S It’s a Water Problem Sodium Emergencies Julia Creider, PGY4 Endocrine

It’s a Water Problem Sodium Emergencies Julia Creider, PGY4 Endocrine.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

S
It’s a Water ProblemSodium Emergencies
Julia Creider, PGY4 Endocrine
Objectives
Overview of sodium and water regulation
Understand the clinical manifestations, diagnosis, and causes of hypo- and hypernatremia
Review the management of hypo- and hypernatremia based on underlying cause

The Players: Water
Most abundant constituent in the body
50% of body weight in women, 60% in men
Two main compartments: Intracellular fluid (ICF), 55-75% Extracellular fluid (ECF), 25-45%
Intravascular Extravascular

The Players: Water
Osmolality = solute or particle concentration of a fluid (mosmol/kg)
Water easily diffuses across cell membranes to achieve osmotic equilibrium (ECF = ICF)
Main solutes of these compartments differ: ECF = Na+
ICF = K+
Determinant of the effective osmolality due to being restricted to their respective compartments
The Players: Sodium
Na+ is actively pumped out of cells by the Na+, K+-ATPase membrane pump
85-90% of body Na+ is extracellular
Hence, predominant ion in ECF and major determinant of ECF osmolality and volume
Regulation System: Antidiuretic Hormone
(ADH)
Peptide hormone consisting of a 6 amino acid ring with a cysteine to cysteine bridge and 3 amino acid tail
Synthesized as part of a precursor molecule consisting of a nonapeptide, a hormone-specific neurophysin, and an additional glycopeptide
Packaged in neurosecretory granules
Cleaved to the products during transport to posterior pituitary

Regulation System: Antidiuretic Hormone
(ADH) Main hormone involved in the regulation of water
homeostasis and osmolality
Half life in the circulation is 10-20min
Stimulation of release Increases in plasma osmolality Reductions in plasma volume

Regulation System: Antidiuretic Hormone
(ADH)

Regulation System: Antidiuretic Hormone
(ADH)
Regulation System: Antidiuretic Hormone
(ADH)
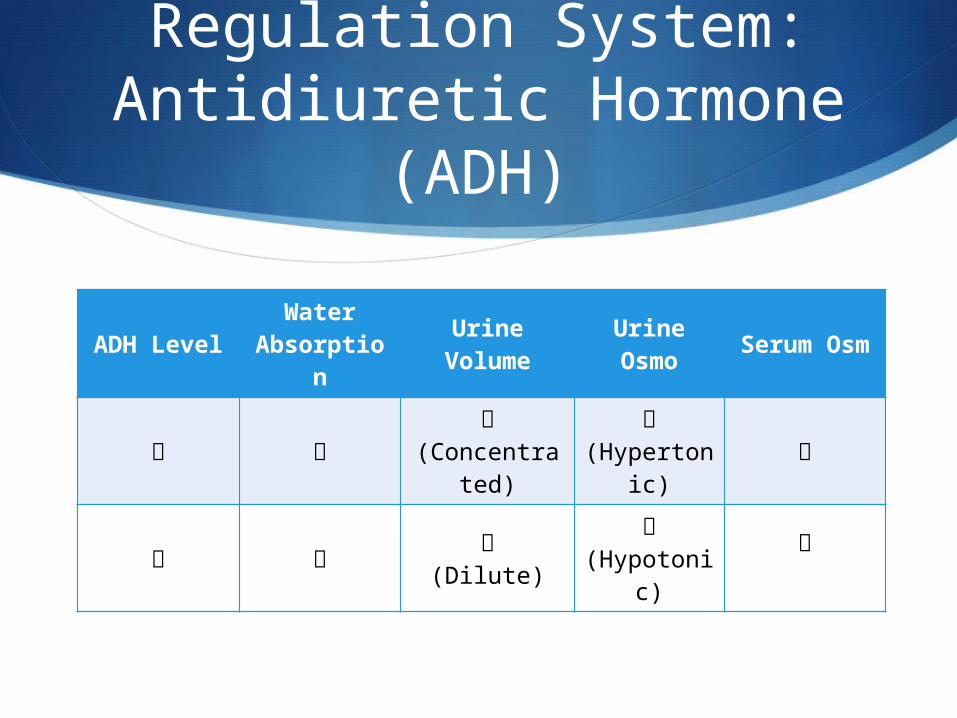
ADH LevelWater
Absorption
Urine Volume
Urine Osmo
Serum Osm
(Concentrated)
(Hypertoni
c)
(Dilute)
(Hypotoni
c)
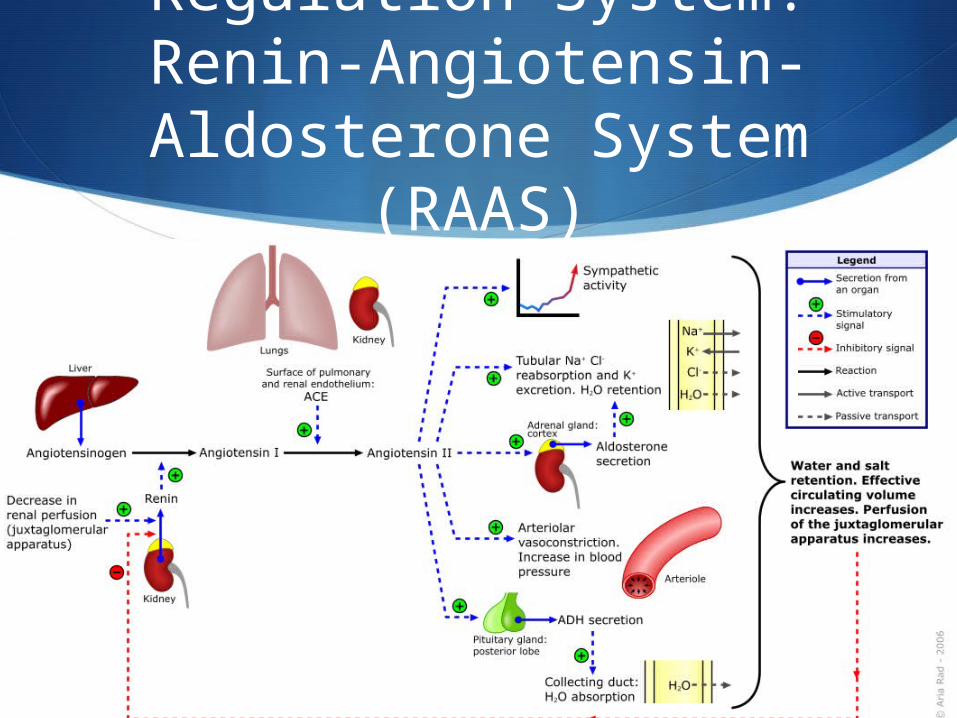
Regulation System: Renin-Angiotensin-Aldosterone
System (RAAS)
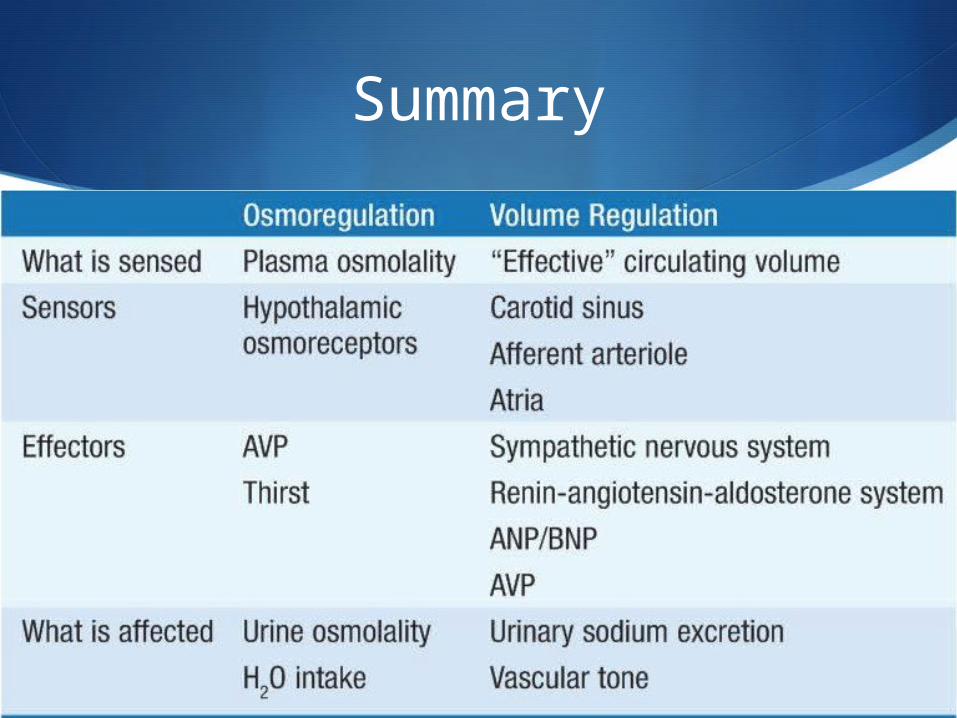
Summary

