National HL7 Standards for National HL7 Standards for Electronic Pathology Reporting to Electronic Pathology Reporting to
Cancer RegistriesCancer Registries
Eric B. Durbin, MSEric B. Durbin, MSDirector of Cancer InformaticsDirector of Cancer Informatics
Markey Cancer Control Program/Kentucky Cancer Markey Cancer Control Program/Kentucky Cancer RegistryRegistry
University of KentuckyUniversity of Kentucky
APIII, August 18, 2006APIII, August 18, 2006Vancouver, British Columbia Vancouver, British Columbia

OverviewOverview Value of electronic pathology (E-Path) reporting Value of electronic pathology (E-Path) reporting
and data standardsand data standards History of North American Association of Central History of North American Association of Central
Cancer Registries (NAACCR) E-Path standardsCancer Registries (NAACCR) E-Path standards NAACCR Standards Volume V: Pathology NAACCR Standards Volume V: Pathology
Laboratory Electronic ReportingLaboratory Electronic Reporting HL7 tutorialHL7 tutorial HL7 E-Path messagesHL7 E-Path messages Alternative delimited layoutAlternative delimited layout
Continuing work (standardized synoptic Continuing work (standardized synoptic reporting)reporting)

Value of E-Path Data Value of E-Path Data StandardsStandards
Facilitate the transmission of electronic Facilitate the transmission of electronic datadata
Define the structure and meaning of the Define the structure and meaning of the data for senders and recipientsdata for senders and recipients
Reduce costs for path labs and cancer Reduce costs for path labs and cancer registriesregistries
Allow senders and recipients to build a Allow senders and recipients to build a single interfacesingle interface Single interface can meet needs of multiple Single interface can meet needs of multiple
senders and receiverssenders and receivers

E-Path Benefits to Oncology E-Path Benefits to Oncology and Pathology Researchand Pathology Research
E-Path implementations reduce the E-Path implementations reduce the time from cancer diagnosis until the time from cancer diagnosis until the availability of high quality, well defined availability of high quality, well defined and structured research dataand structured research data
More timely high quality data offers More timely high quality data offers new opportunities to use registry based new opportunities to use registry based pathology data for research purposespathology data for research purposes Registry data is currently an underutilized Registry data is currently an underutilized
resourceresource

The Gold Standard in The Gold Standard in Quality: Central Cancer Quality: Central Cancer
Registry DataRegistry Data Central cancer registries are in the business of Central cancer registries are in the business of
collecting high quality population based datacollecting high quality population based data Registries routinely collect:Registries routinely collect:
Patient Demographics (current and at diagnosis)Patient Demographics (current and at diagnosis) Race, gender, geography, family historyRace, gender, geography, family history
Site/HistologySite/Histology Staging (TNM, Collaborative Stage, Summary Staging (TNM, Collaborative Stage, Summary
Stage)Stage) Comprehensive therapy dataComprehensive therapy data Long-term survival and follow-up (outcomes) Long-term survival and follow-up (outcomes)
information (for lifetime of patient)information (for lifetime of patient) Many other standard data elementsMany other standard data elements

Professional Data Professional Data CollectionCollection
Registry data is collected by trained Registry data is collected by trained professionalsprofessionals Certified Tumor Registrars (CTR) - ACoSCertified Tumor Registrars (CTR) - ACoS
Registry data is highly scrutinized for data Registry data is highly scrutinized for data quality and consistencyquality and consistency Edit checks during collectionEdit checks during collection Edit checks at central registryEdit checks at central registry Edit checks prior to submissions to federal and Edit checks prior to submissions to federal and
national agenciesnational agencies CDC, NCI/SEER, NAACCR, ACoSCDC, NCI/SEER, NAACCR, ACoS
Frequent audits of data completeness and qualityFrequent audits of data completeness and quality Data standards of quality is required by funding Data standards of quality is required by funding
agenciesagencies

Role of Pathology Data in Role of Pathology Data in Cancer RegistrationCancer Registration
Over 90% of all cancers are microscopically Over 90% of all cancers are microscopically confirmed by pathology reportconfirmed by pathology report
Pathology reports typically provide:Pathology reports typically provide: Demographics (limited)Demographics (limited) Diagnosis datesDiagnosis dates Site/Histology/Grade/LateralitySite/Histology/Grade/Laterality TNM stagingTNM staging Tumor sizeTumor size Identification of sources necessary for follow-back Identification of sources necessary for follow-back
for additional registry datafor additional registry data Physicians, involved institutions, etc.Physicians, involved institutions, etc.
Other valuable data elements and textOther valuable data elements and text

