© Disease Management Purchasing Consortium & Advisory Council (1998) DM in the Private Sector Spring 2003

© Disease Management Purchasing Consortium & Advisory Council (1998) DM in the Private Sector Spring 2003 Job Info Here: Job #, Template used, LIBs, colors,
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© Disease Management Purchasing Consortium & Advisory Council (1998)
DM in the Private Sector
Spring 2003
DM in the Private Sector
Spring 2003
© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI

© DMPC 2003. Www.DisMgmt.com, [email protected])
History of Disease Management in private sector: Milestones

© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI

© DMPC 2003. Www.DisMgmt.com, [email protected]) 3
Industry Trends: Market Sizes and Compositions (1997)
Maternal/Neo39%
Maternal/Neo39%
Asthma19%
Diabetes3%
CHF/Cardio19%
Rare Diseases2%
ESRD1%
Cancer17%
Cancer17%
Total Size: $77MM
© DMPC 2003. Www.DisMgmt.com, [email protected]) 4
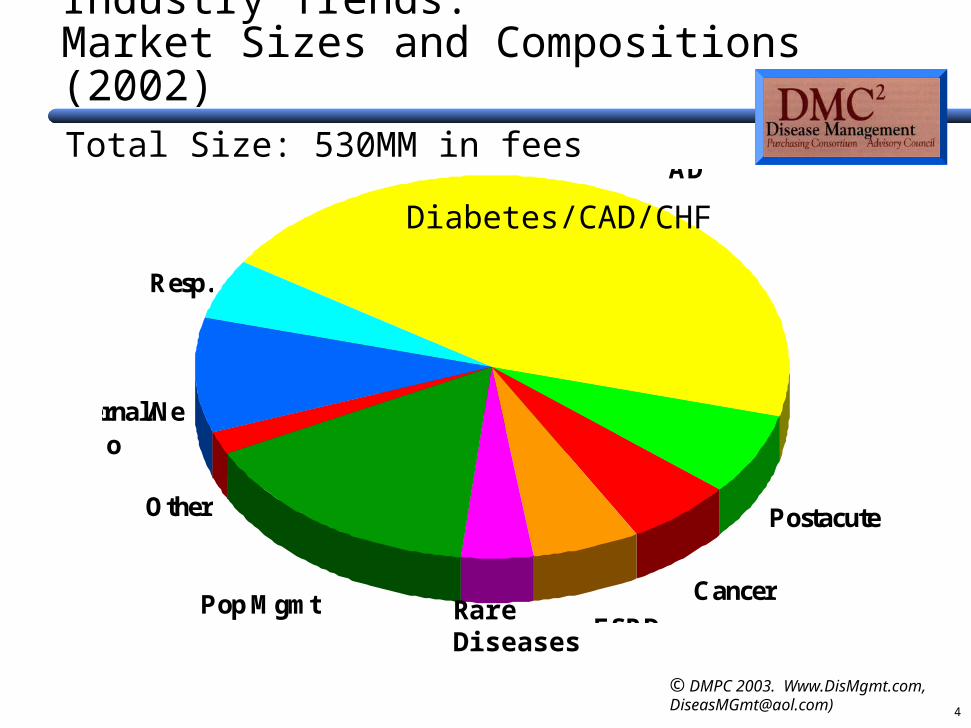
Industry Trends: Market Sizes and Compositions (2002)Total Size: 530MM in fees
Maternal/Neo
Resp.
Diab/CHf/CAD
Postacute
Cancer
ESRDRare DiseasePop Mgmt
Other
Diabetes/CAD/CHF
RareDiseases

© DMPC 2003. Www.DisMgmt.com, [email protected]) 4
Industry Trends: share of industry growth by consultant type
2002-2003Total New Business (to be) Awarded: est. $120-million
DMPC
SelfBenefits Con.
"Big Five"
Self
DMPC

