¢ÈÌËÓÈ·›· ¤Î‰ÔÛË Ù˘ EÏÏËÓÈ΋˜ ¶·È‰È·ÙÚÈ΋˜ EÙ·ÈÚ›·˜ ¶Úfi‰ÚÔ˜ ∞. ∫ˆÓÛÙ·ÓÙfiÔ˘ÏÔ˜ ™˘ÓÙ·ÎÙÈ΋ EÈÙÚÔ‹ ¢È¢ı˘ÓÙ‹˜ ™‡ÓÙ·Í˘ ∫. ™ÙÂÊ·Ó›‰Ë˜ M¤ÏË ™. ∞Ó‰ÚÔÓ›ÎÔ˘ ¶. ∞˘ÁÔ˘ÛÙ›‰Ô˘-™·‚‚ÔÔ‡ÏÔ˘ A. µ·˙·›Ô˘-°ÂÚ·ÛÈÌ›‰Ë °. µ·ÚÏ¿Ì˘ ∂. °·Ï·Ó¿Î˘ §. £ˆÌ·˝‰Ô˘ ª. ∫·Ó¿ÚÈÔ˘ ∂. ∫·ÙÛ·ÚÔ‡-¶ÂÎÙ·Û›‰Ë A. K·ÙÙ¿Ì˘ ™. K›ÙÛÈÔ˘-∆˙¤ÏË ∞. ¶··‰ÔÔ‡ÏÔ˘ ¡. ¶··‰fiÔ˘ÏÔ˜ ∞. ™È·ÌÔÔ‡ÏÔ˘-ª·˘Ú›‰Ô˘ ª. ∆ÛÔÏÈ¿ ÀÔ‚ÔÏ‹ ∂ÚÁ·ÛÈÒÓ e-mail: [email protected] √‰ËÁ›Â˜ ÚÔ˜ ÙÔ˘˜ Û˘ÁÁÚ·Ê›˜: http://www.e-child.gr/Instructions_ to_Authors_GR.pdf ºÈÏÔÏÔÁÈ΋ EÈ̤ÏÂÈ· ∂È̤ÏÂÈ· ÂÏÏËÓÈÎÒÓ ÎÂÈÌ¤ÓˆÓ M. ¡·ÙÛÔ˘Ï›‰Ô˘ EÈ̤ÏÂÈ· ·ÁÁÏÈÎÒÓ ÎÂÈÌ¤ÓˆÓ ™. ¡¿ÎÔ˘ EΉfiÙ˘ K. °ÚÈ‚¤·˜ ™˘ÓÙÔÓÈÛÙ‹˜ ∂ΉfiÛˆ˜ E¶I™THMONIKE™ EK¢O™EI™ E.¶.E. ¶ÈÂÚ›·˜ 1∞ 144 51 MÂÙ·ÌfiÚʈÛË TËÏ.: 210 87 78 810 Fax: 210 87 78 822 I‰ÈÔÎÙ‹Ù˘ EÏÏËÓÈ΋ ¶·È‰È·ÙÚÈ΋ EÙ·ÈÚ›· © Mȯ·Ï·ÎÔÔ‡ÏÔ˘ 92 Aı‹Ó· 115 28 TËÏ.: 210 7771 140 210 7771 663 Fax: 210 7758 354 e-mail: [email protected] EÙ‹ÛÈ· ™˘Ó‰ÚÔÌ‹: 40 € EȉÈ΢fiÌÂÓÔÈ, ºÔÈÙËÙ¤˜: 20 € ¶ÂÚȯfiÌÂÓ· ∞¡∞™∫O¶∏™∂π™ 87 Paediatric liver transplantation: historical notes G. C. Sotiropoulos, S. Nadalin, A. Radtke, H. Lang 92 Childhood obesity – ∞ public health crisis across the European Union A. J. Nicholson, S. Del Torso, A. Hadjipanyidis, D. Van Esso 96 Use of the new World Health Organization growth standards in the prevention of childhood overweight and obesity M. Ponce-Rivera, D. Fuentes-Lugo 105 µ·ÛÈΤ˜ Ù¯ÓÈΤ˜ Ù˘ ÌÔÚȷ΋˜ ‚ÈÔÏÔÁ›·˜ Î·È Ë ÂÊ·ÚÌÔÁ‹ ÙÔ˘˜ ÛÙË ‰È¿ÁÓˆÛË ·È‰È·ÙÚÈÎÒÓ ÓÔÛËÌ¿ÙˆÓ ™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜ 116 ¡ÂfiÙÂÚ· ‰Â‰Ô̤ӷ ÁÈ· ÙË ‰È·ÙÚÔÊ‹ ÙÔ˘ ‚Ú¤ÊÔ˘˜ Ã. ∫ÒÛÙ·ÏÔ˜ 123 ∂Ӊ›ÍÂȘ ¯ÔÚ‹ÁËÛ˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ ÛÙ· ·È‰È¿ Î·È ÙÔ˘˜ ÂÊ‹‚Ô˘˜ E. ∫Ô‡ÛÙ·, ∞. ¶··ı·Ó·Û›Ô˘, Ã. ÷Ù˙Ë·ı·Ó·Û›Ô˘† ∂ƒ∂À¡∏∆π∫∂™ ∂ƒ°∞™π∂™ 128 ∆ÂÏÈÎfi ·Ó¿ÛÙËÌ· Û ·È‰È¿ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Ô˘ ¤Ï·‚·Ó ıÂڷ›· ˘ÔηٿÛÙ·Û˘ ª. ¶··‰ÔÔ‡ÏÔ˘, ™. ¡ÙÔ˘Ì¿, ∫. ∫›ÙÛÈÔ˜, ¡. ∫·‰fiÁÏÔ˘, ∫. ∫ÒÛÙ·, π. ∆ÛÈÔ‡Ú˘ 135 ªÂϤÙË ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ Û ·È‰È¿ Ì Ïԛ̈ÍË ·fi Èfi Epstein-Barr Î·È ÌÂÁ·ÏÔ΢ÙÙ·ÚÔ˚fi Î·È Û˘Û¯¤ÙÈÛË Ì ÙËÓ ÎÏÈÓÈ΋ ¤Î‚·ÛË ∂. ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË, ∞. ºÏ¤‚·, µ. ∞ÓÙ¿ÚË, ∞. ¶·˘Ï›ÙÔ˘-∆ÛÈfiÓÙÛË, ª. ªÔÛÎÔÊ›‰Ë˜, °. µ·ÚÏ¿Ì˘ 141 ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ ÛÙ· ·È‰È¿: ÂÌÂÈÚ›· 15 ÂÙÒÓ Û ¤Ó· ΤÓÙÚÔ Ÿ. µÚ¿ÓË, ª. ¶·ÓÙÈΛ‰Ô˘, °. ÿÌ‚ÚÈÔ˜, π. •˘ÓÈ¿˜, µ. ¢ÂÌÂÚÙ˙›‰Ô˘, ∫. ∫¿ÓÙ˙ÈÔ˘, ∞. ª·˘ÚÔ˘‰‹, ¢. ∆·ÎÔ‡‰·˜, £. ¶··ÛÙ·‡ÚÔ˘, ∫. ™‡ÚÔÁÏÔ˘ 148 √ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙˆÓ Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜, ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ Ù‡Ô˘ C Î·È ÙÔ˘ Ó¢ÌÔÓÈfiÎÔÎÎÔ˘ µ. ∆ÛÈ¿ÓÙÔ˘, ∞. ∫·Úfi΢, ∂. ¶¿‚Ë, °. ∫˘ÚÈfiÔ˘ÏÔ˜ ¶ƒ∞∫∆π∫√ £∂ª∞ 157 ¢È·ÙÚÔÊ‹ ·È‰ÈÒÓ Î·È ÂÊ‹‚ˆÓ ÁÈ· ÚÔ·ÁˆÁ‹ Ù˘ ˘Á›·˜ Î·È Ù˘ ·Ó¿Ù˘Í˘ Î·È ÚfiÏË„Ë ÙˆÓ ¯ÚfiÓÈˆÓ ÓÔÛËÌ¿ÙˆÓ ∞. ∫·Ê¿ÙÔ˜ ∂¡¢π∞º∂ƒ√À™∞ ¶∂ƒπ¶∆ø™∏ 162 Recurrent Respiratory Papillomatosis: case report and literature review D. A. Nunez 165 ∫§π¡π∫√ ∫√Àπ∑ ¶. ™ËÊÈ·ÓÔ‡, ∫. ºˆÙ›Ô˘, ∫. ™ÎÈ·‰¿˜, ∫. ¶··Á·ÚÔ˘Ê¿Ï˘ ∂¶I∫∞πƒ√ £Eª∞ 166 ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ ™À¡∆√ª∞ ¶∞π¢π∞∆ƒπ∫∞ ¡∂∞ 171 ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ 2008 E. °·Ï·Ó¿Î˘ ¡∂∞ ∞¶√ ∆√ ¢π∞¢π∫∆À√ 173 ™‡ÓÙÔÌ· ·È‰È·ÙÚÈο Ó¤· ÛÙÔ ‰È·‰›ÎÙ˘Ô ∫. ™ÙÂÊ·Ó›‰Ë˜ ¶·È‰È·ÙÚÈ΋ ∆fiÌÔ˜ 71 ñ ∆‡¯Ô˜ 2 ñ ª¿ÚÙÈÔ˜-∞Ú›ÏÈÔ˜ 2008 ∫ˆ‰ÈÎfi˜ ¢È‡ı˘ÓÛ˘ ∂ÔÙ›·˜ ªª∂: 3889 ISSN 0377-2551

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
¢ÈÌËÓÈ·›· ¤Î‰ÔÛË Ù˘
EÏÏËÓÈ΋˜ ¶·È‰È·ÙÚÈ΋˜ EÙ·ÈÚ›·˜
¶Úfi‰ÚÔ˜
∞. ∫ˆÓÛÙ·ÓÙfiÔ˘ÏÔ˜
™˘ÓÙ·ÎÙÈ΋ EÈÙÚÔ‹
¢È¢ı˘ÓÙ‹˜ ™‡ÓÙ·Í˘
∫. ™ÙÂÊ·Ó›‰Ë˜
M¤ÏË
™. ∞Ó‰ÚÔÓ›ÎÔ˘
¶. ∞˘ÁÔ˘ÛÙ›‰Ô˘-™·‚‚ÔÔ‡ÏÔ˘
A. µ·˙·›Ô˘-°ÂÚ·ÛÈÌ›‰Ë
°. µ·ÚÏ¿Ì˘
∂. °·Ï·Ó¿Î˘
§. £ˆÌ·˝‰Ô˘
ª. ∫·Ó¿ÚÈÔ˘
∂. ∫·ÙÛ·ÚÔ‡-¶ÂÎÙ·Û›‰Ë
A. K·ÙÙ¿Ì˘
™. K›ÙÛÈÔ˘-∆˙¤ÏË
∞. ¶··‰ÔÔ‡ÏÔ˘
¡. ¶··‰fiÔ˘ÏÔ˜
∞. ™È·ÌÔÔ‡ÏÔ˘-ª·˘Ú›‰Ô˘
ª. ∆ÛÔÏÈ¿
ÀÔ‚ÔÏ‹ ∂ÚÁ·ÛÈÒÓ
e-mail: [email protected]
√‰ËÁ›Â˜ ÚÔ˜ ÙÔ˘˜ Û˘ÁÁÚ·Ê›˜:
http://www.e-child.gr/Instructions_
to_Authors_GR.pdf
ºÈÏÔÏÔÁÈ΋ EÈ̤ÏÂÈ·
∂È̤ÏÂÈ· ÂÏÏËÓÈÎÒÓ ÎÂÈ̤ӈÓ
M. ¡·ÙÛÔ˘Ï›‰Ô˘
EÈ̤ÏÂÈ· ·ÁÁÏÈÎÒÓ ÎÂÈ̤ӈÓ
™. ¡¿ÎÔ˘
EΉfiÙ˘
K. °ÚÈ‚¤·˜
™˘ÓÙÔÓÈÛÙ‹˜ ∂ΉfiÛˆ˜
E¶I™THMONIKE™ EK¢O™EI™ E.¶.E.
¶ÈÂÚ›·˜ 1∞
144 51 MÂÙ·ÌfiÚʈÛË
TËÏ.: 210 87 78 810
Fax: 210 87 78 822
I‰ÈÔÎÙ‹Ù˘
EÏÏËÓÈ΋ ¶·È‰È·ÙÚÈ΋ EÙ·ÈÚ›·©
Mȯ·Ï·ÎÔÔ‡ÏÔ˘ 92
Aı‹Ó· 115 28
TËÏ.: 210 7771 140
210 7771 663
Fax: 210 7758 354
e-mail: [email protected]
EÙ‹ÛÈ· ™˘Ó‰ÚÔÌ‹: 40 €EȉÈ΢fiÌÂÓÔÈ, ºÔÈÙËÙ¤˜: 20 €
¶ÂÚȯfiÌÂÓ·
∞¡∞™∫O¶∏™∂π™
87 Paediatric liver transplantation:
historical notes
G. C. Sotiropoulos, S. Nadalin, A. Radtke, H. Lang
92 Childhood obesity – ∞ public health crisis
across the European Union
A. J. Nicholson, S. Del Torso, A. Hadjipanyidis, D. Van Esso
96 Use of the new World Health Organization
growth standards in the prevention of
childhood overweight and obesity
M. Ponce-Rivera, D. Fuentes-Lugo
105 µ·ÛÈΤ˜ Ù¯ÓÈΤ˜ Ù˘ ÌÔÚȷ΋˜ ‚ÈÔÏÔÁ›·˜ Î·È Ë
ÂÊ·ÚÌÔÁ‹ ÙÔ˘˜ ÛÙË ‰È¿ÁÓˆÛË ·È‰È·ÙÚÈÎÒÓ
ÓÔÛËÌ¿ÙˆÓ
™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
116 ¡ÂfiÙÂÚ· ‰Â‰Ô̤ӷ ÁÈ· ÙË ‰È·ÙÚÔÊ‹ ÙÔ˘
‚Ú¤ÊÔ˘˜
Ã. ∫ÒÛÙ·ÏÔ˜
123 ∂Ӊ›ÍÂȘ ̄ ÔÚ‹ÁËÛ˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
ÛÙ· ·È‰È¿ Î·È ÙÔ˘˜ ÂÊ‹‚Ô˘˜
E. ∫Ô‡ÛÙ·, ∞. ¶··ı·Ó·Û›Ô˘, Ã. ÷Ù˙Ë·ı·Ó·Û›Ô˘†
∂ƒ∂À¡∏∆π∫∂™ ∂ƒ°∞™π∂™
128 ∆ÂÏÈÎfi ·Ó¿ÛÙËÌ· Û ·È‰È¿ Ì ·Ó¿ÚÎÂÈ·
·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Ô˘ ¤Ï·‚·Ó ıÂڷ›·
˘ÔηٿÛÙ·Û˘
ª. ¶··‰ÔÔ‡ÏÔ˘, ™. ¡ÙÔ˘Ì¿, ∫. ∫›ÙÛÈÔ˜, ¡. ∫·‰fiÁÏÔ˘, ∫. ∫ÒÛÙ·, π. ∆ÛÈÔ‡Ú˘
135 ªÂϤÙË ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ Û ·È‰È¿ ÌÂ
Ïԛ̈ÍË ·fi Èfi Epstein-Barr ηÈ
ÌÂÁ·ÏÔ΢ÙÙ·ÚÔ˚fi Î·È Û˘Û¯¤ÙÈÛË Ì ÙËÓ
ÎÏÈÓÈ΋ ¤Î‚·ÛË
∂. ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË, ∞. ºÏ¤‚·, µ. ∞ÓÙ¿ÚË,∞. ¶·˘Ï›ÙÔ˘-∆ÛÈfiÓÙÛË, ª. ªÔÛÎÔÊ›‰Ë˜, °. µ·ÚÏ¿Ì˘
141 ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ ÛÙ· ·È‰È¿:
ÂÌÂÈÚ›· 15 ÂÙÒÓ Û ¤Ó· ΤÓÙÚÔ
Ÿ. µÚ¿ÓË, ª. ¶·ÓÙÈΛ‰Ô˘, °. ÿÌ‚ÚÈÔ˜, π. •˘ÓÈ¿˜, µ. ¢ÂÌÂÚÙ˙›‰Ô˘, ∫. ∫¿ÓÙ˙ÈÔ˘, ∞. ª·˘ÚÔ˘‰‹, ¢. ∆·ÎÔ‡‰·˜, £. ¶··ÛÙ·‡ÚÔ˘, ∫. ™‡ÚÔÁÏÔ˘
148 √ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙˆÓ Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ
Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜, ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘
Ù‡Ô˘ C Î·È ÙÔ˘ Ó¢ÌÔÓÈfiÎÔÎÎÔ˘
µ. ∆ÛÈ¿ÓÙÔ˘, ∞. ∫·Úfi΢, ∂. ¶¿‚Ë, °. ∫˘ÚÈfiÔ˘ÏÔ˜
¶ƒ∞∫∆π∫√ £∂ª∞
157 ¢È·ÙÚÔÊ‹ ·È‰ÈÒÓ Î·È ÂÊ‹‚ˆÓ ÁÈ·
ÚÔ·ÁˆÁ‹ Ù˘ ̆ Á›·˜ Î·È Ù˘ ·Ó¿Ù˘Í˘ ηÈ
ÚfiÏË„Ë ÙˆÓ ̄ ÚfiÓÈˆÓ ÓÔÛËÌ¿ÙˆÓ
∞. ∫·Ê¿ÙÔ˜
∂¡¢π∞º∂ƒ√À™∞ ¶∂ƒπ¶∆ø™∏
162 Recurrent Respiratory Papillomatosis: case
report and literature review
D. A. Nunez
165 ∫§π¡π∫√ ∫√Àπ∑
¶. ™ËÊÈ·ÓÔ‡, ∫. ºˆÙ›Ô˘, ∫. ™ÎÈ·‰¿˜, ∫. ¶··Á·ÚÔ˘Ê¿Ï˘
∂¶I∫∞πƒ√ £Eª∞
166 ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ
™À¡∆√ª∞ ¶∞π¢π∞∆ƒπ∫∞ ¡∂∞
171 ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ 2008
E. °·Ï·Ó¿Î˘
¡∂∞ ∞¶√ ∆√ ¢π∞¢π∫∆À√
173 ™‡ÓÙÔÌ· ·È‰È·ÙÚÈο Ó¤· ÛÙÔ ‰È·‰›ÎÙ˘Ô
∫. ™ÙÂÊ·Ó›‰Ë˜
¶·È‰È·ÙÚÈ΋∆fiÌÔ˜ 71 ñ ∆‡¯Ô˜ 2 ñ ª¿ÚÙÈÔ˜-∞Ú›ÏÈÔ˜ 2008
∫ˆ‰ÈÎfi ̃¢È‡ı˘ÓÛË ̃∂ÔÙ›· ̃ªª∂: 3889
ISSN 0377-2551
Pediatri Mar-Apr 08 10-04-08 12:30 ™ÂÏ›‰·1
Bimonthly Publication of
the Greek Paediatric Society
President
A. Constantopoulos
Editorial Board
Editor-in-Chief
C. Stefanidis
Members
S. Andronikou
P. Augoustides-Savvopoulou
A. Vazeou-Gerasimidi
G. Varlamis
∂. Galanakis
L. Thomaidou
M. Kanariou
∂. Katsarou-Pectasides
A. Kattamis
S. Kitsiou-Tzeli
∞. Papadopoulou
N. Papadopoulos
A. Siamopoulou-Mavridou
M. Tsolia
Manuscript submission
e-mail: [email protected]
Instructions to authors:
http://www.e-child.gr/paediatriki/
iae.pdf
Manuscript Editing
Greek Editing
M. Natsoulidou
English Editing
S. Nakou
Publisher
K. Griveas
Publishing Coordinator
SCIENTIFIC PUBLICATIONS Ltd
1∞ Pierias St.
GR - 144 51, Metamorfossi
Tel.: +30 210 87 78 810
Fax: +30 210 87 78 822
Owner
Greek Paediatric Society©
92 Michalakopoulou St.
GR - 115 28, Athens
Tel.: +30 210 7771 140
+30 210 7771 663
Fax: +30 210 7758 354
e-mail: [email protected]
Annual Subscription
All foreign countries: US $ 50
Contents
REVIEW ARTICLES
87 Paediatric liver transplantation:
historical notes
G. C. Sotiropoulos, S. Nadalin, A. Radtke, H. Lang
92 Childhood obesity – ∞ public health crisis
across the European Union
A. J. Nicholson, S. Del Torso, A. Hadjipanyidis, D. Van Esso
96 Use of the new World Health Organization
growth standards in the prevention of
childhood overweight and obesity
M. Ponce-Rivera, D. Fuentes-Lugo
105 Basic techniques of molecular biology and
their applications in the diagnosis of
childhood diseases
S. Megremis, A. Pampanos
116 New aspects of infant nutrition
C. Costalos
123 Indications for administering growth
hormone to children and adolescents
E. Kousta, A. Papathanassiou, C. Hadjiathanassiou†
ORIGINAL ARTICLES
128 Final height of children with growth
hormone deficiency who received
replacement treatment
M. Papadopoulou, S. Douma, ∫. ∫itsios, ¡. ∫adoglou, ∫. ∫osta, π. Tsiouris
135 Study of the immunophenotype of
peripheral blood lymphocyte subsets in
children with Epstein-Barr virus and
cytomegalovirus infection: association
with outcome
∂. Papadopoulou-Alataki, ∞. Fleva, V. Antari, ∞. Pavlitou-∆siontsi, ª. Moskofidis, G. Varlamis
141 Liver transplantation in children:
15 years experience in one center
O. Vrani, ª. Pantikidou, G. Imvrios, π. Xinias, V. Demertzidou, ∫. ∫antziou, ∞. Mavroudi, D. Takoudas, T. Papastaurou, ∫. Spyroglou
148 Economic evaluation of new vaccines
against varicella, serogroup C
meningococcus and pneumococcus
V. ∆siantou, ∞. ∫arokis, ∂. Pavi, G. ∫yriopoulos
PRACTICAL ISSUE
157 Childhood and adolescent nutrition for
promoting health and growth and
preventing chronic diseases
∞. ∫afatos
CASE REPORT
162 Recurrent Respiratory Papillomatosis:
case report and literature review
D. A. Nunez
165 CLINICAL QUIZ
P. Sifianou, ∫. Fotiou, ∫. Skiadas, ∫. Papagaroufalis
CURRENT ISSUE
166 National Immunization Programme
PAEDIATRIC NEWS IN BRIEF
171 National Immunization Programme 2008
E. Galanakis
NEWS FROM THE INTERNET
173 Paediatric news in brief at the internet
C. Stefanidis
PaediatrikiVolume 71 ñ Number 2 ñ March-April 2008
Pediatri Mar-Apr 08 08-04-08 11:51 ™ÂÏ›‰·3

v™À¡∆∞∫∆π∫∏ E¶π∆ƒ√¶∏ EDITORIAL BOARD
ª¤ÏË Ù˘ ¢ÈÂıÓÔ‡˜ ™˘ÓÙ·ÎÙÈ΋˜ ∂ÈÙÚÔ‹˜ ñ Members of the International Editorial Board
¢È¢ı˘ÓÙ‹˜ ™‡ÓÙ·Í˘
∫ˆÓÛÙ·ÓÙ›ÓÔ˜ ™ÙÂÊ·Ó›‰Ë˜, ∞ı‹Ó·
∂ȉÈÎÔ› ™˘ÓÙ¿ÎÙ˜
™Ù¤ÏÏ· ∞Ó‰ÚfiÓÈÎÔ˘, ¡ÂÔÁÓÔÏÔÁ›·, πˆ¿ÓÓÈÓ·
¶ÂÚÛÂÊfiÓË ∞˘ÁÔ˘ÛÙ›‰Ô˘-™·‚‚ÔÔ‡ÏÔ˘, MÂÙ·‚ÔÏÈο ÓÔÛ‹Ì·Ù·,£ÂÛÛ·ÏÔÓ›ÎË
∞Ó‰ÚÈ·Ó‹ µ·˙·›Ô˘-°ÂÚ·ÛÈÌ›‰Ë, ∂Ó‰ÔÎÚÈÓÔÏÔÁ›·, ∞ı‹Ó·
°ÂÒÚÁÈÔ˜ µ·ÚÏ¿Ì˘, ∫·Ú‰ÈÔÏÔÁ›·, £ÂÛÛ·ÏÔÓ›ÎË
∂ÌÌ·ÓÔ˘‹Ï °·Ï·Ó¿Î˘, ∏ıÈ΋ Î·È ¢ÂÔÓÙÔÏÔÁ›·, ∏Ú¿ÎÏÂÈÔ
§ˆÚ¤ÙÙ· £ˆÌ·˚‰Ô˘, ∞Ó·Ù˘ÍȷΤ˜ ‰È·Ù·Ú·¯¤˜, ∞ı‹Ó·
ª·Ú›· ∫·Ó¿ÚÈÔ˘, ∞ÓÔÛÔÏÔÁ›·, ∞ı‹Ó·
∂˘ÛÙ·ı›· ∫·ÙÛ·ÚÔ‡-¶ÂÎÙ·Û›‰Ë, ¡Â˘ÚÔÏÔÁ›·, ∞ı‹Ó·
∞ÓÙÒÓ˘ ∫·ÙÙ¿Ì˘, ∞ÈÌ·ÙÔÏÔÁ›· - OÁÎÔÏÔÁ›·, ∞ı‹Ó·
™ÔÊ›· ∫›ÙÛÈÔ˘-∆˙¤ÏË, °ÂÓÂÙÈ΋, ∞ı‹Ó·
∞ÏÂÍ¿Ó‰Ú· ¶··‰ÔÔ‡ÏÔ˘, °·ÛÙÚÂÓÙÂÚÔÏÔÁ›· - ¢È·ÙÚÔÊ‹, ∞ı‹Ó·
¡ÈÎfiÏ·Ô˜ ¶··‰fiÔ˘ÏÔ˜, ∞ÏÏÂÚÁÈÔÏÔÁ›· - ¶Ó¢ÌÔÓÔÏÔÁ›·, ∞ı‹Ó·
∞ÓÙÈÁfiÓË ™È·ÌÔÔ‡ÏÔ˘-ª·˘Ú›‰Ô˘, ƒÂ˘Ì·ÙÔÏÔÁ›·, πˆ¿ÓÓÈÓ·
ª·Ú›˙· ∆ÛÔÏÈ¿, §ÔÈ̈ÍÈÔÏÔÁ›·, ∞ı‹Ó·
Editor-in-Chief
Constantinos Stefanidis, Athens
Section Editors
Stella Andronikou, Neonatology, Ioannina
Persefoni Avgoustides-Savvopoulou, Metabolic Disorders, Thessaloniki
Andriani Vazaiou-Gerasimidi, Endocrinology, Athens
George Varlamis, Cardiology, Thessaloniki
Emmanouil Galanakis, Ethics and Deontology, Heraklion
Loretta Thomaidou, Developmental Pediatrics, Athens
Maria Kanariou, Immunology, Athens
Eustathia Katsarou-Pektasides, Neurology, Athens
Antonis Kattamis, Haematology - √ncology, Athens
Sophia Kitsiou-Tzeli, Genetics, Athens
Alexandra Papadopoulou, Gastroenterology - Nutrition, Athens
Nicos Papadopoulos, Allergology - Pneumonology, Athens
Antigoni Siamopoulou-Mavridou, Rheumatology, Ioannina
Marisa Tsolia, Infectious Diseases, Athens
Alexis Arzimanoglou, Paris, France
Ellis D. Avner, Milwaukee, USA
Swati Bhave, New Delhi, India
Alberto Bissot, Panama, Panama
David Branski, Jerusalem, Israel
Francesco Chiarelli, Chieti, Italy
Chok-Wan Chan, Hong Kong, China
Denis Daneman, Toronto, Canada
Jochen Ehrich, Hannover, Germany
Demetrius Ellis, Pittsburgh, USA
Yoshikatsu Eto, Tokyo, Japan
Richard N. Fine, Stony Brook, USA
Margaret C. Fisher, Philadelphia, USA
Raif Geha, Boston, USA
Adenike Grange, Lagos, Nigeria
Judith G. Hall, Vancouver, Canada
Patricia Hamilton, London, UK
Enver Hasanoglu, Ankara, Turkey
Christer Holmberg, Helsinki, Finland
Lewis B. Holmes, Boston, USA
Peter Hoyer, Essen, Germany
Jan Janda, Prague, Czech Republic
Jan Kimpen, Ultrecht, Netherlands
Craig B. Langman, Chicago, USA
John Manis, Boston, USA
Manuel Moya, Alicante, Spain
Hugh O'Brodovich, Toronto, Canada
Ross Petty, Vancouver, Canada
Willem Proesmans, Leuven, Belgium
Jose Ramet, Antwerp, Belgium
Nikolai Shabalov, St. Petersburg, Russia
Alan Sinaiko, Minneapolis, USA
Nick J. Spencer, Coventry, UK
Alfred Tenore, Udine, Italy
Alkis Togias, Bethesda, USA
Eva Tsalikian, Iowa City, USA
Catherine Weil-Olivier, Paris, France
Max Zach, Graz, Austria
Zheng-Yan Zhao, Hangzhou, China
Johannes Zschocke, Heidelberg, Germany
Pediatri Mar-Apr 08 07-04-08 16:22 ™ÂÏ›‰·5

Paediatric liver transplantation: historical notes
G. C. Sotiropoulos1,2, S. Nadalin2, A. Radtke1,2, H. Lang1,2
Abstract: Liver transplantation (LT) is now a standard treatment for children with end-stage liver disease,with very good 1- and 5-year survival rates, which have been achieved through the constant improvementof surgical techniques and clinical management, and use of new immunosuppressive drugs. The indicationsfor LT in infants and children include acute liver failure, chronic liver failure with pruritus, complications ofcholestasis and failure to thrive. In young children the most common liver disease leading to transplantationis biliary atresia, which accounts for at least 50% of all LTs in children and is characterized by the failure ofthe bile ducts to develop normally and drain bile from the liver. Although the majority of transplanted chil-dren enjoy an excellent quality of life, there are still many possible complications, including short-term pri-mary non-function, vascular and biliary problems, bowel perforation, severe rejection, infection, hyperten-sion with long-term renal impairment, chronic rejection, de novo autoimmunity, lymphoproliferative diseaseand cancer, most of which are related to anti-rejection drug toxicity. This paper focuses on the historical de-velopment of surgical techniques in the era of paediatric LT.
Key words: Liver transplantation, paediatric transplant programme, split liver, living donor liver
transplantation, split techniques, liver insufficiency, liver failure, biliary atresia.
87∞¡∞™∫√¶∏™∏ REVIEW ARTICLE
1 Department of General,Abdominal and TransplantSurgery, University Hospital,Johannes GutenbergUniversity Mainz, Germany
2 Department of General,Visceral and TransplantationSurgery, University HospitalEssen, Germany
Correspondence:
Georgios C. [email protected] Klinik für Allgemein-,Abdominal- undTransplantationschirurgie, Klinikum der JohannesGutenberg Universität Mainz, Langenbeckstraße 1, 55131 Mainz, Germany
¶·È‰È·ÙÚÈ΋ 2008;71:87-91
Introduction
Paediatric liver transplantation (LT) is an es-
tablished method of treatment for patients with
end-stage liver failure. Its mortality has de-
creased dramatically since its first description,
thanks to new strategies for immunosuppres-
sion, new surgical techniques (1,2), and the im-
proved overall condition of the patients prior to
transplantation. The introduction of the split-
liver (SL) techniques has dramatically improved
the problem of organ shortage (3,4).
Full-Size LT
The first clinical attempt at liver replacement
was made by Starzl on March 1st, 1963 on a 3
year-old child who had developed end-stage liver
disease from biliary atresia, but “he bled to death
as we worked desperately to stop the haemor-
rhage. The operation could not be completed”
(5). This attempt was followed in 1963 by trans-
plantation of livers into four adult patients, who
all died from pulmonary embolism, after other-
wise successful transplants. Starzl performed the
next eight LTs in infants and children (6) all of
whom survived surgery, but four died after 2-6
months from sepsis. This series of fatal complica-
tions was attributed to inadequate immunosup-
pression, followed by rejection. Between March
1963 and July 1976, 111 LTs were performed at
the University of Colorado, but with a 1-year sur-
vival rate of only 28%. Such poor results were at-
tributed to technical and medical problems (80%)
and acute rejection (20%) (7). From July 1976 to
December 1977, following technical and diagnos-
tic improvements the paediatric 1-year survival
rate doubled from 34 to 62%. Based on these im-
proved results, the development of other LT cen-
tres was undertaken.
In Europe, the first attempt at LT was made on
a 10 month-old child with biliary atresia on June
6th, 1968 in Cambridge, UK, by Sir Roy Calne. As
with Starzl’s first attempt, the child died during
surgery. The first successful LT in Europe was per-
formed by Otte et al. on March 17th, 1971 on a 17
month-old boy with biliary atresia. The recovery
was uneventful until the child developed acute re-
jection, which was reversed by steroids, but he
died 7 weeks after transplantation from massive
intrathoracic bleeding caused by a liver biopsy
(8). Following this case, as in the USA, there was a
long-term moratorium before the LT programme
was finally resumed in 1984. The four children
transplanted that year are still alive, including the
first patient who received a reduced liver graft and
who is currently, worldwide, the longest survivor
with her original cut-down liver (9).
All the early LT patients were treated with a
drug regimen that had been developed for kid-
ney grafts, namely azathioprine and steroids,
sometimes with the addition of antilymphocyte
globulins. Because of inadequate immunosup-
pression, long-term survival was observed in less
than one third of patients. At the beginning of the
1980s, the introduction of cyclosporine led to a
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·87

significant increase of graft and patient survival rates.In March 1980, the liver trials with cyclosporine A im-munosuppression began in Denver. Twelve patientsentered the study between March and September1980, of whom 11 lived for one year or longer (10).
In October 1986 representatives of the eight cen-tres in Europe and the USA with experience of at least20 paediatric LTs (i.e., Boston, Brussels, Cambridge,Dallas, Hannover, Minneapolis, Pittsburgh and LosAngeles) met for an update on the status of paediatricLT: long-term (>1 year) patient survival had reached57-83%; all centres were using cyclosporine-basedprimary immunosuppression; the major indications -biliary atresia being the most frequent - were alreadyclearly delineated.
Since the implementation of LT for end-stage liverdisease there has been a strong disparity between organdemand and the cadaveric donor supply for children.This initially resulted in a pre-transplant mortality for
children on the waiting list for LT of around 25%,which was disproportionably high compared with thatof adult patients (11). The problem of size mismatchand the different epidemiology of paediatric donorshipand terminally diseased children were responsible forthe disparity (12). This stimulated the development oftechnical innovations, based on the segmental anatomyof the liver, which facilitated transplanting parts of alarge cadaveric donor liver into smaller recipients: i.e.reduced size LT, split LT and living donor LT.
Reduced size liver transplantation (RSLT)
The first step in solving the size mismatch prob-lem was the introduction of reduced-size techniques.With this approach, after harvesting the liver from acadaver donor, liver resection is performed on theback table to tailor the size of the graft to that of onesingle recipient. The remaining resected liver tissue isdiscarded. In paediatric RSLT either the left lateral
Figure 1b. Adult split liver transplantationRight versus left liver split for an adult recipient, 3-dimensionalreconstruction of the hepatic veins. The line of division lies exactlyover the MHV-middle hepatic vein (yellow). RHV-right hepaticvein (blue), LHV-left hepatic vein (red).
Figure 1c. Adult split liver transplantationLeft liver graft segments 1-4 for an adult recipient, 3-dimensionalreconstruction. The right-sided border of the MHV-middlehepatic vein (yellow) can be seen exposed on the transectionsurface. All tributaries from segments 5 and 8 are exposed at theirconfluence with the MHV trunk. RHV-right hepatic vein (blue),LHV-left hepatic vein (red).
88 G. C. Sotiropoulos et al.
Paediatriki 2008;71:87-91
Figure 1a. Adult split liver transplantationRight versus left liver split for an adult recipient, 3-dimensionalreconstruction. Right graft segments 5-8 (green), left graft segments1-4 (brown). RHV-right hepatic vein (blue), MHV-middle hepaticvein (yellow), LHV-left hepatic vein (red).
Figure 1d. Adult split liver transplantationRight liver graft segments 5-8 for an adult recipient, 3-dimensionalreconstruction. The left-sided border of the MHV-middle hepaticvein (yellow) can be seen exposed on the transection surface. Alltributaries from segments 4a and 4b are exposed at their confluencewith the MHV trunk. RHV-right hepatic vein (blue), LHV-lefthepatic vein (red).
Pediatri Mar-Apr 08 10-04-08 12:37 ™ÂÏ›‰·88

segment (Couinaud's segments II-III) or the full left
lobe (Couinaud's segments II-IV) is usually retained.
The technique as originally described by Bismuth and
Houssin (13) was validated in the late 1980s and later
became standard practice worldwide with 1-year sur-
vival rates of about 80% (14-18).
Although RSLT increases the number of paediatric
donor organs, it does not increase the total number of
organs available for LT, and indeed, it is actually dis-
advantageous to the adult recipient pool, which is
continuously growing (19).
Split liver transplantation (SLT)
The disadvantage of RSLT, namely, a discarded
liver segment, was solved by the introduction of split
liver techniques. SLT evolved from the RSLT and was
first described by Pichlmayr (20). This technique al-
lowed the preparation of two split grafts by dividing
all vascular and biliary structures and parenchyma for
the benefit of two recipients, one recipient receiving a
right lobe graft, and the other receiving either a left
lobe (segments 2-4, Figure 1) or left lateral segment
graft (segments 2-3, Figure 2). Usually the right lobe istransplanted into an adult and the left lobe or the leftlateral segment into a child. In 1989, Pichlmayr andcolleagues were the first to report the transplantationof one donor liver into two recipients (20,21). Thefirst series was reported by Broelsch and co-workers atthe University of Chicago (22) and in the early 1990sthe technique was further validated (23-25).
Technically, SLT is a complex procedure that canbe performed in two ways, ex situ or in situ, both ofwhich require precise knowledge of the liver anatomyand extensive experience with liver resection tech-niques and all the technical modalities of liver graftimplantation. Unfortunately, the wider application ofthe split technique is still hindered by the lack of ex-perience and unwillingness of some centres to splitevery suitable donor liver (26). Recent comprehensivestudies confirm that SLTs generally lead to lessfavourable results for individual recipients, but they
Figure 2d. Pediatric split liver transplantationRemnant liver (segments 1,4-8) including RHV-right hepatic vein(blue) and MHV-middle hepatic vein (yellow) after retrieval of a leftlateral liver graft (segments 2-3) including LHV-left hepatic vein(red) for a child, 3-dimensional reconstruction.
89Paediatric liver transplantation
¶·È‰È·ÙÚÈ΋ 2008;71:87-91
Figure 2b. Pediatric split liver transplantationLeft lateral liver split for a child, 3-dimensional reconstruction of thehepatic veins. The line of division lies exactly over the LHV-lefthepatic vein (red). Main tributaries of the MHV-middle hepaticvein (yellow) draining segments IVa/IVb in the remnant liver arepreserved. RHV-right hepatic vein (blue).
Figure 2c. Pediatric split liver transplantationLeft lateral graft (segments 2-3) including LHV-left hepatic vein(red) for a child, 3-dimensional reconstruction. RHV-right hepaticvein (blue), MHV-middle hepatic vein (yellow) remained with theremnant liver.
Figure 2a. Pediatric split liver transplantationLeft lateral liver split for a child, 3-dimensional reconstruction of thehepatic vein anatomy. Graft segments 2-3 (brown), remnantsegments 1,4-8 (green), RHV-right hepatic vein (blue), MHV-middle hepatic vein (yellow), LHV-left hepatic vein (red).
Pediatri Mar-Apr 08 10-04-08 12:37 ™ÂÏ›‰·89
also result in more individuals deriving the benefit of
LT. While initially holding great promise and being
adopted as standard policy by many paediatric trans-
plant centres, early experience demonstrated a higher
incidence of technical complications and decreased
graft and patient survival rates in recipients of right
lobe grafts. Unfortunately, relevant extensive, detailed
data on this issue are not yet available.
Living donor liver transplantation (LDLT)
The development of LDLT in the USA and Europe
has been driven by the shortage of donor organs in
spite of the use of innovative techniques for cadaveric
LT, such as RSLT and SLT (27). In Japan, where organ
procurement from brain-dead donors was not legal
until recently, LDLT was the only option.
LDLT was first reported by Raia et al. in two pa-
tients in 1989 (28). Both recipients died shortly after
the procedure of medical complications, but lived long
enough for the technical feasibility of the procedure to
be established. This was soon followed by a report
from Strong et al. in Australia, where the first success-
ful LT of a child using its mother's left lobe was per-
formed in July 1989 (29). Even before the initial re-
ports by Raia and Strong, an extensive ethical appraisal
of the concept of LDLT was in progress at the Univer-
sity of Chicago, where clinical ethicists and transplant
physicians convened a yearlong series of seminars and
discussions open to the entire university community
(30). The introduction of LDLT required a balance be-
tween the presumed benefits of an elective transplant
for the recipient and the risk of morbidity or even
mortality from LDLT for the donor. At the outset the
main ethical problems the Chicago group had to deal
with for the introduction of paediatric LDLT were the
principle of equipoise and the principle of coercion
(30,31). A proposal derived from these meetings was
submitted to the institutional review board and a suc-
cessful LDLT was performed in November 1989 by Dr.
Broelsch, who subsequently initiated the systematic
use of LDLT for children with end-stage liver disease
(32). Between November 1989 and July 1996, 100
LDLTs were performed, with 1-year patient and graft
survival rates of 88% and 72%, respectively. Similar re-
sults were reproduced worldwide, confirming the ef-
fectiveness of the procedure (33,34).
LDLT has several advantages for the child and for
the transplant population as a whole. First, it increases
the number of organs directly available for the paedi-
atric population. Second, most recipients receive their
transplants on an elective basis and thus should incur
lower morbidity and mortality rates and decreased
overall cost. Third, the minimal cold ischaemia time
and the use of healthy donors may contribute to theabsence of primary non-function. The application ofLDLT for children with end-stage liver disease had aprofound impact on organ waiting list times and de-creased waiting list mortality markedly (35). Paedi-atric LDLT is now accepted therapy for childrenthroughout the world and frequently accounts for50% or more of all paediatric LTs performed at re-gional referral centres (35).
Despite the impressive results of LDLT, consider-able debate persists concerning donor safety. Therisks to the donor include those associated with inva-sive pre-surgical testing and with the surgical proce-dure. These risks are accepted by the potential donorsin exchange for the knowledge that the child's life maybe saved without the uncertainty of the cadavericwaiting list. The most recent donor outcomes frommultiple centres have been excellent (36-38).
The development of segmental hepatic grafts hasexpanded the supply of size-appropriate organs, al-lowing children who otherwise would have died onthe waiting list the opportunity to undergo LT. Re-cently the association between graft type, recipient ageand graft survival has been better defined: amongchildren <3 years of age, LDLT provides superiorgraft survival compared to RLT and SLT. In olderchildren it appears that cadaveric organs may offer abetter outcome (39,40). While RLT and SLT graftsproduce an overall inferior outcome in the nationalexperience, they remain an important and necessarytool in paediatric centre armamentarium. They pro-vide appropriately sized grafts for children with nosuitable living donor and for those for whom no ca-daveric paediatric donor is available, and they canyield an excellent outcome in experienced centres. Itis apparent that the technical complexities and peri-operative events surrounding these procedures have asignificant impact on the outcome. This emphasizesthe importance of experience, attention to continuedtechnical refinement, and judicious selection of ap-propriate donors for specific recipients.
References
1. Kim JS, Grotelüschen R, Mueller T, Ganschow R, Bicak T,Wilms C, et al. Pediatric transplantation: the Hamburg ex-perience. Transplantation 2005;79:1206-1209.
2. Burdelski MM, Rogiers X. What lessons have we learned inpediatric liver transplantation? J Hepatol 2005;42:28-33.
3. Rogiers X, Malagfi M, Gawad K, Jauch KW, Olausson M,Knoefel WT, et al. In situ splitting of cadaveric livers. Theultimate expansion of a limited donor pool. Ann Surg1996;224:331-339.
4. Ringe B, Burdelski M, Rodeck B, Pichlmayr R. Experiencewith partial liver transplantation in Hannover. ClinTranspl 1990;4:135-144.
90 G. C. Sotiropoulos et al.
Paediatriki 2008;71:87-91
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·90

5. Starzl TE. The Puzzle People: Memoirs of a TransplantSurgeon. Pittsburgh, Pennsylvania: University of Pitts-burgh Press; 1992.
6. Starzl TE, Groth CG, Brettschneider L, Penn I, FulginitiVA, Moon JB, et al. Orthotopic homotransplantation ofthe human liver. Ann Surg 1968;168:392-415.
7. Starzl TE, Koep LJ, Halgrimson CG, Hood J, Schroter GP,Porter KA, et al. Fifteen years of clinical liver transplanta-tion. Gastroenterology 1979;77:375-388.
8. Otte JB. History of pediatric liver transplantation. Whereare we coming from? Where do we stand? Pediatr Trans-plant 2002;6:378-387.
9. Otte JB, de Ville de Goyet J, Sokal E, Alberti D, Moulin D,de Hemptinne B, et al. Size reduction of the donor liver is asafe way to alleviate the shortage of size-matched organs inpediatric liver transplantation. Ann Surg 1990;211:146-157.
10. Starzl TE, Klintmalm GB, Porter KA, Iwatsuki S, SchröterGP. Liver transplantation with use of cyclosporin a andprednisone. N Engl J Med 1981;305:266-269.
11. Malagfi M, Rogiers X, Broelsch CE. Reduced-size hepaticallografts. Annu Rev Med 1995;46:507-512.
12. Emond JC, Whitington PF, Thistlethwaite JR, Alonso EM,Broelsch CE. Reduced-size orthotopic liver transplanta-tion: use in the management of children with chronic liverdisease. Hepatology 1989;10:867-872.
13. Bismuth H, Houssin D. Reduced-sized orthotopic livergraft in hepatic transplantation in children. Surgery 1984;95:367-370.
14. Strong R, Ong TH, Pillay P, Wall D, Balderson G, Lynch S.A new method of segmental orthotopic liver transplanta-tion in children. Surgery 1988;104:104-107.
15. Broelsch CE, Emond JC, Thistlethwaite JR, Whitington PF,Zucker AR, Baker AL, et al. Liver transplantation, includ-ing the concept of reduced-size liver transplants in chil-dren. Ann Surg 1988;208:410-420.
16. Broelsch CE, Emond JC, Thistlethwaite JR, Rouch DA,Whitington PF, Lichtor JL. Liver transplantation with re-duced-size donor organs. Transplantation 1988;45:519-524.
17. Ringe B, Pichlmayr R, Burdelski M. A new technique of he-patic vein reconstruction in partial liver transplantation.Transpl Int 1988;1:30-35.
18. Ong TH, Lynch SV, Pillay SP, Balderson GA, Wall DR,Shepherd R, et al. Reduced-size orthotopic liver transplan-tation in children: an experience with seven cases. Trans-plant Proc 1989;21:2443-2444.
19. Busuttil RW, Goss JA. Split liver transplantation. Ann Surg1999;229:313-321.
20. Pichlmayr R, Ringe B, Gubernatis G, Hauss J, BunzendahlH. [Transplantation of a donor liver to 2 recipients (split-ting transplantation)--a new method in the further devel-opment of segmental liver transplantation]. LangenbecksArch Chir 1988;373:127-130.
21. Pichlmayr R, Bretschneider HJ, Kirchner E, Ringe B,Lamesch P, Gubernatis G, et al. [Ex situ operation on theliver. A new possibility in liver surgery]. Langenbecks ArchChir 1988;373:122-126.
22. Broelsch CE, Emond JC, Whitington PF, ThistlethwaiteJR, Baker AL, Lichtor JL. Application of reduced-size liv-er transplants as split grafts, auxiliary orthotopic grafts,and living related segmental transplants. Ann Surg 1990;212: 368-375.
23. Bismuth H, Morino M, Castaing D, Gillon MC, DescorpsDeclere A, Saliba F, et al. Emergency orthotopic liver trans-plantation in two patients using one donor liver. Br J Surg1989;76:722-724.
24. Otte JB, de Ville de Goyet J, Alberti D, Balladur P, deHemptinne B. The concept and technique of the split liverin clinical transplantation. Surgery 1990;107:605-612.
25. Otte JB, de Ville de Goyet J, Reding R, Van Obbergh L,Veyckemans F, Carlier MA, et al. Pediatric liver transplan-tation: from the full-size liver graft to reduced, split, andliving related liver transplantation. Pediatr Surg Int 1998;13:308-318.
26. Colledan M, Segalin A, Spada M, Lucianetti A, Corno V,Gridelli B. Liberal policy of split liver for pediatric livertransplantation. A single centre experience. Transpl Int2000;13:S131-133.
27. Trotter JF, Wachs M, Everson GT, Kam I. Adult-to-adulttransplantation of the right hepatic lobe from a livingdonor. N Engl J Med 2002;346:1074-1082.
28. Raia S, Nery JR, Mies S. Liver transplantation from livedonors. Lancet 1989;2:497.
29. Strong RW, Lynch SV, Ong TH, Matsunami H, Koido Y,Balderson GA. Successful liver transplantation from a liv-ing donor to her son. N Engl J Med 1990;322:1505-1507.
30. Singer PA, Siegler M, Whitington PF, Lantos JD, EmondJC, Thistlethwaite JR, et al. Ethics of liver transplantationwith living donors. N Engl J Med 1989;321:620-622.
31. Singer PA, Lantos JD, Whitington PF, Broelsch CE, SieglerM. Equipoise and the ethics of segmental liver transplanta-tion. Clin Res 1988;36:539-545.
32. Broelsch CE, Whitington PF, Emond JC, Heffron TG,Thistlethwaite JR, Stevens L, et al. Liver transplantation inchildren from living related donors. Surgical techniquesand results. Ann Surg 1991;214:428-437.
33. Reding R, de Goyet Jde V, Delbeke I, Sokal E, Jamart J,Janssen M, et al. Pediatric liver transplantation with cadav-eric or living related donors: comparative results in 90 elec-tive recipients of primary grafts. J Pediatr 1999;134: 280-286.
34. Inomata Y, Tanaka K, Uemoto S, Asonuma K, Egawa H,Kiuchi T, et al. Living donor liver transplantation: an 8-year experience with 379 consecutive cases. TransplantProc 1999;31:381.
35. Emond JC, Heffron TG, Kortz EO, Gonzalez-Vallina R,Contis JC, Black DD, et al. Improved results of living-relat-ed liver transplantation with routine application in a pedi-atric program. Transplantation 1993;55:835-840.
36. Renz JF, Roberts JP. Long-term complications of livingdonor liver transplantation. Liver Transpl 2000;6:S73-76.
37. Lo CM. Complications and long-term outcome of livingliver donors: a survey of 1,508 cases in five Asian centers.Transplantation 2003;75:S12-15.
38. Nadalin S, Heuer M, Wallot M, Auth M, Schaffer R,Sotiropoulos GC, et al. Paediatric acute liver failure andtransplantation: the University of Essen experience.Transpl Int. 2007;20:519-527.
39. Emond JC. Living donor liver transplantation in children:what to recommend? Am J Transplant 2004;4:293-294.
40. Abt PL, Rapaport-Kelz R, Desai NM, Frank A, Sonnad S,Rand E, et al. Survival among pediatric liver transplant re-cipients: impact of segmental grafts. Liver Transpl 2004;10:1287-1293.
91Paediatric liver transplantation
¶·È‰È·ÙÚÈ΋ 2008;71:87-91
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·91

92 ∞¡∞™∫√¶∏™∏ REVIEW ARTICLE
Paediatriki 2008;71:92-95
The definition of childhood obesity
The Body Mass Index (BMI) is the most prac-
tical measure of obesity and it is used in growth
monitoring to assess fatness. The BMI charts for
boys and girls (Tables 1 and 2) show the recom-
mended International Obesity Task Force cut-off
points for obesity and overweight in children. Th-
ese correspond to the adult definitions of over-
weight (BMI >25) and obesity (BMI >30) at age
18 years. Rapid changes in BMI can occur during
normal growth. The BMI is recommended as a
practical estimate of overweight in children and
adolescents, but it needs to be interpreted with
caution as it is not a direct measure of adiposity.
For epidemiological purposes overweight
should be defined as BMI greater than or equal to
the 85th centile of the 1990 reference data, and
obesity as BMI greater than or equal to the 95th
centile of the 1990 reference data.
The international epidemic of childhood
obesity
The definitions of overweight and obesity in
children differ between epidemiological studies,
making comparisons of cross-sectional data dif-ficult. The rates have increased threefold over 25years in the USA and fourfold over 18 years inEgypt (see the international childhood obesitymap) (1,2).
Consequences of childhood obesity
Childhood obesity is a multisystem diseasewith potentially devastating consequences. Itcauses hypertension, dyslipidaemia, increasedblood clotting tendency, endothelial dysfunctionand hyperinsulinism. Type 2 diabetes mellitus,once virtually unknown in adolescence, is largelyattributable to childhood obesity (4). A prediabet-ic state of glucose intolerance and insulin resis-tance appears to be highly prevalent among se-verely obese children irrespective of ethnic group.Type 2 diabetes is almost entirely attributable tothe childhood obesity epidemic, although heredi-tary and life-style factors affect individual risk.
Pulmonary complications include sleep-dis-ordered breathing (sleep apnoea), asthma andexercise intolerance. The development of exer-cise intolerance in an obese child can limit phys-ical activity and thus lead to further weight gain.
Childhood obesity – A public health crisis across the
European Union
A. J. Nicholson, S. Del Torso, A. Hadjipanyidis, D. Van Esso
Abstract: In the past, a fat child meant a healthy child, but in the last decade, excessive fatness or obesityhas become the primary paediatric health issue in the EU. It is known that some 10% of children are eitheroverweight or obese, and that obesity worldwide, apart from in sub-Saharan Africa, has reached epidemicproportions, with a threefold or more rise in most European countries since the 1980s (1,2,14,18). The maincauses of the obesity epidemic are clear - overeating, especially of foods rich in fats, extracted sugars orrefined starches, and a progressive decline in physical activity. The management of this epidemic dependson the successful motivation of people to eat less, to eat healthier foods and to exercise more, all of whichare difficult to achieve in societies where fruit and vegetables are less available than high-fat processedfoods, and where exercise no longer plays a regular part in most people’s lives. Management of childhoodobesity is time-consuming, frustrating, difficult and expensive (18). Adult obesity is the strongest predictorof childhood obesity; if both parents are obese, the chance of their child being obese increases tenfold.Breast feeding exerts a small protective effect against obesity. Television viewing is important, as it is knownthat for each additional hour of television watched at 5 years of age, the risk of adult obesity rises by 8%(7,8,18). Long-term increase or decrease in activity levels will influence whether a child becomes obese.Studies have implicated inactivity, with over 4 hours TV or computer use, and consumption of takeawayfoods more than twice weekly and fizzy drinks in the rising rates of obesity. Prevention of obesity will occuronly if there are fundamental changes in society, involving the production and availability of cheap healthyfoods, urban planning to ensure that people exercise more, education about eating, beginning in schools,and a global code to promote only healthy food and drink to children and adolescents. The vast majority ofobese children have primary obesity due to a disturbed energy balance. A very small percentage (5%) havea genetic cause for their obesity, and only very rarely are hormonal causes found.
Key words: Childhood obesity, epidemiology, management, prevention.
Primary / Secondary CareGroup of the EuropeanAcademy of Paediatrics
Correspondence:
Alf [email protected] Lady of Lourdes Hospital,Drogheda, Co. Louth, Ireland
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·92

93Childhood obesity
¶·È‰È·ÙÚÈ΋ 2008;71:92-95
Childhood obesity, of course, has substantial psy-chosocial consequences, and overweight children candevelop a negative self-image at as early as 5 years ofage, while obese adolescents show diminishing de-grees of self-esteem associated with sadness, loneli-ness and risk-taking behaviour (3,15).
Causes of childhood obesity
Genetic causes
In 1997, two massively obese Pakistani children ofconsanguineous parents were found to have a muta-tion in the gene encoding leptin and since then fivegenetic mutations causing obesity have been identi-fied, all presenting in childhood (5,6).
Prader-Willi syndrome (PWS) is a rare cause ofobesity, with a deletion of chromosome 15 and fea-tures of a voracious appetite, poor linear growth,small hands and genitalia and dysmorphic features.Progress has been made in mapping the genetic loci ofPWS but the molecular cause of this obesity syn-drome has not yet been identified.
Thus, single gene defects account for a very smallfraction of human obesity and predisposition to obe-sity appears to be related to a complex interaction be-tween at least 250 obesity-associated genes.
Physical activity
A lifestyle characterized by a lack of physical activ-ity and excessive television viewing has been shown tobe associated with childhood obesity. Among chil-dren from Mexico City, the risk of obesity decreasedby 10% for each hour of moderate to vigorous physi-cal activity and increased by 12% for each hour perday of television viewing.
Television viewing
Television viewing is thought to promote weightgain not only by displacing physical activity but alsoby increasing energy intake (7,8). Children tend topassively consume excessive amounts of energy-dense
foods while watching television. Furthermore, televi-
sion advertising could adversely influence dietary pat-
terns at other times throughout the day. Screen time
for children of over 2 years should be limited to no
more than 1 to 2 hours per day (18).
Diet
Children who were bottle fed appear to be at
greater risk of obesity later in childhood than those
who were breast fed (9).
Sugar-sweetened soft drinks have been the subject of
several studies, which have shown that the total energy
intake was 10% greater among children who consumed
soft drinks than in those who did not (18). Increasing
portion sizes are also a factor. Fast food typically incor-
porates potentially adverse dietary factors including sat-
urated fat, a high glycaemic index, high energy density
and, increasingly, large portion size. A large fast food
meal could contain 2,200 kcal, which, at 85 kcal per
mile, would require a full Marathon to burn off.
Breakfast skipping, snacking and eating out (in par-
ticular at fast food establishments) are all associated
with obesity (18). The ‘traffic light diet’, recommended
for consumption by children in the age-group 6 to 12
years, consists of low energy, high nutrient foods such
as fruit and vegetables (green), moderate energy foods
(orange) and high energy foods (red). ‘Green’ foods
may be eaten often, ‘orange’ foods in moderation and
‘red’ foods should be eaten sparingly (10,18).
Family factors
Parent-child interactions and the home environ-
ment can affect the risk of developing obesity. Tradi-
tional family meals tend to decrease television viewing
and improve dietary quality; the child takes a diet with
less saturated and trans fats, less fried foods, lower
glycaemic load, more fibre, fewer soft drinks and
more fruit and vegetables.
Table 2. Tests to be considered in obesity
Secondary causes of obesity are exceedingly rare; most obesityis what is termed simple obesity, and no investigations arerequired. - Short stature/hypertension/striae - morning and evening
cortisol levels (to exclude Cushings disease)- Short stature/goitre/hip pain - thyroid function tests , hip
X-ray to exclude slipped capital femoral epiphysis- Small hands and feet/voracious appetite - karyotype, FISH
(Prader-Willi syndrome)- Excessive thirst/increased urine output - fasting + 2 hour
blood sugar levels, glucose tolerance test (Diabetes)- Hirsutism/obesity/absence of periods - blood testosterone
level, ultrasound scan of ovaries showing numerous cysts(polycystic ovary syndrome)
Table 1. Complications of obesity
Short-term Long-term
Poor self-esteem/depression Persistence of obesityAsthma Social stigmatisation Sleep apnoea Sleep apnoeaType 2 diabetes mellitus Type 2 diabetes mellitusOrthopaedic problems Osteoarthritis(e.g. slipped epiphysis)Hypertension/ Hypertension/high cholesterol high cholesterolEarly puberty/ Menstrual irregularities/polycystic ovaries hirsutismGallstones Gallstones
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·93

Prevention and treatment
Prevention and treatment ultimately involves eat-
ing less and exercising more. Most efforts to reduce
obesity in children have used family-based or school-
based approaches and only in severe cases are phar-
macological and surgical treatments considered. Fol-
lowing a review of randomised controlled trials, Eb-
stein et al. (10) concluded, somewhat soberly, that
most interventions to treat childhood obesity are
marked by only small changes in weight or BMI and
very high rates of subsequent relapse.
School-based interventions have been oriented to-
wards prevention of obesity, targeting all children. The
Pathways programme (12), for American Indian chil-
dren at high risk of type 2 diabetes and cardiovascular
disease, aimed to reduce dietary fat consumption and
increase physical activity. This 3-year programme pro-
duced a significant decrease in fat consumption and a
trend towards increased physical activity but the BMI
did not differ between children in the intervention and
the control schools at the end of the programme. The
Planet Earth trial (11) focussed largely on changing the
school environment over two school years to include
reduced television viewing, increased physical activity,
decreased fat intake, increased fruit and vegetable in-
take, altered class curricula and extensive education of
families. In this trial there was a significant reduction
in obesity in girls (absolute risk 0.47, CI 0.24-0.93),
with trends in the same direction in boys, although not
reaching statistical significance. The authors reported
that the effect observed was largely attributable to ob-
served reductions in television viewing.
Most children managed in the community will have
simple obesity with no underlying medical cause and
without comorbidity. Treatment should be offered
when the obese child and family are willing to make the
necessary life-style changes. For children who are over-
weight and most children who are obese, weight main-
tenance is an acceptable goal (13). Weight maintenance
can only be achieved by sustained behavioural changes,
including healthier eating, an increase in physical activ-
ity to a minimum of 30 minutes per day and reduction
of physical inactivity (e.g., watching television or play-
ing computer games) to less than 2 hours per day. Par-
ticular attention should be given to methods for in-
creasing physical activity in adolescents (18).
Suggestions for parents
Suggestions for increasing physical activity:
- any increase in activity will help,
- aim for simple changes at first, such as walking,
cycling and using stairs rather than lifts,
- develop an active life-style for the whole family,
- encourage active play that is enjoyable and do all
you can to keep exercise fun,
- decrease TV viewing and other sedentary activities,
- schedule unstructured free playtime on a daily
basis.
Dietary suggestions:
- a balanced, varied diet for the whole family,
- serve meals at regular times; avoid ‘grazing’ and
TV snacks,
- serve smaller portions,
- avoid snacks as rewards or treats,
- offer healthy snacks (e.g., fruit) as alternatives to
sweets, chocolates, potato crisps, biscuits and cakes,
- use less energy dense food (e.g., semi-skimmed
milks and low fat spreads),
- provide whole foods that take time to eat (e.g.,
fruits and wholemeal bread),
- promote low calorie drinks (preferably water),
- ensure at least five portions of fruit and vegeta-
bles per day,
- grill, boil or bake foods rather than frying them,
- “Eat to live, don’t live to eat”,
- pare down the amount of ‘junk’ food in the house,
- comfort with attention, listening and hugs in-
stead of food.
The perfect meal plan
Modern families may rarely sit down to a meal
all together, and one major suggestion is to bring
back the traditional family meal; the perfect meal
plan entails:
- firstly turn off the TV,
- involve children in the cooking process,
- switch mobile phones to silent,
- make sure that everyone sits down together at the
table,
- serve the plates from a central location to ensure
control over portion sizes,
- the meal should last at least 20 minutes,
- share the positive events of the day,
- be mindful while eating of the colour, texture
and smell of the food,
- make dessert a continuation of the meal and not
something too special,
- substitute fruit for dessert at times,
- parents, not children, should be responsible for
food decision making,
- limit soft drink consumption.
Drug treatment for obesity
Drug treatment is not recommended for chil-
dren under 12 years, and in adolescence it is only
94 A. J. Nicholson et al.
Paediatriki 2008;71:92-95
Pediatri Mar-Apr 08 09-04-08 10:36 ™ÂÏ›‰·94

95Childhood obesity
¶·È‰È·ÙÚÈ΋ 2008;71:92-95
recommended in situations where there are medicalcomplications (orthopaedic complications or sleep ap-noea) or severe psychological issues arising from theobesity. Medication used as part of a structured life-stylemodification produces an average weight loss of 5 to10%, which typically reaches a plateau at 4 to 6 monthsof treatment, and weight regain is common after thedrug is withdrawn (16,18). Prescribing should be madeby a specialist multidisciplinary team. The drugs usedare orlistat and sibutramine and they are generally usedfor a 6-12 month trial with regular reviews of effective-ness, adverse effects and adherence. Sibutramine is anappetite suppressant and orlistat works as a reversible li-pase inhibitor (18). Drug treatment may be used to helpthe adolescent maintain weight loss as well as to contin-ue to lose weight. Four experimental drugs have pro-duced weight loss in small studies involving childrenwith special conditions, specifically, metformin in obeseadolescents with insulin resistance, octeotride for hypo-thalamic obesity, growth hormone in Prader-Willi syn-drome and leptin for congenital leptin deficiency (17).
Bariatric surgery for obesity
Surgery is generally not recommended for chil-dren and adolescents and constitutes, at best, a last re-sort for severely obese adolescents. Exceptional cir-cumstances in which surgery might be considered arewhen the BMI is >40, or when in the case of a signifi-cant complication, such as hypertension or type 2 di-abetes that could be improved by weight loss, all ap-propriate non-surgical measures have failed or whenthey are receiving intensive care.
Key points to remember
- Obesity is now the commonest chronic condi-tion affecting children across the EU.
- Obesity is due to an imbalance between energyconsumption and energy expenditure. Obese childrendo not have low energy needs.
- Family support is necessary for treatment tosucceed.
- Generally the aim of treatment is to help childrenand adolescents to maintain their weight.
- In younger children the main impact of obesity issocial and emotional rather than medical.
- A medical cause for obesity is more likely in chil-dren who are both short and obese for age.
- Most children are not obese because of an under-lying medical problem, but rather as a result of theirlife-style.
- Weight reduction or stabilization goals shouldalways be kept reasonable.
- The major calorie culprits are high-fat fast food,large portions and sugar-containing soft drinks.
- If a child is at risk of obesity due to family histo-
ry, the earlier the modifications (e.g., reducing TV
time) the better.
References
1. Strauss RS, Pollack HA. Epidemic increase in childhood
overweight, 1986-1998. JAMA 2001;286:2845-2848.
2. Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity:
public-health crisis, common sense cure. Lancet 2002;360:
473-482.
3. Strauss RS. Childhood obesity and self-esteem. Paediatrics
2000;105:e15.
4. Sinha R, Fisch G, Teague B, Tamborlane WV, Banyas B,
Allen K, et al. Prevalence of impaired glucose tolerance
among children and adolescents with marked obesity. N
Eng J Med 2002;346:802-810.
5. Montague CT, Farooqi IS, Whitehead JP, Soos MA, Rau H,
Wareham NJ, et al. Congenital leptin deficiency is associat-
ed with severe early-onset obesity in humans. Nature 1997;
387:903-908.
6. Farooqi IS, O’Rahilly S. Recent advances in the genetics of
severe childhood obesity. Arch Dis Child 2000;83:31-34.
7. Robinson TN. Does television cause childhood obesity?
JAMA 1998;279: 959-960.
8. Robinson TN. Reducing children’s television viewing to
prevent obesity: a randomized controlled trial. JAMA
1999;282:1561-1567.
9. Ludwig DS, Peterson KE, Gortmaker SL. Causes of obesity.
Lancet 2001;357:1978-1979.
10. Epstein LH, Roemmich JN, Raynor HA. Behavioral thera-
py in the treatment of pediatric obesity. Pediatr Clin North
Am 2001;48:981-993.
11. Sahota P, Rudolf MC, Dixey R, Hill AJ, Barth JH, Cade J.
Randomised controlled trial of primary school based inter-
vention to reduce risk factors for obesity. BMJ 2001;323:
1029-1032.
12. Lohman TG, Going S, Stewart D, et al. The effect of Path-
ways obesity prevention study on body composition in
American children. FASEB J 2001;15:A1093.
13. Summerbell CD, Ashton V, Campbell KJ, Edmunds L, Kel-
ly S, Waters E. Interventions for treating obesity in chil-
dren. Cochrane Database Syst Rev 2003;(3):CD001872.
14. Wiegand S, Maikowski U, Blankenstein O, Biebermann H,
Tarnow P, Grüters A. Type 2 diabetes and impaired glu-
cose tolerance in European children and adolescents with
obesity - a problem that is no longer restricted to minority
groups. Eur J Endocrinol 2004;151:199-206.
15. Sabin MA, Ford AL, Holly JM, Hunt LP, Crowne EC,
Shield JP. Characterisation of morbidity in a UK, hospital
based, obesity clinic. Arch Dis Child 2006;91:126-130.
16. Glazer G. Long-term pharmacotherapy of obesity 2000: a
review of efficacy and safety. Arch Intern Med 2001;161:
1814-1824.
17. Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham
CH, Prentice AM, et al. Effects of recombinant leptin ther-
apy in a child with congenital leptin deficiency. N Eng J
Med 1999;341:879-884.
18. Spear BA, Barlow SE, Ervin C, Ludwig DS, Saelens BE,
Schetzina KE, et al. Recommendations for treatment of
child and adolescent overweight and obesity. Pediatrics
2007;120:S254-S288.
Pediatri Mar-Apr 08 09-04-08 10:36 ™ÂÏ›‰·95

96 ∞¡∞™∫√¶∏™∏ REVIEW ARTICLE
Paediatriki 2008;71:96-104
Use of the new World Health Organization growth standards
in the prevention of childhood overweight and obesity
M. Ponce-Rivera, D. Fuentes-Lugo
Abstract: The prevalence of overweight and obesity in young children continues to rise in most parts ofthe world. Obese children have a significantly higher risk of becoming obese adults, which underlinesthe importance of adequate growth monitoring from early ages. Different international references forgrowth assessment are currently being used by paediatricians in most countries. This review examinesthe differences between the Centers for Disease Control (CDC) growth reference and the new WorldHealth Organization (WHO) growth standards for children of less than five years when used asdiagnostic tools for the detection of excess weight. It also includes preliminary results from aretrospective study conducted in a cohort of 300 healthy children from a paediatric clinic in Mexicoevaluating differences in overweight prevalence depending on the growth reference employed. Resultsshowed a higher prevalence of overweight and obesity with WHO standards than with the CDCreference in children from 1 through 5 years of age, independent of gender, in agreement with otherstudies. Use of the new WHO growth standards is emphatically encouraged for both routine clinicalpractice and epidemiological research, in order to avoid potential pitfalls and inaccuracies whenmonitoring child growth and to detect childhood overweight and obesity effectively. The new WHOstandards provide a unique opportunity for redesigning child overweight surveillance and preventionprogrammes so that they become more useful for detection and decision making and less complicatedfor gathering epidemiological data.
Key words: Childhood obesity, childhood overweight, growth reference, growth standard.
Facultad de Ciencias de laSalud, UniversidadAutonoma del Carmen,Ciudad del Carmen,Campeche, Mexico
Correspondence:
Daniel [email protected] de Ciencias de la Salud,Universidad Autonoma del Carmen,Ciudad del Carmen, Mexico
Childhood globesity: understanding the
magnitude of the problem
Overweight and obesity have achieved global
acknowledgement during the past decade. Excess
body weight is now considered one of the most
important risk factors contributing to the overall
burden of disease. Worldwide, around 1.2 billion
adults are classified as being overweight, of which
312 million are considered obese (1). The preva-
lence of obesity has reached alarming levels, affect-
ing both developed and developing countries and
all socioeconomic groups, irrespective of age, sex
or ethnicity. If effective preventive measures are
not implemented soon, this public health problem
will continue to expand to the extent that it will be-
come out of control. For example, it is estimated
that in the US by 2015, 75% of adults will be over-
weight, of which more than half will be obese (2).
Concerning childhood obesity, around 10%
of children in the world have some degree of
overweight and over 22 million children under
the age of 5 are already obese (3). The prevalence
of overweight is dramatically higher in the eco-
nomically developed regions, but it is also rising
significantly in most other parts of the world. In
developing nations, childhood obesity is most
prevalent in the wealthier sections of the popula-
tion. However, it is also increasing among the ur-
ban poor in these countries, possibly due to their
exposure to westernized diets. The prevalence of
childhood overweight in America is currently
above 20%, reaching up to 40% in the case of the
US and Mexico. In Europe, the number of chil-
dren who are overweight is expected to rise by 1.3
million children per year, with more than
300,000 of them becoming obese each year (4).
By 2010 it is estimated that 26 million children in
European countries will be overweight, including
6.4 million who will be obese (5). Such rapid
changes in the numbers of obese children within
a relatively stable population indicate that genet-
ic factors are not the primary reason for change,
although they play a role that is yet to be precise-
ly determined.
Childhood obesity is usually associated with
complications that include diabetes types 1 and 2
(6,7), insulin resistance, atherosclerosis (8,9),
hypertension, dyslipidaemia, polycystic ovary
disease, kidney disease (10) and fatty liver
among many others (11). Children with body
mass index (BMI) and waist circumference ex-
ceeding the established normal values are at in-
creased risk for metabolic syndrome when they
reach adulthood (12,13). A higher BMI during
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·96

97Prevention of childhood overweight and obesity
¶·È‰È·ÙÚÈ΋ 2008;71:96-104
childhood is also associated with an increased risk for
coronary heart disease (CHD) in adulthood (14) and
this association appears to be stronger in boys than in
girls and to increase with age in both sexes (15).
In addition, excess body weight appears to be an
important risk factor for some cancers. A systematic
review compared associations between 20 cancer types
and BMI (16). Their results show that a higher BMI is
associated with an increased risk of thyroid, renal and
colon cancers, oesophageal adenocarcinoma, multiple
myeloma, leukaemia and non-Hodgkin lymphoma in
both sexes, rectal cancer and malignant melanoma in
men, and gallbladder, pancreas, endometrial and post-
menopausal breast cancers in women.
Several theories have been formulated to account
for the obesity epidemic. Clearly, the main causes are
overeating and lack of physical activity. However, it is
of paramount importance to identify all the risk factors
that predispose an individual to become obese (17).
There appears to be a direct causal relationship be-
tween childhood overweight and maternal pre-preg-
nancy body size, maternal smoking during pregnancy
(18), early weaning (19), rapid growth (20) and chil-
dren’s use of television and media, while breastfeeding
appears to have a protective effect against overweight
(21). Further studies are needed to elucidate the exact
mechanisms by which these factors influence child-
hood adiposity, for example, its relationship with so-
cioeconomic status (22). Some authors have claimed
that, although clinically irrelevant, temperament may
be slightly related to overweight and rapid early weight
gain in infants (23). Others have proposed that a high
early protein intake, particularly from dairy products,
increases obesity risk (24,25). Some studies suggest that
sleep deprivation may influence weight through effects
on appetite, physical activity, and thermoregulation
(26). Short sleep duration appears independently asso-
ciated with weight gain in younger age groups (27).
Unfortunately, to date, scientific evidence regarding
risk factors for childhood obesity is still insufficient,
with much of the literature being of limited quality, in-
conclusive and contradictory (28).
There is strong evidence to suggest a direct rela-
tionship between weight status in childhood and
eventual adult obesity, but many studies are based on
cross-sectional data or have relatively long periods of
time between measurements. It is now accepted that
obesity in adolescence is highly predictive of obesity
in adulthood. Therefore, an important next step will
be to identify those young children at greatest risk of
developing obesity in adolescence, and to intervene
before chronic overweight is established during early
childhood. Children who are found to be overweight
at least once at ages 24, 36 or 54 months during the
preschool period are 5 times more likely to be over-
weight at age 12 years than those who are below the
85th percentile for BMI at all three of the preschool
ages. The longer a child remains in the lower range of
normal BMI, the less likelihood there is that the child
will become overweight by early adolescence (29).
Adequate detection of overweight and
obesity in childhood
Not long ago, a fat child meant a healthy child, and
the concept of “bigger is better” was widely accepted by
parents, paediatricians and caregivers. Such a point of
view belongs to the past, however (30), and at present,
child obesity is one of the most evident, yet most ne-
glected public health problems in the world. Although
the problem is well recognized, most obesity preven-
tion measures worldwide have been small, timid and
ineffective to halt the epidemic (31). Arguably, ‘globe-
sity’ might have been detectable earlier if a prescriptive
reference had been available 20 years ago, and even
now the first problem that needs to be addressed is
agreement of a definition of true obesity. Some of the
contradictory childhood obesity rates seen in the liter-
ature are a direct consequence of using different crite-
ria to define overweight and obesity. The main pur-
poses for defining overweight and obesity are to pre-
dict health risks and to provide comparisons between
populations. For practical reasons, the definitions have
usually been based on anthropometry, but regardless of
which definition is used, the increasing rates have high-
lighted the relevance of the problem (32).
Obesity is defined as an excess of body fat or adipose
tissue. It is actually fat and not weight which is associat-
ed with all the comorbid conditions. Measuring fat is
not as straightforward as measuring weight; therefore
weight, rather than adiposity, is the usual clinical mark-
er for identifying obesity. Although body weight tends
to be associated with adiposity, weight alone is an insuf-
ficient measure of obesity by itself, because it is correlat-
ed with height (33). To avoid this limitation, a number
of measures of weight in relation to height have been
devised over the years. The simplest and most frequent-
ly used are weight-for-height and the BMI.
BMI is a practical indirect measure of adiposity, al-
though the relationship changes according to age, sex
and ethnicity, but also degree of fatness. A child’s BMI
can be compared with a reference data set and be con-
verted into a Z-score. A BMI Z-score of 0 is equivalent
to the median or 50th percentile value, a Z-score of
+2.00 is approximately equivalent to the 98th per-
centile and a Z-score of +2.85 is >99th percentile.
Some authors postulate that even though BMI Z-score
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·97

98 M. Ponce-Rivera, D. Fuentes-Lugo
Paediatriki 2008;71:96-104
is optimal for assessing adiposity on a single occasion,
it is not necessarily the best scale for measuring change
in adiposity, as the within-child variability over time
depends on the child’s level of adiposity (34).
Use of BMI index charts during a paediatric health
supervision visit increases physician recognition of
overweight patients better than height-for-weight
charts (35). Regrettably, BMI charts are not routinely
used (36) and due to ineffective detection not all chil-
dren with overweight receive either a formal diagnosis
or treatment (37). A study conducted among public
and private practice paediatricians in the US revealed
that they identified overweight in only 27% of children
with BMI at the 85th-94.9th percentile and up to 86%
with a BMI at or above the 95th percentile (38). Rate
recognition by physicians increased as the severity of
obesity increased. US paediatricians may not use BMI
charts because they recognize obesity empirically when
they see it, at least when the BMI is above the 95th per-
centile. However, they may overlook excess weight in
children with BMI at the 85th-94th percentile, perhaps
because these children seem fairly normal.
Adequate growth and weight gain should concern
not only paediatricians and child caretakers but also
parents (39). One study showed that parents of
younger children were significantly more likely to un-
derestimate overweight (65%) than parents of adoles-
cents (51%). Overweight parents were not more like-
ly to underestimate weight, nor was accuracy associat-
ed with parental education or socieconomic status.
Parental recognition of childhood overweight may be
improved with BMI screening and feedback (40).
Growth references versus growth standards:
which should be used?
Growth references are a fundamental tool for the
interpretation of anthropometric data. Classifying a
child as overweight or obese assumes that such a child
is comparable to the reference population, so choos-
ing the right tool for proper detection is mandatory
(41). In the US, reference growth charts based on na-
tionally representative surveys have been produced
since 1977. An expert committee recommended their
use for children and adolescents, with the 95th BMI
percentile for age and sex (or BMI 30 kg/m2) as the
cutoff points for overweight and the 85th percentile as
“at risk of overweight” for screening purposes. The
fact that the committee decided not to use the term
‘obese’, which they associated with excess fat rather
than weight, has lead to some confusion (42).
In May 2000 the US Centers for Disease Control
(CDC) released new growth charts to replace the 1977
NCHS reference. The CDC-2000 charts were based
on five nationally representative surveys conducted
between 1963 and 1994. This reference, currently
used in about 100 countries, is based on data from
several samples of children from a single country and
suffers from a number of technical drawbacks that
makes it inadequate for monitoring growth in early
childhood. A survey reported that CDC-2000 is the
growth reference most commonly used worldwide.
Another interesting fact from this international study
is that most paediatricians prefer using percentiles
rather than Z-scores (43). The use of Z-scores offers
advantages over the use of percentiles; for instance,
when conducting epidemiological studies, Z-scores
allow easier comparison between growth references.
In the late 1990s, the International Obesity Task
Force (IOTF) determined that although BMI was not
ideal as a measure of adiposity, it could be used to de-
fine overweight and obesity in children and adoles-
cents. IOTF recommended cutoff points based on
age-specific values that project to the adult cutoff
points of 25 kg/m2 for overweight and 30 kg/m2 for
obesity. Using data collected between 1963 and 1993
from six different populations (Great Britain, Brazil,
the Netherlands, Hong Kong, Singapore and USA)
IOTF published their reference curves in 2000 (44).
These are useful mainly for epidemiological research,
since children and adolescents can only be categorized
as non-overweight or overweight/obese. Since the
adult cutoff points of BMI 25 and 30 may not be uni-
versally applicable, the IOTF curves are inappropriate
for some child populations. A number of reports have
shown that these cutoff points substantially underes-
timate the prevalence of childhood obesity in differ-
ent settings (45). In short, the IOTF reference appears
to be a less adequate tool for detecting overweight and
obesity in clinical practice compared with methods
based on percentiles or Z-scores.
WHO 2006 Child Growth Standards
The WHO 2006 Child Growth Standards are the
product of a long systematic process which started in
the early 1990s. They are based for the first time on a
prospective, prescriptive, international sample of in-
fants selected to represent optimum growth (46). The
WHO Multicenter Growth Reference Study (MGRS)
was designed to provide data that describe how chil-
dren should grow from birth to five years under opti-
mal environmental conditions, rather than describing
their growth in a particular time and place, and there-
fore, they can be applied to all children everywhere,
regardless of ethnicity, socioeconomic status and type
of feeding (47).
The MGRS was carried out from July 1997 to
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·98
December 2003 as a population-based study coveringthe cities of Davis, California, USA; Muscat, Oman;Oslo, Norway; and Pelotas, Brazil, together with se-lected affluent neighborhoods of Accra, Ghana andSouth Delhi, India. The WHO combined a longitudi-nal follow-up from birth to 24 months with a cross-sectional component of children aged 18-71 months.The study population lived under socioeconomicconditions favourable to growth. The individual in-clusion criteria were: no known health or environ-mental constraints to growth, mothers willing to fol-low MGRS feeding recommendations (exclusive orpredominant breast-feeding for at least 4 months, in-troduction of complementary foods by 6 months ofage, and continued breast-feeding to at least 12months of age), no maternal smoking before and afterdelivery, single term birth and absence of significantmorbidity (48). Prior to their release, the standardswere field-tested in four countries: Argentina, Italy,Maldives and Pakistan (49).
One important feature of the WHO standards tobear in mind is that it makes breast-feeding the bio-logical norm and establishes the breast-fed infant asthe normative growth model (50). The previous refer-ences were based mostly on the growth pattern of ar-tificially-fed children. The WHO-2006 standardsdemonstrate that healthy children from around theworld who are raised in healthy environments andfollow recommended feeding practices have similarpatterns of growth. This indicates that the same po-tential for growth should be expected in any country.It also implies that deviations from this ideal growthpattern must be assumed to reflect adverse conditionsthat require correction (51).
Since there are substantial differences in methodol-ogy, cutoff values and selected population between thevarious growth references, it is expected that signifi-cant changes would be found when one reference iscompared to another, even if they are from the samecountry. For instance, the CDC-2000 reference under-
estimates the weight-for-height Z-scores of individual
children compared to the 1977 NCHS reference, both
of which are references derived from American chil-
dren. A child classified as close to +3 Z-score using the
1977 NCHS reference will be just below +2 Z-score
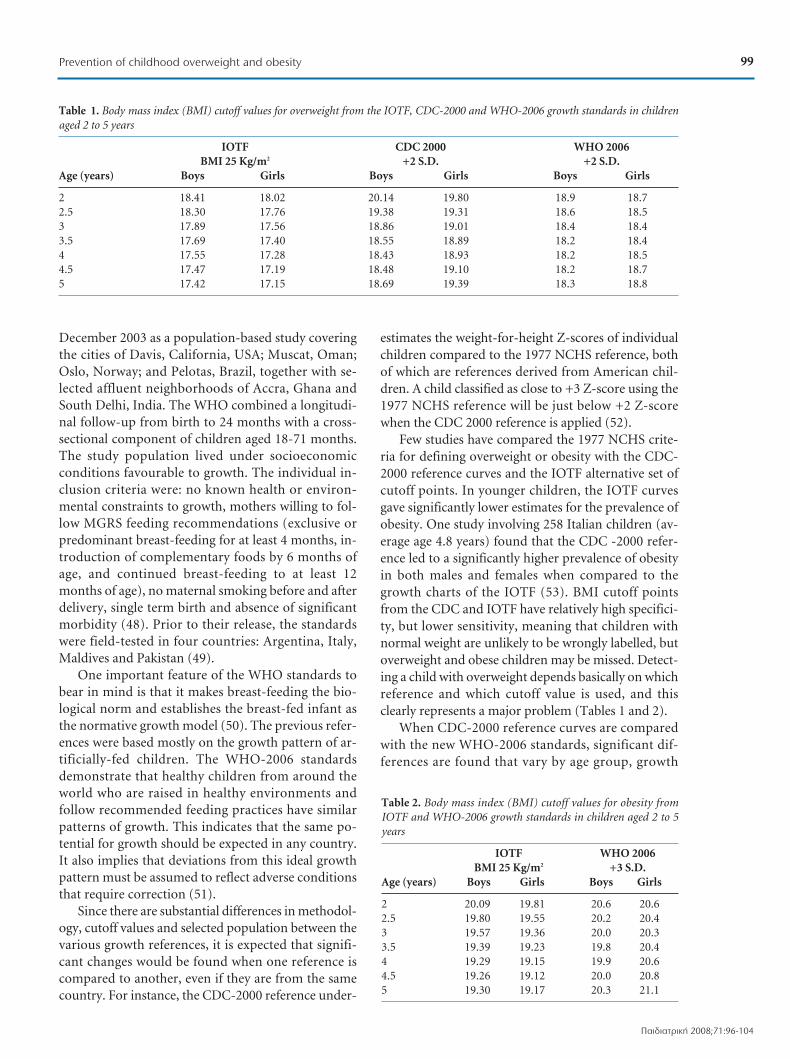
when the CDC 2000 reference is applied (52).
Few studies have compared the 1977 NCHS crite-
ria for defining overweight or obesity with the CDC-
2000 reference curves and the IOTF alternative set of
cutoff points. In younger children, the IOTF curves
gave significantly lower estimates for the prevalence of
obesity. One study involving 258 Italian children (av-
erage age 4.8 years) found that the CDC -2000 refer-
ence led to a significantly higher prevalence of obesity
in both males and females when compared to the
growth charts of the IOTF (53). BMI cutoff points
from the CDC and IOTF have relatively high specifici-
ty, but lower sensitivity, meaning that children with
normal weight are unlikely to be wrongly labelled, but
overweight and obese children may be missed. Detect-
ing a child with overweight depends basically on which
reference and which cutoff value is used, and this
clearly represents a major problem (Tables 1 and 2).
When CDC-2000 reference curves are compared
with the new WHO-2006 standards, significant dif-
ferences are found that vary by age group, growth
Table 2. Body mass index (BMI) cutoff values for obesity fromIOTF and WHO-2006 growth standards in children aged 2 to 5years
IOTF WHO 2006BMI 25 Kg/m2 +3 S.D.
Age (years) Boys Girls Boys Girls
2 20.09 19.81 20.6 20.62.5 19.80 19.55 20.2 20.43 19.57 19.36 20.0 20.33.5 19.39 19.23 19.8 20.44 19.29 19.15 19.9 20.64.5 19.26 19.12 20.0 20.85 19.30 19.17 20.3 21.1
99Prevention of childhood overweight and obesity
¶·È‰È·ÙÚÈ΋ 2008;71:96-104
Table 1. Body mass index (BMI) cutoff values for overweight from the IOTF, CDC-2000 and WHO-2006 growth standards in childrenaged 2 to 5 years
IOTF CDC 2000 WHO 2006BMI 25 Kg/m2 +2 S.D. +2 S.D.
Age (years) Boys Girls Boys Girls Boys Girls
2 18.41 18.02 20.14 19.80 18.9 18.72.5 18.30 17.76 19.38 19.31 18.6 18.53 17.89 17.56 18.86 19.01 18.4 18.43.5 17.69 17.40 18.55 18.89 18.2 18.44 17.55 17.28 18.43 18.93 18.2 18.54.5 17.47 17.19 18.48 19.10 18.2 18.75 17.42 17.15 18.69 19.39 18.3 18.8
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·99
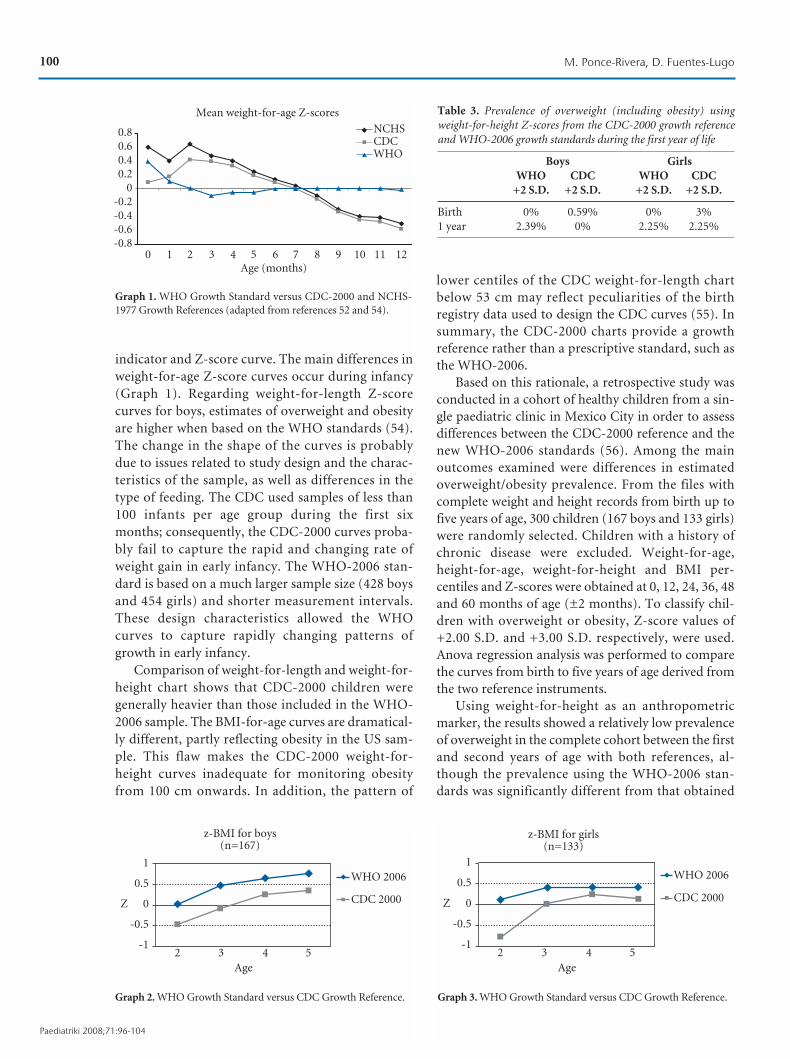
indicator and Z-score curve. The main differences in
weight-for-age Z-score curves occur during infancy
(Graph 1). Regarding weight-for-length Z-score
curves for boys, estimates of overweight and obesity
are higher when based on the WHO standards (54).
The change in the shape of the curves is probably
due to issues related to study design and the charac-
teristics of the sample, as well as differences in the
type of feeding. The CDC used samples of less than
100 infants per age group during the first six
months; consequently, the CDC-2000 curves proba-
bly fail to capture the rapid and changing rate of
weight gain in early infancy. The WHO-2006 stan-
dard is based on a much larger sample size (428 boys
and 454 girls) and shorter measurement intervals.
These design characteristics allowed the WHO
curves to capture rapidly changing patterns of
growth in early infancy.
Comparison of weight-for-length and weight-for-
height chart shows that CDC-2000 children were
generally heavier than those included in the WHO-
2006 sample. The BMI-for-age curves are dramatical-
ly different, partly reflecting obesity in the US sam-
ple. This flaw makes the CDC-2000 weight-for-
height curves inadequate for monitoring obesity
from 100 cm onwards. In addition, the pattern of
lower centiles of the CDC weight-for-length chart
below 53 cm may reflect peculiarities of the birth
registry data used to design the CDC curves (55). In
summary, the CDC-2000 charts provide a growth
reference rather than a prescriptive standard, such as
the WHO-2006.
Based on this rationale, a retrospective study was
conducted in a cohort of healthy children from a sin-
gle paediatric clinic in Mexico City in order to assess
differences between the CDC-2000 reference and the
new WHO-2006 standards (56). Among the main
outcomes examined were differences in estimated
overweight/obesity prevalence. From the files with
complete weight and height records from birth up to
five years of age, 300 children (167 boys and 133 girls)
were randomly selected. Children with a history of
chronic disease were excluded. Weight-for-age,
height-for-age, weight-for-height and BMI per-
centiles and Z-scores were obtained at 0, 12, 24, 36, 48
and 60 months of age (±2 months). To classify chil-
dren with overweight or obesity, Z-score values of
+2.00 S.D. and +3.00 S.D. respectively, were used.
Anova regression analysis was performed to compare
the curves from birth to five years of age derived from
the two reference instruments.
Using weight-for-height as an anthropometric
marker, the results showed a relatively low prevalence
of overweight in the complete cohort between the first
and second years of age with both references, al-
though the prevalence using the WHO-2006 stan-
dards was significantly different from that obtained
z-BMI for girls(n=133)
Age
2 3 4 5
Z
1
0.5
0
-0.5
-1
WHO 2006
CDC 2000
Graph 3. WHO Growth Standard versus CDC Growth Reference.
z-BMI for boys(n=167)
Age
2 3 4 5
Z
1
0.5
0
-0.5
-1
WHO 2006
CDC 2000
Graph 2. WHO Growth Standard versus CDC Growth Reference.
Table 3. Prevalence of overweight (including obesity) usingweight-for-height Z-scores from the CDC-2000 growth referenceand WHO-2006 growth standards during the first year of life
Boys GirlsWHO CDC WHO CDC
+2 S.D. +2 S.D. +2 S.D. +2 S.D.
Birth 0% 0.59% 0% 3%1 year 2.39% 0% 2.25% 2.25%
100 M. Ponce-Rivera, D. Fuentes-Lugo
Paediatriki 2008;71:96-104
0.80.60.40.2
0-0.2-0.4-0.6-0.8
0 1 2 3 4 5 6 7 8 9 10 11 12Age (months)
Mean weight-for-age Z-scores
NCHSCDCWHO
Graph 1. WHO Growth Standard versus CDC-2000 and NCHS-1977 Growth References (adapted from references 52 and 54).
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·100

101Prevention of childhood overweight and obesity
¶·È‰È·ÙÚÈ΋ 2008;71:96-104
with the CDC-2000 reference (1.33% versus 0.66%
overweight). The main differences in the weight-for-
height Z-score were observed from 12 to 36 months of
age. At 1 year of age, differences were found for the
boys but not the girls (Table 3). The prevalence of
overweight increased markedly at age 4-5, but with
significant differences between CDC and WHO
scores regardless of gender.
It was not possible to compare Z-BMI curves be-
tween the two references during the first two years be-
cause such data is not included in the CDC-2000
growth curves. When BMI Z-score was used to iden-
tify overweight (+2.0) and obesity (+3.0), there were
statistically significant differences between the two
references (p<0.001) for both boys and girls from 2 to
5 years of age. Although the median values of the BMI
Z-score were within the normal weight range with
both references, the WHO-2006 curve pattern was al-
ways above the CDC curve pattern for both boys and
girls from age 2 years to 5 years (Graphs 2 and 3). In
addition, the prevalence of overweight and obesity us-
ing WHO standards was higher than the prevalence
found when CDC growth references were used
(Graphs 4 and 5). Furthermore, as pointed out else-
where, the weight-for-height Z-score proved to be of
lesser sensitivity in detecting overweight accurately
when compared to the BMI Z-score, with both refer-
ences (p<0.001).
Final comments
The shift to the new WHO standards provides a
unique opportunity not only to monitor linear
growth, but also to redesign surveillance programmes
so that they are more useful for problem detection
and decision making, and less complicated for gather-
ing epidemiological data (57). The WHO standards
would set a markedly lower standard for weight gain
beyond 4 months of age, and could thus support ef-
forts to avoid future childhood obesity (58). Howev-
er, there is evidence that they might not be appropri-
ate for use across all populations, and specifically
some populations in Asia (59) and Africa (60). One
study conducted in refugee camps in Algeria, Kenya
and Bangladesh showed important differences in the
weight-for-height cutoff points used for defining
acute malnutrition between those obtained from the
WHO standards and those derived from the NCHS
reference. The WHO standards apparently resulted in
a higher measured prevalence of severe acute malnu-
trition. For such reasons, assessment of the new WHO
growth standards in different populations and envi-
ronments is recommended. Compared to previous
international references they appear to be more accu-
rate and easier to interpret. In addition, last year
WHO published a second set of standards that in-
clude head circumference-for-age, arm circumfer-
ence-for-age, triceps and subscapular skinfold-for-
age, and new international growth standards for the
screening, surveillance and monitoring of school-age
children and adolescents (61-63), all available at the
WHO website.
Prevention is perhaps the only effective way to stop
this childhood obesity epidemic, and the first step for
proper prevention, is proper detection. The WHO
2006 standards were created basically for that purpose.
The authors agree with others who suggest that all the
demographic surveys should now be derived using the
Table 4. Prevalence of overweight (including obesity) using bodymass index (BMI) Z-scores from the CDC-2000 growth referenceand WHO-2006 growth standards
Age Boys Girls(years) WHO CDC WHO CDC
2 3.58% 0% 3% 0.75%3 7.77% 4.18% 6.76% 4.50%4 11.97% 7.77% 5.26% 4.50%5 11.36% 8.97% 6.76% 3.75%
WHO 2006CDC 2000
Age (years)2 3 4 5
12
10
8
6
4
2
0
%
Graph 4. Prevalence of overweight/obesity in boys (BMI Z-score=/>2.0) (n=167).
WHO 2006CDC 2000
Age (years)2 3 4 5
7
6
5
4
3
2
1
0
%
Graph 5. Prevalence of overweight/obesity in girls (BMI Z-score=/>2.0) (n=133).
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·101

WHO standards (64). Perhaps in the future techno-logical advances will allow a more direct assessment ofadiposity than BMI, and new charts will need to becreated (65). Currently, there are few reports in theliterature of studies assessing the level of body fat inchildhood (66-68) and only one that has actually pro-duced body fat reference curves for children aged old-er than five (69).
There is a marked mismatch between the publichealth importance of childhood obesity and thenumber and quality of studies conducted so far toassess preventive interventions (70,71). There is anurgent need for well-designed intervention studiesto demonstrate the long-term effectiveness of pre-ventive strategies that would provide a basis for evi-dence-based recommendations (72,73). In Europe, aseries of initiatives and actions have been launchedin recent years, one of which is the creation of na-tional centres for collecting country-specific data toback up concrete strategies for future policy building(74). In the US, the new National Children’s Studywill seek information on enviromental risks and in-dividual susceptibility factors for obesity, amongother diseases. This will be conducted in a cohort of100,000 US born children, which will be followedfrom conception to 21 years of age. Environmentalexposures will be assessed repeatedly during preg-nancy and throughout childhood in the children’shomes, schools and communities. Chemical assayswill be performed by the CDC and banks of biologi-cal and genetic material and environmental sampleswill be collected. Recruitment started in 2007 at 7sites and will be extended to 105 sites across the US(75). Unfortunately, it will be a long time before pre-liminary results are available. In the meantime, untilall these studies start to answer some of the numer-ous questions regarding childhood obesity, it wouldbe advisable to promote physical activity and healthyeating habits among children and to encourage ade-quate monitoring of growth and weight gain fromearly infancy.
References
1. Maziak W, Ward KD, Stockton MB. Childhood obesity:are we missing the big picture? Obes Rev 2008;9:35-42.
2. Wang Y, Beydoun MA. The obesity epidemic in the UnitedStates-gender, age, socioeconomic, racial/ethnic, and geo-graphic characteristics: a systematic review and meta-re-gression analysis. Epidemiol Rev 2007;29:6-28.
3. Wang Y, Lobstein T. Worldwide trends in childhood over-weight and obesity. Int J Pediatr Obes 2006;1:11-25.
4. Jackson-Leach R, Lobstein T. Estimated burden of paedi-atric obesity and co-morbidities in Europe. Part 1. The in-crease in the prevalence of child obesity in Europe is itselfincreasing. Int J Pediatr Obes 2006;1:26-32.
5. Kosti RI, Panagiotakos DB. The epidemic of obesity in
children and adolescents in the world. Cent Eur J Public
Health 2006;14:151-159.
6. Knip M, Reunanen A, Virtanen SM, Nuutinen M, Viikari J,
Akerblom HK. Does the secular increase in body mass in
children contribute to the increasing incidence of type 1
diabetes? Pediatr Diabetes 2008 [Epub ahead of print].
7. Jones KL. Role of obesity in complicating and confusing
the diagnosis and treatment of diabetes in children. Pedi-
atrics 2008;121:361-368.
8. Freedman DS, Patel DA, Srinivasan SR, Chen W, Tang R,
Bond MG, et al. The contribution of childhood obesity to
adult carotid intima-media thickness: the Bogalusa Heart
Study. Int J Obes (Lond) 2008 [Epub ahead of print].
9. Beauloye V, Zech F, Tran HT, Clapuyt P, Maes M, Brichard
SM. Determinants of early atherosclerosis in obese children
and adolescents. J Clin Endocrinol Metab 2007;92:3025-3032.
10. Wang Y, Chen X, Klag MJ, Caballero B. Epidemic of child-
hood obesity: implications for kidney disease. Adv Chron-
ic Kidney Dis 2006;13:336-351.
11. Nathan BM, Moran A. Metabolic complications of obesity
in childhood and adolescence: more than just diabetes.
Curr Opin Endocrinol Diabetes Obes 2008;15:21-29.
12. Sun SS, Liang R, Huang TT, Daniels SR, Arslanian S, Liu K,
et al. Childhood obesity predicts adult metabolic syndrome:
the Fels Longitudinal Study. J Pediatr 2008;152:191-200.
13. Morrison JA, Friedman LA, Wang P, Glueck CJ. Metabolic
syndrome in childhood predicts adult metabolic syndrome
and type 2 diabetes mellitus 25 to 30 years later. J Pediatr
2008;152:201-206.
14. Celermajer DS, Ayer JG. Childhood risk factors for adult
cardiovascular disease and primary prevention in child-
hood. Heart 2006;92:1701-1706.
15. Baker JL, Olsen LW, So/rensen TI. Childhood body-mass
index and the risk of coronary heart disease in adulthood.
N Engl J Med 2007;357:2329-2337.
16. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M.
Body-mass index and incidence of cancer: a systematic re-
view and meta-analysis of prospective observational stud-
ies. Lancet 2008;371:569-578.
17. Reilly JJ, Ness AR, Sherriff A. Epidemiological and physio-
logical approaches to understanding the etiology of pedi-
atric obesity: finding the needle in the haystack. Pediatr Res
2007;61:646-652.
18. Oken E, Levitan EB, Gillman MW. Maternal smoking dur-
ing pregnancy and child overweight: systematic review and
meta-analysis. Int J Obes (Lond) 2008;32:201-210.
19. Sloan S, Gildea A, Stewart M, Sneddon H, Iwaniec D. Ear-
ly weaning is related to weight and rate of weight gain in in-
fancy. Child Care Health Dev 2008;34:59-64.
20. Monteiro PO, Victora CG. Rapid growth in infancy and
childhood and obesity in later life--a systematic review.
Obes Rev 2005;6:143-154.
21. Buyken AE, Karaolis-Danckert N, Remer T, Bolzenius K,
Landsberg B, Kroke A. Effects of breastfeeding on trajecto-
ries of body fat and BMI throughout childhood. Obesity
(Silver Spring) 2008;16:389-395.
22. Shrewsbury V, Wardle J. Socioeconomic status and adipos-
ity in childhood: a systematic review of cross-sectional stud-
ies 1990-2005. Obesity (Silver Spring) 2008;16:275-284.
23. Niegel S, Ystrom E, Vollrath ME. Is difficult tempera-
ment related to overweight and rapid early weight gain in
102 M. Ponce-Rivera, D. Fuentes-Lugo
Paediatriki 2008;71:96-104
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·102

103Prevention of childhood overweight and obesity
¶·È‰È·ÙÚÈ΋ 2008;71:96-104
infants? A prospective cohort study. J Dev Behav Pediatr
2007;28: 462-466.
24. Ong KK, Emmett PM, Noble S, Ness A, Dunger DB;
ALSPAC Study Team. Dietary energy intake at the age of 4
months predicts postnatal weight gain and childhood body
mass index. Pediatrics 2006;117:e503-e508.
25. Günther AL, Remer T, Kroke A, Buyken AE. Early protein
intake and later obesity risk: which protein sources at
which time points throughout infancy and childhood are
important for body mass index and body fat percentage at
7 y of age? Am J Clin Nutr 2007;86:1765-1772.
26. Al Mamun A, Lawlor DA, Cramb S, O'Callaghan M, Wil-
liams G, Najman J. Do childhood sleeping problems predict
obesity in young adulthood? Evidence from a prospective
birth cohort study. Am J Epidemiol 2007;166:1368-1373.
27. Chen X, Beydoun MA, Wang Y. Is sleep duration associat-
ed with childhood obesity? A systematic review and meta-
analysis. Obesity (Silver Spring) 2008;16:265-274.
28. Hawkins SS, Law C. A review of risk factors for overweight
in preschool children: a policy perspective. Int J Pediatr
Obes 2006;1:195-209.
29. Nader PR, O'Brien M, Houts R, Bradley R, Belsky J, Cros-
noe R, et al. Identifying risk for obesity in early childhood.
Pediatrics 2006;118:e594-e601.
30. Weaver LT. Rapid growth in infancy: balancing the interests
of the child. J Pediatr Gastroenterol Nutr 2006;43:428-432.
31. Wofford LG. Systematic review of childhood obesity pre-
vention. J Pediatr Nurs 2008;23:5-19.
32. Sweeting HN. Measurement and definitions of obesity in
childhood and adolescence: a field guide for the uninitiat-
ed. Nutr J 2007;6:32.
33. De Onis M. The use of anthropometry in the prevention of
childhood overweight and obesity. Int J Obes Relat Metab
Disord 2004;28:S81-S85.
34. Cole TJ, Faith MS, Pietrobelli A, Heo M. What is the best
measure of adiposity change in growing children: BMI,
BMI %, BMI z-score or BMI centile? Eur J Clin Nutr 2005;
59:419-425.
35. Gilbert MJ, Fleming MF. Use of enhanced body mass index
charts during the pediatric health supervision visit increas-
es physician recognition of overweight patients. Clin Pedi-
atr (Phila) 2007;46:689-697.
36. Perrin EM, Flower KB, Ammerman AS. Body mass index
charts: useful yet underused. J Pediatr 2004;144:455-460.
37. Dorsey KB, Wells C, Krumholz HM, Concato JC. Diagno-
sis, evaluation, and treatment of childhood obesity in pedi-
atric practice. Arch Pediatr Adolesc Med 2005;159:632-638.
38. Barlow SE, Bobra SR, Elliott MB, Brownson RC, Haire-
Joshu D. Recognition of childhood overweight during
health supervision visits: Does BMI help pediatricians?
Obesity (Silver Spring) 2007;15:225-232.
39. Golan M. Parents as agents of change in childhood obesity-
-from research to practice. Int J Pediatr Obes 2006;1:66-76.
40. West DS, Raczynski JM, Phillips MM, Bursac Z, Heath
Gauss C, Montgomery BE. Parental Recognition of Over-
weight in School-age Children. Obesity (Silver Spring)
2008;16:630-636.
41. Ogden CL. Defining overweight in children using growth
charts. Md Med 2004;5:19-21.
42. Wang Y, Moreno LA, Caballero B, Cole TJ. Limitations of the
current world health organization growth references for chil-
dren and adolescents. Food Nutr Bull 2006;27:S175-S188.
43. De Onis M, Wijnhoven TM, Onyango AW. Worldwide
practices in child growth monitoring. J Pediatr 2004;144:
461-465.
44. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a
standard definition for child overweight and obesity world-
wide: international survey. BMJ 2000;320:1240-1243.
45. Serra-Majem L, Ribas-Barba L, Pérez-Rodrigo C, Ngo J,
Aranceta J. Methodological limitations in measuring child-
hood and adolescent obesity and overweight in epidemio-
logical studies: does overweight fare better than obesity?
Public Health Nutr 2007;10:1112-1120.
46. De Onis M, Garza C, Victora CG, Onyango AW, Frongillo
EA, Martines J. The WHO Multicentre Growth Reference
Study: planning, study design, and methodology. Food
Nutr Bull 2004;25:S15-S26.
47. WHO Multicentre Growth Reference Study Group. Relia-
bility of anthropometric measurements in the WHO Mul-
ticentre Growth Reference Study. Acta Paediatr Suppl
2006;450:38-46.
48. WHO Multicentre Growth Reference Study Group. WHO
Child Growth Standards based on length/height, weight
and age. Acta Paediatr Suppl 2006;450:76-85.
49. Onyango AW, de Onis M, Caroli M, Shah U, Sguassero Y,
Redondo N, et al. Field-testing the WHO child growth
standards in four countries. J Nutr 2007;137:149-152.
50. WHO Multicentre Growth Reference Study Group.
Breastfeeding in the WHO Multicentre Growth Reference
Study. Acta Paediatr Suppl 2006;450:16-26.
51. Garza C. New growth standards for the 21st century: a pre-
scriptive approach. Nutr Rev 2006;64:S55-S59.
52. De Onis M, Onyango AW. The Centers for Disease Con-
trol and Prevention 2000 growth charts and the growth of
breastfed infants. Acta Paediatr 2003;92:413-419.
53. Vidal E, Carlin E, Driul D, Tomat M, Tenore A. A compar-
ison study of the prevalence of overweight and obese Ital-
ian preschool children using different reference standards.
Eur J Pediatr 2006;165:696-700.
54. De Onis M, Garza C, Onyango AW, Borghi E. Comparison
of the WHO child growth standards and the CDC 2000
growth charts. J Nutr 2007;137:144-148.
55. De Onis M, Onyango AW, Borghi E, Garza C, Yang H;
WHO Multicentre Growth Reference Study Group. Com-
parison of the World Health Organization (WHO) Child
Growth Standards and the National Center for Health
Statistics/WHO international growth reference: implica-
tions for child health programmes. Public Health Nutr
2006;9:942-947.
56. Ponce M, Blanco A, Reyes H, Lfipez C, Fuentes D. Utilidad
de las nueva curvas de crecimiento de la OMS para la de-
teccifin del sobrepeso y obesidad en nin~os menores de cin-
co an~os. Pediaãtrika 2007;27(4):48.
57. Garza C, de Onis M. Rationale for developing a new inter-
national growth reference. Food Nutr Bull 2004; 25:S5-S14.
58. Wright C, Lakshman R, Emmett P, Ong K. Implications of
adopting the WHO 2006 Child Growth Standard in the
UK: two prospective cohort studies. Arch Dis Child 2007
[Epub ahead of print].
59. Hui LL, Schooling CM, Cowling BJ, Leung SS, Lam TH,
Leung GM. Are universal standards for optimal infant
growth appropriate? Evidence from a Hong Kong Chinese
birth cohort. Arch Dis Child 2007 [Epub ahead of print].
60. Seal A, Kerac M. Operational implications of using 2006
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·103

World Health Organization growth standards in nutritionprogrammes: secondary data analysis. BMJ 2007;334:733.
61. Butte NF, Garza C, de Onis M. Evaluation of the feasibilityof international growth standards for school-aged childrenand adolescents. J Nutr 2007;137:153-157.
62. De Onis M, Onyango AW, Borghi E, Siyam A, Nishida C,Siekmann J. Development of a WHO growth reference forschool-aged children and adolescents. Bull World HealthOrgan 2007;85:660-667.
63. Butte NE, Garza C, de Onis M. Evaluation of the feasibilityof international growth standards for school-aged childrenand adolescents. Food Nutr Bull 2006;27:S169-S174.
64. Deshmukh PR, Dongre AR, Gupta SS, Garg BS. Newly de-veloped WHO growth standards: implications for demo-graphic surveys and child health programs. Indian J Pedia-tr 2007;74:987-990.
65. Wells JC, Fewtrell MS. Is body composition important forpaediatricians? Arch Dis Child 2008;93:168-172.
66. Williams J, Wake M, Campbell M. Comparing estimates ofbody fat in children using published bioelectrical imped-ance analysis equations. Int J Pediatr Obes 2007;2:174-179.
67. Burdette HL, Whitaker RC, Hall WC, Daniels SR. Breast-feeding, introduction of complementary foods, and adi-posity at 5 y of age. Am J Clin Nutr 2006;83:550-558.
68. Cleary J, Daniells S, Okely AD, Batterham M, Nicholls J.Predictive validity of four bioelectrical impedance equa-tions in determining percent fat mass in overweight andobese children. J Am Diet Assoc 2008;108:136-139.
69. McCarthy HD, Cole TJ, Fry T, Jebb SA, Prentice AM. Bodyfat reference curves for children. Int J Obes (Lond) 2006;30:598-602.
70. Isganaitis E, Levitsky LL. Preventing childhood obesity: canwe do it? Curr Opin Endocrinol Diabetes Obes 2008;15:1-8.
71. Davis MM, Gance-Cleveland B, Hassink S, Johnson R, Par-adis G, Resnicow K. Recommendations for prevention ofchildhood obesity. Pediatrics 2007;120:S229-S253.
72. Connelly JB, Duaso MJ, Butler G. A systematic review ofcontrolled trials of interventions to prevent childhood obe-sity and overweight: a realistic synthesis of the evidence.Public Health 2007;121:510-517.
73. Barlow SE; Expert Committee. Expert committee recom-mendations regarding the prevention, assessment, andtreatment of child and adolescent overweight and obesity:summary report. Pediatrics 2007;120:S164-S192.
74. Fussenegger D, Pietrobelli A, Widhalm K. Childhood obesi-ty: political developments in Europe and related perspectivesfor future action on prevention. Obes Rev 2008;9:76-82.
75. Landrigan PJ, Trasande L, Thorpe LE, Gwynn C, Lioy PJ,D'Alton ME, et al. The National Children's Study: a 21-yearprospective study of 100,000 American children. Pediatrics2006;118:2173-2186.
104 M. Ponce-Rivera, D. Fuentes-Lugo
Paediatriki 2008;71:96-104
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·104

105∞¡∞™∫√¶∏™∏ REVIEW ARTICLE
¶·È‰È·ÙÚÈ΋ 2008;71:105-115
™˘ÓÙÔÌÔÁڷʛ˜:
PCR Polymerase Chain ReactiondNTP diNucleotideTriPhosphataseddNTP didiNucleotideTriPhosphataseQRT PCR Quantitative Real Time PCRRFLP Restriction Fragment Length
PolymorphismVNTR Variable Number Tandem RepeatSTR Short Tandem RepeatDHPLC Denaturant High Performance Liquid
Chromatography
∂ÈÛ·ÁˆÁ‹ - πÛÙÔÚÈ΋ ∞Ó·‰ÚÔÌ‹
∏ °ÂÓÂÙÈ΋ ‚·Û›˙ÂÙ·È ÛÙȘ ÁÓÒÛÂȘ Ù˘ π·-ÙÚÈ΋˜ Î·È Ù˘ µÈÔÏÔÁ›·˜ Î·È ÂȯÂÈÚ› Ó· ‰Ò-ÛÂÈ ··ÓÙ‹ÛÂȘ Û ÂÚˆÙ‹Ì·Ù· fiÛÔÓ ·ÊÔÚ¿
ÙÔ˘˜ Ì˯·ÓÈÛÌÔ‡˜ Ù˘ ÎÏËÚÔÓÔÌÈÎfiÙËÙ·˜ ηÈ
Ù˘ ‚ÈÔÔÈÎÈÏfiÙËÙ·˜. √ fiÚÔ˜ ÁÂÓÂÙÈ΋ ¯ÚËÛÈ-
ÌÔÔÈ‹ıËÎÂ ÁÈ· ÚÒÙË ÊÔÚ¿ ·fi ÙÔÓ ÕÁÁÏÔ
ÁÂÓÂÙÈÛÙ‹ Bateson ÙÔ 1905 (1). ∂›ÛËÌ·, ·Ù¤-
Ú·˜ Ù˘ ÁÂÓÂÙÈ΋˜ ıˆÚÂ›Ù·È Ô ªendel, Ô ÔÔ›-
Ô˜ ÙÔ 1865 ‰È·Ù‡ˆÛ ÙÔ˘˜ ÓfiÌÔ˘˜ Ô˘ ʤ-
ÚÔ˘Ó ÙÔ fiÓÔÌ¿ ÙÔ˘ (2). ∏ ·Ï‹ıÂÈ·, fï˜, ›ӷÈ
fiÙÈ ÙÔ ˙‹ÙËÌ· Ù˘ ÌÂÙ·‚›‚·Û˘ ¯·Ú·ÎÙËÚÈÛÙÈ-
ÎÒÓ ·fi ÁÂÓÈ¿ Û ÁÂÓÈ¿ ¤¯ÂÈ ··Û¯ÔÏ‹ÛÂÈ ÙÔÓ
¿ÓıÚˆÔ ·fi ÙËÓ ·Ú¯·ÈfiÙËÙ·. °È· ·Ú¿‰ÂÈÁ-
Ì·, ÔÈ ·Ú¯·›ÔÈ µ·‚˘ÏÒÓÈÔÈ ÁÓÒÚÈ˙·Ó fiÙÈ ÁÈ· Ó·
·Ú·¯ı› ηÚfi˜ Û ÊÔÈÓÈÎfi‰ÂÓÙÚ· ¤Ú ӷ
ÌÂÙ·ÊÂÚı› Á‡ÚË ·fi ¿ÚÚÂÓ· Ê˘Ù¿ ÛÙÔ˘˜ ‡Â-
ÚÔ˘˜ ÙˆÓ ıËÏ˘ÎÒÓ Ê˘ÙÒÓ (1). ™ÙËÓ ·Ú¯·›·
µ·ÛÈΤ˜ Ù¯ÓÈΤ˜ Ù˘ ÌÔÚȷ΋˜ ‚ÈÔÏÔÁ›·˜ Î·È Ë ÂÊ·ÚÌÔÁ‹
ÙÔ˘˜ ÛÙË ‰È¿ÁÓˆÛË ·È‰È·ÙÚÈÎÒÓ ÓÔÛËÌ¿ÙˆÓ
™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
¶ÂÚ›ÏË„Ë: OÈ Ù¯ÓÈΤ˜ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÛÙË ÌÔÚȷ΋ ‚ÈÔÏÔÁ›· ·ÔÛÎÔÔ‡Ó ÛÙÔ ¯·Ú·ÎÙËÚÈÛÌfi,ÙËÓ ·ÔÌfiÓˆÛË Î·È ÙËÓ ÙÚÔÔÔ›ËÛË ÙˆÓ ÌÔÚÈ·ÎÒÓ Û˘ÛÙ·ÙÈÎÒÓ ÂÓfi˜ ΢ÙÙ¿ÚÔ˘. ∆· Û˘ÛÙ·ÙÈο ·˘Ù¿ Â-ÚÈÏ·Ì‚¿ÓÔ˘Ó ÙÔ DNA, Ô˘ ·ÔÙÂÏ› ÙËÓ “·Ôı‹ÎË” Ù˘ ÁÂÓÂÙÈ΋˜ ÏËÚÔÊÔÚ›·˜, ÙÔ RNA Î·È ÙȘ Úˆ-Ù½Ó˜. ∆· ÁÔÓ›‰È· Â›Ó·È ÔÈ ÏÂÈÙÔ˘ÚÁÈΤ˜ ÌÔÓ¿‰Â˜ ÙÔ˘ DNA Î·È Î·ıÔÚ›˙Ô˘Ó ÙË ‰ÔÌ‹ ÙˆÓ ÚˆÙÂ˚ÓÒÓ. ™‡Ì-ʈӷ Ì ÙÔ ÚfiÁÚ·ÌÌ· ·ÔΈ‰ÈÎÔÔ›ËÛ˘ ÁÔÓȉÈÒÌ·ÙÔ˜ ˘¿Ú¯Ô˘Ó ÂÚ›Ô˘ 24.000 ÁÔÓ›‰È·. ∏ ÏÂÈÔ-„ËÊ›· ÙˆÓ ÌÔÚÈ·ÎÒÓ ÂϤÁ¯ˆÓ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÛÙËÓ ÎÏÈÓÈ΋ ‰È¿ÁÓˆÛË ·ÔÛÎÔÔ‡Ó ÛÙËÓ ¤ÚÂ˘Ó·Î·È ÌÂϤÙË ÏËıÒÚ·˜ ÁÔÓȉ›ˆÓ ÁÈ· Û˘ÁÎÂÎÚÈ̤Ó˜ ‹ ÌË ÌÂÙ·ÏÏ¿ÍÂȘ. ™ÙȘ ̤Ú˜ Ì·˜, ÛËÌ·ÓÙÈΤ˜ ‰È·ÁÓˆ-ÛÙÈΤ˜ Î·È ÚÔÁÓˆÛÙÈΤ˜ ÏËÚÔÊÔڛ˜ Â›Ó·È ‰˘Ó·Ùfi Ó· ‰ÔıÔ‡Ó ·fi ÙËÓ ·ÍÈÔÏfiÁËÛË ÂÓfi˜ ÌÂÁ¿ÏÔ˘ ·ÚÈı-ÌÔ‡ ÁÂÓÂÙÈÎÒÓ ÂÍÂÙ¿ÛˆÓ. √È ÂÚÈÛÛfiÙÂÚ˜ ·fi ·˘Ù¤˜ ÙȘ ÂÍÂÙ¿ÛÂȘ Â›Ó·È ÂÊÈÎÙ¤˜, ÂÂȉ‹ ÙÔ DNA ¤¯ÂÈ ÙËÊ˘ÛÈ΋ ȉÈfiÙËÙ· Ó· ·Ô‰È·Ù¿ÛÛÂÙ·È Î·È Ó· ˘‚Úȉ›˙ÂÙ·È. ™ÙËÓ ·Ó·ÛÎfiËÛË ·˘Ù‹, ·Ó·Ê¤ÚÔÓÙ·È ÔÈ ‚·ÛÈ-ÎfiÙÂÚ˜ Ù¯ÓÈΤ˜ ·Ó¿Ï˘Û˘. fiˆ˜ Ë ·Ï˘ÛȉˆÙ‹ ·ÓÙ›‰Ú·ÛË ÔÏ˘ÌÂÚ¿Û˘, Ë ·Ó¿Ï˘ÛË Ù˘ ÚˆÙÔÙ·ÁÔ‡˜·ÏÏËÏÔ˘¯›·˜ DNA, Ë Ì¤ıÔ‰Ô˜ DHPLC Î·È ÔÈ ˘‚ÚȉÈÛÌÔ› southern Î·È northern.
§¤ÍÂȘ ÎÏÂȉȿ: °ÂÓÂÙÈ΋, ÌÔÚȷ΋ ‰È¿ÁÓˆÛË, ·È‰È·ÙÚÈ΋.
Basic techniques of molecular biology and their applications in the
diagnosis of childhood diseases
S. Megremis, ∞. Pampanos
Abstract: All the techniques applied in molecular biology focus on the characterization, isolation andmanipulation of the molecular components of the cell. These components include DNA, which is therepository of genetic information, RNA and proteins. Genes are the functional units of the DNA, specifyingthe structure of proteins. There are about 24,000 protein-coding genes in the human genome as estimatedby the Human Genome Project. Most of the molecular tests that are used in clinical diagnosis screenmultiple genes for specific and/or non-specific mutations. Nowadays, a vast variety of genetic tests areavailable for use by clinicians in order to obtain diagnostic and prognostic information. Most of these testsare feasible because of the capability of the DNA double helix to denature and anneal or hybridize. In thisreview some of the basic molecular diagnostic techniques are presented, such as the polymerase chainreaction, DNA sequencing, DHPLC, and the southern and northern blotting techniques.
Key words: Genetics, molecular diagnostics, paediatrics.
∂ÚÁ·ÛÙ‹ÚÈÔ π·ÙÚÈ΋˜°ÂÓÂÙÈ΋˜¶·ÓÂÈÛÙËÌ›Ô˘ ∞ıËÓÒÓ,ÈڤÌÂÈÔ ∂Ú¢ÓËÙÈÎfi∂ÚÁ·ÛÙ‹ÚÈÔ, ¡ÔÛÔÎÔÌÂ›Ô ¶·›‰ˆÓ “∞Á›· ™ÔÊ›·”
AÏÏËÏÔÁÚ·Ê›·:
∞Ó‰Ú¤·˜ ¶¿Ì·ÓÔ˜ [email protected]∂ÚÁ·ÛÙ‹ÚÈÔ π·ÙÚÈ΋˜°ÂÓÂÙÈ΋˜ ¶·ÓÂÈÛÙËÌ›Ô˘ ∞ıËÓÒÓ,ÈڤÌÂÈÔ ∂Ú¢ÓËÙÈÎfi∂ÚÁ·ÛÙ‹ÚÈÔ,¡ÔÛÔÎÔÌÂ›Ô ¶·›‰ˆÓ “∞Á›· ™ÔÊ›·”£Ë‚ÒÓ Î·È §Â‚·‰Â›·˜,∆.∫. 115 27, ∞ı‹Ó·
Medical GeneticsLaboratory,University of Athens,Choremio ResearchLaboratory,“Aghia Sophia” Children’sHospital, Athens, Greece
Correspondence:
Andreas [email protected] Genetics Laboratory,University of Athens,Choremio Research Laboratory,“Aghia Sophia” Children’sHospitalThivon & Levadias St.,115 27, Athens, Greece
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·105