Additional Benefits of E-Additional Benefits of E-Path to Cancer RegistriesPath to Cancer Registries
Rapid case ascertainment for research Rapid case ascertainment for research studiesstudies Before patient is deceasedBefore patient is deceased Prior to confounding effects of treatmentPrior to confounding effects of treatment
Clinical trials patient identification and Clinical trials patient identification and recruitmentrecruitment
Central registry audits of reporting Central registry audits of reporting hospital registries (hospital based E-Path)hospital registries (hospital based E-Path)
Earlier assessment of incidence ratesEarlier assessment of incidence rates

Benefits of E-Path to Tissue Benefits of E-Path to Tissue BankingBanking
Short termShort term Automated, near real-time annotation of Automated, near real-time annotation of
path based data soon after specimen path based data soon after specimen collectioncollection
Targeted specimen identificationTargeted specimen identification Long termLong term
Availability of long term outcome dataAvailability of long term outcome data Ability to associate specimen data with Ability to associate specimen data with
population based data for patients with population based data for patients with similar or dissimilar characteristicssimilar or dissimilar characteristics

NAACCR, Inc.NAACCR, Inc. North American Association of Central Cancer North American Association of Central Cancer
RegistriesRegistries Professional organization established in 1987Professional organization established in 1987
Enhancing quality and use of cancer registry data Enhancing quality and use of cancer registry data Develops and promotes uniform data standards for Develops and promotes uniform data standards for
cancer registriescancer registries First data exchange standard published in 1994First data exchange standard published in 1994
Members include central cancer registries and Members include central cancer registries and many other govt. agencies, organizations and many other govt. agencies, organizations and individualsindividuals
Governed by elected board of directorsGoverned by elected board of directors Funds an executive officeFunds an executive office Various committees, sub-committees and work Various committees, sub-committees and work
groupsgroups http://www.naaccr.orghttp://www.naaccr.org

Acknowledgements:Acknowledgements:E-Path Transmissions Work E-Path Transmissions Work
Group 2005-2006Group 2005-2006Eric B. Durbin, MS (Chair)Eric B. Durbin, MS (Chair)Kentucky Cancer RegistryKentucky Cancer Registry
Lori A. Havener, CTRLori A. Havener, CTRNAACCRNAACCR
Toshi Abe, MSW, CTRToshi Abe, MSW, CTRNew Jersey State Cancer New Jersey State Cancer
RegistryRegistry
Mayra Alvarez, RHIT, CTRMayra Alvarez, RHIT, CTRFlorida Cancer Data SystemFlorida Cancer Data System
Steve BartaSteve BartaIMPACIMPAC
Victor BrunkaVictor BrunkaArtificial Intelligence In Artificial Intelligence In
Medicine, Inc.Medicine, Inc.
Ken Gerlach, MPH, CTRKen Gerlach, MPH, CTRCDC/NPCRCDC/NPCR
Barry Gordon, PhDBarry Gordon, PhDCalifornia Cancer RegistryCalifornia Cancer Registry
Jovanka Harrison, PhDJovanka Harrison, PhDNew York State Cancer RegistryNew York State Cancer Registry
Keith Laubham, MSKeith Laubham, MSArizona Cancer RegistryArizona Cancer Registry
J. A. Magnuson, PhD, RSJ. A. Magnuson, PhD, RSOregon Health ServicesOregon Health Services
Mark Rudolph (Alternate)Mark Rudolph (Alternate)Florida Cancer Data SystemsFlorida Cancer Data Systems
Wendy Scharber, RHIT, CTRWendy Scharber, RHIT, CTRMinnesota Cancer Surveillance Minnesota Cancer Surveillance SystemSystem
Advisors to Work Group:Advisors to Work Group:
Mary HamiltonMary HamiltonCDCCDCAustin KrieslerAustin KrieslerCDCCDC
Margaret MarshburnMargaret MarshburnCDCCDC

Brief History of the Brief History of the Quest for E-Path Quest for E-Path
StandardsStandards NAACCR board commissioned the quest in NAACCR board commissioned the quest in
20032003 IT CommitteeIT Committee
E-Path Sub-committeeE-Path Sub-committee E-Path Transmission Work Group was formedE-Path Transmission Work Group was formed
Built on previous work by NAACCR and CDCBuilt on previous work by NAACCR and CDC Conducted monthly and bi-weekly Conducted monthly and bi-weekly
teleconferences for over two yearsteleconferences for over two years NAACCR Volume V was ratified and NAACCR Volume V was ratified and
published in November 2005published in November 2005

Alas, the Holy Grail!Alas, the Holy Grail!

