SSC 2012 Guidelines Nutrition F. Machado, D. Angus • Nutrition – General – Other Copyright 2014 SCCM/ESICM

07_SSC_Nutrition_06_03_14.pptx
Dec 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SSC 2012 Guidelines Nutrition
F. Machado, D. Angus
• Nutrition– General– Other
Copyright 2014 SCCM/ESICM

SSC Nutrition• Extensive literature
– Often not recent– Often small studies with methodological
issues– Often not directly assessing sepsis
• Only four statements included in guidelines– When to start– Amounts to be given– The use of parenteral nutrition– Immunonutrition
Slide 2Copyright 2014 SCCM/ESICM

Nutrition• We suggest administering oral or enteral
feedings, as tolerated, rather than complete fasting or provision of only intravenous glucose within the first 48 hours after a diagnosis of severe sepsis/septic shock (Grade 2C).
Slide 3Copyright 2014 SCCM/ESICM
Marik and Zaloga. Crit Care Med. 2001;29:2264–2270 Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27:355-373
Doig et al. Intensive Care Med. 2009;35:2018–2027
Reviews of Early Feeding
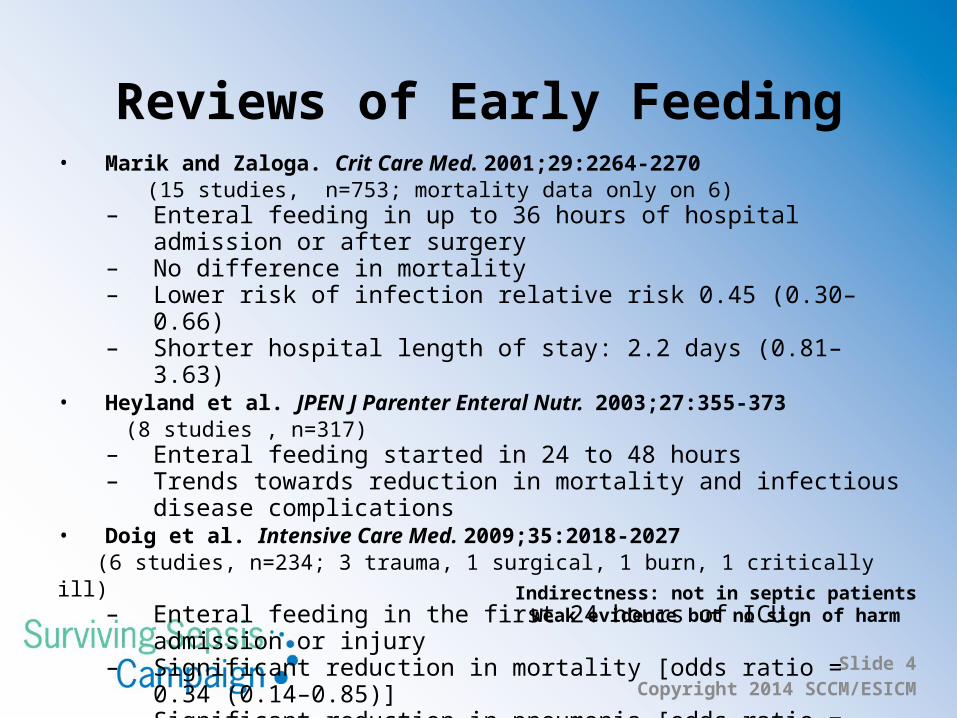
Indirectness: not in septic patientsWeak evidence but no sign of harm
Slide 4Copyright 2014 SCCM/ESICM
• Marik and Zaloga. Crit Care Med. 2001;29:2264-2270 (15 studies, n=753; mortality data only on 6)
– Enteral feeding in up to 36 hours of hospital admission or after surgery– No difference in mortality – Lower risk of infection relative risk 0.45 (0.30–0.66) – Shorter hospital length of stay: 2.2 days (0.81–3.63)
• Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27:355-373 (8 studies , n=317)
– Enteral feeding started in 24 to 48 hours– Trends towards reduction in mortality and infectious disease
complications • Doig et al. Intensive Care Med. 2009;35:2018-2027 (6 studies, n=234; 3 trauma, 1 surgical, 1 burn, 1 critically ill)
– Enteral feeding in the first 24 hours of ICU admission or injury– Significant reduction in mortality [odds ratio = 0.34 (0.14–0.85)] – Significant reduction in pneumonia [odds ratio = 0.31 (0.12–0.78)]