106 ™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
Paediatriki 2008;71:105-115
∂ÏÏ¿‰·, Ô ¶˘ı·ÁfiÚ·˜ ‰È·Ù‡ˆÛ ÙËÓ ˘fiıÂÛË fiÙÈ
Ë ˙ˆ‹ ÍÂÎÈÓ¿ Ì ÙËÓ ·Ó¿ÌÂÈÍË ·ÚÛÂÓÈÎÒÓ Î·È ıËÏ˘-
ÎÒÓ ÛÂÚÌ¿ÙˆÓ (1). ∆ÔÓ 4o ·ÈÒÓ· .Ã., Ô ∞ÚÈÛÙÔÙ¤-
Ï˘ ˘ÔÛÙ‹ÚÈÍ fiÙÈ Ô Î¿ı ÁÔÓ¤·˜ Û˘Ì‚¿ÏÏÂÈ ÛÙË
ÌÂÙ·ÊÔÚ¿ ¯·Ú·ÎÙËÚÈÛÙÈÎÒÓ ÛÙÔ˘˜ ·ÔÁfiÓÔ˘˜ (1).
™ÙȘ ·Ú¯¤˜ ÙÔ˘ 19Ô˘ ·ÈÒÓ·, Ô °¿ÏÏÔ˜ Ê˘ÛÈÔ‰›Ê˘
Lamarck ˘ÔÛÙ‹ÚÈÍ fiÙÈ Ù· ›ÎÙËÙ· ¯·Ú·ÎÙËÚÈÛÙÈ-
ο ÎÏËÚÔÓÔÌÔ‡ÓÙ·È (3), ÂÓÒ ÙÔ 1859 Ô Darwin ÙfiÓÈ-
Û ÙË ÛËÌ·Û›· ÙˆÓ Ì˯·ÓÈÛÌÒÓ Ù˘ ÎÏËÚÔÓÔÌÈÎfi-
ÙËÙ·˜ ÛÙË ÌÂϤÙË Ù˘ ÂͤÏÈ͢ ÙˆÓ ÂȉÒÓ (1). §›Á·
¯ÚfiÓÈ· ·ÚÁfiÙÂÚ·, ÙÔ 1865, Ô Mendel ‰ËÌÔÛȇÂÈ ÙȘ
ıˆڛ˜ ÙÔ˘. ∆Ô 1903 ·Ô‰ÂÈÎÓ‡ÂÙ·È fiÙÈ Ù· ¯ÚˆÌÔ-
ÛÒÌ·Ù· Â›Ó·È ÊÔÚ›˜ ÙÔ˘ ÁÂÓÂÙÈÎÔ‡ ˘ÏÈÎÔ‡ (1), ÂÓÒ
ÙÔ 1910 Ô Morgan ÂÎÙÈÌ¿ fiÙÈ Ù· ÁÔÓ›‰È· ÂÓÙÔ›˙Ô-
ÓÙ·È ÛÙ· ¯ÚˆÌÔÛÒÌ·Ù· (4). ∆Ô DNA ·Ú¯Èο ÔÓÔÌ¿-
ÛÙËΠÓÔ˘ÎϽÓË Î·È ·Ó·Î·Ï‡ÊıËΠ·fi ÙÔÓ
Meischer ÙÔ 1867 (4), ·ÏÏ¿ ÙÔ ÛËÌ·ÓÙÈÎfiÙÂÚÔ ÁÂÁÔ-
Ófi˜ Û˘ÓÙÂÏÂ›Ù·È ÙÔ 1953, fiÙ·Ó ÔÈ Watson Î·È Crick
ÚÔÙ›ÓÔ˘Ó ÙÔ ÌÔÓÙ¤ÏÔ Ù˘ ‰ÈÏ‹˜ ¤ÏÈη˜ ÙÔ˘ DNA
(4,5), ÂÓÒ ÙÔ 1956 ÔÈ Tjio Î·È Levan ·Ô‰ÂÈÎÓ‡Ô˘Ó
fiÙÈ Ô ·ÚÈıÌfi˜ ÙˆÓ ¯ÚˆÌÔÛˆÌ¿ÙˆÓ ÙÔ˘ ·ÓıÚÒÔ˘
Â›Ó·È 46 (1).
∞fi ÙfiÙÂ Ë ÂͤÏÈÍË Ù˘ ÌÔÚȷ΋˜ ‚ÈÔÏÔÁ›·˜ ηÈ
ÁÂÓÂÙÈ΋˜ Â›Ó·È Ù¤ÙÔÈ·, ÒÛÙ ӷ ıˆÚÂ›Ù·È Ï¤ÔÓ ‰Â-
‰Ô̤ÓË Ë ¯Ú‹ÛË ÙˆÓ ÌÂıfi‰ˆÓ ÙÔ˘˜ ÛÙËÓ ÎÏÈÓÈ΋
‰È¿ÁÓˆÛË. ∏ ÂÈÏÔÁ‹ Ù˘ ÌÂıfi‰Ô˘ Ô˘ ı· ¯ÚËÛÈÌÔ-
ÔÈËı› ÁÈ· ÙË ÌÔÚȷ΋ ‰È¿ÁÓˆÛË ÌÈ·˜ ÁÂÓÂÙÈ΋˜
·Ûı¤ÓÂÈ·˜ ηıÔÚ›˙ÂÙ·È ·fi ÙÔ Ì˯·ÓÈÛÌfi Ô˘ ÚÔ-
ηÏ› ÙËÓ ›‰È· ÙË ÓfiÛÔ. ™Ùfi¯Ô˜ ÙÔ˘ ¿ÚıÚÔ˘ Â›Ó·È Ë
·Ó·ÊÔÚ¿ ÛÙȘ ‚·ÛÈÎfiÙÂÚ˜ ÌÔÚȷΤ˜ Ù¯ÓÈΤ˜ ·Ó¿-
Ï˘Û˘ DNA, ÔÈ Ôԛ˜ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ˆ˜ › ÙÔ
Ï›ÛÙÔÓ ÛÙË ‰È¿ÁÓˆÛË ÁÂÓÂÙÈÎÒÓ ÓfiÛˆÓ Î·È ·Ó‹-
ÎÔ˘Ó Ï¤ÔÓ ÛÙËÓ Î·ıËÌÂÚÈÓ‹ Ú¿ÍË ÙˆÓ ÂÚÈÛÛÔÙ¤-
ÚˆÓ ·È‰È·ÙÚÈÎÒÓ ˘ÔÂȉÈÎÔÙ‹ÙˆÓ (¶›Ó·Î·˜ 1).
∆Ô ‰ÂÔ͢ÚÈ‚ÔÓÔ˘ÎÏÂ˚Îfi Ô͇ (DNA)
∂›Ó·È ÁÓˆÛÙfi fiÙÈ ÔÈ ÎÏËÚÔÓÔÌÈΤ˜ ÏËÚÔÊÔڛ˜
ÌÂÙ·‚È‚¿˙ÔÓÙ·È ·fi οı ·ÙÙ·ÚÔ ÛÙ· ı˘Á·ÙÚÈο
ÙÔ˘, ηٿ ÙËÓ Î˘ÙÙ·ÚÈ΋ ‰È·›ÚÂÛË, ‰È·Ì¤ÛÔ˘ ÙˆÓ ÁÔ-
Óȉ›ˆÓ. ◊‰Ë, ·fi ÙȘ ·Ú¯¤˜ ÙÔ˘ ÂÈÎÔÛÙÔ‡ ·ÈÒÓ·, ÔÈ
ÂÈÛÙ‹ÌÔÓ˜ ıˆÚÔ‡Û·Ó ‰Â‰Ô̤ÓÔ fiÙÈ Ù· ÁÔÓ›‰È·
‚Ú›ÛÎÔÓÙ·È ÛÙ· ¯ÚˆÌÔÛÒÌ·Ù·, Ù· ÔÔ›· ÙfiÙ ‹Ù·Ó
ÁÓˆÛÙ¿ ˆ˜ ÓËÌ·ÙÔÂȉ›˜ ‰Ô̤˜ ÙÔ˘ ˘Ú‹Ó· ÙˆÓ Â˘-
ηڢˆÙÈÎÒÓ Î˘ÙÙ¿ÚˆÓ Ô˘ Á›ÓÔÓÙ·È ÔÚ·Ù¿ fiÙ·Ó ÙÔ
·ÙÙ·ÚÔ ·Ú¯›˙ÂÈ Ó· ‰È·ÈÚ›ٷÈ. ªÂ ÙËÓ ¿ÚÔ‰Ô ‰Â
ÙÔ˘ ¯ÚfiÓÔ˘ Î·È Ì ÙËÓ ÂͤÏÈÍË ÙˆÓ ‚ÈÔ¯ËÌÈÎÒÓ ·Ó·-
χÛÂˆÓ ÂȂ‚·ÈÒıËΠfiÙÈ Ù· ¯ÚˆÌÔÛÒÌ·Ù· ·ÔÙÂ-
ÏÔ‡ÓÙ·È ·fi DNA Î·È ÚˆÙ½Ó˜.
∞Ú¯Èο, ÔÈ ÂÈÛÙ‹ÌÔÓ˜ ‰˘ÛÎÔχÔÓÙ·Ó Ó· ‰Â-
¯ÙÔ‡Ó ÙÔ Ì·ÎÚ‡ ·˘Ùfi ÔÏ˘ÌÂÚ¤˜ ˘ÏÈÎfi Ô˘ ·ÔÙÂ-
ÏÔ‡ÓÙ·Ó ·fi 4 ÌfiÓÔ Â›‰Ë ˘ÔÔÌ¿‰ˆÓ, ˆ˜ ÁÂÓÂÙÈÎfi
˘ÏÈÎfi, ÏfiÁˆ Ù˘ Ê·ÈÓÔÌÂÓÈ΋˜ ·ÏfiÙËÙ·˜ Ù˘ ¯Ë-
Ì›·˜ ÙÔ˘. ∆Ô 1953, fï˜, ÔÈ J. Watson & F. Crick
(4,5) ˘¤‚·Ï·Ó Û ·Ó¿Ï˘ÛË ÂÚ›ıÏ·Û˘ ·ÎÙ›ÓˆÓ Ã
(Ù¯ÓÈ΋ ηıÔÚÈÛÌÔ‡ ÙÚÈۉȿÛÙ·Ù˘ ·ÙÔÌÈ΋˜ ‰Ô-
Ì‹˜ ÙˆÓ ÌÔÚ›ˆÓ) ÙÔ ‰ÂÔ͢ÚÈ‚ÔÓÔ˘ÎÏÂ˚Îfi Ô͇ (DNA)
·Ô‰›‰ÔÓÙ¿˜ ÙÔ˘ ÙË ‰›ÎψÓË ÂÏÈÎÔÂȉ‹ ÌÔÚÊ‹, ‰›-
ÓÔÓÙ·˜ ¤ÙÛÈ ·¿ÓÙËÛË Û ÂÚˆÙ‹Ì·Ù· ÙÔ˘ Ù‡Ô˘: ‰˘-
Ó·ÙfiÙËÙ· ·ÎÚÈ‚Ô‡˜ ·ÓÙÈÁÚ·Ê‹˜ ÙˆÓ 2 ÎÏÒÓˆÓ Î·È
ÌÂÙ·ÊÔÚ¿ ÏËÚÔÊÔÚÈÒÓ, ˘fi ¯ËÌÈ΋ ÌÔÚÊ‹, ÁÈ· ÙË
‰ËÌÈÔ˘ÚÁ›· ÂÓfi˜ ÔÚÁ·ÓÈÛÌÔ‡.
∏ ¤Ó·ÚÍË Ù˘ Û‡ÓıÂÛ˘ ÙÔ˘ DNA, fiˆ˜ ·Ú·ÙË-
ÚÂ›Ù·È ÛÙÔ ËÏÂÎÙÚÔÓÈÎfi ÌÈÎÚÔÛÎfiÈÔ, Ú·ÁÌ·ÙÔÔÈ›-
Ù·È ÛÙȘ ÏÂÁfiÌÂÓ˜ ‰È¯¿Ï˜ ·ÓÙÈÁÚ·Ê‹˜ (replication
forks) ̆ fi ÙËÓ ·ÚÔ˘Û›· ÂȉÈÎÒÓ ÂÓ·ÚÎÙ‹ÚÈˆÓ ÚˆÙÂ-
˚ÓÒÓ Ô˘ ·Ó·ÁÓˆÚ›˙Ô˘Ó Û˘ÁÎÂÎÚÈ̤Ó˜ ·ÏÏËÏÔ˘¯›Â˜
ÙÔ˘ DNA ÛÙȘ ·ÊÂÙËڛ˜ ·ÓÙÈÁÚ·Ê‹˜ Î·È ·Ô‰È·Ù¿Û-
ÛÔ˘Ó ÙÔÈο ÙÔ˘˜ 2 ÎÏÒÓÔ˘˜ Ù˘ ‰ÈÏ‹˜ ¤ÏÈη˜. √È
ÚÔ·ÙÔÓÙ˜ ÂÎÙÂıÂÈ̤ÓÔÈ ÌÔÓÔ› ÎÏÒÓÔÈ ·Ú·Ì¤-
ÓÔ˘Ó ·Ó¤·ÊÔÈ Î·È ÏÂÈÙÔ˘ÚÁÔ‡Ó ˆ˜ ÂÎÌ·Á›· ÁÈ· ÙÔ
Û¯ËÌ·ÙÈÛÌfi Û˘ÌÏËڈ̷ÙÈÎÒÓ ÎÏÒÓˆÓ DNA (∂ÈÎfi-
Ó˜ 1· Î·È 1‚) ˘fi ÙËÓ Â›‰Ú·ÛË ÙÔ˘ ÂÓ˙‡ÌÔ˘ DNA
ÔÏ˘ÌÂÚ¿ÛË Î·È ¿ÓÙÔÙ ÚÔ˜ ÙËÓ Î·Ù‡ı˘ÓÛË 5ã→3ã.
∆· ·ÙÙ·Ú· ÂÎÊÚ¿˙Ô˘Ó ÙȘ ÁÂÓÂÙÈΤ˜ ÙÔ˘˜ Ô‰Ë-
Á›Â˜, Ù· ÁÔÓ›‰È¿ ÙÔ˘˜, ̤ۈ Ù˘ ÌÂÙ·ÁÚ·Ê‹˜ Î·È Ù˘
ÌÂÙ¿ÊÚ·Û˘, ¤ÙÛÈ ÒÛÙÂ Ë ÚÔ‹ ÙˆÓ ÁÂÓÂÙÈÎÒÓ ÏËÚÔ-
ÊÔÚÈÒÓ Ó· Â›Ó·È ¿ÓÙ· Ë ÂÍ‹˜:
DNA→RNA→¶ÚˆÙ½Ó˜.
∆Ô RNA ‰È·‰Ú·Ì·Ù›˙ÂÈ Î˘Ú›ˆ˜ ÙÔ ÚfiÏÔ ÂÓfi˜ ÌÂ-
Û¿˙ÔÓÙ· (∂ÈÎfiÓ· 2). ∫·Ù¿ Û˘Ó¤ÂÈ·, Ù· ÁÔÓ›‰È· ‰ÂÓ
Â›Ó·È Ù›ÔÙ ¿ÏÏÔ ·fi ÙȘ ıÂÌÂÏÈÒ‰ÂȘ ÏÂÈÙÔ˘ÚÁÈΤ˜
ÌÔÓ¿‰Â˜ ÎÏËÚÔÓÔÌÈÎfiÙËÙ·˜ οı ˙ÒÓÙÔ˜ ÔÚÁ·ÓÈ-
ÛÌÔ‡ Ô˘ ηٷϷ̂¿ÓÔ˘Ó ¤Ó·Ó ÂȉÈÎfi ÙfiÔ-ı¤ÛË
(locus) ¿Óˆ Û οı ¯ÚˆÌfiۈ̷. ∏ ‰ÔÌ‹ ÙÔ˘ οıÂ
¶›Ó·Î·˜ 1. ∂Ӊ›ÍÂȘ ·Ó¿Ï˘Û˘ DNA
ÃÚfiÓÔ˜ DNA ∂Ӊ›ÍÂȘ (·Ú·‰Â›ÁÌ·Ù·)·Ó¿Ï˘Û˘
¶ÚÔÁÂÓÓËÙÈο ñ ¢È¿ÁÓˆÛË Î‡ËÛ˘ ˘„ËÏÔ‡ ÎÈÓ‰‡ÓÔ˘ (.¯.ÈÛÙÔÚÈÎfi Ì˘˚΋˜ ‰˘ÛÙÚÔÊ›·˜ Duchenne)
¡ÂÔÁÓ¿ - µÚ¤ÊË ñ ∂Ȃ‚·›ˆÛË ÎÏÈÓÈ΋˜ ‰È¿ÁÓˆÛ˘ (.¯.Ê·ÈÓfiÙ˘Ô˜ ΢ÛÙÈ΋˜ ›ÓˆÛ˘ Ì ıÂÙÈÎfiÙÂÛ٠ȉÚÒÙ·)
¶·È‰È¿ ñ ¢ÈÂÚ‡ÓËÛË ÓÔËÙÈ΋˜ ˘ÛÙ¤ÚËÛ˘ (.¯.·ÔÎÏÂÈÛÌfi˜ Û˘Ó‰ÚfiÌÔ˘ ¢ıÚ·‡ÛÙÔ˘¯ÚˆÌÔÛÒÌ·ÙÔ˜ Ã)
ñ ∂Ȃ‚·›ˆÛË ‰È¿ÁÓˆÛ˘ ÓÔÛ‹Ì·ÙÔ˜ ̤ӷÚÍË ÂΉËÏÒÛÂˆÓ ÛÙËÓ ·È‰È΋ ËÏÈΛ·(.¯ Ì˘˚΋ ‰˘ÛÙÚÔÊ›· Duchenne)
∂Ó‹ÏÈΘ ñ ŒÏÂÁ¯Ô˜ ÊÔÚ¤ˆÓ (.¯. ÔÈÎÔÁÂÓÂÈ·Îfi ÈÛÙÔ-ÚÈÎfi ΢ÛÙÈ΋˜ ›ÓˆÛ˘)
ñ ¶ÚÔÛ˘Ìو̷ÙÈÎfi˜ ¤ÏÂÁ¯Ô˜ (ÔÈÎÔÁÂÓÂÈ·Îfi ÈÛÙÔÚÈÎfi ηÚΛÓÔ˘ Ì·ÛÙÔ‡/ˆÔıËÎÒÓ)
ñ ∂Ȃ‚·›ˆÛË ‰È¿ÁÓˆÛ˘ ÓÔÛ‹Ì·ÙÔ˜ ̤ӷÚÍË ÂΉËÏÒÛÂˆÓ ÛÙËÓ ÂÓ‹ÏÈÎË ˙ˆ‹(.¯. ÓfiÛÔ˜ Huntington)
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·106
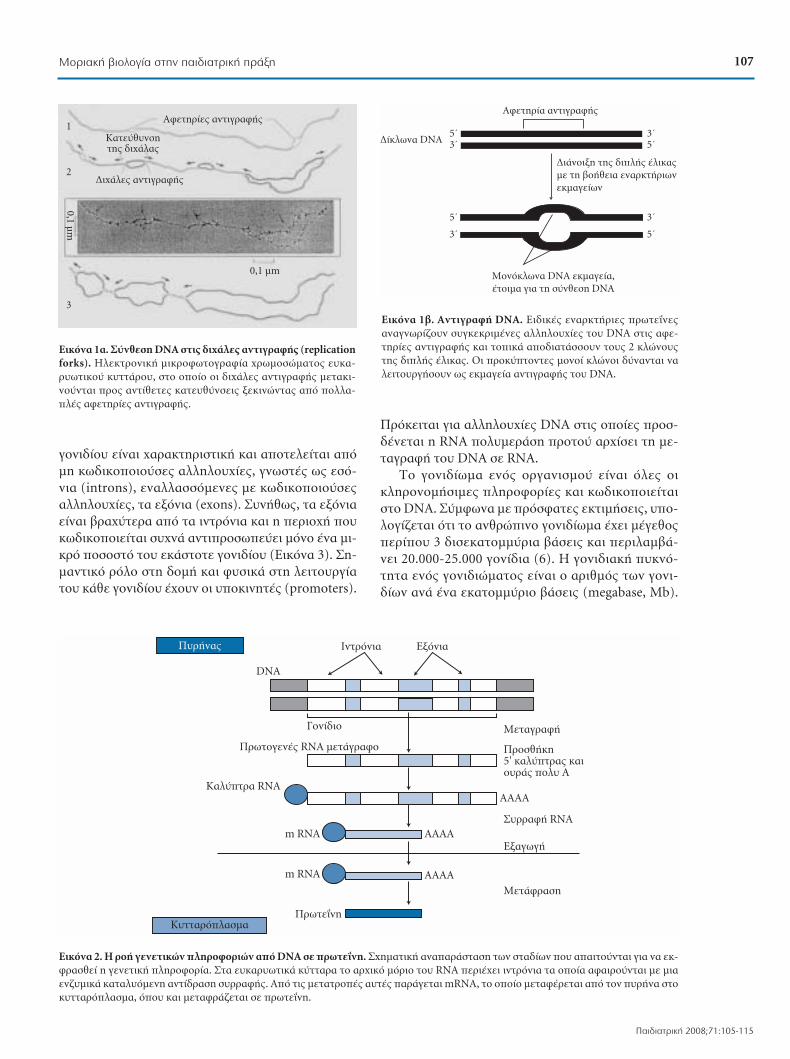
ÁÔÓȉ›Ô˘ Â›Ó·È ¯·Ú·ÎÙËÚÈÛÙÈ΋ Î·È ·ÔÙÂÏÂ›Ù·È ·fiÌË Îˆ‰ÈÎÔÔÈÔ‡Û˜ ·ÏÏËÏÔ˘¯›Â˜, ÁÓˆÛÙ¤˜ ˆ˜ ÂÛfi-ÓÈ· (introns), ÂÓ·ÏÏ·ÛÛfiÌÂÓ˜ Ì Έ‰ÈÎÔÔÈÔ‡Û˜·ÏÏËÏÔ˘¯›Â˜, Ù· ÂÍfiÓÈ· (exons). ™˘Ó‹ıˆ˜, Ù· ÂÍfiÓÈ·Â›Ó·È ‚Ú·¯‡ÙÂÚ· ·fi Ù· ÈÓÙÚfiÓÈ· Î·È Ë ÂÚÈÔ¯‹ Ô˘Îˆ‰ÈÎÔÔÈÂ›Ù·È Û˘¯Ó¿ ·ÓÙÈÚÔۈ‡ÂÈ ÌfiÓÔ ¤Ó· ÌÈ-ÎÚfi ÔÛÔÛÙfi ÙÔ˘ ÂοÛÙÔÙ ÁÔÓȉ›Ô˘ (∂ÈÎfiÓ· 3). ™Ë-Ì·ÓÙÈÎfi ÚfiÏÔ ÛÙË ‰ÔÌ‹ Î·È Ê˘ÛÈο ÛÙË ÏÂÈÙÔ˘ÚÁ›·ÙÔ˘ οı ÁÔÓȉ›Ô˘ ¤¯Ô˘Ó ÔÈ ˘ÔÎÈÓËÙ¤˜ (promoters).
¶ÚfiÎÂÈÙ·È ÁÈ· ·ÏÏËÏÔ˘¯›Â˜ DNA ÛÙȘ Ôԛ˜ ÚÔÛ-‰¤ÓÂÙ·È Ë RNA ÔÏ˘ÌÂÚ¿ÛË ÚÔÙÔ‡ ·Ú¯›ÛÂÈ ÙË ÌÂ-Ù·ÁÚ·Ê‹ ÙÔ˘ DNA Û RNA.
∆Ô ÁÔÓȉ›ˆÌ· ÂÓfi˜ ÔÚÁ·ÓÈÛÌÔ‡ Â›Ó·È fiϘ ÔÈÎÏËÚÔÓÔÌ‹ÛÈ̘ ÏËÚÔÊÔڛ˜ Î·È Îˆ‰ÈÎÔÔÈ›ٷÈÛÙÔ DNA. ™‡Ìʈӷ Ì ÚfiÛÊ·Ù˜ ÂÎÙÈÌ‹ÛÂȘ, ̆ Ô-ÏÔÁ›˙ÂÙ·È fiÙÈ ÙÔ ·ÓıÚÒÈÓÔ ÁÔÓȉ›ˆÌ· ¤¯ÂÈ Ì¤ÁÂıÔ˜ÂÚ›Ô˘ 3 ‰ÈÛÂηÙÔÌ̇ÚÈ· ‚¿ÛÂȘ Î·È ÂÚÈÏ·Ì‚¿-ÓÂÈ 20.000-25.000 ÁÔÓ›‰È· (6). ∏ ÁÔÓȉȷ΋ ˘ÎÓfi-ÙËÙ· ÂÓfi˜ ÁÔÓȉÈÒÌ·ÙÔ˜ Â›Ó·È Ô ·ÚÈıÌfi˜ ÙˆÓ ÁÔÓÈ-‰›ˆÓ ·Ó¿ ¤Ó· ÂηÙÔÌ̇ÚÈÔ ‚¿ÛÂȘ (megabase, Mb).
¶˘Ú‹Ó·˜
∫˘ÙÙ·ÚfiÏ·ÛÌ·
¶ÚˆÙÔÁÂÓ¤˜ RNA ÌÂÙ¿ÁÚ·ÊÔ
πÓÙÚfiÓÈ·
°ÔÓ›‰ÈÔ
∂ÍfiÓÈ·
∞∞∞∞m RNA
∫·Ï‡ÙÚ· RNA
DNA
m RNA
¶ÚˆÙ½ÓË
∞∞∞∞
∞∞∞∞
MÂÙ·ÁÚ·Ê‹
MÂÙ¿ÊÚ·ÛË
¶ÚÔÛı‹ÎË5' ηχÙÚ·˜ ηÈÔ˘Ú¿˜ ÔÏ˘ ∞
™˘ÚÚ·Ê‹ RNA
EÍ·ÁˆÁ‹
∂ÈÎfiÓ· 2. ∏ ÚÔ‹ ÁÂÓÂÙÈÎÒÓ ÏËÚÔÊÔÚÈÒÓ ·fi DNA Û ڈÙ½ÓË. ™¯ËÌ·ÙÈ΋ ·Ó··Ú¿ÛÙ·ÛË ÙˆÓ ÛÙ·‰›ˆÓ Ô˘ ··ÈÙÔ‡ÓÙ·È ÁÈ· Ó· ÂÎ-ÊÚ·Ûı› Ë ÁÂÓÂÙÈ΋ ÏËÚÔÊÔÚ›·. ™Ù· ¢ηڢˆÙÈο ·ÙÙ·Ú· ÙÔ ·Ú¯ÈÎfi ÌfiÚÈÔ ÙÔ˘ RNA ÂÚȤ¯ÂÈ ÈÓÙÚfiÓÈ· Ù· ÔÔ›· ·Ê·ÈÚÔ‡ÓÙ·È Ì ÌÈ·ÂÓ˙˘ÌÈο Î·Ù·Ï˘fiÌÂÓË ·ÓÙ›‰Ú·ÛË Û˘ÚÚ·Ê‹˜. ∞fi ÙȘ ÌÂÙ·ÙÚÔ¤˜ ·˘Ù¤˜ ·Ú¿ÁÂÙ·È mRNA, ÙÔ ÔÔ›Ô ÌÂٷʤÚÂÙ·È ·fi ÙÔÓ ˘Ú‹Ó· ÛÙÔ΢ÙÙ·ÚfiÏ·ÛÌ·, fiÔ˘ Î·È ÌÂÙ·ÊÚ¿˙ÂÙ·È Û ڈÙ½ÓË.
5ã3ã
5ã
3ã
3ã5ã
3ã
5ã
∞ÊÂÙËÚ›· ·ÓÙÈÁÚ·Ê‹˜
ªÔÓfiÎψӷ DNA ÂÎÌ·Á›·,¤ÙÔÈÌ· ÁÈ· ÙË Û‡ÓıÂÛË DNA
¢È¿ÓÔÈÍË Ù˘ ‰ÈÏ‹˜ ¤ÏÈη˜ Ì ÙË ‚Ô‹ıÂÈ· ÂÓ·ÚÎÙ‹ÚȈÓÂÎÌ·Á›ˆÓ
¢›Îψӷ DNA
∂ÈÎfiÓ· 1‚. ∞ÓÙÈÁÚ·Ê‹ DNA. ∂ȉÈΤ˜ ÂÓ·ÚÎÙ‹ÚȘ ÚˆÙ½Ó˜·Ó·ÁÓˆÚ›˙Ô˘Ó Û˘ÁÎÂÎÚÈ̤Ó˜ ·ÏÏËÏÔ˘¯›Â˜ ÙÔ˘ DNA ÛÙȘ ·ÊÂ-ÙËڛ˜ ·ÓÙÈÁÚ·Ê‹˜ Î·È ÙÔÈο ·Ô‰È·Ù¿ÛÛÔ˘Ó ÙÔ˘˜ 2 ÎÏÒÓÔ˘˜Ù˘ ‰ÈÏ‹˜ ¤ÏÈη˜. √È ÚÔ·ÙÔÓÙ˜ ÌÔÓÔ› ÎÏÒÓÔÈ ‰‡Ó·ÓÙ·È Ó·ÏÂÈÙÔ˘ÚÁ‹ÛÔ˘Ó ˆ˜ ÂÎÌ·Á›· ·ÓÙÈÁÚ·Ê‹˜ ÙÔ˘ DNA.
∂ÈÎfiÓ· 1·. ™‡ÓıÂÛË DNA ÛÙȘ ‰È¯¿Ï˜ ·ÓÙÈÁÚ·Ê‹˜ (replicationforks). ∏ÏÂÎÙÚÔÓÈ΋ ÌÈÎÚÔʈÙÔÁÚ·Ê›· ¯ÚˆÌÔÛÒÌ·ÙÔ˜ ¢η-Ú˘ˆÙÈÎÔ‡ ΢ÙÙ¿ÚÔ˘, ÛÙÔ ÔÔ›Ô ÔÈ ‰È¯¿Ï˜ ·ÓÙÈÁÚ·Ê‹˜ ÌÂÙ·ÎÈ-ÓÔ‡ÓÙ·È ÚÔ˜ ·ÓÙ›ıÂÙ˜ ηÙ¢ı‡ÓÛÂȘ ÍÂÎÈÓÒÓÙ·˜ ·fi ÔÏÏ·-Ϥ˜ ·ÊÂÙËڛ˜ ·ÓÙÈÁÚ·Ê‹˜.
∞ÊÂÙËڛ˜ ·ÓÙÈÁÚ·Ê‹˜
∫·Ù‡ı˘ÓÛËÙ˘ ‰È¯¿Ï·˜
1
2
3
0,1 Ìm
0,1 Ìm
¢È¯¿Ï˜ ·ÓÙÈÁÚ·Ê‹˜
107ªÔÚȷ΋ ‚ÈÔÏÔÁ›· ÛÙËÓ ·È‰È·ÙÚÈ΋ Ú¿ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:105-115
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·107

H ÁÔÓȉȷ΋ ˘ÎÓfiÙËÙ· ÙÔ˘ ·ÓıÚÒÈÓÔ˘ ÁÔÓȉÈÒ-Ì·ÙÔ˜ Â›Ó·È Û¯Â‰fiÓ 12-15 ÁÔÓ›‰È·/ÌÂÁ·‚¿ÛË (7).
√È ‰ÈÂÚÁ·Û›Â˜ ·ÓÙÈÁÚ·Ê‹˜ Î·È ÂȉÈfiÚıˆÛ˘ ÙÔ˘ÁÂÓÂÙÈÎÔ‡ ˘ÏÈÎÔ‡ οı ΢ÙÙ¿ÚÔ˘ Û¿ÓÈ· ·ÔÙ˘Á¯¿-ÓÔ˘Ó Î·È ¤ÙÛÈ ‰È·ÙËÚÂ›Ù·È Ë ÓÔ˘ÎÏÂÔÙȉÈ΋ ÙÔ˘ ·Ï-ÏËÏÔ˘¯›· ÛÙ·ıÂÚ‹. ∂Ó›ÔÙÂ, fï˜, ‰‡Ó·Ù·È Ó· ·Ú·-ÙËÚËıÔ‡Ó ÓÔ˘ÎÏÂÔÙȉÈΤ˜ ·ÏÏ·Á¤˜, ÛËÌÂȷΤ˜ ‹ ÌË,Ì ·ÔÙ¤ÏÂÛÌ· Ó· Ô‰ËÁԇ̷ÛÙ Û ۇÓıÂÛË ·ıÔ-ÏÔÁÈÎÒÓ ÚˆÙÂ˚ÓÒÓ Î·È Î·Ù¿ Û˘Ó¤ÂÈ· ÙË ÌË Ê˘ÛÈÔ-ÏÔÁÈ΋ Û˘ÁΤÓÙÚˆÛË ÙÔ˘ ·Ú·ÁÒÁÔ˘ ÙÔ˘ ÁÔÓȉ›Ô˘ÛÙÔÓ ÔÚÁ·ÓÈÛÌfi. √ÔÈ·‰‹ÔÙ ٤ÙÔÈ· ·ÏÏ·Á‹ η-ÏÂ›Ù·È ÌÂÙ¿ÏÏ·ÍË. ∂ÓÙÔ‡ÙÔȘ, ÛËÌÂȷΤ˜ ·ÏÏ·Á¤˜ ÛÂÁÔÓ›‰ÈÔ, ÔÈ Ôԛ˜ ‰ÂÓ ¤¯Ô˘Ó ›وÛË ÛÙË ÏÂÈÙÔ˘Ú-Á›· Ù˘ Έ‰ÈÎÔÔÈÔ‡Û·˜ ÚˆÙ½Ó˘, ¯·Ú·ÎÙËÚ›˙Ô-ÓÙ·È ˆ˜ ÔÏ˘ÌÔÚÊÈÛÌÔ› ‹ ÔÏ˘ÌÔÚÊÈΤ˜ ı¤ÛÂȘ.ªÂÙ·ÏÏ¿ÍÂȘ ‰ÂÓ ·Ú·ÙËÚÔ‡ÓÙ·È ÌfiÓÔ ÛÙȘ Έ‰È-ÎÔÔÈÔ‡Û˜ ÂÚÈÔ¯¤˜ ÙˆÓ ÁÔÓȉ›ˆÓ, ·ÏÏ¿ Î·È Û ÌËΈ‰ÈÎÔÔÈÔ‡Û˜, Ì ٷ ›‰È· ·ÔÙÂϤÛÌ·Ù· (8). OÈ΢ÚÈfiÙÂÚÔÈ Ù‡ÔÈ ÌÂÙ·ÏÏ¿ÍÂˆÓ ·Ó·Ê¤ÚÔÓÙ·È ÛÙÔÓ¶›Ó·Î· 2.
∞ÔÌfiÓˆÛË DNA
∏ ÂͤٷÛË ÙÔ˘ ÁÔÓȉÈÒÌ·ÙÔ˜ ÚÔ¸Ôı¤ÙÂÈ ÛÂÚÒÙË Ê¿ÛË ÙËÓ ÂÍ·ÁˆÁ‹ Î·È ·ÔÌfiÓˆÛË ÙÔ˘ DNA(ÁÂÓˆÌÈÎÔ‡, ÌÈÙÔ¯ÔÓ‰ÚÈ·ÎÔ‡ ‹ ÈÈÎÔ‡) ·fi ÂÚÈÊÂÚÈ-Îfi ·›Ì· ‹ ¿ÏÏÔ˘˜ ÈÛÙÔ‡˜, Ì ÛÎÔfi ÙÔ ‰È·¯ˆÚÈÛÌfiÙÔ˘ ·fi Ù· ˘fiÏÔÈ· Û˘ÛÙ·ÙÈο ÙˆÓ Î˘ÙÙ¿ÚˆÓ(ÚˆÙ½Ó˜, ÏÈ›‰È·, RNA, Î.Ï.). √È ‰È¿ÊÔÚ˜ ̤ıÔ-‰ÔÈ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÂÚÈÏ·Ì‚¿ÓÔ˘Ó ÙË Ì˯·-ÓÈ΋ ıÚ·‡ÛË ÙˆÓ Î˘ÙÙ¿ÚˆÓ, ÒÛÙ ӷ ·ÓÔ›ÍÔ˘Ó Ì Ù˯ڋÛË ‰È¿ÊÔÚˆÓ ¯ËÌÈÎÒÓ Ô˘ÛÈÒÓ Î·È ÂÓ˙‡ÌˆÓ, ÌÂÛÎÔfi ÙËÓ Î·Ù·ÛÙÚÔÊ‹ ÙˆÓ ÌÂÌ‚Ú·ÓÒÓ Î·È ÙˆÓ ÙÔÈ-¯ˆÌ¿ÙˆÓ ÙˆÓ Î˘ÙÙ¿ÚˆÓ (9-11).
À¿Ú¯Ô˘Ó ‰‡Ô ̤ıÔ‰ÔÈ ·ÔÌfiÓˆÛ˘ DNA ·fiÂÚÈÊÂÚÈÎfi ·›Ì· ‹ ·fi ‰È¿ÊÔÚÔ˘˜ ÈÛÙÔ‡˜, Ë Ì¤ıÔ-‰Ô˜ ÙÔ˘ NaCl (10) Î·È Ë ¯Ú‹ÛË ÙˆÓ ÂÌÔÚÈο ‰È·ı¤-ÛÈÌˆÓ ‘kits’, Ù· ÔÔ›· ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È Ï¤ÔÓ Â-ÚÈÛÛfiÙÂÚÔ ÏfiÁˆ Ù˘ ˘ÂÚÔ¯‹˜ ÙÔ˘˜ Û ٷ¯‡ÙËÙ·(ÂÚ›Ô˘ 25 ÏÂÙ¿, ¤Ó·ÓÙÈ ‰‡Ô ËÌÂÚÒÓ ÛÙË Ì¤ıÔ‰ÔÙÔ˘ NaCl) (12) Î·È Ù˘ ηı·ÚfiÙËÙ·˜ ÙÔ˘ ÂÍ·ÁfiÌÂ-ÓÔ˘ DNA. ∆· ÂÌÔÚÈο ‰È·ı¤ÛÈÌ· kits Â›Ó·È Û¯Â‰È·-
Ṳ̂ӷ Ì ٤ÙÔÈÔ ÙÚfiÔ, ÒÛÙ ӷ ·Ô‰›‰Ô˘Ó ÂÚ›-
Ô˘ 6 Ìg DNA ·fi 200 Ìl ÂÚÈÊÂÚÈÎÔ‡ ÔÏÈÎÔ‡ ·›Ì·-
ÙÔ˜ Ì ·ÓÙÈËÎÙÈÎÔ‡˜ ·Ú¿ÁÔÓÙ˜ -fiˆ˜ EDTA-
Î·È Ì¤¯ÚÈ 50 Ìg DNA ·fi Ù· ÂÈıËÏȷο ·ÙÙ·Ú·
Ù˘ ÛÙÔÌ·ÙÈ΋˜ ÎÔÈÏfiÙËÙ·˜ Ô˘ ÂÚȤ¯ÔÓÙ·È Û 200
Ìl ÛȤÏÔ˘ (13).
AÓ¿Ï˘ÛË Î·È ÌÂϤÙË ÙÔ˘ DNA
∞Ï˘ÛȉˆÙ‹ ·ÓÙ›‰Ú·ÛË ÔÏ˘ÌÂÚ¿Û˘ (Polymerase
Chain Reaction, PCR)
∏ ̤ıÔ‰Ô˜ ·Ó·Î·Ï‡ÊıËΠÙÔ 1987 ·fi ÙÔÓ
Mullis (14), Ô ÔÔ›Ô˜ ‚Ú·‚‡ÙËΠ̠Nobel ÙÔ 1995,
Î·È ·ÔÛÎÔ› ÛÙÔÓ ÂÎıÂÙÈÎfi ÔÏÏ·Ï·ÛÈ·ÛÌfi ÌÈ-
ÎÚÒÓ ÙÌËÌ¿ÙˆÓ DNA ÌÂ ÙË ¯Ú‹ÛË Û˘ÓıÂÙÈÎÒÓ ÔÏÈ-
ÁÔÓÔ˘ÎÏÂÔÙȉ›ˆÓ (ÂÎÎÈÓËÙ¤˜-primers) Î·È ıÂÚÌÔ·Ó-
ıÂÎÙÈÎÔ‡ ÂÓ˙‡ÌÔ˘ (15-17). √ ÔÏÏ·Ï·ÛÈ·ÛÌfi˜
·ÊÔÚ¿ Û˘ÁÎÂÎÚÈ̤Ó˜ ÂÚÈÔ¯¤˜ DNA Ô˘ ÌÔÚ› Ó·
ÂÚȤ¯Ô˘Ó ›Ù ¤Ó· ·Ïfi ÁÔÓ›‰ÈÔ ‹ ̤ÚÔ˜ ·˘ÙÔ‡ ‹ ÌË
Έ‰ÈÎÔÔÈÔ‡Û˜ ÂÚÈÔ¯¤˜, ÌÂÁ¤ıÔ˘˜ ̤¯ÚÈ 10.000
‚¿ÛÂȘ (bp) (18-21). ∏ Ù¯ÓÈ΋ PCR ‚·Û›˙ÂÙ·È ÛÙËÓ
ÂÓ˙˘Ì·ÙÈ΋ ÎψÓÔÔ›ËÛË ÙÔ˘ ÁÂÓˆÌÈÎÔ‡ ˘ÏÈÎÔ‡,
¯ˆÚ›˜ ÙË ¯Ú‹ÛË ˙ÒÓÙˆÓ ÔÚÁ·ÓÈÛÌÒÓ fiˆ˜ ∂. coli ‹
̇ÎËÙ˜ (14-17).
∏ ̤ıÔ‰Ô˜ ÂÊ·ÚÌfi˙ÂÙ·È Â˘Ú‡Ù·Ù· ÛÙËÓ ÎÏÈÓÈ΋
Ú¿ÍË Î·È ÙË ‚ÈÔÏÔÁÈ΋ ¤Ú¢ӷ ‰Â‰Ô̤ÓÔ˘ fiÙÈ
ÌÔÚ› Ó· ÂÓÙÔ›ÛÂÈ ÌÈ· Û˘ÁÎÂÎÚÈ̤ÓË ·ÏÏËÏÔ˘¯›·
DNA ‹ RNA Û ÔÔÈÔ‰‹ÔÙ ˘fi ÂͤٷÛË ÎÏÈÓÈÎfi
‰Â›ÁÌ· (22). ∫Ï·ÛÈο ·Ú·‰Â›ÁÌ·Ù· Â›Ó·È ÔÈ ÁÂÓÂÙÈ-
Τ˜ ·ı‹ÛÂȘ ÁÓˆÛÙÒÓ ÌÔÓÔÁÔÓȉȷÎÒÓ ‹ ÔÏ˘ÁÔ-
ÓȉȷÎÒÓ ÓÔÛËÌ¿ÙˆÓ, fiÔ˘ Ì PCR ·ÓȯÓ‡ÂÙ·È Ë
ÌÂÙ·‚ÔÏ‹ ¤ÛÙˆ Î·È ÌÈ·˜ ÌfiÓÔ ‚¿Ûˆ˜ Î·È ‰È·ÁÈÁÓÒ-
ÛÎÔÓÙ·È ÔÌfi˙˘Á˜ ‹ ÂÙÂÚfi˙˘Á˜ ηٷÛÙ¿ÛÂȘ, η-
Ù·Ï˘ÙÈ΋˜ ÛËÌ·Û›·˜ ÁÈ· ÙËÓ ÂÍÂÏÈÎÙÈ΋ ÔÚ›· Ù˘
ÓfiÛÔ˘ (¶›Ó·Î·˜ 3). ªÂ ÙÔÓ ÙÚfiÔ ·˘Ùfi, ηı›ÛٷٷÈ
ÂÊÈÎÙfi˜ Ô ÚÔÁÂÓÓËÙÈÎfi˜, ·fi ·ÌÓÈ·Îfi ˘ÁÚfi (23) ‹
¯ÔÚȷΤ˜ Ï¿¯Ó˜ (24,25), ηıÒ˜ Î·È Ë ÚÔÂÌÊ˘Ù¢-
ÙÈ΋ ‰È¿ÁÓˆÛË ·fi ‚Ï·ÛÙÔ·ÛÙË (26) ‹ ÔÏÈÎfi Ûˆ-
Ì¿ÙÈÔ (27).
¶›Ó·Î·˜ 2. ∆‡ÔÈ ÌÂÙ·ÏϿ͈Ó
1. ∂ÏÏ›„ÂȘ ‹ ‰ÈÏ·ÛÈ·ÛÌÔ› ÂÓfi˜ ‹ ÂÚÈÛÛfiÙÂÚˆÓ ÂÍÔÓ›ˆÓÂÓfi˜ ÁÔÓȉ›Ô˘.
2. ªÂÙ·ÏÏ¿ÍÂȘ ÛÙËÓ ÂÚÈÔ¯‹ ÙÔ˘ ˘ÔÎÈÓËÙ‹.3. ªÂÙ·ÏÏ¿ÍÂȘ Ô˘ ÂËÚ¿˙Ô˘Ó ÙË ‰È·‰Èηۛ· ÙÔ˘ Ì·Ù›-
ÛÌ·ÙÔ˜.4. ªÂÙ·ÏÏ¿ÍÂȘ Ô˘ ·ÏÏ¿˙Ô˘Ó ÙÔ Ï·›ÛÈÔ ·Ó¿ÁÓˆÛ˘
(frameshifts).5. ªÂÙ·ÏÏ¿ÍÂȘ Ô˘ ‰ËÌÈÔ˘ÚÁÔ‡Ó Îˆ‰ÈÎfiÓÈÔ ÙÂÚÌ·ÙÈÛÌÔ‡
(nonsense mutation).6. ªÂÙ·ÏÏ¿ÍÂȘ Ô˘ ·ÏÏ¿˙Ô˘Ó ¤Ó· ·ÌÈÓÔ͇ Ù˘ Ê˘ÛÈÔÏÔÁÈ-
΋˜ ÚˆÙ½Ó˘ Ì ¤Ó· ¿ÏÏÔ (missense mutation).7. MÂÙ·ÏÏ¿ÍÂȘ Ô˘, ÂÓÒ ·ÏÏ¿˙Ô˘Ó ÙÔ Îˆ‰ÈÎfiÓÈÔ ÂÓfi˜ ·ÌÈ-
ÓÔͤԘ, ‰ÂÓ ·ÏÏ¿˙Ô˘Ó ÙÔ ·ÌÈÓÔ͇ Ô˘ Έ‰ÈÎÔÔÈ›ٷÈ(silent mutation).
πÓÙÚfiÓÈÔ
∂ÍfiÓÈÔ
™ËÌÂ›Ô ÂÎΛÓËÛ˘ÌÂÙ·ÁÚ·Ê‹˜ Û RNA
TGA-Έ‰ÈÎfiÓÈÔÙÂÚÌ·ÙÈÛÌÔ‡ ÌÂÙ¿ÊÚ·Û˘
tga-1
∂ÈÎfiÓ· 3. ∆˘ÈÎfi ÁÔÓ›‰ÈÔ Â˘Î·Ú˘ˆÙÈÎÔ‡ ΢ÙÙ¿ÚÔ˘. ∫¿ı ÁÔÓ›-‰ÈÔ ·ÔÙÂÏÂ›Ù·È ·fi Έ‰ÈÎÔÔÈÔ‡Û˜ (ÂÍÒÓÈ·) Î·È ÌË Îˆ‰ÈÎÔ-ÔÈÔ‡Û˜ ÂÚÈÔ¯¤˜ (ÂÛfiÓÈ· ‹ ÈÓÙÚfiÓÈ·).
108 ™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
Paediatriki 2008;71:105-115
Pediatri Mar-Apr 08 10-04-08 12:42 ™ÂÏ›‰·108

∏ ¯Ú‹ÛË Ù˘ PCR ÂӉ›ÎÓ˘Ù·È Â›Û˘ ÛÙË ‰È¿ÁÓˆ-ÛË ÈÔÁÂÓÒÓ ÏÔÈÌÒ͈Ó, ‰ÈfiÙÈ Ë Â˘·ÈÛıËÛ›· Ù˘ ›ӷÈÌÂÁ·Ï‡ÙÂÚË ·ÎfiÌ· Î·È ·fi ·˘Ù‹ ÙˆÓ ·ÓÔÛÔÂÓ˙˘ÌÈ-
ÎÒÓ ÌÂıfi‰ˆÓ (Elisa) (28) Î·È ··ÈÙÂ›Ù·È ÂÏ¿¯ÈÛÙÔ ÁÂ-ÓÂÙÈÎfi ˘ÏÈÎfi ÙÔ˘ ·ıÔÁfiÓÔ˘ ·ÈÙ›Ô˘ (¤Ó· ÌfiÓÔ ·ÓÙ›-ÁÚ·ÊÔ), ÒÛÙ ӷ ÌË ‚·Û›˙ÂÙ·È Ë ‰È¿ÁÓˆÛË ÛÙËÓ ‡·Ú-ÍË ‹ ÌË ÙˆÓ ·ÓÙÈÛˆÌ¿ÙˆÓ ÙÔ˘ (¶›Ó·Î·˜ 4). ∏ PCR¯ÚËÛÈÌÔÔÈÂ›Ù·È Â›Û˘ ÛÙËÓ ·Ó›¯Ó¢ÛË ·ÏÏËÏÔ˘¯ÈÒÓÁÔÓȉÈÒÌ·ÙÔ˜ ÈÒÓ Ô˘ Û¯ÂÙ›˙ÔÓÙ·È ¿ÌÂÛ· Ì ηÎÔ‹-ıÂȘ fiÁÎÔ˘˜ ‹ ÛÙËÓ ·Ó›¯Ó¢ÛË ÌÂÙ·ÏÏ¿ÍÂˆÓ Û ÔÁÎÔ-ÁÔÓ›‰È· ‹/Î·È ÔÁÎÔηٷÛÙ·ÏÙÈο ÁÔÓ›‰È· (¶›Ó·Î·˜ 4).
∏ ·ÓÙ›‰Ú·ÛË Ú·ÁÌ·ÙÔÔÈÂ›Ù·È ÛÙÔ ıÂÚÌÈÎfi ΢-ÎÏÔÔÈËÙ‹, Ô ÔÔ›Ô˜ ·˘ÍÔÌÂÈÒÓÂÈ ÙË ıÂÚÌÔÎÚ·Û›· Ù˘·ÓÙ›‰Ú·Û˘, Ì ÛÎÔfi ÙË ‰È·‰Ô¯È΋ ·Ô‰È¿Ù·ÍË Î·È˘‚ÚȉÔÔ›ËÛË Ù˘ ‰ÈÏ‹˜ ¤ÏÈη˜ DNA. H ·ÓÙ›‰Ú·ÛËPCR ÂÚÈÏ·Ì‚¿ÓÂÈ ÙÚ›· ÛÙ¿‰È· (∂ÈÎfiÓ˜ 4 Î·È 5):
1. AԉȿٷÍË ÙÔ˘ ˘ÔÛÙÚÒÌ·ÙÔ˜ (templatedenaturation) Û ˘„ËÏ‹ ıÂÚÌÔÎÚ·Û›· (94ÔC-96ÔC)Ì ‰È¿ÚÎÂÈ· ÂÓfi˜ ÏÂÙÔ‡.
2. ™‡Ó‰ÂÛË (annealing) ÙˆÓ ÂÎÎÈÓËÙÒÓ Ì ÙȘ Û˘-ÌÏËڈ̷ÙÈΤ˜ ÙÔ˘˜ ·ÏÏËÏÔ˘¯›Â˜ ÛÙÔ DNA Û ıÂÚ-ÌÔÎÚ·Û›· ÌÂٷ͇ 37ÔC-70ÔC Û˘Ó‹ıˆ˜ ÁÈ· ¤Ó· ÏÂÙfi.
3. ∂ÈÌ‹Î˘ÓÛË ÙˆÓ ˘‚ÚȉÈÛÌ¤ÓˆÓ ÂÎÎÈÓËÙÒÓ(primer extension), Ë ÔÔ›· Á›ÓÂÙ·È Û ıÂÚÌÔÎÚ·Û›·
¶›Ó·Î·˜ 3. ¶·Ú·‰Â›ÁÌ·Ù· ÎÏËÚÔÓÔÌÈÎÒÓ ÓÔÛËÌ¿ÙˆÓ Ô˘ ‰‡Ó·-ÓÙ·È Ó· ‰È·ÁÓˆÛıÔ‡Ó Ì PCR
ñ A˘ÙÔۈ̷ÙÈÎfi˜ EÈÎÚ·ÙËÙÈÎfi˜ ∫ˆ‰ÈÎfi˜ PubMed
¶ÔÏ˘Î˘ÛÙÈ΋ ÓfiÛÔ˜ ÙˆÓ ÓÂÊÚÒÓ OMIM 600666¡fiÛÔ˜ ÙÔ˘ Huntington OMIM 143100ª˘ÔÙÔÓÈ΋ ‰˘ÛÙÚÔÊ›· OMIM 160900√˙҉˘ ÛÎÏ‹Ú˘ÓÛË OMIM 191100∫ÒʈÛË DFN∞5 OMIM 608798ÀÂÚ¯ÔÏËÛÙÂÚÔÏ·ÈÌ›· √ªπª 44010ƒÂÙÈÓÔ‚Ï¿Ûو̷ OMIM 180200
ñ ∞˘ÙÔۈ̷ÙÈÎfi˜ YÔÏÂÈfiÌÂÓÔ˜ ∫ˆ‰ÈÎfi˜ PubMed™˘ÁÁÂÓ¤˜ ÓÂÊÚˆÙÈÎfi Û‡Ó‰ÚÔÌÔ √ªπª 600995∫˘ÛÙÈ΋ ›ÓˆÛË √ªπª 219700¡Â˘ÚÔ·ÈÛıËÙ‹ÚÈ· ‚·ÚËÎÔ˝· DFNB1 √ªπª 220290µ ÌÂÛÔÁÂȷ΋ ·Ó·ÈÌ›· √ªπª 141900º·ÈÓ˘ÏÔÎÂÙÔÓÔ˘Ú›· √ªπª 261600™‡Ó‰ÚÔÌÔ Usher 1 OMIM 276900ŒÏÏÂÈ„Ë 21-˘‰ÚÔÍ˘Ï¿Û˘ OMIM 201910NfiÛÔ˜ Tay-Sachs OMIM 272800¡fiÛÔ˜ Gaucher OMIM 230800™‡Ó‰ÚÔÌÔ Bloom OMIM 210900¡ˆÙÈ·›· Ì˘˚΋ ·ÙÚÔÊ›· (SMA) OMIM 253300
ñ à º˘ÏÔÛ‡Ó‰ÂÙÔ˜ ∫ˆ‰ÈÎfi˜ PubMed™‡Ó‰ÚÔÌÔ Â‡ıÚ·˘ÛÙÔ˘ ¯ÚˆÌÔÛÒÌ·ÙÔ˜ à OMIM 300624¡ÂÊÚÔÏÈı›·ÛË OMIM 310468∞ÈÌÔÊÈÏ›· ∞/µ √ªπª 306700/
306900ª˘˚΋ ‰˘ÛÙÚÔÊ›· Duchenne √ªπª 310200ª˘˚΋ ‰˘ÛÙÚÔÊ›· Becker √ªπª 300376∞¯ÚˆÌ·ÙÔ„›· ÂÚ˘ıÚÔ‡-Ú·Û›ÓÔ˘ (‰·ÏÙÔÓÈÛÌfi˜) √ªπª 303900X Ê˘ÏÔÛ‡Ó‰ÂÙË È¯ı‡·ÛË √ªπª 607602Ã Ê˘ÏÔÛ‡Ó‰ÂÙË ·Á·ÌÌ·ÛÊ·ÈÚÈÓ·ÈÌ›· √ªπª 300300ŒÏÏÂÈ„Ë ÁÏ˘Îfi˙˘ 6 ʈÛÊ·Ù¿Û˘ ·Ê˘‰ÚÔÁÔÓ¿Û˘ √ªπª 305900
¶›Ó·Î·˜ 4. ¶·Ú·‰Â›ÁÌ·Ù· ›ÎÙËÙˆÓ ÓÔÛËÌ¿ÙˆÓ Ô˘ ‰‡Ó·ÓÙ·ÈÓ· ‰È·ÁÓˆÛıÔ‡Ó Ì PCR
§ÔÈÌÒ‰Ë ÓÔÛ‹Ì·Ù· ÕÚıÚÔ ∞Ó·ÊÔÚ¿˜πfi˜ ÙÔ˘ Epstein-Barr (EBV) 49∫˘ÙÙ·ÚÔÌÂÁ·ÏÔ˚fi˜ (CMV) 50πfi˜ ·ÏÔ‡ ¤ÚËÙÔ˜ (HSV) 51πfi˜ ÙˆÓ ·ÓıÚˆ›ÓˆÓ ıËÏˆÌ¿ÙˆÓ (HPV) 28ª˘ÎÔ‚·ÎÙ‹ÚÈÔ Ê˘Ì·Ù›ˆÛ˘ 29¡ÂÔϷۛ˜ ∫ˆ‰ÈÎfi˜ PubMed√ÁÎÔηٷÛÙ·ÏÙÈο ÁÔÓ›‰È· BRCA1/ √ªπª 113705/BRCA2 600185P53 √ªπª 191170MYC √ªπª 190080RAS √ªπª 190020
£¤ÚÌ·ÓÛË ÁÈ· ÙÔ
‰È·¯ˆÚÈÛÌfi ÙˆÓ
ÎÏÒÓˆÓ
À‚ÚȉÈÛÌfi˜ ÙˆÓ
ÂÎÎÈÓËÙÒÓ
+DNA ÔÏ˘ÌÂÚ¿ÛË
+dNTPs
¢›ÎψÓÔ DNA
™Ù¿‰ÈÔ 3™Ù¿‰ÈÔ 2
1Ô˜ ·ÎÏÔ˜
™Ù¿‰ÈÔ 1
∂ÈÎfiÓ· 4. ∏ ‚·ÛÈ΋ ·Ú¯‹ Ù˘ ÌÂıfi‰Ô˘ Ù˘ PCR.∏ ‚·ÛÈ΋ ·Ú¯‹ Ù˘ ÌÂıfi‰Ô˘ PCR, fiˆ˜ Ú·ÁÌ·ÙÔÔÈÂ›Ù·È Î·Ù¿ ÙË ‰È¿ÚÎÂÈ· ÂÓfi˜ ·ÎÏÔ˘. √È ‰‡Ô ·Ï˘Û›‰Â˜ DNA ·Ô‰È·Ù¿ÛÛÔÓÙ·È(ÛÙ¿‰ÈÔ 1) Î·È Ô Î¿ı ÂÎÎÈÓËÙ‹˜ ÚÔÛÎÔÏÏ¿Ù·È ÛÙÔ Û˘ÌÏËڈ̷ÙÈÎfi ÙÔ˘ ÎÏÒÓÔ (ÛÙ¿‰ÈÔ 2). √È ÂÎÎÈÓËÙ¤˜ ÂÈÌË·ÓÔÓÙ·È Ì ÙË ‰Ú¿ÛËÙ˘ DNA ÔÏ˘ÌÂÚ¿Û˘ ·ÓÙÈÁÚ¿ÊÔÓÙ·˜ ÙËÓ ÂÚÈÔ¯‹ ÛÙfi¯Ô ÙÔ˘ DNA (ÛÙ¿‰ÈÔ 3).
109ªÔÚȷ΋ ‚ÈÔÏÔÁ›· ÛÙËÓ ·È‰È·ÙÚÈ΋ Ú¿ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:105-115
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·109
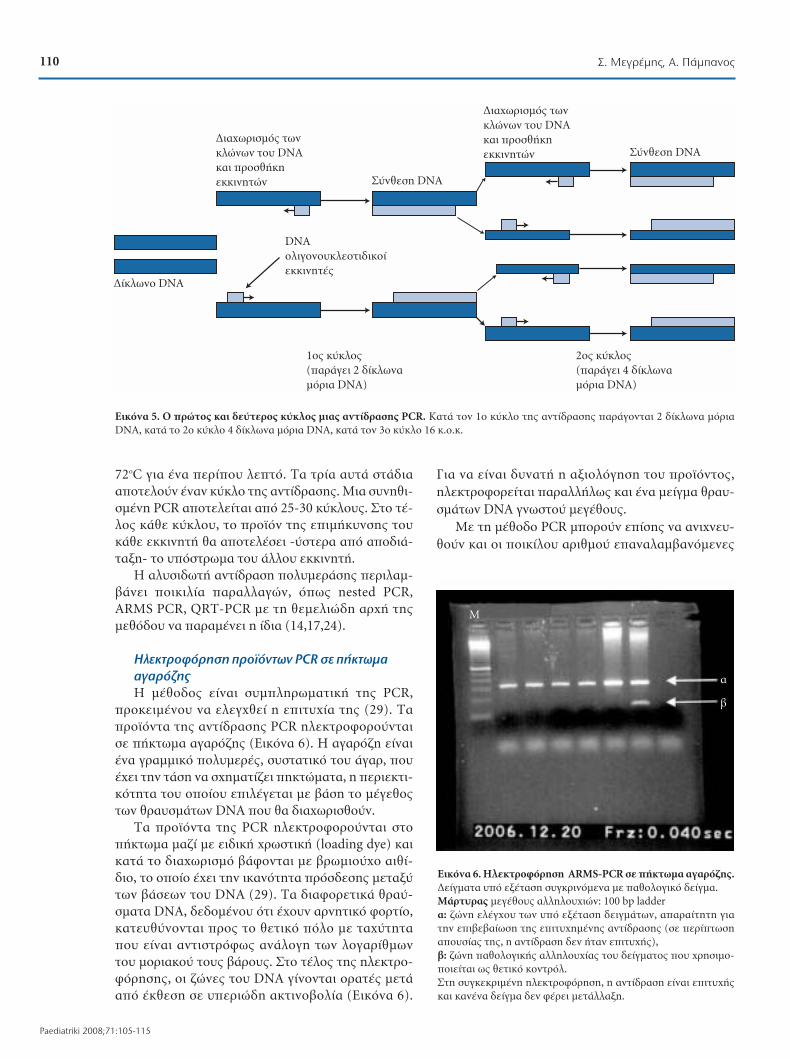
72ÔC ÁÈ· ¤Ó· ÂÚ›Ô˘ ÏÂÙfi. ∆· ÙÚ›· ·˘Ù¿ ÛÙ¿‰È··ÔÙÂÏÔ‡Ó ¤Ó·Ó ·ÎÏÔ Ù˘ ·ÓÙ›‰Ú·Û˘. ªÈ· Û˘ÓËıÈ-Ṳ̂ÓË PCR ·ÔÙÂÏÂ›Ù·È ·fi 25-30 ·ÎÏÔ˘˜. ™ÙÔ Ù¤-ÏÔ˜ οı ·ÎÏÔ˘, ÙÔ ÚÔ˚fiÓ Ù˘ ÂÈÌ‹Î˘ÓÛ˘ ÙÔ˘Î¿ı ÂÎÎÈÓËÙ‹ ı· ·ÔÙÂϤÛÂÈ -‡ÛÙÂÚ· ·fi ·Ô‰È¿-Ù·ÍË- ÙÔ ˘fiÛÙڈ̷ ÙÔ˘ ¿ÏÏÔ˘ ÂÎÎÈÓËÙ‹.
∏ ·Ï˘ÛȉˆÙ‹ ·ÓÙ›‰Ú·ÛË ÔÏ˘ÌÂÚ¿Û˘ ÂÚÈÏ·Ì-‚¿ÓÂÈ ÔÈÎÈÏ›· ·Ú·ÏÏ·ÁÒÓ, fiˆ˜ nested PCR,ARMS PCR, QRT-PCR Ì ÙË ıÂÌÂÏÈÒ‰Ë ·Ú¯‹ Ù˘ÌÂıfi‰Ô˘ Ó· ·Ú·Ì¤ÓÂÈ Ë ›‰È· (14,17,24).
∏ÏÂÎÙÚÔÊfiÚËÛË ÚÔ˚fiÓÙˆÓ PCR Û ‹Îو̷
·Á·Úfi˙˘
∏ ̤ıÔ‰Ô˜ Â›Ó·È Û˘ÌÏËڈ̷ÙÈ΋ Ù˘ PCR,ÚÔÎÂÈ̤ÓÔ˘ Ó· ÂÏÂÁ¯ı› Ë ÂÈÙ˘¯›· Ù˘ (29). ∆·ÚÔ˚fiÓÙ· Ù˘ ·ÓÙ›‰Ú·Û˘ PCR ËÏÂÎÙÚÔÊÔÚÔ‡ÓÙ·ÈÛ ‹Îو̷ ·Á·Úfi˙˘ (∂ÈÎfiÓ· 6). ∏ ·Á·Úfi˙Ë Â›Ó·È¤Ó· ÁÚ·ÌÌÈÎfi ÔÏ˘ÌÂÚ¤˜, Û˘ÛÙ·ÙÈÎfi ÙÔ˘ ¿Á·Ú, Ô˘¤¯ÂÈ ÙËÓ Ù¿ÛË Ó· Û¯ËÌ·Ù›˙ÂÈ ËÎÙÒÌ·Ù·, Ë ÂÚÈÂÎÙÈ-ÎfiÙËÙ· ÙÔ˘ ÔÔ›Ô˘ ÂÈϤÁÂÙ·È Ì ‚¿ÛË ÙÔ Ì¤ÁÂıÔ˜ÙˆÓ ıÚ·˘ÛÌ¿ÙˆÓ DNA Ô˘ ı· ‰È·¯ˆÚÈÛıÔ‡Ó.
∆· ÚÔ˚fiÓÙ· Ù˘ PCR ËÏÂÎÙÚÔÊÔÚÔ‡ÓÙ·È ÛÙÔ‹Îو̷ Ì·˙› Ì ÂȉÈ΋ ¯ÚˆÛÙÈ΋ (loading dye) ηÈηٿ ÙÔ ‰È·¯ˆÚÈÛÌfi ‚¿ÊÔÓÙ·È Ì ‚ÚˆÌÈÔ‡¯Ô ·Èı›-‰ÈÔ, ÙÔ ÔÔ›Ô ¤¯ÂÈ ÙËÓ ÈηÓfiÙËÙ· ÚfiÛ‰ÂÛ˘ ÌÂÙ·Í‡ÙˆÓ ‚¿ÛÂˆÓ ÙÔ˘ DNA (29). ∆· ‰È·ÊÔÚÂÙÈο ıÚ·‡-ÛÌ·Ù· DNA, ‰Â‰Ô̤ÓÔ˘ fiÙÈ ¤¯Ô˘Ó ·ÚÓËÙÈÎfi ÊÔÚÙ›Ô,ηÙ¢ı‡ÓÔÓÙ·È ÚÔ˜ ÙÔ ıÂÙÈÎfi fiÏÔ Ì ٷ¯‡ÙËÙ·Ô˘ Â›Ó·È ·ÓÙÈÛÙÚfiʈ˜ ·Ó¿ÏÔÁË ÙˆÓ ÏÔÁ·Ú›ı̈ÓÙÔ˘ ÌÔÚÈ·ÎÔ‡ ÙÔ˘˜ ‚¿ÚÔ˘˜. ™ÙÔ Ù¤ÏÔ˜ Ù˘ ËÏÂÎÙÚÔ-ÊfiÚËÛ˘, ÔÈ ˙ÒÓ˜ ÙÔ˘ DNA Á›ÓÔÓÙ·È ÔÚ·Ù¤˜ ÌÂÙ¿·fi ¤ÎıÂÛË Û ˘ÂÚÈÒ‰Ë ·ÎÙÈÓÔ‚ÔÏ›· (∂ÈÎfiÓ· 6).
°È· Ó· Â›Ó·È ‰˘Ó·Ù‹ Ë ·ÍÈÔÏfiÁËÛË ÙÔ˘ ÚÔ˚fiÓÙÔ˜,
ËÏÂÎÙÚÔÊÔÚÂ›Ù·È ·Ú·Ïϋψ˜ Î·È ¤Ó· Ì›ÁÌ· ıÚ·˘-
ÛÌ¿ÙˆÓ DNA ÁÓˆÛÙÔ‡ ÌÂÁ¤ıÔ˘˜.
ªÂ ÙË Ì¤ıÔ‰Ô PCR ÌÔÚÔ‡Ó Â›Û˘ Ó· ·ÓȯÓ¢-
ıÔ‡Ó Î·È ÔÈ ÔÈΛÏÔ˘ ·ÚÈıÌÔ‡ ·ӷϷ̂·ÓfiÌÂÓ˜
M
·
‚
∂ÈÎfiÓ· 6. ∏ÏÂÎÙÚÔÊfiÚËÛË ARMS-PCR Û ‹Îو̷ ·Á·Úfi˙˘.¢Â›ÁÌ·Ù· ˘fi ÂͤٷÛË Û˘ÁÎÚÈÓfiÌÂÓ· Ì ·ıÔÏÔÁÈÎfi ‰Â›ÁÌ·.ª¿ÚÙ˘Ú·˜ ÌÂÁ¤ıÔ˘˜ ·ÏÏËÏÔ˘¯ÈÒÓ: 100 bp ladder·: ˙ÒÓË ÂϤÁ¯Ô˘ ÙˆÓ ˘fi ÂͤٷÛË ‰ÂÈÁÌ¿ÙˆÓ, ··Ú·›ÙËÙË ÁÈ·ÙËÓ ÂȂ‚·›ˆÛË Ù˘ ÂÈÙ˘¯Ë̤Ó˘ ·ÓÙ›‰Ú·Û˘ (Û ÂÚ›ÙˆÛË·Ô˘Û›·˜ Ù˘, Ë ·ÓÙ›‰Ú·ÛË ‰ÂÓ ‹Ù·Ó ÂÈÙ˘¯‹˜),‚: ˙ÒÓË ·ıÔÏÔÁÈ΋˜ ·ÏÏËÏÔ˘¯›·˜ ÙÔ˘ ‰Â›ÁÌ·ÙÔ˜ Ô˘ ¯ÚËÛÈÌÔ-ÔÈÂ›Ù·È ˆ˜ ıÂÙÈÎfi ÎÔÓÙÚfiÏ.™ÙË Û˘ÁÎÂÎÚÈ̤ÓË ËÏÂÎÙÚÔÊfiÚËÛË, Ë ·ÓÙ›‰Ú·ÛË Â›Ó·È ÂÈÙ˘¯‹˜Î·È ηӤӷ ‰Â›ÁÌ· ‰ÂÓ Ê¤ÚÂÈ ÌÂÙ¿ÏÏ·ÍË.
110 ™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
Paediatriki 2008;71:105-115
¢›ÎψÓÔ DNA
™‡ÓıÂÛË DNA
¢È·¯ˆÚÈÛÌfi˜ ÙˆÓ
ÎÏÒÓˆÓ ÙÔ˘ DNA
Î·È ÚÔÛı‹ÎË
ÂÎÎÈÓËÙÒÓ
¢È·¯ˆÚÈÛÌfi˜ ÙˆÓ
ÎÏÒÓˆÓ ÙÔ˘ DNA
Î·È ÚÔÛı‹ÎË
ÂÎÎÈÓËÙÒÓ
2Ô˜ ·ÎÏÔ˜
(·Ú¿ÁÂÈ 4 ‰›Îψӷ
ÌfiÚÈ· DNA)
™‡ÓıÂÛË DNA
1Ô˜ ·ÎÏÔ˜
(·Ú¿ÁÂÈ 2 ‰›Îψӷ
ÌfiÚÈ· DNA)
DNA
ÔÏÈÁÔÓÔ˘ÎÏÂÔÙȉÈÎÔ›
ÂÎÎÈÓËÙ¤˜
∂ÈÎfiÓ· 5. √ ÚÒÙÔ˜ Î·È ‰Â‡ÙÂÚÔ˜ ·ÎÏÔ˜ ÌÈ·˜ ·ÓÙ›‰Ú·Û˘ PCR. ∫·Ù¿ ÙÔÓ 1Ô Î‡ÎÏÔ Ù˘ ·ÓÙ›‰Ú·Û˘ ·Ú¿ÁÔÓÙ·È 2 ‰›Îψӷ ÌfiÚÈ·DNA, ηٿ ÙÔ 2Ô Î‡ÎÏÔ 4 ‰›Îψӷ ÌfiÚÈ· DNA, ηٿ ÙÔÓ 3Ô Î‡ÎÏÔ 16 Î.Ô.Î.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·110

·ÏÏËÏÔ˘¯›Â˜ (Variable Number of Tandem Repeats,
VNTRs), Ì‹ÎÔ˘˜ 14-100 ‚¿ÛˆÓ. ÷ڷÎÙËÚ›˙ÔÓÙ·È
·fi ÌÈ· ÎÂÓÙÚÈ΋ ·ÏÏËÏÔ˘¯›· Ô˘ ·ÔÙÂÏÂ›Ù·È ·fi
¤Ó·Ó ·ÚÈıÌfi Ù·˘ÙfiÛËÌˆÓ Â·Ó·Ï·Ì‚·ÓfiÌÂÓˆÓ ·Ï-
ÏËÏÔ˘¯ÈÒÓ, ÔÈ Ôԛ˜ ÔÚÁ·ÓÒÓÔÓÙ·È Û ÔÌ¿‰Â˜ (ÌÂ
·ÚÈıÌfi ·ӿÏ˄˘ 4 ¤ˆ˜ 40 ÊÔÚ¤˜). ∞˘Ù¤˜ ÔÈ ÔÌ¿-
‰Â˜ ‚Ú›ÛÎÔÓÙ·È Û fiÏ· Ù· ¯ÚˆÌÔÛÒÌ·Ù· Î·È ÎÏËÚÔ-
ÓÔÌÔ‡ÓÙ·È Î·È ·fi ÙÔ˘˜ ‰‡Ô ÁÔÓ›˜.
OÈ VNTRs ¯ˆÚ›˙ÔÓÙ·È Û ‰‡Ô ηÙËÁÔڛ˜ Ì ‚¿-
ÛË ÙÔ Ì¤ÁÂıfi˜ ÙÔ˘˜: 1) ÛÙȘ Ì›ÓÈ-‰ÔÚ˘ÊÔÚÈΤ˜ ·ÏÏË-
ÏÔ˘¯›Â˜ (minisatellites) Î·È 2) ÛÙȘ ÌÈÎÚÔ‰ÔÚ˘ÊÔÚÈ-
Τ˜ ·ÏÏËÏÔ˘¯›Â˜ (microsatellites).
OÈ Ì›ÓÈ-‰ÔÚ˘ÊÔÚÈΘ ·ÏÏËÏÔ˘¯›Â˜ ·ÔÙÂÏÔ‡ÓÙ·È
·fi 10-100 bp Î·È ·Ó¢ڛÛÎÔÓÙ·È Û ÂÚÈÛÛfiÙÂÚ˜
·fi 1000 ÂÚÈÔ¯¤˜ ÙÔ˘ ·ÓıÚÒÈÓÔ˘ ÁÔÓȉÈÒÌ·ÙÔ˜.
™˘Û¯ÂÙ›˙ÔÓÙ·È Ì ¯ÚˆÌÔÛˆÌÈΤ˜ ÂÚÈÔ¯¤˜, ÔÈ Ôԛ˜
Â›Ó·È ÂÈÚÚ›˜ Û ıÚ˘ÌÌ·ÙÈÛÌÔ‡˜, fiˆ˜ ÙÂÏÔÌÂÚ›-
‰È·, ÂÓÒ ‚Ú›ÛÎÔÓÙ·È ÎÔÓÙ¿ Û ÛËÌ›· ÌÂÙ·ı¤ÛˆÓ
(30). ∂ÈÚÔÛı¤Ùˆ˜, ÔÈ ÂÚÈÔ¯¤˜ Ô˘ ηχÙÔÓÙ·È
·fi Ì›ÓÈ-‰ÔÚ˘ÊÔÚÈΤ˜ ·ÏÏËÏÔ˘¯›Â˜ Â›Ó·È ÔÈ ÂÚÈÛÛfi-
ÙÂÚÔ ·ÛÙ·ı›˜ ÛÙÔ ·ÓıÚÒÈÓÔ ÁÔÓȉ›ˆÌ· (31). ∏ ¯·Ú-
ÙÔÁÚ¿ÊËÛ‹ ÙÔ˘˜ ‚Ô‹ıËÛ Û ÌÂÁ¿ÏÔ ‚·ıÌfi ÙË ÁÂÓÂÙÈ-
΋ Ù·˘ÙÔÔ›ËÛË (DNA fingerprint) Ô˘ Â›Ó·È ··Ú·›-
ÙËÙË ÛÙËÓ È·ÙÚÔ‰ÈηÛÙÈ΋ Î·È Â›Û˘ ÛÙË ‰È¿ÁÓˆÛË
ÁÂÓÂÙÈÎÒÓ ·ı‹ÛÂˆÓ Ô˘ ÔÊ›ÏÔÓÙ·È Û ÌË Ê˘ÛÈÔÏÔ-
ÁÈÎfi ·Ó·‰ÈÏ·ÛÈ·ÛÌfi ÙÔ˘ DNA (ÔÏ˘ÌÔÚÊÈÛÌÔ›
·ÚÈıÌÔ‡ ·ÓÙÈÁÚ¿ÊˆÓ - copy number variation) (32).
√È ÌÈÎÚÔ‰ÔÚ˘ÊÔÚÈΤ˜ ·ÏÏËÏÔ˘¯›Â˜ (microsatellite
or Small Tandem Repeats, STRs) ·ÔÙÂÏÔ‡ÓÙ·È ·fi
100-200 ‚¿ÛÂȘ. ∂ÎÙÈÌ¿Ù·È fiÙÈ ÔÈ ÌÈÎÚÔ‰ÔÚ˘ÊÔÚÈΤ˜
·ÏÏËÏÔ˘¯›Â˜ ‰ÂÓ ÌÔÚÔ‡Ó Ó· ıˆÚËıÔ‡Ó ˘Â‡ı˘Ó˜
ÁÈ· ÙËÓ ÚfiÎÏËÛË ÓfiÛÔ˘, ·ÏÏ¿ ·ÔÙÂÏÔ‡Ó ÂÍ·ÈÚÂÙÈ-
ÎÔ‡˜ ‰Â›ÎÙ˜ ÁÈ· ÙËÓ Ù·˘ÙÔÔ›ËÛË ÂÓfi˜ ¯ÚˆÌÔÛÒÌ·-
ÙÔ˜ ‹ ÌÈ·˜ ÁÂÓÂÙÈ΋˜ ı¤Û˘ Î·È ‚Ú›ÛÎÔ˘Ó ÂÊ·ÚÌÔÁ‹
ÛÙË ¯·ÚÙÔÁÚ¿ÊËÛË ÁÔÓȉ›ˆÓ Î·È ÛÙoÓ ¤ÏÂÁ¯Ô ·ÙÚfi-
ÙËÙ·˜ (33) (∂ÈÎfiÓ· 7).
∞Ó¿Ï˘ÛË Ù˘ ·ÏÏËÏÔ˘¯›·˜ Ù˘ ÚˆÙÔÙ·ÁÔ‡˜
‰ÔÌ‹˜ ÙÔ˘ DNA (Sequencing)
ªÂ ÙË Ì¤ıÔ‰Ô ·˘Ù‹ ·Ó·ÁÓˆÚ›˙ÂÙ·È Ë ÓÔ˘ÎÏÂÔÙÈ-
‰È΋ ·ÏÏËÏÔ˘¯›· ÂÓfi˜ ÙÌ‹Ì·ÙÔ˜ DNA (.¯. ÁÔÓ›‰ÈÔ),
ÂÈÙÚ¤ÔÓÙ·˜ ¤ÙÛÈ ÙËÓ ·Ó›¯Ó¢ÛË ÌÂÙ·ÏϿ͈Ó
(34,35). ∆Ô ÙÌ‹Ì· Ô˘ ·Ó·Ï‡ÂÙ·È ·Ô‰È·Ù¿ÛÛÂÙ·È
Î·È ÏÂÈÙÔ˘ÚÁ› ˆ˜ Ì‹ÙÚ· ÛÙËÓ ÔÔ›· ˘‚Úȉ›˙ÂÙ·È
¤Ó·˜ ÂÎÎÈÓËÙ‹˜ ÚÔÎÂÈ̤ÓÔ˘ Ó· ÍÂÎÈÓ‹ÛÂÈ Ë ÂÓ˙˘Ì·-
ÙÈ΋ ÂÈÌ‹Î˘ÓÛË Ù˘ ÂÚÈÔ¯‹˜-ÛÙfi¯Ô˘.
∞·Ú·›ÙËÙË ÚÔ¸fiıÂÛË ÁÈ· ÙËÓ ·Ó¿Ï˘ÛË Ù˘
·ÏÏËÏÔ˘¯›·˜ Â›Ó·È Ë Ú·ÁÌ·ÙÔÔ›ËÛË ·ÓÙ›‰Ú·Û˘,
Û‡ÓıÂÛ˘ ·ÓÙÈÁÚ¿ÊˆÓ ÙÔ˘ ȉ›Ô˘ ÌÔÓfiÎψÓÔ˘ DNA-
Ì‹ÙÚ·, Ì ÙË ¯Ú‹ÛË 4 ddNTPs, ηı¤Ó· ·fi Ù· ÔÔ›·
ʤÚÂÈ Û‹Ì·ÓÛË Ì ‰È·ÊÔÚÂÙÈ΋ ÊıÔÚ›˙Ô˘Û· ¯ÚˆÛÙÈ-
΋. ∆Ô ÚÔ˚fiÓ Ù˘ ·ÓÙ›‰Ú·Û˘ ‰È·¯ˆÚ›˙ÂÙ·È Ì ο-
ıÂÙË ËÏÂÎÙÚÔÊfiÚËÛË Û ‹Îو̷ ·ÎÚ˘Ï·Ì›‰Ë˜ ηÈ
‰‡Ó·Ù·È Ó· ·ÓȯÓ¢ı› Ì ‰¤ÛÌË ÊˆÙfi˜ laser (36-39).
∏ ·ÓÙ›‰Ú·ÛË Ï·Ì‚¿ÓÂÈ ¯ÒÚ· Û ıÂÚÌÈÎfi ΢ÎÏÔÔÈË-
Ù‹ (40). ∫·Ù¿ ̤ÛÔ fiÚÔ ··ÈÙÔ‡ÓÙ·È 30-35 ·ÎÏÔÈ,
¤ÙÛÈ ÒÛÙ ӷ ‰È·ÛÊ·ÏÈÛı› Ë ·Ú·ÁˆÁ‹ ·ÚÎÔ‡˜
·ÚÈıÌÔ‡ ·ÓÙÈÁÚ¿ÊˆÓ (∂ÈÎfiÓ· 8).
∏ ¢·ÈÛıËÛ›· Ù˘ ÌÂıfi‰Ô˘ Sequencing Â›Ó·È Ù¤-
ÙÔÈ· ÒÛÙ ӷ ÂÈÙÚ¤ÂÈ ÙËÓ ·Ó›¯Ó¢ÛË ·ÏÏ·Á‹˜ ·Îfi-
ÌË Î·È ÌÈ·˜ ÌfiÓÔ ‚¿Û˘ ÛÙËÓ ˘fi ÌÂϤÙË ·ÏÏËÏÔ˘-
¯›·. ¶ÚfiÎÂÈÙ·È ‰ËÏ·‰‹ ÁÈ· ÌÈ· ÂÍ·ÈÚÂÙÈο ¯Ú‹ÛÈÌË
Ù¯ÓÈ΋, Ë ÔÔ›· ÌÔÚ› Ó· ¯ÚËÛÈÌÔÔÈËı› ÁÈ· ÙËÓ
·Ó›¯Ó¢ÛË ÌÂÙ·ÏÏ¿ÍÂˆÓ Û ÔÔÈÔ‰‹ÔÙ ÁÂÓÂÙÈÎfi
ÓfiÛËÌ·, ÂÊfiÛÔÓ ÁÓˆÚ›˙Ô˘Ì ÙË Ê˘ÛÈÔÏÔÁÈ΋ ÓÔ˘-
ÎÏÂÔÙȉÈ΋ ·ÏÏËÏÔ˘¯›· Ù˘ ÂÚÈÔ¯‹˜-ÛÙfi¯Ô˘.
M C F
Human paternity analysis using NICETM probe 33.6
∂ÈÎfiÓ· 7. ŒÏÂÁ¯Ô˜ ·ÙÚfiÙËÙ·˜ Ì ¯Ú‹ÛË ÙˆÓ VNTRs. M=MËÙ¤Ú·, F= ¶·Ù¤Ú·˜, C= ¶·È‰›.∫¿ı ˙ÒÓË ·ÓÙÈÚÔۈ‡ÂÈ ÌÈÎÚÔ-‰ÔÚ˘ÊÔÚÈΤ˜ ı¤ÛÂȘ(microsatellites). ™Â οı ı¤ÛË ·ÓÙÈÛÙÔÈ¯Ô‡Ó 2 ·ÏÏËÏfiÌÔÚÊ·.º·›ÓÔÓÙ·È ÔÈ ÌÈÎÚÔ-‰ÔÚ˘ÊÔÚÈΤ˜ ı¤ÛÂȘ Ô˘ ¤¯Ô˘Ó ÎÏËÚÔÓÔÌË-ı› ·fi ÙÔÓ Î¿ı ÁÔÓ¤· (ÎfiÎÎÈÓ· ‚¤ÏË-ı¤ÛÂȘ Ô˘ ÎÏËÚÔÓÔÌÔ‡-ÓÙ·È ·fi ÙÔÓ ·Ù¤Ú·, ÌϤ ‚¤ÏË-ı¤ÛÂȘ Ô˘ ÎÏËÚÔÓÔÌÔ‡ÓÙ·È·fi ÙË ÌËÙ¤Ú·).
A C A T C (g>a) A T C C C
∂ÈÎfiÓ· 8. ∞Ó¿Ï˘ÛË Ù˘ ·ÏÏËÏÔ˘¯›·˜ Ù˘ ÚˆÙÔÙ·ÁÔ‡˜ ‰ÔÌ‹˜ÙÔ˘ DNA (Sequencing). ¶·Ú·ÙËÚÂ›Ù·È ·ÓÙÈηٿÛÙ·ÛË ÁÔ˘·Ó›-Ó˘ ·fi ·‰ÂÓ›ÓË.
111ªÔÚȷ΋ ‚ÈÔÏÔÁ›· ÛÙËÓ ·È‰È·ÙÚÈ΋ Ú¿ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:105-115
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·111

ªÂÚÈο ·fi Ù· ÂηÙÔÓÙ¿‰Â˜ ·Ú·‰Â›ÁÌ·Ù· ÁÂÓÂ-
ÙÈÎÒÓ ·ı‹ÛˆÓ, fiÔ˘ Ë Ù¯ÓÈ΋ ·˘Ù‹ ‚Ú›ÛÎÂÈ ÂÊ·Ú-
ÌÔÁ‹ ÁÈ· ÙË ‰È¿ÁÓˆÛË, Â›Ó·È Ë Î˘ÛÙÈ΋ ›ÓˆÛË, Ë Ì˘˚΋
‰˘ÛÙÚÔÊ›·, ÙÔ Û‡Ó‰ÚÔÌÔ Rett, ÔÈ ·ÈÌÔÛÊ·ÈÚÈÓÔ¿ıÂÈ-
˜, Ë Ô˙҉˘ ÛÎÏ‹Ú˘ÓÛË Î·È Ë ÓfiÛÔ˜ Wilson (41,42).
∞ԉȷٷÎÙÈ΋ ̄ ڈ̷ÙÔÁÚ·Ê›· ̆ ÁÚ‹˜ Ê¿Û˘
(Denaturing High Performance Liquid
Chromatography, DHPLC)
¶ÚfiÎÂÈÙ·È ÁÈ· ¤Ó· ÂÍ·ÈÚÂÙÈο ·ÍÈfiÈÛÙÔ Û‡ÛÙËÌ·
·Ó›¯Ó¢Û˘ ÌÂÙ·ÏÏ¿ÍÂˆÓ Î·È Û˘Á¯ÚfiÓˆ˜ ÁÚ‹ÁÔÚÔ,
‰Â‰Ô̤ÓÔ˘ fiÙÈ ÌÔÚ› Ó· Ú·ÁÌ·ÙÔÔÈ‹ÛÂÈ ÙÔÓ
¤ÏÂÁ¯Ô ÂÓfi˜ ‰Â›ÁÌ·ÙÔ˜ Û 6 ÏÂÙ¿. ø˜ ÂÎ ÙÔ‡ÙÔ˘,
ÛÙË ‰È¿ÚÎÂÈ· ÂÓfi˜ 24ÒÚÔ˘ ÌÔÚ› Ó· Ú·ÁÌ·ÙÔÔÈ-
Ëı› Ô ¤ÏÂÁ¯Ô˜ ÂÚ›Ô˘ 240 ‰ÂÈÁÌ¿ÙˆÓ.
∏ Ù¯ÓÈ΋ DHPLC ÌÔÚ› Ó· ¯ÚËÛÈÌÔÔÈËı› ÁÈ·
ÙËÓ ·Ó›¯Ó¢ÛË ÌÂÙ·ÏÏ¿ÍÂˆÓ ÌÈÙÔ¯ÔÓ‰ÚÈ·ÎÔ‡ DNA ‹
ÛËÌÂÈ·ÎÒÓ ÌÂÙ·ÏϿ͈Ó, fiˆ˜ ÂÓı¤ÛˆÓ, ÂÏÏ›„Â-
ˆÓ, ·ÓÙÈηٷÛÙ¿ÛˆÓ, ÛËÌÂÈ·ÎÒÓ ÔÏ˘ÌÔÚÊÈÛÌÒÓ
(SNPs) Î·È ‰È·‰Ô¯ÈÎÒÓ Â·Ó·Ï‹„ÂˆÓ (∂ÈÎfiÓ· 9). √
ÂÓÙÔÈÛÌfi˜ ÙˆÓ ÌÂÙ·ÏÏ¿ÍÂˆÓ Ú·ÁÌ·ÙÔÔÈÂ›Ù·È Ì¤-
Ûˆ Ù˘ ·Ó›¯Ó¢Û˘ ÂÙÂÚÔ‰ÈÌÂÚÒÓ Ô˘ ‰ËÌÈÔ˘ÚÁÔ‡-
ÓÙ·È ÏfiÁˆ ÌË Û˘ÌÏËڈ̷ÙÈÎÒÓ ‚¿ÛÂˆÓ ÛÙÔ ˘fi
ÌÂϤÙË ÙÌ‹Ì· ÙÔ˘ DNA. ∂ÈÚÔÛı¤Ùˆ˜, ÌÔÚ› Ó·
Ú·ÁÌ·ÙÔÔÈËı› ‰È·¯ˆÚÈÛÌfi˜ Ì ‚¿ÛË ÙÔ Ì‹ÎÔ˜
(fragment analysis), ÙËÓ ·Ó¿Ï˘ÛË Î·È ÙÔÓ Î·ı·ÚÈÛÌfi
ÔÏÈÁÔÓÔ˘ÎÏÂÔÙȉ›ˆÓ (Ôligonucleotide purification
and analysis). ∏ ¢·ÈÛıËÛ›· Ù˘ ·Ó›¯Ó¢Û˘ ÌÂÙ·Ï-
Ï¿ÍÂˆÓ Î·È Ë ·ÎÚ›‚ÂÈ· ÙÔ˘ ·ÔÙÂϤÛÌ·ÙÔ˜ ·ÁÁ›˙ÂÈ
ÙÔ 100%, ÂÓÒ Ë ÂÏ¿¯ÈÛÙË ÔÛfiÙËÙ· ÙˆÓ ·ÓÙȉڷÛÙË-
Ú›ˆÓ Î·È ÙÔ ¯·ÌËÏfi ÎfiÛÙÔ˜ ÙÔ˘˜, ÛÂ Û˘Ó‰˘·ÛÌfi ÌÂ
ÙËÓ ·ÔÊ˘Á‹ ¯Ú‹Û˘ ÂÈΛӉ˘ÓˆÓ ¯ËÌÈÎÒÓ Ô˘ÛÈÒÓ,
ηıÈÛÙÔ‡Ó ÙË Ì¤ıÔ‰Ô ·˘Ù‹ ÌÈ· ·fi ÙȘ ϤÔÓ ‰È·‰Â-
‰Ô̤Ó˜ Ù¯ÓÈΤ˜ ÌÔÚÈ·ÎÔ‡ ÂϤÁ¯Ô˘. ÷ڷÎÙËÚÈÛÙÈ-
Îfi ·Ú¿‰ÂÈÁÌ· Ù˘ ÂÊ·ÚÌÔÁ‹˜ ÙÔ˘ DHPLC ·ÔÙÂ-
Ï› Ë ·Ó›¯Ó¢ÛË ÌÂÙ·ÏÏ¿ÍÂˆÓ ÛÙ· 2 ÁÔÓ›‰È· Ô˘ ÂÓ¤-
¯ÔÓÙ·È ÛÙÔÓ Î·ÚΛÓÔ ÙÔ˘ Ì·ÛÙÔ‡ Î·È ÙˆÓ ˆÔıËÎÒÓ,
BRCA1 Î·È BRCA2 (43,44).
ª¤ıÔ‰ÔÈ ̆ ‚ÚȉÔÔ›ËÛ˘: Southern Blotting ηÈ
Northern Blotting
∆Ô Ê·ÈÓfiÌÂÓÔ Ù˘ ˘‚ÚȉÔÔ›ËÛ˘, ‰ËÏ·‰‹ Ù˘
‰˘Ó·ÙfiÙËÙ·˜ ÂÓfi˜ ÌÔÓfiÎψÓÔ˘ ÌÔÚ›Ô˘ ÓÔ˘ÎÏÂ˚ÎÔ‡
ÔͤԘ Ó· Û¯ËÌ·Ù›˙ÂÈ ‰›ÎψÓË ¤ÏÈη Ì ¤Ó· ¿ÏÏÔ ÌÔ-
ÓfiÎψÓÔ ÌfiÚÈÔ, ·ÔÙÂÏ› ÙË ‚¿ÛË ÁÈ· ÔÏϤ˜ Ù¯ÓÈ-
Τ˜ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÙfiÛÔ ÛÙË ÌÔÚȷ΋ ‰È¿-
ÁÓˆÛË, fiÛÔ Î·È ÛÙË ÁÂÓÂÙÈ΋ Ì˯·ÓÈ΋. ªÂٷ͇ ·˘-
ÙÒÓ Û˘ÌÂÚÈÏ·Ì‚¿ÓÔÓÙ·È ÔÈ Ù¯ÓÈΤ˜ Southern ηÈ
NÔrthern Blot.
Southern Blotting
∏ ̤ıÔ‰Ô˜ ÙÔ˘ Southern Blotting ‹Ú ÙÔ fiÓÔÌ¿
Ù˘ ·fi ÙÔÓ Edwin Southern Î·È ÌÔÚ› Ó· ‰È·¯ˆÚ›-
ÛÂÈ, Ì ‚¿ÛË ÙÔ Ì¤ÁÂıÔ˜, Û˘ÁÎÂÎÚÈ̤ӷ ÙÌ‹Ì·Ù· ÁÂ-ÓˆÌÈÎÔ‡ ˘ÏÈÎÔ‡ ·fi ¤Ó· Ì›ÁÌ· ÔÏÏÒÓ ‰È·ÊÔÚÂÙÈ-ÎÒÓ ÙÌËÌ¿ÙˆÓ (45). ∆Ô ÚÔ˜ ·Ó¿Ï˘ÛË DNA (.¯. ÙÔDNA ÂÓfi˜ ÔÚÁ·ÓÈÛÌÔ‡) ˆ¿˙ÂÙ·È Ì ÙË ¯Ú‹ÛË Â-ÚÈÔÚÈÛÙÈÎÔ‡ ÂÓ˙‡ÌÔ˘. °È· ¤Ó·Ó ÔÚÁ·ÓÈÛÌfi Ì ۇÓıÂ-ÙÔ ÁÔÓȉ›ˆÌ·, ·˘Ù‹ Ë ¤„Ë ÌÔÚ› Ó· ‰ËÌÈÔ˘ÚÁ‹ÛÂÈÂηÙÔÌ̇ÚÈ· ‰È·ÊÔÚÂÙÈο ÚÔ˚fiÓÙ· ÎÔ‹˜ (ÎÏ¿-ÛÌ·Ù· ÂÚÈÔÚÈÛÌÔ‡).
∆· ÚÔ˚fiÓÙ· Ù˘ ¤„˘ ‰È·¯ˆÚ›˙ÔÓÙ·È Ì ËÏÂ-ÎÙÚÔÊfiÚËÛË Û ‹Îو̷ ·Á·Úfi˙˘. ªÂÙ¿ ÙËÓ ÔÏÔ-ÎÏ‹ÚˆÛË Ù˘ ËÏÂÎÙÚÔÊfiÚËÛ˘ ÙÔ ‹Îو̷ ÂÎÙ›ıÂ-Ù·È Û ˘ÂÚÈÒ‰Ë ·ÎÙÈÓÔ‚ÔÏ›· Î·È ÙÔ DNA ·ÂÈÎÔÓ›-˙ÂÙ·È ˆ˜ Û˘Ó¯fiÌÂÓË Ù·ÈÓ›·. ¶ÚÔÎÂÈ̤ÓÔ˘ Ó· Á›ÓÔ˘ÓÂÌÊ·Ó‹ Ù· ‰È·ÊÔÚÂÙÈο ıÚ·‡ÛÌ·Ù· Ô˘ ÚÔ·-ÙÔ˘Ó ·fi ÙËÓ ¤„Ë, ÌÂٷʤÚÔÓÙ·È Û ıÂÙÈο ÊÔÚ-ÙÈṲ̂ÓË ÌÂÌ‚Ú¿ÓË Ó¿ÈÏÔÓ ‹ ÓÈÙÚÔ΢ÙÙ·Ú›Ó˘. ¶ÚÈÓÎ·È Î·Ù¿ ÙË ‰È¿ÚÎÂÈ· Ù˘ ÌÂÙ·ÊÔÚ¿˜, ÙÔ ‹Îو̷·Ú·Ì¤ÓÂÈ Û ·ÏηÏÈÎfi ‰È¿Ï˘Ì· ÚÔÎÂÈ̤ÓÔ˘ Ó··Ô‰È·Ù·¯ı› ÙÔ DNA Î·È Ó· Á›ÓÂÈ ÌÔÓfiÎψÓÔ. ∆ÔÊ›ÏÙÚÔ ÛÙË Û˘Ó¤¯ÂÈ· ˘‚Úȉ›˙ÂÙ·È Ì ÛËÌ·Ṳ̂ÓÔ˘˜·ÓȯÓÂ˘Ù¤˜ Ô˘ ʤÚÔ˘Ó ·ÏÏËÏÔ˘¯›Â˜ ÙÔ˘ ˘fi ‰ÈÂ-Ú‡ÓËÛË ÁÔÓȉ›Ô˘, Ì ·ÔÙ¤ÏÂÛÌ· ÙÔ ÌÔÓfiÎψÓÔDNA Ù˘ ÂÚÈÔ¯‹˜ ÙÔ˘ ÁÔÓȉ›Ô˘ Ó· ÛËÌ·›ÓÂÙ·È Î·È¿Ú· Ó· ·ÓȯÓ‡ÂÙ·È. ∆ÂÏÈο, Ë ÊˆÙÔÁÚ¿ÊËÛË ÌÂÊÈÏÌ ·ÎÙ›ÓˆÓ Ã ·ÔηχÙÂÈ Ù· ÛËÌ·Ṳ̂ӷ ıÚ·‡-ÛÌ·Ù· (45) (∂ÈÎfiÓ· 10).
ªÂ ÙË Ì¤ıÔ‰Ô ·˘Ù‹ ÌÔÚÔ‡Ó Ó· ·ÓȯÓ¢ıÔ‡Ó΢ڛˆ˜ ÌÔÚȷΤ˜ ‚Ï¿‚˜ Ô˘ ·ÏÏÔÈÒÓÔ˘Ó ÙÔ Ì‹-ÎÔ˜ ÂÓfi˜ ÙÌ‹Ì·ÙÔ˜ DNA (.¯. ÂÏÏ›ÌÌ·Ù·, ‰ÈÏ·-ÛÈ·ÛÌÔ›), ·ÏÏ¿ fi¯È ÛËÌÂȷΤ˜ ÌÂÙ·ÏÏ¿ÍÂȘ . ∆Ë ÌÂ-Á·Ï‡ÙÂÚË ›Ûˆ˜ ·Í›· ÛÙËÓ ÎÏÈÓÈ΋ Ú¿ÍË Â›¯Â ËÂÊ·ÚÌÔÁ‹ ÙÔ˘ Southern Blotting ÁÈ· ÙËÓ ·Ó›¯Ó¢ÛËÙˆÓ ÔÏ˘ÌÔÚÊÈÛÌÒÓ ÌÂÁ¤ıÔ˘˜ ÎÏ·ÛÌ¿ÙˆÓ ÂÚÈÔ-ÚÈÛÌÔ‡ (RFLP: Ê˘ÛÈÔÏÔÁÈο ÎÏËÚÔÓÔÌÔ‡ÌÂÓ˜
112 ™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
Paediatriki 2008;71:105-115
8
7
6
5
4
3
2
1
0
-1
3,94
4
4,61
2
8,24
8
4,41
2
mV
min765432
∂ÈÎfiÓ· 9. ŒÏÂÁ¯Ô˜ ÌÂÙ·ÏÏ¿ÍÂˆÓ Ì ÙË Ì¤ıÔ‰Ô DHPLC.DHPLC: ∞ԉȷٷÎÙÈ΋ Ãڈ̷ÙÔÁÚ·Ê›· ÀÁÚ‹˜ º¿Û˘. ™‡ÁÎÚÈ-ÛË ‰Â›ÁÌ·ÙÔ˜ ̆ fi ÂͤٷÛË (Ú¿ÛÈÓÔ) Ì ·ıÔÏÔÁÈÎfi ‰Â›ÁÌ· (η-ʤ) ˆ˜ ÛËÌÂ›Ô ·Ó·ÊÔÚ¿˜. ∏ η̇ÏË Ô˘ ˘Ô‰ÂÈÎÓ‡ÂÙ·È ·Ô ÙÔ‚¤ÏÔ˜ ·ÓÙÈÛÙÔȯ› ÛÙËÓ ¤ÎÏÔ˘ÛË ÙˆÓ ÂÙÂÚÔ‰ËÌÂÚÒÓ Ô˘ ‰ËÌÈ-Ô˘ÚÁÔ‡ÓÙ·È ÏfiÁˆ Ù˘ ˘¿Ú¯Ô˘Û·˜ ÌÂÙ¿ÏÏ·Í˘.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·112
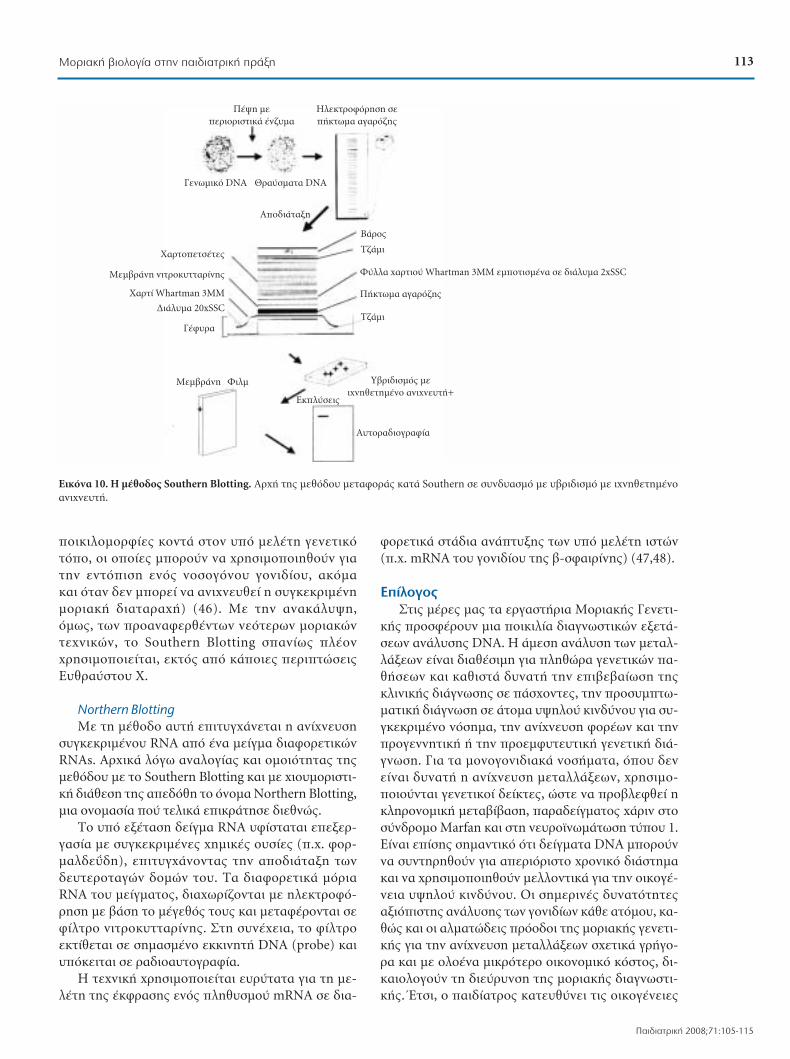
ÔÈÎÈÏÔÌÔÚʛ˜ ÎÔÓÙ¿ ÛÙÔÓ ˘fi ÌÂϤÙË ÁÂÓÂÙÈÎfiÙfiÔ, ÔÈ Ôԛ˜ ÌÔÚÔ‡Ó Ó· ¯ÚËÛÈÌÔÔÈËıÔ‡Ó ÁÈ·ÙËÓ ÂÓÙfiÈÛË ÂÓfi˜ ÓÔÛÔÁfiÓÔ˘ ÁÔÓȉ›Ô˘, ·ÎfiÌ· Î·È fiÙ·Ó ‰ÂÓ ÌÔÚ› Ó· ·ÓȯÓ¢ı› Ë Û˘ÁÎÂÎÚÈ̤ÓËÌÔÚȷ΋ ‰È·Ù·Ú·¯‹) (46). ªÂ ÙËÓ ·Ó·Î¿Ï˘„Ë,fï˜, ÙˆÓ ÚÔ·Ó·ÊÂÚı¤ÓÙˆÓ ÓÂfiÙÂÚˆÓ ÌÔÚÈ·ÎÒÓÙ¯ÓÈÎÒÓ, ÙÔ Southern Blotting Û·Ó›ˆ˜ ϤÔÓ¯ÚËÛÈÌÔÔÈ›ٷÈ, ÂÎÙfi˜ ·fi οÔȘ ÂÚÈÙÒÛÂȘ∂˘ıÚ·‡ÛÙÔ˘ Ã.
Northern Blotting
ªÂ ÙË Ì¤ıÔ‰Ô ·˘Ù‹ ÂÈÙ˘Á¯¿ÓÂÙ·È Ë ·Ó›¯Ó¢ÛËÛ˘ÁÎÂÎÚÈ̤ÓÔ˘ RNA ·fi ¤Ó· Ì›ÁÌ· ‰È·ÊÔÚÂÙÈÎÒÓRNAs. ∞Ú¯Èο ÏfiÁˆ ·Ó·ÏÔÁ›·˜ Î·È ÔÌÔÈfiÙËÙ·˜ Ù˘ÌÂıfi‰Ô˘ Ì ÙÔ Southern µlotting Î·È Ì ¯ÈÔ˘ÌÔÚÈÛÙÈ-΋ ‰È¿ıÂÛË Ù˘ ·Â‰fiıË ÙÔ fiÓÔÌ· Northern µlotting,ÌÈ· ÔÓÔÌ·Û›· Ô‡ ÙÂÏÈο ÂÈÎÚ¿ÙËÛ ‰ÈÂıÓÒ˜.
∆Ô ˘fi ÂͤٷÛË ‰Â›ÁÌ· RNA ˘Ê›ÛÙ·Ù·È ÂÂÍÂÚ-Á·Û›· ÌÂ Û˘ÁÎÂÎÚÈ̤Ó˜ ¯ËÌÈΤ˜ Ô˘Û›Â˜ (.¯. ÊÔÚ-Ì·Ï‰Â˛‰Ë), ÂÈÙ˘Á¯¿ÓÔÓÙ·˜ ÙËÓ ·Ô‰È¿Ù·ÍË ÙˆÓ‰Â˘ÙÂÚÔÙ·ÁÒÓ ‰ÔÌÒÓ ÙÔ˘. T· ‰È·ÊÔÚÂÙÈο ÌfiÚÈ·RNA ÙÔ˘ Ì›ÁÌ·ÙÔ˜, ‰È·¯ˆÚ›˙ÔÓÙ·È Ì ËÏÂÎÙÚÔÊfi-ÚËÛË Ì ‚¿ÛË ÙÔ Ì¤ÁÂıfi˜ ÙÔ˘˜ Î·È ÌÂٷʤÚÔÓÙ·È ÛÂÊ›ÏÙÚÔ ÓÈÙÚÔ΢ÙÙ·Ú›Ó˘. ™ÙË Û˘Ó¤¯ÂÈ·, ÙÔ Ê›ÏÙÚÔÂÎÙ›ıÂÙ·È Û ÛËÌ·Ṳ̂ÓÔ ÂÎÎÈÓËÙ‹ DNA (probe) Î·È˘fiÎÂÈÙ·È Û ڷ‰ÈÔ·˘ÙÔÁÚ·Ê›·.
∏ Ù¯ÓÈ΋ ¯ÚËÛÈÌÔÔÈÂ›Ù·È Â˘Ú‡Ù·Ù· ÁÈ· ÙË ÌÂ-ϤÙË Ù˘ ¤ÎÊÚ·Û˘ ÂÓfi˜ ÏËı˘ÛÌÔ‡ mRNA Û ‰È·-
ÊÔÚÂÙÈο ÛÙ¿‰È· ·Ó¿Ù˘Í˘ ÙˆÓ ˘fi ÌÂϤÙË ÈÛÙÒÓ(.¯. mRNA ÙÔ˘ ÁÔÓȉ›Ô˘ Ù˘ ‚-ÛÊ·ÈÚ›Ó˘) (47,48).
∂›ÏÔÁÔ˜
™ÙȘ ̤Ú˜ Ì·˜ Ù· ÂÚÁ·ÛÙ‹ÚÈ· ªÔÚȷ΋˜ °ÂÓÂÙÈ-΋˜ ÚÔÛʤÚÔ˘Ó ÌÈ· ÔÈÎÈÏ›· ‰È·ÁÓˆÛÙÈÎÒÓ ÂÍÂÙ¿-ÛÂˆÓ ·Ó¿Ï˘Û˘ DNA. ∏ ¿ÌÂÛË ·Ó¿Ï˘ÛË ÙˆÓ ÌÂÙ·Ï-Ï¿ÍÂˆÓ Â›Ó·È ‰È·ı¤ÛÈÌË ÁÈ· ÏËıÒÚ· ÁÂÓÂÙÈÎÒÓ ·-ı‹ÛÂˆÓ Î·È Î·ıÈÛÙ¿ ‰˘Ó·Ù‹ ÙËÓ ÂȂ‚·›ˆÛË Ù˘ÎÏÈÓÈ΋˜ ‰È¿ÁÓˆÛ˘ Û ¿Û¯ÔÓÙ˜, ÙËÓ ÚÔÛ˘ÌÙˆ-Ì·ÙÈ΋ ‰È¿ÁÓˆÛË Û ¿ÙÔÌ· ˘„ËÏÔ‡ ÎÈÓ‰‡ÓÔ˘ ÁÈ· Û˘-ÁÎÂÎÚÈ̤ÓÔ ÓfiÛËÌ·, ÙËÓ ·Ó›¯Ó¢ÛË ÊÔÚ¤ˆÓ Î·È ÙËÓÚÔÁÂÓÓËÙÈ΋ ‹ ÙËÓ ÚÔÂÌÊ˘Ù¢ÙÈ΋ ÁÂÓÂÙÈ΋ ‰È¿-ÁÓˆÛË. °È· Ù· ÌÔÓÔÁÔÓȉȷο ÓÔÛ‹Ì·Ù·, fiÔ˘ ‰ÂÓÂ›Ó·È ‰˘Ó·Ù‹ Ë ·Ó›¯Ó¢ÛË ÌÂÙ·ÏϿ͈Ó, ¯ÚËÛÈÌÔ-ÔÈÔ‡ÓÙ·È ÁÂÓÂÙÈÎÔ› ‰Â›ÎÙ˜, ÒÛÙ ӷ ÚÔ‚ÏÂÊı› ËÎÏËÚÔÓÔÌÈ΋ ÌÂÙ·‚›‚·ÛË, ·Ú·‰Â›ÁÌ·ÙÔ˜ ¯¿ÚÈÓ ÛÙÔÛ‡Ó‰ÚÔÌÔ Marfan Î·È ÛÙË Ó¢ÚÔ˚ӈ̿وÛË Ù‡Ô˘ 1.∂›Ó·È ›Û˘ ÛËÌ·ÓÙÈÎfi fiÙÈ ‰Â›ÁÌ·Ù· DNA ÌÔÚÔ‡ÓÓ· Û˘ÓÙËÚËıÔ‡Ó ÁÈ· ·ÂÚÈfiÚÈÛÙÔ ¯ÚÔÓÈÎfi ‰È¿ÛÙËÌ·Î·È Ó· ¯ÚËÛÈÌÔÔÈËıÔ‡Ó ÌÂÏÏÔÓÙÈο ÁÈ· ÙËÓ ÔÈÎÔÁ¤-ÓÂÈ· ˘„ËÏÔ‡ ÎÈÓ‰‡ÓÔ˘. √È ÛËÌÂÚÈÓ¤˜ ‰˘Ó·ÙfiÙËÙ˜·ÍÈfiÈÛÙ˘ ·Ó¿Ï˘Û˘ ÙˆÓ ÁÔÓȉ›ˆÓ οı ·ÙfiÌÔ˘, η-ıÒ˜ Î·È ÔÈ ·ÏÌ·ÙÒ‰ÂȘ ÚfiÔ‰ÔÈ Ù˘ ÌÔÚȷ΋˜ ÁÂÓÂÙÈ-΋˜ ÁÈ· ÙËÓ ·Ó›¯Ó¢ÛË ÌÂÙ·ÏÏ¿ÍÂˆÓ Û¯ÂÙÈο ÁÚ‹ÁÔ-Ú· Î·È Ì ÔÏÔ¤Ó· ÌÈÎÚfiÙÂÚÔ ÔÈÎÔÓÔÌÈÎfi ÎfiÛÙÔ˜, ‰È-ηÈÔÏÔÁÔ‡Ó ÙË ‰È‡ڢÓÛË Ù˘ ÌÔÚȷ΋˜ ‰È·ÁÓˆÛÙÈ-΋˜. ŒÙÛÈ, Ô ·È‰›·ÙÚÔ˜ ηÙ¢ı‡ÓÂÈ ÙȘ ÔÈÎÔÁ¤ÓÂȘ
¶¤„Ë ÌÂ
ÂÚÈÔÚÈÛÙÈο ¤Ó˙˘Ì·
°ÂÓˆÌÈÎfi DNA £Ú·‡ÛÌ·Ù· DNA
÷ÚÙÔÂÙÛ¤Ù˜
ªÂÌ‚Ú¿ÓË ÓÈÙÚÔ΢ÙÙ·Ú›Ó˘
÷ÚÙ› Whartman 3MM
¢È¿Ï˘Ì· 20xSSC
°¤Ê˘Ú·
ªÂÌ‚Ú¿ÓË ºÈÏÌ
∂ÎχÛÂȘ
∞˘ÙÔÚ·‰ÈÔÁÚ·Ê›·
∆˙¿ÌÈ
À‚ÚȉÈÛÌfi˜ ÌÂ
ȯÓËıÂÙË̤ÓÔ ·ÓȯÓÂ˘Ù‹+
∆˙¿ÌÈ
µ¿ÚÔ˜
∞ԉȿٷÍË
¶‹Îو̷ ·Á·Úfi˙˘
º‡ÏÏ· ¯·ÚÙÈÔ‡ Whartman 3MM ÂÌÔÙÈṲ̂ӷ Û ‰È¿Ï˘Ì· 2xSSC
∏ÏÂÎÙÚÔÊfiÚËÛË ÛÂ
‹Îو̷ ·Á·Úfi˙˘
∂ÈÎfiÓ· 10. ∏ ̤ıÔ‰Ô˜ Southern Blotting. AÚ¯‹ Ù˘ ÌÂıfi‰Ô˘ ÌÂÙ·ÊÔÚ¿˜ ηٿ Southern ÛÂ Û˘Ó‰˘·ÛÌfi Ì ˘‚ÚȉÈÛÌfi Ì ȯÓËıÂÙË̤ÓÔ·ÓȯÓÂ˘Ù‹.
113ªÔÚȷ΋ ‚ÈÔÏÔÁ›· ÛÙËÓ ·È‰È·ÙÚÈ΋ Ú¿ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:105-115
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·113

Ì ÙÔ ÁÂÓÂÙÈÎfi Úfi‚ÏËÌ· ÛÙȘ ηٿÏÏËϘ ˘ËÚÂ-ۛ˜ ÎÏÈÓÈ΋˜ Î·È ÌÔÚȷ΋˜ ÁÂÓÂÙÈ΋˜, ÒÛÙ ÂÁη›-Úˆ˜ Î·È ̆ ‡ı˘Ó· Ó· ÂÓËÌÂÚÒÓÔÓÙ·È ÁÈ· ÙȘ ‰˘Ó·Ùfi-ÙËÙ˜ Ô˘ ÌÔÚÔ‡Ó Ó· ÙÔ˘˜ ÚÔÛÊÂÚıÔ‡Ó ÛÙ· Ï·›-ÛÈ· Ù˘ ÌÔÚȷ΋˜ ‰È¿ÁÓˆÛ˘.
µÈ‚ÏÈÔÁÚ·Ê›·
1. DNA From The Beginning.org [Webpage, Internet]. ColdSpring Harbor Laboratory; 2002: http://www.dnaftb.org/
2. πÛÙÔÚ›· Ù˘ ∆¯ÓÔÏÔÁ›·˜. ªÂ ·ÚÂ΂¿ÛÂȘ ÛÂ Û˘Ó·Ê‹ÁÂÁÔÓfiÙ· Ô˘ ÂËÚ¤·Û·Ó ÙËÓ ÂÈÛÙ‹ÌË, ÙËÓ Ù¯ÓÔÏÔÁ›·Î·È ÙÔÓ ÔÏÈÙÈÛÌfi. [Webpage, Internet]. Styl. G. Fran-gopoulos; 2007: http://www.sfrang.com/historia/
3. π∞™¶π™ π‰Â҉˜ ∞™ÎÏËÈ·Îfi ¶¿ÚÎÔ π·ÙÚÈ΋˜ ™¯ÔÏ‹˜[Webpage, Internet]. ∞ÛÎÏËÈ·Îfi ¶¿ÚÎÔ π·ÙÚÈ΋˜™¯ÔÏ‹˜ ¶·ÓÂÈÛÙËÌ›Ô˘ ∞ıËÓÒÓ; 2006: http://panacea.med.uoa.gr/
4. Morgan TH. Chromosomes and Heredity. The AmericanNaturalist 1910;44:449-496. [Internet] ElectronicallyScholarly Publishing. Webpage: http://www.esp.org/foun-dations/
5. History of Genetics: the Discovery of the Watson-CrickModel of DNA from World of Genetics 2005-2006. Thom-son Gale, a part of the Thomson Corporation. [Webpage,Internet]. http://www.bookrags.com/research/history-of-genetics-the-discovery-o-wog/
6. International Human Genome Sequencing Consortium.Finishing the euchromatic sequence of the human genome.Nature 2004;431 (7011):931-45.
7. Watson JD, Balker TA, Bell SP, Gann A, Levine M, LosickR. Molecular Biology of the Gene, 5th ed. Benjamin Cum-mings, Pearson Education & Cold Spring Harbor Labora-tory Press; 2004.
8. Read A, Donnai D. New Clinical Genetics. Scion Publish-ing Ltd.; 2007.
9. Böyum A. Isolation of mononuclear cells and granulocytesfrom human blood. Isolation of mononuclear cells by onecentrifugation, and of granulocytes by combining centrifu-gation and sedimentation at 1 g. Scand J Clin Lab InvestSuppl. 1968;97:77-89.
10. Hoopes BC, McClure WR. Studies on the selectivity ofDNA precipitation by spermine. Nucleic Acids Res. 1981;9:5493-5504.
11. Miller SA, Dykes DD, Polesky HF. A simple salting outprocedure for extracting DNA from human nucleatedcells. Nucleic Acids Res. 1988;16:1215.
12. Wolff RK, Frazer KA, Jakler RK, Lanser MJ, Pitts LH, CoxDR. Analysis of chromosome 22 deletions in neurofibro-matosis type 2-related tumors. Am J Hum Genet. 1992;51:478-485.
13. Birren B, Green ED, Klapholz S, Myers RM, Roskams J, ed-itors. Genome Analysis: A Laboratory Manual. Vol. 1: An-alyzing DNA. Cold Spring Harbor Laboratory Press; 1997.
14. Mullis KB, Faloona FA. Specific synthesis of DNA in vitrovia a polymerase-catalyzed chain reaction. Methods Enzy-mol. 1987;155:335-350.
15. Abramson RD. Thermostable DNA polymerases. In: InnesMA, Gelfand DH, Sninsky JJ, editors. PCR strategies. SanDiego: Academic Press; 1995. p. 39-55.
16. Bej AK, Mahbubani MH. Thermostable DNA polymerasesfor in vitro DNA amplifications. In: Griffen HG, Griffen
AM, editors. PCR Technology, Current Innovations. Flori-
da: CRC Press, Inc., Boca Raton; 1994. p. 219-237.
17. Mullis KB. The unusual origin of the polymerase chain re-
action. Sci Am. 1990;262:56-61, 64-65.
18. Barnes WM. PCR amplification of up to 35-kb DNA with
high fidelity and high yield from lambda bacteriophage
templates. Proc Natl Acad Sci USA. 1994;91:2216-2220.
19. Cheng S, Chang SY, Gravitt P, Respess R. Long PCR. Na-
ture 1994;369:684-685.
20. Cheng, S, Fockler C, Barnes WM, Higuchi R. Effective am-
plification of long targets from cloned inserts and human
genomic DNA. Proc Natl Acad Sci USA 1994;91:5695-
5699.
21. Li YY, Hengstenberg C, Maisch B. Whole mitochondrial
genome amplification reveals basal level multiple deletions
in mtDNA of patients with dilated cardiomyopathy.
Biochem Biophys Res Commun. 1995;210:211-218.
22. Chelly J, Kahn A. RT-PCR and mRNA quantitation. In:
Mullis DB, Ferre F, Gibbs R, editors. The Polymerase
Chain Reaction. Boston: Birkhäuser; 1994. p. 97-109.
23. Moatter T, Khilji Z, Murad F, Munim S. Analysis of amni-
otic fluid specimens for common chromosome disorders
using interphase fluorescence in situ hybridization. J Pak
Med Assoc. 2007;57:189-192.
24. Nagel HTC, Knegt AC, Kloosterman MD, Wildschut HIJ,
Leschot NJ, Vandenbussche FPHA. Prenatal diagnosis in
the Netherlands, 1991-2000: Number of invasive proce-
dures, indications, abnormal results and terminations of
pregnancy. Prenat Diagn. 2007;27:251-257.
25. Caughey AB, Hopkins LM, Norton ME. Chorionic villus
sampling compared with amniocentesis and the difference
in the rate of pregnancy loss. Obstet Gynecol. 2006;108:
612-616.
26. Kokkali G, Traeger-Synodinos J, Vrettou C, Stavrou D,
Jones GM, Cram DS, et al. Blastocyst biopsy versus cleav-
age stage biopsy and blastocyst transfer for preimplanta-
tion genetic diagnosis of beta-thalassaemia: a pilot study.
Hum Reprod. 2007;22:1443-1449.
27. Miny P, De Geyter Ch, Holzgreve W. New options in pre-
natal and preimplantation diagnosis of genetic disorders.
Ther Umsch. 2006;63:703-709.
28. Yoshida T, Sano T, Kanuma T, Owada N, Sakurai S, Fuku-
da T, et al. Quantitative real-time polymerase chain reac-
tion analysis of the type distribution, viral load, and physi-
cal status of human papillomavirus in liquid-based cytol-
ogy samples from cervical lesions. Int J Gynecol Cancer.
2008;18:121-127.
29. Liu KT, Su WJ, Perng RP. Clinical utility of polymerase
chain reaction for diagnosis of smear-negative pleural tu-
berculosis. J Chin Med Assoc. 2007;70:148-151.
30. Du J, Zhu Y, Shanmugam A, Kenter AL. ∞nalysis of im-
munoglobulin Sgamma3 recombination breakpoints by
PCR: implications for the mechanism of isotype switching.
Nucleic Acids Res. 1997;25:3066-3073.
31. Edwards A, Hammond HA, Jin L, Caskey CT, Chakraborty
R. Genetic variation at five trimeric and tetrameric tandem
repeat loci in four human population groups. Genomics.
1992;12:241-253.
32. Redon R, Ishikawa S, Fitch KR, Feuk L, Perry GH, Andrews
TD, et al. Global variation in copy number in the human
genome. Nature. 2006;444:444-454.
33. Li YC, Korol AB, Fahima T, Beiles A, Nevo E. Microsatellites:
114 ™. ªÂÁÚ¤Ì˘, ∞. ¶¿Ì·ÓÔ˜
Paediatriki 2008;71:105-115
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·114
115ªÔÚȷ΋ ‚ÈÔÏÔÁ›· ÛÙËÓ ·È‰È·ÙÚÈ΋ Ú¿ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:105-115
genomic distribution, putative functions and mutationalmechanisms: a review. Mol Ecol. 2002;11:2453-2465.
34. Kessler C. The digoxigenin:anti-digoxigenin (DIG) tech-nology--a survey on the concept and realization of a novelbioanalytical indicator system. Mol Cell Probes. 1991;5:161-205.
35. Saiki RK, Gelfand DH, Stoffel S, Scharf SJ, Higuchi R,Horn GT, et al. Primer-directed enzymatic amplificationof DNA with a thermostable DNA polymerase. Science.1988;239:487-491.
36. Sanger F, Nicklen S, Coulson AR. DNA sequencing withchain-terminating inhibitors. Proc Natl Acad Sci USA.1977;74:5463-5467.
37. Maxam AM, Gilbert W. A new method for sequencingDNA. Proc Natl Acad Sci USA. 1977;74:560-564.
38. Zimmermann J, Voss H, Schwager C, Stegemann J, An-sorge W. Automated Sanger dideoxy sequencing reactionprotocol. FEBS Lett. 1988;233:432-436.
39. Mardis ER, Roe BA. Automated methods for single-stranded DNA isolation and dideoxynucleotide DNA se-quencing reactions on a robotic workstation. Biotech-niques. 1989;7:840-850.
40. Oste CC. PCR Instrumentation: Where Do We Stand? In:Mullis K, Ferré F, Gibbs RA, editors. The PolymeraseChain Reaction. Boston: Birkhäuser; 1994. p. 165-173.
41. Wilson RK, Chen C, Avdalovic N, Burns J, Hood L. Devel-opment of an automated procedure for fluorescent DNAsequencing. Genomics. 1990;6:626-634.
42. Koop BF, Wilson RK, Chen C, Halloran N, Sciammis R,Hood L, et al. Sequencing reactions in microtiter plates.Biotechiques. 1990;9:32, 34-37.
43. Konstantopoulou I, Rampias T, Ladopoulou A, Kout-sodontis G, Armaou S, Anagnostopoulos T, et. al. GreekBRCA1 and BRCA2 mutation spectrum: two BRCA1 mu-tations account for half the carriers found among high-riskbreast/ovarian cancer patients. Breast Cancer Res Treat.2008;107:431-441.
44. Lim KS, Naviaux RK, Haas RH. Quantitative mitochondr-ial DNA mutation analysis by denaturing HPLC. ClinChem. 2007;53:1046-1052.
45. Southern EM. Detection of specific sequences among DNAfragments separated by gel electrophoresis. J Mol Biol.1975;98:503-517.
46. Harper P. Practical Genetic Counselling. 5th ed. London:Reed Educational and Professional Publishing Ltd; 1998.
47. Kingston HM. ABC of Clinical Genetics. 3rd ed. London:BMJ Books; 2002.
48. Wahl GM, Meinkoth JL, Kimmel AR. Northern andSouthern blots. Methods Enzymol. 1987;152:572-581.
49. Prichard MN, Daily SL, Jefferson GM, Perry AL, Kern ER.A rapid DNA hybridization assay for the evaluation of an-tiviral compounds against Epstein-Barr virus. J VirolMethods. 2007;144:86-90.
50. Caliendo AM, Ingersoll J, Fox-Canale AM, Pargman S,Bythwood T, Hayden MK, et al. Evaluation of real-timePCR laboratory-developed tests using analyte-specificreagents for cytomegalovirus quantification. J Clin Micro-biol. 2007;45:1723-1727.
51. Strick LB, Wald A. Diagnostics for herpes simplex virus: isPCR the new gold standard? Mol Diagn Ther. 2006;10:17-28.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·115

