1 Terlipressin /Medical Management in Hepatorenal Syndrome Akash Deep, Director - PICU King’s College Hospital London

00 Terlipressin /Medical Management in Hepatorenal Syndrome Akash Deep, Director - PICU King’s College Hospital London.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

11
Terlipressin /Medical Management in
Hepatorenal Syndrome
Akash Deep, Director - PICU
King’s College Hospital London


HRS in children
• No literature on HRS in children exists
• All evidence extracted from adult literature.
3

Prevention - Potential targets
• Portal Hypertension• Bacterial translocation • Splanchnic vasodilators and
mediators –TNF- alpha• Raised IAP• Iatrogenic factors

Prevention
• Norfloxacin: Ascitic protein < 15g/L, Bilirubin > 50 + Crea > 106 µmol/L or Na < 130 mmol/L, CPC >10
• Daily norfloxacin was associated with lower 1-year SBP probability (7% compared with 61%)and lower 1-year HRS probability.

Prevention with Pentoxifylline –anti TNF-alpha
Mortality– 12/49 (24.5%) PTX – 24/52 (46.1%) – p=0.036
HRS as cause of death– 6/12 (50%) PTX vs – 22/24 (91.7%) – p=0.009
E Akriviadas Gastroenterology 2000; 119 : 1637; 119 : 1637
Pentoxifylline
Placebo
nonsurvivors
survivors
Survival : Age, creatinine level on randomization, and treatment with PTX
Pentoxifylline

Prevention • Avoid intravascular volume depletion & maintain an
effective circulating volumeo Gastrointestinal bleedingo Diureticso Diarrheao Large-volume paracentesis without adequate volume
repletion• Prompt diagnosis and treatment of infections (peritonitis,
sepsis)• Bleeding and associated management• Temporary omission of nephrotoxic drugs together with
appropriate adjustment of drug doses for the eGFR.
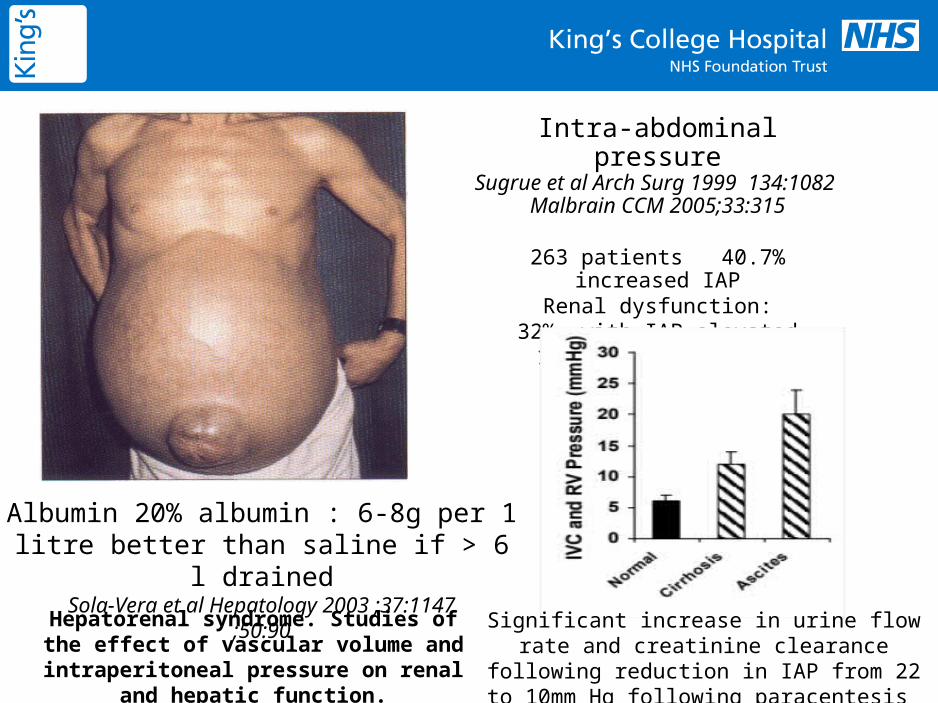
Intra-abdominal pressureSugrue et al Arch Surg 1999 134:1082
Malbrain CCM 2005;33:315
263 patients 40.7% increased IAPRenal dysfunction:
32% with IAP elevated14% with normal IAP
Albumin 20% albumin : 6-8g per 1 litre better than saline if > 6 l drained
Sola-Vera et al Hepatology 2003 ;37:1147;50:90
Hepatorenal syndrome. Studies of the effect of vascular volume and intraperitoneal pressure on renal and hepatic function.
Significant increase in urine flow rate and creatinine clearance following reduction in IAP from 22 to 10mm Hg following paracentesis

