Hypercoagulability andDuration of Anticoagulation:How Long is Long Enough?
Kathryn Hassell, MDProfessor of Medicine
Division of HematologyUniversity of Colorado Denver

Disclosures
• No financial or other conflicts of interest
• Off label use: discussion not planned

Objectives
• Assist patients with decision-making about duration of anticoagulation by providing information about:– risk of recurrent venous thrombosis – risk of complications of therapy (bleeding)
• Decide if hypercoagulabile testing will be useful for a patient

24 year old man with unprovoked PE.No bleeding problems, negative hypercoag testing.
How long should he take anticoagulation?
• 3 months• 6 months• One year• Lifelong

19 year old woman with DVT while on OCPs for 3 years.No bleeding problems, Factor V Leiden positive.
How long should she take anticoagulation?
• 3 months• 6 months• One year• Lifelong

45 year old man with history of 2 clots, (calf, popliteal), each after arthroscopy. No bleeding, negative testingHow long should he take anticoagulation?
• 3 months• 6 months• One year• Lifelong

60 year old woman with history of PE on tamoxifen for metastatic breast cancer. No bleeding, no testing.
How long should she take anticoagulation?
• 3 months• 6 months• One year• Lifelong

64 year old man with history of PE after bladder cancer surgery 5 months ago. “Too much bleeding” to take anticoagulation after surgery, but in your office now.
How long should he start anticoagulation for his PE?If yes, for how long?
• 3 months• 6 months• One year• Lifelong

Outline of Presentation• Management of current VTE episode
– Duration of initial/acute therapy (e.g. LMWH)– Duration of subsequent/chronic therapy
• Based on time (e.g. 3 vs. 6 months)• Role of other factors (e.g. residual clot or symptoms)• Impact of hypercoagulable tests
• Prevention of subsequent new episodes– Balancing risk for recurrent clot vs. bleeding– Role of factors which may impact estimate of risk
• Review major basic principles along the way

Principle of Acute Treatment
• Anticoagulation given to reduce the risk of new thrombosis– Anticoagulation doesn’t actively change an acute
thrombus – endogenous thrombolysis occurs whether or not someone is on anticoagulation
– Anticoagulation simply prevents new thrombosis from forming
• In areas of recannalization• Extension beyond original

Treatment for Acute VTE
• Risk of no treatment for acute DVT or PE:– Untreated PE → fatal PE: 26% at 1 year– Untreated proximal DVT → fatal PE: 5% at 10 days,
10% at 30 days– No reduction in mortality with IVC filters
Young, Cochrane Database Sys Rev 17:CD006212, 2010
• Judged to be sufficiently high enough to create a standard to treat of all PE/proximal DVT (VTE) unless bleeding is likely to be life-threatening– Guidelines favor treatment of even calf DVT

Eighth ACCP 2012 – DVT or PE• Acute Management
– Subcutaneous LMWH
– Intravenous or subcutaneous UFH
– Fondaparinux
– Rivaroxaban, Apixaban (FDA approved after the guidelines were developed)

Eighth ACCP 2012 – DVT or PE• Other Management Considerations
– Initiation of VKA (warfarin) on first day (if using LMWH/heparin/fondaparinux)
– Continue LMWH/UFH until INR stable and ≥ 2.0 for at least 24 hours
– Treatment with LMWH/UFH for at least 5 days
– Switch to dabigatran after 5-10 days of LMWH

Initial Management of Thrombosis
• Acute intervention: 5 days of active therapy– Active antithrombotic therapy (e.g. heparin/LMWH/new
oral agents)– Initiation of long-term maintenance (e.g. warfarin/new
oral agents)
• Underlying thrombophilia does not impact selection or intensity of anticoagulation– Heparin OK for AT def– Warfarin OK for PC/PS deficiencies
Kearon, Current Opin Hematol 19:1, 2012

• VERY RARE– As likely related to acquired/transient protein C/S
deficiency as inherited state– Not a contraindication to initiate warfarin
• “Active” anticoagulation (e.g. heparin) protects against the initial further drop in levels with warfarin
Warfarin-Induced Skin Necrosis
Crowther, Arch Intern Med 159:46, 1999; Kearon, Current Opin Hematol 19:1, 2012