116 ∞¡∞™∫√¶∏™∏ REVIEW ARTICLE
Paediatriki 2008;71:116-122
¡ÂfiÙÂÚ· ‰Â‰Ô̤ӷ ÁÈ· ÙË ‰È·ÙÚÔÊ‹ ÙÔ˘ ‚Ú¤ÊÔ˘˜
Ã. ∫ÒÛÙ·ÏÔ˜
¶ÂÚ›ÏË„Ë: ∏ ÚÔÛ¿ıÂÈ· Ì›ÌËÛ˘ ÙÔ˘ ÌËÙÚÈÎÔ‡ Á¿Ï·ÎÙÔ˜ ÁÈ· ÙË ‰È·ÙÚÔÊ‹ ÙÔ˘ ‚Ú¤ÊÔ˘˜ Ô‰‹ÁËÛ ÛÂÛÔ‚·Ú¿ Ï¿ıË ÎÈ ·˘Ùfi ‰ÈfiÙÈ Ë Û‡ÛÙ·ÛË ÙÔ˘ ·ÓıÚˆ›ÓÔ˘ Á¿Ï·ÎÙÔ˜ ‰ÂÓ Â›Ó·È ÛÙ·ıÂÚ‹ Î·È ÂÍ¿ÏÏÔ˘ Ë ‚ÈÔ-‰È·ıÂÛÈÌfiÙËÙ· ÙˆÓ ‰È·ÊfiÚˆÓ Û˘ÛÙ·ÙÈÎÒÓ ÛÙÔ ÌËÙÚÈÎfi Á¿Ï· Â›Ó·È ‰È·ÊÔÚÂÙÈ΋ ·’ fi,ÙÈ ÛÙ· ÙÚÔÔÔÈË-̤ӷ Á¿Ï·Ù·. ∏ ·ÚÔ‡Û· ·Ó·ÛÎfiËÛË ÂȯÂÈÚ› Ó· Ú›ÍÂÈ ÌÈ· ÎÚÈÙÈ΋ Ì·ÙÈ¿ Û ÔÚÈṲ̂ӷ ÓÂfiÙÂÚ· Û˘-ÛÙ·ÙÈο ÙÔ˘ ÚÔÛ·ÚÌÔṲ̂ÓÔ˘ ÚÔ˜ ÙÔ ÌËÙÚÈÎfi Á¿Ï·, fiˆ˜ Â›Ó·È Ù· ÓÔ˘ÎÏÂÔÙ›‰È·, Ù· ÔÏ˘·ÎfiÚÂÛÙ· ÏÈ-·Ú¿ Ôͤ·, Ë ÁÏÔ˘Ù·Ì›ÓË, Ë ·ÚÁÈÓ›ÓË, Ë Î·ÚÓÈÙ›ÓË, Ô Û›‰ËÚÔ˜, Ù· Ú‚ÈÔÙÈο, Ù· ÚÔ‚ÈÔÙÈο Î·È Ù· Á¿-Ï·Ù· ˘„ËÏ‹˜ ıÚÂÙÈ΋˜ ·Í›·˜. ∞fi ÙË Û˘˙‹ÙËÛË ÚÔ·ÙÂÈ fiÙÈ ÁÈ· ÔÚÈṲ̂Ó˜ Ô˘Û›Â˜ ‰ÂÓ ˘¿Ú¯Ô˘Ó·Ú΋ ÛÙÔȯ›· Ô˘ Ó· ‰ÈηÈÔÏÔÁÔ‡Ó ÙËÓ ÚÔÛı‹ÎË ÙÔ˘˜. ø˜ ÂÎ ÙÔ‡ÙÔ˘, ÔÔÈ·‰‹ÔÙ ÙÚÔÔÔ›ËÛË ˆ˜ÚÔ˜ ÙË Û‡ÓıÂÛË ÙˆÓ ¯ÔÚËÁÔ‡ÌÂÓˆÓ Á·Ï¿ÙˆÓ ı· Ú¤ÂÈ Ó· Á›ÓÂÙ·È ÌfiÓÔ ¤ÂÈÙ· ·fi ÂÓ‰Âϯ›˜ ÎÏÈÓÈΤ˜ÌÂϤÙ˜, Ì ÛÙfi¯Ô fi¯È ÌfiÓÔ Ù˘¯fiÓ ‚Ú·¯˘ÚfiıÂÛÌÔ fiÊÂÏÔ˜, ·ÏÏ¿ Î·È ÙËÓ Â˘ÓÔ˚΋ ›وÛË ÂÓfi˜ Û˘ÁÎÂ-ÎÚÈ̤ÓÔ˘ ÙÚÔÊÈÎÔ‡ ·Ú¿ÁÔÓÙ· ÛÙË ÓÔËÙÈ΋ ÂͤÏÈÍË ÙÔ˘ ‚Ú¤ÊÔ˘˜, ηıÒ˜ Î·È Û ¯ÚfiÓÈ· ÓÔÛ‹Ì·Ù· Ù˘ÂÓËÏ›ÎÔ˘ ˙ˆ‹˜.
§¤ÍÂȘ ÎÏÂȉȿ: ¢È·ÙÚÔÊ‹ ‚Ú¤ÊÔ˘˜, ÓÔ˘ÎÏÂÔÙ›‰È·, ÔÏ˘·ÎfiÚÂÛÙ· ÏÈ·Ú¿ Ôͤ·, ÁÏÔ˘Ù·Ì›ÓË, ·ÚÁÈÓ›ÓË, ηÚÓÈÙ›ÓË,
Û›‰ËÚÔ˜, Ú‚ÈÔÙÈο, ÚÔ‚ÈÔÙÈο, Á¿Ï·Ù· ˘„ËÏ‹˜ ‰È·ÙÚÔÊÈ΋˜ ·Í›·˜.
New aspects of infant nutrition
C. Costalos
Abstract: Efforts to imitate human milk for feeding the infant led to serious miscalculations of the levelsof supplementation needed, with resultant dangers. As the exact content of human milk is difficult toestimate due to its wide fluctuations, only limited information can be deduced from measurement ofthe levels of specific components of human milk. In addition, there may be possible differences inbioavailability and substances other than components of human milk may be needed to achieve thedesired effect. This article provides a critical review of these factors, which include nucleotides,polyunsaturated fatty acids, glutamine, arginine, carnitine, iron, prebiotics, probiotics and high energyformulae. Following discussion of these nutrients, it is concluded that for some of them there isinsufficient data to justify their use and that there may even be potential dangers from their inclusion.Independent scientific bodies should evaluate any proposed modification of infant formulae beyondthe established standards before permission is given for introduction of such products into the market.It is important that such research considers not only the short-term effects of the nutrients on growth,but also safety aspects and the possibility of evaluating long-term effects on neurodevelopmentalachievement and the incidence of chronic diseases.
Key words: Infant nutrition, nucleotides, polyunsaturated fatty acids, glutamine, arginine, carnitine, iron,
prebiotics, probiotics, high energy formulae.
¡ÂÔÁÓÔÏÔÁÈÎfi ∆Ì‹Ì· ¶ÂÚÈÊÂÚÂÈ·ÎÔ‡ °ÂÓÈÎÔ‡¡ÔÛÔÎÔÌ›Ԣ“∞ÏÂÍ¿Ó‰Ú·” ∞ıËÓÒÓ
AÏÏËÏÔÁÚ·Ê›·:
Ã. ∫ÒÛÙ·ÏÔ˜[email protected]¡ÂÔÁÓÔÏÔÁÈÎfi ∆Ì‹Ì·,¶ÂÚÈÊÂÚÂÈ·Îfi °ÂÓÈÎfi¡ÔÛÔÎÔÌ›ԓ∞ÏÂÍ¿Ó‰Ú·” ∞ıËÓÒÓ
Neonatal Unit, Alexandra Regional GeneralHospital, Athens, Greece
Correspondence:
C. Costalos [email protected] Unit, Alexandra Regional GeneralHospital, Athens, Greece
∆· ÙÂÏÂ˘Ù·›· ¯ÚfiÓÈ· Á›Ó·Ì ̿ÚÙ˘Ú˜ ÌÈ·˜ÌÂÙ·ÛÙÚÔÊ‹˜ ˆ˜ ÚÔ˜ ÙÔ˘˜ ÛÙfi¯Ô˘˜ Ù˘ ‰È·-ÙÚÔÊ‹˜ ÙÔ˘ ‚Ú¤ÊÔ˘˜. EÓÒ ·Ï·ÈfiÙÂÚ· Ô Î‡ÚÈÔ˜ÛÙfi¯Ô˜ ηٿ ÙËÓ ·Ú·Û΢‹ ÂÓfi˜ ÚÔÛ·ÚÌÔ-Ṳ̂ÓÔ˘ ÚÔ˜ ÙÔ ÌËÙÚÈÎfi Á¿Ï· ‹Ù·Ó Ë ·ÚÔ¯‹ÛˆÛÙ‹˜ ÔÛfiÙËÙ·˜ Î·È ·Ó·ÏÔÁ›·˜ ÌÂÁ·ÏÔÌÔ-ÚÈ·ÎÒÓ Û˘ÛÙ·ÙÈÎÒÓ, Û‹ÌÂÚ· Ë ¤Ú¢ӷ ·Ô‚Ϥ-ÂÈ ÛÙÔÓ ÂÌÏÔ˘ÙÈÛÌfi ÙÔ˘ Á¿Ï·ÎÙÔ˜ Ì ÂȉÈÎ¿Û˘ÛÙ·ÙÈο Ù˘ ÙÚÔÊ‹˜, Ù· ÔÔ›· ·ÓȯÓ‡ÔÓÙ·ÈÛÙÔ ÌËÙÚÈÎfi Á¿Ï· ηÈ, ÂÎÙfi˜ ·fi ÙȘ ηı·Ú¿‰È·ÙÚÔÊÈΤ˜ ÙÔ˘˜ ·Í›Â˜, ÂËÚ¿˙Ô˘Ó ÙË ÁÂÓÈÎfi-ÙÂÚË ˘Á›· ÙÔ˘ ·È‰ÈÔ‡. ŒÙÛÈ, Ë ‰È·›ÛÙˆÛË Ù˘
·ÚÔ˘Û›·˜ ÛÙÔ ·ÓıÚÒÈÓÔ Á¿Ï· ·Ú¯Èο Ù˘ Ù·˘-Ú›Ó˘ Î·È ÛÙË Û˘Ó¤¯ÂÈ· ÙˆÓ ÓÔ˘ÎÏÂÔÙȉ›ˆÓ ÙˆÓÔÏ˘·ÎfiÚÂÛÙˆÓ ÏÈ·ÚÒÓ ÔͤˆÓ, ÙˆÓ Ú‚ÈÔÙÈ-ÎÒÓ, ÙˆÓ ÚÔ‚ÈÔÙÈÎÒÓ, Ù˘ ÁÏÔ˘Ù·Ì›Ó˘, Ù˘ ·Ú-ÁÈÓ›Ó˘ Ô‰‹ÁËÛ ÛÙËÓ ÚÔÛı‹ÎË ÙˆÓ Ô˘ÛÈÒÓ ·˘-ÙÒÓ ÛÙ· ÙÚÔÔÔÈË̤ӷ Á¿Ï·Ù·. ¶·Ú¿ ÙȘ ÊÈÏfi-ÙÈ̘ ÚÔÛ¿ıÂȘ, ηӤӷ ÚÔÛ·ÚÌÔṲ̂ÓÔÚÔ˜ ÙÔ ÌËÙÚÈÎfi Á¿Ï· ‰ÂÓ ÌÔÚ› Ó· ¤¯ÂÈ ÙȘȉÈfiÙËÙ˜ ÙÔ˘ ·ÓıÚˆ›ÓÔ˘, ÎÈ ·˘Ùfi ÁÈ·Ù› Ë Û‡Ó-ıÂÛË ÙÔ˘ ÌËÙÚÈÎÔ‡ Á¿Ï·ÎÙÔ˜ ‰ÂÓ Â›Ó·È ÛÙ·ıÂÚ‹,·ÏÏ¿ ÌÂÙ·‚¿ÏÏÂÙ·È Ì ÙËÓ ¿ÚÔ‰Ô ÙÔ˘ ¯ÚfiÓÔ˘.ŒÙÛÈ, Â›Ó·È ‰‡ÛÎÔÏÔ˜ Ô ·ÎÚÈ‚‹˜ ˘ÔÏÔÁÈÛÌfi˜
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·116
117¢È·ÙÚÔÊ‹ ÙÔ˘ ‚Ú¤ÊÔ˘˜
¶·È‰È·ÙÚÈ΋ 2008;71:116-122
Ù˘ ··ÈÙÔ‡ÌÂÓ˘ ÔÛfiÙËÙ·˜ ÁÈ· οı ÛÙÔȯ›Ô. ∏
‚ÈԉȷıÂÛÈÌfiÙËÙ· ÂÍ¿ÏÏÔ˘ Î·È Ë Â›‰Ú·ÛË ÛÙÔ ÌÂ-
Ù·‚ÔÏÈÛÌfi Û˘ÁÎÂÎÚÈÌ¤ÓˆÓ Ô˘ÛÈÒÓ ÌÔÚ› Ó· ›ӷÈ
‰È·ÊÔÚÂÙÈ΋ ÛÙÔ ÌËÙÚÈÎfi Á¿Ï· ·’ fi,ÙÈ ÛÙÔ Í¤ÓÔ
Á¿Ï·. ∆Ô ÌËÙÚÈÎfi Á¿Ï· ÂÚȤ¯ÂÈ Ï‹ıÔ˜ ÔÚÌÔÓÒÓ
Î·È ·˘ÍËÙÈÎÒÓ ·Ú·ÁfiÓÙˆÓ Ô˘ ÌÔÚ› Ó· ¢ԉÒ-
ÓÔ˘Ó ‹ Ó· ÂÚÈÔÚ›˙Ô˘Ó ÙË ‰Ú¿ÛË ÌÈ·˜ Û˘ÁÎÂÎÚÈ̤-
Ó˘ Ô˘Û›·˜, ÁÂÁÔÓfi˜ Ô˘ ‰ÂÓ Û˘Ì‚·›ÓÂÈ Ì ÙÔ Í¤ÓÔ
Á¿Ï·. ™ÙËÓ Ú¿ÍË ·Ô‰Â›¯ıËΠfiÙÈ Ù· ÔÏ˘‰È·ÊË-
ÌÈ˙fiÌÂÓ· ÔʤÏË ÁÈ· ÔÏϤ˜ Ô˘Û›Â˜ Â›Ó·È ·Ó‡·Ú-
ÎÙ· ‹ ÛÙËÓ Î·Ï‡ÙÂÚË ÂÚ›ÙˆÛË ÔÚȷο, ÂÓÒ
˘¿Ú¯Ô˘Ó Î·È Î›Ó‰˘ÓÔÈ ·fi ÙËÓ ·ÓÂͤÏÂÁÎÙË ¯Ú‹-
ÛË ÙÔ˘˜. ™ÙË Û˘Ó¤¯ÂÈ· ı· ÚÔÛ·ı‹ÛÔ˘Ì ӷ ο-
ÓÔ˘Ì ÌÈ· ·ÓÙÈÎÂÈÌÂÓÈ΋ ·ÍÈÔÏfiÁËÛË Î¿ı ÌÈ·˜ ·fi
·˘Ù¤˜ ÙȘ Ô˘Û›Â˜.
¡Ô˘ÎÏÂÔÙ›‰È· (¡∫)
∞ÔÙÂÏÔ‡Ó Úfi‰ÚÔ̘ Ô˘Û›Â˜ ÙÔ˘ RNA Î·È ÙÔ˘
DNA. £ÂˆÚÔ‡ÓÙ·È ··Ú·›ÙËÙ· ÛÙËÓ ·‡ÍËÛË Î·È
ÙËÓ ˆÚ›Ì·ÓÛË ÙÔ˘ ÂÙÈÎÔ‡, ÛÙË ‚ÂÏÙ›ˆÛË Ù˘
ÂÓÙÂÚÈ΋˜ ¯ÏˆÚ›‰·˜, ÛÙËÓ ÂÓ›Û¯˘ÛË ÙÔ˘ ·ÓÔÛÔÔÈ-
ËÙÈÎÔ‡, ÛÙË Ì›ˆÛË Ù˘ Á·ÛÙÚÂÓÙÂÚ›Ùȉ·˜ Î·È ÙˆÓ
ÏÔÈÌÒÍÂˆÓ ÁÂÓÈÎfiÙÂÚ·, ηıÒ˜ Î·È ÛÙË ÛˆÌ·ÙÈ΋
·‡ÍËÛË ÓÂÔÁÓÒÓ Ì ÂÓ‰ÔÌ‹ÙÚÈ· ηı˘ÛÙ¤ÚËÛË ÛÙËÓ
·Ó¿Ù˘ÍË (1).
∞. ∂›‰Ú·ÛË ÛÙËÓ ·Ó¿Ù˘ÍË ÙÔ˘ ÂÙÈÎÔ‡
£ÂÙÈ΋ ›‰Ú·ÛË ÙˆÓ ¡∫ ÛÙÔ ÂÙÈÎfi ‚Ú¤ıËÎÂ
Û ÌÂϤÙË Ô˘ ¤ÁÈÓ Û ÔÓÙ›ÎÈ· Ô˘ ¤Ï·‚·Ó 2 ÙÚÔ-
ʤ˜, ÂÎ ÙˆÓ ÔÔ›ˆÓ Ë Ì›· ÂÚÈ›¯Â ¡∫ Î·È Ë ¿ÏÏË
‰ÂÓ ÂÚÈ›¯Â ηıfiÏÔ˘ ¡∫. ™ÙËÓ Ú¿ÍË, fï˜, ‰ÂÓ
˘¿Ú¯ÂÈ Î·Ó¤Ó· Á¿Ï· Ô˘ Ó· ÌËÓ ÂÚȤ¯ÂÈ Î·ıfiÏÔ˘
¡∫. ∂›Û˘, ÂÓÒ ÛÙËÓ ÔÌ¿‰· ÙˆÓ ÔÓÙÈÎÒÓ Ô˘
¤Ï·‚ Á¿Ï· ÂÌÏÔ˘ÙÈṲ̂ÓÔ Ì ÓÔ˘ÎÏÂÔÙ›‰È· ·Ú·-
ÙËÚ‹ıËΠÌÂÁ·Ï‡ÙÂÚË ·‡ÍËÛË Ù˘ ÂÚÈÂÎÙÈÎfiÙËÙ·˜
ÙÔ˘ ÙÔȯÒÌ·ÙÔ˜ ÙÔ˘ ·ÓÒÙÂÚÔ˘ ÂÓÙ¤ÚÔ˘, ÂÓÒ ·Ú·-
‰fi͈˜ Û ڈÙ½ÓË ‰ÂÓ ·Ú·ÙËÚ‹ıËΠη̛· ‰È·-
ÊÔÚ¿ ÛÙÔ Ì¤ÛÔ Î·È ÙÔ ÙÂÏÈÎfi ÙÌ‹Ì· ÙÔ˘ ÂÓÙ¤ÚÔ˘ (2).
ŒÙÛÈ, ¯ÚÂÈ¿˙ÔÓÙ·È ÂÈϤÔÓ ÌÂϤÙ˜ ÁÈ· ÙËÓ ÂÈ‚Â-
‚·›ˆÛË ÙˆÓ ·Ú·¿Óˆ.
µ. ∂ÓÙÂÚÈ΋ ̄ ψڛ‰·
∂˘ÓÔ˚ο ·ÔÙÂϤÛÌ·Ù· ÙˆÓ ¡∫ ·Ó·Ê¤ÚÔÓÙ·È ÛÂ
ÌÈ· ÌÂϤÙË, fiÔ˘ Û˘ÁÎÚ›ıËΠÌÈ· ÔÌ¿‰· ÓÂÔÁÓÒÓ
Ô˘ ¤·ÈÚÓ Á¿Ï· ÂÌÏÔ˘ÙÈṲ̂ÓÔ Ì ¡∫ Ì ¿ÏÏË
Ô˘ ¤·ÈÚÓ Á¿Ï· ¯ˆÚ›˜ ¡∫. ∏ ÌÂϤÙË ÂÚÈ›¯Â ÌÈ-
ÎÚfi ·ÚÈıÌfi Û˘ÌÌÂÙ¯fiÓÙˆÓ ¯ˆÚ›˜ ÛˆÛÙ‹ Ù˘¯·ÈÔÔ›-
ËÛË. ¢ÂÓ ‚Ú¤ıËΠÛËÌ·ÓÙÈ΋ ‰È·ÊÔÚ¿ ˆ˜ ÚÔ˜ ÙÔÓ
·fiÏ˘ÙÔ ·ÚÈıÌfi ÙˆÓ ·ÔÈÎÈÒÓ ÙˆÓ ÌÈÎÚÔ‚›ˆÓ ÛÙ·
ÎfiÚ·Ó·. ªfiÓÔ fiÙ·Ó ¤ÁÈÓ ۇÁÎÚÈÛË ÌÂٷ͇ ÙˆÓ
ÔÛÔÛÙÒÓ Î¿ı ÌÈÎÚÔ‚›Ô˘ ÛÙ· ÎfiÚ·Ó· ‚Ú¤ıËÎÂ
οÔÈ· ‰È·ÊÔÚ¿ (3). ™Ù· ›‰È· Û˘ÌÂÚ¿ÛÌ·Ù· ηٷ-
Ï‹ÁÂÈ Î·È ÈÔ ÚfiÛÊ·ÙË ÌÂϤÙË (4).
°. ∂›‰Ú·ÛË ÛÙÔ ·ÓÔÛÔÔÈËÙÈÎfi
∞Ó Î·È ·Ó·Ê¤ÚıËΠ‚ÂÏÙ›ˆÛË Ù˘ ÏÂÈÙÔ˘ÚÁ›·˜
ÙˆÓ Ê˘ÛÈÎÒÓ Î˘ÙÙ·ÚÔÎÙfiÓˆÓ Î˘ÙÙ¿ÚˆÓ (¡∫ cells)
Î·È ˘„ËÏfiÙÂÚÔÈ Ù›ÙÏÔÈ ·ÓÙÈÛˆÌ¿ÙˆÓ Î·Ù¿ ÙÔ˘ ·ÈÌfi-
ÊÈÏÔ˘ Ù˘ ÈÓÊÏÔ˘¤ÓÙ˙·˜ Î·È Ù˘ ‰ÈÊıÂÚ›Ùȉ·˜ ÌÂÙ¿
·fi ÂÌ‚ÔÏÈ·ÛÌfi ÛÙÔ˘˜ 2 Ì‹Ó˜ ˙ˆ‹˜ Û ‚Ú¤ÊË Ô˘
¤Ï·‚·Ó Á¿Ï· ÂÌÏÔ˘ÙÈṲ̂ÓÔ Ì ¡∫, ‰ÂÓ ˘‹Ú¯Â η-
Ì›· ‰È·ÊÔÚ¿ ÛÙËÓ ËÏÈΛ· ÙˆÓ 4 ÌËÓÒÓ (5) Û ۯ¤ÛË
Ì ÙÔ˘˜ Ì¿ÚÙ˘Ú˜. ¢ÂÓ ·Ú·ÙËÚ‹ıËΠ›Û˘ ÛËÌ·-
ÓÙÈ΋ ‰È·ÊÔÚ¿ ̂ ˜ ÚÔ˜ ÙË Û˘¯ÓfiÙËÙ· ‹ ÙË ‚·Ú‡ÙËÙ·
ÙˆÓ ÏÔÈÌÒÍÂˆÓ ÌÂٷ͇ ÙˆÓ ‰‡Ô ÔÌ¿‰ˆÓ.
¢. ¢È¿ÚÚÔÈ·-ÏÔÈÌÒÍÂȘ
∞Ó Î·È ÔÈ ÚÒÙ˜ ÌÂϤÙ˜ Û ÂÈÚ·Ì·Ùfi˙ˆ· ¤‰ÂÈ-
Í·Ó Î·Ï‡ÙÂÚË ÂԇψÛË ÙÔ˘ ‚ÏÂÓÓÔÁfiÓÔ˘ ÙÔ˘ ÂÓÙ¤-
ÚÔ˘ ÌÂÙ¿ ·fi ÚÔÎÏËÙ‹ ‚Ï¿‚Ë (2) ÌÂÙ¿ ÙË ¯ÔÚ‹ÁË-
ÛË ¡∫, ÎÏÈÓÈ΋ ÌÂϤÙË Û ·È‰È¿ ‰ÂÓ ¤‰ÂÈÍ ÛËÌ·-
ÓÙÈ΋ ‰È·ÊÔÚ¿ ÛÙÔ Û˘ÓÔÏÈÎfi ·ÚÈıÌfi ÙˆÓ ÂÂÈÛÔ‰›ˆÓ
‰È¿ÚÚÔÈ·˜ Î·È ÙË ¯ÚÔÓÈ΋ ‰È¿ÚÎÂÈ· οı ÂÂÈÛÔ‰›Ô˘.
¢ÂÓ ·Ú·ÙËÚ‹ıËΠ›Û˘ ‰È·ÊÔÚ¿ ˆ˜ ÚÔ˜ ÙË Û˘-
¯ÓfiÙËÙ· ÙˆÓ ÏÔÈÌÒÍÂˆÓ ÙÔ˘ ·ÓˆÙ¤ÚÔ˘ Î·È ÙÔ˘ η-
و٤ÚÔ˘ ·Ó·Ó¢ÛÙÈÎÔ‡, ÙÔ˘ ‰¤ÚÌ·ÙÔ˜, ÙÔ˘ ÔÊı·Ï-
ÌÔ‡ Î·È Ù˘ ·Ú·ÌÔÓ‹˜ ÛÙÔ ÓÔÛÔÎÔÌÂ›Ô Û ۯ¤ÛË ÌÂ
Ì¿ÚÙ˘Ú˜ (6).
∂. ∂›‰Ú·ÛË ÛÙË ÛˆÌ·ÙÈ΋ ·‡ÍËÛË
ªÈ· ÌÂϤÙË ¤‰ÂÈÍ ηχÙÂÚË ·ÓÙÈÚÚÔÈÛÙÈ΋ ·‡-
ÍËÛË Û ÙÂÏÂÈfiÌËÓ· Ì ÂÓ‰ÔÌ‹ÙÚÈ· ηı˘ÛÙ¤ÚËÛË
Ù˘ ·Ó¿Ù˘Í˘ (7) ÌÂÙ¿ ÙË Ï‹„Ë ¡∫. ÕÏϘ ÌÂϤÙ˜
‰ÂÓ ÂȂ‚·›ˆÛ·Ó ·˘Ù‹ ÙËÓ ¿Ô„Ë (8,9). À„ËϤ˜
‰fiÛÂȘ ¡∫ ‚Ú¤ıËΠfiÙÈ ·˘Í¿ÓÔ˘Ó ÙÔÓ Î›Ó‰˘ÓÔ ·Ó·-
Ó¢ÛÙÈÎÒÓ ÏÔÈÌÒÍÂˆÓ (10). ¢È΋ Ì·˜ Ù˘¯·ÈÔÔÈË-
̤ÓË Ù˘ÊÏ‹ ÌÂϤÙË ‰ÂÓ ¤‰ÂÈÍ ›‰Ú·ÛË ÙˆÓ ÓÔ˘-
ÎÏÂÔÙȉ›ˆÓ ÛÙËÓ ·ÔÚÚfiÊËÛË Ï›Ô˘˜ Î·È ˘‰·Ù·Ó-
ıÚ¿ÎˆÓ Ô‡ÙÂ Î·È Ì›ˆÛË ÙÔ˘ ÏËı˘ÛÌÔ‡ ÙˆÓ ÂÓÙÂ-
ÚÔ·ıÔÁfiÓˆÓ ÛÙ· ÎfiÚ·Ó· (11). ªÈ· Èı·Ó‹ ÂÍ‹ÁË-
ÛË Ù˘ ÌË ·Ó‡ÚÂÛ˘ ıÂÙÈÎÔ‡ ·ÔÙÂϤÛÌ·ÙÔ˜ ›Ûˆ˜
Ó· Â›Ó·È fiÙÈ Ë ÌÂϤÙË ‰ÂÓ ÂÚÈÂÏ¿Ì‚·Ó ·Ú΋
·ÚÈıÌfi ÓÂÔÁÓÒÓ Ì ÂÓ‰ÔÌ‹ÙÚÈ· ‰˘ÛÙÚÔÊ›·, Ù·
ÔÔ›·, ηٿ ÙË ÁÓÒÌË Ì·˜, ı· ˆÊÂÏÔ‡ÓÙ·Ó ÂÚÈÛÛfi-
ÙÂÚÔ ·fi ÙËÓ ÚÔÛı‹ÎË ÙˆÓ ÓÔ˘ÎÏÂÔÙȉ›ˆÓ.
¶ÔÏ˘·ÎfiÚÂÛÙ· ÏÈ·Ú¿ Ôͤ· (¶∞§√)
∞ÔÙÂÏÔ‡Ó Úfi‰ÚÔ̘ Ô˘Û›Â˜ ÚÔÛÙ·ÁÏ·Ó‰È-
ÓÒÓ, ÚÔÛÙ·Î˘ÎÏ›Ó˘, ıÚÔÌ‚ÔÍ¿Ó˘, Ï¢ÎÔÙÚÈÂÓ›ˆÓ
Î·È ıˆÚÔ‡ÓÙ·È ··Ú·›ÙËÙ· ÁÈ· ÙËÓ ·Ó¿Ù˘ÍË ÙÔ˘
ÓÂÔÁÓÈÎÔ‡ ÂÁÎÂÊ¿ÏÔ˘ Î·È Ù˘ ÔÙÈ΋˜ ÏÂÈÙÔ˘ÚÁ›·˜.
¶·›˙Ô˘Ó ÛËÌ·ÓÙÈÎfi ÚfiÏÔ ÛÙËÓ ·Ó¿Ù˘ÍË ÙˆÓ Ó¢ÚÈ-
ÎÒÓ Û˘Ó¿„ÂˆÓ (12-14). ∂ȉÚÔ‡Ó, ›Û˘, ÛÙÔ ·ÓÔ-
ÛÔÔÈËÙÈÎfi, ÙË ÊÏÂÁÌÔÓÒ‰Ë ·ÓÙ›‰Ú·ÛË, ÙÔ ÌÂÙ·‚Ô-
ÏÈÛÌfi ÙˆÓ ÔÛÙÒÓ (15).
∞Ó¿ÏÔÁ· Ì ÙË ı¤ÛË ÙÔ˘ ÚÒÙÔ˘ ‰ÈÏÔ‡ ‰ÂÛÌÔ‡
·fi ÙÔ ÌÂı˘ÏÈÎfi ¿ÎÚÔ ‰È·ÎÚ›ÓÔÓÙ·È Û ˆ-3 Î·È ˆ-6.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·117

∆· ΢ÚÈfiÙÂÚ· Â›Ó·È ÙÔ ·Ú·¯È‰ÔÓÈÎfi Î·È ÙÔ 22-ÂÍ·ÓÔ˚-
Îfi Ô͇ (DHA). ∞ÔÙÂÏÔ‡Ó Û˘ÛÙ·ÙÈÎfi Ù˘ ΢ÙÙ·ÚÈ-
΋˜ ÌÂÌ‚Ú¿Ó˘, Ë ÔÔ›· Â›Ó·È Â˘·ı‹˜ Û ÔÍÂȉˆÙÈ-
΋ ‰Ú¿ÛË ÂχıÂÚˆÓ ÚÈ˙ÒÓ Ô͢ÁfiÓÔ˘. ÀÂÚ‚ÔÏÈ΋
¯ÔÚ‹ÁËÛË ¶∞§√ ·˘Í¿ÓÂÈ ÙËÓ ·ÈÌfiÏ˘ÛË ÂÚ˘ıÚÒÓ ·È-
ÌÔÛÊ·ÈÚ›ˆÓ, ÂÈÙ›ÓÂÈ ÙËÓ ˘ÂÚÔÍÈ΋ ‚Ï¿‚Ë ÙˆÓ
Ó¢ÌfiÓˆÓ Î·È ÙË ÊˆÙÔÙÔÍÈ΋ ‚Ï¿‚Ë ÙˆÓ Ú·‚‰›ˆÓ
ÙÔ˘ ·ÌÊÈ‚ÏËÛÙÚÔÂȉԇ˜, Úԉȷı¤ÙÔÓÙ·˜ ›Ûˆ˜ ÛÂ
˘„ËÏfiÙÂÚ· ÔÛÔÛÙ¿ ¯ÚfiÓÈ·˜ Ó¢ÌÔÓÔ¿ıÂÈ·˜
(ö), ÓÂÎÚˆÙÈ΋˜ ÂÓÙÂÚÔÎÔÏ›Ùȉ·˜ (¡∂∫), ·ÌÊÈ-
‚ÏËÛÙÚÔÂȉԿıÂÈ·˜ Ù˘ ÚÔˆÚfiÙËÙ·˜ (∞¶) (16).
¶ÚfiˆÚ· Ô˘ ¤Ï·‚·Ó ȯı˘¤Ï·ÈÔ Â›¯·Ó ¯·ÌËÏfiÙÂÚË
·‡ÍËÛË ÙÔ˘ ۈ̷ÙÈÎÔ‡ ÙÔ˘˜ ‚¿ÚÔ˘˜ Û ۯ¤ÛË ÌÂ
Ì¿ÚÙ˘Ú˜ (17). ∞˘Ùfi ÔÊÂÈÏfiÙ·Ó Û ·ÚÂÌfi‰ÈÛË
·fi Ù· ˆ-3 ÏÈ›‰È· Ù˘ ÌÂÙ·ÙÚÔ‹˜ ÙÔ˘ ÏÈÓÔÏÂ˚ÎÔ‡
ÔͤԘ Û ·Ú·¯È‰ÔÓÈÎfi. ªÂ ‚¿ÛË ·˘Ù¿, Ë ∂˘Úˆ·˚΋
∂Ù·ÈÚ›· ¶·È‰È·ÙÚÈ΋˜ °·ÛÙÚÂÓÙÂÚÔÏÔÁ›·˜, ∏·ÙÔ-
ÏÔÁ›·˜ Î·È ¢È·ÙÚÔÊ‹˜ ÚÔÙ›ÓÂÈ Ë ÔÛfiÙËÙ· ÙÔ˘
DHA ÛÙÔ ÚÔÛ·ÚÌÔṲ̂ÓÔ ÚÔ˜ ÙÔ ÌËÙÚÈÎfi Á¿Ï· Ó·
ÌËÓ ˘ÂÚ‚·›ÓÂÈ ÙÔ 0,5% ÙÔ˘ Û˘ÓÔÏÈÎÔ‡ Ï›Ô˘˜ Î·È Ë
ÂÚÈÂÎÙÈÎfiÙËÙ· Û ∞∞ Ó· Â›Ó·È ÙÔ˘Ï¿¯ÈÛÙÔÓ ›ÛË ÌÂ
·˘Ù‹ ÙÔ˘ DHA (18).
∆· ÙÂÏÂ˘Ù·›· ¯ÚfiÓÈ· ÔÏÔ¤Ó· Î·È ÂÚÈÛÛfiÙÂÚ˜
‚ÈÔÌ˯·Ó›Â˜ ·Ú·Û΢‹˜ ‚ÚÂÊÈÎÒÓ Á·Ï¿ÙˆÓ ÚÔ-
Ûı¤ÙÔ˘Ó ¶∞§√ ÛÙ· ÚÔ˚fiÓÙ· ÙÔ˘˜. Œ¯Ô˘Ó Á›ÓÂÈ ÔÏ-
Ϥ˜ ÌÂϤÙ˜ ÙfiÛÔ Û ÚfiˆÚ· fiÛÔ Î·È Û ÙÂÏÂÈfiÌËÓ·
ÓÂÔÁÓ¿ Ô˘ ·Ó·Ê¤ÚÔÓÙ·È ÛÙË ¯Ú‹ÛË ÙˆÓ ¶∞§√ η-
Ù¿ ÙË ‚ÚÂÊÈ΋ ÂÚ›Ô‰Ô Î·È Ù· Û˘ÌÂÚ¿ÛÌ·Ù· ›ӷÈ
·ÓÙÈÊ·ÙÈο. £· ÛÙ·¯˘ÔÏÔÁ‹ÛÔ˘Ì ÌÂÚÈΤ˜ ·fi ·˘-
Ù¤˜ ÙȘ ÌÂϤÙ˜.
ªÂϤÙ˜ Û ÚfiˆÚ· ÓÂÔÁÓ¿
ªÂÁ¿ÏË ÚfiÛÊ·ÙË ·Ó·ÛÎfiËÛË Ô˘ Û˘ÌÂÚȤ-
Ï·‚ 11 ÌÂϤÙ˜ ¤‰ÂÈÍ fiÙÈ Ë ÚÔÛı‹ÎË ¶∞§√ ÛÂ
ÚfiˆÚ· ‰ÂÓ Â›¯Â η̛· ıÂÙÈ΋ ›‰Ú·ÛË ÛÙË ÛˆÌ·-
ÙÈ΋ Î·È ÓÔËÙÈ΋ ÂͤÏÈÍ‹ ÙÔ˘˜ (19). √È ÌÂϤÙ˜ ‰ÂÓ
ÂÚÈÂÏ¿Ì‚·Ó·Ó fï˜ ÓÂÔÁÓ¿ Ì ÂÍ·ÈÚÂÙÈο ¯·ÌËÏfi
‚¿ÚÔ˜ Á¤ÓÓËÛ˘. ÕÏÏË Ù˘¯·ÈÔÔÈË̤ÓË ÌÂϤÙË
¤‰ÂÈÍ fiÙÈ Ë ÚÔÛı‹ÎË ¶∞§√ ÛÙË ‰È·ÙÚÔÊ‹ ÚÔÒ-
ÚˆÓ Ô‰‹ÁËÛ Û ηχÙÂÚË ·Ó¿Ù˘ÍË Û ‚¿ÚÔ˜ ηÈ
Ì‹ÎÔ˜ ÛÙËÓ ËÏÈΛ· ÙˆÓ 9 ÌËÓÒÓ. ∆· ·ÁfiÚÈ· Ù˘ ÌÂ-
ϤÙ˘ ›¯·Ó ÛÙÔ˘˜ 18 Ì‹Ó˜ ˙ˆ‹˜ ˘„ËÏfiÙÂÚÔ ÓÔËÙÈ-
Îfi ‰Â›ÎÙË Û ۯ¤ÛË Ì ÙÔ˘˜ Ì¿ÚÙ˘Ú˜ (20). ÕÏÏË
ÌÂϤÙË ¤‰ÂÈÍ ¿ÏÈ fiÙÈ ÚfiˆÚ· Ô˘ ¤Ï·‚·Ó ¶∞§√
›¯·Ó ÛÙË ‰ÈÔÚıˆÌ¤ÓË ËÏÈΛ· ÙˆÓ 18 ÌËÓÒÓ ˘„ËÏfi-
ÙÂÚÔ˘˜ ‰Â›ÎÙ˜ ÓÔËÌÔÛ‡Ó˘ Û‡Ìʈӷ Ì ÙËÓ Îϛ̷-
η Bayley (21).
ªÂϤÙ˜ Û ÙÂÏÂÈfiÌËÓ· ÓÂÔÁÓ¿
√È ÌÂϤÙ˜ Ô˘ ¤ÁÈÓ·Ó Û ÙÂÏÂÈfiÌËÓ· ¤‰ÂÈÍ·Ó
·ÓÙÈÊ·ÙÈο ·ÔÙÂϤÛÌ·Ù·. ªÂÁ¿ÏË ·Ó·ÛÎfiËÛË
Ô˘ ÂÚÈÂÏ¿Ì‚·Ó 10 ÎÏÈÓÈΤ˜ ÌÂϤÙ˜ ‰ÂÓ ¤‰ÂÈÍÂ
ηӤӷ fiÊÂÏÔ˜ ·fi ÙË ̄ Ú‹ÛË ÙˆÓ ¶∞§√ (22). ™Â ¿Ï-
ÏË ·Ó·ÛÎfiËÛË ¿ÏÈ ‚Ú¤ıËÎÂ fiÙÈ Ô ÂÌÏÔ˘ÙÈÛÌfi˜ ÌÂ
¶∞§√ ›¯Â ıÂÙÈ΋ ‰Ú¿ÛË ÛÙËÓ ÔÙÈ΋ Ô͇ÙËÙ· ÓÂÔ-
ÁÓÒÓ ÛÙÔ 2Ô Ì‹Ó· ˙ˆ‹˜ (23). À¿Ú¯ÂÈ, fï˜, Î·È ÌÂ-
ϤÙË Ô˘ ‰Â›¯ÓÂÈ ¯ÂÈÚfiÙÂÚË ÓÔËÙÈ΋ ¤Î‚·ÛË ÛÙËÓ
ËÏÈΛ· ÙˆÓ 39 ÌËÓÒÓ Û ۇÁÎÚÈÛË Ì ̿ÚÙ˘Ú˜ (24).
Ÿˆ˜ ·Ó·Ê¤ÚÂÈ Ë Fewtrell (25), ÌÂÚÈÎÔ› ·fi ÙÔ˘˜
ÏfiÁÔ˘˜, ÁÈ· ÙÔ˘˜ ÔÔ›Ô˘˜ Ù· ·ÔÙÂϤÛÌ·Ù· ÙˆÓ ÎÏÈ-
ÓÈÎÒÓ ÌÂÏÂÙÒÓ ¿Óˆ ÛÙ· ¶∞§√ Â›Ó·È ·ÓÙÈÊ·ÙÈο, ›-
Ó·È ÔÈ ÂÍ‹˜: ·) √È ÂÏ¿¯ÈÛÙ˜ ·Ó·Áη›Â˜ ËÌÂÚ‹ÛȘ
·Ó¿ÁΘ ‰ÂÓ Â›Ó·È ÁÓˆÛÙ¤˜. ‚) ∏ Û¯¤ÛË 18:ˆ-3/18:ˆ-
6 ÛÙ· ¯ÔÚËÁÔ‡ÌÂÓ· ¶∞§√ Î·È Ë ÚÔ¤ÏÂ˘Û‹ ÙÔ˘˜
ÔÈΛÏÏÂÈ. Á) ∏ ¯ÔÚËÁÔ‡ÌÂÓË ÔÛfiÙËÙ·, ›Û˘, ÔÈ-
ΛÏÏÂÈ. ‰) ¢ÂÓ ˘¿Ú¯Ô˘Ó, Ù¤ÏÔ˜, Ì·ÎÚfi¯ÚÔÓ˜ ÌÂϤ-
Ù˜ Û¯ÂÙÈο Ì ÙËÓ ¤Î‚·ÛË ÙˆÓ ˘fi ÌÂϤÙË ·È‰ÈÒÓ.
∞fi Ù· ·Ú·¿Óˆ Ê·›ÓÂÙ·È fiÙÈ ·˘Ù¿ Ô˘ ˆÊÂ-
ÏÔ‡ÓÙ·È ÂÚÈÛÛfiÙÂÚÔ ·fi ÙË ¯Ú‹ÛË ÙˆÓ ¶∞§√ ›ӷÈ
Ù· Ôχ ÚfiˆÚ· ÓÂÔÁÓ¿, Ù· ÔÔ›· ¤¯Ô˘Ó Î·È Ù· ¯·-
ÌËÏfiÙÂÚ· ·Ôı¤Ì·Ù· ÙˆÓ ÏÈ·ÚÒÓ ·˘ÙÒÓ ÔͤˆÓ η-
Ù¿ ÙË Á¤ÓÓËÛË. ∏ ·Ó·ÁηÈfiÙËÙ· ̄ ÚËÛÈÌÔÔ›ËÛ‹˜ ÙˆÓ
¶∞§√ ÛÙ· ÙÂÏÂÈfiÌËÓ· ÓÂÔÁÓ¿ ̤ÓÂÈ Ó· ·Ô‰Âȯı›.
°ÏÔ˘Ù·Ì›ÓË
∞ÔÙÂÏ› ËÁ‹ ÂÓ¤ÚÁÂÈ·˜ ÁÈ· Ù· ÂÓÙÂÚÔ·ÙÙ·Ú·
Î·È ·Ú¤¯ÂÈ ¿˙ˆÙÔ ÁÈ· ÙË Û‡ÓıÂÛË ·ÌÈÓÔͤˆÓ Ô˘
Â›Ó·È ··Ú·›ÙËÙ· ÁÈ· ÙÔÓ ÔÏÏ·Ï·ÛÈ·ÛÌfi ÙˆÓ
ÂÓÙÂÚÔ΢ÙÙ¿ÚˆÓ, ÙËÓ ·Ú·ÁˆÁ‹ ‚ϤÓÓ˘, ÙËÓ ·ÓÔ-
ÛÔÏÔÁÈ΋ ÏÂÈÙÔ˘ÚÁ›· ÙÔ˘ ÂÓÙ¤ÚÔ˘, ÙËÓ ·ÎÂÚ·ÈfiÙËÙ·
ÙÔ˘ ÂÓÙÂÚÈÎÔ‡ ÊÚ·ÁÌÔ‡ (26). ¶ÚfiˆÚ· ÛÂ ·ÚÂÓÙÂÚÈ-
΋ ‰È·ÙÚÔÊ‹ Ô˘ ¤Ï·‚·Ó ÂÏ¿¯ÈÛÙË ÂÓÙÂÚÈ΋ ‰È·ÙÚÔ-
Ê‹ Ô˘ ‹Ù·Ó ÂÌÏÔ˘ÙÈṲ̂ÓË Ì ÁÏÔ˘Ù·Ì›ÓË Â›¯·Ó
¯·ÌËÏfiÙÂÚË Û˘¯ÓfiÙËÙ· ÛË„·ÈÌ›·˜ Î·È ·˘ÍË̤ÓË
·ÓÔ¯‹ ÂÓÙÂÚÈ΋˜ ÙÚÔÊ‹˜ (27). ∏ ·ÔÙÂÏÂÛÌ·ÙÈÎfi-
ÙËÙ· Ù˘ ÁÏÔ˘Ù·Ì›Ó˘ ·ÌÊÈÛ‚ËÙÂ›Ù·È Û ·ı‹ÛÂȘ,
fiˆ˜ Û‡Ó‰ÚÔÌÔ ÙÔ˘ ‚Ú·¯¤Ô˜ ÂÓÙ¤ÚÔ˘, ÊÏÂÁÌÔÓÒ‰Ë
ÂÓÙÂÚÔ¿ıÂÈ· Î·È ·ÎÙÈÓÈ΋ ‚Ï¿‚Ë ÙÔ˘ ÂÓÙ¤ÚÔ˘ (28),
ÂÓÒ ÌÂϤÙ˜ Û ÓÂÔÁÓ¿ ¤‰ÂÈÍ·Ó fiÙÈ Ë ¯Ú‹ÛË Ù˘ ‰ÂÓ
ÌÂÈÒÓÂÈ ÙË Û˘¯ÓfiÙËÙ· ÂÌÊ¿ÓÈÛ˘ ÏÔÈÌÒÍÂˆÓ Î·È
¡∂∫, ·ÏÏ¿ Ô‡ÙÂ Î·È Ô‰ËÁ› Û ηχÙÂÚË ·ÓÔ¯‹ ÂÓÙÂ-
ÚÈ΋˜ ÙÚÔÊ‹˜ (29,30). ∂›Û˘, ·Ó·Ê¤ÚÂÙ·È Î·È Èı·-
Ó‹ ÙÔÍÈ΋ ‰Ú¿ÛË Ù˘ ÁÏÔ˘Ù·Ì›Ó˘ ‹ ÙÔ˘ ÁÏÔ˘Ù·ÌÈ-
ÎÔ‡, Ô˘ ·ÔÙÂÏ› ·Ú¿ÁˆÁfi Ù˘, ÛÙÔ ∫¡™. ∏ ÁÏÔ˘-
Ù·Ì›ÓË, Ù¤ÏÔ˜, ÌÔÚ› Ó· ·Ú¤Ì‚ÂÈ ·ÚÓËÙÈο ÛÙÔ ÌÂ-
Ù·‚ÔÏÈÛÌfi ¿ÏÏˆÓ ·ÌÈÓÔͤˆÓ (31).
∞ÚÁÈÓ›ÓË
∂›Ó·È ··Ú·›ÙËÙË ÁÈ· ÙË Û‡ÓıÂÛË ÔÍÂȉ›Ô˘ ÙÔ˘
·˙ÒÙÔ˘, ÙËÓ ÂÓÙÂÚÈ΋ ·ÈÌ·ÙÈ΋ ÚÔ‹, ÙËÓ ÂÓ›Û¯˘ÛË ÙÔ˘
·ÓÔÛÔÔÈËÙÈÎÔ‡, ÙËÓ ·Ú·ÁˆÁ‹ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
(32). ∏ ̄ ÔÚ‹ÁËÛ‹ Ù˘ Û ·ÛıÂÓ›˜ ÓÔÛËÏ¢fiÌÂÓÔ˘˜ ÛÂ
ÂÓÙ·ÙÈ΋ ÌÔÓ¿‰· ‚ÂÏÙ›ˆÛ ÙËÓ ÂÈ‚›ˆÛË (33). ¶Úfiˆ-
Ú· Ô˘ ·Ó¤Ù˘Í·Ó ¡∂∫ ›¯·Ó ¯·ÌËÏfiÙÂÚ· ›‰·
·ÚÁÈÓ›Ó˘ ·›Ì·ÙÔ˜ (34) Û ۯ¤ÛË Ì ̿ÚÙ˘Ú˜. ∆Ô ·ÌÈ-
ÓÔ͇ ·˘Ùfi ÌÔÚ› Ó· ÂËÚ¿ÛÂÈ ÙÔ ÌÂÙ·‚ÔÏÈÛÌfi Ù˘
118 Ã. ∫ÒÛÙ·ÏÔ˜
Paediatriki 2008;71:116-122
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·118

119¢È·ÙÚÔÊ‹ ÙÔ˘ ‚Ú¤ÊÔ˘˜
¶·È‰È·ÙÚÈ΋ 2008;71:116-122
ÁÏ˘Îfi˙˘, ¤¯ÂÈ ÈÛÙ·ÌÈÓÈ΋ ‰Ú¿ÛË (35), ÂÓÒ ·˘Í¿ÓÂÈ ÙË
Û‡ÓıÂÛË ÔÍÂȉ›Ô˘ ÙÔ˘ ·˙ÒÙÔ˘ Ô˘ ÌÔÚ› Ó· Ô‰ËÁ‹-
ÛÂÈ Û ·Ó·ÓfiÚıˆÙÔ ÛËÙÈÎfi ÛÔÎ (36).
∫·ÚÓÈÙ›ÓË
∂›Ó·È ··Ú·›ÙËÙË ÁÈ· ÙËÓ ÔÍ›‰ˆÛË ÙˆÓ ÏÈ·ÚÒÓ
ÔͤˆÓ ÛÙ· ÌÈÙÔ¯fiÓ‰ÚÈ· Î·È ÙËÓ ·ÔÌ¿ÎÚ˘ÓÛË ·ÎÂ-
Ù˘ÏÈˆÌ¤ÓˆÓ ÚÔ˚fiÓÙˆÓ ÌÂÙ·‚ÔÏÈÛÌÔ‡ (37). ¡ÂfiÙÂ-
Ú˜ ÌÂϤÙ˜ ·ÌÊÈÛ‚ËÙÔ‡Ó ÙË ¯ÚËÛÈÌfiÙËÙ¿ Ù˘ (38),
ÂÓÒ ÔÚÈṲ̂ÓÔÈ ıˆÚÔ‡Ó fiÙÈ ÌÔÚ› Î·È Ó· ‚Ï¿ÙÂÈ
·Ó ¯ÔÚËÁËı› Û ·˘ÍË̤ÓË ‰fiÛË (39).
™›‰ËÚÔ˜
∂ÌÔ‰›˙ÂÈ ÙËÓ ·ÔÚÚfiÊËÛË „¢‰·ÚÁ‡ÚÔ˘ ηÈ
¯·ÏÎÔ‡ ·fi ÙÔ ÂÙÈÎfi. ∂›Ó·È ÈÛ¯˘Úfi ÔÍÂȉˆÙÈÎfi ηÈ
ÌÔÚ› Ó· ‰ËÌÈÔ˘ÚÁ‹ÛÂÈ ÔÍÂȉˆÙÈ΋ ‚Ï¿‚Ë. ™Â ÂÓ‹-
ÏÈΘ ˘¿Ú¯ÂÈ ¿ÌÂÛË Û¯¤ÛË ÌÂٷ͇ ·ÔıÂÌ¿ÙˆÓ ÛÈ-
‰‹ÚÔ˘ Î·È Î·Ú‰È·ÁÁÂȷ΋˜ ÓfiÛÔ˘ (40). ™Â ÌÂϤÙË
·fi ÙË ™Ô˘Ë‰›· Û ‚Ú¤ÊË ËÏÈΛ·˜ 4-9 ÌËÓÒÓ ÌÂ
·Ú΋ ·Ôı¤Ì·Ù· Ûȉ‹ÚÔ˘, Ë ¯ÔÚ‹ÁËÛË ÂÈϤÔÓ
Ûȉ‹ÚÔ˘ ·fi ÙÔ ÛÙfiÌ· Ô‰‹ÁËÛ Û ÌÂȈ̤ÓË ·‡ÍË-
ÛË ÂȘ Ì‹ÎÔ˜ ÛÙËÓ ËÏÈΛ· ÙˆÓ 5 ÂÙÒÓ. ∂›Û˘, Ù·
‚Ú¤ÊË ÂÌÊ¿ÓÈÛ·Ó, Û˘ÁÎÚÈÙÈο Ì ̿ÚÙ˘Ú˜, ˘„ËÏfi-
ÙÂÚË Û˘¯ÓfiÙËÙ· ‰È¿ÚÚÔÈ·˜ Î·È ÏÔÈÌÒÍÂȘ ÙÔ˘ ·ÓÒÙÂ-
ÚÔ˘ ·Ó·Ó¢ÛÙÈÎÔ‡ (41).
¶Ú‚ÈÔÙÈο
∆Ô ÌËÙÚÈÎfi Á¿Ï· ÂÎÙfi˜ ·fi ÙȘ ¿ÏϘ ÙÔ˘ ȉÈfiÙË-
Ù˜ ÂÓÈÛ¯‡ÂÈ ÂÈϤÔÓ ÙËÓ ¿Ì˘Ó· ÙÔ˘ ÔÚÁ·ÓÈÛÌÔ‡ ̤-
Ûˆ Ù˘ ¢ÂÚÁÂÙÈ΋˜ ÙÔ˘ ‰Ú¿Û˘ ÛÙÔ ·ÓÔÛÔÔÈËÙÈÎfi
Û‡ÛÙËÌ· ÙÔ˘ ÓÂÔÁÓÔ‡, ÂÓÒ ·Ú¿ÏÏËÏ· ÌÂÈÒÓÂÈ ÙËÓ
ÂΉ‹ÏˆÛË ·ÏÏÂÚÁÈÎÒÓ ÓÔÛËÌ¿ÙˆÓ (42). ª¤ÚÔ˜ Ù˘
¢ÓÔ˚΋˜ ÙÔ˘ ‰Ú¿Û˘ ÔÊ›ÏÂÙ·È ÛÙËÓ ·ÚÔ˘Û›· Á·Ï·-
ÎÙÔ-ÔÏÈÁÔ۷ί·Úȉ›ˆÓ, Ù· ÔÔ›· ÚÔ¿ÁÔ˘Ó ÙËÓ ·Ó¿-
Ù˘ÍË ÙˆÓ bifidobacteria Î·È Á·Ï·ÎÙÔ‚·Î›ÏÏˆÓ ÛÙÔ
·¯‡ ¤ÓÙÂÚÔ (43). ŒÙÛÈ, ηıÈÂÚÒıËÎÂ Ô fiÚÔ˜ «Ú‚ÈÔ-
ÙÈο», Ô˘ ̆ Ô‰ËÏÒÓÂÈ ÔÚÈṲ̂ӷ ›‰Ë ̆ ‰·Ù·ÓıڿΈÓ
Ê˘ÙÈ΋˜ ÚÔ¤Ï¢Û˘ Ô˘ ‰ÂÓ ‰È·ÛÒÓÙ·È ÛÙÔ ÏÂÙfi
¤ÓÙÂÚÔ, ·ÏÏ¿ Êı¿ÓÔ˘Ó ·Ó·ÏÏÔ›ˆÙ· ÛÙÔ ·¯‡ ¤ÓÙÂÚÔ,
fiÔ˘ ÚÔ¿ÁÔ˘Ó ÙÔÓ ÔÏÏ·Ï·ÛÈ·ÛÌfi Ù˘ ÂÓ‰ÔÁÂ-
ÓÔ‡˜ ÂÓÙÂÚÈ΋˜ ¯ÏˆÚ›‰·˜ Ì ¢ÓÔ˚Τ˜ Û˘Ó¤ÂȘ ÁÈ·
ÙÔÓ ÍÂÓÈÛÙ‹ (44). À¿Ú¯Ô˘Ó ‰È¿ÊÔÚ· ›‰Ë Ú‚ÈÔÙÈ-
ÎÒÓ, Ì ΢ÚÈfiÙÂÚ· Ù· ÊÚÔ˘ÎÙÔ-ÔÏÈÁÔ۷ί·Ú›‰È·
(º√™), Ô˘ ÚÔ¤Ú¯ÔÓÙ·È ·fi Ê˘Ù¿ .¯. Ì·Ó¿Ó·,
Ú·‰›ÎÈ·, ÛÈÙ¿ÚÈ, ÎÚÂÌ̇‰È·, Î·È Ù· Á·Ï·ÎÙÔ-ÔÏÈÁÔ-
۷ί·Ú›‰È· (°√™) Ô˘ ÚÔ¤Ú¯ÔÓÙ·È ·fi ÙÔ Á¿Ï·
(45). √È ‚ÈÔÌ˯·Ó›Â˜ ·È‰ÈÎÒÓ ÙÚÔÊÒÓ ·Ú‹Á·Á·Ó
ÚÔÛ·ÚÌÔṲ̂ӷ ÚÔ˜ ÙÔ ÌËÙÚÈÎfi Á¿Ï· ÂÚȤ¯ÔÓÙ·
Ì›ÁÌ· º√™ Î·È °√™ Ô˘ ÌÈÌÔ‡ÓÙ·È ÙË ÌÔÚȷ΋ ‰ÔÌ‹
ÙˆÓ ÔÏÈÁÔ۷ί·Úȉ›ˆÓ ÙÔ˘ ÌËÙÚÈÎÔ‡ Á¿Ï·ÎÙÔ˜ (46).
∏ ¯ÔÚ‹ÁËÛË ÙÔ˘ Ì›ÁÌ·ÙÔ˜ ·˘ÙÔ‡ ÙfiÛÔ Û ÙÂÏÂÈfiÌË-
Ó· (47,48) fiÛÔ Î·È Û ÚfiˆÚ· ÓÂÔÁÓ¿ (49,50) ‹Ù·Ó η-
Ï¿ ·ÓÂÎÙ‹ Î·È Û˘Óԉ‡ÙËΠ·fi ·˘ÍË̤ÓË ·Ó¿Ù˘ÍË
bifidobacteria ÛÙÔ ·¯‡ ¤ÓÙÂÚÔ, Î·È Û ÔÚÈṲ̂Ó˜ Â-
ÚÈÙÒÛÂȘ Ì ηٷÛÙÔÏ‹ ÙÔ˘ ÏËı˘ÛÌÔ‡ ÙˆÓ ·ıÔ-
ÁfiÓˆÓ ÂÓÙÂÚÔ‚·ÎÙËÚȉ›ˆÓ. ¶·Ú¿ÏÏËÏ·, Ô ·ÚÈıÌfi˜
ÙˆÓ ÎÂÓÒÛÂˆÓ Î·È Ë Û‡ÛÙ·ÛË ÙˆÓ ÎÔÚ¿ÓˆÓ, fiˆ˜
Î·È ÙÔ pH, ·ÚÔÌÔ›·˙·Ó Ì ÂΛӷ ÓÂÔÁÓÒÓ Ô˘ ÙÚ¤-
ÊÔÓÙ·Ó Ì ÌËÙÚÈÎfi Á¿Ï·. ¶ÚfiÛÊ·Ù·, ·Ó·Ê¤ÚıËΠηÈ
¢ÓÔ˚΋ ‰Ú¿ÛË ÙˆÓ Ú‚ÈÔÙÈÎÒÓ ÛÙËÓ ÚfiÏË„Ë Ù˘
·ÙÔÈ΋˜ ‰ÂÚÌ·Ù›Ùȉ·˜ (51).
∞Ó Î·È Ù· Ú‚ÈÔÙÈο ·ÎfiÌ· ‰ÂÓ ıˆÚÔ‡ÓÙ·È
·fiÏ˘Ù· ·ÛÊ·Ï‹, ı· Ú¤ÂÈ Ó· ‰›ÓÔÓÙ·È Ì ÚÔÛÔ-
¯‹ ÂȉÈο Û ÚfiˆÚ· ‹ ‰˘ÛÙÚÔÊÈο ÓÂÔÁÓ¿ ÁÈ·Ù›
ÌÔÚ› Ó· ÌÂÈÒÛÔ˘Ó ÙËÓ ¤„Ë Î·È ÙËÓ ·ÔÚÚfiÊËÛË
Ï›Ô˘˜ Î·È ˘‰·Ù·ÓıÚ¿ÎˆÓ ·fi ÙÔ ¤ÓÙÂÚÔ (52).
¶ÚÔ‚ÈÔÙÈο
∂›Ó·È ˙ÒÓÙ˜ ÌÈÎÚÔÔÚÁ·ÓÈÛÌÔ› Ô˘ ¯ÔÚËÁÔ‡ÌÂÓÔÈ
Û ·ÚΛ˜ ÔÛfiÙËÙ˜ ÚÔ¿ÁÔ˘Ó ÙËÓ ˘Á›· ÙÔ˘ ÍÂ-
ÓÈÛÙ‹. ∆· ÂÚÈÛÛfiÙÂÚÔ ¯ÚËÛÈÌÔÔÈÔ‡ÌÂÓ· Â›Ó·È Á·-
Ï·ÎÙÔ‚¿ÎÈÏÏÔÈ Î·È bifidobacteria, Ù· ÔÔ›· ̆ ¿Ú¯Ô˘Ó
Ê˘ÛÈÔÏÔÁÈο Î·È ÛÙÔ ¤ÓÙÂÚÔ ‚ÚÂÊÒÓ Ô˘ ·›ÚÓÔ˘Ó
ÌËÙÚÈÎfi Á¿Ï·. ∏ ·ÚÔ˘Û›· ÙÔ˘˜ ÛÙÔ ¤ÓÙÂÚÔ Î·Ù·-
ÛÙ¤ÏÏÂÈ ÙÔÓ ÔÏÏ·Ï·ÛÈ·ÛÌfi ÙˆÓ ·ıÔÁfiÓˆÓ ÌÈÎÚÔ-
‚›ˆÓ, ÌÂÈÒÓÂÈ ÙË ÊÏÂÁÌÔÓÒ‰Ë ·ÓÙ›‰Ú·ÛË ÙÔ˘ ÂÓÙ¤-
ÚÔ˘ Î·È ÙËÓ ·ÓÙ›‰Ú·ÛË ˘ÂÚ¢·ÈÛıËÛ›·˜ Û ·ÏÏÂÚ-
ÁÈÔÁfiÓ· (53,54). ¶ÚÔ‚ÈÔÙÈο ¤¯Ô˘Ó ¯ÚËÛÈÌÔÔÈËı›
Ì ÂÈÙ˘¯›· Û Á·ÛÙÚÂÓÙÂÚ›Ùȉ· ·fi ROTA Èfi (55),
ÛÙË ‰È¿ÚÚÔÈ· ·fi ¯ÔÚ‹ÁËÛË ·ÓÙÈ‚ÈÔÙÈÎÒÓ (56), ÛÙËÓ
ÚfiÏË„Ë ÙÚÔÊÈ΋˜ ·ÏÏÂÚÁ›·˜ (57) Î·È ÈÔ ÚfiÛÊ·Ù·
ÛÙËÓ ÚfiÏË„Ë Ù˘ ¡∂∫ Û ÚfiˆÚ· ÓÂÔÁÓ¿ (58,59).
°È· Ù· ÚÔ‚ÈÔÙÈο ··ÈÙÔ‡ÓÙ·È ÂÚ·ÈÙ¤Úˆ ÌÂϤ-
Ù˜. ¶·ÚÂÓ¤ÚÁÂȘ ·Ó·Ê¤ÚÔÓÙ·È Ôχ Û¿ÓÈ· ÌÂÙ¿ ÙË
¯ÔÚ‹ÁËÛË Á·Ï·ÎÙÔ‚¿ÎÈÏÏˆÓ Î·È ˙˘ÌÔ̇ÎËÙˆÓ Î·È
ÂÚÈÏ·Ì‚¿ÓÔ˘Ó Û˘ÛÙËÌ·ÙÈΤ˜ ÏÔÈÌÒÍÂȘ, ÂȉÈο ÛÂ
·ÓÔÛÔηٷÛÙ·Ï̤ӷ ¿ÙÔÌ·, ÌÂÙ·‚ÔÏÈ΋ ÔͤˆÛË (Á·-
Ï·ÎÙÔ‚¿ÎÈÏÏÔÈ Ô˘ ·Ú¿ÁÔ˘Ó Á·Ï·ÎÙÈÎfi Ô͇), ÌÂÙ·-
ÊÔÚ¿ ÁÂÓÂÙÈÎÔ‡ ˘ÏÈÎÔ‡ ÚÔ˜ ¿ÏÏ· ÌÈÎÚfi‚È·, ÌÂ Û˘Ó¤-
ÂÈ· ÙË ‰ËÌÈÔ˘ÚÁ›· ·ÓıÂÎÙÈÎÒÓ ÛÙÂϯÒÓ (60,61).
™˘Ì‚ÈÔÙÈο
ŒÓ· ÌÂÈÔÓ¤ÎÙËÌ· ÙˆÓ ÚÔ‚ÈÔÙÈÎÒÓ Â›Ó·È fiÙÈ
¤¯Ô˘Ó ‚Ú·¯Â›· ‰Ú¿ÛË, ÌÂ Û˘Ó¤ÂÈ· Ó· Ú¤ÂÈ Ó· ¯Ô-
ÚËÁÔ‡ÓÙ·È Î·ıËÌÂÚÈÓ¿ .∏ ÚÔÛı‹ÎË Ú‚ÈÔÙÈÎÒÓ
ÛÙ· ÚÔ‚ÈÔÙÈο ·˘Í¿ÓÂÈ ÙÔ ¯ÚfiÓÔ ‰Ú¿Û˘ ÙÔ˘˜ ÎÈ
¤ÙÛÈ ‰ÂÓ ··ÈÙÂ›Ù·È Û˘¯Ó‹ ¯ÔÚ‹ÁËÛ‹ ÙÔ˘˜ (62). ∏
¯Ú‹ÛË ÙÔ˘˜, fï˜, ‰ÂÓ ¤¯ÂÈ ·ÎfiÌË ÙÂÎÌËÚȈı› ÛÙË
‚È‚ÏÈÔÁÚ·Ê›·.
°¿Ï·Ù· ·˘ÍË̤Ó˘ ıÚÂÙÈ΋˜ ·Í›·˜
∏ ÂÓ‰ÔÌ‹ÙÚÈ· ‰˘ÛÙÚÔÊ›·, ·ÏÏ¿ Î·È Ë Î·Î‹ ıÚ¤-
„Ë Ì¤Û· ÛÙÔ˘˜ ÚÒÙÔ˘˜ ÎÚ›ÛÈÌÔ˘˜ Ì‹Ó˜ ˙ˆ‹˜,
ÌÔÚ› Ó· ¤¯ÂÈ ÛÔ‚·Úfiٷ٘ Û˘Ó¤ÂȘ ÛÙËÓ „˘¯Ô-
ÎÈÓËÙÈ΋ Î·È ÛˆÌ·ÙÈ΋ ·Ó¿Ù˘ÍË ÙÔ˘ ‚Ú¤ÊÔ˘˜
(63,64). H Û˘¯ÓfiÙËÙ· ÂÓ‰ÔÌ‹ÙÚÈ·˜ ‰˘ÛÙÚÔÊ›·˜ ÛÂ
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·119

120 Ã. ∫ÒÛÙ·ÏÔ˜
Paediatriki 2008;71:116-122
ÓÂÔÁÓ¿ Ì Ôχ ¯·ÌËÏfi ‚¿ÚÔ˜ Á¤ÓÓËÛ˘ Êı¿ÓÂÈ Î·ÈÙÔ 30%. ªÂÁ¿ÏÔ˜ ·ÚÈıÌfi˜ ·˘ÙÒÓ ÙˆÓ ·È‰ÈÒÓ ÂÍ·-ÎÔÏÔ˘ıÔ‡Ó Ó· ˘ÔÛÈÙ›˙ÔÓÙ·È Î·È ÌÂÙ¿ ÙË Á¤ÓÓËÛË,ÏfiÁˆ Ù˘ ÏËıÒÚ·˜ ÙˆÓ ÚÔ‚ÏËÌ¿ÙˆÓ Ô˘ ·ÓÙÈÌÂ-Ùˆ›˙Ô˘Ó Î·Ù¿ ÙË ÓÔÛËÏ›· ÙÔ˘˜ Û ÂÓÙ·ÙÈ΋ ÌÔÓ¿-‰·, ÌÂ Û˘Ó¤ÂÈ· Ó· ÂÌÊ·Ó›˙ÔÓÙ·È ‰˘ÛÙÚÔÊÈο ηٿÙËÓ ¤ÍÔ‰Ô ·fi ÙÔ ÓÔÛÔÎÔÌÂ›Ô (65).
ŒÙÛÈ ÙÔ ‚¿ÚÔ˜ ¤¯ÂÈ ÂÈÎÂÓÙÚˆı› ÛÙË ÛˆÛÙ‹ Û›ÙÈ-ÛË ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ ÌÂÙ¿ ÙËÓ ¤ÍÔ‰Ô ·fi ÙÔ ÓÔÛÔ-ÎÔÌ›Ô. ∆· ·ÔÙÂϤÛÌ·Ù· Â›Ó·È ·ÓÙÈÎÚÔ˘fiÌÂÓ·.À¿Ú¯Ô˘Ó ÌÂϤÙ˜ Ô˘ ‰Â›¯ÓÔ˘Ó fiÙÈ Ë Ù·¯Â›· ·Ó·-ÏËڈ̷ÙÈ΋ ·‡ÍËÛË ÌÂÙ¿ ÙË Á¤ÓÓËÛË Û ÂÏÏÈÔ-‚·Ú‹ ÓÂÔÁÓ¿ Ô‰ËÁ› Û ηχÙÂÚË ÓÔËÙÈ΋ ÂͤÏÈÍË(66,67). À¿Ú¯ÂÈ, fï˜, Î·È Ë ¿Ô„Ë fiÙÈ Ù·¯Â›· Úfi-ÛÏË„Ë ‚¿ÚÔ˘˜ ÌÂÙ¿ ÙË Á¤ÓÓËÛË ÌÔÚ› Ó· Úԉȷ-ı¤ÛÂÈ Û ¯ÚfiÓÈ· ηډȷÁÁÂȷ΋ ÓfiÛÔ, ˘¤ÚÙ·ÛË,۷ί·ÚÒ‰Ë ‰È·‚‹ÙË Ù‡Ô˘ 2 Î·È ÔÛÙÂÔfiÚˆÛË ÛÙËÓÂÓ‹ÏÈÎË ˙ˆ‹ (68). ªÈ· ÌÂÁ¿ÏË ·Ó·ÛÎfiËÛË ‰ÂÓ¤‰ÂÈÍ ηӤӷ fiÊÂÏÔ˜ ˆ˜ ÚÔ˜ ÙË ÛˆÌ·ÙÈ΋ Î·È æ∫ÂͤÏÈÍË (69).
∞fi Ù· ·Ú·¿Óˆ Û˘ÌÂÚ·›ÓÂÙ·È fiÙÈ ÛÙÔ ı¤Ì·Ù˘ ‰È·ÙÚÔÊ‹˜ ÙÔ˘ ÓÂÔÁÓÔ‡ ··ÈÙÂ›Ù·È Û‡ÓÂÛË Î·ÈÚÔÛÔ¯‹ ÛÙËÓ ˘ÈÔı¤ÙËÛË Ó¤ˆÓ ·Ú¯ÒÓ. Àfi ·˘Ùfi ÙÔÓ‡̷, Ë ESPGHAN Âͤ‰ˆÛ ԉËÁ›Â˜ Ô˘ ÂÈÛË-Ì·›ÓÔ˘Ó fiÙÈ “Ë ·Ï‹ ·ÚÔ˘Û›· ÌÈ·˜ Ô˘Û›·˜ ÛÙÔ ÌË-ÙÚÈÎfi Á¿Ï· ‰ÂÓ ‰ÈηÈÔÏÔÁ› ÙËÓ ·˘ÙfiÌ·ÙË ÚÔÛı‹ÎËÙ˘ ÛÙÔ Û˘ÓıÂÙÈÎfi Á¿Ï·, ¯ˆÚ›˜ ÚÔËÁÔ˘Ì¤Óˆ˜ Ó·‰È·ÈÛÙˆı› fi¯È ÌfiÓÔ ÙÔ ‚Ú·¯˘ÚfiıÂÛÌÔ, ·ÏÏ¿ ηÈÙÔ Ì·ÎÚÔÚfiıÂÛÌÔ fiÊÂÏÔ˜ Ô˘ ·ÔʤÚÂÈ ÛÙÔÓ ·Ó·-Ù˘ÛÛfiÌÂÓÔ ÔÚÁ·ÓÈÛÌfi” (70).
µÈ‚ÏÈÔÁÚ·Ê›·
1. Carver JD. Dietary nucleotides: effects on the immune andgastrointestinal systems. Acta Paediatr Suppl 1999;88:83-88.
2. Uauy R, Stringel G, Thomas R, Quan R. Effect of dietary nu-cleosides on growth and maturation of the developing gut inthe rat. J Pediatr Gastroenterol Nutr 1990;10:497-503.
3. Gil A, Corral E, Martinez A, Molina JA. Effects of the addi-tion of nucleotides to an adapted milk formula on the mi-crobial pattern of feces in at term newborn infants. ClinNutr Gastroenterol 1986;1:127-132.
4. Balmer SE, Hanvey LS, Wharton BA. Diet and faecal florain the newborn: nucleotides. Arch Dis Child Fetal Neona-tal Ed 1994;70:F137-F140.
5. Carver JD, Pimentel B, Cox WI, Barness LA. Dietary nu-cleotide effects upon immune function in infants. Pedi-atrics 1991;88:359-363.
6. Brunser O, Espinoza J, Araya M, Cruchet S, Gil A. Effect ofdietary nucleotide supplementation on diarrhoeal diseasein infants. Acta Paediatr 1994;83:188-191.
7. Cosgrove M, Davies DP, Jenkins HR. Nucleotide supplemen-tation and the growth of term small for gestational age in-fants. Arch Dis Child Fetal Neonatal Ed 1996;74:F122-F125.
8. Carver JD, Walker WA. The role of nucleotides in humannutrition. J Nutr Biochem 1995;6:58-72.
9. Yu VY. The role of dietary nucleotides in neonatal and in-fant nutrition. Singapore Med J 1998;39:145-150.
10. Yau KI, Huang CB, Chen W, Chen SJ, Chou YH, Huang
FY, et al. Effect of nucleotides on diarrhea and immune re-
sponses in healthy term infants in Taiwan. J Pediatr Gas-
troenterol Nutr 2003;36:37-43.
11. ™ÎÔ˘Ù¤ÚË µ, ∫ÒÛÙ·ÏÔ˜ Ã, ™Â‚·ÛÙÈ¿‰Ô˘ ™, °·‚Ú›ÏË ™,
¢·ÓÂÏ¿ÙÔ˘ ∫, µÔÁÈ·Ù˙‹ ∞, Î·È Û˘Ó. ∏ ›‰Ú·ÛË ÂÓfi˜
ÂÌÏÔ˘ÙÈṲ̂ÓÔ˘ Ì ÓÔ˘ÎÏÂÔÙ›‰È· Á¿Ï·ÙÔ˜ ÛÙÔ ÂÙÈÎfi
Û‡ÛÙËÌ· ÚÔÒÚˆÓ ÓÂÔÁÓÒÓ. ¶·È‰È·ÙÚÈ΋ 2002;65:52-56.
12. Litman BJ, Mitchell DC. A role for phospholipid polyun-
saturation in modulating membrane protein function.
Lipids 1996;31:S193-S197.
13. Neuringer M, Jeffrey BG. Visual development: Neural basis
and new assessment methods. J Pediatr 2003;143:S87-S95.
14. Mitchell DC, Niu SL, Litman BJ. DHA-rich phospholipids
optimize G-Protein-coupled signaling. J Pediatr 2003:143:
S80-S86.
15. Calder PC. ˆ3 Polyunsaturated Fatty Acids, Inflammation
and Immunity. In: ∏amazaki T, Okuyama H, editors. Fat-
ty Acids and Lipids - New Findings. World Rev Nutr Diet.
Basel: Karger; 2001. p. 109-116.
16. Jensen CL, Heird WC. Lipids with an emphasis on long-
chain polyunsaturated fatty acids. Clin Perinatol 2002;
29:261-281, vi.
17. Carlson SE, Cooke RJ, Werkman SH, Tolley EA. First year
growth of preterm infants fed standard compared to marine
oil n-3 supplemented formula. Lipids 1992;27:901-907.
18. Koletzko B, Baker S, Cleghorn G, Neto UF, Gopalan S,
Hernell O, et al. Global standard for the composition of in-
fant formula: recommendations of an ESPGHAN coordi-
nated international expert group. J Pediatr Gastroenterol
Nutr 2005;41:584-599.
19. Simmer K, Patole S. Longchain polyunsaturated fatty acid
supplementation in preterm infants. Cohrane Review. The
Cohrane Library. Issue 3. Chichester: Wiley; 2004.
20. Fewtrell MS, Abbott RA, Kennedy K, Singhal A, Morley R,
Caine E, et al. Randomized, double-blind trial of long-
chain polyunsaturated fatty acid supplementation with fish
oil and borage oil in preterm infants. J Pediatr 2004;144:
471-479.
21. Clandinin M, VanAerde J, Antonson D, Lim M, Stevens D,
Merkel K, et al. Formulas with docosahexaenoic acid
(DHA) and arachidonic acid (AA) promote better growth
and development scores in very-low-birth-weight infants
(VLBW). Pediatr Res 2002;51:187A-188A.
22. Simmer K. Longchain polyunsaturated fatty acid supple-
mentation in infants born at term. Cochrane Review. The
Cochrane Library. Issue 4. Oxford: Update Software; 2004.
23. SanGiovanni JP, Berkey CS, Dwyer JT, Colditz GA. Dietary
essential fatty acids, long-chain polyunsaturated fatty acids,
and visual resolution acuity in healthy fullterm infants: a
systematic review. Early Hum Dev 2000;57:165-188.
24. Auestad N, Scott DT, Janowsky JS, Jacobsen C, Carroll RE,
Montalto MB, et al. Visual, cognitive, and language assess-
ments at 39 months: a follow-up study of children fed for-
mulas containing long-chain polyunsaturated fatty acids to
1 year of age. Pediatrics 2003;112:e177-183.
25. Fewtrell MS. Long-Chain Polyunsaturated Fatty Acids in
Early Life: Effects on Multiple Health Outcomes. Lucas A,
Sampson HA, editors. Primary Prevention by Nutrition
Intervention in Infancy and Childhood. Nestlé Nutr
Workshop Ser Pediatr Program. Nestec Ltd., Vevey/S
Karger AG, Basel, 2006, vol 57. p. 203-221.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·120

121¢È·ÙÚÔÊ‹ ÙÔ˘ ‚Ú¤ÊÔ˘˜
¶·È‰È·ÙÚÈ΋ 2008;71:116-122
26. Souba WW. Intestinal glutamine metabolism and nutri-
tion. J Nutr Biochem 1993;4:2-9.
27. Neu J, De Marco V, Weiss M.Glutamine supplementation
in low-birth-weight infants: mechanisms of action. J Par-
enter Enteral Nutr 1999;23:S49-S51.
28. Buchman AL. Glutamine: commercially essential or condi-
tionally essential? A critical appraisal of the human data.
Am J Clin Nutr 2001;74:25-32.
29. Tubman TR, Thompson SW, McGuire W. Glutamine sup-
plementation to prevent morbidity and mortality in
preterm infants. Cochrane Database Syst Rev 2005;(1):
CD001457.
30. Burrin DG, Shulman RJ, Langston C, Storm MC. Supple-
mental alanylglutamine, organ growth, and nitrogen me-
tabolism in neonatal pigs fed by total parenteral nutrition.
JPEN J Parenter Enteral Nutr 1994;18:313-319.
31. Garlick PJ. Assessment of the safety of glutamine and oth-
er amino acids. J Nutr 2001;131:2556S-2561S.
32. Daly JM, Reynolds J, Thom A, Kinsley L, Dietrick-Gallagher
M, Shou J, et al. Immune and metabolic effects of arginine in
the surgical patient. Ann Surg 1988;208:512-523.
33. Efron D, Barbul A. Role of arginine in immunonutrition. J
Gastroenterol 2000;35:20-23.
34. Becker RM, Wu G, Galanko JA, Chen W, Maynor AR, Bose
CL, et al. Reduced serum amino acid concentrations in infants
with necrotizing enterocolitis. J Pediatr 2000;137:785-793.
35. Vosatka RJ, Kashyap S, Trifiletti RR. Arginine deficiency
accompanies persistent pulmonary hypertension of the
newborn. Biol Neonate 1994;66:65-70.
36. Thiemermann C, Vane J. Inhibition of nitric oxide synthe-
sis reduces the hypertension induced by bacterial lipopoly-
saccharides in the rat in vivo. Eur J Pharmacol 1990;182:
591-595.
37. Schmidt-Sommerfeld E, Penn D. Carnitine and total par-
enteral nutrition of the neonate. Biol Neonate 1990;58;81-88.
38. Cairns PA, Stalker DJ. Carnitine supplementation of par-
enterally fed neonates. Cochrane Database Syst Rev 2000;
(4):CD000950.
39. Borum PR. Should carnitine be added to parenteral nutri-
tion solutions? Nutr Clin Prac 2000;15:153-154.
40. Lönnerdal B, Hernell O. Iron, zinc, copper and selenium
status of breast-fed infants and infants fed trace element
fortified milk-based infant formula. Acta Paediatr 1994;83:
367-373.
41. Dewey KG, Domellöf M, Cohen RJ, Landa Rivera L, Her-
nell O, Lönnerdal B. Iron supplementation affects growth
and morbidity of breast-fed infants: results of a random-
ized trial in Sweden and Honduras. J Nutr 2002;132:3249-
3255.
42. Kunz C, Rudloff S, Baier W, Klein N, Strobel S. Oligosac-
charides in human milk: structural, functional, and meta-
bolic aspects. Annu Rev Nutr 2000;20:699-722.
43. Fanaro S, Chierici R, Guerrini P, Vigi V. Intestinal mi-
croflora in early infancy: composition and development.
Acta Paediatr Suppl 2003;91:48-55.
44. Gibson GR, Roberfroid MB. Dietary modulation of the hu-
man colonic microbiota: introducing the concept of prebi-
otics. J Nutr 1995;125:1401-1412.
45. Veereman-Wauters G. Application of prebiotics in infant
foods. Br J Nutr 2005;93:S57-S60.
46. Fanaro S, Boehm G, Garssen J, Knol J, Mosca F, Stahl B, et
al. Galacto-oligosaccharides and long-chain fructo-oligo-
saccharides as prebiotics in infant formulas: a review. Acta
Paediatr Suppl 2005;94:22-26.
47. Moro G, Minoli I, Mosca M, Fanaro S, Jelinek J, Stahl B, et
al. Dosage-related bifidogenic effects of galacto- and fruc-
tooligosaccharides in formula-fed term infants. J Pediatr
Gastroenterol Nutr 2002;34:291-295.
48. Knol J, Van der Linde EGM, Wells JCK, Böckler HM. An
infant formula containing prebiotics changes the intestinal
microflora of term infants. J Pediatr Gastroenterol Nutr
2003;36:566.
49. Boehm G, Lidestri M, Casetta P, Jelinek J, Negretti F, Stahl
B, et al. Supplementation of a bovine milk formula with an
oligosaccharide mixture increases counts of faecal bifi-
dobacteria in preterm infants. Arch Dis Child Fetal Neona-
tal Ed 2002;86:F178-F181.
50. Kapiki A, Costalos C, Oikonomidou C, Triantafyllidou A,
Loukatou E, Petrohilou V. The effect of a fructo-oligosac-
charide supplemented formula on gut flora of preterm in-
fants. Early Hum Dev 2007;83:335-339.
51. Moro G, Arslanoglu S, Stahl B, Jelinek J, Wahn U, Boehm
G. A mixture of prebiotic oligosaccharides reduces the in-
cidence of atopic dermatitis during the first six months of
age. Arch Dis Child 2006;91:814-819.
52. Koletzko B, Baker S, Cleghorn G, Neto UF, Gopalan S,
Hernell O, et al. Global standard for the composition of in-
fant formula: recommendations of an ESPGHAN coordi-
nated international expert group. J Pediatr Gastroenterol
Nutr 2005;41:584-599.
53. Isolauri E, Sütas Y, Kankaanpää P, Arvilommi H, Salminen
S. Probiotics: effects on immunity. Am J Clin Nutr 2001;
73:444S-450S.
54. Neu J, Bernstein H. Update on host defense and im-
munonutrients. Clin Perinatol 2002;29:41-64.
55. Majamaa H, Isolauri E, Saxelin M, Vesikari T. Lactic acid
bacteria in the treatment of acute rotavirus gastroenteritis.
J Pediatr Gastroenterol Nutr 1995;20:333-338.
56. Arvola T, Laiho K, Torkkeli S, Mykkänen H, Salminen S,
Maunula L, et al. Prophylactic Lactobacillus GG reduces
antibiotic-associated diarrhea in children with respiratory
infections: a randomized study. Pediatrics 1999;104:e64.
57. Prescott SL, Macaubas C, Smallacombe T, Holt BJ, Sly PD,
Holt PG. Development of allergen-specific T-cell memory
in atopic and normal children. Lancet 1999;353:196-200.
58. Lin HC, Su BH, Chen AC, Lin TW, Tsai CH, Yeh TF, et al.
Oral probiotics reduce the incidence and severity of necro-
tizing enterocolitis in very low birth weight infants. Pedi-
atrics 2005;115:1-4.
59. Bin-Nun A, Bromiker R, Wilschanski M, Kaplan M, Ru-
densky B, Caplan M. Oral probiotics prevent necrotizing
enterocolitis in very low birth weight neonates. J Pediatr
2005;147:192-196.
60. Szajewska H, Setty M, Mrukowicz J, Guandalini S. Probi-
otics in gastrointestinal diseases in children: hard and not-
so-hard evidence of efficacy. J Pediatr Gastroenterol Nutr
2006;42:454-475.
61. Yamashiro Y, Castaneda C, Davidson G, Gibson G, Penna
FJ, Mack D, et al. Biotherapeutic and nutraceutical
agents:Working Group report of the second World
Congress of Pediatric Gastroenterology, Hepatology, and
Nutrition. J Pediatr Gastroenterol Nutr 2004;39:S596-S600.
62. Rastall RA, Maitin V. Prebiotics and synbiotics: towards the
next generation. Cur Opin Biotechnol 2002;13:490-496.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·121

63. Lucas A, Morley R, Cole TJ. Randomised trial of early dietin preterm babies and later intelligence quotient. BMJ1998;317:1481-1487.
64. Hack M, Schluchter M, Cartar L, Rahman M, Cuttler L,Borawski E. Growth of very low birth weight infants to age20 years. Pediatrics 2003;112:e30-38.
65. Dusick AM, Poindexter BB, Ehrenkranz RA, Lemons JA.Growth failure in the preterm infant: can we catch up?Semin Perinatol 2003;27:302-310.
66. Latal-Hajnal B, von Siebenthal K, Kovari H, Bucher HU,Largo RH. Postnatal growth in VLBW infants: significantassociation with neurodevelopmental outcome. J Pediatr2003;143:163-170.
67. Hack M, Weissman B, Borawski-Clark E. Catch-up growthduring childhood among very low-birth-weight children.Acta Pediatr Adolesc Med 1996;150:1122-1129.
68. Barker DJ, Eriksson JG, Forsén T, Osmond C. Fetal originsof adult disease: strength of effects and biological basis. IntJ Epidemiol 2002;31:1235-1239.
69. ∂hrenkranz RA. Cohrane Database Syst Rev 2005;15;CD004696.
70. ESPGHAN Committee on Nutrition, Aggett PJ, AgostoniC, Axelsson I, De Curtis M, Goulet O, et al. Feedingpreterm infants after hospital discharge: a commentary bythe ESPGHAN Committee on Nutrition. J Pediatr Gas-troenterol Nutr 2006;42:596-603.
122 Ã. ∫ÒÛÙ·ÏÔ˜
Paediatriki 2008;71:116-122
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·122

123∞¡∞™∫√¶∏™∏ REVIEW ARTICLE
¶·È‰È·ÙÚÈ΋ 2008;71:123-127
∂Ӊ›ÍÂȘ ¯ÔÚ‹ÁËÛ˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ ÛÙ· ·È‰È¿ ηÈ
ÙÔ˘˜ ÂÊ‹‚Ô˘˜
E. ∫Ô‡ÛÙ·, ∞. ¶··ı·Ó·Û›Ô˘, Ã. ÷Ù˙Ë·ı·Ó·Û›Ô˘†
¶ÂÚ›ÏË„Ë: ª¤¯ÚÈ ÙË ‰ÂηÂÙ›· ÙÔ˘ 1980, Ë ·˘ÍËÙÈ΋ ÔÚÌfiÓË (GH) ›¯Â ¯ÚËÛÈÌÔÔÈËı› ·ÔÎÏÂÈÛÙÈο ÁÈ·ÙË ıÂڷ›· ·È‰ÈÒÓ Ì ÛÔ‚·Ú‹ ηı˘ÛÙ¤ÚËÛË ÛˆÌ·ÙÈ΋˜ ·Ó¿Ù˘Í˘, ÔÊÂÈÏfiÌÂÓË Û ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ-΋˜ ÔÚÌfiÓ˘ (GHD). ∏ GHD ·ÊÔÚ¿ Û˘Ó‰˘·ÛÌfi ÎÏÈÓÈÎÒÓ, ·ÎÙÈÓÔÏÔÁÈÎÒÓ, ÌÂÙ·‚ÔÏÈÎÒÓ Î·È ÔÚÌÔÓÔÏÔÁÈ-ÎÒÓ Â˘ÚËÌ¿ÙˆÓ. ∏ ÂÈÏÔÁ‹ ÙˆÓ ÂÚÈÛÙ·ÙÈÎÒÓ, ÛÙ· ÔÔ›· ı· Á›ÓÔ˘Ó ‰È·ÁÓˆÛÙÈΤ˜ ‰ÔÎÈ̷ۛ˜ ¤ÎÎÚÈÛ˘ ·˘-ÍËÙÈ΋˜ ÔÚÌfiÓ˘, ÚÔ¸Ôı¤ÙÂÈ ÙË ÛˆÛÙ‹ ·ÍÈÔÏfiÁËÛË ÙˆÓ ÎÏÈÓÈÎÒÓ Â˘ÚËÌ¿ÙˆÓ Î·È Î˘Ú›ˆ˜ ÙÔ˘ ‰È·ÁÚ¿ÌÌ·-ÙÔ˜ ·‡ÍËÛ˘. ∏ ıÂڷ›· Ì G∏ ÛÙ· ·È‰È¿ Ì GHD Ô‰ËÁ› Û ÂÈÙ¿¯˘ÓÛË ÙÔ˘ Ú˘ıÌÔ‡ ·‡ÍËÛ˘ Î·È Â›Ó·È‰˘Ó·Ùfi Ó· ÊÙ¿ÛÔ˘Ó ÛÂ Ê˘ÛÈÔÏÔÁÈÎfi ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·, Â¿Ó Ë ıÂڷ›· ·Ú¯›ÛÂÈ ÂÁη›Úˆ˜. E›Û˘, ÂÎÙfi˜ ·fiÙÔ ‡„Ô˜, Ë GH ¤¯ÂÈ Â˘ÂÚÁÂÙÈ΋ ›‰Ú·ÛË ÛÙË ÛˆÌ·ÙÈ΋ Û‡ÛÙ·ÛË, ÂÏ·ÙÙÒÓÔÓÙ·˜ ÙÔ ÏÈÒ‰Ë ÈÛÙfi, ·˘Í¿ÓÔ-ÓÙ·˜ ÙË Ì˘˚΋ Ì¿˙· Î·È ·˘Í¿ÓÔÓÙ·˜ ÙËÓ ÔÛÙÈ΋ ˘ÎÓfiÙËÙ·, ¯ˆÚ›˜ Ó· ˘¿Ú¯Ô˘Ó ÛÔ‚·Ú¤˜ ·ÚÂÓ¤ÚÁÂȘ. ∫·-Ù¿ ÙË ‰È¿ÚÎÂÈ· ÙˆÓ ÙÂÏÂ˘Ù·›ˆÓ 20 ÂÙÒÓ, ÔÈ ÂӉ›ÍÂȘ ¤¯Ô˘Ó ÂÂÎÙ·ı› Î·È ¤¯ÂÈ ÂÁÎÚÈı› Ë ¯ÔÚ‹ÁËÛ‹ Ù˘ ÛÙ·ÎÔÚ›ÙÛÈ· Ì ۇӉÚÔÌÔ Turner Î·È Û ·È‰È¿ Ì ̄ ÚfiÓÈ· ÓÂÊÚÈ΋ ·Ó¿ÚÎÂÈ· Î·È Û‡Ó‰ÚÔÌÔ Prader-Willi. ™ÙȘ∏¶∞ Î·È ÙȘ ¯ÒÚ˜ Ù˘ ∂˘Úˆ·˚΋˜ ŒÓˆÛ˘ ¤¯ÂÈ ÂÁÎÚÈı› Ë ¯ÔÚ‹ÁËÛË ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Û ·È‰È¿ ÌÈÎÚfi-ۈ̷ ÁÈ· ÙËÓ ËÏÈΛ· ·ËÛ˘, ÂÓÒ Ë ¯ÔÚ‹ÁËÛË GH Û ·È‰È¿ Ì ȉÈÔ·ı¤˜ ¯·ÌËÏfi ·Ó¿ÛÙËÌ· ¤¯ÂÈ ÂÁÎÚÈı›ÌfiÓÔ ÛÙȘ ∏¶∞. ∏ ıÂڷ›· fï˜ ÛÙ· ·È‰È¿ ·˘Ù¿ ‰ÂÓ ¤¯ÂÈ ÂÁÎÚÈı› ÛÙË ¯ÒÚ· Ì·˜. ∆· ÙÂÏÂ˘Ù·›· ¯ÚfiÓÈ·¤¯ÂÈ ÂÂÎÙ·ı› Ë ̄ Ú‹ÛË Ù˘ ÛÙÔ˘˜ ÂÊ‹‚Ô˘˜ Î·È ÙÔ˘˜ ÂÓ‹ÏÈΘ Ì ÛÔ‚·ÚÔ‡ ‚·ıÌÔ‡ GHD. ∏ ıÂڷ›· Ì GHÂ›Ó·È ÌÈ· ·ÎÚÈ‚‹ ıÂڷ›· Î·È ¯ÚÂÈ¿˙ÂÙ·È Ù·ÎÙÈ΋ ·Ú·ÎÔÏÔ‡ıËÛË ·fi ÂÍÂȉÈÎÂ˘Ì¤Ó· ΤÓÙÚ·.
§¤ÍÂȘ ÎÏÂȉȿ: ∞˘ÍËÙÈ΋ ÔÚÌfiÓË, ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘, Û‡Ó‰ÚÔÌÔ ∆urner, Û‡Ó‰ÚÔÌÔ Prader-Willi,
¯ÚfiÓÈ· ÓÂÊÚÈ΋ ·Ó¿ÚÎÂÈ·.
Indications for administering growth hormone to children and
adolescents
∂. Kousta, A. Papathanassiou, C. Hadjiathanassiou†
Abstract: Recombinant growth hormone (GH) was used exclusively for the treatment of children withsevere growth retardation due to GH deficiency (GHD) up until the end of the 1980’s. GHD is characterizedby a combination of clinical, radiological, metabolic and hormonal abnormalities. The selection of cases forwhom there is a need to proceed to stimulation tests requires accurate auxological data and correctinterpretation of the growth curve. GH treatment in children with GHD leads to acceleration of growthvelocity and, if treatment is started early enough, to a final height within the normal range. Treatment withGH improves not only the height, but also body composition, by decreasing fat mass and increasing bonedensity, without significant side effects. During the last 20 years, the indications for treatment with GH havebeen expanded and its use has been approved for girls with Turner syndrome and for children with chronicrenal failure and Prader-Willi syndrome. In the USA and some countries of the EU, GH treatment is approvedfor children born small for gestational age. Treatment for idiopathic short stature has been approved only inthe USA. These indications have not been approved in Greece. Over the last few years its use has beenextended to adolescents and adults with severe GH deficiency. GH treatment is an expensive therapy andregular monitoring of its use needs to be made in specialised centres.
Key words: Growth hormone, growth hormone deficiency, Tyrner syndrome, Prader-Willi syndrome, chronic
renal failure.
∂Ó‰ÔÎÚÈÓÔÏÔÁÈÎfi ∆Ì‹Ì·¡ÔÛÔÎÔÌ›Ԣ ¶·›‰ˆÓ “¶. & ∞. ∫˘ÚÈ·ÎÔ‡”, ∞ı‹Ó·
AÏÏËÏÔÁÚ·Ê›·:
∂ϤÓË ∫Ô‡ÛÙ·[email protected]™. ∞Ú‚·ÓÈÙ¿ÎË 6∆.∫. 491 00, ∫¤Ú΢ڷ
Department ofEndocrinology, “P. & A. Kyriakou”Children’s Hospital, Athens
Correspondence:
Eleni [email protected], Sp. ∞rvanitaki St., 491 00, Corfu, Greece
™˘ÓÙÔÌÔÁڷʛ˜
GH A˘ÍËÙÈ΋ ÔÚÌfiÓËGHD AÓ¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘IGFs A˘ÍËÙÈÎÔ› ·Ú¿ÁÔÓÙ˜ISS I‰ÈÔ·ı¤˜ ¯·ÌËÏfi ·Ó¿ÛÙËÌ·SGA ¶·È‰È¿ Ô˘ ÁÂÓÓÈÔ‡ÓÙ·È ÌÈÎÚfiۈ̷ ÁÈ· ÙËÓ
ËÏÈΛ· ·ËÛ˘
á∞ ÃÚfiÓÈ· ÓÂÊÚÈ΋ ·Ó¿ÚÎÂÈ·
EÈÛ·ÁˆÁ‹
∏ GH ¯ÚËÛÈÌÔÔÈÂ›Ù·È ÂÈÙ˘¯Ò˜ ÁÈ· ÙË ıÂ-
ڷ›· ·È‰ÈÒÓ Ì ¯·ÌËÏfi ·Ó¿ÛÙËÌ· ÁÈ· Û¯Â-
‰fiÓ 50 ¯ÚfiÓÈ·. ∞Ú¯Èο, ¯ÚËÛÈÌÔÔÈ‹ıËΠGH
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·123

124 E. ∫Ô‡ÛÙ· Î·È Û˘Ó.
Paediatriki 2008;71:123-127
ÚÔÂÚ¯fiÌÂÓË ·fi ·ÓıÚÒÈÓÔ ÈÛÙfi ̆ fiÊ˘Û˘, Ë ̄ Ú‹-
ÛË Ù˘ ÔÔ›·˜ fï˜ ‰È·ÎfiËΠÏfiÁˆ Ù˘ ·ÈÙÈÔÏÔÁÈ-
΋˜ Û˘Û¯¤ÙÈÛ‹˜ Ù˘ Ì ÙË ÓfiÛÔ Creutzfeldt-Jakob,
ÌÈ· Û¿ÓÈ· ı·Ó·ÙËÊfiÚÔ, ÛÔÁÁÔÂȉ‹ ÂÁÎÂÊ·ÏÔ¿-
ıÂÈ·. ∏ ·Ú·ÁˆÁ‹ ‚ÈÔÛ˘ÓıÂÙÈ΋˜ GH Ô‰‹ÁËÛ ÛÙËÓ
¢ڇÙÂÚË ¯Ú‹ÛË Ù˘ GH. M¤¯ÚÈ Ù· ̤۷ Ù˘ ‰ÂηÂ-
Ù›·˜ ÙÔ˘ 1980, Ë GH ¯ÚËÛÈÌÔÔÈ‹ıËΠ·ÔÎÏÂÈÛÙÈο
ÁÈ· ÙË ıÂڷ›· ·È‰ÈÒÓ Ì ÛÔ‚·Ú‹ ηı˘ÛÙ¤ÚËÛË
ۈ̷ÙÈ΋˜ ·Ó¿Ù˘Í˘, ÔÊÂÈÏfiÌÂÓË Û GHD. ∫·Ù¿
ÙË ‰È¿ÚÎÂÈ· ÙˆÓ ÙÂÏÂ˘Ù·›ˆÓ 20 ÂÙÒÓ, ÔÈ ÂӉ›ÍÂȘ
¤¯Ô˘Ó ÂÂÎÙ·ı› Î·È ÂÚÈÏ·Ì‚¿ÓÔ˘Ó ÙÔ Û‡Ó‰ÚÔÌÔ
Turner (1), ÙË ¯ÚfiÓÈ· ÓÂÊÚÈ΋ ·Ó¿ÚÎÂÈ· (2) Î·È ÙÔ
Û‡Ó‰ÚÔÌÔ Prader-Willi (3). H GH ¯ÚËÛÈÌÔÔÈ›ٷÈ
·ÎfiÌË Û ·È‰È¿ Ô˘ ÁÂÓÓÈÔ‡ÓÙ·È ÌÈÎÚfiۈ̷ ÁÈ· ÙËÓ
ËÏÈΛ· ·ËÛ˘ (Small for Gestational Age - SGA) (4).
∏ ¤Ó‰ÂÈÍË ·˘Ù‹ ¤¯ÂÈ ÂÁÎÚÈı› Û ∞ÌÂÚÈ΋ Î·È ∂˘ÚÒË
Î·È ÛÙËÓ ∂ÏÏ¿‰· ¤¯ÂÈ ÂÁÎÚÈı› ·fi ÙÔÓ ∂√º Î·È ÙÔ
∫∂™À Î·È ‚Ú›ÛÎÂÙ·È ÛÙÔ ÙÂÏÈÎfi ÛÙ¿‰ÈÔ ˘ÔÁÚ·Ê‹˜.
∞ÎfiÌ·, Ë GH ¤¯ÂÈ ¯ÔÚËÁËı› Û ·È‰È¿ Ì ȉÈÔ·ı¤˜
¯·ÌËÏfi ·Ó¿ÛÙËÌ· (Idiopathic Short Stature - ISS) (5).
™ÙȘ ∏¶∞ ¤¯ÂÈ ‰Ôı› ¤ÁÎÚÈÛË ÌfiÓÔ Û ¤Ó· Û··ÛÌ·
Î·È ÚÔ˜ ÙÔ ·ÚfiÓ Ë ¯ÔÚ‹ÁËÛ‹ Ù˘ ÛÙ· ·È‰È¿ ·˘Ù¿
ı· Ú¤ÂÈ Ó· Á›ÓÂÙ·È ÌfiÓÔ ÛÙ· Ï·›ÛÈ· ÂÚ¢ÓËÙÈÎÒÓ
ÚˆÙÔÎfiÏψÓ.
ª¤¯ÚÈ ÚfiÛÊ·Ù·, ÛÙ· ·È‰È¿ Ì GHD ÁÈÓfiÙ·Ó
‰È·ÎÔ‹ Ù˘ ıÂڷ›·˜ ÌÂÙ¿ ÙÔ Ù¤ÏÔ˜ Ù˘ ÂÚÈfi‰Ô˘
·Ó¿Ù˘Í˘. ∆ÒÚ·, Û˘ÓÈÛÙ¿Ù·È Ó· Á›ÓÂÙ·È Â·Ó¤ÏÂÁ-
¯Ô˜ Ù˘ ¤ÎÎÚÈÛ˘ Ù˘ GH ÌÂÙ¿ ÙË ‰È·ÎÔ‹ Ù˘ ıÂ-
ڷ›·˜ ηٿ ÙË Û‡ÁÎÏÂÈÛË ÙˆÓ ÂÈʇÛˆÓ, ȉȷÈÙ¤-
Úˆ˜ ÙˆÓ ·È‰ÈÒÓ Ì Ôχ ¯·ÌËϤ˜ ÙÈ̤˜ GH Î·È ÌÂ
·ıÔÏÔÁÈ΋ Ì·ÁÓËÙÈ΋ ÙÔÌÔÁÚ·Ê›· ˘fiÊ˘Û˘ (ÌÈ-
ÎÚfi ‡„Ô˜, ¤ÎÙÔË ˘fiÊ˘ÛË) ‹ ÈÛÙÔÚÈÎfi fiÁÎÔ˘ ‹
·ÎÙÈÓÔ‚ÔÏ›·˜. ™Â fiÛÔ˘˜ ÏËÚÔ‡Ó Ù· ÎÚÈÙ‹ÚÈ· ¯·ÌË-
Ï‹˜ ¤ÎÎÚÈÛ˘ GH Ì ‚¿ÛË Ù· ÎÚÈÙ‹ÚÈ· ÙˆÓ ÂÓËÏ›-
ΈÓ, Û˘ÓÈÛÙ¿Ù·È Û˘Ó¤¯ÈÛË Ù˘ ıÂڷ›·˜ Ì ‰ÔÛÔÏÔ-
Á›· ÂÓËϛΈÓ, ÏfiÁˆ ÙˆÓ ÌÂÙ·‚ÔÏÈÎÒÓ ÂÈÙÒÛˆÓ
Ù˘ ÛÔ‚·Ú‹˜ ·Ó¿ÚÎÂÈ·˜ ÛÙËÓ ÂÓ‹ÏÈÎÔ ˙ˆ‹. ∫¿-
ÔÈÔÈ ÂÚ¢ÓËÙ¤˜ Û˘ÓÈÛÙÔ‡Ó ÙË Û˘Ó¤¯ÈÛË Ù˘ ıÂÚ·-
›·˜ ÛÙÔ˘˜ ÂÊ‹‚Ô˘˜ ÁÈ· οÔÈÔ ‰È¿ÛÙËÌ· ÌÂÙ¿ ÙË
Û‡ÁÎÏÂÈÛË ÙˆÓ ÂÈʇÛˆÓ, ÏfiÁˆ Ù˘ ıÂÙÈ΋˜ ›-
‰Ú·Û˘ ÛÙËÓ ÔÛÙÈ΋ ˘ÎÓfiÙËÙ· (6).
∏ ıÂڷ›· Ì GH ¯ÚÂÈ¿˙ÂÙ·È Ù·ÎÙÈ΋ ·Ú·ÎÔ-
ÏÔ‡ıËÛË ·fi ÂÍÂȉÈÎÂ˘Ì¤Ó· ΤÓÙÚ·. ∆Ô ÎfiÛÙÔ˜ Ù˘
ıÂڷ›·˜ Â›Ó·È ÌÂÁ¿ÏÔ, ȉȷ›ÙÂÚ· ÛÙ· ·È‰È¿ ÌÂ
Û‡Ó‰ÚÔÌÔ Turner, ¯ÚfiÓÈ· ÓÂÊÚÈ΋ ·Ó¿ÚÎÂÈ· ηÈ
ȉÈÔ·ı¤˜ ¯·ÌËÏfi ·Ó¿ÛÙËÌ·, Ù· ÔÔ›· ¯ÚÂÈ¿˙ÔÓÙ·È
ÌÂÁ·Ï‡ÙÂÚË ‰fiÛË GH. ∂ÈϤÔÓ, ÚÈÓ ·ÔÊ·ÛÈÛÙ›
Ë ıÂڷ›· Ì GH, Ú¤ÂÈ ¤Ú· ·fi ÙËÓ Â˘ÓÔ˚΋
›‰Ú·ÛË Ù˘ ıÂڷ›·˜ ÛÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·, Ó·
ÏËÊıÔ‡Ó ˘fi„Ë „˘¯ÔÎÔÈÓˆÓÈÎÔ› ·Ú¿ÁÔÓÙ˜ Î·È Ë
Ù˘¯fiÓ ·ÚÓËÙÈ΋ ›وÛË Ù˘ ıÂڷ›·˜ ÛÙËÓ ÔÈfi-
ÙËÙ· ˙ˆ‹˜ ÙÔ˘ ·È‰ÈÔ‡ Î·È Ù˘ ÔÈÎÔÁ¤ÓÂÈ·˜ ·fi ÙȘ
ηıËÌÂÚÈÓ¤˜ ˘Ô‰fiÚȘ ÂÓ¤ÛÂȘ. ¶·ÚfiÏÔ Ô˘ ÙÔ ¯·-
ÌËÏfi ·Ó¿ÛÙËÌ· ·Ó·Ê¤ÚÂÙ·È fiÙÈ ÌÔÚ› Ó· ÂÈ‚·Ú‡-
ÓÂÈ „˘¯ÔÏÔÁÈο οÔÈ· ·È‰È¿, Ú¤ÂÈ Ó· ÙÔÓÈÛÙ›
fiÙÈ ‰ÂÓ ¤¯ÂÈ ÙÂÎÌËÚȈı› Î·È ‰ÂÓ Â›Ó·È ·fi fiÏÔ˘˜
·Ô‰ÂÎÙ‹ Ë Â˘ÓÔ˚΋ ›‰Ú·ÛË Ù˘ ıÂڷ›·˜ Ì GH
ÛÙÔÓ „˘¯ÈÛÌfi ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ.
∞Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ (GHD)
∏ GHD ÛÙ· ·È‰È¿ ¯·Ú·ÎÙËÚ›˙ÂÙ·È ·fi ÙÔ Û˘Ó-
‰˘·ÛÌfi ÎÏÈÓÈÎÒÓ Î·È ÂÚÁ·ÛÙËÚÈ·ÎÒÓ Â˘ÚËÌ¿ÙˆÓ, Ù·
ÔÔ›· ÌÔÚ› Ó· Û˘Ó˘¿Ú¯Ô˘Ó Û ÌÈÎÚfi ‹ ÌÂÁ¿ÏÔ
‚·ıÌfi ·Ó¿ÏÔÁ· Ì ÙËÓ Ï‹ÚË ‹ ÌÂÚÈ΋ ·Ó¿ÚÎÂÈ·
‹ ÌË ¤ÎÎÚÈÛË ‰Ú·ÛÙÈ΋˜ GH ‹ ÂÏ¿ÙÙˆÛË ·˘ÍËÙÈÎÒÓ
·Ú·ÁfiÓÙˆÓ (IGFs) (7).
∏ ‰È¿ÁÓˆÛË Ù˘ GHD ÛÙËÓ ·È‰È΋ ËÏÈΛ· ›ӷÈ
¤Ó· ‰‡ÛÎÔÏÔ ı¤Ì·, ‰ÈfiÙÈ Ë ¤ÎÎÚÈÛË Ù˘ GH ÛÙ· ·È-
‰È¿ ηχÙÂÈ ¤Ó· Û˘Ó¯¤˜ Ê¿ÛÌ·, ÙÔ ÔÔ›Ô ÂÎÙ›ÓÂ-
Ù·È ·fi Ù· fiÚÈ· ÙÔ˘ Ê˘ÛÈÔÏÔÁÈÎÔ‡ ¤ˆ˜ ÙË Ì¤ÙÚÈ·
·Ó¿ÚÎÂÈ· ¤ÎÎÚÈÛ˘ (ÌÂÌÔӈ̤ÓË GHD) ̤¯ÚÈ ÙË
ÛÔ‚·Ú‹ ·Ó¿ÚÎÂÈ· (fiˆ˜ Û˘Ì‚·›ÓÂÈ Û ÔÏÏ·Ï‹
˘ÔÊ˘Ûȷ΋ ·Ó¿ÚÎÂÈ· ‹ ‰È·Ù·Ú·¯‹ ÙÔ˘ ̆ Ô‰Ô¯¤·
ÙÔ˘ ˘Ôı·Ï·ÌÈÎÔ‡ ÂÎÏ˘ÙÈÎÔ‡ ·Ú¿ÁÔÓÙ·) ‹ Ï‹ÚË
¤ÏÏÂÈ„Ë (·¿ÏÂÈ„Ë ÁÔÓȉ›Ô˘ Ù˘ GH). ™˘Ó‹ıˆ˜, ‰ÂÓ
˘¿Ú¯ÂÈ ‰˘ÛÎÔÏ›· ÛÙËÓ ·Ó·ÁÓÒÚÈÛË Ù˘ ‘ÎÏ·ÛÈ΋˜’,
Ï‹ÚÔ˘˜ GHD, fï˜ Ë ·Ó·ÁÓÒÚÈÛË Ù˘ ÔÌ¿‰·˜ ÙˆÓ
·È‰ÈÒÓ, Ù· ÔÔ›·, ÂÓÒ ·ÚÔ˘ÛÈ¿˙Ô˘Ó ÔÚȷ΋ ‰È·Ù·-
Ú·¯‹ ÛÙËÓ ¤ÎÎÚÈÛË Ù˘ GH, ı· ˆÊÂÏËıÔ‡Ó ·fi
ÙË ¯ÔÚ‹ÁËÛ‹ Ù˘, ·Ú·Ì¤ÓÂÈ ÌÈ· ÚfiÎÏËÛË (8,9).
¶ÚfiÛÊ·Ù·, ηıÈÂÚÒıËÎ·Ó ÎÏÈÓÈο Î·È ·˘ÍÔÏÔÁÈο
‰ÈÂıÓ‹ ‰È·ÁÓˆÛÙÈο ÎÚÈÙ‹ÚÈ· ÁÈ· ÙË GHD, Ù· ÔÔ›·
‚·Û›˙ÔÓÙ·È Û ·ÍÈÔÏfiÁËÛË Ù˘ ·‡ÍËÛ˘, ηıÒ˜ ηÈ
ÙÔ˘ ¿ÍÔÓ· GH-IGF. ∆· ÎÏÈÓÈο Î·È ·˘ÍÔÏÔÁÈο ÎÚÈ-
Ù‹ÚÈ· ¤ÏÏÂȄ˘ GH ·Ó·Ê¤ÚÔÓÙ·È ÛÙÔÓ ¶›Ó·Î· 1.
∏ GH ÂÎÎÚ›ÓÂÙ·È Î·Ù¿ ÒÛÂȘ ÛÙË ‰È¿ÚÎÂÈ· ÙÔ˘
‡ÓÔ˘. ∂Ô̤ӈ˜, Ô ÚÔÛ‰ÈÔÚÈÛÌfi˜ Ù˘ GH ÛÙÔ
Ï¿ÛÌ·, ¯ˆÚ›˜ Ó· ÚÔËÁËı› ‰È¤ÁÂÚÛË, ‰ÂÓ ¤¯ÂÈ ‰È·-
ÁÓˆÛÙÈ΋ ·Í›· Î·È ‰ÂÓ Ú¤ÂÈ Ó· ¯ÚËÛÈÌÔÔÈ›ٷÈ.
°È· ÙË ‰È¿ÁÓˆÛË Ù˘ GHD ··ÈÙÂ›Ù·È Ì¤ÁÈÛÙË ·ÓÙ·-
fiÎÚÈÛË GH (peak) οو ·fi Ù· fiÚÈ· ÙÔ˘ Ê˘ÛÈÔÏÔ-
ÁÈÎÔ‡ (GH <10 ng/ml) Û ‰‡Ô ÙÔ˘Ï¿¯ÈÛÙÔÓ ‰ÔÎÈÌ·-
ۛ˜ ‰È¤ÁÂÚÛ˘. ™ÎÔfi˜ ÙˆÓ ‰ÔÎÈÌ·ÛÈÒÓ Â›Ó·È Ó·
¶›Ó·Î·˜ 1. ∫ÏÈÓÈο Î·È ·˘ÍÔÏÔÁÈο ÎÚÈÙ‹ÚÈ· GHD
ñ ™ËÌ·ÓÙÈÎÔ‡ ‚·ıÌÔ‡ ηı˘ÛÙ¤ÚËÛË ‡„Ô˘˜ (<3 SD)ñ ⁄„Ô˜ <1,5 SD οو ·fi ÙÔ ‡„Ô˜-ÛÙfi¯Ôñ ⁄„Ô˜ <-2 SD Î·È Ú˘ıÌfi˜ ·Ó¿Ù˘Í˘ <1 SD οو ·fi ÙÔ
̤ÛÔ fiÚÔ ÙÔÓ ÚÔËÁÔ‡ÌÂÓÔ ¯ÚfiÓÔ (‹ -0,5 SD ÁÈ· ·È‰È¿Î¿Ùˆ ÙˆÓ 2 ÂÙÒÓ)
ñ ™Â ·È‰È¿ Ê˘ÛÈÔÏÔÁÈÎÔ‡ ‡„Ô˘˜, ÙÒÛË Ú˘ıÌÔ‡ ·Ó¿Ù˘Í˘<1,5 SD › 2 ¯ÚfiÓÈ·
ñ ™ËÌ›· ÂÓ‰ÔÎÚ·Óȷ΋˜ ‚Ï¿‚˘ ‹ ÔÏÏ·Ï‹˜ ˘ÔÊ˘Ûȷ΋˜·Ó¿ÚÎÂÈ·˜
ñ ™˘ÌÙÒÌ·Ù· Î·È ÛËÌ›· ¤ÏÏÂȄ˘ GH ÛÙÔ ÓÂÔÁÓfi (˘ÔÁÏ˘Î·ÈÌ›·, ÌÈÎÚfi ¤Ô˜)
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·124

125∂Ӊ›ÍÂȘ ¯ÔÚ‹ÁËÛ˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
¶·È‰È·ÙÚÈ΋ 2008;71:123-127
Û˘ÌÏËÚÒÛÔ˘Ó ÙËÓ ÎÏÈÓÈ΋ ˘Ô„›· Ù˘ GHD Û ٤-
ÙÔÈÔ ‚·ıÌfi, ÒÛÙ ӷ ÌÂȈıÔ‡Ó ÛÙÔ ÂÏ¿¯ÈÛÙÔ „¢‰Ò˜
ıÂÙÈΤ˜ ‹ „¢‰Ò˜ ·ÚÓËÙÈΤ˜ ‰È·ÁÓÒÛÂȘ (10). √
ÚÔÛ‰ÈÔÚÈÛÌfi˜ ÙÔ˘ IGF-1, Â¿Ó ¤¯Ô˘Ó ·ÔÎÏÂÈÛı›
¿ÏϘ ·Èٛ˜ (Ë·ÙÔ¿ıÂÈ·, ¯ÚfiÓÈ· ·Ó·ÈÌ›·, Î.Ï.),
‚ÔËı¿ ÛÙË ‰È¿ÁÓˆÛË Û ·È‰› Ì ÈÛÙÔÚÈÎfi Î·È Î·-
̇ÏË ·Ó¿Ù˘Í˘ Ô˘ ı¤ÙÔ˘Ó ÙËÓ ˘Ô„›· GHD.
¶ÚÔËÁÔ˘Ì¤Óˆ˜, Ú¤ÂÈ Ó· ·ÔÎÏÂÈÛıÔ‡Ó Î·Ù·ÛÙ¿-
ÛÂȘ, fiˆ˜ Ô ˘Ôı˘ÚÂÔÂȉÈÛÌfi˜, ¯ÚfiÓÈ· Û˘ÛÙËÌ·ÙÈ-
ο ÓÔÛ‹Ì·Ù·, ÙÔ Û‡Ó‰ÚÔÌÔ Turner Î·È ÛÎÂÏÂÙÈΤ˜
·ÓˆÌ·Ï›Â˜. ™ÙË ‰ÈÂÚ‡ÓËÛË Ù˘ GHD ÛÙ· ·È‰È¿
ÌÔÚ› ›Û˘ Ó· ‚ÔËı‹ÛÂÈ Ë Ì·ÁÓËÙÈ΋ ÙÔÌÔÁÚ·-
Ê›· Ù˘ ˘fiÊ˘Û˘, Ì ÙËÓ ÔÔ›· ÌÔÚ› Ó· ‰È·ÁÓˆ-
Ûı› Ë ˘ÔÏ·Û›· ÙÔ˘ ÚÔÛı›Ô˘ ÏÔ‚Ô‡ Ù˘ ˘fiÊ˘-
Û˘, Ë ÂÎÙÔ›· ÙÔ˘ ÔÈÛı›Ô˘ ÏÔ‚Ô‡, Ë ·ÁÂÓÂÛ›· ÙÔ˘
Ì›Û¯Ô˘, ηıÒ˜ Î·È ¿ÏϘ ·ıÔÏÔÁÈΤ˜ ηٷÛÙ¿ÛÂȘ.
∏ ·ÍÈÔÈÛÙ›· ÙˆÓ Ê·ÚÌ·ÎÔÏÔÁÈÎÒÓ ‰ÔÎÈÌ·ÛÈÒÓ
‰È¤ÁÂÚÛ˘ ÁÈ· ÙÔÓ ¤ÏÂÁ¯Ô ¤ÎÎÚÈÛ˘ GH ¤¯ÂÈ ·ÌÊÈ-
Û‚ËÙËı› ·fi ÔÏÏÔ‡˜ ÂÚ¢ÓËÙ¤˜ (11). ™ÙȘ ·Ó·-
ÛÎÔ‹ÛÂȘ ÔÏ˘ÎÂÓÙÚÈÎÒÓ ÌÂÏÂÙÒÓ Ì ÌÂÁ¿ÏÔ ·ÚÈı-
Ìfi ·ÛıÂÓÒÓ, ÛÙÔ˘˜ ÔÔ›Ô˘˜ ¯ÔÚËÁ‹ıËΠıÂڷ›·
Ì GH, ·Ó·Ê¤ÚÂÙ·È fiÙÈ Ú¤ÂÈ Ó· ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È
Ôχ Ï›Á˜ ·ÍÈfiÈÛÙ˜ ‰ÔÎÈ̷ۛ˜ ‰È¤ÁÂÚÛ˘ Î·È Ó·
Á›ÓÂÈ ÚÔÛ¿ıÂÈ· Ó· ηıÔÚÈÛıÔ‡Ó Ê˘ÛÈÔÏÔÁÈΤ˜ ÙÈ-
̤˜ ÁÈ· ÙȘ ‰È¿ÊÔÚ˜ ËÏÈ˘ (12,13).
H ÂÙ·ÈÚ›· ¤Ú¢ӷ˜ GH (Growth Hormone
Research Society) ¤¯ÂÈ ÂΉÒÛÂÈ Î·Ù¢ı˘ÓÙ‹ÚȘ Ô‰Ë-
Á›Â˜ ÁÈ· ÙË ‰È¿ÁÓˆÛË Î·È ÙË ıÂڷ›· Ù˘ GHD ÛÙ·
·È‰È¿ (14). ŒÓ· ÌÂÁ¿ÏÔ ÔÛÔÛÙfi ÙˆÓ ·È‰ÔÂÓ‰Ô-
ÎÚÈÓÔÏfiÁˆÓ ·ÎÔÏÔ˘ı› ·˘Ù¤˜ ÙȘ Ô‰ËÁ›Â˜, ·ÚfiÙÈ
˘¿Ú¯Ô˘Ó ·ÚÎÂÙ¤˜ ·ÔÎÏ›ÛÂȘ ÛÙȘ ‰È¿ÊÔÚ˜ Â˘Úˆ-
·˚Τ˜ ¯ÒÚ˜ (15,16).
∏ ıÂڷ›· Ì G∏ Ô‰ËÁ› Û ÂÈÙ¿¯˘ÓÛË ÙÔ˘
Ú˘ıÌÔ‡ ·‡ÍËÛ˘ ηÈ, Â¿Ó Ë ıÂڷ›· ·Ú¯›ÛÂÈ ÂÁη›-
Úˆ˜, Û ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ÂÓÙfi˜ ÙˆÓ Ê˘ÛÈÔÏÔÁÈÎÒÓ
ÔÚ›ˆÓ. ÃÚÂÈ¿˙ÂÙ·È ÚÔԉ¢ÙÈ΋ ·‡ÍËÛË Ù˘ ‰fiÛ˘
Ì ÙËÓ ËÏÈΛ·, ÒÛÙ ÙÔ ·È‰› Ó· ‚Ú›ÛÎÂÙ·È ÛÙ· Ê˘-
ÛÈÔÏÔÁÈο fiÚÈ· Ù˘ η̇Ï˘ ·‡ÍËÛ˘ Î·È Ó· ÂÈÙ‡-
¯ÂÈ ÙÔ ÁÂÓÂÙÈÎÒ˜ ·Ó·ÌÂÓfiÌÂÓÔ ·Ó¿ÛÙËÌ·. ∏ ıÂÚ·-
›· Ì GH, ¤Ú· ·fi ÙÔ ‡„Ô˜, ¤¯ÂÈ Â˘ÂÚÁÂÙÈ΋ ›-
‰Ú·ÛË ÛÙË ÛˆÌ·ÙÈ΋ Û‡ÛÙ·ÛË (body composition),
ÂÏ·ÙÙÒÓÔÓÙ·˜ ÙÔ ÏÈÒ‰Ë ÈÛÙfi, ·˘Í¿ÓÔÓÙ·˜ ÙË Ì˘˚΋
Ì¿˙· Î·È ·˘Í¿ÓÔÓÙ·˜ ÙËÓ ÔÛÙÈ΋ ˘ÎÓfiÙËÙ·. Œ¯ÂÈ
›Û˘ ¢ÂÚÁÂÙÈΤ˜ ÌÂÙ·‚ÔÏÈΤ˜ ÂȉڿÛÂȘ: ÌÂÈÒ-
ÓÂÈ ÙÔ ÏfiÁÔ Ù˘ ÔÏÈ΋˜ ¯ÔÏËÛÙÂÚfiÏ˘ ÚÔ˜ ÙËÓ
HDL-¯ÔÏËÛÙÂÚfiÏË Î·È ‚ÂÏÙÈÒÓÂÈ ÙËÓ ·ÓÙ›ÛÙ·ÛË
ÛÙËÓ ÈÓÛÔ˘Ï›ÓË. ∏ ‰fiÛË Ù˘ ıÂڷ›·˜ Î˘Ì·›ÓÂÙ·È
·fi 0,15 ¤ˆ˜ 0,30 mg/Kg/‚‰ÔÌ¿‰·, Û ηıËÌÂÚÈÓ¤˜
˘Ô‰fiÚȘ ÂÓ¤ÛÂȘ.
¶·ÚfiÏÔ Ô˘ Ë ıÂڷ›· Ì GH Ô‰ËÁ› Û ·‡ÍË-
ÛË ÙÔ˘ IGF-1, ÙÔ ÔÔ›Ô ¤¯ÂÈ ÌÈÙÔÁfiÓÔ ‰Ú¿ÛË, ‰ÂÓ
¤¯ÂÈ ·Ú·ÙËÚËı› ·˘ÍË̤ÓÔ˜ ΛӉ˘ÓÔ˜ ÁÈ· ·Ó¿Ù˘-
ÍË Î·ÎÔ‹ıÂÈ·˜ ÛÙ· ·È‰È¿ Ô˘ ·›ÚÓÔ˘Ó ÙË ıÂÚ·-
›· (17). Œ¯Ô˘Ó ·Ó·ÊÂÚı› Û¿ÓÈ· ηÏÔ‹ı˘ ÂÓ‰Ô-
ÎÚ·Óȷ΋ ˘¤ÚÙ·ÛË, ÂÚÈÊÂÚÈÎfi Ô›‰ËÌ·, ÂÈÊ˘ÛÈÔ-
Ï›ÛıËÛË Ù˘ ÎÂÊ·Ï‹˜ ÙÔ˘ ÌËÚÈ·›Ô˘, Âȉ›ӈÛË Ù˘
ÛÎÔÏ›ˆÛ˘ Î·È Á˘Ó·ÈÎÔÌ·ÛÙ›· (17).
™‡Ó‰ÚÔÌÔ Turner
∏ Û˘¯ÓfiÙËÙ· ÙÔ˘ Û˘Ó‰ÚfiÌÔ˘ Â›Ó·È 1/2.500 -
1/3.000 ÁÂÓÓ‹ÛÂȘ ÎÔÚÈÙÛÈÒÓ (1). T· ÎÔÚ›ÙÛÈ· ·˘Ù¿,
·Ú¿ ÙË Ê˘ÛÈÔÏÔÁÈ΋ ÂÓ‰ÔÁÂÓ‹ ¤ÎÎÚÈÛË GH, ·ÚÔ˘-
ÛÈ¿˙Ô˘Ó ¯·ÌËÏfi ·Ó¿ÛÙËÌ·, Ë ·ÈÙÈÔÏÔÁ›· ÙÔ˘ ÔÔ›Ô˘
Â›Ó·È Èı·ÓfiÓ ÔÏ˘·Ú·ÁÔÓÙÈ΋. ¢È¿ÊÔÚÔÈ Ì˯·ÓÈ-
ÛÌÔ› ¤¯Ô˘Ó ÂÓÔ¯ÔÔÈËı›, fiˆ˜: ÂÏ·Ùو̤ÓË ‚ÈÔ‰Ú·-
ÛÙÈÎfiÙËÙ· Ù˘ GH, ‰È·Ù·Ú·¯¤˜ ÙÔ˘ ¿ÍÔÓ· IGF, ÌÔÓÔ-
ۈ̛· ÙÔ˘ Ã-¯ÚˆÌÔÛÒÌ·ÙÔ˜ (·Ô˘Û›· ÙÔ˘ ÁÔÓȉ›Ô˘
SHOX, Ô˘ ηıÔÚ›˙ÂÈ ÙÔ ·Ó¿ÛÙËÌ· Î·È ‚Ú›ÛÎÂÙ·È ÛÙÔ
‚Ú·¯‡ ÛΤÏÔ˜ ÙÔ˘ ¯ÚˆÌÔÛÒÌ·ÙÔ˜ Ã) Î·È Èı·ÓfiÓ Î·È
Ë Ï‹Ú˘ ·Ó¿ÚÎÂÈ· ÔÈÛÙÚÔÁfiÓˆÓ Î·Ù¿ ÙËÓ ·È‰È΋
Î·È ÂÊË‚È΋ ËÏÈΛ· (1,18). ∂Âȉ‹ ‰ÂÓ ˘¿Ú¯ÂÈ GHD,
‰ÂÓ ¯ÚÂÈ¿˙ÂÙ·È ÔÈ ·ÛıÂÓ›˜ Ó· ˘Ô‚¿ÏÏÔÓÙ·È Û ‰ÔÎÈ-
̷ۛ˜ ‰È¤ÁÂÚÛ˘ ÚÈÓ ·fi ÙË ¯ÔÚ‹ÁËÛË G∏. ∆Ô
‡„Ô˜ ÙˆÓ ·ÛıÂÓÒÓ Ì ۇӉÚÔÌÔ Turner Ú¤ÂÈ Ó·
ÚÔ‚¿ÏÏÂÙ·È ÛÙ· ÂȉÈο ‰È·ÁÚ¿ÌÌ·Ù· ·‡ÍËÛ˘ (19).
∏ ¯ÔÚ‹ÁËÛË GH Û ·È‰È¿ Ô˘ ¿Ú¯ÈÛ·Ó ÙË ıÂÚ·-
›· ÛÙËÓ ËÏÈΛ· ÙˆÓ 7-13 ÂÙÒÓ Ô‰ËÁ› Û ‚ÂÏÙ›ˆÛË
ÙÔ˘ Ú˘ıÌÔ‡ ·‡ÍËÛ˘ Î·È ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜
·fi 3 ¤ˆ˜ 12 cm (1,20,21). H ·ÓÙ·fiÎÚÈÛË ÛÙË ıÂÚ·-
›· Ì GH, fiÛÔÓ ·ÊÔÚ¿ ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·, ›ӷÈ
ηχÙÂÚË fiÛÔ ÓˆÚ›ÙÂÚ· ·Ú¯›˙ÂÈ Ë ıÂڷ›· (20,22).
∏ ıÂڷ›· Ì GH Á›ÓÂÙ·È Û˘Ó‹ıˆ˜ Ôχ ηϿ ·ÓÂ-
ÎÙ‹, Ë Î·ÏÔ‹ı˘ ÂÓ‰ÔÎÚ¿ÓÈ· ˘¤ÚÙ·ÛË Î·È Ë ‹È·
·ÓÙ›ÛÙ·ÛË ÛÙËÓ ÈÓÛÔ˘Ï›ÓË Ô˘ ÌÔÚ› Ó· ÂÌÊ·ÓÈ-
ÛÙÔ‡Ó Â›Ó·È ·Ó·ÛÙÚ¤„È̘, ·ÏÏ¿ Ë ÂÌÊ¿ÓÈÛË Ì¤Û˘
ˆÙ›Ùȉ·˜ Î·È Ë ·Ó¿ÁÎË ¯ÂÈÚÔ˘ÚÁÈ΋˜ ¤̂·Û˘ (ÛÙ·
·˘ÙÈ¿, ÙË Ì‡ÙË Î·È ÙÔ Ï¿Ú˘ÁÁ·) ·Ó·Ê¤ÚÂÙ·È Û˘¯ÓfiÙÂ-
ÚË ÛÙ· ·È‰È¿ Ô˘ ¤Ï·‚·Ó ıÂڷ›· Ì GH (1,20). √È
Ì·ÎÚÔÚfiıÂÛ̘ ÂÈÙÒÛÂȘ Ù˘ ıÂڷ›·˜ Ì G∏,
fiÛÔÓ ·ÊÔÚ¿ ÙÔ Î·Ú‰È·ÁÁÂÈ·Îfi Û‡ÛÙËÌ· Î·È ÙÔ ÌÂÙ¤-
ÂÈÙ· ΛӉ˘ÓÔ ÂÌÊ¿ÓÈÛ˘ ‰È·‚‹ÙË Ù‡Ô˘ 2 Û ÎÔÚ›-
ÙÛÈ· Ì ۇӉÚÔÌÔ Turner, ‰ÂÓ Â›Ó·È ·ÎfiÌ· Ï‹Úˆ˜
ÁÓˆÛÙ¤˜ (1). ÃÚÂÈ¿˙ÂÙ·È Ó· Á›ÓÔ˘Ó ÂÚÈÛÛfiÙÂÚ˜ Ì·-
ÎÚÔÚfiıÂÛ̘ ÌÂϤÙ˜, Ì ÌÂÁ¿ÏÔ ·ÚÈıÌfi ·ÛıÂÓÒÓ,
ÁÈ· Ó· ÂÍ·¯ıÔ‡Ó ÔÚÈÛÙÈο Û˘ÌÂÚ¿ÛÌ·Ù·.
∏ ÂÈÎÚ·ÙÔ‡Û· ¿Ô„Ë Â›Ó·È Ó· ¯ÔÚËÁÂ›Ù·È G∏
Û οı ·È‰› Ì ۇӉÚÔÌÔ Turner (1). ∏ Û˘Ó‹ı˘
‰fiÛË Â›Ó·È 0,30-0,35 mg/Kg/‚‰ÔÌ¿‰·. ∏ ıÂڷ›·
Û˘Ó‰˘¿˙ÂÙ·È Ì ÙË ¯ÔÚ‹ÁËÛË ÔÈÛÙÚÔÁfiÓˆÓ ÌÂÙ¿ ÙËÓ
ËÏÈΛ· ÙˆÓ 12 ÂÙÒÓ.
ÃÚfiÓÈ· ÓÂÊÚÈ΋ ·Ó¿ÚÎÂÈ· (á∞)
∆Ô ¯·ÌËÏfi ·Ó¿ÛÙËÌ· ·ÔÙÂÏ› ÛÔ‚·Úfi Úfi-
‚ÏËÌ· ÛÙ· ·È‰È¿ Ì á∞. H ·ÈÙÈÔÏÔÁ›· ÙÔ˘ ¯·ÌË-
ÏÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜ Â›Ó·È ÔÏ˘·Ú·ÁÔÓÙÈ΋ Î·È ·ÊÔ-
Ú¿ ÙfiÛÔ ‰È·Ù·Ú·¯¤˜ ÛÙÔÓ ¿ÍÔÓ· GH-πGF-1, fiÛÔ Î·È
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·125