Albumin
9
Antioxidant effects and/or its high capacity to bind toxic substances

Stick to basics

Treatment - General
Treat associated conditions1.GI bleeding / hypovolaemia ( Surviving
Sepsis guidelines, measurement of haemodynamics, problems associated with IAP )
2.Infection3.Diuretics / nephrotoxic drugs4.Large volume ascites - TIPS / paracentesis5.Adrenal insufficiency.

Goals of treatment • Assessment for OLT should start early
– HRS -1 realistic expectations, HRS-2 case by case
• Prolong survival until a liver transplant becomes available and to optimize conditions for successful liver transplantation.
12
Treatment• Vasoconstrictor therapy + “Albumin”
survival versus live longer• RRT in non responders especially if
OLT considered – no head to head comparison
• Target portal hypertension -TIPS• MARS no evidence of benefit• OLT.

Vasoconstrictors to improve circulatory function:• Vasopressin analogueso Ornipressin- improvement of renal function but limited by
ischemic complicationso Terlipressin - lesser incidence of ischemia
• Midodrineo alpha-agonist, systemic vasoconstrictor
• Noradrenaline o alpha-agonist, systemic vasoconstrictor
• Octreotideo analogue of somatostatin, inhibitor of vasodilation.
Treatment

Vasopressin 8-Arginine Vasopressin- Synthesised as a pro-
hormone in the paraventricular and supra-optic nuclei of the hypothalamus
Migrates and stored in pars nervosa of the posterior pituitary
Vasopressin is a direct systemic vasoconstrictor (mediated by V1 receptors)
Osmoregulation and maintenance of normovolaemia (mediated by renal V2 receptors)
It also maintains haemostasis, plays a role in temperature regulation Plasma half life of vasopressin is 24 min

V2
V1a
V1b
Functional coupling
ATP
cAMPH
R s AC
PIP2
IP3, Ca2+
DAG, PKCH
R q/11 PLC
Asn5
NH2Arg8
Gly9
Pro7
Cys6
Cys1
Gln4
Phe3
Tyr2
SS
Vasopressin : Natural compound

Asn5
NH2Arg8
Gly9
Pro7
Cys6
Cys1
Gln4
Phe3
Tyr2
SS
Gly9
Gly9
Gly9
Asn5
NH2Lys8 Gly9
Pro7
Cys6
Cys1
Gln4
Phe3
Tyr2
SS
AVPAsn5
NH2Lys8 Gly9
Pro7
Cys6
Cys1
Gln4
Phe3
Tyr2
SS
LVP
Terlipressin
Vasopressin: Synthetic compounds

Pharmacology of Terlipressin• Prodrug - converted to its active form lysine
vasopressin - ‘slow release’ of the vasoactive lysine vasopressin
• Half–life - 6 hrs• Bolus dosage 1-2 mg 4-6 hourly ( some centres
use infusion – no real benefit over boluses)• Elimination half-life - 50 min • Maximum serum concentration occurs after 120
min• Degradation by endo and exopeptidases (1%
through kidneys).18
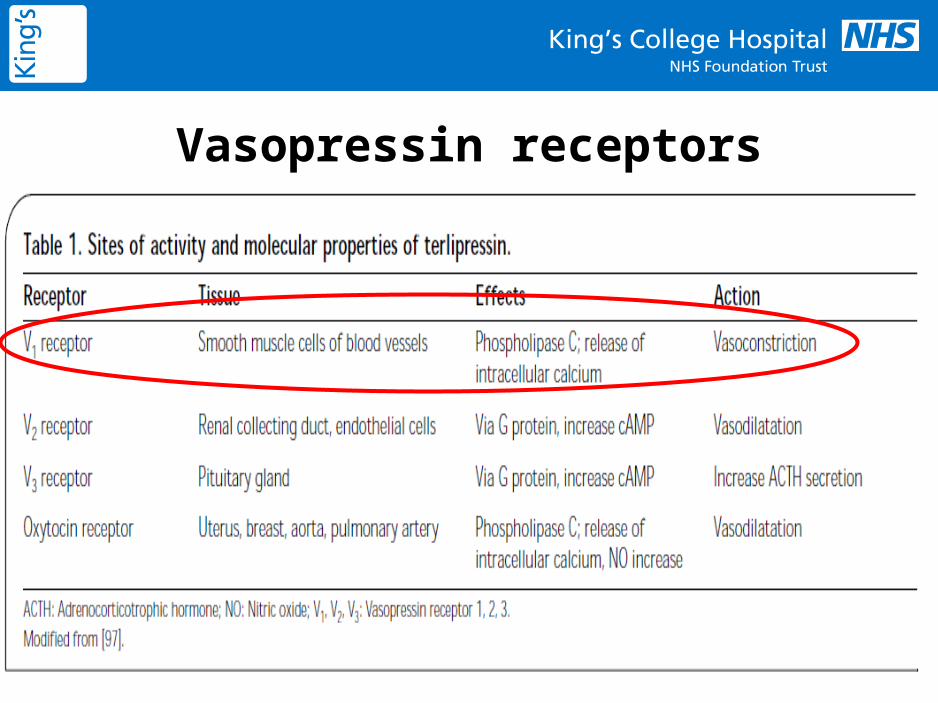
Vasopressin receptors