Case
32F from home
Admitted to Neurology with decreased LOC and increase in frequency of seizures
Past Medical History: Glioblastoma, unresectable Seizures
Meds: Lamotrigine Etoposide

Case
Initial Investigations: Na+ 130 MRI – slight increase in size of tumor and increased edema EEG – + seizure activity
Initial Management: Neuro Observation Dilantin loaded Dexamethasone started for edema Due to decrease LOC and inability to eat, IV changed to
D5W/0.45NS

Case
End of the day: Patient condition not improving Team decides to recheck Na+
On call: Na+ 110
Hyponatremia: Definition
Plasma Na+ < 135 mmol
Very common, up to 30% of hospitalized patients
Disorder of water balance
Relative excess of body water compared to total body Na+
Usually associated with disturbance in ADH
Acute < 48hr
Chronic > 48hr
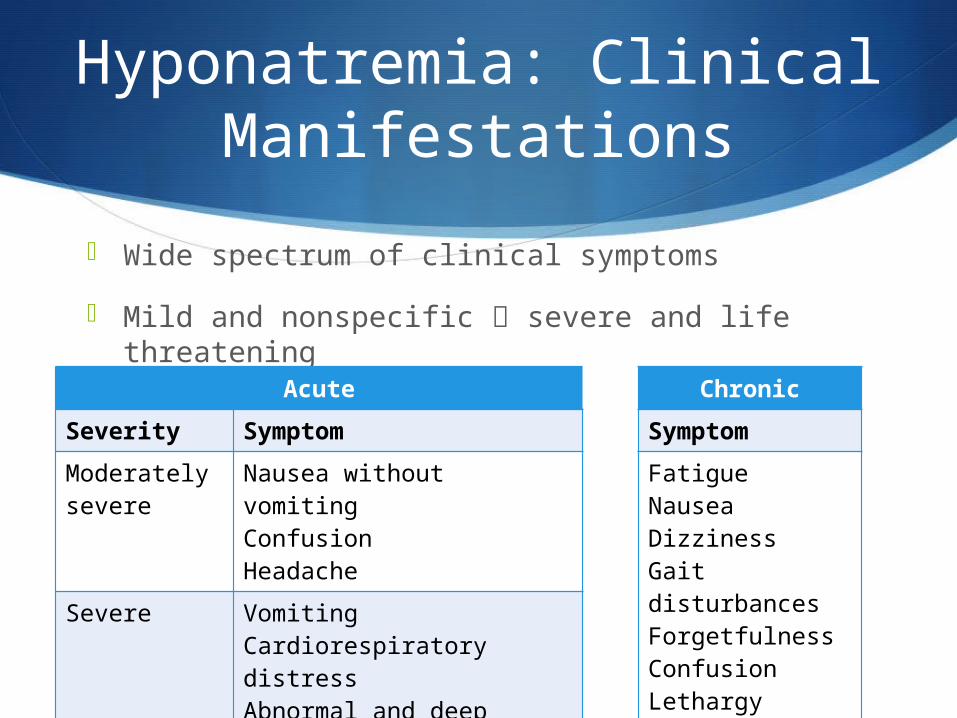
Hyponatremia: Clinical Manifestations
