The Kidney in Tuberous Sclerosis
Robert Isom, MDClinical Associate Professor
Stanford University School of Medicine
- A genetic disease with an autosomal dominant pattern of inheritance, giving rise to the formation of benign tumors (hamartomas) in multiple organ systems – brain, lung, kidney, heart, skin, eye, & others
- Autosomal dominant inheritance : only one copy of the two inherited alleles for a particular gene need to be mutated to give rise to the characteristic manifestations of disease; 50-50% chance of an affected
patient passing the disease to offspring
- 2nd somatic mutation (during a patient’s lifetime) required during a patient’s lifetime to give rise to actual lesion development (“2nd hit hypothesis” – loss of heterozygosity)
- Although autosomal dominant inheritance, the majority (2/3) of patients present with de novo, or sporadic mutations (no evidence of disease in either parent; mutation probably occurs during early embryonic development)
Tuberous Sclerosis -- Background
Epidemiology
- Affects approximately 1/6,000 live births
-Males and females affected equally
-Different races and ethnicities affected equally
Genetics and pathophysiology
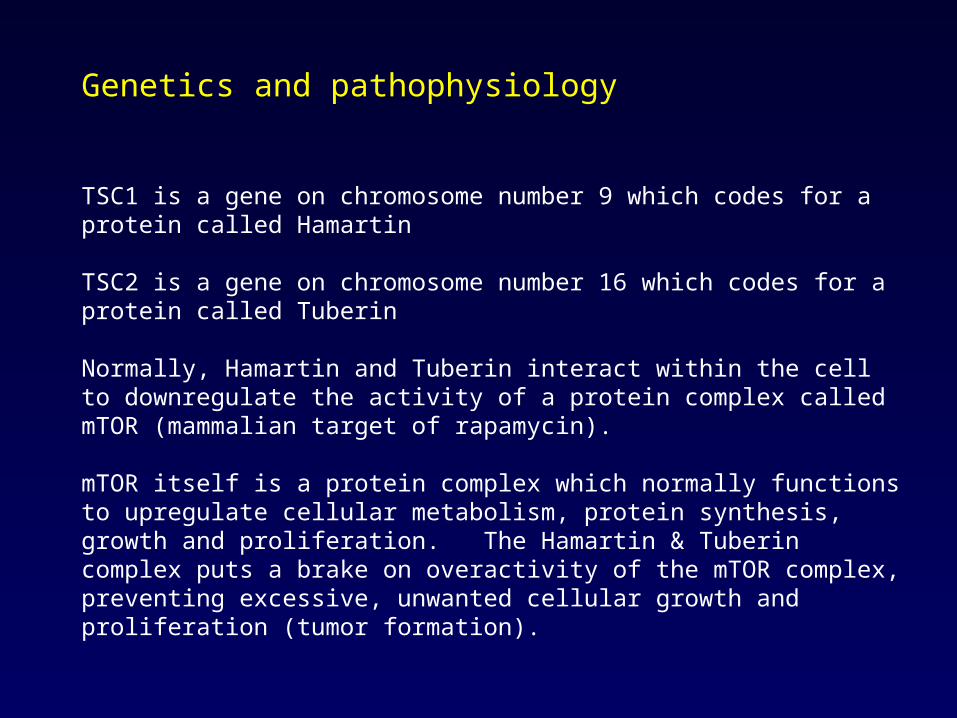
TSC1 is a gene on chromosome number 9 which codes for a protein called Hamartin
TSC2 is a gene on chromosome number 16 which codes for a protein called Tuberin
Normally, Hamartin and Tuberin interact within the cell to downregulate the activity of a protein complex called mTOR (mammalian target of rapamycin).
mTOR itself is a protein complex which normally functions to upregulate cellular metabolism, protein synthesis, growth and proliferation. The Hamartin & Tuberin complex puts a brake on overactivity of the mTOR complex, preventing excessive, unwanted cellular growth and proliferation (tumor formation).