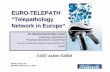
Typical E-Path Data FlowTypical E-Path Data Flow
Lab Information
System
Internet(Secure/
Encrypted)
PathReports in
HL7
HL7 Parser/Translator
Central Registry
HL7 WriterConfigured to
exportNAACCR
HL7Messages
Path Reportsin NAACCRDelimited
Layout
Optional Simultaneous Transmissionto Hospital Registry

Path Lab E-Path Path Lab E-Path TransmissionsTransmissions

Registry E-Path Registry E-Path ReceivingReceiving

What’s In NAACCR What’s In NAACCR Volume V?Volume V?
Chapter 1: IntroductionChapter 1: Introduction Chapter 2: Implementation Guide Chapter 2: Implementation Guide
for Transmission of Laboratory-for Transmission of Laboratory-Based Reports to Cancer Registries Based Reports to Cancer Registries Using Version 2.3.1 of the HL7 Using Version 2.3.1 of the HL7 Standard ProtocolStandard Protocol
Chapter 3: Pipe-Delimited FormatChapter 3: Pipe-Delimited Format

Two Standard FormatsTwo Standard Formats Health Level Seven (HL7)Health Level Seven (HL7)
http://www.hl7.org/http://www.hl7.org/ Flexible and robust protocol widely utilized Flexible and robust protocol widely utilized
for electronic data transmissions by medical for electronic data transmissions by medical facilities and pathology Laboratoriesfacilities and pathology Laboratories
Pipe-Delimited FormatPipe-Delimited Format Less sophisticated (less technically Less sophisticated (less technically
challenging)challenging) Retained for legacy e-path reporting systemsRetained for legacy e-path reporting systems May be used alone or in conjunction with HL7May be used alone or in conjunction with HL7

NAACCR Volume V: Chapter 2NAACCR Volume V: Chapter 2HL7 Implementation GuideHL7 Implementation Guide
Based upon CDC’s infection disease reporting Based upon CDC’s infection disease reporting HL7 implementation guideHL7 implementation guide
Explicitly defines the HL7 format necessary to Explicitly defines the HL7 format necessary to transmit a pathology report to a cancer registrytransmit a pathology report to a cancer registry
Specifies how and where to place each Specifies how and where to place each pathology report data elementpathology report data element
Defines requirement status for each variableDefines requirement status for each variable RequiredRequired Required when availableRequired when available OptionalOptional
Provides examples throughoutProvides examples throughout

The HL7 StandardThe HL7 Standard
NAACCR Standard is for HL7 Version 2.3.1NAACCR Standard is for HL7 Version 2.3.1 American National Standards Institute (ANSI) American National Standards Institute (ANSI)
approved in 1999approved in 1999 HL7 Versions 2.4, 2.5 also approvedHL7 Versions 2.4, 2.5 also approved 2.3.1 still most commonly supported version2.3.1 still most commonly supported version HL7 Version 3.x radically different from 2.x HL7 Version 3.x radically different from 2.x
versionsversions Clinical Document Architecture (CDA) is appealingClinical Document Architecture (CDA) is appealing
XMLXML But, not yet widely supported by AP-LIS vendorsBut, not yet widely supported by AP-LIS vendors

HL7 Basics: ORU^R01 HL7 Basics: ORU^R01 Message TypeMessage Type
Lab result information is reported Lab result information is reported through Observational Results through Observational Results (Unsolicited) (ORU)/Event R01 messages(Unsolicited) (ORU)/Event R01 messages
Unsolicited messages are transmitted at Unsolicited messages are transmitted at will from the sender and do not require will from the sender and do not require an electronic request from the recipientan electronic request from the recipient
ORU^R01 messages are composed of ORU^R01 messages are composed of specifically defined HL7 segmentsspecifically defined HL7 segments