Wide spectrum of clinical symptoms
Mild and nonspecific severe and life threatening
Acute
Severity Symptom
Moderately severe
Nausea without vomitingConfusionHeadache
Severe VomitingCardiorespiratory distressAbnormal and deep somnolenceSeizuresComa
Chronic
Symptom
FatigueNauseaDizzinessGait disturbancesForgetfulnessConfusionLethargyMuscle crampsFractures
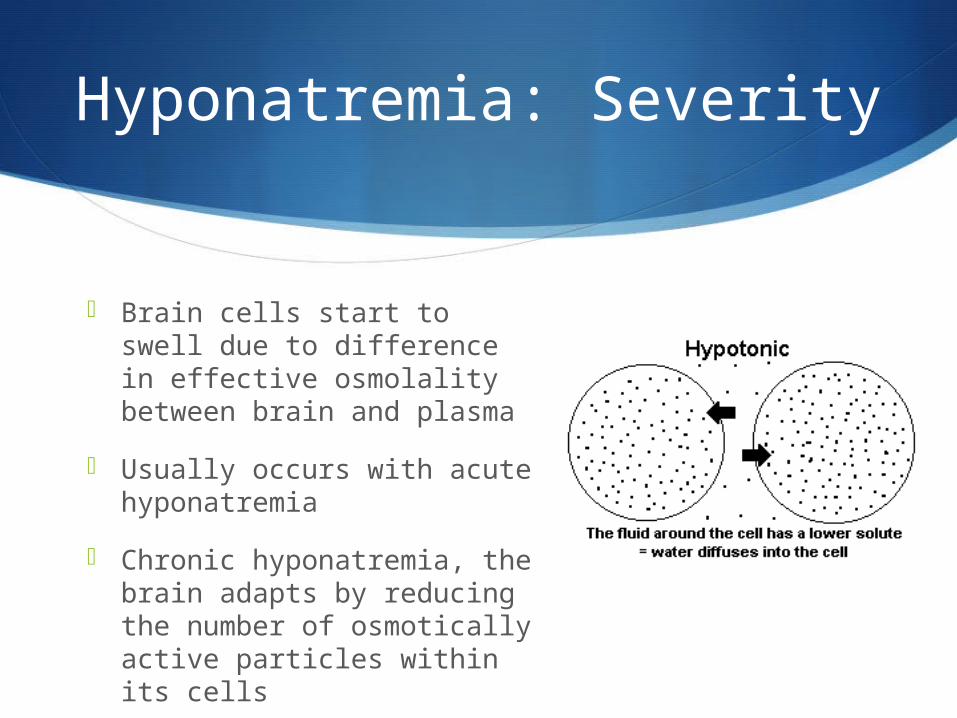
Hyponatremia: Severity
Brain cells start to swell due to difference in effective osmolality between brain and plasma
Usually occurs with acute hyponatremia
Chronic hyponatremia, the brain adapts by reducing the number of osmotically active particles within its cells
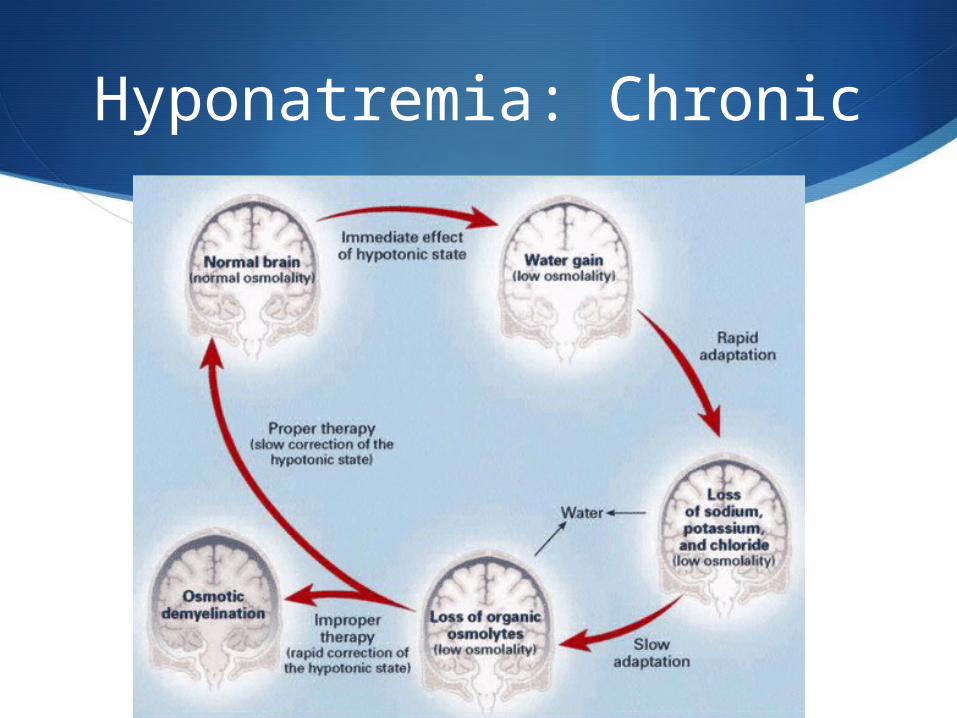
Hyponatremia: Chronic
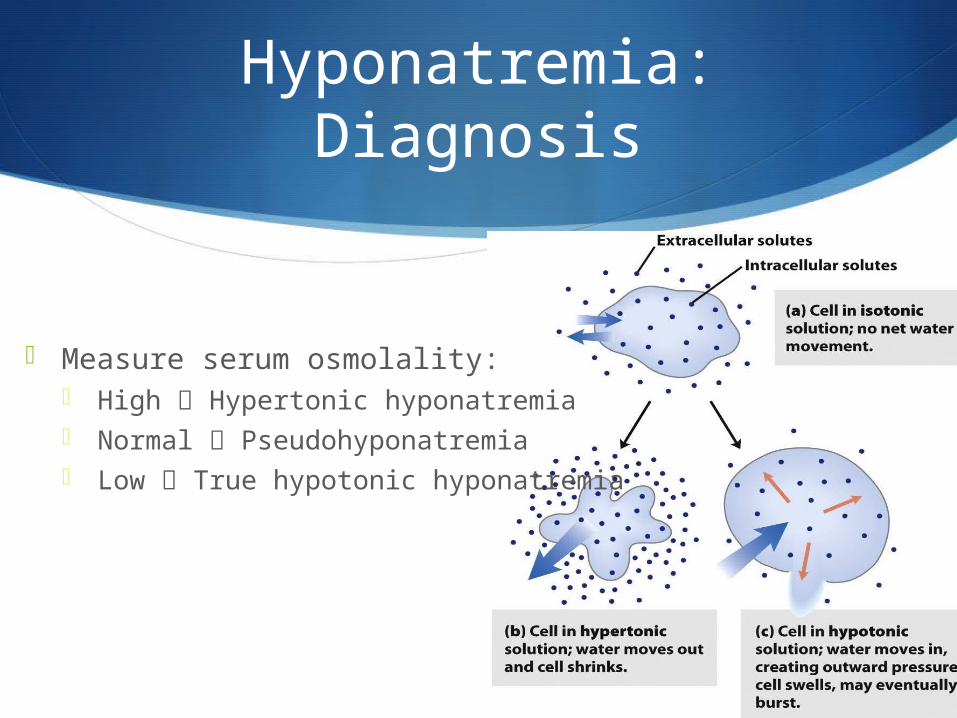
Hyponatremia: Diagnosis
Measure serum osmolality: High Hypertonic hyponatremia Normal Pseudohyponatremia Low True hypotonic hyponatremia