© DMPC 2003. Www.DisMgmt.com, [email protected]) 4
Industry Trends: Consulting industry revenues
Total consulting revenues in DM 2002-2003 est. $15MM
DMPC
Benefits Con.
"Big Five"
© DMPC 2003. Www.DisMgmt.com, [email protected])
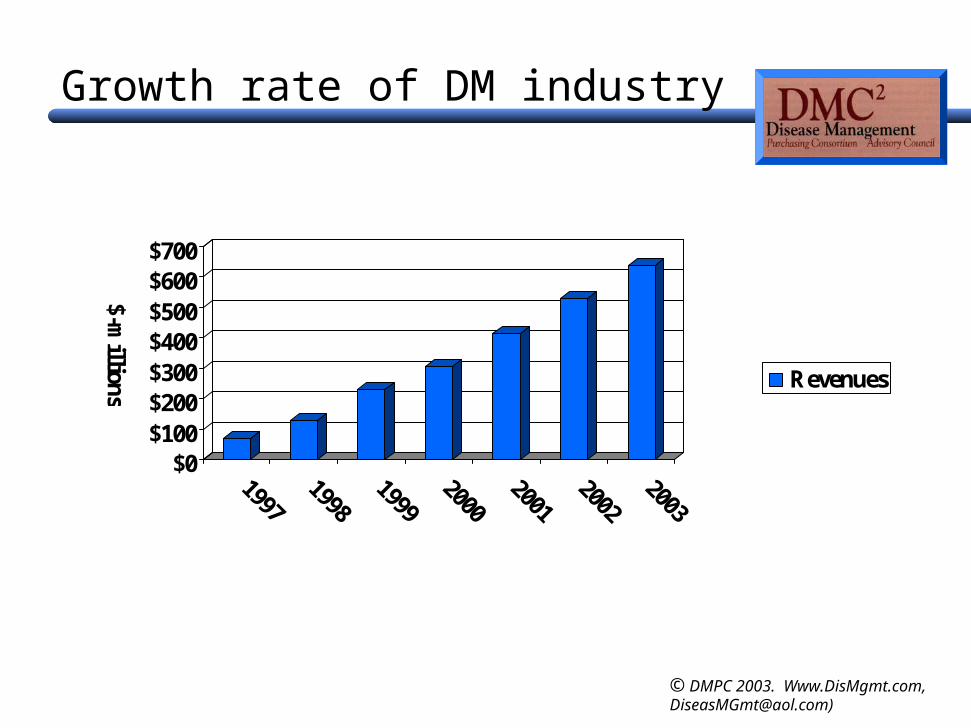
Growth rate of DM industry
$0$100$200$300$400$500$600$700
$-millions Revenues
© DMPC 2003. Www.DisMgmt.com, [email protected])
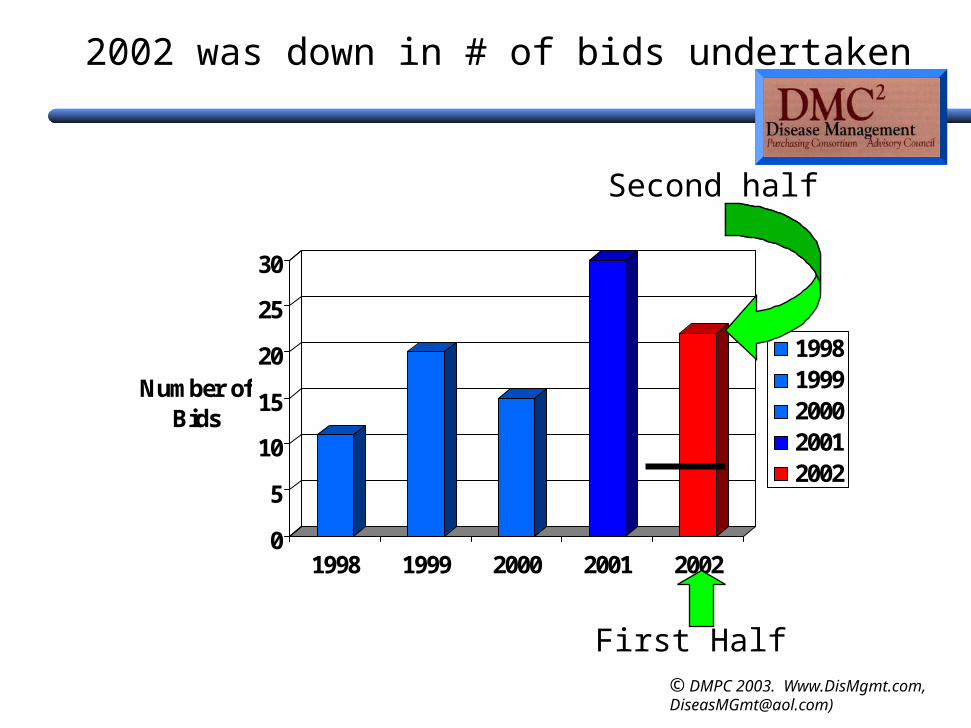
You can’t tell from that slide but…
Much of 2002 growth was add-ons and implementations of contracts signed in 2001 or early 2002
© DMPC 2003. Www.DisMgmt.com, [email protected])
2002 was down in # of bids undertaken
0
5
10
15