HL7 Basics: Delimited Data HL7 Basics: Delimited Data FieldsFields
HL7 messages are ASCII textHL7 messages are ASCII text All data fields in an HL7 message are All data fields in an HL7 message are
delimited by a specified separatordelimited by a specified separator The delimiter is defined at the The delimiter is defined at the
beginning of an HL7 messagebeginning of an HL7 message Usually the ‘|’ (pipe) characterUsually the ‘|’ (pipe) character
Field in each position is defined Field in each position is defined (MSH-1, MSH-2, MSH-3… MSH-21) (MSH-1, MSH-2, MSH-3… MSH-21)
MSH|^~\&|HLS|HITECK PATH LAB-ATLANTA^3D9328409^CLIA||STJ|20031124122230||ORU^R01|200311241222300023|P|2.3.1|||||||||2.0 <CR>

HL7 Basics: SegmentsHL7 Basics: Segments
Various HL7 segments carry categories of Various HL7 segments carry categories of informationinformation
Each segment type is identified by a three Each segment type is identified by a three character id at the beginning of the character id at the beginning of the segment such as MSH, PID, OBR, OBXsegment such as MSH, PID, OBR, OBX
Some segments can be repeated in a Some segments can be repeated in a messagemessage
Repeating segments are sequentially Repeating segments are sequentially numberednumberedOBX|1|TX|22637-3^FINAL DIAGNOSIS^LN^^DIAGNOSIS^L|1|LEFT
INGUINAL LYMPH NODE - GRANULOMATOUS LYMPHADENITIS||||||F<CR>OBX|2|TX|22637-3^FINAL DIAGNOSIS^LN^^DIAGNOSIS^L|1|/ljm <CR>OBX|3|TX|^^^^Clinical History^L|2|? lymphoma Quick Section||||||F<CR>

NAACCR HL7 E-Path NAACCR HL7 E-Path Message StructureMessage Structure
ORU - Unsolicited Observation Message (event R01)
ORU^R01Observational Results (Unsolicited) Section
MSH Message Header segment 2.6.1
PID Patient Identification segment 2.6.2
[{NK1}] Next-Of-Kin segment 2.6.2
[PV1] Patient Visit segment 2.6.2
{
[ORC] Order common segment 2.6.3
OBR Observations Report ID segment 2.6.3
{[NTE] } Notes and comments segment
2.6.4
{
[OBX] Observation/Result segment
2.6.4
{ [NTE] } Notes and comments segment
2.6.4
}
}

HL7 E-Path MSH, PID, NK1 HL7 E-Path MSH, PID, NK1 SegmentsSegments
Message Header (MSH) SegmentMessage Header (MSH) Segment Message Control/Routing InformationMessage Control/Routing Information
Sending facilitySending facility Date and time of transmissionDate and time of transmission
Patient Identification (PID) SegmentPatient Identification (PID) Segment Patient Identification and DemographicsPatient Identification and Demographics
Patient namePatient name SSNSSN GenderGender Birth DateBirth Date
Next of Kin/Associated Parties (NK1) Segment Next of Kin/Associated Parties (NK1) Segment (Optional)(Optional) Next of kinNext of kin Contact informationContact information

HL7 E-Path PV1, ORC, OBR HL7 E-Path PV1, ORC, OBR SegmentsSegments
Patient Visit (PV1) SegmentPatient Visit (PV1) Segment Provider informationProvider information
Attending physicianAttending physician Referring physicianReferring physician
Common Order (ORC) SegmentCommon Order (ORC) Segment Pathology order informationPathology order information
Ordering facilityOrdering facility Ordering facility addressOrdering facility address Ordering facility AHA numberOrdering facility AHA number
Observation Request (OBR) SegmentObservation Request (OBR) Segment Information specific to the pathology request/orderInformation specific to the pathology request/order
Type of report (i.e. final diagnosis, correction,…)Type of report (i.e. final diagnosis, correction,…) Date and time specimen receivedDate and time specimen received Pathologist interpreting the observationPathologist interpreting the observation