Hyponatremia: Diagnosis
Hypertonic hyponatremia occurs when the serum contains additional osmoles that increase the effective osmolality
Reduces the serum Na+ concentration by attracting water from the intracellular compartment
Causes Hyperglycemia Mannitol administration Glycine Sorbitol
Hyponatremia: Diagnosis
Pseudohyponatremia is a laboratory artifact
Occurs when abnormally high concentrations of lipids or proteins in the blood interfere with the accurate measurement of Na+
Causes: Hyperlipidemia or hyperproteinemia

Hyponatremia: Diagnosis

Hyponatremia: Diagnosis
Hypotonic hyponatremia
Assess volume status Vital signs Orthostatic vitals JVP Skin turgor Mucous membranes Peripheral edema
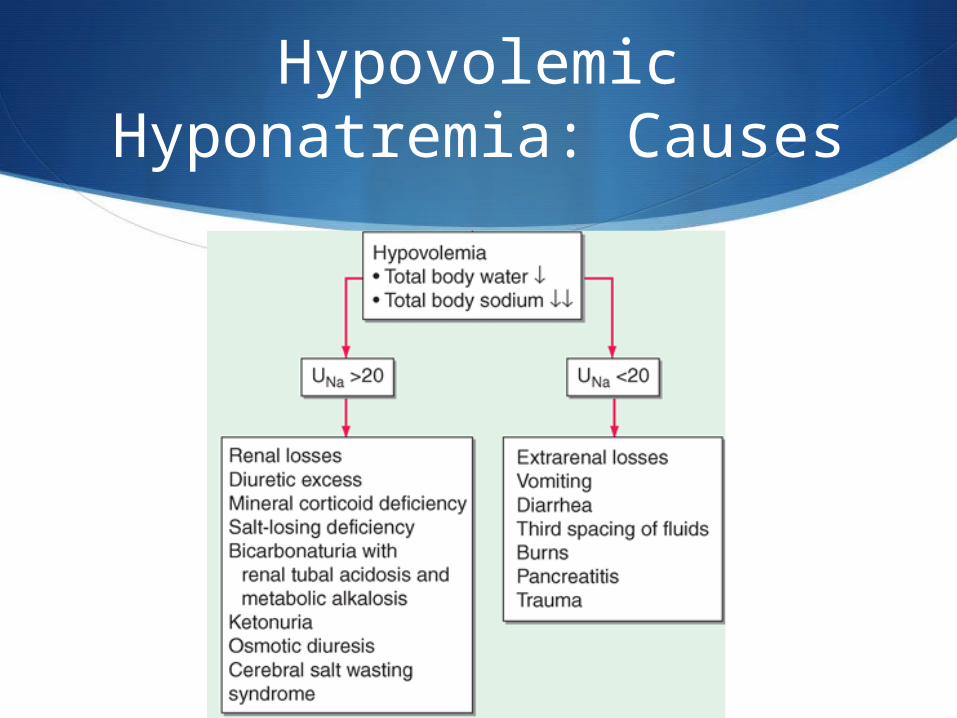
Hypovolemic Hyponatremia: Causes

Hypervolemic Hyponatremia: Causes
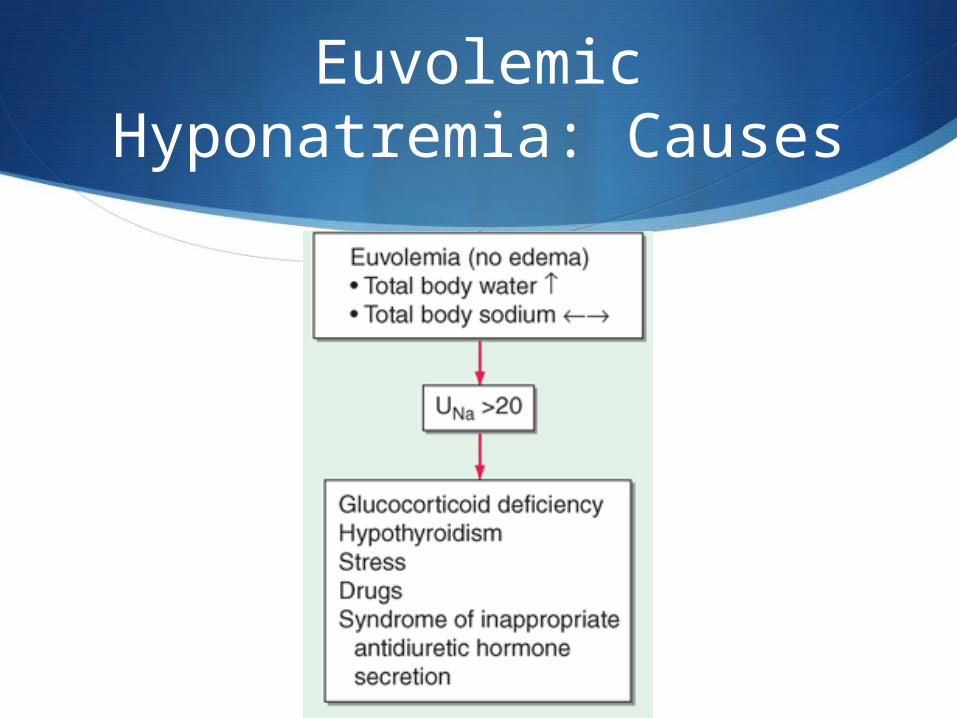
Euvolemic Hyponatremia: Causes
Syndrome of Inappropriate Antidiuresis (SIADH)
Most common cause of euvolemic hyponatremia
Inappropriate secretion of ADH independently from effective serum osmolality or circulating volume
Causes progressive hyponatremia until expression of vasopressin V2 receptors and aquaporin-2 water channels are down-regulated, called “vasopression escape”
A diagnosis of exclusion