20
25
30
Number of Bids
1998 1999 2000 2001 2002
19981999200020012002
Second half
First Half
© DMPC 2003. Www.DisMgmt.com, [email protected])
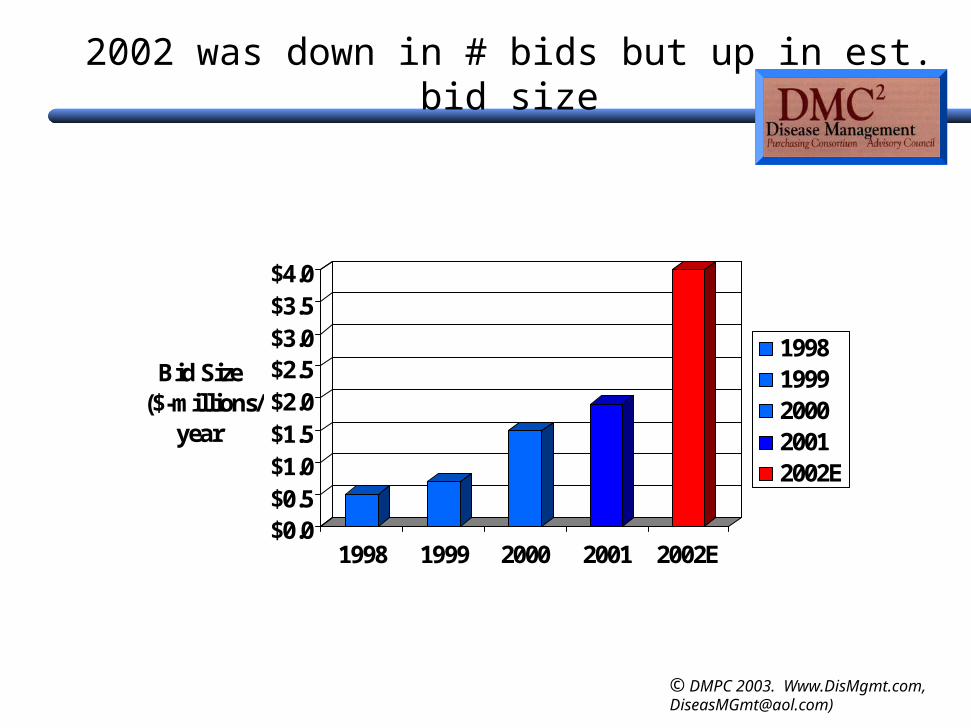
2002 was down in # bids but up in est. bid size
$0.0$0.5$1.0$1.5$2.0$2.5$3.0$3.5$4.0
Bid Size ($-millions/
year
1998 1999 2000 2001 2002E
19981999200020012002E
© DMPC 2003. Www.DisMgmt.com, [email protected])
Other 2002 observations
Growth was from expanding in existing business, not new business
Many bids undertakenPurchase cycle hasn’t gotten shorter so……Few contracts awardedEven fewer scale contracts consummated and
announced
Many awards and announcements being made in 2003