HL7 E-Path OBX SegmentHL7 E-Path OBX Segment
Observation/Result (OBX) SegmentObservation/Result (OBX) Segment Specific observation identifier (OBX-3)Specific observation identifier (OBX-3)
Identified by Logical Observation Identifiers Names and Identified by Logical Observation Identifiers Names and Codes (LOINC) or SNOMED CT CodesCodes (LOINC) or SNOMED CT Codes
Examples:Examples: Path-Final DiagnosisPath-Final Diagnosis Path-Gross PathologyPath-Gross Pathology
Specific observation (OBX-5)Specific observation (OBX-5) Examples:Examples:
Text of Gross PathologyText of Gross Pathology Text of the Final DiagnosisText of the Final Diagnosis
OBX Segment carries the results of the OBX Segment carries the results of the pathology report as blocks of textpathology report as blocks of text

HL7 E-Path NTE, FHS, FTS, HL7 E-Path NTE, FHS, FTS, BHS, BTS SegmentsBHS, BTS Segments
Notes and Comments (NTE) Segment Notes and Comments (NTE) Segment (Optional)(Optional) Comments from the laboratoryComments from the laboratory
When transmitting batches of HL7 When transmitting batches of HL7 messages using a file transfer protocol or messages using a file transfer protocol or offline via tape, diskettes or other mediaoffline via tape, diskettes or other media Batch Header (BHS) SegmentBatch Header (BHS) Segment Batch Trailer (BTS) SegmentBatch Trailer (BTS) Segment File Header (FHS) Segment (Optional)File Header (FHS) Segment (Optional) File Trailer (FTS) Segment (Optional)File Trailer (FTS) Segment (Optional)

Volume V HL7 Volume V HL7 Implementation Guide Implementation Guide Segment SpecificationsSegment Specifications
Each segment specification provides:Each segment specification provides: Attribute tableAttribute table An example segmentAn example segment Each segment field definitionEach segment field definition
NAACCR segments and fields are NAACCR segments and fields are “tightly” defined“tightly” defined

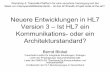
NAACCR OBX Attribute NAACCR OBX Attribute TableTableSeq Len DT Opt RP# Tbl# Item# Element Name NAACCR Item # NAACCR Opt
1 4 SI O 00569 Set ID-OBX R
2 3 ID C 0125 00570 Value type R
3 80 CE R 00571 Observation identifier*
7400, 7410, 7420, 7430, 7440, 7450, 7460, 7470
R
4 20 ST C 00572 Observation sub-ID O
5 655361 ** C Y2 00573 Observation value* R
6 60 CE O 00574 Units R*
7 60 ST O 00575 Reference ranges O
8 5 ID O Y/5 0078 00576 Abnormal flags O
9 5 NM O 00577 Probability O
10 2 ID O Y 0080 00578 Nature of abnormal test
O
11 1 ID R 0085 00579 Observation result status
7330 R*
12 26 TS O 00580 Date last Obs normal values
O
13 20 ST O 00581 User defined access checks
O
14 26 TS O 00582 Date/time of the observation
O
15 60 CE O 00583 Producer's ID O
16 80 XCN O Y 00584 Responsible observer O
17 60 CE O Y 00936 Observation method O

Excerpt from NAACCR OBX-Excerpt from NAACCR OBX-3 Field Definition3 Field Definition
OBX-3 Observation identifier (CE-590, Required) 00571Definition: This field contains a unique identifier for the observation. It identifies what is being reported in OBX-5 – for example, the specific test, or observation method, or component of the pathology report being reported. The CE data type transmits codes and the text associated with the code. This type has six components arranged in two groups as follows:
<identifier (ST)>^<text (ST)>^<name of coding system (ST)>^ <alternate identifier (ST)>^<alternate text (ST)> ^<name of alternate coding system (ST)>
CE data type components are defined as follows: (1)Identifier (ST). The code that uniquely identifies the item being referenced by the <text>. Different coding schemes will have different elements here.
(2) Text (ST). Name or description of the item in question. (1)Name of coding system (ST). Identifies the coding system used. The combination of the identifier and the name of the coding system components will be a unique code for a data item.
(4-6) Three components analogous to 1-3 for the alternate or local coding system. Note: This is the field and components that will contain the text, LOINC, or SNOMED CT codes for the following NAACCR items:
NAACCR Item Name LOINC Code
Path-Final Diagnosis 22637-3
Path-Text Diagnosis 33746-9
Path-Clinical History 22636-5
Path-Nature of Specimen 22633-2
Path-Gross Pathology 22634-0
Path-Micro Pathology 22635-7
Path-Comment Section 22638-1
Path-Suppl Reports 22639-9