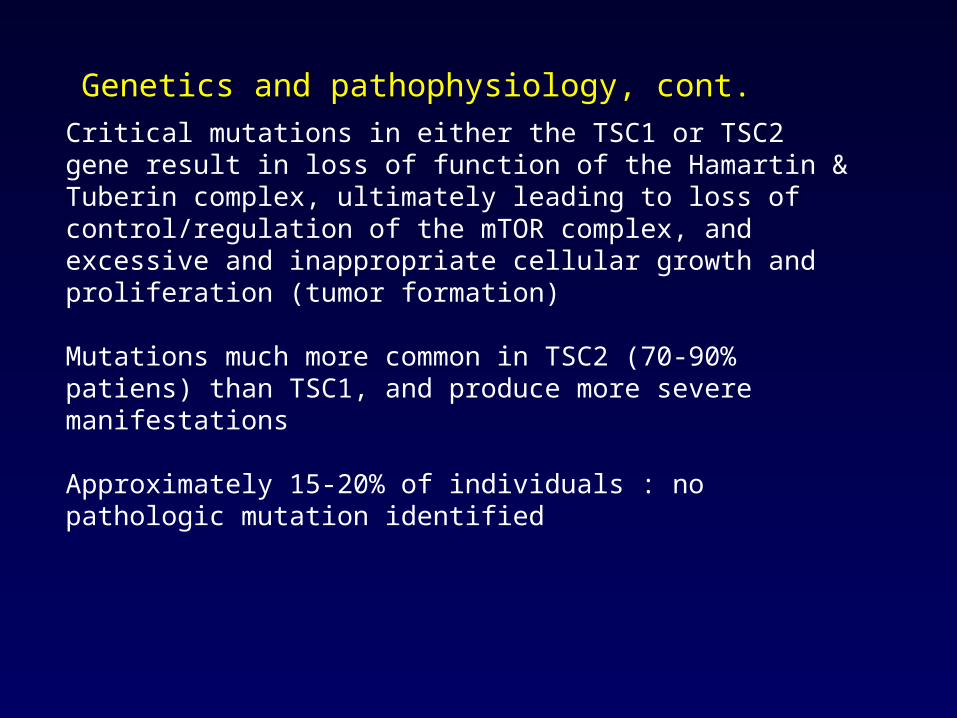
Critical mutations in either the TSC1 or TSC2 gene result in loss of function of the Hamartin & Tuberin complex, ultimately leading to loss of control/regulation of the mTOR complex, and excessive and inappropriate cellular growth and proliferation (tumor formation)
Mutations much more common in TSC2 (70-90% patiens) than TSC1, and produce more severe manifestations
Approximately 15-20% of individuals : no pathologic mutation identified
Genetics and pathophysiology, cont.
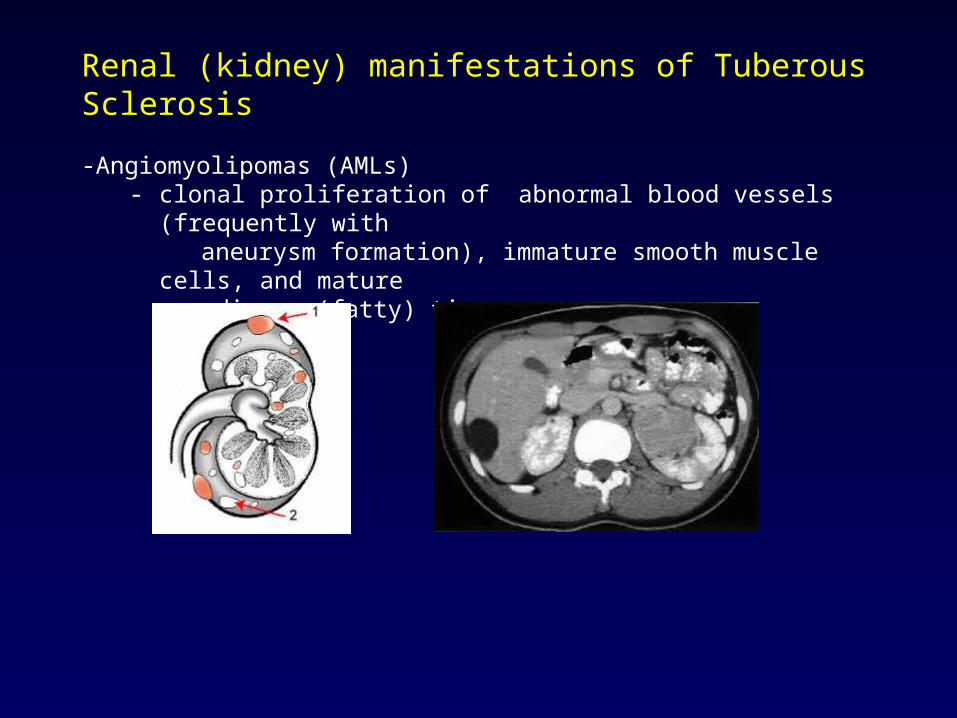
Renal (kidney) manifestations of Tuberous Sclerosis
-Angiomyolipomas (AMLs) - clonal proliferation of abnormal blood vessels (frequently with aneurysm formation), immature smooth muscle cells, and mature adipose (fatty) tissue
- Cystic disease
- Spectrum of manifestation from small microcystic disease, to multiple, large bilateral cysts
- Contiguous gene deletion syndrome : simultaneous disruption of the adjacent genes on the same chromosome (16p), PKD1 and TSC2, gives rise to a severe version of Polycystic Kidney Disease, with early (childhood) onset of chronic kidney disease and progression to End Stage Renal Disease, requiring dialysis or transplantation (2-5% affected TSC2 patients)
- Renal cell carcinoma (cancer) : risk increases with age, with peak incidence in the age group 20-50 years old. Relatively rare, approx 2% affected patients; more common in TSC2 patieints
The incidence of renal lesions increases with age, such that by late childhood - early adulthood, approximately 80% of patients will have AMLs, and 50% of patients will have cystic involvement.
