Reduced treatment delays for drug-resistant TB/HIV co-infected patients
with decentralised care and rapid Xpert MTB/Rif test in Khayelitsha, South
Africa
Helen Cox, Jennifer Hughes, Sizulu Moyo, Johnny Daniels, Vivian Cox, Mark Nicol, Gilles
van Cutsem and Virginia Azevedo

The global TB situationThe global TB situationEstimated
incidence, 2012Estimated number
of deaths, 2012
940,000*(0.8–1.1 million)
8.6 million(8.3–9.0 million)
450,000(300,000–600,000)
All forms of TB
Multidrug-resistant TB
HIV-associated TB 1.1 million (1.0–1.2 million)
320,000(300,000–340,000)
Source: WHO Global Tuberculosis Report 2013 * Excluding deaths attributed to HIV/TB
170,000(100,000–240,000)

Access to DR-TB treatment
WHO TB Report 2013
~450,000 incident cases annually<20% of estimated cases receive treatment
Target
Projected
Actual

South Africa• 18% Adult HIV prevalence• 1,000/100,000/year TB
incidence• 63% of TB patients are HIV
infected• TB is the leading cause of
death (54,000 deaths in 2011)
• ~14,000 cases of rifampicin-resistant TB (DR-TB) diagnosed in 2012

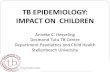
The DR-TB treatment gap in South Africa
2007 2008 2009 2010 2011 20120
2000
4000
6000
8000
10000
12000
14000
16000
0
10
20
30
40
50
60
70
80
74298198
9070
7386
10085
14161
4349
46
72
56
46
Diagnosed % Treated
MD
R-TB
dia
gnos
ed
Star
ted
on tr
eatm
ent (
%)
Source: NDOH data 2013

Delays to DR-TB treatment initiation (South Africa)
Setting Diagnostic method Median time to DR-TB treatment initiation
Northern Cape, 2009-10 Line probe assay 62 days
Western Cape, 2007-11 Line probe assay 55 days
Western Cape Hospital, 2007
Culture and DST 44 days (hospitalised patients)
KwaZulu Natal, 2001-2008 Culture and DST 84 days
KwaZulu Natal, 2008-09 Culture and DST 72 days
References: Hanrahan et al PLoS ONE 2012; Jacobson et al Clin Inf Dis 2011; Bamford et al SAMJ 2010; Heller et al IJTBLD 2010; Loveday et al IJTBLD 2012

Xpert MTB/Rif for TB and DR-TB diagnosis rolled out across South Africa
GeneXpert instrument placement across South Africa, May 2014
Time to result = 1.5 hours
• Xpert for all presumptive TB• To date, 3.5 million specimens have been tested

Benefits of rapid treatment initiation
Gandhi et al, Am J Resp Crit Care Med 2010
Rapid mortality (<1 month) among diagnosed patients in Tugela Ferry, KZN
90% HIV infected
98% HIV infected

Aim
• To assess the impact of Xpert for RR-TB diagnosis on treatment initiation in the context of decentralised DR-TB treatment in Khayelitsha, Cape Town

Khayelitsha
• Population ~ 400,000• Antenatal HIV prevalence 37%
(26,000 pts on ART)• ~ 5,100 TB cases registered each
year (75% HIV infected)• DOTS treatment success ~ 80%• Approximately 200 rifampicin-
resistant cases/year (75% HIV-infected)
• 10 health facilities providing HIV/TB/DR-TB diagnosis and treatment

Khayelitsha decentralised model• Hospital admission only if clinically indicated• PHC doctors initiate treatment and review monthly in
local clinics• Daily DOT and nurse management in clinics• Integration with ART provision • Specialist paediatric outreach support• Local audiometry screening service• Individual counselling, home visits, support groups,
social worker support• Recording and reporting at sub-district level

Implementation of interventions by year
Year 2003-2006
2007-2008 2009 2010 2011 2012 2013
DST Method
Culture (phenotypic)
Mix of Culture (phenotypic) and
LPA
LPA Xpert
RR-TB model of care
Centralized Limited decentralization
Improved programme
implementation
Full decentralization

Cases diagnosed and treated by year
2003-06 2007-08 2009 2010 2011 2012 2013
No. diagnosed
Not available 218 212 195 219 210
No. treated 158 257 182 182 173 191 197
% treated Not available 83.5 85.8 88.7 87.2 93.8
Consistently high % of patients initiate treatment

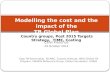
Time to DR-TB treatment
2003-06 Cult
2007-08 Cult
2007-08 LPA
2009 LPA
2010 LPA
2011 LPA
2012 Xpert
2013 Xpert
0
20
40
60
80
100
120
140
71 76 50 40 34 28
137M
edia
n da
ys to
trea
tmen
t ini
tiatio
n
Xpert impact
p<0.0001
p<0.0001
p<0.001
Decentralisation impact
LPA impact

HIV and time to RR-TB treatment
2009 2010 2011 2012 20130
5
10
15
20
25
30
35
40
45
34 34
25
12
8
42
34
28
14
7
HIV negative HIV positive
Med
ian
time
to D
R-TB
trea
tmen
t (da
ys)

HIV and % initiating RR-TB treatment
2010 2011 2012 20130
20
40
60
80
100 9891.2
100 100
85.189.6 86.3
94.4
HIV negative HIV-infected
Trea
tmen
t ini
tiatio
n am
ong
diag
nose
d (%
)
Xpert
Across 2012-13, significant difference in treatment initiation between HIV negative and HIV infected, p<0.0001

Time to treatment (2011-12, Xpert)
● deaths, censoredP=0.134, Not significant

Conclusions• Decentralisation of DR-TB treatment reduced
time to treatment from 2.5 months to <1 month• Xpert reduced time to treatment to a median of
7 days, with more than 90% of HIV infected RR-TB cases starting treatment
• Rapid diagnosis is likely to reduce early mortality among HIV infected, although earlier presentation still required
• With well functioning systems, new diagnostic tests can translate into reduced time to treatment

Acknowledgments
• City of Cape Town Health Department
• Western Cape Province• National Health
Laboratory Service• Staff in Khayelitsha clinics• Médecins sans Frontières
staff• DR-TB patients in
Khayelitsha