Action of Terlipressin
20

Pathophysiology of CLD
Peripheral and splanchnic arterial dilatation
Reduced effective blood volume
Activation of renin-angiotensin-aldosterone systemSympathetic nervous system
ADH
Na retention &
Water retentionLow urinary Na
Dilutional hyponatraemia
AscitesSchrier et al Hepatol 1988
Plasma volume expansion
Renal vasoconstrictionReduced GFR
Ascites and OedemaHRS
Portal Hypertension
Vasopressin/
Terlipressin Increased blood volume
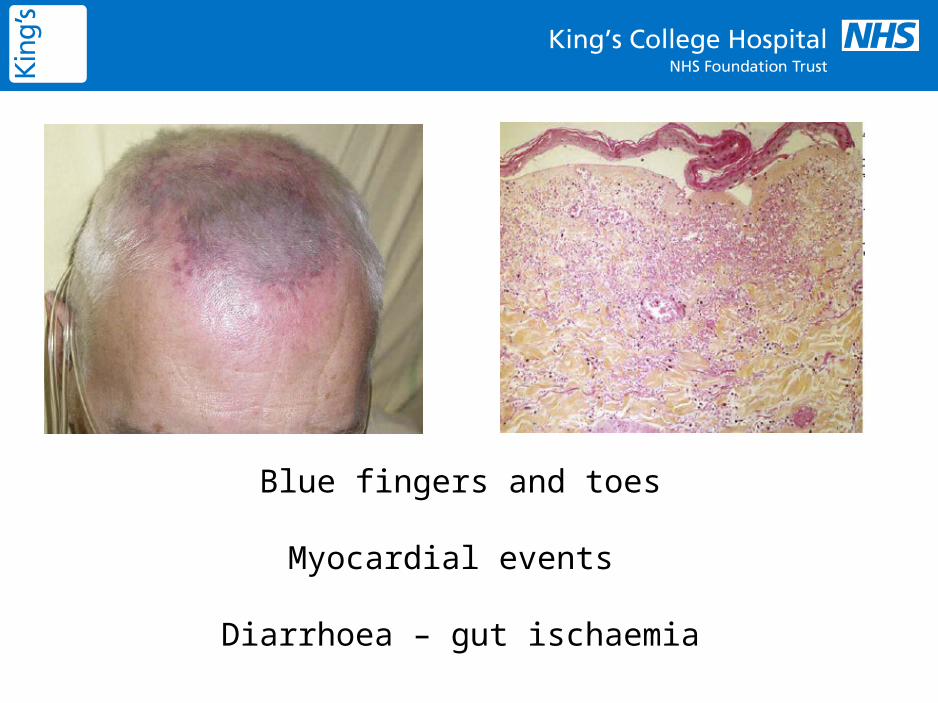
Blue fingers and toes
Myocardial events
Diarrhoea – gut ischaemia


