11/17/2014
1
Principles of Pain Assessment
and Management in Older Nursing
Home Patients
Shaida Talebreza M.D.
Assistant Professor, Division of Geriatrics,
University of Utah School of Medicine
Palliative Care Specialist, Home Based Primary Care (HBPC)
George E. Wahlen Salt Lake City Veterans Affairs Medical Center
Medical Director, Inspiration Hospice
Pain Assessment Outline
• What is Pain
• Prevalence of Pain in Older Adults
• Geriatric Pain Special Considerations
• Types of Physical Pain
• Geriatric Pain Assessment: Physical Pain
History
– PQRST
– Cognitively Impaired Adults
What is Pain?
• An unpleasant sensory and emotional
experience associated with actual or
potential tissue damage
• Pain is also a perceptual experience that
has an impact on all aspects of a person’s
emotional, psychological, social and
physical functioning.
Hadjistavropoulos T, Herr K, Turk D, et al. An Interdisciplinary Expert Consensus Statement on Assessment of Pain in Older Persons.
Clin J Pain. 2007;23:S1-S43

11/17/2014
2
What is Pain?
• Physical, psychological, social, and spiritual problems can affect a patient’s perception and tolerance of pain
• Multidisciplinary approach to assessment and treatment is very important and effective
Prevalence of Pain in Older
Adults
• Substantial pain is experienced by:
– 25%-50% of community dwelling adults
– 45%-80% of nursing home residents
GRS Teaching Slides Web site http://www.frycomm.com/ags/teachingslides.
Geriatric Pain is Undertreated
• Geriatric patients may: – Minimize their symptoms
– Not voluntarily report pain
– Be unable to report pain due to cognitive impairment
• Clinicians may: – Inadequately assess pain
– Treat pain with ineffective therapies
– Encounter adverse effects with otherwise effective therapies
GRS Teaching Slides Web site http://www.frycomm.com/ags/teachingslides.

11/17/2014
3
Types of Physical Pain Pain Type Nociceptive
Somatic
Nociceptive
Visceral
Neuropathic
Description Activation of
nociceptive sensory
receptors
Activation of
nociceptive sensory
receptors
Irritation of
components of the
CNS or PNS
Source •Tissue injury
•Bones
•Soft tissue
•Joints
•Muscles
•Viscera
•Cardiac
•Lung
•GI
•GU
Peripheral or central
nervous system
Examples •Arthritis
•Fracture
•Bone metastases
•Post-op pain
•Renal Colic
•Constipation
•Trigeminal
neuralgia
•PHN
•Diabetic
neuropathy
•Herniated disc
•Post-stroke
syndrome
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried

11/17/2014
4
Provocative and Palliating
Factors
• What makes the pain better or
worse?
– Rest
– Movement
– Positioning
– Eating
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried
Quality
Aching Dull Sharp
Stabbing Colicky Burning
Gnawing Squeezing Pricking
Throbbing Deep Tingling
Cramping

11/17/2014
5
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried
Region (Location) of Pain
• Where do you hurt?
• Can use a pain map:
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried

11/17/2014
6
Pain Severity
Number Severity
0 None
1-3 Mild
(Background Pain)
4-6 Moderate
(Generally interferes with function and
sleep)
7-10 Severe
(Generally interferes with function, sleep
and concentration)
Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
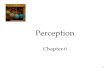
Severity of Pain: Scales
Numeric Rating Scale Faces Pain Scale
•Good Validity •Fair Validity
•Fair Reliability •Fair Reliability
•Easy to use •Requires hearing or vision and cognition
•Requires vision, attention, and cognition
Halter JB, Ouslander JG, Tinetti ME, et al. Hazzard’s Geriatric Medicine and Gerontology, 6th Edition. New York: McGraw Hill; 2009.
Severity: Numeric Rating Scale

11/17/2014
7
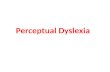
Severity: FACES Pain Scale –
Revised (FPS-R)
Severity: Wong-Baker FACES
• Developed for pediatric patients
Cognitively Impaired Patients
• It has been shown that pain reports from
those with mild to moderate cognitive
impairment are no less valid than other
patients with normal cognitive function
• The NRS and FPS-R are feasible for use
in most patients with cognitive impairment
Halter JB, Ouslander JG, Tinetti ME, et al. Hazzard’s Geriatric Medicine and Gerontology, 6th Edition. New York: McGraw Hill; 2009.