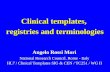
Report Identification
Patient Information
Institution: 3932 Chart/MRN: 00466144 Address 112 Broad Street
Pathology ID: 97 810430 SSN/SIN: Apartment 10
Report Date: 2003-11-24 Surname: SAMPLE30 City/Town: ATLANTA
Report Type: Correction Given Name: ALLEN State/Prov: GA
Requester ID: Sex: M Zip/Post Code:
30301
Requester: Date of Birth: 1953-06-21 Country: Procedure Date: 2003-09-22 Age: 47 (at procedure
date)
Surgeon ID: 163741 Insurer: USHC Surgeon: CHARLES,
HANNAHInsurance No: 3270686987
Pathologist ID: 109771 Race: Pathologist: MARTIN,
QUINCYEthnicity:
DIAGNOSIS LEFT INGUINAL LYMPH NODE - GRANULOMATOUS LYMPHADENITIS
jlm
Clinical History 47-year old white female with (L) UOQ breast mass Tissue Submitted Left inguinal node Gross Pathology: The specimen is received fresh labeled lymph node. The specimen
consists of two nodes 2.3 and 2.2. cm each. The cut surface is bulky tanto pink in colour and fleshy.
MQ/jlm
Sample Path ReportSample Path Report

Sample Path Report Page Sample Path Report Page 22Microscopic Sections of left inguinal lymph node demonstrated an encapsulated node
which is largely replaced by epithelioid granulomate without necrosis.Special stains do not reveal the presence of organisms. The backgroundlymphocytes are both B and T lymphocytes and include macrophages andoccasional neutrophils and plasma cells. Reed-Sternberg cells are notdemonstrated.
Supplements/Addenda Material was requested by Dr. D. Bannerly, Saint Joseph’s Hospital forreview.
A report from Dr. Patterson was received.
DIAGNOSIS: Consistent with peripheral T-cell lymphoma wilh epithelioidhistocytes (Lennert's lymphoma), see description and comment- lymph node, left inguinal (biopsy from November 24, 2003)
(See attached report).
/hmb
Tissue was submitted for lymph node protocol. A report from Dr. H.Perez, Chandler Health Science Center was received.DIAGNOSIS: (See attached report).LYMPH NODE; INGUINAL REGION, BIOPSY:NON-NECROTIZING GRANULOMATOUS LYMPHADENITIS.
/hmb
HITECK PATHOLOGY LABORATORY
ATLANTA, GA 30303
HTECK LABORATORY SYSTEMS, INC.