126 E. ∫Ô‡ÛÙ· Î·È Û˘Ó.
Paediatriki 2008;71:123-127
ÌÂÙ·‚ÔÏÈΤ˜ ‰È·Ù·Ú·¯¤˜ Î·È ‰È·Ù·Ú·¯¤˜ Ù˘ ıÚ¤„˘
(23,24). ∂Âȉ‹ ‰ÂÓ ˘¿Ú¯ÂÈ ·Ó¿ÚÎÂÈ·, ·ÏÏ¿ ·ÓÙ›-
ÛÙ·ÛË ÛÙË ‰Ú¿ÛË Ù˘ GH, ‰ÂÓ ¯ÚÂÈ¿˙ÂÙ·È ÔÈ ·ÛıÂÓ›˜
Ó· ˘Ô‚¿ÏÏÔÓÙ·È Û ‰ÔÎÈ̷ۛ˜ ‰È¤ÁÂÚÛ˘ ÚÈÓ ·fi
ÙË ¯ÔÚ‹ÁËÛË G∏. ∏ ıÂڷ›· Ì GH, Â¿Ó ‰Ôı› Óˆ-
Ú›˜, ÂÈÙ·¯‡ÓÂÈ ÙÔ Ú˘ıÌfi ·‡ÍËÛ˘ Î·È ‚ÂÏÙÈÒÓÂÈ ÙÔ
ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·, ¯ˆÚ›˜ Ó· ˘¿Ú¯Ô˘Ó ÛËÌ·ÓÙÈΤ˜
·ÚÂÓ¤ÚÁÂȘ (2,23,24). ∏ ıÂڷ›· ¤¯ÂÈ ÂÁÎÚÈı›
·fi ÙÔ 1996 Î·È ̄ ÔÚËÁÂ›Ù·È Û ·ÛıÂÓ›˜ Ì á∞ ÚÔ-
ÂÊË‚È΋˜ ËÏÈΛ·˜ ÚÔÙÂÏÈÎÔ‡ Î·È ÙÂÏÈÎÔ‡ ÛÙ·‰›Ô˘.
∏ ıÂڷ›· Ú¤ÂÈ Ó· ·Ú¯›˙ÂÈ Û fiÛÔ ‰˘Ó·ÙfiÓ ÌÈ-
ÎÚfiÙÂÚË ËÏÈΛ·, ÂÊfiÛÔÓ Ô Ú˘ıÌfi˜ ·‡ÍËÛ˘ ÂÌÊ·Ó›-
˙ÂÈ ÙÒÛË, Ë ÔÔ›· ‰ÂÓ ÔÊ›ÏÂÙ·È Û ·Ó·Ú΋ ıÚ¤-
„Ë ‹ ÌÂÙ·‚ÔÏÈΤ˜ ‰È·Ù·Ú·¯¤˜. ∏ ‰fiÛË Ù˘ GH ÛÙË
á∞ Â›Ó·È 0,35 mg/Kg/‚‰ÔÌ¿‰·.
™‡Ó‰ÚÔÌÔ Prader-Willi
¶ÚfiÎÂÈÙ·È ÁÈ· Û¿ÓÈÔ ÁÂÓÂÙÈÎfi Û‡Ó‰ÚÔÌÔ (Û˘-
¯ÓfiÙËÙ· 1/10.000-15.000), ÙÔ ÔÔ›Ô ÔÊ›ÏÂÙ·È ÛÙËÓ
·ÒÏÂÈ· Ù˘ ÁÔÓȉȷ΋˜ ¤ÎÊÚ·Û˘ Ù˘ ÂÚÈÔ¯‹˜
15q11-q13 ÙÔ˘ ·ÙÚÈÎÔ‡ ·ÏÏËÏfiÌÔÚÊÔ˘ ·ÔÙ˘ˆ-
̤ÓÔ˘ ÁÔÓȉ›Ô˘ (imprinted gene) Î·È ¯·Ú·ÎÙËÚ›˙ÂÙ·È
·fi ˘ÂÚÊ·Á›·, ·¯˘Û·ÚΛ·, ˘ÔÁÔÓ·‰ÈÛÌfi, ¯·ÌË-
Ïfi ·Ó¿ÛÙËÌ· Î·È GHD ÔÊÂÈÏfiÌÂÓË Û ˘Ôı·Ï·ÌÈ΋
‰È·Ù·Ú·¯‹ (3,25). ∏ ıÂڷ›· Ì GH ÂÈÙ·¯‡ÓÂÈ ÙÔ
Ú˘ıÌfi ·‡ÍËÛ˘, ‚ÂÏÙÈÒÓÂÈ ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ηÈ
¤¯ÂÈ È‰È·›ÙÂÚ· ¢ÂÚÁÂÙÈ΋ ›‰Ú·ÛË ÛÙË ÛˆÌ·ÙÈ΋
Û‡ÛÙ·ÛË, ÂÏ·ÙÙÒÓÔÓÙ·˜ ÙÔ ÏÈÒ‰Ë ÈÛÙfi Î·È ·˘Í¿ÓÔ-
ÓÙ·˜ ÙË Ì˘˚΋ Ì¿˙· (3,25). ∏ Û˘ÓÈÛÙÒÌÂÓË ‰fiÛË Â›-
Ó·È 0,25 mg/Kg/‚‰ÔÌ¿‰·. ¶ÚfiÛÊ·Ù· ·Ó·Ê¤ÚıËηÓ
·ÈÊÓ›‰ÈÔÈ ı¿Ó·ÙÔÈ, ΢ڛˆ˜ ·fi ÏÔÈÌÒÍÂȘ ÙÔ˘ ·Ó·-
Ó¢ÛÙÈÎÔ‡ Î·È ˘Ô·ÂÚÈÛÌfi Û ·È‰È¿ Ì ÙÔ Û‡Ó-
‰ÚÔÌÔ, Ù· ÔÔ›· ÂÏ¿Ì‚·Ó·Ó ıÂڷ›· Ì GHØ ·Úfi-
ÏÔ Ô˘ ‰ÂÓ ¤¯ÂÈ ·Ô‰Âȯı› Ë Û˘Û¯¤ÙÈÛË Ù˘ ıÂÚ·-
›·˜ Ì GH, ¯ÚÂÈ¿˙ÂÙ·È Ó· Á›ÓÂÙ·È ÚÔÛÂÎÙÈÎfi˜
ˆÙÔÚÈÓÔÏ·Ú˘ÁÁÔÏÔÁÈÎfi˜ Î·È ·Ó·Ó¢ÛÙÈÎfi˜ ¤ÏÂÁ¯Ô˜
ÚÈÓ ·fi ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ (26).
ÕÏϘ ÂÚÈÙÒÛÂȘ ÛÙȘ Ôԛ˜ ¯ÔÚËÁÂ›Ù·È GH
Û ·È‰È¿, ÔÈ Ôԛ˜ fï˜ ‰ÂÓ ¤¯Ô˘Ó ¿ÚÂÈ
¤ÁÎÚÈÛË ÛÙË ¯ÒÚ· Ì·˜
¶·È‰È¿ Ô˘ ÁÂÓÓÈÔ‡ÓÙ·È ÌÈÎÚfiۈ̷ ÁÈ· ÙËÓ ËÏÈΛ·
·ËÛ˘ (Small for Gestational Age, SGA)
¶ÂÚ›Ô˘ 10% ÙˆÓ ·È‰ÈÒÓ Ì SGA (‚¿ÚÔ˜ ‹/ηÈ
Ì‹ÎÔ˜ <2 SD) ‰ÂÓ ÂÌÊ·Ó›˙Ô˘Ó ÂÈÙ¿¯˘ÓÛË ÙÔ˘ Ú˘ı-
ÌÔ‡ ·‡ÍËÛ˘ ηٿ ÙË ‰È¿ÚÎÂÈ· ÙˆÓ 2 ÚÒÙˆÓ ÂÙÒÓ
Ù˘ ˙ˆ‹˜, Ì ·ÔÙ¤ÏÂÛÌ· ¯·ÌËÏfi ·Ó¿ÛÙËÌ· ÛÙËÓ
·È‰È΋ ËÏÈΛ· Î·È ¯·ÌËÏfi ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· (ÂÚ›-
Ô˘ 1 SD οو ÙÔ˘ ̤ÛÔ˘ fiÚÔ˘) (27). ™Â ·È‰È¿ 2-4
ÂÙÒÓ Ì SGA, Ù· ÔÔ›· ‰ÂÓ ÂÌÊ·Ó›˙Ô˘Ó ÂÈÙ¿¯˘ÓÛË
ÙÔ˘ Ú˘ıÌÔ‡ ·‡ÍËÛ˘ Î·È ¤¯Ô˘Ó ‡„Ô˜ <-2,5 SD (‹ ÛÂ
·È‰È¿ Ì SGA ÌÂÁ·Ï‡ÙÂÚ· ÙˆÓ 4 ÂÙÒÓ Ì ‡„Ô˜ <-2
SD), Û˘ÓÈÛÙ¿Ù·È Ó· Ï·Ì‚¿ÓÔ˘Ó ıÂڷ›· Ì GH
(27). ∏ ¯ÔÚ‹ÁËÛË GH ‚ÂÏÙÈÒÓÂÈ ÙÔ Ú˘ıÌfi ·‡ÍËÛ˘
Î·È ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ·˘ÙÒÓ ÙˆÓ ·ÛıÂÓÒÓ (4). §fi-
Áˆ ÙˆÓ Â˘ÓÔ˚ÎÒÓ ·ÔÙÂÏÂÛÌ¿ÙˆÓ ÙˆÓ ÎÏÈÓÈÎÒÓ ÌÂ-
ÏÂÙÒÓ ˆ˜ ÚÔ˜ ÙËÓ ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ· Ù˘ ıÂÚ·-
›·˜, ·Ó Î·È Û ÂÚÈÔÚÈṲ̂ÓÔ ·ÚÈıÌfi ·ÛıÂÓÒÓ, ¤¯ÂÈ
‹‰Ë ÂÁÎÚÈı› Ë ıÂڷ›· Û ·˘Ù¿ Ù· ·È‰È¿ Û ∞ÌÂ-
ÚÈ΋ Î·È ∂˘ÚÒË Î·È ÛÙËÓ ∂ÏÏ¿‰· ¤¯ÂÈ ÂÁÎÚÈı› ·fi
ÙÔÓ ∂√º Î·È ÙÔ ∫∂™À Î·È ‚Ú›ÛÎÂÙ·È ÛÙÔ ÙÂÏÈÎfi ÛÙ¿-
‰ÈÔ ̆ ÔÁÚ·Ê‹˜. √È Ì·ÎÚÔÚfiıÂÛ̘, fï˜, ÌÂÙ·‚Ô-
ÏÈΤ˜ ÂÈÙÒÛÂȘ Ù˘ ıÂڷ›·˜ Ì GH, fiÛÔÓ ·ÊÔÚ¿
ÙËÓ ·ÓÙ›ÛÙ·ÛË ÛÙËÓ ÈÓÛÔ˘Ï›ÓË Î·È ÙËÓ ˘ÂÚÈÓÛÔ˘ÏÈ-
Ó·ÈÌ›· Û ·˘Ù¿ Ù· ·È‰È¿, Â›Ó·È ·ÎfiÌË ̆ fi ÌÂϤÙË. ∏
Û˘ÓÈÛÙÒÌÂÓË ‰fiÛË Â›Ó·È 0,25 mg/Kg/‚‰ÔÌ¿‰·.
¶·È‰È¿ Ì ȉÈÔ·ı¤˜ ̄ ·ÌËÏfi ·Ó¿ÛÙËÌ·
(Idiopathic Short Stature, ISS)
T· ·È‰È¿ Ì ȉÈÔ·ı¤˜ ¯·ÌËÏfi ·Ó¿ÛÙËÌ· (<2,25
SD) Â›Ó·È ÌÈ· ÂÙÂÚÔÁÂÓ‹˜ ÔÌ¿‰·, Ù· ÂÚÈÛÛfiÙÂÚ·
·fi ·˘Ù¿ (·ÏÏ¿ fi¯È fiÏ·) ‰ÂÓ ÊÙ¿ÓÔ˘Ó ÛÙÔ Ê˘ÛÈÔÏÔ-
ÁÈÎfi ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·. ∏ ıÂڷ›· Ì GH ÁÈ· ·ÚÎÂ-
Ù¿ ¯ÚfiÓÈ· ·Ó·Ê¤ÚÂÙ·È fiÙÈ ÂÈÙ·¯‡ÓÂÈ ÙÔ Ú˘ıÌfi ·‡-
ÍËÛ˘, Â¿Ó ‰Ôı› ÓˆÚ›˜, ȉ›ˆ˜ ÛÙËÓ ·Ú¯‹ Ù˘ ıÂÚ·-
›·˜ Î·È ‚ÂÏÙÈÒÓÂÈ ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ηٿ 4-7
cm, Û οÔȘ, ·ÏÏ¿ fi¯È Û fiϘ ÙȘ ÌÂϤÙ˜ (5). T·
̤¯ÚÈ Û‹ÌÂÚ· ·ÔÙÂϤÛÌ·Ù·, ·ÚfiÙÈ ‰Â›¯ÓÔ˘Ó fiÙÈ Ë
ıÂڷ›· Ì GH Â›Ó·È ·ÛÊ·Ï‹˜ ÛÙ· ·È‰È¿ ·˘Ù¿, ›-
Ó·È ·ÓÙÈÎÚÔ˘fiÌÂÓ· (5). ™ÙȘ ∏¶∞ ¤¯ÂÈ ‰Ôı› ¤ÁÎÚÈÛË
ÌfiÓÔ Û ¤Ó· Û··ÛÌ·. ¶ÚÔ˜ ÙÔ ·ÚfiÓ, Ë ¯ÔÚ‹ÁËÛË
GH ÛÙ· ·È‰È¿ ·˘Ù¿ Â›Ó·È ˘fi ÌÂϤÙË Î·È ı· Ú¤ÂÈ
Ó· Á›ÓÂÙ·È ÛÙ· Ï·›ÛÈ· ÂÚ¢ÓËÙÈÎÒÓ ÚˆÙÔÎfiÏψÓ.
∏ Û˘ÓÈÛÙÒÌÂÓË ‰fiÛË Â›Ó·È 0,30 mg/Kg/‚‰ÔÌ¿‰·.
ÕÏϘ ÂÚÈÙÒÛÂȘ ̄ ÔÚ‹ÁËÛ˘ GH
H GH ¤¯ÂÈ Â›Û˘ ̄ ÔÚËÁËı› Ì ¢ÓÔ˚ο ·ÔÙÂϤ-
ÛÌ·Ù· Û ·È‰È¿ ÌÂ Û˘ÁÁÂÓ‹ ˘ÂÚÏ·Û›· ÂÈÓÂÊÚÈ-
‰›ˆÓ (28) Î·È Û ·È‰È¿ Ì ÈÓÔ΢ÛÙÈ΋ ÓfiÛÔ (29), Ë
¯Ú‹ÛË Ù˘, fï˜, Û ·˘Ù¿ Ù· ·È‰È¿ ·ÎfiÌË ÌÂÏÂٿٷÈ.
GHD Û ÂÓ‹ÏÈΘ
∞ÊÔÚ¿ ÂÚ›Ô˘ 200 ·ÛıÂÓ›˜ ·Ó¿ 1.000.000. ∏
ıÂڷ›· ¯ÔÚËÁÂ›Ù·È Û ·ÛıÂÓ›˜ Ì ÛÔ‚·ÚÔ‡ ‚·ı-
ÌÔ‡ ·Ó¿ÚÎÂÈ·, ‰ËÏ·‰‹ Ì ̤ÁÈÛÙË ·¿ÓÙËÛË GH
ÛÙË ‰ÔÎÈÌ·Û›· ˘ÔÁÏ˘Î·ÈÌ›·˜, ÌÂÙ¿ ·fi ¯ÔÚ‹ÁËÛË
ÈÓÛÔ˘Ï›Ó˘ <3 ng/ml. ∏ ¤ÏÏÂÈ„Ë GH ÛÙÔ˘˜ ÂÓ‹ÏÈΘ
Ô‰ËÁ› Û ÎÂÓÙÚÈ΋ ·¯˘Û·ÚΛ·, ÂÏ·Ùو̤ÓË ¿ÏÈÔ
Ì¿˙· (lean body mass), ÂÏ·Ùو̤ÓË ÔÛÙÈ΋ ˘ÎÓfi-
ÙËÙ·, ·˘ÍË̤ÓË Î·Ú‰È·ÁÁÂȷ΋ ÓÔÛËÚfiÙËÙ· ηÈ
ÂËÚ·Ṳ̂ÓË ÔÈfiÙËÙ· ˙ˆ‹˜, ÂÓÒ Ë ¯ÔÚ‹ÁËÛË GH
‚ÂÏÙÈÒÓÂÈ ÙË ÛˆÌ·ÙÈ΋ Û‡ÛÙ·ÛË Î·È ÙËÓ ÔÈfiÙËÙ·
˙ˆ‹˜ ÛÙÔ˘˜ ÂÚÈÛÛfiÙÂÚÔ˘˜ ·ÛıÂÓ›˜ (30). ∏ ‰fiÛË
ηٿ ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ Î˘Ì·›ÓÂÙ·È ·fi
0,15-0,3 mg/Ë̤ڷ, Ì ÚÔԉ¢ÙÈ΋ ·‡ÍËÛË, Ô˘
ηıÔÚ›˙ÂÙ·È ·fi Ù· ›‰· ÙÔ˘ IGF-1 (30).
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·126

127∂Ӊ›ÍÂȘ ¯ÔÚ‹ÁËÛ˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
¶·È‰È·ÙÚÈ΋ 2008;71:123-127
BÈ‚ÏÈÔÁÚ·Ê›·
1. Sybert VP, McCauley E. Turner's syndrome. N Engl J Med2004;351:1227-1238.
2. Vimalachandra D, Hodson EM, Willis NS, Craig JC, Cow-ell C, Knight JF. Growth hormone for children with chron-ic kidney disease. Cochrane Database Syst Rev 2006;3:CD003264.
3. Burman P, Ritzén EM, Lindgren AC. Endocrine dysfunc-tion in Prader-Willi syndrome: a review with special refer-ence to GH. Endocr Rev 2001;22:787-799.
4. Ong K, Beardsall K, de Zegher F. Growth hormone therapyin short children born small for gestational age. Early HumDev 2005;81:973-980.
5. Cuttler L. Safety and efficacy of growth hormone treatmentfor idiopathic short stature. J Clin Endocrinol Metab 2005;90:5502-5504.
6. Saggese G, Baroncelli GI, Vanacore T, Fiore L, Ruggieri S,Federico G. Indications and strategies for continuing GHtreatment during transition from late adolescence to earlyadulthood in patients with GH deficiency: the impact onbone mass. J Endocrinol Invest 2004;27:596-602.
7. Sizonenko ƒC, Clayton ƒE, Cohen ƒ, Hintz RL. Tanaka T,Laron Z. Diagnosis and management of growth hormonedeficiency in childhood and adolescence. Part 1: diagnosisof growth hormone deficiency. Growth Horm IGF Res2001;11:137-165.
8. Rosenfeld RG, Albertsson-Wikland K, Cassorla F, FrasierSD, Hasegawa Y, Hintz RL, et al. Diagnostic controversy:the diagnosis of childhood growth hormone deficiency re-visited. J Clin Endocrinol Metab 1995;80:1532-1540.
9. Van den Broeck J, Arends N, Hokken-Koelega A. Growthresponse to recombinant human growth hormone (GH) inchildren with idiopathic growth retardation by level ofmaximum GH peak during GH stimulation tests. HormRes 2000;53:267-273.
10. Hindmarsh PC, Swift PG. An assessment of growth hor-mone provocation tests. Arch Dis Child 1995;72:362-368.
11. Gandrud LM, Wilson DM. Is growth hormone stimulationtesting in children still appropriate? Growth Horm IGF Res2004;14:185-194.
12. Carel JC, Tresca JP, Letrait ª, Chaussain JL, Lebouc Y, JobJC, et al. Growth hormone testing for the diagnosis ofgrowth hormone deficiency in childhood: a populationregister-based study. J Clin Endocrinol Metab 1997;82:2117-2121.
13. Ghigo E, Bellone J, Aimaretti G, Bellone S, Loche S, CappaM, et al. Reliability of provocative tests to assess growthhormone secretory status. Study in 472 normally growingchildren. J Clin Endocrinol Metab 1996;81:3323-3327.
14. Growth Hormone Research Society. Consensus guidelinesfor the diagnosis and treatment of growth hormone (GH)deficiency in childhood and adolescence: summary state-ment of the GH Research Society. GH Research Society. JClin Endocrinol Metab 2000;85:3990-3993.
15. Frasier SD. Editorial: the diagnosis and treatment of child-hood and adolescent growth hormone deficiency--consen-sus or confusion? J Clin Endocrinol Metab 2000;85:3988-3989.
16. Juul A, Bernasconi S, Clayton PE, Kiess W, DeMuinck-Keizer Schrama S; Drugs and Therapeutics Committee ofthe European Society for Paediatric Endocrinology(ESPE). European audit of current practice in diagnosisand treatment of childhood growth hormone deficiency.Horm Res 2002;58:233-241.
17. Bowlby DA, Rapaport R. Safety and efficacy of growth hor-mone therapy in childhood. Pediatr Endocrinol Rev 2004;2Suppl 1:68-77.
18. Rao E, Weiss B, Fukami M, Rump A, Niesler B, Mertz A, etal. Pseudoautosomal deletions encompassing a novelhomeobox gene cause growth failure in idiopathic shortstature and Turner syndrome. Nat Genet 1997;16:54-63.
19. Lyon AJ, Preece MA, Grant DB. Growth curve for girlswith Turner syndrome. Arch Dis Child 1985;60:932-935.
20. Stephure DK; Canadian Growth Hormone Advisory Com-mittee. Impact of growth hormone supplementation onadult height in turner syndrome: results of the Canadianrandomized controlled trial. J Clin Endocrinol Metab2005;90:3360-3366.
21. Baxter L, Bryant J, Cave CB, Milne R. Recombinant growthhormone for children and adolescents with Turner syn-drome. Cochrane Database Syst Rev 2007;(1):CD003887.
22. Ranke MB, Lindberg A, Ferrãandez Long ãas A, DarendelilerF, Albertsson-Wikland K, Dunger D, et al. Major determi-nants of height development in Turner syndrome (TS) pa-tients treated with GH: analysis of 987 patients from KIGS.Pediatr Res 2007;61:105-110.
23. Mahan JD, Warady BA; the Consensus Committee. Assess-ment and treatment of short stature in pediatric patientswith chronic kidney disease: a consensus statement. Pedia-tr Nephrol 2006;21:917-930.
24. Stefanidis CJ, Klaus G. Growth of prepubertal children ondialysis. Pediatr Nephrol. 2007;22:1251-1259.
25. Goldstone AP. Prader-Willi syndrome: advances in genet-ics, pathophysiology and treatment. Trends EndocrinolMetab 2004;15:12-20.
26. Eiholzer U. Deaths in children with Prader-Willi syn-drome. A contribution to the debate about the safety ofgrowth hormone treatment in children with PWS. HormRes 2005;63:33-39.
27. Clayton PE, Cianfarani S, Czernichow P, Johannsson G,Rapaport R, Rogol A. Management of the child born smallfor gestational age through to adulthood: a consensusstatement of the International Societies of Pediatric En-docrinology and the Growth Hormone Research Society. JClin Endocrinol Metab 2007;92:804-810.
28. Gallagher MP, Levine LS, Oberfield SE. A review of the ef-fects of therapy on growth and bone mineralization in chil-dren with congenital adrenal hyperplasia. Growth HormIGF Res 2005;15 Suppl A:S26-30.
29. Hardin DS, Ferkol T, Ahn C, Dreimane D, Dyson M,Morse M, et al. A retrospective study of growth hormoneuse in adolescents with cystic fibrosis. Clin Endocrinol(Oxf) 2005;62:560-566.
30. Drake WM, Howell SJ, Monson JP, Shalet SM. Optimizinggh therapy in adults and children. Endocr Rev 2001;22:425-450.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·127

∆ÂÏÈÎfi ·Ó¿ÛÙËÌ· Û ·È‰È¿ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfi-
Ó˘ Ô˘ ¤Ï·‚·Ó ıÂڷ›· ˘ÔηٿÛÙ·Û˘
ª. ¶··‰ÔÔ‡ÏÔ˘1, ™. ¡ÙÔ˘Ì¿2, ∫. ∫›ÙÛÈÔ˜3, ¡. ∫·‰fiÁÏÔ˘3, ∫. ∫ÒÛÙ·1, π. ∆ÛÈÔ‡Ú˘1
¶ÂÚ›ÏË„Ë
∂ÈÛ·ÁˆÁ‹: ™ÎÔfi˜ Ù˘ ÌÂϤÙ˘ ‹Ù·Ó Ë ÂÎÙ›ÌËÛË ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜ Û ·È‰È¿ Ì ·Ó¿ÚÎÂÈ· ·˘-ÍËÙÈ΋˜ ÔÚÌfiÓ˘ (GH) Ô˘ ¤Ï·‚·Ó ıÂڷ›· ˘ÔηٿÛÙ·Û˘ Ì ·Ó·Û˘Ó‰˘·Ṳ̂ÓË GH Î·È Ô ÚÔÛ‰ÈÔ-ÚÈÛÌfi˜ ·Ú·ÁfiÓÙˆÓ Ô˘ Û˘Û¯ÂÙ›˙ÔÓÙ·È Ì ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ: ªÂÏÂÙ‹ıËÎ·Ó 72 ·È‰È¿ (25 ÚÔÂÊË‚Èο) Ì ÌÂÌÔӈ̤ÓË (61/72) ‹ Û˘Ó‰˘·Ṳ̂ÓË(11/72) ·Ó¿ÚÎÂÈ· GH, Ô˘ ‰È·ÁÓÒÛÙËΠÌÂÙ¿ ·fi ÚÔÛ‰ÈÔÚÈÛÌfi Ù˘ GH Ì ‰ÔÎÈ̷ۛ˜ ‰È¤ÁÂÚÛ˘. ∆··È‰È¿ ¤Ï·‚·Ó ıÂڷ›· ˘ÔηٿÛÙ·Û˘ Ì GH sc, 3, 6 ‹ 7 ÊÔÚ¤˜ ‚‰ÔÌ·‰È·›ˆ˜. ¶ÚÔÛ‰ÈÔÚ›ÛÙËΠÁȷοı ·È‰› ÙÔ ‡„Ô˜-ÛÙfi¯Ô˜. ∫·Ù·ÁÚ¿ÊËÎ·Ó Î·Ù¿ ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ Î·È ·ÎÔÏÔ‡ıˆ˜ ·Ó¿ ÂÍ¿ÌË-ÓÔ ÙÔ ‡„Ô˜ Û fiÚıÈ· ı¤ÛË, Ë ÔÛÙÈ΋ ËÏÈΛ·, Ô ÂÙ‹ÛÈÔ˜ Ú˘ıÌfi˜ ·‡ÍËÛ˘ Î·È ÙÔ ÛÙ¿‰ÈÔ ÂÓ‹‚ˆÛ˘.
∞ÔÙÂϤÛÌ·Ù·: ∏ ‰È·ÊÔÚ¿ Ù˘ ̤Û˘ ÛÙ·ıÂÚ‹˜ ·fiÎÏÈÛ˘ ·Ó·ÛÙ‹Ì·ÙÔ˜ ÛÙÔ Ù¤ÏÔ˜ Ù˘ ıÂڷ›·˜ ÛÂÛ¯¤ÛË Ì ٷ ÚÔ ·˘Ù‹˜ ›‰· ‹Ù·Ó 1,3. ™ÙÔ ‡„Ô˜-ÛÙfi¯Ô ¤ÊÙ·Û·Ó 23 ·È‰È¿ (32%). À‹Ú¯Â ÛËÌ·ÓÙÈ-΋ Û˘Û¯¤ÙÈÛË ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜ Ì ÙÔ ·Ú¯ÈÎfi ‡„Ô˜, ÙÔ ‡„Ô˜-ÛÙfi¯Ô Î·È ÙÔÓ ·ÚÈıÌfi ÙˆÓ ÂÓ¤Ûˆӷӿ ‚‰ÔÌ¿‰·, ÂÓÒ ‰ÂÓ ‰È·ÈÛÙÒıËΠÛËÌ·ÓÙÈ΋ Û˘Û¯¤ÙÈÛË Ì ÙËÓ ËÏÈΛ· ¤Ó·Ú͢ Ù˘ ıÂڷ›·˜, ÙˉȿÚÎÂÈ· Ù˘ ıÂڷ›·˜, ÙÔ Ê‡ÏÔ Î·È ÙÔ Ú˘ıÌfi ·‡ÍËÛ˘ ηٿ ÙÔ ÚÒÙÔ ¤ÙÔ˜ Ù˘ ıÂڷ›·˜. ∆· ·È‰È¿ ÌÂÛ˘Ó‰˘·Ṳ̂ÓË ·Ó¿ÚÎÂÈ· ÔÚÌÔÓÒÓ Î¤Ú‰ÈÛ·Ó ÂÚÈÛÛfiÙÂÚÔ ‡„Ô˜ Ì ÙË ıÂڷ›· Û ۯ¤ÛË Ì ÂΛӷ ÌÂÌÂÌÔӈ̤ÓË ·Ó¿ÚÎÂÈ· GH.
™˘ÌÂÚ¿ÛÌ·Ù·: ∏ ¯ÔÚ‹ÁËÛË GH ·ÔÙÂÏ› ·ÔÙÂÏÂÛÌ·ÙÈ΋ ıÂڷ›· ÁÈ· ·È‰È¿ Ì ¯·ÌËÏfi ·Ó¿ÛÙËÌ·ÔÊÂÈÏfiÌÂÓÔ Û ·Ó¿ÚÎÂÈ· ·˘Ù‹˜. ∆Ô ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ÛÙ· ·È‰È¿ ·˘Ù¿ Ê·›ÓÂÙ·È ˆ˜ ηıÔÚ›˙ÂÙ·È Û ÌÂ-Á¿ÏÔ ‚·ıÌfi ·fi ÙÔ ‡„Ô˜-ÛÙfi¯Ô Î·È ·fi ÙÔÓ ·ÚÈıÌfi ÙˆÓ ÂÓ¤ÛÂˆÓ GH ·Ó¿ ‚‰ÔÌ¿‰·.
§¤ÍÂȘ ÎÏÂȉȿ: A˘ÍËÙÈ΋ ÔÚÌfiÓË, ‹‚Ë, Û˘Ó‰˘·Ṳ̂ÓË ·Ó¿ÚÎÂÈ· ÔÚÌÔÓÒÓ, ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·, ‡„Ô˜-ÛÙfi¯Ô˜.
Final height of children with growth hormone deficiency who
received replacement treatment
M. Papadopoulou1, S. Douma2, K. Kitsios3, N. Kadoglou3, K. Kosta1, I. Tsiouris1
Abstract
Background: The aim of the study was the evaluation of the final height of children with Growth Hormone(GH) deficiency treated with recombinant GH, and of the factors related to their final height.
Methods: Seventy two children (25 prepubertal) with isolated (61/72) or combined (11/72) GHdeficiency, diagnosed after measurement of GH following stimulation tests with clonidin or insulin, weremonitored. The children were treated with 3, 6 or 7 weekly subcutaneous injections of recombinant GH.The target height (TH) was calculated for each child. Height, bone age, growth velocity and pubertal stagewere recorded at the beginning of treatment and every 6 months. Final height was defined as the heightat the time of the complete fusion of the epiphyses observed in a plain X-ray of the hand and wrist.
Results: The difference in the SDS of the mean final height before and after GH treatment was 1.3. Twentythree children (32%) reached the TH. The final height was associated statistically with the initial height, theTH and the number of weekly injections, while no relationship was observed with the age at the beginningof treatment, the duration of treatment, the growth velocity during the first year of treatment or the sex ofthe child. Children with combined hormone deficiency gained more height than those with isolated GHdeficiency, but they also had a greater TH.
Conclusions: GH replacement therapy is beneficial for children with small height due to deficiency of thehormone. The final height in these children appears to be highly predictable by the TH and the number ofGH injections given weekly.
Key words: Growth hormone, puberty, combined hormone deficiency, final height, target height.
128 ∂ƒ∂À¡∏∆π∫∏ ∂ƒ°∞™π∞ ORIGINAL ARTICLE
1. °’ ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋∞¶£, πÔÎÚ¿ÙÂÈÔ °¶¡£
2. ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋,°ÂÓÈÎfi ¡ÔÛÔÎoÌÂ›Ô ∫ÈÏΛ˜
3. ∞’ ¶·ıÔÏÔÁÈ΋ ∫ÏÈÓÈ΋,πÔÎÚ¿ÙÂÈÔ °¶¡£
AÏÏËÏÔÁÚ·Ê›·:
∫ˆÓÛÙ·ÓÙ›Ó· ∫ÒÛÙ·,[email protected]°’ ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋ ∞¶£,πÔÎÚ¿ÙÂÈÔ °¶¡£
1. 3rd PaediatricDepartment, AristotleUniversity of Thessaloniki,Hippokration GeneralHospital of Thessaloniki
2. Paediatric Department,General Hospital of Kilkis
3. 1st Department ofInternal Medicine,Hippokration GeneralHospital of Thessaloniki
Correspondence:
∫onstantina Kosta,[email protected] Paediatric Department,Aristotle University of Thessaloniki,Hippokration GeneralHospital of Thessaloniki
Paediatriki 2008;71:128-134
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·128

∂ÈÛ·ÁˆÁ‹
∏ ·ÓıÚÒÈÓË ·˘ÍËÙÈ΋ ÔÚÌfiÓË (GH) Â›Ó·È Ë Î‡-
ÚÈ· ‰Ú·ÛÙÈ΋ ÔÚÌfiÓË Ô˘ ÚÔ¿ÁÂÈ ÙËÓ ·‡ÍËÛË ÛÙËÓ
·È‰È΋ ËÏÈΛ·, ȉ›ˆ˜ ÌÂÙ¿ ÙÔÓ ÚÒÙÔ ¯ÚfiÓÔ Ù˘ ˙ˆ-
‹˜ (1). ∏ GH Â›Ó·È ·Ó·‚ÔÏÈÎfi˜ ·Ú¿ÁÔÓÙ·˜ Ô˘
ÚÔ¿ÁÂÈ ÙËÓ ·‡ÍËÛË fiÏˆÓ ÙˆÓ ÈÛÙÒÓ ÙÔ˘ ÛÒÌ·ÙÔ˜.
√È ‰Ú¿ÛÂȘ Ù˘ Â›Ó·È ·) ¿ÌÂÛ˜ ÌÂÙ·‚ÔÏÈΤ˜ Ô˘ ‰È-
¢ÎÔχÓÔ˘Ó ÙËÓ ·‡ÍËÛË ÙˆÓ Ì˘ÒÓ Î·È ÙËÓ ÂÍÔÈÎÔÓfi-
ÌËÛË Ù˘ ÁÏ˘Îfi˙˘ Î·È ‚) ·˘ÍËÙÈΤ˜ ÛÙÔ ÛÎÂÏÂÙfi. ∏
·‡ÍËÛË ÙÔ˘ ÛÎÂÏÂÙÔ‡ Ï·Ì‚¿ÓÂÈ ̄ ÒÚ· ÛÙȘ ÂÈʇÛÂȘ
ÙˆÓ Ì·ÎÚÒÓ ÔÛÙÒÓ Î·È Ë Â›‰Ú·ÛË ·˘Ù‹ ‰È·ÎfiÙÂ-
Ù·È Ì ÙË Û‡ÁÎÏÈÛË ÙˆÓ ÂÈʇÛˆÓ. ∏ GH ‰Ú· ÛÙÔ
Û˘˙¢ÎÙÈÎfi ¯fiÓ‰ÚÔ, fiÔ˘ ‰ÈÂÁ›ÚÂÈ ÙÔÓ ÔÏÏ·Ï·-
ÛÈ·ÛÌfi ÙˆÓ ¯ÔÓ‰ÚÔ΢ÙÙ¿ÚˆÓ ·ÊÂÓfi˜ Î·È ·ÊÂÙ¤ÚÔ˘
ÙËÓ ·Ú·ÁˆÁ‹ ÙˆÓ ÈÓÛÔ˘ÏÈÓoÌfiÚÊˆÓ ·˘ÍËÙÈÎÒÓ ·-
Ú·ÁÔÓÙˆÓ (IGF). √ ÈÓÛÔ˘ÏÈÓfiÌÔÚÊÔ˜ ·Ú¿ÁÔÓÙ·˜ π
(IGF-1) ‰ÈÂÁ›ÚÂÈ ÙÔÓ ÔÏÏ·Ï·ÛÈ·ÛÌfi Î·È ÙË ‰È·-
ÊÔÚÔÔ›ËÛË ÙˆÓ ¯ÔÓ‰ÚÔ΢ÙÙ¿ÚˆÓ. ∏ ¤ÏÏÂÈ„Ë ·˘-
ÍËÙÈ΋˜ ÔÚÌfiÓ˘ ÂΉËÏÒÓÂÙ·È ˆ˜: ·) ¯·ÌËÏfi ·Ó¿-
ÛÙËÌ· (2,5 ÛÙ·ıÂÚ¤˜ ·ÔÎÏ›ÛÂȘ (SDS) οو ·fi ÙÔ
̤ÛÔ fiÚÔ ÁÈ· ÙËÓ ËÏÈΛ· Î·È ÙÔ Ê‡ÏÔ), ‚) ηı˘ÛÙ¤ÚË-
ÛË ÛÙËÓ ˆÚ›Ì·ÓÛË ÙˆÓ ÔÛÙÒÓ, Á) ¯·ÌËÏ‹ Ù·¯‡ÙËÙ·
·‡ÍËÛ˘ Î·È ‰) ¯·ÌËÏ‹ ¤ÎÎÚÈÛË Ù˘ ·˘ÍËÙÈ΋˜ ÔÚ-
ÌfiÓ˘ ÌÂÙ¿ ·fi ‰ÔÎÈÌ·Û›· ‰È¤ÁÂÚÛ˘.
™Â ·È‰È¿ Ì ¤ÏÏÂÈ„Ë ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘, ¯ÔÚË-
ÁÂ›Ù·È ıÂڷ¢ÙÈο ‚ÈÔÛ˘ÓıÂÙÈ΋ GH Ô˘ ·Ú¿ÁÂ-
Ù·È Ì ÙË Ì¤ıÔ‰Ô ÙÔ˘ ·Ó·Û˘Ó‰˘·Ṳ̂ÓÔ˘ DNA. ∏ ̄ Ô-
Ú‹ÁËÛË Á›ÓÂÙ·È Ì ÙË ÌÔÚÊ‹ ˘Ô‰ÔÚ›ˆÓ ÂÓ¤ÛˆÓ. ∏
‚ÈÔÛ˘ÓıÂÙÈ΋ GH ·Ú·Û΢¿ÛÙËΠ·Ú¯Èο ÙÔ 1979,
·ÏÏ¿ ¿Ú¯ÈÛ ӷ ¯ÚËÛÈÌÔÔÈÂ›Ù·È Â˘Ú¤ˆ˜ ·fi ÙÔ
1985, ÔfiÙÂ Î·È ·ÓÙÈηٿÛÙËÛ ÙËÓ ÙˆÌ·ÙÈ΋ ·˘-
ÍËÙÈ΋ ÔÚÌfiÓË Ô˘ ¯ÚËÛÈÌÔÔÈ‹ıËΠ·fi ÙÔ 1957.
∏ ıÂڷ›· ·ÔÛÎÔ› ÛÙÔ Ó· ÂÈÙ¢¯ı› ÙÂÏÈÎfi
‡„Ô˜ ̤۷ ÛÙ· Ï·›ÛÈ· ÙÔ˘ ·Ó·ÌÂÓfiÌÂÓÔ˘ ÁÈ· ÙËÓ
ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˘˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ˘ ÛÙÔ Ê‡ÏÔ.
™ÎÔfi˜ Ù˘ ·ÚÔ‡Û·˜ ÌÂϤÙ˘ Â›Ó·È Ë ÂÎÙ›ÌËÛË
ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜ Û ·È‰È¿ Ì ·Ó¿ÚÎÂÈ·
·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Ô˘ ¤Ï·‚·Ó ıÂڷ›· ˘Ôηٿ-
ÛÙ·Û˘ Î·È Ô ÚÔÛ‰ÈÔÚÈÛÌfi˜ ·Ú·ÁfiÓÙˆÓ Ô˘ Û˘-
Û¯ÂÙ›˙ÔÓÙ·È Ì ·˘Ùfi.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ
ªÂÏÂÙ‹ıËÎ·Ó 72 ·È‰È¿, 43 ·ÁfiÚÈ· Î·È 29 ÎÔÚ›ÙÛÈ·, ÌÂ
¯·ÌËÏfi ·Ó¿ÛÙËÌ· Î·È ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘, Ô˘
¤Ï·‚·Ó ıÂڷ›· ˘ÔηٿÛÙ·Û˘ Ì ·˘ÍËÙÈ΋ ÔÚÌfiÓË (GH)
¯ÔÚËÁÔ‡ÌÂÓË ˘Ô‰fiÚÈ·. ∆· 61 ›¯·Ó ÌÂÌÔӈ̤ÓË ·Ó¿Ú-
ÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Î·È Ù· 11 Û˘Ó‰˘·Ṳ̂ÓË. ∂ȉÈÎfiÙÂÚ·:
6 ·È‰È¿, 4 ·ÁfiÚÈ· Î·È 2 ÎÔÚ›ÙÛÈ·, ›¯·Ó ·Ó¿ÚÎÂÈ· ı˘ÚÔÍ›-
Ó˘ (∆4), 1 ·ÁfiÚÈ Â›¯Â ·Ó¿ÚÎÂÈ· ∆4 Î·È ÙÂÛÙÔÛÙÂÚfiÓ˘, 1
ÎÔÚ›ÙÛÈ Â›¯Â ·Ó¿ÚÎÂÈ· ∆4 Î·È ÔÈÛÙÚÔÁfiÓˆÓ, 1 ·ÁfiÚÈ Â›¯Â
·Ó¿ÚÎÂÈ· ∆4 Î·È ¿ÔÈÔ ‰È·‚‹ÙË Î·È 2 ÎÔÚ›ÙÛÈ· ·Ó˘ÔÊ˘-
ÛÈÛÌfi ÌÂÙ¿ ·fi ¯ÂÈÚÔ˘ÚÁËı¤ÓÙ˜ ÂÁÎÂÊ·ÏÈÎÔ‡˜ fiÁÎÔ˘˜. ∏
̤ÛË ËÏÈΛ· ÙˆÓ ·È‰ÈÒÓ Î·Ù¿ ÙËÓ ¤Ó·ÚÍË Ù˘ ·ÁˆÁ‹˜ ‹Ù·Ó
11,6±2,9 ¤ÙË Î·È Î·Ù¿ ÙÔ ¤Ú·˜ ·˘Ù‹˜ 16,2±1,6. ∞ÓıÚˆÔÌÂ-
ÙÚÈΤ˜ ÌÂÙÚ‹ÛÂȘ Á›ÓÔÓÙ·Ó Ì ·Ó·ÛÙËÌfiÌÂÙÚÔ Harpenden
ÛÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ Î·È ·Ó¿ ÂÍ¿ÌËÓÔ Î·ı’ fiÏË ÙË ‰È¿Ú-
ÎÂÈ¿ Ù˘. ∏ ̤ÙÚËÛË ÙÔ˘ ‡„Ô˘˜ οı ·È‰ÈÔ‡ ÁÈÓfiÙ·Ó Û fiÚıÈ·
ı¤ÛË Î·È ÙÔ ·ÔÙ¤ÏÂÛÌ· ÛËÌÂȈÓfiÙ·Ó ÛÙȘ η̇Ϙ ·‡ÍËÛ˘
ÙˆÓ Tanner Î·È Whitehouse ÁÈ· ÙËÓ ÂÎÙ›ÌËÛË Ù˘ ÂηÙÔÛÙÈ·›-
·˜ ı¤Û˘ (∂£). ¶ÚÔÛ‰ÈÔÚÈ˙fiÙ·Ó Ô ÂÙ‹ÛÈÔ˜ Ú˘ıÌfi˜ ·‡ÍËÛ˘
(∂ƒ∞). √ ∂ƒ∞ ‹ height velocity Â›Ó·È Ë ‰È·ÊÔÚ¿ ÙÔ˘ ‡„Ô˘˜ ÛÂ
¤Ó· ¯ÚfiÓÔ. ¶ÚÔÛ‰ÈÔÚ›˙ÂÙ·È ·fi ÙÔ ËÏ›ÎÔ Ù˘ ‰È·ÊÔÚ¿˜ ÙÔ˘
‡„Ô˘˜ ·Ó¿ÌÂÛ· Û ‰‡Ô ÌÂÙÚ‹ÛÂȘ ‰È· ÙÔ˘ ̄ ÚfiÓÔ˘ Ô˘ ÌÂÛÔÏ¿-
‚ËÛÂ Î·È ÂÎÊÚ¿˙ÂÙ·È Û cm/¤ÙÔ˜. ∆Ô ̄ ÚÔÓÈÎfi ‰È¿ÛÙËÌ· ̆ ÔÏÔ-
Á›˙ÂÙ·È ·ÎÚÈ‚Ò˜ Ì ÙÔ ‰Âη‰ÈÎfi ËÌÂÚÔÏfiÁÈÔ. √È ÌÂÙÚ‹ÛÂȘ ÙÔ˘
‡„Ô˘˜ Î·È ÙÔ˘ ∂ƒ∞ ÙÔ˘ οı ·È‰ÈÔ‡ ÂÎÊÚ¿ÛÙËÎ·Ó Û ‰Â›ÎÙ˜
ÛÙ·ıÂÚ‹˜ ·fiÎÏÈÛ˘ (Standard Deviation Score, SDS) Ì ‚¿ÛË
ÙË ¯ÚÔÓÔÏÔÁÈ΋ ËÏÈΛ·. √ ‰Â›ÎÙ˘ ·˘Ùfi˜ ‰Â›¯ÓÂÈ fiÛ˜ ·ÎÚÈ-
‚Ò˜ ÛÙ·ıÂÚ¤˜ ·ÔÎÏ›ÛÂȘ ·fi ÙÔ Ì¤ÛÔ fiÚÔ ‚Ú›ÛÎÂÙ·È ÙÔ ‡„Ô˜
‹ ¿ÏÏË Ì¤ÙÚËÛË ÙÔ˘ ·È‰ÈÔ‡. √ ‰Â›ÎÙ˘ ·˘Ùfi˜ ˘ÔÏÔÁ›˙ÂÙ·È
·fi ÙÔÓ Ù‡Ô: SDS=(X-XÌÙ) / SD, fiÔ˘ Ã: ‡„Ô˜ (‹ ¿ÏÏË Ì¤-
ÙÚËÛË ÙÔ˘ ·È‰ÈÔ‡), ÃÌÙ: Ë Ì¤ÛË ÙÈÌ‹ ÙÔ˘ ‡„Ô˘˜ (·fi ›Ó·-
Θ) Ô˘ ·ÓÙÈÛÙÔȯ› ÛÙËÓ ËÏÈΛ· Î·È ÙÔ Ê‡ÏÔ ÙÔ˘ ·È‰ÈÔ‡ ηÈ
SD: Ë ÛÙ·ıÂÚ‹ ·fiÎÏÈÛË Ù˘ ›‰È·˜ ËÏÈΛ·˜ (2).
∂›Û˘, ˘ÔÏÔÁ›ÛÙËΠÙÔ ‡„Ô˜-ÛÙfi¯Ô˜ (target height,
TH) ÁÈ· Ó· ÂÏÂÁ¯ı› ·Ó ÙÔ ÙÂÏÈÎfi ‡„Ô˜ ÙÔ˘ ·È‰ÈÔ‡ ‚Ú›ÛÎÂÙ·È
ÂÓÙfi˜ ÙÔ˘ ÁÂÓÂÙÈÎÔ‡ ‰˘Ó·ÌÈÎÔ‡ ÙÔ˘. ∆Ô TH ˘ÔÏÔÁ›˙ÂÙ·È ·Ó
ÛÙÔ Ì¤ÛÔ ‡„Ô˜ ÙˆÓ ÁÔÓ¤ˆÓ ÚÔÛÙÂıÔ‡Ó 6,5 cm, ÚÔÎÂÈ̤ÓÔ˘
ÁÈ· ·ÁfiÚÈ, ‹ ·Ê·ÈÚÂıÔ‡Ó 6,5 cm, ÚÔÎÂÈ̤ÓÔ˘ ÁÈ· ÎÔÚ›ÙÛÈ.
°ÈÓfiÙ·Ó ˘ÔÏÔÁÈÛÌfi˜ Ù˘ ÔÛÙÈ΋˜ ËÏÈΛ·˜ ÛÙËÓ ¤Ó·ÚÍË
Ù˘ ·ÁˆÁ‹˜ Î·È ·Ó¿ ¤ÙÔ˜, Û‡Ìʈӷ Ì ÙÔÓ ¿ÙÏ·ÓÙ· TWRUS.
∂›Û˘, ÁÈÓfiÙ·Ó ÛÙ·‰ÈÔÔ›ËÛË Ù˘ ÂÊ˂›·˜ ηٿ Tanner
ÛÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ Î·È ·Ó¿ ÂÍ¿ÌËÓÔ. ¶ÚÔÂÊË‚ÈÎfi
ıˆÚ›ÙÔ Î¿ı ÎÔÚ›ÙÛÈ ̄ ˆÚ›˜ „ËÏ·ÊËÙfi Ì·˙ÈÎfi ·‰¤Ó· Î·È Î¿-
ı ·ÁfiÚÈ Ì fiÁÎÔ fiÚ¯ÂˆÓ <4 ml. ∆Ô Ì¤ÁÂıÔ˜ ÙˆÓ fiÚ¯ÂˆÓ ÂÎÙÈ-
Ì‹ıËΠ̠ÔگȉfiÌÂÙÚÔ Prader.
ø˜ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ıˆڋıËΠÙÔ ‡„Ô˜ ÙÔ˘ ·È‰ÈÔ‡ ÙË
¯ÚÔÓÈ΋ ÛÙÈÁÌ‹ Ô˘ ÛÙËÓ ·Ï‹ ·ÎÙÈÓÔÁÚ·Ê›· ¯ÂÈÚÒÓ ‰È·È-
ÛÙˆÓfiÙ·Ó Ï‹Ú˘ Û‡ÁÎÏÈÛË ÙˆÓ ÂÈʇÛÂˆÓ ÙˆÓ Ì·ÎÚÒÓ
ÔÛÙÒÓ.
∂ÚÁ·ÛÙËÚÈ·Îfi˜ ¤ÏÂÁ¯Ô˜
™Â οı ·È‰› ÂÎÙÈÌ‹ıËÎÂ Ë ¤ÎÎÚÈÛË GH ÌÂÙ¿ ·fi ‰ÔÎÈ-
Ì·Û›· ‰È¤ÁÂÚÛ˘ Ì ÎÏÔÓȉ›ÓË ‹ ‰È·Ï˘Ù‹ ÈÓÛÔ˘Ï›ÓË Ì ÚÔÛ-
‰ÈÔÚÈÛÌfi Ù˘ GH Û ¯ÚfiÓÔ˘˜ 0, 15, 30, 45, 60, 90, 120 min.
¶·ıÔÏÔÁÈ΋ ıˆÚ›ÙÔ ÙÈÌ‹ GH <10 ng/ml Ô˘ ÂȂ‚·ÈˆÓfi-
Ù·Ó Û ‰Â‡ÙÂÚË ‰ÔÎÈÌ·Û›· ÂÓÙfi˜ ÂÓfi˜ ÌËÓfi˜.
°È· ÙÔÓ ¤ÏÂÁ¯Ô ¤Ó·Ú͢ Ù˘ ÂÊ˂›·˜ ÁÈÓfiÙ·Ó ‰ÔÎÈÌ·Û›·
LHRH Ì ÚÔÛ‰ÈÔÚÈÛÌfi ÙÈÌÒÓ LH, FSH Û ¯ÚfiÓÔ˘˜ 0, 30, 60
min. ŒÓ·ÚÍË Ù˘ ÂÊ˂›·˜ ıˆÚ›ÙÔ ÙÈÌ‹ LH >15 IU/L (3).
∂›Û˘, ÁÈÓfiÙ·Ó ‰ÔÎÈÌ·Û›· TRH ÁÈ· ÙÔÓ ¤ÏÂÁ¯Ô Ù˘ ı˘ÚÂ-
ÔÂȉÈ΋˜ ÏÂÈÙÔ˘ÚÁ›·˜ Ì ÚÔÛ‰ÈÔÚÈÛÌfi Ù˘ TSH (Ê˘ÛÈÔÏÔÁÈ-
Τ˜ ÙÈ̤˜ TSH: 0,4-4 ÌπU/ml) Û ̄ ÚfiÓÔ˘˜ 0, 30, 60 min Î·È Ù˘
∆4 Û ¯ÚfiÓÔ 0 (Ê˘ÛÈÔÏÔÁÈΤ˜ ÙÈ̤˜ ∆4: 5,6-12 Ìg/dl).
∞Ó¿ ÂÍ¿ÌËÓÔ ÁÈÓfiÙ·Ó ¤ÏÂÁ¯Ô˜ ÁÏ˘Îfi˙˘ ÔÚÔ‡, ÁÏ˘ÎÔ˙˘-
ÏȈ̤Ó˘ ·ÈÌÔÛÊ·ÈÚ›Ó˘ (HbA1c%), ı˘ÚÂÔÂȉÈ΋˜ ÏÂÈÙÔ˘Ú-
Á›·˜ (TSH, T3, T4), ÁÂÓÈ΋ ·›Ì·ÙÔ˜ Î·È ÚÔÛ‰ÈÔÚÈÛÌfi˜ ÔÛÙÈ-
΋˜ ËÏÈΛ·˜ ÛÙ· ·È‰È¿ Ô˘ Ë ÂÊ˂›· ›¯Â ÍÂÎÈÓ‹ÛÂÈ.
™Ù·ÙÈÛÙÈ΋ ·Ó¿Ï˘ÛË
√È ÔÛÔÙÈΤ˜ ÌÂÙ·‚ÏËÙ¤˜ Û˘ÓÔ„›ÛÙËÎ·Ó ¯ÚËÛÈÌÔÔÈÒ-
ÓÙ·˜ ̤ÛÔ˘˜ fiÚÔ˘˜ Î·È Ù˘ÈΤ˜ ·ÔÎÏ›ÛÂȘ (standard
deviation). °È· ÙË Û‡ÁÎÚÈÛË ‰‡Ô Ì¤ÛˆÓ fiÚˆÓ ¯ÚËÛÈÌÔÔÈ‹ıË-
ÎÂ Ë ‰ÔÎÈÌ·Û›· ηٿ Student’s t-test. ¶·Ú¿ÏÏËÏ· ¤ÁÈÓ ¤ÏÂÁ-
¯Ô˜ ÁÈ· ÙËÓ Î·ÓÔÓÈÎfiÙËÙ· ÙˆÓ ÌÂÙ·‚ÏËÙÒÓ ¯ÚËÛÈÌÔÔÈÒÓÙ·˜
ÙË ‰ÔÎÈÌ·Û›· ηٿ Shapiro-Wilk, fiÔ˘ ‰ÂÓ ‰È·ÈÛÙÒıËÎÂ
·fiÎÏÈÛË ·fi ÙËÓ Î·ÓÔÓÈÎfiÙËÙ· Î·È ÁÈ· ÙÔ ÏfiÁÔ ·˘Ùfi ‰ÂÓ
129AÓ¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
¶·È‰È·ÙÚÈ΋ 2008;71:128-134
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·129
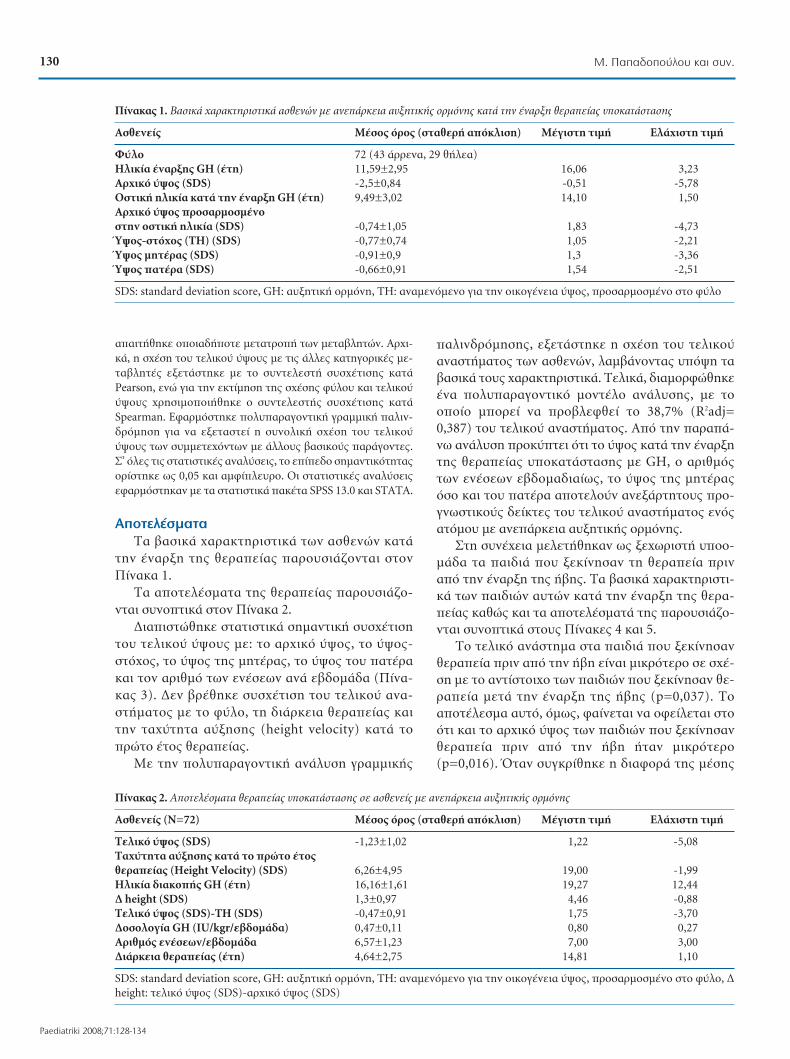
··ÈÙ‹ıËΠÔÔÈ·‰‹ÔÙ ÌÂÙ·ÙÚÔ‹ ÙˆÓ ÌÂÙ·‚ÏËÙÒÓ. ∞Ú¯È-
ο, Ë Û¯¤ÛË ÙÔ˘ ÙÂÏÈÎÔ‡ ‡„Ô˘˜ Ì ÙȘ ¿ÏϘ ηÙËÁÔÚÈΤ˜ ÌÂ-
Ù·‚ÏËÙ¤˜ ÂÍÂÙ¿ÛÙËΠ̠ÙÔ Û˘ÓÙÂÏÂÛÙ‹ Û˘Û¯¤ÙÈÛ˘ ηٿ
Pearson, ÂÓÒ ÁÈ· ÙËÓ ÂÎÙ›ÌËÛË Ù˘ Û¯¤Û˘ ʇÏÔ˘ Î·È ÙÂÏÈÎÔ‡
‡„Ô˘˜ ¯ÚËÛÈÌÔÔÈ‹ıËÎÂ Ô Û˘ÓÙÂÏÂÛÙ‹˜ Û˘Û¯¤ÙÈÛ˘ ηٿ
Spearman. ∂Ê·ÚÌfiÛÙËΠÔÏ˘·Ú·ÁÔÓÙÈ΋ ÁÚ·ÌÌÈ΋ ·ÏÈÓ-
‰ÚfiÌËÛË ÁÈ· Ó· ÂÍÂÙ·ÛÙ› Ë Û˘ÓÔÏÈ΋ Û¯¤ÛË ÙÔ˘ ÙÂÏÈÎÔ‡
‡„Ô˘˜ ÙˆÓ Û˘ÌÌÂÙ¯fiÓÙˆÓ Ì ¿ÏÏÔ˘˜ ‚·ÛÈÎÔ‡˜ ·Ú¿ÁÔÓÙ˜.
™’ fiϘ ÙȘ ÛÙ·ÙÈÛÙÈΤ˜ ·Ó·Ï‡ÛÂȘ, ÙÔ Â›Â‰Ô ÛËÌ·ÓÙÈÎfiÙËÙ·˜
ÔÚ›ÛÙËΠˆ˜ 0,05 Î·È ·ÌʛϢÚÔ. √È ÛÙ·ÙÈÛÙÈΤ˜ ·Ó·Ï‡ÛÂȘ
ÂÊ·ÚÌfiÛÙËÎ·Ó Ì ٷ ÛÙ·ÙÈÛÙÈο ·Î¤Ù· SPSS 13.0 Î·È STATA.
∞ÔÙÂϤÛÌ·Ù·
∆· ‚·ÛÈο ¯·Ú·ÎÙËÚÈÛÙÈο ÙˆÓ ·ÛıÂÓÒÓ Î·Ù¿
ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È ÛÙÔÓ
¶›Ó·Î· 1.
∆· ·ÔÙÂϤÛÌ·Ù· Ù˘ ıÂڷ›·˜ ·ÚÔ˘ÛÈ¿˙Ô-
ÓÙ·È Û˘ÓÔÙÈο ÛÙÔÓ ¶›Ó·Î· 2.
¢È·ÈÛÙÒıËΠÛÙ·ÙÈÛÙÈο ÛËÌ·ÓÙÈ΋ Û˘Û¯¤ÙÈÛË
ÙÔ˘ ÙÂÏÈÎÔ‡ ‡„Ô˘˜ ÌÂ: ÙÔ ·Ú¯ÈÎfi ‡„Ô˜, ÙÔ ‡„Ô˜-
ÛÙfi¯Ô˜, ÙÔ ‡„Ô˜ Ù˘ ÌËÙ¤Ú·˜, ÙÔ ‡„Ô˜ ÙÔ˘ ·Ù¤Ú·
Î·È ÙÔÓ ·ÚÈıÌfi ÙˆÓ ÂÓ¤ÛÂˆÓ ·Ó¿ ‚‰ÔÌ¿‰· (¶›Ó·-
η˜ 3). ¢ÂÓ ‚Ú¤ıËÎÂ Û˘Û¯¤ÙÈÛË ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·-
ÛÙ‹Ì·ÙÔ˜ Ì ÙÔ Ê‡ÏÔ, ÙË ‰È¿ÚÎÂÈ· ıÂڷ›·˜ ηÈ
ÙËÓ Ù·¯‡ÙËÙ· ·‡ÍËÛ˘ (height velocity) ηٿ ÙÔ
ÚÒÙÔ ¤ÙÔ˜ ıÂڷ›·˜.
ªÂ ÙËÓ ÔÏ˘·Ú·ÁÔÓÙÈ΋ ·Ó¿Ï˘ÛË ÁÚ·ÌÌÈ΋˜
·ÏÈÓ‰ÚfiÌËÛ˘, ÂÍÂÙ¿ÛÙËÎÂ Ë Û¯¤ÛË ÙÔ˘ ÙÂÏÈÎÔ‡·Ó·ÛÙ‹Ì·ÙÔ˜ ÙˆÓ ·ÛıÂÓÒÓ, Ï·Ì‚¿ÓÔÓÙ·˜ ˘fi„Ë Ù·‚·ÛÈο ÙÔ˘˜ ̄ ·Ú·ÎÙËÚÈÛÙÈο. ∆ÂÏÈο, ‰È·ÌÔÚÊÒıËΤӷ ÔÏ˘·Ú·ÁÔÓÙÈÎfi ÌÔÓÙ¤ÏÔ ·Ó¿Ï˘Û˘, Ì ÙÔÔÔ›Ô ÌÔÚ› Ó· ÚÔ‚ÏÂÊı› ÙÔ 38,7% (R2adj=0,387) ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜. ∞fi ÙËÓ ·Ú·¿-Óˆ ·Ó¿Ï˘ÛË ÚÔ·ÙÂÈ fiÙÈ ÙÔ ‡„Ô˜ ηٿ ÙËÓ ¤Ó·ÚÍËÙ˘ ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘ Ì GH, Ô ·ÚÈıÌfi˜ÙˆÓ ÂÓ¤ÛÂˆÓ Â‚‰ÔÌ·‰È·›ˆ˜, ÙÔ ‡„Ô˜ Ù˘ ÌËÙ¤Ú·˜fiÛÔ Î·È ÙÔ˘ ·Ù¤Ú· ·ÔÙÂÏÔ‡Ó ·ÓÂÍ¿ÚÙËÙÔ˘˜ ÚÔ-ÁÓˆÛÙÈÎÔ‡˜ ‰Â›ÎÙ˜ ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜ ÂÓfi˜·ÙfiÌÔ˘ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘.
™ÙË Û˘Ó¤¯ÂÈ· ÌÂÏÂÙ‹ıËÎ·Ó ˆ˜ ͯˆÚÈÛÙ‹ ˘ÔÔ-Ì¿‰· Ù· ·È‰È¿ Ô˘ ÍÂΛÓËÛ·Ó ÙË ıÂڷ›· ÚÈÓ·fi ÙËÓ ¤Ó·ÚÍË Ù˘ ‹‚˘. ∆· ‚·ÛÈο ¯·Ú·ÎÙËÚÈÛÙÈ-ο ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ Î·Ù¿ ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂÚ·-›·˜ ηıÒ˜ Î·È Ù· ·ÔÙÂϤÛÌ·Ù¿ Ù˘ ·ÚÔ˘ÛÈ¿˙Ô-ÓÙ·È Û˘ÓÔÙÈο ÛÙÔ˘˜ ¶›Ó·Î˜ 4 Î·È 5.
∆Ô ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ÛÙ· ·È‰È¿ Ô˘ ÍÂΛÓËÛ·ÓıÂڷ›· ÚÈÓ ·fi ÙËÓ ‹‚Ë Â›Ó·È ÌÈÎÚfiÙÂÚÔ Û ۯ¤-ÛË Ì ÙÔ ·ÓÙ›ÛÙÔÈ¯Ô ÙˆÓ ·È‰ÈÒÓ Ô˘ ÍÂΛÓËÛ·Ó ıÂ-ڷ›· ÌÂÙ¿ ÙËÓ ¤Ó·ÚÍË Ù˘ ‹‚˘ (p=0,037). ∆Ô·ÔÙ¤ÏÂÛÌ· ·˘Ùfi, fï˜, Ê·›ÓÂÙ·È Ó· ÔÊ›ÏÂÙ·È ÛÙÔfiÙÈ Î·È ÙÔ ·Ú¯ÈÎfi ‡„Ô˜ ÙˆÓ ·È‰ÈÒÓ Ô˘ ÍÂΛÓËÛ·ÓıÂڷ›· ÚÈÓ ·fi ÙËÓ ‹‚Ë ‹Ù·Ó ÌÈÎÚfiÙÂÚÔ(p=0,016). ŸÙ·Ó Û˘ÁÎÚ›ıËÎÂ Ë ‰È·ÊÔÚ¿ Ù˘ ̤Û˘
¶›Ó·Î·˜ 2. ∞ÔÙÂϤÛÌ·Ù· ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘ Û ·ÛıÂÓ›˜ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
∞ÛıÂÓ›˜ (¡=72) ª¤ÛÔ˜ fiÚÔ˜ (ÛÙ·ıÂÚ‹ ·fiÎÏÈÛË) ª¤ÁÈÛÙË ÙÈÌ‹ ∂Ï¿¯ÈÛÙË ÙÈÌ‹
∆ÂÏÈÎfi ‡„Ô˜ (SDS) -1,23±1,02 1,22 -5,08∆·¯‡ÙËÙ· ·‡ÍËÛ˘ ηٿ ÙÔ ÚÒÙÔ ¤ÙÔ˜ ıÂڷ›·˜ (Height Velocity) (SDS) 6,26±4,95 19,00 -1,99∏ÏÈΛ· ‰È·ÎÔ‹˜ GH (¤ÙË) 16,16±1,61 19,27 12,44¢ height (SDS) 1,3±0,97 4,46 -0,88∆ÂÏÈÎfi ‡„Ô˜ (SDS)-∆∏ (SDS) -0,47±0,91 1,75 -3,70¢ÔÛÔÏÔÁ›· GH (IU/kgr/‚‰ÔÌ¿‰·) 0,47±0,11 0,80 0,27∞ÚÈıÌfi˜ ÂÓ¤ÛˆÓ/‚‰ÔÌ¿‰· 6,57±1,23 7,00 3,00¢È¿ÚÎÂÈ· ıÂڷ›·˜ (¤ÙË) 4,64±2,75 14,81 1,10
SDS: standard deviation score, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ, ¢height: ÙÂÏÈÎfi ‡„Ô˜ (SDS)-·Ú¯ÈÎfi ‡„Ô˜ (SDS)
130 ª. ¶··‰ÔÔ‡ÏÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:128-134
¶›Ó·Î·˜ 1. µ·ÛÈο ¯·Ú·ÎÙËÚÈÛÙÈο ·ÛıÂÓÒÓ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ ηٿ ÙËÓ ¤Ó·ÚÍË ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘
∞ÛıÂÓ›˜ ª¤ÛÔ˜ fiÚÔ˜ (ÛÙ·ıÂÚ‹ ·fiÎÏÈÛË) ª¤ÁÈÛÙË ÙÈÌ‹ ∂Ï¿¯ÈÛÙË ÙÈÌ‹
º‡ÏÔ 72 (43 ¿ÚÚÂÓ·, 29 ı‹Ï·)∏ÏÈΛ· ¤Ó·Ú͢ GH (¤ÙË) 11,59±2,95 16,06 3,23∞Ú¯ÈÎfi ‡„Ô˜ (SDS) -2,5±0,84 -0,51 -5,78√ÛÙÈ΋ ËÏÈΛ· ηٿ ÙËÓ ¤Ó·ÚÍË GH (¤ÙË) 9,49±3,02 14,10 1,50∞Ú¯ÈÎfi ‡„Ô˜ ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙËÓ ÔÛÙÈ΋ ËÏÈΛ· (SDS) -0,74±1,05 1,83 -4,73⁄„Ô˜-ÛÙfi¯Ô˜ (∆∏) (SDS) -0,77±0,74 1,05 -2,21⁄„Ô˜ ÌËÙ¤Ú·˜ (SDS) -0,91±0,9 1,3 -3,36⁄„Ô˜ ·Ù¤Ú· (SDS) -0,66±0,91 1,54 -2,51
SDS: standard deviation score, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·130

Ù˘È΋˜ ·fiÎÏÈÛ˘ ÙÂÏÈÎÔ‡ ‡„Ô˘˜-·Ú¯ÈÎÔ‡ ‡„Ô˘˜
(¢ height SDS), ·˘Ù‹ ‰ÂÓ ‰È¤ÊÂÚ ÛËÌ·ÓÙÈο ÛÙȘ 2
˘ÔÔÌ¿‰Â˜ (p=0,9). ∆· ·ÓˆÙ¤Úˆ Û˘ÓÔ„›˙ÔÓÙ·È
ÛÙÔÓ ¶›Ó·Î· 6.
ªÈ· ¿ÏÏË ˘ÔÔÌ¿‰· ·ÛıÂÓÒÓ Ô˘ ÌÂÏÂÙ‹ıËÎÂ
ͯˆÚÈÛÙ¿ ‹Ù·Ó Ù· ·È‰È¿ Ì ¤ÏÏÂÈ„Ë Î·È ¿ÏÏˆÓ ÔÚ-
ÌÔÓÒÓ ÏËÓ Ù˘ ·˘ÍËÙÈ΋˜. ∆Ô ¢ height ÛÙ· ·È‰È¿
·˘Ù¿ ‹Ù·Ó ÌÂÁ·Ï‡ÙÂÚÔ Û ۯ¤ÛË Ì ÂΛӷ Ô˘ ›¯·Ó
ÌÂÌÔӈ̤ÓË ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
(p=0,001), ·Ó Î·È ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ‰ÂÓ ‰È¤ÊÂÚÂ
ÛËÌ·ÓÙÈο ÛÙȘ 2 ·˘Ù¤˜ ˘ÔÔÌ¿‰Â˜ (p=0,091). ∆·
·ÓˆÙ¤Úˆ Û˘ÓÔ„›˙ÔÓÙ·È ÛÙÔÓ ¶›Ó·Î· 7.
™˘˙‹ÙËÛË
∏ ̤ÛË Ù˘È΋ ·fiÎÏÈÛË ÙÔ˘ ‡„Ô˘˜ ÙˆÓ ·È‰ÈÒÓ
ηٿ ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ (HtSDS) ‹Ù·Ó -2,5,
ÂÓÒ Ë Ì¤ÛË Ù˘È΋ ·fiÎÏÈÛË ÙÔ˘ ÙÂÏÈÎÔ‡ ‡„Ô˘˜
(FHSDS) ‹Ù·Ó -1,22. ∏ ıÂڷ›· ˘ÔηٿÛÙ·Û˘
‚ÂÏÙ›ˆÛ ۷ÊÒ˜ ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ÙˆÓ ·È‰ÈÒÓ
·˘ÙÒÓ, ·Ó Î·È ÌfiÓÔ 23 ·È‰È¿ (32%) ¤ÊÙ·Û·Ó ÙÔ
‡„Ô˜-ÛÙfi¯Ô (TH). ¶·È‰È¿ Ì ȉÈÔ·ı‹ ·Ó¿ÚÎÂÈ·
·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ (GHD) ‹ ˘ÔÊ˘ÛÈÛÌfi Ô˘ ‰ÂÓ
Ï·Ì‚¿ÓÔ˘Ó ıÂڷ›· ·ÚÔ˘ÛÈ¿˙Ô˘Ó FHSDS ÌÂٷ͇
-4 Î·È -6 (4). ™Â ÌÈ· ÛÂÈÚ¿ ·fi ·Ó¿ÏÔÁ˜ ÂÚÁ·Û›Â˜Ô˘ ‰ËÌÔÛȇÙËÎ·Ó ÌÂٷ͇ 1995 Î·È 2006, ÙÔFHSDS ·Ó·Ê¤ÚÂÙ·È ÌÂٷ͇ -0,4 Î·È -2,0 (5-13). ™ÂÌÂϤÙ˜ Ô˘ ‰ËÌÔÛȇÙËÎ·Ó ÌÂٷ͇ 1981 Î·È 1989,ÙÔ FHSDS ·Ó·Ê¤ÚÂÙ·È ÌÂٷ͇ -1,75 Î·È -3,0 (14-20).∆· Ùˆ¯fiÙÂÚ· ·ÔÙÂϤÛÌ·Ù· ÙˆÓ ·Ï·ÈfiÙÂÚˆÓ ·˘-ÙÒÓ ÌÂÏÂÙÒÓ ÔÊ›ÏÔÓÙ·È ÛÙË ¯Ú‹ÛË ÚÈÓ ·fi ÙÔ1985 Ù˘ و̷ÙÈ΋˜ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ ηıÒ˜ ηÈÛÙË ıÂڷ›· Û ÔÏϤ˜ ÂÚÈÙÒÛÂȘ Ì 3 ÌfiÓÔ ÂÓ¤-ÛÂȘ GH ‚‰ÔÌ·‰È·›ˆ˜.
∏ ¿ÚÈÛÙË ‰fiÛË Ù˘ GH ¤¯ÂÈ ÔÚÈÛı› ÛÙȘ 0,3-0,6πU/kg/‚‰ÔÌ¿‰· ηٿ ÙËÓ ÂÚ›Ô‰Ô Ù˘ ·È‰È΋˜ËÏÈΛ·˜ (21). ™ÙË ‰È¿ÚÎÂÈ· Ù˘ ÂÊ˂›·˜, Ë ¤ÎÎÚÈÛËÙ˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ ·˘Í¿ÓÂÙ·È Î·È Û˘ÓÂÒ˜ ı·Ú¤ÂÈ Ë ‰fiÛË Ù˘ ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Ó· ·Ó·ÚÔ-Û·ÚÌfi˙ÂÙ·È ·Ó¿ÏÔÁ· Ì ÙȘ ·Ó¿ÁΘ (22). √È RankeÎ·È Butendandt (1989) (19) ηıÒ˜ Î·È Ë ÌÂϤÙËKIGS (20,23) ¤‰ÂÈÍ·Ó fiÙÈ ÙÔ FHSDS Û˘Û¯ÂÙ›˙ÂÙ·È ÌÂÙÔÓ ·ÚÈıÌfi ÙˆÓ ÂÓ¤ÛÂˆÓ GH. ∞˘Ùfi ‰È·ÈÛÙÒıËÎÂÎ·È ÛÙË ‰È΋ Ì·˜ ÌÂϤÙË, ÛÙËÓ ÔÔ›· 6 ·È‰È¿ ¤Î·-Ó·Ó 3 ÌfiÓÔ ÂÓ¤ÛÂȘ ‚‰ÔÌ·‰È·›ˆ˜, ÂÓÒ 66 ·È‰È¿·ÎÔÏÔ‡ıËÛ·Ó Û¯‹Ì· 6 ‹ 7 ÂÓ¤ÛÂˆÓ Â‚‰ÔÌ·‰È·›ˆ˜.∂ÓÙÔ‡ÙÔȘ, Û¯‹Ì·Ù· Ì ÂÚÈÛÛfiÙÂÚ˜ Ù˘ ÌÈ·˜ ¤ÓÂ-Û˘ ËÌÂÚËÛ›ˆ˜ ‰ÂÓ Ê·›ÓÂÙ·È Ó· ÚÔÛʤÚÔ˘Ó ÌÂÁ·-χÙÂÚÔ fiÊÂÏÔ˜ (24).
√ ·Ú¿ÁÔÓÙ·˜ Ô˘ ‚Ú¤ıËΠӷ ¤¯ÂÈ ÙËÓ ÈÛ¯˘Úfi-ÙÂÚË Û˘Û¯¤ÙÈÛË Ì ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ‹Ù·Ó ÛÙË ÌÂ-ϤÙË Ì·˜ ÙÔ ‡„Ô˜-ÛÙfi¯Ô˜ (·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈ-ÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ) (T∏). ∏Û˘Û¯¤ÙÈÛË ·˘Ù‹ ¤¯ÂÈ ·Ó·ÊÂÚı› Î·È Û ÚÔËÁÔ‡ÌÂ-Ó˜ ÌÂϤÙ˜ (12,14,19,20,23,25). º·›ÓÂÙ·È ÙÂÏÈοˆ˜ ÙÔ ÁÂÓÂÙÈÎfi ‰˘Ó·ÌÈÎfi Â›Ó·È ·˘Ùfi Ô˘ Û ÌÂÁ¿ÏÔ‚·ıÌfi ηıÔÚ›˙ÂÈ ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ·. ∂›Û˘, ÙÔ ÙÂ-ÏÈÎfi ·Ó¿ÛÙËÌ· Û˘Û¯ÂÙ›ÛÙËΠÛÙË ÌÂϤÙË Ì·˜ Î·È ÌÂÙÔ ‡„Ô˜ ηٿ ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ (12,26).
∞ÍÈÔÛËÌ›ˆÙÔ Â›Ó·È ÙÔ ÁÂÁÔÓfi˜ Ù˘ ÌË ·Ó‡ÚÂ-Û˘ ÛÙË ÌÂϤÙË Ì·˜ Û˘Û¯¤ÙÈÛ˘ ÌÂٷ͇ ÙÂÏÈÎÔ‡·Ó·ÛÙ‹Ì·ÙÔ˜ Î·È ‰È¿ÚÎÂÈ·˜ ıÂڷ›·˜. ™ÙË ÌÂϤÙËKIGS (20,23) ˘‹ÚÍ ÔÚȷ΋ Û˘Û¯¤ÙÈÛË ÙˆÓ ‰˘Ô
¶›Ó·Î·˜ 4. µ·ÛÈο ¯·Ú·ÎÙËÚÈÛÙÈο ·ÛıÂÓÒÓ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Î·È ¤Ó·ÚÍË ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘ ηٿ ÙËÓ ÚÔÂÊË-‚È΋ ËÏÈΛ·
∞ÛıÂÓ›˜ ª¤ÛÔ˜ fiÚÔ˜ (ÛÙ·ıÂÚ‹ ·fiÎÏÈÛË) ª¤ÁÈÛÙË ÙÈÌ‹ ∂Ï¿¯ÈÛÙË ÙÈÌ‹
º‡ÏÔ 25 (11 ¿ÚÚÂÓ·, 14 ı‹Ï·)∏ÏÈΛ· ¤Ó·Ú͢ GH (¤ÙË) 8,4±2,39 10,99 3,23∞Ú¯ÈÎfi ‡„Ô˜ (SDS) -2,89±1,08 -0,51 -5,78√ÛÙÈ΋ ËÏÈΛ· ηٿ ÙËÓ ¤Ó·ÚÍË GH (¤ÙË) 6,32±2,64 10,10 1,50∞Ú¯ÈÎfi ‡„Ô˜ ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙËÓ ÔÛÙÈ΋ ËÏÈΛ· (SDS) -0,855±1,45 1,83 -4,73∆∏ ‡„Ô˜ (SDS) -0,9±0,78 1,01 -2,21⁄„Ô˜ ÌËÙ¤Ú·˜ (SDS) -1,06±1,05 1,11 -3,36⁄„Ô˜ ·Ù¤Ú· (SDS) -0,76±0,89 1,51 -2,21
SDS: standard deviation, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ(target height)
131AÓ¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
¶·È‰È·ÙÚÈ΋ 2008;71:128-134
¶›Ó·Î·˜ 3. ¶·Ú¿ÁÔÓÙ˜ Ô˘ ηıÔÚ›˙Ô˘Ó ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· Û·ÛıÂÓ›˜ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
¶·Ú¿ÁÔÓÙ˜ ∆ÂÏÈÎfi ·Ó¿ÛÙËÌ·™˘Û¯¤ÙÈÛË p
∞Ú¯ÈÎfi ‡„Ô˜ (SDS) r=0,474 <0,01∞ÚÈıÌfi˜ ÂÓ¤ÛˆÓ/‚‰ÔÌ¿‰· r=0,265 0,024∞Ú¯ÈÎfi ‡„Ô˜ ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙËÓ ÔÛÙÈ΋ ËÏÈΛ· (SDS) r=0,384 <0,01TH (SDS) r=0,51 <0,001⁄„Ô˜ ÌËÙ¤Ú·˜ (SDS) r=0,394 <0,01⁄„Ô˜ ·Ù¤Ú· (SDS) r=0,434 <0,001
SDS: standard deviation, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·-ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔʇÏÔ
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·131

·˘ÙÒÓ ·Ú·Ì¤ÙÚˆÓ (Ú=0,06) Î·È ÈÛ¯˘Ú‹ Û˘Û¯¤ÙÈÛË
ÌÂٷ͇ Ù˘ ‰È·ÊÔÚ¿˜ ÙÂÏÈÎÔ‡-·Ú¯ÈÎÔ‡ ·Ó·ÛÙ‹Ì·-
ÙÔ˜ (¢ height) Î·È Ù˘ ‰È¿ÚÎÂÈ·˜ ıÂڷ›·˜
(p=0,001). ∂ȯÂÈÚÒÓÙ·˜ Û‡ÁÎÚÈÛË ÙÔ˘ ÙÂÏÈÎÔ‡
·Ó·ÛÙ‹Ì·ÙÔ˜ ÌÂٷ͇ ÙˆÓ ·È‰ÈÒÓ Ô˘ ÍÂΛÓËÛ·Ó
ıÂڷ›· ÚÈÓ ·fi ÙËÓ ¤Ó·ÚÍË Ù˘ ‹‚˘ Î·È ·˘ÙÒÓ
Ô˘ ÍÂΛÓËÛ·Ó ÌÂÙ¿, ‰È·ÈÛÙÒıËΠˆ˜ ÙÔ ¢ height
‰ÂÓ ‰È¤ÊÂÚ ÛËÌ·ÓÙÈο ÛÙȘ ‰‡Ô ˘ÔÔÌ¿‰Â˜
(p=0,9). ∆· ·È‰È¿ Ô˘ ÍÂΛÓËÛ·Ó ıÂڷ›· ÚÔÂ-
ÊË‚Èο ›¯·Ó ÛËÌ·ÓÙÈο ÌÈÎÚfiÙÂÚÔ ·Ú¯ÈÎfi ‡„Ô˜
(p=0,016) Î·È ÛËÌ·ÓÙÈο ÌÈÎÚfiÙÂÚÔ ÙÂÏÈÎfi ‡„Ô˜
(p=0,037) Û ۯ¤ÛË Ì ٷ ·È‰È¿ Ô˘ ÍÂΛÓËÛ·Ó
·ÁˆÁ‹ ηٿ ÙËÓ ÂÊ˂›·. ∆Ô fiÊÂÏÔ˜ ·fi ÙË ıÂÚ·-
›·, fiˆ˜ ·ÓÙÈηÙÔÙÚ›˙ÂÙ·È ÛÙÔ ÎÂÚ‰Ëı¤Ó ·Ó¿-
ÛÙËÌ·, ‹Ù·Ó ÙÔ ›‰ÈÔ ÛÙȘ ‰‡Ô ·˘Ù¤˜ ˘ÔÔÌ¿‰Â˜.
∂ÓÙÔ‡ÙÔȘ, ÙÔ 54% ÙˆÓ ·È‰ÈÒÓ Ì ¤Ó·ÚÍË ıÂڷ›-
·˜ ÚÔÂÊË‚Èο Êı¿ÓÂÈ ÛÙÔ ‡„Ô˜-ÛÙfi¯Ô, ÂÓÒ ÙÔ
·ÓÙ›ÛÙÔÈ¯Ô ÔÛÔÛÙfi ÁÈ· Ù· ·È‰È¿ Ì ¤Ó·ÚÍË ıÂÚ·-
›·˜ ηٿ ÙËÓ ÂÊ˂›· Â›Ó·È ÌfiÏȘ 18,4% (13,27).
£· Ú¤ÂÈ Ó· ÛËÌÂȈı›, ˆÛÙfiÛÔ, fiÙÈ Ù· ·È‰È¿ Ô˘
ÍÂΛÓËÛ·Ó ·˘ÍËÙÈ΋ ÔÚÌfiÓË ÚÈÓ ·fi ÙËÓ ÂÊ˂›·
‹Ú·Ó ıÂڷ›· ÁÈ· ÛËÌ·ÓÙÈο ÌÂÁ·Ï‡ÙÂÚÔ ¯ÚÔÓÈÎfi
‰È¿ÛÙËÌ· Î·È Û ˘„ËÏfiÙÂÚË ‰fiÛË Û ۯ¤ÛË Ì ٷ
·È‰È¿ Ô˘ ÍÂΛÓËÛ·Ó ıÂڷ›· ηٿ ÙË ‰È¿ÚÎÂÈ·
Ù˘ ÂÊ˂›·˜ (p<0,001 Î·È p=0,001).
∞ÍÈÔÛËÌ›ˆÙÔ Â›Ó·È ˆ˜ ÛÙÔ Û‡ÓÔÏÔ, ÌfiÓÔ Ù· 23
·fi Ù· 72 ·È‰È¿ Ô˘ ÌÂÏÂÙ‹ıËÎ·Ó (32%) ¤ÊÙ·Û·Ó
ÛÙÔ ‡„Ô˜-ÛÙfi¯Ô (∆∏). ™Â 47 ·fi Ù· 72 ·È‰È¿, Ë ‹‚Ë
›¯Â ‹‰Ë ÍÂÎÈÓ‹ÛÂÈ Î·Ù¿ ÙËÓ ¤Ó·ÚÍË Ù˘ ·ÁˆÁ‹˜. ∂›-
Ó·È ÁÓˆÛÙfi fiÙÈ ÙÔ 80-85% Ù˘ ·‡ÍËÛ˘ Ï·Ì‚¿ÓÂÈ ̄ Ò-
Ú· ÚÈÓ ·fi ÙËÓ ‹‚Ë Î·È ¤ÙÛÈ Ù· ·È‰È¿ Ô˘ ÌÂÏÂÙ‹-
ıËÎ·Ó ¤¯·Û·Ó ¤Ó· ÛËÌ·ÓÙÈÎfi ¯ÚÔÓÈÎfi ‰È¿ÛÙËÌ·,
¶›Ó·Î·˜ 6. ™˘ÁÎÚÈÙÈ΋ ·ÍÈÔÏfiÁËÛË Ù˘ ›‰Ú·Û˘ Ù˘ ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘ Ì ·˘ÍËÙÈ΋ ÔÚÌfiÓË ÛÙËÓ ÚÔÂÊË‚È΋ Î·È ÂÊË‚È΋ ËÏÈΛ·
∞ÛıÂÓ›˜ (¡=72) ¶ÚÔÂÊË‚È΋ ËÏÈΛ· ∂ÊË‚È΋ ËÏÈΛ· p
AÚÈıÌfi˜ - º‡ÏÔ 25 (11 ¿ÚÚÂÓ·, 14 ı‹Ï·) 47 (32 ¿ÚÚÂÓ·, 15 ı‹Ï·) 0,01∏ÏÈΛ· ¤Ó·Ú͢ GH (¤ÙË) 8,4±2,39 13,29±1,39 <0,001∞Ú¯ÈÎfi ‡„Ô˜ (SDS) -2,89±1,08 -2,29±0,59 0,016√ÛÙÈ΋ ËÏÈΛ· ηٿ ÙËÓ ¤Ó·ÚÍË GH (¤ÙË) 6,32±2,64 11,18±1,43 <0,001∞Ú¯ÈÎfi ‡„Ô˜ ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙËÓ ÔÛÙÈ΋ ËÏÈΛ· (SDS) -0,855±1,45 -0,67±0,76 0,56∆∏ ‡„Ô˜ (SDS) -0,9±0,78 -0,7±0,71 0,29⁄„Ô˜ ÌËÙ¤Ú·˜ (SDS) -1,06±1,05 -0,83±0,82 0,30⁄„Ô˜ ·Ù¤Ú· (SDS) -0,76±0,89 -0,6±0,93 0,48∆ÂÏÈÎfi ‡„Ô˜ (SDS) -1,56±1,3 -1,04±0,79 0,037∆·¯‡ÙËÙ· ·‡ÍËÛ˘ ηٿ ÙÔ ÚÒÙÔ ¤ÙÔ˜ıÂڷ›·˜ (height velocity) (SDS) 5,93±4,66 6,43±5,14 0,69∏ÏÈΛ· ‰È·ÎÔ‹˜ GH (¤ÙË) 15,36±1,8 16,58±1,34 0,005¢ height (SDS) 1,32±1,37 1,28±0,69 0,9∆ÂÏÈÎfi ‡„Ô˜( SDS)-∆∏ (SDS) -0,66±1,2 -0,36±0,71 0,26¢ÔÛÔÏÔÁ›· GH (IU/kgr/‚‰ÔÌ¿‰·) 0,54±0,13 0,43±0,09 0,001∞ÚÈıÌfi˜ ÂÓ¤ÛˆÓ/‚‰ÔÌ¿‰· 6,08±1,68 6,83±0,82 0,044¢È¿ÚÎÂÈ· ıÂڷ›·˜ (¤ÙË) 6,97±3,13 3,4±1,42 <0,001
SDS: standard deviation, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ(target height), ¢ height: ÙÂÏÈÎfi ‡„Ô˜ (SDS)-·Ú¯ÈÎfi ‡„Ô˜ (SDS)
132 ª. ¶··‰ÔÔ‡ÏÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:128-134
¶›Ó·Î·˜ 5. ∞ÔÙÂϤÛÌ·Ù· ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘ Û ·ÛıÂÓ›˜ Ì ·Ó¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘ Î·È ¤Ó·ÚÍË ıÂڷ›·˜ ˘ÔηٿÛÙ·-Û˘ ηٿ ÙËÓ ÚÔÂÊË‚È΋ ËÏÈΛ·
∞ÛıÂÓ›˜ (¡=25) ª¤ÛÔ˜ fiÚÔ˜ (ÛÙ·ıÂÚ‹ ·fiÎÏÈÛË) ª¤ÁÈÛÙË ÙÈÌ‹ ∂Ï¿¯ÈÛÙË ÙÈÌ‹
∆ÂÏÈÎfi ‡„Ô˜ (SDS) -1,56±1,3 1,22 -5,08∆·¯‡ÙËÙ· ·‡ÍËÛ˘ ηٿ ÙÔ ÚÒÙÔ ¤ÙÔ˜ ıÂڷ›·˜ (height velocity) (SDS) 5,93±4,66 17,97 -0,37∏ÏÈΛ· ‰È·ÎÔ‹˜ GH (¤ÙË) 15,36±1,8 18,1 12,44¢ height (SDS) 1,32±1,37 4,46 -0,88∆ÂÏÈÎfi ‡„Ô˜ (SDS)-TH (SDS) -0,66±1,2 1,75 -3,70¢ÔÛÔÏÔÁ›· GH (IU/kgr/‚‰ÔÌ¿‰·) 0,54±0,13 0,80 0,35∞ÚÈıÌfi˜ ÂÓ¤ÛˆÓ/‚‰ÔÌ¿‰· 6,08±1,68 7,00 3,00¢È¿ÚÎÂÈ· ıÂڷ›·˜ (¤ÙË) 6,97±3,13 14,81 2,72
SDS: standard deviation, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ(target height), ¢ height: ÙÂÏÈÎfi ‡„Ô˜ (SDS)-·Ú¯ÈÎfi ‡„Ô˜ (SDS)
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·132

ÏfiÁˆ ηı˘ÛÙ¤ÚËÛ˘ ÛÙËÓ ·Ó·˙‹ÙËÛË ÂÍÂȉÈÎÂ˘Ì¤-
Ó˘ ·Ú¤Ì‚·Û˘ (28-30).
ªÂÙ¿ ÙËÓ ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜ Ì ·˘ÍËÙÈ΋
ÔÚÌfiÓË, Ù· ·È‰È¿ ‚ÂÏÙÈÒÓÔ˘Ó ÙÔÓ ÂÙ‹ÛÈÔ Ú˘ıÌfi
·‡ÍËÛ˘ ηٿ 2 ÊÔÚ¤˜ Û ۯ¤ÛË Ì ÂΛÓÔÓ ÚÈÓ
·fi ÙË ıÂڷ›·. ŸÛÔ ÌÈÎÚfiÙÂÚÔ Â›Ó·È ÙÔ ·È‰›, Ùfi-
ÛÔ ÌÂÁ·Ï‡ÙÂÚË ‚ÂÏÙ›ˆÛË ÙÔ˘ Ú˘ıÌÔ‡ ·‡ÍËÛ˘ ÂÈ-
Ù˘Á¯¿ÓÂÈ Ì ÙËÓ ¤ÁηÈÚË ¤Ó·ÚÍË Ù˘ ıÂڷ›·˜. ∏
Ù·¯‡ÙËÙ· ·‡ÍËÛ˘ ηٿ ÙÔÓ ÚÒÙÔ ¯ÚfiÓÔ Ù˘ ıÂÚ·-
›·˜ Â›Ó·È Û˘Ó‹ıˆ˜ Î·È Ë Ì¤ÁÈÛÙË Ô˘ ÂÈÙ˘Á¯¿ÓÂ-
Ù·È Î·ı’ fiÏË ÙË ‰È¿ÚÎÂÈ· ¯ÔÚ‹ÁËÛ˘ Ù˘ GH (27). ∏
ÌË ·Ó‡ÚÂÛË ÛÙË ÌÂϤÙË Ì·˜ Û˘Û¯¤ÙÈÛ˘ ÙÔ˘ ÙÂÏÈ-
ÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜ Ì ÙËÓ Ù·¯‡ÙËÙ· ·‡ÍËÛ˘ ηٿ
ÙÔÓ ÚÒÙÔ ¯ÚfiÓÔ Ù˘ ıÂڷ›·˜ ÔÊ›ÏÂÙ·È Èı·ÓÒ˜
ÛÙË ÌÂÁ¿ÏË Û¯ÂÙÈο ËÏÈΛ· ÙˆÓ ·È‰ÈÒÓ Î·Ù¿ ÙËÓ
¤Ó·ÚÍË Ù˘ ıÂڷ›·˜.
™˘ÁÎÚ›ÓÔÓÙ·˜ Ù· ·È‰È¿ Ì ÔÏÏ·Ï‹ ·Ó¿Ú-
ÎÂÈ· ÔÚÌÔÓÒÓ Ì ÂΛӷ Ì ÌÂÌÔӈ̤ÓË ·Ó¿ÚÎÂÈ·
GH, ‰È·ÈÛÙÒıËΠfiÙÈ ÙÔ ÙÂÏÈÎfi ·Ó¿ÛÙËÌ· ‰ÂÓ ‰È¤-
ÊÂÚ ÛÙ·ÙÈÛÙÈÎÒ˜ ÛËÌ·ÓÙÈο ÛÙȘ 2 ˘ÔÔÌ¿‰Â˜,
fiˆ˜ ¤¯ÂÈ ·Ú·ÙËÚËı› Î·È Û ¿ÏϘ ÌÂϤÙ˜
(12,31). ∆Ô 45,5% ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ ¤ÊÙ·Û ÛÙÔ
‡„Ô˜-ÛÙfi¯Ô. ∂ÓÙÔ‡ÙÔȘ, ÙÔ ¢ height ‹Ù·Ó ÛËÌ·ÓÙÈο
ÌÂÁ·Ï‡ÙÂÚÔ (p=0,001) ÛÙ· ·È‰È¿ Ì ÔÏÏ·Ï‹ ·ÓÂ-
¿ÚÎÂÈ· ÔÚÌÔÓÒÓ, Ù· ÔÔ›· Ê·›ÓÂÙ·È Ó· ˆÊÂÏ‹ıË-
Î·Ó ÂÚÈÛÛfiÙÂÚÔ ·fi ÙË ıÂڷ›· (13). £· Ú¤ÂÈ
Ó· ÛËÌÂȈı›, ˆÛÙfiÛÔ, fiÙÈ Ë ·ÚÔ‡Û· ÔÌ¿‰· ÙˆÓ 11
·È‰ÈÒÓ Ì ·Ó¿ÚÎÂÈ· ÔÏÏÒÓ ÔÚÌÔÓÒÓ ·ÚÔ˘Û›·-
˙ ÛËÌ·ÓÙÈο ÌÈÎÚfiÙÂÚË SDS ÁÈ· ÙÔ TH Û ۯ¤ÛË ÌÂ
Ù· ·È‰È¿ Ì ÌÂÌÔӈ̤ÓË ¤ÏÏÂÈ„Ë ·˘ÍËÙÈ΋˜ ÔÚÌfi-
Ó˘ ηÈ, Û˘ÓÂÒ˜, ˘‹Ú¯Â ‰È·ÊÔÚ¿ ˆ˜ ÚÔ˜ ÙÔ ÁÂÓÂ-
ÙÈο ηıÔÚÈṲ̂ÓÔ ·Ó¿ÛÙËÌ·. ∞·ÈÙ›ٷÈ, ÂÔ̤ӈ˜,
ÌÂÁ·Ï‡ÙÂÚÔ˜ ·ÚÈıÌfi˜ ·È‰ÈÒÓ ÁÈ· ÙËÓ ÂÍ·ÁˆÁ‹
·ÛÊ·ÏÒÓ Û˘ÌÂÚ·ÛÌ¿ÙˆÓ .
™˘ÌÂÚ·ÛÌ·ÙÈο, Ù· ·ÔÙÂϤÛÌ·Ù· Ù˘ ÌÂϤÙ˘
Ì·˜, ηıÒ˜ Î·È ¿ÏÏˆÓ ·ÓÙ›ÛÙÔȯˆÓ ÌÂÏÂÙÒÓ ‰ÈÂ-
ıÓÒ˜, ‰Â›¯ÓÔ˘Ó ÌÈ· Û·Ê‹ ‚ÂÏÙ›ˆÛË ÛÙÔ ÙÂÏÈÎfi ·Ó¿-
ÛÙËÌ· Ì ÙË ¯Ú‹ÛË Ù˘ ‚ÈÔÛ˘ÓıÂÙÈ΋˜ GH 6 ‹ 7 ÊÔ-
Ú¤˜ ‚‰ÔÌ·‰È·›ˆ˜, Û ۯ¤ÛË Ì ÙË ¯ÔÚ‹ÁËÛË 3 ‰fiÛÂ-
ˆÓ Ô˘ ·ÔÙÂÏÔ‡ÛÂ Û˘Ó‹ıË Ú·ÎÙÈ΋ ÛÙÔ ·ÚÂÏ-
ıfiÓ. ∂ÓÙÔ‡ÙÔȘ, ÙÔ ÙÂÏÈÎfi ·ÔÙ¤ÏÂÛÌ· ÌÔÚ› Ó·
ÌËÓ Â›Ó·È ÈηÓÔÔÈËÙÈÎfi ÁÈ· fiÏÔ˘˜ ÙÔ˘ ·ÛıÂÓ›˜ ηÈ
ȉ›ˆ˜ ÁÈ· ÂΛÓÔ˘˜ Ô˘ ÍÂΛÓËÛ·Ó ÙËÓ ·ÁˆÁ‹ Û¯ÂÙÈ-
ο ·ÚÁ¿. ∏ ‚ÂÏÙ›ˆÛË ÙÔ˘ Ú˘ıÌÔ‡ ·‡ÍËÛ˘ ηٿ ÙËÓ
ÂÊ˂›· Ê·›ÓÂÙ·È Ó· ··ÈÙ› ÌÈ· ·‡ÍËÛË Î·Ù¿ 50%
ÂÚ›Ô˘ Ù˘ ¯ÔÚËÁÔ‡ÌÂÓ˘ ‰fiÛ˘ ÚÈÓ ·fi ÙËÓ
‹‚Ë. ∆¤ÏÔ˜, ‰ÂÓ ı· Ú¤ÂÈ Ó· ·Ú·‚ϤÂÈ Î·Ó›˜ ÙÔ
ÚfiÏÔ Ô˘ ·›˙ÂÈ ÙÔ ÁÂÓÂÙÈÎfi ‰˘Ó·ÌÈÎfi ÛÙÔÓ Î·ıÔÚÈ-
ÛÌfi ÙÔ˘ ÙÂÏÈÎÔ‡ ·Ó·ÛÙ‹Ì·ÙÔ˜.
µÈ‚ÏÈÔÁÚ·Ê›·
1. Hindmarsh PC, Dattani MT. Use of growth hormone in
children. Nat Clin Pract Endocrinol Metab 2006;2:260-268.
2. ÃÈÒÙ˘ ¢, ∆ÛÈÊÙ‹˜ °, ÷Ù˙ËÛ˘ÌÂÒÓ ª, ª·ÓÈ¿ÙË-
ÃÚËÛÙ›‰Ë ª, ∫Ú›ÎÔ˜ •, ¢¿ÎÔ˘-µÔ˘ÙÂÙ¿ÎË ∞. ∞Ó¿ÛÙËÌ·
Î·È ÛˆÌ·ÙÈÎfi ‚¿ÚÔ˜ ÂÏÏËÓÔ·›‰ˆÓ ËÏÈΛ·˜ 0-18 ÂÙÒÓ
(2001-2002): Û‡ÁÎÚÈÛË Ì ‰Â‰Ô̤ӷ ÌÂϤÙ˘ ÙÔ˘ 1978-
1979. ¢ÂÏÙ›Ô ∞ã ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋˜ 2003;50:136-156.
3. Cavallo A, Richards GE, Busey S, Michaels SE. A simplified
133AÓ¿ÚÎÂÈ· ·˘ÍËÙÈ΋˜ ÔÚÌfiÓ˘
¶·È‰È·ÙÚÈ΋ 2008;71:128-134
¶›Ó·Î·˜ 7. ™˘ÁÎÚÈÙÈ΋ ·ÍÈÔÏfiÁËÛË Ù˘ ›‰Ú·Û˘ Ù˘ ıÂڷ›·˜ ˘ÔηٿÛÙ·Û˘ Ì ·˘ÍËÙÈ΋ ÔÚÌfiÓË Û ·È‰È¿ ÌÂ Û˘Ó‰˘·Ṳ̂ÓË Î·È ·È‰È¿Ì ÌÂÌÔӈ̤ÓË ·Ó¿ÚÎÂÈ· GH
∞ÛıÂÓ›˜ (¡=72) ∞Ó¿ÚÎÂÈ· ªÂÌÔӈ̤ÓË pÔÏÏ·ÏÒÓ ÔÚÌÔÓÒÓ ·Ó¿ÚÎÂÈ· GH
º‡ÏÔ 11 (6 ¿ÚÚÂÓ·, 5 ı‹Ï·) 61 (37 ¿ÚÚÂÓ·, 24 ı‹Ï·) NS∏ÏÈΛ· ¤Ó·Ú͢ GH (¤ÙË) 10,26±3,38 11,83±2,82 0,1∞Ú¯ÈÎfi ‡„Ô˜ (SDS) -2,91±0,78 -2,42±0,83 0,075√ÛÙÈ΋ ËÏÈΛ· ηٿ ÙËÓ ¤Ó·ÚÍË GH (¤ÙË) 7,17±3,71 9,91±2,71 0,005∞Ú¯ÈÎfi ‡„Ô˜ ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙËÓ ÔÛÙÈ΋ ËÏÈΛ· (SDS) -0,52±1,05 -0,77±1,05 0,47∆∏ ‡„Ô˜ (SDS) -0,183±1,02 -0,88±0,63 0,003⁄„Ô˜ ÌËÙ¤Ú·˜ (SDS) -0,5±1,41 -0,98±0,78 0,29⁄„Ô˜ ·Ù¤Ú· (SDS) 0,08±0,87 -0,79±0,86 0,003∆ÂÏÈÎfi ‡„Ô˜ (SDS) -0,75±1,18 -1,31±0,97 0,091∆·¯‡ÙËÙ· ·‡ÍËÛ˘ ηٿ ÙÔ ÚÒÙÔ ¤ÙÔ˜ ıÂڷ›·˜ (height velocity) (SDS) 6,62±4,71 6,19±5,03 0,79∏ÏÈΛ· ‰È·ÎÔ‹˜ GH (¤ÙË) 16,8±1,07 16,04±1,67 0,15¢ height (SDS) 2,17±1,1 1,14±0,87 0,001∆ÂÏÈÎfi ‡„Ô˜ (SDS)-∆∏ (SDS) -0,56±1,01 -0,45±0,9 0,71¢ÔÛÔÏÔÁ›· GH (IU/kgr/‚‰ÔÌ¿‰·) 0,52±0,14 0,46±0,11 0,14∞ÚÈıÌfi˜ ÂÓ¤ÛˆÓ/‚‰ÔÌ¿‰· 6±1,73 6,67±1,11 0,24¢È¿ÚÎÂÈ· ıÂڷ›·˜ (¤ÙË) 6,55±3,2 4,29±2,54 0,011
SDS: standard deviation, GH: ·˘ÍËÙÈ΋ ÔÚÌfiÓË, ∆∏: ·Ó·ÌÂÓfiÌÂÓÔ ÁÈ· ÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ‡„Ô˜, ÚÔÛ·ÚÌÔṲ̂ÓÔ ÛÙÔ Ê‡ÏÔ(target height), NS: non significant, ¢ height: ÙÂÏÈÎfi ‡„Ô˜ (SDS)-·Ú¯ÈÎfi ‡„Ô˜ (SDS)
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·133

gonadotrophin-releasing hormone test for precocious pu-berty. Clin Endocrinol (Oxf) 1995;42:641-646.
4. Wit JM, Kamp GA, Rikken B. Spontaneous growth and re-sponse to growth hormone treatment in children withgrowth hormone deficiency and idiopathic short stature.Pediatr Res 1996;39:295-302.
5. De Angelis R, di Natale B, Lukezic M, Bozzato N, Mora C,Pozzobon G, Vigano G, Chiumello G. Final height in idio-pathic growth hormone deficient children after optimizedrhGH treatment [abstract]. Horm Res 1997;48:149.
6. Barsanti S, Saggese G. Final height in children with growthhormone deficiency treated with recombinant growth hor-mone (abstract). Horm Res 1997;48:151.
7. Brämswig JH, Schlösser H, Kiese K. Final height in chil-dren with growth hormone deficiency. Horm Res1995;43:126-128.
8. De Luca F, Maghnie M, Arrigo T, Lombardo F, MessinaMF, Bernasconi S. Final height outcome of growth hor-mone-deficient patients treated since less than five years ofage. Acta Paediatr 1996;85:1167-1171.
9. Coste J, Letrait M, Carel JC, Tresca JP, Chatelain P, Rochic-cioli P, et al. Long-term results of growth hormone treat-ment in France in children of short stature: population,register based study. BMJ 1997;315:708-713.
10. Cacciari E, Cicognani A, Pirazzoli P, Zucchini S, Salardi S,Balsamo A, et al. Final height of patients treated for isolat-ed GH deficiency: examination of 83 patients. Eur J En-docrinol 1997 Jul;137:53-60.
11. Thomas M, Massa G, Bourguignon JP, Craen M, DeSchepper J, de Zegher F, et al. Final height in children withidiopathic growth hormone deficiency treated with recom-binant growth hormone: the Belgian experience. HormRes 2001;55:88-94.
12. Karavanaki K, Kontaxaki C, Maniati-Christidi M, PetrouV, Dacou-Voutetakis C. Growth response, pubertalgrowth and final height in Greek children with growthhormone (GH) deficiency on long-term GH therapy andfactors affecting outcome. J Pediatr Endocrinol Metab2001;14:397-405.
13. Reiter EO, Price DA, Wilton P, Albertsson-Wikland K,Ranke MB. Effect of growth hormone (GH) treatment onthe near-final height of 1258 patients with idiopathic GHdeficiency: analysis of a large international database. J ClinEndocrinol Metab 2006;91:2047-2054.
14. Burns EC, Tanner JM, Preece MA, Cameron N. Finalheight and pubertal development in 55 children with idio-pathic growth hormone deficiency, treated for between 2and 15 years with human growth hormone. Eur J Pediatr1981;137:155-164.
15. Lenko HL, Leisti S, Perheentupa J. The efficacy of growthhormone in different types of growth failure. An analysis of101 cases. Eur J Pediatr 1982;138:241-249.
16. Joss E, Zuppinger K, Schwarz HP, Roten H. Final height ofpatients with pituitary growth failure and changes ingrowth variables after long term hormonal therapy. Pedia-tr Res 1983;17:676-679.
17. Job JC, Joab N, Toublanc JE, Canlorbe P. Résultats à termedes traitments par l’hormone de croissance humaine. ArchFr Pediatr 1984;41:477-482.
18. Hibi I, Tanaka T, Tanae A, Kagawa J, Hashimoto N,
Yoshizawa A, et al. The influence of gonadal function andthe effect of gonadal suppression treatment on final heightin growth hormone (GH)-treated GH-deficient children. JClin Endocrinol Metab 1989;69:221-226.
19. Ranke MB, Butenandt O. Idiopathic growth hormone de-ficiency: final height to treatment with growth hormoneand effects of puberty and sex steroids. In: Frisch H, ZaronZ, editors. Induction of puberty in hypopituitarism.Serono Symposia Review No. 16. Rome: Ares-Serono Sym-posia; 1988. p. 84-89.
20. Ranke MB, Guilbaud O. Growth response in prepubertalchildren with idiopathic growth hormone deficiency dur-ing the first two years of treatment with human growthhormone. Analysis of the Kabi Pharmacia InternationalGrowth Stydy. Acta Paediatr Scand Suppl 1991;379:109-115.
21. Radetti G, D’Addato G, Gatti D, Bozzola M, Adami S. In-fluence of two different GH dosage regimens on finalheight, bone geometry and bone strength in GH-deficientchildren. Eur J Endocrinol 2006;154:479-482.
22. Ranke MB, Price DA, Albertsson-Wikland K, Maes M,Lindberg A. Factors determining pubertal growth and finalheight in growth hormone treatment of idiopathic growthhormone deficiency. Analysis of 195 Patients of the KabiPharmacia International Growth Study. Horm Res1997;48:62-71.
23. Ranke MB, Guilbaud O, Lindberg A, Cole T. Prediction ofthe growth response in children with various growth disor-ders treated with growth hormone: analyses of data fromthe Kabi Pharmacia International Growth Study. Interna-tional Board of the Kabi Pharmacia International GrowthStudy. Acta Paediatr Suppl 1993;82 Suppl 391:82-88.
24. Hakeem V, Hindmarsh PC, Brook CG. Intermittent versuscontinuous administration of growth hormone treatment.Arch Dis Child 1993;68:783-784.
25. Hilczer M, Smyczy‹ska J, Lewi‹ski A. Parentally-adjusteddeficit of height as a prognostic factor of the effectivenessof growth hormone (GH) therapy in children with GH de-ficiency. Neuro Endocrinol Lett 2006;27:149-152.
26. Chen YD, Shu SG, Chi CS. Growth response and finalheight in growth hormone-deficient patients treated withbiosynthetic growth hormone. Acta Paediatr Taiwan2001;42:291-296.
27. Bajpai A, Kabra M, Gupta AK, Menon PS. Growth patternand skeletal maturation following growth hormone thera-py in growth hormone deficiency: factors influencing out-come. Indian Pediatr 2006;43: 593-599.
28. Frisch H, Birnbacher R. Final height and pubertal develop-ment in children with growth hormone deficiency afterlong-term treatment. Horm Res 1995;43:132-134.
29. August GP, Julius JR, Blethen SL. Adult height in childrenwith growth hormone deficiency who are treated withbiosynthetic growth hormone: the National CooperativeGrowth Study experience. Pediatrics 1998;102:512-516.
30. Saggese G, Federico G, Barsanti S. Growth Hormone Defi-ciency. In: Hindmarsh PC, editor. Current Indications forGrowth Hormone Therapy. Endocr Dev. Basel, Karger,1999, vol 1, pp 55-67.
31. Severi F. Final height in children with growth hormone de-ficiency. Horm Res 1995;43:138-140.
134 ª. ¶··‰ÔÔ‡ÏÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:128-134
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·134

135∂ƒ∂À¡∏∆π∫∏ ∂ƒ°∞™π∞ ORIGINAL ARTICLE
¶·È‰È·ÙÚÈ΋ 2008;71:135-140
ªÂϤÙË ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ Û ·È‰È¿ Ì Ïԛ̈ÍË ·fi Èfi
Epstein-Barr Î·È ÌÂÁ·ÏÔ΢ÙÙ·ÚÔ˚fi Î·È Û˘Û¯¤ÙÈÛË Ì ÙËÓ ÎÏÈÓÈ΋
¤Î‚·ÛË
∂. ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË1, ∞. ºÏ¤‚·2, µ. ∞ÓÙ¿ÚË1, ∞. ¶·˘Ï›ÙÔ˘-∆ÛÈfiÓÙÛË2, ª. ªÔÛÎÔÊ›‰Ë˜3, °. µ·ÚÏ¿Ì˘1
¶ÂÚ›ÏË„Ë
∂ÈÛ·ÁˆÁ‹: ™ÎÔfi˜ Ù˘ ÂÚÁ·Û›·˜ ‹Ù·Ó Ë ÌÂϤÙË ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ ÙˆÓ ·È‰ÈÒÓ Ì ۇӉÚÔÌÔ ÏÔÈ-ÌÒ‰Ô˘˜ ÌÔÓÔ˘Ú‹ÓˆÛ˘ (™§ª) ηٿ ÙËÓ ÔÍ›· Ê¿ÛË Î·È ÌÂÙ¿ ÙËÓ ·Ô‰ÚÔÌ‹ Ù˘ Ïԛ̈͢, ηıÒ˜ ηÈË Û˘Û¯¤ÙÈÛ‹ ÙÔ˘ Ì ÙËÓ ÎÏÈÓÈ΋ ¤Î‚·ÛË.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ: ªÂÏÂÙ‹ıËÎ·Ó 26 ·È‰È¿ Ì ™§ª, Ì ̤ÛÔ fiÚÔ ËÏÈΛ·˜ 6,6±3,5 ¤ÙË. ¶·Ú·ÎÔÏÔ˘ı‹ıËÎÂË ÎÏÈÓÈ΋ ÂÈÎfiÓ· Î·È ÔÚ›· Î·È ¤ÁÈÓ ¤ÏÂÁ¯Ô˜ Ì ˘ÂÚ˯ÔÁÚ¿ÊËÌ· ÛÏËÓfi˜, ̤ÙÚËÛË ÙˆÓ ·ÓÙÈ-ÈÈÎÒÓ ·ÓÙÈ-ۈ̿وÓ, ÁÂÓÈ΋ ·›Ì·ÙÔ˜, ÚÔÛ‰ÈÔÚÈÛÌfi ÙÚ·ÓÛ·ÌÈÓ·ÛÒÓ, Á-GT, ·ÓÔÛÔÛÊ·ÈÚÈÓÒÓ (IgG, IgA, IgM) Î·È ÙˆÓ΢ÙÙ·ÚÈÎÒÓ ˘ÔÏËı˘ÛÌÒÓ, ∆ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ (CD3+, CD3+/CD4+, CD3+/CD8+), µ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ(CD19+) Î·È Ê˘ÛÈÎÒÓ Î˘ÙÙ·ÚÔÎÙfiÓˆÓ (CD3-/CD16+56+) ηٿ ÙËÓ ÔÍ›· Ê¿ÛË Î·È ÌÂÙ¿ ·fi 3-6 Ì‹Ó˜.
∞ÔÙÂϤÛÌ·Ù·: ∆Ô 69% ÙˆÓ ·È‰ÈÒÓ ·ÚÔ˘Û›·˙ Ïԛ̈ÍË ·fi Èfi Epstein-Barr (EBV), ÂÓÒ ÙÔ 31% ·fi ÌÂÁ·-ÏÔ΢ÙÙ·ÚÔ˚fi (CMV). ∫·Ù¿ ÙÔÓ Â·Ó¤ÏÂÁ¯Ô, ·Ú·ÙËÚ‹ıËΠ̛ˆÛË ÙˆÓ ÂȤ‰ˆÓ IgM Î·È ·‡ÍËÛË ÙˆÓ IgG·ÓÙÈ-ÈÈÎÒÓ ·ÓÙÈÛˆÌ¿ÙˆÓ Ì ·Ú¿ÏÏËÏË ÎÏÈÓÈ΋ ·ÔηٿÛÙ·ÛË. ∏ ÛÏËÓÔÌÂÁ·Ï›·, Ë ÏÂÌÊÔ΢ÙÙ¿ÚˆÛË Î·È Ë·‡ÍËÛË ÙˆÓ ÙÚ·ÓÛ·ÌÈÓ·ÛÒÓ ˘Ô¯ÒÚËÛ·Ó ÛËÌ·ÓÙÈο. ∏ ˘ÂÚÁ·ÌÌ·ÛÊ·ÈÚÈÓ·ÈÌ›·, ΢ڛˆ˜ Ù˘ IgM, ·Ôη-Ù·ÛÙ¿ıËÎÂ. ∫·Ù¿ ÙËÓ ÔÍ›· Ïԛ̈ÍË, Ù· CD3+/CD8+ ·ÚÔ˘Û›·Û·Ó ÛËÌ·ÓÙÈ΋ ·‡ÍËÛË, Ì ÂÏ¿ÙÙˆÛË ÙÔ˘ ÏfiÁÔ˘CD4+/CD8+, ÂÓÒ Ù· CD19+ Î·È Ù· CD3+/CD4+ ‹Ù·Ó ÂÏ·Ùو̤ӷ. ™ÙÔÓ Â·Ó¤ÏÂÁ¯Ô, Ù· CD3+ Î·È CD3+/CD8+ ·-ÚÔ˘Û›·˙·Ó ÛËÌ·ÓÙÈ΋ ÂÏ¿ÙÙˆÛË, ÂÓÒ Ù· CD3+/CD4+, Ù· CD19+ Î·È Ô ÏfiÁÔ˜ CD4+/CD8+ ·ÚÔ˘Û›·˙·Ó ·‡ÍËÛË.
™˘ÌÂÚ¿ÛÌ·Ù·: ∆· CD3+/CD8+ ∆ ÏÂÌÊÔ·ÙÙ·Ú· ·ÔÙÂÏÔ‡Ó ÙËÓ Î˘ÙÙ·ÚÔÙÔÍÈ΋ ∆ ÏÂÌÊÔ΢ÙÙ·ÚÈ΋ ·¿-ÓÙËÛË ÛÙ· EBV Î·È CMV ·ÓÙÈÁfiÓ· Î·È Ë Ì›ˆÛ‹ ÙÔ˘˜ Û¯ÂÙ›˙ÂÙ·È Ì ÙËÓ ‡ÊÂÛË Ù˘ Û˘Ìو̷ÙÔÏÔÁ›·˜.∞fi ÙË ÌÂϤÙË ÚÔ·ÙÂÈ Ë ̄ ÚËÛÈÌfiÙËÙ· ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ ÁÈ· ÙËÓ ·Ú·ÎÔÏÔ‡ıËÛË ÙˆÓ ·È‰ÈÒÓ Ì™§ª Ô˘ ¯ÚÔÓ›˙ÂÈ.
§¤ÍÂȘ ÎÏÂȉȿ: ∞ÓÔÛÔÊ·ÈÓfiÙ˘Ô˜, EBV, CMV Ïԛ̈ÍË, ÎÏÈÓÈ΋ ¤Î‚·ÛË.
Study of the immunophenotype of peripheral blood lymphocyte
subsets in children with Epstein-Barr virus and cytomegalovirus
infection: association with outcome
E. Papadopoulou-Alataki1, A. Fleva2, V. Antari1, A. Pavlitou-Tsiontsi2, M. Moskofidis3, G. Varlamis1
Abstract
Background: The purpose of this study was to identify the immunophenotype of children withinfectious mononucleosis during the acute phase of the disease and convalescence and to investigateits association with the disease outcome.
Methods: A study was made of 26 children aged 6.6±3.5 years, affected by infectious mononucleosis. Theclinical presentation, spleen size, peripheral blood count, anti-virus specific antibodies, levels of SGOT,SGPT, Á-GT, IgG, IgA and IgM, and immunophenotype of blood T, B and NK cells were studied during theacute phase and 3-6 months later.
Results: Of the 26 children, 69% were infected by Epstein-Barr virus (EBV) and 31% by cytomegalovirus(CMV). At 3-6 month reevaluation a significant decrease in IgM and an increase in IgG antivirus antibodieswere observed, and the splenomegaly, lymphocytosis and high initial levels of SGOT were restored tonormal. At the time of onset of symptoms, the CD3+/CD8+ cells were considerably increased, CD19+ andCD3+/CD4+ percentages were low and a marked lowering of the CD4+/CD8+ ratio was observed. Atreevaluation, CD3+ and CD3+/CD8+ were lower, while CD3+/CD4+, CD19+ cells and the CD4+/CD8+ ratiowere significantly increased.
Conclusions: The increase in CD3+/CD8+ cells represents the cytotoxic response to the proliferation of EBVand CMV antigens, and may be related with the remission of symptoms. Immunophenotyping ofperipheral blood could be helpful in the follow-up of children with persistent infectious mononucleosis.
Key words: Immunophenotype, EBV, CMV infection, clinical outcome.
1 ¢’ ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋∞¶£, °ÂÓÈÎfi ¡ÔÛÔÎÔÌ›ԓ¶··ÁˆÚÁ›Ô˘”,£ÂÛÛ·ÏÔÓ›ÎË
2 ∂ÚÁ·ÛÙ‹ÚÈÔ ∞ÓÔÛÔÏÔÁ›·˜-πÛÙÔÛ˘Ì‚·ÙfiÙËÙ·˜, °ÂÓÈÎfi¡ÔÛÔÎÔÌ›ԓ¶··ÁˆÚÁ›Ô˘”,£ÂÛÛ·ÏÔÓ›ÎË
3 ªÈÎÚÔ‚ÈÔÏÔÁÈÎfi-µÈÔ¯ËÌÈÎfi-πÔÏÔÁÈÎfi∆Ì‹Ì·, °ÂÓÈÎfi¡ÔÛÔÎÔÌ›ԓ¶··ÁˆÚÁ›Ô˘”,£ÂÛÛ·ÏÔÓ›ÎË
AÏÏËÏÔÁÚ·Ê›·:
∂˘ÊËÌ›· ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË [email protected] °ÂÓÈÎfi ¡ÔÛÔÎÔÌ›ԓ¶··ÁˆÚÁ›Ô˘”,¶ÂÚÈÊÂÚÂȷ΋ Ô‰fi˜¡. ∂˘Î·Ú›·, ∆.∫. 564 03, £ÂÛÛ·ÏÔÓ›ÎË
1 4th Department ofPaediatrics, AristotleUniversity of Thessaloniki,Papageorgiou GeneralHospital, Thessaloniki
2 Immunology-HistocompatibilityLaboratory, PapageorgiouGeneral Hospital,Thessaloniki
3 Microbiological-Biochemical-VirologicalDepartment,Papageorgiou GeneralHospital, Thessaloniki
Correspondence:
Efimia [email protected] Papageorgiou GeneralHospital, Ring road,564 03, ¡. Efkarpia, Thessaloniki, Greece
Pediatri Mar-Apr 08 07-04-08 17:16 ™ÂÏ›‰·135