11/17/2014
8
Cognitively Impaired Patients
• Use both self-report and observational
measures when possible
• Solicit the assistance of caregivers familiar
with the patient
• Determine if analgesic medications lead to
a reduction in pain behaviors
Hadjistavropoulos T, Herr K, Turk D, et al. An Interdisciplinary Expert Consensus Statement on Assessment of Pain in Older Persons.
Clin J Pain. 2007;23:S1-S43
Cognitively Impaired Patients
• The Interdisciplinary Expert Consensus
Statement on Assessment of Pain in Older
Persons could not reach definitive
recommendation of any particular scale for
patients with severe dementia
Cognitively Impaired Patients
• Promising tools:
– PACSLAC
– Doloplus 2
• American Academy of Hospice and
Palliative Medicine
– PAINAD

11/17/2014
9
Physical Pain Assessment in
Cognitively Impaired Patients PACSLAC DOLOPLUS-2 PAINAD
60 item checklist
Present/Absent
10 items
0-3 Scale
Five Items
0-2 Scale
5 minutes to
administer
<5 minutes to
administer
<5 minutes to
administer
Strong Internal
Consistency
Strong Internal
Consistency
Lower Internal
Consistency
Strong Interrater
Reliability
Not Reported Strong Interrater
Reliability
Validity based on
retrospective RN
reports
Validated by
correlation with other
scales
Validated by
correlation with other
scales
Hadjistavropoulos T, Herr K, Turk D, et al. An Interdisciplinary Expert Consensus Statement on Assessment of Pain in Older Persons.
Clin J Pain. 2007;23:S1-S43

11/17/2014
10
Pain Assessment in Advanced
Dementia (PAINAD) Scale
Items 0 1 2 Score
Breathing Normal •Occasional
labored breathing
•Short period
hyperventilation
•Noisy labored
breathing
•Long period
hyperventilation
•Cheyne-Stokes
Vocalization None •Occasional
moan or groan
•Low-level
speech with a
negative or
disapproving
quality
•Repeated troubled
calling out
•Loud moaning or
groaning
•Crying
Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
Pain Assessment in Advanced
Dementia (PAINAD) Scale
Items 0 1 2 Score
Facial
Expression
Smiling or
inexpressive
•Sad
•Frightened
•Frown
•Facial grimacing
Body
Language
Relaxed •Tense
•Distressed
pacing
•Fidgeting
•Rigid
•Fists clenched
•Knees pulled up
•Pulling or pushing
away
•Striking out
Consolabillity No need •Distracted or
reassured by
voice or touch
•Unable to console,
distract or reassure
Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
MDS Indicators of Pain
• J8. Indicators of pain or possible pain. • Select all that apply in last 5 days: • Check all that apply. • a. Non-verbal sounds (crying, whining, gasping, moaning,
or groaning) • b. Vocal complaints of pain (that hurts, ouch, stop) • c. Facial expressions (grimaces, winces, wrinkled forehead,
furrowed brow, clenched teeth or jaw) • d. Protective body movements or postures (bracing,
guarding, rubbing or massaging a body part/area, clutching or holding a body part during movement)
• e. None of these signs observed or documented

11/17/2014
11
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried
Timing
• Onset (When does it start)
• Frequency (How often does it happen)
• Duration (How long does it last)
Geriatric Pain Assessment:
Physical Pain History
• Provocative (aggravating) factors
• Palliative (relieving) factors
• Quality
• Region (location)
• Severity
• Timing
• Treatments tried

11/17/2014
12
Treatments Tried
• Current and previous prescription drugs
• Review pain medication dosage and
frequency
• Over the counter medications
• Natural remedies
• Nondrug treatments
• Assess all for:
– Effectiveness and adverse events
Nociceptive Somatic Pain Examples •Arthritis
•Fracture
•Bone metastases
•Post-op pain
Pain source •Tissue injury
•Bones
•Soft tissue
•Joints
•Muscles
Quality •Aching
•Stabbing
•Gnawing
•Throbbing
Region Well-Localized
Timing Constant
Effective Drug Therapy •APAP (A)
•Opioid (B)
•PT and CBT (B)
Pacala JT, Sullivan GM, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine, 7th ed. New York: American Geriatrics Society; 2010.
Nociceptive Visceral Pain Examples •Renal Colic
•Constipation
Pain source •Viscera
•Cardiac
•Lung
•GI
•GU
Quality •Dull
•Colicky
•Deep
•Cramping
•Squeezing
Region •Poorly localized
•Diffuse
Timing •Intermittent
•Paroxysmal
Effective Drug Therapy •Treat Underlying Cause
Pacala JT, Sullivan GM, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine, 7th ed. New York: American Geriatrics Society; 2010.