Management of Thrombosis
• Different INR intensity for APS? No
104 patients with APS (Finazzi, J Thromb Haemost 3:848, 2005) 2-3 >3
Recurrent thrombosis 5.5% 11.1% All bleeding 14.6% 27.8% Major bleeding 3.6% 5.3%
106 patients with APS (Crowther, NEJM 349:1133, 2003) 2-3 3-4 Recurrent thrombosis 3% 10.7% Per pt-yr 1.3% 4.1% Major bleeding 4 (19%) 3 (27%) Anticoagulation stopped 13 21
INR 2-3 is current standard

Duration of Treatment For A Given VTE Episode
• For DVT/PE, 3 months appears to be the minimum time needed – HR 1.52 (1.14-2.02) if treated only 1-1.5 months
vs. 3 months or longer Boutitie, BMJ 342;
d3036, 2011
• Up to 40% recurrence if anticoagulation interrupted during the first 3 months– 100-fold increase in peri-operative VTE risk if
interruption in the first monthKearon, NEJM
336:1506, 1997

Balancing Risks and Benefits
• Analysis of rate of fatal events and case fatality rates in the first 3 months on therapy
Event Rate of Fatal Event Case Fatality Rate
Fatal PE 0.4% (0.3-0.6) 11.3% (8.0-15.2)
Fatal bleed 0.2% (0.1-0.3) 11.3% (7.5-15.9)
Carrier, Ann Intern Med 152:578. 2010 Schulman, Sem Thromb Hemost 39:141, 2013

Principle: 3 Months of Time Not 3 Months of Anticoagulation
• Adequacy of anticoagulation doesn’t matter–Leiden Thrombophilia Study (2003)
– 234 patients followed for recurrence after stopping their anticoagulation
» Treated for 3, 6, or >6 months
– No increase in long-term recurrence risk for those who spent more time out of range
» No difference in recurrence risk based on duration of therapy, either
Gadisseur, J Thromb Hemostas 5:931, 2007

Are longer finite periods better?
• No evidence to indicate periods longer than 3 months is helpful to reduce risk of recurrence– Meta-analysis of 7 studies comparing 3, 6, 12, and
27 months showed no difference is subsequent recurrence after therapy stopped
– Included provoked, unprovoked, DVT and PE– Some authors cite “trend” to increased recurrence
after 3 vs. 6 months for unprovoked events:• HR 1.39 (0.96-2.01)
Boutitie, BMJ 342; d3036, 2011; de Jong, BJH 158:433, 2012

• Anticoagulation does not make the clot go away– Complete residual occlusion can be asymptomatic
• DVT doesn’t usually go away: e.g. DACUS Study
• After 3 months of therapy: 66.8% had residual vein thrombosis (RVT) >40% of vein diameter
• The rest could still have clot, just less
What if the clot isn’t gone?
Siragusa, Amer J Hematol 86:914, 2011

Residual Vein Thrombosis
• Conflicting evidence about the role of RVT predicting recurrence (more later)
• No evidence staying on anticoagulation will improve resolution of RVT– Sustaining anticoagulation because of RVT doesn’t
make it go away, doesn’t change outcomesPrandoni, Ann Intern Med 150:577,
2009

What if there’s still symptoms?
• May not be related to residual thrombus• Anticoagulation does not change the way the blood
flows; the blood is not “thinner”– Factors are still present, they simply lack carboxyl
groups (due to warfarin) or are bound by drug when activated (heparin/LMWH/new oral anticoagulants)
– Remember, anticoagulation doesn’t promote resolution of thrombosis
• The symptoms will not worsen off anticoagulation unless new clot forms

Post-Thrombotic Symptoms• Rate of chronic PTS symptoms ~25% de Jong, BJH, 2012
• Use of compression stockings: S.O.X. Trial– Randomized controlled comparison of graded compression
stocking to placebo stockings (no significant pressure applied)
– Started within a mean of 4 days, used up to 2 years– 80% of subjects used more than 3 days/week– No SAEs related to either stocking
• 2% had leg rash/itching
Kahn, Lancet 383(9920):880, 2014

Post-Thrombotic Symptoms• No difference between stockings in moderate/severe
PTS (14-16%), ulceration (3-4%), recurrent VTE
Kahn, Lancet 383(9920):880, 2014

Principles (But No Data)
• Some people choose to sustain anticoagulation hoping for:– Continued recannulization/resorption of clot– Symptom improvement with recannulization and/or
collateral formation• Role of anticoagulation: prevent new thrombosis
from “undoing” the gains made; NOT active therapy• Duration individualized: continued until desired
improvement attained or the “best it’ll be”

What if they havea hypercoagulable state?
• They HAVE a hypercoagulable state, as demonstrated by their episode of thrombosis
– Most people don’t ever clot (1:1000)
– Most people don’t clot even when faced with prothrombotic risk factors
– Some people who clot with prothrombotic risk factors may not even know they had a clot
• Does it matter if we give it a name?