© DMPC 2003. Www.DisMgmt.com, [email protected])
How does the rest of 2003 look?
3 new bids (small)3 more large bids expected soon (private sector)2 major Medicaid bids expected soon
Action definitely shifting to public sector

© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI
© DMPC 2003. Www.DisMgmt.com, [email protected])
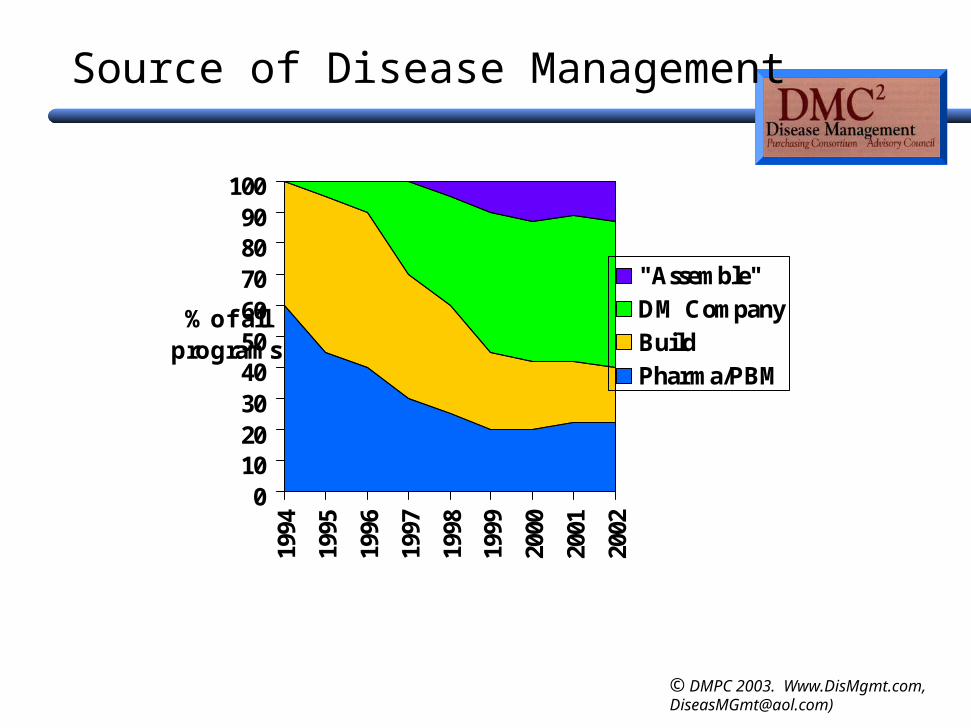
Source of Disease Management
0102030405060708090
100
1994
1995
1996
1997
1998
1999
2000
2001
2002
% of all programs
"Assemble"DM CompanyBuildPharma/PBM

© DMPC 2003. Www.DisMgmt.com, [email protected])
Why Building is Declining
Very few health plans get it rightMost need to account for it in admin (guaranteed
“bought” plans accounted for in medical)Takes a long timeEmployers looking for “Intel Inside” in DM programsTwo issues in detail:
Most built programs measure wrongNetwork health plans are a different business from DM

© DMPC 2003. Www.DisMgmt.com, [email protected])
Issue #1—How built Programs Measure WrongDollars spent per $20 in claims— typical built vs. bought
$0.00 $0.10 $0.20 $0.30 $0.40
Enrollment
Basel/Strat
EducOB
Unsched IB
Materials/Fulfillment
MD Interf
Superv/training
Facilities
Analysis/Reporting
Vendors
Health Plans