11/17/2014
13
Neuropathic Pain Examples •Trigeminal neuralgia
•PHN
•Diabetic neuropathy
•Herniated disc
•Post-stroke syndrome
Pain Source Peripheral or central nervous system
Quality •Sharp
•Burning
•Pricking
•Tingling
•Squeezing
Region Varies
Timing Usually constant but can have paroxysms
Effective Drug Therapy •TCA (A)
•SNRI (A)
•Anticonvulsant (A)
•Opioid (B)
•Topical anesthetics (C)
•PT and CBT (C)
Pacala JT, Sullivan GM, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine, 7th ed. New York: American Geriatrics Society; 2010.
Summary
• Pain requires a thorough assessment to determine its source, severity, and impact on the well-being of the patient:
– Provocative (aggravating) factors
– Palliative (relieving) factors
– Quality
– Region (location)
– Severity
– Timing
– Treatments tried
Summary
• Use the same pain severity scale to assess response to treatment
– NRS or Faces for cognitive intact older adults
– PACSLAC, Doloplus or PainAD for non-communicative older adults
• Differentiate between nociceptive somatic or visceral pain and neuropathic pain as treatment differs

11/17/2014
14
PHYSICAL PAIN MANAGEMENT
Pain Management Outline
• World Health Organization (WHO) Pain Ladder
• Acetaminophen
• NSAIDS
• Tramadol
• Opioids
• Adjuvant Medications
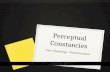
WHO 3-Step Ladder
1-3 mild
4-6 moderate
7-10 severe
Morphine
Oxycodone
Hydromorphone
Methadone
Fentanyl
± Adjuvants
A/Codeine
A/Hydrocodone
A/Oxycodone
Tramadol
± Adjuvants
ASA
Acetaminophen
NSAID’s
± Adjuvants WHO Geneva, 1996.

11/17/2014
15
Treating Mild To Moderate Pain
Acetaminophen:
Recommended as first-line therapy for
mild persistent pain in older adults
Particularly effective for musculoskeletal
pain from osteoarthritis
For chronic pain it is most effective if
scheduled regularly rather than as-needed
Starting dose: 325-500 mg q4-6 hrs
Slide 43
Treating Mild To Moderate Pain
• Acetaminophen
• No more than 4g/24h; or 2g/24h if on coumadin due to increase in INR
• Lower the dose by 50-75%, or avoid, in patients at risk of liver dysfunction, especially with history of heavy alcohol intake
• Know all meds the patient is taking, as acetaminophen is a common ingredient in prescription and OTC drugs
Treating Mild To Moderate Pain
• NSAIDs
Use judiciously if at all only after acetaminophen has been tried and only in highly select individuals due to significant adverse effects
Use COX-2 inhibitor with extreme caution, if at all, in older persons
Topical NSAIDs appear to be safe and effective in the short term, but no long-term studies

11/17/2014
16
Treating Mild To Moderate Pain
• NSAIDs
Many significant adverse effects in older adults:
Renal dysfunction
GI bleeding
Platelet dysfunction
Fluid retention
Worsening HTN
Precipitate Heart Failure
Precipitate Delirium
Treating Mild To Moderate Pain
• Tramadol
– Great potential for precipitating seizures even at therapeutic dosages
• Although this risk is likely only 1%, it is increased among people with multiple comorbidities
– Tramadol has a ceiling effect at 300 mg/day for its analgesic effect
– In general, cost, side effects and the ceiling effect make it less attractive option for pain management in the palliative care setting
Treating Moderate To Severe
Pain o Opioids:
o Equianalgesic Dose Relative Strength
o Onset, Peak Effect, Duration
o Opioids in Renal and Hepatic Insufficiency
o Initiating Immediate Release/Short Acting (IR/SA) Opioids
o Initiating Extended Release/Long Acting (ER/LA) Opioids
o Side Effects
o Medications to Avoid in Older Adults