Corresponding NAACCR Corresponding NAACCR HL7 MessageHL7 Message
MSH|^~\&|HLS|HITECK PATH LAB-ATLANTA^3D9328409^CLIA||STJ|20031124122230||ORU^R01|200311241222300023|P|2.3.1 <CR>PID|1||97 810430^^^^PI^HITECK PATH LAB-ATLANTA &3D9328409&CLIA~00466144^^^^PT^ST JOSEPH’S&3932&CMA~3270686987^^^^PN^US HEALTHCARE||SAMPLE30^ALLAN||19530621|M|||112 BROAD STREET^APT 10^ATLANTA^GA^30301^ <CR>PV1|1||||||ATTENDINGID^ATTENDINGDR^MANAGING|REFERRINGID^REFERRER^FOLLOWUP^^^DR| <CR>ORC|RE||||||||||||||||||||ATLANTA CANCER SPECIALISTS|STREET ADDRESS 1^SUITE #^ATLANTA^GA^30303<CR>OBR|1||97810430|11529-5^SURGICAL PATH REPORT^LN^^PATHOLOGY REPORT^L|||20030922|||EMLOYEEID^PHLEBOTOMIST^PAMELA|||||164341^SURGEON^HANNAH^^^DR||||||||||F||||||||109772&PATHOLOGIST&QUINCY <CR>OBX|1|TX|22637-3^FINAL DIAGNOSIS^LN^^DIAGNOSIS^L|1|LEFT INGUINAL LYMPH NODE - GRANULOMATOUS LYMPHADENITIS||||||F<CR>OBX|2|TX|22637-3^FINAL DIAGNOSIS^LN^^DIAGNOSIS^L|1|/ljm <CR>OBX|3|TX|^^^^Clinical History^L|2|? lymphoma Quick Section||||||F<CR>OBX|4|TX|22633-2^Nature of Specimen^NS^^Tissue Submitted^L|3|Left inguinal node||||||F<CR>OBX|5|TX|22634-0^Gross Pathology^LN^^Gross Pathology^L|4|The specimen is received fresh labelled lymph node. The specimen consists of two nodes 2.3 and 2.2. cm each. The cut surface is bulky tan to pink in colour and fleshy.||||||F<CR>OBX|6|TX|22634-0^Gross Pathology^LN^^Gross Pathology^L|4|QP/jlm||||||F<CR>OBX|7|TX|11529-5^SURGICAL PATH^LN^^Microscopic^L|5|Sections of left inguinal lymph node demonstrated an encapsulated node which is largely replaced by epithelioid granulomata without necrosis. Special stains do not reveal the presence of organisms. The background lymphocytes are both B and T lymphocytes and include macrophages and occasional neutrophils and plasma cells. Reed-Sternberg cells are not demonstrated.||||||F<CR>OBX|8|TX|22639-9^Supplemental Reports/Addendum^LN^^Supplements/Addenda^L|6| Material was requested by Dr. D. Consult, Saint Joseph’s Hospital forreview. ||||||C<CR>OBX|9|TX|22639-9^Supplemental Reports/Addendum^LN^^Supplements/Addenda^L|6|A report from Dr. C. Darwin was received.||||||C<CR>OBX|10|TX|22639-9^Supplemental Reports/Addendum^LN^^Supplements/Addenda^L|6|DIAGNOSIS: Consistent with peripheral T-cell lymphoma wilh epithelioid histocytes (Lennert's lymphoma), see description and comment - lymph node, left inguinal (biopsy from November 24, 1997). (See attached report). /HMB||||||C<CR>OBX|11|TX|22639-9^Supplemental Reports/Addendum^LN^^Supplements/Addenda^L|6|Tissue was submitted for lymph node protocol. A report from Dr. B. Study, Sunnybrook Health Science Center was received.||||||C<CR>OBX|12|TX|^^^^Supplements/Addenda^L|7|DIAGNOSIS: (See attached report). LYMPH NODE; INGUINAL REGION, BIOPSY. NON-NECROTIZING GRANULOMATOUS LYMPHADENITIS. /hmb||||||C<CR>OBX|13|SN|21612-7^Reported PatientAge^LN^^Pat_age^L|1|^050|Y||||||F<CR>

NAACCR Volume V: NAACCR Volume V: Chapter 3Chapter 3
Pipe-Delimited FormatPipe-Delimited Format ASCII pipe (‘|’) delimited layoutASCII pipe (‘|’) delimited layout Defines 77 key data fieldsDefines 77 key data fields Similar look and feel as NAACCR Volume II Similar look and feel as NAACCR Volume II
(Registry Data Exchange Standard)(Registry Data Exchange Standard) Dictionary definition for each fieldDictionary definition for each field
Name, NAACCR Item #, max length, standard, field Name, NAACCR Item #, max length, standard, field positionposition
Includes a pipe-delimited/HL7 comparison Includes a pipe-delimited/HL7 comparison tabletable
Can be used alone or in conjunction with HL7 Can be used alone or in conjunction with HL7 messagesmessages
Simple but not as robust and flexible as HL7Simple but not as robust and flexible as HL7

Real World Experience with Real World Experience with NAACCR HL7 E-Path NAACCR HL7 E-Path
StandardStandard Labcorp has been working with CDC to Labcorp has been working with CDC to
implement NAACCR HL7 messages as implement NAACCR HL7 messages as part of a pilot project in 2005part of a pilot project in 2005
Initial feedback: Initial feedback: ““They felt it was a piece of cake”– Wendy They felt it was a piece of cake”– Wendy
Scharber, Federal ContractorScharber, Federal Contractor Difficulties encountered with required Difficulties encountered with required
when available (R*) fieldswhen available (R*) fields Otherwise, has been largely successfulOtherwise, has been largely successful