© DMPC 2003. Www.DisMgmt.com, [email protected])
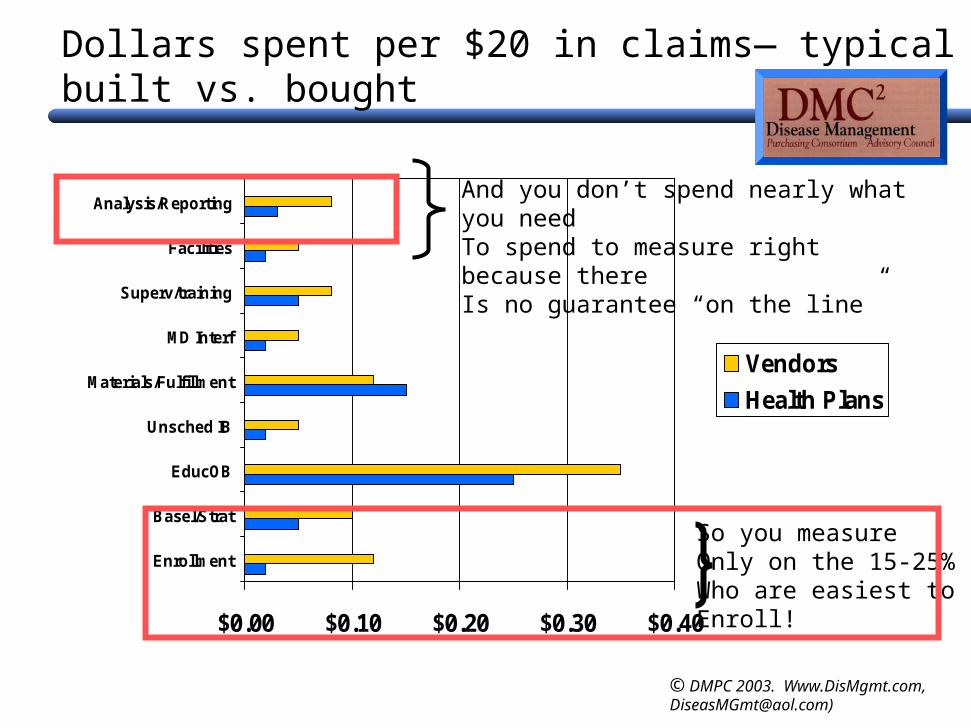
Dollars spent per $20 in claims— typical built vs. bought
$0.00 $0.10 $0.20 $0.30 $0.40
Enrollment
Basel/Strat
EducOB
Unsched IB
Materials/Fulfillment
MD Interf
Superv/training
Facilities
Analysis/Reporting
Vendors
Health Plans
So you measureOnly on the 15-25%Who are easiest toEnroll!
© DMPC 2003. Www.DisMgmt.com, [email protected])
Dollars spent per $20 in claims— typical built vs. bought
$0.00 $0.10 $0.20 $0.30 $0.40
Enrollment
Basel/Strat
EducOB
Unsched IB
Materials/Fulfillment
MD Interf
Superv/training
Facilities
Analysis/Reporting
Vendors
Health Plans
So you measureOnly on the 15-25%Who are easiest toEnroll!
And you don’t spend nearly what you needTo spend to measure right because there Is no guarantee “on the line”

© DMPC 2003. Www.DisMgmt.com, [email protected])
Issue #2: How Health Plans are a different business
“It’s our core competency”
© DMPC 2003. Www.DisMgmt.com, [email protected])
Myths of “Building”
“It’s our core competency” No--it’s a highly specialized “custom shop” vs. an HMO throughput shop
Buying is itself a core competency
© DMPC 2003. Www.DisMgmt.com, [email protected])
Myths of “Building”
“It’s our core competency”
“Why should we pay someone to do what we can do ourselves?”
No--it’s a highly specialized “custom shop” vs. an HMO throughput shop
Buying is itself a core competency
© DMPC 2003. Www.DisMgmt.com, [email protected])
Myths of “Building”
“It’s our core competency”
“Why should we pay someone to do what we can do ourselves?”
No--it’s a highly specialized “custom shop” vs. an HMO throughput shop
Buying is itself a core competency
You can also deliver your own packages absolutely, positively overnight
© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI

© DMPC 2003. Www.DisMgmt.com, [email protected])
Fee Migration (index 1997 to 100)
050
100150
1997 1998 1999 2000 2001 2002 2003
1997 = 100
DiabetesTPMAsthmaCHF

© DMPC 2003. Www.DisMgmt.com, [email protected])
Why have prices come down?
Vendors more efficientFewer home visits (except in COPD)Larger contractsBuyer purchasing power increasingly concentrated

© DMPC 2003. Www.DisMgmt.com, [email protected])
Guaranteed Savings falling due to better contracting
00.5
11.5
1997 1998 1999 2000 2001 2002 2003
% guaranteed net savings
AsthmaDiabetesCHFCADESRD

© DMPC 2003. Www.DisMgmt.com, [email protected])
Guaranteed Savings still popular
0
2
4
6
8
10
12
1996
All
Co
nso
rtiu
m C
on
trac
ts
19991997 1998 2000
Not Guaranteed
Guaranteed No LOC/Reinsurance
Guaranteed with LOC or Reinsurance
2001 2002
© DMPC 2003. Www.DisMgmt.com, [email protected])
Why are guarantees falling?
“Usual care” improving (example: ESRD)Competition is more fee-based once guarantees are
high enoughGuarantees aren’t falling much—counting is getting
better (example: asthma)
source; gregg meyer © DMPC 2003. Www.DisMgmt.com, [email protected])
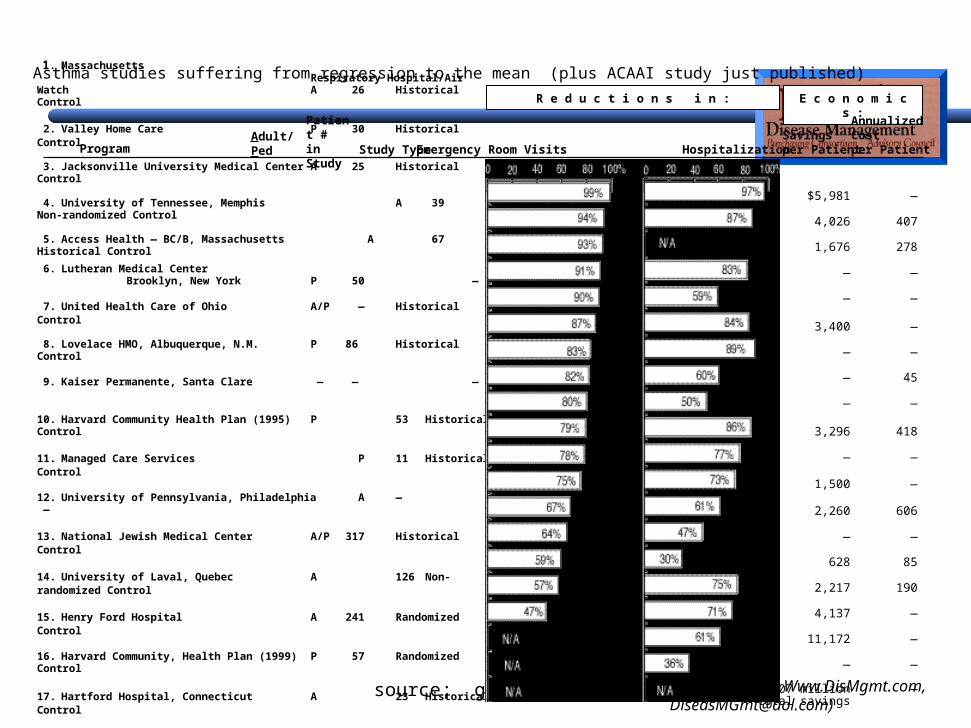
Asthma studies suffering from regression to the mean (plus ACAAI study just published)
Program Study Type
1. Massachusetts Respiratory Hospital/Air Watch A 26 Historical Control
2. Valley Home Care P 30 Historical Control
3. Jacksonville University Medical Center A 25 Historical Control
4. University of Tennessee, Memphis A 39 Non-randomized Control
5. Access Health — BC/B, Massachusetts A 67 Historical Control
6. Lutheran Medical Center Brooklyn, New York P 50 —
7. United Health Care of Ohio A/P — Historical Control
8. Lovelace HMO, Albuquerque, N.M. P 86 Historical
Control
9. Kaiser Permanente, Santa Clare — — —
10. Harvard Community Health Plan (1995) P 53 Historical Control
11. Managed Care Services P 11 Historical Control
12. University of Pennsylvania, Philadelphia A — —
13. National Jewish Medical Center A/P 317 Historical Control
14. University of Laval, Quebec A 126 Non-randomized Control
15. Henry Ford Hospital A 241 Randomized Control
16. Harvard Community, Health Plan (1999) P 57 Randomized Control
17. Hartford Hospital, Connecticut A 23 Historical Control
18. Olsten Kimberly Quality Care A/P 257 —
19. Blue Cross/Blue Shield of South Carolina — 3,000 —
20. Harvard Pilgrim Health Care, Boston — — —
Emergency Room Visits Hospitalization
AnnualizedSavingsper Patient
R e d u c t i o n s i n : E c o n o m i c s :
$5,981 —
4,026 407
1,676 278
— —
— —
3,400 —
— —
— 45
— —
3,296 418
— —
1,500 —
2,260 606
— —
628 85
2,217 190
4,137 —
11,172 —
— —
$1.07 million —total savings
Patient #in Study
Adult/Ped
AnnualizedCostper Patient
© DMPC 2003. Www.DisMgmt.com, [email protected])
To guarantee or not to guarantee
ProAssures return on investmentEasier to compare vendorsTests for confidence in vendor outcomesEasier to sell internallyEasier to get budget for scale programLess career risk if program doesn’t save money (may
even boost career)No need to micro-manage vendor