SIADH: Diagnostic Criteria
SIADH: Causes
Physiologic
Malignancy
Pulmonary disorders
CNS disorders
Drugs
SIADH: Causes
Physiologic General anesthesia Nausea Pain Stress

SIADH: Causes
Malignancy Lung cancer Oropharynx GI tract – stomach, duodenum,
pancreas GU tract – ureter, bladder,
prostate, endometrium Lymphomas Sarcomas

SIADH: Causes
Pulmonary disorders Bacterial and viral pneumonia Pulmonary abscess TB Aspergillosis Asthma Cystic fibrosis Respiratory failure associated
with positive-pressure breathing

SIADH: Causes
CNS disorders Infection
Meningitis Brain abscess
Vascular and masses Subdural hematoma Subarachnoid hemorrhage Stroke Brain tumour Head trauma
Other Hydrocephalus Cavernous sinus thrombosis Multiple sclerosis Guillain-Barre syndrome Shy-Drager syndrome Delirium tremens
SIADH: Causes
Drugs Antidepressants
SSRIs Tricyclic MAOI Venlafaxine
Anticonvulsants Carbamazepine Valproate Lamotrigine
Anticancer drugs Platinum-based Cyclophospham
ide Methotrexate Vinca alkaloids
Vassopressin analogues Desmopressin Oxytocin Vasopressin
Miscellaneous Opiates MDMA Interferon NSAIDs Nicotine Amiodarone PPIs HCTZ
Cerebral Salt Wasting
Occurs in patients with CNS disease
Characterized by hyponatremia and extracellular fluid depletion due to inappropriate Na+ wasting in urine
Mechanism poorly understood Loss of sympathetic nervous system effect on
proximal tubule Release of circulating factor that impairs renal
tubular Na+ resorption
Similar to SIADH, except for hypovolemia
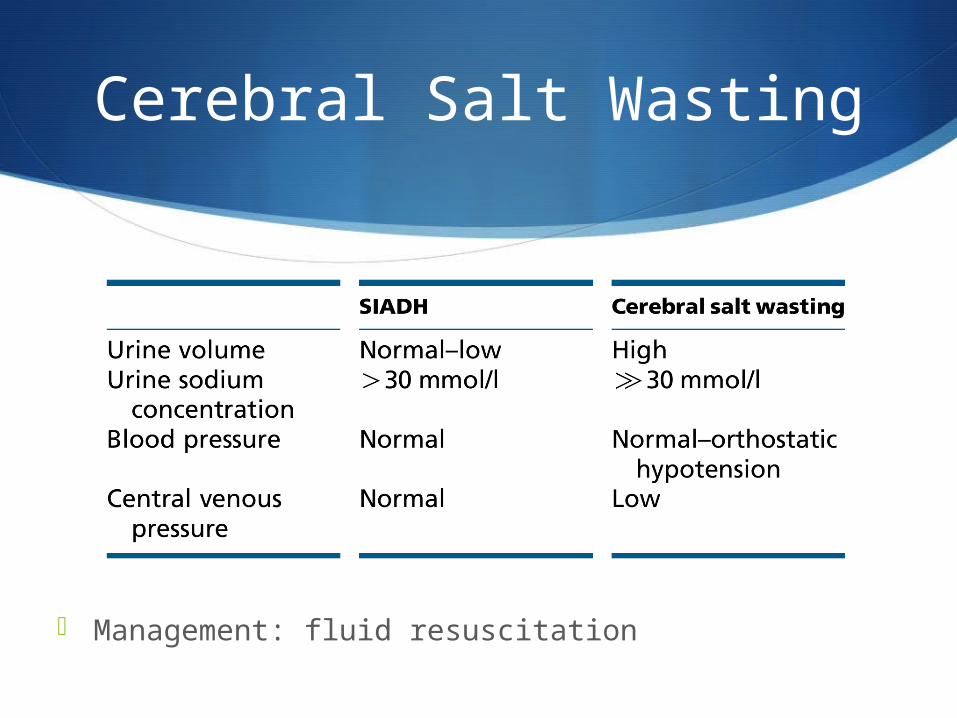
Cerebral Salt Wasting
Management: fluid resuscitation
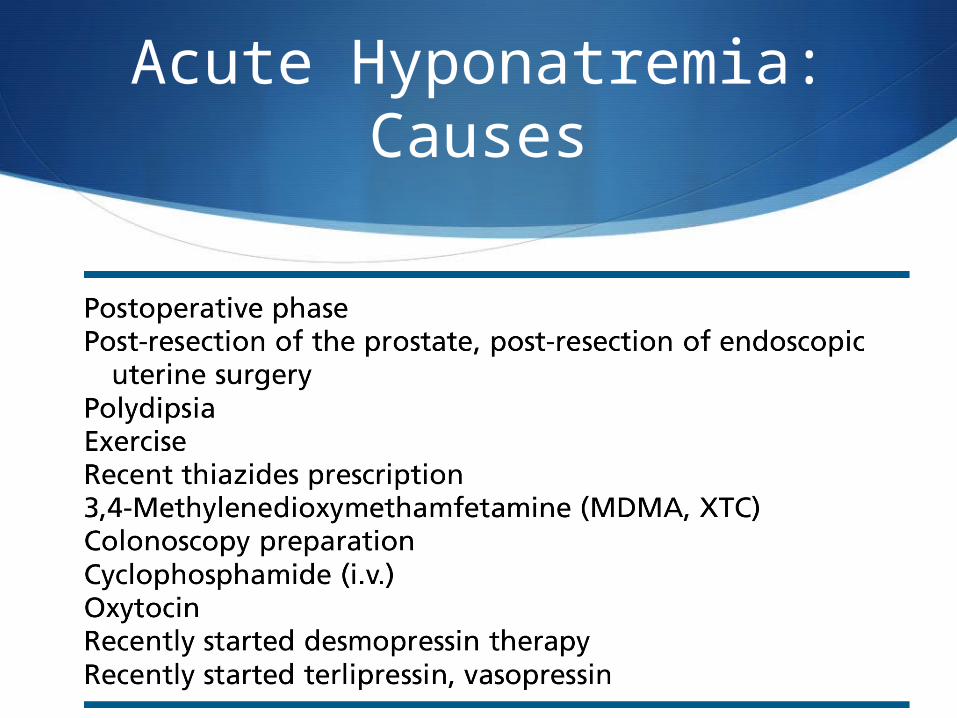
Acute Hyponatremia: Causes