136 ∂. ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË Î·È Û˘Ó.
Paediatriki 2008;71:135-140
™˘ÓÙÔÌÔÁڷʛ˜
EBV πfi˜ Epstein-Barr
CMV ªÂÁ·ÏÔ΢ÙÙ·ÚÔ˚fi˜
™§ª ™‡Ó‰ÚÔÌÔ §ÔÈÌÒ‰Ô˘˜ ªÔÓÔ˘Ú‹ÓˆÛ˘
§ª §ÔÈÌ҉˘ ªÔÓÔ˘Ú‹ÓˆÛË
SGOT OÍ·ÏÔÍÈ΋ ÙÚ·ÓÛ·ÌÈÓ¿ÛË
SGPT ¶˘ÚÔÛÙ·Ê˘ÏÈ΋ ÙÚ·ÓÛ·ÌÈÓ¿ÛË
Á-GT Á-ÁÏÔ˘Ù·Ì˘ÏÔÙÚ·ÓÛÊÂÚ¿ÛË
CD3+ flÚÈÌ· ∆ ÏÂÌÊÔ·ÙÙ·Ú· Ì TCR ˘Ô‰Ô¯¤·
CD3+/CD4+ µÔËıËÙÈο ∆ ÏÂÌÊÔ·ÙÙ·Ú·
CD3+/CD8+ ∫·Ù·ÛÙ·ÏÙÈο/΢ÙÙ·ÚÔÙÔÍÈο ∆ ÏÂÌÊÔ-
·ÙÙ·Ú·
CD19+ µ ÏÂÌÊÔ·ÙÙ·Ú·
CD3-/16+56+ º˘ÛÈο ΢ÙÙ·ÚÔÎÙfiÓ· (NK)
∂ÈÛ·ÁˆÁ‹
∏ §ÔÈÌ҉˘ ªÔÓÔ˘Ú‹ÓˆÛË (§ª) Â›Ó·È ¤Ó·
ÎÏÈÓÈÎfi Û‡Ó‰ÚÔÌÔ Ô˘ ¯·Ú·ÎÙËÚ›˙ÂÙ·È ·fi ˘ÚÂÙfi,
Ê·Ú˘ÁÁÔ·Ì˘Á‰·Ï›Ùȉ· Î·È ÏÂÌÊ·‰ÂÓÔ¿ıÂÈ·. ∞Ó Î·È
Ë ÏÂÈÔÓfiÙËÙ· ÙˆÓ ÂÚÈÙÒÛÂˆÓ ÔÊ›ÏÔÓÙ·È ÛÙÔÓ Èfi
Epstein-Barr (EBV), ÏÔÈÌÒÍÂȘ ·fi ¿ÏÏ· ·›ÙÈ·, fiˆ˜
Ô ÌÂÁ·ÏÔ΢ÙÙ·ÚÔ˚Ô˜ (CMV), Ô ÂÚËÙÔ˚fi˜ 6 (HSV), Ô
Èfi˜ Ù˘ ·ÓıÚÒÈÓ˘ ·ÓÔÛÔ·Ó¿ÚÎÂÈ·˜ (HIV), ÔÈ
·‰ÂÓÔ˚Ô›, Ô Èfi˜ Ù˘ ÂÚ˘ıÚ¿˜, Ô Èfi˜ Parvo µ19, ÔÈ ÈÔ›
Ù˘ Ë·Ù›Ùȉ·˜ ∞ Î·È µ, ÙÔ ÙÔÍfiÏ·ÛÌ·, ·ÚÔ˘ÛÈ¿-
˙Ô˘Ó ·ÚfiÌÔÈ· ÎÏÈÓÈ΋ Î·È ·ÈÌ·ÙÔÏÔÁÈ΋ ÂÈÎfiÓ· ηÈ
ÚÔηÏÔ‡Ó ÙÔ Û‡Ó‰ÚÔÌÔ Ù˘ ÏÔÈÌÒ‰Ô˘˜ ÌÔÓÔ˘Ú‹-
ÓˆÛ˘ (™§ª) (1-3).
∏ ‰È¿ÁÓˆÛË Ù˘ ÚfiÛÊ·Ù˘ Ïԛ̈͢ ‚·Û›˙Â-
Ù·È ÛÙËÓ ·ÚÔ˘Û›· ·ÓÙÈ-ÈÈÎÒÓ ·ÓÙÈÛˆÌ¿ÙˆÓ Ù˘ Ù¿-
͢ IgM. ∂ȉÈο ÁÈ· ÙÔÓ EBV, Ë ·Ó›¯Ó¢ÛË ·ÓÙÈÛˆ-
Ì¿ÙˆÓ Î·Ù¿ ÙˆÓ Î·„ȉÈÎÒÓ, ÚÒÈÌˆÓ Î·È ˘ÚËÓÈ-
ÎÒÓ ·ÓÙÈÁfiÓˆÓ ˘Ô‚ÔËıÔ‡Ó ÙË ‰È¿ÁÓˆÛË. ∏ ·-
ÚÔ˘Û›· ·ÓÙÈη„ȉÈÎÒÓ ·ÓÙÈÛˆÌ¿ÙˆÓ Î·È Ë ·Ô˘Û›·
·ÓÙÈ˘ÚËÓÈÎÒÓ ·ÓÙÈÛˆÌ¿ÙˆÓ Â›Ó·È ÂÓ‰ÂÈÎÙÈΤ˜ Ù˘
ÔÍ›·˜ Ïԛ̈͢, ‰ÈfiÙÈ Ù· EBV ·ÓÙÈ˘ÚËÓÈο ·ÓÙÈ-
ÛÒÌ·Ù· ÂÌÊ·Ó›˙ÔÓÙ·È Î·Ù¿ ÙË ‰È¿ÚÎÂÈ· Ù˘ ·Ó¿Ú-
ÚˆÛ˘ (4,5).
∏ ÔÍ›· §ª Â›Ó·È Û˘Ó‹ıˆ˜ ·˘ÙÔÂÚÈÔÚÈ˙fiÌÂÓË
ÓfiÛÔ˜ (6). øÛÙfiÛÔ, Û ÔÚÈṲ̂ÓÔ˘˜ ·ÛıÂÓ›˜ ηٷϋ-
ÁÂÈ Û ¯ÚfiÓÈ· ÂÓÂÚÁfi Ïԛ̈ÍË Ô˘ ¯·Ú·ÎÙËÚ›˙ÂÙ·È
·fi ˘ÔÙÚÔ¤˜ ÙˆÓ Û˘ÌÙˆÌ¿ÙˆÓ Î·È Ùˆ¯‹ Úfi-
ÁÓˆÛË (7,8). ∞ÔÙÂÏ› ÌÈ· ÛÔ‚·Ú‹ ·Ûı¤ÓÂÈ· ÌÂ
¿ÁÓˆÛÙË ·ıÔÁ¤ÓÂÈ· Ô˘ ÂÈ̤ÓÂÈ ¿Óˆ ·fi 3-6
Ì‹Ó˜ ¤ˆ˜ Î·È ¯ÚfiÓÈ·, ÂÓÒ ÌÔÚ› Ó· ·ÚÔ˘ÛÈ·ÛÙ›
Î·È Û ¿ÙÔÌ· Ì ηϋ ·ÓÔÛÔÏÔÁÈ΋ ηٿÛÙ·ÛË (9-
11). ∂ÈϤÔÓ, Û ·È‰È¿ Ì ‰È·Ù·Ú·¯‹ ÙˆÓ ∆ ÏÂÌ-
ÊÔ΢ÙÙ¿ÚˆÓ, Ë EBV Ïԛ̈ÍË Ô‰ËÁ› Û˘¯Ó¿ Û ¯Úfi-
ÓÈ· ÂÓÂÚÁfi Ïԛ̈ÍË Ì Èı·Ó‹ ÂͤÏÈÍË Û ηÎÔ‹ıÂÈ·
ÙÔ˘ ÏÂÌÊÈÎÔ‡ ÈÛÙÔ‡. ™Â ÔÚÈṲ̂ÓÔ˘˜ ·ÛıÂÓ›˜, Ë §ª
ÌÔÚ› Ó· ·ÎÔÏÔ˘ı‹ÛÂÈ ÂÈıÂÙÈ΋ ÔÚ›· Ì ·ÂÈ-
ÏËÙÈΤ˜ ÁÈ· ÙË ˙ˆ‹ ÂÈÏÔΤ˜ (7,12,13).
™ÎÔfi˜ Ù˘ ·ÚÔ‡Û·˜ ÌÂϤÙ˘ ‹Ù·Ó Ë ·Ó·˙‹ÙËÛË
ÙˆÓ ·ÓÔÛÔÏÔÁÈÎÒÓ ÌÂÙ·‚ÔÏÒÓ ÙˆÓ ·È‰ÈÒÓ Ì ™§ª
ηٿ ÙËÓ ÔÍ›· Ê¿ÛË Î·È ÌÂÙ¿ ÙËÓ ·Ô‰ÚÔÌ‹ Ù˘ ÏÔ›-
̈͢, ηıÒ˜ Î·È Ë ‰ÈÂÚ‡ÓËÛË Ù˘ Û¯¤Û˘ ÙÔ˘˜ ÌÂÙËÓ ÎÏÈÓÈ΋ ¤Î‚·ÛË Î·È ÙËÓ ÂÁηٿÛÙ·ÛË ·ÓÔÛ›·˜.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ
ªÂÏÂÙ‹ıËÎ·Ó 26 ·ÛıÂÓ›˜, 15 ·ÁfiÚÈ· Î·È 11 ÎÔÚ›ÙÛÈ·, ËÏÈ-Λ·˜ 2-14 ÂÙÒÓ, Ì ̤ÛÔ fiÚÔ ËÏÈΛ·˜ 6,6±3,5 ¤ÙË. √È ·ÛıÂÓ›˜ÓÔÛËχıËÎ·Ó ÛÙËÓ ÎÏÈÓÈ΋ Ì·˜ ηٿ ÙË ‰È¿ÚÎÂÈ· ÙˆÓ ÂÙÒÓ2005-2006 Î·È ÏËÚÔ‡Û·Ó Ù· ÂÍ‹˜ ‰È·ÁÓˆÛÙÈο ÎÚÈÙ‹ÚÈ·: ·)ÙÔ˘Ï¿¯ÈÛÙÔÓ ÙÚ›· ·fi Ù· ·Ú·Î¿Ùˆ: ˘ÚÂÙfi˜, Ê·Ú˘ÁÁÔ·Ì˘-Á‰·Ï›Ùȉ·, ÙÚ·¯ËÏÈ΋ ÏÂÌÊ·‰ÂÓ›Ùȉ·, ÛÏËÓÔÌÂÁ·Ï›·, ÙÚ·Ó-Û·ÌÈÓ·Û·ÈÌ›· Î·È ‚) ıÂÙÈο IgM ·ÓÙÈÛÒÌ·Ù· ˆ˜ ÚÔ˜ EBV ‹CMV. √ ¤ÏÂÁ¯Ô˜ ·ÓÙÈÛˆÌ¿ÙˆÓ ¿ÏÏˆÓ ·ÈÙ›ˆÓ Ô˘ ÂÓ¤¯ÔÓÙ·ÈÛÙÔ ™§ª (ÂÚËÙÔ˚Ô‡ 6, Parvo B19, ·‰ÂÓÔ˚Ô‡ Î·È ÙÔÍÔÏ¿ÛÌ·-ÙÔ˜) ·¤‚Ë ·ÚÓËÙÈÎfi˜. ∫·Ó¤Ó·˜ ·fi ÙÔ˘˜ ·ÛıÂÓ›˜ Ì·˜ ‰ÂÓ Â›-¯Â ÁÓˆÛÙ‹ ·ÓÔÛÔ·Ó¿ÚÎÂÈ· ‹ ·ÓÔÛÔηٷÛÙÔÏ‹. √ ÛÎÔfi˜Ù˘ ÌÂϤÙ˘ ÂÍËÁ‹ıËΠÛÙÔ˘˜ ÁÔÓ›˜ Î·È fiÏÔÈ ÔÈ ÁÔÓ›˜ ¤‰ˆ-Û·Ó ÁÚ·Ù‹ Û˘ÁηٿıÂÛË ÚÈÓ ·fi ÙËÓ ¤Ó·ÚÍË Ù˘ ÌÂϤÙ˘.
™Â fiÏ· Ù· ·È‰È¿ ¤ÁÈÓ ÎÏÈÓÈ΋ ÂͤٷÛË Î·È Î·Ù·ÁÚ·Ê‹ÙˆÓ ÎÏÈÓÈÎÒÓ Â˘ÚËÌ¿ÙˆÓ, ηıÒ˜ Î·È ˘ÂÚ˯ÔÁÚ·ÊÈÎfi˜ ¤ÏÂÁ-¯Ô˜ ÙÔ˘ ÛÏËÓfi˜. ∆· ·È‰È¿ Ù˘ ÌÂϤÙ˘ Ù·ÍÈÓÔÌ‹ıËÎ·Ó Û‰‡Ô ÔÌ¿‰Â˜, ·Ó¿ÏÔÁ· Ì ÙÔ ·›ÙÈÔ Ù˘ Ïԛ̈͢: Ë Ì›· ÔÌ¿‰·ÂÚÈÂÏ¿Ì‚·Ó 18 ·È‰È¿ Ô˘ ›¯·Ó ıÂÙÈο EBV IgM ·ÓÙÈÛÒ-Ì·Ù· Î·È Ë ¿ÏÏË ÂÚÈÂÏ¿Ì‚·Ó 8 ·È‰È¿ Ô˘ ›¯·Ó ıÂÙÈοCMV IgM ·ÓÙÈÛÒÌ·Ù·. √ ÂÚÁ·ÛÙËÚÈ·Îfi˜ ¤ÏÂÁ¯Ô˜ ÂÚÈÂÏ¿Ì-‚·ÓÂ: ÁÂÓÈ΋ ·›Ì·ÙÔ˜, SGOT, SGPT, Á-GT, ·ÓÔÛÔÛÊ·ÈÚ›Ó˜IgG, IgA, IgM Î·È ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô ∆, µ Î·È ¡∫ ÏÂÌÊÔ΢ÙÙ¿-ÚˆÓ. ∆ÚÂȘ ¤ˆ˜ ¤ÍÈ Ì‹Ó˜ ÌÂÙ¿, ¤ÁÈÓ ÂÎÙ›ÌËÛË Ù˘ ÎÏÈÓÈ΋˜ÔÚ›·˜ Î·È Â·Ó¿ÏË„Ë ÙÔ˘ ÂÚÁ·ÛÙËÚÈ·ÎÔ‡ ÂϤÁ¯Ô˘.
∏ ·Ó›¯Ó¢ÛË ·ÓÙÈÛˆÌ¿ÙˆÓ IgG ¤Ó·ÓÙÈ ÙÔ˘ ÌÂÁ·ÏÔ΢ÙÙ·-ÚÔ˚Ô‡, ÙÔ˘ ·‰ÂÓÔ˚Ô‡ Î·È ÙÔ˘ ÙÔÍÔÏ¿ÛÌ·ÙÔ˜ (Toxoplasmagondii) ¤ÁÈÓ ÔÛÔÙÈο, Ë ‰Â ·Ó›¯Ó¢ÛË ·ÓÙÈÛˆÌ¿ÙˆÓ IgM¤ÁÈÓ ÔÈÔÙÈο Ì ÙË ÌÈÎÚÔۈ̷Ùȉȷ΋ ·ÓÔÛÔÂÓ˙˘ÌÈ΋ ̤-ıÔ‰Ô (MEIA, Axsym, Abbott). ∏ ·Ó›¯Ó¢ÛË ÙˆÓ ·ÓÙÈۈ̿وÓIgG Î·È IgM ¤Ó·ÓÙÈ ÙÔ˘ η„ȉÈÎÔ‡ ·ÓÙÈÁfiÓÔ˘ ÙÔ˘ EBV (EBV-VCA IgG/IgM, Virotech), ÙÔ˘ HSV (HSV-IgG/IgM, Virotech)Î·È ÙÔ˘ Parvo µ19 (Parvovirus B19 IgG/IgM, Focus) ¤ÁÈÓ·Ó ÌÂÙËÓ ¤ÌÌÂÛË ·ÓÔÛÔÂÓ˙˘ÌÈ΋ ̤ıÔ‰Ô (Elisa). √ ÚÔÛ‰ÈÔÚÈÛÌfi˜ÙˆÓ ΢ÙÙ·ÚÈÎÒÓ ÏËı˘ÛÌÒÓ (CD3+, CD3+/CD4+, CD3+/CD8+,CD19+, CD3-/CD16+56+, ÏfiÁÔ˘ CD4+/CD8+) ¤ÁÈÓ Ì ΢ÙÙ·-ÚÔÌÂÙÚ›· ÚÔ‹˜ Û ·Ó·Ï˘Ù‹ Epics Elite ESP, Coulter Î·È Ì Ù˯ڋÛË ÌÔÓÔÎψÓÈÎÒÓ ·ÓÙÈÛˆÌ¿ÙˆÓ Ù˘ ÂÙ·ÈÚ›·˜ BeckmanCoulter, Immunotech. ∏ ÔÛÔÙÈ΋ ̤ÙÚËÛË ÙˆÓ ·ÓÔÛÔÛÊ·È-ÚÈÓÒÓ (IgG, IgA Î·È πgM) Ú·ÁÌ·ÙÔÔÈ‹ıËΠ̠ÙË ÓÂÊÂÏÔ-ÌÂÙÚÈ΋ ̤ıÔ‰Ô ÛÙÔÓ ·Ó·Ï˘Ù‹ Beckman Immage ¯ÚËÛÈÌÔ-ÔÈÒÓÙ·˜ ·ÓÙȉڷÛÙ‹ÚÈ· Ù˘ ÂÙ·ÈÚ›·˜ Beckman Coulter.
™Ù·ÙÈÛÙÈ΋ ·Ó¿Ï˘ÛË
∏ ÛÙ·ÙÈÛÙÈ΋ ·Ó¿Ï˘ÛË ÙˆÓ ‰Â‰ÔÌ¤ÓˆÓ ¤ÁÈÓ Ì ÙË ¯Ú‹ÛËÙÔ˘ ÛÙ·ÙÈÛÙÈÎÔ‡ ÚÔÁÚ¿ÌÌ·ÙÔ˜ SPSS 11.0. ∏ ‰È·‰Èηۛ· ÛÙ·ÙÈ-ÛÙÈ΋˜ ·Ó¿Ï˘Û˘ ÂÚÈÂÏ¿Ì‚·Ó ̆ ÔÏÔÁÈÛÌfi ÁÈ· οı ÌÂÙ·‚ÏË-Ù‹ Ù˘ ̤Û˘ ÙÈÌ‹˜ (mean) Î·È Ù˘ Ù˘È΋˜ ·fiÎÏÈÛ˘ (SD).
∏ Û‡ÁÎÚÈÛË ÙˆÓ ÂÚÁ·ÛÙËÚÈ·ÎÒÓ Î·È ÎÏÈÓÈÎÒÓ ·Ú·Ì¤ÙÚˆÓÌÂٷ͇ ÙˆÓ ÔÌ¿‰ˆÓ ÙˆÓ ·È‰ÈÒÓ ¤ÁÈÓ Ì t-test. √ Û¯ÂÙÈÎfi˜Û˘ÓÙÂÏÂÛÙ‹˜ Pearson ̆ ÔÏÔÁ›ÛıËΠÁÈ· ÙËÓ ÂÚ·ÈÙ¤Úˆ ·Ó¿Ï˘-ÛË Ù˘ Û˘Û¯¤ÙÈÛ˘ ÌÂٷ͇ ÙˆÓ Î˘ÙÙ·ÚÈÎÒÓ ˘ÔÏËı˘ÛÌÒÓÎ·È ÙˆÓ ¿ÏÏˆÓ ÂÚÁ·ÛÙËÚÈ·ÎÒÓ Î·È ÎÏÈÓÈÎÒÓ ·Ú·Ì¤ÙÚˆÓ. ø˜fiÚÈÔ ÛÙ·ÙÈÛÙÈ΋˜ ÛËÌ·ÓÙÈÎfiÙËÙ·˜ ıˆڋıËÎÂ Ë ÙÈÌ‹ p<0,05.
∞ÔÙÂϤÛÌ·Ù·
∞fi Ù· 26 ·È‰È¿ Ù˘ ÌÂϤÙ˘, Ù· 18 ›¯·Ó EBVÏԛ̈ÍË, ÂÓÒ Ù· ˘fiÏÔÈ· ›¯·Ó CMV Ïԛ̈ÍË. √
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·136

¯ÚfiÓÔ˜ ÓÔÛËÏ›·˜ Î˘Ì·ÈÓfiÙ·Ó ·fi 3 ¤ˆ˜ Î·È 10
Ë̤Ú˜.
√ ˘ÚÂÙfi˜ ‹Ù·Ó ÙÔ Û‡Ìو̷ Ô˘ ·ÚÔ˘Û›·˙·Ó
fiÏ· Ù· ·È‰È¿ Î·È ·ÔÙ¤ÏÂÛ ÙËÓ Î‡ÚÈ· ·ÈÙ›· ÚÔÛ¤-
Ï¢Û˘. ∆ËÓ ÎÏ·ÛÈ΋ ÎÏÈÓÈ΋ ÙÚÈ¿‰· (˘ÚÂÙfi˜, ÏÂÌ-
Ê·‰ÂÓ›Ùȉ· Î·È Ê·Ú˘ÁÁÔ·Ì˘Á‰·Ï›Ùȉ·) ·ÚÔ˘Û›·ÛÂ
ÙÔ 65% ÙˆÓ ·È‰ÈÒÓ. √›‰ËÌ· ‚ÏÂÊ¿ÚˆÓ ‰È·ÈÛÙÒ-
ıËÎÂ ÛÙÔ 23%, ·fiÊÚ·ÍË ·ÂÚÔÊfiÚˆÓ Ô‰ÒÓ 23%,
ÂÍ¿ÓıËÌ· 11%, ÂÚÈηډ›Ùȉ· 11%, ÂÓÒ Ó¢ÌÔÓ›·,
·ÁÎÚ·ٛÙȉ· Î·È ·Ó΢ÙÙ·ÚÔÂÓ›· ·fi ¤Ó· ·È‰›
·ÓÙ›ÛÙÔȯ·.
ŸÏ· Ù· ·È‰È¿ Ù˘ ÌÂϤÙ˘ ·ÚÔ˘Û›·Û·Ó ·‡ÍËÛË
ÙÔ˘ ÌÂÁ¤ıÔ˘˜ ÙÔ˘ ÛÏËÓfi˜ ¿Óˆ ·fi Ù· ·ÓÒÙÂÚ·
fiÚÈ· ÁÈ· ÙËÓ ËÏÈΛ· ÙÔ˘˜, Û‡Ìʈӷ Ì ÙÔÓ ˘ÂÚ˯Ô-
ÁÚ·ÊÈÎfi ¤ÏÂÁ¯Ô. ∆Ô Ì¤ÁÂıÔ˜ ÙÔ˘ ÛÏËÓfi˜ ‹Ù·Ó
11,5±1,9 cm ÛÙËÓ ÔÌ¿‰· EBV Î·È 9,8±1,8 cm ÛÙËÓ
ÔÌ¿‰· CMV (p=0,04).
∞fi ÙËÓ ·Ó¿Ï˘ÛË ÙÔ˘ ÂÚÈÊÂÚÈÎÔ‡ ·›Ì·ÙÔ˜ ‚Ú¤-
ıËΠfiÙÈ ÙÔ 77% ÙˆÓ ·ÛıÂÓÒÓ Â›¯Â ÔÛÔÛÙfi ÏÂÌÊÔ-
΢ÙÙ¿ÚˆÓ >50% ÙˆÓ Û˘ÓÔÏÈÎÒÓ Ï¢ÎÒÓ Î·È ·fiÏ˘-
ÙÔ ·ÚÈıÌfi ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ >5000, ÂÓÒ ÛÙÔ 54%
‚Ú¤ıËÎ·Ó ¿Ù˘· ÏÂÌÊÔ·ÙÙ·Ú· Û ÔÛÔÛÙfi 4-29%
ÙÔ˘ Û˘ÓfiÏÔ˘ ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ. ™ÙÔ 81% ‰È·È-
ÛÙÒıËΠ·‡ÍËÛË Ù˘ SGOT Î·È Ù˘ SGPT. √È Ì¤Û˜
ÙÈ̤˜ ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ, ÙˆÓ ¿Ù˘ˆÓ ÏÂÌÊÔ΢Ù-Ù¿ÚˆÓ Î·È ÙˆÓ Ë·ÙÈÎÒÓ ‰ÂÈÎÙÒÓ Ê·›ÓÔÓÙ·È ÛÙÔÓ¶›Ó·Î· 1.
ÀÂÚÁ·ÌÌ·ÛÊ·ÈÚÈÓ·ÈÌ›·, ÙÔ˘Ï¿¯ÈÛÙÔÓ Û ̛· Ù¿ÍË·ÓÔÛÔÛÊ·ÈÚÈÓÒÓ, ·ÚÔ˘Û›·Û ÙÔ 69% ÙˆÓ ·È‰ÈÒÓÛÙËÓ IgM 53% Î·È ÛÙËÓ IgG 16%. ∞fi ÙËÓ ·ÓÔÛÔÊ·È-ÓÔÙ˘È΋ ·Ó¿Ï˘ÛË ÙÔ˘ ÂÚÈÊÂÚÈÎÔ‡ ·›Ì·ÙÔ˜, ÚԤ΢-„ fiÙÈ ÙÔ 58% ÙˆÓ ·È‰ÈÒÓ ÂÌÊ¿ÓÈ˙ ·‡ÍËÛË ÙˆÓCD3+ (̤ÛÔ˜ fiÚÔ˜ >80%), ÙÔ 46% ÂÏ¿ÙÙˆÛË ÙˆÓCD3+/CD4+ Î·È ÙÔ 58% ÂÏ¿ÙÙˆÛË ÙˆÓ CD19+ (ηÙÒ-ÙÂÚË ÙÈÌ‹ 1,9%). ™Â fiÏ· Ù· ·È‰È¿ ·Ú·ÙËÚ‹ıËΠÛË-Ì·ÓÙÈ΋ ·‡ÍËÛË ÙˆÓ CD3+/CD8+ Ì ۇÁ¯ÚÔÓË ÂÏ¿Ù-ÙˆÛË ÙÔ˘ ÏfiÁÔ˘ CD4+/CD8+ Ô˘ Î˘Ì·ÈÓfiÙ·Ó ·fi 0,12¤ˆ˜ Î·È 1. ∫·Ó¤Ó· ·È‰› ‰ÂÓ Â›¯Â ·ıÔÏÔÁÈ΋ ÙÈÌ‹ ÙˆÓCD3-/CD16+56+. ∞fi ÙË Û‡ÁÎÚÈÛË ÙˆÓ Ì¤ÛˆÓ ÙÈÌÒÓÙˆÓ ·Ú·¿Óˆ ·Ú·Ì¤ÙÚˆÓ ‰ÂÓ ‚Ú¤ıËÎ·Ó ÛËÌ·ÓÙÈ-Τ˜ ‰È·ÊÔÚ¤˜ ÌÂٷ͇ ÙˆÓ ·È‰ÈÒÓ Ì EBV Ïԛ̈ÍËÎ·È CMV Ïԛ̈ÍË Î·Ù¿ ÙËÓ ÔÍ›· Ê¿ÛË (¶›Ó·Î·˜ 2).
∫·Ù¿ ÙÔÓ Â·Ó¤ÏÂÁ¯Ô, fiÏ· Ù· ·È‰È¿ ‹Ù·Ó ÂχıÂ-Ú· Û˘ÌÙˆÌ¿ÙˆÓ Î·È ·ÚÔ˘Û›·˙·Ó Ì›ˆÛË ÙˆÓ ÂÈ-¤‰ˆÓ IgM Î·È ·‡ÍËÛË ÙˆÓ IgG ·ÓÙÈ-ÈÈÎÒÓ ·ÓÙÈۈ̿-ÙˆÓ, ÏËÓ Ì›·˜ ·ÛıÂÓÔ‡˜, Ù˘ ÔÔ›·˜ Ë ·Ó¿ÚÚˆÛˉȋÚÎÂÛ 8 Ì‹Ó˜. ™ÙÔ Û‡ÓÔÏÔ ÙˆÓ ·ÛıÂÓÒÓ, Ë Ì¤ÛËÙÈÌ‹ ÙÔ˘ ÌÂÁ¤ıÔ˘˜ ÙÔ˘ ÛÏËÓfi˜ (8,7±1,4 cm) ‹Ù·ÓÛËÌ·ÓÙÈο ¯·ÌËÏfiÙÂÚË (p<0,001), Û ۇÁÎÚÈÛË ÌÂÙËÓ ·ÓÙ›ÛÙÔÈ¯Ë Ù˘ ÔÍ›·˜ Ïԛ̈͢. √È Ì¤Û˜ ÙÈ̤˜Ù˘ ÂηÙÔÛÙÈ·›·˜ ·Ó·ÏÔÁ›·˜ ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ(47±10%), ÙÔ˘ ·fiÏ˘ÙÔ˘ ·ÚÈıÌÔ‡ ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿-ÚˆÓ (3817±1136/Ìl), Ù˘ IgM (1±0,4 g/L) ‹Ù·Ó ÛÙ·ÙÈ-ÛÙÈο ¯·ÌËÏfiÙÂÚ˜ (p<0,001), ÂÓÒ ÔÈ Ì¤Û˜ ÙÈ̤˜ Ù˘IgG (11,4±3,1 g/L) Î·È Ù˘ IgA (1,7±1 g/L) ‰ÂÓ Â›¯·ÓÛÙ·ÙÈÛÙÈο ÛËÌ·ÓÙÈΤ˜ ÌÂÙ·‚ÔϤ˜. √È Ì¤Û˜ ÙÈ̤˜ÙˆÓ CD3+ (72±5%), ÙˆÓ CD3/+CD8+ (26±6%) ‹Ù·ÓÛËÌ·ÓÙÈο ¯·ÌËÏfiÙÂÚ˜ (p<0,001), ÂÓÒ ÙˆÓCD3+/CD4+ (38±7%) Î·È CD19+ (18,37±12,7%) ‹Ù·ÓÛËÌ·ÓÙÈο ·˘ÍË̤Ó˜. ¢ÂÓ ·Ú·ÙËÚ‹ıËΠη̛··ÍÈÔÛËÌ›ˆÙË ÌÂÙ·‚ÔÏ‹ ÛÙ· ¡∫ ·ÙÙ·Ú· (∂ÈÎfiÓ· 1).∏ ̤ÛË ÙÈÌ‹ ÙÔ˘ ÏfiÁÔ˘ CD4+/CD8+ (1,55±0,6) ‹Ù·ÓÛËÌ·ÓÙÈο ˘„ËÏfiÙÂÚË ÛÙÔÓ Â·Ó¤ÏÂÁ¯Ô Û ۇÁÎÚÈÛËÌ Ù˘ ÔÍ›·˜ Ïԛ̈͢ (p<0,001) (∂ÈÎfiÓ· 2).
∏ ‰ÔÎÈÌ·Û›· Pearson ¤‰ÂÈÍ fiÙÈ ÙÔ Ì¤ÁÂıÔ˜ ÙÔ˘
¶›Ó·Î·˜ 1. ∫ÏÈÓÈο ¯·Ú·ÎÙËÚÈÛÙÈο, ·ÈÌ·ÙÔÏÔÁÈÎÔ› Î·È Ë·ÙÈÎÔ› ‰Â›ÎÙ˜ ÙˆÓ ·È‰ÈÒÓ Ì ™§ª ηٿ ÙËÓ ÂÈÛ·ÁˆÁ‹
™‡ÓÔÏÔ EBV Ïԛ̈ÍË CMV Ïԛ̈ÍË p
∞ÛıÂÓ›˜ 26 18 8∏ÏÈΛ· (¤ÙË) 6,6±3,5 7±3,6 5,7±3,1 ª™ÃÚfiÓÔ˜ ÓÔÛËÏ›·˜ (Ë̤Ú˜) 6,2±1,9 6,3±1,8 6±2,4 ª™§Â˘Î¿ (Î/Ìl) 15.917±7.130 14.828±6.008 18.366±9.159 ª™§ÂÌÊÔ·ÙÙ·Ú· (%) 57,1±10,31 56,51±10,3 58,42±10,3 ª™ÕÙ˘· ÏÂÌÊÔ·ÙÙ·Ú· (%) 14,6±7,17 14,37±7,15 15,25±8,3 ª™SGPT (U/L) 147±130 173±160 84±51 ª™SGOT (U/L) 110±84,38 124±96 77,14±27,5 ª™
ª™: ªË ÛÙ·ÙÈÛÙÈο ÛËÌ·ÓÙÈÎfi
137∞ÓÔÛÔÊ·ÈÓfiÙ˘Ô˜ ·È‰ÈÒÓ Ì EBV Î·È CMV Ïԛ̈ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:135-140
82%72%
23%38%
49%26%
8%18%
10% 9%
10% 60% 0% 20% 30% 40% 50% 70% 80% 90%
√Í›· Ïԛ̈ÍË ∂·Ó¤ÏÂÁ¯Ô˜
CD3+
CD3+/CD4+
CD3+/CD8+
CD19+
NK
∂ÈÎfiÓ· 1. ª¤Û˜ ÙÈ̤˜ ̆ ÔÏËı˘ÛÌÒÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ ÙˆÓ ·È-‰ÈÒÓ Ì ™§ª ÛÙËÓ ÔÍ›· Ïԛ̈ÍË Î·È ÛÙÔÓ Â·Ó¤ÏÂÁ¯Ô.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·137

ÛÏËÓfi˜ ›¯Â ıÂÙÈ΋ Û˘Û¯¤ÙÈÛË Ì ٷ CD3+/CD8+
ÏÂÌÊÔ·ÙÙ·Ú· Î·È ·ÚÓËÙÈ΋ Û˘Û¯¤ÙÈÛË Ì ÙÔ ÏfiÁÔ
CD4+/CD8+. ªÂٷ͇ Ù˘ IgA Î·È ÙˆÓ Ë·ÙÈÎÒÓ ‰ÂÈ-
ÎÙÒÓ ‚Ú¤ıËΠıÂÙÈ΋ Û˘Û¯¤ÙÈÛË, ÂÓÒ ·ÚÓËÙÈ΋ ‹Ù·Ó
Ë Û˘Û¯¤ÙÈÛË ÌÂٷ͇ Ù˘ IgA Î·È ÙˆÓ CD3+/CD4+ ηÈ
ÙÔ˘ ÏfiÁÔ˘ CD4+/CD8+ Î·È ÈÛ¯˘Ú¿ ıÂÙÈ΋ Ì ٷ
CD3+/CD8+. ∏ IgG ›¯Â ıÂÙÈ΋ Û˘Û¯¤ÙÈÛË Ì ÙËÓ IgA
Î·È Ù· CD3+/CD8+ (¶›Ó·Î·˜ 3).
∞fi ÙÔ Û‡ÓÔÏÔ ÙˆÓ ·È‰ÈÒÓ Ô˘ ·ÓÂϤÁ¯ıË-
ηÓ, ÙÚ›· ·È‰È¿ (‰‡Ô ·ÁfiÚÈ· Î·È ¤Ó· ÎÔÚ›ÙÛÈ) ËÏÈ-
Λ·˜ 9-11 ÂÙÒÓ, ·ÚÔ˘Û›·˙·Ó ηٷ‚ÔÏ‹ Î·È ÌÂȈ̤-
ÓË ‰Ú·ÛÙËÚÈfiÙËÙ·. ∆· ‰‡Ô ·fi ·˘Ù¿ ›¯·Ó Ïԛ̈ÍË
·fi EBV Î·È ·¤ÎÙËÛ·Ó ·ÓÔÛ›· 3 Ì‹Ó˜ ÌÂÙ¿ ÙËÓ
ÔÍ›· Ê¿ÛË. ™ÙÔ ÙÚ›ÙÔ ·È‰›, ÎÔÚ›ÙÛÈ, Ì CMV ÏÔ›-
̈ÍË, Ë ÂÁηٿÛÙ·ÛË ·ÓÔÛ›·˜ ηı˘ÛÙ¤ÚËÛÂ, Ì ÂÈ-
ÌÔÓ‹ ÙˆÓ ·ÓÙÈ-CMV IgM ·ÓÙÈÛˆÌ¿ÙˆÓ Â› 8 Ì‹Ó˜,
ÙˆÓ ÔÔ›ˆÓ Ô Ù›ÙÏÔ˜ ÛÙ·‰È·Î¿ ÌˉÂÓ›ÛÙËÎÂ Î·È ·-
Ú·ÙËÚ‹ıËÎÂ ÂÈÎÚ¿ÙËÛË ÙˆÓ ·ÓÙÈ-CMV IgG ·ÓÙÈ-
ۈ̿وÓ. ∆ËÓ ·ÈÌ·ÙÔÏÔÁÈ΋ ÙÔ˘˜ ÂÈÎfiÓ· ¯·Ú·ÎÙ‹-
ÚÈ˙ ›ÌÔÓË ÏÂÌÊÔ΢ÙÙ¿ÚˆÛË (>50%), ηıÒ˜ ηÈ
·ÚÔ˘Û›· ¿Ù˘ˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ Â› 3 Ì‹Ó˜. ∏
·Ú·ÎÔÏÔ‡ıËÛË ÙˆÓ ˘ÔÏËı˘ÛÌÒÓ ÙˆÓ ÏÂÌÊÔ-
΢ÙÙ¿ÚˆÓ ¤‰ÂÈÍ fiÙÈ ÛÙËÓ ÔÍ›· Ê¿ÛË Ù· ‰‡Ô ·È‰È¿
Ì EBV Ïԛ̈ÍË Î·È ÙÔ ¤Ó· ·È‰› Ì CMV Ïԛ̈ÍË
›¯·Ó ˘„ËÏ¿ CD3+/CD8+: 40%, 70% Î·È 70% ·ÓÙ›-
ÛÙÔȯ·, ÂÓÒ Ô ÏfiÁÔ˜ CD4+/CD8+ ‹Ù·Ó ¯·ÌËÏfi˜: 0,5,
0,15 Î·È 0,23 ·ÓÙ›ÛÙÔȯ·. ™ÙÔ ·È‰› Ì ÙË CMV ÏÔ›-
̈ÍË, Ô ÏfiÁÔ˜ CD4+/CD8+ ·Ú¤ÌÂÈÓ <1 ÁÈ· ¯ÚÔÓÈÎfi
‰È¿ÛÙËÌ· ÌÂÁ·Ï‡ÙÂÚÔ ÙˆÓ 8 ÌËÓÒÓ.
™˘˙‹ÙËÛË
™ÙË ÌÂϤÙË Ì·˜ ‰È·ÈÛÙÒıËΠfiÙÈ Ù· ·È‰È¿ ÌÂ
ÔÍ›· EBV Î·È CMV Ïԛ̈ÍË ·ÚÔ˘Û›·Û·Ó ·‡ÍËÛË
ÙˆÓ CD8+ ∆ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ, Ù· ÔÔ›· ÂÏ·ÙÙÒıËηÓ
·Ú¿ÏÏËÏ· Ì ÙËÓ ÎÏÈÓÈ΋ ·ÔηٿÛÙ·ÛË. ∞Ó¿ÏÔ-
Á˜ ÌÂϤÙ˜, ·Ó·ÊÔÚÈο Ì ÙÔÓ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô
ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ ÙˆÓ ·È‰ÈÒÓ Î·Ù¿ ÙË ‰È¿ÚÎÂÈ·
Ù˘ ·Ó¿ÚÚˆÛ˘, Â›Ó·È Ôχ ÂÚÈÔÚÈṲ̂Ó˜ Î·È ·ÊÔ-
ÚÔ‡Ó ÌfiÓÔ ÙÔÓ EBV (14,15). √ EBV ·ÔÙ¤ÏÂÛ ·›ÙÈÔ
ÙÔ˘ ™§ª ÛÙÔ 69% ÙˆÓ ·È‰ÈÒÓ, Û˘¯ÓfiÙËÙ· ̄ ·ÌËÏfi-
ÙÂÚË ·fi ÙÔ 85-90% ÚÔËÁÔ‡ÌÂÓ˘ ÌÂϤÙ˘ ÛÂ
ÂÓ‹ÏÈΘ (3). ∏ ̤ÛË ËÏÈΛ· ÓfiÛËÛ˘ ‹Ù·Ó 6,6 ¤ÙË,
CD
4+/C
D8+
√Í›· Ïԛ̈ÍË ∂·Ó¤ÏÂÁ¯Ô˜
4
3
2
1
0
-1
∂ÈÎfiÓ· 2. ¢È·Î‡Ì·ÓÛË ÙˆÓ ÙÈÌÒÓ ÙÔ˘ ÏfiÁÔ˘ CD4+/CD8+ Î·È Ë Ì¤-ÛË ÙÈÌ‹ ÙÔ˘ (ÔÚÈ˙fiÓÙÈ· ÁÚ·ÌÌ‹ ÂÓÙfi˜ ÙˆÓ ·Ú·ÏÏËÏÔÁÚ¿Ì̈Ó)ÛÙÔ˘˜ ‰È·ÊÔÚÂÙÈÎÔ‡˜ ¯ÚfiÓÔ˘˜ ̤ÙÚËÛ˘. TÔ 1o Î·È 3o ÙÂÙ·ÚÙË-ÌfiÚÈÔ (25% Î·È 75% ÙˆÓ ·Ú·ÙËÚ‹ÛˆÓ) ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È Ì ÙËÓ¿Óˆ Î·È Î¿Ùˆ ÏÂ˘Ú¿ ÙÔ˘ ·Ú·ÏÏËÏÔÁÚ¿ÌÌÔ˘. √È ÔÚÈ˙fiÓÙȘÁÚ·Ì̤˜ Ô˘ ÚÔ‚¿ÏÏÔ˘Ó ÂÎÙfi˜ ÙÔ˘ ·Ú·ÏÏËÏÔÁÚ¿ÌÌÔ˘ ‰ËÏÒ-ÓÔ˘Ó ÙÔ ·ÓÙ›ÛÙÔÈ¯Ô 95% ‰È¿ÛÙËÌ· ÂÌÈÛÙÔÛ‡Ó˘ Ù˘ ̤Û˘ ÙÈÌ‹˜ÙÔ˘ ÏfiÁÔ˘ CD4+/CD8+.
¶›Ó·Î·˜ 2. ∞ÓÔÛÔÛÊ·ÈÚ›Ó˜ Î·È ˘ÔÏËı˘ÛÌÔ› ∆ Î·È µ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ ÙˆÓ ·ÛıÂÓÒÓ Ì ™§ª ηٿ ÙËÓ ÂÈÛ·ÁˆÁ‹
™‡ÓÔÏÔ EBV Ïԛ̈ÍË CMV Ïԛ̈ÍË p
IgG (g/L) 13±3,9 13,5±4,1 12,1±3,3 ª™IgA (g/L) 2,1±1,3 2,1±1,1 2,2±1,7 ª™IgM (g/L) 2,2±0,9 2,2±0,9 2,15±1,04 ª™CD3+ (%) 82±9 78,6±10,2 81,1±6,5 ª™CD3+/CD4+ (%) 22,9±10,6 22,3±10,1 24,2±12,5 ª™CD3+/CD8+ (%) 48,5±15,5 47,8±14,3 49,9±17,5 ª™CD19+ (%) 7,7±4,9 7,8±4,3 7,4±6,2 ª™CD3-/CD16+56+ (%) 9,4±3,7 9,3±3,2 9,4±4,9 ª™CD4+/CD8+ 0,4±0,3 0,5±0,3 0,4±0,2 ª™
ª™: ªË ÛÙ·ÙÈÛÙÈο ÛËÌ·ÓÙÈÎfi
138 ∂. ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË Î·È Û˘Ó.
Paediatriki 2008;71:135-140
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·138

ȉȷÈÙ¤Úˆ˜ ¯·ÌËÏ‹ Û ۇÁÎÚÈÛË Ì ÙËÓ ·Ó·ÊÂÚfiÌÂ-ÓË Û ¿ÏϘ ÌÂϤÙ˜, ÔÈ Ôԛ˜ ˘ÔÛÙËÚ›˙Ô˘Ó fiÙÈ ËÏԛ̈ÍË Â›Ó·È Û˘¯ÓfiÙÂÚË Û ÂÊ‹‚Ô˘˜ Î·È Ó·ÚÔ‡˜ÂÓ‹ÏÈΘ ˘„ËÏÒÓ ÎÔÈÓˆÓÈÎÔÔÈÎÔÓÔÌÈÎÒÓ ÔÌ¿‰ˆÓ(16), ηıÒ˜ Î·È Û ËÏÈ˘ 10-19 ÂÙÒÓ, ȉ›ˆ˜ Û ÎÏÂÈ-ÛÙÔ‡˜ ÏËı˘ÛÌÔ‡˜ ÛÙÚ·ÙȈÙÈÎÒÓ Î·È ÊÔÈÙËÙÒÓ(17). ™Â ¿ÙÔÌ· ¯·ÌËÏÔ‡ ÎÔÈÓˆÓÈÎÔÔÈÎÔÓÔÌÈÎÔ‡ ÂÈ-¤‰Ô˘ Î·È Û ÙÚÔÈΤ˜ Î·È ·Ó·Ù˘ÛÛfiÌÂÓ˜ ¯ÒÚ˜,Ë Ïԛ̈ÍË Â›Ó·È Û·ÓÈfiÙÂÚË Î·È ÂÌÊ·Ó›˙ÂÙ·È Î˘Ú›ˆ˜Û ÌÈÎÚ‹ ·È‰È΋ ËÏÈΛ· ˆ˜ ·Û˘Ìو̷ÙÈ΋ (9,18).
√ CMV ˘‹ÚÍ ·ÍÈÔÛËÌ›ˆÙÔ ·›ÙÈÔ ™§ª, ηıÒ˜ÚÔÛ¤‚·Ï 8 ·fi Ù· 26 ·È‰È¿ Ù˘ ÌÂϤÙ˘. ŸÌˆ˜,‰ÂÓ Â›Ó·È ‰˘Ó·Ùfi Ó· ÂÍ·¯ıÔ‡Ó Û¯ÂÙÈο ·ÍÈfiÈÛÙ· Û˘-ÌÂÚ¿ÛÌ·Ù· ÛÙË Û‡ÁÎÚÈÛË ÙˆÓ Â˘ÚËÌ¿ÙˆÓ ÙˆÓ ·È-‰ÈÒÓ Ì CMV Î·È EBV Ïԛ̈ÍË, ÏfiÁˆ ÙÔ˘ ÌÈÎÚÔ‡‰Â›ÁÌ·ÙÔ˜ ÙˆÓ ·ÛıÂÓÒÓ.
ø˜ ÚÔ˜ ÙËÓ ÎÏÈÓÈ΋ ÂÈÎfiÓ·, ÔÈ ÂΉËÏÒÛÂȘ ›ӷÈÌÂÓ ¯·Ú·ÎÙËÚÈÛÙÈΤ˜, ·ÏÏ¿ fi¯È ÂȉÈΤ˜, fiˆ˜ ÂÚÈ-ÁÚ¿ÊÂÙ·È Î·È ·ÏÏÔ‡ (19). ŸÏ· Ù· ·È‰È¿ Ù˘ ÌÂϤÙ˘̷˜ ·ÚÔ˘Û›·Û·Ó ˘ÚÂÙfi Î·È ÛÏËÓÔÌÂÁ·Ï›· ηٿÙË ‰È¿ÚÎÂÈ· Ù˘ ÔÍ›·˜ Ïԛ̈͢. ∆· Û˘ÌÙÒÌ·Ù··˘Ù¿ ›¯·Ó ÌÂÁ·Ï‡ÙÂÚË Û˘¯ÓfiÙËÙ· ·fi Ù· ·ÓÙ›ÛÙÔÈ-¯· (84% Î·È 64%) Û ·Ó¿ÏÔÁË ÌÂϤÙË (14). ŸÛÔÓ·ÊÔÚ¿ ÙȘ ·Ú·ÙËÚÔ‡ÌÂÓ˜ ÎÏÈÓÈΤ˜ ÂÈÏÔΤ˜, Ë·fiÊÚ·ÍË ÙˆÓ ·ÓÒÙÂÚˆÓ ·Ó·Ó¢ÛÙÈÎÒÓ Ô‰ÒÓ ÂÌ-Ê·Ó›ÛÙËΠ۠Ôχ ÏÈÁfiÙÂÚ· ·È‰È¿ (23%) ÛÙË ÌÂ-ϤÙË Ì·˜ Û ۇÁÎÚÈÛË Ì ٷ ·È‰È¿ (64%) Ù˘ ·Óˆ-Ù¤Úˆ ÌÂϤÙ˘, ÂÓÒ ÙÔ Ô›‰ËÌ· ‚ÏÂÊ¿ÚˆÓ ·Ú·ÙËÚ‹-ıËΠÛÙÔ ›‰ÈÔ ÂÚ›Ô˘ ÔÛÔÛÙfi (23% Î·È 29% ·ÓÙ›-ÛÙÔȯ·). ¶Ï‹Ú˘ ·Ó¿ÚÚˆÛË ·Ú·ÙËÚ‹ıËΠ۠¯ÚÔ-ÓÈÎfi ‰È¿ÛÙËÌ· 3-6 ÌËÓÒÓ ÛÙÔ Û‡ÓÔÏÔ ÙˆÓ ·È‰ÈÒÓ,ÂÎÙfi˜ ·fi Ì›· ·ÛıÂÓ‹, ÁÂÁÔÓfi˜ Ô˘ ‰È·Ê¤ÚÂÈ ·fiÙȘ ÌÂϤÙ˜ Û ÂÓ‹ÏÈΘ, fiÔ˘ Ë ‰È¿ÚÎÂÈ· ‹Ù·Ó ÌÂÁ·-χÙÂÚË ·fi 6 Ì‹Ó˜ (19,20). ™ÙÔ ‰È¿ÛÙËÌ· ·˘Ùfi, ÔÈÂÓ‹ÏÈΘ Ì¿ÏÏÔÓ ·Ú·Ì¤ÓÔ˘Ó ÌÂÙ·‰ÔÙÈÎÔ›, fiˆ˜ÚÔ·ÙÂÈ ·fi ÙËÓ ÂÈÌÔÓ‹ ÙÔ˘ ˘„ËÏÔ‡ ∂µV DNAÊÔÚÙ›Ô˘ ÛÙÔ Û›ÂÏfi ÙÔ˘˜ (21).
§ÂÌÊÔ΢ÙÙ¿ÚˆÛË ·Ú·ÙËÚ‹ıËΠÛÙÔ 77% وӷȉÈÒÓ Û ۇÁÎÚÈÛË Ì ÙÔ 32% Î·È ÙÔ 85% ¿ÏÏˆÓ ÌÂ-ÏÂÙÒÓ Û ÂÓ‹ÏÈΘ (3,22). ∞‡ÍËÛË ÙˆÓ ÙÚ·ÓÛ·ÌÈÓ·-ÛÒÓ ‰È·ÈÛÙÒıËÎÂ Û˘¯ÓfiÙÂÚ· ÛÙ· ·È‰È¿ Ù˘ ‰È΋˜
Ì·˜ ÌÂϤÙ˘ (80%) Û ۇÁÎÚÈÛË Ì ÙÔ 59% ·Ó¿ÏÔÁ˘ÌÂϤÙ˘ (14). ÀÂÚÁ·ÌÌ·ÛÊ·ÈÚÈÓ·ÈÌ›·, ΢ڛˆ˜ IgMÙ¿Í˘, ·Ú·ÙËÚ‹ıËΠÛÙÔ 50% ÙˆÓ ·ÛıÂÓÒÓ Ì·˜.
∞fi ÙËÓ ·Ó¿Ï˘ÛË ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ وӷȉÈÒÓ Î·Ù¿ ÙË ‰È¿ÚÎÂÈ· Ù˘ ÔÍ›·˜ Ïԛ̈͢ ÚÔ-·ÙÂÈ fiÙÈ Ù· CD3+ ‹Ù·Ó ·˘ÍË̤ӷ ÛÙÔ 50% ÙˆÓ·ÛıÂÓÒÓ, ‡ÚËÌ· Ô˘ Û˘ÌʈÓ› Ì ¿ÏÏÔ˘˜ ÂÚ¢ÓË-Ù¤˜ (9,22). ∆Ô 50% ÙˆÓ ·ÛıÂÓÒÓ Ì·˜ ·ÚÔ˘Û›·Û ȉÈ-·›ÙÂÚË Ì›ˆÛË ÙˆÓ CD3+/CD4+ Î·È ÙˆÓ CD19+, Û·ÓÙ›ıÂÛË Ì ÌÂϤÙË ÂÓËϛΈÓ, fiÔ˘ ‰ÂÓ ‰È·ÈÛÙÒ-ıËΠ·ÍÈÔÛËÌ›ˆÙË ÌÂÙ·‚ÔÏ‹ (22). ∫·Ó¤Ó· ·È‰› ‰ÂÓ·ÚÔ˘Û›·Û ÌÂÙ·‚ÔÏ‹ ÛÙ· Ê˘ÛÈο ΢ÙÙ·ÚÔÎÙfiÓ·¡∫, fiˆ˜ ‰È·ÈÛÙÒıËÎÂ Î·È ·fi ÙÔ˘˜ WeisbergerÎ·È Û˘Ó. (23), ÂÓÒ ·ÓÙ›ıÂÙ· ÔÈ Williams Î·È Û˘Ó. (22)·Ó¤‰ÂÈÍ·Ó ÛËÌ·ÓÙÈο ·˘ÍË̤ӷ ›‰· ¡∫ ΢ÙÙ¿-ÚˆÓ Û ÂÓ‹ÏÈΘ Ì ÔÍ›· §ª. ™Â fiÏ· Ù· ·È‰È¿, ·-Ú·ÙËÚ‹ıËΠ·‡ÍËÛË ÙˆÓ CD3+/CD8+ (̤ÛË ÙÈÌ‹:48,5%). ¶Èı·Ófiٷٷ, Ù· CD3+/CD8+ Û˘ÓÈÛÙÔ‡Ó Ù·ÂÓÂÚÁÔÔÈË̤ӷ ∆ ÏÂÌÊÔ·ÙÙÙ·Ú· Ô˘ ÌÔÚÊÔÏÔÁÈ-ο ÔÚ›˙ÔÓÙ·È ˆ˜ ‘¿Ù˘·’ ÏÂÌÊÔ·ÙÙ·Ú· Î·È ·ÔÙÂ-ÏÔ‡Ó ¤ˆ˜ Î·È ÙÔ 50% ÙÔ˘ Û˘ÓÔÏÈÎÔ‡ ÏÂÌÊÔ΢ÙÙ·ÚÈ-ÎÔ‡ ÏËı˘ÛÌÔ‡ (20). ∏ ·‡ÍËÛË ÙˆÓ CD3+/CD8+
ÛÙËÓ ÔÍ›· Ïԛ̈ÍË Û ÂÓ‹ÏÈΘ ÂÈÛËÌ·›ÓÂÙ·È Î·È·fi ¿ÏÏÔ˘˜ ÂÚ¢ÓËÙ¤˜ (20,22,24,25). ∆· CD3+/CD8+,ˆ˜ Ô Î˘Ú›·Ú¯Ô˜ ̆ ÔÏËı˘ÛÌfi˜ ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ,·›˙Ô˘Ó ÚˆÙ·Ú¯ÈÎfi ÚfiÏÔ ÛÙËÓ Î·Ù·ÛÙÔÏ‹ ÙÔ˘ ÔÏ-Ï·Ï·ÛÈ·ÛÌÔ‡ ÙÔ˘ ÈÔ‡. ∞ÛÎÔ‡Ó Î˘ÙÙ·ÚÔÙÔÍÈ΋ ‰Ú¿-ÛË ¤Ó·ÓÙÈ ÙˆÓ ÚÔÛ‚ÏËı¤ÓÙˆÓ ·fi ÙÔÓ Èfi µ ÏÂÌÊÔ-΢ÙÙ¿ÚˆÓ, ‰ÈηÈÔÏÔÁÒÓÙ·˜ Èı·ÓÒ˜ ÙËÓ ÙÒÛË ÙˆÓCD19+ Ô˘ ‰È·ÈÛÙÒıËΠÛÙË ÌÂϤÙË Ì·˜. ∏ ·Ú·-ÙËÚÔ‡ÌÂÓË Î˘ÙÙ·ÚÔÙÔÍÈ΋ ‰Ú¿ÛË ÙˆÓ CD3+/CD8+
ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ ·Ú·ÙËÚÂ›Ù·È Î·È Û ¿ÏϘ ÏÔÈÌÒ-ÍÂȘ, fiˆ˜ ÛÙËÓ ∏IV Î·È ÙËÓ HCV Ïԛ̈ÍË. øÛÙfiÛÔ,ÛÙË §ª Ù· CD3+/CD8+ ¤¯Ô˘Ó Ê·ÈÓfiÙ˘Ô CD45R0+/CD45RA-, Û˘Ì‚·Ùfi Ì ∆ ÌÓËÌÔÓÈο ·ÙÙ·Ú· ·Ú¿ Ì·Úı¤Ó· ∆ ÏÂÌÊÔ·ÙÙ·Ú· (20). ™Â fiÏ· Ù· ·È‰È¿, ÔÏfiÁÔ˜ CD4+/CD8+ ‹Ù·Ó ÂÏ·Ùو̤ÓÔ˜ (0,12-1), ÁÂÁÔ-Ófi˜ ·Ó·ÌÂÓfiÌÂÓÔ ·fi ÙË ÛËÌ·ÓÙÈ΋ ·‡ÍËÛË ÙˆÓCD3+/CD8+ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ, ‡ÚËÌ· Ô˘ Û˘Ìʈӛ̠ÙÔ˘˜ Weisberger Î·È Û˘Ó. (0,1-0,9) (23) Î·È LimaÎ·È Û˘Ó. (0,11-1,23) (25).
¶›Ó·Î·˜ 3. ™˘Û¯¤ÙÈÛË ÌÂٷ͇ ÙˆÓ ˘ÔÏËı˘ÛÌÒÓ ÙˆÓ ∆, µ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ, ÙÔ˘ ÏfiÁÔ˘ CD4+/CD8+, ÙˆÓ ·ÓÔÛÔÛÊ·ÈÚÈÓÒÓ, ÙÔ˘ ÌÂÁ¤ıÔ˘˜ÙÔ˘ ÛÏËÓfi˜ Î·È ÙˆÓ ‚ÈÔ¯ËÌÈÎÒÓ ‰ÂÈÎÙÒÓ
CD3+ CD4+ CD8+ CD19+ NK CD4/CD8 IgA
ª¤ÁÂıÔ˜ ÛÏËÓfi˜ 0,97 -0,44 0,52** -0,75 0,18 -0,5** 0,32SGOT -0,08 -0,19 0,06 -0,04 -0,01 -0,08 0,48*SGPT 0,03 -0,24 0,36 -0,11 0,07 -0,21 0,58*Á-GT -0,41* -0,26 0,16 0,23 0,05 -0,19 0,51**IgG 0,22 -0,06 0,47* -0,1 0,21 -0,37 0,48*IgA 0,18 -0,42* 0,50** -0,2 0,19 -0,48*IgM -0,24 -0,31 0,38 0,03 -0,26 -0,39* 0,21
∆· ‰Â‰Ô̤ӷ ‰›ÓÔÓÙ·È ̂ ̃Û˘ÓÙÂÏÂÛÙ‹ ̃Û˘Û¯¤ÙÈÛË ̃(r). T· p ·Ó·Ê¤ÚÔÓÙ·È fiÙ·Ó Â›Ó·È ÛËÌ·ÓÙÈο (*p<0,05, **p<0,001)
139∞ÓÔÛÔÊ·ÈÓfiÙ˘Ô˜ ·È‰ÈÒÓ Ì EBV Î·È CMV Ïԛ̈ÍË
¶·È‰È·ÙÚÈ΋ 2008;71:135-140
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·139

∫·Ù¿ ÙÔÓ Â·Ó¤ÏÂÁ¯Ô, Ë Û˘ÓÙÚÈÙÈ΋ ÏÂÈÔ„ËÊ›·
ÙˆÓ ·È‰ÈÒÓ ·ÚÔ˘Û›·Û ›·ÛË. ¶·Ú·ÙËÚ‹ıËΠÙÒ-
ÛË ÙˆÓ ÏÂÌÊÔ΢ÙÙ¿ÚˆÓ Î·È ÙˆÓ CD3+/CD8+ Î·È Â¿-
ÓÔ‰Ô˜ ÙˆÓ CD3+/CD4+, CD19+ Î·È ÙÔ˘ ÏfiÁÔ˘
CD4+/CD8+. ∏ ÎÏÈÓÈ΋ ›·ÛË Û˘Ì‚¿‰È˙ Ì ÙËÓ ·Ô-
ηٿÛÙ·ÛË ÙˆÓ ÙÈÌÒÓ ÙˆÓ ·ÓÔÛÔÛÊ·ÈÚÈÓÒÓ Î·È ÙˆÓ
Ë·ÙÈÎÒÓ ‰ÂÈÎÙÒÓ. ¢È·ÈÛÙÒıËΠfiÙÈ Ù· CD3+/CD8+
›¯·Ó ÛËÌ·ÓÙÈ΋ ıÂÙÈ΋ Û˘Û¯¤ÙÈÛË Ì ÙË ÛÏËÓÔÌÂ-
Á·Ï›·, ηıÒ˜ Î·È Ì ÙȘ IgG Î·È IgA. ™Â ÙÚ›· ·fi Ù· 26
·È‰È¿, Ë ÎÏÈÓÈ΋ ·ÔηٿÛÙ·ÛË Î·ı˘ÛÙ¤ÚËÛ ¤ˆ˜
Î·È 8 Ì‹Ó˜, ηٿ ÙË ‰È¿ÚÎÂÈ· ÙˆÓ ÔÔ›ˆÓ ÔÈ ÏfiÁÔÈ
CD4+/CD8+ ·Ú¤ÌÂÓ·Ó ¯·ÌËÏÔ›. ∫·ı˘ÛÙ¤ÚËÛË Ù˘
·Ó¿ÚÚˆÛ˘ ̤¯ÚÈ Î·È 18 Ì‹Ó˜, Ë ÔÔ›· ‰ÂÓ Û˘Ó‰¤Â-
Ù·È fï˜ Ì ٷ ·˘ÍË̤ӷ ›‰· ÙˆÓ CD3+/CD8+,
·Ó·Ê¤ÚÂÙ·È Î·È Û ¿ÏÏË ÌÂϤÙË (15). ∂›Ó·È ÂӉȷʤ-
ÚÔÓ fiÙÈ ˘ÔÛÙËÚ›˙ÂÙ·È fiÙÈ Ë ·Ú¿Ù·ÛË Ù˘ Ïԛ̈͢
‰ÂÓ ÔÊ›ÏÂÙ·È ÛÙÔ ·˘ÍË̤ÓÔ ÈÈÎfi ÊÔÚÙ›Ô, ·ÏÏ¿ ÛÙËÓ
ÂËÚ·Ṳ̂ÓË ·ÓÔÛȷ΋ ηٿÛÙ·ÛË ÙÔ˘ ÍÂÓÈÛÙ‹ (20).
™˘ÌÂÚ·ÛÌ·ÙÈο, ‰È·ÈÛÙÒıËΠfiÙÈ Ù· ·È‰È¿
Ô˘ ÌÂÏÂÙ‹Û·Ì ηٿ ÙËÓ ÔÍ›· Ê¿ÛË Ù˘ EBV ηÈ
Ù˘ CMV Ïԛ̈͢ ··ÓÙÔ‡Ó Ì ÂÍ·ÈÚÂÙÈο ÌÂÁ¿ÏË
·‡ÍËÛË ÙˆÓ CD3+/CD8+. ∏ ‡ÊÂÛË ÙˆÓ Û˘Ìو̿-
ÙˆÓ Ù˘ ÔÍ›·˜ Ïԛ̈͢ Ê·›ÓÂÙ·È fiÙÈ Â›Ó·È ÙÔ ·Ô-
Ù¤ÏÂÛÌ· Ù˘ ¢Ú›·˜ ΢ÙÙ·ÚÔÙÔÍÈ΋˜ ∆ ÏÂÌÊÔ΢Ù-
Ù·ÚÈ΋˜ (CTL) ·¿ÓÙËÛ˘ ÛÙ· ·ÓÙÈÁfiÓ· ÙÔ˘ ÈÔ‡. ™˘-
ÓÂÒ˜, Ë ÂÎÙ›ÌËÛË ÙÔ˘ ·ÓÔÛÔÊ·ÈÓfiÙ˘Ô˘ Î·È ÙÔ˘
ÏfiÁÔ˘ CD4+/CD8+ Â›Ó·È ¯Ú‹ÛÈÌË ÛÙËÓ ÎÏÈÓÈ΋ Ú¿ÍË
ÁÈ· ÙËÓ ·Ú·ÎÔÏÔ‡ıËÛË ÙˆÓ ·È‰ÈÒÓ Ì ¯ÚfiÓÈ· EBV
‹ CMV Ïԛ̈ÍË.
µÈ‚ÏÈÔÁÚ·Ê›·
1. Jenson HB. Epstein-Barr Virus. In: Behrman RE, Klieg-
man RM, Jenson HB, editors. Nelson Textbook of Pedi-
atrics. 17th edition. Saunders; 2004. p. 1062-1066.
2. American Academy of Pediatrics. Epstein-Barr Virus In-
fections. In: Pickering LK, Baker CJ, Long SS, McMillan
JA, eds. Red Book: 2006 Report of the Committee on In-
fectious Diseases. 27th edition. p. 286-288.
3. Ventura KC, Hudnall SD. Hematologic differences in het-
erophile-positive and heterophile negative infectious
mononucleosis. Am J Hematol 2004;76:315-318.
4. Koch HG, Harms E. Infektionen mit dem Epstein-Barr
Virus. Deutsches Arzteblatt 1995;92:7-17.
5. Okay TS, Del Negro GM, Yamamoto L, Raiz Junior R. De-
tection of EBV-DNA in serum samples of an immunosup-
pressed child during a three years follow-up: association of
clinical and PCR data with active infection. Rev Inst Med
Trop Sao Paulo 2005;47:99-102.
6. Sitki-Green D, Covington M, Raab-Traub N. Compart-
mentalization and transmission of multiple Epstein-Barr
virus strains in asymptomatic carriers. J Virol 2003;77:
1840-1847.
7. Kano K, Yamada Y, Sato Y, Arisaka O, Ono Y, Ueda Y.
Glomerulonephritis in a patient with chronic active Ep-
stein-Barr virus infection. Pediatr Nephrol 2005;20:89-92.
8. Roth DE, Jones A, Smith L, Lai R, Preiksaitis J, Robinson J.
Severe chronic active Epstein-Barr virus infection mimic-
king steroid-dependent inflammatory bowel disease. Pedi-atr Infect Dis J 2005;24:261-264.
9. Sugaya N, Kimura H, Hara S, Hoshino Y, Kojima S, Mor-ishima T, et al. Quantitative analysis of Epstein-Barr virus(EBV)-specific CD8+ T cells in patients with chronic activeEBV infection. J Infect Dis 2004;190:985-988.
10. Yuge A, Kinoshita E, Moriuchi M, Ohno Y, Haga H, Mo-riuchi H. Persistent hepatitis associated with chronic ac-tive Epstein-Barr virus infection. Pediatr Infect Dis J 2004;23:74-76.
11. Okano M, Kawa K, Kimura H, Yachie A, Wakiguchi H,Maeda A, et al. Proposed guidelines for diagnosing chron-ic active Epstein-Barr virus infection. Am J Hematol2005;80:64-69.
12. Hara S, Hoshino Y, Naitou T, Nagano K, Iwai M, SuzukiK, et al. Association of virus infected-T cell in severe he-patitis caused by primary Epstein-Barr virus infection. JClin Virol 2006;35:250-256.
13. Jenson HB. Acute complications of Epstein-Barr virusinfectious mononucleosis. Curr Opin Pediatr 2000;12:263-268.
14. Chan CW, Chiang AK, Chan KH, Lau AS. Epstein-Barrvirus-associated infectious mononucleosis in Chinese chil-dren. Pediatr Infect Dis J 2003;22:974-978.
15. Novitskii VV, Urazova OI, Naslednikova IO, PomogaevaAP, Syusina LV. Subpopulation composition of peripheralblood lymphocytes in children with infectious mononu-cleosis. Bull Exp Biol Med 2002;134:57-59.
16. Grotto I, Mimouni D, Huerta M, Mimouni M, Cohen D,Robin G, et al. Clinical and Laboratory presentation ofEBV positive infectious mononucleosis in young adults.Epidemiol Infect 2003;131:683-689.
17. Ebell MH. Epstein-Barr virus infectious mononucleosis.Am Fam Physician 2004;70:1279-1287.
18. Cohen JI. Epstein-Barr virus infection. New Engl J Med2000;343:481-492.
19. Rea TD, Russo JE, Katon W, Ashley RL, Buchwald DS.Prospective study of the natural history of infectiousmononucleosis caused by Epstein-Barr virus. J Am BoardFam Pract 2001;14:234-242.
20. Cameron B, Bharadwaj M, Burrows J, Fazou C, WakefieldD, Hickie I, et al; Dubbo Infection Outcomes Study. Pro-longed illness after infectious mononucleosis is associatedwith altered immunity but not with increased viral load. JInfect Dis 2006;193:664-671.
21. Fafi-Kremer S, Morand P, Brion JP, Pavese P, Baccard M,Germi R, et al. Long-term shedding of infectious Epstein-Barr virus after infectious mononucleosis. J Infect Dis2005;191:985-989.
22. Williams H, Macsween K, McAulay K, Higgins C, Harri-son N, Swerdlow A, et al. Analysis of immune activationand clinical events in acute infectious mononucleosis. J In-fect Dis 2004;190:63-71.
23. Weisberger J, Cornfield D, Gorczyca W, Liu Z. Down-regu-lation of pan-T-cell antigens, particularly CD7, in acute in-fectious mononucleosis. Am J Clin Pathol 2003;120:49-55.
24. Ohga S, Nomura A, Takada H, Hara T. Immunological as-pects of Epstein-Barr virus infection. Crit Rev Oncol He-matol 2002;44:203-215.
25. Lima M, Teixeira Mdos A, Queirfis ML, Santos AH, Gon-çalves C, Correia J, et al. Immunophenotype and TCR-Vbeta repertoire of peripheral blood T-cells in acute infec-tious mononucleosis. Blood Cells Mol Dis 2003;30:1-12.
140 ∂. ¶··‰ÔÔ‡ÏÔ˘-∞Ï·Ù¿ÎË Î·È Û˘Ó.
Paediatriki 2008;71:135-140
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·140

ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ ÛÙ· ·È‰È¿: ÂÌÂÈÚ›· 15 ÂÙÒÓ Û ¤Ó·
ΤÓÙÚÔ
Ÿ. µÚ¿ÓË1, ª. ¶·ÓÙÈΛ‰Ô˘1, °. ÿÌ‚ÚÈÔ˜2, π. •˘ÓÈ¿˜1, µ. ¢ÂÌÂÚÙ˙›‰Ô˘1, ∫. ∫¿ÓÙ˙ÈÔ˘1, ∞. ª·˘ÚÔ˘‰‹1,
¢. ∆·ÎÔ‡‰·˜2, £. ¶··ÛÙ·‡ÚÔ˘1, ∫. ™‡ÚÔÁÏÔ˘1
¶ÂÚ›ÏË„Ë
∂ÈÛ·ÁˆÁ‹: ∏ ÌÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ (ª∏) ÛÙ· ·È‰È¿ ·ÔÙÂÏ› ÙË ÌÔÓ·‰È΋ ıÂڷ›· ÁÈ· ÙËÓ ·ÓÙÈÌÂÙÒÈÛËÙ˘ ÌË ·Ó·ÛÙÚ¤„ÈÌ˘ Ë·ÙÈ΋˜ ·Ó¿ÚÎÂÈ·˜ ÙÂÏÈÎÔ‡ ÛÙ·‰›Ô˘. ™ÎÔfi˜ Ù˘ ·ÚÔ‡Û·˜ ÌÂϤÙ˘ ‹Ù·Ó Ë ·Ó·-ÊÔÚ¿ Ù˘ ÂÌÂÈÚ›·˜ Ì·˜ ·fi ÙËÓ ·Ú·ÎÔÏÔ‡ıËÛË ·È‰ÈÒÓ Ô˘ ¤¯Ô˘Ó ˘Ô‚ÏËı› Û ÌÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ: ∞fi ÙÔ 1990 ̤¯ÚÈ Û‹ÌÂÚ·, 16 ·ÛıÂÓ›˜ Ù˘ °’ ¶·È‰È·ÙÚÈ΋˜ ∫ÏÈÓÈ΋˜, ËÏÈΛ·˜ 6 ÌË-ÓÒÓ ¤ˆ˜ 13 ÂÙÒÓ, ˘Ô‚Ï‹ıËÎ·Ó Û ª∏. ∞fi Ù· ·È‰È¿ ·˘Ù¿, 9 ›¯·Ó ·ÙÚËÛ›· Â͈˷ÙÈÎÒÓ ¯ÔÏËÊfiÚˆÓfiÚˆÓ, 2 ÔÍ›· Ë·ÙÈ΋ Ó¤ÎÚˆÛË ÌÂÙ¿ ÙË ‚ÚÒÛË ÙÔÍÈÎÒÓ Ì·ÓÈÙ·ÚÈÒÓ, 1 Û‡Ó‰ÚÔÌÔ Alagille, 1 ÂÓ‰ÔË·-ÙÈ΋ ˘ÔÏ·Û›· ÙˆÓ ¯ÔÏËÊfiÚˆÓ fiÚˆÓ ÌË Û˘Ó‰ÚÔÌÈÎÔ‡ Ù‡Ô˘, 1 ÓfiÛÔ ÙÔ˘ Wilson, 1 ÚˆÙÔ·ı‹ ˘Â-ÚÔÍ·ÏÔ˘Ú›· Î·È 1 Ë·ÙÔ‚Ï¿Ûو̷. ¢¤Î· ·È‰È¿ ˘Ô‚Ï‹ıËÎ·Ó Û ª∏ ÛÙË ÃÂÈÚÔ˘ÚÁÈ΋ ∫ÏÈÓÈ΋ ªÂÙ·-ÌÔۯ‡ÛÂˆÓ ÙÔ˘ ∞¶£ Î·È Ù· ˘fiÏÔÈ· Û ΤÓÙÚ· ÙÔ˘ Â͈ÙÂÚÈÎÔ‡. ∆ÚÂȘ ÌÂÙ·ÌÔۯ‡ÛÂȘ ¤ÁÈÓ·Ó ·fi ˙Ò-ÓÙ· Û˘ÁÁÂÓ‹ ‰fiÙË Î·È 13 ·fi و̷ÙÈÎfi ‰fiÙË. ŒÍÈ ·È‰È¿ ¤Ï·‚·Ó ·ÓÔÛÔηٷÛÙ·ÏÙÈ΋ ·ÁˆÁ‹ Ì ΢ÎÏÔ-ÛÔÚ›ÓË, MMF Î·È ÎÔÚÙÈÎÔÛÙÂÚÔÂȉ‹ Î·È 7 ·È‰È¿ tacrolimus ·ÓÙ› ΢ÎÏÔÛÔÚ›Ó˘.
∞ÔÙÂϤÛÌ·Ù·: ∞fi Ù· 16 ·È‰È¿ Ô˘ ˘Ô‚Ï‹ıËÎ·Ó Û ÌÂÙ·ÌfiÛ¯Â˘ÛË, 3 η٤ÏËÍ·Ó ÙÔÓ ÚÒÙÔ ÌÂÙÂÁ¯ÂÈÚË-ÙÈÎfi Ì‹Ó·. ∞fi Ù· ˘fiÏÔÈ· Ô˘ ·Ú·ÎÔÏÔ˘ıԇ̠¤ˆ˜ Û‹ÌÂÚ·, 3 ·ÚÔ˘Û›·Û·Ó ÔÍ›· Î·È 1 ¯ÚfiÓÈ· ·fiÚ-ÚÈ„Ë ÙÔ˘ ÌÔۯ‡̷ÙÔ˜. ¶¤ÓÙ ·È‰È¿ ÂÌÊ¿ÓÈÛ·Ó Ïԛ̈ÍË ·fi CMV, 5 ·fi EBV, 2 Ïԛ̈ÍË ·fi HSV, 2 ·fiÈfi Parvo µ19, 1 ·fi Èfi Coxsackie Î·È 1 ·fi Candida albicans. ∂›Û˘, ¤Ó· ·È‰› ·ÚÔ˘Û›·Û ·ÈÌÔÚÚ·Á›· ÙÔ˘·ÓÒÙÂÚÔ˘ °∂™ Î·È ¤Ó· ·ÚÔ˘Û›·Û ÓfiÛÔ ÂÍ·Ê¿ÓÈÛ˘ ÙˆÓ ÌÈÎÚÒÓ ¯ÔÏËÊfiÚˆÓ fiÚˆÓ. ∏ ¤Î‚·ÛË ÛÙȘ ÂÚÈÛ-ÛfiÙÂÚ˜ ÂÚÈÙÒÛÂȘ ‹Ù·Ó ηϋ, Ì ηϋ ÏÂÈÙÔ˘ÚÁ›· ÙˆÓ Ë·ÙÈÎÒÓ ÌÔÛ¯Â˘Ì¿ÙˆÓ, ÂÎÙfi˜ ·fi ÙËÓ ÂÚ›ÙˆÛËÙÔ˘ ·È‰ÈÔ‡ Ì ÙË ÓfiÛÔ ÂÍ·Ê¿ÓÈÛ˘ ÙˆÓ ÌÈÎÚÒÓ ¯ÔÏËÊfiÚˆÓ Ô˘ ¯ÚÂÈ¿ÛÙËΠӤ· ÌÂÙ·ÌfiÛ¯Â˘ÛË.
™˘ÌÂÚ¿ÛÌ·Ù·: ∏ Ì·ÎÚÔ¯ÚfiÓÈ· ÔÚ›· Î·È ¤Î‚·ÛË ·È‰ÈÒÓ Ì ˷ÙÈ΋ ÌÂÙ·ÌfiÛ¯Â˘ÛË Â›Ó·È Û¯ÂÙÈο η-Ï‹ Ì ÙËÓ ÚÔ¸fiıÂÛË Ó· ·Ú·ÎÔÏÔ˘ıÔ‡ÓÙ·È Û ÂÍÂȉÈÎÂ˘Ì¤Ó· ΤÓÙÚ·.
§¤ÍÂȘ ÎÏÂȉȿ: ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜, ·È‰È¿.
Liver transplantation in children: 15 years experience in one center
O. Vrani1, M. Pantikidou1, G. Imvrios2, I. Xinias1, V. Demertzidou1, K. Kantziou1, A. Mavroudi1,
D. Takoudas2, T. Papastaurou1, K. Spyroglou1
Abstract
Background: Liver transplantation (LT) is the only treatment for children with irreversible liver failure. Thisis a report of the follow-up of a series of 16 children who underwent LT.
Methods: Since 1990, 16 patients of the 3rd Paediatric Clinic of the Hippocration General Hospital of Thes-saloniki, aged 6 months to 13 years, underwent LT. Nine children presented initially with extrahepatic bil-iary atresia, 2 with acute liver failure following toxic mushroom ingestion, 1 with Alagille syndrome, 1 withnon-syndromic intrahepatic biliary paucity, 1 with Wilson’s disease, 1 with primary hyperoxaluria and 1with hepatoblastoma. Ten children underwent LT in the Organ Transplantation Unit of the Aristotle Univer-sity of Thessaloniki and the others in various medical centers in other countries. Three transplants came fromliving-related donors and 13 from deceased donors. Six children went under immunosuppressive treatmentwith cyclosporine, MMF and corticosteroids and seven with tacrolimus, MMF and corticosteroids.
Results: Three of the 16 children died within the first month after transplantation due to post-transplantcomplications, and eleven have survived. Three children presented with acute rejection and one with chron-ic organ rejection, which was successfully managed. Five children developed CMV infection, 5 EBV infection,2 HSV infection, 2 Parvo B19 virus and 1 Candida Albicans infection. One child had upper GI haemorrhageand one presented with small biliary paucity. The outcome was satisfactory in most cases, with good graftfunction, except in the case of the patient with small biliary paucity, who required retransplantation.
Conclusions: The long-term clinical course of children following LT is good, provided that they are moni-tored in specialized centres.
Key words: Liver transplantation, children.
141∂ƒ∂À¡∏∆π∫∏ ∂ƒ°∞™π∞ ORIGINAL ARTICLE
1 °’ ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋∞¶£, πÔÎÚ¿ÙÂÈÔ °ÂÓÈÎfi¡ÔÛÔÎÔÌ›ԣÂÛÛ·ÏÔӛ΢
2 ÃÂÈÚÔ˘ÚÁÈ΋ ∫ÏÈÓÈ΋ªÂÙ·ÌÔۯ‡ÛÂˆÓ ∞¶£,πÔÎÚ¿ÙÂÈÔ °ÂÓÈÎfi¡ÔÛÔÎÔÌ›ԣÂÛÛ·ÏÔӛ΢
AÏÏËÏÔÁÚ·Ê›·:
∫ÏÂÔ̤Ó˘ ™‡ÚÔÁÏÔ˘[email protected]°’ ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋ ∞¶£,πÔÎÚ¿ÙÂÈÔ °ÂÓÈÎfi¡ÔÛÔÎÔÌÂ›Ô £ÂÛÛ·ÏÔӛ΢∫ˆÓÛÙ·ÓÙÈÓÔ˘fiψ˜ 49∆.∫. 546 39, £ÂÛÛ·ÏÔÓ›ÎË
1. 3rd Department ofPaediatrics, AristotleUniversity,Hippokration GeneralHospital, Thessaloniki,Greece
2. Department of Surgery,Organ TransplantationUnit, Aristotle University,Hippokration GeneralHospital, Thessaloniki,Greece
Correspondence:
∫leomenis [email protected] Department of Paediatrics, Aristotle University,Hippokration GeneralHospital of Thessaloniki49 Konstantinoupoleos St.,546 39, Thessaloniki,Greece
¶·È‰È·ÙÚÈ΋ 2008;71:141-147
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·141
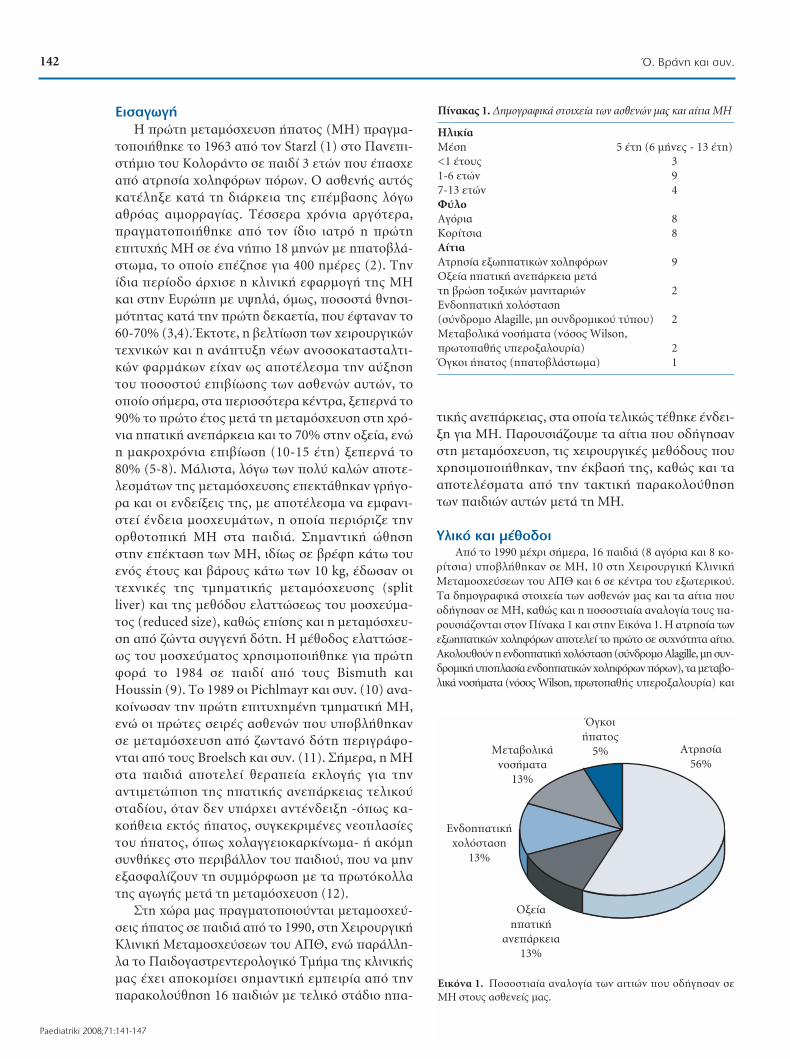
∂ÈÛ·ÁˆÁ‹
∏ ÚÒÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ (ª∏) Ú·ÁÌ·-
ÙÔÔÈ‹ıËÎÂ ÙÔ 1963 ·fi ÙÔÓ Starzl (1) ÛÙÔ ¶·ÓÂÈ-
ÛÙ‹ÌÈÔ ÙÔ˘ ∫ÔÏÔÚ¿ÓÙÔ Û ·È‰› 3 ÂÙÒÓ Ô˘ ¤·Û¯Â
·fi ·ÙÚËÛ›· ¯ÔÏËÊfiÚˆÓ fiÚˆÓ. √ ·ÛıÂÓ‹˜ ·˘Ùfi˜
η٤ÏËÍ ηٿ ÙË ‰È¿ÚÎÂÈ· Ù˘ ¤̂·Û˘ ÏfiÁˆ
·ıÚfi·˜ ·ÈÌÔÚÚ·Á›·˜. ∆¤ÛÛÂÚ· ¯ÚfiÓÈ· ·ÚÁfiÙÂÚ·,
Ú·ÁÌ·ÙÔÔÈ‹ıËΠ·fi ÙÔÓ ›‰ÈÔ È·ÙÚfi Ë ÚÒÙË
ÂÈÙ˘¯‹˜ ª∏ Û ¤Ó· Ó‹ÈÔ 18 ÌËÓÒÓ Ì ˷ÙÔ‚Ï¿-
Ûو̷, ÙÔ ÔÔ›Ô Â¤˙ËÛ ÁÈ· 400 Ë̤Ú˜ (2). ∆ËÓ
›‰È· ÂÚ›Ô‰Ô ¿Ú¯ÈÛÂ Ë ÎÏÈÓÈ΋ ÂÊ·ÚÌÔÁ‹ Ù˘ ª∏
Î·È ÛÙËÓ ∂˘ÚÒË Ì ˘„ËÏ¿, fï˜, ÔÛÔÛÙ¿ ıÓËÛÈ-
ÌfiÙËÙ·˜ ηٿ ÙËÓ ÚÒÙË ‰ÂηÂÙ›·, Ô˘ ¤ÊÙ·Ó·Ó ÙÔ
60-70% (3,4). ŒÎÙÔÙÂ, Ë ‚ÂÏÙ›ˆÛË ÙˆÓ ̄ ÂÈÚÔ˘ÚÁÈÎÒÓ
Ù¯ÓÈÎÒÓ Î·È Ë ·Ó¿Ù˘ÍË Ó¤ˆÓ ·ÓÔÛÔηٷÛÙ·ÏÙÈ-
ÎÒÓ Ê·ÚÌ¿ÎˆÓ Â›¯·Ó ˆ˜ ·ÔÙ¤ÏÂÛÌ· ÙËÓ ·‡ÍËÛË
ÙÔ˘ ÔÛÔÛÙÔ‡ ÂÈ‚›ˆÛ˘ ÙˆÓ ·ÛıÂÓÒÓ ·˘ÙÒÓ, ÙÔ
ÔÔ›Ô Û‹ÌÂÚ·, ÛÙ· ÂÚÈÛÛfiÙÂÚ· ΤÓÙÚ·, ÍÂÂÚÓ¿ ÙÔ
90% ÙÔ ÚÒÙÔ ¤ÙÔ˜ ÌÂÙ¿ ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË ÛÙË ̄ Úfi-
ÓÈ· Ë·ÙÈ΋ ·Ó¿ÚÎÂÈ· Î·È ÙÔ 70% ÛÙËÓ ÔÍ›·, ÂÓÒ
Ë Ì·ÎÚÔ¯ÚfiÓÈ· ÂÈ‚›ˆÛË (10-15 ¤ÙË) ÍÂÂÚÓ¿ ÙÔ
80% (5-8). ª¿ÏÈÛÙ·, ÏfiÁˆ ÙˆÓ Ôχ ηÏÒÓ ·ÔÙÂ-
ÏÂÛÌ¿ÙˆÓ Ù˘ ÌÂÙ·ÌfiÛ¯Â˘Û˘ ÂÂÎÙ¿ıËÎ·Ó ÁÚ‹ÁÔ-
Ú· Î·È ÔÈ ÂӉ›ÍÂȘ Ù˘, Ì ·ÔÙ¤ÏÂÛÌ· Ó· ÂÌÊ·ÓÈ-
ÛÙ› ¤Ó‰ÂÈ· ÌÔÛ¯Â˘Ì¿ÙˆÓ, Ë ÔÔ›· ÂÚÈfiÚÈ˙ ÙËÓ
ÔÚıÔÙÔÈ΋ ª∏ ÛÙ· ·È‰È¿. ™ËÌ·ÓÙÈ΋ ÒıËÛË
ÛÙËÓ Â¤ÎÙ·ÛË ÙˆÓ ª∏, ȉ›ˆ˜ Û ‚Ú¤ÊË Î¿Ùˆ ÙÔ˘
ÂÓfi˜ ¤ÙÔ˘˜ Î·È ‚¿ÚÔ˘˜ οو ÙˆÓ 10 kg, ¤‰ˆÛ·Ó ÔÈ
Ù¯ÓÈΤ˜ Ù˘ ÙÌËÌ·ÙÈ΋˜ ÌÂÙ·ÌfiÛ¯Â˘Û˘ (split
liver) Î·È Ù˘ ÌÂıfi‰Ô˘ ÂÏ·ÙÙÒÛˆ˜ ÙÔ˘ ÌÔۯ‡̷-
ÙÔ˜ (reduced size), ηıÒ˜ ›Û˘ Î·È Ë ÌÂÙ·ÌfiÛ¯Â˘-
ÛË ·fi ˙ÒÓÙ· Û˘ÁÁÂÓ‹ ‰fiÙË. ∏ ̤ıÔ‰Ô˜ ÂÏ·ÙÙÒÛÂ-
ˆ˜ ÙÔ˘ ÌÔۯ‡̷ÙÔ˜ ¯ÚËÛÈÌÔÔÈ‹ıËΠÁÈ· ÚÒÙË
ÊÔÚ¿ ÙÔ 1984 Û ·È‰› ·fi ÙÔ˘˜ Bismuth ηÈ
Houssin (9). ∆Ô 1989 ÔÈ Pichlmayr Î·È Û˘Ó. (10) ·Ó·-
ÎÔ›ÓˆÛ·Ó ÙËÓ ÚÒÙË ÂÈÙ˘¯Ë̤ÓË ÙÌËÌ·ÙÈ΋ ª∏,
ÂÓÒ ÔÈ ÚÒÙ˜ ÛÂÈÚ¤˜ ·ÛıÂÓÒÓ Ô˘ ˘Ô‚Ï‹ıËηÓ
Û ÌÂÙ·ÌfiÛ¯Â˘ÛË ·fi ˙ˆÓÙ·Ófi ‰fiÙË ÂÚÈÁÚ¿ÊÔ-
ÓÙ·È ·fi ÙÔ˘˜ Broelsch Î·È Û˘Ó. (11). ™‹ÌÂÚ·, Ë ª∏
ÛÙ· ·È‰È¿ ·ÔÙÂÏ› ıÂڷ›· ÂÎÏÔÁ‹˜ ÁÈ· ÙËÓ
·ÓÙÈÌÂÙÒÈÛË Ù˘ Ë·ÙÈ΋˜ ·Ó¿ÚÎÂÈ·˜ ÙÂÏÈÎÔ‡
ÛÙ·‰›Ô˘, fiÙ·Ó ‰ÂÓ ˘¿Ú¯ÂÈ ·ÓÙ¤Ó‰ÂÈÍË -fiˆ˜ η-
ÎÔ‹ıÂÈ· ÂÎÙfi˜ ‹·ÙÔ˜, Û˘ÁÎÂÎÚÈ̤Ó˜ ÓÂÔϷۛ˜
ÙÔ˘ ‹·ÙÔ˜, fiˆ˜ ¯ÔÏ·ÁÁÂÈÔηÚΛӈ̷- ‹ ·ÎfiÌË
Û˘Óı‹Î˜ ÛÙÔ ÂÚÈ‚¿ÏÏÔÓ ÙÔ˘ ·È‰ÈÔ‡, Ô˘ Ó· ÌËÓ
ÂÍ·ÛÊ·Ï›˙Ô˘Ó ÙË Û˘ÌÌfiÚʈÛË Ì ٷ ÚˆÙfiÎÔÏÏ·
Ù˘ ·ÁˆÁ‹˜ ÌÂÙ¿ ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË (12).
™ÙË ¯ÒÚ· Ì·˜ Ú·ÁÌ·ÙÔÔÈÔ‡ÓÙ·È ÌÂÙ·ÌÔۯ‡-
ÛÂȘ ‹·ÙÔ˜ Û ·È‰È¿ ·fi ÙÔ 1990, ÛÙË ÃÂÈÚÔ˘ÚÁÈ΋
∫ÏÈÓÈ΋ ªÂÙ·ÌÔۯ‡ÛÂˆÓ ÙÔ˘ ∞¶£, ÂÓÒ ·Ú¿ÏÏË-
Ï· ÙÔ ¶·È‰ÔÁ·ÛÙÚÂÓÙÂÚÔÏÔÁÈÎfi ∆Ì‹Ì· Ù˘ ÎÏÈÓÈ΋˜
Ì·˜ ¤¯ÂÈ ·ÔÎÔÌ›ÛÂÈ ÛËÌ·ÓÙÈ΋ ÂÌÂÈÚ›· ·fi ÙËÓ
·Ú·ÎÔÏÔ‡ıËÛË 16 ·È‰ÈÒÓ Ì ÙÂÏÈÎfi ÛÙ¿‰ÈÔ Ë·-
ÙÈ΋˜ ·Ó¿ÚÎÂÈ·˜, ÛÙ· ÔÔ›· ÙÂÏÈÎÒ˜ Ù¤ıËΠ¤Ó‰ÂÈ-
ÍË ÁÈ· ª∏. ¶·ÚÔ˘ÛÈ¿˙Ô˘Ì ٷ ·›ÙÈ· Ô˘ Ô‰‹ÁËÛ·Ó
ÛÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË, ÙȘ ¯ÂÈÚÔ˘ÚÁÈΤ˜ ÌÂıfi‰Ô˘˜ Ô˘
¯ÚËÛÈÌÔÔÈ‹ıËηÓ, ÙËÓ ¤Î‚·Û‹ Ù˘, ηıÒ˜ Î·È Ù·
·ÔÙÂϤÛÌ·Ù· ·fi ÙËÓ Ù·ÎÙÈ΋ ·Ú·ÎÔÏÔ‡ıËÛË
ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ ÌÂÙ¿ ÙË ª∏.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ
∞fi ÙÔ 1990 ̤¯ÚÈ Û‹ÌÂÚ·, 16 ·È‰È¿ (8 ·ÁfiÚÈ· Î·È 8 ÎÔ-
Ú›ÙÛÈ·) ˘Ô‚Ï‹ıËÎ·Ó Û ª∏, 10 ÛÙË ÃÂÈÚÔ˘ÚÁÈ΋ ∫ÏÈÓÈ΋
ªÂÙ·ÌÔۯ‡ÛÂˆÓ ÙÔ˘ ∞¶£ Î·È 6 Û ΤÓÙÚ· ÙÔ˘ Â͈ÙÂÚÈÎÔ‡.
∆· ‰ËÌÔÁÚ·ÊÈο ÛÙÔȯ›· ÙˆÓ ·ÛıÂÓÒÓ Ì·˜ Î·È Ù· ·›ÙÈ· Ô˘
Ô‰‹ÁËÛ·Ó Û ª∏, ηıÒ˜ Î·È Ë ÔÛÔÛÙÈ·›· ·Ó·ÏÔÁ›· ÙÔ˘˜ ·-
ÚÔ˘ÛÈ¿˙ÔÓÙ·È ÛÙÔÓ ¶›Ó·Î· 1 Î·È ÛÙËÓ ∂ÈÎfiÓ· 1. ∏ ·ÙÚËÛ›· ÙˆÓ
Â͈˷ÙÈÎÒÓ ¯ÔÏËÊfiÚˆÓ ·ÔÙÂÏ› ÙÔ ÚÒÙÔ ÛÂ Û˘¯ÓfiÙËÙ· ·›ÙÈÔ.
∞ÎÔÏÔ˘ıÔ‡Ó Ë ÂÓ‰ÔË·ÙÈ΋ ̄ ÔÏfiÛÙ·ÛË (Û‡Ó‰ÚÔÌÔ Alagille, ÌË Û˘Ó-
‰ÚÔÌÈ΋ ̆ ÔÏ·Û›· ÂÓ‰ÔË·ÙÈÎÒÓ ̄ ÔÏËÊfiÚˆÓ fiÚˆÓ), Ù· ÌÂÙ·‚Ô-
ÏÈο ÓÔÛ‹Ì·Ù· (ÓfiÛÔ ̃Wilson, ÚˆÙÔ·ı‹˜ ˘ÂÚÔÍ·ÏÔ˘Ú›·) ηÈ
142 Ÿ. µÚ¿ÓË Î·È Û˘Ó.
Paediatriki 2008;71:141-147
¶›Ó·Î·˜ 1. ¢ËÌÔÁÚ·ÊÈο ÛÙÔȯ›· ÙˆÓ ·ÛıÂÓÒÓ Ì·˜ Î·È ·›ÙÈ· ª∏
∏ÏÈΛ·ª¤ÛË 5 ¤ÙË (6 Ì‹Ó˜ - 13 ¤ÙË)<1 ¤ÙÔ˘˜ 31-6 ÂÙÒÓ 97-13 ÂÙÒÓ 4º‡ÏÔ ∞ÁfiÚÈ· 8∫ÔÚ›ÙÛÈ· 8∞›ÙÈ·∞ÙÚËÛ›· Â͈˷ÙÈÎÒÓ ¯ÔÏËÊfiÚˆÓ 9√Í›· Ë·ÙÈ΋ ·Ó¿ÚÎÂÈ· ÌÂÙ¿ ÙË ‚ÚÒÛË ÙÔÍÈÎÒÓ Ì·ÓÈÙ·ÚÈÒÓ 2∂Ó‰ÔË·ÙÈ΋ ¯ÔÏfiÛÙ·ÛË (Û‡Ó‰ÚÔÌÔ Alagille, ÌË Û˘Ó‰ÚÔÌÈÎÔ‡ Ù‡Ô˘) 2ªÂÙ·‚ÔÏÈο ÓÔÛ‹Ì·Ù· (ÓfiÛÔ˜ Wilson, ÚˆÙÔ·ı‹˜ ˘ÂÚÔÍ·ÏÔ˘Ú›·) 2ŸÁÎÔÈ ‹·ÙÔ˜ (Ë·ÙÔ‚Ï¿Ûو̷) 1
∞ÙÚËÛ›·
56%
∂Ó‰ÔË·ÙÈ΋
¯ÔÏfiÛÙ·ÛË
13%
ªÂÙ·‚ÔÏÈο
ÓÔÛ‹Ì·Ù·
13%
ŸÁÎÔÈ
‹·ÙÔ˜
5%
√Í›·
Ë·ÙÈ΋
·Ó¿ÚÎÂÈ·
13%
∂ÈÎfiÓ· 1. ¶ÔÛÔÛÙÈ·›· ·Ó·ÏÔÁ›· ÙˆÓ ·ÈÙÈÒÓ Ô˘ Ô‰‹ÁËÛ·Ó Ûª∏ ÛÙÔ˘˜ ·ÛıÂÓ›˜ Ì·˜.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·142

Ë ÔÍ›· Ë·ÙÈ΋ ·Ó¿ÚÎÂÈ· ÌÂÙ¿ ·fi ‚ÚÒÛË ÙÔÍÈÎÒÓ Ì·ÓÈÙ·-
ÚÈÒÓ, ηÈ, Ù¤ÏÔ˜, ÔÈ fiÁÎÔÈ ÙÔ˘ ‹·ÙÔ˜.
∞fi Ù· 9 ·È‰È¿ Ì ·ÙÚËÛ›· ÙˆÓ Â͈˷ÙÈÎÒÓ ¯ÔÏËÊfi-
ÚˆÓ, 3 ›¯·Ó ˘Ô‚ÏËı› Û ¤̂·ÛË Kasai (Ë·ÙÔ˘ÏÔÂÓÙÂ-
ÚÔ·Ó·ÛÙfïÛË) ÚÈÓ ·fi ÙË ª∏ Û ËÏÈΛ· 1, 2 Î·È 4 ÌËÓÒÓ.
™Â 2 ·È‰È¿ Ú·ÁÌ·ÙÔÔÈ‹ıËΠ¤̂·ÛË Kasai Ù‡Ô˘ II,
ηٿ ÙËÓ ÔÔ›· ‰ËÌÈÔ˘ÚÁÂ›Ù·È ÂÓÙÂÚÔÛÙÔÌ›· ÁÈ· ÙÔ ÂӉ¯fi-
ÌÂÓÔ ·Ú¤Ì‚·Û˘ ̤ۈ ·˘Ù‹˜ ÛÙË ¯ÔÏÔÂÙÈ΋ ·Ó·ÛÙfï-
ÛË, Î·È Û ¤Ó· ·È‰› Kasai Ù‡Ô˘ I. ™Â fiÏ· Ù· ·È‰È¿, ÚÈÓ ·fi
ÙË ª∏, Ù·ÍÈÓÔÌ‹ıËÎÂ Ë Ë·ÙÈ΋ ÏÂÈÙÔ˘ÚÁ›· Û‡Ìʈӷ Ì ٷ
ÎÚÈÙ‹ÚÈ· ηٿ Child-Pugh (9). ŒÓ· ·È‰› ‹Ù·Ó ÛÙ·‰›Ô˘ ∞, 7
ÛÙ·‰›Ô˘ µ, Î·È 8 ÛÙ·‰›Ô˘ C.
™Â 3 ·È‰È¿ ‰fiÙ˘ ‹Ù·Ó Ë ÌËÙ¤Ú·, ·fi ÙËÓ ÔÔ›· ÂÏ‹-
ÊıËÛ·Ó Ù· ÙÌ‹Ì·Ù· II & III ÙÔ˘ ‹·ÙÔ˜. ™Ù· ˘fiÏÔÈ· 13
·È‰È¿ ÙÔ ÌfiÛ¯Â˘Ì· ÚÔÂÚ¯fiÙ·Ó ·fi و̷ÙÈÎfi ‰fiÙË. ™Â 7
ÂÚÈÙÒÛÂȘ Ô ‰fiÙ˘ ‹Ù·Ó ·È‰›, ÂÓÒ Û 6 ¯ÚËÛÈÌÔÔÈ‹ıËÎÂ
ÌfiÛ¯Â˘Ì· ·fi ÂÓ‹ÏÈη ‰fiÙË. ∞fi ·˘Ù¤˜ ÙȘ 6 ÂÚÈÙÒÛÂȘ,
ÛÙȘ 4 ÂÊ·ÚÌfiÛÙËÎÂ Ë Ù¯ÓÈ΋ split liver, Û‡Ìʈӷ Ì ÙËÓ
ÔÔ›· ÌÂÙ·ÌÔۯ‡ıËÎ·Ó Ù· ÙÌ‹Ì·Ù· ππ & πππ ÙÔ˘ ‹·ÙÔ˜, ÂÓÒ
Ô ‰ÂÍÈfi˜ ÏÔ‚fi˜ ÌÂÙ·ÌÔۯ‡ıËΠ۠ÂÓ‹ÏÈη Ï‹ÙË, Î·È ÛÙȘ
¿ÏϘ 2 ÌÂÙ·ÌÔۯ‡ıËÎ·Ó Â›Û˘ Ù· ÙÌ‹Ì·Ù· ππ & πππ, ÁÈ· ÙÔ
‰È·¯ˆÚÈÛÌfi ÙˆÓ ÔÔ›ˆÓ, fï˜, ¯ÚËÛÈÌÔÔÈ‹ıËÎÂ Ë Ù¯ÓÈ΋
reduced-size, ηٿ ÙËÓ ÔÔ›· ÙÔ ÂÓ·ÔÌÂ›Ó·Ó ÙÌ‹Ì· ÙÔ˘
‹·ÙÔ˜ Â›Ó·È ÌË ¯ÚËÛÈÌÔÔÈ‹ÛÈÌÔ.
ªÂÙ¿ ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË ÔÈ ·ÛıÂÓ›˜ ·Ú¤ÌÂÈÓ·Ó Û˘Ó‰Â-
‰Â̤ÓÔÈ Ì ÙÔÓ ·Ó·Ó¢ÛÙ‹Ú· ÁÈ· 24 ¤ˆ˜ 48 ÒÚ˜ Î·È ‚Ú›ÛÎÔ-
ÓÙ·Ó ˘fi ÛÙÂÓ‹ ·Ú·ÎÔÏÔ‡ıËÛË ÚÔÎÂÈ̤ÓÔ˘ Ó· ·ÓÙÈÌÂÙˆ-
ÈÛÙÔ‡Ó ÔÈ ·ÈÌÔ‰˘Ó·ÌÈΤ˜, ÌÂÙ·‚ÔÏÈΤ˜ Î·È ËÏÂÎÙÚÔÏ˘ÙÈΤ˜
‰È·Ù·Ú·¯¤˜, Ë ·ÒÏÂÈ· ·›Ì·ÙÔ˜ Î·È ÔÈ ÏÔÈÌÒÍÂȘ. ø˜ ·ÓÔÛÔ-
ηٷÛÙ·ÏÙÈ΋ ·ÁˆÁ‹ ¯ÔÚËÁ‹ıËΠ·Ú¯ÈÎÒ˜ methylpredni-
zolone (2 mg/kg IV) Î·È ·ÎÔÏÔ‡ıˆ˜ prednizolone (0,2 mg/kg,
per os), ÛÂ Û˘Ó‰˘·ÛÌfi Ì mycophenolate mofetil/ MMF
(CellCept) Î·È Î˘ÎÏÔÛÔÚ›ÓË (Neoral) Û 6 ·È‰È¿, ÂÓÒ Û 7
·È‰È¿, ·ÓÙ› Ù˘ ΢ÎÏÔÛÔÚ›Ó˘, ¯ÔÚËÁ‹ıËΠFK506/
tacrolimus (Prograf).
∞ÔÙÂϤÛÌ·Ù·
∆Ú›· ·È‰È¿ η٤ÏËÍ·Ó ÙÔÓ ÚÒÙÔ ÌÂÙÂÁ¯ÂÈÚËÙÈ-
Îfi Ì‹Ó· ·fi ÌÂÙÂÁ¯ÂÈÚËÙÈΤ˜ ÂÈÏÔΤ˜: ¤Ó· ·fi
ıÚfiÌ‚ˆÛË Ù˘ Ë·ÙÈ΋˜ ·ÚÙËÚ›·˜, ¤Ó· ·fi ıÚfiÌ-
‚ˆÛË Ù˘ ˘Ï·›·˜ ÊϤ‚·˜ Î·È ¤Ó· ·fi ηډÈÔ·Ó·-
Ó¢ÛÙÈ΋ ·Ó¿ÚÎÂÈ·. ∞fi Ù· 13 ·È‰È¿ Ô˘ ·Ú·-
ÎÔÏÔ˘ıԇ̠¤ˆ˜ Û‹ÌÂÚ·, 4 ÂÌÊ¿ÓÈÛ·Ó ÙÔ˘Ï¿¯ÈÛÙÔÓ
¤Ó· ÂÂÈÛfi‰ÈÔ ÔÍ›·˜ ·fiÚÚȄ˘ ÙÔ˘ ÌÔۯ‡̷ÙÔ˜
Ì ̤ÛÔ fiÚÔ ¯ÚfiÓÔ ÂÌÊ¿ÓÈÛ˘ ÙÔ˘˜ 25,7 Ì‹Ó˜ ÌÂÙ¿
ÙË ª∏. ™Ù· ‰‡Ô ·È‰È¿ Ù· ÂÂÈÛfi‰È· ·ÓÙÈÌÂÙˆ›-
ÛÙËÎ·Ó ÂÈÙ˘¯Ò˜ Ì ÒÛÂȘ ÎÔÚÙÈ˙fiÓ˘. ™Ù· ˘fiÏÔÈ-
· ‰‡Ô ··ÈÙ‹ıËΠ¯ÔÚ‹ÁËÛË ·ÓÙÈı˘ÌÔ΢ÙÙ·ÚÈÎÔ‡
ÔÚÔ‡ (ATG), ÏfiÁˆ ·ÓıÂÎÙÈÎfiÙËÙ·˜ Ù˘ ·ÔÚÚÈÙÈ-
΋˜ ‰È·‰Èηۛ·˜ ÛÙ· ÎÔÚÙÈÎÔÛÙÂÚÔÂȉ‹. ™ÙË Ì›· Â-
Ú›ÙˆÛË Ë ·ÓÙ›ÛÙ·ÛË ÛÙË Ê·Ú̷΢ÙÈ΋ ·ÁˆÁ‹
ÔÊ›ÏÂÙÔ ÛÙÔ fiÙÈ Ô ‰fiÙ˘ ‹Ù·Ó Û˘Ì‚·Ù‹˜ Î·È fi¯È
›‰È·˜ ÔÌ¿‰·˜ ·›Ì·ÙÔ˜. √ ·ÛıÂÓ‹˜ ·˘Ùfi˜ ·ÚÔ˘Û›·ÛÂ
¯ÚfiÓÈ· ·fiÚÚÈ„Ë ÙÔ˘ ÌÔۯ‡̷ÙÔ˜, Ë ÔÔ›· fï˜
ÌÂÙÚÈ¿ÛÙËΠ̠·ÏÏ·Á‹ Ù˘ ·ÓÔÛÔηٷÛÙ·ÏÙÈ΋˜
·ÁˆÁ‹˜ ·fi ΢ÎÏÔÛÔÚ›ÓË Û tacrolimus.
∆ÚÔÔÔ›ËÛË Ù˘ ·ÓÔÛÔηٷÛÙ·ÏÙÈ΋˜ ·ÁˆÁ‹˜
ÎÚ›ıËΠ··Ú·›ÙËÙË Û 3 Û˘ÓÔÏÈο ·ÛıÂÓ›˜. ™ÙÔ˘˜
2 ¤ÁÈÓ ·ÏÏ·Á‹ ÙÔ˘ Û¯‹Ì·ÙÔ˜ ·fi cyclosporine ÛÂ
tacrolimus, ÂÍ·ÈÙ›·˜ ¯ÚfiÓÈ·˜ ·fiÚÚȄ˘ ÛÙË Ì›· Â-
Ú›ÙˆÛË -Ë ÔÔ›· ‰ÈÂÁÓÒÛıË Ì ÎÏÂÈÛÙ‹ ‚ÈÔ„›· ÙÔ˘
ÌÔۯ‡̷ÙÔ˜-, Î·È ÓÂÊÚÔÙÔÍÈÎfiÙËÙ·˜ ÛÙËÓ ¿ÏÏË. ∏
ÓÂÊÚÔÙÔÍÈÎfiÙËÙ· ÂΉËÏÒıËΠ̠·‡ÍËÛË Ù˘ ·ÚÙË-
Úȷ΋˜ ›ÂÛ˘, ·‡ÍËÛË Ù˘ Ô˘Ú›·˜ Î·È Ù˘ ÎÚ·ÙÈÓ›-
Ó˘ ÙÔ˘ ÔÚÔ‡ Î·È ÂÏ¿ÙÙˆÛË ÙÔ˘ GFR ηٿ ÙË Ú·‰ÈÔ˚-
ÛÔÙÔÈ΋ ÌÂϤÙË. ∆¤ÏÔ˜, Û ¤Ó· ·È‰› Ú·ÁÌ·ÙÔ-
ÔÈ‹ıËΠ·ÏÏ·Á‹ ·fi tacrolimus Û ΢ÎÏÔÛÔÚ›ÓË,
ÏfiÁˆ ·Ú¯fiÌÂÓ˘ ·ÁÎÚ·ٛÙȉ·˜.
™Â fi,ÙÈ ·ÊÔÚ¿ ÙȘ ÏÔÈÌÒÍÂȘ (¶›Ó·Î·˜ 2), ·ÓÈ-
¯Ó‡ıËÎ·Ó Î˘Ú›ˆ˜ ÔÈ ÈÔ› CMV, EBV Î·È Parvo µ19 ÌÂ
ÙË Ì¤ıÔ‰Ô Ù˘ ·Ï˘ÛȉˆÙ‹˜ ·ÓÙ›‰Ú·Û˘ Ù˘ ÔÏ˘ÌÂ-
Ú¿Û˘ (PCR). ∂›Û˘, 2 ·È‰È¿ ·ÚÔ˘Û›·Û·Ó Ïԛ̈-
ÍË ·fi HSV, 1 ·fi Coxsackie Î·È 1 ·fi Candida
albicans. √È ÏÔÈÌÒÍÂȘ ·˘Ù¤˜ ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó ÂÈ-
Ù˘¯Ò˜ Ì ÂÏ¿ÙÙˆÛË Ù˘ ·ÓÔÛÔηٷÛÙÔÏ‹˜ Î·È ÙË
¯ÔÚ‹ÁËÛË gancyclovir, acyclovir ‹ amphotericin B.
ªÈÎÚԂȷ΋ Ïԛ̈ÍË ‰ÂÓ ÂÌÊ¿ÓÈÛ ηӤӷ˜ ·fi
ÙÔ˘˜ ·ÛıÂÓ›˜ Ì·˜.
ÕÏϘ ÂÈÏÔΤ˜ Ù˘ ·ÓÔÛÔηٷÛÙ·ÏÙÈ΋˜ ·Áˆ-
Á‹˜, ‹Ù·Ó Á·ÛÙÚÔÚÚ·Á›· Î·È ˘ÂÚÔ˘Úȯ·ÈÌ›·. ∆¤ÏÔ˜,
¤Ó·˜ ·ÛıÂÓ‹˜ ÂÌÊ¿ÓÈÛ ÓfiÛÔ ÂÍ·Ê¿ÓÈÛ˘ ÙˆÓ ÌÈ-
ÎÚÒÓ ¯ÔÏËÊfiÚˆÓ fiÚˆÓ ‡ÛÙÂÚ· ·fi ‰È·‰Ô¯ÈΤ˜
ÏÔÈÌÒÍÂȘ ·fi ÙÔ˘˜ ÈÔ‡˜ Parvo B19, CMV Î·È EBV
ηٿ ÙËÓ ÚÒÙË ÌÂÙÂÁ¯ÂÈÚËÙÈ΋ ÂÚ›Ô‰Ô, Ë ÔÔ›·
Ô‰‹ÁËÛ Û ΛÚÚˆÛË Î·È ˘Ï·›· ˘¤ÚÙ·ÛË, Ì ·Ô-
Ù¤ÏÂÛÌ· Ó· ¯ÚÂÈ·ÛÙ› ·ӷÌÂÙ·ÌfiÛ¯Â˘ÛË.
™Â fi,ÙÈ ·ÊÔÚ¿ ÙË ÛˆÌ·ÙÈ΋ ·Ó¿Ù˘ÍË, ¤ÍÈ ·È‰È¿
¤¯Ô˘Ó Û‹ÌÂÚ· ‚¿ÚÔ˜ ÛÒÌ·ÙÔ˜ ¿Óˆ ·fi ÙËÓ 50‹
ÂηÙÔÛÙÈ·›· ı¤ÛË Ì ‚¿ÛË ÙȘ η̇Ϙ ·Ó¿Ù˘Í˘,
2 ÌÂٷ͇ 50‹˜ Î·È 25˘ ∂£ Î·È Ù· ˘fiÏÔÈ· οو
·fi ÙË 10Ë ∂£. ∆· ·È‰È¿ Ô˘ ‚Ú›ÛÎÔÓÙ·È ¿Óˆ ·fi
ÙËÓ 50‹ ∂£ ˘Ô‚Ï‹ıËÎ·Ó ÛÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË ÛÂ
ËÏÈ˘ ·fi 3 ¤ˆ˜ 8 ÂÙÒÓ Î·È ‚Ú›ÛÎÔÓÙ·Ó ÛÙȘ ›‰È˜
∂£ ÚÈÓ ·fi ÙË ª∏. ŸÛÔÓ ·ÊÔÚ¿ ÙÔ ‡„Ô˜, 7 ·È‰È¿
‚Ú›ÛÎÔÓÙ·È Û‹ÌÂÚ· ¿Óˆ ·fi ÙË 50‹ ∂£, ÂÓÒ 6
¤¯Ô˘Ó ‡„Ô˜ ›ÛÔ ‹ οو ·fi ÙËÓ 10Ë ∂£. ∆· ·È‰È¿
143ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ ÛÙ· ·È‰È¿
¶·È‰È·ÙÚÈ΋ 2008;71:141-147
¶›Ó·Î·˜ 2. ∂ÈÏÔΤ˜ Ô˘ ·Ú·ÙËÚ‹ıËÎ·Ó Î·Ù¿ ÙËÓ ·Ú·ÎÔÏÔ‡-ıËÛË ÙˆÓ ·ÛıÂÓÒÓ Ì·˜
∂ÈÏÔ΋ ∞ÚÈıÌfi˜ ·ÛıÂÓÒÓ
§Ô›ÌˆÍËñ CMV 5ñ EBV 5ñ Parvo B19 2ñ HSV1,2 2ñ Coxsackie 1ñ Candida albicans 1
∞fiÚÚÈ„Ë ÌÔۯ‡̷ÙÔ˜ 4∞ÈÌÔÚÚ·Á›· ·ÓÒÙÂÚÔ˘ °∂™ 1ÀÂÚÔ˘Úȯ·ÈÌ›· 1∂Í·Ê¿ÓÈÛË ÌÈÎÚÒÓ ¯ÔÏËÊfiÚˆÓ fiÚˆÓ 1
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·143
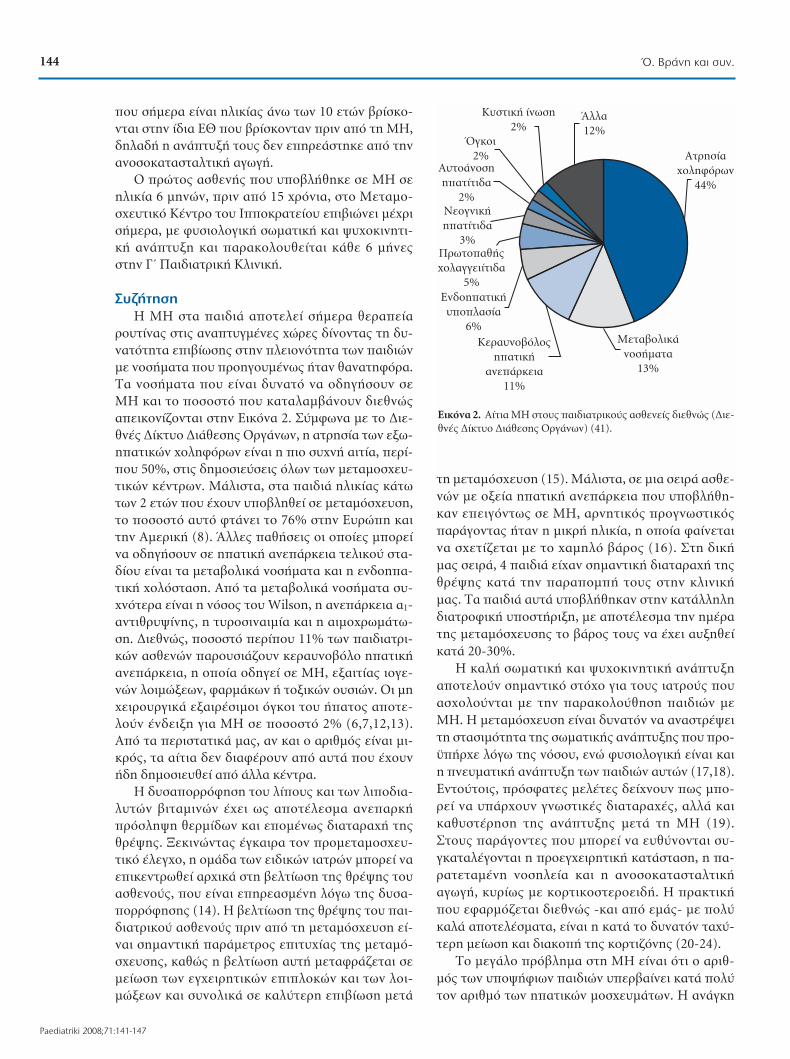
Ô˘ Û‹ÌÂÚ· Â›Ó·È ËÏÈΛ·˜ ¿Óˆ ÙˆÓ 10 ÂÙÒÓ ‚Ú›ÛÎÔ-
ÓÙ·È ÛÙËÓ ›‰È· ∂£ Ô˘ ‚Ú›ÛÎÔÓÙ·Ó ÚÈÓ ·fi ÙË ª∏,
‰ËÏ·‰‹ Ë ·Ó¿Ù˘Í‹ ÙÔ˘˜ ‰ÂÓ ÂËÚ¿ÛÙËΠ·fi ÙËÓ
·ÓÔÛÔηٷÛÙ·ÏÙÈ΋ ·ÁˆÁ‹.
√ ÚÒÙÔ˜ ·ÛıÂÓ‹˜ Ô˘ ˘Ô‚Ï‹ıËΠ۠ª∏ ÛÂ
ËÏÈΛ· 6 ÌËÓÒÓ, ÚÈÓ ·fi 15 ¯ÚfiÓÈ·, ÛÙÔ ªÂÙ·ÌÔ-
Û¯Â˘ÙÈÎfi ∫¤ÓÙÚÔ ÙÔ˘ πÔÎÚ·Ù›Ԣ ÂÈ‚ÈÒÓÂÈ Ì¤¯ÚÈ
Û‹ÌÂÚ·, ÌÂ Ê˘ÛÈÔÏÔÁÈ΋ ۈ̷ÙÈ΋ Î·È „˘¯ÔÎÈÓËÙÈ-
΋ ·Ó¿Ù˘ÍË Î·È ·Ú·ÎÔÏÔ˘ıÂ›Ù·È Î¿ı 6 Ì‹Ó˜
ÛÙËÓ °ã ¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋.
™˘˙‹ÙËÛË
∏ ª∏ ÛÙ· ·È‰È¿ ·ÔÙÂÏ› Û‹ÌÂÚ· ıÂڷ›·
ÚÔ˘Ù›Ó·˜ ÛÙȘ ·Ó·Ù˘Á̤Ó˜ ¯ÒÚ˜ ‰›ÓÔÓÙ·˜ ÙË ‰˘-
Ó·ÙfiÙËÙ· ÂÈ‚›ˆÛ˘ ÛÙËÓ ÏÂÈÔÓfiÙËÙ· ÙˆÓ ·È‰ÈÒÓ
Ì ÓÔÛ‹Ì·Ù· Ô˘ ÚÔËÁÔ˘Ì¤Óˆ˜ ‹Ù·Ó ı·Ó·ÙËÊfiÚ·.
∆· ÓÔÛ‹Ì·Ù· Ô˘ Â›Ó·È ‰˘Ó·Ùfi Ó· Ô‰ËÁ‹ÛÔ˘Ó ÛÂ
ª∏ Î·È ÙÔ ÔÛÔÛÙfi Ô˘ ηٷϷ̂¿ÓÔ˘Ó ‰ÈÂıÓÒ˜
·ÂÈÎÔÓ›˙ÔÓÙ·È ÛÙËÓ ∂ÈÎfiÓ· 2. ™‡Ìʈӷ Ì ÙÔ ¢ÈÂ-
ıÓ¤˜ ¢›ÎÙ˘Ô ¢È¿ıÂÛ˘ √ÚÁ¿ÓˆÓ, Ë ·ÙÚËÛ›· ÙˆÓ Â͈-
Ë·ÙÈÎÒÓ ¯ÔÏËÊfiÚˆÓ Â›Ó·È Ë ÈÔ Û˘¯Ó‹ ·ÈÙ›·, ÂÚ›-
Ô˘ 50%, ÛÙȘ ‰ËÌÔÛȇÛÂȘ fiÏˆÓ ÙˆÓ ÌÂÙ·ÌÔÛ¯Â˘-
ÙÈÎÒÓ Î¤ÓÙÚˆÓ. ª¿ÏÈÛÙ·, ÛÙ· ·È‰È¿ ËÏÈΛ·˜ οو
ÙˆÓ 2 ÂÙÒÓ Ô˘ ¤¯Ô˘Ó ˘Ô‚ÏËı› Û ÌÂÙ·ÌfiÛ¯Â˘ÛË,
ÙÔ ÔÛÔÛÙfi ·˘Ùfi ÊÙ¿ÓÂÈ ÙÔ 76% ÛÙËÓ ∂˘ÚÒË Î·È
ÙËÓ ∞ÌÂÚÈ΋ (8). ÕÏϘ ·ı‹ÛÂȘ ÔÈ Ôԛ˜ ÌÔÚ›
Ó· Ô‰ËÁ‹ÛÔ˘Ó Û ˷ÙÈ΋ ·Ó¿ÚÎÂÈ· ÙÂÏÈÎÔ‡ ÛÙ·-
‰›Ô˘ Â›Ó·È Ù· ÌÂÙ·‚ÔÏÈο ÓÔÛ‹Ì·Ù· Î·È Ë ÂÓ‰ÔË·-
ÙÈ΋ ¯ÔÏfiÛÙ·ÛË. ∞fi Ù· ÌÂÙ·‚ÔÏÈο ÓÔÛ‹Ì·Ù· Û˘-
¯ÓfiÙÂÚ· Â›Ó·È Ë ÓfiÛÔ˜ ÙÔ˘ Wilson, Ë ·Ó¿ÚÎÂÈ· ·1-
·ÓÙÈıÚ˘„›Ó˘, Ë Ù˘ÚÔÛÈÓ·ÈÌ›· Î·È Ë ·ÈÌԯڈ̿و-
ÛË. ¢ÈÂıÓÒ˜, ÔÛÔÛÙfi ÂÚ›Ô˘ 11% ÙˆÓ ·È‰È·ÙÚÈ-
ÎÒÓ ·ÛıÂÓÒÓ ·ÚÔ˘ÛÈ¿˙Ô˘Ó ÎÂÚ·˘ÓÔ‚fiÏÔ Ë·ÙÈ΋
·Ó¿ÚÎÂÈ·, Ë ÔÔ›· Ô‰ËÁ› Û ª∏, ÂÍ·ÈÙ›·˜ ÈÔÁÂ-
ÓÒÓ ÏÔÈÌÒ͈Ó, Ê·ÚÌ¿ÎˆÓ ‹ ÙÔÍÈÎÒÓ Ô˘ÛÈÒÓ. √È ÌË
¯ÂÈÚÔ˘ÚÁÈο ÂÍ·ÈÚ¤ÛÈÌÔÈ fiÁÎÔÈ ÙÔ˘ ‹·ÙÔ˜ ·ÔÙÂ-
ÏÔ‡Ó ¤Ó‰ÂÈÍË ÁÈ· ª∏ Û ÔÛÔÛÙfi 2% (6,7,12,13).
∞fi Ù· ÂÚÈÛÙ·ÙÈο Ì·˜, ·Ó Î·È Ô ·ÚÈıÌfi˜ Â›Ó·È ÌÈ-
ÎÚfi˜, Ù· ·›ÙÈ· ‰ÂÓ ‰È·Ê¤ÚÔ˘Ó ·fi ·˘Ù¿ Ô˘ ¤¯Ô˘Ó
‹‰Ë ‰ËÌÔÛÈ¢ı› ·fi ¿ÏÏ· ΤÓÙÚ·.
∏ ‰˘Û·ÔÚÚfiÊËÛË ÙÔ˘ Ï›Ô˘˜ Î·È ÙˆÓ ÏÈԉȷ-
Ï˘ÙÒÓ ‚ÈÙ·ÌÈÓÒÓ ¤¯ÂÈ ˆ˜ ·ÔÙ¤ÏÂÛÌ· ·Ó·Ú΋
ÚfiÛÏË„Ë ıÂÚÌ›‰ˆÓ Î·È ÂÔ̤ӈ˜ ‰È·Ù·Ú·¯‹ Ù˘
ıÚ¤„˘. •ÂÎÈÓÒÓÙ·˜ ¤ÁηÈÚ· ÙÔÓ ÚÔÌÂÙ·ÌÔÛ¯Â˘-
ÙÈÎfi ¤ÏÂÁ¯Ô, Ë ÔÌ¿‰· ÙˆÓ ÂȉÈÎÒÓ È·ÙÚÒÓ ÌÔÚ› Ó·
ÂÈÎÂÓÙÚˆı› ·Ú¯Èο ÛÙË ‚ÂÏÙ›ˆÛË Ù˘ ıÚ¤„˘ ÙÔ˘
·ÛıÂÓÔ‡˜, Ô˘ Â›Ó·È ÂËÚ·Ṳ̂ÓË ÏfiÁˆ Ù˘ ‰˘Û·-
ÔÚÚfiÊËÛ˘ (14). ∏ ‚ÂÏÙ›ˆÛË Ù˘ ıÚ¤„˘ ÙÔ˘ ·È-
‰È·ÙÚÈÎÔ‡ ·ÛıÂÓÔ‡˜ ÚÈÓ ·fi ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË Â›-
Ó·È ÛËÌ·ÓÙÈ΋ ·Ú¿ÌÂÙÚÔ˜ ÂÈÙ˘¯›·˜ Ù˘ ÌÂÙ·Ìfi-
Û¯Â˘Û˘, ηıÒ˜ Ë ‚ÂÏÙ›ˆÛË ·˘Ù‹ ÌÂÙ·ÊÚ¿˙ÂÙ·È ÛÂ
Ì›ˆÛË ÙˆÓ ÂÁ¯ÂÈÚËÙÈÎÒÓ ÂÈÏÔÎÒÓ Î·È ÙˆÓ ÏÔÈ-
ÌÒÍÂˆÓ Î·È Û˘ÓÔÏÈο Û ηχÙÂÚË ÂÈ‚›ˆÛË ÌÂÙ¿
ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË (15). ª¿ÏÈÛÙ·, Û ÌÈ· ÛÂÈÚ¿ ·ÛıÂ-
ÓÒÓ Ì ÔÍ›· Ë·ÙÈ΋ ·Ó¿ÚÎÂÈ· Ô˘ ˘Ô‚Ï‹ıË-
Î·Ó ÂÂÈÁfiÓÙˆ˜ Û ª∏, ·ÚÓËÙÈÎfi˜ ÚÔÁÓˆÛÙÈÎfi˜
·Ú¿ÁÔÓÙ·˜ ‹Ù·Ó Ë ÌÈÎÚ‹ ËÏÈΛ·, Ë ÔÔ›· Ê·›ÓÂÙ·È
Ó· Û¯ÂÙ›˙ÂÙ·È Ì ÙÔ ¯·ÌËÏfi ‚¿ÚÔ˜ (16). ™ÙË ‰È΋
Ì·˜ ÛÂÈÚ¿, 4 ·È‰È¿ ›¯·Ó ÛËÌ·ÓÙÈ΋ ‰È·Ù·Ú·¯‹ Ù˘
ıÚ¤„˘ ηٿ ÙËÓ ·Ú·ÔÌ‹ ÙÔ˘˜ ÛÙËÓ ÎÏÈÓÈ΋
Ì·˜. ∆· ·È‰È¿ ·˘Ù¿ ˘Ô‚Ï‹ıËÎ·Ó ÛÙËÓ Î·Ù¿ÏÏËÏË
‰È·ÙÚÔÊÈ΋ ˘ÔÛÙ‹ÚÈÍË, Ì ·ÔÙ¤ÏÂÛÌ· ÙËÓ Ë̤ڷ
Ù˘ ÌÂÙ·ÌfiÛ¯Â˘Û˘ ÙÔ ‚¿ÚÔ˜ ÙÔ˘˜ Ó· ¤¯ÂÈ ·˘ÍËı›
ηٿ 20-30%.
∏ ηϋ ۈ̷ÙÈ΋ Î·È „˘¯ÔÎÈÓËÙÈ΋ ·Ó¿Ù˘ÍË
·ÔÙÂÏÔ‡Ó ÛËÌ·ÓÙÈÎfi ÛÙfi¯Ô ÁÈ· ÙÔ˘˜ È·ÙÚÔ‡˜ Ô˘
·Û¯ÔÏÔ‡ÓÙ·È Ì ÙËÓ ·Ú·ÎÔÏÔ‡ıËÛË ·È‰ÈÒÓ ÌÂ
ª∏. ∏ ÌÂÙ·ÌfiÛ¯Â˘ÛË Â›Ó·È ‰˘Ó·ÙfiÓ Ó· ·Ó·ÛÙÚ¤„ÂÈ
ÙË ÛÙ·ÛÈÌfiÙËÙ· Ù˘ ۈ̷ÙÈ΋˜ ·Ó¿Ù˘Í˘ Ô˘ ÚÔ-
¸‹Ú¯Â ÏfiÁˆ Ù˘ ÓfiÛÔ˘, ÂÓÒ Ê˘ÛÈÔÏÔÁÈ΋ Â›Ó·È Î·È
Ë ÓÂ˘Ì·ÙÈ΋ ·Ó¿Ù˘ÍË ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ (17,18).
∂ÓÙÔ‡ÙÔȘ, ÚfiÛÊ·Ù˜ ÌÂϤÙ˜ ‰Â›¯ÓÔ˘Ó ˆ˜ ÌÔ-
Ú› Ó· ˘¿Ú¯Ô˘Ó ÁÓˆÛÙÈΤ˜ ‰È·Ù·Ú·¯¤˜, ·ÏÏ¿ ηÈ
ηı˘ÛÙ¤ÚËÛË Ù˘ ·Ó¿Ù˘Í˘ ÌÂÙ¿ ÙË ª∏ (19).
™ÙÔ˘˜ ·Ú¿ÁÔÓÙ˜ Ô˘ ÌÔÚ› Ó· ¢ı‡ÓÔÓÙ·È Û˘-
ÁηٷϤÁÔÓÙ·È Ë ÚÔÂÁ¯ÂÈÚËÙÈ΋ ηٿÛÙ·ÛË, Ë ·-
Ú·ÙÂٷ̤ÓË ÓÔÛËÏ›· Î·È Ë ·ÓÔÛÔηٷÛÙ·ÏÙÈ΋
·ÁˆÁ‹, ΢ڛˆ˜ Ì ÎÔÚÙÈÎÔÛÙÂÚÔÂȉ‹. ∏ Ú·ÎÙÈ΋
Ô˘ ÂÊ·ÚÌfi˙ÂÙ·È ‰ÈÂıÓÒ˜ -Î·È ·fi ÂÌ¿˜- Ì Ôχ
ηϿ ·ÔÙÂϤÛÌ·Ù·, Â›Ó·È Ë Î·Ù¿ ÙÔ ‰˘Ó·ÙfiÓ Ù·¯‡-
ÙÂÚË Ì›ˆÛË Î·È ‰È·ÎÔ‹ Ù˘ ÎÔÚÙÈ˙fiÓ˘ (20-24).
∆Ô ÌÂÁ¿ÏÔ Úfi‚ÏËÌ· ÛÙË ª∏ Â›Ó·È fiÙÈ Ô ·ÚÈı-
Ìfi˜ ÙˆÓ ˘Ô„‹ÊÈˆÓ ·È‰ÈÒÓ ˘ÂÚ‚·›ÓÂÈ Î·Ù¿ Ôχ
ÙÔÓ ·ÚÈıÌfi ÙˆÓ Ë·ÙÈÎÒÓ ÌÔÛ¯Â˘Ì¿ÙˆÓ. ∏ ·Ó¿ÁÎË
144 Ÿ. µÚ¿ÓË Î·È Û˘Ó.
Paediatriki 2008;71:141-147
∞ÙÚËÛ›·
¯ÔÏËÊfiÚˆÓ
44%
ªÂÙ·‚ÔÏÈο
ÓÔÛ‹Ì·Ù·
13%
∫ÂÚ·˘ÓÔ‚fiÏÔ˜
Ë·ÙÈ΋
·Ó¿ÚÎÂÈ·
11%
∂Ó‰ÔË·ÙÈ΋
˘ÔÏ·Û›·
6%
¶ÚˆÙÔ·ı‹˜
¯ÔÏ·ÁÁÂÈ›Ùȉ·
5%
¡ÂÔÁÓÈ΋
Ë·Ù›Ùȉ·
3%
∞˘ÙÔ¿ÓÔÛË
Ë·Ù›Ùȉ·
2%
ŸÁÎÔÈ
2%
∫˘ÛÙÈ΋ ›ÓˆÛË
2%ÕÏÏ·
12%
∂ÈÎfiÓ· 2. ∞›ÙÈ· ª∏ ÛÙÔ˘˜ ·È‰È·ÙÚÈÎÔ‡˜ ·ÛıÂÓ›˜ ‰ÈÂıÓÒ˜ (¢ÈÂ-ıÓ¤˜ ¢›ÎÙ˘Ô ¢È¿ıÂÛ˘ √ÚÁ¿ÓˆÓ) (41).
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·144