Nutrition• We suggest avoiding mandatory full caloric
feeding in the first week, but rather suggest low-dose feeding (e.g., up to 500 kcal per day), advancing only as tolerated (Grade 2B).
Slide 5Copyright 2014 SCCM/ESICM
Taylor et al. Crit Care Med. 1999;27:2525–2531 Ibrahim et al. JPEN J Parenter Enteral Nutr. 2002;26:174–181
Arabi et al. Am J Clin Nutr. 2011;93:569–577 Rice et al. Crit Care Med. 2011;39:967–974
Rice et al. JAMA. 2012;137:795–803

n= 200
Target Control: 25-30 kcal/kg/day
Trophic feeding : 240-480 kcal/day
Up to day 6
Slide 6Copyright 2014 SCCM/ESICM

• Possible increase in gastrointestinal complications with enhanced feeding
Slide 7Copyright 2014 SCCM/ESICM

JAMA. 2012;137:795–803
Slide 8Copyright 2014 SCCM/ESICM

JAMA. 2012;137:795–803
Slide 9Copyright 2014 SCCM/ESICM

N= 233 Target: permissive 60%-70%; enhanced: 90%-100%
Hospital mortality Underfeeding 30.0% vs. target group 42.5%
Relative risk, 0.71 (0.50, 0.99); P= 0.04Not powered for mortality assessment
Percentage of energy intake requirementsPermissive 60% vs enhanced 71%
Target not achieved in the enhanced group
Slide 10Copyright 2014 SCCM/ESICM

Nutrition• We suggest using intravenous glucose and
enteral nutrition rather than total parenteral nutrition alone or in conjunction with enteral feeding (Grade 2B).
Slide 11Copyright 2014 SCCM/ESICM
Braunschweig et al. Am J Clin Nutr. 2001;74:534–542 Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27:355–373
Gramlich et al. Nutrition. 2004;20:843–848 Dhaliwal et al. Intensive Care Med. 2004;30:1666–1671
Peter et al. Crit Care Med. 2005; 33:213–220 Simpson and Doig. Intensive Care Med. 2005;31:12–23
Casaer et al. N Engl J Med. 2011;365:506–517

N = 4640Early parenteral nutrition: within 48 hours of ICU admission
Late parenteral nutrition: on day 8
Slide 12Copyright 2014 SCCM/ESICM

Slide 13Copyright 2014 SCCM/ESICM

Nutrition• We suggest using nutrition with no specific
immunomodulating supplementation in patients with severe sepsis (Grade 2C).
Slide 14Copyright 2014 SCCM/ESICM
Arginine• Arginine should not be used• Can lead to unwanted vasodilation,
hypotension, and enhanced inflammation• Only small and underpowered studies
reported
Slide 15Copyright 2014 SCCM/ESICM
Bower et al. Crit Care Med. 1995;23:436–449. Galbán et al. Crit Care Med. 2000;28:643–648.
Caparrós et al. JPEN J Parenter Enteral Nutr. 2001;25:299–308 Preiser et al. JPEN J Parenter Enteral Nutr. 2001;25:182–18

Glutamine• Glutamine should not be used • No impact on mortality • Some positive secondary outcomes
(reduction in infections and organ dysfunction)
Slide 16Copyright 2014 SCCM/ESICM
– Meta-analyses• Heyland et al. JPEN. 2003;27:355• Jian et al. Zhonghua Shao Shang Za
Zhi. 2009;25:325• Avenell A et al. Proc Nutr Soc.
2006;65:236• Avenell A et al. Proc Nutr Soc.
2009;68:261• Novak et al. Crit Care Med.
2002;30:2022
– Single Studies• Fuentes-Orozco et al. Clin Nutr.
2004;23:13• Beale et al. Crit Care Med.
2008;36:131• Grau et al. Crit Care Med.
2011;39:1263• Wernerman et al. Acta Anaesthesiol
Scand. 2011;55:812• Andrews et al. BMJ. 2011;342:d1542