Hyponatremia: Diagnosis Summary
1. Measure serum osmolality
2. Volume status
3. Urine Osmolality and Na+

Hyponatremia: Management
Factors influencing management: Treatment based on underlying
cause Acute (<48hr) or chronic (>48hr) Severity of symptoms
Hyponatremia: Management
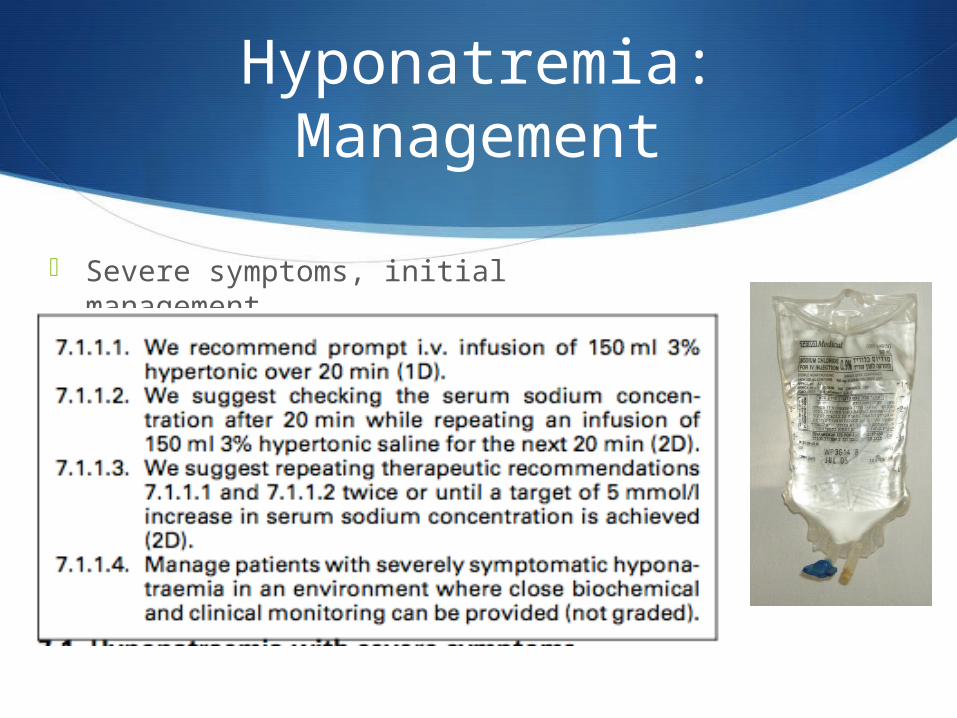
Severe symptoms, initial management

Hyponatremia: Management
Severe symptoms, now raised by 5mmol/l and symptoms improved

Hyponatremia: Management
Severe symptoms, now raised by 5mmol/l and symptoms persist
Hyponatremia: Management
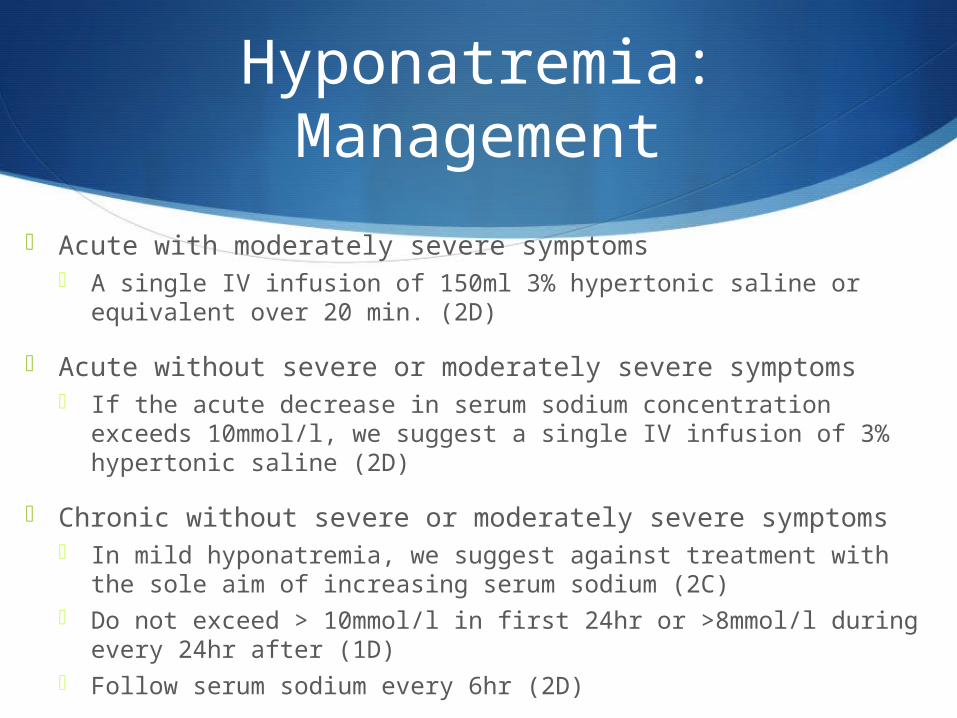
Acute with moderately severe symptoms A single IV infusion of 150ml 3% hypertonic saline or equivalent
over 20 min. (2D)
Acute without severe or moderately severe symptoms If the acute decrease in serum sodium concentration exceeds
10mmol/l, we suggest a single IV infusion of 3% hypertonic saline (2D)
Chronic without severe or moderately severe symptoms In mild hyponatremia, we suggest against treatment with the sole
aim of increasing serum sodium (2C) Do not exceed > 10mmol/l in first 24hr or >8mmol/l during every
24hr after (1D) Follow serum sodium every 6hr (2D)