Vasopressin : Gut ischaemia

Terlipresin +Albumin vs
Albumin
25

RCT Terlipressin in Type I HRSSanyal A Gatroenterology 2008 :134:1360
1 mg 6 hrly vs placeboAlbumin in both groupsIf no response (30% decrease in creat) at day 4- dose doubled to 2mg 6 hrly14 days Rx : 56 in each grpSuccess defined as creatinine < 1.5 mg/dl for 48 hrs by Day 14Rx success : 34 vs 12.5 %
Best Predictor – Low baseline Serum creatinine
Similar survival between grps
HRS reversal improved180 day outcome

Sanyal A Gatroenterology 2008 :134:1360

• 1-2 mg 4hrly• Albumin daily 1g/kg• N=23 each group• Primary outcome-Renal function & survival• Improved renal function 43 vs 8%• No difference in 2 month survival • Predictors of response – Baseline creat,
treatment with terlipressin +albumin
Terlipressin and albumin vs albuminMartin-Llahi M Gastroenterology 2008:134

Previous studies CP score 11
Martin-Llahi M Gastroenterology 2008:134

• Six randomised trials were eligible for inclusion• 3 trials (total 51 patients) assessed terlipressin 1 mg bd for 2 to 15 days • Co-interventions included albumin, fresh frozen plasma, and cimetidine
• Terlipressin reduced mortality rates by 34% • The control group mortality rate was 65%
• Terlipressin improved renal function assessed by creatinine clearance, serum creatinine and urine output.
2009

Conclusion• Terlipressin appears to have an
independent beneficial effect on HRS reversal.
• Best response in those with low baseline serum creatinine
• HRS at transplantation – high morbidity and mortality
• Though no survival benefit, improved renal function improved post transplant outcomes.
31

• Do all patients treated with terlipressin respond ? 52% HRS respond to terlipressin
(Meta-analysis: terlipressin therapy for the hepatorenal syndrome F. Fabrizi, V. Dixit & P. Martin APT 2006 24:935-44 )
• If not, can we identify those who will not respond ?
• Side effect profile, implications for transplantation and development of new therapies.
32

Best response - SCr <3.0 mg/dl Highest baseline serum creatinine in a terlipressin responder - 5.6 mg/dl.
No response – SCr > 7mg/dlWill there be a response in advanced disease ?????
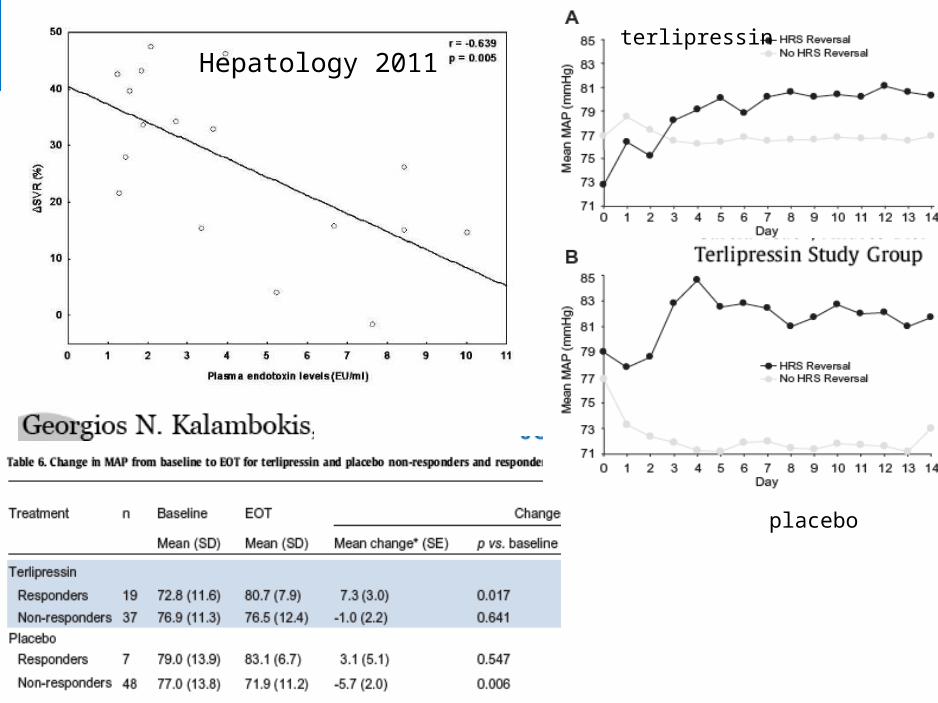
terlipressin
placebo
Hepatology 2011

