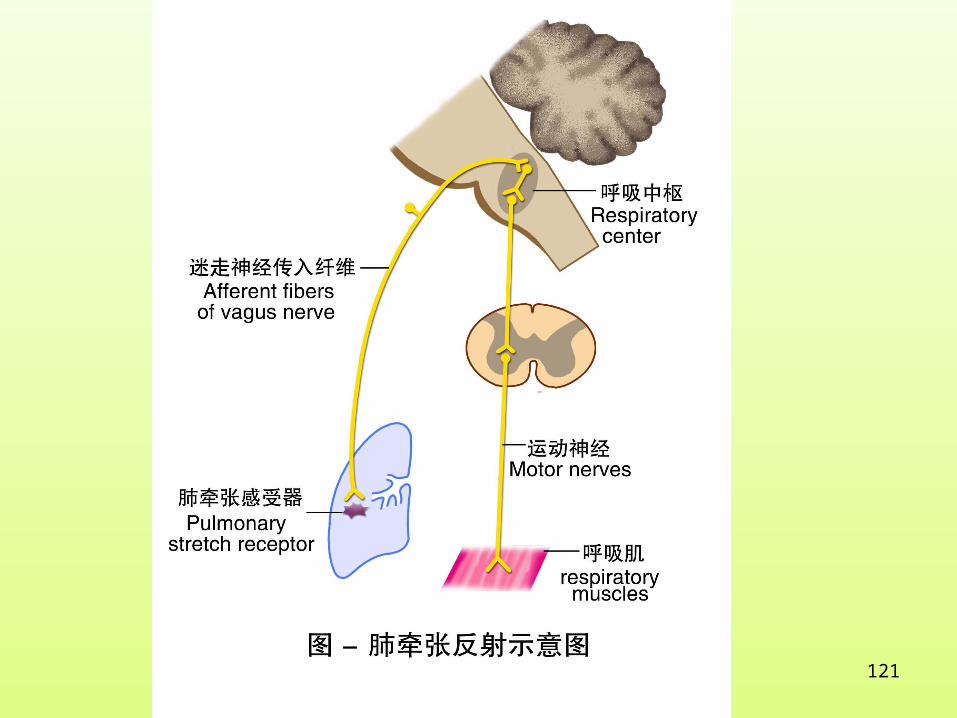
Ⅳ Pulmonary Stretch Reflex
Inflation of the lungs caused inhibition of ins
piration, while collapse of the lungs enhanced in
spiration. This reflex is termed Pulmonary Stret
ch Reflex.

120
reflex
• Reflex arc
stimulation
receptor afferent nerve center efferent nerve effector
response
121
122
Pulmonary Pulmonary
inflation reflex deflation reflex
Part of sensor Smooth muscle of bronchus and bronchiole
Stimulation property dilatate diminish
Effect relax(expiration) Shrink(inspiration)
Significance Urge inspiration urge expiration change
change into expiration into inspiration promptly, promptly,inhibit too deep inhibit too expiration. or too long inspiration.
Related Documents