ÌÈÎÚÔ‡ ÌÂÁ¤ıÔ˘˜ ÌÔÛ¯Â˘Ì¿ÙˆÓ ÛÂ Û˘Ó¿ÚÙËÛË ÌÂ
ÙËÓ ¤ÏÏÂÈ„Ë ÙˆÌ·ÙÈÎÒÓ ‰ÔÙÒÓ ÌÈÎÚ‹˜ ËÏÈΛ·˜
ÚÔοÏÂÛ ÙËÓ ·Ó·˙‹ÙËÛË ÂÓ·ÏÏ·ÎÙÈÎÒÓ ËÁÒÓ
ÌÔÛ¯Â˘Ì¿ÙˆÓ. ¢‡Ô ÂÁ¯ÂÈÚËÙÈΤ˜ ̤ıÔ‰ÔÈ Ô˘ ÚÔ-
ÛʤÚÔ˘Ó ÂÓı·ÚÚ˘ÓÙÈο ·ÔÙÂϤÛÌ·Ù·, Â›Ó·È Ë Ï‹„Ë
ÙÌ‹Ì·ÙÔ˜ ÙÔ˘ ‹·ÙÔ˜ ·fi ˙ÒÓÙ· ‰fiÙË Î·È Ë ¯ÂÈ-
ÚÔ˘ÚÁÈ΋ ‰È·›ÚÂÛË Û ‰‡Ô ÏÂÈÙÔ˘ÚÁÈο ÙÌ‹Ì·Ù· ÙÔ˘
و̷ÙÈÎÔ‡ ÌÔۯ‡̷ÙÔ˜ ÂÓ‹ÏÈη ‰fiÙË, ÒÛÙ ӷ
ÌÂÙ·ÌÔÛ¯Â˘ı› Û ‰‡Ô Ï‹Ù˜ (11,25). √È Ì¤ıÔ‰ÔÈ
·˘Ù¤˜ ·ÚÔ˘ÛÈ¿˙Ô˘Ó Î·Ïfi ÔÛÔÛÙfi ÂÈ‚›ˆÛ˘ ÙÔ˘
ÌÔۯ‡̷ÙÔ˜ Î·È ÙÔ˘ Ï‹ÙË Î·È ¤¯Ô˘Ó ϤÔÓ Î·ıÈÂ-
Úˆı› ÛÙÔ˘˜ ·È‰È·ÙÚÈÎÔ‡˜ ·ÛıÂÓ›˜ (26-30). ∆Ô ÁÂ-
ÁÔÓfi˜ ·˘Ùfi ÂȂ‚·ÈÒÓÂÈ ÌÈ· ÌÂÁ¿ÏË ÌÂÙ·-·Ó¿Ï˘ÛË,
Ë ÔÔ›· ‰Â›¯ÓÂÈ fiÙÈ Ë ÂÈ‚›ˆÛË Â›Ó·È Î·Ï‡ÙÂÚË ÁÈ·
ÙÔ˘˜ ·ÛıÂÓ›˜ ‡ÛÙÂÚ· ·fi ÌÂÙ·ÌfiÛ¯Â˘ÛË ·fi ˙Ò-
ÓÙ· ‰fiÙË Û˘ÁÎÚÈÙÈο Ì ·˘Ù‹ ·fi و̷ÙÈÎfi ‰fiÙË,
·ÊÂÓfi˜ ‰ÈfiÙÈ ÔÈ ·ÛıÂÓ›˜ ‰ÂÓ ÂÈ‚·Ú‡ÓÔ˘Ó ÙË ÁÂÓÈ΋
ÙÔ˘˜ ηٿÛÙ·ÛË ·Ó·Ì¤ÓÔÓÙ·˜ و̷ÙÈÎfi ÌfiÛ¯Â˘Ì·
Î·È ·ÊÂÙ¤ÚÔ˘ ÁÈ·Ù› ÔÈ ¯ÚfiÓÔÈ ıÂÚÌ‹˜ Î·È „˘¯Ú‹˜
ÈÛ¯·ÈÌ›·˜ Â›Ó·È ÌÈÎÚfiÙÂÚÔÈ (31). ∂ÓÙÔ‡ÙÔȘ, ı· Ú¤-
ÂÈ Ó· ÂÈϤÁÔÓÙ·È Ôχ ÚÔÛÂÎÙÈο ÔÈ ˘Ô„‹ÊÈÔÈ
˙ÒÓÙ˜ ‰fiÙ˜ Ë·ÙÈÎÔ‡ ÌÔۯ‡̷ÙÔ˜, ÂÍ·ÈÙ›·˜ ÙˆÓ
ÂÈÏÔÎÒÓ Ô˘ ÌÔÚ› Ó· ·ÚÔ˘ÛÈ·ÛÙÔ‡Ó ÛÙÔ ‰fiÙË
ÌÂÙ¿ ÙËÓ Ë·ÙÂÎÙÔÌ‹ (.¯. ¯ÔÏfiÚÚÔÈ·, ıÚfiÌ‚ˆÛË
˘Ï·›·˜ ‹ Û‡ÛÙÔÈ¯Ë Ó¢ÌÔÓÈ΋ Û˘ÏÏÔÁ‹), ·ÏÏ¿ ηÈ
Ù˘ ıÓËÛÈÌfiÙËÙ·˜ ·ÎfiÌË, Ë ÔÔ›·, fï˜, Â›Ó·È ÂÍ·È-
ÚÂÙÈο ÌÈÎÚ‹ (0,01%).
ªÂ ÙË Û˘Ó¯fiÌÂÓË ·‡ÍËÛË ÙˆÓ ˘Ô„ËÊ›ˆÓ ÁÈ·
ª∏ -ηıÒ˜ Ì ÙËÓ ·‡ÍËÛË Ù˘ ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙË-
Ù·˜ Ù˘ ‰È¢ڇÓıËÎ·Ó Î·È ÔÈ ÂӉ›ÍÂȘ Ù˘-, ÚԤ΢-
„ ¤Ó· ·ÎfiÌË ˙‹ÙËÌ·: Ë ÛˆÛÙ‹ ¯Ú‹ÛË ÙˆÓ ‰È·ÙÈı¤-
ÌÂÓˆÓ ÔÚÁ¿ÓˆÓ. ŸÙ·Ó ¿Ú¯ÈÛ ӷ ÂÊ·ÚÌfi˙ÂÙ·È Ë ª∏,
Ë ‰È¿ıÂÛË ÙˆÓ ÔÚÁ¿ÓˆÓ ÁÈÓfiÙ·Ó Ì ‚¿ÛË ÙÔ ¯ÚfiÓÔ
·Ó·ÌÔÓ‹˜. °Ú‹ÁÔÚ·, fï˜, ¤ÁÈÓ ·ÈÛıËÙ‹ Ë ·Ó¿ÁÎË
‡·Ú͢ ÂÓfi˜ Û˘ÛÙ‹Ì·ÙÔ˜ ·ÍÈÔÏfiÁËÛ˘ Ô˘ ı· η-
ıfiÚÈ˙ ÙËÓ ÚÔÙÂÚ·ÈfiÙËÙ· ÙˆÓ ˘Ô„‹ÊÈˆÓ ÏËÙÒÓ.
∏ ·ÍÈÔÏfiÁËÛË ‚·Û›ÛÙËΠÛÙÔ ÛÙ¿‰ÈÔ Ù˘ Ë·ÙÈ΋˜
ÓfiÛÔ˘ ηٿ Child-Turcotte-Pugh Î·È ÛÙȘ Ù˘¯fiÓ Û˘-
Ó˘¿Ú¯Ô˘Û˜ ÂÈÏÔΤ˜ Ù˘, fiˆ˜ ·ÛΛÙ˘, ÎÈÚÛÔÚ-
Ú·Á›· ‹ Ë·ÙÔ΢ÙÙ·ÚÈÎfi˜ ηÚΛÓÔ˜ (32). ∏ ÏÂÈÔÓfi-
ÙËÙ· ÙˆÓ ÌÂÙ·ÌÔÛ¯Â˘ÙÈÎÒÓ Î¤ÓÙÚˆÓ ÛÙËÓ ∂˘ÚÒË
-Û˘ÌÂÚÈÏ·Ì‚·ÓÔ̤Ó˘ Î·È Ù˘ ∫ÏÈÓÈ΋˜ ªÂÙ·ÌÔ-
ۯ‡ÛÂˆÓ ÙÔ˘ ∞¶£- Î·È ÛÙËÓ ∞˘ÛÙÚ·Ï›·, Û˘Ó¯›-
˙Ô˘Ó Ó· ¯ÚËÛÈÌÔÔÈÔ‡Ó ·˘Ùfi ÙÔ Û‡ÛÙËÌ·. ™ÙȘ ∏¶∞
ÂÈÛ‹¯ıË ·fi ÙȘ ·Ú¯¤˜ ÙÔ˘ 2002 ¤Ó· Ó¤Ô Û‡ÛÙËÌ·, ÙÔ
ÔÔ›Ô ‚·Û›˙ÂÙ·È ÛÙËÓ ·ÍÈÔÏfiÁËÛË ÙÔ˘ ÎÈÓ‰‡ÓÔ˘ Ô˘
·ÔÚÚ¤ÂÈ ·fi ÙË ÌË ‰ÈÂÓ¤ÚÁÂÈ· ÌÂÙ·ÌfiÛ¯Â˘Û˘, ÙÔ
ÏÂÁfiÌÂÓÔ MELD (Model for End-Stage Liver Disease)
ÁÈ· ÙÔ˘˜ ÂÓ‹ÏÈΘ Î·È PELD (Pediatric End-Stage
Liver Disease) ÁÈ· Ù· ·È‰È¿. ∆Ô ·Ó ·˘Ùfi ÙÔ Û‡ÛÙËÌ·
Á›ÓÂÈ Î·ıÔÏÈο ·Ô‰ÂÎÙfi ·fi ÙË ÌÂÙ·ÌÔÛ¯Â˘ÙÈ΋
ÎÔÈÓfiÙËÙ·, ̤ÓÂÈ Ó· ·Ô‰Âȯı› ÛÙÔ Ì¤ÏÏÔÓ (33,34).
√È ÏÔÈÌÒÍÂȘ ·ÔÙÂÏÔ‡Ó ÙËÓ ÈÔ ÛËÌ·ÓÙÈ΋ ÂÈ-
ÏÔ΋ Ù˘ ª∏ ÌÂÙ¿ ÙË ıÚfiÌ‚ˆÛË Ù˘ Ë·ÙÈ΋˜ ·Ú-
ÙËÚ›·˜, Ë ÔÔ›· ÂÌÊ·Ó›˙ÂÙ·È Î·Ù¿ ÙȘ ÚÒÙ˜ ÌÂÙÂÁ-
¯ÂÈÚËÙÈΤ˜ Ë̤Ú˜. ∆ËÓ ÚÒÙË ÌÂÙÂÁ¯ÂÈÚËÙÈ΋ Â-
Ú›Ô‰Ô Î˘ÚÈ·Ú¯Ô‡Ó ÔÈ ÌÈÎÚԂȷΤ˜ ÏÔÈÌÒÍÂȘ, ÂÓÒ Â-
Ú›Ô˘ 2 ‚‰ÔÌ¿‰Â˜ ·ÚÁfiÙÂÚ· ˘¿Ú¯ÂÈ ÌÂÁ·Ï‡ÙÂÚÔ˜
ΛӉ˘ÓÔ˜ ÏÔÈÌÒÍÂˆÓ ·fi ̇ÎËÙ˜. ™ÙË Û˘Ó¤¯ÂÈ·, ÌÂ-
Ù¿ ÙȘ 6 ‚‰ÔÌ¿‰Â˜ Î·È ÁÈ· fiÏË ÙË ‰È¿ÚÎÂÈ· ˙ˆ‹˜ ÙÔ˘
·ÛıÂÓÔ‡˜, ÂÈÎÚ·Ù› Ô Î›Ó‰˘ÓÔ˜ ÈÔÁÂÓÒÓ ÏÔÈÌÒ͈Ó.
°È· ÙÔ ÏfiÁÔ ·˘Ùfi, ÔÏÏÔ› ·ÛıÂÓ›˜ Ï·Ì‚¿ÓÔ˘Ó ¯ËÌÂÈ-
ÔÚÔʇϷÍË ÌÂÙ¿ ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË. ∆· ·ÓÙÈ‚ÈÔÙÈο
Î·È Ù· ·ÓÙÈÌ˘ÎËÙÈ·ÛÈο ‰È·ÎfiÙÔÓÙ·È ÌÂÚÈΤ˜ ‚‰Ô-
Ì¿‰Â˜ ÌÂÙ¿ ÙË ÌÂÙ·ÌfiÛ¯Â˘ÛË, Â¿Ó ‰ÂÓ ˘¿Ú¯Ô˘Ó ÂÓ-
‰Â›ÍÂȘ Ïԛ̈͢, ÂÓÒ Ù· ·ÓÙÈ-ÈÈο ¤¯Ô˘Ó ı¤ÛË ÙÔ˘˜
ÚÒÙÔ˘˜ Ì‹Ó˜. √È ÈÔ Û˘¯ÓÔ› ÈÔ› Â›Ó·È Ô CMV, o
EBV, ÔÈ ·‰ÂÓÔ˚Ô› Î·È Ô RSV (35). √ EBV Â›Ó·È È‰È·›ÙÂ-
Ú· ÛËÌ·ÓÙÈÎfi˜ Èfi˜, ηıÒ˜ Û¯ÂÙ›˙ÂÙ·È Ì ÙË ÏÂÌÊÔ¸-
ÂÚÏ·ÛÙÈ΋ ÓfiÛÔ (post transplant lympho-
proliferative disease, PTLD) (36). ™‡Ìʈӷ Ì ٷ Â-
ÚÈÛÙ·ÙÈο Ì·˜, Û˘¯ÓfiÙÂÚË ÂÌÊ¿ÓÈÛË ¤¯Ô˘Ó ÔÈ ÈÔ› EBV
Î·È CMV Î·È ·ÎÔÏÔ˘ıÔ‡Ó Ô Parvo B19, Ô HSV1,2, Ô
Coxsackie Î·È Ë Candida albicans.
∂ÎÙfi˜ ·fi ÙÔÓ Î›Ó‰˘ÓÔ Ù˘ ·fiÚÚȄ˘ ÙÔ˘ ÌÔ-
ۯ‡̷ÙÔ˜, ¿ÏÏÔÈ ·Ú¿ÁÔÓÙ˜ Ô˘ ·˘Í¿ÓÔ˘Ó ÙË ÓÔ-
ÛËÚfiÙËÙ· ÙˆÓ ·È‰ÈÒÓ ÌÂÙ¿ ÙË ª∏ Â›Ó·È ÔÈ ÂÈÏÔ-
Τ˜ Ù˘ ·ÓÔÛÔηٷÛÙ·ÏÙÈ΋˜ ·ÁˆÁ‹˜, fiˆ˜ Ë ÓÂ-
ÊÚÔÙÔÍÈÎfiÙËÙ· ÙˆÓ ·Ó·ÛÙÔϤˆÓ Ù˘ ηÏÛÈÓ¢ڛÓ˘
(Neoral, Prograf), Ë Ó¢ÚÔÙÔÍÈÎfiÙËÙ·, Ë ÔÛÙÂÔ-
fiÚˆÛË Î·È Ë Î·Ú‰È·ÁÁÂȷ΋ ÓfiÛÔ˜ (37-39). ∏ ‰È·-
Ù‹ÚËÛË Î·Ï‹˜ ÓÂÊÚÈ΋˜ ÏÂÈÙÔ˘ÚÁ›·˜ Ï·Ì‚¿ÓÂÙ·È ÛÔ-
‚·Ú¿ ˘fi„Ë ÛÙÔÓ Î·ıÔÚÈÛÌfi Ù˘ ·ÓÔÛÔηٷÛÙ·ÏÙÈ-
΋˜ ·ÁˆÁ‹˜. ∆· ÓÂfiÙÂÚ· Ê¿Ú̷η, mycophenolate
mofetil (CellCept) Î·È Ù· ÈÔ ÚfiÛÊ·Ù· mycopheno-
late sodium (Myfortic) Î·È sirolimus (Rapamycin), Ù·
ÔÔ›· ‰ÂÓ ÂËÚ¿˙Ô˘Ó ÙË ÓÂÊÚÈ΋ ÏÂÈÙÔ˘ÚÁ›·, ¤‰ˆ-
Û·Ó ÙË ‰˘Ó·ÙfiÙËÙ· Ó· ¯ÔÚËÁÔ‡ÓÙ·È ÔÈ ·Ó·ÛÙÔÏ›˜
ηÏÛÈÓ¢ڛÓ˘ Û ÌÈÎÚfiÙÂÚ˜ ‰fiÛÂȘ, Ì ·ÔÙ¤ÏÂÛÌ·
ÙÔÓ ÂÚÈÔÚÈÛÌfi ÙˆÓ ·ÚÂÓÂÚÁÂÈÒÓ ÙÔ˘˜ (40-43). ∞fi
Ù· ÂÚÈÛÙ·ÙÈο Ì·˜, 1 ·È‰›, ÙÔ ÔÔ›Ô Ï¿Ì‚·Ó ΢-
ÎÏÔÛÔÚ›ÓË ÁÈ· ¤Ó· ¤ÙÔ˜, ·ÚÔ˘Û›·Û ÚÔԉ¢ÙÈ΋
¤ÎÙˆÛË Ù˘ ÓÂÊÚÈ΋˜ ÏÂÈÙÔ˘ÚÁ›·˜, ·‡ÍËÛË Ù˘ Ô˘-
Ú›·˜ ÙÔ˘ ÔÚÔ‡ Î·È ·‡ÍËÛË Ù˘ ·ÚÙËÚȷ΋˜ ›ÂÛ˘.
∞ÓÙÈÌÂÙˆ›ÛÙËΠ·Ú¯ÈÎÒ˜ Ì Ì›ˆÛË Ù˘ ‰fiÛ˘ Ù˘
΢ÎÏÔÛÔÚ›Ó˘ Î·È ÛÙË Û˘Ó¤¯ÂÈ· Ì ·ÏÏ·Á‹ Ù˘ ·ÓÔ-
ÛÔηٷÛÙ·ÏÙÈ΋˜ ·ÁˆÁ‹˜ Û tacrolimus.
™Â ·ÓÙ›ıÂÛË Ì ÙÔ˘˜ ÂÓ‹ÏÈΘ, ÔÈ ÔÔ›ÔÈ Â›Ó·È È-
ı·Ófi Ó· ·ÚÔ˘ÛÈ¿ÛÔ˘Ó ˘ÔÙÚÔ‹ Ù˘ Ë·ÙÈ΋˜ Ófi-
ÛÔ˘ ÌÂÙ¿ ÙË ª∏, ÙÔ ÌÂÁ·Ï‡ÙÂÚÔ ÔÛÔÛÙfi ÙˆÓ ·È-
‰ÈÒÓ ‰ÂÓ ÎÈÓ‰˘Ó‡ÂÈ ·fi ˘ÔÙÚÔ‹ Ù˘ ÚˆÙ·Ú¯È-
΋˜ ÓfiÛÔ˘. ∏ ·Ú·Ù‹ÚËÛË ·˘Ù‹ ÂȂ‚·ÈÒÓÂÙ·È Î·È
·fi Ù· ηχÙÂÚ· ÔÛÔÛÙ¿ ÂÈ‚›ˆÛ˘ ÙˆÓ ÌÔÛ¯Â˘-
Ì¿ÙˆÓ ÛÙÔ˘˜ ·È‰È·ÙÚÈÎÔ‡˜ ·ÛıÂÓ›˜ (44).
™˘ÌÂÚ·ÛÌ·ÙÈο, Ë ª∏ ·ÔÙÂÏ› Û‹ÌÂÚ· ÙË Ìfi-
ÓË ‰È·ı¤ÛÈÌË ıÂڷ›· Û ·È‰È¿ Ì ÌË ·Ó·ÛÙÚ¤„ÈÌË
145ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ ÛÙ· ·È‰È¿
¶·È‰È·ÙÚÈ΋ 2008;71:141-147
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·145

Ë·ÙÈ΋ ·Ó¿ÚÎÂÈ· Ô˘ ÚÔηÏÂ›Ù·È ·fi ÏÂÈ¿‰·ÓÔÛËÌ¿ÙˆÓ, Ù· ÔÔ›· ÛÙÔ ·ÚÂÏıfiÓ ‹Ù·Ó ‰‡ÛÎÔÏÔÓ· ÂÏÂÁ¯ıÔ‡Ó Î·È Ó· ·ÓÙÈÌÂÙˆÈÛÙÔ‡Ó. ∏ ηϋ Û˘-ÓÂÚÁ·Û›· Ù˘ ÔÌ¿‰·˜ ÂȉÈÎÒÓ (¯ÂÈÚÔ˘ÚÁÒÓ, ·È‰Ô-Á·ÛÙÚÂÓÙÂÚÔÏfiÁˆÓ, ·È‰Ô„˘¯È¿ÙÚˆÓ, ÓÔÛËÏ¢-ÙÚÈÒÓ, ÎÔÈÓˆÓÈÎÒÓ ÏÂÈÙÔ˘ÚÁÒÓ) Ì ÙËÓ ÔÈÎÔÁ¤ÓÂÈ·Â›Ó·È ıÂÌÂÏÈÒ‰Ô˘˜ ÛËÌ·Û›·˜ ÁÈ· ÙËÓ ÔÌ·Ï‹ ÔÚ›·ÙˆÓ ·È‰ÈÒÓ ·˘ÙÒÓ. √È ÌÂÏÏÔÓÙÈΤ˜ ÂÍÂÏ›ÍÂȘ ÛÙ˯ڋÛË ÂÙÂÚÔÌÔÛ¯Â˘Ì¿ÙˆÓ ‹ Ë·ÙÔ΢ÙÙ¿ÚˆÓ, η-ıÒ˜ Î·È ÔÈ È‰ÈfiÙËÙ˜ Ô˘ ‰È·Ê·›ÓÔÓÙ·È ÛÙ· ‚Ï·ÛÙÔ-·ÙÙ·Ú·, ›Ûˆ˜ ÂÚÈÔÚ›ÛÔ˘Ó ÙÔÓ ·ÚÈıÌfi ÙˆÓ ·È‰ÈÒÓÔ˘ ·Ó·Ì¤ÓÔ˘Ó Ë·ÙÈÎfi ÌfiÛ¯Â˘Ì·.
µÈ‚ÏÈÔÁÚ·Ê›·
1. Starzl TE, Marchioro TL, Vonkaulla KN, Hermann G,Brittain RS, Waddell WR. Homotransplantation of the liv-er in humans. Surg Gynecol Obstet 1963;117:659-676.
2. Starzl TE. History of Liver and Other Splanchnic OrganTransplantation. In: Busutill RW, Klintmalm GB, editors.Transplantation of the Liver. Philadelphia, Pa: W.B. Saun-ders; 1996. p. 3-22.
3. Otte JB. History of pediatric liver transplantation. Whereare we coming from? Where do we stand? Pediatr Trans-plant 2002;6:378-387.
4. Alagille D. History of pediatric liver transplantation inEurope. Acta Gastroenterol Belg 2004;67:172-175.
5. Schafer DF. Liver transplantation. Looking back, lookingforward. In: Maddrey WC, Schiff ER, Sorrell MF, editors.Transplantation of the Liver. Philadelphia, Pa: Lippincott,Williams & Wilkins; 2001.
6. Busuttil RW, Farmer DG, Yersiz H, Hiatt JR, McDiarmidSV, Goldstein LI, et al. Analysis of long-term outcomes of3200 liver transplantations over two decades: a single-cen-ter experience. Ann Surg 2005;241:905-916.
7. Lee WS, McKiernan P, Kelly DA. Etiology, outcome andprognostic indicator of childhood fulminant hepatic fail-ure in the United Kingdom. J Pediatr Gastroenterol Nutr2005;40:575-581.
8. Kelly DA. Current results and evolving indications for liv-er transplantation in children. J Pediatr Gastroenterol Nutr1998;27:214-221.
9. Bismuth H, Houssin D. Reduced-size orthotopic liver graftin hepatic transplantation in children. Surgery 1984;95:367-372.
10. Pichlmayr R, Ringe B, Gubernatis G, Hauss J, BunzendahlH. [Transplantation of a donor liver to 2 recipients (split-ting transplantation) -- a new method in the further devel-opment of segmental liver transplantation]. LangenbecksArchiv Chir 1988;373:127-130.
11. Broelsch CE, Emond JC, Whitington PF, Thistlethwaite JR,Baker AL, Lichtor JL. Application of reduced-size livertransplants as split grafts, auxiliary orthotopic grafts, andliving related segmental transplants. Ann Surg 1990;212:368-375.
12. Dhawan A, Cheeseman P, Mieli-Vergani G. Approaches toacute liver failure in children. Pediatr Transplant 2004;8:584-588.
13. Kelly DA. Liver Transplantation. In: Walker WA et al, edi-tors. Pediatric Gastrointestinal Disease. Philadelphia, Pa:BC Decker; 2000. p. 1272-1290.
14. Tiao GM, Alonso M, Bezerra J, Yazigi N, Heubi J, Balisteri
W, et al. Liver transplantation in children younger than 1
year - the Cincinnati experience. J Pediatr Surg 2005;40:
268-273.
15. Kelly DA. Nutritional factors affecting growth before and
after liver transplantation. Ped Transplant 1997;1:80-84.
16. Nadalin S, Heuer M, Wallot M, Auth M, Schaffer R,
Sotiropoulos GC, et al. Paediatric acute liver failure and
transplantation: the University of Essen experience.
Transpl Int 2007;20:519-527.
17. Holt RI, Broide E, Buchanan CR, Miell JP, Baker AJ,
Mowat AP, et al. Orthotopic liver transplantation reverses
the adverse nutritional changes of end-stage liver disease in
children. Am J Clin Nutr 1997;65:534-542.
18. Burdelski M, Nolkemper D, Ganschow R, Sturm E, Mala-
go M, Rogiers X, et al. Liver transplantation in children:
long-term outcome and quality of life. Eur J Pediatr 1999;
158:S34-S42.
19. Van Mourik ID, Beath SV, Brook GA, Cash AJ, Mayer AD,
Buckels JA, et al. Long term nutritional and neurodevel-
opmental outcome of liver transplantation in infants aged
less than 12 months. J Pediatr Gastroenterol Nutr 2000;30:
269-275.
20. Bartosh SM, Thomas SE, Sutton MM, Brady LM, Whiting-
ton PF. Linear growth after pediatric liver transplantation.
J Pediatr 1999;135: 624-631.
21. Melter M, Briscoe DM. Challenges after pediatric trans-
plantation. Semin Nephrol 2000; 20:199-208.
22. Ramaccioni V, Soriano HE, Arumugam R, Klish WJ.
Nutritional aspects of chronic liver disease and liver trans-
plantation in children. J Pediatr Gastroenterol Nutr 2000;
30:361-367.
23. Viner RM, Forton JT, Cole TJ, Clark IH, Noble-Jamieson
G, Barnes ND. Growth of long-term survivors of liver
transplantation. Arch Dis Child 1999;80:235-240.
24. Reding R, Gras J, Sokal E, Otte JB, Davies HF. Steroid-free
liver transplantation in children. Lancet 2003;362:2068-2070.
25. Magee JC, Bucuvalas JC, Farmer DG, Harmon WE, Hul-
bert-Shearon TE, Mendeloff EN. Pediatric transplantation.
Am J Transplant 2004;4:54-71.
26. Lfipez-Santamaria M, de Vicente E, Gaãmez M, Murcia M,
Leal N, Hernandez F, et al. Pediatric living donor liver
transplantation. Transplant Proc 2003;35:1808-1809.
27. Takada Y, Tanaka K. Living related liver transplantation.
Transplant Proc 2004;36:271-273.
28. Chen CL, Concejero A, Wang CC, Wang SH, Lin CC, Liu
YW, et al. Living donor liver transplantation for biliary
atresia: a single-center experience with first 100 cases. Am J
Transplant 2006;6:2672-2679.
29. Hattori H, Higuchi Y, Tsuji M, Inomata Y, Uemoto S,
Asonuma K, et al. Living-related liver transplantation and
neurological outcome in children with fulminant hepatic
failure. Transplantation 1998;65:686-692.
30. Yersiz H, Renz JF, Farmer DG, Hisatake GM, McDiarmid SV,
Busuttil RW. One hundred in situ split-liver transplantations:
a single-center experience. Ann Surg 2003;238:496-505.
31. Austin MT, Feuer ID, Chari RS, Gorden DL, Wright JK,
Pinson CW. Survival after pediatric liver transplantation.
Why does living donation offer an advantage? Arch Surg
2005;140:465-470.
32. Sundaram SS, Alonso EM, Whitington PF. Liver trans-
plantation in neonates. Liver Transpl 2003;9:783-788.
146 Ÿ. µÚ¿ÓË Î·È Û˘Ó.
Paediatriki 2008;71:141-147
Pediatri Mar-Apr 08 08-04-08 11:32 ™ÂÏ›‰·146

33. Graziadei I. Liver transplantation organ allocation betweenChild and MELD. Wien Med Wochenschr 2006;156:410-415.
34. Evrard V, Otte JB, Sokal E, Rochet JS, Haccourt F, GennariF, et al. Impact of surgical and immunological parametersin pediatric liver transplantation: a multivariate analysis in500 consecutive recipients of primary grafts. Ann Surg2004; 239:272-280.
35. Brown RS, Kumar KS, Russo MW, Kinkhabwala M, Ru-dow DL, Harren P, et al. Model for end-stage liver diseaseand Child-Turcotte-Pugh score as predictors of pretrans-plantation disease severity, posttransplantation outcome,and resource utilization in United Network for OrganSharing status 2A patients. Liver Transpl 2002;8:278-284.
36. Chang FY, Singh N, Gayowski T, Wagener MM, MarinoIR. Fever in liver transplant recipients: changing spectrumof etiologic agents. Clin Infect Dis 1998;26:59-65.
37. Guthery SL, Heubi JE, Bucuvalas JC, Gross TG, RyckmanFC, Alonso MH, et al. Determination of risk factors for Ep-stein-Barr virus-associated posttransplant lymphoprolifer-ative disorder in pediatric liver transplant recipients usingobjective case ascertainment. Transplantation 2003;75:987-993.
38. Kling K, Lau H, Colombani P. Biliary complications of liv-
ing related pediatric liver transplant patients. PediatrTransplant 2004;8:178-184.
39. Araz C, Pirat A, Torgay A, Zeyneloglu P, Arslan G. Earlypostoperative complications of pediatric liver transplanta-tion: experience at one center. Transplant Proc 2004;36:214-217.
40. Reding R. Tacrolimus in pediatric liver transplantation.Pediatr Transplant 2002;6:447-451.
41. Nobili V, Comparcola D, Sartorelli MR, Diciommo V,Marcellini M. Mycophenolate mofetil in pediatric livertransplant patients with renal dysfunction: preliminary da-ta. Pediatr Transplant 2003;7:454-457.
42. Evans HM, McKiernan PJ, Kelly DA. Mycophenolatemofetil for renal dysfunction after pediatric liver trans-plantation. Transplantation 2005;79:1575-1580.
43. Mahadevan SBK, Beath SV, Davids P, Lloyd C, James C,van Mourik IDM, et al. Safety and efficacy of Sirolimus inchildren following chronic rejection and/or nephrotoxicitypost intestinal transplant (Itx) and liver transplantation(LTx). J Pediatr Gastroenterol Nutr 2004;39:S152.
44. Bucuvalas JC, Ryckman FC. Long-term outcome after livertransplantation in children. Pediatr Transplant 2002;6:30-36.
45. United Network for Organ Sharing [Webpage, Internet].http://www.unos.org/
147ªÂÙ·ÌfiÛ¯Â˘ÛË ‹·ÙÔ˜ ÛÙ· ·È‰È¿
¶·È‰È·ÙÚÈ΋ 2008;71:141-147
Pediatri Mar-Apr 08 08-04-08 11:32 ™ÂÏ›‰·147

√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙˆÓ Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜,
ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ Ù‡Ô˘ C Î·È ÙÔ˘ Ó¢ÌÔÓÈfiÎÔÎÎÔ˘
µ. ∆ÛÈ¿ÓÙÔ˘1, ∞. ∫·Úfi΢2, ∂. ¶¿‚Ë1, °. ∫˘ÚÈfiÔ˘ÏÔ˜1
¶ÂÚ›ÏË„Ë
∂ÈÛ·ÁˆÁ‹: ∆· ÂÌ‚fiÏÈ· ·ÔÙÂÏÔ‡Ó ¤Ó· ·fi Ù· ÛËÌ·ÓÙÈÎfiÙÂÚ· ÂÚÁ·Ï›· ÚˆÙÔÁÂÓÔ‡˜ ÚfiÏ˄˘. øÛÙfi-ÛÔ, ÔÈ Û˘Ó¯Ҙ ·˘Í·ÓfiÌÂÓ˜ ·Ó¿ÁΘ, ÛÂ Û˘Ó‰˘·ÛÌfi Ì ÙÔ˘˜ ÂÚÈÔÚÈṲ̂ÓÔ˘˜ ÔÈÎÔÓÔÌÈÎÔ‡˜ fiÚÔ˘˜,ÂÈ‚¿ÏÏÔ˘Ó ÂÚÈÔÚÈÛÌÔ‡˜ ÛÙȘ ·ÔÊ¿ÛÂȘ ¤ÓÙ·Í‹˜ ÙÔ˘˜ ÛÙ· ∂ıÓÈο ¶ÚÔÁÚ¿ÌÌ·Ù· ∂Ì‚ÔÏÈ·ÛÌÒÓ. ™ÎÔ-fi˜ Ù˘ ÂÚÁ·Û›·˜ ·˘Ù‹˜ Â›Ó·È Ó· ·Ó·‰Â›ÍÂÈ ÙË Û˘Ì‚ÔÏ‹ Ù˘ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÛÙË Ï‹„Ë ·ÔÊ¿-ÛÂˆÓ ÛÙÔÓ Â˘·›ÛıËÙÔ ÙÔ̤· ÙˆÓ ÚÔÁÚ·ÌÌ¿ÙˆÓ ·ÓÔÛÔÔ›ËÛ˘ Î·È ÂÌ‚ÔÏÈ·ÛÌÔ‡.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ: ŒÁÈÓÂ Û˘ÛÙËÌ·ÙÈ΋ ·Ó·ÛÎfiËÛË ÂÈÛÙËÌÔÓÈÎÒÓ ¿ÚıÚˆÓ Ô˘ ·ÊÔÚÔ‡Ó Û ÌÂϤÙ˜ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÙˆÓ Û˘ÁÎÂÎÚÈÌ¤ÓˆÓ ÂÌ‚ÔÏ›ˆÓ ηٿ ÙËÓ ÂÚ›Ô‰Ô 1999-2006. ø˜ ·Ú¯È΋ ËÁ‹Â‡ÚÂÛ˘ ¿ÚıÚˆÓ ¯ÚËÛÈÌÔÔÈ‹ıËÎÂ Ë ËÏÂÎÙÚÔÓÈ΋ ‚È‚ÏÈÔı‹ÎË PubMed.
∞ÔÙÂϤÛÌ·Ù·: ™ÙȘ ÂÚÈÛÛfiÙÂÚ˜ ·ÓÂÙ˘Á̤Ó˜ ¯ÒÚ˜ ‰ËÌÔÛȇÙËÎ·Ó ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ÚÈÓ ·fi ÙË Ï‹„Ë Ù˘ ·fiÊ·Û˘ ÁÈ· ÙËÓ ¤ÓÙ·ÍË ‹ ÌË ÙˆÓ Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ ÛÙ· ∂ıÓÈο ¶ÚÔÁÚ¿ÌÌ·Ù· ∂Ì‚Ô-ÏÈ·ÛÌÒÓ. ∫·Ù¿ ÙË ‰ÈÂÍ·ÁˆÁ‹ ÙÔ˘˜ ÌÂÏÂÙ‹ıËÎ·Ó fiÏ· Ù· Èı·Ó¿ ÛÂÓ¿ÚÈ· Î·È ÔÈ ·Ú¿ÁÔÓÙ˜ Ô˘ ÂËÚ¿-˙Ô˘Ó ÙÔ ‰Â›ÎÙË ÎfiÛÙÔ˘˜-·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ·fi ‰È¿ÊÔÚ˜ ·Ó·Ï˘ÙÈΤ˜ ÚÔÔÙÈΤ˜.
™˘ÌÂÚ¿ÛÌ·Ù·: ∞Ó Î·È ÔÏϤ˜ ·fi ÙȘ ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ‰ÂÓ ‹Ù·Ó ¿ÓÙÔÙ ‹ ·Ôχو˜ ¢-ÓÔ˚Τ˜ ÁÈ· ÙËÓ ¿ÌÂÛË ¤ÓÙ·ÍË ÙˆÓ ÂÌ‚ÔÏ›ˆÓ ÛÙ· ∂ıÓÈο ¶ÚÔÁÚ¿ÌÌ·Ù· ∂Ì‚ÔÏÈ·ÛÌÒÓ, ÂÓ Î·ÈÚÒ, ÔÈ ¯ÒÚ˜ÚÔ¤‚ËÎ·Ó ÛÙËÓ ¤ÓÙ·Í‹ ÙÔ˘˜, ·ÊÔ‡ ·ÍÈÔÏfiÁËÛ·Ó ·fi ÎÔÈÓÔ‡ ÙÔ˘˜ ‰Â›ÎÙ˜ ÓÔÛËÚfiÙËÙ·˜ Î·È ıÓËÛÈÌfiÙË-Ù·˜, ÙËÓ ·ÓËÛ˘¯›· ÙÔ˘ ÎÔÈÓÔ‡ Î·È ÙÔ ÎÔÈÓˆÓÈÎfi Î·È ÔÈÎÔÓÔÌÈÎfi ÊÔÚÙ›Ô Ù˘ ÓfiÛÔ˘. √È ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜·ÍÈÔÏfiÁËÛ˘ Û˘Ó¤‚·Ï·Ó ÛÙËÓ ÙÂÎÌËÚȈ̤ÓË ·ÔÙ›ÌËÛË ÙˆÓ ‰È·ÊÔÚÂÙÈÎÒÓ ÛÙÚ·ÙËÁÈÎÒÓ ÂÌ‚ÔÏÈ·ÛÌÔ‡.
§¤ÍÂȘ ÎÏÂȉȿ: √ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË, ÂÌ‚fiÏÈ·, ·ÓÂÌ¢ÏÔÁÈ¿, ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˜ Ù‡Ô˘ C, Ó¢ÌÔÓÈfiÎÔÎÎÔ˜.
Economic evaluation of new vaccines against varicella, serogroup C
meningococcus and pneumococcus
V. Tsiantou1, A. Karokis2, E. Pavi1, G. Kyriopoulos1
Abstract
Background: Vaccines are one of the most important tools for the primary prevention of infectiousdiseases. Decisions on the inclusion of new vaccines in the National Immunization Schedule need toaddress competing priorities, which stem from the lack of health care resources and the growing healthcare needs of the population. The objective of this study is to highlight the importance of economicevaluation in the sensitive field of immunization programs and vaccines.
Methods: A systematic review of papers on the economic evaluation of new vaccines published inscientific journals between 1999 and 2006 was conducted through PubMed.
Results: In the majority of the health care systems of developed countries, ex ante economic evaluationswere published, which evaluated all the possible scenarios and factors influencing the cost-effectivenessratio of the vaccines before their introduction.
Conclusions: Economic evaluations were not always clearly in favour of the introduction of new vaccinesinto the vaccination schedules. However, countries usually adopted the vaccines for inclusion in theNational Immunization Schedules after assessing additional parameters, such as the mortality andmorbidity ratios, the economic and social burden of disease and the anxiety of the population regardingthe risk of infection.
Key words: Economic evaluation, vaccines, varicella, serogroup meningococcus, pneumococcus vaccination.
148 ∂ƒ∂À¡∏∆π∫∏ ∂ƒ°∞™π∞ ORIGINAL ARTICLE
1 ∆Ô̤·˜ √ÈÎÔÓÔÌÈÎÒÓ Ù˘ÀÁ›·˜, ∂ıÓÈ΋ ™¯ÔÏ‹¢ËÌfiÛÈ·˜ ÀÁ›·˜
2 ∂Ù·ÈÚÈΤ˜ ÀÔı¤ÛÂȘ,Wyeth Hellas A.E.B.E.
AÏÏËÏÔÁÚ·Ê›·:
µ·ÛÈÏÈ΋ ∆ÛÈ¿ÓÙÔ˘[email protected]∆Ô̤·˜ √ÈÎÔÓÔÌÈÎÒÓ Ù˘ÀÁ›·˜,∂ıÓÈ΋ ™¯ÔÏ‹ ¢ËÌfiÛÈ·˜ÀÁ›·˜§ÂˆÊ. ∞ÏÂÍ¿Ó‰Ú·˜ 196∆.∫. 115 21, ∞ı‹Ó·
1 Department of HealthEconomics, NationalSchool of Public Health
2 Corporate Affairs, WyethHellas S.A.
Correspondence:
Vasiliki [email protected] Economics Sector,National School of PublicHealth196, Alexandras Avenue 115 21, Athens, Greece
Paediatriki 2008;71:148-156
∂ÈÛ·ÁˆÁ‹
∆· ÂÌ‚fiÏÈ· ·ÔÙÂÏÔ‡Ó Ù· ÛËÌ·ÓÙÈÎfiÙÂÚ·
ÂÚÁ·Ï›· ÁÈ· ÙËÓ ÚˆÙÔÁÂÓ‹ ÚfiÏË„Ë ÙˆÓ ÓÔ-
ÛËÌ¿ÙˆÓ, Û˘ÓÂÈÛʤÚÔÓÙ·˜ ıÂÙÈο ÛÙË ‰ËÌfiÛÈ·
˘Á›· Î·È ÙËÓ ÔÈÎÔÓÔÌÈ΋ ˙ˆ‹. ∏ ¯ÔÚ‹ÁËÛË ÙˆÓ
ÂÌ‚ÔÏ›ˆÓ Ô‰ËÁ› ÛÙË Ì›ˆÛË ‹ ·ÎfiÌ· Î·È ÛÙËÓ
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·148
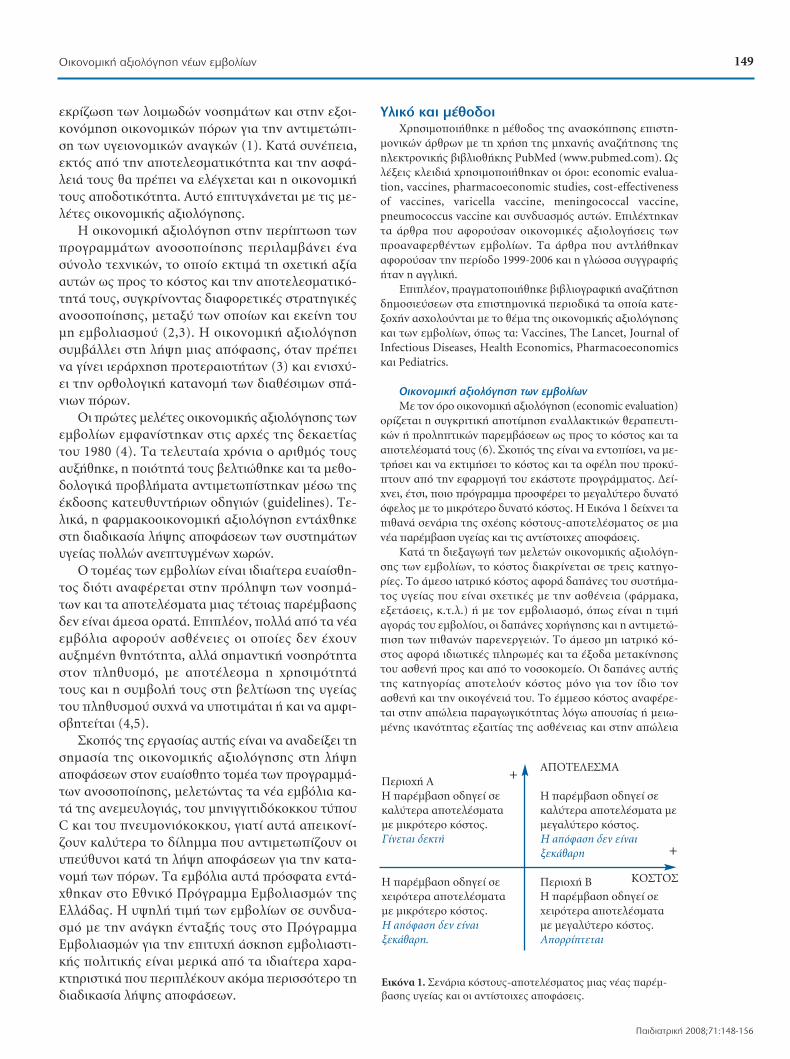
ÂÎÚ›˙ˆÛË ÙˆÓ ÏÔÈ̈‰ÒÓ ÓÔÛËÌ¿ÙˆÓ Î·È ÛÙËÓ ÂÍÔÈ-
ÎÔÓfiÌËÛË ÔÈÎÔÓÔÌÈÎÒÓ fiÚˆÓ ÁÈ· ÙËÓ ·ÓÙÈÌÂÙÒÈ-
ÛË ÙˆÓ ˘ÁÂÈÔÓÔÌÈÎÒÓ ·Ó·ÁÎÒÓ (1). ∫·Ù¿ Û˘Ó¤ÂÈ·,
ÂÎÙfi˜ ·fi ÙËÓ ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ· Î·È ÙËÓ ·ÛÊ¿-
ÏÂÈ¿ ÙÔ˘˜ ı· Ú¤ÂÈ Ó· ÂϤÁ¯ÂÙ·È Î·È Ë ÔÈÎÔÓÔÌÈ΋
ÙÔ˘˜ ·Ô‰ÔÙÈÎfiÙËÙ·. ∞˘Ùfi ÂÈÙ˘Á¯¿ÓÂÙ·È Ì ÙȘ ÌÂ-
ϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘.
∏ ÔÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÛÙËÓ ÂÚ›ÙˆÛË ÙˆÓ
ÚÔÁÚ·ÌÌ¿ÙˆÓ ·ÓÔÛÔÔ›ËÛ˘ ÂÚÈÏ·Ì‚¿ÓÂÈ ¤Ó·
Û‡ÓÔÏÔ Ù¯ÓÈÎÒÓ, ÙÔ ÔÔ›Ô ÂÎÙÈÌ¿ ÙË Û¯ÂÙÈ΋ ·Í›·
·˘ÙÒÓ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ Î·È ÙËÓ ·ÔÙÂÏÂÛÌ·ÙÈÎfi-
ÙËÙ¿ ÙÔ˘˜, Û˘ÁÎÚ›ÓÔÓÙ·˜ ‰È·ÊÔÚÂÙÈΤ˜ ÛÙÚ·ÙËÁÈΤ˜
·ÓÔÛÔÔ›ËÛ˘, ÌÂٷ͇ ÙˆÓ ÔÔ›ˆÓ Î·È ÂΛÓË ÙÔ˘
ÌË ÂÌ‚ÔÏÈ·ÛÌÔ‡ (2,3). ∏ ÔÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË
Û˘Ì‚¿ÏÏÂÈ ÛÙË Ï‹„Ë ÌÈ·˜ ·fiÊ·Û˘, fiÙ·Ó Ú¤ÂÈ
Ó· Á›ÓÂÈ ÈÂÚ¿Ú¯ËÛË ÚÔÙÂÚ·ÈÔÙ‹ÙˆÓ (3) Î·È ÂÓÈÛ¯‡-
ÂÈ ÙËÓ ÔÚıÔÏÔÁÈ΋ ηٷÓÔÌ‹ ÙˆÓ ‰È·ı¤ÛÈÌˆÓ Û¿-
ÓÈˆÓ fiÚˆÓ.
√È ÚÒÙ˜ ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÙˆÓ
ÂÌ‚ÔÏ›ˆÓ ÂÌÊ·Ó›ÛÙËÎ·Ó ÛÙȘ ·Ú¯¤˜ Ù˘ ‰ÂηÂÙ›·˜
ÙÔ˘ 1980 (4). ∆· ÙÂÏÂ˘Ù·›· ¯ÚfiÓÈ· Ô ·ÚÈıÌfi˜ ÙÔ˘˜
·˘Í‹ıËÎÂ, Ë ÔÈfiÙËÙ¿ ÙÔ˘˜ ‚ÂÏÙÈÒıËÎÂ Î·È Ù· ÌÂıÔ-
‰ÔÏÔÁÈο ÚÔ‚Ï‹Ì·Ù· ·ÓÙÈÌÂÙˆ›ÛÙËÎ·Ó Ì¤Ûˆ Ù˘
¤Î‰ÔÛ˘ ηÙ¢ı˘ÓÙ‹ÚÈˆÓ Ô‰ËÁÈÒÓ (guidelines). ∆Â-
ÏÈο, Ë Ê·ÚÌ·ÎÔÔÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÂÓÙ¿¯ıËÎÂ
ÛÙË ‰È·‰Èηۛ· Ï‹„˘ ·ÔÊ¿ÛÂˆÓ ÙˆÓ Û˘ÛÙËÌ¿ÙˆÓ
˘Á›·˜ ÔÏÏÒÓ ·ÓÂÙ˘ÁÌ¤ÓˆÓ ¯ˆÚÒÓ.
√ ÙÔ̤·˜ ÙˆÓ ÂÌ‚ÔÏ›ˆÓ Â›Ó·È È‰È·›ÙÂÚ· ¢·›ÛıË-
ÙÔ˜ ‰ÈfiÙÈ ·Ó·Ê¤ÚÂÙ·È ÛÙËÓ ÚfiÏË„Ë ÙˆÓ ÓÔÛËÌ¿-
ÙˆÓ Î·È Ù· ·ÔÙÂϤÛÌ·Ù· ÌÈ·˜ Ù¤ÙÔÈ·˜ ·Ú¤Ì‚·Û˘
‰ÂÓ Â›Ó·È ¿ÌÂÛ· ÔÚ·Ù¿. ∂ÈϤÔÓ, ÔÏÏ¿ ·fi Ù· Ó¤·
ÂÌ‚fiÏÈ· ·ÊÔÚÔ‡Ó ·Ûı¤ÓÂȘ ÔÈ Ôԛ˜ ‰ÂÓ ¤¯Ô˘Ó
·˘ÍË̤ÓË ıÓËÙfiÙËÙ·, ·ÏÏ¿ ÛËÌ·ÓÙÈ΋ ÓÔÛËÚfiÙËÙ·
ÛÙÔÓ ÏËı˘ÛÌfi, Ì ·ÔÙ¤ÏÂÛÌ· Ë ¯ÚËÛÈÌfiÙËÙ¿
ÙÔ˘˜ Î·È Ë Û˘Ì‚ÔÏ‹ ÙÔ˘˜ ÛÙË ‚ÂÏÙ›ˆÛË Ù˘ ˘Á›·˜
ÙÔ˘ ÏËı˘ÛÌÔ‡ Û˘¯Ó¿ Ó· ˘ÔÙÈÌ¿Ù·È ‹ Î·È Ó· ·ÌÊÈ-
Û‚ËÙÂ›Ù·È (4,5).
™ÎÔfi˜ Ù˘ ÂÚÁ·Û›·˜ ·˘Ù‹˜ Â›Ó·È Ó· ·Ó·‰Â›ÍÂÈ ÙË
ÛËÌ·Û›· Ù˘ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÛÙË Ï‹„Ë
·ÔÊ¿ÛÂˆÓ ÛÙÔÓ Â˘·›ÛıËÙÔ ÙÔ̤· ÙˆÓ ÚÔÁÚ·ÌÌ¿-
ÙˆÓ ·ÓÔÛÔÔ›ËÛ˘, ÌÂÏÂÙÒÓÙ·˜ Ù· Ó¤· ÂÌ‚fiÏÈ· η-
Ù¿ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜, ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ Ù‡Ô˘
C Î·È ÙÔ˘ Ó¢ÌÔÓÈfiÎÔÎÎÔ˘, ÁÈ·Ù› ·˘Ù¿ ·ÂÈÎÔÓ›-
˙Ô˘Ó Î·Ï‡ÙÂÚ· ÙÔ ‰›ÏËÌÌ· Ô˘ ·ÓÙÈÌÂÙˆ›˙Ô˘Ó ÔÈ
˘Â‡ı˘ÓÔÈ Î·Ù¿ ÙË Ï‹„Ë ·ÔÊ¿ÛÂˆÓ ÁÈ· ÙËÓ Î·Ù·-
ÓÔÌ‹ ÙˆÓ fiÚˆÓ. ∆· ÂÌ‚fiÏÈ· ·˘Ù¿ ÚfiÛÊ·Ù· ÂÓÙ¿-
¯ıËÎ·Ó ÛÙÔ ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ Ù˘
∂ÏÏ¿‰·˜. ∏ ˘„ËÏ‹ ÙÈÌ‹ ÙˆÓ ÂÌ‚ÔÏ›ˆÓ ÛÂ Û˘Ó‰˘·-
ÛÌfi Ì ÙËÓ ·Ó¿ÁÎË ¤ÓÙ·Í‹˜ ÙÔ˘˜ ÛÙÔ ¶ÚfiÁÚ·ÌÌ·
∂Ì‚ÔÏÈ·ÛÌÒÓ ÁÈ· ÙËÓ ÂÈÙ˘¯‹ ¿ÛÎËÛË ÂÌ‚ÔÏÈ·ÛÙÈ-
΋˜ ÔÏÈÙÈ΋˜ Â›Ó·È ÌÂÚÈο ·fi Ù· ȉȷ›ÙÂÚ· ¯·Ú·-
ÎÙËÚÈÛÙÈο Ô˘ ÂÚÈϤÎÔ˘Ó ·ÎfiÌ· ÂÚÈÛÛfiÙÂÚÔ ÙË
‰È·‰Èηۛ· Ï‹„˘ ·ÔÊ¿ÛˆÓ.
ÀÏÈÎfi Î·È Ì¤ıÔ‰ÔÈ
ÃÚËÛÈÌÔÔÈ‹ıËÎÂ Ë Ì¤ıÔ‰Ô˜ Ù˘ ·Ó·ÛÎfiËÛ˘ ÂÈÛÙË-
ÌÔÓÈÎÒÓ ¿ÚıÚˆÓ Ì ÙË ¯Ú‹ÛË Ù˘ Ì˯·Ó‹˜ ·Ó·˙‹ÙËÛ˘ Ù˘
ËÏÂÎÙÚÔÓÈ΋˜ ‚È‚ÏÈÔı‹Î˘ PubMed (www.pubmed.com). ø˜
ϤÍÂȘ ÎÏÂȉȿ ¯ÚËÛÈÌÔÔÈ‹ıËÎ·Ó ÔÈ fiÚÔÈ: economic evalua-
tion, vaccines, pharmacoeconomic studies, cost-effectiveness
of vaccines, varicella vaccine, meningococcal vaccine,
pneumococcus vaccine Î·È Û˘Ó‰˘·ÛÌfi˜ ·˘ÙÒÓ. ∂ÈϤ¯ÙËηÓ
Ù· ¿ÚıÚ· Ô˘ ·ÊÔÚÔ‡Û·Ó ÔÈÎÔÓÔÌÈΤ˜ ·ÍÈÔÏÔÁ‹ÛÂȘ ÙˆÓ
ÚÔ·Ó·ÊÂÚı¤ÓÙˆÓ ÂÌ‚ÔÏ›ˆÓ. ∆· ¿ÚıÚ· Ô˘ ·ÓÙÏ‹ıËηÓ
·ÊÔÚÔ‡Û·Ó ÙËÓ ÂÚ›Ô‰Ô 1999-2006 Î·È Ë ÁÏÒÛÛ· Û˘ÁÁÚ·Ê‹˜
‹Ù·Ó Ë ·ÁÁÏÈ΋.
∂ÈϤÔÓ, Ú·ÁÌ·ÙÔÔÈ‹ıËΠ‚È‚ÏÈÔÁÚ·ÊÈ΋ ·Ó·˙‹ÙËÛË
‰ËÌÔÛȇÛÂˆÓ ÛÙ· ÂÈÛÙËÌÔÓÈο ÂÚÈÔ‰Èο Ù· ÔÔ›· ηÙÂ-
ÍÔ¯‹Ó ·Û¯ÔÏÔ‡ÓÙ·È Ì ÙÔ ı¤Ì· Ù˘ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘
Î·È ÙˆÓ ÂÌ‚ÔÏ›ˆÓ, fiˆ˜ Ù·: Vaccines, The Lancet, Journal of
Infectious Diseases, Health Economics, Pharmacoeconomics
Î·È Pediatrics.
√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙˆÓ ÂÌ‚ÔÏ›ˆÓ
ªÂ ÙÔÓ fiÚÔ ÔÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË (economic evaluation)
ÔÚ›˙ÂÙ·È Ë Û˘ÁÎÚÈÙÈ΋ ·ÔÙ›ÌËÛË ÂÓ·ÏÏ·ÎÙÈÎÒÓ ıÂڷ¢ÙÈ-
ÎÒÓ ‹ ÚÔÏËÙÈÎÒÓ ·ÚÂÌ‚¿ÛÂˆÓ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ Î·È Ù·
·ÔÙÂϤÛÌ·Ù¿ ÙÔ˘˜ (6). ™ÎÔfi˜ Ù˘ Â›Ó·È Ó· ÂÓÙÔ›ÛÂÈ, Ó· ÌÂ-
ÙÚ‹ÛÂÈ Î·È Ó· ÂÎÙÈÌ‹ÛÂÈ ÙÔ ÎfiÛÙÔ˜ Î·È Ù· ÔʤÏË Ô˘ ÚÔ·-
ÙÔ˘Ó ·fi ÙËÓ ÂÊ·ÚÌÔÁ‹ ÙÔ˘ ÂοÛÙÔÙ ÚÔÁÚ¿ÌÌ·ÙÔ˜. ¢Â›-
¯ÓÂÈ, ¤ÙÛÈ, ÔÈÔ ÚfiÁÚ·ÌÌ· ÚÔÛʤÚÂÈ ÙÔ ÌÂÁ·Ï‡ÙÂÚÔ ‰˘Ó·Ùfi
fiÊÂÏÔ˜ Ì ÙÔ ÌÈÎÚfiÙÂÚÔ ‰˘Ó·Ùfi ÎfiÛÙÔ˜. ∏ ∂ÈÎfiÓ· 1 ‰Â›¯ÓÂÈ Ù·
Èı·Ó¿ ÛÂÓ¿ÚÈ· Ù˘ Û¯¤Û˘ ÎfiÛÙÔ˘˜-·ÔÙÂϤÛÌ·ÙÔ˜ Û ÌÈ·
Ó¤· ·Ú¤Ì‚·ÛË ˘Á›·˜ Î·È ÙȘ ·ÓÙ›ÛÙÔȯ˜ ·ÔÊ¿ÛÂȘ.
∫·Ù¿ ÙË ‰ÈÂÍ·ÁˆÁ‹ ÙˆÓ ÌÂÏÂÙÒÓ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁË-
Û˘ ÙˆÓ ÂÌ‚ÔÏ›ˆÓ, ÙÔ ÎfiÛÙÔ˜ ‰È·ÎÚ›ÓÂÙ·È Û ÙÚÂȘ ηÙËÁÔ-
ڛ˜. ∆Ô ¿ÌÂÛÔ È·ÙÚÈÎfi ÎfiÛÙÔ˜ ·ÊÔÚ¿ ‰·¿Ó˜ ÙÔ˘ Û˘ÛÙ‹Ì·-
ÙÔ˜ ˘Á›·˜ Ô˘ Â›Ó·È Û¯ÂÙÈΤ˜ Ì ÙËÓ ·Ûı¤ÓÂÈ· (Ê¿Ú̷η,
ÂÍÂÙ¿ÛÂȘ, Î.Ù.Ï.) ‹ Ì ÙÔÓ ÂÌ‚ÔÏÈ·ÛÌfi, fiˆ˜ Â›Ó·È Ë ÙÈÌ‹
·ÁÔÚ¿˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘, ÔÈ ‰·¿Ó˜ ¯ÔÚ‹ÁËÛ˘ Î·È Ë ·ÓÙÈÌÂÙÒ-
ÈÛË ÙˆÓ Èı·ÓÒÓ ·ÚÂÓÂÚÁÂÈÒÓ. ∆Ô ¿ÌÂÛÔ ÌË È·ÙÚÈÎfi Îfi-
ÛÙÔ˜ ·ÊÔÚ¿ ȉȈÙÈΤ˜ ÏËڈ̤˜ Î·È Ù· ¤ÍÔ‰· ÌÂٷΛÓËÛ˘
ÙÔ˘ ·ÛıÂÓ‹ ÚÔ˜ Î·È ·fi ÙÔ ÓÔÛÔÎÔÌ›Ô. √È ‰·¿Ó˜ ·˘Ù‹˜
Ù˘ ηÙËÁÔÚ›·˜ ·ÔÙÂÏÔ‡Ó ÎfiÛÙÔ˜ ÌfiÓÔ ÁÈ· ÙÔÓ ›‰ÈÔ ÙÔÓ
·ÛıÂÓ‹ Î·È ÙËÓ ÔÈÎÔÁ¤ÓÂÈ¿ ÙÔ˘. ∆Ô ¤ÌÌÂÛÔ ÎfiÛÙÔ˜ ·Ó·Ê¤ÚÂ-
Ù·È ÛÙËÓ ·ÒÏÂÈ· ·Ú·ÁˆÁÈÎfiÙËÙ·˜ ÏfiÁˆ ·Ô˘Û›·˜ ‹ ÌÂȈ-
̤Ó˘ ÈηÓfiÙËÙ·˜ ÂÍ·ÈÙ›·˜ Ù˘ ·Ûı¤ÓÂÈ·˜ Î·È ÛÙËÓ ·ÒÏÂÈ·
∞¶√∆∂§∂™ª∞¶ÂÚÈÔ¯‹ ∞∏ ·Ú¤Ì‚·ÛË Ô‰ËÁ› Û ∏ ·Ú¤Ì‚·ÛË Ô‰ËÁ› Û ηχÙÂÚ· ·ÔÙÂϤÛÌ·Ù· ηχÙÂÚ· ·ÔÙÂϤÛÌ·Ù· ÌÂÌ ÌÈÎÚfiÙÂÚÔ ÎfiÛÙÔ˜. ÌÂÁ·Ï‡ÙÂÚÔ ÎfiÛÙÔ˜.°›ÓÂÙ·È ‰ÂÎÙ‹ ∏ ·fiÊ·ÛË ‰ÂÓ Â›Ó·È
ÍÂοı·ÚË
∏ ·Ú¤Ì‚·ÛË Ô‰ËÁ› Û ¶ÂÚÈÔ¯‹ µ¯ÂÈÚfiÙÂÚ· ·ÔÙÂϤÛÌ·Ù· ∏ ·Ú¤Ì‚·ÛË Ô‰ËÁ› Û Ì ÌÈÎÚfiÙÂÚÔ ÎfiÛÙÔ˜. ¯ÂÈÚfiÙÂÚ· ·ÔÙÂϤÛÌ·Ù· ∏ ·fiÊ·ÛË ‰ÂÓ Â›Ó·È Ì ÌÂÁ·Ï‡ÙÂÚÔ ÎfiÛÙÔ˜.ÍÂοı·ÚË. ∞ÔÚÚ›ÙÂÙ·È
∂ÈÎfiÓ· 1. ™ÂÓ¿ÚÈ· ÎfiÛÙÔ˘˜-·ÔÙÂϤÛÌ·ÙÔ˜ ÌÈ·˜ Ó¤·˜ ·Ú¤Ì-‚·Û˘ ˘Á›·˜ Î·È ÔÈ ·ÓÙ›ÛÙÔȯ˜ ·ÔÊ¿ÛÂȘ.
+
∫√™∆√™
+
149√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ
¶·È‰È·ÙÚÈ΋ 2008;71:148-156
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·149

·Ú·ÁˆÁÈÎfiÙËÙ·˜, ¯ÚfiÓÔ˘ Î·È ÂÈÛÔ‰‹Ì·ÙÔ˜ ÙˆÓ Û˘ÁÁÂÓÒÓ
Î·È Ê›ÏˆÓ ÚÔÎÂÈ̤ÓÔ˘ Ó· ÊÚÔÓÙ›ÛÔ˘Ó ÙÔÓ ·ÛıÂÓ‹ (2,3). ∆Ô
¤ÌÌÂÛÔ ÎfiÛÙÔ˜ ıˆÚÂ›Ù·È Î·È ÎÔÈÓˆÓÈÎfi ÎfiÛÙÔ˜, ηıÒ˜ ·Ó·-
ʤÚÂÙ·È Û ÔÈÎÔÓÔÌÈΤ˜ ·ÒÏÂȘ Ù˘ ÎÔÈÓˆÓ›·˜.
∏ ÚÔÔÙÈ΋ Ù˘ ÌÂϤÙ˘ ηıÔÚ›˙ÂÈ ÔȘ ‰·¿Ó˜ ı·
ÂÚÈÏËÊıÔ‡Ó Û ÌÈ· ÌÂϤÙË Î·È ı· ·Ó·Ï˘ıÔ‡Ó (2,6). ∏ ÎÔÈ-
ÓˆÓÈ΋ ÚÔÔÙÈ΋ ÂÚÈÏ·Ì‚¿ÓÂÈ fiϘ ÙȘ ηÙËÁÔڛ˜ Îfi-
ÛÙÔ˘˜ Î·È Û˘Ó˘ÔÏÔÁ›˙ÂÈ fiÏ· Ù· ÔʤÏË, ÂÓÒ ·Ú¿ÏÏËÏ·
ıˆÚÂ›Ù·È Î·Ù·ÏÏËÏfiÙÂÚË ÁÈ· ÙËÓ ÔÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË
ÙˆÓ ÚÔÁÚ·ÌÌ¿ÙˆÓ ·ÓÔÛÔÔ›ËÛ˘ ÏfiÁˆ Ù˘ Û˘ÏÏÔÁÈ΋˜
·ÓÔÛ›·˜, Ë ÔÔ›· ¤¯ÂÈ ıÂÙÈΤ˜ ÂÈÙÒÛÂȘ Û fiÏÔ ÙÔÓ ÏË-
ı˘ÛÌfi (7,8).
√È Ù¯ÓÈΤ˜ Ô˘ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÁÈ· ÙËÓ ÔÈÎÔÓÔÌÈ΋
·ÍÈÔÏfiÁËÛË ÙˆÓ ÂÌ‚ÔÏ›ˆÓ Â›Ó·È ÔÈ ·ÎfiÏÔ˘ı˜ (1-3,7-9):
1. ∞Ó¿Ï˘ÛË ÂÏ·¯ÈÛÙÔÔ›ËÛ˘ ÎfiÛÙÔ˘˜. √È ÂÓ·ÏÏ·ÎÙÈΤ˜
ÛÙÚ·ÙËÁÈΤ˜ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Û˘ÁÎÚ›ÓÔÓÙ·È ÌfiÓÔ ˆ˜ ÚÔ˜ ÙÔ Îfi-
ÛÙÔ˜, ÂÊfiÛÔÓ ¤¯Ô˘Ó ·Ô‰Â‰ÂÈÁ̤ӷ ›‰È· ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙË-
Ù·, ÒÛÙ ӷ ÂÈÏÂÁ› Ë ÊıËÓfiÙÂÚË ·fi ·˘Ù¤˜.
2. ∞Ó¿Ï˘ÛË ÎfiÛÙÔ˘˜-ÔʤÏÔ˘˜. ∞ÔÙÈÌ¿ ÙfiÛÔ ÙÔ ÎfiÛÙÔ˜
fiÛÔ Î·È Ù· ·ÔÙÂϤÛÌ·Ù· ÙˆÓ ÚÔÁÚ·ÌÌ¿ÙˆÓ ÂÌ‚ÔÏÈ·ÛÌÔ‡
Û ÓÔÌÈÛÌ·ÙÈΤ˜ ÌÔÓ¿‰Â˜ Î·È ·ÍÈÔÏÔÁ› ·Ó ÌÈ· ·Ú¤Ì‚·ÛË
˘Á›·˜ ·Í›˙ÂÈ Ó· ¯ÚËÌ·ÙÔ‰ÔÙËı›.
3. ∞Ó¿Ï˘ÛË ÎfiÛÙÔ˘˜-·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜. ∂›Ó·È Ë
Û˘¯ÓfiÙÂÚ· ÂÊ·ÚÌÔ˙fiÌÂÓË Ù¯ÓÈ΋, fiÔ˘ ÙÔ ÎfiÛÙÔ˜ ·ÔÙÈÌ¿-
Ù·È Û ÓÔÌÈÛÌ·ÙÈΤ˜ ÌÔÓ¿‰Â˜ Î·È Ù· ÔʤÏË ÛÂ Ê˘ÛÈΤ˜ ÌÔÓ¿-
‰Â˜ ·Ú·ÁfiÌÂÓÔ˘ ¤ÚÁÔ˘, fiˆ˜ ¤ÙË ˙ˆ‹˜ Ô˘ ÛÒ˙ÔÓÙ·È ‹ Â-
ÚÈÛÙ·ÙÈο Ô˘ ·ÔÙÚ¤ÔÓÙ·È.
4. ∞Ó¿Ï˘ÛË ÎfiÛÙÔ˘˜-¯ÚËÛÈÌfiÙËÙ·˜. ∂‰Ò ÙÔ fiÊÂÏÔ˜ ÌÂ-
ÙÚ¿Ù·È ˆ˜ Û˘Ó‰˘·ÛÌfi˜ ·Ú¿Ù·Û˘ Ù˘ ÂÈ‚›ˆÛ˘ Î·È ‚ÂÏÙ›ˆ-
Û˘ Ù˘ ÔÈfiÙËÙ·˜ ˙ˆ‹˜. ∞˘Ù‹ Ë ÚÔÛ¤ÁÁÈÛË Â›Ó·È È‰È·›ÙÂÚ·
¯Ú‹ÛÈÌË ÁÈ· ÙȘ ·ÚÂÌ‚¿ÛÂȘ ˘Á›·˜ Ô˘ ·Ú¿ÁÔ˘Ó ÔʤÏË fi¯È
ÌfiÓÔ fiÛÔÓ ·ÊÔÚ¿ ÙË ıÓËÛÈÌfiÙËÙ·, ·ÏÏ¿ Î·È ÙË ÓÔÛËÚfiÙËÙ·.
√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ÙÔ˘ ÌËÓÈÁÁÈÙȉfi-
ÎÔÎÎÔ˘ Ù‡Ô˘ C
∏ ÌËÓÈÁÁ›Ùȉ· Â›Ó·È ÌÈ· ÊÏÂÁÌÔÓ‹ ÙˆÓ ÌËÓ›ÁÁˆÓ Ô˘ Â-
ÚÈÎÏÂ›Ô˘Ó ÙÔÓ ÂÁΤʷÏÔ Î·È ÙÔ ÓˆÙÈ·›Ô Ì˘ÂÏfi, Ë ÔÔ›· Û˘Ó‹-
ıˆ˜ ÚÔηÏÂ›Ù·È ·fi ‚·ÎÙ‹ÚÈ· ‹ ÈÔ‡˜. ¶¤ÓÙ ÔÚfiÙ˘ÔÈ ÙÔ˘
‚·ÎÙËÚ›Ô˘ Neisseria meningitidis (A, B, C, Y Î·È W-135) ÚÔ-
ηÏÔ‡Ó ÂÚÈÛÛfiÙÂÚ· ·fi ÙÔ 90% ÙˆÓ ÎÚÔ˘ÛÌ¿ÙˆÓ ÌËÓÈÁÁ›ÙÈ-
‰·˜ ·ÁÎÔÛÌ›ˆ˜ (10). ™‡Ìʈӷ Ì ÙÔÓ ¶·ÁÎfiÛÌÈÔ √ÚÁ·ÓÈ-
ÛÌfi ÀÁ›·˜ (¶√À), ÔÈ Ù‡ÔÈ ∞ Î·È C Â›Ó·È ÔÈ Î‡ÚȘ ·Èٛ˜ Ù˘
ÂȉËÌÈ΋˜ ÌËÓÈÁÁ›Ùȉ·˜. Èڛ˜ ıÂڷ¢ÙÈ΋ ·ÁˆÁ‹, ÂÚÈÛ-
ÛfiÙÂÚ· ·fi ÙÔ 50% ÙˆÓ ÎÚÔ˘ÛÌ¿ÙˆÓ Î·Ù·Ï‹ÁÔ˘Ó Û ı¿Ó·ÙÔ.
∞ÎfiÌ· fï˜ Î·È Ì ¤ÁηÈÚË ‰È¿ÁÓˆÛË Î·È Î·Ù¿ÏÏËÏË ıÂÚ·-
¢ÙÈ΋ ·ÁˆÁ‹, ÂÚ›Ô˘ 5-10% ÙˆÓ ÎÚÔ˘ÛÌ¿ÙˆÓ Î·Ù·Ï‹-
ÁÔ˘Ó ÛÂ ı¿Ó·ÙÔ, ÂÓÒ ÂÚ›Ô˘ ÙÔ 15-20% fiÛˆÓ ÂÈ‚ÈÒÓÔ˘Ó
˘ÔʤÚÔ˘Ó ·fi Ó¢ÚÔÏÔÁÈΤ˜ ‰È·Ù·Ú·¯¤˜, fiˆ˜ ÎÒʈÛË
Î·È ÓÂ˘Ì·ÙÈ΋ ηı˘ÛÙ¤ÚËÛË. ∆Ô Ó¤Ô Û˘˙¢Á̤ÓÔ ÂÌ‚fiÏÈÔ
ηٿ ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ Ù‡Ô˘ C, ÚÔÛʤÚÂÈ ÚÔÛÙ·Û›·
ÌfiÓÔ ¤Ó·ÓÙÈ ·˘ÙÔ‡ ÙÔ˘ Ù‡Ô˘ (11,12). ™ÙËÓ ∂ÏÏ¿‰·, Ë Î˘ÎÏÔ-
ÊÔÚ›· ÙÔ˘ ÂÁÎÚ›ıËΠÙÔ ™Â٤̂ÚÈÔ ÙÔ˘ 2000, Ì ‰ÂÛ̇ÛÂȘ
ÁÈ· ‰ÈÂÚ‡ÓËÛË Ù˘ ·Ó·ÁηÈfiÙËÙ·˜ ·Ó·ÌÓËÛÙÈÎÔ‡ ÂÌ‚ÔÏÈ·-
ÛÌÔ‡ Î·È ÁÈ· Û˘ÛÙËÌ·ÙÈ΋ ˘Ô‚ÔÏ‹ ÛÙÔȯ›ˆÓ ·Ó·ÊÔÚÈο ÌÂ
ÙȘ ·ÓÂÈı‡ÌËÙ˜ ÂÓ¤ÚÁÂȘ (13).
™ÙÔÓ ¶›Ó·Î· 1 ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È Ù· ‚·ÛÈο ÛÙÔȯ›· ÙˆÓ
ÔÈÎÔÓÔÌÈÎÒÓ ·ÍÈÔÏÔÁ‹ÛÂˆÓ ÙÔ˘ Û˘ÁÎÂÎÚÈ̤ÓÔ˘ ÂÌ‚ÔÏ›Ô˘. ∏
Ù¯ÓÈ΋ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ Ô˘ ΢ڛˆ˜ ¯ÚËÛÈÌÔÔÈ‹-
ıËΠ‹Ù·Ó Ë ·Ó¿Ï˘ÛË ÎfiÛÙÔ˘˜-·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ Î·È Ë
·Ó¿Ï˘ÛË Ú·ÁÌ·ÙÔÔÈ‹ıËΠ˘fi ÙËÓ ÚÔÔÙÈ΋ Ù˘ ÎÔÈÓˆ-
Ó›·˜ Î·È ÙˆÓ ·ÛÊ·ÏÈÛÙÈÎÒÓ Ù·Ì›ˆÓ. √È Û˘ÁÎÚÈÓfiÌÂÓ˜ ÛÙÚ·-
ÙËÁÈΤ˜ ·ÓÔÛÔÔ›ËÛ˘ ‹Ù·Ó Û ÁÂÓÈΤ˜ ÁÚ·Ì̤˜ ›‰È˜ Û fiϘ
ÙȘ ¯ÒÚ˜ Ô˘ ‰ÈÂÓ‹ÚÁËÛ·Ó Ù¤ÙÔȘ ÌÂϤÙ˜ Î·È ·ÊÔÚÔ‡Û·Ó
΢ڛˆ˜, ÂÓ·ÏÏ·ÎÙÈΤ˜ ÂÈÏÔÁ¤˜ Û¯ÂÙÈο Ì ÙÔÓ ·ÚÈıÌfi ÙˆÓ
¯ÔÚËÁÔ‡ÌÂÓˆÓ ‰fiÛˆÓ. £· Ú¤ÂÈ Ó· ÛËÌÂȈı› fiÙÈ, ÂÓÒ ÛÂ
ÔÏϤ˜ ÂÚÈÙÒÛÂȘ Ë ÔÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË Ô‰ËÁÔ‡Û ÛÂ
ÂÈÏÔÁ¤˜ ÚÔÁÚ·ÌÌ¿ÙˆÓ Ì›·˜ ‰fiÛ˘, Ù· ÎÏÈÓÈο ‰Â‰Ô̤ӷ
¤‚·ÏÏ·Ó ÙËÓ ˘ÈÔı¤ÙËÛË ÛÙÚ·ÙËÁÈÎÒÓ 2 Û˘Ó 1 ‰fiÛÂˆÓ ÛÙ·
ÂÚÈÛÛfiÙÂÚ· Û˘ÛÙ‹Ì·Ù· ˘Á›·˜.
√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ÙÔ˘
Ó¢ÌÔÓÈfiÎÔÎÎÔ˘
ªÂ ÙÔÓ fiÚÔ Ó¢ÌÔÓÈÔÎÔÎÎÈ΋ ÓfiÛÔ˜ ÔÚ›˙ÂÙ·È ÌÈ· ÔÌ¿‰·
ÓÔÛËÌ¿ÙˆÓ Ô˘ ÚÔηÏÔ‡ÓÙ·È ·fi ÙÔ ‚·ÎÙ‹ÚÈÔ Streptococcus
pneumoniae. ™Ù· ÓÔÛ‹Ì·Ù· ·˘Ù¿ ÂÚÈÏ·Ì‚¿ÓÔÓÙ·È ‰ÈÂÈÛ‰˘ÙÈ-
Τ˜ ÏÔÈÌÒÍÂȘ, fiˆ˜ ‚·ÎÙËÚÈ·ÈÌ›·, ÌËÓÈÁÁ›Ùȉ· Î·È ‚·ÎÙËÚÈ-
·ÈÌÈ΋ Ó¢ÌÔÓ›·. √ Ó¢ÌÔÓÈfiÎÔÎÎÔ˜ ÚÔηÏ› ›Û˘ ÌË
‰ÈÂÈÛ‰˘ÙÈΤ˜ Ó¢ÌÔÓÈÔÎÔÎÎÈΤ˜ ·Ûı¤ÓÂȘ, fiˆ˜ Ë Ì¤ÛË
ˆÙ›Ùȉ· (10). √ Ó¢ÌÔÓÈfiÎÔÎÎÔ˜ Â›Ó·È Î‡ÚÈ· ·ÈÙ›· ÓÔÛËÚfi-
ÙËÙ·˜ Î·È ıÓËÛÈÌfiÙËÙ·˜ ·ÁÎÔÛÌ›ˆ˜ Î·È Â˘ı‡ÓÂÙ·È ÁÈ· Â-
ÚÈÛÛfiÙÂÚÔ˘˜ ·fi 1 ÂηÙÔÌ̇ÚÈÔ ı·Ó¿ÙÔ˘˜ Û ‚Ú¤ÊË Î·È ·È-
‰È¿ οو ÙˆÓ 2 ÂÙÒÓ (18).
™ÙËÓ ∂ÏÏ¿‰·, Ë Â›ÙˆÛË Ù˘ Ó¢ÌÔÓÈÔÎÔÎÎÈ΋˜ ÓfiÛÔ˘
Û ·È‰È¿ οو ÙˆÓ 5 ÂÙÒÓ Â›Ó·È 43-100 ·Ó¿ 100.000 ·È‰È¿,
ÔÛÔÛÙfi ˘„ËÏfiÙÂÚÔ ·fi ¿ÏϘ Â˘Úˆ·˚Τ˜ ¯ÒÚ˜. ∆· ·Ô-
ÙÂϤÛÌ·Ù· ÌÈ·˜ ·ÓÂÏÏ‹ÓÈ·˜ ÌÂϤÙ˘ ¤‰ÂÈÍ·Ó fiÙÈ ÛÙ· ·È‰È¿
ÌÈÎÚfiÙÂÚ· ÙˆÓ 2 ÂÙÒÓ, 88% ÙˆÓ ÎÚÔ˘ÛÌ¿ÙˆÓ Ó¢ÌÔÓÈÔÎÔÎ-
ÎÈ΋˜ ÓfiÛÔ˘ ÚÔηÏÔ‡ÓÙ·È ·fi ÙÔ˘˜ ÔÚfiÙ˘Ô˘˜ Ô˘ ÂÚÈ-
Ï·Ì‚¿ÓÔÓÙ·È ÛÙÔ ÂÌ‚fiÏÈÔ. ∂ÓÒ ÁÈ· Ù· ÌÂÁ·Ï‡ÙÂÚ· ·È‰È¿, ÙÔ
ÔÛÔÛÙfi ·˘Ùfi ÌÂÈÒÓÂÙ·È ÛÙÔ 50% (19). ∂ÈϤÔÓ, ÙÔ ÂÌ‚fiÏÈÔ
ÚÔÛٷهÂÈ ¤Ó·ÓÙÈ Ù˘ ÔÍ›·˜ ̤Û˘ ˆÙ›Ùȉ·˜ Î·È Ù˘ Ó¢-
ÌÔÓ›·˜ Ô˘ ÔÊ›ÏÔÓÙ·È ÛÙÔ˘˜ ÔÚfiÙ˘Ô˘˜, ÔÈ ÔÔ›ÔÈ ÂÚȤ¯Ô-
ÓÙ·È ÛÙÔ ÂÌ‚fiÏÈÔ.
™ÙÔÓ ¶›Ó·Î· 2 ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È Ù· ‚·ÛÈο ÛÙÔȯ›· ÙˆÓ
ÌÂÏÂÙÒÓ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÁÈ· ÙÔ ÂÌ‚fiÏÈÔ ÙÔ˘ Ó¢-
ÌÔÓÈfiÎÔÎÎÔ˘. ∏ ·Ó¿Ï˘ÛË ÎfiÛÙÔ˘˜-·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜
Î·È Ë ÎÔÈÓˆÓÈ΋ ÚÔÔÙÈ΋ Ù˘ ·Ó¿Ï˘Û˘ Â›Ó·È Ù· ·ÚÈ· ¯·-
Ú·ÎÙËÚÈÛÙÈο ÙˆÓ ÌÂÏÂÙÒÓ ·˘ÙÒÓ.
√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜
∏ ·ÓÂÌ¢ÏÔÁÈ¿ Â›Ó·È ¤Ó· ÓfiÛËÌ· Ì ÌÂÁ¿ÏË ÌÂÙ·‰ÔÙÈÎfi-
ÙËÙ· Î·È Â˘Ú‡ Ê¿ÛÌ· ÂÈÏÔÎÒÓ. ŸÛÔ ÌÂÁ·Ï‡ÙÂÚË Â›Ó·È Ë
ËÏÈΛ· ÓfiÛËÛ˘ ÙfiÛÔ ÛÔ‚·ÚfiÙÂÚ˜ ÂÈÏÔΤ˜ ·ÚÔ˘ÛÈ¿˙Ô-
ÓÙ·È. ∂›Û˘, ÛÔ‚·Ú¤˜ ÂÈÏÔΤ˜ ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È ·Ó ÌÈ·
¤ÁÎ˘Ô˜ ÓÔÛ‹ÛÂÈ Î·Ù¿ ÙË ‰È¿ÚÎÂÈ· ÙÔ˘ ÚÒÙÔ˘ ‹ ÙÔ˘ ‰Â‡ÙÂÚÔ˘
ÙÚÈÌ‹ÓÔ˘ ·ËÛ˘. ™‡Ìʈӷ Ì ¤Ú¢Ó˜ ÂÚ›Ô˘ ÙÔ 90% ÙÔ˘
ÏËı˘ÛÌÔ‡ Â›Ó·È Èı·Ófi Ó· ÚÔÛ‚ÏËı› ·fi ÙË ÓfiÛÔ (10).
∆Ô ÂÌ‚fiÏÈÔ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜ ÂÚȤ¯ÂÈ ˙ÒÓÙ˜ ÂÍ·ÛıÂÓË-
̤ÓÔ˘˜ ·ıÔÁfiÓÔ˘˜ ÌÈÎÚÔÔÚÁ·ÓÈÛÌÔ‡˜. ∏ ‰È¿ÚÎÂÈ· Ù˘ ·ÓÔ-
Û›·˜ Ô˘ ÚÔÛʤÚÂÈ ÙÔ ÂÌ‚fiÏÈÔ ‰ÂÓ ¤¯ÂÈ ·ÎfiÌ· ÂÍ·ÎÚÈ‚ˆı›,
·ÏÏ¿ Ë ÂÌÂÈÚ›· ·fi ¿ÏÏ· ÂÌ‚fiÏÈ· ·˘Ù‹˜ Ù˘ ηÙËÁÔÚ›·˜
‰Â›¯ÓÂÈ fiÙÈ Ë ·ÓÔÛ›· ·Ú·Ì¤ÓÂÈ ̆ „ËÏ‹ Û fiÏË ÙË ‰È¿ÚÎÂÈ· Ù˘
˙ˆ‹˜. ∏ ̄ ÔÚ‹ÁËÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Ô‰ËÁ› Û ‹È˜ ·ÓÙȉڿÛÂȘ
Ô˘ ·ÊÔÚÔ‡Ó Î¿ÔÈ· ÂÍ·Óı‹Ì·Ù· ‹ ÂΉ‹ÏˆÛË ˘ÚÂÙÔ‡.
™·ÓÈfiÙÂÚ· ÂÌÊ·Ó›˙ÔÓÙ·È ÛÔ‚·ÚfiÙÂÚ˜ ·ÓÙȉڿÛÂȘ fiˆ˜
ÂÁÎÂÊ·Ï›Ùȉ˜, Ó¢ÌÔÓ›·, Û·ÛÌÔ› ·ÎfiÌË Î·È ı¿Ó·ÙÔ˜. ∆Ô
Û˘ÁÎÂÎÚÈ̤ÓÔ ÂÌ‚fiÏÈÔ ÂӉ›ÎÓ˘Ù·È ÁÈ· ÂÓÂÚÁËÙÈ΋ ·ÓÔÛÔ-
Ô›ËÛË ÂÓ·ÓÙ›ÔÓ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜ Û ¿ÙÔÌ· Ô˘ Ë ÚÔÛ‚Ô-
Ï‹ ÙÔ˘˜ ·fi ÙË ÓfiÛÔ ÌÔÚ› Ó· ÚÔηϤÛÂÈ ÛÔ‚·Ú¤˜ ÂÈÏÔ-
Τ˜ (13,30).
∆· ÙÂÏÂ˘Ù·›· ¯ÚfiÓÈ· ¤¯Ô˘Ó ‰ËÌÔÛÈ¢Ù› ÔÏϤ˜ ·Ó·Ï‡-
ÛÂȘ ÎfiÛÙÔ˘˜-·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ÙˆÓ ÚÔÁÚ·ÌÌ¿ÙˆÓ ÂÌ-
‚ÔÏÈ·ÛÌÔ‡ ¤Ó·ÓÙÈ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜. √È ‚·ÛÈÎfiÙÂÚ˜ ÌÂϤÙ˜
·ÚÔ˘ÛÈ¿˙ÔÓÙ·È ÛÙÔÓ ¶›Ó·Î· 3.
150 µ. ∆ÛÈ¿ÓÙÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:148-156
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·150

∞ÔÙÂϤÛÌ·Ù·
√È ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÙÔ˘ ÂÌ‚Ô-Ï›Ô˘ ηٿ ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ Ù‡Ô˘ C, ·ÏÏ¿ ηÈÙ· ‰È·ı¤ÛÈÌ· ÂȉËÌÈÔÏÔÁÈο ‰Â‰Ô̤ӷ ÚÈÓ Î·È ÌÂ-Ù¿ ÙËÓ ÂÊ·ÚÌÔÁ‹ ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡, Û˘ÓËÁÔÚÔ‡Ó˘¤Ú Ù˘ ¿Ô„˘ fiÙÈ Ë ÂÊ·ÚÌÔÁ‹ ÙÔ˘ Ì·˙ÈÎÔ‡ ÂÌ-‚ÔÏÈ·ÛÌÔ‡ ÛÙËÓ ÂÚ›ÙˆÛË ·˘Ù‹ Â›Ó·È ·ÔÙÂÏÂÛÌ·-ÙÈ΋ Î·È ÔÈÎÔÓÔÌÈο ·Ô‰ÔÙÈ΋. ∆Ô ÂÌ‚fiÏÈÔ Â›Ó·È·ÔÙÂÏÂÛÌ·ÙÈÎfi ηıÒ˜ ÚÔηÏ› ¿ÌÂÛË ÚÔÛÙ·Û›·ÛÙ· ÂÌ‚ÔÏÈ·Ṳ̂ӷ ¿ÙÔÌ·, ·ÏÏ¿ Î·È ¤ÌÌÂÛË ÚÔÛÙ·-Û›· ̤ۈ Ù˘ ÂÏ¿ÙÙˆÛ˘ Ù˘ ‰È·ÛÔÚ¿˜ ÙÔ˘ ÌÈÎÚÔ-ÔÚÁ·ÓÈÛÌÔ‡ (36). ¢ÂÓ ·ÚÔ˘ÛÈ¿˙ÂÈ ·ÚÂÓ¤ÚÁÂȘ,ÁÂÁÔÓfi˜ Ô˘ ı· ‰ËÌÈÔ˘ÚÁÔ‡Û ÌÂÁ·Ï‡ÙÂÚ· ÚÔ‚Ï‹-Ì·Ù· ˘Á›·˜ Î·È ÂÈϤÔÓ ÎfiÛÙÔ˜ ÁÈ· ÙË ÛÙÚ·ÙËÁÈ΋·ÓÔÛÔÔ›ËÛ˘. ª¿ÏÈÛÙ·, fiÛÔ ÌÂÁ·Ï‡ÙÂÚÔ ÙÔ ÔÛÔ-ÛÙfi ÂÌ‚ÔÏÈ·ÛÙÈ΋˜ Î¿Ï˘„˘, ÙfiÛÔ Î·Ï‡ÙÂÚ· Ù··ÔÙÂϤÛÌ·Ù·, ηıÒ˜ ÂÈÙ˘Á¯¿ÓÂÙ·È Ì·ÎÚÔ¯ÚfiÓÈ·Û˘ÏÏÔÁÈ΋ ·ÓÔÛ›·. °È· ÙÔ ÏfiÁÔ ·˘Ùfi, ÔÏϤ˜ ¯ÒÚ˜·ÔÊ¿ÛÈÛ·Ó Ó· ÂÓÙ·¯ı› ÙÔ ÂÓ ÏfiÁˆ ÂÌ‚fiÏÈÔ ÛÙ· Ù·-ÎÙÈο ÚÔÁÚ¿ÌÌ·Ù· ÂÌ‚ÔÏÈ·ÛÌÔ‡.
√È ex ante ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘1 ÙÔ˘Ó¢ÌÔÓÈÔÎÔÎÎÈÎÔ‡ ÂÌ‚ÔÏ›Ô˘ ηٷϋÁÔ˘Ó ÛÙÔ Û˘-̤ڷÛÌ· fiÙÈ ·Ó Î·È ÙÔ ÂÌ‚fiÏÈÔ Â›Ó·È Ôχ ‰Ú·ÛÙÈ-Îfi Î·È ÌÂÈÒÓÂÈ ÙËÓ Â›ÙˆÛË Ù˘ ÓfiÛÔ˘, ˆÛÙfiÛÔ, ÌÂÙȘ ‰Â‰Ô̤Ó˜ ÙÈ̤˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘, Ë Â˘Ú›· ¯Ú‹ÛËÙÔ˘ ‰ÂÓ ¯·Ú·ÎÙËÚ›˙ÂÙ·È ¿ÓÙÔÙ ˆ˜ ÔÈÎÔÓÔÌÈο·Ô‰ÔÙÈ΋. √È ex post2 ÔÈÎÔÓÔÌÈΤ˜ ·ÍÈÔÏÔÁ‹ÛÂȘ¤‰ÂÈÍ·Ó fiÙÈ ·Ó ÏËÊı› ̆ fi„Ë Ë Â›‰Ú·ÛË Ù˘ Û˘ÏÏÔ-ÁÈ΋˜ ·ÓÔÛ›·˜, ÙfiÙÂ Ë ÛÙÚ·ÙËÁÈ΋ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ›ӷÈȉȷ›ÙÂÚ· ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ (36).øÛÙfiÛÔ, Ù· ¤ÌÌÂÛ· ·ÔÙÂϤÛÌ·Ù· ÙÔ˘ Ì·˙ÈÎÔ‡ ÂÌ-‚ÔÏÈ·ÛÌÔ‡ Á›ÓÔÓÙ·È Ê·ÓÂÚ¿ Ì·ÎÚÔ¯ÚfiÓÈ· Î·È ÁÈ· ÙÔÏfiÁÔ ·˘Ùfi ‰ÂÓ ÌÔÚÔ‡Ó Ó· Û˘Ó˘ÔÏÔÁÈÛÙÔ‡Ó ÛÙȘ exante ÔÈÎÔÓÔÌÈΤ˜ ·ÍÈÔÏÔÁ‹ÛÂȘ.
™ÙȘ ∏¶∞ ÙÔ ÂÙ·‰‡Ó·ÌÔ Û˘˙¢Á̤ÓÔ ÂÌ‚fiÏÈÔ΢ÎÏÔÊfiÚËÛ ÙÔ ºÂ‚ÚÔ˘¿ÚÈÔ ÙÔ˘ 2000 Î·È ˆ˜ ÂÎÙÔ‡ÙÔ˘, ÔÈ ¤ÌÌÂÛ˜ ÂȉڿÛÂȘ ÙÔ˘ Ì·˙ÈÎÔ‡ ÂÌ‚ÔÏÈ·-ÛÌÔ‡ Â›Ó·È ÂÚÈÛÛfiÙÂÚÔ ÂÌÊ·Ó›˜. ™˘ÁÎÂÎÚÈ̤ӷ,ÌÂÙ¿ ÙËÓ ÂÊ·ÚÌÔÁ‹ ÙÔ˘ ÚÔÁÚ¿ÌÌ·ÙÔ˜ ÌÂÈÒıËÎ·Ó ÔÈÏÔÈÌÒÍÂȘ Ô˘ ÚÔ¤Ú¯ÔÓÙ·Ó ·fi ÙÔ˘˜ ÔÚfiÙ˘Ô˘˜
151√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ
¶·È‰È·ÙÚÈ΋ 2008;71:148-156
¶›Ó·Î·˜ 1. ªÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÁÈ· ÙÔ ÂÌ‚fiÏÈÔ ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ Ù‡Ô˘ C
ÃÒÚ· Î·È ª¤ıÔ‰Ô˜ ¶ÚÔÔÙÈ΋ ™˘ÁÎÚÈÓfiÌÂÓ˜ ∞ÔÙÂϤÛÌ·Ù·¯ÚfiÓÔ˜ ·Ó¿Ï˘Û˘ ÛÙÚ·ÙËÁÈΤ˜‰ÈÂÍ·ÁˆÁ‹˜
∞ÁÁÏ›· ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ™‡ÛÙËÌ· ÀÁ›·˜ ¢È¿ÊÔÚ˜ ÛÙÚ·ÙËÁÈΤ˜ 1. √ ÂÌ‚ÔÏÈ·ÛÌfi˜ Â›Ó·È ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ 2002 ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Ô˘ ‰È¤ÊÂÚ·Ó ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ fiÙ·Ó Ë Â›ÙˆÛË Ù˘ ÓfiÛÔ˘ (14) ÛÙÔÓ ÙÚfiÔ ¯ÔÚ‹ÁËÛ‹˜ ÙÔ˘ Â›Ó·È ˘„ËÏ‹
Î·È ÛÙËÓ ËÏÈΛ· ¤Ó·Ú͢ 2. °È· ÙȘ ËÏÈ˘ 1-4 ÂÙÒÓ, Ë ¯ÔÚ‹ÁËÛË ÙÔ˘ ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ÂÌ‚ÔÏ›Ô˘ Â›Ó·È ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ
ÎfiÛÙÔ˜ fiÙ·Ó Á›ÓÂÙ·È ·fi ÙÔ˘˜ ÁÂÓÈÎÔ‡˜ È·ÙÚÔ‡˜3. °È· ÙȘ ÌÂÁ·Ï‡ÙÂÚ˜ ËÏÈ˘ (5-17 ÂÙÒÓ), Ë ¯Ô-
Ú‹ÁËÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Â›Ó·È ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈ-΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ fiÙ·Ó Á›ÓÂÙ·È ÛÙ· Û¯ÔÏ›·
∂Ï‚ÂÙ›· ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∞ÛÊ·ÏÈÛÙÈο 1. ∂Ì‚ÔÏÈ·ÛÌfi˜ 3 ‰fiÛÂˆÓ 1. ÀÔı¤ÙÔÓÙ·˜ ÂÌ‚ÔÏÈ·ÛÙÈ΋ Î¿Ï˘„Ë 80% Î·È 2003 ÃÚËÛÈÌfiÙËÙ·˜ ∆·Ì›· 2. ∂Ì‚ÔÏÈ·ÛÌfi˜ 1 ‰fiÛ˘ ·ÚÈıÌfi ÁÂÓÓ‹ÛÂˆÓ 80.000, Ë ¤ÓÙ·ÍË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ (15) ÛÙÔÓ Ù·ÎÙÈÎfi ÂÌ‚ÔÏÈ·ÛÌfi Â›Ó·È ·ÔÙÂÏÂÛÌ·ÙÈ-
΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜2. ∏ ÛÙÚ·ÙËÁÈ΋ 3 ‰fiÛÂˆÓ ÂÈÙ˘Á¯¿ÓÂÈ ÙÔ ÌÂÁ·-
χÙÂÚÔ fiÊÂÏÔ˜ ÁÈ· ÙËÓ ˘Á›·√ÏÏ·Ó‰›· ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›·, 1. ∂Ì‚ÔÏÈ·ÛÌfi˜ 3 ‰fiÛÂˆÓ 1. √ ÂÌ‚ÔÏÈ·ÛÌfi˜ Ô˘ Á›ÓÂÙ·È Ì¤¯ÚÈ ÙËÓ ‡ÊÂÛË 2004 ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ∞ÛÊ·ÏÈÛÙÈο 2. ∂Ì‚ÔÏÈ·ÛÌfi˜ 2 ‰fiÛÂˆÓ Ù˘ ÂȉËÌ›·˜ Â›Ó·È Ô ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ (16) ∆·Ì›· 3. ∂Ì‚ÔÏÈ·ÛÌfi˜ 1 ‰fiÛ˘ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜
4. ∂Ì‚ÔÏÈ·ÛÌfi˜ ̤¯ÚÈ ÙËÓ 2. ∞fi ÙȘ ÛÙÚ·ÙËÁÈΤ˜ ÙÔ˘ Ù·ÎÙÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡,‡ÊÂÛË Ù˘ ÂȉËÌ›·˜ Ë ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ›ӷÈ
·˘Ù‹ Ù˘ Ì›·˜ ‰fiÛ˘, ·Ó Î·È Ë ·ÔÙÂÏÂÛÌ·ÙÈÎfi-ÙËÙ· ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ‹Ù·Ó Ï›ÁÔ ÂÚÈÔÚÈṲ̂ÓË ÛÂÛ¯¤ÛË Ì ÙȘ ˘fiÏÔȘ ÛÙÚ·ÙËÁÈΤ˜
Quebec ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›· 1. ∂Ì‚ÔÏÈ·ÛÌfi˜ ̤¯ÚÈ ÙËÓ 1. ¶ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ∫·Ó·‰¿˜ ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ‡ÊÂÛË Ù˘ ÂȉËÌ›·˜ ÛÙÚ·ÙËÁÈ΋ ·ÓÔÛÔÔ›ËÛ˘ Â›Ó·È Ô Ù·ÎÙÈÎfi˜ 2004 2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1 ‰fiÛ˘ (17) 3 ‰fiÛÂˆÓ 2. ¶ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈ΋ ÎÏÈÓÈο Â›Ó·È Ë
3. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÛÙÚ·ÙËÁÈ΋ ÙÔ˘ Ù·ÎÙÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡ 1 ‰fiÛ˘ 3 ‰fiÛˆÓ
1 ªÂϤÙ˜ Ô˘ Ú·ÁÌ·ÙÔÔÈÔ‡ÓÙ·È ÚÈÓ ·fi ÙË Ï‹„Ë Ù˘ ·fiÊ·Û˘ ÁÈ· ÙËÓ ˘ÏÔÔ›ËÛË Ù˘ ·Ú¤Ì‚·Û˘.2 ªÂϤÙ˜ Ô˘ Ú·ÁÌ·ÙÔÔÈÔ‡ÓÙ·È ÌÂÙ¿ ÙË Ï‹„Ë Ù˘ ·fiÊ·Û˘ ÁÈ· ÙËÓ ˘ÏÔÔ›ËÛË Ù˘ ·Ú¤Ì‚·Û˘.
Pediatri Mar-Apr 08 09-04-08 10:36 ™ÂÏ›‰·151

ÙÔ˘ ÂÌ‚ÔÏ›Ô˘, Ì›ˆÛË Ô˘ Î˘Ì·ÈÓfiÙ·Ó ÛÙÔ 80% Â-
Ú›Ô˘ ÛÙ· ·È‰È¿ οو ÙˆÓ 2 ÂÙÒÓ (20), ÂÓÒ ÂÈϤ-
ÔÓ, ηٷÁÚ¿ÊËΠÂÏ¿ÙÙˆÛË ÙˆÓ ‰ÈÂÈÛ‰˘ÙÈÎÒÓ Ó¢-
ÌÔÓÈÔÎÔÎÎÈÎÒÓ ÏÔÈÌÒÍÂˆÓ Î·Ù¿ 54% Û ¿ÙÔÌ· 20-
39 ÂÙÒÓ, ηٿ 25% Û ¿ÙÔÌ· 40-64 ÂÙÒÓ Î·È Î·Ù¿
39% ÛÂ ¿ÙÔÌ· ¿Óˆ ÙˆÓ 65 ÂÙÒÓ (37).
ŒÓ· ¿ÏÏÔ ÛËÌ·ÓÙÈÎfi fiÊÂÏÔ˜ ‹Ù·Ó Ë Ì›ˆÛË Ù˘
·ÓÙÈÌÈÎÚԂȷ΋˜ ·ÓÙÔ¯‹˜, ηıÒ˜ Ù· ÙÂÏÂ˘Ù·›· ¯Úfi-
ÓÈ· Ù· ÛÙÂϤ¯Ë Ù˘ Ó¢ÌÔÓÈÔÎÔÎÎÈ΋˜ ÓfiÛÔ˘ ·-
ÚÔ˘ÛÈ¿˙Ô˘Ó ·ÓıÂÎÙÈÎfiÙËÙ· ÛÙ· ·ÓÙÈ‚ÈÔÙÈο, ÌÂ
·ÔÙ¤ÏÂÛÌ· Ó· Á›ÓÂÙ·È ‰‡ÛÎÔÏË Ë ·ÓÙÈÌÂÙÒÈÛ‹
ÙÔ˘˜ Î·È Ë Èı·ÓfiÙËÙ· ÂÈÏÔÎÒÓ Ó· Â›Ó·È ÌÂÁ·Ï‡-
ÙÂÚË (20). ∆Ô 2006 ‰ËÌÔÛȇÙËΠÌÈ· ÌÂϤÙË ÔÈÎÔ-
ÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÙÔ˘ Ó¢ÌÔÓÈÔÎÔÎÎÈÎÔ‡ ÂÌ-
‚ÔÏ›Ô˘, Ë ÔÔ›· ‚·Û›ÛÙËΠ۠ÛÙÔȯ›· ·fi ÙËÓ Â-
ÓÙ·ÂÙ‹ ÂÌÂÈÚ›· Ù˘ ÂÊ·ÚÌÔÁ‹˜ ÙÔ˘ ÛÙȘ ∏¶∞ (22).
∏ ex ante ÌÂϤÙË ÎfiÛÙÔ˘˜-·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜
ÂÎÙÈÌÔ‡ÛÂ fiÙÈ ÙÔ ÂÌ‚fiÏÈÔ ı· ÎfiÛÙÈ˙Â 176.000 ‰ÔÏ¿-
ÚÈ· ·Ó¿ ¤ÙÔ˜ ˙ˆ‹˜ Ô˘ ÛÒ˙ÂÙ·È, fiÙ·Ó ˘ÔÏÔÁÈ˙fiÙ·Ó
ÌfiÓÔ ÙÔ ¿ÌÂÛÔ È·ÙÚÈÎfi ÎfiÛÙÔ˜, ÂÓÒ ·Ó Û˘Ó˘ÔÏÔÁÈ-
˙fiÙ·Ó ÙÔ ¤ÌÌÂÛÔ ÎfiÛÙÔ˜ Î·È ÙÔ ÌË È·ÙÚÈÎfi ¿ÌÂÛÔ Îfi-
ÛÙÔ˜, ÙfiÙÂ ÙÔ ÂÌ‚fiÏÈÔ ı· ÎfiÛÙÈ˙Â 80.000 ‰ÔÏ¿ÚÈ·
·Ó¿ ¤ÙÔ˜ ˙ˆ‹˜ Ô˘ ÛÒ˙ÂÙ·È. ∆· ÛÙÔȯ›· Ô˘ ÚÔ¤-
΢„·Ó ·fi ÙËÓ ÂÓÙ·ÂÙ‹ ¯Ú‹ÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ¤‰ÂÈ-
Í·Ó fiÙÈ ÙÔ ÂÌ‚fiÏÈÔ Â¤‰Ú·ÛÂ Î·È ÛÙ· ÌË ÂÌ‚ÔÏÈ·-
Ṳ̂ӷ ¿ÙÔÌ·, ÛÙ· ÔÔ›· ·ÚÔ˘ÛÈ¿ÛÙËΠ̛ˆÛË ÙˆÓ
ÎÚÔ˘ÛÌ¿ÙˆÓ Ù˘ Ó¢ÌÔÓÈÔÎÔÎÎÈ΋˜ ÓfiÛÔ˘ Ô˘
¤ÊÙ·Û ÙÔ 68%. µ¿ÛÂÈ ·˘ÙÒÓ ÙˆÓ ÛÙÔȯ›ˆÓ ÙÔ Îfi-
ÛÙÔ˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ·Ó¿ ¤ÙÔ˜ ˙ˆ‹˜ Ô˘ ÛÒ˙ÂÙ·È ˘Ô-
ÏÔÁ›ÛÙËΠÛÙ· 7.500 ‰ÔÏ¿ÚÈ·.
∆· ·ÔÙÂϤÛÌ·Ù· ÙˆÓ ÌÂÏÂÙÒÓ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔ-
ÏfiÁËÛ˘ Û¯ÂÙÈο Ì ÙÔ ÂÌ‚fiÏÈÔ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜ ‰ÂÓ
152 µ. ∆ÛÈ¿ÓÙÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:148-156
¶›Ó·Î·˜ 2. ªÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÁÈ· ÙÔ ÂÌ‚fiÏÈÔ ÙÔ˘ Ó¢ÌÔÓÈfiÎÔÎÎÔ˘
ÃÒÚ· Î·È ª¤ıÔ‰Ô˜ ¶ÚÔÔÙÈ΋ ™˘ÁÎÚÈÓfiÌÂÓ˜ ∞ÔÙÂϤÛÌ·Ù·¯ÚfiÓÔ˜ ·Ó¿Ï˘Û˘/ ÛÙÚ·ÙËÁÈΤ˜‰ÈÂÍ·ÁˆÁ‹˜ ÀÔÏÔÁÈÛÌfi˜
ÎfiÛÙÔ˘˜
2001 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›·, 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÌÔÚ› Ó· ÌÂÙ·‚¿ÏÂÈ Kaiser ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ™‡ÛÙËÌ· ÀÁ›·˜ 4 ‰fiÛÂˆÓ Û ‚Ú¤ÊË ÙËÓ ÂȉËÌÈÔÏÔÁ›· Ù˘ ÓfiÛÔ˘Permanente, (2-15 ÌËÓÒÓ) Î·È 2. ∞ÎfiÌ· ÌÔÚ› Ó· ·Ô‰Âȯı› ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ Oakland ÂÌ‚ÔÏÈ·ÛÌfi˜ Ì›·˜ ‰fiÛ˘ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ·Ó¿ÏÔÁ· Ì ÙÔ ÎfiÛÙÔ˜ ÙÔ˘ ∫·ÏÈÊfiÚÓÈ·, Û ·È‰È¿ 2-5 ÂÙÒÓ Û˘ÓÔÏÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡∏¶∞ (20) 2. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜
2003 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›· 1. ∆·ÎÙÈÎfi˜ ∂Ì‚ÔÏÈ·ÛÌfi˜ 1. ¶ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ Â›Ó·È ∫·Ó·‰¿˜ ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ 4 ‰fiÛÂˆÓ Ô Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜(21) 2. ŒÎÙ·ÎÙÔ˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 2. øÛÙfiÛÔ, Ô ÂÌ‚ÔÏÈ·ÛÌfi˜ ı· Â›Ó·È ÈÔ ·Ô‰ÔÙÈÎfi˜
3 ‰fiÛÂˆÓ ÁÈ· ÙËÓ ÎÔÈÓˆÓ›·, ·Ó Ë ÙÈÌ‹ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ 3. ŒÎÙ·ÎÙÔ˜ 2 ‰fiÛÂˆÓ ÌÂȈı› ÛÙ· $30/‰fiÛË4. ŒÎÙ·ÎÙÔ˜ 1 ‰fiÛ˘
2003 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›· 1. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÌÔÚ› Ó· ·ÔÙÚ¤„ÂÈ √ÏÏ·Ó‰›· ÃÚËÛÈÌfiÙËÙ·˜ 2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÌÂÁ¿ÏÔ ·ÚÈıÌfi Ó¢ÌÔÓÈÔÎÔÎÎÈÎÒÓ ÏÔÈÌÒÍÂˆÓ (22) Î·È Ó· ÌÂÈÒÛÂÈ ÙË ıÓËÛÈÌfiÙËÙ· Î·È ÙË
ÓÔÛËÚfiÙËÙ·2. √ ‰Â›ÎÙ˘ ÎfiÛÙÔ˘˜- ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ‰ÂÓ
Â›Ó·È Â˘ÓÔ˚Îfi˜ (83.226 – ·Ó¿ ¤ÙÔ˜ ˙ˆ‹˜ Ô˘ ÛÒ-˙ÂÙ·È), ÁÈ’ ·˘Ùfi ÚÔÙ›ÓÂÙ·È Ó· ÌËÓ ÂÓÙ·¯ı› ÙÔÂÌ‚fiÏÈÔ ÛÙÔÓ Ù·ÎÙÈÎfi ÂÌ‚ÔÏÈ·ÛÌfi
2003 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∞ÛÊ·ÏÈÛÙÈο 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. ∞fi ÙËÓ ÚÔÔÙÈ΋ ÙˆÓ ·ÛÊ·ÏÈÛÙÈÎÒÓ Ù·Ì›ˆÓ °ÂÚÌ·Ó›· ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ∆·Ì›·, ∫ÔÈÓˆÓ›· ‚ÚÂÊÒÓ Î·È ·È‰ÈÒÓ ÙÔ ÂÌ‚fiÏÈÔ ÂÍÔÈÎÔÓÔÌ› 51,1% ÙˆÓ ‰··ÓÒÓ ÙÔ˘(23) ÌÈÎÚfiÙÂÚ· ÙˆÓ 2 ÂÙÒÓ 2. √ ÂÌ‚ÔÏÈ·ÛÌfi˜ Â›Ó·È ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ ÚÔ˜
2. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜ ÙÔ ÎfiÛÙÔ˜ ·fi ÙËÓ ÎÔÈÓˆÓÈ΋ ÚÔÔÙÈ΋
2004 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ™‡ÛÙËÌ· ÀÁ›·˜, 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. ∏ ÂÈÛ·ÁˆÁ‹ ÙÔ˘ Ó¢ÌÔÓÈÔÎÔÎÎÈÎÔ‡ ÂÌ‚ÔÏ›Ô˘ πÛ·Ó›· ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ∫ÔÈÓˆÓ›· fiÏˆÓ ÙˆÓ ‚ÚÂÊÒÓ ËÏÈΛ·˜ ÛÙÔ ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ ı· ÌÂÈÒÛÂÈ (24) 6 ‚‰ÔÌ¿‰ˆÓ-7 ÌËÓÒÓ ÛËÌ·ÓÙÈο ÙË ıÓËÛÈÌfiÙËÙ· Î·È ÙË ÓÔÛËÚfiÙËÙ·
2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ Ô˘ Û¯ÂÙ›˙ÂÙ·È Ì ÙËÓ Ó¢ÌÔÓÈÔÎÔÎÎÈ΋ fiÏˆÓ ÙˆÓ ·È‰ÈÒÓ Î¿Ùˆ Ïԛ̈ÍË ÛÙ· ·È‰È¿ÙˆÓ 5 ÂÙÒÓ 2. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ fiÏˆÓ ÙˆÓ ·È‰ÈÒÓ <5
ÂÙÒÓ Â›Ó·È ·Ô‰ÔÙÈÎfi˜ ·fi ÙËÓ ÎÔÈÓˆÓÈ΋ ÛÎÔÈ¿ Î·È ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜·fi ÙË ÛÎÔÈ¿ ÙÔ˘ Û˘ÛÙ‹Ì·ÙÔ˜ ˘Á›·˜
Pediatri Mar-Apr 08 09-04-08 10:37 ™ÂÏ›‰·152
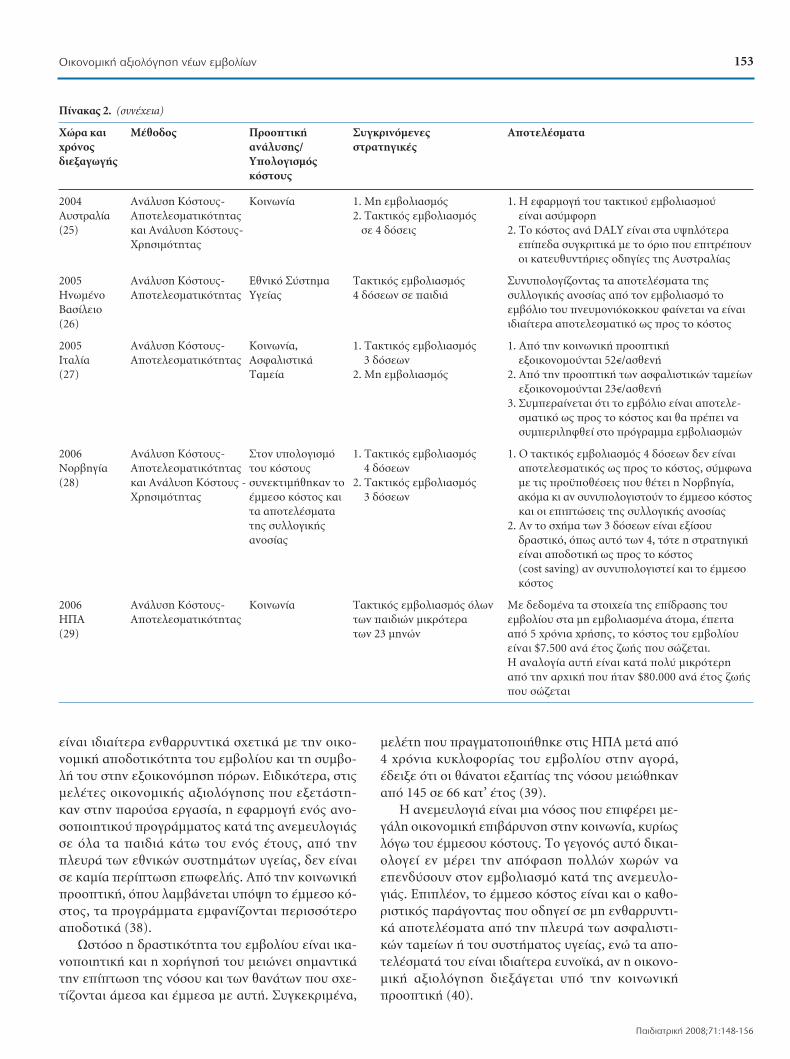
Â›Ó·È È‰È·›ÙÂÚ· ÂÓı·ÚÚ˘ÓÙÈο Û¯ÂÙÈο Ì ÙËÓ ÔÈÎÔ-ÓÔÌÈ΋ ·Ô‰ÔÙÈÎfiÙËÙ· ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Î·È ÙË Û˘Ì‚Ô-Ï‹ ÙÔ˘ ÛÙËÓ ÂÍÔÈÎÔÓfiÌËÛË fiÚˆÓ. ∂ȉÈÎfiÙÂÚ·, ÛÙȘÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ Ô˘ ÂÍÂÙ¿ÛÙË-Î·Ó ÛÙËÓ ·ÚÔ‡Û· ÂÚÁ·Û›·, Ë ÂÊ·ÚÌÔÁ‹ ÂÓfi˜ ·ÓÔ-ÛÔÔÈËÙÈÎÔ‡ ÚÔÁÚ¿ÌÌ·ÙÔ˜ ηٿ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜Û fiÏ· Ù· ·È‰È¿ οو ÙÔ˘ ÂÓfi˜ ¤ÙÔ˘˜, ·fi ÙËÓÏÂ˘Ú¿ ÙˆÓ ÂıÓÈÎÒÓ Û˘ÛÙËÌ¿ÙˆÓ ˘Á›·˜, ‰ÂÓ Â›Ó·ÈÛ η̛· ÂÚ›ÙˆÛË ÂˆÊÂÏ‹˜. ∞fi ÙËÓ ÎÔÈÓˆÓÈ΋ÚÔÔÙÈ΋, fiÔ˘ Ï·Ì‚¿ÓÂÙ·È ˘fi„Ë ÙÔ ¤ÌÌÂÛÔ Îfi-ÛÙÔ˜, Ù· ÚÔÁÚ¿ÌÌ·Ù· ÂÌÊ·Ó›˙ÔÓÙ·È ÂÚÈÛÛfiÙÂÚÔ·Ô‰ÔÙÈο (38).
øÛÙfiÛÔ Ë ‰Ú·ÛÙÈÎfiÙËÙ· ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Â›Ó·È Èη-ÓÔÔÈËÙÈ΋ Î·È Ë ¯ÔÚ‹ÁËÛ‹ ÙÔ˘ ÌÂÈÒÓÂÈ ÛËÌ·ÓÙÈοÙËÓ Â›ÙˆÛË Ù˘ ÓfiÛÔ˘ Î·È ÙˆÓ ı·Ó¿ÙˆÓ Ô˘ Û¯Â-Ù›˙ÔÓÙ·È ¿ÌÂÛ· Î·È ¤ÌÌÂÛ· Ì ·˘Ù‹. ™˘ÁÎÂÎÚÈ̤ӷ,
ÌÂϤÙË Ô˘ Ú·ÁÌ·ÙÔÔÈ‹ıËΠÛÙȘ ∏¶∞ ÌÂÙ¿ ·fi4 ¯ÚfiÓÈ· ΢ÎÏÔÊÔÚ›·˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ÛÙËÓ ·ÁÔÚ¿,¤‰ÂÈÍ fiÙÈ ÔÈ ı¿Ó·ÙÔÈ ÂÍ·ÈÙ›·˜ Ù˘ ÓfiÛÔ˘ ÌÂÈÒıËηӷfi 145 Û 66 ηْ ¤ÙÔ˜ (39).
∏ ·ÓÂÌ¢ÏÔÁÈ¿ Â›Ó·È ÌÈ· ÓfiÛÔ˜ Ô˘ ÂÈʤÚÂÈ ÌÂ-Á¿ÏË ÔÈÎÔÓÔÌÈ΋ ÂÈ‚¿Ú˘ÓÛË ÛÙËÓ ÎÔÈÓˆÓ›·, ΢ڛˆ˜ÏfiÁˆ ÙÔ˘ ¤ÌÌÂÛÔ˘ ÎfiÛÙÔ˘˜. ∆Ô ÁÂÁÔÓfi˜ ·˘Ùfi ‰ÈηÈ-ÔÏÔÁ› ÂÓ Ì¤ÚÂÈ ÙËÓ ·fiÊ·ÛË ÔÏÏÒÓ ¯ˆÚÒÓ Ó·ÂÂÓ‰‡ÛÔ˘Ó ÛÙÔÓ ÂÌ‚ÔÏÈ·ÛÌfi ηٿ Ù˘ ·ÓÂÌ¢ÏÔ-ÁÈ¿˜. ∂ÈϤÔÓ, ÙÔ ¤ÌÌÂÛÔ ÎfiÛÙÔ˜ Â›Ó·È Î·È Ô Î·ıÔ-ÚÈÛÙÈÎfi˜ ·Ú¿ÁÔÓÙ·˜ Ô˘ Ô‰ËÁ› Û ÌË ÂÓı·ÚÚ˘ÓÙÈ-ο ·ÔÙÂϤÛÌ·Ù· ·fi ÙËÓ ÏÂ˘Ú¿ ÙˆÓ ·ÛÊ·ÏÈÛÙÈ-ÎÒÓ Ù·Ì›ˆÓ ‹ ÙÔ˘ Û˘ÛÙ‹Ì·ÙÔ˜ ˘Á›·˜, ÂÓÒ Ù· ·Ô-ÙÂϤÛÌ·Ù¿ ÙÔ˘ Â›Ó·È È‰È·›ÙÂÚ· ¢ÓÔ˚ο, ·Ó Ë ÔÈÎÔÓÔ-ÌÈ΋ ·ÍÈÔÏfiÁËÛË ‰ÈÂÍ¿ÁÂÙ·È ˘fi ÙËÓ ÎÔÈÓˆÓÈ΋ÚÔÔÙÈ΋ (40).
153√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ
¶·È‰È·ÙÚÈ΋ 2008;71:148-156
¶›Ó·Î·˜ 2. (Û˘Ó¤¯ÂÈ·)
ÃÒÚ· Î·È ª¤ıÔ‰Ô˜ ¶ÚÔÔÙÈ΋ ™˘ÁÎÚÈÓfiÌÂÓ˜ ∞ÔÙÂϤÛÌ·Ù·¯ÚfiÓÔ˜ ·Ó¿Ï˘Û˘/ ÛÙÚ·ÙËÁÈΤ˜‰ÈÂÍ·ÁˆÁ‹˜ ÀÔÏÔÁÈÛÌfi˜
ÎfiÛÙÔ˘˜
2004 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›· 1. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. ∏ ÂÊ·ÚÌÔÁ‹ ÙÔ˘ Ù·ÎÙÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ∞˘ÛÙÚ·Ï›· ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ 2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ Â›Ó·È ·Û‡ÌÊÔÚË(25) Î·È ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- Û 4 ‰fiÛÂȘ 2. ∆Ô ÎfiÛÙÔ˜ ·Ó¿ DALY Â›Ó·È ÛÙ· ˘„ËÏfiÙÂÚ·
ÃÚËÛÈÌfiÙËÙ·˜ ›‰· Û˘ÁÎÚÈÙÈο Ì ÙÔ fiÚÈÔ Ô˘ ÂÈÙÚ¤Ô˘ÓÔÈ Î·Ù¢ı˘ÓÙ‹ÚȘ Ô‰ËÁ›Â˜ Ù˘ ∞˘ÛÙÚ·Ï›·˜
2005 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∂ıÓÈÎfi ™‡ÛÙËÌ· ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ™˘Ó˘ÔÏÔÁ›˙ÔÓÙ·˜ Ù· ·ÔÙÂϤÛÌ·Ù· Ù˘ ∏ӈ̤ÓÔ ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ÀÁ›·˜ 4 ‰fiÛÂˆÓ Û ·È‰È¿ Û˘ÏÏÔÁÈ΋˜ ·ÓÔÛ›·˜ ·fi ÙÔÓ ÂÌ‚ÔÏÈ·ÛÌfi ÙÔ µ·Û›ÏÂÈÔ ÂÌ‚fiÏÈÔ ÙÔ˘ Ó¢ÌÔÓÈfiÎÔÎÎÔ˘ Ê·›ÓÂÙ·È Ó· Â›Ó·È (26) ȉȷ›ÙÂÚ· ·ÔÙÂÏÂÛÌ·ÙÈÎfi ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜
2005 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›·, 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. ∞fi ÙËÓ ÎÔÈÓˆÓÈ΋ ÚÔÔÙÈ΋ πÙ·Ï›· ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ∞ÛÊ·ÏÈÛÙÈο 3 ‰fiÛÂˆÓ ÂÍÔÈÎÔÓÔÌÔ‡ÓÙ·È 52–/·ÛıÂÓ‹(27) ∆·Ì›· 2. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜ 2. ∞fi ÙËÓ ÚÔÔÙÈ΋ ÙˆÓ ·ÛÊ·ÏÈÛÙÈÎÒÓ Ù·Ì›ˆÓ
ÂÍÔÈÎÔÓÔÌÔ‡ÓÙ·È 23–/·ÛıÂÓ‹3. ™˘ÌÂÚ·›ÓÂÙ·È fiÙÈ ÙÔ ÂÌ‚fiÏÈÔ Â›Ó·È ·ÔÙÂÏÂ-
ÛÌ·ÙÈÎfi ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ Î·È ı· Ú¤ÂÈ Ó·Û˘ÌÂÚÈÏËÊı› ÛÙÔ ÚfiÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÒÓ
2006 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ™ÙÔÓ ˘ÔÏÔÁÈÛÌfi 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 4 ‰fiÛÂˆÓ ‰ÂÓ Â›Ó·È ¡ÔÚ‚ËÁ›· ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ÙÔ˘ ÎfiÛÙÔ˘˜ 4 ‰fiÛÂˆÓ ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜, Û‡Ìʈӷ (28) Î·È ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜ - Û˘ÓÂÎÙÈÌ‹ıËÎ·Ó ÙÔ 2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ Ì ÙȘ ÚÔ¸Ôı¤ÛÂȘ Ô˘ ı¤ÙÂÈ Ë ¡ÔÚ‚ËÁ›·,
ÃÚËÛÈÌfiÙËÙ·˜ ¤ÌÌÂÛÔ ÎfiÛÙÔ˜ Î·È 3 ‰fiÛÂˆÓ ·ÎfiÌ· ÎÈ ·Ó Û˘Ó˘ÔÏÔÁÈÛÙÔ‡Ó ÙÔ ¤ÌÌÂÛÔ ÎfiÛÙÔ˜ Ù· ·ÔÙÂϤÛÌ·Ù· Î·È ÔÈ ÂÈÙÒÛÂȘ Ù˘ Û˘ÏÏÔÁÈ΋˜ ·ÓÔÛ›·˜Ù˘ Û˘ÏÏÔÁÈ΋˜ 2. ∞Ó ÙÔ Û¯‹Ì· ÙˆÓ 3 ‰fiÛÂˆÓ Â›Ó·È ÂÍ›ÛÔ˘ ·ÓÔÛ›·˜ ‰Ú·ÛÙÈÎfi, fiˆ˜ ·˘Ùfi ÙˆÓ 4, ÙfiÙÂ Ë ÛÙÚ·ÙËÁÈ΋
Â›Ó·È ·Ô‰ÔÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ (cost saving) ·Ó Û˘Ó˘ÔÏÔÁÈÛÙ› Î·È ÙÔ ¤ÌÌÂÛÔÎfiÛÙÔ˜
2006 ∞Ó¿Ï˘ÛË ∫fiÛÙÔ˘˜- ∫ÔÈÓˆÓ›· ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ fiÏˆÓ ªÂ ‰Â‰Ô̤ӷ Ù· ÛÙÔȯ›· Ù˘ ›‰Ú·Û˘ ÙÔ˘ ∏¶∞ ∞ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ·˜ ÙˆÓ ·È‰ÈÒÓ ÌÈÎÚfiÙÂÚ· ÂÌ‚ÔÏ›Ô˘ ÛÙ· ÌË ÂÌ‚ÔÏÈ·Ṳ̂ӷ ¿ÙÔÌ·, ¤ÂÈÙ· (29) ÙˆÓ 23 ÌËÓÒÓ ·fi 5 ¯ÚfiÓÈ· ¯Ú‹Û˘, ÙÔ ÎfiÛÙÔ˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘
Â›Ó·È $7.500 ·Ó¿ ¤ÙÔ˜ ˙ˆ‹˜ Ô˘ ÛÒ˙ÂÙ·È. ∏ ·Ó·ÏÔÁ›· ·˘Ù‹ Â›Ó·È Î·Ù¿ Ôχ ÌÈÎÚfiÙÂÚË·fi ÙËÓ ·Ú¯È΋ Ô˘ ‹Ù·Ó $80.000 ·Ó¿ ¤ÙÔ˜ ˙ˆ‹˜Ô˘ ÛÒ˙ÂÙ·È
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·153