Hyponatremia: Management
Correction calculation: Women TBW:
≈ 0.5 x body weight (young) ≈ 0.45 x body weight (elderly)
Men TBW: ≈ 0.6 x body weight (young) ≈ 0.5 x body weight (elderly)
Infusate Na+ content/L 3% Saline = 513 mmol/L 0.9% NS = 154 mmol/L 0.45% NS = 77 mmol/L Ringer’s = 130 mmol/L D5W = 0 mmol/L
Hyponatremia: Management
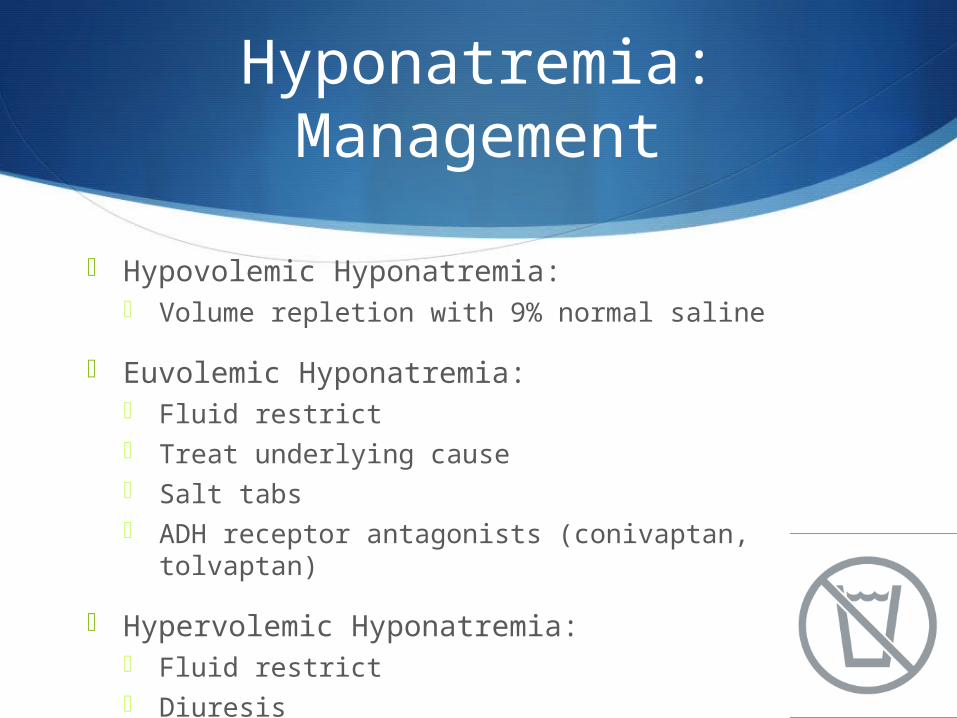
Hypovolemic Hyponatremia: Volume repletion with 9% normal saline
Euvolemic Hyponatremia: Fluid restrict Treat underlying cause Salt tabs ADH receptor antagonists (conivaptan, tolvaptan)
Hypervolemic Hyponatremia: Fluid restrict Diuresis
Hyponatremia: Osmotic Demyelination Syndrome
Occurs with overly rapid correction of severe hyponatremia that has been present for more than 2-3 days
Cerebral adaptation occurs with loss of organic osmolites that take time to return, leading to a drop in brain volume
Mechanism of how decreased brain volume leads to demyelination is unknown
Risk Factors: Serum Na+ level at presentation Duration of hyponatremia Rate of correction

Hyponatremia: Osmotic Demyelination Syndrome
Clinical Manifestations: Typically delayed for 2-6 days after correction Often irreversible Dysarthria Dysphagia Paraparesis or quadriparesis Behaviour changes Confusion, lethargy and coma
Overcorrection: Can re-lower Na+ by giving free water +/- DDAVP

Hyponatremia: Management
Principals: Severe symptoms aim for a quicker initial rise in Na+
Treat the underlying cause Do not over correct
~10 mmol in first 24hr than ~ 8mmol following 24hr intervals
Monitor serum Na+ levels frequently Allows for adjustments in treatment Ensures not over correcting

S
Hypernatremia
Case
21 M
Post car accident and traumatic brain injury
Received mannitol and hypertonic saline for raised ICP
Serum Na+ 160

Hypernatremia
Serum Na+ > 145 mmol/L
Water deficit
Usually loss of hypotonic fluid AND impaired access to free water
Hypernatremia is a powerful thirst stimulus
Thus usually develops in patients without access to water Impaired mental status (eg elderly or critically ill) Infants

Hypernatremia: Clinical Manifestations
Acute Hypernatremia: Rapid decrease in brain volume Leads to rupture of cerebral veins Causing focal intracerebral and subarachnoid
hemorrhages Also demyelinating brain lesions
Symptoms: Lethargy, weakness, irritability Twitching, seizures, coma
Chronic Hypernatremia: Less likely to have neurological sysmptoms
Hypernatremia: Causes
Unreplaced Water Loss
•Insensible and sweat losses•Gastrointestinal losses•Central or nephrogenic diabetes insipidus•Osmotic diuresis•Hypothalamic lesions impairing thirst or osmoreceptor function
Water Loss into Cells •Severe exercise or seizures
Sodium Overload•Intake or administration of hypertonic sodium solutions