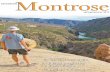
An Example: Orthopedic Surgery• Even without anticoagulation, only a subset clot, and
fewer have symptoms – those who do are different
0 20 40 60 80 100
Hip Fracture
TKA
THA
Arthroscopy
Distal DVT Proximal DVT PE
6th ACCP Conf on Antithrombotic and ThrombolyticTherapy; Chest, 2001

TEST ABNORMAL RESULTFactor V Leiden (FVL) PresentProthrombin G20210A mutation (PGM) PresentProtein C*/Antithrombin activity* Low (<30-40%/<50%)Protein S free antigen* Low (<30-40%)Anticardiolipin antibodies Mod-High Positive2glyoprotein-1 antibodies Mod-High PositiveLupus anticoagulant (e.g. dRVVT) PresentHomocysteine >ULN (12-15)
Testing for Thrombophilia
*should not be measured during acute event and/or on anticoagulation
INH
ERIT
EDAC
QU
IRED

Testing for Thrombophilia: Pitfalls
• Sensitive activity assays (Protein C/Protein S) – Affected by oral contraceptive use, inflammation,
antiphospholipid antibodies – Values of 50-60% of unclear clinical significance
• Protein S testing: low values (<40%) expected during pregnancy, may take weeks to months to recover post-partum
• Antiphospholipid antibodies may be reactive• Always repeat abnormal values to confirm
Favaloro, Sem Thromb Haemost 35:695, 2009

Optimal Timing of Testing
• No active thrombosis – consumes factors• No anticoagulants
– AT low with heparin/LMWH/fondaparinux therapy– PC/PS low with warfarin therapy, dabigatran
• If patient unsure about stopping anticoagulation, can do testing on warfarin (except Protein C/S)

Negative Thrombophilia Testing
• We can detect 7 conditions, but most people with clots don’t have these conditions– Example: RVT study of unprovoked VTE
• 1.7% had PC/PS/AT def or LA• 21% had FVL and/or PGM, which have minimal
impact on risk of recurrence• “Normal panel” doesn’t change the history of
clotting or risk estimate of recurrence
Prandoni, Ann Intern Med, 2009

Role of Positive Thrombophilia Testing to Predict Recurrence
• Modest or no effect from known inherited thrombophilias – FVL: OR=1.39 (1.15-1.67) PGM: OR=1.20 (0.89-1.61)
Marchiori, Haematologica 92:1250, 2008
– PC/PS/AT deficiencies: HR=1.8 (0.9-3.7) Christiansen, JAMA 293:2352, 2008
– Exceptions may be antithrombin deficiency, homozygotes for FVL or PGM but limited data
• Stronger effect likely with antiphospholipid antibody syndrome (OR=4.0 [1.2-13]) for unprovoked VTE
Kearon, Clin Chest Med 31:719, 2010

Effect of Inherited Thrombophilias on VTE Recurrence
• 304 patients with single VTE + family hx
Patients On anticoagulation %/year (n=124)
Off anticoagulation %/year (n=180)
Males Females
All 1.1% 9.6% 2.8%PC def 0.6% 10.8% 2.9%PS def 0.6% 10.5% 3.1%AT def 2.7% 11.6% 9.5%FVL 0% 7.2% 2.2%Multiple 0.9% 10.7% 2.1%
Vossen, Arterioscler Thromb Vasc Biol 25:1992; 2005