© DMPC 2003. Www.DisMgmt.com, [email protected])
To guarantee or not to guarantee
ConsComplexity of baseline and reconciliation (easier to put the
complexity in the RFP and contract)Higher price (not much higher)Most people will contract incorrectly anyway (example),
giving the worst of both worlds
Synthesis
© DMPC 2003. Www.DisMgmt.com, [email protected])
To guarantee or not to guarantee
SynthesisALWAYS ask for guarantees even if you aren’t going to
use them– A lot of the “pro’s” (comparability, selling internally,
confidence in outcomes) are in the purchase processAfter a few years of positive reconciliations, switch to FFS
(e.g., Humana--COR)
© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI
© DMPC 2003. Www.DisMgmt.com, [email protected])
Employers and Disease Management
What mattersMarket sizePlayersThrough health plan vs. independentlyMarkup
© DMPC 2003. Www.DisMgmt.com, [email protected])
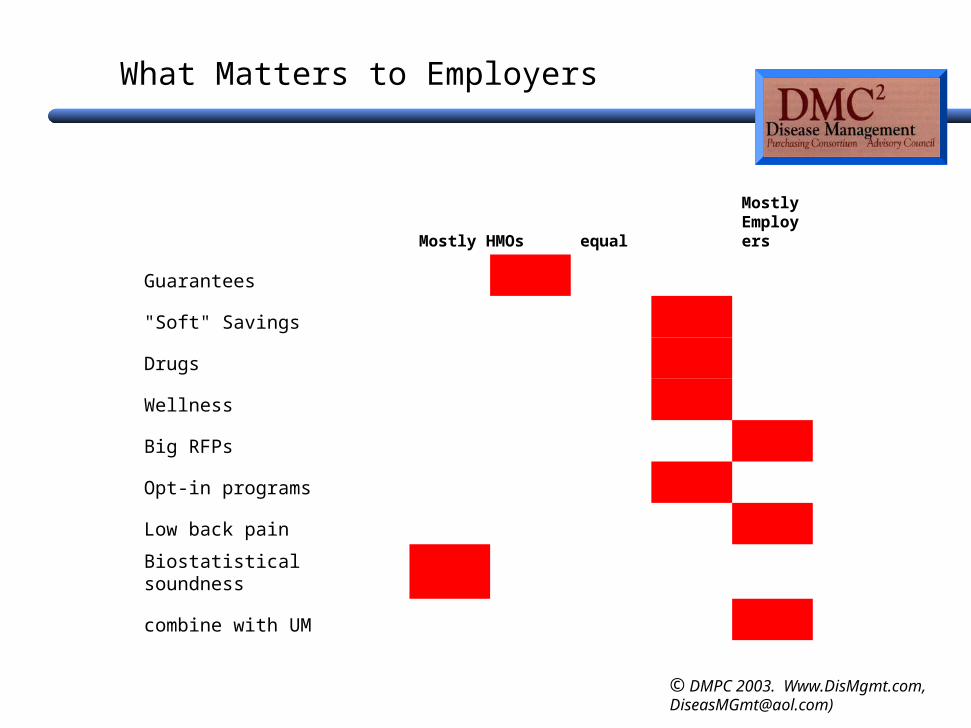
Mostly HMOs equal
Mostly Employers
Guarantees
"Soft" Savings
Drugs
Wellness
Big RFPs
Opt-in programs
Low back pain
Biostatistical soundness
combine with UM
What Matters to Employers