¶›Ó·Î·˜ 3. ªÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜
ÃÒÚ· Î·È ª¤ıÔ‰Ô˜ ¶ÚÔÔÙÈ΋ ·Ó¿Ï˘Û˘/ ™˘ÁÎÚÈÓfiÌÂÓ˜ ∞ÔÙÂϤÛÌ·Ù·¯ÚfiÓÔ˜ ÀÔÏÔÁÈÛÌfi˜ ÛÙÚ·ÙËÁÈΤ˜‰ÈÂÍ·ÁˆÁ‹˜ ÎfiÛÙÔ˘˜
1999 ∞Ó¿Ï˘ÛË ∂ıÓÈÎfi 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. ∏ ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ∞˘ÛÙÚ·Ï›· ∫fiÛÙÔ˘˜- ™‡ÛÙËÌ· ÀÁ›·˜ fiÏˆÓ ÙˆÓ ·È‰ÈÒÓ ÛÙÚ·ÙËÁÈ΋ ‹Ù·Ó ·˘Ù‹ ÙÔ˘ Ù·ÎÙÈÎÔ‡ (31) ∞ÔÙÂÏÂÛÌ·ÙÈ- 2. ∂Ì‚ÔÏÈ·ÛÌfi˜ ÂÊ‹‚ˆÓ Ô˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ fiÏˆÓ ÙˆÓ ·È‰ÈÒÓ
ÎfiÙËÙ·˜ ‰ÂÓ Â›¯·Ó ÓÔÛ‹ÛÂÈ ·fi ·ÓÂÌ¢- 2. ¶ÈÔ ‰Ú·ÛÙÈ΋ ÛÙÚ·ÙËÁÈ΋ ÁÈ· ÙËÓ ·ÓÙÈÌÂÙÒ-ÏÔÁÈ¿ Û ÌÈÎÚfiÙÂÚË ËÏÈΛ· ÈÛË Ù˘ ·Ûı¤ÓÂÈ·˜ ‹Ù·Ó ·˘Ù‹ ÙÔ˘ Û˘Ó‰˘·-
3. ™˘Ó‰˘·ÛÌfi˜ ÙˆÓ ‰‡Ô ·Ú·¿Óˆ ÛÌÔ‡ (ÂÌ‚ÔÏÈ·ÛÌfi˜ ·È‰ÈÒÓ Î·È ÂÊ‹‚ˆÓ), 4. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜ ·ÏÏ¿ ‰ÂÓ ‹Ù·Ó ÔÈÎÔÓÔÌÈο ·Ô‰ÔÙÈ΋
2002 ∞Ó¿Ï˘ÛË ∫ÔÈÓˆÓ›·, 1. ªË ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. ∆Ș ηχÙÂÚ˜ ÂÈÙÒÛÂȘ ÛÙËÓ ˘Á›· ›¯Â Ë ∫·Ó·‰¿˜ ∫fiÛÙÔ˘˜- ™‡ÛÙËÌ· ÀÁ›·˜ 2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÛÙÚ·ÙËÁÈ΋ ÙÔ˘ ÌÈÎÙÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡, ·ÏÏ¿ ‰ÂÓ (32) ∞ÔÙÂÏÂÛÌ·ÙÈ- fiÏˆÓ ÙˆÓ ·È‰ÈÒÓ ‹Ù·Ó ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ·fi
ÎfiÙËÙ·˜ 3. ∂Ì‚ÔÏÈ·ÛÌfi˜ ÂÊ‹‚ˆÓ Ô˘ ÙË ÛÎÔÈ¿ ÙÔ˘ Û˘ÛÙ‹Ì·ÙÔ˜ ˘Á›·˜‰ÂÓ Â›¯·Ó ÓÔÛ‹ÛÂÈ ·fi 2. ∞fi ÙËÓ ÔÙÈ΋ Ù˘ ÎÔÈÓˆÓ›·˜, Ë ÈÔ·ÓÂÌ¢ÏÔÁÈ¿ Û ÌÈÎÚfiÙÂÚË ·ÔÙÂÏÂÛÌ·ÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ËÏÈΛ· ÛÙÚ·ÙËÁÈ΋ ‹Ù·Ó ·˘Ù‹ ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ fiψÓ
4. ™˘Ó‰˘·ÛÌfi˜ ÙˆÓ ‰‡Ô ÙˆÓ ·È‰ÈÒÓ ÛÙËÓ ËÏÈΛ· ÙÔ˘ ÂÓfi˜ ¤ÙÔ˘˜·Ú·¿Óˆ 3. ∏ ÛÙÚ·ÙËÁÈ΋ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ÌfiÓÔ ÙˆÓ ÂÊ‹‚ˆÓ
·ÚÔ˘ÛÈ¿˙ÂÙ·È ·ÔÙÂÏÂÛÌ·ÙÈ΋ ̂ ̃ÚÔ ̃ÙÔ ÎfiÛÙÔ˜ÌfiÓÔ ·fi ÙËÓ ÔÙÈ΋ ÙÔ˘ Û˘ÛÙ‹Ì·ÙÔ˜ ˘Á›·˜
2003 ∞Ó¿Ï˘ÛË ∫ÔÈÓˆÓ›·, 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. √ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÙˆÓ ÂÊ‹‚ˆÓ Â›Ó·È Ô ÈÔ ·ÛÊ·Ï‹˜ ∞ÁÁÏ›·- ∫fiÛÙÔ˘˜- ™‡ÛÙËÌ· ÀÁ›·˜ ‚ÚÂÊÒÓ Î·È Ô ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ √˘·Ï›· ÃÚËÛÈÌfiÙËÙ·˜ 2. ŒÎÙ·ÎÙÔ˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ·fi ÙËÓ ÚÔÔÙÈ΋ ÙÔ˘ Û˘ÛÙ‹Ì·ÙÔ˜ ˘Á›·˜(33) ·È‰ÈÒÓ 2-11 ÂÙÒÓ 2. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÙˆÓ ‚ÚÂÊÒÓ Â›Ó·È
3. ∂Ì‚ÔÏÈ·ÛÌfi˜ ÂÊ‹‚ˆÓ ·›ı·ÓÔ Ó· Â›Ó·È ·ÔÙÂÏÂÛÌ·ÙÈÎfi˜ ˆ˜ ÚÔ˜ ¿Óˆ ÙˆÓ 11 ÂÙÒÓ ÙÔ ÎfiÛÙÔ˜
2004 ∞Ó¿Ï˘ÛË ∫ÔÈÓˆÓ›·, 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ 1. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ¯ˆÚ›˜ ·ÌÊÈ‚ÔÏ›· πÙ·Ï›· ∫fiÛÙÔ˘˜- ™‡ÛÙËÌ· ÀÁ›·˜ ·È‰ÈÒÓ ËÏÈΛ·˜ 1-2 ÂÙÒÓ ¤¯ÂÈ ıÂÙÈ΋ ›‰Ú·ÛË ÛÙË ÓÔÛËÚfiÙËÙ· ÏfiÁˆ (34) √ʤÏÔ˘˜ (Ï·Ì‚¿ÓÔÓÙ·˜ ˘fi„Ë ·ÓÂÌ¢ÏÔÁÈ¿˜. ∆· ÌÂÁ·Ï‡ÙÂÚ· ıÂÙÈο
‰È·ÊÔÚÂÙÈο ›‰· ·ÔÙÂϤÛÌ·Ù· ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È fiÙ·Ó ÙÔ ÔÛÔ-ÂÌ‚ÔÏÈ·ÛÙÈ΋˜ Î¿Ï˘„˘ ÛÙfi Ù˘ ÂÌ‚ÔÏÈ·ÛÙÈ΋˜ Î¿Ï˘„˘ Â›Ó·È 90%
2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ·È‰ÈÒÓ 2. ∆Ô ÛÂÓ¿ÚÈÔ ÙÔ˘ Ù·ÎÙÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Ì ËÏÈΛ·˜ (1-2 ÂÙÒÓ) ÛÂ Û˘Ó‰˘·- ÔÛÔÛÙfi ÂÌ‚ÔÏÈ·ÛÙÈ΋˜ Î¿Ï˘„˘ 90%, Â›Ó·È ÛÌfi Ì ¤Ó· ÚfiÁÚ·ÌÌ· ÂÌ‚Ô- ·Ô‰ÔÙÈÎfi ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜, ÙfiÛÔ ·fi ÙËÓ ÏÈ·ÛÌÔ‡ ÙˆÓ ·ÙfiÌˆÓ Ô˘ ‰ÂÓ ÎÔÈÓˆÓÈ΋ ÚÔÔÙÈ΋, fiÛÔ Î·È ·fi ÙËÓ Â›¯·Ó ÂÌ‚ÔÏÈ·ÛÙ› ÛÙË Û˘ÓÈ- ÚÔÔÙÈ΋ ÙÔ˘ Û˘ÛÙ‹Ì·ÙÔ˜ ˘Á›·˜ÛÙÒÌÂÓË ËÏÈΛ· (ÙÔ ÔÔ›Ô ı· 3. ŸÛÔ ÌÂÈÒÓÂÙ·È ÙÔ Â›Â‰Ô Ù˘ ÂÌ‚ÔÏÈ·ÛÙÈ΋˜ ‰È·ÚÎÔ‡Û ٷ 5 ÚÒÙ· ¤ÙË Ù˘ Î¿Ï˘„˘ ÙfiÛÔ ÏÈÁfiÙÂÚÔ ·Ô‰ÔÙÈÎfi ˆ˜ ÚÔ˜ ÙÔ Î˘ÎÏÔÊÔÚ›·˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘) ÎfiÛÙÔ˜ Á›ÓÂÙ·È ÙÔ ÚfiÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÔ‡.
3. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ·È‰ÈÒÓ ¶·ÚfiÏ· ·˘Ù¿ ·ÎfiÌ· Î·È ÛÙÔ ¯ÂÈÚfiÙÂÚÔ ÛÂÓ¿ÚÈÔ ËÏÈΛ·˜ (1-2 ÂÙÒÓ) Û ÙÔ ÂÌ‚fiÏÈÔ ·Ú·Ì¤ÓÂÈ ·ÔÙÂÏÂÛÌ·ÙÈÎfi ˆ˜ Û˘Ó‰˘·ÛÌfi Ì ¤Ó· ÚfiÁÚ·ÌÌ· ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ÂÌ‚ÔÏÈ·ÛÌÔ‡ ÙˆÓ ·ÙfiÌˆÓ Ô˘ ‰ÂÓ Â›¯·Ó ÂÌ‚ÔÏÈ·ÛÙ› ÛÙË Û˘ÓÈÛÙÒÌÂÓË ËÏÈΛ· (ÙÔ ÔÔ›Ô ı· ‰È·ÚÎÔ‡Û ÙÔ ÚÒÙÔ ¤ÙÔ˜ Ù˘ ΢ÎÏÔÊÔÚ›·˜ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘)
2006 Dynamic model ∫ÔÈÓˆÓ›·, 1. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÁÈ· 1. √ Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ¤¯ÂÈ ıÂÙÈ΋ ›‰Ú·ÛË πÛ·Ó›· ∞ÛÊ·ÏÈÛÙÈο ·È‰È¿ 1-2 ÂÙÒÓ Î·È ÛÙË ÓÔÛËÚfiÙËÙ· Ô˘ Û¯ÂÙ›˙ÂÙ·È Ì ÙËÓ (35) ∆·Ì›· 2. ∆·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ Û ·ÓÂÌ¢ÏÔÁÈ¿. ª¿ÏÈÛÙ· ·fi ÎÔÈÓˆÓÈ΋ ÛÎÔÈ¿
Û˘Ó‰˘·ÛÌfi Ì ÂÌ‚ÔÏÈ·ÛÌfi Ë ÛÙÚ·ÙËÁÈ΋ ·˘Ù‹ ÂÌÊ·Ó›˙ÂÙ·È È‰È·›ÙÂÚ· ·ÙfiÌˆÓ Ô˘ ‰ÂÓ Â›¯·Ó ·Ô‰ÔÙÈ΋ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ›Ù ÏËÊı› ÂÌ‚ÔÏÈ·ÛÙ› ÛÙË Û˘ÓÈÛÙÒÌÂÓË ˘fi„Ë ÙÔ ¤ÌÌÂÛÔ ÎfiÛÙÔ˜ ›Ù fi¯ÈËÏÈΛ· (catch-up program) 2. ∞fi ÙË ÛÎÔÈ¿ ÙˆÓ ·ÛÊ·ÏÈÛÙÈÎÒÓ ÊÔÚ¤ˆÓ, Ô
Ù·ÎÙÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ıˆÚÂ›Ù·È ·ÔÙÂÏÂ-ÛÌ·ÙÈÎfi˜ ˆ˜ ÚÔ˜ ÙÔ ÎfiÛÙÔ˜ ·Ó Î·È ·˘Í¿ÓÂÙ·ÈÏ›ÁÔ ÙÔ ÎfiÛÙÔ˜
154 µ. ∆ÛÈ¿ÓÙÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:148-156
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·154

√ ¶√À Û˘ÓÈÛÙ¿ ÙÔÓ Ù·ÎÙÈÎfi ÂÌ‚ÔÏÈ·ÛÌfi fiψÓ
ÙˆÓ ·È‰ÈÒÓ ÛÙȘ ¯ÒÚ˜ fiÔ˘ Ë ·ÓÂÌ¢ÏÔÁÈ¿ ·Ô-
ÙÂÏ› ÛËÌ·ÓÙÈÎfi Úfi‚ÏËÌ· Ù˘ ‰ËÌfiÛÈ·˜ ˘Á›·˜
Î·È Ù˘ ÎÔÈÓˆÓÈÎÔÔÈÎÔÓÔÌÈ΋˜ ηٿÛÙ·Û˘ Ù˘
¯ÒÚ·˜. ª¤¯ÚÈ ÙÔ 2004 ÙÔ ÂÌ‚fiÏÈÔ Î˘ÎÏÔÊÔÚÔ‡ÛÂ
ÛÙȘ ÂÚÈÛÛfiÙÂÚ˜ Â˘Úˆ·˚Τ˜ ¯ÒÚ˜ Î·È ÔÚÈṲ̂-
Ó˜ ·fi ·˘Ù¤˜ ÙÔ Â›¯·Ó ÂÓÙ¿ÍÂÈ ÛÙÔÓ Ù·ÎÙÈÎfi ÂÌ‚Ô-
ÏÈ·ÛÌfi (40).
™˘˙‹ÙËÛË
∆· ÚÔÁÚ¿ÌÌ·Ù· ·ÓÔÛÔÔ›ËÛ˘ Â›Ó·È ¯ˆÚ›˜ ·Ì-
ÊÈ‚ÔÏ›· Ë ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙÂÚË ·Ú¤Ì‚·ÛË ÁÈ· ÙË
Ì›ˆÛË Ù˘ ıÓËÛÈÌfiÙËÙ·˜, Ù˘ ÓÔÛËÚfiÙËÙ·˜ Î·È ÙÔ˘
ÎfiÛÙÔ˘˜ Ô˘ Û¯ÂÙ›˙ÂÙ·È Ì ٷ ÏÔÈÌÒ‰Ë ÓÔÛ‹Ì·Ù·.
∏ ·fiÊ·ÛË ÁÈ· ÙËÓ ¤ÓÙ·ÍË ÂÓfi˜ ÂÌ‚ÔÏ›Ô˘ ÛÙÔ
∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ ÌÈ·˜ ¯ÒÚ·˜ Ï·Ì-
‚¿ÓÂÙ·È ‚¿ÛÂÈ ÂȉËÌÈÔÏÔÁÈÎÒÓ, ÔÈÎÔÓÔÌÈÎÒÓ, ÔÏÈ-
ÙÈÎÒÓ Î·È ÎÔÈÓˆÓÈÎÒÓ ÎÚÈÙËÚ›ˆÓ. ∏ Ù¯ÓÈ΋ Ù˘ ÔÈ-
ÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘, ·Ó Î·È ·ÊÔÚ¿ Ì›· ÌfiÓÔ
ÏÂ˘Ú¿ ·˘Ù‹˜ Ù˘ ‰È·‰Èηۛ·˜, Â›Ó·È È‰È·›ÙÂÚ· ÛË-
Ì·ÓÙÈ΋ ÏfiÁˆ ·ÊÂÓfi˜ Ù˘ Û·ÓÈfiÙËÙ·˜ ÙˆÓ ‰È·ı¤ÛÈ-
ÌˆÓ ÔÈÎÔÓÔÌÈÎÒÓ fiÚˆÓ Î·È ·ÊÂÙ¤ÚÔ˘ ÙˆÓ ·˘Í·Ófi-
ÌÂÓˆÓ ˘ÁÂÈÔÓÔÌÈÎÒÓ ·Ó·ÁÎÒÓ.
øÛÙfiÛÔ, ÔÈ ÌÂϤÙ˜ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘
‰ÂÓ ·ÔÙÂÏÔ‡Ó ÙÔ ÌÔÓ·‰ÈÎfi ÎÚÈÙ‹ÚÈÔ Ï‹„˘ ·ÔÊ¿-
ÛˆÓ. ∞˘Ùfi Á›ÓÂÙ·È ÈÔ Î·Ù·ÓÔËÙfi ÛÙËÓ ÂÚ›ÙˆÛË
ÙˆÓ Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ. ∞Ó Î·È ·fi ÔÈÎÔÓÔÌÈ΋˜ Ï¢-
Ú¿˜ ÔÈ Û˘ÁÎÂÎÚÈ̤Ó˜ ·ÚÂÌ‚¿ÛÂȘ ‰ÂÓ ‹Ù·Ó ¿ÓÙÔ-
Ù ÔÈ Ï¤ÔÓ ·Ô‰ÔÙÈΤ˜, ·fi È·ÙÚÈ΋˜ ·fi„ˆ˜ ‹Ù·Ó
ȉȷ›ÙÂÚ· ·ÔÙÂÏÂÛÌ·ÙÈΤ˜ Î·È ¤ÙÛÈ, ÌÔÚÔ‡Û·Ó Ó·
ηıËÛ˘¯¿ÛÔ˘Ó ¤Ó· ÌÂÁ¿ÏÔ ÙÌ‹Ì· ÙÔ˘ ÏËı˘ÛÌÔ‡
Ô˘ ·ÓËÛ˘¯Ô‡Û ÁÈ· ·˘Ù¿ Ù· ÏÔÈÌÒ‰Ë ÓÔÛ‹Ì·Ù·.
µÂ‚·›ˆ˜, Ù· ·ÔÙÂϤÛÌ·Ù· ÙˆÓ ÔÈÎÔÓÔÌÈÎÒÓ
·ÍÈÔÏÔÁ‹ÛÂˆÓ ‰ÂÓ Ì¤ÓÔ˘Ó ·ÓÂÎÌÂÙ¿ÏÏÂ˘Ù·. ∞ÓÙ›ıÂ-
Ù· Û˘Ì‚¿ÏÏÔ˘Ó ÛÙËÓ ÂÈÏÔÁ‹ Ù˘ ·Ô‰ÔÙÈÎfiÙÂÚ˘
ÛÙÚ·ÙËÁÈ΋˜ ·ÓÔÛÔÔ›ËÛ˘ Î·È ÛÙÔÓ Û¯Â‰È·ÛÌfi ÙˆÓ
ÈÔ ·ÔÙÂÏÂÛÌ·ÙÈÎÒÓ ·ÚÂÌ‚¿ÛˆÓ.
∆· ‚·ÛÈο ÂÚˆÙ‹Ì·Ù· ÛÙ· ÔÔ›· ÔÈ ‰È·ÌÔÚʈ٤˜
Ù˘ ÔÏÈÙÈ΋˜ ˘Á›·˜ ηÏÔ‡ÓÙ·È Ó· ··ÓÙ‹ÛÔ˘Ó
ÚÈÓ Ï¿‚Ô˘Ó ÔÔÈ·‰‹ÔÙ ·fiÊ·ÛË Â›Ó·È (41):
1. √È ÛÙÚ·ÙËÁÈΤ˜ ·ÓÔÛÔÔ›ËÛ˘ ı· ÌÂÈÒÛÔ˘Ó
ÙËÓ Â›ÙˆÛË Ù˘ ÓfiÛÔ˘;
2. ¶ÔÈÔ Â›Ó·È ÙÔ ·Ó·ÌÂÓfiÌÂÓÔ fiÊÂÏÔ˜ ÁÈ· ÙËÓ
˘Á›·;
3. ™Â fiÛÔ ¯ÚfiÓÔ ı· Á›ÓÔ˘Ó ÂÌÊ·Ó‹ ·˘Ù¿ Ù·
ÔʤÏË;
4. ¶fiÛÔ ÎÔÛÙ›˙ÂÈ Ë ÛÙÚ·ÙËÁÈ΋ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ηÈ
ÔÈÔ ÙÔ ÎfiÛÙÔ˜ Ô˘ ·ÔÙÚ¤ÂÙ·È;
5. ∆· ·ÔÙÂϤÛÌ·Ù· ·Ú·Ì¤ÓÔ˘Ó ›‰È·, ·Ó ·ÏÏ¿-
ÍÔ˘Ó Î¿ÔȘ ·fi ÙȘ ·Ú·Ì¤ÙÚÔ˘˜;
6. ¶ÔÈÔ˜ Â›Ó·È Ô ·Ô‰ÂÎÙfi˜ ‰Â›ÎÙ˘ ÎfiÛÙÔ˘˜-
·ÔÙÂϤÛÌ·ÙÔ˜ ÁÈ· Ù· ÚÔÁÚ¿ÌÌ·Ù· ÂÌ‚ÔÏÈ·ÛÌÔ‡;
√˘ÛÈ·ÛÙÈο ÔÈ ˘Â‡ı˘ÓÔÈ Ï‹„˘ ·ÔÊ¿ÛˆÓ
Ú¤ÂÈ Ó· ÛÙ·ıÌ›ÛÔ˘Ó Î·È Ó· Û˘Ì‚È‚¿ÛÔ˘Ó ÙÔ˘˜ ÂÈ-
‰ËÌÈÔÏÔÁÈÎÔ‡˜, ÔÈÎÔÓÔÌÈÎÔ‡˜, ÎÔÈÓˆÓÈÎÔ‡˜ Î·È Ô-
ÏÈÙÈÎÔ‡˜ ·Ú¿ÁÔÓÙ˜ ÒÛÙ ӷ Ï¿‚Ô˘Ó ÙËÓ ÈÔ ·Ô-
ÙÂÏÂÛÌ·ÙÈ΋, ·Ô‰ÔÙÈ΋ Î·È ÎÔÈÓˆÓÈο ·Ô‰ÂÎÙ‹
·fiÊ·ÛË.
∂˘¯·ÚÈÛٛ˜
∂˘¯·ÚÈÛÙԇ̠Ôχ ÁÈ· ÙËÓ ÔχÙÈÌË Û˘Ì‚ÔÏ‹ ÙÔ˘ ÛÙËÓ
·Ó·˙‹ÙËÛË Ù˘ ‚È‚ÏÈÔÁÚ·Ê›·˜ -ÂȉÈο fiÛÔÓ ·ÊÔÚ¿ ÛÙÔ ÂÌ‚fi-
ÏÈÔ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜- ÙÔÓ Î. ∫ˆÙÛfiÔ˘ÏÔ ¡›ÎÔ, Health
Economics Manager ÛÙËÓ ÂÙ·ÈÚ›· GlaxoSmithCline.
µÈ‚ÏÈÔÁÚ·Ê›·
1. Jefferson T. Do vaccines make best use of available re-
sources? (in other words are they cost-effective?). Vaccine
1999;17:S69-S73.
2. Van Damme P, Beutels P. Economic evaluation of vaccina-
tion. Pharmacoeconomics 1996;9:8-15.
3. Ess SM, Szucs TD. Economic evaluation of immunization
strategies. Clin Infect Dis 2002;35:294-297.
4. Spier R, Jefferson TO, Demicheli V. An editorial policy
statement: Submission of economic evaluation of vaccines.
[Editorial]. Vaccine 2002;20:1693-1695.
5. Kimman TG, Boot HJ, Berbers GA, Vermeer-de Bondt PE,
Ardine de Wit G, de Melker HE. Developing a vaccination
evaluation model to support evidence-based decision mak-
ing on national immunization programs. Vaccine 2006;24:
4769-4778.
6. Drummond MF, O’ Brien BJ, Stoddart GL, Torrance G.
ª¤ıÔ‰ÔÈ ÔÈÎÔÓÔÌÈ΋˜ ·ÍÈÔÏfiÁËÛ˘ ÙˆÓ ÚÔÁÚ·ÌÌ¿ÙˆÓ
˘Á›·˜. ∞ı‹Ó·: ∂ΉfiÛÂȘ ∫ÚÈÙÈ΋. 2002.
7. Szucs TD. Health economic research on vaccinations and
immunisation practices - an introductory primer. Vaccine
2005;23:2095-2103.
8. Chabot I, Goetghebeur MM, Gregoire JP. The societal val-
ue of universal childhood vaccination. Vaccine 2004;22:
1992-2005.
9. Szucs ∆. Cost-benefits of vaccination programmes. Vac-
cine 2000;18:S49-S51.
10. ¶···Ó·ÁÈÒÙÔ˘ π, ∫˘ÚÈ·˙ÔÔ‡ÏÔ˘-¢·Ï·˝Ó· µ. π·ÙÚÈ΋
ÌÈÎÚÔ‚ÈÔÏÔÁ›· Î·È ÈÔÏÔÁ›·. £ÂÛÛ·ÏÔÓ›ÎË: ∂ΉfiÛÂȘ
University Studio Press. 2001.
11. Wyeth Hellas [Webpage, Internet]. £Âڷ¢ÙÈ΋ ÂÓfiÙËÙ·:
ªËÓÈÁÁ›Ùȉ·. http://www.wyeth.gr/th_areas/th_area_main.
asp?th_ar_id=32
12. World Health Organization [Webpage, Internet]. Menin-
gitis. http://www.who.int/topics/meningitis/en
13. ∂ıÓÈÎfi˜ √ÚÁ·ÓÈÛÌfi˜ º·Ú̿ΈÓ, ∂√º [Webpage, Inter-
net]. http://www.eof.gr
14. Trotter CL, Edmunds WJ. Modelling cost-effectiveness of
meningococcal serogroup C conjugate vaccination cam-
paign in England and Wales. BMJ 2002;324:809.
15. Ruedin HJ, Ess S, Zimmermann HP, Szucks T. Invasive
meningococcal and pneumococcal disease in Switzerland:
cost-utility analysis of different vaccine strategies. Vaccine
2003;21:4145-4152.
16. Welte R, Van den Dobbelsteen G, Bos JM, de Melker H,
van Alphen L, Spanjaard L, et al, Economic evaluation of
meningococcal serogroup C conjugate vaccination pro-
grammes in The Netherlands and its impact on decision-
making. Vaccine 2004;23:470-479.
155√ÈÎÔÓÔÌÈ΋ ·ÍÈÔÏfiÁËÛË Ó¤ˆÓ ÂÌ‚ÔÏ›ˆÓ
¶·È‰È·ÙÚÈ΋ 2008;71:148-156
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·155

17. De Wals P, Nguyen VH, Erickson LJ, Guay M, Drapeau J,St-Laurent J. Cost-effectiveness of immunization strategiesfor the control of serogroup C meningococcal disease. Vac-cine 2004;22:1233-1240.
18. Beutels P, Thiry N, Van Damme P. Convincing or confus-ing? Economic evaluations of childhood pneumococcalconjugate vaccination - a review (2002-2006). Vaccine 2007;25:1355-1367.
19. Zissis NP, Syriopoulou V, Kafetzis D, Daikos GL, Tsil-imingaki A, Galanakis E, et al. Serotype distribution andantimicrobial susceptibility of Streptococcus pneumoniaecausing invasive infections and acute otitis media in chil-dren. Eur J Pediatr 2004;163:364-368.
20. Black S, Lieu TA, Ray GT, Capra A, Shinefield HR. Assess-ing costs and cost effectiveness of pneumococcal diseaseand vaccination within Kaiser Permanente. Vaccine 2000;19:S83-S86.
21. De Wals P, Petit G, Erickson LJ, Guay M, Tam T, Law B, etal. Benefits and costs of immunization of children withpneumococcal conjugate vaccine in Canada. Vaccine2003;21:3757-3764.
22. Bos JM, Rumke H, Welte R, Postma MJ. Epidemiologicimpact and cost-effectiveness of universal infant vaccina-tion with a 7-valent conjugated pneumococcal vaccine inthe Netherlands. Clin Ther 2003;25:2614-2630.
23. Claes C, Schulenburg JM Graf von der. Cost effectivenessof pneumococcal vaccination for infants and children withthe conjugate vaccine PnC-7 in Germany. Pharmacoeco-nomics 2003;21:587-600.
24. Asensi F, De Jose M, Lorente M, Moraga F, Ciuryla V,Arikian S, et al. A pharmacoeconomic evaluation of seven-valent pneumococcal conjugate vaccine in Spain. ValueHealth 2004;7:36-51.
25. Butler JR, McIntyre P, MacIntyre CR, Gilmour R, HowarthAL, Sander B. The Cost- Effectiveness of pneumococcal con-jugate vaccination in Australia. Vaccine 2004;22:1138-1149.
26. McIntosh ED, Conway P, Willingham J, Hollingsworth R,Lloyd A. Pneumococcal pneumonia in the UK - how herdimmunity affects the cost-effectiveness of 7-valent pneumo-coccal conjugate vaccine (PCV). Vaccine 2005;23:1739-1745.
27. Marchetti M, Colombo GL. Cost-effectiveness of universalpneumococcal vaccination for infants in Italy. Vaccine2005;23:4565-4576.
28. Wisloff T, Abrahamsen T, Bergsaker MA, Lovoll O, MollerP, Pedersen MK, et al. Cost effectiveness of adding 7-valentpneumococcal conjugate (PCV-7) vaccine to the Norwe-gian childhood vaccination program. Vaccine 2006;24:5690-5699.
29. Ray GT, Whitney CG, Fireman BH, Ciuryla V, Black SB.Cost-effectiveness of pneumococcal conjugate vaccine: evi-dence from the first 5 years of use in the United States incor-porating herd effects. Pediatr Infect Dis J 2006;25:494-501.
30. GlaxoSmithCline [Webpage, Internet]. Varilrix http://emc.medicines.org.uk/emc/assets/c/html/displaydoc.asp?docu-mentid=9453
31. Scuffham PA, Lowin AV, Burgess MA. The cost-effective-ness of varicella vaccine programs for Australia. Vaccine1999;18:407-415.
32. Brisson M, Edmunds WJ. The cost-effectiveness of varicel-la vaccination in Canada. Vaccine 2002;20:1113-1125.
33. Brisson M, Edmunds WJ. Varicella vaccination in Englandand Wales: cost-utility analysis. Arch Dis Child 2003;88:862-869.
34. Coudeville L, Paree F, Lebrun T, Sailly J. The value of vari-cella vaccination in healthy children: cost-benefit analysisof the situation in France. Vaccine 1999;17:142-151.
35. Lenne X, Diez Domingo J, Gil A, Ridao M, Lluch J, Der-vaux B. Economic evaluation of varicella vaccination inSpain: results from a dynamic model. Vaccine 2006;24:6980-6989.
36. Trotter CL, Edmunds WJ. Reassessing the cost-effective-ness of meningococcal serogroup C conjugate (MCC) vac-cines using a transmission dynamic model. Med DecisMaking 2006;26:38-47.
37. McIntosh ED, Conway P, Willingham J, Hollingsworth R,Lloyd A. Pneumococcal pneumonia in the UK - how herdimmunity affects the cost-effectiveness of 7-valent pneu-mococcal conjugate vaccine (PCV). Vaccine 2005;23:1739-1745.
38. Diez Domingo J, Ridao M, Latour J, Ballester A, Morant A.A cost benefit analysis of routine varicella vaccination inSpain. Vaccine 1999;17:1306-1311.
39. Nguyen HQ, Jumaan AO, Seward JF. Decline in mortalitydue to varicella after implementation of varicella vaccina-tion in the United States. N Engl J Med 2005;352:450-458.
40. Rentier B, Gershon AA; European Working Group on Vari-cella. Consensus: varicella vaccination of healthy children - achallenge for Europe. Pediatr Infect Dis J 2004;23: 379-389.
41. Welte R, Trotter CL, Edmunds WJ, Postma MJ, Beutels P.The role of economic evaluation in vaccine decision mak-ing: focus on meningococcal group C conjugate vaccine.Pharmacoeconomics 2005;23:855-874.
156 µ. ∆ÛÈ¿ÓÙÔ˘ Î·È Û˘Ó.
Paediatriki 2008;71:148-156
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·156

157¶ƒ∞∫∆π∫√ £∂ª∞ PRACTICAL ISSUE
¶·È‰È·ÙÚÈ΋ 2008;71:157-161
¢È·ÙÚÔÊ‹ ·È‰ÈÒÓ Î·È ÂÊ‹‚ˆÓ ÁÈ· ÚÔ·ÁˆÁ‹ Ù˘ ˘Á›·˜ ηÈ
Ù˘ ·Ó¿Ù˘Í˘ Î·È ÚfiÏË„Ë ÙˆÓ ¯ÚfiÓÈˆÓ ÓÔÛËÌ¿ÙˆÓ
∞. ∫·Ê¿ÙÔ˜
¶ÂÚ›ÏË„Ë: ∏ ÂȉËÌÈ΋ ¤Í·ÚÛË Ù˘ ·È‰È΋˜ ·¯˘Û·ÚΛ·˜ ·fi ÙË ‰ÂηÂÙ›· ÙÔ˘ 1980 ̤¯ÚÈ Û‹ÌÂÚ· η-ıÈÛÙ¿ ·Ó·Áη›· ÙËÓ ÂÓË̤ڈÛË ÙˆÓ ·È‰È¿ÙÚˆÓ Î·È ÙˆÓ ÁÔÓÈÒÓ ÁÈ· ÙË ÛˆÛÙ‹ ‰È·ÙÚÔÊ‹ ÙˆÓ ·È‰ÈÒÓ. ∏ÂÓË̤ڈÛË ·˘Ù‹ ı· ‚ÔËı‹ÛÂÈ ÛÙËÓ ·ÔÊ˘Á‹ ÙÚÔÊ›ÌˆÓ ˘„ËÏ‹˜ ÂÓÂÚÁÂȷ΋˜ ˘ÎÓfiÙËÙ·˜, ÁÈ· ·Ú¿-‰ÂÈÁÌ· ·Ù¿Ù˜ ÙÛȘ Ì 530 kcal/100 ÁÚ·Ì., ÌÈÛÎfiÙ· Ì ÛÔÎÔÏ¿Ù· Ì 524 kcal/100 ÁÚ·Ì. Î·È ¯·ÌËÏ‹˜ÂÚÈÂÎÙÈÎfiÙËÙ·˜ Û ıÚÂÙÈο Û˘ÛÙ·ÙÈο. ∆· ÙÚfiÊÈÌ· ·˘Ù¿ ÚÔÛʤÚÔ˘Ó ÂÏ¿¯ÈÛÙ· ıÚÂÙÈο Û˘ÛÙ·ÙÈÎ¿Ô˘ Â›Ó·È ··Ú·›ÙËÙ· ÁÈ· ÙËÓ ·Ó¿Ù˘ÍË Î·È ÙËÓ ÚÔ·ÁˆÁ‹ Ù˘ ˘Á›·˜. ∆· ··Ú·›ÙËÙ· ıÚÂÙÈο Û˘ÛÙ·-ÙÈο ÂÍ·ÛÊ·Ï›˙ÔÓÙ·È fiÙ·Ó Ï·Ì‚¿ÓÔÓÙ·È ÔÈ Û˘ÓÈÛÙÒÌÂÓ˜ ÌÂÚ›‰Â˜ ·fi ηıÂÌÈ¿ ·fi ÙȘ 5 ηÙËÁÔڛ˜ ÙÚÔ-Ê›ÌˆÓ Î·È Î·Ù·Ó¤ÌÔÓÙ·È Û 3 ·ÚÈ· Î·È 2 ÌÈÎÚfiÙÂÚ· ÂӉȿÌÂÛ· Á‡̷ٷ. ∞·ÈÙÂ›Ù·È È‰È·›ÙÂÚË ÚÔÛ¿-ıÂÈ· ÂΠ̤ÚÔ˘˜ ÙˆÓ ÁÔÓÈÒÓ, ÒÛÙ ӷ ¤¯Ô˘Ó Ù· ·È‰È¿ 2-3 Á‡̷ٷ ÙËÓ Â‚‰ÔÌ¿‰· Ì ÌÈÎÚ¿ ÏÈ·Ú¿ „¿-ÚÈ·, 2-8 ÌÂÚ›‰Â˜ Ï·¯·ÓÈÎÒÓ ËÌÂÚËÛ›ˆ˜, ·Ó¿ÏÔÁ· Ì ÙËÓ ËÏÈΛ·, 2-5 ÊÚÔ‡Ù· ÙËÓ Ë̤ڷ, 2-3 ÌÂÚ›‰Â˜ Á·-Ï·ÎÙÔÎÔÌÈÎÒÓ, ÂÏ¿¯ÈÛÙÔ ÎfiÎÎÈÓÔ ÎÚ¤·˜ Î·È Î·ıfiÏÔ˘ ÂÂÍÂÚÁ·Ṳ̂ÓÔ ÎÚ¤·˜ (.¯. ˙·ÌfiÓ). ∆Ô ·Ú¿‰ÂÈÁ-Ì· ÙˆÓ ÁÔÓÈÒÓ ¯ˆÚ›˜ ÏfiÁÈ· Â›Ó·È Ô Î·Ï‡ÙÂÚÔ˜ ÙÚfiÔ˜ ‰È‰·Ûηϛ·˜ (ÛÙËÓ ¿ÛÎËÛË Î·È ÛÙÔ Ê·ÁËÙfi). ∏‰È·ÙÚÔÊ‹ ÙˆÓ ·È‰ÈÒÓ, ‚·ÛÈṲ̂ÓË ÛÙÔÓ ·Ú·‰ÔÛÈ·Îfi ÙÚfiÔ ‰È·ÙÚÔÊ‹˜ ÙˆÓ ∂ÏÏ‹ÓˆÓ Ì·˙› Ì ÙÔ˘Ï¿¯È-ÛÙÔÓ 2-3 ÒÚ˜ ¤ÓÙÔÓ˘ ۈ̷ÙÈ΋˜ ¿ÛÎËÛ˘ ηıËÌÂÚÈÓ¿, ı· ÂÍ·ÛÊ·Ï›ÛÂÈ ¿ÚÈÛÙË ·Ó¿Ù˘ÍË Î·È ÚfiÏË„ËÙˆÓ ¯ÚfiÓÈˆÓ ÓÔÛËÌ¿ÙˆÓ.
§¤ÍÂȘ ÎÏÂȉȿ: ¢È·ÙÚÔÊ‹ ·È‰ÈÒÓ, ·Ó¿Ù˘ÍË, ·¯˘Û·ÚΛ·, ¯ÚfiÓÈ· ÓÔÛ‹Ì·Ù·, ıÚÂÙÈο Û˘ÛÙ·ÙÈο, ۈ̷ÙÈ΋
¿ÛÎËÛË.
Childhood and adolescent nutrition for promoting health and
growth and preventing chronic diseases
A. Kafatos
Abstract: Paediatric obesity has been increasing since the 1980s in an epidemic mode. Due to this fact,it has become necessary to provide information for paediatricians and parents about the dietappropriate for growth and avoidance of obesity of children. The primary target should be theelimination of foods of high energy density and low nutrient content (e.g., chips, chocolate biscuits)from the diet of children, with emphasis on the traditional Greek diet. The intake of essential nutrientsis ensured when children consume the recommended portions from each of the 5 categories of foods,and when these portions are distributed between 3 main and 2 smaller intermediate meals on a dailybasis. Particular effort is required on the part of the parents to ensure that children consume 2-3portions of small oily fish per week, 2-8 portions of vegetables daily, depending on age, and 2-5portions of fruits and 2-3 portions of dairy products on a daily basis. The best way of teaching childrenabout diet and physical activity is for parents to set an example by practising these habits themselves athome. The adoption of the traditional Greek diet, low in saturated fat and high in olive oil, vegetables,fruit and legumes, with at least 2-3 hours of daily intense physical activity will ensure excellent growthand development of the children and help in the prevention of chronic diseases.
Key words: Childhood nutrition, growth, obesity, chronic diseases, nutrients, physical activity.
∫ÏÈÓÈ΋ ¶ÚÔÏËÙÈ΋˜π·ÙÚÈ΋˜ Î·È ¢È·ÙÚÔÊ‹˜, ∆Ì‹Ì· π·ÙÚÈ΋˜, ¶·ÓÂÈÛÙ‹ÌÈÔ ∫Ú‹Ù˘
AÏÏËÏÔÁÚ·Ê›·:
∞ÓÙÒÓ˘ ∫·Ê¿ÙÔ˜[email protected]∫ÏÈÓÈ΋ ¶ÚÔÏËÙÈ΋˜π·ÙÚÈ΋˜ Î·È ¢È·ÙÚÔÊ‹˜, ∆Ì‹Ì· π·ÙÚÈ΋˜,¶·ÓÂÈÛÙ‹ÌÈÔ ∫Ú‹Ù˘
Division of PreventiveMedicine and Nutrition, Faculty of Medicine, University of Crete
Correspondence:
Antonis [email protected] of PreventiveMedicine and Nutrition, Faculty of Medicine, University of Crete
∏ Ê˘ÛÈÔÏÔÁÈ΋ ·Ó¿Ù˘ÍË ÙÔ˘ ·È‰ÈÔ‡ ÚÔ-¸Ôı¤ÙÂÈ ÙË Ï‹„Ë ÂÚ›Ô˘ 50 ··Ú·›ÙËÙˆÓıÚÂÙÈÎÒÓ Û˘ÛÙ·ÙÈÎÒÓ ÛÙȘ Û˘ÓÈÛÙÒÌÂÓ˜ ËÌÂ-Ú‹ÛȘ ÔÛfiÙËÙ˜ ·fi ÙȘ ÙÚÔʤ˜ ÁÈ· ÙË Û‡ÓıÂ-ÛË ÙˆÓ ‰È·ÊfiÚˆÓ ÈÛÙÒÓ. ∞Ó·Ú΋˜ Ï‹„Ë ÂÓfi˜‹ ÂÚÈÛÛfiÙÂÚˆÓ ıÚÂÙÈÎÒÓ Û˘ÛÙ·ÙÈÎÒÓ ‹˘ÂÚ‚ÔÏÈ΋ Ï‹„Ë ¿ÏÏˆÓ ÌÔÚ› Ó· ÚÔηϤ-ÛÂÈ ÛÔ‚·Ú¤˜ ‰È·Ù·Ú·¯¤˜ ÛÙË ıÚ¤„Ë Î·È ÙËÓ
·Ó¿Ù˘ÍË ÙÔ˘ ·È‰ÈÔ‡. °È’ ·˘Ùfi, οı ·È‰È·-ÙÚÈ΋ ÂͤٷÛË Ú¤ÂÈ Ó· ÂÚÈÏ·Ì‚¿ÓÂÈ ÂÎÙ›ÌË-ÛË Ù˘ ıÚ¤„˘ ÙÔ˘ ·È‰ÈÔ‡. ∏ ÂÎÙ›ÌËÛË ·˘Ù‹ÂÚÈÏ·Ì‚¿ÓÂÈ (1):
1. ÎÏÈÓÈ΋ ÂͤٷÛË ÁÈ· ÛËÌ›· ·Ó·ÚÎÔ‡˜ıÚ¤„˘ ‹ ÙÔÍÈ΋ ›‰Ú·ÛË ·fi ˘ÂÚ‚ÔÏÈ΋ϋ„Ë ıÚÂÙÈÎÒÓ Û˘ÛÙ·ÙÈÎÒÓ,
2. ۈ̷ÙÔÌÂÙÚÈΤ˜ ÌÂÙÚ‹ÛÂȘ (‚¿ÚÔ˜, Ì‹ÎÔ˜
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·157

158 ∞. ∫·Ê¿ÙÔ˜
Paediatriki 2008;71:157-161
‹ ·Ó¿ÛÙËÌ·, ÂÚ›ÌÂÙÚÔ˜ ÎÂÊ·Ï‹˜, ÂÚ›ÌÂÙÚÔ˜ ̤-
Û˘, ÏÂοÓË Î·È ‚Ú·¯›ÔÓ· Î·È ÔÚÈṲ̂Ó˜ ‰ÂÚÌ·ÙÈΤ˜
Ù˘¯¤˜) Î·È Û‡ÁÎÚÈÛË Ì ηٿÏÏËϘ η̇Ϙ
·Ó¿Ù˘Í˘,
3. ‰È·ÈÙËÙÈÎfi ÈÛÙÔÚÈÎfi Ô˘ ÂÚÈÏ·Ì‚¿ÓÂÈ ÙË Û˘-
¯ÓfiÙËÙ· Ï‹„˘ ÙÚÔÊ›ÌˆÓ ·fi οı ηÙËÁÔÚ›· ̤-
Û· Û ÌÈ· ‚‰ÔÌ¿‰· (¤ÓÙ ηÙËÁÔڛ˜ ÙÚÔʛ̈Ó,
ηıÒ˜ Î·È ·Ó·„˘ÎÙÈο, ÁÏ˘Î¿, snacks, Ê·ÁËÙ¿ ·fi
Ù·¯˘ÂÛÙÈ·ÙfiÚÈ·), ȉȷÈÙÂÚfiÙËÙ˜ ÛÙË ‰È·ÙÚÔÊ‹,
.¯. Ê˘ÙÔÊ·Á›· ‹ ·fiÏ˘ÙË Ê˘ÙÔÊ·Á›·. ∆Ô ‰È·ÈÙÔ-
ÏfiÁÈÔ ÙÔ˘ ÙÂÏÂ˘Ù·›Ô˘ ÂÈÎÔÛÈÙÂÙÚ·ÒÚÔ˘ ‰›ÓÂÈ ÙȘ
ÔÛfiÙËÙ˜ Ê·ÁËÙÔ‡ Î·È ÌÔÚ› Ó· ·Ó·Ï˘ı› ÛÂ
ıÚÂÙÈο Û˘ÛÙ·ÙÈο Û‡Ìʈӷ Ì ËÏÂÎÙÚÔÓÈ΋ ‚¿-
ÛË ÙÚÔʛ̈Ó,
4. ÂÎÙ›ÌËÛË Ê˘ÛÈ΋˜ ‰Ú·ÛÙËÚÈfiÙËÙ·˜ (›‰Ô˜, Û˘-
¯ÓfiÙËÙ· Î·È ‰È¿ÚÎÂÈ· ۈ̷ÙÈ΋˜ ¿ÛÎËÛ˘ ‹ ·‰Ú¿-
ÓÂÈ·˜, Û˘¯ÓfiÙËÙ· Î·È ‰È¿ÚÎÂÈ· ηıÈÛÙÈ΋˜ ÂÚÁ·Û›·˜
ÛÙÔ˘˜ ˘ÔÏÔÁÈÛÙ¤˜ ‹ ÙËÏÂfiÚ·ÛË, Î.Ù.Ï.), ‰È¿ÚÎÂÈ·
‡ÓÔ˘, ηıÒ˜ Î·È Ì¤ÙÚËÛË Ù˘ ηډÈÔ·Ó·Ó¢ÛÙÈ-
΋˜ ·ÓÙÔ¯‹˜,
5. ‚ÈÔ¯ËÌÈ΋ ÂÎÙ›ÌËÛË ıÚ¤„˘ ÁÈ· ÎÏÈÓÈΤ˜ ηÈ
˘ÔÎÏÈÓÈΤ˜ ÌÔÚʤ˜ ·Ó·ÚÎÔ‡˜ ıÚ¤„˘ (.¯. ·ÈÌÔ-
ÛÊ·ÈÚ›ÓË, ·ÈÌÔÛÊ·ÈÚÈÓÈÎÔ› ‰Â›ÎÙ˜, ÊÂÚÚÈÙ›ÓË, Ê˘Ï-
ÏÈÎfi Ô͇ Î·È µ12, ηıÒ˜ Î·È ¿ÏϘ ‚Èٷ̛Ә Î·È È¯ÓÔ-
ÛÙÔȯ›· ÛÙÔ ·›Ì·),
6. ·ÓÔÛÔ‚ÈÔÏÔÁÈ΋ ÂÎÙ›ÌËÛË Ù˘ ¯˘ÌÈ΋˜ ηÈ
΢ÙÙ·ÚÈ΋˜ ·ÓÔÛ›·˜ ÙÔ˘ ·ÛıÂÓÔ‡˜ Ô˘ Û¯ÂÙ›˙ÂÙ·È
ÛÙÂÓ¿ Ì ÙË ıÚ¤„Ë ÙÔ˘,
7. ·ÂÈÎÔÓÈÛÙÈΤ˜ ̤ıÔ‰ÔÈ, fiˆ˜ Ë ·ÍÔÓÈ΋ ÙÔ-
ÌÔÁÚ·Ê›·, Ë Ì·ÁÓËÙÈ΋ ÙÔÌÔÁÚ·Ê›· Î·È ÙÔ DEXA,
ηıÔÚ›˙Ô˘Ó Ì ·ÎÚ›‚ÂÈ· ÙË Û‡ÓıÂÛË ÙÔ˘ ÛÒÌ·ÙÔ˜ ÛÂ
Ì˘˚΋ Ì¿˙·, ÔÏÈÎfi ϛԘ Î·È ÔÛÙÈ΋ Ì¿˙·. ¶Ï¤ÔÓ Â‡-
¯ÚËÛÙË Î·È ÏÈÁfiÙÂÚÔ ‰··ÓËÚ‹ Â›Ó·È Ë ‚ÈÔËÏÂÎÙÚÈ΋
·ÁˆÁÈÌfiÙËÙ· ÁÈ· ÙË Û‡ÓıÂÛË ÙÔ˘ ÛÒÌ·ÙÔ˜.
™ÙÔ ·ÚfiÓ ¿ÚıÚÔ ı· ÂÚÈÔÚÈÛÙԇ̠ÛÙȘ Û˘ÛÙ¿-
ÛÂȘ Û ÙÚfiÊÈÌ· Î·È ıÚÂÙÈο Û˘ÛÙ·ÙÈο, ÒÛÙ ӷ
ÂÈÙ‡¯ÂÈ ÙÔ ·È‰› ¿ÚÈÛÙË ÛˆÌ·ÙÈ΋ Î·È „˘¯ÔÎÈÓËÙÈ-
΋ ·Ó¿Ù˘ÍË.
√ ¶›Ó·Î·˜ 1 ‰›ÓÂÈ ÙȘ ÂÓÂÚÁÂȷΤ˜ ·Ó¿ÁΘ ÙˆÓ
·È‰ÈÒÓ Î·Ù¿ ËÏÈΛ· Î·È Ê‡ÏÔ, ηıÒ˜ Î·È ÙȘ Û˘ÓÈ-
ÛÙÒÌÂÓ˜ ÔÛfiÙËÙ˜ ÙˆÓ ‚·ÛÈÎÒÓ ıÚÂÙÈÎÒÓ Û˘-
ÛÙ·ÙÈÎÒÓ (2-5).
°È· ¤Ó· ·È‰› 5 ÂÙÒÓ, ÙÔ 50% ÂÚ›Ô˘ Ù˘ ÂÓ¤Ú-
ÁÂÈ·˜ Ô˘ Ï·Ì‚¿ÓÂÙ·È Î·ıËÌÂÚÈÓ¿ ηχÙÂÈ ÙȘ ·Ó¿-
ÁΘ ÙÔ˘ ‚·ÛÈÎÔ‡ ÌÂÙ·‚ÔÏÈÛÌÔ‡, ÙÔ 5% Íԉ‡ÂÙ·È
ÛÙËÓ ÂȉÈ΋ ‰˘Ó·ÌÈ΋ ÂÓ¤ÚÁÂÈ· Ù˘ ·ÔÚÚfiÊËÛ˘,
ȉȷ›ÙÂÚ· ÙˆÓ ÚˆÙÂ˚ÓÒÓ, Î·È ÙȘ ·Ó¿ÁΘ ÁÈ· ÙÔ ÌÂ-
Ù·‚ÔÏÈÛÌfi ÙÔ˘˜. ∆Ô 25% ÂÚ›Ô˘ Ù˘ ÂÓ¤ÚÁÂÈ·˜ ÍÔ-
‰Â‡ÂÙ·È ÁÈ· ̤ÙÚÈ· Ê˘ÛÈ΋ ‰Ú·ÛÙËÚÈfiÙËÙ·, ÙÔ 12%
ÁÈ· ÙËÓ ·Ó¿Ù˘ÍË ÙˆÓ ÈÛÙÒÓ Î·È ÂÚ›Ô˘ 7% ̄ ¿ÓÂÙ·È
ÛÙ· ÎfiÚ·Ó· (6).
°È· ÙËÓ ÚÔ·ÁˆÁ‹ Ù˘ ˘Á›·˜ Î·È Ù˘ ·Ó¿Ù˘Í˘
ÙÔ˘ ·È‰ÈÔ‡ ··Ú·›ÙËÙË ÚÔ¸fiıÂÛË Â›Ó·È Ë ¤ÁÎ˘Ô˜
Ó· ¤¯ÂÈ ¿ÚÈÛÙË ‰È·ÙÚÔÊ‹ Ì ·ÔÊ˘Á‹ ÙˆÓ ÙÔÍÈÎÒÓ
Ô˘ÛÈÒÓ, fiˆ˜ ÙÔ ¿ÌÂÛÔ Î·È ¤ÌÌÂÛÔ Î¿ÓÈÛÌ·, Î·È ÙˆÓ
ÔÈÓÔÓÂ˘Ì·Ùˆ‰ÒÓ ÔÙÒÓ (7). ™ÙÔ ÙÂÏÂ˘Ù·›Ô ÙÚ›ÌËÓÔ
Ù˘ ·ËÛ˘, Ë ¤ÁÎ˘Ô˜ Ú¤ÂÈ Ó· ÚÔÂÙÔÈÌ·Ûı› ÁÈ·
ÂÈÙ˘¯‹ ıËÏ·ÛÌfi. ∂ÈÙ˘¯‹˜ ıËÏ·ÛÌfi˜ ÛËÌ·›ÓÂÈ ·Ô-
ÎÏÂÈÛÙÈÎfi˜ ıËÏ·ÛÌfi˜ ÁÈ· 6 Ì‹Ó˜ Î·È Û˘Ó¤¯ÈÛË ÙÔ˘
ıËÏ·ÛÌÔ‡ ̤¯ÚÈ ÙÔ 12Ô Ì‹Ó· Ì ÚÔԉ¢ÙÈ΋ ÚÔ-
Ûı‹ÎË ¿ÏÏˆÓ ÙÚÔÊÒÓ. ∆Ô ÓÔÛËÏ¢ÙÈÎfi ÚÔÛˆÈÎfi
Î·È ÔÈ ÁÈ·ÙÚÔ› ÛÙ· Ì·ÈÂ˘Ù‹ÚÈ· ‰ÂÓ ı· Ú¤ÂÈ Ó· ÂÈ-
ÙÚ¤Ô˘Ó ÛÙÔ˘˜ ·ÓÙÈÚÔÛÒÔ˘˜ ÙˆÓ ·È‰ÈÎÒÓ ÙÚÔ-
ÊÒÓ Ó· ‰›ÓÔ˘Ó ‰ÒÚ· ÛÙȘ ÌËÙ¤Ú˜ Ô‡Ù ӷ ‰Ôı› ͤÓÔ
Á¿Ï· ÌÂ ÌÈÌÂÚfi ÌÂÙ¿ ÙÔÓ ÙÔÎÂÙfi. ∏ ¯ÔÚ‹ÁËÛË ÌÈ-
ÌÂÚÔ‡ ÚÈÓ ·fi ÙËÓ ¤Ó·ÚÍË ÙÔ˘ ıËÏ·ÛÌÔ‡ ·ÔÎÏ›-
ÂÈ ÙË ‰˘Ó·ÙfiÙËÙ· ÂÈÙ˘¯Ô‡˜ ıËÏ·ÛÌÔ‡. √ ·ÔÎÏÂÈ-
ÛÙÈÎfi˜ ıËÏ·ÛÌfi˜ ¤¯ÂÈ ÔÏÏ¿ ÏÂÔÓÂÎÙ‹Ì·Ù· ¤Ó·ÓÙÈ
ÙÔ˘ ·ÁÂÏ·‰ÈÓÔ‡ Á¿Ï·ÙÔ˜, ·ÏÏ¿ ΢ڛˆ˜ ÂÏ·ÙÙÒÓÂÈ ÙËÓ
Èı·ÓfiÙËÙ· ÌÂÏÏÔÓÙÈ΋˜ ·¯˘Û·ÚΛ·˜ Î·È fiÏˆÓ ÙˆÓ
Û˘ÓÔ‰ÒÓ ÚÔ‚ÏËÌ¿ÙˆÓ (˘ÂÚ¯ÔÏËÛÙÂÚÔÏ·ÈÌ›·˜,
˘¤ÚÙ·Û˘, ۷ί·ÚÒ‰Ô˘˜ ‰È·‚‹ÙË Ù‡Ô˘ 2 Î·È ·˘ÍË-
̤ÓÔ˘ ΛӉ˘ÓÔ˘ Û ÔÚÈṲ̂ÓÔ˘˜ ηÚΛÓÔ˘˜, Î.¿.).
ªÂÙ¿ ÙËÓ ËÏÈΛ· ÙˆÓ 6 ÌËÓÒÓ ÙÔ˘ ·ÔÎÏÂÈÛÙÈÎÔ‡
ıËÏ·ÛÌÔ‡ Ú¤ÂÈ Ó· ·Ú¯›ÛÂÈ ÚÔԉ¢ÙÈ΋ ÂÈÛ·ÁˆÁ‹
fiÏˆÓ ÙˆÓ ÙÚÔÊÒÓ ÛÙË ‰È·ÙÚÔÊ‹ ÙˆÓ ·È‰ÈÒÓ Î·È Û˘-
Ó¤¯ÈÛË ÙÔ˘ ıËÏ·ÛÌÔ‡ ̤¯ÚÈ ÙÔ 12Ô Ì‹Ó·.
∏ ηıËÌÂÚÈÓ‹ ‰È·ÙÚÔÊ‹ ÙÔ˘ ·È‰ÈÔ‡ ıˆÚ›ٷÈ
¿ÚÈÛÙË fiÙ·Ó ÂÚȤ¯ÂÈ ÙÚfiÊÈÌ· Î·È ·fi ÙȘ 5 ηÙËÁÔ-
ڛ˜ ÙˆÓ ÙÚÔÊ›ÌˆÓ Ô˘ Ê·›ÓÔÓÙ·È ÛÙÔÓ ¶›Ó·Î· 2 (8).
√È ··Ú·›ÙËÙ˜ ÌÂÚ›‰Â˜ Î·È ÙÔ Ì¤ÁÂıfi˜ ÙÔ˘˜ ÂÍ·ÚÙÒ-
ÓÙ·È ·fi ÙËÓ ËÏÈΛ· Î·È ·ÚÔ˘ÛÈ¿˙ÔÓÙ·È Û ·˘Ùfi ÙÔÓ
›Ó·Î·. ∏ ÂÈÏÔÁ‹ ÙˆÓ ··Ú·›ÙËÙˆÓ ÌÂÚ›‰ˆÓ ÁÈ· ο-
ı ËÏÈΛ· ·fi fiϘ ÙȘ ηÙËÁÔڛ˜ ÙÚÔÊ›ÌˆÓ Î·ıËÌÂ-
ÚÈÓ¿ ÂÍ·ÛÊ·Ï›˙ÂÈ ÙË Ï‹„Ë fiÏˆÓ ÙˆÓ ··Ú·›ÙËÙˆÓ
ıÚÂÙÈÎÒÓ Û˘ÛÙ·ÙÈÎÒÓ ÛÙȘ Û˘ÓÈÛÙÒÌÂÓ˜ ÔÛfiÙËÙ˜.
∆· ¯·Ú·ÎÙËÚÈÛÙÈο Ù˘ ¿ÚÈÛÙ˘ ‰È·ÙÚÔÊ‹˜ ÙÔ˘
·È‰ÈÔ‡ Î·È ÂÊ‹‚Ô˘ Â›Ó·È Ù· ·ÎfiÏÔ˘ı· (9):
1. ¶ÔÈÎÈÏ›· ÛÙË ‰È·ÙÚÔÊ‹ Ì ÂÈÏÔÁ‹ ÙÚÔʛ̈Ó
ηıËÌÂÚÈÓ¿ ·’ fiϘ ÙȘ 5 ηÙËÁÔڛ˜ Ô˘ ı· ηٷ-
Ó¤ÌÔÓÙ·È Û ÙÚ›· ·ÚÈ· Á‡̷ٷ Î·È 2-3 ÌÈÎÚfiÙÂÚ·
ÂӉȿÌÂÛ·, .¯. Ï›ÁÔ „ˆÌ›, Ù˘Ú›, ÊÚÔ‡ÙÔ, ÁÈ·Ô‡ÚÙÈ,
¤Ó· ηÚfiÙÔ, ÌÈ· ÓÙÔÌ¿Ù·, Î.¿. (¶›Ó·Î·˜ 2).
2. ¡· ÌËÓ ÚÔÛÙ›ıÂÙ·È Î·ıfiÏÔ˘ ·Ï¿ÙÈ Î·È ̇ ¿¯·ÚË
Ô‡Ù ηٿ ÙÔ Ì·Á›ÚÂÌ· Ô‡Ù ηٿ ÙÔ ÛÂÚ‚›ÚÈÛÌ·.
3. ¡· ¯ÚËÛÈÌÔÔÈÂ›Ù·È ·ÔÎÏÂÈÛÙÈο ·ÁÓfi ·Ú-
ı¤ÓÔ ÂÏ·ÈfiÏ·‰Ô ηٿ ÚÔÙ›ÌËÛË ˆÌfi Î·È Î·ıfiÏÔ˘
Ì·ÚÁ·Ú›Ó˜, ÛÔڤϷÈÔ, ‚Ô‡Ù˘ÚÔ ‹ ¿ÏÏ· ˙ˆÈο ηÈ
Ê˘ÙÈο Ï›Ë.
4. ¡· ÌËÓ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÂÂÍÂÚÁ·Ṳ̂ӷ
ÙÚfiÊÈÌ· Ì ϋıÔ˜ ÚfiÛıÂÙˆÓ Ô˘ÛÈÒÓ, fiˆ˜ ÂÂ-
ÍÂÚÁ·Ṳ̂ӷ ÎÚ¤·Ù· (·ÏÏ·ÓÙÈο, ˙·ÌfiÓ, ÏÔ˘Î¿ÓÈη,
Î.¿.), ÌÈÛÎfiÙ·, ÛÔÎÔÏ¿Ù˜, ¤ÙÔÈ̘ ·È‰ÈΤ˜ ÙÚÔ-
ʤ˜, ·Ù·Ù¿ÎÈ·, Á·Úȉ¿ÎÈ·, ÎÚÔ˘·Û¿Ó, Î.¿. ¡· ·Ô-
ʇÁÔÓÙ·È Ù· Ù·¯˘ÂÛÙÈ·ÙfiÚÈ· ÁÈ·Ù› Ù· Ê·ÁËÙ¿ ÙÔ˘˜
Â›Ó·È ˘„ËÏ‹˜ ÂÓÂÚÁÂȷ΋˜ ˘ÎÓfiÙËÙ·˜ Î·È ¤¯Ô˘Ó
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·158
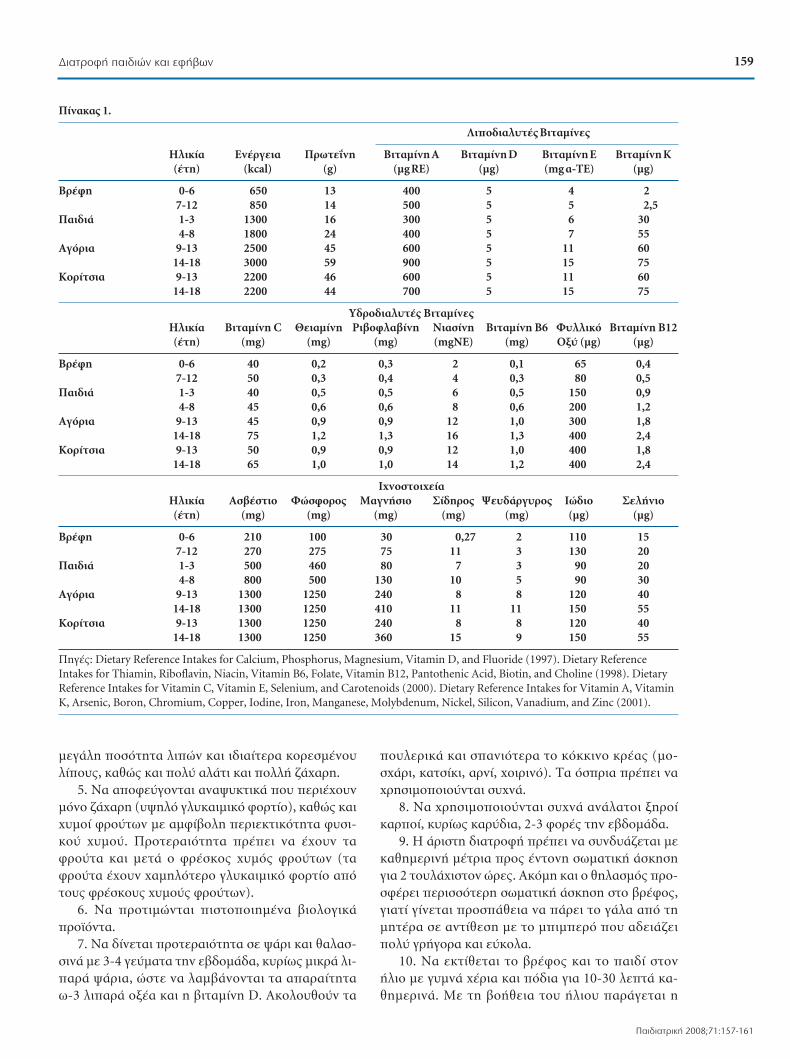
159¢È·ÙÚÔÊ‹ ·È‰ÈÒÓ Î·È ÂÊ‹‚ˆÓ
¶·È‰È·ÙÚÈ΋ 2008;71:157-161
ÌÂÁ¿ÏË ÔÛfiÙËÙ· ÏÈÒÓ Î·È È‰È·›ÙÂÚ· ÎÔÚÂṲ̂ÓÔ˘
Ï›Ô˘˜, ηıÒ˜ Î·È Ôχ ·Ï¿ÙÈ Î·È ÔÏÏ‹ ˙¿¯·ÚË.
5. ¡· ·ÔʇÁÔÓÙ·È ·Ó·„˘ÎÙÈο Ô˘ ÂÚȤ¯Ô˘Ó
ÌfiÓÔ ˙¿¯·ÚË (˘„ËÏfi ÁÏ˘Î·ÈÌÈÎfi ÊÔÚÙ›Ô), ηıÒ˜ ηÈ
¯˘ÌÔ› ÊÚÔ‡ÙˆÓ Ì ·ÌÊ›‚ÔÏË ÂÚÈÂÎÙÈÎfiÙËÙ· Ê˘ÛÈ-
ÎÔ‡ ¯˘ÌÔ‡. ¶ÚÔÙÂÚ·ÈfiÙËÙ· Ú¤ÂÈ Ó· ¤¯Ô˘Ó Ù·
ÊÚÔ‡Ù· Î·È ÌÂÙ¿ Ô ÊÚ¤ÛÎÔ˜ ¯˘Ìfi˜ ÊÚÔ‡ÙˆÓ (Ù·
ÊÚÔ‡Ù· ¤¯Ô˘Ó ¯·ÌËÏfiÙÂÚÔ ÁÏ˘Î·ÈÌÈÎfi ÊÔÚÙ›Ô ·fi
ÙÔ˘˜ ÊÚ¤ÛÎÔ˘˜ ¯˘ÌÔ‡˜ ÊÚÔ‡ÙˆÓ).
6. ¡· ÚÔÙÈÌÒÓÙ·È ÈÛÙÔÔÈË̤ӷ ‚ÈÔÏÔÁÈο
ÚÔ˚fiÓÙ·.
7. ¡· ‰›ÓÂÙ·È ÚÔÙÂÚ·ÈfiÙËÙ· Û „¿ÚÈ Î·È ı·Ï·Û-
ÛÈÓ¿ Ì 3-4 Á‡̷ٷ ÙËÓ Â‚‰ÔÌ¿‰·, ΢ڛˆ˜ ÌÈÎÚ¿ ÏÈ-
·Ú¿ „¿ÚÈ·, ÒÛÙÂ Ó· Ï·Ì‚¿ÓÔÓÙ·È Ù· ··Ú·›ÙËÙ·
ˆ-3 ÏÈ·Ú¿ Ôͤ· Î·È Ë ‚ÈÙ·Ì›ÓË D. ∞ÎÔÏÔ˘ıÔ‡Ó Ù·
Ô˘ÏÂÚÈο Î·È Û·ÓÈfiÙÂÚ· ÙÔ ÎfiÎÎÈÓÔ ÎÚ¤·˜ (ÌÔ-
Û¯¿ÚÈ, ηÙÛ›ÎÈ, ·ÚÓ›, ¯ÔÈÚÈÓfi). ∆· fiÛÚÈ· Ú¤ÂÈ Ó·
¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È Û˘¯Ó¿.
8. ¡· ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È Û˘¯Ó¿ ·Ó¿Ï·ÙÔÈ ÍËÚÔ›
ηÚÔ›, ΢ڛˆ˜ ηڇ‰È·, 2-3 ÊÔÚ¤˜ ÙËÓ Â‚‰ÔÌ¿‰·.
9. ∏ ¿ÚÈÛÙË ‰È·ÙÚÔÊ‹ Ú¤ÂÈ Ó· Û˘Ó‰˘¿˙ÂÙ·È ÌÂ
ηıËÌÂÚÈÓ‹ ̤ÙÚÈ· ÚÔ˜ ¤ÓÙÔÓË ÛˆÌ·ÙÈ΋ ¿ÛÎËÛË
ÁÈ· 2 ÙÔ˘Ï¿¯ÈÛÙÔÓ ÒÚ˜. ∞ÎfiÌË Î·È Ô ıËÏ·ÛÌfi˜ ÚÔ-
ÛʤÚÂÈ ÂÚÈÛÛfiÙÂÚË ÛˆÌ·ÙÈ΋ ¿ÛÎËÛË ÛÙÔ ‚Ú¤ÊÔ˜,
ÁÈ·Ù› Á›ÓÂÙ·È ÚÔÛ¿ıÂÈ· Ó· ¿ÚÂÈ ÙÔ Á¿Ï· ·fi ÙË
ÌËÙ¤Ú· Û ·ÓÙ›ıÂÛË Ì ÙÔ ÌÈÌÂÚfi Ô˘ ·‰ÂÈ¿˙ÂÈ
Ôχ ÁÚ‹ÁÔÚ· Î·È Â‡ÎÔÏ·.
10. ¡· ÂÎÙ›ıÂÙ·È ÙÔ ‚Ú¤ÊÔ˜ Î·È ÙÔ ·È‰› ÛÙÔÓ
‹ÏÈÔ Ì Á˘ÌÓ¿ ¯¤ÚÈ· Î·È fi‰È· ÁÈ· 10-30 ÏÂÙ¿ η-
ıËÌÂÚÈÓ¿. ªÂ ÙË ‚Ô‹ıÂÈ· ÙÔ˘ ‹ÏÈÔ˘ ·Ú¿ÁÂÙ·È Ë
¶›Ó·Î·˜ 1.
§ÈÔ‰È·Ï˘Ù¤˜ µÈٷ̛Ә
∏ÏÈΛ· ∂Ó¤ÚÁÂÈ· ¶ÚˆÙ½ÓË µÈÙ·Ì›ÓË ∞ µÈÙ·Ì›ÓË D µÈÙ·Ì›ÓË ∂ µÈÙ·Ì›ÓË ∫(¤ÙË) (kcal) (g) (Ìg RE) (Ìg) (mg ·-TE) (Ìg)
µÚ¤ÊË 0-6 650 13 400 5 4 27-12 850 14 500 5 5 2,5
¶·È‰È¿ 1-3 1300 16 300 5 6 304-8 1800 24 400 5 7 55
∞ÁfiÚÈ· 9-13 2500 45 600 5 11 6014-18 3000 59 900 5 15 75
∫ÔÚ›ÙÛÈ· 9-13 2200 46 600 5 11 6014-18 2200 44 700 5 15 75
À‰ÚÔ‰È·Ï˘Ù¤˜ µÈٷ̛Ә∏ÏÈΛ· µÈÙ·Ì›ÓË C £ÂÈ·Ì›ÓË ƒÈ‚ÔÊÏ·‚›ÓË ¡È·Û›ÓË µÈÙ·Ì›ÓË µ6 º˘ÏÏÈÎfi µÈÙ·Ì›ÓË µ12(¤ÙË) (mg) (mg) (mg) (mgNE) (mg) √͇ (Ìg) (Ìg)
µÚ¤ÊË 0-6 40 0,2 0,3 2 0,1 65 0,47-12 50 0,3 0,4 4 0,3 80 0,5
¶·È‰È¿ 1-3 40 0,5 0,5 6 0,5 150 0,94-8 45 0,6 0,6 8 0,6 200 1,2
∞ÁfiÚÈ· 9-13 45 0,9 0,9 12 1,0 300 1,814-18 75 1,2 1,3 16 1,3 400 2,4
∫ÔÚ›ÙÛÈ· 9-13 50 0,9 0,9 12 1,0 400 1,814-18 65 1,0 1,0 14 1,2 400 2,4
π¯ÓÔÛÙÔȯ›·∏ÏÈΛ· ∞Û‚¤ÛÙÈÔ ºÒÛÊÔÚÔ˜ ª·ÁÓ‹ÛÈÔ ™›‰ËÚÔ˜ 梉¿ÚÁ˘ÚÔ˜ πÒ‰ÈÔ ™ÂÏ‹ÓÈÔ(¤ÙË) (mg) (mg) (mg) (mg) (mg) (Ìg) (Ìg)
µÚ¤ÊË 0-6 210 100 30 0,27 2 110 157-12 270 275 75 11 3 130 20
¶·È‰È¿ 1-3 500 460 80 7 3 90 204-8 800 500 130 10 5 90 30
∞ÁfiÚÈ· 9-13 1300 1250 240 8 8 120 4014-18 1300 1250 410 11 11 150 55
∫ÔÚ›ÙÛÈ· 9-13 1300 1250 240 8 8 120 4014-18 1300 1250 360 15 9 150 55
¶ËÁ¤˜: Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride (1997). Dietary ReferenceIntakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline (1998). DietaryReference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids (2000). Dietary Reference Intakes for Vitamin A, VitaminK, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc (2001).
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·159
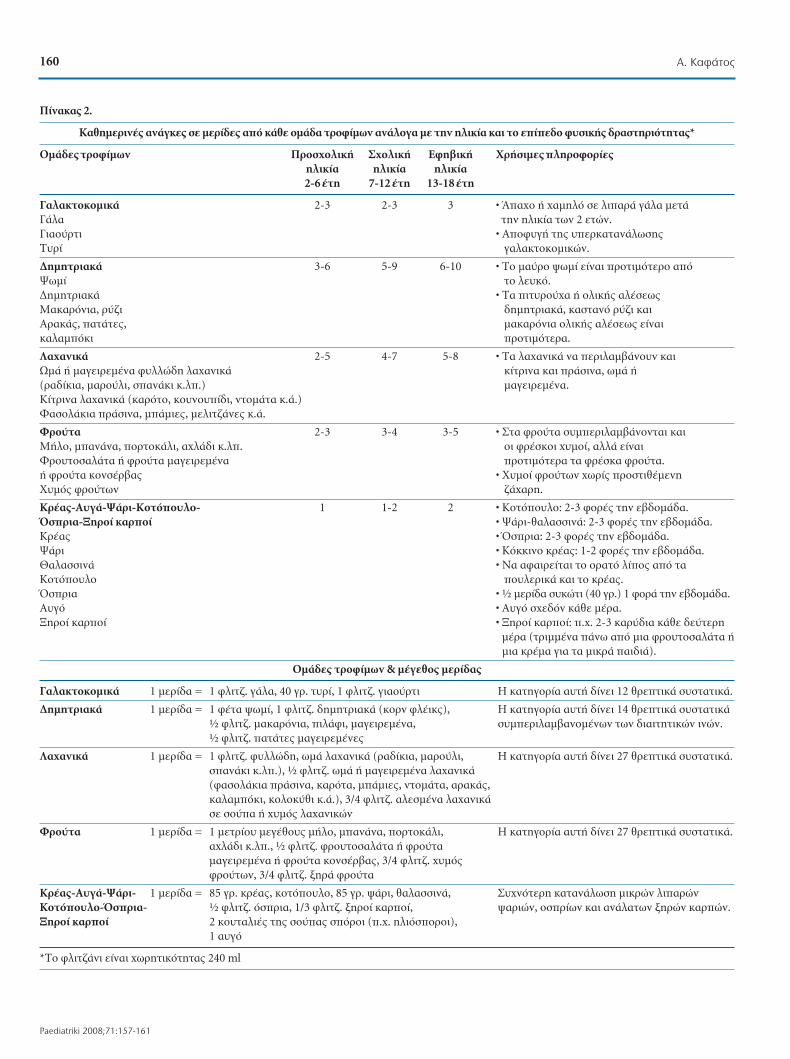
160 ∞. ∫·Ê¿ÙÔ˜
Paediatriki 2008;71:157-161
¶›Ó·Î·˜ 2.
∫·ıËÌÂÚÈÓ¤˜ ·Ó¿ÁΘ Û ÌÂÚ›‰Â˜ ·fi οı ÔÌ¿‰· ÙÚÔÊ›ÌˆÓ ·Ó¿ÏÔÁ· Ì ÙËÓ ËÏÈΛ· Î·È ÙÔ Â›Â‰Ô Ê˘ÛÈ΋˜ ‰Ú·ÛÙËÚÈfiÙËÙ·˜*
√Ì¿‰Â˜ ÙÚÔÊ›ÌˆÓ ¶ÚÔÛ¯ÔÏÈ΋ ™¯ÔÏÈ΋ ∂ÊË‚È΋ ÃÚ‹ÛÈ̘ ÏËÚÔÊÔڛ˜ËÏÈΛ· ËÏÈΛ· ËÏÈΛ·2-6 ¤ÙË 7-12 ¤ÙË 13-18 ¤ÙË
°·Ï·ÎÙÔÎÔÌÈο 2-3 2-3 3 ñ Õ·¯Ô ‹ ¯·ÌËÏfi Û ÏÈ·Ú¿ Á¿Ï· ÌÂÙ¿ °¿Ï· ÙËÓ ËÏÈΛ· ÙˆÓ 2 ÂÙÒÓ.°È·Ô‡ÚÙÈ ñ ∞ÔÊ˘Á‹ Ù˘ ˘ÂÚηٷӿψÛ˘ ∆˘Ú› Á·Ï·ÎÙÔÎÔÌÈÎÒÓ.
¢ËÌËÙÚȷο 3-6 5-9 6-10 ñ ∆Ô Ì·‡ÚÔ „ˆÌ› Â›Ó·È ÚÔÙÈÌfiÙÂÚÔ ·fi æˆÌ› ÙÔ Ï¢Îfi.¢ËÌËÙÚȷο ñ ∆· ÈÙ˘ÚÔ‡¯· ‹ ÔÏÈ΋˜ ·Ï¤Ûˆ˜ ª·Î·ÚfiÓÈ·, Ú‡˙È ‰ËÌËÙÚȷο, ηÛÙ·Ófi Ú‡˙È Î·È ∞ڷο˜, ·Ù¿Ù˜, ̷ηÚfiÓÈ· ÔÏÈ΋˜ ·Ï¤Ûˆ˜ Â›Ó·È Î·Ï·ÌfiÎÈ ÚÔÙÈÌfiÙÂÚ·.
§·¯·ÓÈο 2-5 4-7 5-8 ñ ∆· Ï·¯·ÓÈο Ó· ÂÚÈÏ·Ì‚¿ÓÔ˘Ó Î·È øÌ¿ ‹ Ì·ÁÂÈÚÂ̤ӷ Ê˘ÏÏÒ‰Ë Ï·¯·ÓÈο ΛÙÚÈÓ· Î·È Ú¿ÛÈÓ·, ˆÌ¿ ‹ (Ú·‰›ÎÈ·, Ì·ÚÔ‡ÏÈ, Û·Ó¿ÎÈ Î.Ï.) Ì·ÁÂÈÚÂ̤ӷ.∫›ÙÚÈÓ· Ï·¯·ÓÈο (ηÚfiÙÔ, ÎÔ˘ÓÔ˘›‰È, ÓÙÔÌ¿Ù· Î.¿.)º·ÛÔÏ¿ÎÈ· Ú¿ÛÈÓ·, Ì¿ÌȘ, ÌÂÏÈÙ˙¿Ó˜ Î.¿.
ºÚÔ‡Ù· 2-3 3-4 3-5 ñ ™Ù· ÊÚÔ‡Ù· Û˘ÌÂÚÈÏ·Ì‚¿ÓÔÓÙ·È Î·È ª‹ÏÔ, Ì·Ó¿Ó·, ÔÚÙÔοÏÈ, ·¯Ï¿‰È Î.Ï. ÔÈ ÊÚ¤ÛÎÔÈ ¯˘ÌÔ›, ·ÏÏ¿ Â›Ó·È ºÚÔ˘ÙÔÛ·Ï¿Ù· ‹ ÊÚÔ‡Ù· Ì·ÁÂÈÚÂ̤ӷ ÚÔÙÈÌfiÙÂÚ· Ù· ÊÚ¤Ûη ÊÚÔ‡Ù·.‹ ÊÚÔ‡Ù· ÎÔÓÛ¤Ú‚·˜ ñ Ã˘ÌÔ› ÊÚÔ‡ÙˆÓ ¯ˆÚ›˜ ÚÔÛÙÈı¤ÌÂÓË Ã˘Ìfi˜ ÊÚÔ‡ÙˆÓ ˙¿¯·ÚË.
∫Ú¤·˜-∞˘Á¿-æ¿ÚÈ-∫ÔÙfiÔ˘ÏÔ- 1 1-2 2 ñ ∫ÔÙfiÔ˘ÏÔ: 2-3 ÊÔÚ¤˜ ÙËÓ Â‚‰ÔÌ¿‰·.ŸÛÚÈ·-•ËÚÔ› ηÚÔ› ñ æ¿ÚÈ-ı·Ï·ÛÛÈÓ¿: 2-3 ÊÔÚ¤˜ ÙËÓ Â‚‰ÔÌ¿‰·.∫Ú¤·˜ ñ ŸÛÚÈ·: 2-3 ÊÔÚ¤˜ ÙËÓ Â‚‰ÔÌ¿‰·.æ¿ÚÈ ñ ∫fiÎÎÈÓÔ ÎÚ¤·˜: 1-2 ÊÔÚ¤˜ ÙËÓ Â‚‰ÔÌ¿‰·.£·Ï·ÛÛÈÓ¿ ñ ¡· ·Ê·ÈÚÂ›Ù·È ÙÔ ÔÚ·Ùfi ϛԘ ·fi Ù· ∫ÔÙfiÔ˘ÏÔ Ô˘ÏÂÚÈο Î·È ÙÔ ÎÚ¤·˜.ŸÛÚÈ· ñ ó ÌÂÚ›‰· Û˘ÎÒÙÈ (40 ÁÚ.) 1 ÊÔÚ¿ ÙËÓ Â‚‰ÔÌ¿‰·.∞˘Áfi ñ ∞˘Áfi ۯ‰fiÓ Î¿ı ̤ڷ.•ËÚÔ› ηÚÔ› ñ •ËÚÔ› ηÚÔ›: .¯. 2-3 ηڇ‰È· οı ‰Â‡ÙÂÚË
̤ڷ (ÙÚÈÌ̤ӷ ¿Óˆ ·fi ÌÈ· ÊÚÔ˘ÙÔÛ·Ï¿Ù· ‹ÌÈ· Îڤ̷ ÁÈ· Ù· ÌÈÎÚ¿ ·È‰È¿).
√Ì¿‰Â˜ ÙÚÔÊ›ÌˆÓ & ̤ÁÂıÔ˜ ÌÂÚ›‰·˜
°·Ï·ÎÙÔÎÔÌÈο 1 ÌÂÚ›‰· = 1 ÊÏÈÙ˙. Á¿Ï·, 40 ÁÚ. Ù˘Ú›, 1 ÊÏÈÙ˙. ÁÈ·Ô‡ÚÙÈ ∏ ηÙËÁÔÚ›· ·˘Ù‹ ‰›ÓÂÈ 12 ıÚÂÙÈο Û˘ÛÙ·ÙÈο.
¢ËÌËÙÚȷο 1 ÌÂÚ›‰· = 1 ʤٷ „ˆÌ›, 1 ÊÏÈÙ˙. ‰ËÌËÙÚȷο (ÎÔÚÓ ÊϤÈΘ), ∏ ηÙËÁÔÚ›· ·˘Ù‹ ‰›ÓÂÈ 14 ıÚÂÙÈο Û˘ÛÙ·ÙÈο ó ÊÏÈÙ˙. ̷ηÚfiÓÈ·, ÈÏ¿ÊÈ, Ì·ÁÂÈÚÂ̤ӷ, Û˘ÌÂÚÈÏ·Ì‚·ÓÔÌ¤ÓˆÓ ÙˆÓ ‰È·ÈÙËÙÈÎÒÓ ÈÓÒÓ.ó ÊÏÈÙ˙. ·Ù¿Ù˜ Ì·ÁÂÈÚÂ̤Ó˜
§·¯·ÓÈο 1 ÌÂÚ›‰· = 1 ÊÏÈÙ˙. Ê˘ÏÏÒ‰Ë, ˆÌ¿ Ï·¯·ÓÈο (Ú·‰›ÎÈ·, Ì·ÚÔ‡ÏÈ, ∏ ηÙËÁÔÚ›· ·˘Ù‹ ‰›ÓÂÈ 27 ıÚÂÙÈο Û˘ÛÙ·ÙÈο.Û·Ó¿ÎÈ Î.Ï.), ó ÊÏÈÙ˙. ˆÌ¿ ‹ Ì·ÁÂÈÚÂ̤ӷ Ï·¯·ÓÈο(Ê·ÛÔÏ¿ÎÈ· Ú¿ÛÈÓ·, ηÚfiÙ·, Ì¿ÌȘ, ÓÙÔÌ¿Ù·, ·Ú·Î¿˜, ηϷÌfiÎÈ, ÎÔÏÔ·ıÈ Î.¿.), 3/4 ÊÏÈÙ˙. ·ÏÂṲ̂ӷ Ï·¯·ÓÈο Û ÛÔ‡· ‹ ¯˘Ìfi˜ Ï·¯·ÓÈÎÒÓ
ºÚÔ‡Ù· 1 ÌÂÚ›‰· = 1 ÌÂÙÚ›Ô˘ ÌÂÁ¤ıÔ˘˜ Ì‹ÏÔ, Ì·Ó¿Ó·, ÔÚÙÔοÏÈ, ∏ ηÙËÁÔÚ›· ·˘Ù‹ ‰›ÓÂÈ 27 ıÚÂÙÈο Û˘ÛÙ·ÙÈο.·¯Ï¿‰È Î.Ï., ó ÊÏÈÙ˙. ÊÚÔ˘ÙÔÛ·Ï¿Ù· ‹ ÊÚÔ‡Ù· Ì·ÁÂÈÚÂ̤ӷ ‹ ÊÚÔ‡Ù· ÎÔÓÛ¤Ú‚·˜, 3/4 ÊÏÈÙ˙. ¯˘Ìfi˜ ÊÚÔ‡ÙˆÓ, 3/4 ÊÏÈÙ˙. ÍËÚ¿ ÊÚÔ‡Ù·
∫Ú¤·˜-∞˘Á¿-æ¿ÚÈ- 1 ÌÂÚ›‰· = 85 ÁÚ. ÎÚ¤·˜, ÎÔÙfiÔ˘ÏÔ, 85 ÁÚ. „¿ÚÈ, ı·Ï·ÛÛÈÓ¿, ™˘¯ÓfiÙÂÚË Î·Ù·Ó¿ÏˆÛË ÌÈÎÚÒÓ ÏÈ·ÚÒÓ ∫ÔÙfiÔ˘ÏÔ-ŸÛÚÈ·- ó ÊÏÈÙ˙. fiÛÚÈ·, 1/3 ÊÏÈÙ˙. ÍËÚÔ› ηÚÔ›, „·ÚÈÒÓ, ÔÛÚ›ˆÓ Î·È ·Ó¿Ï·ÙˆÓ ÍËÚÒÓ Î·ÚÒÓ.•ËÚÔ› ηÚÔ› 2 ÎÔ˘Ù·ÏȤ˜ Ù˘ ÛÔ‡·˜ ÛfiÚÔÈ (.¯. ËÏÈfiÛÔÚÔÈ),
1 ·˘Áfi
*∆Ô ÊÏÈÙ˙¿ÓÈ Â›Ó·È ¯ˆÚËÙÈÎfiÙËÙ·˜ 240 ml
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·160

161¢È·ÙÚÔÊ‹ ·È‰ÈÒÓ Î·È ÂÊ‹‚ˆÓ
¶·È‰È·ÙÚÈ΋ 2008;71:157-161
··Ú·›ÙËÙË ÁÈ· ÙËÓ ·Ó¿Ù˘ÍË ‚ÈÙ·Ì›ÓË D. ∞fi Ù·ÏÈ·Ú¿ „¿ÚÈ· ÙÔ ·È‰› ·›ÚÓÂÈ ÙfiÛÔ ÙË ‚ÈÙ·Ì›ÓË DfiÛÔ Î·È Ù· ··Ú·›ÙËÙ· ˆ-3 ÏÈ·Ú¿ Ôͤ·.
¢Â‰Ô̤Ó˘ Ù˘ ÂȉËÌÈ΋˜ ¤Í·ÚÛ˘ Ù˘ ·¯˘-Û·ÚΛ·˜ Û ·È‰È¿ Î·È ÂÓ‹ÏÈΘ Ù˘ ¯ÒÚ·˜ Ì·˜, ı·Ú¤ÂÈ Ó· ·ÔʇÁÔÓÙ·È ÙÚfiÊÈÌ· ˘„ËÏ‹˜ ÂÓÂÚÁÂÈ-·Î‹˜ ˘ÎÓfiÙËÙ·˜ Î·È Ó· ÚÔÙÈÌÒÓÙ·È ÙÚfiÊÈÌ·˘„ËÏ‹˜ ÂÚÈÂÎÙÈÎfiÙËÙ·˜ Û ‚Èٷ̛Ә Î·È È¯ÓÔ-ÛÙÔȯ›·.
°È’ ·˘Ùfi Ë ÂÓ¤ÚÁÂÈ· ·fi ÏÈ·Ú¿ ‰ÂÓ ı· Ú¤ÂÈ Ó·˘ÂÚ‚·›ÓÂÈ ÙÔ 35% Ù˘ Û˘ÓÔÏÈ΋˜ ÂÓ¤ÚÁÂÈ·˜ ËÌÂÚË-Û›ˆ˜. ∆Ô ˘fiÏÔÈÔ ı· Â›Ó·È 55-65% ·fi Û‡ÓıÂÙÔ˘˜,΢ڛˆ˜, ˘‰·Ù¿ÓıڷΘ, ÂÓÒ ÙÔ 10-20% Ó· ÚÔ¤Ú¯Â-Ù·È ·fi ÚˆÙ½Ó˜. ∆· ÏÈ·Ú¿ ı· Ú¤ÂÈ Û¯Â‰fiÓ ÂÍ’ÔÏÔÎÏ‹ÚÔ˘ Ó· ÚÔ¤Ú¯ÔÓÙ·È ·fi ÂÏ·ÈfiÏ·‰Ô, ÂÓÒ ¤Ó·ÌÈÎÚfi ̤ÚÔ˜, 1-2 ÁÚ·ÌÌ¿ÚÈ· ÙËÓ Ë̤ڷ, ·fi ˆ-3 ÏÈ-·Ú¿ Ôͤ· Ì·ÎÚ¿˜ ·Ï‡ÛÛÔ˘ („¿ÚÈ·) ‹ 5-6 ÁÚ·ÌÌ¿-ÚÈ· ÙËÓ Ë̤ڷ ·fi ·-ÏÈÓÔÓÂÏÈÎfi Ô͇ (ηڇ‰È·, ¿ÁÚÈ·¯fiÚÙ·, fiÛÚÈ·, Î.¿.). ∆· ˆ-6 ÏÈ·Ú¿ Ôͤ· ÚÔ¤Ú¯Ô-ÓÙ·È ·fi ÛÔڤϷȷ, ÍËÚÔ‡˜ ηÚÔ‡˜, fiÛÚÈ· ηȉÂÓ ı· Ú¤ÂÈ Ó· ˘ÂÚ‚·›ÓÔ˘Ó Ù· 6-10 ÁÚ·ÌÌ¿ÚÈ·ÙËÓ Ë̤ڷ. ∞˘Ùfi Â›Ó·È ‰˘Ó·ÙfiÓ Ó· ÂÈÙ¢¯ı›, fiÙ·Ó‰ÂÓ ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È Î·ıfiÏÔ˘ ÛÔڤϷȷ (8). ∆ÔÎÔÚÂṲ̂ÓÔ Ï›Ô˜ ‰ÂÓ ı· Ú¤ÂÈ Ó· ˘ÂÚ‚·›ÓÂÈ Ù·15-20 ÁÚ·ÌÌ¿ÚÈ· ÙËÓ Ë̤ڷ.
√ ˘ÔÏÔÁÈÛÌfi˜ ÙÔ˘ ‚·ÛÈÎÔ‡ ÌÂÙ·‚ÔÏÈÛÌÔ‡ ηÈÙÔ˘ ›‰Ԣ Ê˘ÛÈ΋˜ ‰Ú·ÛÙËÚÈfiÙËÙ·˜, ηıÒ˜ ηÈÙÔ Û‡ÓÔÏÔ ÙˆÓ ··ÈÙÔ‡ÌÂÓˆÓ ÂÓÂÚÁÂÈ·ÎÒÓ ·Ó·ÁÎÒÓı· ‰ÔıÔ‡Ó Û ¿ÏÏÔ ¿ÚıÚÔ, ηıÒ˜ ›Û˘ Î·È Ô ÙÚfi-
Ô˜ ·ÓÙÈÌÂÙÒÈÛ˘ ˘¤Ú‚·ÚˆÓ Î·È ·¯‡Û·ÚΈӷȉÈÒÓ Î·È ÂÊ‹‚ˆÓ.
µÈ‚ÏÈÔÁÚ·Ê›·
1. ∫·Ê¿ÙÔ˜ ∞°, §·Ì·‰¿ÚÈÔ˜ ¢. ∆ÂÏÂ˘Ù·›Â˜ ÂÍÂÏ›ÍÂȘ ÛÙËÓÎÏÈÓÈ΋ ‰È·ÙÚÔÊ‹ Î·È ÂȉËÌÈÔÏÔÁ›· ÙˆÓ ÓÔÛËÌ¿ÙˆÓ ‰È·-ÙÚÔÊ‹˜. ∆Ì‹Ì· π·ÙÚÈ΋˜, ∆Ô̤·˜ ∫ÔÈÓˆÓÈ΋˜ π·ÙÚÈ΋˜,∫ÏÈÓÈ΋ ¶ÚÔÏËÙÈ΋˜ π·ÙÚÈ΋˜ Î·È ¢È·ÙÚÔÊ‹˜, ¶·ÓÂÈ-ÛÙ‹ÌÈÔ ∫Ú‹Ù˘. ∏Ú¿ÎÏÂÈÔ: 1990.
2. Dietary Reference Intakes for Calcium, Phosphorus, Mag-nesium, Vitamin D, and Fluoride. National Academy ofSciences; 1997.
3. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin,Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin,and Choline. Washington DC: Food and Nutrition Board,Institute of Medicine, National Academy Press; 1998.
4. Dietary Reference Intakes for Vitamin C, Vitamin E, Seleni-um, and Carotenoids. National Academy of Sciences; 2000.
5. Dietary Reference Intakes for Vitamin A, Vitamin K,Arsenic, Boron, Chromium, Copper, Iodine, Iron, Man-ganese, Molybdenum, Nickel, Silicon, Vanadium, andZinc National Academy of Sciences; 2001.
6. Williams SR. Nutrition and Diet Therapy. 8th ed. St Louis:Mosby Publishing Co.; 1997.
7. ¢È·ÙÚÔÊ‹ ÁÈ· ¶ÚÔ·ÁˆÁ‹ Ù˘ ˘Á›·˜ Î·È ÚfiÏË„Ë ÙˆÓ¯ÚfiÓÈˆÓ ·ÛıÂÓÂÈÒÓ. ∏Ú¿ÎÏÂÈÔ: ∆À¶√∫ƒ∂∆∞ ∞µ∂; πÔ‡-ÏÈÔ˜ 2007.
8. Kafatos A, Codrington CA. Nutrition and diet for healthylifestyles in Europe: the ‘Eurodiet’ Project. Public HealthNutr.1999;2:327-328.
9. ∫·Ê¿ÙÔ˜ ∞°. ÀÁ›·, ‰È·ÙÚÔÊ‹ Î·È ·Ó¿Ù˘ÍË ·È‰ÈÒÓÚÔÛ¯ÔÏÈ΋˜ ËÏÈΛ·˜. ∫Ú‹ÙË: ¡Ô̷گȷ΋ ∞˘ÙÔ‰ÈÔ›ÎËÛË÷ӛˆÓ; 2004.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·161

162 ∂¡¢π∞º∂ƒ√À™∞ ¶∂ƒπ¶∆ø™∏ CASE REPORT
Paediatriki 2008;71:162-164
Recurrent Respiratory Papillomatosis: case report and
literature review
D. A. Nunez
Abstract: Juvenile onset recurrent respiratory papillomatosis (RRP) is a rare but potentially lifethreatening disease caused by Human papilloma virus (HPV) infection, primarily HPV types 6 and 11. Ittypically presents in children with an onset at 3-4 years. The incidence estimates vary widely, but inEurope a rate of approximately 3.5 cases per million is reported. The vocal folds are the commonest siteof involvement. Dysphonia and/or stridor are the main clinical features of respiratory papillomatosis. Atypical case in a 3 year-old boy is presented. Laryngoscopy to visualise the larynx is required to arrive atthe diagnosis. The mainstay of treatment is surgical resection using the CO2 laser or the laryngeal micro-shaver (microdebrider) under micro-laryngoscopic control. It is not unusual for a typical case to require3 surgical interventions a year over a period of several years. In more aggressive cases adjuvanttreatment is indicated, which includes systemic interferon and intra-lesional Cidofovir. Fatality isassociated with loss of the airway, distal spread into the lungs or malignant transformation. An overviewof the clinical condition and current treatment is presented.
Key words: Larynx, papilloma, Human papilloma virus 6, Human papilloma virus 11, voice disorders.
Academic Unit ofOtolaryngology,North Bristol NHS Trust, Southmead Hospital,
Correspondence:
D. A. Nunez [email protected] Unit of Otolaryngology, North Bristol NHS Trust, Southmead Hospital, Bristol BS10 5NB, United Kingdom
Case Report
A 3 year-old boy presented to his paediatri-
cian with a 4-month history of a persistent
hoarse voice, with no history of preceding upper
respiratory tract infection or trauma. He had no
dysphagia or dyspnoea. His single mother re-
ported that he was her first child, delivered nor-
mally at full term when she was 19 years old, af-
ter an uncomplicated pregnancy and delivery.
On examination he was apyrexial and not
distressed, and he was not jaundiced. He
weighed 15 kg and was 105 cm tall. There was no
stridor or cyanosis, his respiratory rate was 24
per minute, the trachea was central and the chest
clear on auscultation. There were no abnormal
heart sounds. Anterior rhinoscopy and oral cav-
ity examination were normal.
He was referred to an otolaryngologist who
undertook a micro-laryngoscopic examination.
The laryngoscopic appearance is as illustrated in
the clinical photograph (Figure 1).
Discussion
Figure 1 shows a larynx of grossly abnormal
appearance, in stark contrast to the appearance of
the normal larynx, Figure 2. The mucosa of the
vocal folds and vestibular folds is oedematous and
polypoid in keeping with the typical appearance
of widespread laryngeal papillomatosis. This pat-
tern of presentation is to be distinguished from
the single solitary often pedunculated upper aero-
digestive tract papilloma. The latter is more com-
mon and often presents in the oropharynx arising
from the soft palate, uvula or palatopharyngeal
arches. Excision is usually curative.
The laryngeal papilloma is the commonest
benign neoplasm of the larynx (1). Laryngeal in-
volvement when widespread, as demonstrated in
this case, is not easily cured and the condition is
known as recurrent laryngeal papillomatosis or
recurrent respiratory papillomatosis (RRP). The
term RRP is to be preferred because while the
larynx at the level of the vocal cords (glottis) is
the site predominantly affected, the papillomata
may extend above and below this level into the
trachea and bronchi. RRP is an uncommon con-
dition with a bimodal peak age incidence of 3-5
years in children and in the third decade in
adults (2). The distribution of age of onset has
lead to the condition being sub-classified as ju-
venile onset RRP or adult onset RRP.
RRP can be life threatening because of airway
compromise, especially in children, or due to ma-
lignant degeneration (3). The reported prevalence
of juvenile onset laryngeal papillomatosis is lower
in Europe (approximately 3.5 per million) than in
the US (4.3 per 100,000) (4,5). The presenting fea-
tures are hoarseness and stridor (2). Males and fe-
males are equally affected in childhood but in the
adult onset disease males are more commonly af-
fected in the ratio of 2-4 to 1 (6,7).
The Human papilloma (wart) virus (HPV) is
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·162

163Recurrent Respiratory Papillomatosis
¶·È‰È·ÙÚÈ΋ 2008;71:162-164
the causative agent for RRP, and specifically HPV sub-
types 6 and 11 (8). There are reports that HPV 11 la-
ryngeal disease is more aggressive, with a greater
predilection for relapse and malignant degeneration
(9). Malignant degeneration is usually associated with
other cofactors such as tobacco use (10), or irradiation,
which was an early therapy for RRP, however some cas-
es undergo malignant change in the absence of any
known cofactors (11). HPV subtypes 6 and 11 are not
associated with a high risk of malignant change, in con-
trast to other subtypes such as 16 and 18, which have
been established as causative agents of cancer of the
uterine cervix (12,13). In the head and neck region high
risk types of HPV have been isolated, predominantly
from cancers of the oral cavity and oropharynx but al-
so from the larynx. The degree of positivity, depending
on the identification method, varies between 0% and
75% (14). This is in contrast to uterine cervical invasive
squamous cell carcinoma, where the level of positivity
is 86-94% (15). It would therefore seem that HPV has a
causative role only in certain anatomical sites in the
head and neck or in particular subgroups of patients.
The mechanism of HPV transmission is uncertain
but vertical materno-fetal transmission is the most
favoured route. This is supported by the 231-fold in-
crease in risk of juvenile onset recurrent respiratory
papillomatosis in children born to mothers with cer-
vical condoylomata (16). The birth canal is not the
only route of transmission, as Armbruster-Moraes
and colleagues demonstrated that HPV DNA can be
isolated in amniotic fluid aspirates from women who
had clinical and slot hybridisation evidence of cervical
papilloma, providing evidence of in-utero transmis-
sion (17). This can explain the failure of Caesarean
section to abolish the development of juvenile onset
laryngeal papilloma disease (18,19).
The presence of HPV6 and/or 11 is not in itself suf-
ficient to cause the development of laryngeal papillo-
matosis, as up to 25% of histologically normal larynges
are positive for HPV6 and 11 DNA (20). Restricted
host immune response is believed to play a role.
The mainstay of treatment is surgery. Microlaryn-
goscopy provides the opportunity not only for tissue
diagnosis by biopsy but also for excision of the papil-
lomata. The surgeon must exercise caution in the pur-
suit of disease eradication in order to avoid damage to
the laryngeal structure and thus irreversible impair-
ment of laryngeal function. Stenosis and webbing of
the anterior glottis can leave the patient with the same
symptoms that the therapy is intended to treat, name-
ly a restricted airway and a life-long hoarse voice. A
CO2 laser beam controlled by a micromanipulator
gives the surgeon microscopic guided accuracy in the
control of papilloma excision. The 10,600 nm wave-
length CO2 provides the advantage of haemostasis
and this is the technique most widely used for treat-
ment of laryngeal papillomata in the UK (21). A num-
ber of other laser types are also used, including the
potassium titanyl phosphate laser delivered by a flexi-
ble fibre that facilitates treatment of papillomata in
the tracheobronchial tree (1).
A recent survey of members of American Society
of Paediatric Otolaryngologists demonstrated the
popularity of the laryngeal shaver (microdebrider)
(22). This is a sleeved rotating blade with continuous
saline irrigation and suction allowing for almost
bloodless removal of laryngeal papillomata.
RRP is a difficult condition to treat in many pa-
tients and in some patients it follows a relentless
course requiring multiple surgeries with only short in-
tervals between treatment schedules when the patient
is clinically free of disease. This is due to the difficulty
Figure 1. Figure 2.
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·163

of eradicating the papilloma virus, which is presenteven in normal appearing laryngeal tissue of the affect-ed patients (19). For this reason a number of adjuvanttreatments have been tried and put into use with theaim of reducing the relapse rate. Alpha interferon andindole-3-carbinol are two popular adjuvant therapiesbut they are not always effective (1,22). Intra-lesionalCidofovir is gaining in popularity because of the goodearly results obtained with this antimetabolite by someclinicians in controlling the disease (23). Photodynam-ic therapy is also under investigation (24). The launchof a highly efficacious HPV vaccine that targets HPV 6and 11 in addition to 16 and 18 (25) offers the potentialto eradicate this disease for future generations.
References
1. Derkay CS. Recurrent respiratory papillomatosis. Laryngo-scope 2001;111:57-69.
2. Quiney RE, Hall D, Croft CB. Laryngeal papillomatosis:analysis of 113 patients. Clin Otolaryngol Allied Sci1989;14:217-225.
3. Zarod AP, Rutherford JD, Corbitt G. Malignant progres-sion of laryngeal papilloma associated with human papillo-ma virus type 6 (HPV-6) DNA. J Clin Pathol 1988;41:280-283.
4. Silverberg MJ, Thorsen P, Lindeberg H, Ahdieh-Grant L,Shah KV. Clinical course of recurrent respiratory papillo-matosis in Danish children. Arch Otolaryngol Head NeckSurg 2004;130:711-716.
5. Derkay CS. Task force on recurrent respiratory papillomas.A preliminary report. Arch Otolaryngol Head Neck Surg1995;121:1386-1391.
6. Lindeberg H, Elbro/nd O. Laryngeal papillomas: clinical as-pects in a series of 231 patients. Clin Otolaryngol Allied Sci1989;14:333-342.
7. Capper JW, Bailey CM, Michaels L. Squamous papillomasof the larynx in adults. A review of 63 cases. Clin Otolaryn-gol 1983;8:109-119.
8. Terry RM, Lewis FA, Griffiths S, Wells M, Bird CC. De-monstration of human papillomavirus types 6 and 11 injuvenile laryngeal papillomatosis by in-situ DNA hy-bridization. J Pathol 1987;153:245-248.
9. Rimell FL, Shoemaker DL, Pou AM, Jordan JA, Post JC,Ehrlich GD. Pediatric respiratory papillomatosis: prognos-tic role of viral typing and cofactors. Laryngoscope 1997;107:915-918.
10. Kashima HK, Mounts P, Shah K. Recurrent respiratory pa-pillomatosis. Obstet Gynecol Clin North Am 1996;23:699-706.
11. Lindeberg H, Elbro/nd O. Malignant tumours in patients
with a history of multiple laryngeal papillomas: the signifi-cance of irradiation. Clin Otolaryngol Allied Sci 1991;16:149-151.
12. Zur Hausen H. Human papillomaviruses in the pathogen-esis of anogenital cancer. Virology 1991;184:9-13.
13. Zur Hausen H. Papillomaviruses in human cancer. ApplPathol 1987;5:19-24.
14. McKaig RG, Baric RS, Olshan AF. Human papillomavirusand head and neck cancer: epidemiology and molecular bi-ology. Head Neck 1998;20:250-265.
15. Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, WinerR, et al. Human papillomavirus type distribution in inva-sive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer. 2007 Aug 1;121(3):621-632.
16. Silverberg MJ, Thorsen P, Lindeberg H, Grant LA, ShahKV. Condyloma in pregnancy is strongly predictive of ju-venile-onset recurrent respiratory papillomatosis. ObstetGynecol 2003;101:645-652.
17. Armbruster-Moraes E, Ioshimoto LM, Lea~o E, Zugaib M.Presence of human papillomavirus DNA in amniotic fluidsof pregnant women with cervical lesions. Gynecol Oncol1994;54:152-158.
18. Shah K, Kashima H, Polk BF, Shah F, Abbey H, AbramsonA. Rarity of cesarean delivery in cases of juvenile-onset res-piratory papillomatosis. Obstet Gynecol 1986;68:795-799.
19. Abramson AL, Steinberg BM, Winkler B. Laryngeal papil-lomatosis: clinical, histopathologic and molecular studies.Laryngoscope 1987;97:678-685.
20. Nunez DA, Astley SM, Lewis FA, Wells M. Human papillo-ma viruses: a study of their prevalence in the normal lar-ynx. J Laryngol Otol 1994;108:319-320.
21. Tasca RA, McCormick M, Clarke RW. British Associationof Paediatric Otorhinolaryngology members experiencewith recurrent respiratory papillomatosis. Int J PediatrOtorhinolaryngol 2006;70:1183-1187.
22. Schraff S, Derkay CS, Burke B, Lawson L. American Societyof Pediatric Otolaryngology members' experience with re-current respiratory papillomatosis and the use of adjuvanttherapy. Arch Otolaryngol Head Neck Surg 2004;130:1039-1042.
23. Naiman AN, Ayari S, Nicollas R, Landry G, Colombeau B,Froehlich P. Intermediate-term and long-term results aftertreatment by cidofovir and excision in juvenile laryngeal pa-pillomatosis. Ann Otol Rhinol Laryngol 2006;115:667-672.
24. Shikowitz MJ, Abramson AL, Freeman K, Steinberg BM,Nouri M. Efficacy of DHE photodynamic therapy for res-piratory papillomatosis: immediate and long-term results.Laryngoscope 1998;108:962-967.
25. Ault KA; Future II Study Group. Effect of prophylactic hu-man papillomavirus L1 virus-like-particle vaccine on riskof cervical intraepithelial neoplasia grade 2, grade 3, andadenocarcinoma in situ: a combined analysis of four ran-domised clinical trials. Lancet. 2007;369:1861-1868.
164 D. A. Nunez
Paediatriki 2008;71:162-164
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·164

165∫§π¡π∫√ ∫√Àπ∑
¶·È‰È·ÙÚÈ΋ 2007;70:165,176
¶. ™ËÊÈ·ÓÔ‡1, ∫. ºˆÙ›Ô˘1, ∫. ™ÎÈ·‰¿˜2, ∫. ¶··Á·ÚÔ˘Ê¿Ï˘1
¡ÂÔÁÓfi Ô˘ ÁÂÓÓ‹ıËΠ̠ÚÔÁÚ·ÌÌ·ÙÈṲ̂ÓË
ηÈÛ·ÚÈ΋ ÙÔÌ‹, ÏfiÁˆ ÂÈı˘Ì›·˜ Ù˘ ÌËÙ¤Ú·˜,
ÛÙȘ 38 ‚‰ÔÌ¿‰Â˜ ·ËÛ˘. ∂›¯Â ‰‡Ô ÂÚÈÙ˘Ï›ÍÂȘ
ÂÚ› ÙÔÓ ·˘¯¤Ó·, ·Ó¤Ó¢Û fï˜ ·Ì¤Ûˆ˜ Î·È ‰ÂÓ
¯ÚÂÈ¿ÛÙËΠ·Ó¿ÓË„Ë. ∏ ÂÁ΢ÌÔÛ‡ÓË ‹Ù·Ó ÔÌ·Ï‹
Î·È Ô ÎÏÈÓÈÎfi˜ Î·È ·Ú·ÎÏÈÓÈÎfi˜ ¤ÏÂÁ¯Ô˜ Ê˘ÛÈÔ-
ÏÔÁÈÎfi˜, Ì ÂÍ·›ÚÂÛË ÙËÓ ·ÌÊÔÙÂÚfiÏ¢ÚË ‰È¿-
Ù·ÛË ÙˆÓ ˘ÂÏÔÎ·Ï˘ÎÈÎÒÓ Û˘ÛÙËÌ¿ÙˆÓ ÙÔ˘ ÂÌ-
‚Ú‡Ô˘ ÛÙÔ ˘ÂÚ˯ÔÁÚ¿ÊËÌ· µ ÂȤ‰Ô˘. ™ÙËÓ
·Ú¯È΋ ÎÏÈÓÈ΋ ÂͤٷÛË ÙÔ˘ ÓÂÔÁÓÔ‡ ‰ÂÓ ‰È·È-
ÛÙÒıËÎ·Ó ‰˘ÛÌÔÚʛ˜ ‹ ¿ÏÏ· ·ıÔÏÔÁÈο ¢ڋ-
Ì·Ù·. ™ÙÔ Ù¤ÏÔ˜ ÙÔ˘ 1Ô˘ 24ÒÚÔ˘ ̇ ˆ‹˜, ·ÚÔ˘Û›·-
Û ‡ÔÙÔ ÂÂÈÛfi‰ÈÔ Û·ÛÌÒÓ ‰È¿ÚÎÂÈ·˜ ‰‡Ô Â-
Ú›Ô˘ ÏÂÙÒÓ. ∆Ô ÂÂÈÛfi‰ÈÔ ÂÚÈÏ¿Ì‚·Ó ‚Ú·-
¯Â›Â˜ Û˘Û¿ÛÂȘ ÙˆÓ ¿Óˆ, ΢ڛˆ˜, ·ÏÏ¿ Î·È ÙˆÓ
οو ¿ÎÚˆÓ. ∏ ÛÙÔȯÂÈ҉˘ Ì˘ÔÛÎÂÏÂÙÈ΋ ‰Ú·-
ÛÙËÚÈfiÙËÙ· ÚÔÛÔÌÔ›·˙Â ÌÂ Ù· «ÙÈÓ¿ÁÌ·Ù·» ÙˆÓ
ÓÂÔÁÓÒÓ, ‰Ú·ÛÙËÚÈfiÙËÙ· Ô˘ fï˜ ›¯Â Û˘ÚÚ¤Ô-
ÓÙ· ¯·Ú·ÎÙ‹Ú·, Ì ÙËÓ ·ÚÂÌ‚ÔÏ‹ ‚Ú·¯‡Ù·Ù˘
Ê¿Û˘ Ì˘˚΋˜ ËÚÂÌ›·˜ ÛÙ· ÌÂÛԉȷÛÙ‹Ì·Ù·. √È
ÎfiÚ˜ Î·È Ë ı¤ÛË ÙˆÓ ‚ÔÏ‚ÒÓ ‰ÂÓ ‹Ù·Ó ÔÚ·Ù¿,
·ÊÔ‡ ÙÔ ÓÂÔÁÓfi ÎÔÈÌfiÙ·Ó Î·Ù¿ ÙÔ ÂÂÈÛfi‰ÈÔ. ¶·-
ÚfiÌÔÈ· ÂÂÈÛfi‰È· ·ӷϋÊıËÎ·Ó Î·È ÛÙȘ Âfi-
ÌÂÓ˜ ̤Ú˜, ¯ˆÚ›˜ Ó· Û˘Óԉ‡ÔÓÙ·È Ì ηډÈÔ·-
Ó·Ó¢ÛÙÈ΋ ‰˘ÛÏÂÈÙÔ˘ÚÁ›· (ÙÒÛË ÎÔÚÂÛÌÔ‡ ‹
‚Ú·‰˘Î·Ú‰›·). ∆Ô ÓÂÔÁÓfi Û˘Ó¤¯ÈÛ ӷ ÛÈÙ›˙ÂÙ·È
Ì ÌËÙÚÈÎfi Á¿Ï· Î·È Ù¯ÓËÙ‹ ‰È·ÙÚÔÊ‹ Î·È ¿Ú¯ÈÛÂ
Ó· ÎÂÚ‰›˙ÂÈ ‚¿ÚÔ˜. ∫·ı’ fiÏË ÙË ‰È¿ÚÎÂÈ· Ù˘ ÓÔ-
ÛËÏ›·˜ ÙÔ˘ ‰ÂÓ ‰È·ÈÛÙÒıËΠ·ıÔÏÔÁÈ΋ Ó¢-
ÚÔÏÔÁÈ΋ ÛËÌÂÈÔÏÔÁ›· (.¯. ‰È·Ù·Ú·¯¤˜ Ì˘˚ÎÔ‡ÙfiÓÔ˘, ·ÓÙ·Ó·ÎÏ·ÛÙÈÎÒÓ Î.Ï.).
∆Ô U/S ÂÁÎÂÊ¿ÏÔ˘ Ô˘ ¤ÁÈÓ ÙÔ 2Ô 24ˆÚÔ ˙ˆ-‹˜ ¤‰ÂÈÍ ˘¤Ú˯˜ ÂÚÈÔ¯¤˜ ÛÙȘ ÁˆÓ›Â˜ ÙÔ˘ÛÒÌ·ÙÔ˜. ™ÙË CT ÂÁÎÂÊ¿ÏÔ˘, ÙÔ 8Ô 24ˆÚÔ, ‰ÂÓ·Ú·ÙËÚ‹ıËÎ·Ó ·ıÔÏÔÁÈο Â˘Ú‹Ì·Ù·. √ ¤ÏÂÁ-¯Ô˜ Ù˘ ÁÏ˘Îfi˙˘, ÙˆÓ ËÏÂÎÙÚÔÏ˘ÙÒÓ Î·È ÙÔ˘·Û‚ÂÛÙ›Ô˘-Ì·ÁÓËÛ›Ô˘ ‹Ù·Ó Ê˘ÛÈÔÏÔÁÈÎfi˜, ÂÓÒ·˘ÍË̤Ó˜ ‹Ù·Ó ÔÈ CPK, LDH Î·È SGOT (884U/L, 624 U/L Î·È 47 U/L, ·ÓÙÈÛÙÔ›¯ˆ˜) ÛÙÔ 2Ô24ˆÚÔ Ù˘ ˙ˆ‹˜.
ªÂÙ¿ ÙÔ 2Ô 24ˆÚÔ Ù˘ ˙ˆ‹˜ ÙÔ˘, ÙÔ ÓÂÔÁÓfiÛ˘Ó‰ÂfiÙ·Ó ÂÚÈÔ‰Èο Ì CFM (CerebralFunction Monitor). ∏ ‚·ÛÈ΋ ηٷÁÚ·Ê‹ ‹Ù·ÓÊ˘ÛÈÔÏÔÁÈ΋ Î·È Ë ·Ó¿Ï˘ÛË Ù˘ ηٷÁÚ·Ê‹˜ ÛÙˉȿÚÎÂÈ· ÂÓfi˜ ÎÏÈÓÈÎÔ‡ ÂÂÈÛÔ‰›Ô˘ ‰ÂÓ ‹Ù·Ó ÂÓ-‰ÂÈÎÙÈ΋ ÂÈÏËÙÈ΋˜ ‰Ú·ÛÙËÚÈfiÙËÙ·˜. ∆Ô ∏∂°Ô˘ ¤ÁÈÓ ÛÙȘ 30 ̤Ú˜ Ù˘ ˙ˆ‹˜ (Î·È ÂÓfiÛˆ Û˘-Ó¯›˙ÔÓÙ·Ó Ù· ÂÂÈÛfi‰È·) ¤‰ÂÈÍÂ Ê˘ÛÈÔÏÔÁÈ΋‚·ÛÈ΋ ‰Ú·ÛÙËÚÈfiÙËÙ· Î·È ·Ô˘Û›· ·ıÔÏÔÁÈ-ÎÒÓ ÂÎÊÔÚÙ›ÛˆÓ.
∏ ‰È¿ÁÓˆÛË Ù¤ıËΠ̠¤Ó·Ó ·Ïfi ¯ÂÈÚÈÛÌfi.
¶Èı·Ó¤˜ ‰È·ÁÓÒÛÂȘ:
1. ™·ÛÌÔ› 5˘ ̤ڷ˜2. ™·ÛÌÔ› › ‰¿ÊÔ˘˜ ˘ÔÍÈ΋˜-ÈÛ¯·ÈÌÈ΋˜
‚Ï¿‚˘3. ¶ÚÒÈÌË Ì˘ÔÎÏÔÓÈ΋ ÂÁÎÂÊ·ÏÔ¿ıÂÈ·4. ∫·ÏÔ‹ıÂȘ Ì˘ÔÎÏÔӛ˜ ‡ÓÔ˘
∏ ·¿ÓÙËÛË ·ÎÔÏÔ˘ı› ÛÙË ÛÂÏ›‰· 176
1 ¡ÂÔÁÓÔÏÔÁÈÎfi ∆Ì‹Ì·,°.¡.-ª·ÈÂ˘Ù‹ÚÈÔ “ŒÏÂÓ· µÂÓÈ˙¤ÏÔ˘”
2 ¡Â˘ÚÔÏÔÁÈÎfi ∆Ì‹Ì·,¡ÔÛÔÎÔÌÂ›Ô ¶·›‰ˆÓ “∞Á›· ™ÔÊ›·”
AÏÏËÏÔÁÚ·Ê›·:
¶fiË ™ËÊÈ·ÓÔ‡[email protected]¡ÂÔÁÓÔÏÔÁÈÎfi ∆Ì‹Ì·,°.¡.-ª·ÈÂ˘Ù‹ÚÈÔ “ŒÏÂÓ· µÂÓÈ˙¤ÏÔ˘”¶Ï·Ù›· ŒÏÂÓ·˜ µÂÓÈ˙¤ÏÔ˘ 2, ∆.∫. 115 21, ∞ı‹Ó·
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·165