The Next Challenge: The Next Challenge: Encoded Synoptic Encoded Synoptic Pathology ReportsPathology Reports
College of American Pathologists (CAP) have College of American Pathologists (CAP) have defined standard Cancer Protocols and defined standard Cancer Protocols and Checklists for pathology reportsChecklists for pathology reports http://www.cap.org/http://www.cap.org/
Protocols and checklists are provided by SiteProtocols and checklists are provided by Site Breast, Colon and Rectum, Lung, Prostate, etc.Breast, Colon and Rectum, Lung, Prostate, etc.
Computerized checklists are being implemented Computerized checklists are being implemented by Laboratory Information System vendorsby Laboratory Information System vendors
Computerized, “synoptic” reports following CAP Computerized, “synoptic” reports following CAP protocols are represented by encoded data protocols are represented by encoded data elements instead of text blobselements instead of text blobs
NAACCR HL7 standard is being extended to NAACCR HL7 standard is being extended to accommodate synoptic pathology reportsaccommodate synoptic pathology reports

Progress Towards Synoptic Progress Towards Synoptic ReportingReporting
CDC/NPCR has sponsored two pilot CDC/NPCR has sponsored two pilot projects using synoptic reportsprojects using synoptic reports Reporting Pathology Protocols (RPP) Project IReporting Pathology Protocols (RPP) Project I
ColorectalColorectal RPP IIRPP II
Breast, Prostate, MelanomaBreast, Prostate, Melanoma Path reports transmitted with HL7Path reports transmitted with HL7
E-Path Transmission Work Group is E-Path Transmission Work Group is building upon efforts of the RPP projectsbuilding upon efforts of the RPP projects Face to face meeting in May began work on Face to face meeting in May began work on
LungLung

Continuing WorkContinuing Work
Revise Volume V with lessons Revise Volume V with lessons learned from real world learned from real world implementationsimplementations
Continue to expand support for Continue to expand support for synoptic reporting to include all CAP synoptic reporting to include all CAP Checklist sitesChecklist sites
Support for tissue bankingSupport for tissue banking Conformance testing toolsConformance testing tools

NAACCR HL7 Standard and NAACCR HL7 Standard and HL7 Pathology Special HL7 Pathology Special
Interest GroupInterest Group HL7 Path SIG chaired by John HL7 Path SIG chaired by John
Madden and John GilbertsonMadden and John Gilbertson Plan to recognize NAACCR 2.3.1 Plan to recognize NAACCR 2.3.1
standardstandard Moving forward with development of Moving forward with development of
a HL7 Version 3 CDA model to a HL7 Version 3 CDA model to facilitate other immediate needsfacilitate other immediate needs imagingimaging

Issues/Challenges with Issues/Challenges with NAACCR HL7 StandardNAACCR HL7 Standard
Less technical cancer registries may Less technical cancer registries may have difficulties implementing an HL7 have difficulties implementing an HL7 interfaceinterface
Path vendors may be slow to implement Path vendors may be slow to implement standardstandard
Defining a “standard” does not make it Defining a “standard” does not make it a standard that gets used!a standard that gets used!
NAACCR needs to “market” standardNAACCR needs to “market” standard HL7 Version 3 CDAHL7 Version 3 CDA

ConclusionsConclusions E-Path implementations between path labs E-Path implementations between path labs
and cancer registries will continue to expand and cancer registries will continue to expand at a rapid paceat a rapid pace
NAACCR HL7 standards will facilitate and NAACCR HL7 standards will facilitate and reduce implementation costsreduce implementation costs
As a result of standards based E-Path As a result of standards based E-Path reporting, opportunities for collaboration reporting, opportunities for collaboration between cancer registries and pathology between cancer registries and pathology research will growresearch will grow
Collaborations between pathology and cancer Collaborations between pathology and cancer registries has the potential to enhance the registries has the potential to enhance the data necessary for both interestsdata necessary for both interests

Contact InformationContact InformationEric B. Durbin, MSEric B. Durbin, MS
Director of Cancer InformaticsDirector of Cancer Informatics
Markey Cancer Control Program/Kentucky Cancer Markey Cancer Control Program/Kentucky Cancer RegistryRegistry
University of KentuckyUniversity of Kentucky
2365 Harrodsburg Rd, Ste A2302365 Harrodsburg Rd, Ste A230
Lexington, KY 40504-3381Lexington, KY 40504-3381
[email protected]@kcr.uky.edu
(859)219-0773 x223(859)219-0773 x223
http://www.kcr.uky.eduhttp://www.kcr.uky.edu