11/17/2014
17
Equianalgesic Dose of Opioid
Analgesic
Oral/Rectal Dose
(MG)
Medication IV/SC Dose (MG)
200 mg Codeine 130 mg
30 mg Hydrocodone Not available
30 mg Morphine 10 mg
20 mg Oxycodone Not available
7.5 mg Hydromorphone
(Dilaudid)
1.5 mg
12.5 mcg patch = for
patients >60 mg
morphine in 24 hours
Fentanyl 0.1 mg
S
T
R
O
N
G
E
R
Equianalgesic Dose of Opioid
Analgesic
Oral/Rectal Dose (MG) Medication IV/IM Dose (MG)
24 hr oral morphine
Morphine:Methadone
Ratio
<30 mg 2:1
31-99 mg 4:1
100-299 mg 8:1
300-499 mg 12:1
500-999 mg 15:1
1000-1200 mg 20:1
>1200 mg Consult
Methadone ½ oral dose
2 mg po
methadone=
1 mg IM/IV
methadone
Treatments Tried
• Review pain medication dosage and frequency:
– Does the pain medication relieve some pain in 15-60 minutes (or 3-4 hours)?
• If not you may need to increase the dosage of medication (if possible) or change the class of medication
– Does the pain medication relieve pain in 15-60 (or 3-4 hours) minutes but wear off before the next dose is given?
• If so you many need to increase the frequency of medication (if possible)

11/17/2014
18
Opioids
Medication Onset of
Analgesia in
Hours
Peak Effect
in Hours
Duration of
Analgesia in
Hours
Half-Life in
Hours*
Morphine
SC, IV
0.25-0.5 hour
0.5-1 hour
3-6 hours
2-3 hours
Morphine
PO
0.5-1 hour
1.5-2 hours
4-7 hours
2-3 hours
Sustained-
Release
Morphine
0.5-1 hour 3-6 hours 8-24 hours 2-3 hours as
drug is
released/
absorbed
•*Half-Life becomes longer with impaired renal function
Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
Doyle D, Hanks G, Cherny N, et al. Oxford Textbook of Palliative Medicine: 2005, 3rd Edition. New York: Oxford Press; 2005
Opioids
Medication Onset of
Analgesia
in Hours
Peak Effect
in Hours
Duration of
Analgesia
in Hours
Half-Life in
Hours
Hydrocodone 0.5 -1 hour 0.5 -1 hour
4-6 hours 2-4 hours
Oxycodone 0.5 -1 hour 1 hour 3-6 hours 2-3 hours
Sustained-
Release
Oxycodone
0.5 -1 hour 3-4 hours 8-12 hours 2-3 hours as
drug is
released/
absorbed
Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
Doyle D, Hanks G, Cherny N, et al. Oxford Textbook of Palliative Medicine: 2005, 3rd Edition. New York: Oxford Press; 2005
Opioids
Medication Onset of
Analgesia
in Hours
Peak Effect
in Hours
Duration of
Analgesia
in Hours
Half-Life in
Hours
Dilaudid
SC/IV
0.25-0.5
hour
0.5-1.5
hours
3-4 hours 2-3 hours
Dilaudid PO 0.5 -1 hour 1-2 hours 3-4 hours 2-3 hours
Methadone 0.5 -1 hour 0.5-1.5
hours
4-8 hours 12 >150
hours
Fentanyl
Patch
-------------
(of first
dose)
18-24 hrs
48-72 hours 13-22 hours
Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
Doyle D, Hanks G, Cherny N, et al. Oxford Textbook of Palliative Medicine: 2005, 3rd Edition. New York: Oxford Press; 2005

11/17/2014
19
Renal Insufficiency
Appear Optimal Use with Caution Avoid
Fentanyl Hydromorphone (Dilaudid)
Morphine
Methadone Oxycodone
Hepatic Insufficiency
Appear Optimal Use with Caution Avoid
Fentanyl Morphine
Hydromorphone (Dilaudid)
Oxycodone
Methadone
Moderate to Severe Pain in Opioid
Non-Tolerant Patients
• In general, start at lowest dose of Immediate Release/ Short Acting (IR/SA) opioid and titrate slowly
• If the patient is in pain crisis, do not withhold medications – may need higher starting dose
• Strongly consider scheduled medication rather than only prn dosing
– Scheduled dosing is vital for patients with cognitive impairment who cannot request prn doses
• Do not start with ER/LA opioids in opioid non-tolerant patients!