Predictors of response to Terlipressin

Conclusions• Best response - SCr < 3 mg/dl or 3-5
mg/dl• Poor response - SCr > 7 Mg/dl• If no response by Day 4 - NO
response thereafter• Sustained rise in MAP rather than
only initial rise required for response• Therefore start treatment early!!!
36

37
Reversal of HRS with Terlipressin

Survival outcome with Terlipressin
38

Duvoux et al. Hepatology 2002
NA 0.5-3mg/hMAP >100mmHg increaase
or U.O >50ml/h
0
100
200
300
400
500
600
700
Day 0 Day 5 Day 10
Se
r. C
rea
t (u
mo
les
/l)
Norepinephrine for the treatment of HRS ?
HRS reversal -83% Almost all respond – Day 5
40
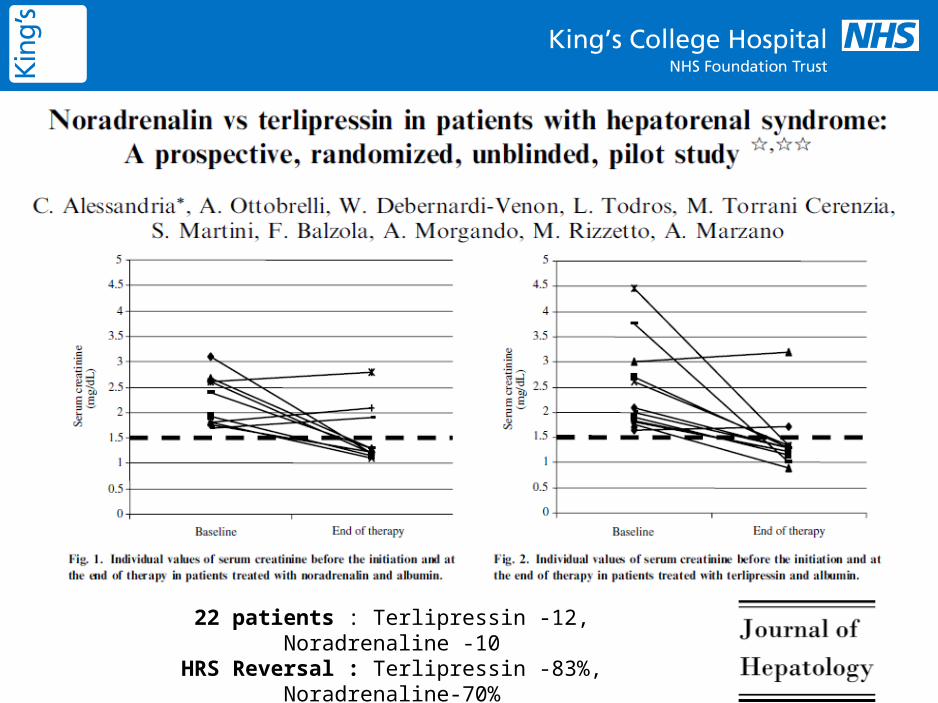
22 patients : Terlipressin -12, Noradrenaline -10HRS Reversal : Terlipressin -83%, Noradrenaline-70%

41
Cost of noradrenaline 15 times << terlipressin82 % nor-ad responders – Transplant
80% terlipressin responders – Transplant80% Non-responders - DEATH
Noradrenalin is as effective and safe as terlipressin in patients with HRS.