© DMPC 2003. Www.DisMgmt.com, [email protected])
Market Size of employer-direct market in 2002
Health PlansMedicaidCMS DemosEmployer-direct

© DMPC 2003. Www.DisMgmt.com, [email protected])
Why so little employer-direct?
A lot of employers looking…but median is c. 10,000 employees
Programs are more likely to be “lite” and opt-in (chart is revenue-based)
Some very large employers still on sidelinesSome don’t think it works (GE)Biggest waiting for its UM vendor to come up with
somethingSome don’t interfere with employees
Many go through health plans Note: A lot of heat (“big” RFPs) but not much light
© DMPC 2003. Www.DisMgmt.com, [email protected])
Arguments to go independently vs. through health plan
IndependentlyMakes more sense with
multiple health plansDon’t like your health plan’s
own offeringContinuity if you change
health plans
Through health planEasier (if there is only one)More will enroll—won’t be
obvious it’s coming from you– Can do opt-out
Uses the UM and other tools to enroll members
Should be a better financial deal (but often isn’t)

© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI

© DMPC 2003. Www.DisMgmt.com, [email protected])
2003-4: What’s hot and what’s not
Hot COPD Post-acute care (Medicare
plans) “Significant Medical conditions” Medicaid disabled Total population management Vendors with correct metrics Cancer PPOs
Not Single-disease RFPs in
diabetes, CHF, asthma Medicaid HMOs Large straight HMO bids (not
many left to bid) “Builds” Pharmaceutical company
initiatives (except PHS) “Soft” savings

© DMPC 2003. Www.DisMgmt.com, [email protected])
Agenda
History of Disease Management in the Private SectorSize and Growth Rates Build vs. Buy trendsPricing and FeesEmployers vs. Health PlansWhat's Hot and What's Not Issues facing the industry
ROIROIROI

© DMPC 2003. Www.DisMgmt.com, [email protected])
Issues facing the Industry: ROI
Still a great deal of skepticism about ROI “Peer review” in published accounts can be worthless
“Peer reviewers” usually physicians, not actuaries – Trust your in-house actuary!
Proliferation of “experts” making things more confusingHopkins paper an excellent starting point (though other
methodologies are valid) “Built” programs measure ROI too highA good rule of thumb from yesterday’s workshop: If you
show more than 2:1 ROI in first year, you measured wrong
Related Documents










