© 2015 Direct One Communications, Inc. All rights reserved. 1 Changes in the Default Mode Network and Functional Connectivity in Epilepsy Ambica M. Tumkur, MD Emory University School of Medicine, Atlanta, Georgia A REPORT FROM THE 68 th ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY

© 2015 Direct One Communications, Inc. All rights reserved. 1 Changes in the Default Mode Network and Functional Connectivity in Epilepsy Ambica M. Tumkur,
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© 2015 Direct One Communications, Inc. All rights reserved. 1
Changes in the Default Mode Network and Functional Connectivity in Epilepsy
Ambica M. Tumkur, MD
Emory University School of Medicine, Atlanta, Georgia
A REPORT FROM THE 68th ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
© 2015 Direct One Communications, Inc. All rights reserved. 2
Background
From 1% to 3% of the general population and greater than 2 million people suffer from epilepsy.
As many as 30% of patients with epilepsy are refractory to treatment.
The annual cost of epilepsy care in the United States totals $12.5 billion (in 2003 dollars).
New therapies for epilepsy are available, including pharmacologic therapy, surgical procedures, responsive neurostimulation (RNS), and thermal ablation.
Bernhardt BC et al. Front Hum Neurosci. 2013;7:1; Chang BS, Lowenstein DH. N Engl J Med. 2003;349:1257; Wilner AN et al. Epilepsy Behav. 2014;41:83
© 2015 Direct One Communications, Inc. All rights reserved. 3
Hot Topics at the 2014 AES Meeting
Do seizures (even infrequent ones) result in permanent brain damage?
Effects of epilepsy on structural and functional connectivity were addressed.
Dr. Jean Gotman reviewed the effect of epilepsy on the default mode network.
Dr. Andrea Bernasconi discussed the effect of seizures on neural connectivity in the brain.
A variety of studies using multimodal techniques (PET, SPECT, functional MRI with blood oxygen level–dependent signaling, MRI with diffuse tensor imaging (Dti), and EEG) were presented.

© 2015 Direct One Communications, Inc. All rights reserved. 4
Epilepsy Pathophysiology Revisited
Epilepsy traditionally has been compared with a forest fire, with seizures starting as a single “spark” (ie, a focal epileptic discharge) in one region that quickly spreads and picks up momentum, engulfing the surrounding areas.
The introduction of new imaging techniques, with greatly improved temporal and spatial resolution, has forced us to abandon this concept.
We now know that focal epileptic discharges can affect a vast array of distant interconnected networks controlling such functions as attention, cognition, and memory.

© 2015 Direct One Communications, Inc. All rights reserved. 5
Resting Mode Networks
The brain is composed of billions of neurons that synapse with each other, creating an intricate web or schema of neural connections known as functional networks.
Resting mode networks are discrete groups of neurons whose activity is synchronized while the person is at rest but become deactivated during the engagement of a task.
Biswal B et al. Magn Reson Med. 1995;34:537; Cataldi M et al. Epilepsia. 2013;54:2048

© 2015 Direct One Communications, Inc. All rights reserved. 6
Default Mode Network
The default mode network (DMN) is the most consistent and prominent resting-state network.
Positron emission tomography (PET) in normal subjects reveals different areas of deactivation in the brain during attention-demanding cognitive tasks.
Raichle ME et al. Proc Natl Acad Sci U S A. 2001;98:676

© 2015 Direct One Communications, Inc. All rights reserved. 7
Epileptic Discharges and the DMN
Five of six patients showed deactivation of BOLD and SPECT signaling in the DMN regions during seizures.
Intracranial EEG recordings from electrode contacts placed in DMN areas demonstrated decreased power of faster (g) frequencies in the DMN regions and increased d frequencies in the DMN during the course of seizures, confirming that the BOLD/SPECT signal changes correlated with changes in functional neuronal activity in the brain.
In 2013, Fahoum et al investigated the impact of epileptic discharges emerging from the temporal lobe, supplementary motor area, and temporoparietal and inferior parietal regions of the DMN.
Fahoum F et al. PLoS One. 2013;8:e68038.