166 ∂¶π∫∞πƒ√ £∂ª∞ CURRENT ISSUE
Paediatriki 2008;71:166-170
“¡¤Ô ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ
(2008)”
™ÙȘ 4/12/2007 Û˘Ó‹Ïı ÛÙËÓ ∞ı‹Ó· (¢È‡-ı˘ÓÛË ¢ËÌfiÛÈ·˜ ÀÁ›·˜) Ë ∂ıÓÈ΋ ∂ÈÙÚÔ‹∂Ì‚ÔÏÈ·ÛÌÒÓ (∂∂∂) ÁÈ· Ó· ·Ó·ıˆڋÛÂÈ ÙÔ ∂ıÓÈ-Îfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ (∂¶∂) Î·È Ó· ÚÔ-Ù›ÓÂÈ ÔÚÈṲ̂Ó˜ ·ÏÏ·Á¤˜ Û‡Ìʈӷ Ì ÙȘ ÙÚ¤-¯Ô˘Û˜ ÂȉËÌÈÔÏÔÁÈΤ˜ Û˘Óı‹Î˜ Ù˘ ¯ÒÚ·˜,ÙȘ ‰ÈÂıÓ›˜ Ù¿ÛÂȘ Î·È ÙËÓ Î˘ÎÏÔÊÔÚ›· Ó¤ˆÓ, Ô-χ ÛËÌ·ÓÙÈÎÒÓ ÁÈ· ÙË ¢ËÌfiÛÈ· ÀÁ›· ∂Ì‚ÔÏ›ˆÓ.
ªÂÙ¿ ·fi ÂÈÛٷ̤ÓË ÌÂϤÙË ÙˆÓ ÚÔ·Ó·-ÊÂÚı¤ÓÙˆÓ ‰Â‰ÔÌ¤ÓˆÓ Î·È ÂÎÙÂÓ‹ Û˘˙‹ÙËÛËÌÂٷ͇ ÙˆÓ ÌÂÏÒÓ Ù˘ ∂ÈÙÚÔ‹˜ › ÙˆÓ ‰Â-‰ÔÌ¤ÓˆÓ ·˘ÙÒÓ ‰È·ÌÔÚÊÒıËΠÙÔ Ó¤Ô ∂¶∂, ÙÔÔÔ›Ô ¤ÁÈÓ ·Ô‰ÂÎÙfi ·fi ÙËÓ ÔÏÈÙÈ΋ ËÁÂÛ›·ÙÔ˘ ÀÔ˘ÚÁ›Ԣ ÀÁ›·˜ Î·È ∫ÔÈÓˆÓÈ΋˜ ∞ÏÏË-ÏÂÁÁ‡Ë˜, fiˆ˜ ·ÎÚÈ‚Ò˜ ÚÔÙ¿ıËÎÂ. √È ·ÏÏ·-Á¤˜ Ô˘ ¤ÁÈÓ·Ó ÛÙÔ ∂¶∂ Û˘ÓÔ„›˙ÔÓÙ·È ˆ˜ ÂÍ‹˜:
1. ∂Ì‚fiÏÈÔ ‰ÈÊıÂÚ›Ùȉ·˜, ÙÂÙ¿ÓÔ˘, ÎÔη-ÙË (DTaP). ¶ÚÔÛÙ›ıÂÙ·È Ì›· ÂÈϤÔÓ ‰fiÛËÛÙËÓ ËÏÈΛ· 11-12 ÂÙÒÓ Ì ÙÔ Û··ÛÌ· TdaP(‚Ϥ ÂÂÍ‹ÁËÛË 2·, 2‚).
2. ∂Ì‚fiÏÈÔ ·ÓÂÌ¢ÏÔÁÈ¿˜ (Var). ¶ÚÔÛÙ›ıÂ-Ù·È 2Ë ‰fiÛË ÛÙËÓ ËÏÈΛ· 4-6 ÂÙÒÓ.
3. ∂Ì‚fiÏÈÔ Î·Ù¿ ÙÔ˘ ÈÔ‡ ÙˆÓ ·ÓıÚÒÈÓˆÓıËÏˆÌ¿ÙˆÓ (Human Papilloma Virus ‹HPV). ¶ÚÔÛÙ›ıÂÙ·È Ó¤Ô ÂÌ‚fiÏÈÔ Î·Ù¿ ÙÔ˘ HPVÔ˘ Û˘ÓÈÛÙ¿Ù·È ÌfiÓÔ ÁÈ· Ù· ÎÔÚ›ÙÛÈ· ËÏÈΛ·˜12-15 ÂÙÒÓ ‹ ̤¯ÚÈ 26 ÂÙÒÓ, ÂÊfiÛÔÓ ‰ÂÓ ÂÌ‚Ô-ÏÈ¿ÛÙËÎ·Ó ÛÙË Û˘ÓÈÛÙÒÌÂÓË ËÏÈΛ· (‚ϤÂÂÂÍ‹ÁËÛË 9 Î·È ÙË Û¯ÂÙÈ΋ ÂÁ·ÎÏÈÔ Ô˘
·ÊÔÚ¿ ÙÔ ÂÌ‚fiÏÈÔ ·˘Ùfi ÛÙË ÛÙ‹ÏË Ù˘ ¢ËÌfi-ÛÈ·˜ ÀÁ›·˜).
4. ∂Ì‚fiÏÈÔ Î·Ù¿ Ù˘ Ë·Ù›Ùȉ·˜ ∞ (Hep A).¶ÂÚÈÏ·Ì‚¿ÓÂÙ·È ÛÙ· ··Ú·›ÙËÙ· ϤÔÓ ÂÌ‚fi-ÏÈ· ÙÔ˘ ∂¶∂ ·fi ÙÔ 12Ô Ì‹Ó· Î·È ÌÂÙ¿ (‚ϤÂÂÂÍ‹ÁËÛË 10) Î·È Û˘Ó¯›˙ÂÈ Ó· Á›ÓÂÙ·È ÛÙȘÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ (¶›Ó·Î·˜ 3).
°È· ÙȘ ÂÚÈÙÒÛÂȘ ÙˆÓ ·È‰ÈÒÓ, Ô˘ ÁÈ·‰È¿ÊÔÚÔ˘˜ ÏfiÁÔ˘˜ ‰ÂÓ ÂÌ‚ÔÏÈ¿ÛÙËÎ·Ó ÛÙË Û˘-ÓÈÛÙÒÌÂÓË ·fi ÙÔ ∂¶∂ ËÏÈΛ·, ˘¿Ú¯Ô˘Ó ÂȉÈ-ο ¯ÚÔÓԉȿÁÚ·ÌÌ·Ù· (¶›Ó·Î˜ 5 Î·È 6) Ì ÙȘۯÂÙÈΤ˜ ÂÂÍËÁ‹ÛÂȘ.
∆Ô Ó¤Ô ∂¶∂, fiˆ˜ ‰È·ÌÔÚÊÒıËΠÁÈ· ÙÔ2008, Û˘ÓÔ„›˙ÂÙ·È ÛÙËÓ ∂ÈÎfiÓ· 1 Î·È ÛÙÔ˘˜ ¶›-ӷΘ 5 Î·È 6.
∏ ∂ıÓÈ΋ ∂ÈÙÚÔ‹ ∂Ì‚ÔÏÈ·ÛÌÒÓ√ ¶Úfi‰ÚÔ˜: ∫ˆÓÛÙ·ÓÙfiÔ˘ÏÔ˜ ∞Ó‰Ú¤·˜∆· ̤ÏË: µÈÔÏ¿ÎË ª., £ÂÔ‰ˆÚ›‰Ô˘ ª.,
∫·Ó·ÎÔ‡‰Ë-∆۷ηϛ‰Ô˘ º., ∫·ÊÂÙ˙‹˜ ¢., ∫¯·ÁÈ·‰¿Î˘ °., ∫‡ÚÏÂÛË ∞., ™¿Ï· °.,™ÙÚ·ÙËÁ¿ÎË ̃ª., ™˘ÚÈÔÔ‡ÏÔ ̆µ., ÃÚÔ‡ÛÔ˜ °.
∏ °Ú·ÌÌ·Ù¤·˜: ™ˆÙ‹Ú¯Ô˘ ∞.
¶›Ó·Î·˜ 3. ∂Ӊ›ÍÂȘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ηٿ Ù˘ ∏·Ù›Ùȉ·˜ ∞Û ¯ÒÚ˜ Ì ¯·ÌËÏ‹ Î·È Ì¤ÛË ÂÓ‰ËÌÈÎfiÙËÙ·
ñ ∆·ÍȉÈÒÙ˜.ñ ∂·ÁÁÂÏ̷ٛ˜ ˘Á›·˜.ñ ∂·ÁÁÂÏ̷ٛ˜ ‰È·Î›ÓËÛ˘ ÙÚÔʛ̈Ó.ñ ¶ÚÔÛˆÈÎfi È‰Ú˘Ì¿ÙˆÓ.ñ ¶ÚÔÛˆÈÎfi ηı·ÚÈfiÙËÙ·˜ ‰ËÌfiÛÈˆÓ Î·È È‰ÈˆÙÈÎÒÓ
ÂÎ·È‰Â˘ÙÈÎÒÓ È‰Ú˘Ì¿ÙˆÓ.ñ ∫ÏÂÈÛÙÔ› ÏËı˘ÛÌÔ›*.ñ √ÌÔÊ˘ÏfiÊÈÏÔÈ - ∆ÔÍÈÎÔÌ·Ó›˜.ñ ÕÙÔÌ· Ì ¯ÚfiÓÈ· Ïԛ̈ÍË Ì ÙÔÓ Èfi Ù˘ ∏µ.
* ‚Ϥ ˘ÔÛËÌ›ˆÛË ¶›Ó·Î· 4
¶›Ó·Î·˜ 1. ÕÙÔÌ· Ì ·˘ÍË̤ÓÔ Î›Ó‰˘ÓÔ ÁÈ· ÛÔ‚·Ú¤˜ Ó¢-ÌÔÓÈÔÎÔÎÎÈΤ˜ ÏÔÈÌÒÍÂȘ
ñ ªÈÎÚ¿ ·È‰È¿ ¿Óˆ ÙˆÓ 2 ÂÙÒÓ Î·È ÂÓ‹ÏÈΘ >60 ÂÙÒÓ.ñ ÕÙÔÌ· ÌÂ Û˘ÁÁÂÓ›˜ ·ÓÙÈۈ̷ÙÈΤ˜ ·Ó¿ÚÎÂȘ
(΢ڛˆ˜ ¤ÏÏÂÈ„Ë Ù˘ IgG2).ñ ÕÙÔÌ· Ô˘ ¤¯Ô˘Ó ÌÔÏ˘Óı› Ì ÙÔÓ Èfi HIV.ñ ÕÙÔÌ· Ì ›ÎÙËÙË ·ÓÔÛÔηٷÛÙÔÏ‹, ÂÍ·ÈÙ›·˜
ÓÔÛ‹Ì·ÙÔ˜ ‹ ıÂڷ›·˜ ‹ ¿ÏÏ˘ (ÂÎÙfi˜ ÙÔ˘ HIV)ÈÔÁÂÓÔ‡˜ Ïԛ̈͢.
ñ ÕÙÔÌ· Ì ÌÂÈÔÓÂÎÙÈ΋ ÛÏËÓÈ΋ ÏÂÈÙÔ˘ÚÁ›· ‹ ·ÛÏËÓ›·.¯. Ì ‰Ú·ÓÔ΢ÙÙ·ÚÈ΋ ÓfiÛÔ, Ì ˘ÂÚÛÏËÓÈÛÌfi, ̯ÂÈÚÔ˘ÚÁÈ΋ ·Ê·›ÚÂÛË ÙÔ˘ ÛÏ‹Ó·.
ñ ÕÙÔÌ· Ì ÓÂÊÚˆÛÈÎfi Û‡Ó‰ÚÔÌÔ ‹ ¯ÚfiÓÈ· ÓÂÊÚÈ΋·Ó¿ÚÎÂÈ·.
ñ ÕÙÔÌ· Ì ۷ί·ÚÒ‰Ë ‰È·‚‹ÙË.ñ ÕÙÔÌ· Ì ¯ÚfiÓÈ· Û˘ÌÊÔÚËÙÈ΋ ηډȷ΋ ·Ó¿ÚÎÂÈ·.ñ ÕÙÔÌ· Ì ¯ÚfiÓȘ Ó¢ÌÔÓÔ¿ıÂȘ.ñ ÕÙÔÌ· Ì ‰È·Ê˘Á‹ ÂÁÎÂÊ·ÏÔÓˆÙÈ·›Ô˘ ˘ÁÚÔ‡ ·fi
Û˘ÁÁÂÓ›˜ ‹ ›ÎÙËÙ˜ ·Èٛ˜.
¶›Ó·Î·˜ 2. ¶·È‰È¿ Ô˘ ·Ó‹ÎÔ˘Ó Û ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ-‰‡ÓÔ˘ ÁÈ· Ê˘Ì·ÙÈ΋ ÌfiÏ˘ÓÛË/Ê˘Ì·Ù›ˆÛË
ñ ªÂÙ·Ó¿ÛÙ˜ ·fi ¯ÒÚ˜ Ì ˘„ËÏfi ‹ ̤ÛÔ ‰Â›ÎÙËÂÓ‰ËÌÈÎfiÙËÙ·˜.
ñ ∫·Ù·˘ÏÈÛÌÔ› ·ıÈÁÁ¿ÓˆÓ Î·È ¿ÏÏˆÓ ÏËı˘ÛÌÈ·ÎÒÓÔÌ¿‰ˆÓ Ô˘ ˙Ô˘Ó ÛÂ Û˘Óı‹Î˜ ÔÌ·‰È΋˜ ‰È·‚›ˆÛ˘.
ñ ¶·È‰È¿ Ì Mantoux (-) ÛÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ÙˆÓ ÔÔ›ˆÓ˘¿Ú¯ÂÈ ¿ÙÔÌÔ ÌÂ Ê˘Ì·Ù›ˆÛË (ıÂÙÈο Ù‡ÂÏ·).
ñ ¡ÂÔÁÓ¿ ÌËÙ¤ÚˆÓ Ô˘ ¤¯Ô˘Ó ÌÔÏ˘Óı› Ì ÙÔÓ Èfi HIV(fi¯È ‚Ú¤ÊË Û˘Ìو̷ÙÈο ÁÈ· AIDS).
ñ ¡ÂÔÁÓ¿, ÛÙÔ ¿ÌÂÛÔ ÂÚÈ‚¿ÏÏÔÓ ÙˆÓ ÔÔ›ˆÓ ˘¿Ú¯ÂÈ¿ÙÔÌÔ ÌÂ Ê˘Ì·Ù›ˆÛË (ÂÌ‚ÔÏÈ¿˙ÔÓÙ·È Î·Ù¿ ÙË Á¤ÓÓËÛË).
∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ
∂ıÓÈ΋ ∂ÈÙÚÔ‹ ∂Ì‚ÔÏÈ·ÛÌÒÓ
Pediatri Mar-Apr 08 08-04-08 11:34 ™ÂÏ›‰·166

167∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ
¶·È‰È·ÙÚÈ΋ 2008;71:166-170
∂ÂÍËÁ‹ÛÂȘ ∂ÈÎfiÓ·˜ 1
1. HepB = ∞Ó·Û˘Ó‰˘·Ṳ̂ÓÔ ÂÌ‚fiÏÈÔ Î·Ù¿ Ù˘ ∏·Ù›Ùȉ·˜ µ.
1·. ∏ 1Ë ‰fiÛË ÙÔ˘ HepB ¯ÔÚËÁÂ›Ù·È ·Ì¤Ûˆ˜ ÌÂÙ¿ ÙË Á¤ÓÓËÛË ÌfiÓÔÓ fiÙ·Ó Ë ÌËÙ¤Ú· Â›Ó·È ÊÔÚ¤·˜ ÙÔ˘ ÂÈÊ·ÓÂÈ·ÎÔ‡ ·ÓÙÈÁfiÓÔ˘
(HBsAg) ‹ fiÙ·Ó Â›Ó·È ¿ÁÓˆÛÙÔ ·Ó Ë ÌËÙ¤Ú· Â›Ó·È ÊÔÚ¤·˜ ‹ fi¯È. ™ÙËÓ ÂÚ›ÙˆÛË ·˘Ù‹ ·Ó·ÁηÛÙÈο Ë 1Ë ‰fiÛË ÙÔ˘ HepB ¯ÔÚËÁ›-
Ù·È ˆ˜ ÌÔÓÔ‰‡Ó·ÌÔ ÂÌ‚fiÏÈÔ.
1‚. ™ÙËÓ ÂÚ›ÙˆÛË Ô˘ Ë 1Ë ‰fiÛË ¯ÔÚËÁÂ›Ù·È ·Ì¤Ûˆ˜ ÌÂÙ¿ ÙË Á¤ÓÓËÛË, Ô ‚·ÛÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÂÚÈÏ·Ì‚¿ÓÂÈ Û˘ÓÔÏÈο 4
‰fiÛÂȘ ·ÓÙ› ÁÈ· 3 ‰fiÛÂȘ (Ë 2Ë ÛÙÔ Ù¤ÏÔ˜ ÙÔ˘ 1Ô˘ Ì‹Ó· Î·È Ë 3Ë ÛÙÔ Ù¤ÏÔ˜ ÙÔ˘ 2Ô˘ Ì‹Ó·). ∆Ô ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· ÌÂٷ͇ 1˘
Î·È 2˘ ηıÒ˜ Î·È 2˘ Î·È 3˘ ‰fiÛ˘ Â›Ó·È 4 ‚‰ÔÌ¿‰Â˜. ∆Ô ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· ÌÂٷ͇ ÚÔÙÂÏÂ˘Ù·›·˜ (3˘) Î·È ÙÂÏÂ˘Ù·›-
·˜ (4˘) ‰fiÛ˘ ÙÔ˘ ‚·ÛÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Â›Ó·È 8-16 ‚‰ÔÌ¿‰Â˜ Î·È ‰ÂÓ ¯ÔÚËÁÂ›Ù·È ÓˆÚ›ÙÂÚ· ·fi ÙËÓ ËÏÈΛ· ÙˆÓ 24 ‚‰ÔÌ¿‰ˆÓ
(6 ÌËÓÒÓ).
¶ƒ√™√Ã∏! ™Â ÂÚ›ÙˆÛË Ô˘ ÙÔ ÂÌ‚fiÏÈÔ Ù˘ ∏·Ù›Ùȉ·˜ µ ¯ÔÚËÁËı› ˆ˜ Û˘Ó‰˘·Ṳ̂ÓÔ ÂÌ‚fiÏÈÔ, Ô ÁÈ·ÙÚfi˜ Ú¤ÂÈ Ó·
ÁÓˆÚ›˙ÂÈ fiÙÈ Ù· Û˘Ó‰˘·Ṳ̂ӷ ÂÌ‚fiÏÈ· ‰ÂÓ ¯ÔÚËÁÔ‡ÓÙ·È ÚÈÓ ·fi ÙËÓ 6Ë Â‚‰ÔÌ¿‰· Ù˘ ˙ˆ‹˜. ∂Ô̤ӈ˜, ÙÔ ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· Ô˘
ÌÂÛÔÏ·‚› ·fi ÙË Á¤ÓÓËÛË, Ô˘ ¯ÔÚËÁÂ›Ù·È ÙÔ ÌÔÓÔ‰‡Ó·ÌÔ ÂÌ‚fiÏÈÔ Ù˘ ∏·Ù›Ùȉ·˜ µ, Â›Ó·È 6 ‚‰ÔÌ¿‰Â˜ ·ÓÙ› 1 Ì‹Ó·˜.
¶·Ú¿ÏÏËÏ· Ì ÙËÓ 1Ë ‰fiÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘, Û’ fiÏ· Ù· ÓÂÔÁÓ¿ ÌËÙ¤ÚˆÓ, ÊÔÚ¤ˆÓ ÙÔ˘ ÂÈÊ·ÓÂÈ·ÎÔ‡ ·ÓÙÈÁfiÓÔ˘, Î·È Ì¤Û· ÛÙȘ
ÚÒÙ˜ 12 ÒÚ˜ ÌÂÙ¿ ÙË Á¤ÓÓËÛË ¯ÔÚËÁÔ‡ÓÙ·È 0,5 ml ˘ÂÚ¿ÓÔÛ˘ ·ÓÔÛÔÛÊ·ÈÚ›Ó˘ ÁÈ· ∏·Ù›Ùȉ· µ. ∏ ¤ÓÂÛË Á›ÓÂÙ·È Û ‰È·ÊÔÚÂÙÈ-
Îfi ̤ÚÔ˜ ·’ ·˘Ùfi Ô˘ ¤ÁÈÓ (‹ ı· Á›ÓÂÈ) ÙÔ ÂÌ‚fiÏÈÔ. ŸÏ· Ù· ·È‰È¿ Ô˘ ÁÂÓÓ‹ıËÎ·Ó ·fi ÌËÙ¤Ú˜ ÊÔÚ›˜ Î·È ‹Ú·Ó ÙÔ ÂÌ‚fi-
ÏÈÔ Î·È ÙËÓ ˘ÂÚ¿ÓÔÛË ·ÓÔÛÔÛÊ·ÈÚ›ÓË Ú¤ÂÈ Ó· ÂϤÁ¯ÔÓÙ·È ÁÈ· ÂÈÊ·ÓÂÈ·Îfi ·ÓÙÈÁfiÓÔ (HBsAg) Î·È ·ÓÙÈÛÒÌ·Ù· (·ÓÙÈ-HBs)
ÛÙËÓ ËÏÈΛ· ÙˆÓ 9 ¤ˆ˜ 15 ÌËÓÒÓ.
ŸÙ·Ó Ë ÌËÙ¤Ú· Â›Ó·È ¿ÁÓˆÛÙÔ ·Ó Â›Ó·È ‹ fi¯È ÊÔÚ¤·˜ ÙÔ˘ ÂÈÊ·ÓÂÈ·ÎÔ‡ ·ÓÙÈÁfiÓÔ˘ ηٿ ÙÔÓ ÙÔÎÂÙfi Î·È ÛÙË Û˘Ó¤¯ÂÈ· ·Ô-
‰ÂȯÙ› fiÙÈ ‰ÂÓ Â›Ó·È, ·fi ÙË 2Ë ‰fiÛË Î·È ¤ÂÈÙ· ·ÎÔÏÔ˘ıÂ›Ù·È ÙÔ Û¯‹Ì· ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Ô˘ ÈÛ¯‡ÂÈ ÁÈ· Ù· ÓÂÔÁÓ¿ ÌËÙ¤ÚˆÓ
Ô˘ ‰ÂÓ Â›Ó·È ÊÔÚ›˜ ÙÔ˘ HbsAg, ‰ËÏ·‰‹ ·ÁÓÔÂ›Ù·È Ë 1Ë ‰fiÛË.
1Á. ŸÙ·Ó Ë ÌËÙ¤Ú· Â›Ó·È ·ÚÓËÙÈ΋ ÁÈ· ÂÈÊ·ÓÂÈ·Îfi ·ÓÙÈÁfiÓÔ, Ô ‚·ÛÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÂÚÈÏ·Ì‚¿ÓÂÈ 3 ‰fiÛÂȘ (‰‡Ô ·Ú¯ÈΤ˜
∏ÏÈΛ· °¤ÓÓËÛË 1 2 4 6 12 15 18 24 4-6 11-12 13-18∂Ì‚fiÏÈÔ ÌËÓfi˜ ÌËÓÒÓ ÌËÓÒÓ ÌËÓÒÓ ÌËÓÒÓ ÌËÓÒÓ ÌËÓÒÓ ÌËÓÒÓ ÂÙÒÓ ÂÙÒÓ ÂÙÒÓ
Hep B1· Hep B1‚ (1-2 ‰fiÛÂȘ) Hep B∏·Ù›Ùȉ·˜ µ (∏ep µ)1
Hep B1Á Hep B Hep B Hep B (fiϘ ÔÈ ‰fiÛÂȘ)
¢ÈÊıÂÚ›Ùȉ·˜, ∆ÂÙ¿ÓÔ˘, DTaP DTaP DTaP DTaP DTaP D∆aP2·,2‚
∫ÔηÙË (D∆aP)2
¶ÔÏÈÔÌ˘ÂÏ›Ùȉ·˜ IPV(IPV)3 IPV IPV IPV IPV
AÈÌfiÊÈÏÔ˘ Ù‡Ô˘ µ4 Hib Hib Hib Hib
MËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ C (MCC)5 MCC MCC MCC
¶Ó¢ÌÔÓÈfiÎÔÎÎÔ˘ (PCV)6 PCV PCV PCV PCV PCV (PPV)6·
πÏ·Ú¿˜, ¶·ÚˆÙ›Ùȉ·˜,MMR MMR
∂Ú˘ıÚ¿˜ (MMR)7
AÓÂÌ¢ÏÔÁÈ¿˜ (Var)8 Var Var
HPVπfi˜ ∞ÓıÚÒÈÓˆÓ ÎÔÚ›ÙÛÈ·£ËÏˆÌ¿ÙˆÓ (∏PV)9 12-15 ÂÙ.
3 ‰fiÛÂȘ
∏·Ù›Ùȉ·˜ A (Hep A)10 Hep A (2 ‰fiÛÂȘ)
º˘Ì·Ù›ˆÛ˘ (BCG)11 MantouxMantoux11·
Mantoux11‚
BCG
°Ú›Ë˜ (πNFL)12 π¡FL (ÂÙËÛ›ˆ˜)
∂ÈÎfiÓ· 1. ÃÚÔÓԉȿÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÒÓ ÁÈ· ·È‰È¿ Î·È ÂÊ‹‚Ô˘˜.------ ∆· ÂÌ‚fiÏÈ· οو ·fi ÙË ‰È·ÎÂÎÔÌ̤ÓË ÁÚ·ÌÌ‹ Û˘ÓÈÛÙÒÓÙ·È ÁÈ· ÂÈÏÂÎÙÈÎfi ÂÌ‚ÔÏÈ·ÛÌfi (‚Ϥ ÂÂÍËÁ‹ÛÂȘ Ù˘ ∂ÈÎfiÓ·˜ 1).
∂‡ÚÔ˜ ËÏÈÎÈÒÓ ‰ÈÂÓ¤ÚÁÂÈ·˜ ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡. ™ÙËÓ ·Ú¤ÓıÂÛË ·Ó·ÁÚ¿ÊÔÓÙ·È ÔÈ ‰fiÛÂȘ ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Ô˘ Á›ÓÔÓÙ·È Û’ ·˘Ùfi ÙÔ Â‡ÚÔ˜ ËÏÈ-ÎÈÒÓ, fiÙ·Ó Â›Ó·È ÂÚÈÛÛfiÙÂÚ˜ ·fi Ì›·. ∆Ô Â‡ÚÔ˜ ËÏÈÎÈÒÓ ‰ÈÂÓ¤ÚÁÂÈ·˜ ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ‰›ÓÂÈ ÙË ‰˘Ó·ÙfiÙËÙ· Ó· ¯ÚËÛÈÌÔÔÈÔ‡ÓÙ·È ÌÔ-ÓÔ‰‡Ó·Ì· ‹ ÔÏ˘‰‡Ó·Ì· (Û˘Ó‰˘·Ṳ̂ӷ) ÂÌ‚fiÏÈ· ‹/Î·È Û˘Ó‰˘·ÛÌfi˜ ÌÔÓÔ‰‡Ó·ÌˆÓ-Û˘Ó‰˘·Ṳ̂ӈÓ.∂‡ÚÔ˜ ËÏÈÎÈÒÓ ‰ÈÂÓ¤ÚÁÂÈ·˜ ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ fiÙ·Ó ·˘Ùfi˜ ‰ÂÓ ¤¯ÂÈ ÚÔËÁËı› ηٿ ÙÔ Û˘ÓÈÛÙÒÌÂÓÔ Û¯‹Ì· ˆ˜ ÚÔ˜ ÙËÓ ËÏÈΛ· Î·È ÙȘ ‰fiÛÂȘ(‚Ϥ ÂÂÍËÁ‹ÛÂȘ ¶ÈÓ¿ÎˆÓ 5 Î·È 6).
��
∂£¡π∫√ ¶ƒ√°ƒ∞ªª∞ ∂ªµ√§π∞™ªø¡ - ÃÚÔÓԉȿÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ ÁÈ· ¶·È‰È¿ Î·È ∂Ê‹‚Ô˘˜
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·167

168 ∂ıÓÈ΋ ∂ÈÙÚÔ‹ ∂Ì‚ÔÏÈ·ÛÌÒÓ
Paediatriki 2008;71:166-170
Ì ÌÂÛԉȿÛÙËÌ· 6-8 ‚‰ÔÌ¿‰ˆÓ Î·È ÌÈ· ÙÚ›ÙË Û ËÏÈΛ· 6-18 ÌËÓÒÓ Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· ·fi ÙË 2Ë ‰fiÛË 8-16 ‚‰ÔÌ¿-
‰Â˜ Î·È fi¯È ÓˆÚ›ÙÂÚ· ·fi ÙËÓ ËÏÈΛ· ÙˆÓ 6 ÌËÓÒÓ).
2. DTaP = ∂Ì‚fiÏÈÔ Î·Ù¿ Ù˘ ‰ÈÊıÂÚ›Ùȉ·˜, ÙÔ˘ ÙÂÙ¿ÓÔ˘, ÙÔ˘ ÎÔηÙË Ô˘ ÂÚȤ¯ÂÈ Ù· ÙÔÍÔÂȉ‹ (‹ ·ÙÔ͛Ә) ÙÔ˘ ÎÔÚ˘ÓÔ-
‚·ÎÙËÚȉ›Ô˘ Ù˘ ‰ÈÊıÂÚ›Ùȉ·˜ Î·È ÙÔ˘ ÎψÛÙËÚȉ›Ô˘ ÙÔ˘ ÙÂÙ¿ÓÔ˘ Î·È ÌfiÓÔ ·ÓÙÈÁfiÓ· Ù˘ µ. pertussis (fi¯È ÔÏfiÎÏËÚÔ ÙÔ ÌÈÎÚÔ-
ÔÚÁ·ÓÈÛÌfi ÓÂÎÚfi, fiˆ˜ Ù· ·Ï·ÈfiÙÂÚ· “ÔÏÔ΢ÙÙ·ÚÈο” ÂÌ‚fiÏÈ·), ÁÈ’ ·˘Ùfi Î·È Î·ÏÂ›Ù·È “·Î˘ÙÙ·ÚÈÎfi” ηٿ ÙÔ˘ ÎÔηÙË
(acellular pertussis ‹ ·P) ÂÌ‚fiÏÈÔ.
2·. TdaP = ∂Ì‚fiÏÈÔ Î·Ù¿ Ù˘ ‰ÈÊıÂÚ›Ùȉ·˜, ÙÔ˘ ÙÂÙ¿ÓÔ˘, ÙÔ˘ ÎÔηÙË, Ì ÌÈÎÚfiÙÂÚË ‰fiÛË ‰ÈÊıÂÚÈÙÈ΋˜ ·ÙÔ͛Ӣ. ™ÙË ¯Ò-
Ú· Ì·˜ ÂÚȤ¯ÂÈ Î·È IPV Î·È ‰‡Ó·Ù·È Ó· ¯ÔÚËÁËı› ̤¯ÚÈ ÙËÓ ËÏÈΛ· ÙˆÓ 18 ÂÙÒÓ. ∆Ô TdaP Û˘ÓÈÛÙ¿Ù·È Ó· Á›ÓÂÙ·È ÁÈ· ·ӷÏË-
ÙÈ΋ ‰fiÛË ÛÙËÓ ËÏÈΛ· ÙˆÓ 11-12 ÂÙÒÓ ‹ Î·È ·ÚÁfiÙÂÚ· (̤¯ÚÈ ÙËÓ ËÏÈΛ· ÙˆÓ 64 ÂÙÒÓ) ηٿ ÚÔÙ›ÌËÛË fiÙ·Ó ÛÙËÓ ÔÈÎÔÁ¤ÓÂÈ·
·ÔÎÙ¿Ù·È ÓÂÔÁ¤ÓÓËÙÔ. ™˘ÓÈÛÙ¿Ù·È Ó· ·¤¯ÂÈ 5 ¯ÚfiÓÈ· ·fi ÙÔ DTaP ‹ ÙÔ ∆d ÁÈ· ÏÈÁfiÙÂÚ˜ ÙÔÈΤ˜ ·ÓÙȉڿÛÂȘ, ÌÔÚ› fï˜
Ó· ¯ÔÚËÁËı› Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· Î·È ‰‡Ô ÂÙÒÓ. ∂¿Ó ‰ÂÓ Î˘ÎÏÔÊÔÚ› ÙÔ TdaP ÌfiÓÔ ÙÔ˘ (¯ˆÚ›˜ IPV) ¯ÔÚËÁÂ›Ù·È ÙÔ Td
ÂÓËϛΈÓ. √È ˘fiÏÔȘ ‰fiÛÂȘ ı· Â›Ó·È Î¿ı 10 ¯ÚfiÓÈ· Ì Td ÂÓËϛΈÓ.
2‚. Td = ∂Ì‚fiÏÈÔ Î·Ù¿ ÙÔ˘ ÙÂÙ¿ÓÔ˘ Î·È Ù˘ ‰ÈÊıÂÚ›Ùȉ·˜ Ì ÌÈÎÚfiÙÂÚË ‰fiÛË ‰ÈÊıÂÚÈÙÈ΋˜ ·ÙÔ͛Ӣ. ™˘ÓÈÛÙ¿Ù·È Ó· Á›ÓÂÙ·È Î¿-
ı 10 ¯ÚfiÓÈ· ÌÂÙ¿ ÙË ¯ÔÚ‹ÁËÛË ÙÔ˘ TdaP ÛÙËÓ ÂÊË‚È΋ ËÏÈΛ·. ∆Ô ÂÌ‚fiÏÈÔ ÙÔ˘ ÙÂÙ¿ÓÔ˘ ÌÔÚ› Ó· Á›ÓÂÙ·È ‰È· ‚›Ô˘ Ì ·ÛÊ¿ÏÂÈ·.
3. IPV = ∂Ó¤ÛÈÌÔ ÂÓÈÛ¯˘Ì¤ÓÔ ÂÌ‚fiÏÈÔ Î·Ù¿ Ù˘ ÔÏÈÔÌ˘ÂÏ›Ùȉ·˜.
4. Hib = ™˘˙¢Á̤ÓÔ ÂÌ‚fiÏÈÔ Î·Ù¿ ÙÔ˘ ·ÈÌfiÊÈÏÔ˘ Ù‡Ô˘ ‚. ∂¿Ó Ë ÚˆÙ½ÓË Û‡˙¢Í˘ Â›Ó·È Ë PRP-OMP (ÚˆÙÂ˚ÓÈÎfi Û‡-
ÌÏÂÁÌ· Ù˘ Â͈ÙÂÚÈ΋˜ ÌÂÌ‚Ú¿Ó˘ ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘), ÙfiÙÂ Ë 3Ë ·fi ÙȘ 3 ·Ú¯ÈΤ˜ ‰fiÛÂȘ ÌÔÚ› Ó· ·Ú·ÏËÊı› Î·È ÙÔ
Û¯‹Ì· Ó· Â›Ó·È (2Ô˜, 4Ô˜ Î·È 12Ô˜-15Ô˜ Ì‹Ó·˜).
5. MCC = ™˘˙¢Á̤ÓÔ, ÔÏ˘Û·Î¯·ÚȉÈÎfi ÂÌ‚fiÏÈÔ Î·Ù¿ ÙÔ˘ ÌËÓÈÁÁÈÙȉfiÎÔÎÎÔ˘ ÔÚÔÔÌ¿‰·˜ C. ™˘ÓÈÛÙ¿Ù·È Ë ¤Ó·ÚÍË ÂÌ‚Ô-
ÏÈ·ÛÌÔ‡ Û ËÏÈΛ· 2 ÌËÓÒÓ Î·È ·ÎÔÏÔ˘ıÂ›Ù·È Û¯‹Ì· 3 ‰fiÛÂˆÓ - ÔÈ 2 ÚÒÙ˜ ‰fiÛÂȘ Ì ÌÂÛԉȿÛÙËÌ· 2 ÌËÓÒÓ Î·È Â·Ó·ÏËÙÈ-
΋ ‰fiÛË Û ËÏÈΛ· 15-18 ÌËÓÒÓ. ™Â ÂÚ›ÙˆÛË ¤Ó·Ú͢ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Û ËÏÈΛ· >12 ÌËÓÒÓ, ·ÎÔÏÔ˘ıÂ›Ù·È Û¯‹Ì· 1 ‰fiÛ˘.
6. PCV = ¡ÂÎÚfi, Û˘˙¢Á̤ÓÔ, ÔÏ˘Û·Î¯·ÚȉÈÎfi, ÂÙ·‰‡Ó·ÌÔ ÂÌ‚fiÏÈÔ Î·Ù¿ ÙÔ˘ ÛÙÚÂÙfiÎÔÎÎÔ˘ Ù˘ Ó¢ÌÔÓ›·˜ (Ó¢ÌÔ-
ÓÈfiÎÔÎÎÔ˘). ™˘ÓÈÛÙ¿Ù·È Û’ fiÏ· Ù· ·È‰È¿ ËÏÈΛ·˜ 2-23 ÌËÓÒÓ. ∏ ÙÂÏÂ˘Ù·›· ‰fiÛË (4Ë) Á›ÓÂÙ·È Û ËÏÈΛ· ≥12 ÌËÓÒÓ. ∆Ô ÂÌ‚fiÏÈÔ
ÌÔÚ› Ó· Á›ÓÂÈ Î·È Û ÌÂÁ·Ï‡ÙÂÚË ËÏÈΛ· Î·È È‰È·›ÙÂÚ· Û ¿ÙÔÌ· Ô˘ ·Ó‹ÎÔ˘Ó Û ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ (‚Ϥ ˘ÔÛË-
ÌÂÈÒÛÂȘ 6,7 ÛÙÔ ÚfiÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÒÓ ÁÈ· ·È‰È¿ Ô˘ ‰ÂÓ ÂÌ‚ÔÏÈ¿ÛıËÎ·Ó ÛÙË ‚ÚÂÊÈ΋ ËÏÈΛ·, ¶›Ó·Î˜ 5 Î·È 6). ™ÙËÓ ÙÂ-
ÏÂ˘Ù·›· ÂÚ›ÙˆÛË, ÔÈ Â·Ó·ÏËÙÈΤ˜ ‰fiÛÂȘ ÌÔÚ› Ó· Á›ÓÔÓÙ·È Î·È Ì ÙÔ 23‰‡Ó·ÌÔ ÔÏ˘Û·Î¯·ÚȉÈÎfi ÌË Û˘˙¢Á̤ÓÔ ÂÌ‚fi-
ÏÈÔ (PPV).
6·. PPV = ªË Û˘˙¢Á̤ÓÔ, ÔÏ˘Û·Î¯·ÚȉÈÎfi ÂÌ‚fiÏÈÔ (23‰‡Ó·ÌÔ) ηٿ ÙÔ˘ ÛÙÚÂÙfiÎÔÎÎÔ˘ Ù˘ Ó¢ÌÔÓ›·˜ (Ó¢ÌÔÓÈÔ-
ÎfiÎÎÔ˘). ™˘ÓÈÛÙ¿Ù·È ÁÈ· ·ӷÏËÙÈΤ˜ ‰fiÛÂȘ Û ·È‰È¿ Ô˘ ·Ó‹ÎÔ˘Ó Û ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ ÁÈ· ÛÔ‚·Ú‹ Ó¢ÌÔ-
ÓÈÔÎÔÎÎÈ΋ Ïԛ̈ÍË (¶›Ó·Î·˜ 1), ÂÎÙfi˜ ·fi ˘ÁÈ‹ ‚Ú¤ÊË Î·È ·È‰È¿ ËÏÈΛ·˜ 2-23 ÌËÓÒÓ.
7. MMR = ∂Ì‚fiÏÈÔ Ô˘ ÂÚȤ¯ÂÈ ˙ÒÓÙ˜ ÂÍ·ÛıÂÓË̤ÓÔ˘˜ ÈÔ‡˜ Ù˘ ÈÏ·Ú¿˜, ·ÚˆÙ›Ùȉ·˜ Î·È ÂÚ˘ıÚ¿˜. ÃÔÚËÁÂ›Ù·È ÛÙËÓ ËÏÈ-
Λ· ÙˆÓ 12-15 ÌËÓÒÓ. ™˘ÓÈÛÙ¿Ù·È 2Ë ‰fiÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ÛÙËÓ ËÏÈΛ· ÙˆÓ 4-6 ÂÙÒÓ, ·ÏÏ¿ Î·È Û ÔÔÈ·‰‹ÔÙ ¿ÏÏË ËÏÈΛ·, ·Ú-
Λ Ó· ·¤¯ÂÈ 2 Ì‹Ó˜ ·fi ÙËÓ 1Ë ‰fiÛË. √ ·È‰›·ÙÚÔ˜ Ú¤ÂÈ Ó· ÂϤÁ¯ÂÈ ·Ó ¤ÁÈÓ ‹ fi¯È Ë 2Ë ‰fiÛË Î·È ·Ó fi¯È ¯ÔÚËÁÂ›Ù·È Ë 2Ë ‰fi-
ÛË Û ÔÔÈ·‰‹ÔÙ ËÏÈΛ·.
8. Var = ∂Ì‚fiÏÈÔ Ô˘ ÂÚȤ¯ÂÈ ˙ÒÓÙ· ÂÍ·ÛıÂÓË̤ÓÔ Èfi Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜. ÃÔÚËÁÂ›Ù·È Û’ fiÏ· Ù· ·È‰È¿ ÛÙËÓ ËÏÈΛ· ÙˆÓ 12-
18 ÌËÓÒÓ (ηٿ ÚÔÙ›ÌËÛË ÌÂÙ¿ ÙÔ 15Ô Ì‹Ó·), ·ÏÏ¿ Î·È Û’ ÔÔÈ·‰‹ÔÙ ¿ÏÏË ËÏÈΛ·, ÂÊfiÛÔÓ ÙÔ ¿ÙÔÌÔ ‰ÂÓ ¤¯ÂÈ ÓÔÛ‹ÛÂÈ. ™˘ÓÈ-
ÛÙ¿Ù·È 2Ë ‰fiÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ ÛÙËÓ ËÏÈΛ· ÙˆÓ 4-6 ÂÙÒÓ, ·ÏÏ¿ Î·È Û ÔÔÈ·‰‹ÔÙ ¿ÏÏË ËÏÈΛ· ·ÚΛ Ó· ·¤¯ÂÈ 2 Ì‹Ó˜ ·fi ÙËÓ
1Ë ‰fiÛË. √ ·È‰›·ÙÚÔ˜ Ú¤ÂÈ Ó· ÂϤÁ¯ÂÈ ·Ó ¤ÁÈÓ ‹ fi¯È Ë 2Ë ‰fiÛË Î·È ·Ó fi¯È ¯ÔÚËÁÂ›Ù·È Ë 2Ë ‰fiÛË Û ÔÔÈ·‰‹ÔÙ ËÏÈΛ·.
9. HPV = ∞Ó·Û˘Ó‰˘·Ṳ̂ÓÔ ÂÌ‚fiÏÈÔ Î·Ù¿ ÙÔ˘ ÈÔ‡ ÙˆÓ ·ÓıÚÒÈÓˆÓ ıËψ̿وÓ. ™‡Ìʈӷ Ì ٷ ̤¯ÚÈ ÛÙÈÁÌ‹˜ ÂÈÛÙËÌÔÓÈ-
ο ‰Â‰Ô̤ӷ, ÌÔÚ› Ó· ¯ÔÚËÁËı› ·fi ÙËÓ ËÏÈΛ· ÙˆÓ 9-26 ÂÙÒÓ. ™ÙË ¯ÒÚ· Ì·˜ Û˘ÓÈÛÙ¿Ù·È ÌfiÓÔ Û ÎÔÚ›ÙÛÈ· ËÏÈΛ·˜ 12-15
ÂÙÒÓ, ·ÏÏ¿ Î·È Û ÎÔÚ›ÙÛÈ· ËÏÈΛ·˜ 15-26 ÂÙÒÓ, Â¿Ó ‰ÂÓ ¤¯Ô˘Ó ÂÌ‚ÔÏÈ·ÛÙ› ÛÙË Û˘ÓÈÛÙÒÌÂÓË ËÏÈΛ· (¯ˆÚ›˜ Ó· ‰È·ÛÊ·Ï›˙ÂÙ·È Ë
ÚÔʇϷ͋ ÙÔ˘˜, Â¿Ó ‹‰Ë ¤¯Ô˘Ó ÌÔÏ˘Óı› ·fi Ù‡Ô ÙÔ˘ ÈÔ‡ Ô˘ ÂÚȤ¯ÂÙ·È ÛÙÔ ÂÌ‚fiÏÈÔ, ȉȷ›ÙÂÚ· ·Ó ¤¯Ô˘Ó ·ÏÏ¿ÍÂÈ 3-4 ÛÂ-
ÍÔ˘·ÏÈÎÔ‡˜ Û˘ÓÙÚfiÊÔ˘˜). ™ÙË ¯ÒÚ· Ì·˜ ΢ÎÏÔÊÔÚÔ‡Ó ‰‡Ô ÂÌ‚fiÏÈ·. ∆Ô ¤Ó· Â›Ó·È ‰È‰‡Ó·ÌÔ Î·È ÙÔ ¿ÏÏÔ ÙÂÙÚ·‰‡Ó·ÌÔ. ∫·È Ù·
‰‡Ô ÂÌ‚fiÏÈ· ÂÚȤ¯Ô˘Ó Ù· ÔÁÎÔÁfiÓ· ÛÙÂϤ¯Ë 16 Î·È 18. ∆Ô ÙÂÙÚ·‰‡Ó·ÌÔ ÂÚȤ¯ÂÈ ÂÈϤÔÓ ‰‡Ô ·ÎfiÌ· Ù‡Ô˘˜ ÈÒÓ (6 Î·È 11),
Ô˘ ·ÛÎÔ‡Ó ÚÔÛٷ٢ÙÈ΋ ‰Ú¿ÛË Î·Ù¿ ÙˆÓ ıËÏˆÌ¿ÙˆÓ (ÎÔÓ‰˘ÏˆÌ¿ÙˆÓ). ∆Ô ‰ÔÛÔÏÔÁÈÎfi Û¯‹Ì· Î·È ÁÈ· Ù· ‰‡Ô ÂÌ‚fiÏÈ· ÂÚÈ-
Ï·Ì‚¿ÓÂÈ 3 ‰fiÛÂȘ. °È· ÌÂÓ ÙÔ ‰È‰‡Ó·ÌÔ, ÔÈ ‰fiÛÂȘ Â›Ó·È 0-1-6 Ì‹Ó˜, ÂÓÒ ÁÈ· ÙÔ ÙÂÙÚ·‰‡Ó·ÌÔ Â›Ó·È 0-2-6 Ì‹Ó˜. ™Â ÂÚ›ÙˆÛË
Ô˘ ‰ÂÓ ÙËÚËı› ÙÔ ·ÎÚÈ‚¤˜ ¯ÚÔÓԉȿÁÚ·ÌÌ·, Ô ÁÈ·ÙÚfi˜ ÌÔÚ› Ó· Û˘Ó¯›ÛÂÈ ÙÔÓ ÂÌ‚ÔÏÈ·ÛÌfi, ¯ˆÚ›˜ Ó· ¯¿ÓÔÓÙ·È ÔÈ ÚÔËÁÔ‡-
ÌÂÓ˜ ‰fiÛÂȘ. ∆¤ÏÔ˜, Ë Û˘Á¯ÔÚ‹ÁËÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘ Ì ¿ÏÏ· ÂÌ‚fiÏÈ· ¤¯ÂÈ ·Ô‰Âȯı› ̤¯ÚÈ ÛÙÈÁÌ‹˜ ·ÛÊ·Ï‹˜ ÌfiÓÔ fiÛÔÓ ·ÊÔÚ¿
ÙÔ ÂÌ‚fiÏÈÔ Ù˘ ∏·Ù›Ùȉ·˜ µ.
10. Hep A = ∞‰Ú·ÓÔÔÈË̤ÓÔ ÔÏÔ΢ÙÙ·ÚÈÎfi ÂÌ‚fiÏÈÔ Î·Ù¿ Ù˘ ∏·Ù›Ùȉ·˜ ∞. ÃÔÚËÁÂ›Ù·È Û ÔÔÈ·‰‹ÔÙ ËÏÈΛ· ¿Óˆ ÙÔ˘
ÂÓfi˜ (1) ¤ÙÔ˘˜ Û 2 ‰fiÛÂȘ, Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· 6 ÌËÓÒÓ, ηıÒ˜ Î·È Û fiϘ ÙȘ ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ ÁÈ· ∏·Ù›-
Ùȉ· ∞ (¶›Ó·Î·˜ 3).
11. BCG = ∑ˆÓ ÂÍ·ÛıÂÓË̤ÓÔ ÂÌ‚fiÏÈÔ Î·Ù¿ Ù˘ Ê˘Ì·Ù›ˆÛ˘. ™‡Ìʈӷ Ì ÙȘ ÚfiÛÊ·Ù˜ Ô‰ËÁ›Â˜ Ù˘ ¢ÈÂıÓÔ‡˜ ŒÓˆÛ˘ η-
Ù¿ Ù˘ Ê˘Ì·Ù›ˆÛ˘ Î·È Ù˘ ¶·ÁÎfiÛÌÈ·˜ √ÚÁ¿ÓˆÛ˘ ÀÁ›·˜, Ë ¯ÒÚ· Ì·˜ ‰ÂÓ ÏËÚÔ› ÙȘ ÚÔ¸Ôı¤ÛÂȘ ÁÈ· ÙË ‰È·ÎÔ‹ ÙÔ˘ ·ÓÙÈ-
Ê˘Ì·ÙÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡, Ô ÔÔ›Ô˜ ÂÍ·ÎÔÏÔ˘ı› Ó· Á›ÓÂÙ·È ÛÙËÓ ËÏÈΛ· ÙˆÓ 6 ÂÙÒÓ. π‰È·›ÙÂÚË ¤ÌÊ·ÛË Ú¤ÂÈ Ó· ‰Ôı› ΢ڛˆ˜
ÛÙÔÓ ÂÌ‚ÔÏÈ·ÛÌfi ÙˆÓ ·È‰ÈÒÓ Ô˘ ·Ó‹ÎÔ˘Ó ÛÙȘ ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ (¶›Ó·Î·˜ 2). ¶·Ú¿ÏÏËÏ·, Û˘ÓÈÛÙ¿Ù·È Ì·˙ÈÎfi˜
ÚÔÏËÙÈÎfi˜ ¤ÏÂÁ¯Ô˜ Ì ‰ÂÚÌÔ·ÓÙ›‰Ú·ÛË Mantoux ÛÙȘ ËÏÈ˘ 1, 4-6 ÂÙÒÓ (ÚÈÓ ·fi ÙÔÓ ÂÌ‚ÔÏÈ·ÛÌfi Ì BCG, 11·) Î·È ÛÙ·
·ÓÂÌ‚ÔÏ›·ÛÙ· ·È‰È¿, ÛÙËÓ ËÏÈΛ· 11-12 ÂÙÒÓ (fiÙ·Ó Á›ÓÂÙ·È Ë ÂÎÙ›ÌËÛË Ù˘ ÂÌ‚ÔÏÈ·ÛÙÈ΋˜ ÙÔ˘˜ Î¿Ï˘„˘, 11‚).
12. INFL = ∞‰Ú·ÓÔÔÈË̤ÓÔ ÔÏÔ΢ÙÙ·ÚÈÎfi ‹ ·Î˘ÙÙ·ÚÈÎfi (ÙÌËÌ·ÙÈÎfi) ÂÌ‚fiÏÈÔ Î·Ù¿ Ù˘ Áڛ˘ Ô˘ Û˘ÓÈÛÙ¿Ù·È Ó· Á›ÓÂÙ·È
ÂÙËÛ›ˆ˜, Û 1 ‰fiÛË Î·È Û ËÏÈΛ· ¿Óˆ ·fi 6 ÌËÓÒÓ. ¶ÚÔ˜ ÙÔ ·ÚfiÓ, ÂӉ›ÎÓ˘Ù·È ÌfiÓÔ ÁÈ· ·È‰È¿ Ô˘ ·Ó‹ÎÔ˘Ó Û ÔÌ¿‰Â˜ ·˘-
ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ Ó· ÓÔÛ‹ÛÔ˘Ó ÛÔ‚·Ú¿ ·fi ÁÚ›Ë (¶›Ó·Î·˜ 4). ¶·È‰È¿ οو ÙˆÓ 8 ÂÙÒÓ Ô˘ ı· ÂÌ‚ÔÏÈ·ÛıÔ‡Ó ÁÈ· ÚÒÙË ÊÔ-
Ú¿ ı· ¿ÚÔ˘Ó 2 ‰fiÛÂȘ ÂÌ‚ÔÏ›Ô˘ (0,25 ml <3 ÂÙÒÓ Î·È 0,5 ml ≥3 ÂÙÒÓ) Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· 4 ‚‰ÔÌ¿‰ˆÓ.
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·168

169∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ
¶·È‰È·ÙÚÈ΋ 2008;71:166-170
¶›Ó·Î·˜ 4. ∂Ӊ›ÍÂȘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ ηٿ Ù˘ Áڛ˘
¶·ÚÔ˘Û›· ÂÓfi˜ ‹ ÂÚÈÛÛÔÙ¤ÚˆÓ ·fi ÙÔ˘˜ ·Ú·Î¿Ùˆ ÂÈ‚·Ú˘ÓÙÈÎÔ‡˜ ·Ú¿ÁÔÓÙ˜ ‹ ¯ÚfiÓÈ· ÓÔÛ‹Ì·Ù·: ñ ÕÛıÌ· ‹ ¿ÏϘ ¯ÚfiÓȘ Ó¢ÌÔÓÔ¿ıÂȘ.ñ ∫·Ú‰È·Î‹ ÓfiÛÔ˜ Ì ÛÔ‚·Ú¤˜ ηډÈÔ‰˘Ó·ÌÈΤ˜ ‰È·Ù·Ú·¯¤˜.ñ ∞ÓÔÛÔηٷÛÙÔÏ‹ (ÂÍ·ÈÙ›·˜ ÓÔÛ‹Ì·ÙÔ˜ ‹ ıÂڷ›·˜).ñ ¢Ú·ÓÔ΢ÙÙ·ÚÈ΋ ÓfiÛÔ˜ (Î·È ¿ÏϘ ·ÈÌÔÛÊ·ÈÚÈÓÔ¿ıÂȘ).ñ ¶·È‰È¿ Ô˘ ·›ÚÓÔ˘Ó ·ÛÈÚ›ÓË Ì·ÎÚÔ¯ÚfiÓÈ· (.¯. ÓfiÛÔ˜ Kawasaki) ÁÈ· Ó· ÂÏ·ÙÙˆı› Ô Î›Ó‰˘ÓÔ˜ ÂÌÊ¿ÓÈÛ˘ Û˘Ó‰ÚfiÌÔ˘ Reye
ÌÂÙ¿ ·fi ÁÚ›Ë.ñ ™·Î¯·Ú҉˘ ‰È·‚‹Ù˘ ‹ ¿ÏÏÔ ¯ÚfiÓÈÔ ÌÂÙ·‚ÔÏÈÎfi ÓfiÛËÌ·.ñ ÃÚfiÓÈ· ÓÂÊÚÔ¿ıÂÈ·.ñ ∫ÏÂÈÛÙÔ› ÏËı˘ÛÌÔ›*.ñ ∂·ÁÁÂÏ̷ٛ˜ ˘Á›·˜.ñ ∂·ÁÁÂÏ̷ٛ˜ Ô˘ ·Û¯ÔÏÔ‡ÓÙ·È Ì ԢÏÂÚÈο**.ñ ÕÙÔÌ· ËÏÈΛ·˜ 60 ÂÙÒÓ Î·È ¿Óˆ.
* ¶ÚÔÛˆÈÎfi Î·È ÂÛˆÙÂÚÈÎÔ› ÛÔ˘‰·ÛÙ¤˜ Á˘ÌÓ·Û›ˆÓ-Ï˘Î›ˆÓ, ÛÙÚ·ÙȈÙÈÎÒÓ Î·È ·ÛÙ˘ÓÔÌÈÎÒÓ Û¯ÔÏÒÓ, ÂȉÈÎÒÓ Û¯ÔÏ›ˆÓ ‹Û¯ÔÏÒÓ, ÙÚfiÊÈÌÔÈ Î·È ÚÔÛˆÈÎfi È‰Ú˘Ì¿ÙˆÓ Î.¿.** √ Èfi˜ Ù˘ Áڛ˘ ÙˆÓ Ô˘ÏÂÚÈÎÒÓ Î·ÓÔÓÈο ‰ÂÓ ÚÔηÏ› ÓfiÛËÛË ÛÙÔÓ ¿ÓıÚˆÔ. ∂›Ó·È ‰˘Ó·ÙfiÓ fï˜, Û ÂÚ›ÙˆÛË Û˘ÏÏԛ̈-͢ Ì ÙÔÓ Èfi Ù˘ Áڛ˘ ÙˆÓ ·ÓıÚÒˆÓ, Ó· ÚÔ·„ÂÈ ÌÂÙ·ÏÏ·Á̤ÓÔ˜ Èfi˜ Ô˘ Ó· ÚÔÛ‚¿ÏÏÂÈ Î·È ÙÔÓ ¿ÓıÚˆÔ. °È· ÙÔ ÏfiÁÔ ·˘Ùfi,Û˘ÓÈÛÙ¿Ù·È Ô ÂÌ‚ÔÏÈ·ÛÌfi˜ ·ÙfiÌˆÓ Ô˘ ·Û¯ÔÏÔ‡ÓÙ·È Ì ԢÏÂÚÈο.
∂›Û˘, Û˘ÓÈÛÙ¿Ù·È ÂÙ‹ÛÈÔ˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ fiÏˆÓ ÙˆÓ˘ÁÈÒÓ ·ÙfiÌˆÓ ËÏÈΛ·˜ ¿Óˆ ÙˆÓ 60 ÂÙÒÓ Î·È ÙˆÓ ·ÙfïÓÔ˘ ·Ó‹ÎÔ˘Ó Û ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘, ·ÓÂÍ·ÚÙ‹-Ùˆ˜ ËÏÈΛ·˜.
™Â ÂÚ›ÙˆÛË ·ÏÏ·Á‹˜ ÙˆÓ ÂȉËÌÈÔÏÔÁÈÎÒÓ Û˘ÓıË-ÎÒÓ (.¯. ÂȉËÌ›·, ·Ó‰ËÌ›·) ÔÈ Û˘ÛÙ¿ÛÂȘ ·ÏÏ¿˙Ô˘Ó.
ŸÏ· Ù· ·È‰È¿ Ú¤ÂÈ Ó· ÂÈÛΤÙÔÓÙ·È ÙÔ ÁÈ·ÙÚfi ÙÔ˘˜ÛÙËÓ ËÏÈΛ· ÙˆÓ 11-12 ÂÙÒÓ (Ù¤ÏÔ˜ ‰ËÌÔÙÈÎÔ‡, ¤Ó·ÚÍË ÊÔ›-ÙËÛ˘ ÛÙÔ Á˘ÌÓ¿ÛÈÔ), ÒÛÙ ӷ Á›ÓÂÙ·È ¤ÏÂÁ¯Ô˜ Ù˘ ÂÌ‚Ô-
ÏÈ·ÛÙÈ΋˜ ÙÔ˘˜ Î¿Ï˘„˘ Î·È Î·Ù·ÁÚ·Ê‹ Ù˘ ÛÙËÓ ÂȉÈ΋ ÛÂ-Ï›‰· ÙÔ˘ ·ÙÔÌÈÎÔ‡ ‚È‚ÏÈ·Ú›Ô˘ ˘Á›·˜.
∫¿ı ÛÔ‚·Ú‹ ·ÓÂÈı‡ÌËÙË ÂÓ¤ÚÁÂÈ· ÌÂÙ¿ ÙÔÓ ÂÌ‚ÔÏÈ·-ÛÌfi Ô˘ ÂÈÛËÌ·›ÓÂÈ Ô ÎÏÈÓÈÎfi˜ ÁÈ·ÙÚfi˜, Ú¤ÂÈ Ó· ·Ó·Ê¤-ÚÂÙ·È ÛÙÔÓ ∂√º (Ó· Û˘ÌÏËÚÒÓÂÙ·È Ë Î›ÙÚÈÓË Î¿ÚÙ·).
™ÙÔ˘˜ ¶›Ó·Î˜ 5 Î·È 6 Û˘ÓÔ„›˙ÂÙ·È ÙÔ ¯ÚÔÓԉȿÁÚ·Ì-Ì· ÙˆÓ ÂÌ‚ÔÏÈ·ÛÌÒÓ ÁÈ· Ù· ·È‰È¿ Ô˘ ηı˘ÛÙ¤ÚËÛ·Ó Ó·ÂÌ‚ÔÏÈ·ÛÙÔ‡Ó.
¶›Ó·Î·˜ 5. ¶ÚfiÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÒÓ ÁÈ· ·È‰È¿ ËÏÈΛ·˜ ̤¯ÚÈ 6 ÂÙÒÓ Ô˘ ‰ÂÓ ÂÌ‚ÔÏÈ¿ÛıËÎ·Ó ÛÙË Û˘ÓÈÛÙÒÌÂÓË ·fi ÙÔ ∂ıÓÈÎfi ¶Úfi-ÁÚ·ÌÌ· ËÏÈΛ·
∂Ì‚fiÏÈÔ 1Ë ‰fiÛË 2Ë ‰fiÛË 3Ë ‰fiÛË 4Ë ‰fiÛË 5Ë ‰fiÛËËÌ/Ó›· 1Ë-2Ë ËÌ/Ó›· 2Ë-3Ë ËÌ/Ó›· 3Ë-4Ë ËÌ/Ó›· 4Ë-5Ë ËÌ/Ó›·
‰fiÛË1 ‰fiÛË1 ‰fiÛË1 ‰fiÛË1
∏·Ù›Ùȉ·˜ µ (Hep B) 4 ‚‰. 3 ÌËÓ.¢ÈÊıÂÚ›Ùȉ·˜, ∆ÂÙ¿ÓÔ˘, ∫ÔηÙË (D∆aP)Ç 4 ‚‰. 4 ‚‰. 6 ÌËÓ. 3-4 ¯ÚfiÓÈ·¶ÔÏÈÔÌ˘ÂÏ›Ùȉ·˜ IPV3 4 ‚‰. 4 ‚‰. 4 ‚‰.∞ÈÌfiÊÈÏÔ˘ Ù‡Ô˘ ‚ (Hib)4 4 ‚‰. 4 ‚‰. 8 ‚‰.ªËÓÈÁÁÈÙȉÔÎfiÎÎÔ˘ C (MCC)5 4 ‚‰. 4 ‚‰. 8 ‚‰.¶Ó¢ÌÔÓÈoÎfiÎÎÔ˘ (7‰‡Ó·ÌÔ) (PCV)6 4 ‚‰. 4 ‚‰. 8 ‚‰.πÏ·Ú¿˜, ¶·ÚˆÙ›Ùȉ·˜, ∂Ú˘ıÚ¿˜ (MMR)7 4 ‚‰.∞ÓÂÌ¢ÏÔÁÈ¿˜ (Var)8 8 ‚‰.∏·Ù›Ùȉ·˜ ∞ (Hep ∞)9 6 ÌËÓ.º˘Ì·Ù›ˆÛ˘ (BCG)10
º˘Ì·ÙÈÓ·ÓÙ›‰Ú·ÛË11 (Mantoux)°Ú›Ë˜ (INFL)12 4 ‚‰.
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·169
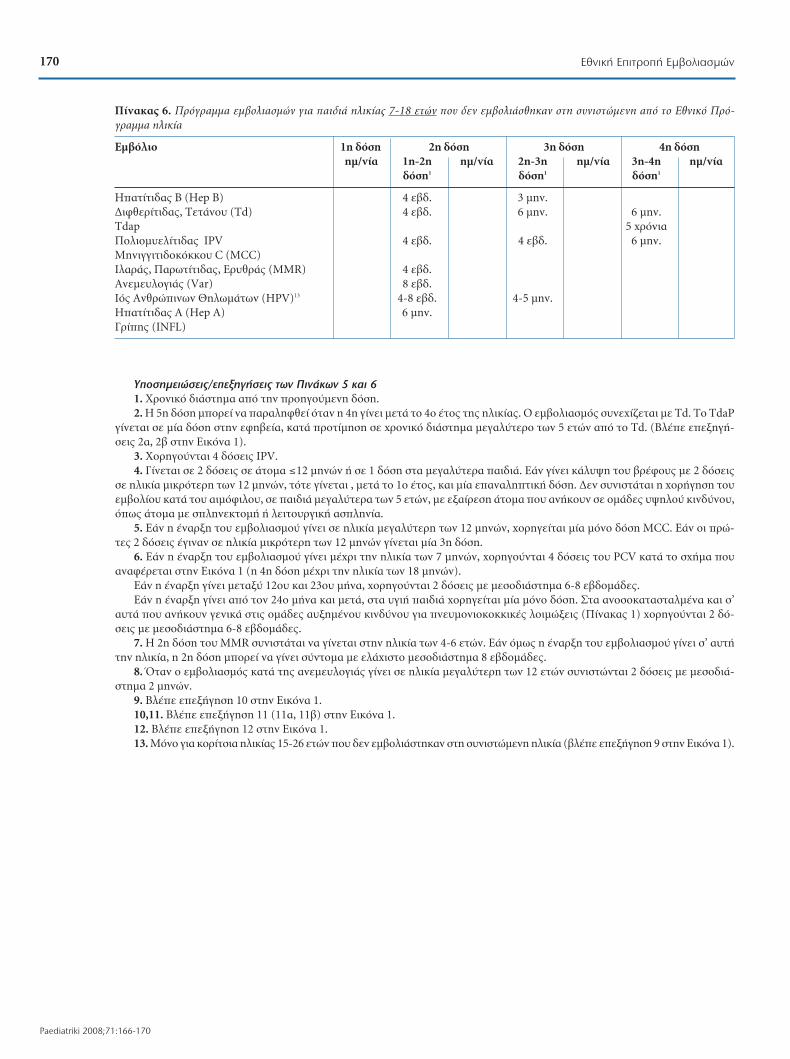
170 ∂ıÓÈ΋ ∂ÈÙÚÔ‹ ∂Ì‚ÔÏÈ·ÛÌÒÓ
Paediatriki 2008;71:166-170
ÀÔÛËÌÂÈÒÛÂȘ/ÂÂÍËÁ‹ÛÂȘ ÙˆÓ ¶ÈÓ¿ÎˆÓ 5 Î·È 6
1. ÃÚÔÓÈÎfi ‰È¿ÛÙËÌ· ·fi ÙËÓ ÚÔËÁÔ‡ÌÂÓË ‰fiÛË.2. ∏ 5Ë ‰fiÛË ÌÔÚ› Ó· ·Ú·ÏËÊı› fiÙ·Ó Ë 4Ë Á›ÓÂÈ ÌÂÙ¿ ÙÔ 4Ô ¤ÙÔ˜ Ù˘ ËÏÈΛ·˜. √ ÂÌ‚ÔÏÈ·ÛÌfi˜ Û˘Ó¯›˙ÂÙ·È Ì Td. To TdaP
Á›ÓÂÙ·È Û ̛· ‰fiÛË ÛÙËÓ ÂÊ˂›·, ηٿ ÚÔÙ›ÌËÛË Û ¯ÚÔÓÈÎfi ‰È¿ÛÙËÌ· ÌÂÁ·Ï‡ÙÂÚÔ ÙˆÓ 5 ÂÙÒÓ ·fi ÙÔ Td. (µÏ¤Â ÂÂÍËÁ‹-ÛÂȘ 2·, 2‚ ÛÙËÓ ∂ÈÎfiÓ· 1).
3. ÃÔÚËÁÔ‡ÓÙ·È 4 ‰fiÛÂȘ IPV. 4. °›ÓÂÙ·È Û 2 ‰fiÛÂȘ Û ¿ÙÔÌ· ≤12 ÌËÓÒÓ ‹ Û 1 ‰fiÛË ÛÙ· ÌÂÁ·Ï‡ÙÂÚ· ·È‰È¿. ∂¿Ó Á›ÓÂÈ Î¿Ï˘„Ë ÙÔ˘ ‚Ú¤ÊÔ˘˜ Ì 2 ‰fiÛÂȘ
Û ËÏÈΛ· ÌÈÎÚfiÙÂÚË ÙˆÓ 12 ÌËÓÒÓ, ÙfiÙ Á›ÓÂÙ·È , ÌÂÙ¿ ÙÔ 1Ô ¤ÙÔ˜, Î·È Ì›· ·ӷÏËÙÈ΋ ‰fiÛË. ¢ÂÓ Û˘ÓÈÛÙ¿Ù·È Ë ¯ÔÚ‹ÁËÛË ÙÔ˘ÂÌ‚ÔÏ›Ô˘ ηٿ ÙÔ˘ ·ÈÌfiÊÈÏÔ˘, Û ·È‰È¿ ÌÂÁ·Ï‡ÙÂÚ· ÙˆÓ 5 ÂÙÒÓ, Ì ÂÍ·›ÚÂÛË ¿ÙÔÌ· Ô˘ ·Ó‹ÎÔ˘Ó Û ÔÌ¿‰Â˜ ̆ „ËÏÔ‡ ÎÈÓ‰‡ÓÔ˘,fiˆ˜ ¿ÙÔÌ· Ì ÛÏËÓÂÎÙÔÌ‹ ‹ ÏÂÈÙÔ˘ÚÁÈ΋ ·ÛÏËÓ›·.
5. ∂¿Ó Ë ¤Ó·ÚÍË ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Á›ÓÂÈ Û ËÏÈΛ· ÌÂÁ·Ï‡ÙÂÚË ÙˆÓ 12 ÌËÓÒÓ, ¯ÔÚËÁÂ›Ù·È Ì›· ÌfiÓÔ ‰fiÛË MCC. ∂¿Ó ÔÈ ÚÒ-Ù˜ 2 ‰fiÛÂȘ ¤ÁÈÓ·Ó Û ËÏÈΛ· ÌÈÎÚfiÙÂÚË ÙˆÓ 12 ÌËÓÒÓ Á›ÓÂÙ·È Ì›· 3Ë ‰fiÛË.
6. ∂¿Ó Ë ¤Ó·ÚÍË ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Á›ÓÂÈ Ì¤¯ÚÈ ÙËÓ ËÏÈΛ· ÙˆÓ 7 ÌËÓÒÓ, ¯ÔÚËÁÔ‡ÓÙ·È 4 ‰fiÛÂȘ ÙÔ˘ PCV ηٿ ÙÔ Û¯‹Ì· Ô˘·Ó·Ê¤ÚÂÙ·È ÛÙËÓ ∂ÈÎfiÓ· 1 (Ë 4Ë ‰fiÛË Ì¤¯ÚÈ ÙËÓ ËÏÈΛ· ÙˆÓ 18 ÌËÓÒÓ).
∂¿Ó Ë ¤Ó·ÚÍË Á›ÓÂÈ ÌÂٷ͇ 12Ô˘ Î·È 23Ô˘ Ì‹Ó·, ¯ÔÚËÁÔ‡ÓÙ·È 2 ‰fiÛÂȘ Ì ÌÂÛԉȿÛÙËÌ· 6-8 ‚‰ÔÌ¿‰Â˜. ∂¿Ó Ë ¤Ó·ÚÍË Á›ÓÂÈ ·fi ÙÔÓ 24Ô Ì‹Ó· Î·È ÌÂÙ¿, ÛÙ· ˘ÁÈ‹ ·È‰È¿ ¯ÔÚËÁÂ›Ù·È Ì›· ÌfiÓÔ ‰fiÛË. ™Ù· ·ÓÔÛÔηٷÛÙ·Ï̤ӷ Î·È Û’
·˘Ù¿ Ô˘ ·Ó‹ÎÔ˘Ó ÁÂÓÈο ÛÙȘ ÔÌ¿‰Â˜ ·˘ÍË̤ÓÔ˘ ÎÈÓ‰‡ÓÔ˘ ÁÈ· Ó¢ÌÔÓÈÔÎÔÎÎÈΤ˜ ÏÔÈÌÒÍÂȘ (¶›Ó·Î·˜ 1) ¯ÔÚËÁÔ‡ÓÙ·È 2 ‰fi-ÛÂȘ Ì ÌÂÛԉȿÛÙËÌ· 6-8 ‚‰ÔÌ¿‰Â˜.
7. ∏ 2Ë ‰fiÛË ÙÔ˘ MMR Û˘ÓÈÛÙ¿Ù·È Ó· Á›ÓÂÙ·È ÛÙËÓ ËÏÈΛ· ÙˆÓ 4-6 ÂÙÒÓ. ∂¿Ó fï˜ Ë ¤Ó·ÚÍË ÙÔ˘ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Á›ÓÂÈ Û’ ·˘Ù‹ÙËÓ ËÏÈΛ·, Ë 2Ë ‰fiÛË ÌÔÚ› Ó· Á›ÓÂÈ Û‡ÓÙÔÌ· Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· 8 ‚‰ÔÌ¿‰Â˜.
8. ŸÙ·Ó Ô ÂÌ‚ÔÏÈ·ÛÌfi˜ ηٿ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜ Á›ÓÂÈ Û ËÏÈΛ· ÌÂÁ·Ï‡ÙÂÚË ÙˆÓ 12 ÂÙÒÓ Û˘ÓÈÛÙÒÓÙ·È 2 ‰fiÛÂȘ Ì ÌÂÛԉȿ-ÛÙËÌ· 2 ÌËÓÒÓ.
9. µÏ¤Â ÂÂÍ‹ÁËÛË 10 ÛÙËÓ ∂ÈÎfiÓ· 1.10,11. µÏ¤Â ÂÂÍ‹ÁËÛË 11 (11·, 11‚) ÛÙËÓ ∂ÈÎfiÓ· 1.12. µÏ¤Â ÂÂÍ‹ÁËÛË 12 ÛÙËÓ ∂ÈÎfiÓ· 1.13. ªfiÓÔ ÁÈ· ÎÔÚ›ÙÛÈ· ËÏÈΛ·˜ 15-26 ÂÙÒÓ Ô˘ ‰ÂÓ ÂÌ‚ÔÏÈ¿ÛÙËÎ·Ó ÛÙË Û˘ÓÈÛÙÒÌÂÓË ËÏÈΛ· (‚Ϥ ÂÂÍ‹ÁËÛË 9 ÛÙËÓ ∂ÈÎfiÓ· 1).
¶›Ó·Î·˜ 6. ¶ÚfiÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÒÓ ÁÈ· ·È‰È¿ ËÏÈΛ·˜ 7-18 ÂÙÒÓ Ô˘ ‰ÂÓ ÂÌ‚ÔÏÈ¿ÛıËÎ·Ó ÛÙË Û˘ÓÈÛÙÒÌÂÓË ·fi ÙÔ ∂ıÓÈÎfi ¶Úfi-ÁÚ·ÌÌ· ËÏÈΛ·
∂Ì‚fiÏÈÔ 1Ë ‰fiÛË 2Ë ‰fiÛË 3Ë ‰fiÛË 4Ë ‰fiÛËËÌ/Ó›· 1Ë-2Ë ËÌ/Ó›· 2Ë-3Ë ËÌ/Ó›· 3Ë-4Ë ËÌ/Ó›·
‰fiÛË1 ‰fiÛË1 ‰fiÛË1
∏·Ù›Ùȉ·˜ µ (Hep B) 4 ‚‰. 3 ÌËÓ.¢ÈÊıÂÚ›Ùȉ·˜, ∆ÂÙ¿ÓÔ˘ (Td) 4 ‚‰. 6 ÌËÓ. 6 ÌËÓ.Tdap 5 ¯ÚfiÓÈ·¶ÔÏÈÔÌ˘ÂÏ›Ùȉ·˜ IPV 4 ‚‰. 4 ‚‰. 6 ÌËÓ.ªËÓÈÁÁÈÙȉÔÎfiÎÎÔ˘ C (MCC)πÏ·Ú¿˜, ¶·ÚˆÙ›Ùȉ·˜, ∂Ú˘ıÚ¿˜ (MMR) 4 ‚‰.∞ÓÂÌ¢ÏÔÁÈ¿˜ (Var) 8 ‚‰.πfi˜ ∞ÓıÚÒÈÓˆÓ £ËÏˆÌ¿ÙˆÓ (HPV)13 4-8 ‚‰. 4-5 ÌËÓ.∏·Ù›Ùȉ·˜ ∞ (Hep ∞) 6 ÌËÓ.°Ú›Ë˜ (INFL)
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·170

171™À¡∆√ª∞ ¶∞π¢π∞∆ƒπ∫∞ ¡∂∞
¶·È‰È·ÙÚÈ΋ 2008;71:171-172
¶ÚÈÓ ·fi Ï›Á˜ ‚‰ÔÌ¿‰Â˜ ·Ó·ÎÔÈÓÒıËÎÂ
·fi ÙÔ ÀÔ˘ÚÁÂ›Ô ÀÁ›·˜ Î·È ∫ÔÈÓˆÓÈ΋˜
∞ÏÏËÏÂÁÁ‡Ë˜ ÙÔ “¡¤Ô ∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ·
∂Ì‚ÔÏÈ·ÛÌÒÓ” (À1.°.¶.158238, 23 π·Ó. 2008)
Ì ÙȘ Û¯ÂÙÈΤ˜ ÁÓˆÌÔ‰ÔÙ‹ÛÂȘ Ù˘ ∂ıÓÈ΋˜
∂ÈÙÚÔ‹˜ ∂Ì‚ÔÏÈ·ÛÌÒÓ. ∏ ·fiÊ·ÛË Û˘ÓÔ-
‰Â‡ÂÙ·È ·fi ¶›Ó·Î˜ Ì ¯ÚÔÓԉȷÁÚ¿ÌÌ·Ù·
‚·ÛÈÎÔ‡ ÂÌ‚ÔÏÈ·ÛÌÔ‡ Î·È ÂÌ‚ÔÏÈ·ÛÌÔ‡ ·È-
‰ÈÒÓ Ô˘ ‰ÂÓ ¤¯Ô˘Ó ÂÌ‚ÔÏÈ·Ûı› ÛÙË Û˘ÓÈÛÙÒ-
ÌÂÓË ËÏÈΛ·. ∞Ó·Ï˘ÙÈΤ˜ √‰ËÁ›Â˜ Â›Ó·È ‰È·ı¤-
ÛÈ̘ ÛÙËÓ ˘Ô˘ÚÁÈ΋ ·fiÊ·ÛË ÙÔ˘ ÀÀÎ∫∞
Î·È ÛÙËÓ ÈÛÙÔÛÂÏ›‰· ÙÔ˘ (www.mohaw.gr →
ÛÙÔ ·‡ÚÈÔ → ·Ó·ÎÔÈÓÒÛÂȘ-ÂÁ·ÎÏÈÔÈ) ηıÒ˜
Î·È ÛÙÔ ·ÚfiÓ Ù‡¯Ô˜ Ù˘ ¶∞π¢π∞∆ƒπ∫∏™.
™ÙÔ Ó¤Ô ÂıÓÈÎfi ÚfiÁÚ·ÌÌ· ÂÌ‚ÔÏÈ·ÛÌÒÓ
¤¯Ô˘Ó Á›ÓÂÈ ÛËÌ·ÓÙÈΤ˜ ·ÏÏ·Á¤˜ ÛÙ·:
∂Ì‚fiÏÈÔ ÙÔ˘ ÈÔ‡ ÙˆÓ ·ÓıÚˆ›ÓˆÓ ıËψ-
Ì¿ÙˆÓ. ¡¤Ô, ·Ó·Û˘Ó‰˘·Ṳ̂ÓÔ ÂÌ‚fiÏÈÔ. ™˘ÓÈ-
ÛÙ¿Ù·È Û ÎÔÚ›ÙÛÈ· ËÏÈΛ·˜ 12-15 ÂÙÒÓ Î·È ÛÂ
ÎÔÚ›ÙÛÈ· Î·È Á˘Ó·›Î˜ 15-26 ÂÙÒÓ, Ô˘ ‰ÂÓ
¤¯Ô˘Ó ÂÌ‚ÔÏÈ·Ûı›. ™ÙËÓ ∂ÏÏ¿‰· ΢ÎÏÔÊÔ-
ÚÔ‡Ó ¤Ó· ‰È‰‡Ó·ÌÔ (3 ‰fiÛÂȘ, 0-1-6 Ì‹Ó˜) ηÈ
¤Ó· ÙÂÙÚ·‰‡Ó·ÌÔ (3 ‰fiÛÂȘ, 0-2-6 Ì‹Ó˜).
∂Ì‚fiÏÈÔ Ù˘ ·ÓÂÌ¢ÏÔÁÈ¿˜: ÚÔÛı‹ÎË
‰Â‡ÙÂÚ˘ ‰fiÛ˘. ∏ 1Ë ‰fiÛË ¯ÔÚËÁÂ›Ù·È ÛÙËÓ
ËÏÈΛ· ÙˆÓ 12-18 ÌËÓÒÓ (ηٿ ÚÔÙ›ÌËÛË ÌÂ-
Ù¿ ÙÔ 15Ô Ì‹Ó·), ·ÏÏ¿ Î·È Û οı ¿ÏÏË ËÏÈΛ·,
ÂÊfiÛÔÓ ÙÔ ¿ÙÔÌÔ ‰ÂÓ ¤¯ÂÈ ÓÔÛ‹ÛÂÈ. ∏ 2Ë ‰fiÛË
Û˘ÓÈÛÙ¿Ù·È ÛÙËÓ ËÏÈΛ· ÙˆÓ 4-6 ÂÙÒÓ, ·ÏÏ¿ ηÈ
Û οı ¿ÏÏË ËÏÈΛ·, ·ÚΛ Ó· ·¤¯ÂÈ 2 Ì‹Ó˜
·fi ÙËÓ 1Ë ‰fiÛË.
∂Ì‚fiÏÈÔ Ù˘ Ë·Ù›Ùȉ·˜ ∞. ™˘ÓÈÛÙ¿Ù·È ÁÈ·
fiÏ· Ù· ·È‰È¿ ¿Óˆ ÙÔ˘ 1 ¤ÙÔ˘˜. ÃÔÚËÁÂ›Ù·È ÛÂ
ÔÔÈ·‰‹ÔÙ ËÏÈΛ· ¿Óˆ ÙÔ˘ 1 ¤ÙÔ˘˜ Û 2 ‰fi-
ÛÂȘ Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· 6 ÌËÓÒÓ.
∂Ì‚fiÏÈÔ ‰ÈÊıÂÚ›Ùȉ·˜-ÙÂÙ¿ÓÔ˘-ÎÔηÙË
ÁÈ· ÂÊ‹‚Ô˘˜. ∂ÈÛ·ÁˆÁ‹ ÙÔ˘ ∆daP ÁÈ· Ù· ·È-
‰È¿ Î·È ÙÔ˘˜ ÂÊ‹‚Ô˘˜ ¿Óˆ ÙˆÓ 11 ÂÙÒÓ. ∆Ô
TdaP ÂÚȤ¯ÂÈ ÌÈÎÚfiÙÂÚË ‰fiÛË ÙÔÍÔÂȉԇ˜ Ù˘
‰ÈÊıÂÚ›Ùȉ·˜ ·fi ÙÔ DTaP. ∆· ÂÌ‚fiÏÈ· TdaP
Ô˘ ‰È·Ù›ıÂÓÙ·È ÛÙËÓ ∂ÏÏ¿‰· ÂÚȤ¯Ô˘Ó ηÈ
IPV Î·È ¯ÔÚËÁÂ›Ù·È ˆ˜ ÙËÓ ËÏÈΛ· ÙˆÓ 18 ÂÙÒÓ.
™˘ÓÈÛÙ¿Ù·È 1 ·ӷÏËÙÈ΋ ‰fiÛË TdaP ÛÙËÓ
ËÏÈΛ· ÙˆÓ 12 ÂÙÒÓ ‹ Î·È ·ÚÁfiÙÂÚ· (¤ˆ˜ ÙËÓ
ËÏÈΛ· ÙˆÓ 64 ÂÙÒÓ), ηٿ ÚÔÙ›ÌËÛË fiÙ·Ó
ÛÙËÓ ÔÈÎÔÁ¤ÓÂÈ· ˘¿Ú¯ÂÈ ÓÂÔÁ¤ÓÓËÙÔ. ™˘ÓÈ-
ÛÙ¿Ù·È ÌÂÛԉȿÛÙËÌ· 5 ÂÙÒÓ ·fi ÙÔ DTaP ‹
ÙÔ Td ÁÈ· ÏÈÁfiÙÂÚ˜ ÙÔÈΤ˜ ·ÓÙȉڿÛÂȘ, ÌÔ-
Ú› fï˜ Ó· ¯ÔÚËÁËı› Î·È Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛÔ-
‰È¿ÛÙËÌ· 2 ÂÙÒÓ. ∂¿Ó ‰ÂÓ ‰È·Ù›ıÂÙ·È ÙÔ TdaP
ÌfiÓÔ ÙÔ˘ (¯ˆÚ›˜ IPV) ¯ÔÚËÁÂ›Ù·È ÙÔ Td ÂÓËÏ›-
ΈÓ. √È ˘fiÏÔȘ ‰fiÛÂȘ Á›ÓÔÓÙ·È Ì Ì Td
ÂÓËÏ›ÎˆÓ ·Ó¿ 10ÂÙ›·.
∂Ì‚fiÏÈÔ Ù˘ Ë·Ù›Ùȉ·˜ µ. ªËÙ¤Ú·
HBsAg(+), ‰ËÏ·‰‹ ÊÔÚ¤·˜ ÙÔ˘ ·ÓÙÈÁfiÓÔ˘ ÂÈ-
Ê·Ó›·˜ ‹ ÌËÙ¤Ú· Ì ¿ÁÓˆÛÙË Î·Ù¿ÛÙ·ÛË
HBsAg: Ô ‚·ÛÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ ÂÚÈÏ·Ì‚¿ÓÂÈ
4 ‰fiÛÂȘ: Ë 1Ë Á›ÓÂÙ·È ·Ì¤Ûˆ˜ ÌÂÙ¿ ÙË Á¤ÓÓËÛË
(ˆ˜ ÌÔÓÔ‰‡Ó·ÌÔ ÂÌ‚fiÏÈÔ, ÔÏ˘‰‡Ó·Ì· ‰ÂÓ
¯ÔÚËÁÔ‡ÓÙ·È ÚÈÓ ·fi ÙËÓ 6Ë Â‚‰ÔÌ¿‰· ˙ˆ‹˜)
Ë 2Ë ÛÙÔ Ù¤ÏÔ˜ ÙÔ˘ 1Ô˘ Ì‹Ó·, Ë 3Ë ÛÙÔ Ù¤ÏÔ˜
ÙÔ˘ 2Ô˘ Ì‹Ó· Î·È Ë 4Ë ÛÙÔ˘˜ 6-18 Ì‹Ó˜ ˙ˆ‹˜
(ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· ÌÂٷ͇ 1˘-2˘ ηÈ
2˘-3˘ ‰fiÛ˘: 4 ‚‰ÔÌ¿‰Â˜ Î·È ÌÂٷ͇ 3˘-
4˘ ‰fiÛ˘: 8 ‚‰ÔÌ¿‰Â˜). ™Â fiÏ· Ù· ÓÂÔÁÓ¿
ÌËÙ¤ÚˆÓ HBsAg(+) ¯ÔÚËÁ›ٷÈ, ·Ú¿ÏÏËÏ· ÌÂ
ÙËÓ 1Ë ‰fiÛË ÙÔ˘ ÂÌ‚ÔÏ›Ô˘, ˘ÂÚ¿ÓÔÛË ·ÓÔÛÔ-
ÛÊ·ÈÚ›ÓË Ë·Ù›Ùȉ·˜ µ (0,5 ml, ÛÙȘ 12 ÚÒÙ˜
AÏÏËÏÔÁÚ·Ê›·:
∂ÌÌ·ÓÔ˘‹Ï °·Ï·Ó¿Î˘[email protected]¶·È‰È·ÙÚÈ΋ ∫ÏÈÓÈ΋¶·ÓÂÈÛÙËÌ›Ô˘ ∫Ú‹Ù˘
∂ıÓÈÎfi ¶ÚfiÁÚ·ÌÌ· ∂Ì‚ÔÏÈ·ÛÌÒÓ 2008
∂. °·Ï·Ó¿Î˘
Pediatri Mar-Apr 08 08-04-08 12:26 ™ÂÏ›‰·171

172 PAEDIATRIC NEWS IN BRIEF
Paediatriki 2008;71:171-172
ÒÚ˜ ÌÂÙ¿ ÙË Á¤ÓÓËÛË, Û ‰È·ÊÔÚÂÙÈÎfi ÛËÌ›Էfi ÙÔ ÂÌ‚fiÏÈÔ). ∆· ·È‰È¿ ·˘Ù¿ Ú¤ÂÈ Ó·ÂϤÁ¯ÔÓÙ·È ÁÈ· HBsAg Î·È ·ÓÙÈ-HBs ÛÙËÓ ËÏÈ-Λ· ÙˆÓ 9-15 ÌËÓÒÓ. ∞Ó Î·Ù¿ ÙÔÓ ÙÔÎÂÙfi Ë ÌË-Ù¤Ú· Â›Ó·È ¿ÁÓˆÛÙÔ ·Ó Â›Ó·È ‹ fi¯È ÊÔÚ¤·˜HBsAg Î·È ·ÎÔÏÔ‡ıˆ˜ ·Ô‰Âȯı› fiÙÈ ‰ÂÓ Â›-Ó·È, ÙfiÙ ÙÔ ÓÂÔÁÓfi ·ÎÔÏÔ˘ı› ÙÔ Û¯‹Ì· ÂÌ‚Ô-ÏÈ·ÛÌÔ‡ ÁÈ· Ù· ÓÂÔÁÓ¿ ÌËÙ¤ÚˆÓ HBsAg(-), ‰Ë-Ï·‰‹ ·ÁÓÔÂ›Ù·È Ë 1Ë ‰fiÛË.
ªËÙ¤Ú· HBsAg(-): o ‚·ÛÈÎfi˜ ÂÌ‚ÔÏÈ·ÛÌfi˜ÂÚÈÏ·Ì‚¿ÓÂÈ 3 ‰fiÛÂȘ (ÌÂÛԉȿÛÙËÌ· 6-8
‚‰ÔÌ¿‰ˆÓ ÌÂٷ͇ 1˘ Î·È 2˘ ‰fiÛ˘ Î·È Ë 3ËÛÙÔ˘˜ 6-18 Ì‹Ó˜, Ì ÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ·8 ‚‰ÔÌ¿‰ˆÓ ·fi ÙË 2Ë ‰fiÛË).
∂Ì‚fiÏÈÔ ÁÈ· ÙË ÁÚ›Ë. ∂Í·ÎÔÏÔ˘ı› Ó· Û˘-ÓÈÛÙ¿Ù·È ÌfiÓÔ Û ÔÌ¿‰Â˜ ÏËı˘ÛÌÔ‡ ˘„ËÏÔ‡ÎÈÓ‰‡ÓÔ˘ ÌÂÙ¿ ÙËÓ ËÏÈΛ· ÙˆÓ 6 ÌËÓÒÓ, Û 1 ‰fi-ÛË ÂÙËÛ›ˆ˜. ™Â ·È‰È¿ οو ÙˆÓ 8 ÂÙÒÓ Ô˘ ÂÌ-‚ÔÏÈ¿˙ÔÓÙ·È ÁÈ· ÚÒÙË ÊÔÚ¿ Á›ÓÔÓÙ·È 2 ‰fiÛÂȘÂÌ‚ÔÏ›Ô˘ (<3 ÂÙÒÓ: 0,25 ml, ≥3 ÂÙÒÓ: 0,5 ml) ÌÂÂÏ¿¯ÈÛÙÔ ÌÂÛԉȿÛÙËÌ· 4 ‚‰ÔÌ¿‰ˆÓ.
Pediatri Mar-Apr 08 08-04-08 11:52 ™ÂÏ›‰·172

173¡∂∞ ∞¶√ ∆√ ¢π∞¢π∫∆À√
¶·È‰È·ÙÚÈ΋ 2008;71:173-175
™‡ÓÙÔÌ· ·È‰È·ÙÚÈο Ó¤· ÛÙÔ ‰È·‰›ÎÙ˘Ô
∫. ™ÙÂÊ·Ó›‰Ë˜
™ÙȘ ̤Ú˜ Ì·˜, ¤Ó·˜ ‰È·ÚÎÒ˜ ·˘Í·ÓfiÌÂÓÔ˜ ·ÚÈıÌfi˜ ‰ËÌÔÛȇÛÂˆÓ Ì·˜ ηٷÎχ˙ÂÈ. ∫¿ÔȘ·fi ·˘Ù¤˜ ÌÔÚ› Ó· ¤¯Ô˘Ó ¿ÌÂÛË Â›‰Ú·ÛË ÛÙËÓ Î·ıËÌÂÚÈÓ‹ Ì·˜ Ú¿ÍË. ªÂÚÈΤ˜ ÌÔÚ› Ó·Ì·˜ ‚ÔËı‹ÛÔ˘Ó ÛÙËÓ Î·Ï‡ÙÂÚË ·ÓÙÈÌÂÙÒÈÛË ·È‰ÈÒÓ Ì ۿÓÈ· ÚÔ‚Ï‹Ì·Ù·. ŸÌˆ˜ Ë ÚfiÛ‚·-ÛË Û ·˘Ù¤˜ ÙȘ Ӥ˜ ÏËÚÔÊÔڛ˜ ÌÔÚ› Ó· Â›Ó·È ‰˘Û¯ÂÚ‹˜ Î·È Ô ¯ÚfiÓÔ˜ Ì·˜ ÁÈ· ÏÂÙÔÌÂÚ‹ ÂÓË-̤ڈÛË ÂÚÈÔÚÈṲ̂ÓÔ˜. ŒÙÛÈ, ÚfiÛÊ·Ù· ¤ÁÈÓ ȉȷ›ÙÂÚ· ‰ËÌÔÊÈÏ‹˜ Ë Û˘ÓÔÙÈ΋ ·ÚÔ˘Û›·ÛË ÙˆÓ‚·ÛÈÎÒÓ ÛÙÔȯ›ˆÓ ÚfiÛÊ·ÙˆÓ ‰ËÌÔÛȇۈÓ. ∞Í›˙ÂÈ Ó· ÛËÌÂȈı› fiÙÈ Ë ÛÙ‹ÏË ÙˆÓ “™‡ÓÙÔ̈Ӷ·È‰È·ÙÚÈÎÒÓ ¡¤ˆÓ” ÙÔ˘ ÂÚÈÔ‰ÈÎÔ‡ ·Ú·Ì¤ÓÂÈ Ë ÚÒÙË ÚÔÙ›ÌËÛË ÙˆÓ ·Ó·ÁÓˆÛÙÒÓ. ∞ÚÎÂÙ¤˜ÈÛÙÔÛÂÏ›‰Â˜ ÛÙÔ ‰È·‰›ÎÙ˘Ô ÂÚȤ¯Ô˘Ó ¯Ú‹ÛÈ̘ ÏËÚÔÊÔڛ˜ ·fi ÚfiÛÊ·Ù· ¿ÚıÚ·. ª¿ÏÈÛÙ·ÔÏϤ˜ ÊÔÚ¤˜ ÛÙ¤ÏÓÔÓÙ·È Î·È Ì ËÏÂÎÙÚÔÓÈο ÌËӇ̷ٷ Ù· Û‡ÓÙÔÌ· ·È‰È·ÙÚÈο Ó¤· ÛÙÔ˘˜ Û˘Ó-‰ÚÔÌËÙ¤˜, Û˘Ó‹ıˆ˜ ¯ˆÚ›˜ ÔÈÎÔÓÔÌÈ΋ ÂÈ‚¿Ú˘ÓÛË. ŒÁÈÓ ÂÈÏÔÁ‹ ÙÂÛÛ¿ÚˆÓ ÈÛÙÔÛÂÏ›‰ˆÓ, ÔÈÔԛ˜ ¤¯Ô˘Ó ÙÔ ÌÂÁ·Ï‡ÙÂÚÔ ·ÚÈıÌfi ÂÈÛΤ„ÂˆÓ Î·È ÂÚȤ¯Ô˘Ó ÏËÚÔÊÔڛ˜ Ô˘ ÂÏ›˙ˆ fiÙÈ ı·Û·˜ ÂӉȷʤÚÔ˘Ó.
∏ ÈÛÙÔÛÂÏ›‰· “Pediatric News” - http://www.pediatricnews.com/issues
™ÙËÓ ÈÛÙÔÛÂÏ›‰· ·˘Ù‹ ÂÚÈ-Ï·Ì‚¿ÓÔÓÙ·È ÔÈ ÌËÓÈ·›Â˜ ‰ËÌÔÛÈ-‡ÛÂȘ ÙˆÓ ÙÂÏÂ˘Ù·›ˆÓ ÂÙ¿ ÂÙÒÓ.ªÈ· ÏËıÒÚ· ·fi ¯Ú‹ÛÈ̘ ÏË-ÚÔÊÔڛ˜ ·Ú¤¯ÔÓÙ·È ÛÙÔ˘˜ Û˘Ó-‰ÚÔÌËÙ¤˜. ∂›Û˘, ˘¿Ú¯Ô˘Ó ȉÈ-·›ÙÂÚ· ¯Ú‹ÛÈ̘ ÏËÚÔÊÔڛ˜ ÁÈ·ÏÔÈÌÒ‰Ë ÓÔÛ‹Ì·Ù·, ÂÌ‚ÔÏÈ·-ÛÌÔ‡˜, ·ÓÙÈÌÂÙÒÈÛË ÙÔ˘ ÂÊ‹‚Ô˘Ì ·¯˘Û·ÚΛ· Î·È ÁÈ· ¿ÏÏ· Û˘Ó‹-ıË ÚÔ‚Ï‹Ì·Ù·. π‰È·›ÙÂÚË ·Ó·ÊÔ-Ú¿ Á›ÓÂÙ·È ÛÙÔ ÌÂÙ·‚ÔÏÈÎfi Û‡Ó-‰ÚÔÌÔ, Ô˘ ÚÈÓ ·fi 10 ¯ÚfiÓÈ· ÔÈÂÚÈÛÛfiÙÂÚÔÈ ·È‰›·ÙÚÔÈ ‰ÂÓ ›-ÛÙ¢·Ó fiÙÈ Â›Ó·È Úfi‚ÏËÌ· ÛÙËӷȉÈ΋ Î·È ÂÊË‚È΋ ËÏÈΛ·. ™‹ÌÂ-Ú· ·Ó·Ê¤ÚÂÙ·È fiÙÈ ‰È·ÈÛÙÒÓÂÙ·ÈÛÙÔ 2-9% ÙˆÓ ÂÊ‹‚ˆÓ, ·Ó¿ÏÔÁ· ÌÂ
ÙÔÓ ÔÚÈÛÌfi Ô˘ ¯ÚËÛÈÌÔÔÈ›ٷÈ. ∆Ô 8% ÙˆÓ ˘¤Ú‚·ÚˆÓ Î·È ÙÔ 44% ÙˆÓ ·¯‡Û·ÚÎˆÓ ÂÊ‹‚ˆÓ·ÚÔ˘ÛÈ¿ÛÂÈ ÙÔ Úfi‚ÏËÌ· ·˘Ùfi. ∆· ÛÙÔȯ›· ·˘Ù¿ Â›Ó·È ·ÓËÛ˘¯ËÙÈο, ÂÂȉ‹ Ë ·¯˘Û·ÚΛ· ÛÙȘ̤Ú˜ Ì·˜ ¤¯ÂÈ ¿ÚÂÈ ÂȉËÌÈ΋ ‰È¿ÛÙ·ÛË. ∂›Û˘, ÙÔÓ›˙ÂÙ·È Ë ÛËÌ·Û›· Ù˘ ̤ÙÚËÛ˘ Ù˘ ÂÚÈ-̤ÙÚÔ˘ Ù˘ ÎÔÈÏÈ¿˜. ™Â ÚfiÛÊ·ÙË ÈÙ·ÏÈ΋ ÌÂϤÙË (Maffeis C. Î·È Û˘Ó., J Pediatr 2008;152:207-213)·Ó·Ê¤ÚÂÙ·È fiÙÈ Ù· ·¯‡Û·Úη ·È‰È¿ Î·È ÔÈ ¤ÊË‚ÔÈ Ì ÂÚ›ÌÂÙÚÔ ÎÔÈÏ›·˜ ÌÂÁ·Ï‡ÙÂÚË ·fi ÙËÓ90Ë ÂηÙÔÛÙÈ·›· ı¤ÛË Â›¯·Ó 13 ÊÔÚ¤˜ ÌÂÁ·Ï‡ÙÂÚË Èı·ÓfiÙËÙ· Ó· ¤¯Ô˘Ó ‰‡Ô ·Ú¿ÁÔÓÙ˜ ÎÈÓ‰‡-ÓÔ˘ ÁÈ· ÌÂÙ·‚ÔÏÈÎfi Û‡Ó‰ÚÔÌÔ. ∆· ˘¤Ú‚·Ú· ·È‰È¿ Î·È ÔÈ ¤ÊË‚ÔÈ Ì ÂÚ›ÌÂÙÚÔ ÎÔÈÏ›·˜ ÌÂÁ·Ï‡-ÙÂÚË ·fi ÙËÓ 90Ë ÂηÙÔÛÙÈ·›· ı¤ÛË Â›¯·Ó 7 ÊÔÚ¤˜ ÌÂÁ·Ï‡ÙÂÚÔ Î›Ó‰˘ÓÔ. ∆¤ÏÔ˜, Ù· ˘¤Ú‚·Ú· ·È-‰È¿ Ì ÂÚ›ÌÂÙÚÔ ÎÔÈÏ›·˜ ÌÈÎÚfiÙÂÚË ·fi ÙËÓ 90Ë ÂηÙÔÛÙÈ·›· ı¤ÛË ‰ÂÓ ·ÚÔ˘Û›·Û·Ó ÌÂÁ·Ï‡ÙÂ-ÚÔ Î›Ó‰˘ÓÔ.
AÏÏËÏÔÁÚ·Ê›·:
∫ˆÓÛÙ·ÓÙ›ÓÔ˜ ™ÙÂÊ·Ó›‰Ë˜[email protected]¡ÔÛÔÎÔÌÂ›Ô ¶·›‰ˆÓ ∞ıËÓÒÓ“¶. & ∞. ∫˘ÚÈ·ÎÔ‡”
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·173

∏ ÈÛÙÔÛÂÏ›‰· “Medscape Pediatrics” - http://www.medscape.com/pediatrics
™ÙËÓ ÈÛÙÔÛÂÏ›‰· ·˘Ù‹ ÂÚÈ-Ï·Ì‚¿ÓÔÓÙ·È Û¯ÔÏÈ·Ṳ̂Ó˜ ÂÚÈ-Ï‹„ÂȘ ÚfiÛÊ·ÙˆÓ ‰ËÌÔÛȇÛÂ-ˆÓ, ·fi„ÂȘ ÂȉÈÎÒÓ, ÂÓËÌÂÚˆÙÈο¿ÚıÚ· Ì ÂÚˆÙ‹ÛÂȘ ÁÈ· ÙËÓ ·ÍÈÔ-ÏfiÁËÛ‹ Û·˜. ∞ÚÎÂÙ¿ ÂӉȷʤÚÔÓÂ›Ó·È ÙÔ ¿ÚıÚÔ ÁÈ· ÙËÓ ·ÈÙÈÔÏÔÁ›·Î·È ÙËÓ ·ÓÙÈÌÂÙÒÈÛË Ù˘ ÈÓÔ-Ì˘·ÏÁ›·˜ ÛÙ· ·È‰È¿. ∂ÓÒ ·Ï·Èfi-ÙÂÚ· ÙÔ Úfi‚ÏËÌ· ·˘Ùfi ¯·Ú·ÎÙË-ÚÈ˙fiÙ·Ó ·fi Ì˘ÔÛÎÂÏÂÙÈÎÔ‡˜ fi-ÓÔ˘˜, ·Ó¿ÏÔÁÔ˘˜ ¿ÏÏˆÓ ÚÂ˘Ì·ÙÈ-ÎÒÓ ·ı‹ÛˆÓ, Û‹ÌÂÚ· Â›Ó·È ÁÓˆ-ÛÙfi fiÙÈ ÔÈ ·ÛıÂÓ›˜ Ì ÈÓÔÌ˘·ÏÁ›·¤¯Ô˘Ó ¯·ÌËÏfiÙÂÚÔ Ô˘‰fi fiÓÔ˘ ÛÂÛ¯¤ÛË Ì ٷ Ê˘ÛÈÔÏÔÁÈο ¿ÙÔÌ·.∞˘Ùfi ÔÊ›ÏÂÙ·È Û ·ıÔÏÔÁÈ΋ÂÂÍÂÚÁ·Û›· ÙÔ˘ fiÓÔ˘ ÛÙÔÓ
ÂÁΤʷÏÔ Î·È ÙÔ ÓˆÙÈ·›Ô Ì˘ÂÏfi (Clauw DJ, J Clin Rheumatol 2007;13:102-109). ŒÙÛÈ ÂÍËÁÂ›Ù·È Î·ÈË ıÂڷ¢ÙÈ΋ ·ÔÙ˘¯›· ÙˆÓ ÌË ÛÙÂÚÔÂȉÒÓ ·ÓÙÈÊÏÂÁÌÔÓˆ‰ÒÓ. ª¿ÏÈÛÙ· ÚfiÛÊ·Ù· ·Ó·Ê¤ÚÔ-ÓÙ·È ÂÓı·ÚÚ˘ÓÙÈο ·ÔÙÂϤÛÌ·Ù· Ì ÙË ¯Ú‹ÛË ·Ó·ÛÙÔϤˆÓ ÙˆÓ ˘Ô‰Ô¯¤ˆÓ Ù˘ ·ӷÚfiÛÏË-„˘ (dual receptor reuptake inhibitors) (Rooks DS, Curr Opin Rheumat 2007;19:111-117).
∂›Ó·È ÁÓˆÛÙfi fiÙÈ Ù· ·È‰È¿ Ì ÓÂÊÚˆÛÈÎfi Û‡Ó‰ÚÔÌÔ Û˘¯Ó¿ ·ÚÔ˘ÛÈ¿˙Ô˘Ó ˘ÔÙÚÔ¤˜ ÌÂÙ¿·fi ÈÔÁÂÓ›˜ ÏÔÈÌÒÍÂȘ ÙÔ˘ ·ÓˆÙ¤ÚÔ˘ ·Ó·Ó¢ÛÙÈÎÔ‡. ™Â ÚfiÛÊ·ÙË ÌÂϤÙË Ì ·È‰È¿ Ì ıÂÚ·-›· Û˘ÓÙ‹ÚËÛ˘ Ì Ú‰ÓÈ˙ÔÏfiÓË Û ‰fiÛË ÌÈÎÚfiÙÂÚË ·fi 0.6 mg/kg/48ˆÚÔ ‰È·ÈÛÙÒıËΠfiÙÈÙ· ·È‰È¿ Ô˘ Ì ٷ ÚÒÙ· Û˘ÌÙÒÌ·Ù· Ù˘ ›ˆÛ˘ ÙÔ˘˜ ¯ÔÚËÁ‹ıËΠηıËÌÂÚÈÓ¿ 5 mg Ú‰ÓÈ-˙ÔÏfiÓ˘ ÁÈ· 7 ̤Ú˜ ·ÚÔ˘Û›·Û·Ó Û·ÓÈfiÙÂÚ· (18% Û ۯ¤ÛË Ì 48%) ˘ÔÙÚÔ¤˜ Û ۯ¤ÛË Ì ٷ·È‰È¿ Ô˘ ‹Ú·Ó ÂÈÎÔÓÈÎfi Ê¿ÚÌ·ÎÔ (Abeyagunawardena AS, Trompeter RS, Arch Dis Child2008;93:226-228).
∏ ÈÛÙÔÛÂÏ›‰· “Pediatrics Jwatch” - http://pediatrics.jwatch.org/
∏ ÂΉÔÙÈ΋ ÔÌ¿‰· ÙˆÓ ‰¤Î·ÁÓˆÛÙÒÓ ∞ÌÂÚÈηÓÒÓ Î·ıËÁËÙÒӷȉȷÙÚÈ΋˜ ÂÈϤÁÂÈ Î·È Û¯ÔÏÈ¿-˙ÂÈ ÂӉȷʤÚÔÓÙ· ¿ÚıÚ·, Ô˘ ÛÙ¤Ï-ÓÔÓÙ·È Î·ıËÌÂÚÈÓ¿ Ì ËÏÂÎÙÚÔÓÈοÌËӇ̷ٷ ÛÙÔ˘˜ Û˘Ó‰ÚÔÌËÙ¤˜. HÂÈÏÔÁ‹ ÙˆÓ ¿ÚıÚˆÓ Â›Ó·È ÂÍ·ÈÚÂ-ÙÈ΋ Î·È Ù· ı¤Ì·Ù· ÂӉȷʤÚÔÓÙ·.™Â ÂÓÙ·ÂÙ‹ Û˘Á¯ÚÔÓÈ΋ ÌÂϤÙË2.216 ÂÊ‹‚ˆÓ ‰È·ÈÛÙÒıËΠfiÙÈ ÔȤÊË‚ÔÈ Ô˘ ¤ÙÚˆÁ·Ó ηıËÌÂÚÈÓ¿ÚˆÈÓfi ›¯·Ó ¯·ÌËÏfiÙÂÚÔ˘˜ ‰Â›-ÎÙ˜ Ì¿˙·˜ ÛÒÌ·ÙÔ˜ Û ۯ¤ÛË ÌÂÂΛÓÔ˘˜ Ô˘ ÛÔÚ·‰Èο ›¯·ÓÚfiÁÂ˘Ì· (Timlin MT Î·È Û˘Ó.,Pediatrics 2008;121: e638). ∆· ¢-Ú‹Ì·Ù· ·˘Ù¿ ‰Â›¯ÓÔ˘Ó fiÙÈ Ë ·Ú¿-ÏË„Ë ÙÔ˘ ÚˆÈÓÔ‡ Û˘Û¯ÂÙ›˙ÂÙ·È
174
Paediatriki 2008;71:173-175
¡∂∞ ∞¶√ ∆√ ¢π∞¢π∫∆À√
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·174

175NEWS FROM THE INTERNET
¶·È‰È·ÙÚÈ΋ 2008;71:173-175
Ì ·‡ÍËÛË ÙÔ˘ ‚¿ÚÔ˘˜ ÙˆÓ ÂÊ‹‚ˆÓ, οÙÈ Ô˘ ·fi ·ÏÈ¿ ‹Ù·Ó ÁÓˆÛÙfi, fï˜ ÔÙ¤ ‰ÂÓ Â›¯Â ÂÈ-ÛÙËÌÔÓÈο ÙÂÎÌËÚȈı›.
∂ӉȷʤÚÔÓ Â›¯Â Î·È ÙÔ ¿ÚıÚÔ ÁÈ· ÙË ÛËÌ·Û›· Ù˘ ¤ÁηÈÚ˘ ‰È¿ÁÓˆÛ˘ ÙˆÓ ‰È·Ù·Ú·¯ÒÓ Ù˘ ‹-͢ Û ÂÊ‹‚Ô˘˜ Ì ·ıÔÏÔÁÈ΋ ÌËÓÔÚÚ·Á›· (Kulp JL Î·È Û˘Ó., J Pediatr Adolesc Gynecol 2008;21:27),fiˆ˜ Î·È ÙÔ ¿ÚıÚÔ ÁÈ· ÙËÓ ·ÔÙÂÏÂÛÌ·ÙÈÎfiÙËÙ· Ù˘ Û˘ÓÙËÚËÙÈ΋˜ ·ÓÙÈÌÂÙÒÈÛ˘ ÙˆÓ ‚ÚÂÊÒÓ ÌÂÁ·ÛÙÚÔÔÈÛÔÊ·ÁÈ΋ ·ÏÈÓ‰ÚfiÌËÛË, ¯ˆÚ›˜ Ó· ¯ÔÚËÁÔ‡ÓÙ·È Ê¿Ú̷η Ô˘ ÂÏ·ÙÙÒÓÔ˘Ó ÙË Á·ÛÙÚÈ΋Ô͇ÙËÙ· (Hassall E, J Pediatr 2008;152:301).
∏ ÈÛÙÔÛÂÏ›‰· “Pediatric Linx” - http://www.mdlinx.com/pediatriclinx/
™ÙËÓ ÈÛÙÔÛÂÏ›‰· ·˘Ù‹ ˘ÔÛÙË-Ú›˙ÂÙ·È fiÙÈ Ì›· ηıËÌÂÚÈÓ‹ ÂÓÙ¿-ÏÂÙË Â›Û΄‹ Ù˘ ·ÚΛ ÁÈ· ÙËÓÂÓË̤ڈۋ Û·˜. ™Â ·˘Ù¿ Ù· ¤ÓÙÂÏÂÙ¿ ÂÓÙÔ›ÛÙËÎ·Ó ÂӉȷʤÚÔ-ÓÙ· ÛÙÔȯ›· ÁÈ· ÙËÓ ·ÓÙÈÌÂÙÒÈÛËÙÔ˘ ·È‰ÈÔ‡ Ì ÙÚ·¯ËÏÈ΋ ÏÂÌÊ·-‰ÂÓ›Ùȉ·, ÓÂfiÙÂÚ· ‰Â‰Ô̤ӷ ÁÈ·ÙËÓ ÔÍ›· ÏÂÌÊÔ‚Ï·ÛÙÈ΋ Ï¢¯·È-Ì›·, ÙÔÓ ÙÚfiÔ Ì ÙÔÓ ÔÔ›Ô ·ÓÙÈ-Ï·Ì‚¿ÓÔÓÙ·È ÔÈ ¤ÊË‚ÔÈ ÙËÓ ·¯˘-Û·ÚΛ·, ÁÈ· ÙËÓ Ë·ÙÈ΋ ÌÂÙ·Ìfi-Û¯Â˘ÛË Î·È ÁÈ· ÙËÓ Â›‰Ú·ÛË Ù˘ÌÔ˘ÛÈ΋˜ ÛÙÔ ¿Á¯Ô˜ ÙˆÓ ·È‰ÈÒÓÔ˘ ˘Ô‚Ï‹ıËÎ·Ó Û ÂÂÌ‚¿ÛÂȘ.√È ÏËÚÔÊÔڛ˜ ·˘Ù¤˜ ‹Ù·Ó ·ÚÎÂ-Ù¿ Û˘ÓÔÙÈΤ˜ Î·È ‹Ù·Ó ··Ú·›ÙË-ÙË Ë ·Ó¿ÁÓˆÛË ÙˆÓ ¿ÚıÚˆÓ. ŒÙÛÈ
Ù· ¤ÓÙ ÏÂÙ¿ ¤ÊÙ·Ó·Ó ÌfiÓÔ ÁÈ· ÙËÓ ÂÓÙfiÈÛË ÂӉȷÊÂÚfiÓÙˆÓ ıÂÌ¿ÙˆÓ Î·È ¯ÚÂÈ¿ÛÙËΠÂÚÈÛÛfi-ÙÂÚË ÒÚ· ÁÈ· ÙËÓ ·ÍÈÔÏfiÁËÛË ÙÔ˘ ÂÚȯÔ̤ÓÔ˘ ÙÔ˘˜.
Pediatri Mar-Apr 08 08-04-08 11:34 ™ÂÏ›‰·175

176 ∫§π¡π∫√ ∫√Àπ∑
Paediatriki 2008;71:165,176
∫ÏÈÓÈÎfi QUIZ
∞¶∞¡∆∏™∏
√ ‰È·ÁÓˆÛÙÈÎfi˜ ¯ÂÈÚÈÛÌfi˜ ÂÚÈÏ¿Ì‚·ÓÂÙËÓ ·Ê‡ÓÈÛË ÙÔ˘ ÓÂÔÁÓÔ‡ ηٿ ÙË ‰È¿ÚÎÂÈ·ÂÓfi˜ ÂÂÈÛÔ‰›Ô˘ Ô˘ ›¯Â ˆ˜ ·ÔÙ¤ÏÂÛÌ· ÙˉȷÎÔ‹ ÙÔ˘. ∞˘Ùfi Â›Ó·È ÙÔ Î‡ÚÈÔ ‰È·ÁÓˆÛÙÈÎfiÎÚÈÙ‹ÚÈÔ ÁÈ· ÙȘ ηÏÔ‹ıÂȘ Ì˘ÔÎÏÔӛ˜ ‡ÓÔ˘ÙˆÓ ÓÂÔÁÓÒÓ (∫ªÀ¡), ÓÔÛÔÏÔÁÈ΋ ÔÓÙfiÙËÙ·Ô˘ ·ÔÙÂÏ› ÙË ‰È¿ÁÓˆÛË ÛÙËÓ ÚÔÎÂÈ̤ÓËÂÚ›ÙˆÛË.
√È ∫ªÀ¡ ÂÚÈÁÚ¿ÊËÎ·Ó ·fi ÙÔ˘˜ CoulterÎ·È Allen ÙÔ 1982 (1). ÷ڷÎÙËÚ›˙ÔÓÙ·È ·fi Ì˘Ô-ÎÏÔÓÈο ÙÈÓ¿ÁÌ·Ù· (jerks) Ô˘ ÂÌÊ·Ó›˙ÔÓÙ·È·fi ÙȘ ÚÒÙ˜ ̤Ú˜ Ù˘ ˙ˆ‹˜ (1Ë ˆ˜ Î·È 16Ë̤ڷ) (2), Û˘Ì‚·›ÓÔ˘Ó ÌfiÓÔ Î·Ù¿ ÙÔÓ ‡ÓÔ Î·ÈÛÙ·Ì·ÙÔ‡Ó Ì ÙËÓ ·Ê‡ÓÈÛË. √È Ì˘ÔÎÏÔӛ˜ ›-Ó·È Û˘Ó‹ıˆ˜ ·ÌÊÔÙÂÚfiÏ¢Ú˜ Î·È ·ÊÔÚÔ‡Ó΢ڛˆ˜ Ù· ¿Óˆ, ·ÏÏ¿ Î·È Ù· οو ¿ÎÚ·. ¢È·Ú-ÎÔ‡Ó Ï›Á· ‰Â˘ÙÂÚfiÏÂÙ· ˆ˜ Î·È 20 ÏÂÙ¿ ηÈÌÔÚ› Ó· ·ӷϷ̂¿ÓÔÓÙ·È ÌÂÚÈΤ˜ ÊÔÚ¤˜ ÙÔ24ˆÚÔ. ∂ÌÊ·Ó‹˜ ÂÎÏ˘ÙÈÎfi˜ ·Ú¿ÁÔÓÙ·˜ ÙˆÓÂÂÈÛÔ‰›ˆÓ, ¤Ú·Ó ÙÔ˘ ‡ÓÔ˘, ‰ÂÓ Â›Ó·È ÁÓˆ-ÛÙfi˜, ˆÛÙfiÛÔ, Û ϛÁ˜ ÂÚÈÙÒÛÂȘ ¤¯ÂÈ ·Ó·-ÊÂÚı› Ë ÚfiÎÏËÛË ÂÂÈÛÔ‰›ˆÓ Ì ÙÔ ıfiÚ˘‚Ô ‹Ì ÙÔ Ê¿ÛÎȈ̷ ‹ Ì ÙÔ ÎÔ‡ÓËÌ· ÙÔ˘ ÓÂÔÁÓÔ‡.∆· ÂÂÈÛfi‰È· ¤¯Ô˘Ó Û˘Ó‹ıˆ˜ ÛÔÚ·‰ÈÎfi ¯·Ú·-ÎÙ‹Ú·, ˘¿Ú¯Ô˘Ó fï˜ ‰ËÌÔÛȇÛÂȘ ÁÈ· ÙËÓÂÌÊ¿ÓÈÛË ÂÚÈÛÛfiÙÂÚˆÓ ÙÔ˘˜ ÂÓfi˜ ÂÚÈÛÙ·ÙÈ-ÎÒÓ ÛÙËÓ ›‰È· ÔÈÎÔÁ¤ÓÂÈ· (3). ∏ Ó¢ÚÔÊ˘ÛÈÔÏÔ-ÁÈ΋ ‚¿ÛË ÙÔ˘ Ê·ÈÓÔ̤ÓÔ˘ Â›Ó·È ·Û·Ê‹˜. ∞˘ÙfiÔ˘ ¤¯ÂÈ Á›ÓÂÈ ÁÓˆÛÙfi, Ì ÙË ‚Ô‹ıÂÈ· ÔÏ˘ÁÚ·-Ê‹Ì·ÙÔ˜ ‡ÓÔ˘, Â›Ó·È fiÙÈ Ù· ÂÂÈÛfi‰È· Û˘Ì‚·›-ÓÔ˘Ó ÛÙË ‰È¿ÚÎÂÈ· ÙÔ˘ ‹ÚÂÌÔ˘ ‡ÓÔ˘ (quietsleep) ÙˆÓ ÓÂÔÁÓÒÓ (4), Ô˘ ·ÔÙÂÏ› ÙÔ ÈÛÔ‰‡-Ó·ÌÔ ÙÔ˘ NREM (Non Rapid Eye Movement)‡ÓÔ˘ ÙˆÓ ÂÓËϛΈÓ. ∞fi ÙÔ˘˜ ÂÚÈÛÛfiÙÂÚÔ˘˜Û˘ÁÁÚ·Ê›˜ ˘ÔÛÙËÚ›˙ÂÙ·È fiÙÈ Ù· ÂÂÈÛfi‰È· ·-ڷ̤ÓÔ˘Ó ˆ˜ ÙÔ˘˜ 3 Ì‹Ó˜ ˙ˆ‹˜ Î·È ˘Ô¯ˆÚÔ‡ÓÛÙË Û˘Ó¤¯ÂÈ·. √ ¯ÚfiÓÔ˜ ·˘Ùfi˜ Û˘Ì›ÙÂÈ Ì ÙËӈڛ̷ÓÛË ÙˆÓ ÛÙ·‰›ˆÓ ÙÔ˘ ‡ÓÔ˘ ÙÔ˘ ‚Ú¤ÊÔ˘˜Î·È ÙË ÛÙ·‰È·Î‹ ÂÌÊ¿ÓÈÛË ÙˆÓ Ê¿ÛÂˆÓ ‡ÓÔ˘REM (Rapid Eye Movement) Î·È NREM, Û ·ÓÙÈ-ηٿÛÙ·ÛË ÙˆÓ Ê¿ÛÂˆÓ ÙÔ˘ ÂÓÂÚÁÔ‡ (active) ηȋÚÂÌÔ˘ ‡ÓÔ˘ ÙˆÓ ÓÂÔÁÓÒÓ (5). ∆Ô Â‡ÚËÌ· ·˘Ùfi
·Ô‰›‰ÂÙ·È Û ÚÔÛˆÚÈÓ‹ ·ÓˆÚÈÌfiÙËÙ· Ù˘ ÔÚ-
Á¿ÓˆÛ˘ ÙÔ˘ ‡ÓÔ˘ ÙˆÓ ÓÂÔÁÓÒÓ. øÛÙfiÛÔ,
˘¿Ú¯Ô˘Ó ‰ËÌÔÛȇÛÂȘ Ô˘ ·Ó·Ê¤ÚÔ˘Ó Û ÔÚÈ-
Ṳ̂ӷ ‚Ú¤ÊË ÂÈÌÔÓ‹ ÙˆÓ ÂÂÈÛÔ‰›ˆÓ ̤¯ÚÈ Î·È
ÙËÓ ËÏÈΛ· ÙˆÓ 10 ÌËÓÒÓ, ¯ˆÚ›˜ fï˜ ÂÈÙÒ-
ÛÂȘ ÛÙË „˘¯ÔÎÈÓËÙÈ΋ ÙÔ˘˜ ÂͤÏÈÍË.
√È ∫ªÀ¡ Û˘Á¯¤ÔÓÙ·È Û˘¯Ó¿ Ì ۷ÛÌÔ‡˜,
·ÎfiÌ· Î·È Ì status epilepticus, ÌÔÏÔÓfiÙÈ ‰ÂÓ
ÚfiÎÂÈÙ·È ÁÈ· ÂÈÏËÙÈÎfi Ê·ÈÓfiÌÂÓÔ (6). ∏ ·Ó·-
ÁÓÒÚÈÛ‹ ÙÔ˘˜ ¤¯ÂÈ È‰È·›ÙÂÚË ÛËÌ·Û›· ÁÈ· ÙËÓ
·ÔÊ˘Á‹ Ù˘ ·Ó·›ÙÈ·˜ ·ÓËÛ˘¯›·˜ ÙˆÓ ÁÔÓ¤ˆÓ,
Ù˘ ·‰ÈηÈÔÏfiÁËÙ˘ Ú·ÁÌ·ÙÔÔ›ËÛ˘ ÂÍÂȉÈ-
ÎÂ˘Ì¤ÓˆÓ ‰È·ÁÓˆÛÙÈÎÒÓ ÂÍÂÙ¿ÛˆÓ, ·ÏÏ¿ ΢-
Ú›ˆ˜ ÁÈ· ÙËÓ ·ÔÊ˘Á‹ ¯ÔÚ‹ÁËÛ˘ ·ÓÙÈÂÈÏËÙÈ-
ÎÒÓ Ê·Ú̿ΈÓ, Ù· ÔÔ›· ÌÔÚ› Ó· ÚÔηϤ-
ÛÔ˘Ó ˘ÚÔ‰fiÙËÛË Ó¤ˆÓ ÂÂÈÛÔ‰›ˆÓ (6). ™˘ÌÂ-
Ú·ÛÌ·ÙÈο, ÌÔÚÔ‡Ó Ó· ıˆÚËıÔ‡Ó Ì ‚‚·Èfi-
ÙËÙ· ∫ªÀ¡ ÔÈ Ì˘ÔÎÏÔӛ˜ Ô˘ ÂÌÊ·Ó›˙ÔÓÙ·È
ÛÙËÓ ÚÒÈÌË ÓÂÔÁÓÈ΋ ËÏÈΛ·, ·Ú·ÙËÚÔ‡ÓÙ·È
ÌfiÓÔ Î·Ù¿ ÙÔÓ ‡ÓÔ, ̆ Ô¯ˆÚÔ‡Ó Ì ÙËÓ ·Ê‡ÓÈ-
ÛË ÙÔ˘ ÓÂÔÁÓÔ‡ Î·È ‰ÂÓ Û˘Óԉ‡ÔÓÙ·È ·fi ËÏÂ-
ÎÙÚÔÂÁÎÂÊ·ÏÔÁÚ·ÊÈο Â˘Ú‹Ì·Ù· ÂÓ‰ÂÈÎÙÈο
ÂÈÏËÙÈÎÒÓ ÂÎÊÔÚÙ›ÛˆÓ. ∂ÊfiÛÔÓ ÏËÚÔ‡ÓÙ·È
Ù· ÎÚÈÙ‹ÚÈ· ·˘Ù¿, ‰ÂÓ Ú¤ÂÈ Ó· ‰Ôı› Ê·ÚÌ·-
΢ÙÈ΋ ·ÁˆÁ‹ ÛÙÔ ÓÂÔÁÓfi Ô‡Ù ¯ÚÂÈ¿˙ÂÙ·È Ó·
˘Ô‚ÏËı› Û ÂÚ·ÈÙ¤Úˆ ‰È·ÁÓˆÛÙÈÎfi ¤ÏÂÁ¯Ô.
µÈ‚ÏÈÔÁÚ·Ê›·
1. Coulter DL, Allen RJ. Benign neonatal sleep my-
oclonus. Arch Neurol 1982;39:191-192.
2. ParÔ-Panjan D, Neubauer D. Benign neonatal sleep
myoclonus: experience from the study of 38 infants.
Eur J Paediatr Neurol 2008;12:14-18.
3. Cohen R, Shuper A, Straussberg R. Familial benign
neonatal sleep myoclonus. Pediatr Neurol 2007;36:
334-337.
4. Di Capua M, Fusco L, Ricci S, Vigevano F. Benign
neonatal sleep myoclonus: clinical features and video-
polygraphic recordings. Mov Disord 1993;8:191-194.
5. °ÈˆÛ·Ê¿Ù ª, ™ËÊÈ·ÓÔ‡ ¶. º˘ÛÈÔÏÔÁ›· Î·È ‰È·Ù·-
Ú·¯¤˜ ÙÔ˘ ‡ÓÔ˘ ÛÙ· ·È‰È¿. π·ÙÚÈ΋ 1984;46:4-15.
6. Egger J, Grossmann G, Auchterlonie IA. Benign sleep
myoclonus in infancy mistaken for epilepsy. BMJ
2003;326:975-976.
Pediatri Mar-Apr 08 07-04-08 17:43 ™ÂÏ›‰·176

xiii¶ƒ√™∂Ã∏ ™À¡∂¢ƒπ∞
4-6 ∞ÚÈÏ›Ô˘ 2008 2Ô ¶·ÓÂÏÏ‹ÓÈÔ ™˘Ó¤‰ÚÈÔ ¡ÂÔÁÓÔÏÔÁ›·˜ ∞›ÁÏË ∑·Â›Ô˘,
¢ÈÔÚÁ¿ÓˆÛË: ∂ÏÏËÓÈ΋ ¡ÂÔÁÓÔÏÔÁÈ΋ ∂Ù·ÈÚ›· Î·È ∞ı‹Ó·
∂ÏÏËÓÈ΋ ∂Ù·ÈÚ›· ¶ÂÚÈÁÂÓÓËÙÈ΋˜ π·ÙÚÈ΋˜¶ÏËÚÔÊÔڛ˜: Triaena Tours & Congress∆ËÏ.: 0030-210-7499300Fax: 0030-210-7705752E-mail: [email protected]: http://www.neonatology2008.gr
5 ∞ÚÈÏ›Ô˘ 2008 ªÂÙÂÎ·È‰Â˘ÙÈ΋ ∏ÌÂÚ›‰· ∞›ıÔ˘Û· ∂ΉËÏÒÛˆÓ
¶·È‰È·ÙÚÈο ∂›ÁÔÓÙ· & µ·ÛÈ΋ ˘ÔÛÙ‹ÚÈÍË ∑ˆ‹˜ π·ÙÚÈÎÔ‡ ™˘ÏÏfiÁÔ˘
¢ÈÔÚÁ¿ÓˆÛË: π·ÙÚÈÎfi˜ ™‡ÏÏÔÁÔ˜ ∞ıËÓÒÓ Î·È ∂ÏÏËÓÈ΋ ∞ıËÓÒÓ, ∞ı‹Ó·
¶·È‰È·ÙÚÈ΋ ∂Ù·ÈÚ›·¶ÏËÚÔÊÔڛ˜: ∞Ó·ÛÙ¿ÛÈÔ˜ ¢. ÷Ù˙‹˜∆ËÏ.: 0030-210-7488686Website: www.isathens.gr
19 ∞ÚÈÏ›Ô˘ 2008 6Ë ∂ÈÛÙËÌÔÓÈ΋ ∏ÌÂÚ›‰· ∂˘ÚˆÎÏÈÓÈ΋˜ ¶·›‰ˆÓ •ÂÓԉԯ›Ô
“™‡Á¯ÚÔÓ· ¶·È‰È·ÙÚÈο £¤Ì·Ù·” “Royal Olympic”,
¶ÏËÚÔÊÔڛ˜: Firstevent ∞ı‹Ó·
TËÏ.: 0030-210-8228950Fax: 0030-210-8228901E-mail: [email protected]
30 ∞ÚÈÏ›Ô˘- TRANSMED 16 - European Mediterranean Syracusa, Italy
1 ª·˝Ô˘ 2008 Congress about Mother & Child Health
Contact: Kamel BargaouiTel.: 33-607-686-118Fax: 33-143-839-985E-mail: [email protected]
3-6 ª·˝Ô˘ 2008 Pediatric Academic Societies' 2008 Annual Meeting Honolulu, HI,Contact: Meeting Organiser United StatesTel.: 281-419-0052Fax: 281-419-0082E-mail: [email protected]
5-11 ª·˝Ô˘ 2008 XXIth European Society of Pediatric Neurosurgery Montreux,
(ESPN) Meeting Switzerland
Contact: Meeting OrganiserE-mail: [email protected]
9-11 ª·˝Ô˘ 2008 13Ô ¶·ÓÂÏÏ‹ÓÈÔ ™˘ÌfiÛÈÔ √ÚıԷȉÈ΋˜ ¶·›‰ˆÓ •ÂÓԉԯ›Ô
¢ÈÔÚÁ¿ÓˆÛË: ∂ÏÏËÓÈ΋ ∂Ù·ÈÚ›· ÃÂÈÚÔ˘ÚÁÈ΋˜ “Olympian Village -
√ÚıԷȉÈ΋˜ & ∆Ú·˘Ì·ÙÔÏÔÁ›·˜ - Aldemar”,
∆Ì‹Ì· √ÚıԷȉÈ΋˜ ¶·›‰ˆÓ ™Î·Êȉȿ
¶ÏËÚÔÊÔڛ˜: ∫∂°ª ∆Ô˘ÚÈÛÙÈΤ˜ & ™˘Ó‰ÚȷΤ˜ ∂ȯÂÈÚ‹ÛÂȘ ∞∂ - Congress World - ª. ¶···Ó·ÁÈÒÙÔ˘TËÏ.: 0030-210-7210052, 7210001Fax: 0030-210-7210051E-mail: info@[email protected]
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·179

xiv
10 ª·˝Ô˘ 2008 7Ë ∏ÌÂÚ›‰· ∞Ó¿Ó˄˘ «∏ ∞Ó¿ÓË„Ë ÛÙ· ·È‰È¿» ∞ÌÊÈı¤·ÙÚÔ
¢ÈÔÚÁ¿ÓˆÛË: ªÔÓ¿‰· ∂ÓÙ·ÙÈ΋˜ £Âڷ›·˜ °ÂÓÈÎÔ‡ “∫ˆÓÛÙ·ÓÙ›ÓÔ˜
¡ÔÛÔÎÔÌ›Ԣ ¶·›‰ˆÓ ∞ıËÓÒÓ «¶. & ∞. ∫˘ÚÈ·ÎÔ‡» ¶··‰¿ÙÔ˜”,
∂ÈÎÔÈÓˆÓ›·: ¶·ÙÚ›ÙÛÈ· ªfiÓÔ˘ °. ¡. ¶·›‰ˆÓ
∆ËÏ.: 210-7798033 & 2132009443 “¶. & ∞. ∫˘ÚÈ·ÎÔ‡”
15-17 ª·˝Ô˘ 2008 9th Congress of the European Society for •ÂÓԉԯ›Ô
Pediatric Dermatology “Hilton”, ∞ı‹Ó·
¢ÈÔÚÁ¿ÓˆÛË: ∂ÏÏËÓÈ΋ ∂Ù·ÈÚ›· ¶·È‰È·ÙÚÈ΋˜ ¢ÂÚÌ·ÙÔÏÔÁ›·˜& ∂˘Úˆ·˚΋ ∂Ù·ÈÚ›· ¶·È‰È·ÙÚÈ΋˜ ¢ÂÚÌ·ÙÔÏÔÁ›·˜¶ÏËÚÔÊÔڛ˜: Erasmus - ¶ËÓÂÏfiË ªËÙÚÔÁÈ¿ÓÓËTel.: 0030-210-7257693Fax: 0030-210-7257532E-mail: [email protected]
2-4 πÔ˘Ó›Ô˘ 2008 Perinatal Medicine 2008 Harrogate,
Contact: Kate Melton England,
Tel.: 02-0-89-798-300 United Kingdom
Fax: 02-0-89-796-700E-mail: [email protected]
13-15 πÔ˘Ó›Ô˘ 2008 46Ô ¶·ÓÂÏÏ‹ÓÈÔ ¶·È‰È·ÙÚÈÎfi ™˘Ó¤‰ÚÈÔ COREXPO
¶ÏËÚÔÊÔڛ˜: AC&C International ∂ÎıÂÛÈ·Îfi ∫¤ÓÙÚÔ
∆ËÏ.: 0030-210-6889130 ∫¤Ú΢ڷ˜,
Fax: 0030-210-6844777 ∫¤Ú΢ڷ
E-mail: [email protected]:www.pediatric-congress.gr
19-21 πÔ˘Ó›Ô˘ 2008 NHS 2008 - Beyond Newborn Hearing Screening: Cernobbio, Italy
Infant and Childhood Hearing in Science and
Clinical Practice
Contact: Meeting OrganiserTel.: 39-0-498-601-818Fax: 39-0-498-602-389E-mail: [email protected]
11-14 √ÎÙˆ‚Ú›Ô˘ 2008 2008 National Conference & Exhibition of the Boston, MA,
American Academy of Pediatrics United States
Contact: PediaLink Customer ServiceTel.: 866-843-2271E-mail: [email protected] / [email protected]
23-26 √ÎÙˆ‚Ú›Ô˘ 2008 31st Congress of the Union of Middle-Eastern & Tunis, Tunisia
Mediterranean Pediatric Societies
Contact: Prof. Ahmed Sahloul EssoussiTel.: +216.73.219494/221411Fax: +216.73.224899E-mail: [email protected]
24-28 √ÎÙˆ‚Ú›Ô˘ 2008 2nd Congress of the European Academy Nice, France
of Paediatrics - EAP
Contact: KENES InternationalTel: +41 22 908 0488Fax: +41 22 732 2850Email: [email protected]: www.kenes.com/paediatrics
Pediatri Mar-Apr 08 07-04-08 16:23 ™ÂÏ›‰·180
Related Documents