High Risk APS Patients• “High risk” laboratory findings (inconsistent data):
– Lupus anticoagulant > other tests– Anticardiolipin IgG/IgM >40 or >99th %ile– β2glycoprotein-1 IgG/IgM >99th %ile
• Clinical features which may predict thrombosis– Other thrombotic risk factors (e.g. OCP use)– Co-existent autoimmune disease– Suspected but unproven (retrospective, conflicting data)
• ITP, valvular lesions, history of obstetrical complications, livedo rectiularis
Barbhaiya and Erkan, Curr Opin Rheum 13:59, 2011

• Risk factors for thrombosis:– History
• previous thrombosis: 5.4% per pt-yr• asymptomatic: 0.95% per pt-yr
– ACA level• >40 GPL: 6.12% per pt-yr• <40 GPL: 1.25% per pt-yr
– Having SLE/SLE-like disease
Finazzi, Am J Med, 100:530, 1996
Recurrence Risk in APS

Principles Based on Available Hypercoagulable Testing
• Most testing doesn’t matter – negative not useful• What might indicate higher risk or recurrence off
anticoagulation?– Male with family history and named condition
• Annual risk 5-10%/year
– Antithrombin deficiency and family history• Annual risk 9-10%/year
– Antiphospholipid antibody syndrome• Annual risk 5-6%/year

Principle for Continuing After 3 Months
• Role of anticoagulation shifts to prevention of new episodes
• Individual’s assessment of relative risks– Risk (fear) of new thrombosis outweighs risk (fear)
and inconveniences of therapy

Best Predictor of Recurrence: Circumstances Around First Event
• Unprovoked events, independent of testing:– 10-15% recurrence in first 2 years after stopping
warfarin, then 2-3%/year thereafter Ridker, NEJM 348:1425, 2003
– Cumulative risk at 2-5 years 25%, 10 years 30-40% Donadini, J Thromb Thrombolysis, 31:301, 2011
• Risk of PE (vs. DVT) as the next event– 60-70% if first event was PE– 20% if first event was DVT
Agnelli, J Thromb Haemost 25:37, 2008

Recurrence Risk on Placebo• 9% at one year after stopping anticoagulation
Apixaban (AMPLY-Ext) study of unprovoked VTE
Agnelli, NEJM 2013

Recurrence Risk on Placebo• 10% recurrence in first year after discontinuation
(EINSTEIN-EXT)
NEJM 363:2499, 2010

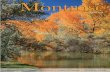
Prediction of VTE Recurrence Risk:Unprovoked vs. Provoked
• Prandoni, Haematologica 92:199, 2007
Unprovoked:~20% at 2 years~50% at 10 years
Provoked:~10% at 2 years~20% at 10 years

Prediction of VTE Recurrence Risk
• Risk varies with triggering event:Idiopathic 3.0-10%/yearVenous insufficiency 5.5%/yearTravel-relatedImmobilizationInfection
3.0-4.2%/year
EstrogensTrauma 1.5-4.2%/year
Postoperative 0.7%/year
Schulman, J Thromb Haemost 4:734, 2006; Iorio, Arch Intern Med 170:1710, 2010

Travel-Related Thrombosis
• Only with flights (no other modalities)• Background risk
– 1.1 events/million person-days overall– 27 clinical VTE/1 million travelers within 14 days– Symptomatic PE “unheard of” in flights <6 hrs– Biggest relative risk in flights >8 hrs (>12 hrs)
• OR 3.6 if clinical VTE risk factors– Mostly asymptomatic calf clot by imaging (1-2%)– Risk of PE up to 4/million if >12 hour flight
Philbrick, JGIM 22:107. 2007; Kahn, Chest 141 (2)(Suppl):e195, 2012

Principle:Lower Risk After Provoked Events
• Assumes risk factor was transient– Persistent malignancy associated with 20+% risk of
recurrence in first year if anticoagulation stoppedde Jong, BJH 158:433,
2012
– Re-use of estrogen-based OCPs after stopping anticoagulation associated with 8-fold risk of recurrence
• Transdermal estrogen and progesterone-only NOT associated with increase risk compared to nonusers
• Risk of recurrence in non-users: 5% in first yearVaillant-Roussel, Contracception 84:e23,
2011

Risk of Venous Thrombosis Increases with Age
AGE
RISK
OF
THRO
MBO
SIS
<1:50,000
1:700
1:200
50 y.o. 80 y.o.
1:25,000 1:2500
Naess, J Thromb Haemost 5:692, 2007; White, Circ 107:1, 2003
Overall risk = 1-2 in 1000/year