Is there a single best vasoconstrictor ?
NO ADVANTAGE OF ONE VASOCONSTRICTOR OVER OTHER
43
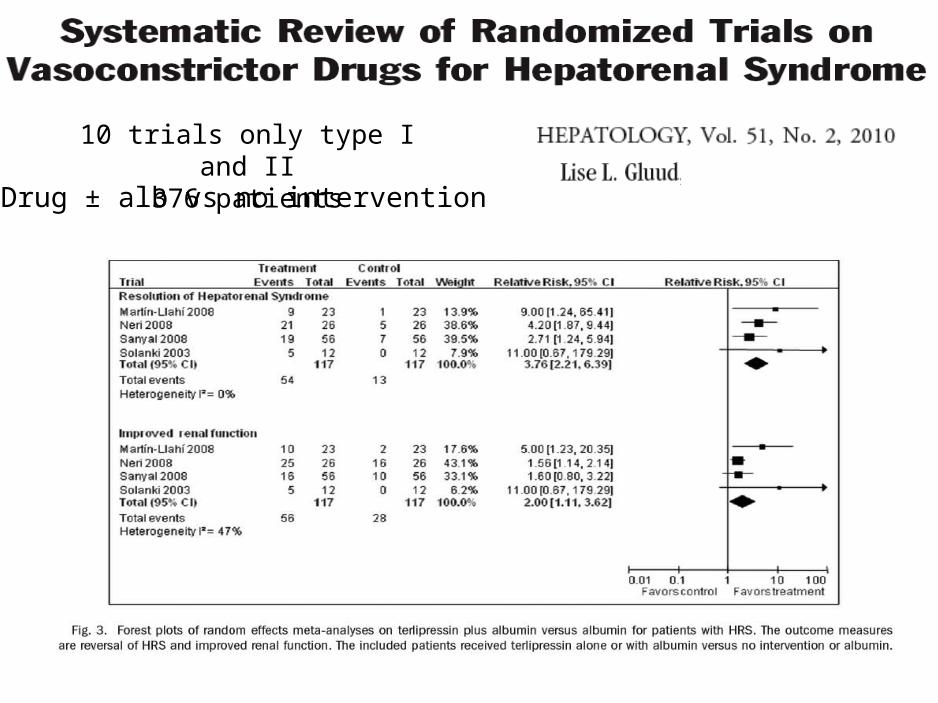
10 trials only type I and II376 patients
Drug ± alb vs no intervention

Vasoconstrictors + Alb : Effect on mortality at 15 days but not at 30, 90 or 180 days RR 0.6 (0.37-0.97)
Terlipressin + Albumin vs Albumin : decreased mortality in type IRR 0.83 (0.65-1.05)
Terlipressin + Albumin vs Albumin

Comparative costs
46
Drug Strength Presentation
Cost Cost/unit
Terlipressin 1mg 1 x 5 vial £69.95 £13.99/ 1mg vial
Vasopressin 20units/ml (2ml)
1 x 10 (2ml amps)
£320.50 £32.50/ vial (40units/2ml)
Vasopressin 20units/ml (1ml)
1 x 25 (1ml amps)
£133 £5.32/ vial (20units/ml)
Noradrenaline 1:1000 (2ml) 1 x 5 (2ml amp)
£9.50 £1.90/vial (2ml)
Noradrenaline 1:1000 (4ml) 1 x 10( 4ml amp)
£19 £1.90/vial (4ml)
Noradrenaline 1:1000 (8ml) 1 x 10 (8ml amp)
£45 £4.50/vial (8ml)

Other treatments
• TIPS – Transjugular Intrahepatic porto-systemic shunts
• Renal Replacement therapy – Volume overload, intractable metabolic acidosis, and hyperkalemia - CRRT/MARS
• Liver Transplantation ( Not all recover kidney function)
• Combined Liver-kidney Transplantation.
47

Comparison of various treatments

What is my management strategy for HRS?
• Differentiate between natural progression of liver disease with its complications versus acute deterioration of kidney function – HRS-1 or AKI
• Fluid resuscitation• Treat raised IAP(Drain and replace with albumin)• Aggressive antibiotics (cephalosporins)• Recognise and treat precipitating factors• Once in ICU – Cardiac output monitoring, fluids,
full organ support, prioritise transplant listing• Early vasoconstrictors
HRS at KCH• Start with noradrenaline, if no response at 0.5
mcg/kg/min , add terlipressin 1mg 6 hourly • Monitor ischaemic side effects• Steroids for adrenal suppression• If no response by day 3 , double terlipressin
2mg• No response Day -5 stop terlipressin• RRT – fluid oveload, high lactate, acidosis• Temporary delisting if progressive MOF
50

Conclusion• HRS often diagnosed - rarely present• Poor prognosis• Prevent infections, raised
IAP(paracentesis) and iatrogenic factors• Treat associated complications rapidly
51
Unanswered questions• Does HRS relapse after stopping
terlipressin ?
• When do you prioritise and at what point should one be denied transplant ?
• Can prolonged vasoconstrictors be used as bridge to transplant?

Acknowledgements
• Jules Wendon and George Auzinger
• Tim and Stuart
• CRRT Working Group at King’s
53
Related Documents