AMLs increase in both size and number as patients mature.
Abnormal blood vessels give rise to micro and macroaneurysm formation,leading to risk of spontaneous rupture and potentially life threatening bleeding.
- lifetime risk ~ 25-50%- risk factors = tumor size > 4 cm, and aneurysm size > 0.5 cm- treatment = selective arterial embolization
Slight female to male predominance in the incidence of AMLs, giving rise to the theory that the female sex hormone estrogen may play a role in AML development. AML growth appears to be accelerated during pregnancy.
Symptoms of enlarging AMLs:
- back, flank or abdominal pain- visible (gross) hematuria – blood in the urine- bleeding from the kidney into the retroperitoneal space – can present with circulatory shock and be life-threatening
- AML size correlates with bleeding risk, esp. when >= 4 cm in diameter
Radiograpahic diagnosis
- Ultrasound- CT scan- MRI
MRI is considered the superior modality since it avoids exposure to ionizing radiation, and is better than CT at characterizing so-called fat-poor lesions in the kidney; and it can be coordinated with brain MRI, thereby limiting the number of times patients need to undergo anesthesia for the MRI procedure.
Frequency of surveillance scan :- yearly if previously documented renal involvement of disease- every three years if no prior documented renal involvement
Management of AMLs
Therapeutic interventions are required only in a minority of patients with TSC renal involvement
Modalities include: - nephron sparing surgery- complete (radical) nephrectomy- selective renal artery embolization – especially for patients with active retroperitoneal bleeding- pharmacologic mTOR inhibition (sirolimus (rapamycin) or everolimus (afinitor))
Surgery consult is usually reserved for situations where AML size is > 4 cm. Interventional Radiology consult for embolization is warranted if size and/or location of AML lesion precludes a surgical approach.
TS-related cystic disease of the kidneys
- occurs in up to 50% of patients with both TSC1 & TSC2 disease
- spectrum of involvement from small microcystic disease to large, multiple bilateral cystic involvement
- associated with development of hypertension and chronic kidney disease
- contiguous gene deletion syndrome : simultaneous mutations/deletions in the adjacent PKD1 & TSC2 genes on chromosome #16 early onset, severe manifestations of polycystic kidney disease, with risk of hypertension and chronic renal failure in childhood; affects approx 2-5% of patients with TSC2-related disease
Kidney cancer (carcinoma)
- principal subtype = renal clear cell carcinoma
- may be multifocal and bilateral
- incidence ~ 2-5% by the age of 30-50 years old
- risk higher in TSC2 related disease
- risk probably highest in those with the contiguous gene deletion syndrome
- MRI not reliable in differentiating fat-poor AML from cancer needle biopsy may be necessary, with specific immunohistochemistry staining (HMB45 & melan A = positive in AML, negative in carcinoma)
- nephron sparing surgery employed where possible to avoid complete nephrectomy
- case reports suggest some response to everolimus therapy
Development of chronic kidney disease
- kidney failure results from a combination of :- renal cystic/polycystic kidney disease- multiple bilateral AMLs encroaching upon and displacing normal kidney tissue- repeated renal surgeries that remove more and more normal kidney tissue along with the pathologic tissue
- incidence is not clearly known- frequently accompanied by development of high blood pressure
- treatment of choice = ACE inhibitors or angiotensin receptor blockers
- may result in the need for either dialysis or kidney transplantation- Renal failure is the leading cause of death in the adult population with TS
mTOR inhibition in the management of AMLs
- in the setting of loss of normal hamartin-tuberin protein complex activity, constitutive upregulation of the mTOR growth and proliferative pathways occurs, leading to tumor formation
- the mTOR inhibitors sirolimus and everolimus work by interfering with the interaction between mTOR and a key regulatory protein called Raptor, leading to down-regulation of the mTOR pathway
- these drugs therefore represent a logical and attractive targeted form of therapy for patients with TS
The EXIST-II trial (2013):