Hypernatremia: Diagnosis

Diabetes Insipidus (DI)
ADH deficiency (central) or resistance (nephrogenic)
Central: hypothalamic or posterior pituitary disease Congenital, trauma/surgery, tumors, infiltrative Idiopathic, hypoxic encephalopathy, anorexia, EtOH
Nephrogenic: Congenital: ADH receptor V2 mutation, aquaporin-2
mutation Drugs: Lithium, amphotericin, demeclocycline, cidofovir Metabolic: hypercalcemia, severe hypokalemia Tubulointerstitial: postobstruction, recovery phase of
ATN, amyloid, pregnancy (placental vasopressinase)
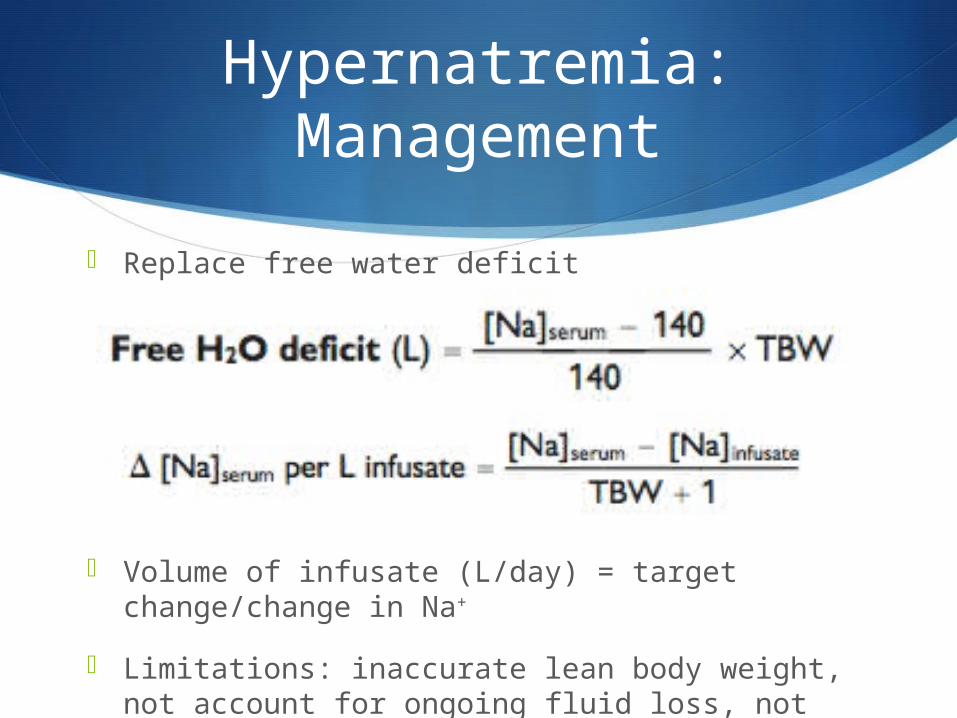
Hypernatremia: Management
Replace free water deficit
Volume of infusate (L/day) = target change/change in Na+
Limitations: inaccurate lean body weight, not account for ongoing fluid loss, not include isoosmotic fluid deficit
Hypernatremia: Management
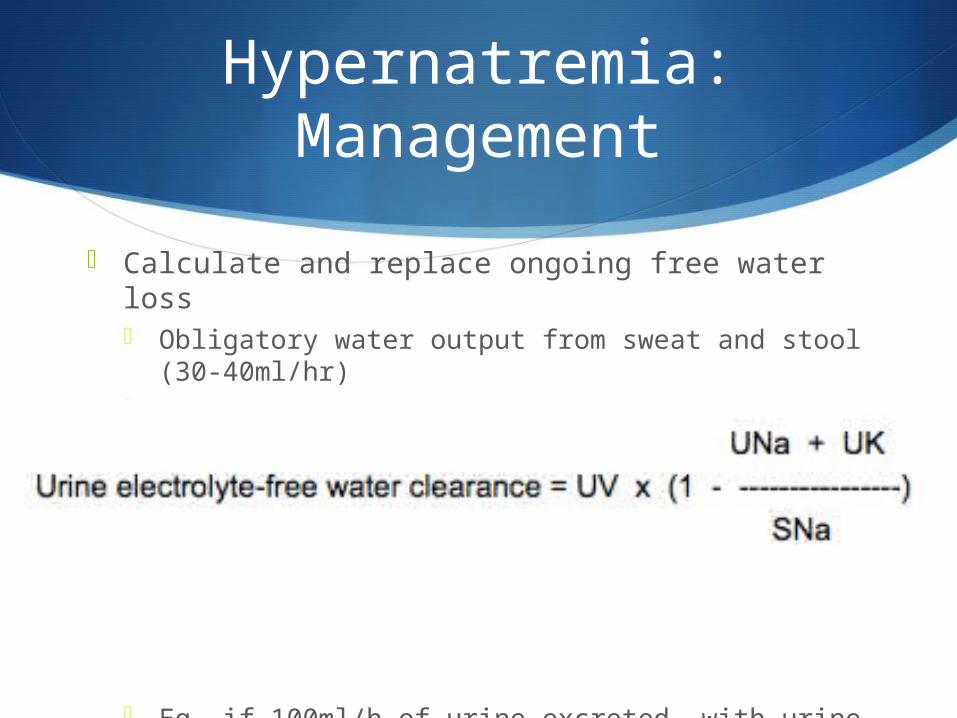
Calculate and replace ongoing free water loss Obligatory water output from sweat and stool (30-
40ml/hr) Ongoing urinary and/or GI losses that have Na+ and
K+ concentrations below the serum Na+ concentration
Eg. if 100ml/h of urine excreted, with urine Na+ and K+ concentration that is ½ of serum Na+
concentration, the free water clearance would be 50ml/h
Hypernatremia: Management
Treat underlying cause
Restore access to water
Replace free water deficit
Check serum Na+ frequently
If central DI give DDAVP
If chronic avoid rapid correction, no more than 10mmol/L per day
Summary
Hypo- and hypernatremia are water handling problems
Many different causes
Treatment must target underlying cause
Frequent Na+ monitoring required
Rate of correction is important to prevent neurological sequela

S
Questions?
References
Longo, D.L. et al. Harrison’s principles of internal medicine 18th edition. Boston: McGraw-Hill Professional. 2011. Print.
Melmed, S. et al. Williams textbook of endocrinology 12th edition. Saunders. 2011. Print.
Sabatine, M.S. et al. Pocke Medicine 4th edition. Philadelphia: Lippincott Williams & Wilkins. 2011. Print.
Spasovski, G. et al. Clinical practice guidelines on diagnosis and treatment of hyponatraemia. Eur J Endocrinol. 2014: 170, G1-G47.
Sterns, R. Etiology and evaluation of hypernatremia. Uptodate. Oct 2013. Accessed Sept 2014.
Sterns, R. Manifestations of hyponatremia and hypernatremia. Uptodate. July 2013. Accessed Sept 2014.
Sterns, R. Treatment of hypernatremia. Uptodate. July 2013. Accessed Sept 2014.
Related Documents