11/17/2014
20
Starting IR/SA Dosages in Opioid
Non-Tolerant Older Adults
Moderate pain: Starting Dose When to titrate dose
Hydrocodone +
APAP
2.5-5 mg po q4-6 hrs
After 3-4 doses
Oxycodone +
APAP
2.5-5 mg po q4-6 hrs
After 3-4 doses
Moderate to
severe pain:
Morphine 2.5-10 mg po q4 hrs
After 1-2 doses
Hydromorphone 1-2 mg po q3-4 hrs
After 3-4 doses
Opioid-Tolerant Patient
• Patients considered opioid tolerant are those who are taking at least
- 60 mg oral morphine/day
- 25 mcg transdermal fentanyl/hour
- 30 mg oral oxycodone/day
- 8 mg oral hydromorphone/day
- 25 mg oral oxymorphone/day
- An equianalgesic dose of another opioid
For 1 week or longer
Appropriate Patient Selection ER/LA
− Opioid tolerant, generally not naive
− Avoid in acute pain
− Avoid when short duration anticipated
− Avoid post-op pain management
− Not for use in mild pain

11/17/2014
21
Extended Release/Long Acting
(ER/LA) Opioids: • ER/LA medication released over 8, 12, 24, 72
hours (depending on the product)
• Pills must be ingested whole, not crushed or chewed
• Patch must not be cut
• Importance of adherence to dosing regimen
• Do not start with ER/LA opioids in opioid non-tolerant patients!
• Patients are first started on IR/SA opioids to determine how much opioid is needed
Extended Release/Long Acting
(ER/LA) Opioids: • After opioid need is determined using IR/SA
opiods (over an appropriate time period):
• Continuous pain is then treated with 24-hour opioids in long-acting or sustained-release formulations
To cover breakthrough pain, combine with IR/SA (fast-onset medications that have short half-lives)
Breakthrough pain typically requires 5%–15% of the daily dose, offered q2 to q4h orally or or q30-60 minutes SC or IV
Extended Release / Long-Acting
(ER/LA) Opioids
Long Half Life Extended Release
Methadone: Morphine:
Dolophine Morphine ER
Methadose MS Contin
Fentanyl Kadian
Avinza
Oxycodone:
OxyContin
Hydromorphone:
Exalgo

11/17/2014
22
ER/LA Starting Dosages
Geriatric Patients
Lowest Starting Dose When to titrate dose
Morphine ER/LA 10-15 mg po q8-24 hrs After 3-5 days
Oxycodone
ER/LA
10 mg po q12 hrs
After 3-5 days
Methadone 1.25-2.5 mg po qd-bid After 1 week in low doses
After 1-2 weeks in higher
doses
Hydromorphone
ER/LA
8 mg qd
Opioid Tolerant Only
After 3-4 days
Fentanyl Patch 12.5 mcg/q72 hrs
Opioid Tolerant Only
After 2-3 patch changes
Medications to Avoid in Older
Adults
• Nalbuphine
– Restlessness and tremulousness
• Butorphanol
– Restlessness and tremulousness
• Meperidine (Demerol)
– Agitation, confusion, delirium, disorientation
Opioid Side Effects
Common Uncommon Constipation Bad dreams / hallucinations
Dry mouth Dysphoria / delirium
Nausea / vomiting Pruritus / urticaria
Sedation Urinary retention
Sweats Myoclonus / seizures
Respiratory depression

11/17/2014
23
Side Effects: Constipation
• Constipation
– Opioids decrease bowel motility
– Constipation develops in almost all patients on chronic opioids
– Constipation should be anticipated and (almost) always treated prophylactically
• With a bowel stimulant (senna, biscodyl)
• If needed addition of osmotic agent (miralax, sorbitol, lactulose)
– Easier to prevent than to treat
– No tolerance to this side effect
Side Effects: Nausea
• Nausea usually resolves after several days as the patient develops tolerance to this side effect
• If Nausea persists make sure the patient isn’t constipated, look for drug interactions
• Consider reducing the dose of the opioid medication or switching to another medication
• May also consider addition of antiemetic: – Haloperidol 0.5-1 mg po before opioid and q6 hrs
for several days
Side Effects: Sedation
• Mild sedation is common when first starting an opioid or when making significant dose increases
• Tolerance to sedation typically develops after several days to weeks of consistent use
• Sedation is dose dependent and should decrease at lower dosages or once medication is stopped
• Consider a limited course of low dose methylphenidate