Am I in the Recurrence Group?• Markers of propensity for recurrence
– Elevated factor VIII activity (especially if >200%)• May double the risk of recurrence
– Elevation of other factors (IX, XI) may be weak predictors of recurrence
• Current areas of interest:– D-dimer– Residual vein thrombosis

Role of D-Dimer in Predicting VTE Recurrence
• Elevation in D-dimer does not indicate the presence of an acute thrombosis– The only diagnostic value is a negative result which
rules out an acute thrombosis Wells, J Thromb Haemost 5 Suppl
1:41, 2007
• However, measurement of D-dimer at least one month off anticoagulation may risk-stratify– Negative D-dimer: 3.5%/year– Positive D-dimer: 8.9%/year
Verhovsek, Ann Intern Med 149:481, 2008
• Which kit? What is “positive”? Age adjusted?

Role of Residual Vein Thrombosis (RVT) in Predicting VTE Recurrence
• Inconsistent association of RVT with increased risk of recurrent VTE– 4 studies suggest increase risk of ~2-fold– 5 studies failed to find an association
• If there is an association, it likely represents a systemic biological - not mechanical - phenomenon– 40-50% of recurrent events are on the opposite leg
• Difficult to standardize (definition, technique)
Kearon, Clin Chest Med 31:719, 2010

Combination of Stratifying Factors• PROLONG: utilization of RVT and/or D-dimer to
guide anticoagulation– 619 subjects with first proximal DVT or PE treated
with anticoagulation for at least 3 months– D-dimer measured 30 days after discontinuation
• Normal D-dimer (n=310): no further anticoagulation• Abnormal D-dimer: randomized
– No further anticoagulation (n=99)– Resume anticoagulation for 18 months (n=81)
– Residual vein thrombosis assessed (as per previous study e.g. 2 mm in common femoral/popliteal vein)
Cosmi, Eur J Endovasc Surg 39:356, 2010

Use of Stratifying Factors• Impact on recurrence:
– D-dimer if anticoagulation discontinued: • Normal: 10% (5.5/100 pt-yrs)• Abnormal: 19% (12/100 pt-yrs) HR=2.1
– RVT: no difference: 11% with vs. 13% without
Cosmi, Eur J Endovasc Surg 39:356, 2010

Bottom Line Principle
• If there were no clear precipitating factors, the likelihood of recurrence VTE is ~20-25% at 2 years, ~50% at 10 years– Comparable to having APS, AT deficiency, or a male with a
family history and some other defined states– Likely similar for people with persistent recognized risk
factors (e.g. cancer)
• The weaker the “precipitating factor”, the higher the risk of recurrence
• D-dimer might discern lower (higher?) risk group

Recurrence Risk on Anticoagulation• Risk of recurrence on warfarin therapy
– Goal INR 2-3: <1%/year– Goal INR 1.5-2.0: 2-2.5%/year
• Risk of recurrence 1-2% over 2 years in studies of extended prophylaxis of new oral anticoagulants
• Risk of recurrence on ASA: 5-7%/year– Same as placebo in one study, better in another and in
meta-analysis (HR ~0.6)
Ridker, NEJM 348:1425, 2003; Kearon, NEJM 349:631, 2003 Agnelli, NEJM 368:699, 2013; Brighton, NEJM 367:1979, 2012
Becattini, NEJM 366:1959, 2012

Bleeding Risk of Long-Term Anticoagulation
• Major bleeding: 0.9-1.4%/year – Risk increases with age (e.g. lower in young people)– May be slightly lower with new oral agents 0.6-1.0%
• Annual long-term fatality estimates
Schulman, Semin Thromb Hemost 39:141, 2013
Event Rate of Fatal Event Case Fatality RateFatal PE (without tx) 0.49% (0.36-0.64) 9.0% (6.8-11.8)
Fatal bleed (with tx) 0.63% (0.61-0.65) 9.1% (2.5-21.7)

Principles Regarding Bleeding
• Anticoagulation doesn’t cause bleeding– Bleeding occurs when a vessel ruptures– Anticoagulation doesn’t weaken vessels
– \
• Risk of major bleeding, including intracranial, does not correlate with history of falls
Donze, Am J Med 125:773, 2012
Outcome Placebo Apixaban 2.5 mg po bid
Apixaban 5.0 mg po bid
Bleeding 22 (2.7%) 27 (3.5%) 35 (4.3%) Major 4 (0.5%) 2 (0.2%) 1 (0.1%)
Agnelli, ASH, 2012