- enrolled patients with TSC or sporadic lymphangioleiomyomatosis (LAM)- assessed response of AML size over time in response to fixed dose 10 mg/day everolimus (Afinitor) vs. placebo- patients came from multiple medical centers in multiple countries- needed to be 18 years of age or older- by consensus guidelines needed to have a definite diagnosis of TSC or LAM- patients needed to have at least one AML 3 cm or more in diameter- the primary end-point measured in the study was the percentage of patients experiencing a 50% reduction or more in the sum of the volumes of target AML lesions identified at baseline- To assess response in AML size, CT or MRI was done at baseline and then at 12, 24, 48 weeks; then annually
EXIST-II, continued
Additional, secondary endpoints measured included: - time needed to detect a response in AML size- duration of response in AML size- duration of skin lesion responses- change in PFT response for LAM patients- change in plasma angiogenic molecules – VEGF-D and collagen IV (potential non-invasive biomarkers of disease burden)
Disease “progression” (treatment failure) was defined as :- >= 25% increase in size of the sum total volume of target lesions identified at start of study- appearance of at least one new lesion of 1 cm or more in diameter- increase in kidney size by 20% or more- episode of retroperitoneal bleeding
EXIST-II, continued- excluded patients from study if :
- AML required surgery at time of enrollment- if patient had undergone embolization procedure in the last 6 months- For LAM patients, if lung diffusion capacity (DLCO) was
< 35%, or if oxygen saturation was < 88% on 6-minute walk test
- Enrolled 118 patients from 24 medical centers in 11 countries
- In a 2:1 ratio, 79 patients were assigned to receive fixed dose everolimus at 10 mg/day, and 39 patients were assigned to receive placebo
- Mean duration of drug exposure was 38 weeks for everolimus patients, 34 weeks for patients assigned to receive placebo
Principal results: - 42% of patients taking Everolimus vs. 0% of patients taking placebo met the primary end point of the study (decrease of at least 50% in the sum total volume of all AMLs identified at the start of the study); mean time to response was 2.9 months
- “Progression” as defined above (treatment failure) was observed in 4% of patients assigned everolimus, vs. 21% of patients assigned placebo
- at baseline, VEGF-D and collagen IV levels correlated with size and number of AMLs, and with time decreased in those patients assigned everolimus, but not placebo – 62% reduction in VEGF-D and 42% reduction in collagen IV
- based on EXIST-II results, everolimus given FDA approval for patients with enlarging AMLs and who do not require immediate surgery
Caveats…
- although retroperitoneal bleeding, development of chronic kidney disease, and cancer represent the major morbid events that can develop in an adult TSC patient, these specific outcomes were NOT formally assessed in this drug trial
- many AMLs are slowly growing and we still cannot predict which patients would benefit most from everolimus treatment, vs. being left alone
- everolimus was associated with adverse events in the form of mouth ulcers, acne, and risk of infection, since it is an immunosuppressant
- reduction in AML size is unfortunately reversible upon discontinuation of treatment
- longer term results are still not in
Conclusions- Mutation induced loss of function in the hamartin-tuberin complex leads
to over-activity of the mTOR regulatory complex, in turn leading to overly rapid cellular metabolism, growth, and proliferation, resulting in benign tumor formation in multiple organ sites; in the kidney, these tumors are known as AMLs
- Renal disease represents the 2nd most common cause of death overall in TSC patients, but in adults is the number 1 cause of death, from complications of end stage kidney failure, kidney bleeding, or cancer
- The mTOR inhibitor everolimus, although it doesn’t restore normal function of the hamartin-tuberin complex, effectively results in down- regulation of the mTOR complex and leads to significant reduction in size of renal AMLs
Future directions:- Clarification of AML size reduction correlates with decreased risk of bleeding, progression to CKD, or development of cancer
- Validation of non-invasive blood biomarkers which would correlate with size and composition of AMLs – VEGF-D and collagen IV
- Refine optimal dosing of and duration of everolimus therapy
- Refine the optimal time for intervention with everolimus therapy – ? prophylactically during childhood when peak AML growth occurs
- Predicting risk of hemorrhage so that pre-emptive embolization could be considered
- Beta blockers (propranolol) for the treatment of AMLs
- Everolimus for the treatment of TS-related kidney cancer