11/17/2014
24
Side Effects: Urticaria
Pruritus
• Mast cell destabilization and histamine
release by morphine, hydromorphone
• Treat with routine long-acting, non-
sedating antihistamines
– Fexofenadine 60 mg PO bid
– Loratadin 5-10 mg qd
• Try a different opioid
Side Effects: Urinary Retention
• Opioids can cause urine retention
• This may require a urinary catheter
Side Effects: Myoclonus
• Some patients develop uncontrolled muscle twitching
• This can usually managed by decreasing the dose, changing the opioid or adding benzodiazepines
• If myoclonus and hyperalgesia occur in the setting of renal impairment it can be opioid induced neurotoxicity – switch to an opioid recommended for renal impairment

11/17/2014
25
Side Effects: Respiratory
Depression
• Respiratory depression is rare when opioid
doses are carefully titrated
• Patients who retain CO2 are at more risk
but this should not be a barrier to opioid
use
• It is almost always preceded by sedation
• Cutting back on dosages if sedation
develops usually avoids respiratory
depression
Adjuvant Analgesics
• Medications that, when added to primary
analgesics, further improve pain control
• May also be primary analgesics or in
combination with opioids to treat
neuropathic pain
• There is no clear consensus on what
adjuvant category to utilize first
Tricyclic Antidepressants (TCA)
• Best studied antidepressant class that show efficacy for neuropathic pain
• Avoid Amitriptyline in older adults
• Use Desipramine or Nortriptyline
– Initial dose 10 mg po qhs
– Effective dose 25-100 mg qhs
– Titrate dose after 3-5 days
– Typically takes 1-2 weeks to titrate up to an effective dose to determine if the therapy is working

11/17/2014
26
Serotonin-Norephinephrine
Reuptake Inhibitor (SNRI)
• Show some evidence of efficacy for
neuropathic pain but they have not been
well studied
• Duloxetine (Cymbalta)
– FDA approved for Diabetic Peripheral
Neuropathy
– Initial dose 20 mg/d
– Effective dose 60 mg/d
– Titrate dose after 7 days
– Contraindicated if CrCl <30
Anticonvulsants
• Gabapentin (Neurontin)
– Approved for Post herpetic neuralgia
– (Off Label) Postoperative pain, Chronic pain
• Pregabalin (Lyrica)
– Post herpetic neuralgia
– Diabetic peripheral neuropathy
– Fibromyalgia
Anticonvulsants
• Gabapentin
– Initial dose 100 mg po qhs
– May need up to 300-900 mg q8h for effect
– Titrate dose after 1-2 days
– CrCl <15: dose @ 100-300 mg/d
– CrCl >15-29: dose @ 200-700 mg/d
– CrCl >30-59: dose @ 200-700 q12h
– Most troubling side effect is lethargy

11/17/2014
27
Anticonvulsants
• Pregabalin (Lyrica):
– Initial dose 50 mg qhs
– Effective dose 300 mg/d
– Titrate dose after 7 days
– Often turned to when gabapentin is not
effective or has intolerable side effects
Summary • A stepped approach to pain treatment is advised,
starting with local and non-pharmacologic approaches
• Consider Tylenol instead of NSAIDS
• Systemic analgesics should not be withheld if needed
initially
• Do not start with ER/LA opioids in opioid non-
tolerant patients!
• Patients being treated with opioids usually develop
tolerance to the respiratory depression, fatigue, and
sedation, but not to the constipating effect
Slide 80
References
• Doyle D, Hanks G, Cherny N, et al. Oxford Textbook of Palliative Medicine: 2005, 3rd Edition. New York: Oxford Press; 2005.
• Emanuel LL, Hauser JM, Bailey FA, Ferris FD, von Gunten CF, Von Roenn J. EPEC for Veterans: Education in Palliative and End-of-life Care for Veterans. Chicago, IL, and Washington, DC, 2010
• GRS Teaching Slides Web site http://www.frycomm.com/ags/teachingslides.
• Hadjistavropoulos T, Herr K, Turk D, et al. An Interdisciplinary Expert Consensus Statement on Assessment of Pain in Older Persons. Clin J Pain. 2007;23:S1-S43
• Halter JB, Ouslander JG, Tinetti ME, et al. Hazzard’s Geriatric Medicine and Gerontology, 6th Edition. New York: McGraw Hill; 2009.
• Pacala JT, Sullivan GM, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine, 7th ed. New York: American Geriatrics Society; 2010.
• Quill TE, Holloway RG, Shah MS, et al. Primer of Palliative Care: 2010, 5th Edition. Illinois: American Academy of Hospice and Palliative Medicine; 2010.
• Reuben DB, Herr KA, Pacala JT, et al. Geriatrics at your Fingertips: 2010, 12th Edition. New York: The American Geriatrics Society; 2010.