Bleeding Prediction Rules• Systematic review and performance analysis
– RIETE, HAS-BLED, mOBRI use similar factors• Age (>65-75), renal/liver disease, history of bleeding,
anemia, hypertension, use of anti-plt agents, alcohol
– Studies often in atrial fibrillation (RIETE in VTE)
– None with sufficient predictive power to distinguish risk groups
• Low RIETE score may predict a very-low bleeding riskLoewen and Dahri, Amer J Hematol 90:1191,
2011

50
ME PT #1PREGNANCY
PREGNANCY
0 100
PT #2
LONG-HAUL FLIGHT (?)
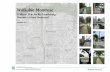
“Clot-ability Scale”: A Conceptual ModelAGE
Everyone has number(inherited/acquired)
We just can’t measure it!
WARFARIN
WARFARIN
WARFARINANTICOAGULATION
ClinicalClotting
ClinicalBleeding

Duration of Anticoagulation:ACCP 2012
• Minimum: 3 months for DVT or PE– Provoked by transient risk factor = sufficient– Unprovoked: favor “extended” over 3 months
• If bleeding risk is moderate or high, favor 3 months over longer, even if 2nd unprovoked event
• If “extended”, annual risk assessment of risk/benefit
Kearon, Chest 141:e419S, 2012

What if they have more than one clot?
• No evidence recurrent provoked events are worse than a single provoked event– Risk estimate of recurrence is the likely same
• Some data for multiple unprovoked events
Adapted from Schulman, Am J Med 104:332, 1998
First unprovoked
event, treated for 6 months (n=412)
Second unprovoked
event14%
6 months
Indefinite 3% recurrence
2.5 years of follow-up
30% recurrence

Duration: A Review of Principles
• Anticoagulation does not make clot go away or the blood to flow better
• The body appears to need 3 months to “stabilize” the situation (time, not days on drug)
• No evidence that more than 3 months is better, but could reason that some might need more time to “heal” before potentially have new clots occur
• A decision to continue otherwise based on more concern about new clotting than bleeding

Deciding on Extended Anticoagulation
• Current literature endorses “acceptable risk” of recurrence of up to 5%/1 year or 15%/5 years
Kearon, J Thromb Heamost 8:2313, 2012
• Individual should decide what level of risk is OK:– Risk of recurrence clotting based on analysis of the
initial clotting event• If unprovoked, risk is 25% at 2 years, 50% at 10 years• Testing usually doesn’t help, D-dimer might
– Anticoagulation doesn’t cause bleeding, but unlucky if you have major bleeding while you’re on it, because it might be worse (0.5-2%/year)

How close to the edge you are on any given day is likely determined by many factors (age, genetics, comorbidities)
Pushes off the edge:e.g. surgery
The closer to the edge you are, the less it takes to push you off
Anticoagulation
Normal Risk1-2 : 1000
Risk OneConceptual
Model

24 year old man with unprovoked PE.No bleeding problems, negative hypercoag testing.
How long should he take anticoagulation?
• 3 months• 6 months• One year• Indefinite

19 year old woman with DVT while on OCPs for 3 years.No bleeding problems, Factor V Leiden positive.
How long should she take anticoagulation?
• 3 months• 6 months• One year• Indefinite

45 year old man with history of 2 clots, (calf, popliteal), each after arthroscopy. No bleeding, negative testingHow long should he take anticoagulation?
• 3 months• 6 months• One year• Indefinite

60 year old woman with history of PE on tamoxifen for metastatic breast cancer. No bleeding, no testing.
How long should she take anticoagulation?
• 3 months• 6 months• One year• Indefinite

64 year old man with history of PE after bladder cancer surgery 5 months ago. “Too much bleeding” to take anticoagulation after surgery, but in your office now.
How long should he start anticoagulation for his PE?If yes, for how long?
• 3 months• 6 months• One year• Lifelong

The “True” Right Answers?
Anticoagulation should be given for as long as the person feels the risks of having a new blood clot are higher or more worrisome than the risks/inconveniences of the therapy.