Glutamine-supplemented parenteral or enteral nutrition in critically ill patients No effect on mortality
Slide 17Copyright 2014 SCCM/ESICM

Slide 18Copyright 2014 SCCM/ESICM

After guidelines were published …
Slide 19Copyright 2014 SCCM/ESICM
Omega-3 Fatty Acids
Slide 20Copyright 2014 SCCM/ESICM
• Omega-3 fatty acids should not be used• Previous studies showing benefit used omega-6
enriched diets in the control arms– Pontes-Arruda et al. Crit Care Med. 2006;34:2325– Gadek et al. Crit Care Med. 1999;27:1409– Singer et al. Crit Care Med. 2006;34:1033
• More recent studies showed no benefit and possible harm– Friesecke et al. Intensive
Care Med. 2008;34:1411– Barbosa et al. Crit Care.
2010;14:R5– Gupta et al. Indian J Crit
Care Med. 2011;15:108
– Rice et al. JAMA. 2011; 306:1574
– Stapleton et al. Crit Care Med. 2011;39:1655
– Grau-Carmona et al. Clin Nutr. 2011;30:578

60-day hospital mortality: 26.6% vs. 16.3%, P=.054
JAMA. 2011;306:1574–1581
75% with sepsis or pneumonia
Slide 21Copyright 2014 SCCM/ESICM
Summary• SSC guidelines
– Generally supportive of minimal nutritional intervention during initial ICU stay• Statements largely suggestions, rather
than recommendations• Lack of large, robust, targeted
randomized controlled trials
Slide 22Copyright 2014 SCCM/ESICM
Related Documents

![[MS-PPTX]: PowerPoint (.pptx) Extensions to the Office ...MS-PPTX].pdfPowerPoint (.pptx) Extensions to the Office Open XML File FormatFile Size: 4MBPage Count: 145](https://static.cupdf.com/doc/110x72/5ed5954ddb0f8b20f04b0446/ms-pptx-powerpoint-pptx-extensions-to-the-office-ms-pptxpdf-powerpoint.jpg)
![钱币.pptx [Autosaved].pptx](https://static.cupdf.com/doc/110x72/55cf91bf550346f57b905058/pptx-autosavedpptx.jpg)
![[MS-PPTX]: PowerPoint (.pptx) Extensions to the Office ...MS-PPTX].pdf · [MS-PPTX]: PowerPoint (.pptx) Extensions to the Office Open XML File Format ... PowerPoint (.pptx) Extensions](https://static.cupdf.com/doc/110x72/5ae7f6357f8b9a6d4f8ed3a1/ms-pptx-powerpoint-pptx-extensions-to-the-office-ms-pptxpdfms-pptx.jpg)
![[MS-PPTX]: PowerPoint (.pptx) Extensions to the Office ...interoperability.blob.core.windows.net/files/MS-PPTX/[MS-PPTX... · 1 / 76 [MS-PPTX] — v20140428 PowerPoint (.pptx) Extensions](https://static.cupdf.com/doc/110x72/5ae7f6357f8b9a6d4f8ed3b3/ms-pptx-powerpoint-pptx-extensions-to-the-office-ms-pptx1-76-ms-pptx.jpg)

![ID 1 SESSION 4.pptx [Autoguardado].pptx](https://static.cupdf.com/doc/110x72/55cf8c675503462b138c00e6/id-1-session-4pptx-autoguardadopptx.jpg)

![Fundamentos de investigación1.pptx [Autoguardado].pptx](https://static.cupdf.com/doc/110x72/56d6bd6c1a28ab30168deddb/fundamentos-de-investigacion1pptx-autoguardadopptx.jpg)