© 2015 Direct One Communications, Inc. All rights reserved. 8
How Do Focal-Onset Seizures Affect Baseline Connectivity in the DMN?
Studies show that patients with temporal-lobe epilepsy demonstrate decreased neural connectivity and activation of the posterior DMN.
The extent of structural changes and connectivity problems is directly proportional to the severity and duration of the patient’s epilepsy.
Imaging shows less connectivity between the posterior cingulate cortex, the precuneus, the medial prefrontal cortex, and the medial temporal lobes in patients with mesial temporal-lobe epilepsy.
Liao W et al. Hum Brain Mapp. 2011;32:883
© 2015 Direct One Communications, Inc. All rights reserved. 9
Generalized Epilepsy and Connectivity
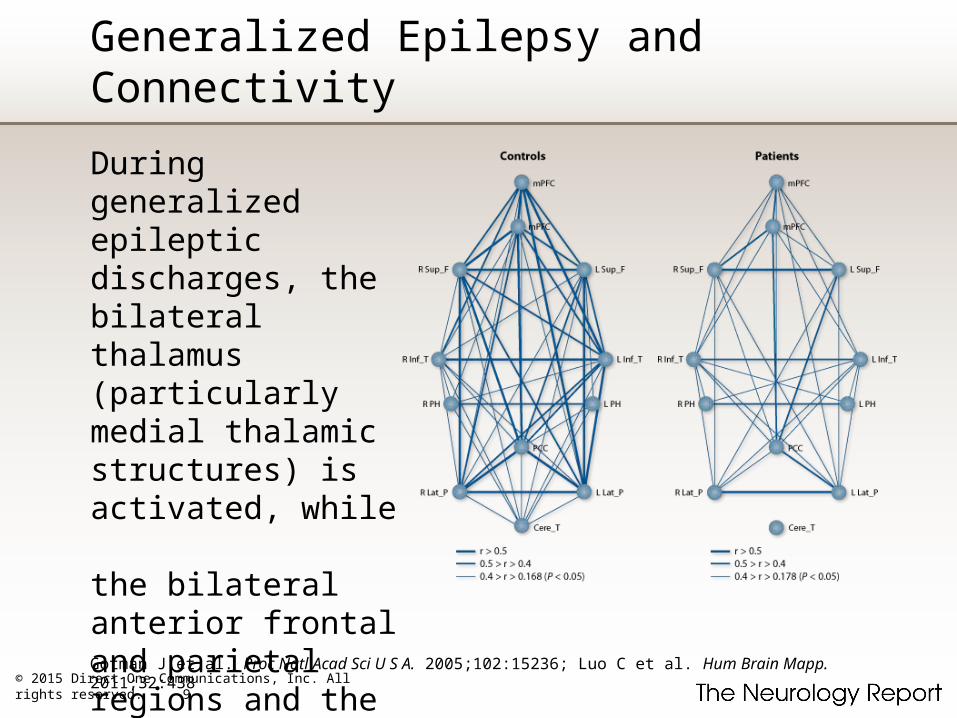
During generalized epileptic discharges, the bilateral thalamus (particularly medial thalamic structures) is activated, while the bilateral anterior frontal and parietal regions and the posterior cingulate gyrus (all portions of the DMN) are deactivated.
Gotman J et al. Proc Natl Acad Sci U S A. 2005;102:15236; Luo C et al. Hum Brain Mapp. 2011;32:438

© 2015 Direct One Communications, Inc. All rights reserved. 10
Epilepsy Treatment and Connectivity
Kay et al found that patients with generalized epilepsy whose seizures were resistant to treatment with valproate had less functional (DMN) connectivity than patients whose seizures responded to the drug.
Seizures+ = seizures uncontrolledSeizures– = seizures well controlledVPA+ = valproate responsiveVPA– = valproate unresponsive
Kay BP et al. Epilepsia. 2013;54:461
© 2015 Direct One Communications, Inc. All rights reserved. 11
Why Should We Care?
The resting mode networks, of which the DMN is a part, are believed to play a crucial role in maintaining consciousness, alertness, and cognitive function.
Disruption of the DMN has been hypothesized to at least partially account for the changes or loss in consciousness and/or awareness that many patients with focal-onset epilepsies experience.
In the generalized epilepsies, suspension and/or disruption of the DMN may dampen perceptual sensory inputs and decrease the ability of activation from the thalamus and mid-frontal regions.
© 2015 Direct One Communications, Inc. All rights reserved. 12
Why Should We Care? continued
Other resting-mode networks also seem to exhibit disruption during epileptic discharges.
These networks include the attentional networks, executive control networks, and reward networks, disruption of which may lead to the depression and attentional and problem-solving difficulties that are often seen in patients with epilepsy.
Disabilities such as memory loss and slowed cognition that once were attributed to structural defects and medication effects actually may be due, at least in part, to disruption of these resting-mode networks.
Related Documents











